Management in Parkinson’s Disease - Khon Kaen University€¦ · Management in Parkinson’s...
143
Management Management in in Parkinson Parkinson ’ ’ s s Disease Disease Apichart Pisarnpong Apichart Pisarnpong , , M M . . D D . . Director of Parkinson Director of Parkinson ’ ’ s Disease Clinic, s Disease Clinic, Siriraj Hospital, Siriraj Hospital, Mahidol Mahidol University University
Transcript of Management in Parkinson’s Disease - Khon Kaen University€¦ · Management in Parkinson’s...

Management Management inin
ParkinsonParkinson’’s s DiseaseDisease
Apichart PisarnpongApichart Pisarnpong,, MM..DD..Director of ParkinsonDirector of Parkinson’’s Disease Clinic, s Disease Clinic,
Siriraj Hospital, Siriraj Hospital, MahidolMahidol UniversityUniversity

overviewoverview
History of ParkinsonHistory of Parkinson’’s Diseases DiseaseClinical manifestation of PDClinical manifestation of PDEtiology and secondary cause of ParkinsonismEtiology and secondary cause of ParkinsonismClassification Classification Treatment : Treatment :
medical medical surgical (new in Thailand)surgical (new in Thailand)
Late complications (motor VS nonLate complications (motor VS non--motor)motor)

overviewoverview
History of ParkinsonHistory of Parkinson’’s Diseases DiseaseClinical manifestation of PDClinical manifestation of PDEtiology and secondary cause of ParkinsonismEtiology and secondary cause of ParkinsonismClassification Classification Treatment : Treatment :
medical medical surgical (new in Thailand)surgical (new in Thailand)
Late complications (motor VS nonLate complications (motor VS non--motor)motor)

History History
18171817: : James Parkinson James Parkinson ““An Essay on the Shaking PalsyAn Essay on the Shaking Palsy””
Almost 200 years agoAlmost 200 years ago
ในประเทศไทยเคยเรียกวาในประเทศไทยเคยเรียกวา ““สันนบิาตลูกนกสันนบิาตลูกนก””




ParkinsonParkinsonประยงคประยงค 44 44--014918.mpg014918.mpg

1961 using IV levodopa to treat PD patients 1961 using IV levodopa to treat PD patients 1966 combine with Decaboxylase inhibitor 1966 combine with Decaboxylase inhibitor (benzerazide) less side effect and more potent(benzerazide) less side effect and more potent

Pathology of ParkinsonPathology of Parkinson’’s Diseases Disease

Normal Basal Ganglia Functional Normal Basal Ganglia Functional AnatomyAnatomy
Cortex
PrefrontalInsular
CingulateSensoryMotor
Suppl. MotorPremotor
PremotorPrefrontal
Striatum
D2 D1ThalamusVA/VL
+ = excitatory- = inhibitory
BrainstemSC
SNc
SNr
GPi
STN
GPe
-
+
+
+-
-
---
-
+
++
+
+
+
Normal

Function Anatomy of ParkinsonFunction Anatomy of Parkinson’’s s DiseaseDisease
Cortex
PrefrontalInsular
CingulateSensoryMotor
Suppl. MotorPremotor
PremotorPrefrontal
Striatum
D2 D1ThalamusVA/VL
+ = excitatory- = inhibitory
BrainstemSC
SNc
SNr
GPi
STN
GPe
-
-
++
++++
-
-----
+
++
+
+
+ - -
Parkinson’s Disease

Cortex
PrefrontalInsular
CingulateSensoryMotor
Suppl. MotorPremotor
PremotorPrefrontal
Striatum
D2 D1ThalamusVA/VL
+ = excitatory- = inhibitory
BrainstemSC
SNc
SNr
GPi
STN
GPe
-
+
+
+-
-
---
-
+
++
+
+
+
NormalCortex
PrefrontalInsular
CingulateSensoryMotor
Suppl. MotorPremotor
PremotorPrefrontal
Striatum
D2 D1ThalamusVA/VL
+ = excitatory- = inhibitory
BrainstemSC
SNc
SNr
GPi
STN
GPe
-
-
++
++++
-
-----
+
++
+
+
+ - -
Parkinson’s Disease

overviewoverview
History of ParkinsonHistory of Parkinson’’s Diseases Disease
Clinical manifestation of PDClinical manifestation of PDEtiology and secondary cause of ParkinsonismEtiology and secondary cause of ParkinsonismClassification Classification Treatment : Treatment :
medical medical surgical (new in Thailand)surgical (new in Thailand)
Late complications (motor VS nonLate complications (motor VS non--motor)motor)

Signs and SymptomsSigns and Symptoms
Cardinal CharacteristicsCardinal Characteristics
Resting tremorResting tremor
BradykinesiaBradykinesia
RigidityRigidity
Later; Postural instability (3Later; Postural instability (3--5 years after 5 years after Dx)Dx)
Gait disturbance esp. dystonic posture of Gait disturbance esp. dystonic posture of feet, fluctuation of symptoms (YOPD)feet, fluctuation of symptoms (YOPD)

Additional Signs and SymptomsAdditional Signs and Symptoms
Difficulty arising from a chairDifficulty arising from a chair
Difficulty turning in bedDifficulty turning in bed
Hypophonic speechHypophonic speech
SialorrheaSialorrhea
Loss of the sense of smellLoss of the sense of smell
Foot dystoniaFoot dystonia

OtherOther
MicrographiaMicrographia
Masked faceMasked face
Slowing of ADLsSlowing of ADLs
Stooped, shuffling gaitStooped, shuffling gait
Decreased arm swing when walkingDecreased arm swing when walking

Clues Suggesting Clues Suggesting Atypical ParkinsonismAtypical Parkinsonism
Early onset Early onset ““offoff””, or rapidly progressing , or rapidly progressing dementiadementia
Rapidly progressive courseRapidly progressive course
Supranuclear gaze palsySupranuclear gaze palsy
Upper motor neuron signsUpper motor neuron signs
Cerebellar signsCerebellar signs——dysmetria, ataxiadysmetria, ataxia
Urinary incontinenceUrinary incontinence
Early symptomatic postural hypotensionEarly symptomatic postural hypotension


Criteria for DiagnosisCriteria for Diagnosis
At least two of three: At least two of three: rest tremor, bradykinesia, rigidityrest tremor, bradykinesia, rigidity
Absence of a secondary cause; drugs, Absence of a secondary cause; drugs, metabolic, etc.metabolic, etc.Definitive diagnosis can only be made Definitive diagnosis can only be made by autopsyby autopsy

overviewoverview
History of ParkinsonHistory of Parkinson’’s Diseases DiseaseClinical manifestation of PDClinical manifestation of PD
Etiology and secondary cause of Etiology and secondary cause of ParkinsonismParkinsonismClassification Classification Treatment : Treatment :
medical medical surgical (new in Thailand)surgical (new in Thailand)
Late complications (motor VS nonLate complications (motor VS non--motor)motor)

Cause of PDCause of PD
Unknown in most casesUnknown in most cases
10% associated with genetic10% associated with genetic

ParkinsonParkinson’’s Disease s Disease Risk FactorsRisk Factors
DefiniteDefinite: Old age: Old ageHighly likelyHighly likely: MZ co: MZ co--twin with earlytwin with early--onset PDonset PDProbableProbable: Positive family history: Positive family historyPossiblePossible: Herbicides, pesticides, heavy metals, proximity : Herbicides, pesticides, heavy metals, proximity to industry, rural residence, well water, repeated head to industry, rural residence, well water, repeated head trauma, etc.trauma, etc.Possible protective effectPossible protective effect: Smoking: Smoking

overviewoverview
History of ParkinsonHistory of Parkinson’’s Diseases DiseaseClinical manifestation of PDClinical manifestation of PDEtiology and secondary cause of PDEtiology and secondary cause of PD
Classification Classification Treatment : Treatment :
medical medical surgical (new in Thailand)surgical (new in Thailand)
Late complications (motor VS nonLate complications (motor VS non--motor)motor)

Parkinsonian syndromeParkinsonian syndrome
Classification Classification 1.1. Idiopathic ParkinsonIdiopathic Parkinson’’s Diseases Disease2.2. Secondary ParkinsonismSecondary Parkinsonism3.3. Parkinson Plus syndromeParkinson Plus syndrome4.4. Associated diseaseAssociated disease

2. 2. SecondarySecondary ParkinsonismParkinsonism
DrugDrug--inducedinducedToxinToxin--inducedinducedMetabolicMetabolicStructural lesions Structural lesions HydrocephalusHydrocephalusInfectionInfection

DrugDrug--Induced ParkinsonismInduced Parkinsonism
Antipsychoticshaloperidol, chlorpromazine, thioridizine, perphenazinerisperidone, olanzapine
Antiemeticsmetoclopramide, prochlorperazine

DrugDrug--Induced ParkinsonismInduced Parkinsonism
Dopamine depletorsmethyldopa, reserpine, tetrabenazine
Antivertigo medicationsCa Channel blockers: flunarizine, cinnerizine
Treatment: Stop offending medicationsTreatment: Stop offending medications

Metabolic Causes of Parkinsonism Metabolic Causes of Parkinsonism
MetabolicOften reversibleHypo- or hyper-thyroidismHypo- or hyper-parathyroidismLiver failureCentral pontine myelinolysis

Infectious Causes of ParkinsonismInfectious Causes of Parkinsonism
InfectiousInfectiousPostPost--encephaliticencephaliticCreutzfeldtCreutzfeldt--Jakob diseaseJakob diseaseInfectious massesInfectious massesHIVHIV

ToxinToxin--induced Parkinsonisminduced Parkinsonism
MPTPMPTPCarbon monoxideCarbon monoxideManganeseManganeseCyanideCyanide

Structural Lesions Causing ParkinsonismStructural Lesions Causing Parkinsonism
Acute or subacute onsetAcute or subacute onsetOther signsOther signs——hemiparesis, hyperreflexia, hemiparesis, hyperreflexia, aphasia, sensory loss, seizuresaphasia, sensory loss, seizuresBrain tumorBrain tumorInfectious massInfectious massAneurysmAneurysm

Vascular ParkinsonismVascular Parkinsonism
Abrupt onset, usually unilateralAbrupt onset, usually unilateralStepStep--wise or no progressionwise or no progressionOther signsOther signs——hemiparesis, aphasia, hyperreflexiahemiparesis, aphasia, hyperreflexiaInfarcts on neuroimaging helpful in confirming Infarcts on neuroimaging helpful in confirming diagnosisdiagnosis

HydrocephalusHydrocephalus--induced Parkinsonisminduced Parkinsonism
Can be communicating or obstructiveNormal pressure hydrocephalus—idiopathicClinical triad:
parkinsonism/gait disorderurinary/fecal incontinencedementia

3. Parkinson Plus Syndrome
Progressive supranuclear palsyProgressive supranuclear palsyMultiple system atrophyMultiple system atrophyCorticobasal ganglia degenerationCorticobasal ganglia degenerationDiffused Lewy body diseaseDiffused Lewy body diseaseParkinsonParkinson--dementia complex dementia complex syndromesyndrome

4 Associated disease4 Associated disease
Essential tremorEssential tremorAlzheimerAlzheimer’’s diseases disease

Classification Classification by age of onsetby age of onset
JuvenileJuvenile--onsetonsetAge of onset less than Age of onset less than 2121 years oldyears old
YoungYoung--onsetonsetAge onset less than Age onset less than 4040 years old years old but but moremore thanthan 2121 years years ololdd

Mean age of onset 60 to 65 yr.Mean age of onset 60 to 65 yr.55--10% start below age of 40 yr.10% start below age of 40 yr.
Incidence about 200Incidence about 200--250 : 100,000 in normal 250 : 100,000 in normal population in developed countrypopulation in developed country
Estimate >100,000 PD patients in ThailandEstimate >100,000 PD patients in Thailand

Siriraj Parkinson's Disease Clinic Jan 2000- June 2002
242 medical recordswere enrolled
224 were reviewed 18 were excluded due to incomplete data
174 medical recordsof IPD 50 medical records
of other diagnosis
Statistical analysisand reported

Demographic dataDemographic data
Sex: Sex: 98 males 98 males (56.3%)(56.3%)76 females 76 females (43.7%)(43.7%)M : F = 1.29 : 1M : F = 1.29 : 1
Age of onset : 12Age of onset : 12--90 y (mean 55.6 y)90 y (mean 55.6 y)age > 40 yr age > 40 yr = 82.3% = 82.3% age 20age 20--40 yr 40 yr = 15.9%= 15.9%age < 20 yr age < 20 yr = 1.8% = 1.8% (age < 40 yr (age < 40 yr = 17.7%)= 17.7%)

Modified Hoehn and Yahr Modified Hoehn and Yahr Clinical staging of PDClinical staging of PD
StageStage00 no signs of diseaseno signs of disease11 Unilateral diseaseUnilateral disease1.51.5 Unilateral plus axial involvementUnilateral plus axial involvement2 2 Bilateral disease, without impairment of balanceBilateral disease, without impairment of balance2.52.5 Mild Bilateral disease, with recovery on pull testMild Bilateral disease, with recovery on pull test33 Mild to moderate bilateral disease: some postural instability: Mild to moderate bilateral disease: some postural instability:
physical independentphysical independent44 Severe disability: still able to walk or stand unassistedSevere disability: still able to walk or stand unassisted55 Wheelchair bound or bedridden unless aided Wheelchair bound or bedridden unless aided


Current concept in treating PDCurrent concept in treating PD(continuous dopaminergic (continuous dopaminergic
stimulation)stimulation)
Tonic and continuous dopaminergicstimulation occurs in normal
circumstances

Pulsatile dopaminergic stimulationPulsatile dopaminergic stimulation
promote more dopaminergic cell lost promote more dopaminergic cell lost (post synaptic change) resulting in (post synaptic change) resulting in
development of motor fluctuation and development of motor fluctuation and dyskinesia dyskinesia
((Mouradian MM. pathogenesis of dyskinesia in ParkinsonMouradian MM. pathogenesis of dyskinesia in Parkinson’’s Disease. Ann neurol 1989)s Disease. Ann neurol 1989)

Lost of striatal dopamine receptor that occurs Lost of striatal dopamine receptor that occurs with disease progression results in a diminished with disease progression results in a diminished capacity of these terminal to buffer in capacity of these terminal to buffer in fluctuation in plasma levodopafluctuation in plasma levodopa
Continuous delivery of dopaminergic agents can Continuous delivery of dopaminergic agents can prevent or attenuate the development of prevent or attenuate the development of
dyskinesiadyskinesia

Motor complications associated with levodopa Motor complications associated with levodopa therapy include motor fluctuations and therapy include motor fluctuations and dyskinesia aredyskinesia areparticular problems in younger patientsparticular problems in younger patientsLess likely to occur in those whose symptoms Less likely to occur in those whose symptoms begin after the age of 70 years begin after the age of 70 years
(Golbe LI, neurology 1991, Quinn N, Mov Disord 1987)(Golbe LI, neurology 1991, Quinn N, Mov Disord 1987)

overviewoverview
History of ParkinsonHistory of Parkinson’’s Diseases DiseaseClinical manifestation of PDClinical manifestation of PDEtiology and secondary cause of ParkinsonismEtiology and secondary cause of ParkinsonismClassification Classification
Treatment : Treatment : medical medical
surgical (new in Thailand)surgical (new in Thailand)Late complications (motor VS nonLate complications (motor VS non--motor)motor)

When to start treatmentWhen to start treatmentDetermine whether the patients haveDetermine whether the patients havefunctional impairment or notfunctional impairment or not
1.1. Whether the symptoms effect the dominant or nonWhether the symptoms effect the dominant or non--dominant handdominant hand
2.2. Whether the patient is employed or employableWhether the patient is employed or employable3.3. The type of parkinsonian symptoms that are present The type of parkinsonian symptoms that are present
(e.g. bradykinesia tends to be more disabling than (e.g. bradykinesia tends to be more disabling than tremor)tremor)
4.4. Individual patient sentimentIndividual patient sentiment5.5. The philosophy of treating physicianThe philosophy of treating physician

Symptomatic treatmentSymptomatic treatment
1.1. LevodopaLevodopa2.2. Dopamine agonistDopamine agonist3.3. COMT inhibitorCOMT inhibitor4.4. MAOMAOBB inhibitorinhibitor5.5. AnticholinergicAnticholinergic6.6. AmantadineAmantadine

Sites of action for two types of Sites of action for two types of medical therapies to treat PDmedical therapies to treat PD

Decision tree for early management of PDDecision tree for early management of PDAmerican Academy of Neurology, 2001American Academy of Neurology, 2001
Olanow CW et al. Neurology. 2001:56(suppl 5):S4.

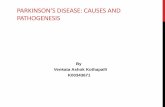
LevodopaLevodopa
MostMost effectiveeffective symptomatically symptomatically antiparkinsonian drugantiparkinsonian drugAll PD patients respondAll PD patients respondImproves disability and prolongs capacity Improves disability and prolongs capacity to maintain employment and independent to maintain employment and independent activities of daily livingactivities of daily livingimproveimprovess mortality ratemortality rate

0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16
Control Group
Years after 1st presentation
Per
cent
Sur
viva
l
P < 0.0001 with control group
P = 0.024 with treated group
Levodopa treated Group N = 565
Levodopa non-treated Group N = 215
P < 0.0292 with control group
Adapt from A.H. Rajput/ Parkinson and related Disorders 8 (2001) 95-100
Levodopa prolongs life expectancy Levodopa prolongs life expectancy and nonand non--toxic to sunstantia nigratoxic to sunstantia nigra

Is Levodopa Toxic?Is Levodopa Toxic?
Early patients develop motor fluctuations, but may be a Early patients develop motor fluctuations, but may be a function of neuronal cell lossfunction of neuronal cell lossIncreased life expectancy with LD introduction Increased life expectancy with LD introduction LDLD--naive advanced PD patients develop fluctuations naive advanced PD patients develop fluctuations almost immediately with LD inductionalmost immediately with LD inductionNo LD neuronal dropout in laboratory animalsNo LD neuronal dropout in laboratory animalsRecent data suggest possible neuroprotectionRecent data suggest possible neuroprotectionSome believe continuous infusion may be safer than Some believe continuous infusion may be safer than pulsatile therapypulsatile therapy

ELLDOPA studyELLDOPA study
360 never360 never--treated PD patients randomized to treated PD patients randomized to placebo or carbidopa/levodopa (37.5/150, placebo or carbidopa/levodopa (37.5/150, 75/300, 150/600 mg/day)75/300, 150/600 mg/day)No evidence that levodopa had any deleterious No evidence that levodopa had any deleterious effect on disease progression and failed to effect on disease progression and failed to support the notion of levodopa toxicitysupport the notion of levodopa toxicityLevodopa is not harmful to Levodopa is not harmful to SNcSNc neuron in PDneuron in PD

LevodopaLevodopa--Induced DyskinesiasInduced Dyskinesias
Manifestation of excessive dopaminergic stimulationManifestation of excessive dopaminergic stimulationTypically late effect, and with higher dosesTypically late effect, and with higher dosesNarrowing of therapeutic windowNarrowing of therapeutic windowRare in LDRare in LD--naive patients on DA monotherapy naive patients on DA monotherapy Most common is Most common is ““peak dosepeak dose”” dyskinesiadyskinesia
disappears with dose reductiondisappears with dose reduction
Choreiform, ballistic and dystonic movementsChoreiform, ballistic and dystonic movementsMost patients prefer some dyskinesias over the Most patients prefer some dyskinesias over the alternative of akinesia and rigidityalternative of akinesia and rigidity

Levodopa/Carbidopa FormulationsLevodopa/Carbidopa Formulations
Onset DurationImmediate Release 20-40 min 2-4 hr10/100, 25/100, 25/250
Controlled Release 30-60 min 3-6 hr25/100, 50/200
“Fast acting” 10-20 min 0.5-1 hr(dissolved tablets)

Levodopa taking alone without DDC Levodopa taking alone without DDC inhinh. only 1 . only 1 % reach the brain% reach the brainWith DDC With DDC inhinh. 10% reach the brain. 10% reach the brain

Prospective, double blind trial in 618 Prospective, double blind trial in 618 levodopalevodopa--nanaïïve patientsve patients
sustainedsustained--release Sinemetrelease Sinemetintermidiateintermidiate--release Sinemetrelease Sinemet
After 5 years there is no difference in the prevalence After 5 years there is no difference in the prevalence of motor complications between two groupsof motor complications between two groups
Similar result with Madopar HBSSimilar result with Madopar HBS
(Block G. Multicenter 5 years study.Eur Neurol 1997)(Block G. Multicenter 5 years study.Eur Neurol 1997)

ControlControl--released levodopareleased levodopa
IndicationEarly morning akinesiaNight time wearing off

Fast acting levodopaFast acting levodopa
Madopar DT 125Madopar DT 125Early morning dystonia or akinesiaEarly morning dystonia or akinesiaEnd of dose wearing offEnd of dose wearing offDysphagiaDysphagiaFaster onset, better absorptionFaster onset, better absorption


DB RANDOMIZEDDB RANDOMIZEDDADA--AGONIST MONOTHERAPYAGONIST MONOTHERAPY--TRIALSTRIALS
-- DropDrop--outs resulting from outs resulting from AEsAEs--
*Calculated from published figure*Calculated from published figure
13%13%15%15%Pramipexole vs. LPramipexole vs. L--DopaDopa
10%10%18%18%Pergolide vs. LPergolide vs. L--DopaDopa
--20%20%BromocriptineBromocriptine
--20%20%Ropinirole Ropinirole vsvs
33%33%27%27%Ropinirole vs. LRopinirole vs. L--DopaDopa
13%13%16%16%Cabergoline Cabergoline vs.Lvs.L--DopaDopa**
LL--DopaDopa--ArmArmAgonistAgonist--ArmArmStudyStudy

DB RANDOMIZEDDB RANDOMIZEDDADA--AGONIST MONOTHERAPYAGONIST MONOTHERAPY--TRIALSTRIALS
-- Incidence of Incidence of HallucinosisHallucinosis--
*2 *2 –– monthsmonths--analysisanalysis
3.3%3.3%9.3%9.3%Pramipexole vs. LPramipexole vs. L--DopaDopa
0%0%3.4%3.4%Pergolide vs. LPergolide vs. L--DopaDopa
--7.7%7.7%BromocriptineBromocriptine
--9.0%9.0%Ropinirole vs.Ropinirole vs.
5.6%5.6%17.3%17.3%Ropinirole vs. LRopinirole vs. L--DopaDopa
1.5%1.5%1.4%1.4%Cabergoline Cabergoline vs.Lvs.L--DopaDopa**
LL--DopaDopa--ArmArmAgonistAgonist--ArmArmStudyStudy


Motor Complication During Motor Complication During LongLong--term Lterm L--DopaDopa TherapyTherapy
DoseDose
a: Lee et all 1971, a: Lee et all 1971, BarbeauBarbeau and Roy 1976, and Roy 1976, BattistinBattistin et al 1978, et al 1978, RajputRajput et alet al
1984, power et al 19861984, power et al 1986
b: Shaw et al 1980, Sweet and McDowell 1975, Markham et al 197b: Shaw et al 1980, Sweet and McDowell 1975, Markham et al 1974, 4, YahrYahr
1976, 1976, BarbeauBarbeau 1976, McDowell and Sweet 1979, 1976, McDowell and Sweet 1979, PoewePoewe et al 1986.et al 1986.
2323--88%88%4141--64%64%PeakPeak--dose dyskinesiasdose dyskinesias
6565--80%80%3535--58%58%Motor fluctuationsMotor fluctuations
>950 mg/d>950 mg/dbb400400--800mg/d800mg/daa

Levodopa Overview Levodopa Overview (cont(cont’’d)d)
Levodopa induces motor complications1-4
Up to 80% of Parkinson’s disease patients suffer from motor fluctuations and dyskinesias after approximately 5 to 10 years of treatment with levodopa4
50% to 75% of patients develop motor fluctuations 3 to 6 years after initiating therapy1-3
1. Fahn S. Adv Neurol. 1996;69:477-486.2. Poewe WH, Wenning GK. Neurology. 1996;47(suppl 3):S146-S152.3. Parkinson Study Group. Ann Neurol. 1996;39:37-45.4. Olanow CW, Stocchi F. Eur J Neurol. 2000;7(suppl 1):3-8.

DykinesiasDykinesias and motor fluctuations in and motor fluctuations in a communitya community--based study of PDbased study of PD
SchragSchrag et al, 2000et al, 2000
DykinesiasDykinesias in 28% of the patients in 28% of the patients Motor fluctuations in 40% of the patientsMotor fluctuations in 40% of the patientsPredictors for the evolution of motor fluctuation:Predictors for the evolution of motor fluctuation:
-- Disease durationDisease duration-- LD doseLD dose
Predictors for the evolution of dyskinesias:Predictors for the evolution of dyskinesias:-- Duration of treatmentDuration of treatment

Mortality of ParkinsonMortality of Parkinson’’s Diseases Disease-- Role of LRole of L--DopaDopa Therapy Therapy --
* pre* pre--LL--DopaDopa
1,581,5848%48%13 years13 years130130HelyHely et al., 1999et al., 1999
0,80,817%17%8 years8 years800800DATATOP, 1988DATATOP, 1988
1,431,43--2,662,663434--63%63%15 years15 years359359Diamond et al. 1987Diamond et al. 1987
1,461,4627%27%13 years13 years178178Shaw et al. 1980Shaw et al. 1980
1, 461, 4612%12%12 years12 years597597YahrYahr, 1976, 1976
2,902,9038%38%9 years9 years241241**Hoehn&YahrHoehn&Yahr, 1967, 1967
Mortality Mortality RatioRatio
Death Death RateRate
FollowFollow--upupnn

Mechanism of developing dyskinesiaMechanism of developing dyskinesia
Risk factorsRisk factors1.1. Chronic exogenous exposure to dopaminergic Chronic exogenous exposure to dopaminergic
drugs (mainly when given intermittently); drugs (mainly when given intermittently); dopamine receptor dopamine receptor supersensitivitysupersensitivity
2.2. Severe dopamine depletion resulting from Severe dopamine depletion resulting from nigrostriatal nigrostriatal denervationdenervation
3.3. The required presence of anatomically intact The required presence of anatomically intact striatal neuronsstriatal neurons

Dopamine Receptor SubtypesDopamine Receptor Subtypes
D1, D2 subcorticalD1, D2 subcorticalD3, D4, D5 corticalD3, D4, D5 corticalDifferentiated biochemically & Differentiated biochemically & pharmacologically into two families:pharmacologically into two families:
D1 family: D1, D5D1 family: D1, D5D2 family: D2, D3, D4D2 family: D2, D3, D4

Dopamine agonistDopamine agonist (1)(1)
ErgotamineErgotamineBromocriptineBromocriptinePergolidePergolideLisurideLisuride* Apomorpine* ApomorpineCarbergolineCarbergoline

Dopamine agonistDopamine agonist (2)(2)
Non ergotamineNon ergotamineRopiniroleRopinirolePramipexolePramipexolePiribedilPiribedil

Dopamine agonistDopamine agonist (3)(3)
Reduced motor complication compare Reduced motor complication compare with levodopawith levodopaAntiparkinsonian effect superior to Antiparkinsonian effect superior to placebo in earlyplacebo in early--stage PDstage PDAntiparkinsonian effect comparable to Antiparkinsonian effect comparable to levodopa in earlylevodopa in early--stage PDstage PDCan use as monotherary up to several yearsCan use as monotherary up to several years

Dopamine agonistDopamine agonist (4)(4)
Supplementation with levodopa Supplementation with levodopa provides clinical benefits comparable provides clinical benefits comparable to levodopa alone but with reduced to levodopa alone but with reduced motor complicationsmotor complications? Neuroprotective effects? Neuroprotective effects


DAs: Common Adverse EffectsDAs: Common Adverse Effects
Nausea, vomitingNausea, vomitingDizziness, postural hypotensionDizziness, postural hypotensionHeadacheHeadacheDizzinessDizziness

Association of Association of effusionseffusions and and fibrosisfibrosis withwithergot vs.ergot vs. nonnon--ergotergot dopaminedopamine agonistsagonists
Cabergoline
1997
12
1
0
13
DHEC
1989
1
0
1
2
Lisuride
1968
6
0
1
7
Pergolide
1988
104
8
19
131
Pramipexole
1997
0
0
0
0
Müller T, Fritze J. Clinical Neuropharmacol 2003; 26: 109-111
Yearof launchin PDPleuralPericardialPeritonealTotal
Bromocriptine
1979
215
0
29
244

DAs: Common Adverse EffectsDAs: Common Adverse Effects
Drowsiness & somnolenceDrowsiness & somnolenceDyskinesias (less than Levodopa)Dyskinesias (less than Levodopa)Confusion, hallucinations, paranoidConfusion, hallucinations, paranoidErythromelalgiaErythromelalgia

DAs: Common Adverse Effects(2)DAs: Common Adverse Effects(2)
Pulmonary & retroperitoneal fibrosis, pleural Pulmonary & retroperitoneal fibrosis, pleural effusion & pleural thickening, Raynaudeffusion & pleural thickening, Raynaud’’s s phenomena. phenomena.
(May be more common with ergotamine DAs)(May be more common with ergotamine DAs)

Dopamine agonist dose rangesDopamine agonist dose ranges
Initiating (mg)
Usual dose range (mg)
Bromocriptine
1.25 bid-tid 7.5-40
Pergolide 0.05 qd 0.75-6 Pramipexole 0.125 tid 0.75-3 Ropinirole 0.25 tid 9-24 Cabergoline 0.25 qd 0.5-5 Peribedil 50 qd 50-250

Dopamine agonistDopamine agonist
Drug T ½ (h) Carbidopa/levodopa 1-1.5 Pergolide 12-27 Pramipexole 8-12 Cabergoline 65+ Ropinirole Bromocriptine
4 6

Dopamine Agonists in Dopamine Agonists in comparisoncomparison
As As monotherapy monotherapy and adjunctive and adjunctive
to levodopato levodopa
As adjunctive As adjunctive to levodopa to levodopa
onlyonly
Not being Not being approvedapproved
As As monotherapy monotherapy
and and adjunctive to adjunctive to
levodopalevodopa
US FDA approvalUS FDA approval(http://(http://www.accewww.accessdata.fda.gov/scrissdata.fda.gov/scripts/cder/drugsatfpts/cder/drugsatfda/index.cfmda/index.cfm))
74.4074.40(10 mg/d)(10 mg/d)
137.60137.60(1 mg/d)(1 mg/d)
43.6843.68(150 mg/d)(150 mg/d)
135.00 135.00 (1.5 mg/d)(1.5 mg/d)
Daily cost (min. Daily cost (min. maint.dosemaint.dose))
18.6018.6015.0015.00--34.4034.4014.5614.5626.0026.00--90.0090.00Price/tabPrice/tab
Tab 2.5 mg.Tab 2.5 mg.Tab 0.05, Tab 0.05, 0.25 mg.0.25 mg.
Tab SR 50 Tab SR 50 mg.mg.
Tab 0.25, 1 Tab 0.25, 1 mg.mg.
PresentationPresentation
1010--40 divided 40 divided t.i.dt.i.d..
11--4 4 divided divided t.i.dt.i.d..
150150--250 250 divided 3divided 3--55
1.51.5--4.5 4.5 divided divided t.i.dt.i.d..
Usual daily dosage Usual daily dosage (mg)(mg)
BromocriptineBromocriptinePergolidePergolidePiribedilPiribedilPramipexolePramipexole

Assessment of Dopamine Agonists for the Assessment of Dopamine Agonists for the treatment of PD according totreatment of PD according to Evidence Based Evidence Based
MedicineMedicine**
Efficacious (maximum strength of evidence)± Likely efficacious ? Insufficient evidence0 No studies
(*adapted from Rascol O. et al. Lancet 2002; 359: 1589-1598)
Category Bromocriptine Cabergoline Lisuride Pergolide Piribedil Pramipexole Ropinirole
Monotherapyin early PD ± ? ± ?Combination therapy with L-Dopa in late PD ± ? ?Treatment of motor fluctuations ± ± ? ?Prevention of motor complications ± ? ? ?Imaging indicates slowed loss of 0 0 0 0 0dopaminergic neurons

Dopamine agonistDopamine agonist
Start lowStart low,, go slow go slow ((gradually titrated over several weeks or monthsgradually titrated over several weeks or months))
Improved motor and ADL scoresImproved motor and ADL scoresDecreases Decreases ““offoff”” timetimeprovided a levodopa sparing effectprovided a levodopa sparing effect

Apomorphine (1)Apomorphine (1)
D1/D2 agonistD1/D2 agonistParenteral delivery (s.c., i.v., sublingual, Parenteral delivery (s.c., i.v., sublingual, intranasal, rectal)intranasal, rectal)Rapid Rapid ““offoff”” period rescueperiod rescue
22--5 mg s.c.; pen injection systems5 mg s.c.; pen injection systems

Apomorphine (2)Apomorphine (2)
Treatment of unpredictable, frequent motor Treatment of unpredictable, frequent motor fluctuationsfluctuations
continuous s.c. infusion via minicontinuous s.c. infusion via mini--pumppump
SE: nausea, vomiting, hypotensionSE: nausea, vomiting, hypotensiontrimethobenzamide 250 mg t.i.d.trimethobenzamide 250 mg t.i.d.domperidone 20 mg t.i.d.; not available in U.S.domperidone 20 mg t.i.d.; not available in U.S.

COMT inhibitorCOMT inhibitor
No titration easy to administerNo titration easy to administerDecreased Decreased ““offoff”” timetime,, increased increased ““onon”” time and time and enhanced motor responses in patients with enhanced motor responses in patients with levodopa motor fluctuationlevodopa motor fluctuationImproved motor and ADL scores in stable Improved motor and ADL scores in stable levodopa responderslevodopa respondersMay reduce risk for motor complications if used May reduce risk for motor complications if used from onset of levodopa therapyfrom onset of levodopa therapy

COMT inhibitorCOMT inhibitor
Entacapone Entacapone 200200 mg with each dose of mg with each dose of levodopalevodopaTalcapone Talcapone 100100--200200 mg tidmg tidSide effect Side effect ;; discoloration of urinediscoloration of urine,, increase increase dyskinesiadyskinesia,, diarrheadiarrhea

COMT inhibitorCOMT inhibitor
Increase plasma levodopa elimination half life by Increase plasma levodopa elimination half life by 50%50% and area under the curve by and area under the curve by 75%75% without without rising of either the maximal plasma rising of either the maximal plasma concentrationconcentration((CmaxCmax)) or the time to reach or the time to reach maximal plasma concentration maximal plasma concentration ((TmaxTmax))

AnticholinergicsAnticholinergics
Dopaminergic Dopaminergic depletiondepletion→→cholinergiccholinergicoveractivityoveractivityInitially used in the 1950sInitially used in the 1950sEffective mainly for tremor (rigidity)Effective mainly for tremor (rigidity)Common agents (Start low, go slow):Common agents (Start low, go slow):
TrihexyphenidylTrihexyphenidyl: 2: 2--15 mg/day15 mg/dayBenztropineBenztropine: 1: 1--8 mg/day8 mg/day

AnticholinergicsAnticholinergics
Side effects:Side effects:DryDry mouth, sedation, delirium, mouth, sedation, delirium, confusion, hallucinations, confusion, hallucinations, constipation, urinary retention, constipation, urinary retention, impaired cognitionimpaired cognition

SelegilineSelegiline
Irreversible MAOIrreversible MAO--B inhibitorB inhibitorClinically active by inhibiting dopamine Clinically active by inhibiting dopamine metabolism in brainmetabolism in brainMay be neuroprotective (DATATOP, May be neuroprotective (DATATOP, SINDEPAR)SINDEPAR)Dosage: 5 mg at breakfast and lunchDosage: 5 mg at breakfast and lunch

SelegilineSelegiline
Side effects: insomnia, hallucinations, Side effects: insomnia, hallucinations, nausea (rarely), dyskinesianausea (rarely), dyskinesiaPotential interactions with tricyclics and Potential interactions with tricyclics and SSRI antidepressantsSSRI antidepressantsAs adjunct to levodopa, provides reduced As adjunct to levodopa, provides reduced motor fluctuations and increased motor fluctuations and increased ““onon””timetime

DATATOP FollowDATATOP Follow--UpUp
DATATOP: 3 year followDATATOP: 3 year follow--up studies (Ann Neurol up studies (Ann Neurol 1996)1996)
subjects requiring levodopa (n=352)subjects requiring levodopa (n=352)selegiline made no difference with regard to disease selegiline made no difference with regard to disease severity, wearingseverity, wearing--off or dyskinesiasoff or dyskinesias
subjects not requiring levodopa (n=162)subjects not requiring levodopa (n=162)No difference in parkinsonian disability between the two No difference in parkinsonian disability between the two groupsgroups
8 year follow8 year follow--up (Ann Neurol 1998)up (Ann Neurol 1998)No increase in mortalityNo increase in mortality

overviewoverview
History of ParkinsonHistory of Parkinson’’s Diseases DiseaseClinical manifestation of PDClinical manifestation of PDEtiology and secondary cause of ParkinsonismEtiology and secondary cause of ParkinsonismClassification Classification Treatment : Treatment :
medical medical surgical (new in Thailand)surgical (new in Thailand)
Late complications:Late complications:motor VS nonmotor VS non--motormotor

Stages in Decline of Response to LDStages in Decline of Response to LD
I: Patient not aware of effect of individual doseI: Patient not aware of effect of individual doseII: MidII: Mid--afternoon loss of benefitafternoon loss of benefitIII: Loss of sleep benefit; earlyIII: Loss of sleep benefit; early--morning akinesia, morning akinesia, possible foot dystoniapossible foot dystoniaIV: Regular IV: Regular ““wearing offwearing off”” every 4 hours at first, every 4 hours at first, shortens with timeshortens with timeV: Frequent wearing off, abrupt onV: Frequent wearing off, abrupt on--off, unpredictable off, unpredictable dose responsedose response

Late ComplicationsLate Complications
MotorMotorresponse fluctuations, dyskinesias, dystonia, freezing, response fluctuations, dyskinesias, dystonia, freezing, fallsfalls
NonNon--motor (Behavioral/neuropsychological)motor (Behavioral/neuropsychological)depression, sleep disorders, psychosisdepression, sleep disorders, psychosis
AutonomicAutonomicorthostatic hypotension; hyperhidrosis, constipation, orthostatic hypotension; hyperhidrosis, constipation, impotence, urinary incontinence or retentionimpotence, urinary incontinence or retention


LD Response FluctuationsLD Response Fluctuations
Peripheral causes:Peripheral causes:delayed gastric emptyingdelayed gastric emptyingdietary proteindietary proteinshort plasma halfshort plasma half--lifelife
Central causes:Central causes:pulsatile delivery to striatal receptorspulsatile delivery to striatal receptorsimpaired storage capacityimpaired storage capacityalteration of DA receptorsalteration of DA receptors

Response Fluctuations: TreatmentResponse Fluctuations: Treatment
Increase LD doseIncrease LD doseIncrease DCI doseIncrease DCI doseAdd dopamine agonistAdd dopamine agonistAdd COMT inhibitorAdd COMT inhibitor
reduce LDreduce LDliver function monitoringliver function monitoring
Apomorphine rescueApomorphine rescue

Peak Dose Dyskinesia or DystoniaPeak Dose Dyskinesia or Dystonia
Chorea more common than dystoniaChorea more common than dystoniaMay be worse on more affected sideMay be worse on more affected sideMay not be as disabling as akinesia/rigidityMay not be as disabling as akinesia/rigidityDose adjustments, addDose adjustments, add--ons:ons:
reduce LD dose, increase dose frequencyreduce LD dose, increase dose frequencyreduce LD, add DA, COMT inhibitorreduce LD, add DA, COMT inhibitor

OffOff--period Dystoniaperiod Dystonia
Appears when LD level is low, especially early Appears when LD level is low, especially early AMAMw/ or w/o parkinsonismw/ or w/o parkinsonismDose adjustments, addDose adjustments, add--ons:ons:
more frequent LD dosing to avoid low plasma levelsmore frequent LD dosing to avoid low plasma levelsadd DA, COMT inhibitor, MAOadd DA, COMT inhibitor, MAO--B inhibitorB inhibitor

Wearing OffWearing Off
Regular and predictable decline in response 2Regular and predictable decline in response 2--4 4 hours after LD dosehours after LD doseMost common motor fluctuationMost common motor fluctuationDose adjustments, addDose adjustments, add--ons:ons:
change to LDchange to LD--CR, or increase LD frequencyCR, or increase LD frequencyreduce LD, add DA or COMT inhibitorreduce LD, add DA or COMT inhibitor

OnOn--off Responseoff Response
Sudden and unpredictable off periods unrelated Sudden and unpredictable off periods unrelated to dosing scheduleto dosing scheduleOne of the hardest features to manageOne of the hardest features to manageDose adjustments, addDose adjustments, add--ons:ons:
reduce LD, add DAreduce LD, add DA

Other Motor ComplicationsOther Motor Complications
Diphasic dyskinesiaDiphasic dyskinesiadyskinesia at beginning and end of dosedyskinesia at beginning and end of doseDose adjustments, addDose adjustments, add--ons: add DAons: add DA
Drug failureDrug failurelate afternoon, probably related to poor gastric emptying or late afternoon, probably related to poor gastric emptying or absorptionabsorptionliquid preparations; increase gastric motility; decrease dietaryliquid preparations; increase gastric motility; decrease dietaryproteinproteinapomorphine rescueapomorphine rescue

Freezing and FallsFreezing and Falls
FreezingFreezingmotoric block; at initiation of gait, turning, narrow spacesmotoric block; at initiation of gait, turning, narrow spacesuse auditory, visual, proprioceptive cuesuse auditory, visual, proprioceptive cues
FallsFallsphysical therapy evaluationphysical therapy evaluationcane, scooter, wheelchair may be necessarycane, scooter, wheelchair may be necessary

PsychosisPsychosis
FeaturesFeaturesVivid dreams/nightmares, disorientation, hallucinations, delusioVivid dreams/nightmares, disorientation, hallucinations, delusional nal thoughtthought
Simplify medical regimenSimplify medical regimenStop unnecessary nonStop unnecessary non--PD medsPD medsStop: anticholinergic drugs, amantadine, selegiline, dopamine agStop: anticholinergic drugs, amantadine, selegiline, dopamine agonists, onists, COMT inhibitorsCOMT inhibitors
Change from CR to standard carbidopa/levodopaChange from CR to standard carbidopa/levodopaTry atypical antipsychotic agentsTry atypical antipsychotic agentsTry lowTry low--potency traditional antipsychotic agentspotency traditional antipsychotic agents

DepressionDepression
Reported in 30Reported in 30--90% of PD patients90% of PD patientsDifficult to discern from vegetative symptomsDifficult to discern from vegetative symptomsRequires inquiry into depression symptomsRequires inquiry into depression symptomsUsually responds quickly to medicationsUsually responds quickly to medications
Tricyclic agentsTricyclic agentsSelective serotonin reSelective serotonin re--uptake inhibitorsuptake inhibitors
If ECT needed, will transiently improve PD symptomsIf ECT needed, will transiently improve PD symptoms

Anxiety/RestlessnessAnxiety/Restlessness
Primary anxiety disorder: treat with Primary anxiety disorder: treat with benzodiazepinesbenzodiazepines
Associated with Associated with ““offoff--periodsperiods”” or lowor low--levodopa levodopa levels: adjust levodopa dosinglevels: adjust levodopa dosing
Restless Leg Syndrome: benzodiazepines, Restless Leg Syndrome: benzodiazepines, narcotics, levodopa, dopamine agonistsnarcotics, levodopa, dopamine agonists

Sleep Disorders (1)Sleep Disorders (1)
InsomniaInsomniacareful historycareful historydifficulty with sleep initiation: tricyclic agents, difficulty with sleep initiation: tricyclic agents, benzodiazepines, diphenhydramine, chloral hydratebenzodiazepines, diphenhydramine, chloral hydratetreat depressiontreat depression
REMREM--behavioral disorder: clonazepambehavioral disorder: clonazepam

Sleep Disorders (2)Sleep Disorders (2)
Excessive daytime sleepinessExcessive daytime sleepinessCorrect poor sleep at nightCorrect poor sleep at nightDiscontinue anticholinergics, amantadineDiscontinue anticholinergics, amantadineReduce dopamine agonist, levodopa dosages if Reduce dopamine agonist, levodopa dosages if possiblepossibleselegiline; caffeine; methylphenidate 5selegiline; caffeine; methylphenidate 5--20 mgs/d20 mgs/d

Orthostatic HypotensionOrthostatic Hypotension
LightLight--headedness, dizziness, fatigue, shoulder or neck headedness, dizziness, fatigue, shoulder or neck pain, blood pressure drops when standingpain, blood pressure drops when standingTaper antiTaper anti--hypertensive agentshypertensive agentsTaper nonTaper non--PD drugsPD drugsIncrease salt intakeIncrease salt intakeCompression stockingsCompression stockingsFludrocortisone (0.1Fludrocortisone (0.1--0.4 mg/d)0.4 mg/d)Midodrine (2.5 Midodrine (2.5 -- 20 mg/d)20 mg/d)

Urinary Incontinence/FrequencyUrinary Incontinence/Frequency
Rule out urinary tract infectionRule out urinary tract infectionBladder evaluation forBladder evaluation for
detrusor hyperactivitydetrusor hyperactivityoxybutinin 5 oxybutinin 5 --30 mg/d; propanthaline 7.5 30 mg/d; propanthaline 7.5 -- 15 mg/d15 mg/d
detrusor hypoactivitydetrusor hypoactivityphenoxybenzamine; prazosinphenoxybenzamine; prazosin
Urinary frequencyUrinary frequencyavoid fluid pooling in feetavoid fluid pooling in feetDDAVP inhaler; tolterodine tartrate 2mg hs to 2mg tidDDAVP inhaler; tolterodine tartrate 2mg hs to 2mg tid

Sexual DysfunctionSexual Dysfunction
Medical screeningMedical screeningdepression, anxiety, iatrogenic causesdepression, anxiety, iatrogenic causes
Endocrinologic evaluationEndocrinologic evaluationprolactin, testosterone, lutenizing hormone, thyroid prolactin, testosterone, lutenizing hormone, thyroid screenscreen
Urologic evaluationUrologic evaluationyohimbine, sildenafilyohimbine, sildenafil

NauseaNausea
LevodopaLevodopa--related: take with meals, add related: take with meals, add carbidopa, add domperidonecarbidopa, add domperidoneOther antiOther anti--PD medications: same. PD medications: same.
If no improvement: withdraw newest agent, reIf no improvement: withdraw newest agent, re--initiate at minimal doses, slowly increaseinitiate at minimal doses, slowly increase

Excessive SweatingExcessive Sweating
Usually levodopa related, and may be seen at Usually levodopa related, and may be seen at peak or trough dose drug levelspeak or trough dose drug levels
reduce levodopareduce levodopaadd dopamine agonist or COMT inhibitoradd dopamine agonist or COMT inhibitoradd carbidopaadd carbidopaadd Betaadd Beta--blockerblocker

Surgical Treatment Surgical Treatment inin
ParkinsonParkinson’’s Diseases DiseasePart 6 of 7

Surgical Treatments for ParkinsonSurgical Treatments for Parkinson’’s Diseases Disease
AblativeAblativethalamotomythalamotomypallidotomypallidotomy
Electrical stimulationElectrical stimulationVIM thalamus, globus pallidus internus, subVIM thalamus, globus pallidus internus, sub--thalamic nucleusthalamic nucleus
TransplantTransplantautologous adrenal, human fetal, xenotransplants, autologous adrenal, human fetal, xenotransplants, genetically engineered transplantsgenetically engineered transplants

ThalamotomyThalamotomy
Significant improvement in contralateral tremorSignificant improvement in contralateral tremordepends on correct placementdepends on correct placement
Minimal improvement in other PD signsMinimal improvement in other PD signsBilateral procedures poorly toleratedBilateral procedures poorly toleratedAEs: bulbar, sensory and motor deficits, gait, AEs: bulbar, sensory and motor deficits, gait, surgical complicationssurgical complicationsGradually being replaced by thalamic DBS Gradually being replaced by thalamic DBS

Deep Brain Stimulation (DBS)Deep Brain Stimulation (DBS)
High frequency, pulsatile, bipolar electrical High frequency, pulsatile, bipolar electrical stimulationstimulationStereotactically placed into target nucleusStereotactically placed into target nucleusCan be activated and deactivated with an Can be activated and deactivated with an external magnetexternal magnetExact physiology unknown, but higher Exact physiology unknown, but higher frequencies mimic cellular ablation, not frequencies mimic cellular ablation, not stimulation stimulation

Movement Disorder SurgeryMovement Disorder Surgery
ศรัณย นันทอารี
Siriraj Movement Disorder Group
อภิชาติ พิศาลพงศ กนกวรรณ บุญญพิสิฎฐ
อรสา ชวาลภาฤทธิ์ นิพนธ พวงวรินทร
ไพรัช สายวิรุณพร
วรพรรณ เสนาณรงค
นันทศักดิ ์ทิศาวิภาค

VIM Thalamic DBSVIM Thalamic DBS
80% reduction in contralateral arm and leg tremor80% reduction in contralateral arm and leg tremorPossible mild improvement in bradykinesia and rigidityPossible mild improvement in bradykinesia and rigidityNo functional improvement (UPDRS part II), but No functional improvement (UPDRS part II), but significant improvement based upon global scoressignificant improvement based upon global scoresNo effect: gait and bulbar symptomsNo effect: gait and bulbar symptomsAEs: bulbar, gait, paresthesia, surgicalAEs: bulbar, gait, paresthesia, surgical

Globus Pallidus internus DBSGlobus Pallidus internus DBS
Effects tend to mimic those of pallidotomyEffects tend to mimic those of pallidotomySignificant improvement in dyskinesiaSignificant improvement in dyskinesiaModerate improvement in cardinal Moderate improvement in cardinal ““offoff”” signssignsNo comparison between unilateral and bilateral No comparison between unilateral and bilateral Bilateral DBS may be better tolerated than bilateral Bilateral DBS may be better tolerated than bilateral pallidotomypallidotomy
AE: surgical complicationsAE: surgical complications

Bilateral Subthalamic DBS Bilateral Subthalamic DBS
Bilateral placement appears to be superior to Bilateral placement appears to be superior to unilateral placementunilateral placementTheorized neuroprotective mechanism, but no Theorized neuroprotective mechanism, but no clinical evidence supporting this clinical evidence supporting this AE: confusion and hallucinations, increased AE: confusion and hallucinations, increased dyskinesia before medication adjustments, eyelid dyskinesia before medication adjustments, eyelid opening apraxia, weight gain, surgical opening apraxia, weight gain, surgical complicationscomplications

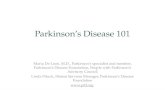
Patient Diary Data Subthalamic Nucleus
Patient Diary Data Patient Diary Data Subthalamic NucleusSubthalamic Nucleus
Clinical Results
Asleep27%
“on” time23%
“off” time35%
“on” withDyskinesia
14%
Asleep33%
“on” time53%
“off” time11%“on” with
Dyskinesia3%
Asleep33%
“on” time53%
“off time”12%“on” with
Dyskinesia2%
Pre-Implant 6 Months 12 Monthsn = 39
L-dopa equiv. = 1325 mg
n = 25
L-dopa equiv. = 1016 mg
n = 12
L-dopa equiv. = 988 mg

Subthalamic DBSSubthalamic DBS
All cardinal features of PD noted to improve All cardinal features of PD noted to improve in open label trialsin open label trials““OffOff”” UPDRS improved 60%UPDRS improved 60%““OnOn”” UPDRS improved 10%UPDRS improved 10%Dyskinesia tends to improve but this is Dyskinesia tends to improve but this is probably due to decreased levodopa doseprobably due to decreased levodopa dose

Activa® Parkinson’s Control SystemActivaActiva®® ParkinsonParkinson’’s Control Systems Control System
Activa® System

Implanted ComponentsImplanted ComponentsImplanted Components
Activa® System

DBS™ Leads DBS™ Leads
Model 3389 Model 3387 Cap, Ring, Stylet
Activa® System

Instruments


T2W FSEaxial coronal
STN

StimulationStimulation--induced effectsinduced effects((sagittalsagittal and frontal sections)and frontal sections)



siamsiamSiamSiam--chronic.mpgchronic.mpg

Cell TransplantsCell TransplantsAutologous adrenal transplantsAutologous adrenal transplants
No efficacyNo efficacy
Allogenic human fetal transplantsAllogenic human fetal transplantsInitial encouraging clinical resultsInitial encouraging clinical results
Xenogenic fetal transplant (porcine and Xenogenic fetal transplant (porcine and bovine) bovine)
Preliminary results pendingPreliminary results pending
Genetically engineered cellsGenetically engineered cellsResearch ongoing Research ongoing

Human Fetal TransplantsHuman Fetal Transplants
EfficacyEfficacyEncouraging preliminary results in young PD ptsEncouraging preliminary results in young PD ptsPET studies consistent with cell functioningPET studies consistent with cell functioningAutopsies (2) show cell survivalAutopsies (2) show cell survival
ProblemsProblems44--10 embryos < 10 weeks gestation needed10 embryos < 10 weeks gestation neededImmunosuppression requirements unknownImmunosuppression requirements unknownNumerous technical problemsNumerous technical problems

Nonpharmacologic Treatments (1)Nonpharmacologic Treatments (1)
Patient/caregiver education Patient/caregiver education Physical therapyPhysical therapyExerciseExerciseOccupational therapyOccupational therapy

Nonpharmacologic Treatments (2)Nonpharmacologic Treatments (2)
Speech/language therapySpeech/language therapyDiet and nutritionDiet and nutritionPsychosocial interventionsPsychosocial interventions

Current management in Current management in Young Young ––onset Parkinsononset Parkinson’’s Disease patientss Disease patients
Start with Dopamine agonistStart with Dopamine agonistAdd levodopa when disability can not overcome Add levodopa when disability can not overcome by DAby DAAdd COMT inhibitor when developing motor Add COMT inhibitor when developing motor fluctuationsfluctuationsConsider start with anticholinergic or Consider start with anticholinergic or amantadine if tremor is the prominent symptomamantadine if tremor is the prominent symptom

Current management in Current management in LateLate––onset Parkinsononset Parkinson’’s Disease patientss Disease patients
Start with dopamine agonist if no Start with dopamine agonist if no contraindication and add on levodopa later contraindication and add on levodopa later Or start with levodopa when reaching dosage of Or start with levodopa when reaching dosage of 400400-- 600 mg add on dopamine agonist600 mg add on dopamine agonistConsidering COMT inhibitor when developing Considering COMT inhibitor when developing motor fluctuationsmotor fluctuations? Start with triple combinations (L? Start with triple combinations (L--dopa+ dopa+ DDC+ COMT inhibitor)DDC+ COMT inhibitor)
กลับสูเมนูหลัก