
Dd’s of esophageal stricture and intra luminal filling defects
Upload
zeeshanrahman86Category
view
55download
2
Management of cervical esophageal anastomotic stricture
Zeeshan
Introduction
• Most common etiology: GERD (75%)• Other causes:- Caustic ingestion- External beam radiotherapy- Surgical anastomoses- Rare dermatological diseases eg.
Epidermolysis bullosa
Rare causes
- Extrinsic compression of esophagus• Tuberculosis• Idiopathic fibrosing mediastinitis
• Eosinophilic esophagitis- Dilatation associated with mucosal tearing and
perforation
Goal of therapy
• Relief of dysphagia
• Prevention of stricture recurrence
Evaluation prior to dilatation
• H/O Dysphagia
D/D• GERD• Motility disturbance• Infection• Malignancy• Esophageal webs/rings
PRIOR TO ENDOSCOPIC DILATATION ALWAYS RULE OUT
OTHER CAUSES

Investigations
• Barium swallow
AFTER CONFIRMATION PROCEED TO ENDOSCOPIC
DILATATION
Contraindication for dilatation
• In acute or incompletely healed esophageal perforation
• In potentially malignant stricture• Patients with pulmonary /cardiac risk factor• EXTREME CARE in cervical deformity/ thoracic
aneurysm/ recent surgery• Eosinophilic esophagitis
Types of esophageal dilators
Mechanical dilators
• Bougie dilators
Balloon dilators
Mechanical dilators
• Divided into 2 types:1. Those that pass freely2. Those that are inserted over guidewire
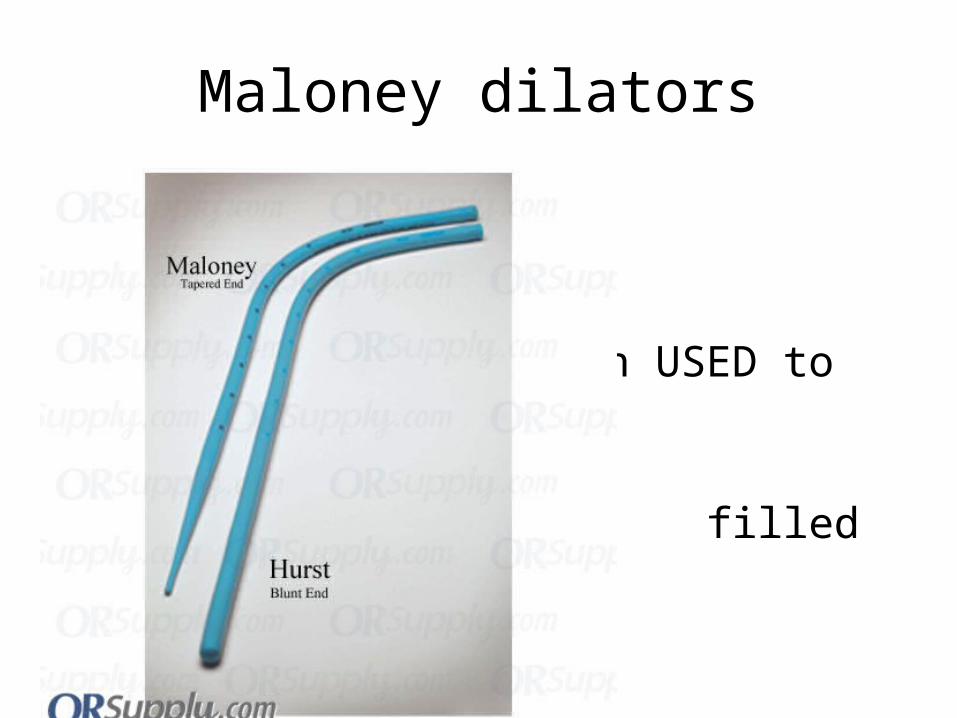
Maloney dilators
• • In USED to be • filled with Hg.• Tungsten used
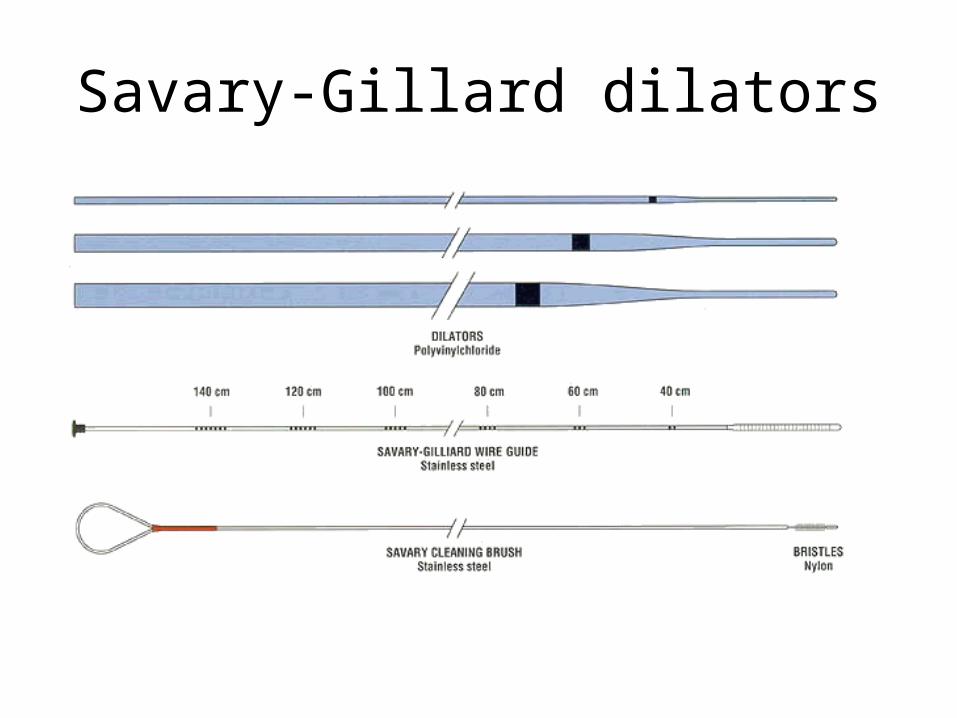
Savary-Gillard dilators
Balloon dilators
• 2 types
1. Through the scope dilators (TTS)
2. Over the guidewire dilators (OTW)

Therapeutic approach
• Simple strictures:- Related to prolonged reflux- Short segment- Scope can be passed easily- Maloney dilators can be safely used
• Complex strictures:- Long narrow and tortuous- Scope cannot be passed easily- Stricture associated with hiatal
hernia/esophageal diverticula

Technique
Number of dilatations per session
• Bougie dilators- No more than 3 dilatations per session- Lumen french should not be increase by > 6Fr
• Ballon dilators- No more than 3 incremental inflations- Very tight or long strictures- 2 dilatations per
sitting
Frequecy of dilatation
• Depends upon1. Success of initial dilatation
2. Response of patient to initial dilatation
• Pt undergoing dilatation fr 1st time – required multiple sittings once every 5-6 days
• Last dilator used in previous session to be passed 1st.
End point of dilatation
• Dilatation to 18mm (56 Fr) – Solid diet
• Dilatation to 13mm (39Fr) – Dysphagia to solids
• Dilatation to 15mm (45Fr) – Soft solids
Refractory strictures
• Patients FAILING to respond to esophageal dilatations
• Poor candidates for surgical repair
Other methods
1. Intralesional injection of steroids
2. Non-metal stents
3. Metal stents
4. Other methods
Intralesional injection of steroids
• Injection of triamcinolone MAY reduce stricture recurrence
• MOA Corticosteroids MAY impede collagen
deposition and enhance its breakdown locally to prevent scar formation
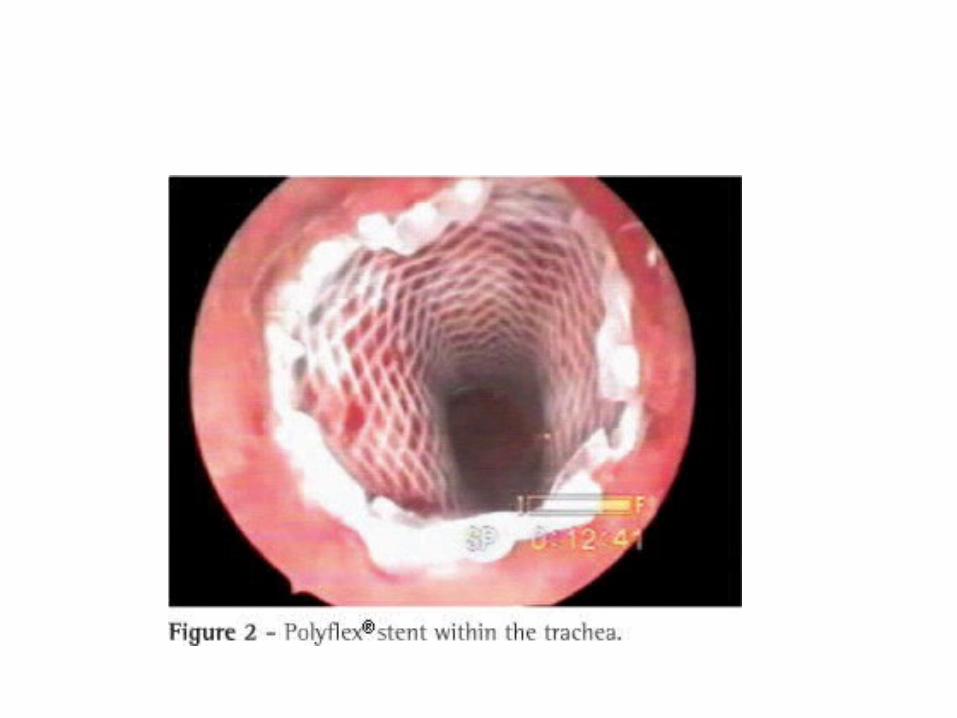
Non-metal expandable stents
• Temporary placement of non-metal expandable stents- effective in management of benign strictures
• Stent: Silicon coated self expanding plastic stent
• To be left in place for 6 weeks to allow remodelling of scar tissue
• Longer time required for anastomotic strictures
• Problem: Stent migration
11 Patients with anastomotic stricture following esophagogastrectomy.
• Stent placed for ALL patients• ALL patients had satisfactory relief of dysphagia• Recurrence of symptoms after stent removal –
23% patients• Mean time for repeat dilatation/stent
reinsertion- 37 days• Clinical outcomes after self-expanding plastic stent placement for
refractory benign esophageal strictures.• Oh YS, Kochman ML, Ahmad NA, Ginsberg GG
• Largest study conducted40 patients with refractory benign esophageal strictures
treated with Polyflex stent x 4 weeks
• Median dysphagia score improved• Follow-up after 1 year – 40% dysphagia FREE• Complications included:- Stent migration- Severe chest pain- Bleeding- Perforation- GERD- Stent impaction- Fistula formation
Others
• Injection of Mitomycin
• Endoscopic electrosurgical incision of peptic ulcer
Surgery
Post- esophagogastrectomy strictures
• Following esophagogastrectomy – Benign esophageal stricture 40%
• Association:- Anastomotic leak- Inadequate/ marginally adequate blood flow
to most cranial part of gastric tube
• Strictures usually respond to endoscopic dilatation
• If NOT responding:- Resection - Transection- Patch repair of stricture
TO RE-ESTABLISH GI CONTINUITY
Options available
• Colon interposition• Mobilisation and advancement of stomach
and reanastomoses• Free jejunal graft• Patch stricturoplasty
Patch stricturoplasty
1. Staged flap
2. Myocutaneous flap
3. Free flap
Staged flaps
• Wookey’s cervical skin flap
• Bakamjiam’s deltopectoral flap
Myocutaneous flaps
• Pectoralis major myocutaneous flap
• Latissimus dorsi myocutaneous flap
• Platysma myocutaneous flap
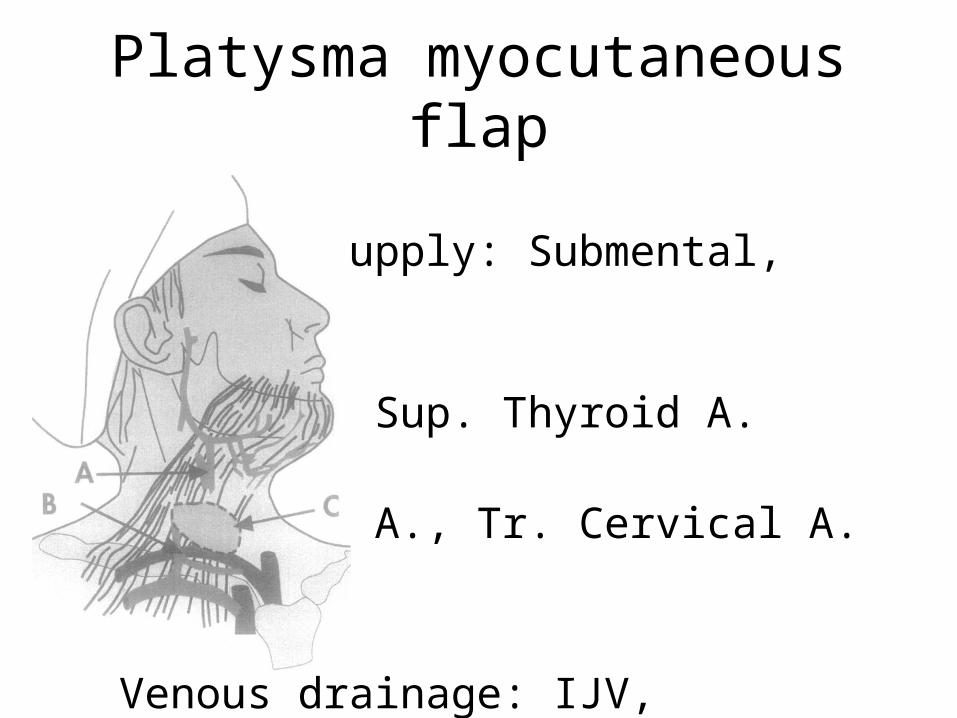
Platysma myocutaneous flap
• Arterial supply: Submental,
• Facial A., Sup. Thyroid A.• Occipital A., Tr. Cervical A.
• Venous drainage: IJV, • Submental V.
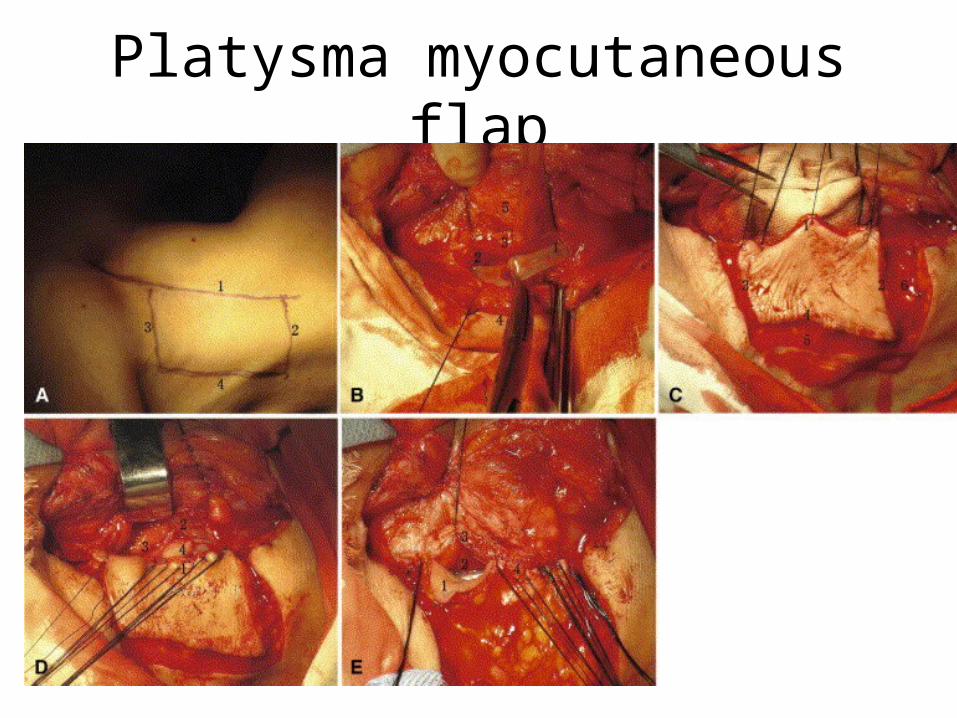
Platysma myocutaneous flap
• Failure rate – 40%
• Leak rate - 10.7 %
• Restenosis rate – 7.1%
• Platysma Myocutaneous Flap for Patch Stricturoplasty in Relieving Short and Benign Cervical Esophageal Strictur Yi-Dan Lin, MD, Yao-Guang Jiang, MD, , Ru-Wen Wang, MD, Tai-Qian Gong, MD, Jing-Hai Zhou,MD
Advantages
• Less bulky compared to PMMC/ LD flap
• Local flap – morbidity of laparotomy avoided
• Leak rate and restenosis rates lower
• Early enteral nutrition can be intiated through NG tube
Disadvantages
• Cannot motivate peristalsis
Free flaps
• Radial fore-arm free flap
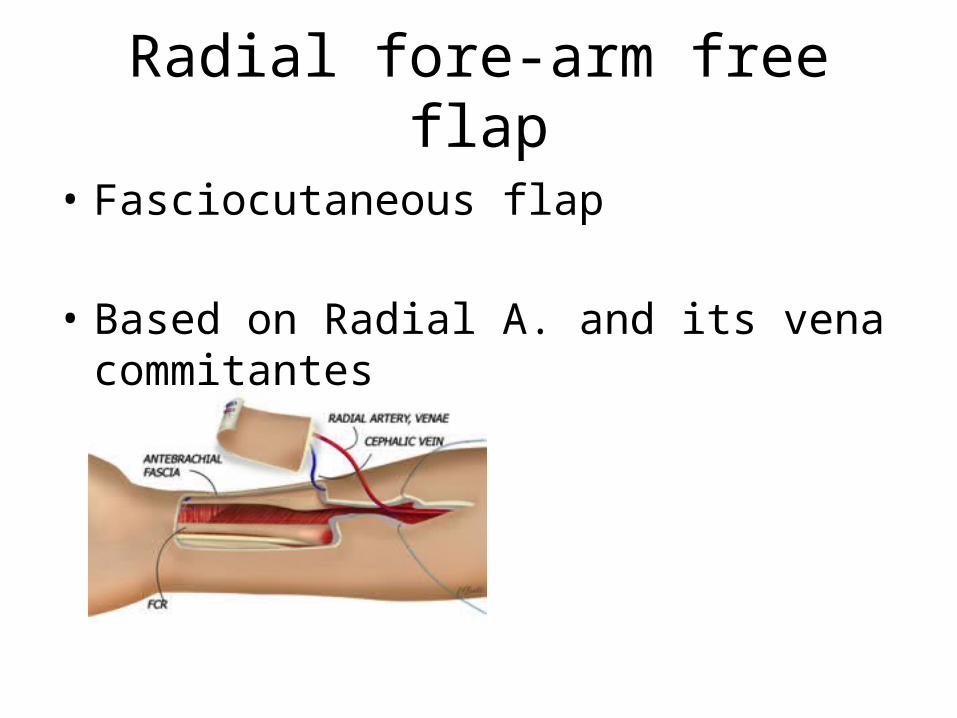
Radial fore-arm free flap
• Fasciocutaneous flap
• Based on Radial A. and its vena commitantes
Advantages over jejunal free flap
1. Does NOT require laparotomy to harvest
2. Pedicle is LONG – giving surgeons the use of several feeding vessels
3. NOT bulky
4. Mucosa DOESNOT secrete mucus
Study
• 5 men and 1 woman• Age between 24- 60 years• Between 1993 – 1996
• All patients had esophageal replacement for non-malignant disease
• All had failed multiple esophageal dilatation• 1 patient 6 weeks post esophagogastrectomy had a
persistent leak with necrosis of 60% of proximal stomach – NOT septic
Procedure
• RFFF was harvested from non-dominant arm unless Allen’s test was positive
• Stricture was transected in longitudinal direction of esophagus and stomach and patch applied
• Size of graft 5x8cm to 5x12cm• Length of graft 8 – 12cm
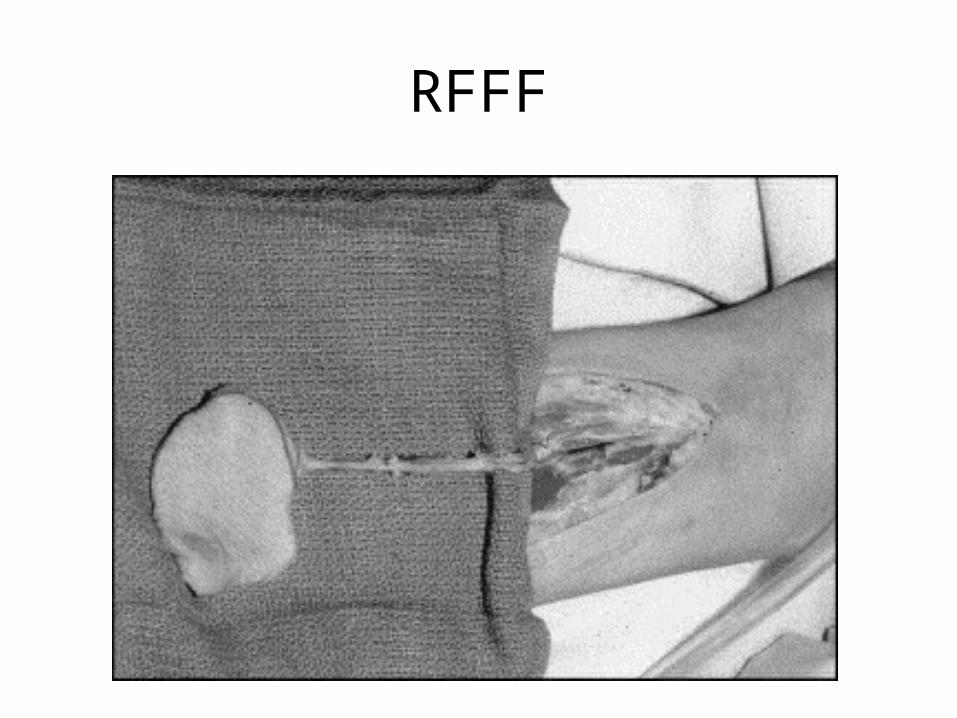
RFFF
• Treatment was accomplished through NECK incision in 5 patients
• Thoracotomy and neck incision in 1 patient
• In patients with VC palsy on the side of the previous incision (2 of 6) – SAME side used
• Patients with no VC palsy – Opposite side used
• Graft sewed using single layer interrupted technique
• Revascularised using microvascular technique
• Artery – anastomosed to Facial A./Inf. Thyroid A./ Transverse cervical A.
• Vein – anastomosed to IJV
• Follow-up
3/12 interval for 1 year
Yearly intervals after that
Results
• 1 patient developed LEAK from graft stomach anastomotic site ---POD 8
• Exsanguinated from venous anastomoses of patch graft ---- POD 12
• Postmortem – GRAFT was viable.
• ONLY patient to be treated in ACUTE phase of illness
• Other 5 patients – normal diet within 4 -6 weeks of surgery
• NO anastomotic leaks• 1 patient developed narrowing of distal
anastomoses of tubularised graft—Dilatation
• ALL patients could eat solid food– 7 years follow up
• When one is confronted with the rare problem of a stricture or persistent fistulae from the cervical esophagogastrectomy anastomosis, we would recommend the use of the radial forearm flap to patch this anastomosis.
• Use of the radial forearm free tissue flap to treat persistent stricture after esophagogastrectomy
• Clifford W Deveney, M.D.a, , Scott Soot, M.D.a, Blair Jobe, M.D.a, James I Cohen, M.D.a, Peter Anderson, M.D.a, Mark K Wax, M.D.a, Michael Wheatley, M.D.a, Brett C Sheppard, M.D.a


















