Malnutrition in developing countries
7
Malnutrition in developing countries Emily Walton Stephen Allen Abstract Although now rare in industrialized countries, severe acute malnutrition is unfortunately still common throughout the developing world and is a key contributor to both global childhood morbidity and mortality. This review describes the epidemiology of malnutrition and the presentation and pathophysiology of the severe syndromic forms e marasmus and kwash- iorkor. The gold standards for diagnosis and management are detailed and the challenges of implementation in the basic healthcare systems of the developing world are discussed. As the leading cause of ill health in the world today, more effective treatment and prevention of malnutri- tion must be a priority for the global healthcare community. Keywords kwashiorkor; marasmus; protein-energy malnutrition; severe acute malnutrition; underweight Underweight: the leading cause of ill health in the world today In 2008, of the 8.8 million global deaths of children under 5 years of age, 93% occurred in the developing countries of Africa and Asia. The highest rates of childhood mortality are found in sub-Saharan Africa where one in seven children die before their fifth birthday. Outside the neonatal period, the most common primary causes of death are pneumonia (19%) and diarrhoea (17%) but over a third of all deaths can be attributed to under- lying undernutrition (see Figure 1). It is estimated that there are 148 million underweight children: 78 million live in South Asia and 36 million in sub-Saharan Africa. In the developing world, 20% of children are underweight and 3.5% (19 million) are severely malnourished. Millennium Development Goal 4 (a reduction in global under-5 mortality by 2/3 between 1990 and 2015) will only be achieved if significant gains in both the prevention and management of malnutrition are made. As well as causing loss of life, malnutrition results in substantial morbidity and loss of quality of life; long-term developmental problems and educational underachievement diminish the ability to work thereby reducing potential for national development. When calculated as disability-adjusted life years, underweight in childhood is the leading global risk factor for ill health in the world today. Definitions and diagnosis The diagnosis of malnutrition is based on measurement of body size (anthropometry) and clinical signs (see Box 1). Based on the 2006 WHO Child Growth Standards, underweight is defined as a weight that is greater than 2 standard deviations (or “z scores”) below the median expected weight for age. This could be due either to stunting (low height for age) or wasting (low weight for height). Moderate wasting is weight for height z score (WHZ) less than 2 and severe wasting WHZ less than 3. Stunting is a result of chronic undernutrition and these chil- dren require multiple interventions to improve their health and well-being. Wasting and/or nutritional oedema signifies acute malnutrition and requires immediate and intense intervention. All degrees of malnutrition impact negatively on health. Because of the large numbers affected, the great majority of malnutrition- associated deaths occur in mild and moderately underweight children. However, compared with children with a WHZ greater than 1, the odds ratio for mortality is estimated to be 3.0 for Based on data of the Child Mortality Estimation Group used in the UNICEF report ‘The State of the World’s Children 2008’ Neonatal 37% AIDS 3% Over a third of all deaths are attributable to undernutrition Injuries 3% Measles 3% Malaria 3% Other 10% Diarrhoea 17% Pneumonia 19% Figure 1 Global cause specific mortality in children under 5 years of age. Criteria for the diagnosis of severe acute malnutrition One or more of:- C Weight for height z score of less than 3 C Presence of bilateral pitting pedal oedema C Mid upper arm circumference (MUAC) of less than 11.5 cm Box 1 Emily Walton MB BS MRCPCH is ST4 in Paediatrics at the West Middlesex University Hospital, Middlesex, UK. Conflict of interest: none. Stephen Allen MB ChB MRCP(UK) Diploma of Tropical Medicine and Hygiene MD is Professor of Paediatrics and International Health at the Swansea Medical School, Swansea UK. Conflict of interest: none. SYMPOSIUM: NUTRITION PAEDIATRICS AND CHILD HEALTH 21:9 418 Ó 2011 Published by Elsevier Ltd.
-
Upload
emily-walton -
Category
Documents
-
view
214 -
download
1
Transcript of Malnutrition in developing countries

Neonatal
37%
AIDS
3%
Injuries
3%
Measles
3%
Malaria
3%
SYMPOSIUM: NUTRITION
Malnutrition in developingcountriesEmily Walton
Stephen Allen
Based on data of the Child Mortality Estimation Group used in the UNICEF
report ‘The State of the World’s Children 2008’
Over a third of
all deaths are
attributable to
undernutrition
Other
10%
Diarrhoea
17%
Pneumonia
19%
AbstractAlthough now rare in industrialized countries, severe acute malnutrition is
unfortunately still common throughout the developing world and is a key
contributor to both global childhood morbidity and mortality. This review
describes the epidemiology of malnutrition and the presentation and
pathophysiology of the severe syndromic forms e marasmus and kwash-
iorkor. The gold standards for diagnosis and management are detailed
and the challenges of implementation in the basic healthcare systems
of the developing world are discussed. As the leading cause of ill health
in the world today, more effective treatment and prevention of malnutri-
tion must be a priority for the global healthcare community.
Keywords kwashiorkor; marasmus; protein-energy malnutrition; severe
acute malnutrition; underweight
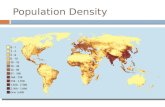
Figure 1 Global cause specific mortality in children under 5 years of age.
Underweight: the leading cause of ill health in the world todayIn 2008, of the 8.8 million global deaths of children under 5 years
of age, 93% occurred in the developing countries of Africa and
Asia. The highest rates of childhood mortality are found in
sub-Saharan Africa where one in seven children die before their
fifth birthday. Outside the neonatal period, the most common
primary causes of death are pneumonia (19%) and diarrhoea
(17%) but over a third of all deaths can be attributed to under-
lying undernutrition (see Figure 1). It is estimated that there are
148 million underweight children: 78 million live in South Asia
and 36 million in sub-Saharan Africa. In the developing world,
20% of children are underweight and 3.5% (19 million) are
severely malnourished. Millennium Development Goal 4
(a reduction in global under-5 mortality by 2/3 between 1990 and
2015) will only be achieved if significant gains in both the
prevention and management of malnutrition are made.
As well as causing loss of life, malnutrition results in
substantial morbidity and loss of quality of life; long-term
developmental problems and educational underachievement
diminish the ability to work thereby reducing potential for
national development. When calculated as disability-adjusted life
years, underweight in childhood is the leading global risk factor
for ill health in the world today.
Emily Walton MB BS MRCPCH is ST4 in Paediatrics at the West Middlesex
University Hospital, Middlesex, UK. Conflict of interest: none.
Stephen Allen MB ChB MRCP(UK) Diploma of Tropical Medicine and Hygiene MD is
Professor of Paediatrics and International Health at the Swansea
Medical School, Swansea UK. Conflict of interest: none.
PAEDIATRICS AND CHILD HEALTH 21:9 418
Definitions and diagnosis
The diagnosis of malnutrition is based on measurement of body
size (anthropometry) and clinical signs (see Box 1).
Based on the 2006WHO Child Growth Standards, underweight
is defined as a weight that is greater than 2 standard deviations
(or “z scores”) below the median expected weight for age. This
could be due either to stunting (low height for age) orwasting (low
weight for height). Moderate wasting is weight for height z score
(WHZ) less than �2 and severe wasting WHZ less than �3.
Stunting is a result of chronic undernutrition and these chil-
dren require multiple interventions to improve their health and
well-being. Wasting and/or nutritional oedema signifies acute
malnutrition and requires immediate and intense intervention.
All degrees of malnutrition impact negatively on health. Because
of the large numbers affected, the great majority of malnutrition-
associated deaths occur in mild and moderately underweight
children. However, compared with children with a WHZ greater
than �1, the odds ratio for mortality is estimated to be 3.0 for
Criteria for the diagnosis of severe acute malnutrition
One or more of:-
C Weight for height z score of less than �3
C Presence of bilateral pitting pedal oedema
C Mid upper arm circumference (MUAC) of less than 11.5 cm
Box 1
� 2011 Published by Elsevier Ltd.

Figure 3 Child with kwashiorkor (lower limb oedema, sparse depigmented
hair, dermatitis with areas of hypo- and hyperpigmentation, angular
stomatitis).
SYMPOSIUM: NUTRITION
WHZ less than �2 and 9.4 for WHZ less than �3. Therefore,
severely wasted children are the focus of in-patient treatment
programmes.
In the resource limited settings where malnutrition is
common, accurate measurement of weight and height may not
be possible and calculation of age and access to, and correct use
of, the reference norms may also be difficult. MUAC (mid upper
arm circumference) may be more appropriate in these situations
as it can be measured more easily. MUAC is relatively constant
from 6 months to 5 years avoiding the requirement for accurate
calculation of age. MUAC of less than 11.5 cm and WHZ of
less �3 identify similar proportions of children and are associ-
ated with similar risks of mortality.
In the most basic settings where no measurements are
possible, diagnosis is based on the presence of visible signs of
severe wasting and nutritional oedema. There are two well-
recognized malnutrition syndromes. Children with marasmus
(see Figure 2) have severe muscle wasting and minimal adipose
tissue; they are often noted to be irritable. Children with
kwashiorkor (see Figure 3) present with oedema and may show
other classical features including dermatitis, sparse depigmented
hair and hepatomegaly; they are typically described as apathetic.
Nutritional oedema (i.e. pitting oedema of both feet with no
identifiable cause such as nephrosis) increases weight and,
therefore, may result in a misleadingly high WHZ score. Many
children present with clinical features of both syndromes.
Whichever diagnostic criteria are used, they must be applied
consistently. All children who present to a health facility, what-
ever the reason, should have their nutritional status assessed. If
treatment is prescribed for the presenting condition but there is
a failure to identify and address underlying malnutrition then an
opportunity to reduce long-term mortality has been lost.
Aetiology and pathophysiology
Impaired growth may result from a combination of inadequate
nutrient intake, increased losses (diarrhoeal episodes, vomiting)
and increased energy expenditure (usually due to infections).
Kwashiorkor is from the Ghanaian Kwa language meaning ‘the
deposed child’ and relates to the child being displaced from the
breast by a newborn sibling. Indeed, malnutrition often presents
around the time of weaning. This is a critical period when breast
milk no longer provides adequate calories for growth but
weaning foods may be nutritionally incomplete and also a source
Figure 2 Child with marasmus (marked wasting, prominent ribs, increased
axillary skin folds, ‘old man’ face).
PAEDIATRICS AND CHILD HEALTH 21:9 419
of infection e especially enteric infections. It is usually difficult to
determine the exact sequence of events in any one child; rather,
malnutrition and infection appear to exist in a vicious circle with
each increasing susceptibility to the other.
Several specific pathological mechanisms have been identified
in malnourished children. Even in the absence of overt infection,
micro-organisms may still play a crucial role. In unhygienic
environments, it is postulated that small bowel bacterial over-
growth leads to a T-cell mediated enteropathy with variable
degrees of villous atrophy and crypt hyperplasia. This enterop-
athy impairs nutrient digestion and absorption and, as a result of
increased mucosal permeability, may result in persistent stimu-
lation of the systemic inflammatory response and sepsis from
bacterial translocation.
Although the nutritional oedema of kwashiorkor was first
described in the 1930s, the underlying pathological mechanism is
still not fully understood. The long held assumption was that
children with kwashiorkor had a disproportionate lack of protein
in their diet resulting in lower plasma albumin concentrations
and reduced oncotic pressure. This caused fluid leak into the
interstitium and the contracted intravascular volume triggered
salt and water retention by the kidney, so further worsening the
oedema. However, the diets of children with marasmus and
kwashiorkor have not been found to be significantly different
and a low protein diet has not consistently produced a kwashi-
orkor-like syndrome in animal models.
� 2011 Published by Elsevier Ltd.

History
History of presenting complaint
C Appetite e recent oral intake
C Recent weight change/swelling of feet
C Diarrhoea (frequency, consistency, presence of blood)
C Fever
C Cough (acute or chronic)
Past medical history
C Pregnancy and neonatal history (preterm? low birthweight? birth
asphyxia?)
C Significant illnesses
C Contact with TB/measles
C Known/suspected HIV
Drug history
C Regular medications (including traditional/herbal)
C Immunizations and routine vitamin A supplementation
Dietary History
C Infant feeding (duration of exclusive/supplementary breast-
feeding, use of infant formula/non-human milk, age and diet at
weaning)
C Current diet (number of meals/snacks per day, type of food,
protein sources, communal serving of food or designated
portion)
Family history
C TB
C HIV
Social history
C Family structure (number of living parents/carers, number of
siblings, birth order, polygamy)
C Economic (parental/carer occupation, household income, food
availability)
C Accommodation (crowding, water source, sanitation)
Box 2
SYMPOSIUM: NUTRITION
One theory is that the scavenger pathways that usually protect
against self-harm from the free radicals produced to destroy
infectious organisms are underactive in children predisposed to
kwashiorkor. A lack of the trace elements and antioxidants
required to dispose of harmful free radicals allows them to
damage cell membranes leading to increased vascular perme-
ability and oedema as well as the other features of tissue damage.
The finding of higher levels of iron (a catalyst for damaging free
radical reactions) in children with kwashiorkor is consistent with
this hypothesis. However, treatment with a variety of antioxi-
dants has not been shown to prevent kwashiorkor.
A recent theory is that children with kwashiorkor have
a genetic predisposition to underexpress certain glycosamino-
glycans in the intestinal mucosa, as well as in other body tissues.
These polysaccharides, found in all connective tissues and
basement membranes, play a role in maintaining mucosal
integrity and their deficiency could result in fluid leak. Duodenal
biopsies of Zambian children with kwashiorkor showed
a marked deficiency of heparin sulphate proteoglycan (HSPG).
As HSPG has multiple functions in the body (including roles in
free fatty acid uptake and keratinocyte adhesion) other features
of kwashiorkor such as fatty liver and exfoliative dermatitis
could be explained and HSPG deficiency may provide a unifying
hypothesis for the syndrome.
In both marasmus and kwashiorkor normal physiology is
deranged by a process called ‘reductive adaptation’ in which the
body attempts to survive on minimal energy. It does this both by
catabolizing tissue reserves of carbohydrate, fat and protein and by
down-regulating certain physiological and metabolic processes.
Physical activity and growth are minimized and basal metabolic
rate is slowed. One outcome is a decrease in the number and
function of NaeK pumps in cell membranes resulting in leakage of
sodium into cells and loss of potassium into the extracellular space
and thence into the urine. The net effects are an increase in total
body sodium with a decrease in plasma and total body potassium.
The function of all the major organs is impaired. The kidneys are
less able to excrete the extra sodium. Cardiac muscle is atrophied
and hypokalaemia also contributes to poor contractility and
reduced cardiac function. Hepatic glucose stores are depleted and
gluconeogenesis impaired. Nutrient digestion and absorption is
impaired by reduced production of acid and enzymes, villous
atrophy and decreased gut motility. The immune and inflamma-
tory systems become dormant and the body does not mount
normal responses to infection or injury.
An understanding of these complex physiological changes is
necessary for the effective management of severe malnutrition. If
treatment does not take account of reductive adaptation, lives
will be lost not just due to the underlying disease processes but
also through faulty management.
Clinical evaluation
History
Aspects of the history to be covered in all malnourished children
are listed in Box 2. A thorough dietary history is necessary to
elicit inappropriate feeding practices such as supplementation of
breast milk with water, early or late weaning and withholding
feeds during diarrhoea. A detailed social history is also vital to
obtain background information on the family and the mother’s
PAEDIATRICS AND CHILD HEALTH 21:9 420
ability to provide nutritional and other care to this child and
other children in the family. This information will also be crucial
in deciding whether in-patient or out-patient care is most
appropriate.
Examination
As well as searching for the specific signs of the malnutrition
syndromes (as detailed in Box 3) a thorough systemic examina-
tion should be performed to detect any co-morbidities (e.g. renal
disease, congenital cardiac defects) that could predispose to
malnutrition. Signs of shock, severe anaemia and hypothermia
should be elicited and appropriate emergency management
initiated.
Accurately assessing the hydration status in a malnourished
child is notoriously difficult. Atrophy of salivary and tear glands
results in dry mucous membranes even when well hydrated. Loss
of subcutaneous tissue gives the impression of persistently
decreased tissue turgor. Poor cardiac output may prolong
� 2011 Published by Elsevier Ltd.

Examination
C Temperature: fever or hypothermia
C Signs of shock: cold hands with capillary refill time greater than
3 s and weak, fast pulse and lethargic or unconscious
C Signs of dehydration (beware: may be unreliable in the
malnourished child)
C Oedema
C Signs of severe wasting (‘old man’ face, emaciated limbs, clearly
visible ribs, increased axillary skin folds, buttock wasting)
C Pallor
C Localizing signs of infection (ear, throat, skin, chest)
C Mouth (ulcers, angular stomatitis, oral thrush)
C Skin (‘flaky paint’ dermatitis, areas of hypo- and hyperpigmen-
tation in kwashiorkor; thin and flaccid in marasmus)
Box 3
SYMPOSIUM: NUTRITION
capillary refill time. Decreased renal blood flow and impaired
renal function decrease urine output. The most reliable measure
of dehydration is current weight in comparison to a recent
accurate weight.
Signs of localizing infection should be searched for whilst
recognizing that theymay be absent even in the presence of severe
infection due to impaired immune and inflammatory responses.
Differentiation fromHIV infection can be difficult but malnutrition
alone does not typically cause generalized lymphadenopathy.
Tuberculosis (TB)may co-present withmalnutrition but diagnosis
can be a challengee particularly because theMantoux test may be
falsely negative.Where malnutrition does not respond to standard
care, a trial of anti-TB treatment may be necessary.
Investigations
Access to investigations is likely to be limited in the resource
limited settings where malnutrition is prevalent. If blood glucose
cannot be measured, then presumptive treatment for hypo-
glycaemia should be initiated. The presence and degree of
anaemia may need to be assessed clinically. In parts of the world
where malaria is endemic, a blood film should be examined for
malarial parasites.
Even if available, measurement of plasma electrolytes may be
misleading as they will not accurately reflect total body stores
and, therefore, empirical management may actually be safer than
using plasma levels to guide fluid therapy.
Other investigations include a chest X-ray (to screen for TB)
and HIV testing (discussed later). It is unlikely that a specific
pathogen will be identified in persistent diarrhoea but stool
culture is indicated in dysentery.
Management
Where should malnourished children be managed?
Current guidelines recommend integrated management involving
both in-patient and community services. Children with compli-
cations (severe infections or metabolic disturbances) should
begin treatment in an in-patient facility whereas those with no
complications can progress directly to an out-patient therapeutic
programme (OTP). A simple test to help discriminate between
PAEDIATRICS AND CHILD HEALTH 21:9 421
these two groups is the ‘appetite test’. A good appetite is a reli-
able sign that the child does not have any serious hidden
complications. The child is encouraged to eat an appropriate
portion of ready-to-use therapeutic food (RUTF) over the course
of about an hour. The child who has appetite and no obvious
complications can embark immediately on an OTP.
RUTFs are high energy and protein foods enriched with
electrolytes, minerals and vitamins. They will keep for months at
ambient temperature in the packaging they are distributed in and
do not require cooking or the addition of water. This makes them
microbiologically safe even in the harsh environments of the
developing world. ‘Plumpy Nut’, the most widely used, is made
from peanut paste, milk powder, oil and sugar with added
potassium, magnesium, vitamins and minerals. Each 92 g sachet
provides 500 kcal.
OTPs are usually based in local health centres. At registration
the child will be given a course of broad spectrum oral antibiotics.
They then attend weekly for weighing and for the distribution of
quantities of RUTF appropriate to their current weight. OTPs are
generally popular with families but weight gain is usually not as
rapid as in in-patient programmes. RUTFs are very palatable and
in home based treatment there may be a temptation to share
rations with other children (and adults!) in the household.
OTPs are also the most appropriate setting to manage
moderate malnutrition. The aim is to provide nutritious food
rations, preferably based on locally available foods, and appro-
priate health education to promote recovery and, critically,
prevent progression to severe malnutrition.
The WHO 10 steps protocol
Admission to hospital has several disadvantages. Overcrowding
permits the spread of nosocomial infections and in-patient treat-
ment can be expensive for the family e either through direct costs
of services or through loss of earnings for the caregiver. The health
of other children in the family and the consequences of removing
the mother from the household should also be taken into account.
However, in-patient treatment is essential for the intensive
management and closemonitoring of childrenwith complications.
Highmortality rates are common: 25e30% case fatality is found in
many hospitals in Africa and rates as high as 50e70% are some-
times reported. High mortality is often attributed to incorrect
management; a review in two South African hospitals in
2000e2001 ascribed 50% of deaths to doctor error and 28% to
nurse error. High mortality results from a failure to take into
account the abnormal physiology of severe malnutrition and to
manage these children by the same principles as those of a normal
weight. Doing so leads to avoidable deaths from hypoglycaemia,
hypothermia, infection, heart failure and electrolyte imbalance.
In an attempt to improve outcomes and reduce deaths, the
WHO has produced a standard protocol for the in-patient
management of both oedematous and non-oedematous malnu-
trition. This protocol consists of 10 steps divided between two
phases e a stabilization and a rehabilitation phase (see Figure 4).
In the stabilization phase, acute problems are tackled in a way
that is specific for the malnourished child. The aim of this phase
is not to achieve weight gain but rather to remedy the metabolic
and biochemical disturbances that have developed and to allow
the child to safely enter the rehabilitation phase e during which
weight should be regained.
� 2011 Published by Elsevier Ltd.

Taken from the World Health Organization’s ‘Pocket book of Hospital care for children’ 2005.
1. Hypoglycaemia
2. Hypothermia
3. Dehydration
4. Electrolytes
5. Infection
6. Micronutrients
7. Initiate feeding
8. Catch-up growth
9. Sensory stimulation
10. Prepare for follow-up
NO IRON WITH IRON
Stabilization
Days 1–2 Days 3–7
Rehabilitation
Weeks 2–6
Figure 4 Outline of priorities and time frame in the management of severe acute malnutrition.
SYMPOSIUM: NUTRITION
Common complications of severe malnutrition that require
specific management:
1. Treat/prevent hypoglycaemia
Unless blood glucose of �3 mmol/L can be demonstrated,
hypoglycaemia should be presumed and treated with enteral
glucose: give 10% dextrose or a milk feed immediately. Only if
the child is unconscious should intravenous glucose be given.
Hypoglycaemia is prevented by giving all new admissions
frequent feeds (2e3 hourly) throughout the day and night.
2. Treat/prevent hypothermia
Malnourished children are at high risk of hypothermia (axil-
lary temperature less than 35 �C or unrecordable) because they
have minimal insulative body fat and no energy stores to produce
their own heat. Hypothermia should be managed with an
immediate feed and active rewarming. An effective way of
rewarming is ‘kangaroo care’: skin-to-skin with the mother with
a blanket covering both.
3. Treat/prevent dehydration
As previously discussed, clinical signs of dehydration can be
difficult to interpret. Therefore, all children with watery diar-
rhoea should be assumed to be dehydrated. Intravenous rehy-
dration should be avoided (unless signs of shock are present) due
to the risk of precipitating heart failure. Enteral rehydration
should be slower than usual and use a modified version of oral
rehydration solution (ORS) known as ReSoMal (Rehydration
Solution for Malnutrition).
4. Correct electrolyte imbalance
ReSoMal contains more potassium and less sodium than
standard ORS and is therefore more suitable for malnourished
children in view of their typical electrolyte shifts and imbalances.
The initial milk formula (F75) recommended for feeding also has
added potassium and magnesium and restricted sodium. The
extra potassium should allow the kidney to excrete the excess
sodium and fluid and oedema should gradually dissipate.
Oedema should never be treated with diuretics.
5. Treat/prevent infection
Infection should be assumed and all children treated empiri-
cally with broad spectrum antibiotics. Local guidelines should be
PAEDIATRICS AND CHILD HEALTH 21:9 422
followed (e.g. i.v. ampicillin/p.o. amoxicillin and i.v. gentamicin
for 7 days). In countries where worm infestation is prevalent,
a course of mebendazole should also be given. Strict handwashing
and other infection control measures should be adhered to.
6. Correct micronutrient deficiencies
Children should receive supplements of important trace
elements (zinc, copper, selenium), folic acid and a multivitamin
preparation. These may be added to the milk feeds at prepara-
tion. A standard dose of vitamin A should be given to all children
and a higher dose to any with ocular signs of deficiency.
Although malnourished children are usually anaemic, iron
should not initially be replaced as iron storage systems are
underactive and free iron can catalyze harmful free radical
reactions as discussed above. Once infections have been treated
and the child has entered the rehabilitation phase, iron can safely
be supplemented.
7. Start cautious feeding
The milk feed recommended for the rehabilitation phase is
F75. This can be made from locally available ingredients (milk
powder, vegetable oil, sugar and water) and contains 75 kcal/100
ml and 0.9 g protein/100 ml. Children are initially fed 130 ml/kg/
day reduced to 100 ml/kg/day in kwashiorkor to allow for the
extra weight of the oedema. Total feed volume and the energy
and protein (and therefore sodium) content of the feed are
restricted to prevent heart failure, osmotic diarrhoea and
a worsening of oedema. Poor appetite, impaired gut motility, and
decreased gastric volume mean that feeding is more successful if
smaller feeds are offered more frequently (2 hourly) and the
interval spaced as the child improves. Children may also need
a nasogastric tube for feeding early in the course of their treat-
ment. Success in refeeding relies on the regular provision of
frequent feeds, encouraging children to complete their feeds, and
accurately recording feeds consumed to assess readiness to move
into the rehabilitation phase. This can be a challenge in busy
hospitals where staffing ratios are often poor and strict time-
keeping not always part of the culture. Empowering mothers to
involve themselves in the care of their children is a means of
attempting to overcome these challenges.
� 2011 Published by Elsevier Ltd.

SYMPOSIUM: NUTRITION
8. Achieve catch-up growth
Once acute medical problems have been dealt with and the
child’s appetite has improved they are ready to enter the reha-
bilitation phase. The starter F75 formula is replaced with F100
formula (100 kcal/100 ml and 2.9 g protein/100 ml) and volumes
increased according to the child’s demand. The higher energy
and protein content of F100 should result in rapid weight gain
assessed in g/kg/day. A weight gain of greater than 10 g/kg/day
is considered good; 5e10 g/kg/day moderate; and less than 5 g/
kg/day poor. At this stage of treatment, dependent on individual
circumstances, children can often be transferred to out-patient
care and RUTF offered instead of F100.
9. Provide sensory stimulation and emotional support
Although usually unintentional, malnourished children have
suffered a form of neglect. They should receive tender nursing
care in a stimulating environment with opportunities for play and
physical therapy as they recover.
10. Prepare for follow-up
Recovery is considered to be a WHZ score of �1. This may
take up to 6 weeks to achieve. Before discharge from in-patient or
out-patient care, endeavours must be made to ensure the child
will not relapse. Caregivers should receive health and nutrition
education and be alerted to the signs of deterioration and when
to seek medical care. Scheduled follow-up appointments should
also be planned over at least the first 6 months.
Special groups
Infants younger than 6 months: traditionally malnutrition has
been considered a condition that develops after the age of 6
months and management guidelines are aimed at children
greater than 6 months old. However, increasing numbers of
young infants are presenting with both non-oedematous and
oedematous malnutrition. Possible reasons for this include
increased survival of low birthweight and premature babies and
failure to exclusively breastfeed (for a variety of reasons
including increased prevalence of maternal HIV). The younger
the child the more likely an organic cause of malnutrition further
highlighting the importance of a thorough assessment to detect
any underlying medical conditions.
Breast milk is the ideal nutrition for these infants but is often
not available in sufficient quantities and the child may be too
unwell to suckle effectively by the time they reach the attention of
health services. There is currently no consensus on the optimum
nutritional management in the rehabilitation phase if breast milk,
or a commercial infant formula, are not available. F100 has a high
potential renal solute load and its use could result in hyper-
natraemic dehydration e particularly in hot, dry environments.
Some practitioners advocate the use of a diluted version of F100 as
a safer alternative. However, studies of its use have not shown it to
consistently support the rapid weight gain required. Additional
guidance on the management of infants less than 6 months is
anticipated in the next edition of the WHO treatment protocol.
HIV positive children: there is debate as to whether malnour-
ished children should be routinely screened for HIV infection.
The increasing availability of antiretroviral medication, as well as
the opportunity to access prophylactic co-trimoxazole, suggest
that it will now be helpful to check HIV status. However, treat-
ment facilities must ensure that nursing staff are educated about
PAEDIATRICS AND CHILD HEALTH 21:9 423
the disease to ensure that families are not stigmatized and that
children do not receive inferior care due to a belief that their
demise is inevitable. HIV positive malnourished children should
follow the same protocol as HIV negative children with the
addition of prophylactic co-trimoxazole. Severe oral thrush can
inhibit feeding and may need treatment with fluconazole. When
to start antiretrovirals should be based on the level of immuno-
suppression (CD4 count) and stage of malnutrition treatment
according to local protocols.
Prevention
As detailed above, management of the severely malnourished
child presents a huge challenge, especially in inadequately staf-
fed and resourced health facilities. Even when the WHO 10 steps
are applied rigorously, mortality often remains high. Therefore,
prevention of malnutrition is a priority for governments and
other organizations interested in reducing child mortality. As
malnutrition is both a medical and socioeconomic condition,
a range of interventions are necessary.
An essential component of any preventive strategy is the
promotion of breastfeeding. The WHO recommends exclusive
breastfeeding until 6 months of age with supplementary breast
milk forming an important part of the diet up to 2 years of age.
Currently only 24e32% of infants in developing countries are
exclusively breastfed up to 6 months. The WHO ranks subop-
timal breastfeeding as the 7th most significant risk factor for
global burden of disease. The uncompromising guidelines of the
Baby Friendly Hospital Initiative e now familiar in many UK
maternity units e were originally intended for use in the devel-
oping world where breastfeeding is truly a life-saving interven-
tion. Infant formula milks are inferior to breast milk both in
nutritional composition and lack of immunological protection
against infectious diseases, in particular gastroenteritis and
pneumonia. In poor societies where many mothers are illiterate
and innumerate, producing appropriately concentrated and
hygienic milk from instructions on a tin of powder is unlikely to
be achieved. Furthermore, the cost may result in a temptation to
over-dilute infant formula or to purchase a cheaper, non-
modified, animal milk.
Other health education approaches include the promotion of
nutrient rich weaning foods and discouraging the over-reliance
on carbohydrate dense staple foods. This is combined with an
active programme of routine child health surveillance with
regular weight monitoring to detect children at risk of severe
malnutrition and target interventions. Increasing coverage of
immunization and vitamin A supplementation should help
prevent the infectious diseases that can often trigger severe
malnutrition in an already undernourished child. Primary care
services must also be available to ensure the prompt treatment of
childhood illnesses that can precipitate or worsen malnutrition.
Improvement of a community’s sanitation and hygiene via the
provision of toilets (currently available to only 59% of the
world’s population) and the promotion of handwashing with
soap will also be crucial in improving children’s nutritional
status e particularly if tropical enteropathy is confirmed as a key
contributing factor to malnutrition.
The large family sizes common in many developing countries
make it difficult for mothers both to offer optimal breastfeeding
� 2011 Published by Elsevier Ltd.

Practice points
C Children presenting to healthcare facilities should routinely
have their nutritional status assessed.
C Treatment of the 2 main forms of malnutrition should be stan-
dardized and take account of reductive adaptation to prevent
avoidable deaths.
C Treatment programmes should be community based where
possible but the most severely affected children will still need
intensive in-patient management.
C Strategies to prevent malnutrition should be aimed at both
individuals and communities and must tackle the wide range of
medical, social and economic causes.
SYMPOSIUM: NUTRITION
to each child, and to provide a diet, once weaned, of appropriate
quantity and quality. Improving availability and accessibility of
family planning services to either limit family size or to space
pregnancies is therefore another important tactic in the preven-
tion of malnutrition. For mothers to act as effective advocates for
their children, the broader aim of empowering women and
improving levels of female education must also be addressed.
With just 5 years left to achieve the Millennium Development
Goals there is a clear need to confront childhood undernutrition
as the single most important risk factor for ill health in the world
today. Mounting evidence for the efficacy of simple interven-
tions, such as exclusive breastfeeding and improved sanitation,
should aid governments and society in tackling this threat. A
FURTHER READING
Amadi B, Fagbemi AO, Kelly P, et al. Reduced production of sulfated
glycosaminoglycans occurs in Zambian children with kwashiorkor but
not marasmus. Am J Clin Nutr 2009; 89: 592e600.
Ashworth A, Chopra M, McCoy D, et al. WHO guidelines for management
of severe malnutrition in rural South African hospitals: effect on case
fatality and the influence of operational factors. Lancet 2004; 363:
1110e5.
Berkley J, Mwangi I, Griffiths K, et al. Assessment of severe malnutrition
among hospitalized children in rural Kenya: comparison of weight for
height and mid upper arm circumference. J Am Med Assoc 2005; 294:
591e7.
Bhutta ZA, Chopra M, Axelson H, et al. Countdown to 2015 decade report
(2000e10): taking stock of maternal, newborn, and child survival.
Lancet 2010; 375: 2032e44.
Black RE, Allen LH, Bhutta ZA, et al. Maternal and child undernutrition:
global and regional exposures and health consequences. Lancet 2008;
371: 243e60.
PAEDIATRICS AND CHILD HEALTH 21:9 424
Hamer C, Kvatum K, Jeffries D, Allen S. Detection of severe protein-energy
malnutrition by nurses in The Gambia. Arch Dis Child 2004; 89:
181e4.
Humphrey JH. Child undernutrition, tropical enteropathy, toilets, and
handwashing. Lancet 2009; 374: 1032e5.
UNICEF. The State of the World’s Children; 2008.
World Health Organization. Global health risks: mortality and burden of
disease attributable to selected major risks; 2009.
World Health Organization. Pocket book of hospital care for children.
Guidelines for the management of common illnesses with limited
resources; 2005.
World Health Organization and United Nations Children’s Fund. WHO child
growth standards and the identification of severe acute malnutrition in
infants and children; 2009.
World Health Organization. Severe malnutrition: report of a consultation
to review current literature; 2005.
� 2011 Published by Elsevier Ltd.