Management of complications of cirrhosis in patients awaiting liver transplantation
10
Management of complications of cirrhosis in patients awaiting liver transplantation Andres Cardenas, Pere Gine `s * Liver Unit, Institut de Malalties Digestives, Hospital Clinic, IDIBAPS, University of Barcelona, Villaroel 170, 08036 Barcelona, Spain 1. Introduction Up to the late 1970’s patients with decompensated cirrhosis in form of ascites, hepatorenal syndrome (HRS), hepatic encephalopathy (HE), spontaneous bacterial perito- nitis (SBP), gastroesophageal variceal bleeding and/or hepatocellular carcinoma had a grim prognosis and therapy was mainly symptomatic and palliative. Introduction of orthotopic liver transplantation (OLT) more than 20 years ago as an established therapy for decompensated liver disease significantly changed the outcome of patients with advanced cirrhosis [1]. Although OLT was a major step in management of decompensated cirrhosis, it took at least a decade to realize that influencing the pre-transplant status of patients would translate into better post-transplant outcomes [2,3]. Since listing criteria for OLT in cirrhosis include complications such as ascites, HRS, variceal bleeding, hepatic encephalopathy, SBP, among others, optimal therapy of these is warranted in order to assure that patients reach OLT and have a good post-transplant outcome. The goals of pre-operative care include the appropriate manage- ment of decompensated liver disease with interventions such as diuretics for ascites, antibiotic prophylaxis against SBP, the use of beta-blockers or banding for the primary or secondary prophylaxis of variceal bleeding, endoscopic variceal banding plus vasoconstrictors for active variceal bleeding, use of oral synthetic disaccharides such as lactulose to prevent recurrences of hepatic encephalopathy, therapeutic paracentesis with albumin for refractory ascites and vasoconstrictors with albumin for HRS. Because the complications of cirrhosis can be life threatening, a patient’s clinical status while listed must be assessed very frequently. Standard medical care of these patients should include screening for colorectal, prostate, breast, and cervical cancer. Smoking cessation is of key importance. If the patient has a history of alcoholism proper measures to ensure abstinence such as an alcohol rehabilitation program must be offered. In addition patients should be vaccinated against hepatitis A and B. This article will focus on the management of ascites, dilutional hyponatremia, HRS, SBP, hepatic encephalopathy, and variceal bleeding in patients awaiting OLT. Hepatocellular carcinoma, commonly encountered in compensated and decompensated cirrhotics should also be managed aggressively, however, this topic is beyond the scope of this review and has been recently reviewed elsewhere [4]. 2. Ascites Ascites is the most common complication of cirrhosis and is associated with 50% mortality at 2 years if patients do not receive OLT [5,6]. It is one of the most frequent reasons for referral for evaluation of OLT in the United States and Europe [7,8]. Ascites in cirrhosis is the first manifestation of the kidney’s inability to handle sodium which occurs mainly due to activation of sodium retaining factors as a consequence of a homeostatic response to arterial under- filling [9]. Recently the International Ascites Club defined ascites into three groups: in Grade 1 ascites fluid is detected only by ultrasound; in Grade 2, ascites is moderate with symmetrical distention of the abdomen; and in Grade 3 ascites is large or tense with marked abdominal distention [10]. The evaluation of patients with ascites involves several steps, but the most important is a diagnostic paracentesis and abdominal ultrasound. Diagnostic paracentesis is required in all patients listed for transplantation requiring hospitalization and those with any evidence of clinical deterioration such as fever, abdominal pain, gastrointestinal bleeding, hepatic encephalopathy, or hypotension [11]. Tests that need to be ordered are cell count, culture in blood Journal of Hepatology 42 (2005) S124–S133 www.elsevier.com/locate/jhep 0168-8278/$30.00 q 2004 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.jhep.2004.12.007 * Corresponding author. Tel.: C34 93 227 5499; fax: C34 93 451 5522. E-mail address: [email protected] (P. Gine `s).
-
Upload
andres-cardenas -
Category
Documents
-
view
216 -
download
1
Transcript of Management of complications of cirrhosis in patients awaiting liver transplantation

Management of complications of cirrhosis in patientsawaiting liver transplantation
Andres Cardenas, Pere Gines*
Liver Unit, Institut de Malalties Digestives, Hospital Clinic, IDIBAPS, University of Barcelona, Villaroel 170, 08036 Barcelona, Spain
1. Introduction
Up to the late 1970’s patients with decompensated
cirrhosis in form of ascites, hepatorenal syndrome (HRS),
hepatic encephalopathy (HE), spontaneous bacterial perito-
nitis (SBP), gastroesophageal variceal bleeding and/or
hepatocellular carcinoma had a grim prognosis and therapy
was mainly symptomatic and palliative. Introduction of
orthotopic liver transplantation (OLT) more than 20 years
ago as an established therapy for decompensated liver
disease significantly changed the outcome of patients with
advanced cirrhosis [1]. Although OLT was a major step in
management of decompensated cirrhosis, it took at least a
decade to realize that influencing the pre-transplant status of
patients would translate into better post-transplant outcomes
[2,3]. Since listing criteria for OLT in cirrhosis include
complications such as ascites, HRS, variceal bleeding,
hepatic encephalopathy, SBP, among others, optimal
therapy of these is warranted in order to assure that patients
reach OLT and have a good post-transplant outcome. The
goals of pre-operative care include the appropriate manage-
ment of decompensated liver disease with interventions
such as diuretics for ascites, antibiotic prophylaxis against
SBP, the use of beta-blockers or banding for the primary or
secondary prophylaxis of variceal bleeding, endoscopic
variceal banding plus vasoconstrictors for active variceal
bleeding, use of oral synthetic disaccharides such as
lactulose to prevent recurrences of hepatic encephalopathy,
therapeutic paracentesis with albumin for refractory ascites
and vasoconstrictors with albumin for HRS. Because the
complications of cirrhosis can be life threatening, a patient’s
clinical status while listed must be assessed very frequently.
Standard medical care of these patients should include
screening for colorectal, prostate, breast, and cervical
0168-8278/$30.00 q 2004 European Association for the Study of the Liver. Pub
doi:10.1016/j.jhep.2004.12.007
* Corresponding author. Tel.: C34 93 227 5499; fax: C34 93 451 5522.
E-mail address: [email protected] (P. Gines).
cancer. Smoking cessation is of key importance. If the
patient has a history of alcoholism proper measures to
ensure abstinence such as an alcohol rehabilitation program
must be offered. In addition patients should be vaccinated
against hepatitis A and B. This article will focus on the
management of ascites, dilutional hyponatremia, HRS, SBP,
hepatic encephalopathy, and variceal bleeding in patients
awaiting OLT. Hepatocellular carcinoma, commonly
encountered in compensated and decompensated cirrhotics
should also be managed aggressively, however, this topic is
beyond the scope of this review and has been recently
reviewed elsewhere [4].
2. Ascites
Ascites is the most common complication of cirrhosis
and is associated with 50% mortality at 2 years if patients do
not receive OLT [5,6]. It is one of the most frequent reasons
for referral for evaluation of OLT in the United States and
Europe [7,8]. Ascites in cirrhosis is the first manifestation of
the kidney’s inability to handle sodium which occurs mainly
due to activation of sodium retaining factors as a
consequence of a homeostatic response to arterial under-
filling [9]. Recently the International Ascites Club defined
ascites into three groups: in Grade 1 ascites fluid is detected
only by ultrasound; in Grade 2, ascites is moderate with
symmetrical distention of the abdomen; and in Grade 3
ascites is large or tense with marked abdominal distention
[10]. The evaluation of patients with ascites involves several
steps, but the most important is a diagnostic paracentesis
and abdominal ultrasound. Diagnostic paracentesis is
required in all patients listed for transplantation requiring
hospitalization and those with any evidence of clinical
deterioration such as fever, abdominal pain, gastrointestinal
bleeding, hepatic encephalopathy, or hypotension [11].
Tests that need to be ordered are cell count, culture in blood
Journal of Hepatology 42 (2005) S124–S133
www.elsevier.com/locate/jhep
lished by Elsevier B.V. All rights reserved.

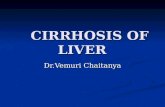
Fig. 1. Treatment strategies for Grade 2 and 3 ascites. Low sodium diet
is recommended with 70–90 mmol/day. Recommended diuretics
include spironolactone (50–200 mg/day) or amiloride (5–10 mg/day).
Low doses of furosemide (20–40 mg/day) may be added to increase
natriuresis in patients with peripheral edema. Albumin replacement is
8 g per liter tapped. Diuretics may be increased every week up to
400 mg/day of spironolactone and 160 mg/day of furosemide if there is
no response. [This figure appears in colour on the web.]
A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133 S125
culture bottles (10 mL of fluid injected at the bedside),
albumin, and total protein. The difference between the
serum albumin concentration and ascites albumin concen-
tration (serum-ascites albumin gradient) in patients with
cirrhosis and ascites is usually greater than 1.1 g/dL [12].
Abdominal ultrasonography in patients with ascites de novo
or already listed is important in order to rule out
hepatocellular carcinoma and/or portal vein thrombosis.
The importance of treating ascites properly relates to an
overall better outcome in the pre-transplant phase by
decreasing the risk of SBP, hospital admissions and
providing a better quality of life for the patient.
2.1. Management
The mainstay of therapy is implementation of a low
sodium diet with 70–90 mmol/day (approximately 1.5–
2 gr of salt/day) as well as diuretics. A nutritionist is very
helpful in these cases. Grade 1 ascites does not need to be
treated, but it is advisable that these patients refrain from
excessive salt intake as this can lead to positive sodium
balance and fluid retention. Diuretics are indicated for all
those patients with Grade 2 ascites. The best initial
regimen is either spironolactone (50–200 mg/day)
or amiloride (5–10 mg/day). Low doses of furosemide
(20–40 mg/day) may be useful in the beginning (particu-
larly in patients with peripheral edema or anasarca) [13].
The goal in these patients is to achieve a reasonable
weight loss of 0.5 kg/day until no ascites or edema is
clinically present. Patients with Grade 3 ascites are best
managed by total paracentesis with albumin adminis-
tration (8 g per liter of fluid removed) after the tap in
order to prevent the post-paracentesis circulatory dysfunc-
tion [13,14]. This option is safe, effective, has signifi-
cantly less side effects than diuretics and gets patients out
of the hospital fast. Albumin is better than other plasma
expanders (dextran-70, polygeline, and saline) for large-
volume paracentesis greater than 5 L [15,16]. Since many
of these patients have marked sodium retention they need
to be started or continued on relatively high doses of
diuretics after paracentesis together with a low sodium
diet (Fig. 1).
About 10% of patients with ascites are refractory to
treatment with diuretics [10]. In refractory ascites, patients
do not respond to highest doses of diuretics (spironolactone
400 mg/day and furosemide 160 mg/day) or develop side
effects (hyperkalemia, hyponatremia, hepatic encephalo-
pathy, or renal failure) that prohibit their use. Patients may
be treated either by repeated large-volume paracentesis plus
albumin or transjugular intrahepatic portosystemic shunts
(TIPS). Therapeutic paracentesis is the most accepted
initial treatment and patients, on average, require a tap
every 2–4 weeks. The majority may be treated as
outpatients, making this option easy to perform and
inexpensive. TIPS by reducing portal pressure decreases
ascites and its reaccumulation as well as diuretic
requirements. Although TIPS is very effective, it frequently
obstructs (70% in 1 year) and may cause hepatic
encephalopathy, congestive heart failure and hemolytic
anemia [10,17]. Newer polytetrafluoroethylene-covered
prostheses improve TIPS patency, decrease the number of
clinical relapses and reinterventions without increasing the
risk of encephalopathy [18]. Five clinical trials comparing
TIPS vs. repeated paracentesis in patients with refractory
ascites show that TIPS is associated with a lower rate of
ascites recurrence, but a higher rate of hepatic encephalo-
pathy compared with those of patients treated with
paracentesis and albumin [19–23]. There is also conflicting
evidence in regards to survival because some studies have
shown survival benefit with TIPS whereas others have not
shown any difference in survival. An important aspect to
consider when treating patients is cost. The price of treating
patients with refractory ascites with TIPS is much higher
than the cost of repeated paracentesis plus albumin [21].
Therefore, large-volume paracentesis appears to be the
treatment of choice because of its wider applicability, lower
cost and less side effects when compared to TIPS.
Additionally there is no strong evidence indicating that
TIPS improves either the likelihood of reaching liver
transplantation or post-transplantation outcome. TIPS can
be a good option for patients with preserved liver function
without hepatic encephalopathy, with loculated fluid, or
those unwilling to undergo frequent paracentesis (Fig. 2).
Finally the presence TIPS may create technical difficulties
for the surgeon at the time transplantation in some patients,
although this seems to be uncommon in high-volume and
experienced centers [24,25].

Fig. 2. Treatment strategy for patients with refractory ascites.
*Consider use of Transjugular intrahepatic portosystemic shunt
(TIPS) in patients with preserved hepatic function, no hepatic
encephalopathy, compartmentalized fluid, and those having repeated
paracentesis more than 3–4! per month. [This figure appears in
colour on the web.]
A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133S126
3. Dilutional hyponatremia
Dilutional hyponatremia in cirrhotic patients is defined as
serum sodium %130 mEq/L in the presence of an expanded
extracellular fluid volume, as indicated by the presence of
ascites and/or edema [26]. This complication of cirrhotic
patients with ascites has recently gained attention given that
several reports indicate that when serum sodium concen-
tration is combined with the Model for End-Stage liver
disease (MELD) it improves the prognostic accuracy of
MELD score in patients awaiting OLT [27–29]. Dilutional
hyponatrema occurs in 30–35% of hospitalized patients
with cirrhosis and ascites [30,31]. This type of hypona-
tremia is secondary to an impaired capacity of the kidneys to
excrete solute-free water due to non-osmotic hypersecretion
of arginine vasopressin (the antidiuretic hormone). Dilu-
tional hyponatremia must be distinguished from true
hyponatremia which commonly occurs in the setting of
volume depletion without ascites and edema due to
overdiuresis secondary to excessive diuretic use.
The clinical consequences of dilutional hyponatremia in
patients with cirrhosis are not completely understood and
are currently being assessed. Because serum sodium
concentration is the major determinant of the osmolality
in the extracellular fluid, the existence of dilutional
hyponatremia is associated with hypoosmolality of the
extracellular fluid. This hypoosmolality causes a shift of
water from the extracellular to the intracellular compart-
ment, which may theoretically affect cell function. It seems
that the major effect of dilutional hyponatremia occurs in
the brain. Brain cells of patients with cirrhosis and
hyponatremia have reduced intracellular content of some
organic osmolytes, particularly myo-inositol, which may
help to prevent the development of brain cell edema as a
consequence of passage of water from the extracellular to
the intracellular compartment [32]. These changes could
affect cell function and predispose to the development of
disturbances in neurological function. Preliminary studies
from our group suggest that dilutional hyponatremia is a
major predisposing factor to the development of hepatic
encephalopathy in patients with cirrhosis (P. Gines,
unpublished data). Further studies in this area are required
to establish this possible pathogenic relationship.
Other potential clinical consequences of dilutional
hyponatremia are the neurological complications that can
occur after a rapid correction of serum sodium levels. It has
been known for many years that in patients without liver
disease with hyponatremia of different etiologies the rapid
correction of hyponatremia may lead to the development
central pontine myelinolysis (CPM), a severe condition with
high mortality in which shrinkage of cerebral tissues leads
to demyelination of pontine and extrapontine neurons
causing seizures and coma [33]. Studies in small series of
patients and isolated reports have described the occurrence
of neurological complications, particularly CPM, in patients
with cirrhosis after OLT [34,35]. In most, if not all cases
CPM was associated with a rapid increase in serum sodium
levels after transplantation, exceeding 20 mEq/L or more
during a period of 24 h [34]. Therefore, every effort should
be made to avoid rapid increases in serum sodium
concentration in patients with cirrhosis transplanted with
low serum sodium levels. In the future, improvement of
serum sodium levels before transplantation with the use of
vasopressin receptor antagonists drugs may help prevent
significant fluctuations in serum sodium levels and sub-
sequent development of neurological complications post-
transplantation (see below).
3.1. Management
The first step in the management of dilutional hypona-
tremia is fluid restriction and discontinuation of diuretics.
Water restriction at 1000 mL/day helps prevent the
progressive decrease in serum sodium concentration but
usually does not correct hyponatremia in most cases [36].
Currently, several pharmaceutical companies are develop-
ing drugs that are active orally and act by selectively
antagonizing the specific receptors (V2 receptor) of arginine
vasopressin. These agents act in the distal collecting ducts of
the kidneys, by increasing solute-free water excretion and,
thus, improving serum sodium concentration in hypona-
tremic patients. Recent reports in patients with cirrhosis
and ascites indicate that these drugs are effective in
improving serum sodium concentration in hyponatremic
patients [36,37]. Large Phase II and III multicenter clinical
trials are currently being conducted in aims of learning more
about the efficacy and safety of these drugs. These
compounds if approved for clinical use could be useful in
managing decompensated cirrhotic patients listed for OLT.

Table 2
Prevention of hepatorenal syndrome
Clinical situation Intervention Comment
Spontaneous
bacterial
peritonitis [40]
Albumin (1.5 g/kg iv
at diagnosis of the
infection and 1 g/kg
after 2 days)
Reduces incidence of renal
failure from 30 to 10% and
improves survival from 29
to 10%
Alcoholic
hepatitis [41]
Oral pentoxifylline
400 mg p.o. t.i.d. for
1 month
Reduces the incidence of
HRS and mortality to 8
and 24%, respectively vs.
controls 35 and 46%,
respectively
A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133 S127
4. Hepatorenal syndrome
HRS is a functional renal failure without any identifiable
kidney pathology that occurs in about 10% of patients with
advanced cirrhosis [9,38]. The diagnosis of HRS is currently
made using criteria to exclude other causes of renal failure
that can occur in cirrhosis (Table 1). HRS is commonly seen
in patients awaiting OLT and remains one of the most
challenging complications of cirrhosis to manage given that
there are limited treatments. It may develop acutely or
subacutely. Type 1 HRS is an acute and rapidly progressive
form of renal failure (serum creatinine O2.5 mg/dL) that
may occur spontaneously or be precipitated by events such as
SBP, alcoholic hepatitis or large volume paracentesis
without albumin expansion. The expected survival of type
1 HRS is of only 2 weeks if not treated or transplanted [39]. In
type 2 HRS, renal failure is usually less severe (serum
creatinine 1.5–2.5 mg/dL) and shows little or no rapid
progression compared to that of type 1 HRS. Prevention of
HRS has been a major step improving care for patients listed
for OLT. There are two clinical situations in which HRS can
be prevented; SBP and alcoholic hepatitis [40,41] (Table 2).
4.1. Management
Although OLT is undoubtedly the best treatment for
HRS, successful pharmacological therapy prior to OLT is
equally important in assuring an optimal outcome similar to
that of patients without HRS. Systemic vasoconstrictors
with plasma expansion are the therapy of choice for HRS
now that several uncontrolled studies have confirmed a
beneficial role in HRS [42–51]. Vasoconstrictors are used
because the initial event in the pathogenesis of HRS is an
arterial splanchnic vasodilation causing activation of
endogenous vasoconstrictors systems with subsequent
renal vasoconstriction. Intravenous terlipressin along with
albumin as a plasma expander is associated with a
significant improvement of renal function and reduction of
serum creatinine to less than 1.5 mg/dL in approximately
60–75% of patients treated for at least 5 days [42–48]. With
this protocol, recurrence is uncommon. Unfortunately,
terlipressin is not available in many countries including
the United States and, therefore, other options such as alpha-
adrenergic agonists are a reasonable alternative given that
they are widely available. Midodrine, an alpha-adrenergic
Table 1
Diagnostic criteria of hepatorenal syndrome proposed by the
International Ascites Club [38]
1. Low glomerular filtration rate, as indicated by serum
creatinine greater than 1.5 mg/dl
2. Exclusion of shock, ongoing bacterial infection,
volume depletion and use of nephrotoxic drugs
3. No improvement in renal function despite stopping
diuretics and volume repletion with 1.5 L of saline
4. No proteinuria or ultrasonographic evidence of
obstructive uropathy or parenchymal renal disease
agonist in association with octreotide, a glucagon inhibitor,
and albumin has also proved efficatious in HRS [49,50].
Noradrenaline, another alpha agonist, in combination with
albumin expansion also improves renal function in HRS
[51]. The recommended doses and duration of vasocon-
strictor therapy are summarized in Fig. 3. In three studies,
patients that responded to therapy of HRS (decrease of
creatinine to !1.5 mg/dL) with terlipressin plus albumin
and octreotide, midodrine and albumin had an increased
survival compared to those that did not respond to this
therapy [43,44,50].
The primary goal of phamacological therapy is normal-
ization of renal function so that suitable transplant
candidates can undergo OLT with less morbidity and have
similar survival compared to that of patients without HRS.
A recent study from our Unit revealed that patients treated
sucessfully with vasopressin analogues and albumin before
OLT had a similar post-transplantation outcome and
survival similar to patients transplanted without HRS [52].
This study supports the concept that HRS should be treated
aggresively before OLT because improvements in renal
function are associated with better outcomes.
TIPS may improve renal function in HRS. In one recent
study of 14 patients with type 1 HRS treated with
midodrine, octreotide, and albumin, 10 had a good response
Fig. 3. Treatment strategy for patients with hepatorenal syndrome.
Terlipressin is widely used in Europe but is not available in many
countries including the United States. [This figure appears in colour on
the web.]

A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133S128
(serum creatinine remained stable at !1.5 mg/dL for 3
days) and were subsequently treated with TIPS if not
contraindicated by INR O2.0, serum bilirubin O5 mg/dL,
and a Child-Pugh score O12 [50]. Five patients underwent
TIPS with very good outcome with one of them successfully
receiving living donor OLT. Interestingly renal function
continued to improve and completely normalized in these
five patients. Of the five that responded to vasoconstrictors
and albumin but did not get TIPS, two underwent successful
OLT, but three died as a consequence of liver failure, sepsis
and arrhythmia. There was improved survival in all
responders, but the real impact of TIPS in improving
survival is difficult to assess given the low number of
patients treated.
4.2. Orthotopic liver transplantation for patients
with hepatorenal syndrome
OLT is the optimal treatment for suitable candidates
with HRS. Unfortunately, transplantation for HRS is
limited by the fact that many of these patients may die
before the operation due to prolonged waiting in the list in
most centers. Priority for OLT in the United States is
based on the MELD score which includes three variables;
bilirubin, serum creatinine and international normalized
ratio (INR) [53]. This scoring system is objective,
includes serum creatinine and predicts survival in
cirrhotics. The score ranges from 6 to 40. Its role in
predicting prognosis in patients with HRS has recently
been confirmed in our Unit in 105 cirrhotic patients with
HRS (P. Gines, unpublished results). Patients with type 1
HRS with a MELD score R20 showed an extremely poor
outcome with a median survival of 1 month and those
with type 2 HRS and a score !20 showed a slightly
better outcome with a median survival of 11 months,
while patients with type 2 HRS and a score O20 had an
intermediate outcome, with a median survival of three
months. In the whole group, the two independent
predictive factors of survival were MELD score and
type of HRS. Other centers outside the United States have
different allocation systems that give higher priority to
patients with HRS. Regardless of the system used for
organ allocation, patients with HRS must be appropriately
treated before transplantation. Since cyclosporine and
tacrolimus treatment may contribute to renal impairment
post-operatively, these drugs should not be given until
diuresis and improvement of renal function is observed,
usually in 3–4 days after transplantation.
5. Bacterial infections and spontaneous bacterial
peritonitis
Bacterial infections are one of the most feared problems
that complicate the course of patients with advanced liver
disease. It is estimated that they occur at admission or
during hospitalization in 20–60% of patients [54]. A recent
prospective study conducted in our Unit between 1998 and
2000 showed that among all admissions, bacterial infections
were present in 32% of cases either at entry or during
hospitalization [55]. Of these the majority were secondary
to SBP (24%), other common causes included urinary tract
infection, pneumonia and bacteremia secondary to invasive
procedures. Only 39% of SBP were culture positive and
among these 84% were due to Gram-negative bacteria.
Aerobic Gram-positive bacteria, mostly Streptococcus
viridans, Staphylococcus aureus and Enterococcus fecalis
were isolated in approximately 20% cases [55].
The prevalence of SBP in hospitalized cirrhotic patients
ranges between 10 and 30% [54]. The 1-year survival
probability after an episode is only 40% and therefore,
patients should be evaluated for OLT once they are cured
[54,56]. The clinical spectrum of SBP is variable and ranges
from no symptoms to fever, chills, abdominal pain, and/or
hepatic encephalopathy to a severe picture of peritonitis.
The diagnosis of SBP relies on the examination of
peritoneal fluid. The diagnosis is made when the poly-
morphonuclear cell count is greater than 250/mm3 or when
urine strips for leukocyte estearase are positive (3 or 4C)
[11–13,54]. For this reason and because of the high
prevalence of SBP in patients with ascites, diagnostic
paracentesis should be performed routinely in all cirrhotic
patients admitted to the hospital with ascites and in
hospitalized patients with systemic or local signs suggestive
of SBP (i.e. fever, leukocytosis, shock, abdominal pain,
rebound tenderness, ileus), hepatic encephalopathy or renal
failure [11–13]. Important clinical features of SBP are the
frequent development of renal function impairment during
the infection and the high recurrence rate [56,57].
5.1. Management of spontaneous bacterial peritonitis
Empiric antibiotic therapy must be commenced when the
PMN count in ascitic fluid is R250/mm3 and before
microbiologic results are obtained. Therapy with an
intravenous third-generation cephalosporin (cefotaxime
2 g every 8–12 h; ceftriaxone 1 g/24 h) for at least 5–7
days, is recommended [11–13]. Therapy modification
depends on results from cultures. Response to therapy
should be monitored by clinical signs, cell blood count and
PMN in ascitic fluid. Therapy should be stopped when
clinical signs of infection have disappeared and cell blood
count and PMN count in the ascitic fluid have normalized.
SBP resolves in approximately 90% of cases if treated
with the above regimens. The most important predictor of
survival in patients with SBP is the development of renal
failure during the infection [57]. Administration of albumin
at a dose of 1.5 g/kg at the diagnosis and 1 g/kg 48 h later
prevents renal failure and reduces mortality from 30 to 10%
[40]. Since recurrence of SBP occurs in 70% of cases and
constitutes a major cause of death in these patients,
prophylaxis is recommended [11,56]. Because most cases

A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133 S129
are caused by Gram-negative bacteria from the intestinal
flora, quinolones such as norfloxacin or ciprofloxacin have
been used with good results and are recommended by the
International Ascites Club [11]. Although long-term
norfloxacin (400 mg/day) is very effective in the prevention
of SBP recurrence (secondary prophylaxis) an emerging
problem has been that of quinolone resistance which may
lead to repeat episodes of SBP or other infections caused by
quinolone resistant bacteria [55]. Unfortunately, it seems
that in years to come more episodes of microorganisms
resistant to quinolones are going to complicate the clinical
course of cirrhotic patients with previous episodes of SBP.
6. Hepatic encephalopathy
Hepatic encephalopathy (HE) is a complex neuropsy-
chiatric syndrome due to hepatic failure. In patients listed
for OLT it is a recurrent theme given that in the last decade
no major breakthrough in therapy has been available.
Patients may exhibit episodic, persistent or minimal features
of HE [58]. HE is diagnosed clinically and with exclusion of
other causes of changes in mental status. In some cases HE
may be difficult to diagnose as other disorders may mimic
its clinical features. Brain imaging (magnetic resonance,
computed tomography, positron emission tomography) may
be helpful in excluding other conditions and in some cases
may help securing a diagnosis, nonetheless there are still
being investigated as a diagnostic tool in HE [58,59].
6.1. Management
The mainstay of therapy is based on supportive care,
identification and removal of precipitating factors, reduction
of nitrogenous load from the gut and assessment of long
term therapy. Common precipitating factors such as
gastrointestinal hemorrhage, infections (in particular
SBP), renal and electrolyte disturbances, psychoactive
medications, volume depletion, constipation, excessive
dietary protein and the presence of shunts (TIPS and/or
surgical portosystemic shunts) should be sought after and
corrected if possible. Although protein restriction of 1.0–
1.5 protein/kg/day has been recommended in HE, recent
data indicate that a normal protein diet is safe and in fact
nutritionally better for patients with episodic hepatic
encephalopathy [60]. Reduction of nitrogenous load by
means of colonic cleansing with non-absorbable disacchar-
ides like lactulose is a standard therapeutic measure that is
very useful in patients that cannot tolerate the oral route
[61]. For acute encephalopathy if patients are awake, oral
lactulose is the first line pharmacological treatment [61].
The recommended dose is 15–45 mL orally every 6–8 h
adjusted to achieve three soft bowel movements, profuse
diarrhea should be avoided. Antibiotics may be used as an
alternative or addition to nonabsorbable dissacharides.
Several oral antibiotics have been used, however, the most
commonly used are neomycin (3–6 g/day), metronidazol
(250 mg/day) and most recently rifaximin (1200 mg/day)
[61,62]. However, their efficacy has not been demonstrated.
Rifaximin is as good as lactulose in all types of encephalo-
pathy and seems to be a promising and safe nonbsorbable
antibiotic but experience is limited [62]. Information on
other therapies such ornithine-aspartate, flumazenil, and
bromocriptine is limited and recommendations cannot be
made on the basis of randomized studies. Usually, episodic
hepatic encephalopathy responds within a few days. Failure
to respond should prompt a search for causes of intractable
encephalopathy such as large spontaneous portosystemic
shunts. Given the widespread use of TIPS in decompensated
cirrhosis, the frequency of hepatic encephalopathy has
increased [17]. In this setting, revision of the stent with
reduction of its diameter may be helpful in selected cases.
7. Variceal bleeding
When cirrhosis is diagnosed, varices are present in
about 30–40% of compensated patients and in 60% of
those who present with ascites [63,64]. Gastrointestinal
bleeding due to ruptured gastro-esophageal varices is a
frequent and severe complication of cirrhosis. It may occur
in patients with relatively preserved liver function as well
as patients with advanced decompensated cirrhosis.
Mortality from variceal bleeding has dramatically changed
in the last 3 decades due to better endoscopic and
pharmacologic therapies and implementation of special-
ized intensive care units [65,66]. Nonetheless variceal
bleeding is still often severe and about 5–8% of patients
die within 48 h from uncontrolled bleeding [67]. Mortality
rates at 6 weeks have decreased from 30 to 50% in the
1970s to 15–17% currently [65,66]. Poor prognostic factors
are active bleeding at endoscopy, bacterial infection, and
hepatic venous pressure gradient (HVPG) greater than
20 mmHg early after admission, and renal failure [64,68].
Rebleeding within the first 6 weeks ranges from 30 to 40%,
with nearly half of these occurring with the first week of
the index bleed [67].
7.1. Management
The management of portal hypertension encompasses
therapy aimed at prevention in patients who have never bled
(primary prophylaxis), those who are actively bleeding and
those who have bled (secondary prophylaxis).
The prevention of the first bleeding should begin with
screening endoscopy in cirrhotic patients candidates to
prophylatic therapies. If no varices or very small varices are
found a repeat endoscopy is recommended in 2 years. Those
with medium or large sized varices should be treated
indefinitely with non-selective beta-blockers (i.e. proprano-
lol or nadolol) if there are no contraindications. These drugs
are given in a stepwise fashion, increasing the dose until

Fig. 4. Treatment strategy for patients with acute variceal bleeding.
Shunt surgery is reserved for patients with Child A cirrhosis. [This
figure appears in colour on the web.]
A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133S130
the resting heart rate decreases by 25% with respect to
baseline, with a heart rate between 50 and 60 beats/min [64,
69]. Those who do not tolerate or cannot take beta-blockers
due to side effects, should be offered endoscopic variceal
band ligation until eradication of varices. Both pharmaco-
logical therapy and endoscopic therapy reduce the risk of
bleeding by 40–50% [70]. Randomized controlled trials
have shown that variceal banding is as effective as beta-
blockers for preventing a first variceal bleed [71–74].
Nonetheless the choice of either beta-blockade vs. endo-
scopic therapy should made depending on the local
resources, availability of experienced endoscopists and
cost of endoscopic therapy [74]. Most authors recommend
starting with beta-blockers if there are no contraindications
because they are inexpensive, easy to use and relatively safe
[71–74].
Active variceal bleeding is a medical emergency and its
management ideally should be performed in an intensive
care setting by a team of experienced nurses, gastroenter-
ologists or hepatologists, endoscopists, interventional radi-
ologists, and surgeons. If these are not available, patients
should be referred to an appropriate institution, preferably
with a liver transplant program. Initial therapy must be
aimed at correcting hypovolemia, achieving hemostasis and
preventing complications (such as renal failure, infection
and hepatic encephalopathy) that increase the risk of
rebleeding [64,68]. Pharmacotherapy must be started as
soon as possible; if available even during transfer to the
hospital. Blood volume replacement is important, but
increased transfusion may lead to a further rise in portal
pressure and additional variceal bleeding, accordingly
the goal is to maintain the hematocrit between 25 and
30% [64,69]. Early administration of antibiotics (norflox-
acin 400 mg/day for 7 days) has been shown to improve
survival [75]. In some cases endotracheal intubation maybe
necessary as these patients have a high risk of aspiration due
to either underlying hepatic encephalopathy and/or the
sedation required for the endoscopy. A recent study
addressing management of coagulopathy showed that the
administration recombinant factor VII by correcting pro-
thrombin time significantly decreased the proportion of
patients who failed to control variceal bleeding [76].
Specific hemostatic treatments for variceal bleeding include
vasoactive drugs that decrease portal pressure, endoscopic
band ligation and surgical portosystemic shunts or TIPS.
Pharmacotherapy for acute variceal bleeding depends on
what is available locally. If available, terlipressin (2 mg/4 h
for the first 48 h, then 1 mg/4 h for up to 5 days) should be the
first choice, as it is superior to placebo in reducing mortality
[77,78]. This medication controls variceal bleeding in
75–80% of cases in 2 days and around 70% at 5 days [79].
Somatostatin (bolus of 250 mg, followed by an infusion of
250 mg/h for 5 days) or octreotide (100 mg bolus followed by
50 mg/h for 5 days) are good options if terlipressin is not
available [80,81]. In the United States octreotide is widely
used as terlipressin is not available. The recommended
treatment for acute variceal bleeding is to begin a vasoactive
drug (within 1 or 2 h if possible) to be continued for 5 days
and therapeutic endoscopy (Fig. 4) [64,68]. This approach
controls bleeding in 75% of cases [77,82]. Although this
combination improves the results of endoscopy and
decreases rebleeding; combination therapy does not improve
6-week mortality compared with endoscopic or drug therapy
alone [83,84].
If the patient has a recurrent bleeding episode a single
endoscopic re-treatment is reasonable if the patient is stable
[64,85]. In hemodynamically unstable patients other defini-
tive measures such as TIPS or surgery need to be considered.
If there is massive bleeding, balloon tamponade may
temporarily aid in controlling the hemorrhage, however, it
has a high incidence of rebleeding when the balloon is
deflated and may cause pressure necrosis of the esophageal
mucosa with prolonged use [85,86]. TIPS is very effective
with control rates around 95%, but since these patients are
very sick mortality rates remain high [64,85,87]. TIPS is
preferred over shunt surgery because it is associated with
less operative morbidity and mortality [17,88]. Moreover, in
patients awaiting liver transplantation, TIPS appears to be a
better option than surgery [88]. In selected cases shunt
surgery, an H—graft mesocaval shunt, for Child A patients
is a viable option if an experienced surgeon is available.
After patients have bled the risk of a repeat episode is
around 60% and mortality from each rebleeding episode is
near 20% [67]. Therefore, these patients need to be treated
very aggressively. Both beta-blockade and endoscopic band
ligation can be used. If possible the effect of beta-blockers
should be monitored with the use of HVPG. The goal is
reduction below 12 mmHg otherwise a goal of reduction of
heart by 25% is acceptable [64,68]. If one of these fails, the
best approach is a combination of beta-blockers plus
endoscopic band ligation, however, information is limited.
Those patients with recurrent bleeding despite the above

A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133 S131
measures should be offered a TIPS or shunt surgery if they
are Child A.
8. Summary
As the demand for OLT increases, patients with advanced
cirrhosis will end up spending a longer time waiting in the list
with an increased risk of developing further decompensation
and dying. Only the expansion of the donor pool will have a
major impact on the survival of patients; however, this seems
to be extremely challenging given that use of marginal
donors and living related liver transplantation has not made a
significant impact on waiting times. Therefore, both preven-
tion and effective treatment of complications such as ascites,
dilutional hyponatremia, hepatorenal syndrome, spon-
taneous bacterial peritonitis, hepatic encephalopathy and
variceal bleeding may improve the likelihood of a patient
surviving until OLT.
References
[1] National Institutes of Health Consensus Development Conference
Statement. Liver transplantation—June 20–23 1983. Hepatology
1984;4:107S–1110.
[2] Starzl TE, Demetris AJ, VanThiel D. Liver Transplantation. N Eng
J Med 1989;321:1014–1022.
[3] Kim WR, Dickson ER. Timing of liver transplantation. Semin Liver
Dis 2000;20:451–464.
[4] Llovet JM, Beaugrand M. Hepatocellular carcinoma: present status
and future prospects. J Hepatol 2003;38:S136–S149.
[5] D’Amico G, Morabito A, Pagliaro L, Marubini E. Survival and
prognostic indicators in compensated and decompensated cirrhosis.
Dig Dis Sci 1986;31:1507–1513.
[6] Fernandez-Esparrach G, Sanchez-Fueyo A, Gines P, Uriz J, Quinto L,
Ventura PJ, et al. A prognostic model for predicting survival in
cirrhosis with ascites. J Hepatol 2001;34:46–52.
[7] Adam R, McMaster P, O’Grady JG, Castaing D, Klempnauer JL,
Jamieson N. Evolution of liver transplantation in Europe: report of the
European Liver Transplant Registry. Liver Transpl 2003;9:
1231–1243.
[8] Carithers RL. Liver transplantation. Liver Transpl 2000;6:122–135.
[9] Arroyo V, Colmenero J. Ascites and hepatorenal syndrome in
cirrhosis: pathophysiological basis of therapy and current manage-
ment. J Hepatol 2003;38:S69–S89.
[10] Moore KP, Wong F, Gines P, Bernardi M, Ochs A, Salerno F, et al.
The management of ascites in cirrhosis: report on the consensus
conference of the International Ascites Club. Hepatology 2003;38:
258–266.
[11] Rimola A, Garcia-Tsao G, Navasa M, Piddock LJ, Planas R,
Bernard B, et al. Diagnosis, treatment and prophylaxis of spontaneous
bacterial peritonitis: a consensus document. International Ascites
Club. J Hepatol 2000;32:142–153.
[12] Runyon B. Management of adult patients with ascites due to cirrhosis.
Hepatology 2004;39:841–856.
[13] Gines P, Cardenas A, Arroyo V, Rodes J. Management of cirrhosis
and ascites. N Engl J Med 2004;350:1646–1654.
[14] Gines P, Tito L, Arroyo V, et al. Randomized comparative study of
therapeutic paracentesis with and without intravenous albumin in
cirrhosis. Gastroenterology 1988;94:1493–1502.
[15] Gines A, Fernandez-Esparrach G, Monescillo A, Vila C,
Domenech E, Abecasis R, et al. Randomized trial comparing albumin,
dextran 70, and polygeline in cirrhotic patients with ascites treated by
paracentesis. Gastroenterology 1996;111:1002–1010.
[16] Sola-Vera J, Minana J, Ricart E, Planella M, Gonzalez B, Torras X,
et al. Randomized trial comparing albumin and saline in the
prevention of paracentesis-induced circulatory dysfunction in cirrho-
tic patients with ascites. Hepatology 2003;37:1147–1153.
[17] Boyer T. Transjugular intrahepatic portosystemic shunt: current
status. Gastroenterology 2003;124:1700–1710.
[18] Bureau C, Garcia-Pagan JC, Otal P, Pomier-Layrargues G,
Chabbert V, Cortez C, et al. Improved clinical outcome using
polytetrafluoroethylene-coated stents for TIPS: results of a random-
ized study. Gastroenterology 2004;126:469–475.
[19] Lebrec D, Giuily N, Hadengue A, Vilgrain V, Moreau R, Poynard T,
et al. Transjugular intrahepatic portosystemic shunts: comparison with
paracentesis in patients with cirrhosis and refractory ascites: a
randomized trial. J Hepatol 1996;25:135–144.
[20] Rossle M, Ochs A, Gulberg V, Siegerstetter V, Holl J, Diebert P, et al.
A comparison of paracentesis and transjugular intrahepatic portosys-
temic shunting in patients with ascites. N Engl J Med 2000;342:
1701–1707.
[21] Gines P, Uriz J, Calahorra B, Garcia-Tsao G, Kamath PS, Ruiz del
Arbol L, et al. Transjugular intrahepatic portosystemic shunting
versus paracentesis plus albumin for refractory ascites in cirrhosis.
Gastroenterology 2002;123:1839–1847.
[22] Sanyal AJ, Genning C, Reddy RK, Wong F, Kowdley K, Benner K,
et al. The North American study for the treatment of refractory ascites.
Gastroenterology 2003;124:634–641.
[23] Salerno F, Merli M, Riggio O, Cazzaniga M, Valeriano V, Pozzi M,
et al. Randomized controlled study of TIPS versus paracentesis plus
albumin in cirrhosis with severe ascites. Hepatology 2004;40:
629–635.
[24] Clavien PA, Selzner M, Tuttle-Newhall JE, Harland RC, Suhocki P.
Liver transplantation complicated by misplaced TIPS in the portal
vein. Ann Surg 1998;227:440–445.
[25] Tripathi D, Therapondos G, Redhead DN, Madhavan KK, Hayes PC.
Transjugular intrahepatic portosystemic stent-shunt and its effects on
orthotopic liver transplantation. Eur J Gastroenterol Hepatol 2002;14:
827–832.
[26] Gines P, Berl T, Bernardi M, Bichet DG, Hamon G, Jimenez W, et al.
Hyponatremia in cirrhosis: from pathogenesis to treatment. Hepatol-
ogy 1998;28:851–864.
[27] Heuman DM, Abou-assi SG, Habib A, Williams LM, Stravitz RT,
Sanyal AJ, et al. Persistent ascites and low serum sodium identify
patients with cirrhosis and low MELD scores who are at high risk for
early death. Hepatology 2004;40:802–810.
[28] Biggins S, Rodriguez HJ, Bass NM, Robert JP, Terrault NA. Serum
sodium predicts mortality in patients listed for liver transplantation.
Hepatology 2005;41:32–39.
[29] Ruf AE, Yantorno SE, Descalzi VI, Andrani OC, Podesta LG,
Villamil FG. Addition of serum sodium into the MELD score predicts
waiting list mortality better than MELD alone: a single-center
experience. Am J Transplant 2004;4:438A.
[30] Arroyo V, Rodes J, Gutierrez-Lizarraga MA, Revert L. Prognostic
value of spontaneous hyponatremia in cirrhosis with ascites. Am J Dig
Dis 1976;21:249–256.
[31] Porcel A, Diaz F, Rendon P, Macias M, Martin-Herrera L, Giron-
Gonzalez JA. Dilutional hyponatremia in patients with cirrhosis and
ascites. Arch Intern Med 2002;162:323–328.
[32] Restuccia T, Gomez-Anson B, Guevera M, Alessandria C, Torre A,
Alayrach ME, et al. Effects of dilutional hyponatremia on brain
organic osmolytes and water content in patients with cirrhosis.
Hepatology 2004;39:1613–1622.
[33] Sterns RH, Riggs JE, Schochet Jr SS. Osmotic demyelination
syndrome following correction of hyponatremia. N Engl J Med
1986;314:1535–1542.

A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133S132
[34] Wszolek ZK, McComb RD, Pfeiffer RF, Steg RE, Wood RP, Shaw
Jr BW, et al. Pontine and extrapontine myelinosis following liver
transplantation. Relationship to serum sodium. Transplantation 1989;
48:1006–1012.
[35] Abbasoglu O, Goldstein RM, Vodapally MS, Jennings LW, Levy MF,
Husberg BS, et al. Liver transplantation in hyponatremic patients with
the emphasis on central pontine myelinolysis. Clin Transplant 1998;
12:263–269.
[36] Gerbes AL, Gulberg V, Gines P, Decaux G, Gross P, Gandjini H, VPA
Study Group, et al. Therapy of hyponatremia in cirrhosis with a
vasopressin receptor antagonist: a randomized double-blind multi-
center trial. Gastroenterology 2003;124:933–939.
[37] Wong F, Blei AT, Blendis LM, Thuluvath PJ. A vasopressin receptor
antagonist (VPA-985) improves serum sodium concentration in
patients with hyponatremia: a multicenter, randomized, placebo-
controlled trial. Hepatology 2003;37:182–191.
[38] Arroyo V, Gines P, Gerbes A, Dudley FJ, Gentilini P, Laffi G, et al.
Definition and diagnostic criteria of refractory ascites and hepatorenal
syndrome in cirrhosis. Hepatology 1996;23:164–176.
[39] Gines A, Escorsell A, Gines P, Salo J, Jimenez W, Inglada L, et al.
Incidence, predictive factors, and prognosis of the hepatorenal
syndrome in cirrhosis with ascites. Gastroenterology 1993;105:
229–236.
[40] Sort P, Navasa M, Arroyo V, Aldeguer X, Planas R, Ruiz-del-Arbol L,
et al. Effect of intravenous albumin on renal impairment and mortality
in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl
J Med 1999;341:403–409.
[41] Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil O.
Pentoxifylline improves short-term survival in severe acute alcoholic
hepatitis: a double-blind, placebo-controlled trial. Gastroenterology
2000;119:1637–1648.
[42] Uriz J, Gines P, Cardenas A, Sort P, Jimenez W, Salmeron JM, et al.
Terlipressin plus albumin infusion: an effective and safe therapy of
hepatorenal syndrome. J Hepatol 2000;33:43–48.
[43] Moreau R, Durand F, Poynard T, Duhamel C, Cervoni JP, Ichai P,
et al. Terlipressin in patients with cirrhosis and type 1 hepatorenal
syndrome: a retrospective multicenter study. Gastroenterology 2002;
122:923–930.
[44] Ortega R, Gines P, Uriz J, Cardenas A, Calahorra B, De Las Heras D,
et al. Terlipressin therapy with and without albumin for patients with
hepatorenal syndrome. Results of a prospective, non-randomized
study. Hepatology 2002;36:941–948.
[45] Mulkay JP, Louis H, Donckier V, Bourgeois N, Adler M, Deviere J,
et al. Long-term terlipressin administration improves renal function in
cirrhotic patients with type 1 hepatorenal syndrome: a pilot study.
Acta Gastroenterol Belg 2001;64:15–19.
[46] Halimi C, Bonnard P, Bernard B, Mathurin P, Mofredj A, di
Martino V, et al. Effect of terlipressin (Glypressin) on hepatorenal
syndrome in cirrhotic patients: results of a multicentre pilot study. Eur
J Gastroenterol Hepatol 2002;14:153–158.
[47] Colle I, Durand F, Pessione F, Rassiat E, Bernuau J, Barriere E,
et al. Clinical course, predictive factors and prognosis in patients
with cirrhosis and type 1 hepatorenal syndrome treated with
Terlipressin: a retrospective analysis. J Gastroenterol Hepatol 2002;
17:882–888.
[48] Solanki P, Chawla A, Garg R, Gupta R, Jain M, Sarin SK. Beneficial
effects of terlipressin in hepatorenal syndrome: a prospective,
randomized placebo-controlled clinical trial. J Gastroenterol Hepatol
2003;18:152–156.
[49] Angeli P, Volpin R, Gerunda G, Craighero R, Roner P, Merenda R,
et al. Reversal of type 1 hepatorenal syndrome with the administration
of midodrine and octreotide. Hepatology 1999;29:1690–1697.
[50] Wong F, Pantea L, Sniderman K. Midodrine, octreotide, albumin, and
TIPS in selected patients with cirrhosis and type 1 hepatorenal
syndrome. Hepatology 2004;40:55–64.
[51] Duvoux C, Zanditenas D, Hezode C, Chauvat A, Monin JL, Roudot-
Thoraval F, et al. Effects of noradrenaline and albumin in patients with
type 1 hepatorenal syndrome: a pilot study. Hepatology 2002;36:
374–380.
[52] Restuccia T, Ortega R, Guevara M, Gines P, Alessandria C,
Ozdogan O, et al. Effects of treatment of hepatorenal syndrome
before transplantation on posttransplantation outcome. A case-control
study. J Hepatol 2004;40:140–146.
[53] Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM,
Kosberg CL, et al. A model to predict survival in patients with end-
stage liver disease. Hepatology 2001;33:464–470.
[54] Garcia-Tsao G. Sponateneous bacterial peritonitis: a historical
perspective. J Hepatol 2004;41:522–527.
[55] Fernandez J, Navasa M, Gomez J, Colmenero J, Vila J, Arroyo V,
et al. Bacterial infections in cirrhosis: epidemiological changes with
invasive procedures and norfloxacin prophylaxis. Hepatology 2002;
35:140–148.
[56] Tito L, Rimola A, Gines P, Llach J, Arroyo V, Rodes J. Recurrence of
spontaneous bacterial peritonitis in cirrhosis. Frequency and pre-
dictive factors. Hepatology 1988;8:27–31.
[57] Follo A, Llovet JM, Navasa M, Planas R, Forns X, Francitorra A, et al.
: Renal impairment after spontaneous bacterial peritonitis in cirrhosis:
incidence, clinical course, predictive factors and prognosis. Hepatol-
ogy 1994;20:495–501.
[58] Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K,
Blei AT. Hepatic encephalopathy—definition, nomenclature, diag-
nosis, and quantification: final report of the working party at the 11th
World Congresses of Gastroenterology, Vienna, 1998. Hepatology
2002;35:716–721.
[59] Butterworth R. Pathogenesis of hepatic encephalopathy: new insights
from neuroimaging and molecular studies. J Hepatol 2003;39:
278–285.
[60] Cordoba J, Lopez-Hellin J, Planas M, Sabin P, Sanpedro F, Castro F,
et al. Normal protein diet for episodic hepatic encephalopathy: results
of a randomized study. J Hepatol 2004;41:38–43.
[61] Blei AT, Cordoba J. Practice parameters committee of the American
college of gastroenterology hepatic encephalopathy. Am
J Gastroenterol 2001;96:1968–1976.
[62] Mas A, Rodes J, Sunyer L, Rodrigo L, Planas R, Vargas V, et al.
Comparison of rifaximin and lactitol in the treatment of acute hepatic
encephalopathy: results of a randomized, double-blind, double-
dummy, controlled clinical trial. J Hepatol 2003;38:51–58.
[63] D’Amico G, Luca A. Natural history. Clinical-hemodynamic
correlations. Prediction of the risk of bleeding. Baillieres Clin
Gastroenterol 1997;11:243–256.
[64] Bosch J, Abraldes JG, Groszmann R. Current management of portal
hypertension. J Hepatol 2003;38:S54–S68.
[65] Chalasani N, Kahi C, Francois F, Pinto A, Marathe A, Bini EJ, et al.
Improved patient survival after acute variceal bleeding: a multicenter,
cohort study. Am J Gastroenterol 2003;98:653–659.
[66] Carbonell N, Pauwels A, Serfaty L, Fourdan O, Levy VG, Poupon R.
Improved survival after variceal bleeding in patients with cirrhosis
over the past two decades. Hepatology 2004;40:652–659.
[67] de Franchis R, Primignani M. Natural history of portal hypertension in
patients with cirrhosis. Clin Liver Dis 2001;5:645–663.
[68] de Franchis R. Updating consensus in portal hypertension: report of
the Baveno III Consensus Workshop on definitions, methodology
and therapeutic strategies in portal hypertension. J Hepatol 2000;33:
846–852.
[69] de Franchis R, Primignani M. Endoscopic treatments for portal
hypertension. Semin Liver Dis 1999;19:439–455.
[70] de Franchis R. Incidental esophageal varices. Gastroenterology 2004;
126:1860–1867.
[71] Schepke M, Kleber G, Nurnberg D, Willert J, Koch L, Veltzke-
Schlieker W, et al. Ligation versus propranolol for the primary prophylaxis
of variceal bleeding in cirrhosis. Hepatology 2004;40:65–72.

A. Cardenas, P. Gines / Journal of Hepatology 42 (2005) S124–S133 S133
[72] Lo GH, Chen WC, Chen MH, Lin CP, Lo CC, Hsu PI, et al. Endoscopic
ligation vs. nadoilol in the prevention of first variceal bleeding in
patients with cirrhosis. Gastrointest Endosc 2004;59:333–338.
[73] Lui HF, Stanley AJ, Forrest EH, Jalan R, Hislop WS, Mills PR, et al.
Primary prophylaxis of variceal hemorrhage: a randomized controlled
trial comparing band ligation, propranolol, and isosorbide mono-
nitrate. Gastroenterology 2002;123:735–744.
[74] Cardenas A, Gines P, Uriz J, Bessa X, Salmeron JM, Mas A, et al.
Renal failure after upper gastrointestinal bleeding in cirrhosis:
incidence, clinical course, predictive factors, and short-term prog-
nosis. Hepatology 2001;34:671–676.
[75] Bernard B, Grange JD, Khac EN, Amiot X, Opolon P, Poynard T.
Antibiotic prophylaxis for the prevention of bacterial infections in
cirrhotic patients with gastrointestinal bleeding: a meta-analysis.
Hepatology 1999;29:1655–1661.
[76] Bosch J, Thabut D, Bendtsen F, D’Amico G, Albillos A, Gonzalez
Abraldes J, et al. Recombinant factor VIIa for upper gastrointestinal
bleeding in patients with cirrhosis: a randomized, double-blind trial.
Gastroenterology 2004;127:1123–1130.
[77] Levacher S, Letoumelin P, Pateron D, Blaise M, Lapandry C,
Pourriat JL. Early administration of terlipressin plus glyceryl trinitrate
to control active upper gastrointestinal bleeding in cirrhotic patients.
Lancet 1995;346:865–868.
[78] Ioannou GN, Doust J, Rockey DC. Systematic review: terlipressin in
acute oesophageal variceal haemorrhage. Aliment Pharmacol Ther
2003;17:53–64.
[79] Escorsell A, Ruiz del Arbol L, Planas R, Albillos A, Banares R,
Cales P, et al. Multicenter randomized controlled trial of terlipressin
versus sclerotherapy in the treatment of acute variceal bleeding: the
TEST study. Hepatology 2000;32:471–476.
[80] Abraldes JG, Bosch J. Somatostatin and analogues in portal
hypertension. Hepatology 2002;35:1305–1312.
[81] Corley DA, Cello JP, Adkisson W, Ko WF, Kerlikowske K.
Octreotide for acute esophageal variceal bleeding: a meta-analysis.
Gastroenterology 2001;120:946–954.
[82] Avgerinos A, Nevens F, Raptis S, Fevery J. Early administration
of somatostatin and efficacy of sclerotherapy in acute oesophageal
variceal bleeds: the European Acute Bleeding Oesophageal
Variceal Episodes (ABOVE) randomised trial. Lancet 1997;350:
1495–1499.
[83] Villanueva C, Ortiz J, Sabat M, Gallego A, Torras X, Soriano G, et al.
Somatostatin alone or combined with emergency sclerotherapy in the
treatment of acute esophageal variceal bleeding: a prospective
randomized trial. Hepatology 1999;30:384–389.
[84] Cales P, Masliah C, Bernard B, Garnier PP, Silvain C, Szostak-
Talbodec N, French Club for the Study of Portal Hypertension, et al.
Early administration of vapreotide for variceal bleeding in patients
with cirrhosis. N Engl J Med 2001;344:23–28.
[85] Mihas AA, Sanyal A. Recurrent variceal bleeding despite endoscopic
and medical therapy. Gastroenterology 2004;127:621–629.
[86] Moreto M, Zaballa M, Bernal A, Ibanez S, Ojembarrena E,
Rodriguez A. A randomized trial of tamponade or sclerotherapy as
immediate treatment for bleeding esophageal varices. Surg Gynecol
Obstet 1988;167:331–334.
[87] Bosch J. Salvage transjugular intrahepatic portosystemic shunt: is it
really life-saving? J Hepatol 2001;35:658–660.
[88] Henderson JM. Salvage therapies for refractory variceal hemorrhage.
Clin Liver Dis 2001;5:709–725.