Management of Biliary Duct Confluence Injuries Produced by Hepatic Hydatidosis
6
World J. Surg. 25, 1264–1269, 2001 DOI: 10.1007/s00268-001-0107-3 WORLD Journal of SURGERY © 2001 by the Socie ´te ´ Internationale de Chirurgie Management of Biliary Duct Confluence Injuries Produced by Hepatic Hydatidosis Emilio Vicente, M.D., Juan C. Meneu, M.D., Pedro L. Hervás, M.D., Javier Nuño, M.D., Yolanda Quijano, M.D., Manuel Devesa, M.D., Alberto Moreno, M.D., Luis Blazquez, M.D. General Surgery Department, Liver Transplantation Unit, Ramón y Cajal University Hospital, Alcalá de Henares University, Ctra. Colmenar km 9’100, Madrid 28034, Spain Published Online: August 20, 2001 Abstract. From 1978 to 1999 a total of 850 patients underwent surgical treatment for hydatid disease of the liver at our surgical department. Biliary duct confluence injuries produced by hepatic hydatidosis (HH) were founded in six patients (0.7%). Surgical intervention was undertaken to relieve the obstructive jaundice and clinical manifestations of cholan- gitis and to treat the hydatid cyst. A partially open cystopericystectomy technique was used in three patients with a double bilioenteric Roux-en-Y reconstruction. The remaining three patients (two with prehepatic portal hypertension and one with triple hepatic duct confluence) were subjected to a cystojejunostomy. There were no hospital deaths. Two cases of anastomotic leakage following a high bilioenteric anastomosis occurred but did not require surgical treatment. During the follow-up (5–19 years) one patient suffered local recurrence of the hydatid disease 7 years after cystojejunostomy. The site of intrahepatic biliary and vascular involve- ment, the presence of biliary duct anomalies, and the presence of portal hypertension are decisive factors when choosing the “ideal” procedure for reconstruction. Conservative surgical approaches (partial cystectomy and cystojejunostomy) are the treatments of choice. Radical surgery is often a serious matter. Echinococcus granulosus is the parasite responsible for hydatido- sis. This disease is an important cause of morbidity and mortality, and it increases public health costs in the areas of the world where the disease is endemic: South America, Australia, East Africa, and Mediterranean countries [1, 2]. Human affectation represents the casual intermediate part of the life cycle of this parasite; the intermediate and definitive host is the dog. The parasite is transported from gut to liver through the portal circulation, leading most often to liver damage. Symptoms of hepatic hydatidosis (HH) are varied. Parasitic cysts may remain silent for long periods of time, sometimes being diagnosed when radiology or echography is performed for other reasons. The volume, localization, and type of cystic complication are factors causing clinical symptomatology. Bile duct communi- cation, suppuration, and rupture of the cyst into the peritoneal cavity through the diaphragm and into a bronchus are the most frequent complications of HH [3–7]. Involvement of the biliary duct in patients with HH is well known. The incidence of intrabiliary rupture varies among studies, from 1% to 17%, owing to different etiologies [8–14]: (1) com- pression of the intra- or extrahepatic biliary tree; (2) biliocystic communications that allow the bile to pass to the cyst cavity or from the cyst to the biliary duct; and (3) destruction of the hilar confluence. These biliary complications produce similar clinical symptoms: biliary colic, obstructive jaundice, or acute cholangitis. However, the frequency, severity, and surgical technique used for treatment as well as its complexity if it is done late are different. Biliary duct confluence injury produced by HH is a rare but serious condition associated with a high morbidity rate with a difficult surgical approach. Few isolated cases have been reported [14, 15], and no series of patients with outcome has been pub- lished. The present work summarizes our experience with the management of patients with biliary duct confluence injuries pro- duced by HH over 21 years. Patients and Methods From 1978 to 1999 the general surgery department at the Ramón y Cajal Hospital admitted a total of 850 patients suffering from hydatid disease of the liver who required surgery. Case reports from six patients presenting with destruction of the hilar conflu- ence caused by the parasitic cyst were reviewed. There were three males and three females whose mean age was 42.5 years (range 12–72 years). All patients underwent conventional liver function tests (serum bilirubin, aspartate aminotransferase, alanine amino- transferase, -glutamyl transpeptidase, alkaline phosphatase), im- munologic screening (indirect hemagglutination, immunoelectro- phoretic assays, histamine release test) and hematologic studies. Plain radiography, abdominal ultrasonography, and computed to- mography scans were routinely performed to evaluate the liver hydatid disease. Endoscopic retrograde cholangiography has been mainly used during the last 10 years. The specific data recorded were related to the presence of referred pain and physical signs, radiographic and echographic findings, symptom duration prior to treatment, indication for surgery, pathologic findings, surgical procedure, and morbidity and mortality if any. Correspondence to: E. Vincente, M.D., e-mail: [email protected]
-
Upload
emilio-vicente -
Category
Documents
-
view
213 -
download
1
Transcript of Management of Biliary Duct Confluence Injuries Produced by Hepatic Hydatidosis

World J. Surg. 25, 1264–1269, 2001DOI: 10.1007/s00268-001-0107-3 WORLD
Journal ofSURGERY© 2001 by the Societe
Internationale de Chirurgie
Management of Biliary Duct Confluence Injuries Produced by HepaticHydatidosis
Emilio Vicente, M.D., Juan C. Meneu, M.D., Pedro L. Hervás, M.D., Javier Nuño, M.D., Yolanda Quijano, M.D.,Manuel Devesa, M.D., Alberto Moreno, M.D., Luis Blazquez, M.D.
General Surgery Department, Liver Transplantation Unit, Ramón y Cajal University Hospital, Alcalá de Henares University, Ctra. Colmenarkm 9’100, Madrid 28034, Spain
Published Online: August 20, 2001
Abstract. From 1978 to 1999 a total of 850 patients underwent surgicaltreatment for hydatid disease of the liver at our surgical department.Biliary duct confluence injuries produced by hepatic hydatidosis (HH)were founded in six patients (0.7%). Surgical intervention was undertakento relieve the obstructive jaundice and clinical manifestations of cholan-gitis and to treat the hydatid cyst. A partially open cystopericystectomytechnique was used in three patients with a double bilioenteric Roux-en-Yreconstruction. The remaining three patients (two with prehepatic portalhypertension and one with triple hepatic duct confluence) were subjectedto a cystojejunostomy. There were no hospital deaths. Two cases ofanastomotic leakage following a high bilioenteric anastomosis occurredbut did not require surgical treatment. During the follow-up (5–19 years)one patient suffered local recurrence of the hydatid disease 7 years aftercystojejunostomy. The site of intrahepatic biliary and vascular involve-ment, the presence of biliary duct anomalies, and the presence of portalhypertension are decisive factors when choosing the “ideal” procedure forreconstruction. Conservative surgical approaches (partial cystectomy andcystojejunostomy) are the treatments of choice. Radical surgery is often aserious matter.
Echinococcus granulosus is the parasite responsible for hydatido-sis. This disease is an important cause of morbidity and mortality,and it increases public health costs in the areas of the world wherethe disease is endemic: South America, Australia, East Africa, andMediterranean countries [1, 2].
Human affectation represents the casual intermediate part ofthe life cycle of this parasite; the intermediate and definitive hostis the dog. The parasite is transported from gut to liver throughthe portal circulation, leading most often to liver damage.
Symptoms of hepatic hydatidosis (HH) are varied. Parasiticcysts may remain silent for long periods of time, sometimes beingdiagnosed when radiology or echography is performed for otherreasons. The volume, localization, and type of cystic complicationare factors causing clinical symptomatology. Bile duct communi-cation, suppuration, and rupture of the cyst into the peritonealcavity through the diaphragm and into a bronchus are the mostfrequent complications of HH [3–7].
Involvement of the biliary duct in patients with HH is well
known. The incidence of intrabiliary rupture varies among studies,from 1% to 17%, owing to different etiologies [8–14]: (1) com-pression of the intra- or extrahepatic biliary tree; (2) biliocysticcommunications that allow the bile to pass to the cyst cavity orfrom the cyst to the biliary duct; and (3) destruction of the hilarconfluence. These biliary complications produce similar clinicalsymptoms: biliary colic, obstructive jaundice, or acute cholangitis.However, the frequency, severity, and surgical technique used fortreatment as well as its complexity if it is done late are different.
Biliary duct confluence injury produced by HH is a rare butserious condition associated with a high morbidity rate with adifficult surgical approach. Few isolated cases have been reported[14, 15], and no series of patients with outcome has been pub-lished. The present work summarizes our experience with themanagement of patients with biliary duct confluence injuries pro-duced by HH over 21 years.
Patients and Methods
From 1978 to 1999 the general surgery department at the Ramóny Cajal Hospital admitted a total of 850 patients suffering fromhydatid disease of the liver who required surgery. Case reportsfrom six patients presenting with destruction of the hilar conflu-ence caused by the parasitic cyst were reviewed. There were threemales and three females whose mean age was 42.5 years (range12–72 years). All patients underwent conventional liver functiontests (serum bilirubin, aspartate aminotransferase, alanine amino-transferase, �-glutamyl transpeptidase, alkaline phosphatase), im-munologic screening (indirect hemagglutination, immunoelectro-phoretic assays, histamine release test) and hematologic studies.Plain radiography, abdominal ultrasonography, and computed to-mography scans were routinely performed to evaluate the liverhydatid disease. Endoscopic retrograde cholangiography has beenmainly used during the last 10 years. The specific data recordedwere related to the presence of referred pain and physical signs,radiographic and echographic findings, symptom duration prior totreatment, indication for surgery, pathologic findings, surgicalprocedure, and morbidity and mortality if any.Correspondence to: E. Vincente, M.D., e-mail: [email protected]

Results
Clinical Symptoms and Diagnosis
All six patients suffered from right upper quadrant abdominalpain; 83% presented with jaundice (5/6) and 66% with a hightemperature (4/6) (Table 1). The average duration of symptomevolution was 4 months (range 1–7 months). Two patients hadundergone previous surgery for HH and pulmonary hydatidosis.
Elevations of the �-glutamyl transpeptidase, alkaline phospha-tase, and serum bilirubin levels were the most important biochem-ical parameter founded in patients with biliary duct confluenceinjuries produced by HH as well as eosinophilia (6/6). Five ofthem had increased serum bilirubin levels and leukocyte counts.
Abdominal ultrasound scanning performed in all patients re-vealed the type of parasitic cyst based on previously establishedechographic patterns [16] together with its anatomic location.Biliary tree involvement was identified by visualization of moder-ate (five patients) or significant (one patient) dilatation of the
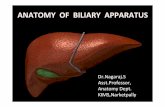
intrahepatic biliary duct. Computed tomography scanning corrob-orated the echographic data, showing in all patients no parasiticdisease in the peritoneal and pleural cavities (Fig. 1). In fourpatients in whom endoscopic retrograde cholangiography wasperformed, intrabiliary rupture of a hydatid cyst was confirmed,although its characteristics and its magnitude were not measur-able. Daughter cysts in the biliary tract were observed in threepatients.
Surgical Technique
Six patients suffered from a hydatid cyst affecting liver segmentsIV and V involving the gallbladder, main extrahepatic biliary duct,and the hilar plate. In three of them there was a significantextrahepatic increase of the parasitic lesion.
Surgery was performed to relieve the obstructive jaundice andclinical manifestations of cholangitis as well as to remove thehydatid cysts. A right subcostal incision running to the left side
Table 1. Patients with biliary confluence injuries produced by hepatic hidatidosis.
Patientno.
Age(years) Clinical presentation Diagnosis Surgery Complication Follow-up
1 47 Abdominal pain, jaundice,fever
US, CT scan,ERCP
Partial cystectomy; double bilioentericRoux-en-Y reconstruction
Biliary leak, subphrenicabscess
Well (7 years)
2 62 Abdominal pain, jaundice US, CT scan,ERCP
Partial cystectomy; double bilioentericRoux-en-Y reconstruction
Biliary leak Well (5 years)
3 29 Abdominal pain, jaundice,fever
US, CT scan,ERCP
Cystojejunostomy None Well (7 years)
4 72 Abdominal pain US, CT scan,ERCP
Cystojejunostomy None Local recurrence(7 years)
5 26 Abdominal pain, jaundice,fever
US, CT scan Partial cystectomy; double bilioentericRoux-en-Y reconstruction
None Well (19 years)
6 12 Abdominal pain, jaundice,Fever
US, CT scan Cystojejunostomy None Well (18 years)
US: ultrasonography; CT: computed tomography; ERCP: endoscopic retrograde cholangiopancreatography.
Fig. 1. Univesicular hydatid cyst localized in the hilum. Note the portal involvement and dilatation of the intrahepatic bile duct.
Vicente et al.: Effect of Hepatic Hydatidosis on Biliary Tract 1265

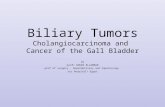
was used in four patients. In the remaining two patients, a midlineincision above and below the umbilicus was the surgical approach.All patients underwent cholecystectomy, intraoperative cholan-giography, and common bile duct exploration (Fig. 2). Liver mo-bilization allowed precise localization of the cyst, recognition of itstight adherence to vasculobiliary structures of the hepatoduode-nal ligament, and control of the liver vascular structures. The cystwas opened owing to its intimate relation to hepatic hilum struc-tures after the surgical field was carefully protected with com-presses soaked in hypertonic sodium chloride solution. The ger-minal layer, daughter cysts, scolices, and bile were removed andaspirated. In all patients, hilar plate destruction was checked byviewing in the cyst cavity the presence of two holes corresponding,respectively, to the right and left hepatic ducts. Intracystic steril-ization was done with hypertonic salt solution or hydrogen per-oxide. The partially open cystopericystectomy technique was usedin three patients, leaving a small portion of the pericyst membraneadherent to the vasculobiliary structures. Once the proximal bili-ary tree was dissected, a double Roux-en-Y bilioenteric recon-struction was carried out on both bile ducts to reestablish biliarydrainage. Anastomosis was achieved by single interrupted sutures5-0 (polyglactin 910; Vicryl) to obtain a mucosa-to-mucosa ap-proximation. In one patient a multiperforated transanastomoticstent was used. In the remaining three patients, who presentedwith significant intrahepatic cyst growth, cystojejunostomy wasperformed with a 60 cm long dysfunctioning enteric loop after itscontent had been emptied. Two patients presented with prehe-patic portal hypertension signs. In one patient intraoperativecholangiography revealed a triple hepatic duct confluence.
Morbidity and Mortality
There were no hospital deaths. Only two surgical complicationsoccurred, consisting in anastomotic leaks following bilioenteric
Roux-en-Y reconstruction. Both fistulas closed spontaneouslywithout surgical treatment. One of these patients later presentedwith a subphrenic abscess that had to be percutaneously drainedunder radiologic control.
Follow-up
Follow-up, which included annual laboratory investigations andultrasonography or computed tomography (or both) ranged from5 to 19 years (median 10 years). One patient who underwentcystojejunostomy 7 years ago suffered local recurrence of thedisease. Surgery was not undertaken because of his advanced agethe absence of symptoms from a hydatid recurrence, and his poorclinical situation. He was treated with albendazole. The remainingpatient is asymptomatic, without recurrence of the parasitic dis-ease.
Discussion
Surgery remains the treatment of choice for HH. The technicalprocedures reported are conservative (marsupialization, simpleexternal tube drainage, resection of the prominent part of the cyst,partial cystectomy, cystojejunostomy) or radical (total cystoperi-cystectomy, liver resection) [10]. Some authors choose conserva-tive procedures because they believe that radical surgery is dis-proportionate and presents high risks for treating a benign disease[17–19]. In contrast those who defend radical procedures arguethat it is necessary to try to avoid postsurgical complicationsderived from pericystic disease close to the hepatic parenchyma(abscess, chronic suppuration, late biliary leakage) and to reducethe length of hospital stay [7, 20, 21]. The cornerstone of bothforms of treatment are similar: neutralize and eliminate the par-asite, treat the residual cavity, and reestablish biliary drainagewhen it is affected by cystic injury [16–22].
Fig. 2. Intraoperative cholangiography showing bile duct confluence injuries produced by hepatic hydatidosis.
1266 World J. Surg. Vol. 25, No. 10, October 2001

During the last three decades the surgical treatment of hepaticpathology went through an important transformation. Refinementof operative techniques and postoperative patient care have maderadical surgery a procedure of choice for patients with HH [7, 21].Complete extirpation of the cyst content and avoiding pericysticadherence to hepatic parenchyma have been associated with ex-cellent results and minimal surgical risk. The use of normothermicischemia techniques for cyst resection makes the dissection easierand reduces intraoperative blood loss [23]. However, this radicalprocedure is conditioned by the number of cysts, their complica-tions, and mainly the degree of their vasculobiliary involvement.
If clinical symptomatology due to a biliary complication sec-ondary to HH is present, it is necessary to know the characteristicsof the type of biliocystic communication prior to surgery. Com-puted tomography of the abdomen and ultrasonography are re-quired for a precise preoperative diagnosis of the HH. However,other diagnostic studies are advisable to delimit the biliary ductmorphology. The technique of choice is endoscopic retrogradecholangiography [24–26], which gives excellent information aboutthe hydatid content of the bile duct. In patients suffering fromobstructive jaundice it permits evacuatetion of the hydatid mate-rial out of the bile duct, thereby avoiding the development ofcholangitis. However, endoscopic retrograde cholangiography hasnot been efficient in our experience for preoperative diagnosis ofbiliary duct confluence injuries produced by HH. The proximallocalization of biliary involvement and the cyst itself make itdifficult to fill both hepathic ducts, and consequently it does notpermit precise evaluation of the alteration. Another techniquethat offers excellent information on intrahepatic biliary tree mor-phology and the biliary area is percutaneous transhepatic cholan-giography, although it is not indicated in patients with HH be-cause of the risk of puncturing the hydatid cyst and producingsecondary peritoneal hydatid disease through dissemination of itscontent [26].
Patients with biliary complications caused by a ruptured hydatidcyst require careful intraoperative radiologic study, including cho-lecystectomy and cholangiography through the cystic duct or com-mon bile duct [26]. In patients with hilar confluence destruction,radiologic evaluation can be performed after the cyst has beenopened. Through cannulation of both bile ducts emptying in thecyst cavity, we can learn about the anatomy and state of theintrahepatic biliary tree.
Hydatid cysts producing hilar lesions were located on liversegments IV and V with variable intrahepatic or extrahepaticgrowth. In all the cases we studied, the cysts had a calcified, rigidadventitia. The loss of elasticity is probably responsible for de-struction of the bifurcation of both hepatic ducts through a me-chanical-compressive action. With these local characteristics, wehypothesize that toxic action would play a more secondary role inthe genesis of biliary complication.
The intimal relation of the hydatid cyst with hilar structuresoccasionally leads to alteration of portal venous flow with prehe-patic portal hypertension [7]. Two of our patients were diagnosedwith such an alteration through preoperative echographic detec-tion of a dilatation of the porta vein and the presence of animportant collateral circulation and splenomegaly. Such a diag-nosis, intraoperatively confirmed, caused difficult cyst dissection.
Among the various effects on the bile duct by HH, destructionof the hilar confluence is least frequent but the one that presentsthe most technical difficulty. The local difficulties determine
whether biliary drainage can be reestablished. Its failure withpersistent cholestasis causes irreversible functional hepatic dam-age whose only solution may be liver transplantation [27].
The technical procedures to be performed in patients sufferingfrom such a complicated biliary disease are as follows from high tolow radicality: (1) total cystopericystectomy, preferably with theopen approach because of the vascular proximity, with bilioentericdrainage upon well vascularized bile ducts; (2) partial cystectomywith bilioenteric Roux-en-Y reconstruction of bile ducts sur-rounded by hydatid pericysts; and (3) cystojejunostomy. Two im-portant factors must be considered prior to choosing the surgicaltechnique: (1) If there is firm adherence of the cyst to vasculo-biliary structures of the hepatic hilum; and (2) the patient’s biliaryanatomy. Normally, the consistency of the cystic wall makes dis-section of the adjacent hepatic parenchyma easier, as does theidentification, liberation, and ligature of the biliary vessels andducts that closely adhere to them. However, in these patientsbiliary destruction and vascular compression due to the cyst makesthe dissection difficult and markedly increases the risk of massivehemorrhage and consequently the surgical risk. Such a risk ismuch more important in patients with prehepatic portal hyper-tension. The second aspect to be taken into acocunt is the fre-quent variations from normal biliary anatomy; the right and lefthepatic ducts join to form the biliary confluence in only 57% [28]and 72% [29] of cases, respectively. A large number of abnormal-ities have been described [28, 29]. Prior to radical surgery inpatients with hilar plate destuction by HH, it is necessary to knowthe variations of the hepatic duct confluence and the intrahepaticductal system, especially for cysts presenting with extensive intra-hepatic growth. Hence intraoperative cholangiography must beperformed to avoid intrapperative lesions and to evaluate the riskof the biliary reconstruction, which depends on the number ofbiliary canaliculi existing after cyst resection and consequently thenumber of bilioenteric anastomoses to be achieved. Sometimes,multiple biliary-enteric anastomoses between segmental hepaticducts and a Roux-en-Y jejunal loop are required to make drain-age of all the liver segments easier.
For the reasons previously described, radical surgery is often aserious matter in patients with biliary duct confluence injuries.Similar to what occurs during surgical treatment of patients suf-fering from benign biliary strictures [30], the viability of thereconstruction is closely related to the possibility of performing atension-free bilioenteric anastomosis in a well vascularized bileduct.
Controversy continues about the use and length of stentingduring intrahepatic cholangiojejunostomy [31–33]. In our opinion,no transanastomotic stent is needed if a wide, technically correctanastomosis is performed: direct mucosa-to-mucosa approxima-tion [34], including patients in whom a small part of the cyst wallshould be left around the bile ducts. If not, a silicone stent shouldbe positioned and maintained postoperatively for 3 months.
Cystojejunostomy is a conservative procedure formerly em-ployed to treat of hilar hydatid cysts affecting the bile duct con-fluence [35]. In our opinion, it is especially indicated for: (1) hilarcysts with extensive intrahepatic growth where there is suspicionor radiologic confirmation of the injury not only of the hilarplaque but of the proximal part of the intrahepatic ductal systemas well; (2) patients with biliary anomalies in whom biliary drain-age reestablishment requires various bilioenteric anastomoses;and (3) patients with prehepatic portal hypertension. Our results
Vicente et al.: Effect of Hepatic Hydatidosis on Biliary Tract 1267

with long-term follow-up confirm that such a technique occupiesa privileged place in the treatment of such a disease.
For all the reasons previously mentioned, we think that themorbidity and prognosis for patients operated on for destructionof hilar plaque caused by HH are related to various factors: thesite of intrahepatic biliary and vascular involvement, biliary ductanomalies, the presence of portal hypertension, choice of the bestprocedure for reconstruction, and the surgeon’s experience withliver surgery.
Conclusions
Hilar lesions produced by HH represent a severe health problem.Correct pre- and intraoperative assessment of the variation of thehepatic duct confluence and intrahepatic duct system togetherwith the extent of the vasculobiliary involvement lead to thechoice of an adequate surgical procedure. The results of ourexperience indicate that these patients can be treated successfullywith conservative surgical procedures. Even with severe hydatidcomplications, radical surgery is rarely needed.
Résumé
Entre 1978 et 1999, 850 patients ont eu une chirurgie pour kystehydatique du foie dans notre département de chirurgie. On atrouvé des lésions du confluent biliaire secondaires à l’hydatitosehépatique (HH) chez six patients (0,7%). Une interventionchirurgicale a été réalisée pour soulager l’ictère et lesmanifestations cliniques de cholangite ainsi que pour traiter lekyste hydatique. On a réalisé une périkystectomie partielle cheztrois patients avec une reconstruction bilioentérique double paranse-en-Y. Chez les trois autres patients, deux avec unehypertension portale préhépatique, et un avec un confluenthépatique triple, on a réalisé une anastomose cystojéjunale. II n’ya eu aucune mortalité hospitalière. On a observé deux fistulesanastomotiques après anastomose bilioentérique haute mais quine nécessitaient pas de traitement supplémentaire. Pendant lesuivi (5 à 19 ans), un patient a eu une récidive locale de sa maladiehydatique sept ans après la construction d’une anastomosecystojéjunale. Le site de l’envahissement intrahépatique etvasculaire, la présence d’anomalies de l’anatomie biliaire et laprésence d’hypertension portale sont des facteurs décisifs dans lechoix du procédé “idéal” de reconstruction. L’approchechirurgicale conservatrice (cystectomie partielle et anastomosecystojéjunale) occupe une place de choix. La chirurgie radicale estsouvent d’un pronostic plus réservé.
Resumen
Entre 1978 y 1999 se operaron 850 pacientes con enfermedadhidatídica del hígado en nuestro Departamento de Cirugía. Seregistró lesión de la confluencia de los canales hepáticosproducida por la hidatidosis hepática (HH) en 6 pacientes (0.7%).Se practicó intervención quirúrgica para control de la ictericiaobstructiva y de las manifestaciones clínicas de colangitis ytratamiento del quiste hidatídico. Se realizó cistopericistectomíaparcialmente abierta con reconstrucción bilioentérica de Roux-en-Y, en 3 pacientes. En los pacientes restantes, 2 conhipertensión portal pre-hepática y 1 con una confluencia triple delos canales hepáticos, se practicó cistoyeyunostomía. No hubo
mortalidad operatoria. Se presentaron dos casos de fugaanastomótica luego de anastomosis bilioentérica alta, los cualesno requirieron tratamiento quirúrgico. En el curso delseguimiento (5 a 19 años), 1 paciente desarrolló recurrencia de laenfermedad hidatídica a los 7 años de la cistoyeyunostomia. Elsitio de la afección biliar y vascular intrahepática, la presencia deanomalías de la vía biliar y la presencia de hipertensión portalconstituyen factores decisorios para la escogencia delprocedimiento ideal de reconstrucción. Los procedimientosquirúrgicos conservadores (cistectomía parcial ycistoyeyunostomía) ocupan el primer lugar. La cirugía radicalgeneralmente debe ser considerada como materia muy seria.
Acknowledgments
This work was supported by the Foundation for Liver Transplan-tation Development.
References
1. Williams, J.F., Lopez-Aderas, H., Trejar, A.: Current prevalence anddistribution of hydatidosis with special reference to the Americas. Am.J. Trop. Med. Hyg. 20:224, 1971
2. Matossian, R.M., Riickard, M.D., Smyth, J.D.: Hydatidosis: a globalproblem of increasing importance. Bull. W.H.O. 55:499, 1977
3. Barros, J.L.: Hydatid disease of the liver. Am. J. Surg. 135:597, 19784. Hankins, J.R.: Management of complicated hepatic hydatid cysts.
Ann. Surg. 158:1020, 19635. Yacoubian, H.D.: Thoracic problems associated with hydatid cyst of
the dome of the liver. Surgery 79:544, 19766. Kattan, Y.B.: Intrabiliary rupture of hydatid cyst of the liver. Br. J.
Surg. 62:885, 19757. Moreno Gonzalez, E., Rico Selas, P., Bercedo Martinez, G.,
García García, I., Palma Carazo, F., Hidalgo Pascual, M.: Results ofsurgical treatment of hepatic hydatidosis: current therapeutic modifi-cations. World J. Surg. 15:254, 1991
8. Sayek, I., Yalin, R., Sanac, Y.: Surgical treatment of hydatid disease ofthe liver. Arch. Surg. 115:847, 1980
9. Dugalic, D., Djukic, V., Milicevic, M., Sterovic, D., Knezevic, J.,Pantic, J.: Operative procedures in the management of liver hydatid-osis. World J. Surg. 6:115, 1982
10. Dadoukis, J., Gamvros, O., Aletras, H.: Intrabiliary rupture of thehydatid disease of the liver. World J. Surg. 8:786, 1984
11. Langer, J.C., Rose, D.B., Keystone, J.S., Taylor, B.R., Langer, B.:Diagnosis and management of hydatid cysts of the liver: a 15-yearNorth American experience. Ann. Surg. 199:412, 1983
12. Lygidakis, N.J.: Diagnosis and treatment of intrabiliary rupture ofhydatid cyst of the liver. Arch. Surg. 118:1186, 1983
13. Ornat, A., Peiser, J., Arinoah, E., Barki, Y., Charuzi, I.: Acute cholan-gitis caused by ruptured hydatid cyst. Surgery 95:497, 1984
14. Soleto, E.: Destruction du confluent biliare par kyste hydatique dufoie. J. Chir. (Paris) 127:561, 1990
15. Martin Molinero, R., Placer Galan, C., Jimenez Garrido, M.,Soleto Saez, E.: Kyste hydatique hepatic qui detruisait le confluencebiliaire. J. Chir. (Paris) 126:672, 1989
16. Bezzi, M., Teggi, A., De Rosa, F., Capozzi, A., Tucci, G.,Bonifacino, A., Angelini, L.: Abdominal hydatid disease: US findingsduring medical treatment. Radiology 162:91, 1987
17. Ekram, Y.: Surgical treatment of hydatid disease of the liver. Arch.Surg. 3:1350, 1976
18. Mottaghian, H., Saidi, F.: Post-operative recurrence of hydatid dis-ease. Br. J. Surg. 65:237, 1978
19. Littele, J.M., Holland, M.J., Ekberg, H.: Recurrence of hydatid dis-ease. World J. Surg. 12:700, 1988
20. Demirci, S., Eraslan, S., Anadol, E., Bozatli, L.: Comparison of theresults of different surgical techniques in the management of hydatidcysts of the liver. World J. Surg. 13:88, 1989
21. Alfieri, S., Doglietto, G.B., Pacelli, F., Costamagna, G., Carviero, C.,
1268 World J. Surg. Vol. 25, No. 10, October 2001

Mutignani, M., Liberatori, M., Crucitti, F.: Radical surgery for liverhydatid disease: a study of 89 consecutive patients. Hepatogastroen-terology 44:496, 1997
22. Ulnalp, K.M., Aydemir, I., Santurk, H., Eyuboglu, E., Cebeci, H.,Unal, G., Unal, H.: Management of intrabiliary rupture of hydatid cystof the liver. World J. Surg. 19:720, 1995
23. Belli, L., Aseni, P., Roudinava, G.F., Bertin, M.: Improved results withpericystectomy in normothermic ischemia for hepatic hydatidosis.Surg. Gynecol. Obstet. 163:127, 1986
24. Cottone, M., Amuso, M., Cotton, B.P.: Endoscopic retrograde cholan-giopancreatography in hepatic hydatid disease. Br. J. Surg. 65:107,1978
25. Shemesh, E., Friedmen, E.: Radiologic and endoscopic appearance ofintrabiliary rupture of hydatid liver disease. Digestion 36:96, 1987
26. Fresneda, V., Vicente, E.: Acute cholangitis caused by ruptured hy-datid cyst. Surgery 97:241, 1985
27. Moreno-Gonzalez, E., Loinaz, C., García, M.A., García, I.,Gómez, R., Jimenez, C., Gonzalez, I., Corral, M.A., Palma, F.: Livertransplantation for Echinococcus granulosus hydatid disease. Trans-plantation 58:797, 1994
28. Couinaud, C.: Le Foie. Etudes Anatomiques et Chirurgicales, vol 1.,Paris, Masson, 1957
29. Healey, J.E., Schroy, P.C.: Anatomy of the biliary ducts within thehuman liver: analysis of the prevailing pattern of branchings and themajor variations of the biliary ducts. Arch. Surg. 66:599, 1953
30. Terblanche, J., Allison, H.F., Northover, J.M.A.: An ischemic basis forbiliary strictures. Surgery 94:52, 1983
31. Pellegrini, C.A., Thomas, M.J., Way, L.W.: Recurrent biliary stricture:patterns of recurrence and outcome of surgical therapy. Am. J. Surg.147:175, 1984
32. Blumgart, L.H., Kelley, C.J.: Hepaticojejunostomy in benign and ma-lignant stricture: approaches to the left hepatic ducts. Br. J. Surg.71:257, 1984
33. Pitt, H.A., Kaufman, S.L., Coleman, J., White, R.I., Cameron, J.L.:Benign postoperative biliary strictures: operate or dilate? Ann. Surg.210:417, 1989
34. Smith, R.: Strictures of the bile ducts. Proc. R. Soc. Med. 62:131, 196935. Pegullo, J., Pelissier, G.: Place de la jysto-jejunostomie dans le trait-
ment du kyste hidatique du foie Ann. Chir. 14:577, 1960
Vicente et al.: Effect of Hepatic Hydatidosis on Biliary Tract 1269