
Management Engineering & Process Improvement Community February...
34
Management Engineering & Process Improvement Community February 6, 2015 Cynthia Hartmann, MBA, CPHIMS, Six Sigma Lean Black Belt Committee Chair
Transcript of Management Engineering & Process Improvement Community February...

Management Engineering & Process Improvement Community
February 6, 2015
Cynthia Hartmann, MBA, CPHIMS, Six Sigma Lean
Black Belt
Committee Chair
MEPI COMMUNITY MISSION
Support and promote the profession of management engineering and process improvement among the members of HIMSS by providing opportunities for networking, collaboration, publication, promotion and professional development of Management Engineers and Process Improvement professionals in healthcare organizations.

©2014 The Advisory Board Company • advisory.com
Rising Consumerism and the Impact on
Patient Experience, Quality, and Safety The New Standard for Hospital Rounding in a Changing Health Care Environment
Presentation Prepared for HIMSS
February 6, 2015
Presented by:
Jeffrey Bunting
Executive Director, Patient Experience
The Advisory Board Company
iRound

©2014 The Advisory Board Company advisory.com 4
No Longer Insulated From Market Forces
Catalyzing a Shift in Network Demands
Source: Health Care Advisory Board interviews and analysis.
Traditional Market Retail Market
Growing number of buyers
1
Proliferation of product options
2
Increased transparency
3
Reduced switching costs
4
Greater consumer cost exposure
5
Passive employer,
price-insulated employee
Activist employer,
price-sensitive individual
Broad, open networks Narrow, custom networks
No platform for apples-to-
apples plan comparison
Clear plan comparison on
exchange platforms
Disruptive for employers to
change benefit options
Easy for individuals to
switch plans annually
Constant employee premium
contribution, low deductibles
Variable individual premium
contribution, high deductibles
Characteristics of a Traditional vs. Retail Market

©2014 The Advisory Board Company advisory.com 5
Exchanges Fuel Patient Consumerism
Health Care Economics Shifting, With Potential to Disrupt Networks
1) “Are You Ready? Private Health Exchanges Are Looming,” Accenture, 2013
Participation in Exchanges Skyrockets…
Annual Exchange Enrollment (Public & Private) in Millions1
…Changing Market Dynamics
1 Increased transparency and plan comparisons
2 Decentralization of purchasing
3 Multiplication of plan options
10
60
2014 2017
4 Decreased switching costs

©2014 The Advisory Board Company advisory.com 6
Welcome to the Renewals Business
New Imperative to Secure Purchaser Choice Year Over Year
Source: Health Care Advisory Board interviews and analysis.
Day 1
Day 365
Care Decision
Network Selection
Care Decision Care Decision
Care Decision
Clinical interactions
represent repeated
opportunities to reinforce
patient preference through
superior experience
Annual network selection in
fluid insurance market
implies consistent
reevaluation of network
performance
Patient
Experience

©2014 The Advisory Board Company advisory.com 7
Service Experience Drives Patients’ Provider Choice
Cultivating Patient Loyalty Increasingly Seen as Mission Critical
1) “Market Insights Survey 2012” by NRC Picker.
2) Assumes 17,500 annual admissions, average 71% likely to recommend, $8-12K average
value of follow-up & ancillary care resulting from typical admission
Patients Make Choices Based on Service & Experience
69%
83%
88%
High scores on patient sat report cards
Previous experience with hospital
Doctor recommendation
Select Factors Influencing Patient Likelihood to Return to Hospital for Care¹
n = 264,892 consumers
Additional reimbursement
from converting 5% of
detractors to loyal patients
for follow-up care²
$2-3M
Consistent Focus on Patient Loyalty Delivers Value

©2014 The Advisory Board Company advisory.com 8
Moving Beyond Quality and Efficiency
Patient Experience = New Battleground
Patient Experience: Common Underpinning of Strategic Initiatives
Broadening Our Definition of “Quality”
“Quality is more than just whether you live or die or not. Quality has to be the clinical experience, the physical experience and the emotional experience,
[…] we realized that the emotional aspect of it was anyone in the hospital could affect the entire outcome, [...] if your room was dirty, it undid the work of
the cardiac surgeon, the anesthesiologist, the cardiologist, the fusionist, the intensive care nurse.”
Delos “Toby” Cosgrove, MD
CEO & President, Cleveland Clinic
Network
Integration
• Visibility into patient encounters
across continuum critical to
delivering consistent service level to
support “brand”
• Substandard service disrupts carefully
constructed referral networks by
encouraging patients defections
Workforce
Alignment
• Diversification of care teams makes
measuring patient perceptions and precisely
attributing feedback more important than
ever
• Putting patients—not process—at center of
care redesign efforts reinforces sense of
“purpose” throughout the workforce
Population Health
Management
• Effectively partnering with patients to
improve outcomes key to managing
risk and population health more broadly
• Ensuring patients stay in-network
requires constant, consistent feedback
and commitment to making
improvements

©2014 The Advisory Board Company advisory.com 9
Meeting Patient Needs is Integral to the Overall Experience
Source: Malott D, et al., “The Root of All Satisfaction,” Partners, Mar/Apr
2010: 12-15; Nursing Executive Center interviews and analysis. 1) Drivers tied for number 5 ranking
Elements of Patient Experience Correlated With Likelihood to Recommend
1
2
3
4
5
How well staff worked together to care for you
Response to concerns/complaints made during your stay
Amount of attention paid to your special or personal needs
How well the nurses kept you informed
Nurses’ attitude toward requests¹
Degree to which hospital staff addressed your emotional needs¹
Driver of Likelihood to Recommend Rank

©2014 The Advisory Board Company advisory.com 10
Crucial System For Surfacing and Addressing Patient Needs
1) “Three Nursing Interventions' Impact on HCAHPS Scores.” Journal of Nursing Care
Quality; March 20, 2013. Bryan Kennedy et al
Rounding Has Rapid Impact, Absence Felt Immediately
% Patients Rating Care “Excellent”¹
52%
71%
46%
Month Prior Month Introduced Month Discontinued
Rounding More Efficacious Than Other Interventions
% Patients Rating Care “Excellent” After Specific Interventions
Were Introduced Sequentially, in Isolation
46%
50%
56%
71%
Dischargecalls
Teach-back
Dischargepacket
Managerrounding

©2014 The Advisory Board Company advisory.com 11
What is Rounding? An Evolution.
PRESENT PAST
Physicians make “rounds”—visiting patients to
assess their conditions and plan care
Physician Physicians Nurses Executives Dept. Leaders
Over the last decade, many different types of rounding have come into
practice in hospitals and other healthcare settings
These newer types of rounding include rounding on patients in a
structured way by nursing, executives, and representatives of different
departments using new technologies
The term has even been extended to observations and audits not even
involving patients.

©2014 The Advisory Board Company advisory.com 12
Hourly and Daily Leader Rounding
Hourly
Rounding
Daily Leader
Rounding
• Nurses visit each patient each hour
• Assess for 3 or 4 P’s (Pain, Potty, Position,
Placement)
• Sets expectation for next visit
• Traditionally not automated; paper-driven
• Aka…Daily Rounding, Leader Rounding,
Purposeful Rounding; typically conducted by
nursing leaders
• Confirm hourly rounding performance, check
overall patient experience (e.g., pain, noise,
room condition, etc.)
• Surface issues driving poor patient experience
and get feedback on caregiver staff
Improved patient and staff satisfaction
Reductions in life-threatening falls,
pressure ulcers (bed sores)
Higher patient satisfaction scores
under Medicare value-based
purchasing
Increase in patient loyalty drives
recurring revenues for health system
Results

©2014 The Advisory Board Company advisory.com 13
Leader Rounding on Staff Physicians
Leader Rounding on Staff Physicians
• Aka Manager or Executive Rounding
• Periodic, face-to-face, one-on-one
discussions between leaders at different
levels and staff
• Identify opportunities for improvement,
surface staff recognition, ensure
communication of strategy
• Important to have buy-in from upper
management
• Studies show can dramatically improve staff
satisfaction and engagement
• In turn, happy employees = happier patients
• Meaningful reduction in staff turnover and
vacancy and resulting cost savings
Results Key Components

©2014 The Advisory Board Company advisory.com 14
Consistent, Systematic Staff Recognition Drives Engagement
Recognition is tightly bound to
hourly, daily and staff rounding
Recognition drives staff engagement
and satisfaction, resulting in
improved performance and retention
Best programs have different forms of
recognition (e.g., executive cards to public
recognition to gifts and rewards)
Important to incorporate
recognition into automated rounding
KEY COMPONENTS OF SUCCESSFUL STAFF ENGAGEMENT

©2014 The Advisory Board Company advisory.com 15
Service Recovery
Solving Issues Before They Affect Satisfaction
The Service Recovery Paradox
The “service recovery paradox” states that with a
highly effective service recovery, a service or
product failure offers a chance to achieve higher
satisfaction ratings from customers than if the
failure had never happened. A little bit less
academically, this means that a good recovery
can turn angry and frustrated customers into
loyal customers. In fact it can create even more
goodwill than if things had gone smoothly in the
first place
Customer Experience Academy
Better Not to Have Asked?
Likelihood of Repeat Purchase After Service Failure
54%
19%
Satisfactory Resolution Non-satisfactory Resolution

©2014 The Advisory Board Company advisory.com 16
Quality and Safety
Quality and Safety: Medication
administration, pressure ulcer audits,
bedside reports, discharge checklists
Critical data is captured without additional
entry steps, saving time and reducing
potential for error
Paper-based checklists
difficult to audit, require data
entry steps
Infection Control: hand sanitation,
Foley/tube/line audits, staff vaccination
tracking
Identified improvement projects are
assigned on-the-spot and tracked in
automated reports
Tracking results of audits,
making hand-washing
observations discreet
Regulatory Compliance: Environment of
care audits, restraint audits, TJC probe
data collection
With mobile devices, staff quickly deploy
any audit they need; improvement
projects are assigned on-the-spot, tracked
in automated reports
Maintaining multiple paper-
based audits is challenging;
following through on issues
can be difficult
POTENTIAL PROBLEMS FROM
SUBOPTIMAL PROCESSES CHALLENGES FACING
HEALTH CARE PROVIDERS
AUTOMATION-DRIVEN
IMPROVEMENTS
Turn Virtually Any Imperfect Process Into a Closed-Loop Reliable System
Example Applications of iRound Enterprise

©2014 The Advisory Board Company advisory.com 17
Lack of Timely and Actionable Insights
• Paper-based daily rounding cumbersome, unsustainable
• Post-discharge surveys with low response rates, delayed insights
• Post-discharge calls conducted inconsistently, generate limited
insights
Lack of Staff Engagement
• Narrow focus, dependence on nursing organization; inadequate resource allocation
• Vague anecdotes without data discourages ownership of performance
improvement
• Inability to emotionally engage staff
Lack of Accountability
• Uneven service recovery processes leave patient issues unresolved
• Absence of tracking mechanisms prevents timely correction of poor
individual performance
Lack of Cross-Departmental Coordination
• Siloed and short-lived improvement campaigns
• Coordination with service departments unwieldy, time and effort wasted
• Performance data not shared broadly, inability to measure impact of initiatives
Doing More of the Same: An Insufficient (and Potentially Harmful) Strategy
Key Challenges to Driving Performance Improvement Using Traditional Processes
* Nurse leaders spent an average of 6 minutes per round, 20 minutes per
issue surfaced, and 4 hours per week on data entry and reporting
A Worthy Aspiration Gone Awry
• 300-bed hospital in Midwest implemented best practice of daily nurse leader rounding on every patient to
improve patient experience
• Conducted paper-based rounding and manual data entry; data was outdated by the time it was available for
review, failed to deliver insight into house-wide performance and trends
• Manual issue resolution processes consumed additional nursing time, issue follow up was poor
• Despite significant investment, daily rounding initiative created staff frustration and diverted significant nursing
time from patient care - which ultimately hurt patient experience
$480K Annualized cost of nurse leader
hours spent on manual rounding,
data analysis, issue resolution*
$376K Estimated cost of replacing
nursing staff frustrated by issues
associated with manual rounding
and issue resolution processes

©2014 The Advisory Board Company advisory.com 18
Case Study
Sightlines to Patients and Staff Produce Bounty of Benefits
Case in Brief: Crosstown Medical Center1
• 300-bed independent hospital with a service area
spanning two states in the Mid-Atlantic region.
• Regional acute care hospital with affiliated
cancer center, diagnostic center, surgery center,
and ambulatory network.
25 Percentile point
improvement in HCAHPS
Overall Hospital Rating
Before iRound After iRound
11-fold
increase
Manager Compliance with Daily Patient Experience Rounds
Patient Experience
• More consistent, productive daily
rounding helped move HCAHPS scores
across multiple dimensions
• Units with the highest rounding rates2
achieved scores on average 9% points
higher across all 10 HCAHPS categories
Staff Engagement
• Automated system used to collect and
disseminate more rapid, meaningful staff
recognition based on real-time feedback
• Automated employee rounds led to quicker
implementation of staff improvement ideas,
further supporting engagement level
Patient Safety
• Automating daily rounding helped nurse
managers ensure that hourly rounding
needs were being met consistently
• Managers able to intervene with individual
caregivers based on data, leading to 20%
lower falls rate after just four months
Virtuous Cycle of Improvements
Visibility Drives Improvements for Patient Experience, Safety, and Staff Engagement

©2014 The Advisory Board Company advisory.com 19
Patient-Centered Approach Impacts Many Outcomes
Visibility Improves Patient Experience, Safety, and Staff Engagement
1) Pseudonym
2) Rounds conducted divided by patients available for rounding
Case in Brief: Brahms Hospital1
• 270-bed hospital in the Northeast U.S.
• Regional acute care hospital with affiliated cancer center, diagnostic center,
surgery center, and ambulatory network.

©2014 The Advisory Board Company advisory.com 20
Levels of Automation Sophistication: Basic Automation of Paper
20
Mobile Rounding WOW
Administration Database

©2014 The Advisory Board Company advisory.com 21
Levels of Automation Sophistication: Use On Any Device
21
Database
Web application
Mobile Rounding WOW
Administration

©2014 The Advisory Board Company advisory.com 22
Levels of Automation Sophistication: Basic Data Integration
22
Database
Web application
Census Interface
HCAHPS Data
Mobile Rounding
WOW
Administration

©2014 The Advisory Board Company advisory.com 23
Levels of Automation Sophistication: Patient Centric
23
Patient Centric
Database
Web application
Census Interface
HCAHPS Data ADT Interface
Mobile Rounding
WOW
Administration

©2014 The Advisory Board Company advisory.com 24
Levels of Automation Sophistication: Fully Integrated
24
Patient Centric
Database
Web application
Census Interface
HCAHPS Data ADT Interface
Task Management / Ticket
Interface(s)
HR Interface –
Staff Reporting
Relationships
Mobile Rounding
WOW
Administration

©2014 The Advisory Board Company advisory.com 25
Nurse Manager Checks Unit Rounding Status
Overall rounding status of
the unit.
Status of each room in each
unit: Who is the patient?
Have we rounded yet? Are
there any issues?

©2014 The Advisory Board Company advisory.com 26
Nurse Manager Checks Patient Service History
Demographic history of
patient and full history of
service issues and rounds

©2014 The Advisory Board Company advisory.com 27
Nurse Manager Rounds on Patient
Forms include both yes/no questions
to allow quick data entry and open-
ended questions to solicit patient
improvement, recognition
suggestions

©2014 The Advisory Board Company advisory.com 28
Nurse Leader Enters Service Recovery Issue

©2014 The Advisory Board Company advisory.com 29
Unit Manager Reviews Patient Comments With Staff at Huddle
Actionable Real-Time Patient Feedback
Capturing patient
comments about individual
staff members
Identifying unmet
patient needs

©2014 The Advisory Board Company advisory.com 30
Hospital COO Reviews Patient Feedback vs. Other System Facilities
©2014 The Advisory Board Company advisory.com 31
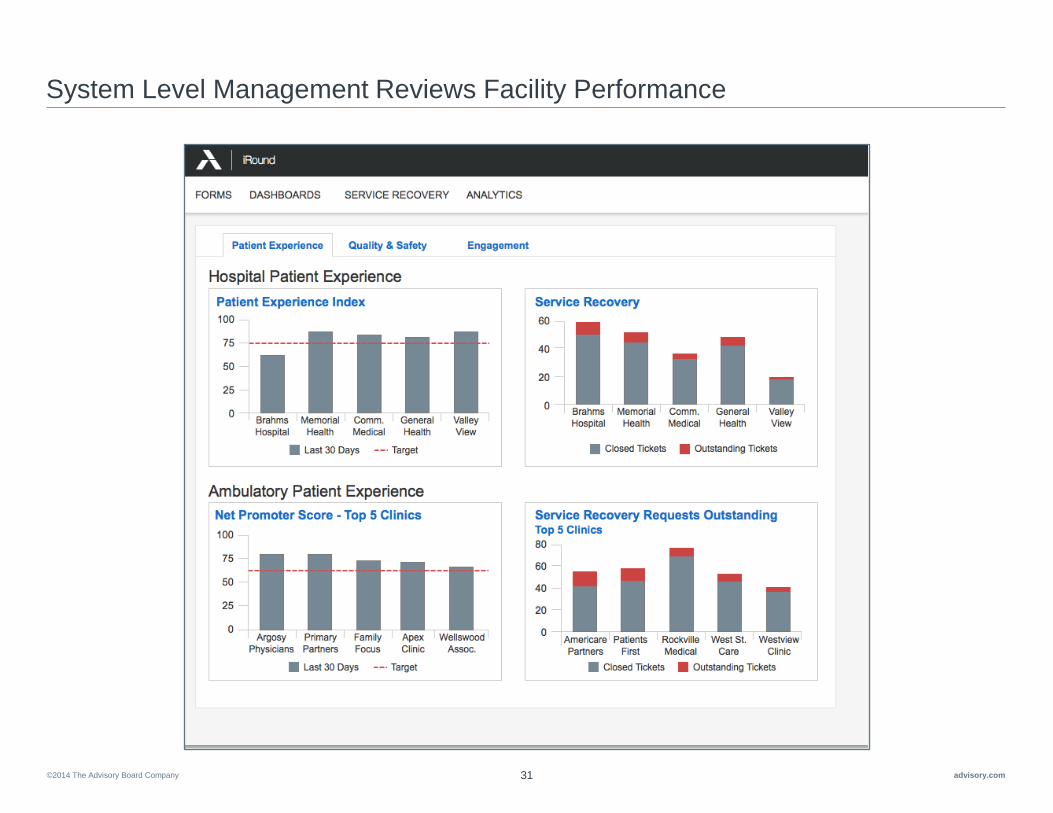
System Level Management Reviews Facility Performance

©2014 The Advisory Board Company advisory.com 32
Other Important Considerations
Mobile Device Policy Integration

©2014 The Advisory Board Company advisory.com 33
Conclusions

©2014 The Advisory Board Company advisory.com 34
Q&A and Contact Information
Jeffrey Bunting
Executive Director, Patient Experience
The Advisory Board Company
(415) 432-3905


















