Malnutrition 2
54
M ana ge m e n t of Severe Acute M al n u triti o n JFK p e d i atric core curric u l um M G H C e n ter for G lobal H ealt h P ediatri c G l o b al H ealt h L ead ers h i p F ell o w s h i p Cr ed i ts: B ret t Ne l s on , M D, M P H R ebecca Bell, M D
Transcript of Malnutrition 2

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 1/54
Management of Severe AcuteMalnutrition JFK pediatric core curriculum
MGH Center for Global HealthPediatric Global Health Leadership Fellowship
Credits:Brett Nelson, MD, MPH
Rebecca Bell, MD

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 2/54
Discussion Overview
•Defining malnutrition
•Physiologic effects of malnutrition by
system•Management of severe malnutrition byproblem
•Integrating outpatient management ofsevere malnutrition

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 3/54
Causes of MalnutritionSection 1Section 1
3
From ICH/UNHCR Handout

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 4/54
Defining Malnutrition
•Malnutrition is diagnosed if one of the following criteriais met:–Weight-for-height < 70% or <-3 SD
–Bilateral pedal oedema
–Clinical signs of severe malnutrition
•Differentiating betweenmarasmus (characterized bysevere wasting) andkwashiorkor (characterized byoedema) is not necessary for treatment as many children
display symptoms of both conditions.•It is important to identify the presence or absence ofoedema, as those children tend to do worse thanmalnourished children without edema.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 5/54
From the WHO “Management of Severe Malnutrition”

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 6/54
Signs of Marasmus
Children with marasmus have severe wasting, particularly of thearms, shoulders, thighs and buttocks. The lack of adipose tissuecauses skin to hang loosely.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 7/54
Signs of Kwashiorkor / OedematousMalnutrition
This child has oedema of the hands and feet as well asdermatosis, most prominently on the legs and groin.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 8/54
Gently press with the thumb, applying pressure to both feet at the same time.Pitting oedema leaves a small indentation which can be seen and felt

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 9/54
Other Anthropometric Indicators ofMalnutrition
•Mid Upper Arm Circumference (MUAC)
–Some studies have shown MUAC to be the single bestpredictor of mortality in children between 1 and 5
years.–Community volunteers can be easily trained tomeasure MUAC.
–MUAC is currently recommended for screening in the
community. Children who meet criteria formalnutrition are referred to a clinic or hospital forfurther evaluation.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 10/54
Measuring
MUAC

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 11/54
Physiological Effects ofMalnutrition By System
•Cardiovascular
•GI
•GU
•Immune•Liver
•Endocrine
•Cellular function
•Circulatory/Temperature regulation•Skin, muscles, glands

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 12/54
Cardiovascular SystemEffects:
•↓ cardiac output and stroke volume•↓ blood pressure•↓ renal perfusion
Concerns:•An increase in blood volume can produce acute heartfailure
•A further decrease in blood volume will compromise tissueperfusion
Management:•If dehydrated, give ReSoMal or F-75•Do not give IV fluids unless child is in shock•If blood transfusion is necessary, restrict to 10 ml/kg and
give a diuretic

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 13/54
Gastrointestinal System
Effects:•↓ production of gastric acid•↓ intestinal motility•↓ production of digestive enzymes secondary topancreatic atrophy
•↓ secretion of digestive enzymes secondary to smallintestinal mucosa atrophy•↓ absorption of nutrients when large amounts of foodingested
Management:•Give small, frequent feeds•If fat malabsorption, can give pancreatic enzymes

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 14/54
Genitourinary SystemEffects:• ↓ glomerular filtration• ↓ ability for renal excretion of acid or water load• ↓ sodium excretion• ↓ urinary phosphate output• ↑ incidence of UTI
Concerns:• A large protein load may not be well tolerated by the kidneys• Further protein deprivation will lead to continued tissue breakdown
Management:• Caloric intake should be targeted at 80-100 kcal/kg/day• Avoid nutrients that can lead to an acid load, such as magnesiumchloride
• Restrict sodium intake• Avoid excessive water intake
8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 15/54
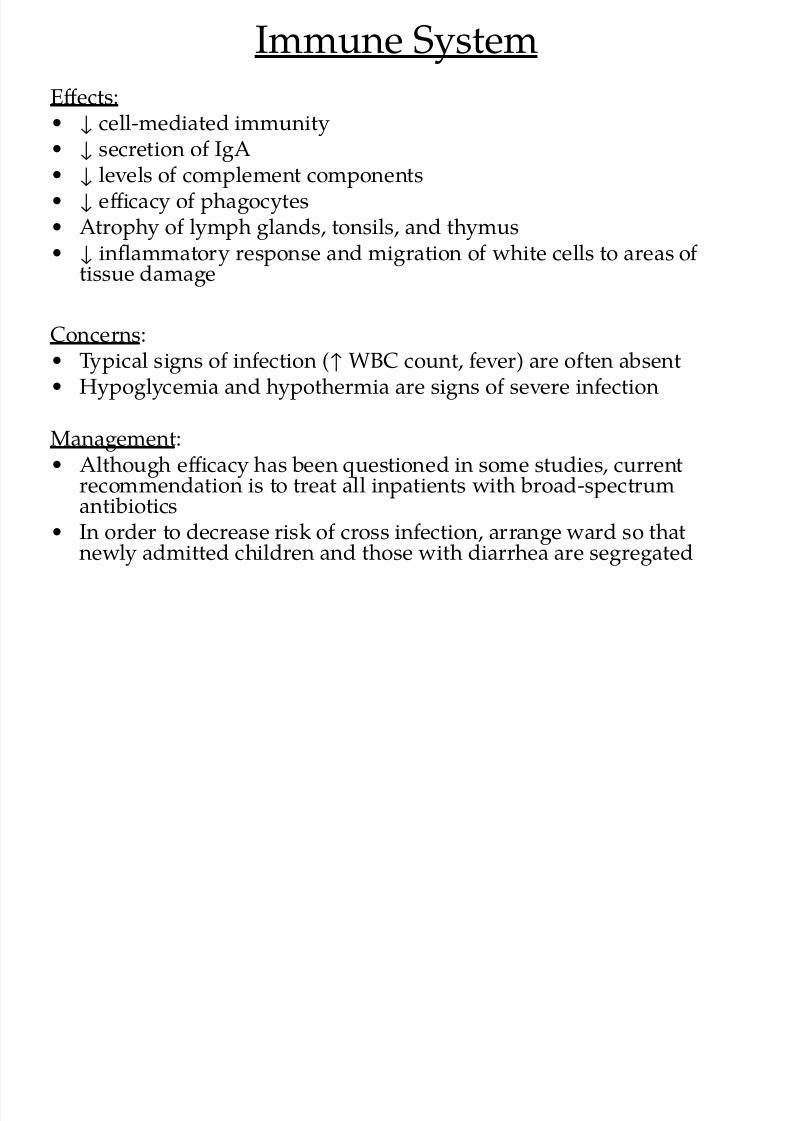
Immune System
Effects:• ↓ cell-mediated immunity• ↓ secretion of IgA• ↓ levels of complement components• ↓ efficacy of phagocytes• Atrophy of lymph glands, tonsils, and thymus• ↓ inflammatory response and migration of white cells to areas of
tissue damage
Concerns:• Typical signs of infection (↑ WBC count, fever) are often absent• Hypoglycemia and hypothermia are signs of severe infection
Management:• Although efficacy has been questioned in some studies, currentrecommendation is to treat all inpatients with broad-spectrumantibiotics
• In order to decrease risk of cross infection, arrange ward so that
newly admitted children and those with diarrhea are segregated

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 16/54
Liver
Effects:• ↓ synthesis of all proteins• ↓ bile secretion• ↓ ability of liver to take up, metabolize, and excrete toxins• ↓ gluconeogenesis• ↓ transferrin levels
Concerns:• Risk of hypoglycemia is high, particularly with infection
Management:• Protein intake should be about 1-2 g/kg/day so as to supportsynthesis of proteins but not to exceed metabolic capacity of liver
• Reduce dosage of meds that are dependent on hepatic metabolism• Ensure sufficient carbohydrate intake to avoid need forgluconeogenesis
• Do not give iron supplements

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 17/54
Endocrine System
Effects:
•↓ insulin levels, leading to glucose intolerance
•↓ levels of IGF-1
•↑ levels of growth hormone
•↑ levels of cortisol
Management:•Do not give steroids

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 18/54
Cellular Function
Effects:
•↓ synthesis of proteins•↓ activity of sodium pump
•↑ permeability of cell membranes
Concerns:
•This leads to anincrease in intracellular sodium and adecrease in intracellular potassium and magnesium
Management:
•Restrict sodium intake
•Give potassium and magnesium to all children

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 19/54
Circulatory System andTemperature Regulation
Effects:•Heat generation as well as heat loss are impaired
•↓ energy expenditure and basic metabolic rate
Concerns:•Child becomes hypothermic in cold environment andhyperthermic in hot environment
Management:•Keep child dry and warm
•Room temperature should be at 25-30 °C
•If child has fever, cool with tepid water

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 20/54
Skin, Muscles, Glands
Effects:•Skin and subcutaneous fat are atrophied
•Atrophy of sweat, tear, and salivary glands
•Respiratory muscles are fatigued easily
Concerns:
•Typical signs of dehydration (sunken eyes, abdominalskin pinch) are unreliable due to the loss ofsubcutaneous fat
Management:
•Rehydrate with ReSoMal when necessary (see protocol)

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 21/54
Inpatient Management Overview
•Management phases:–Stabilization phase: defined as the treatment period fromadmission to the point where the child’s appetite hasreturned. Typically lasts 2-7 days.
–Rehabilitation phase***: goals for this phase are weightgain, emotional development, family education, and lackof oedema, vomiting, diarrhea and fever. Typically,children are discharged 2-3 weeks after admission.
***Recent advances in outpatient management have led to asignificant decrease in the length of the rehabilitation phase, andin some cases, a complete elimination of the phase. Someinstitutions instead have a “transitional phase” where the childis prepared for discharge after stabilization.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 22/54
Evaluation at Presentation
•Medical history:–Usual diet
–Breastfeeding history
–Food and fluids in last few days
–Time when last urine passed–Duration, frequency, appearance of vomit and diarrhea
–Recent sinking of eyes
–Contact with TB or measles
–Birth weight–Developmental milestones reached
–Immunizations

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 23/54
Evaluation at Presentation
•Physical exam:–Weight, length
–Temperature
–Edema
–Hepatomegaly, jaundice
–Abdominal distension, bowel sounds
–Pallor
–Signs of circulatory collapse
–Thirst
–Corneal lesions–Signs of infection in ears, mouth, throat
–Inspect skin for signs of infection, dermatosis, purpura
–Appearance of stool

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 24/54
Goals for Management of aMalnourished Child at Admission
•Treat or prevent hypoglycemia
•Treat or prevent hypothermia
•Treat or prevent dehydration•Treat infection or septic shock, if present
•Begin feeding
•Identify and treat vitamin deficiency, severe anemia, and
heart failure

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 25/54
Hypoglycemia
•Important cause of death during first 48 hoursafter admission
•Signs include low body temperature, lethargy,limpness, loss of consciousness
•Do not wait for lab results before treating:
–give first feed of F-75 diet–If F-75 not immediately available, give 50 ml of 10%glucose or sucrose orally or via NG tube–If unconscious, give 5ml/kg of 10% glucose IV–Give 2-3 hourly feeds, day and night

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 26/54
Hypothermia
•Defined as rectal temp less than 35.5°C
•Keep child clothed, including head, limit exams and
washing, dry immediately after washing, keep heater orlamp nearby
•Check for hypoglycemia any time a child is found to be
hypothermic

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 27/54
Dehydration and Septic Shock
•Malnourished children often do not displaytypical signs and symptoms of dehydration andseptic shock.
–Salivary and lacrimal glands are atrophied so childrenwill have dry mouth and lack of tears regardless offluid status.
–Loss of subcutaneous fat makes the skin thin and
loose so a slow skin pinch does not necessarily meanthe child is dehydrated.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 28/54
Reliable Signs of Dehydration in aMalnourished Child
•History of diarrhea
•Thirst
•Recent development ofsunken eyes
•Weak or absentperipheral pulses
•Cold hands and feet
•↓ urine flow
Marasmic child with sunken eyes

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 29/54
Rehydration Solution for MalnourishedChildren (ReSoMal)
•High sodium and low potassium levels inmalnourished children make standard OralRehydration Salts (ORS) unsuitable.
•ReSoMal is commercially available, but can also be made by diluting one ORS packet in 2 liters of
water instead of 1 and adding 25 g/l of sucroseand 20 ml/l of mineral mix.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 30/54
weight ofchild(kg)
first 30minutes
(ml)
second 30minutes
(ml)2nd hour (ml)
2! " 2# $! $! 2!
%! " %# $& $& %!
'! " '# 2! 2! '!
&! " &# 2& 2& &!
(! " (# %! %! (!
)! " )# %& %& )!
*! " *# '! '! *!
#! " ## '& '& #!
$!! " $!# &! &! $!!
$$! " $$# && && $$!
$2! " $2# (! (! $2!
$%! " $%# (& (& $%!
$'! " $'# )! )! $'!
$&! " $&# )& )& $&!
ReSoMal Protocol(Rehydration solution for marasmicchildren)DO NOT use for oedematous children
To be used ONLY after careful diagnosis ofdehydration (history and clinical signs).
For children with OEDEMA, do not giveReSoMaL in an outpatient setting, use 10%sugar water only.
Monitor regularly. If respiratory rateincreases or there is increasing oedema(e.g. of eyelids) or neck veins becomedistended, stop ReSoMaL. Reassess afterthe 1st hour. If there is improvement in
symptoms advise carer to continue breastfeeding and to give extra water athome (small quantities every hour) untilchild is no longer thirsty.
If no improvement or further deteriorationrefer to inpatient facility.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 31/54
Signs of Septic Shock in aMalnourished Child
•Incipient septic shock:–Limpness, apathy, anorexia, hypothermia, cold handsand feet, weak peripheral pulses, ↓ urine flow
•Developed septic shock:–Dilated superficial veins (scalp and external jugularveins), dilated pulmonary veins leading to grunting,shallow cough, difficulty breathing
–Development of renal, cardiac, liver, and intestinalfailure–Hematemesis, melena, abdominal distension withabdominal splash

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 32/54
Infection in the Malnourished Child
•Malnourished children often have no signs ofinfection. Therefore, on admission, all childrenshould receive antibiotic treatment according to
local resistance patterns.
•Suggested regimen:
–If no signs of infection and no complications•Cotrimoxazole (25/5) PO BID x 5 days

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 33/54
Antibiotic Treatment in Children withComplications
•Complications include:–Septic shock–Hypoglycemia–Hypothermia–Skin infection–UTI–Lethargy
•Suggested regimen:–Ampicillin 50mg/kg IM/IV every 6 hours x 2 days,followed by amoxicillin 15mg/kg PO every 8 hours x5 days

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 34/54
More on Infections
•If child fails to respond in 48 hours, add:–Chloramphenicol 25mg/kg IM/IV every 8 hours x 5days
•Follow WHO or local treatment protocols formanagement of dysentery, candidiasis,helminthiasis
•All children should be tested for malaria upon
admission and treated accordingly•All children should receive a measles vaccine onadmission
8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 35/54
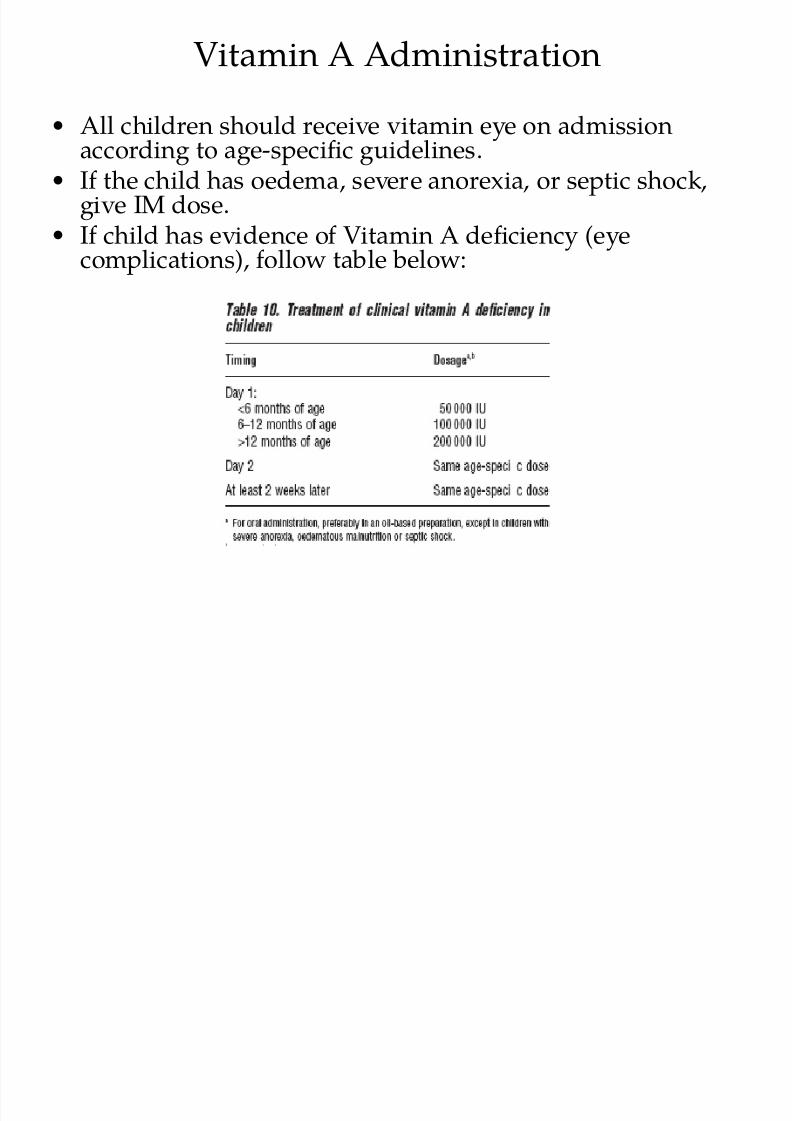
Vitamin A Administration
•All children should receive vitamin eye on admissionaccording to age-specific guidelines.
•If the child has oedema, severe anorexia, or septic shock,give IM dose.
•If child has evidence of Vitamin A deficiency (eyecomplications), follow table below:

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 36/54
Eye Care
•Eyes should be examined gently for signs ofxerophthalmia, corneal xerosis and ulceration,cloudiness and keratomalacia
•Management of ocular inflammation orulceration:
–Cover eyes with pads soaked with 0.9% saline
–Apply 1% tetracycline eye drops 4 times a day

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 37/54
Complications of Vitamin A Deficiency
Keratomalacia with Bitot's Spots:discrete, foamy-appearing spots onthe conjunctiva
Copyright © Online Journal of Ophthalmology
Corneal ulcer: small ulcer withclouding of the central cornea

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 38/54
Severe +nemia
•WHO recommends blood transfusion when the
haemoglobin drops below 30g/l (or packed-cell volume below 10%), or if child is showing signs of life-threatening heart failure.
•Give 10 ml/kg slowly over 3 hours.
,almar -allor in a .everel anemi0 0hild

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 39/54
Dermatosis of Kwashiorkor
• Characterized by hypo- or hyperpigmentation, shedding and
ulceration of the skin especially in legs, perineum, and groin.• Bathe affected areas in 1% KMnO4for 10-15 daily
• Apply zinc and castor oil ointment, petroleum jelly, or paraffin gauzedressings
• All children with dermatosis should receive antibiotics. If areas show
signs of candida infection, treat with topical and oral nystatin.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 40/54
Formula Diets Used in the Treatment ofMalnourished Children
•F-75–75 kcal/100 ml
–Used during initial treatment
•F-100–100 kcal/100 ml
–Used during rehab phase, once appetite has returned
•RUTF(Ready-to-use therapeutic food)
–Mixture of peanut paste, sugar, oil, powdered milk,and vitamin/mineral mix
–Similar composition as F-100, but non-water based sodoes not spoil
–Can be given at home

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 41/54
Feeding Tips
•Strictly follow feeding tables that determine volumeand frequency of feeds for weight.
•Feeding by mouth is always better, but if a child will
not take food, an NG tube must be placed.•Children should continue to breastfeed.
•Children should be fed with cup and spoon, ordropper – never with a bottle as these can be sources
of infection.•Carefully record food intake. Standard recordingforms are available.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 42/54
RUTF1 e.igned 3 Fren0h .0ienti.t +ndre 4riend in $### and
manufa0tured under the 3rand name ,lum-5nut 3Nutri.et
1 In Mala6i7 RU8F i. -rodu0ed in"0ountr u.ing lo0al
ingredient. mi9ed 6ith vitamin/mineral -a0:. from
Nutri.et

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 43/54
Plumpy’nut® (RUTF)
Paste of groundnut composed of vegetable fat, peanut butter, skimmed milkpowder, lactoserum, maltodextrin, sugar and mineral and vitamin complex.
Instructions for use: Clean drinking water must be made available tochildren during consumption of ready-to-eat therapeutic spread. Theproduct should only be given to children who can express their thirst.Contra-indicated for children who are allergic to cows milk, proteins or
peanuts and asthmatic people (risk of allergy).
Recommendations for use: In the management of severe acute malnutritionin therapeutic feeding, it is recommended to use the product in phase 2 (two)in the dietetic management of severe acute malnutrition. In phase 1 (one) use
milk based diet (F75).
Storage of Plumpy’nut: Plumpy’nut has a shelf life of 24 months frommanufacturing date. Keep stored in a cool and dry place.
Packaging: Plumpy’nut is presented in sachets of 92 g. Each carton (around15.1 kg) contains 150 sachets. One sachet = 92 g = 500 Kcal.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 44/54
RUTF in the Field
Child being fed locallyproduced RUTF in Malawi
Zambian child eatingimported Plumpy’nut

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 45/54
Transitioning toRehabilitation Phase
•When a child’s appetite has returned, replaceF-75 with an equal volume of F-100 for 2 days.Then increase volume.
•If RUTF is available, this can be given in place ofF-100.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 46/54
Management Models
•Malnutrition is the result of a combination ofmedical and social problems. A managementmodel that addresses all aspects of malnutrition
will lead to a faster recovery and reduce thechances of relapse.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 47/54
Community-Based Therapeutic Care (CTC)
• In 2007, a joint statement was issued by the WHO, WFP, andUNICEF, promoting community-based management of severe acutemalnutrition.
• Countries are encouraged to adapt national policies to address:– training for community health workers in identifying malnourished
children–ensuring competency in IMCI at the facility level
– establishing referral arrangements for complicated cases
– making RUTF available to children with severe malnutrition
• The CTC approach to malnutrition management has been shown to
be more successful than traditional methods that focus on inpatientmanagement.
• Malnutrition cases that were previously treated as inpatient can bemanaged on an outpatient basis, and severe complicated cases can be discharged home earlier.

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 48/54

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 49/54
Suggested Update of Management of SevereAcute Malnutrition Into IMCI Protocol
Andre Briend, WHO, September 2007
http://www.fantaproject.org/downloads/pdfs/D2.S5.Briend.pdf

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 50/54
Case Question #1
A two year-old boy presents with bilateral pedaloedema and hypothermia. On exam, you are unable toarouse him.
Your next step should be to:
a) Check a stat haemoglobin and transfuse if Hb < 30g/l.
b) Check a stat glucose and replete if necessary
c) Place the child near a heater to warm his body temperature
d) Give 10% glucose IV
e) Give IV ampicillin

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 51/54
Case Question #1
A two year-old boy presents with bilateral pedaloedema and hypothermia. On exam, you are unable toarouse him.
Your next step should be to:
a) Check a stat haemoglobin and transfuse if Hb < 30g/l.
b) Check a stat glucose and replete if necessary
c) Place the child near a heater to warm his body temperature
d)Give 10% glucose IVe) Give IV ampicillin

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 52/54
Case Question #2
An 18 month-old girl whose mother recently died ofTB is admitted to the hospital for severe wasting andanorexia x 2 days. Her weight-for-height is -4 SD. Sheis alert but refuses food. Her vitals are stable.
Your next step should be to:
– Give F-75 by NG tube
– Start anti-tuberculosis medicines
– Send for chest x-ray
– Give ReSoMal by NG tube
– Test for HIV

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 53/54
Case Question #2
An 18 month-old girl whose mother recently died ofTB is admitted to the hospital for severe wasting andanorexia x 2 days. Her weight-for-height is -4 SD. Sheis alert but refuses food. Her vitals are stable.
Your next step should be to:
– Give F-75 by NG tube
– Start anti-tuberculosis medicines– Send for chest x-ray
– Give ReSoMal by NG tube
– Test for HIV

8/18/2019 Malnutrition 2
http://slidepdf.com/reader/full/malnutrition-2 54/54
Resources
•WHO, Management of severe malnutrition: a manual forphysicians and other senior health workers.
–Available online at:http://whqlibdoc.who.int/hq/1999/a57361.pdf
•Valid International’s CTC Manual:http://www.validinternational.org/pages/
•Project Peanut Butter – RUTF factory and feedingprogram in Malawi:http://www.projectpeanutbutter.org/