Malaria Centre Report 2012-14
138
Malaria Centre London School of Hygiene & Tropical Medicine Keppel Street, London, WC1E 7HT, UK http://malaria.lshtm.ac.uk/ [email protected] Copies of this report may be obtained at http://malaria. lshtm.ac.uk/ or by writing to the address above. Cover image: Mala (Matt Murphy/Handsome Frank) Malaria Centre Report 2012-14 The authoritative academic voice on malaria research Improving health worldwide October 2014 Malaria Centre Report 2012-14 London School of Hygiene & Tropical Medicine
-
Upload
london-school-of-hygiene-tropical-medicine -
Category
Documents
-
view
227 -
download
0
description
News, research and updates from the Malaria Centre.
Transcript of Malaria Centre Report 2012-14

Malaria CentreLondon School of Hygiene & Tropical MedicineKeppel Street, London, WC1E 7HT, UKhttp://malaria.lshtm.ac.uk/[email protected]
Copies of this report may be obtained at http://malaria.lshtm.ac.uk/ or by writing to the address above.Cover image: Mala (Matt Murphy/Handsome Frank)
Malaria Centre Report
2012-14
The authoritative academic voice on malaria research
Improving health worldwide October 2014
Malaria C
entre Report 2012-14
London School of H
ygiene & Tropical M
edicine


Contents
Director’s message 2Executive summary 3
Capacity strengthening 4
Malaria biology 10 Parasite biology 12 Immunology and host resistance 24 Vector biology 31
Malaria prevention 38 Vector control 40 Insecticide resistance 51 Chemoprevention 57 Vaccine development 65
Treatment of malaria 66 Drug studies 69 Community-based case management 73 Facility-based case management 84
Malaria moving forward 94 Surveillance, monitoring and evaluation 96 Malaria control and development 110 Future priorities 112 Publications 114 Members 132

Executive summary 3
Malaria Centre Report 2012-14
2 Director’s message
London School of Hygiene & Tropical Medicine
Despite being preventable and treatable,
malaria continues to devastate populations
across the globe. Progress has been made on
many fronts but the Plasmodium parasite remains
a formidable foe, and one that is constantly
evolving. We continue to face many challenges,
from anti-malarial drug and insecticide resistance
to the genetic evolution of mosquitoes. However,
thanks to a combined effort of governments,
researchers, industry, and philanthropic funders,
deaths from malaria have been reduced by one
third in the last decade but in order to maintain
this progress, sustained investment is needed at
all levels.
The London School of Hygiene & Tropical
Medicine has, for over a century, had a
pioneering role in improving prevention,
diagnosis, and treatment of malaria. Established
in 1998, the School’s Malaria Centre has evolved
and grown to include over 300 researchers,
the largest such group under one roof in the
world. It leads and facilitates interdisciplinary
research and crucially, supports collaboration
Peter Piot
London School of Hygiene & Tropical Medicine Director and Professor of Global Health
with external groups, particularly in malaria
endemic countries, where the shortage of trained
personnel and adequate infrastructure continues
to be a major issue for malaria control. This
role in strengthening capacity for research, but
also education and knowledge transfer, is an
increasing focus of our work.
and the Centre works in a variety of malaria
research areas ranging from basic laboratory
science to social and economic studies. The
Centre also has access to our world-class
facilities that contribute to the diagnosis,
treatment and research of malaria, including the
insectaries at Keppel Street, which house the
world’s longest-established colonies of breeding
mosquitoes, the Malaria Reference Laboratory,
Centre.
I hope you will take time to read this report.
It highlights some of the achievements of
the Centre over the past two years and it is
heartening to see the many breakthroughs that
are being made. It is vital we don’t stand still, but
continue to work on improving existing solutions
and developing new ones, so that one day we
may hope to see the end of malaria.
Continued effective malaria control and
progress toward malaria elimination require
a comprehensive range of approaches to develop
and deliver the right tools. These approaches
need to be based on thorough understanding
of parasite and vector biology and interactions
with the human host. This annual report
work conducted by the Malaria Centre at the
London School of Hygiene & Tropical Medicine in
addressing these issues.
The report is structured broadly from the
nature of the Centre’s research. Examples
of excellence are evident at both ends of the
spectrum with parasite genomics outputs
including the barcode for Plasmodium falciparum
at one end and the multifaceted outputs from
also continue to build and evaluate vital research
resources. New parasite isolates are being
collected and established with our partners at the
Hospital for Tropical Diseases which are essential
insecticides and vector control strategies are
routinely being tested with our partners based in
of the Centre continue to be at the forefront of
evaluating both novel control approaches such
as Seasonal Malaria Chemoprophylaxis and
optimal combinations of existing approaches
with multicentre trials of interventions like indoor
residual spraying and long-lasting insecticidal-
programmes investigating the molecular and
spatial epidemiology of a newly emerging threat -
the zoonotic malaria, Plasmodium knowlesi.
Having
address new and emerging challenges such
as Plasmodium knowlesi is testament to core
attributes of the Malaria Centre: world-leading
researchers, strong overseas partnerships,
motivated students, and the prescience of those
that fund them. The ability to integrate new
techniques with established skills in parasitology,
entomology and epidemiology allows the Malaria
Centre to continue, and build on, the work of the
the world’s major public health issues.
Chris Drakeley
Malaria Centre Director and Professor of Infection and Immunity

Executive summary 3
Malaria Centre Report 2012-14
2 Director’s message
London School of Hygiene & Tropical Medicine
Despite being preventable and treatable,
malaria continues to devastate populations
across the globe. Progress has been made on
many fronts but the Plasmodium parasite remains
a formidable foe, and one that is constantly
evolving. We continue to face many challenges,
from anti-malarial drug and insecticide resistance
to the genetic evolution of mosquitoes. However,
thanks to a combined effort of governments,
researchers, industry, and philanthropic funders,
deaths from malaria have been reduced by one
third in the last decade but in order to maintain
this progress, sustained investment is needed at
all levels.
The London School of Hygiene & Tropical
Medicine has, for over a century, had a
pioneering role in improving prevention,
diagnosis, and treatment of malaria. Established
in 1998, the School’s Malaria Centre has evolved
and grown to include over 300 researchers,
the largest such group under one roof in the
world. It leads and facilitates interdisciplinary
research and crucially, supports collaboration
Peter Piot
London School of Hygiene & Tropical Medicine Director and Professor of Global Health
with external groups, particularly in malaria
endemic countries, where the shortage of trained
personnel and adequate infrastructure continues
to be a major issue for malaria control. This
role in strengthening capacity for research, but
also education and knowledge transfer, is an
increasing focus of our work.
and the Centre works in a variety of malaria
research areas ranging from basic laboratory
science to social and economic studies. The
Centre also has access to our world-class
facilities that contribute to the diagnosis,
treatment and research of malaria, including the
insectaries at Keppel Street, which house the
world’s longest-established colonies of breeding
mosquitoes, the Malaria Reference Laboratory,
Centre.
I hope you will take time to read this report.
It highlights some of the achievements of
the Centre over the past two years and it is
heartening to see the many breakthroughs that
are being made. It is vital we don’t stand still, but
continue to work on improving existing solutions
and developing new ones, so that one day we
may hope to see the end of malaria.
Continued effective malaria control and
progress toward malaria elimination require
a comprehensive range of approaches to develop
and deliver the right tools. These approaches
need to be based on thorough understanding
of parasite and vector biology and interactions
with the human host. This annual report
work conducted by the Malaria Centre at the
London School of Hygiene & Tropical Medicine in
addressing these issues.
The report is structured broadly from the
nature of the Centre’s research. Examples
of excellence are evident at both ends of the
spectrum with parasite genomics outputs
including the barcode for Plasmodium falciparum
at one end and the multifaceted outputs from
also continue to build and evaluate vital research
resources. New parasite isolates are being
collected and established with our partners at the
Hospital for Tropical Diseases which are essential
insecticides and vector control strategies are
routinely being tested with our partners based in
of the Centre continue to be at the forefront of
evaluating both novel control approaches such
as Seasonal Malaria Chemoprophylaxis and
optimal combinations of existing approaches
with multicentre trials of interventions like indoor
residual spraying and long-lasting insecticidal-
programmes investigating the molecular and
spatial epidemiology of a newly emerging threat -
the zoonotic malaria, Plasmodium knowlesi.
Having
address new and emerging challenges such
as Plasmodium knowlesi is testament to core
attributes of the Malaria Centre: world-leading
researchers, strong overseas partnerships,
motivated students, and the prescience of those
that fund them. The ability to integrate new
techniques with established skills in parasitology,
entomology and epidemiology allows the Malaria
Centre to continue, and build on, the work of the
the world’s major public health issues.
Chris Drakeley
Malaria Centre Director and Professor of Infection and Immunity

4 Capacity strengthening Capacity strengthening 5
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Members of the Malaria Centre have continued to
play an important role in strengthening research
capacity in the United Kingdom and malaria
endemic countries, particularly in sub-Saharan
Formal teaching and training programmes with
School of Hygiene & Tropical Medicine. There
has been increased interest from post graduate
students and researchers from disease endemic
countries mirroring global investment in control-
increase of registrations for the Distance Learning
from this training between 2011/2 and 2013/4.
The Centre currently supports two PhD students
Thorpe Legacy Studentship Fund but members
The guiding principle of the Malaria Centre’s capacity strengthening activities is to work
within interdisciplinary partnerships that respond to local, national and international
priorities to improve malaria control.
continue to supervise and/or co-supervise many
more students in all three faculties at the School.
The total number of PhD students graduating with
degrees focusing on malaria has continued to
increase, with 22 students successfully defend-
ing their PhDs between 2011/2 and 2013/4. The
geographic spread of our students continues
graduates coming from, and working in, disease
endemic countries.
Every year, Malaria Centre members also con-
tribute to capacity strengthening amongst MSc
students, with specialist malaria teaching forming
an integral part of both London-based and dis-
tance-learning MSc courses. Lectures and labo-
ratory practicals, designed to foster a detailed un-
derstanding of the life history of malaria parasites
and mosquito vectors, form a core component of
In addition, all London-based MSc students
have the option to take a 5-week module on the
Epidemiology and Control of Malaria which aims
to give students a deeper view of malaria as a
public health problem, and generate a compre-
hensive understanding of the environmental,
biological, political and social roots of malaria,
by building connections between a wide variety
of aspects and viewpoints. Strong emphasis is
placed on providing up-to-date knowledge of the
interventions that can be used to control malaria,
as well as a critical understanding of current and
future challenges to their effective use and appli-
cation.
Students apply this knowledge to inform the
design of either a control programme, intervention
trial or elimination strategy according to the
malaria epidemiology of a given setting (selected
from a choice of representative settings in sub-
module, attracting over 40 students each year,
many of whom have gone on to play an active
role either in malaria research and/or control in
academia, non-governmental agencies, national
control programmes and international agencies.

4 Capacity strengthening Capacity strengthening 5
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Members of the Malaria Centre have continued to
play an important role in strengthening research
capacity in the United Kingdom and malaria
endemic countries, particularly in sub-Saharan
Formal teaching and training programmes with
School of Hygiene & Tropical Medicine. There
has been increased interest from post graduate
students and researchers from disease endemic
countries mirroring global investment in control-
increase of registrations for the Distance Learning
from this training between 2011/2 and 2013/4.
The Centre currently supports two PhD students
Thorpe Legacy Studentship Fund but members
The guiding principle of the Malaria Centre’s capacity strengthening activities is to work
within interdisciplinary partnerships that respond to local, national and international
priorities to improve malaria control.
continue to supervise and/or co-supervise many
more students in all three faculties at the School.
The total number of PhD students graduating with
degrees focusing on malaria has continued to
increase, with 22 students successfully defend-
ing their PhDs between 2011/2 and 2013/4. The
geographic spread of our students continues
graduates coming from, and working in, disease
endemic countries.
Every year, Malaria Centre members also con-
tribute to capacity strengthening amongst MSc
students, with specialist malaria teaching forming
an integral part of both London-based and dis-
tance-learning MSc courses. Lectures and labo-
ratory practicals, designed to foster a detailed un-
derstanding of the life history of malaria parasites
and mosquito vectors, form a core component of
In addition, all London-based MSc students
have the option to take a 5-week module on the
Epidemiology and Control of Malaria which aims
to give students a deeper view of malaria as a
public health problem, and generate a compre-
hensive understanding of the environmental,
biological, political and social roots of malaria,
by building connections between a wide variety
of aspects and viewpoints. Strong emphasis is
placed on providing up-to-date knowledge of the
interventions that can be used to control malaria,
as well as a critical understanding of current and
future challenges to their effective use and appli-
cation.
Students apply this knowledge to inform the
design of either a control programme, intervention
trial or elimination strategy according to the
malaria epidemiology of a given setting (selected
from a choice of representative settings in sub-
module, attracting over 40 students each year,
many of whom have gone on to play an active
role either in malaria research and/or control in
academia, non-governmental agencies, national
control programmes and international agencies.

6 Capacity strengthening Capacity strengthening 7
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Palafox
Less than half
of malaria cases
receive the
recommended
treatment, called
artemisinin-based
combination therapy
This is partly due to problems
of drug availability and accessibility in
often turn to the private sector to obtain
treatment where they are more likely to
receive older or less effective medicines.
Using supply- and demand-side data
from four countries, my PhD work aims
to understand why malaria patients who
turn to the private sector are less likely
as facilitators and barriers to receiving
In particular, I focus on the
changes in price. I hope that this new
knowledge will help to design more
effective market interventions and ensure
that malaria infections are optimally
treated.
I was awarded a
Malaria Capacity
Development
studentship in 2009
and successfully
defended my PhD
from the University
of Liverpool/University of Malawi in 2013.
I am currently back in Kenya working as
a visiting Research Fellow at the Centre
for Biotechnology and Bioinformatics.
Here, I am working on an MCDC funded
post-doctoral fellowship and will use this
opportunity to undertake further laboratory
training in Plasmodium falciparum
genotyping, array design and analysis.
I am also supervising an MSc student
and am involved in MCDC’s career
development group.
The Malaria Centre couldn’t be a better
place to train – the excellent assembly
of world experts in malaria can only help
you get better and the interactions with
these researchers are so intense and
elaborate. I particularly want to extend my
gratitude to Dr Taane Clark who was very
supportive during my PhD. I hope our
collaboration will last for years to come.
The Malaria Capacity Development Consortium
to conduct high quality research on malaria.
highlight different aspects of the work being
activities of the MCDC programme for the 6th
Multilateral Initiative on Malaria meeting held
013 where
it was shown to over 1,000 guests at the gala
dinner. It will also be shown to members of the UK
parliament in late 2014.
Examples of work undertaken by the consortium
during the past two years include:
A PhD programme
Five of the 18 MCDC supported PhD students
had obtained their PhDs by the end of 2013, with
the remaining 13 due to graduate by the end
which provides opportunities to further enhance
their skills in this important early stage of their
career. Three such awards had been made by the
end of 2013.

6 Capacity strengthening Capacity strengthening 7
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Palafox
Less than half
of malaria cases
receive the
recommended
treatment, called
artemisinin-based
combination therapy
This is partly due to problems
of drug availability and accessibility in
often turn to the private sector to obtain
treatment where they are more likely to
receive older or less effective medicines.
Using supply- and demand-side data
from four countries, my PhD work aims
to understand why malaria patients who
turn to the private sector are less likely
as facilitators and barriers to receiving
In particular, I focus on the
changes in price. I hope that this new
knowledge will help to design more
effective market interventions and ensure
that malaria infections are optimally
treated.
I was awarded a
Malaria Capacity
Development
studentship in 2009
and successfully
defended my PhD
from the University
of Liverpool/University of Malawi in 2013.
I am currently back in Kenya working as
a visiting Research Fellow at the Centre
for Biotechnology and Bioinformatics.
Here, I am working on an MCDC funded
post-doctoral fellowship and will use this
opportunity to undertake further laboratory
training in Plasmodium falciparum
genotyping, array design and analysis.
I am also supervising an MSc student
and am involved in MCDC’s career
development group.
The Malaria Centre couldn’t be a better
place to train – the excellent assembly
of world experts in malaria can only help
you get better and the interactions with
these researchers are so intense and
elaborate. I particularly want to extend my
gratitude to Dr Taane Clark who was very
supportive during my PhD. I hope our
collaboration will last for years to come.
The Malaria Capacity Development Consortium
to conduct high quality research on malaria.
highlight different aspects of the work being
activities of the MCDC programme for the 6th
Multilateral Initiative on Malaria meeting held
013 where
it was shown to over 1,000 guests at the gala
dinner. It will also be shown to members of the UK
parliament in late 2014.
Examples of work undertaken by the consortium
during the past two years include:
A PhD programme
Five of the 18 MCDC supported PhD students
had obtained their PhDs by the end of 2013, with
the remaining 13 due to graduate by the end
which provides opportunities to further enhance
their skills in this important early stage of their
career. Three such awards had been made by the
end of 2013.

8 Capacity strengthening Capacity strengthening 9
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Establishment of a new molecular laboratory for malaria research in Moshi, Tanzania.
A post-doctoral programme
MCDC continues to support a cohort of 29 well
its ‘Investigator’ programme. Career development
support is provided through innovative mentoring,
Personal Development Planning and small grants
programmes.
A leadership programme
In late 2014, MCDC will launch a leadership
training programme which aims to strengthen the
skills of MCDC scientists to lead and manage
internationally competitive research groups.
The programme will use a series of facilitated
interactions (individual support, peer group
strengthen the leadership skills of investigators
over a 10-month period.
Institutional capacity strengthening
Following on from successes in strengthening
partner PhD programmes in Phase 1 of the
programme, MCDC is now using a similar
partner universities to attract and manage
research funding.
Management Support Systems will be completed
in 2104 and MCDC will provide support to
MCDC has now established working groups at
each partner institution (Career Development
development activities, such as mentoring and
PDP, within institutional structures, thereby
ensuring that career development support is
sustained beyond the lifespan of MCDC.
mcdconsortium.org
LSHTM Investigators: Mark Rowland, Natacha Protopopoff &
Alex Wright.
External Investigators/Collaborators: Franklin Mosha &
Reginald Kavishe (Kilimanjaro Christian Medical Centre,
Tanzania).
Funding: The United States Agency for International Develop-
ment.
The malaria research laboratory in Moshi, Tanzania was established to test human blood and mosquito samples for malaria parasites. The main aim of the
for malaria control trials and to increase capacity
these specialised techniques.The laboratory was originally established to
test samples for a large-scale malaria control study on Lake Victoria from 2011-2013. The techniques were established to run samples with PCR and
detecting mosquito resistance to insecticide. Testing to determine whether mosquitoes contained malaria parasite was also conducted, along with
activities include malaria parasite slide reading, mosquito dissections and trialing new PCR laboratory techniques to detect and speciate the Plasmodium parasite in the blood samples.
The laboratory is now strengthening through collaborations with other institutions from around the world. For the past 9 months, the lab has expanded availability to test samples for projects run by the following organisations: The London School of Hygiene & Tropical Medicine, The Malaria Capacity Development Consortium, THRiVE, Duke University-Medical Education Partnership Initiative, The Liverpool School of Tropical Medicine, The National Institute for Medical Research (Mwanza/Muheza/
Vector Control Consortium. The laboratory hopes to expand opportunities
for collaboration in the upcoming years, and is using
laboratory scientists.

8 Capacity strengthening Capacity strengthening 9
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Establishment of a new molecular laboratory for malaria research in Moshi, Tanzania.
A post-doctoral programme
MCDC continues to support a cohort of 29 well
its ‘Investigator’ programme. Career development
support is provided through innovative mentoring,
Personal Development Planning and small grants
programmes.
A leadership programme
In late 2014, MCDC will launch a leadership
training programme which aims to strengthen the
skills of MCDC scientists to lead and manage
internationally competitive research groups.
The programme will use a series of facilitated
interactions (individual support, peer group
strengthen the leadership skills of investigators
over a 10-month period.
Institutional capacity strengthening
Following on from successes in strengthening
partner PhD programmes in Phase 1 of the
programme, MCDC is now using a similar
partner universities to attract and manage
research funding.
Management Support Systems will be completed
in 2104 and MCDC will provide support to
MCDC has now established working groups at
each partner institution (Career Development
development activities, such as mentoring and
PDP, within institutional structures, thereby
ensuring that career development support is
sustained beyond the lifespan of MCDC.
mcdconsortium.org
LSHTM Investigators: Mark Rowland, Natacha Protopopoff &
Alex Wright.
External Investigators/Collaborators: Franklin Mosha &
Reginald Kavishe (Kilimanjaro Christian Medical Centre,
Tanzania).
Funding: The United States Agency for International Develop-
ment.
The malaria research laboratory in Moshi, Tanzania was established to test human blood and mosquito samples for malaria parasites. The main aim of the
for malaria control trials and to increase capacity
these specialised techniques.The laboratory was originally established to
test samples for a large-scale malaria control study on Lake Victoria from 2011-2013. The techniques were established to run samples with PCR and
detecting mosquito resistance to insecticide. Testing to determine whether mosquitoes contained malaria parasite was also conducted, along with
activities include malaria parasite slide reading, mosquito dissections and trialing new PCR laboratory techniques to detect and speciate the Plasmodium parasite in the blood samples.
The laboratory is now strengthening through collaborations with other institutions from around the world. For the past 9 months, the lab has expanded availability to test samples for projects run by the following organisations: The London School of Hygiene & Tropical Medicine, The Malaria Capacity Development Consortium, THRiVE, Duke University-Medical Education Partnership Initiative, The Liverpool School of Tropical Medicine, The National Institute for Medical Research (Mwanza/Muheza/
Vector Control Consortium. The laboratory hopes to expand opportunities
for collaboration in the upcoming years, and is using
laboratory scientists.

10 Malaria biology Malaria biology 11
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
whether for reducing the intensity of infections
or blocking transmission, is an underlying goal
of several projects on parasite development and
on characterization of antigens to which immune
responses may be most effective.
Immunology studies have focused on the
dynamic responses that are highly dependent
on the varying experiences of natural
infection or the precise vaccination regimens
in experimental trials. There has been an
increased focus on determining how long
protective immune responses last and how this
is determined by memory T and B lymphocyte
populations. Recognition of the importance of
immunopathology in malaria has also continued
to stimulate research on the regulation of
but a murine malaria model has been effective in
identifying targets of cytotoxic CD8+ T cells that
contribute to protection. Trials of the partially-
protective RTS,S vaccine has also provided an
important opportunity to study immune correlates
of protection, with a more controlled framework
than is possible for studies of naturally acquired
immunity.
Vector biology also incorporates a range of
innovative research, from discovery to application.
Many processes in mosquito behaviour, relating
to human-feeding or egg laying for example,
intervention.
Summary
Diverse biological disciplines are applied to understand malaria and the tools available for this have continued to develop. Malaria Centre members work across the spectrum of malaria biology in studies that range from molecular and cellular processes through to whole-organism behavioural assays and population analyses.
The studies presented in this section are ordered
in a manner that allows focus respectively on
parasites, human hosts, and mosquito vectors.
Novel prospects have arisen from the ever
expanding application of genomics, combined
with detailed analyses in clinical and community
settings as well as in experimental laboratories.
Each of these subjects, and the interactions
between them, have always been interesting and
complex, but the period covered by this report
worldwide that affect research priorities. Progress
in malaria control in particular areas is being
countered by the evolution of new mechanisms
of drug and insecticide resistance. Where
reduction of malaria incidence has been achieved
and sustained, this has led to decreasing
levels of acquired immunity and an increase in
average age at which people are infected. Novel
mechanisms and targets for future drugs and
vaccines are sought against this background.
Parasite biology here focuses on both the
sexual stage gametocytes that need to be
transmitted from humans to mosquitoes in a blood
meal, and also on the asexual parasites that
cyclically invade and replicate within red blood
cells. Common to these sexually or asexually
differentiated parasites is the need to escape
from red blood cells to continue the life cycle, with
biochemical processes of egress being studied
as potential steps that could be targeted by new

10 Malaria biology Malaria biology 11
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
whether for reducing the intensity of infections
or blocking transmission, is an underlying goal
of several projects on parasite development and
on characterization of antigens to which immune
responses may be most effective.
Immunology studies have focused on the
dynamic responses that are highly dependent
on the varying experiences of natural
infection or the precise vaccination regimens
in experimental trials. There has been an
increased focus on determining how long
protective immune responses last and how this
is determined by memory T and B lymphocyte
populations. Recognition of the importance of
immunopathology in malaria has also continued
to stimulate research on the regulation of
but a murine malaria model has been effective in
identifying targets of cytotoxic CD8+ T cells that
contribute to protection. Trials of the partially-
protective RTS,S vaccine has also provided an
important opportunity to study immune correlates
of protection, with a more controlled framework
than is possible for studies of naturally acquired
immunity.
Vector biology also incorporates a range of
innovative research, from discovery to application.
Many processes in mosquito behaviour, relating
to human-feeding or egg laying for example,
intervention.
Summary
Diverse biological disciplines are applied to understand malaria and the tools available for this have continued to develop. Malaria Centre members work across the spectrum of malaria biology in studies that range from molecular and cellular processes through to whole-organism behavioural assays and population analyses.
The studies presented in this section are ordered
in a manner that allows focus respectively on
parasites, human hosts, and mosquito vectors.
Novel prospects have arisen from the ever
expanding application of genomics, combined
with detailed analyses in clinical and community
settings as well as in experimental laboratories.
Each of these subjects, and the interactions
between them, have always been interesting and
complex, but the period covered by this report
worldwide that affect research priorities. Progress
in malaria control in particular areas is being
countered by the evolution of new mechanisms
of drug and insecticide resistance. Where
reduction of malaria incidence has been achieved
and sustained, this has led to decreasing
levels of acquired immunity and an increase in
average age at which people are infected. Novel
mechanisms and targets for future drugs and
vaccines are sought against this background.
Parasite biology here focuses on both the
sexual stage gametocytes that need to be
transmitted from humans to mosquitoes in a blood
meal, and also on the asexual parasites that
cyclically invade and replicate within red blood
cells. Common to these sexually or asexually
differentiated parasites is the need to escape
from red blood cells to continue the life cycle, with
biochemical processes of egress being studied
as potential steps that could be targeted by new

12 Malaria biology Malaria biology 13
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The role of the subpellicular network in malaria parasite development and infectivity.
LSHTM Investigators: Annie Tremp, Sadia Saeed & Johannes
Dessens.
Funding: The Wellcome Trust.
parasites is a cortical cytoskeletal structure termed
maintain cell shape. Plasmodium alveolins comprise
Species barriers in ovale malaria parasites.
LSHTM Investigators: Mary Oguike & Colin Sutherland.
External Investigators/Collaborators: Abdoulaye Djimde (Malaria
Research and Training Center, Mali); Alyssa Barry (Walter and Eliza
Hall Institute of Medical Research, Australia).
Funding: The Wellcome Trust.
In this Wellcome Trust funded project, we studied various aspects of parasite biology that may contribute to mainte-nance of the species barrier.
the UK for which we had a blood sample for analysis, the 74 Plasmodium ovale curtisi-infected malaria patients presented on average 85.7 days after arrival in the UK. By contrast, the 60 Plasmodium ovale wallikeri, cases
Both species showed an ability to occur in patients who took chemoprophylaxis, due to the ability to relapse from
biological difference found between these two related parasite species.
We then proceeded with genetic analysis of sexual-stage and fertilisation-related loci in both species, and
provides further evidence to support our favourite hypoth-esis: the species barrier between the two parasites is due to genetic distance that accrued while the two lineages
Parasite biology
A newly ruptured Plasmodium ovale curtisi schizont and gametocyte following in vitro maturation of parasites from patient blood.
were in different primate hosts, before modern Homo sapiens arose. When these two hypothetical proto-ovale lineages separately entered the new host Homo, crucial genetic changes had occurred which prevented cross-mating, and thus genetic isolation has continued.
The role of Plasmodium LCCL proteins in malaria transmission.
LSHTM Investigators: Sadia Saeed, Annie Tremp & Johannes
Dessens.
Funding: The Wellcome Trust.
Plasmodium LCCL proteins comprise a family of six proteins that function as a protein complex and have essential roles in sporozoite transmission. In Plasmodium berghei, family members Pb Pb Pbhave been shown to be expressed in gametocytes and, following gametogenesis and fertilization, to be targeted to distinctive multivesicular organelles termed crystalloids
Schematic diagram of the Plasmodium LAP family. The names given are the most commonly used for these proteins in P. berghei (Pb) and P. falciparum (Pf). All proteins possess a predicted
that form in the ookinete. We have shown, by GFP-tagging, that Pb
Pb Pbassociated with the crystalloids. However, in contrast to their family members, protein expression of PbPb Pbeven though transcription of the corresponding genes is most prominent in the sexual blood stage parasites. These results suggest that translational repression controls expression of the LCCL protein repertoire and, consequently, the temporal function of the protein complex during Plasmodium berghei development in the mosquito.
structural components of the SPN, and alveolin gene knockout causes morphological abnormalities that coincide with markedly reduced tensile strength of the affected zoites, indicating the alveolins are prime cellshape determinants.
We have characterized a novel SPN protein of Plas-modium berghei ookinetes and sporozoites named G2
-veolins. G2 knockout abolishes parasite transmission and causes zoite malformations and motility defects similar to
those observed in alveolin null mutants. Unlike alveolins, however, G2 contributes little to tensile strength, argu-ing against a cause-effect relationship between tensile strength and cell shape. We also show that G2 null mu-tant sporozoites display an abnormal arrangement of their subpellicular microtubules.
These results provide important new understanding of the factors that determine zoite morphogenesis, as well as the potential roles of the cortical cytoskeleton in gliding motility.
Research with a genomic perspective focuses on discovery of parasite mechanisms that can be targeted for future development of drugs and vaccines, and on parasite susceptibility to existing drugs and immune responses in endemic populations.

12 Malaria biology Malaria biology 13
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The role of the subpellicular network in malaria parasite development and infectivity.
LSHTM Investigators: Annie Tremp, Sadia Saeed & Johannes
Dessens.
Funding: The Wellcome Trust.
parasites is a cortical cytoskeletal structure termed
maintain cell shape. Plasmodium alveolins comprise
Species barriers in ovale malaria parasites.
LSHTM Investigators: Mary Oguike & Colin Sutherland.
External Investigators/Collaborators: Abdoulaye Djimde (Malaria
Research and Training Center, Mali); Alyssa Barry (Walter and Eliza
Hall Institute of Medical Research, Australia).
Funding: The Wellcome Trust.
In this Wellcome Trust funded project, we studied various aspects of parasite biology that may contribute to mainte-nance of the species barrier.
the UK for which we had a blood sample for analysis, the 74 Plasmodium ovale curtisi-infected malaria patients presented on average 85.7 days after arrival in the UK. By contrast, the 60 Plasmodium ovale wallikeri, cases
Both species showed an ability to occur in patients who took chemoprophylaxis, due to the ability to relapse from
biological difference found between these two related parasite species.
We then proceeded with genetic analysis of sexual-stage and fertilisation-related loci in both species, and
provides further evidence to support our favourite hypoth-esis: the species barrier between the two parasites is due to genetic distance that accrued while the two lineages
Parasite biology
A newly ruptured Plasmodium ovale curtisi schizont and gametocyte following in vitro maturation of parasites from patient blood.
were in different primate hosts, before modern Homo sapiens arose. When these two hypothetical proto-ovale lineages separately entered the new host Homo, crucial genetic changes had occurred which prevented cross-mating, and thus genetic isolation has continued.
The role of Plasmodium LCCL proteins in malaria transmission.
LSHTM Investigators: Sadia Saeed, Annie Tremp & Johannes
Dessens.
Funding: The Wellcome Trust.
Plasmodium LCCL proteins comprise a family of six proteins that function as a protein complex and have essential roles in sporozoite transmission. In Plasmodium berghei, family members Pb Pb Pbhave been shown to be expressed in gametocytes and, following gametogenesis and fertilization, to be targeted to distinctive multivesicular organelles termed crystalloids
Schematic diagram of the Plasmodium LAP family. The names given are the most commonly used for these proteins in P. berghei (Pb) and P. falciparum (Pf). All proteins possess a predicted
that form in the ookinete. We have shown, by GFP-tagging, that Pb
Pb Pbassociated with the crystalloids. However, in contrast to their family members, protein expression of PbPb Pbeven though transcription of the corresponding genes is most prominent in the sexual blood stage parasites. These results suggest that translational repression controls expression of the LCCL protein repertoire and, consequently, the temporal function of the protein complex during Plasmodium berghei development in the mosquito.
structural components of the SPN, and alveolin gene knockout causes morphological abnormalities that coincide with markedly reduced tensile strength of the affected zoites, indicating the alveolins are prime cellshape determinants.
We have characterized a novel SPN protein of Plas-modium berghei ookinetes and sporozoites named G2
-veolins. G2 knockout abolishes parasite transmission and causes zoite malformations and motility defects similar to
those observed in alveolin null mutants. Unlike alveolins, however, G2 contributes little to tensile strength, argu-ing against a cause-effect relationship between tensile strength and cell shape. We also show that G2 null mu-tant sporozoites display an abnormal arrangement of their subpellicular microtubules.
These results provide important new understanding of the factors that determine zoite morphogenesis, as well as the potential roles of the cortical cytoskeleton in gliding motility.
Research with a genomic perspective focuses on discovery of parasite mechanisms that can be targeted for future development of drugs and vaccines, and on parasite susceptibility to existing drugs and immune responses in endemic populations.

14 Malaria biology Malaria biology 15
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A scalable assessment of malaria transmission in the standard membrane feeding assay using transgenic GFP-luciferase Plasmodium falciparum gametocytes.
LSHTM Investigators: Teun Bousema.
External Investigators/Collaborators: Will Stone, Wouter
Dechering & Robert Sauerwein (Radboud University Medical Center,
Netherlands); Thomas Churcher (Imperial College, UK); Ashley
Research Institute, USA).
Funding:
Foundation.
The development of drugs and vaccines to reduce malaria transmission is an important part of eradication
these agents is currently determined in the standard
microscopical read-outs and with limitations in up-scaling
and throughput. To improve scalability and objectivity, we utilised
a Plasmodium falciparum
dissections in favour of a simple approach where whole mosquitoes are homogenised and examined directly for luciferase activity.
Anopheles stephensi mosquitoes across 68 experimental feeds, showed that the luminescence assay was as sensitive as microscopy for infection detection. The mean luminescence intensity of
mean oocyst intensity and generated comparable
The advantage of the luminescence based assay is a considerable increase in throughput so that 10-30 experimental feeds can be evaluated in a single 96-well plate. This new method of assessing Plasmodium infection and transmission intensity could expedite the screening of novel drug compounds, vaccine candidates
Microscopical and lumines-cence based assessments of the Transmission reducing activity (TRA) of transmission effective mAb
A shows TRA calculated sepa-rately using mean oocyst intensity by microscopy and mean luminescence intensity from individual mosquitoes
-mission reducing agent was applied. Panel B shows the same for pools of
show serial dilutions of a transmission blocking monoclonal antibody (C) and
by microscopical examination of indi-vidual mosquitoes and luminescence assessment of individual mosquitoes
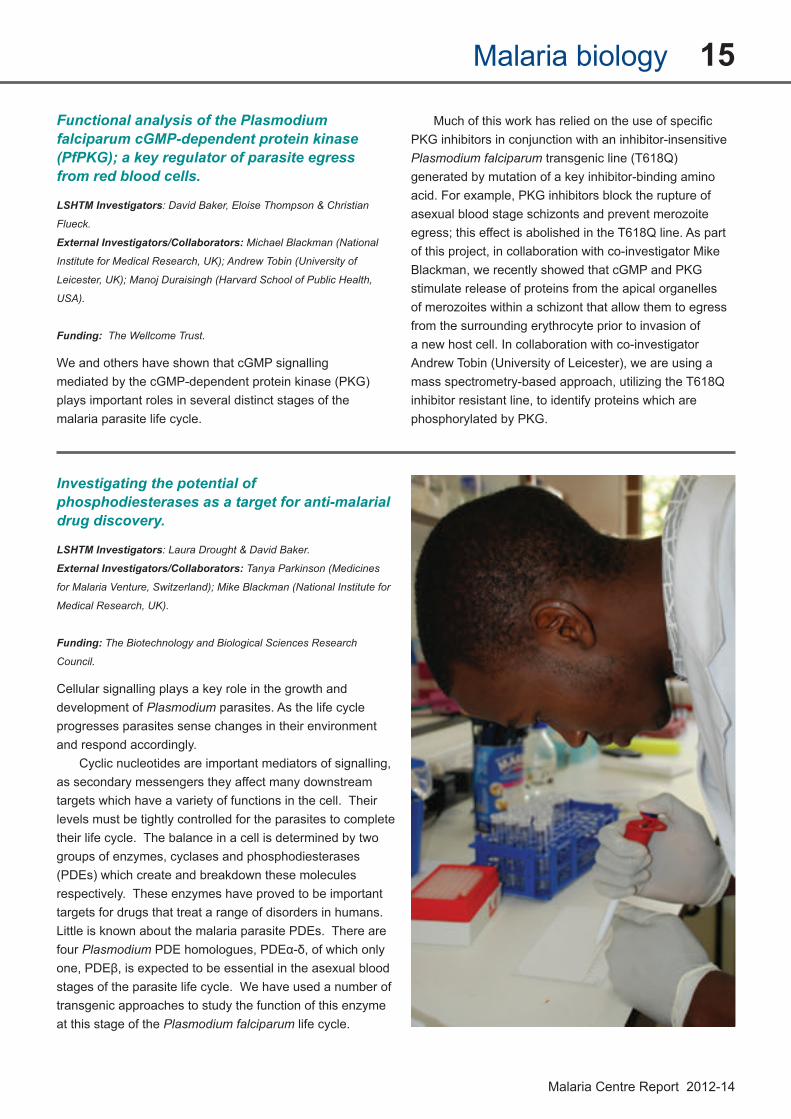
Functional analysis of the Plasmodium falciparum cGMP-dependent protein kinase (PfPKG); a key regulator of parasite egress from red blood cells.
LSHTM Investigators: David Baker, Eloise Thompson & Christian
Flueck.
External Investigators/Collaborators: Michael Blackman (National
Institute for Medical Research, UK); Andrew Tobin (University of
Leicester, UK); Manoj Duraisingh (Harvard School of Public Health,
USA).
Funding: The Wellcome Trust.
We and others have shown that cGMP signalling
plays important roles in several distinct stages of the malaria parasite life cycle.
PKG inhibitors in conjunction with an inhibitor-insensitive Plasmodium falciparum generated by mutation of a key inhibitor-binding amino acid. For example, PKG inhibitors block the rupture of asexual blood stage schizonts and prevent merozoite
of this project, in collaboration with co-investigator Mike Blackman, we recently showed that cGMP and PKG stimulate release of proteins from the apical organelles of merozoites within a schizont that allow them to egress from the surrounding erythrocyte prior to invasion of a new host cell. In collaboration with co-investigator
mass spectrometry-based approach, utilizing the T618Q inhibitor resistant line, to identify proteins which are phosphorylated by PKG.
Investigating the potential of phosphodiesterases as a target for anti-malarial drug discovery.
LSHTM Investigators: Laura Drought & David Baker.
External Investigators/Collaborators: Tanya Parkinson (Medicines
Medical Research, UK).
Funding: The Biotechnology and Biological Sciences Research
Council.
Cellular signalling plays a key role in the growth and development of Plasmodiumprogresses parasites sense changes in their environment and respond accordingly.
Cyclic nucleotides are important mediators of signalling, as secondary messengers they affect many downstream targets which have a variety of functions in the cell. Their levels must be tightly controlled for the parasites to complete their life cycle. The balance in a cell is determined by two groups of enzymes, cyclases and phosphodiesterases
respectively. These enzymes have proved to be important targets for drugs that treat a range of disorders in humans. Little is known about the malaria parasite PDEs. There are four Plasmodium
stages of the parasite life cycle. We have used a number of transgenic approaches to study the function of this enzyme at this stage of the Plasmodium falciparum life cycle.
14 Malaria biology Malaria biology 15
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A scalable assessment of malaria transmission in the standard membrane feeding assay using transgenic GFP-luciferase Plasmodium falciparum gametocytes.
LSHTM Investigators: Teun Bousema.
External Investigators/Collaborators: Will Stone, Wouter
Dechering & Robert Sauerwein (Radboud University Medical Center,
Netherlands); Thomas Churcher (Imperial College, UK); Ashley
Research Institute, USA).
Funding:
Foundation.
The development of drugs and vaccines to reduce malaria transmission is an important part of eradication
these agents is currently determined in the standard
microscopical read-outs and with limitations in up-scaling
and throughput. To improve scalability and objectivity, we utilised
a Plasmodium falciparum
dissections in favour of a simple approach where whole mosquitoes are homogenised and examined directly for luciferase activity.
Anopheles stephensi mosquitoes across 68 experimental feeds, showed that the luminescence assay was as sensitive as microscopy for infection detection. The mean luminescence intensity of
mean oocyst intensity and generated comparable
The advantage of the luminescence based assay is a considerable increase in throughput so that 10-30 experimental feeds can be evaluated in a single 96-well plate. This new method of assessing Plasmodium infection and transmission intensity could expedite the screening of novel drug compounds, vaccine candidates
Microscopical and lumines-cence based assessments of the Transmission reducing activity (TRA) of transmission effective mAb
A shows TRA calculated sepa-rately using mean oocyst intensity by microscopy and mean luminescence intensity from individual mosquitoes
-mission reducing agent was applied. Panel B shows the same for pools of
show serial dilutions of a transmission blocking monoclonal antibody (C) and
by microscopical examination of indi-vidual mosquitoes and luminescence assessment of individual mosquitoes
Functional analysis of the Plasmodium falciparum cGMP-dependent protein kinase (PfPKG); a key regulator of parasite egress from red blood cells.
LSHTM Investigators: David Baker, Eloise Thompson & Christian
Flueck.
External Investigators/Collaborators: Michael Blackman (National
Institute for Medical Research, UK); Andrew Tobin (University of
Leicester, UK); Manoj Duraisingh (Harvard School of Public Health,
USA).
Funding: The Wellcome Trust.
We and others have shown that cGMP signalling
plays important roles in several distinct stages of the malaria parasite life cycle.
PKG inhibitors in conjunction with an inhibitor-insensitive Plasmodium falciparum generated by mutation of a key inhibitor-binding amino acid. For example, PKG inhibitors block the rupture of asexual blood stage schizonts and prevent merozoite
of this project, in collaboration with co-investigator Mike Blackman, we recently showed that cGMP and PKG stimulate release of proteins from the apical organelles of merozoites within a schizont that allow them to egress from the surrounding erythrocyte prior to invasion of a new host cell. In collaboration with co-investigator
mass spectrometry-based approach, utilizing the T618Q inhibitor resistant line, to identify proteins which are phosphorylated by PKG.
Investigating the potential of phosphodiesterases as a target for anti-malarial drug discovery.
LSHTM Investigators: Laura Drought & David Baker.
External Investigators/Collaborators: Tanya Parkinson (Medicines
Medical Research, UK).
Funding: The Biotechnology and Biological Sciences Research
Council.
Cellular signalling plays a key role in the growth and development of Plasmodiumprogresses parasites sense changes in their environment and respond accordingly.
Cyclic nucleotides are important mediators of signalling, as secondary messengers they affect many downstream targets which have a variety of functions in the cell. Their levels must be tightly controlled for the parasites to complete their life cycle. The balance in a cell is determined by two groups of enzymes, cyclases and phosphodiesterases
respectively. These enzymes have proved to be important targets for drugs that treat a range of disorders in humans. Little is known about the malaria parasite PDEs. There are four Plasmodium
stages of the parasite life cycle. We have used a number of transgenic approaches to study the function of this enzyme at this stage of the Plasmodium falciparum life cycle.

16 Malaria biology Malaria biology 17
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Directional selection at the pfmdr1, pfcrt, pfubp1 and pfap2mu loci of Plasmodium falciparum in Kenyan children treated with artemisinin-based combination therapy.
LSHTM Investigators
Beshir, Don van Schalkwyk, Teun Bousema & Colin Sutherland.
External Investigators/Collaborators: Patrick Sawa (International
Centre of Insect Physiology and Ecology, Kenya).
Funding: The European Union through the MALACTRES
Consortium.
Plasmodium falciparum may be threatened by the spread of parasite genotypes with reduced responsiveness to artemisinins.
sub-microscopic persistence of Plasmodium falciparum on day 3 post-treatment was shown to be associated with microscopically detected parasitaemia at day 28 or day 42.
and were determined in the Mbita cohort before treatment, on days 2 and 3 after initiation of treatment and on the day of treatment failure.
population to carry the wildtype haplotypes of pfcrt (NFD
alleles of the novel candidate resistance genes
genetic similarities were found to artemisinin-tolerant parasites recently described in Cambodia.
multi-locus Plasmodium falciparum genotypes are
and contribute to onward transmission and subsequent patent recrudescence. Detection and monitoring of these
determine whether the genotypes we describe pose a public health threat to malaria endemic countries in sub-
In vitro sensitivity of imported malaria parasites.
LSHTM Investigators: Colin Sutherland, Donelly van Schalkwyk &
Rebekah Burrow.
External Investigators/Collaborators: Xavier Ding (Medicines
(Hospital for Tropical Diseases, UK); Christian Hasford (University
College London Hospitals, UK).
Funding:
Many of the parasites used currently to study drug resistance and parasite biology were isolated from patient samples some 20-30 years ago.
However, it is only since 2000 that the World
for Plasmodium falciparum
European travellers presenting to the UK Hospital for Tropical Diseases with malaria to use their parasites for our research. We also noted their travel history. These
to grow in vitro. Thereafter, the isolates were tested for clonality and screened for drug sensitivity against a panel of antimalarial agents supplied by the Medicines for Malaria Venture.
reporting on the clonal diversity, drug sensitivity and mutations in known drug-resistance markers for our “HL” series of isolates. In addition, we have made the adapted isolates available to the wider malaria community. We plan to continue adapting isolates as a platform for measuring differences in drug sensitivity and investigating other aspects of parasite biology related to the genotypes currently circulating in endemic areas.
Alternative molecular mechanisms for erythrocyte invasion by Plasmodium falciparum in Ghana.
LSHTM Investigators: David Conway, Lindsay Stewart, Paul
Bowyer, Craig Duffy & Samuel Assefa.
External Investigators/Collaborators:
Mensah-Brown, James Abugri, Nicholas Amoako & Michael Ofori
Funding: The Leverhulme Trust; The Royal Society.
Development of a blood stage vaccine is hampered by inadequate understanding of the mechanisms by which parasites invade erythrocytes and evade immune responses. The invasive merozoite stage of Plasmodium falciparum has an array of ligands, each interacting with different receptors on the erythrocyte surface, as studied in clinical isolates here.
The aims of this study are to determine the ex vivo erythrocyte invasion phenotypes of Ghanaian Plasmodium falciparum isolates and their dependence on alternative receptors, as well as characterise gene
Plasmodium falciparum ligands involved in alternative invasion pathways. Finally, we aim to identify if parasite gene polymorphisms are under
selection from immune responses blocking particular invasion pathways.
Results so far indicate that a large proportion of parasites in Ghana use sialic acid-independent receptors, suggesting that in highly endemic areas immune selection operates against parasites using sialic acid-bearing
demonstrated by inhibition of invasion using anti-CR1 antibodies. Gene expression assays are testing the prediction that the CR1-cognate parasite ligand Rh4 is
receptor expression knockdown will further characterise selected cultured lines. Initial analyses of almost 100 parasite genome sequences from these populations reveals genes with exceptional allele frequency distributions consistent with balancing selection as expected on targets of acquired immunity. These include
encode proteins under immune selection, as well as other genes that are likely to include relatively uncharacterised targets of immune selection.
-

16 Malaria biology Malaria biology 17
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Directional selection at the pfmdr1, pfcrt, pfubp1 and pfap2mu loci of Plasmodium falciparum in Kenyan children treated with artemisinin-based combination therapy.
LSHTM Investigators
Beshir, Don van Schalkwyk, Teun Bousema & Colin Sutherland.
External Investigators/Collaborators: Patrick Sawa (International
Centre of Insect Physiology and Ecology, Kenya).
Funding: The European Union through the MALACTRES
Consortium.
Plasmodium falciparum may be threatened by the spread of parasite genotypes with reduced responsiveness to artemisinins.
sub-microscopic persistence of Plasmodium falciparum on day 3 post-treatment was shown to be associated with microscopically detected parasitaemia at day 28 or day 42.
and were determined in the Mbita cohort before treatment, on days 2 and 3 after initiation of treatment and on the day of treatment failure.
population to carry the wildtype haplotypes of pfcrt (NFD
alleles of the novel candidate resistance genes
genetic similarities were found to artemisinin-tolerant parasites recently described in Cambodia.
multi-locus Plasmodium falciparum genotypes are
and contribute to onward transmission and subsequent patent recrudescence. Detection and monitoring of these
determine whether the genotypes we describe pose a public health threat to malaria endemic countries in sub-
In vitro sensitivity of imported malaria parasites.
LSHTM Investigators: Colin Sutherland, Donelly van Schalkwyk &
Rebekah Burrow.
External Investigators/Collaborators: Xavier Ding (Medicines
(Hospital for Tropical Diseases, UK); Christian Hasford (University
College London Hospitals, UK).
Funding:
Many of the parasites used currently to study drug resistance and parasite biology were isolated from patient samples some 20-30 years ago.
However, it is only since 2000 that the World
for Plasmodium falciparum
European travellers presenting to the UK Hospital for Tropical Diseases with malaria to use their parasites for our research. We also noted their travel history. These
to grow in vitro. Thereafter, the isolates were tested for clonality and screened for drug sensitivity against a panel of antimalarial agents supplied by the Medicines for Malaria Venture.
reporting on the clonal diversity, drug sensitivity and mutations in known drug-resistance markers for our “HL” series of isolates. In addition, we have made the adapted isolates available to the wider malaria community. We plan to continue adapting isolates as a platform for measuring differences in drug sensitivity and investigating other aspects of parasite biology related to the genotypes currently circulating in endemic areas.
Alternative molecular mechanisms for erythrocyte invasion by Plasmodium falciparum in Ghana.
LSHTM Investigators: David Conway, Lindsay Stewart, Paul
Bowyer, Craig Duffy & Samuel Assefa.
External Investigators/Collaborators:
Mensah-Brown, James Abugri, Nicholas Amoako & Michael Ofori
Funding: The Leverhulme Trust; The Royal Society.
Development of a blood stage vaccine is hampered by inadequate understanding of the mechanisms by which parasites invade erythrocytes and evade immune responses. The invasive merozoite stage of Plasmodium falciparum has an array of ligands, each interacting with different receptors on the erythrocyte surface, as studied in clinical isolates here.
The aims of this study are to determine the ex vivo erythrocyte invasion phenotypes of Ghanaian Plasmodium falciparum isolates and their dependence on alternative receptors, as well as characterise gene
Plasmodium falciparum ligands involved in alternative invasion pathways. Finally, we aim to identify if parasite gene polymorphisms are under
selection from immune responses blocking particular invasion pathways.
Results so far indicate that a large proportion of parasites in Ghana use sialic acid-independent receptors, suggesting that in highly endemic areas immune selection operates against parasites using sialic acid-bearing
demonstrated by inhibition of invasion using anti-CR1 antibodies. Gene expression assays are testing the prediction that the CR1-cognate parasite ligand Rh4 is
receptor expression knockdown will further characterise selected cultured lines. Initial analyses of almost 100 parasite genome sequences from these populations reveals genes with exceptional allele frequency distributions consistent with balancing selection as expected on targets of acquired immunity. These include
encode proteins under immune selection, as well as other genes that are likely to include relatively uncharacterised targets of immune selection.
-

18 Malaria biology Malaria biology 19
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Evaluating evidence of positive directional selection in a genome-wide scan of a malaria parasite population with long term retrospective data on drug resistance emergence.
LSHTM Investigators: Craig Duffy, Chris Drakeley, Colin
Conway.
External Investigators/Collaborators: Davis Nwakanma, Alfred
Amambua-Ngwa, Eniyou Oriero, Margaret Pinder & Kalifa Bojang
Bronwyn MacInnis (Wellcome Trust Sanger Institute, UK).
Funding: The Medical Research Council; The European Research
Council.
organisms has potential to identify genes under recent selection, but data on historical allele frequency changes
in four Plasmodium falciparum drug resistance genes
in 668 archived parasite-positive blood samples of a Gambian population, from eight different years between 1984 and 2008. This covered a period before antimalarial resistance was detected locally, through subsequent failure of multiple drugs until introduction of artemisinin-based combination therapy. We then performed genome-wide sequence analysis of 52 clinical isolates from 2008, to prospect for loci under recent directional selection.
Resistance alleles increased from very low frequencies, peaking in 2000 for chloroquine resistance-associated crt and genes and at the end of the survey period for dhfr and dhps genes respectively associated with pyrimethamine and sulphadoxine
drug resistance loci were in the top four regions under strong selection implicated by the genome-wide analysis.
Genome-wide polymorphism analysis of this endemic
documentation of recent selection, demonstrating power to prospectively detect emerging alleles using such a scan.
allele was of lower frequency).
PlasmoView: the visualisation of Plasmodium falciparum genomic variation.LSHTM Investigators: Mark Preston, Samuel Assefa, Teun Bousema, David Conway, Chris Drakeley, Cally Roper, Colin Sutherland
& Taane Clark.
External Investigators/Collaborators: Harold Ocholla (University of Malawi, Malawi); Steffen Borrmann (Kenya Medical Research
& Ogobara Doumbo (Malaria Research and Training Centre, Mali); Francois Nosten (Mahidol University, Thailand); Rick Fairhurst
(National Institute of Allergy & Infectious Diseases, USA).
Funding: The Medical Research Council.
This project is designed to identify, summarise and visualise all genomic variation in malaria parasite genomes from raw sequences in publicly available archives.
The PlasmoView tool displays over 600k polymorphisms across more than 600 samples sourced from 4 continents. The patterns of variation across genomic regions are displayed, including insights into their frequency and geographical informativeness (e.g. levels of
evolutionary processes, including the spread of drug resistance. The website can be accessed from http://pathogenseq.lshtm.ac.uk/plasmoview.
Mutations in the Plasmodium falciparum chloroquine resistance transporter gene.

18 Malaria biology Malaria biology 19
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Evaluating evidence of positive directional selection in a genome-wide scan of a malaria parasite population with long term retrospective data on drug resistance emergence.
LSHTM Investigators: Craig Duffy, Chris Drakeley, Colin
Conway.
External Investigators/Collaborators: Davis Nwakanma, Alfred
Amambua-Ngwa, Eniyou Oriero, Margaret Pinder & Kalifa Bojang
Bronwyn MacInnis (Wellcome Trust Sanger Institute, UK).
Funding: The Medical Research Council; The European Research
Council.
organisms has potential to identify genes under recent selection, but data on historical allele frequency changes
in four Plasmodium falciparum drug resistance genes
in 668 archived parasite-positive blood samples of a Gambian population, from eight different years between 1984 and 2008. This covered a period before antimalarial resistance was detected locally, through subsequent failure of multiple drugs until introduction of artemisinin-based combination therapy. We then performed genome-wide sequence analysis of 52 clinical isolates from 2008, to prospect for loci under recent directional selection.
Resistance alleles increased from very low frequencies, peaking in 2000 for chloroquine resistance-associated crt and genes and at the end of the survey period for dhfr and dhps genes respectively associated with pyrimethamine and sulphadoxine
drug resistance loci were in the top four regions under strong selection implicated by the genome-wide analysis.
Genome-wide polymorphism analysis of this endemic
documentation of recent selection, demonstrating power to prospectively detect emerging alleles using such a scan.
allele was of lower frequency).
PlasmoView: the visualisation of Plasmodium falciparum genomic variation.LSHTM Investigators: Mark Preston, Samuel Assefa, Teun Bousema, David Conway, Chris Drakeley, Cally Roper, Colin Sutherland
& Taane Clark.
External Investigators/Collaborators: Harold Ocholla (University of Malawi, Malawi); Steffen Borrmann (Kenya Medical Research
& Ogobara Doumbo (Malaria Research and Training Centre, Mali); Francois Nosten (Mahidol University, Thailand); Rick Fairhurst
(National Institute of Allergy & Infectious Diseases, USA).
Funding: The Medical Research Council.
This project is designed to identify, summarise and visualise all genomic variation in malaria parasite genomes from raw sequences in publicly available archives.
The PlasmoView tool displays over 600k polymorphisms across more than 600 samples sourced from 4 continents. The patterns of variation across genomic regions are displayed, including insights into their frequency and geographical informativeness (e.g. levels of
evolutionary processes, including the spread of drug resistance. The website can be accessed from http://pathogenseq.lshtm.ac.uk/plasmoview.
Mutations in the Plasmodium falciparum chloroquine resistance transporter gene.

20 Malaria biology Malaria biology 21
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Genomic epidemiology and population genetic analysis of Plasmodium falciparum malaria.
LSHTM Investigators: Mark Preston, Samuel Assefa, Francesc
Coll, Harold Ocholla, Hanif Samad, Cally Roper, Nuno Sepulveda &
Taane Clark.
External Investigators/Collaborators: Steffen Borrmann (Kenya
Medical Research Institute, Kenya), Rick Fairhurst (National Institute
of Health, USA), Chris Plowe (University of Maryland, USA).
Funding: The Medical Research Council.
We are attempting to mine large public repositories of Plasmodium falciparum sequence data to perform population genetic analyses and develop methods to identify important genomic variations. This work includes:
nuclear and non-nuclear Plasmodium falciparum
geographic origin
positive and balancing selection to inform drug resistance and vaccine candidate studies
performing genome-wide association studies
structural variants, and integrating them into web-based (
and population genetic signatures by accurately imputing missing genotype data using inferred recombination maps
includes investigations into highly variable gene families (e.g. Plasmodium species (e.g. Plasmodium vivax
Genome-wide analysis of selection on the malaria parasite Plasmodium falciparum in a highly endemic population in Guinea compared with a Gambian population of lower endemicity.
LSHTM Investigators
Jones, Lee Murray, Taane Clark & David Conway.
External Investigators/Collaborators: Kovana Marcel Loua &
Eugene Laman (National Institute of Public Health, Republic of
MacInnis (Wellcome Trust Sanger Institute, UK).
Funding: The Medical Research Council; The European Research
Council.
Genome-wide analysis of Plasmodium falciparum sequence variation was undertaken on 100 clinical isolates sampled from a highly endemic region of the Republic of Guinea where transmission occurs for most of each year, and compared with data from 52 clinical isolates from a previously sampled population from The Gambia where there is relatively limited seasonal malaria transmission.
evidence of recent positive directional selection and
and host immunity have been major selective agents. Many of the signatures of recent directional selection
resistance loci due to historically different antimalarial use between the countries. In contrast, both populations showed a similar set of loci likely to be under balancing
genes expressed at the merozoite stage that invades
exceptional differentiation of allele frequencies at a small
polymorphisms covering a 15kb region within and gene that regulates the early stages
of gametocyte development, which is likely related to the extreme differences in mosquito vector abundance and seasonality which determine the transmission opportunities for the sexual stage of the parasite.
ST) between the Plasmodium falciparum
STsingle nucleotide polymorphisms (SNPs) across the genome, with each chromosome identi-
ST
Population genetic structure of Plasmodium knowlesi.
LSHTM Investigators: Paul Divis, David Conway, Samuel Assefa &
Craig Duffy.
External Investigators/Collaborators: Balbir Singh (University of
Malaysia, Malaysia).
Funding: The European Research Council; Ministry of Education,
Malaysia.
Human knowlesi malaria cases have been recently
to be the reservoir hosts in Malaysian Borneo, but no systematic analysis has been performed to study the population structure of Plasmodium knowlesi.
In this study, we develop microsatellite genotyping assays, and apply these on Plasmodium knowlesi isolates to examine the population genetic structure throughout its geographical distribution. In the initial phase, genotyping
of Plasmodium knowlesi was performed on 238 blood samples from human clinical cases in six different areas of mainland Peninsular Malaysia and Malaysian
loci widely distributed in the genome. Most human Plasmodium knowlesi infections contained a single
between the different areas. Linkage disequilibrium was low in all areas, suggesting random assortment of alleles during cross-mating between different parasites. Pairwise genetic differentiation indicated that the Sarawak and Sabah subpopulations were relatively similar, but had marked differentiation from a population in mainland Peninsular Malaysia. Samples from other geographical areas and macaque hosts are being analysed in ongoing work, as well as whole genome sequence data from selected sites.

20 Malaria biology Malaria biology 21
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Genomic epidemiology and population genetic analysis of Plasmodium falciparum malaria.
LSHTM Investigators: Mark Preston, Samuel Assefa, Francesc
Coll, Harold Ocholla, Hanif Samad, Cally Roper, Nuno Sepulveda &
Taane Clark.
External Investigators/Collaborators: Steffen Borrmann (Kenya
Medical Research Institute, Kenya), Rick Fairhurst (National Institute
of Health, USA), Chris Plowe (University of Maryland, USA).
Funding: The Medical Research Council.
We are attempting to mine large public repositories of Plasmodium falciparum sequence data to perform population genetic analyses and develop methods to identify important genomic variations. This work includes:
nuclear and non-nuclear Plasmodium falciparum
geographic origin
positive and balancing selection to inform drug resistance and vaccine candidate studies
performing genome-wide association studies
structural variants, and integrating them into web-based (
and population genetic signatures by accurately imputing missing genotype data using inferred recombination maps
includes investigations into highly variable gene families (e.g. Plasmodium species (e.g. Plasmodium vivax
Genome-wide analysis of selection on the malaria parasite Plasmodium falciparum in a highly endemic population in Guinea compared with a Gambian population of lower endemicity.
LSHTM Investigators
Jones, Lee Murray, Taane Clark & David Conway.
External Investigators/Collaborators: Kovana Marcel Loua &
Eugene Laman (National Institute of Public Health, Republic of
MacInnis (Wellcome Trust Sanger Institute, UK).
Funding: The Medical Research Council; The European Research
Council.
Genome-wide analysis of Plasmodium falciparum sequence variation was undertaken on 100 clinical isolates sampled from a highly endemic region of the Republic of Guinea where transmission occurs for most of each year, and compared with data from 52 clinical isolates from a previously sampled population from The Gambia where there is relatively limited seasonal malaria transmission.
evidence of recent positive directional selection and
and host immunity have been major selective agents. Many of the signatures of recent directional selection
resistance loci due to historically different antimalarial use between the countries. In contrast, both populations showed a similar set of loci likely to be under balancing
genes expressed at the merozoite stage that invades
exceptional differentiation of allele frequencies at a small
polymorphisms covering a 15kb region within and gene that regulates the early stages
of gametocyte development, which is likely related to the extreme differences in mosquito vector abundance and seasonality which determine the transmission opportunities for the sexual stage of the parasite.
ST) between the Plasmodium falciparum
STsingle nucleotide polymorphisms (SNPs) across the genome, with each chromosome identi-
ST
Population genetic structure of Plasmodium knowlesi.
LSHTM Investigators: Paul Divis, David Conway, Samuel Assefa &
Craig Duffy.
External Investigators/Collaborators: Balbir Singh (University of
Malaysia, Malaysia).
Funding: The European Research Council; Ministry of Education,
Malaysia.
Human knowlesi malaria cases have been recently
to be the reservoir hosts in Malaysian Borneo, but no systematic analysis has been performed to study the population structure of Plasmodium knowlesi.
In this study, we develop microsatellite genotyping assays, and apply these on Plasmodium knowlesi isolates to examine the population genetic structure throughout its geographical distribution. In the initial phase, genotyping
of Plasmodium knowlesi was performed on 238 blood samples from human clinical cases in six different areas of mainland Peninsular Malaysia and Malaysian
loci widely distributed in the genome. Most human Plasmodium knowlesi infections contained a single
between the different areas. Linkage disequilibrium was low in all areas, suggesting random assortment of alleles during cross-mating between different parasites. Pairwise genetic differentiation indicated that the Sarawak and Sabah subpopulations were relatively similar, but had marked differentiation from a population in mainland Peninsular Malaysia. Samples from other geographical areas and macaque hosts are being analysed in ongoing work, as well as whole genome sequence data from selected sites.

22 Malaria biology Malaria biology 23
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Determinants of Plasmodium falciparum drug response in vitro.
LSHTM Investigators: Ifeyinwa Aniebo, Colin Sutherland & Taane
Clarke.
This study investigates alternative methods of assaying artemisinin resistance by in vitro exposure to
in vivo and so short drug pulses were applied to parasites in an effort to better mimic in vivo conditions.
were used to observe any differences that may exist in
project hypothesizes that differences in mean IC50 values exist between isolates using both the 6hr pulse assay and standard 48 hour assay methods in determining artemisinin drug sensitivity. These differences could be used to identify a phenotype which could form the basis to which artemisinin resistance can be explored.
values for the 6hr pulse assays were higher than that of the standard 48hr assays. This trend was seen as a shift to the right in the dose response curve. This
experiment had variations which could be explained by the polyclonal nature of the isolates used in this study.
out any differences that may be present and statistical analysis will also be done. Clones of each isolate will be separated using limiting dilution method and each clone would be studied genetically using whole genome sequencing technology. There is an urgent need to develop an in vitro assay that correlate with parasite clearance half life as this will be useful in elucidating the molecular basis of artemisinin resistance.
Development of an anti-malarial drug that targets the Plasmodium falciparum cGMP-dependent protein kinase.
LSHTM Investigators: David Baker, Paul Bowyer, Simon Croft &
Lindsay Stewart.
External Investigators/Collaborators: Katy Kettleborough &
Andrew Merritt (MRC Technology, UK).
Funding: The Medical Research Council .
We are aiming to develop a new antimalarial drug that cures malaria by killing the asexual erythrocytic parasites but also attacks additional life-cycle stages.
Plasmdoium falciparum protein kinase (cGMP-dependent protein kinase, Pf
essential in multiple life-cycle stages. PfPKG is a novel
with antimalarials that hit alternative targets. Selective inhibitors of PKG block Plasmodium blood-stage schizont, gamete and ookinete development. Recent data by others indicate an essential role for PKG in liver stages. Medicinal chemists at MRC Technology have synthesised more than 500 new inhibitors which have being tested at LSHTM for their ability to block the growth of malaria parasites at various life cycle stages. New potent, highly selective compounds have been generated in the low nM range against Plasmodium falciparum growth in vitro.
GENINVADE: parasite population genomics and functional studies towards development of a blood stage malaria vaccine.
LSHTM Investigators: David Conway, Craig Duffy, Paul Bowyer,
Lindsay Stewart & Samuel Assefa.
External Investigators/Collaborators: Alfred Amambua-Ngwa
Hospital, Senegal); Mahamadou Diakite (University of Bamako,
Mali); Dominic Kwiatkowski (Wellcome Trust Sanger Institute, UK);
Manoj Duraisingh (Harvard University, USA).
Funding: The European Research Council.
Understanding of natural selection operating on parasites in local endemic populations can enable understanding of molecular mechanisms of parasite invasion and immune evasion.
Powerful methods are now being developed for population genomic analyses and selection experiments on parasites in culture, including single-cell analysis, and this programme uses these together in an aim to identify optimal candidate components for a vaccine, taking the following approaches:
Plasmodium falciparum in sites of contrasting endemicity in West
hypotheses on mechanisms used by merozoites to invade erythrocytes and evade acquired immune responses
invasion into erythrocytes to identify the receptor-ligand interactions used by different parasite populations ex vivo. Novel receptor knockdown assays on cultured erythrocytes will be employed, and parasite adaptation experiments conducted to identify constraints on the use of alternative invasion pathways
and genome sequences. This is aimed to validate
to genetics and phenotyping of parasites in the future. Candidate molecule discoveries will be taken forwards to receptor-ligand interaction assays, antibody inhibition and immuno-epidemiological studies.
on the erythrocyte surface by neuraminidase).

22 Malaria biology Malaria biology 23
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Determinants of Plasmodium falciparum drug response in vitro.
LSHTM Investigators: Ifeyinwa Aniebo, Colin Sutherland & Taane
Clarke.
This study investigates alternative methods of assaying artemisinin resistance by in vitro exposure to
in vivo and so short drug pulses were applied to parasites in an effort to better mimic in vivo conditions.
were used to observe any differences that may exist in
project hypothesizes that differences in mean IC50 values exist between isolates using both the 6hr pulse assay and standard 48 hour assay methods in determining artemisinin drug sensitivity. These differences could be used to identify a phenotype which could form the basis to which artemisinin resistance can be explored.
values for the 6hr pulse assays were higher than that of the standard 48hr assays. This trend was seen as a shift to the right in the dose response curve. This
experiment had variations which could be explained by the polyclonal nature of the isolates used in this study.
out any differences that may be present and statistical analysis will also be done. Clones of each isolate will be separated using limiting dilution method and each clone would be studied genetically using whole genome sequencing technology. There is an urgent need to develop an in vitro assay that correlate with parasite clearance half life as this will be useful in elucidating the molecular basis of artemisinin resistance.
Development of an anti-malarial drug that targets the Plasmodium falciparum cGMP-dependent protein kinase.
LSHTM Investigators: David Baker, Paul Bowyer, Simon Croft &
Lindsay Stewart.
External Investigators/Collaborators: Katy Kettleborough &
Andrew Merritt (MRC Technology, UK).
Funding: The Medical Research Council .
We are aiming to develop a new antimalarial drug that cures malaria by killing the asexual erythrocytic parasites but also attacks additional life-cycle stages.
Plasmdoium falciparum protein kinase (cGMP-dependent protein kinase, Pf
essential in multiple life-cycle stages. PfPKG is a novel
with antimalarials that hit alternative targets. Selective inhibitors of PKG block Plasmodium blood-stage schizont, gamete and ookinete development. Recent data by others indicate an essential role for PKG in liver stages. Medicinal chemists at MRC Technology have synthesised more than 500 new inhibitors which have being tested at LSHTM for their ability to block the growth of malaria parasites at various life cycle stages. New potent, highly selective compounds have been generated in the low nM range against Plasmodium falciparum growth in vitro.
GENINVADE: parasite population genomics and functional studies towards development of a blood stage malaria vaccine.
LSHTM Investigators: David Conway, Craig Duffy, Paul Bowyer,
Lindsay Stewart & Samuel Assefa.
External Investigators/Collaborators: Alfred Amambua-Ngwa
Hospital, Senegal); Mahamadou Diakite (University of Bamako,
Mali); Dominic Kwiatkowski (Wellcome Trust Sanger Institute, UK);
Manoj Duraisingh (Harvard University, USA).
Funding: The European Research Council.
Understanding of natural selection operating on parasites in local endemic populations can enable understanding of molecular mechanisms of parasite invasion and immune evasion.
Powerful methods are now being developed for population genomic analyses and selection experiments on parasites in culture, including single-cell analysis, and this programme uses these together in an aim to identify optimal candidate components for a vaccine, taking the following approaches:
Plasmodium falciparum in sites of contrasting endemicity in West
hypotheses on mechanisms used by merozoites to invade erythrocytes and evade acquired immune responses
invasion into erythrocytes to identify the receptor-ligand interactions used by different parasite populations ex vivo. Novel receptor knockdown assays on cultured erythrocytes will be employed, and parasite adaptation experiments conducted to identify constraints on the use of alternative invasion pathways
and genome sequences. This is aimed to validate
to genetics and phenotyping of parasites in the future. Candidate molecule discoveries will be taken forwards to receptor-ligand interaction assays, antibody inhibition and immuno-epidemiological studies.
on the erythrocyte surface by neuraminidase).
24 Malaria biology Malaria biology 25
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Immunology and host resistance
Molecular mechanisms of malaria associated lung damage.
LSHTM Investigators: Brian de Souza, Eleanor Riley & Colin
Sutherland.
External Investigators/Collaborators: Alister Craig (Liverpool
School of Tropical Medicine, UK); Dan Milner (Harvard University
& Brigham Women’s Hospital, USA); Kevin Couper (University of
Manchester, UK).
It is clear that a good understanding of the underlying disease processes of malaria-induced lung damage (M-
Post-mortem examination of lung tissue from M-LD individuals shows parasites sequestering to the alveolar microvascular endothelium with vessel damage and
sequestration during infection is thus very important, but not possible to perform in humans.
We believe that studies to determine the fundamental host endothelium/parasite surface receptor interactions responsible for parasite sequestration in the lung, leading to endothelial cell dysfunction and development of M-LD,
can adequately be performed in vitro. Therefore, the primary aim of this proposal is to develop and utilise an in vitro assay system to dissect the pathogenesis of M-LD
host-parasite interactions leading up to endothelial cell damage. This in vitro study is ideal for determining the basic mechanisms of M-LD; the study will serve as a precursor for the development of an in vivo model for
objectives of the project are to:
enable parasite and leukocyte cytoadhesion to human lung endothelium in static in vitro assays then under
samples to verify the above in vitro
lung MVEC and that cytoadhesion of Plasmodium falciparum
Cytoadhesion of infected human RBC (A, B) and Pf PRBC (C, D) to non-activated (A, C) and TNF-activated hu lung
indicate PRBC in contact with endothelium.
Experimental cerebral malaria develops independently of caspase recruitment domain-containing protein 9 signaling.
LSHTM Investigators: Julius Hafalla.
External Investigators/Collaborators: Jan Burgold, Anca Dorhoi,
Stefan Kaufmann & Kai Matuschewski (Max Planck Institute for
Funding: The Royal Society; The European Federation of
Immunological Societies; The Wellcome Trust; The Max Planck
Biology Organisation.
The outcome of infection depends on multiple layers of immune regulation, with innate immunity playing a decisive role in shaping protection or pathogenic sequelae of acquired immunity.
The contribution of pattern recognition receptors and adaptor molecules in immunity to malaria remains poorly understood. Here, we interrogate the role of the caspase recruitment domain-containing protein
Plasmodium bergheiexpression was upregulated in the brains of infected
pathway in ECM pathogenesis. However, Plasmodium bergheineurological signs and presented with disrupted blood-brain barriers similar to WT mice. Furthermore, consistent with the immunological features associated with ECM
cerebral microvasculature. We conclude that ECM
Host candidate genes and malaria susceptibility in African populations.
LSHTM Investigators: Nuno Sepúlveda, Patrick Corran, Hugh
Reyburn, Eleanor Riley, Taane Clark & Chris Drakeley.
External Investigators/Collaborators: Alphaxard Manjurano
Mangano & David Modiamo (Sapienza University of Rome,
Italy); Bakary Maiga, Amagana Dolo, Mahamadou Thera &
Ogobara Doumbo (Malaria Research and Training Centre, Mali);
Consortium (University of Oxford, UK).
Funding:
Trust.
Malaria is a complex disease with many genetic and
variation in response to infection, progression and severity.
Several factors have a role, including parasite genetic make-up, host age, state of immunity and genetic background. Host genetic factors, including
risk. MalariaGEN has genotyped 150 candidate malaria polymorphisms across thousands of individuals from
sectional studies in Burkina Faso, Mali and Tanzania. Immunological titre data, including for IgE and MSP1, is also available. We have found strong protective effects
sectional study in Mali pinpointed the genetic (e.g. G6PD
the Fulani and Dogon, two sympatric populations differing
two association studies using data of asymptomatic individuals from Burkina Faso and Tanzania.
Malaria Centre members focus on identifying protective rather than immunopathological responses and on understanding the nature of immune memory in order to better design effective vaccines.

24 Malaria biology Malaria biology 25
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Immunology and host resistance
Molecular mechanisms of malaria associated lung damage.
LSHTM Investigators: Brian de Souza, Eleanor Riley & Colin
Sutherland.
External Investigators/Collaborators: Alister Craig (Liverpool
School of Tropical Medicine, UK); Dan Milner (Harvard University
& Brigham Women’s Hospital, USA); Kevin Couper (University of
Manchester, UK).
It is clear that a good understanding of the underlying disease processes of malaria-induced lung damage (M-
Post-mortem examination of lung tissue from M-LD individuals shows parasites sequestering to the alveolar microvascular endothelium with vessel damage and
sequestration during infection is thus very important, but not possible to perform in humans.
We believe that studies to determine the fundamental host endothelium/parasite surface receptor interactions responsible for parasite sequestration in the lung, leading to endothelial cell dysfunction and development of M-LD,
can adequately be performed in vitro. Therefore, the primary aim of this proposal is to develop and utilise an in vitro assay system to dissect the pathogenesis of M-LD
host-parasite interactions leading up to endothelial cell damage. This in vitro study is ideal for determining the basic mechanisms of M-LD; the study will serve as a precursor for the development of an in vivo model for
objectives of the project are to:
enable parasite and leukocyte cytoadhesion to human lung endothelium in static in vitro assays then under
samples to verify the above in vitro
lung MVEC and that cytoadhesion of Plasmodium falciparum
Cytoadhesion of infected human RBC (A, B) and Pf PRBC (C, D) to non-activated (A, C) and TNF-activated hu lung
indicate PRBC in contact with endothelium.
Experimental cerebral malaria develops independently of caspase recruitment domain-containing protein 9 signaling.
LSHTM Investigators: Julius Hafalla.
External Investigators/Collaborators: Jan Burgold, Anca Dorhoi,
Stefan Kaufmann & Kai Matuschewski (Max Planck Institute for
Funding: The Royal Society; The European Federation of
Immunological Societies; The Wellcome Trust; The Max Planck
Biology Organisation.
The outcome of infection depends on multiple layers of immune regulation, with innate immunity playing a decisive role in shaping protection or pathogenic sequelae of acquired immunity.
The contribution of pattern recognition receptors and adaptor molecules in immunity to malaria remains poorly understood. Here, we interrogate the role of the caspase recruitment domain-containing protein
Plasmodium bergheiexpression was upregulated in the brains of infected
pathway in ECM pathogenesis. However, Plasmodium bergheineurological signs and presented with disrupted blood-brain barriers similar to WT mice. Furthermore, consistent with the immunological features associated with ECM
cerebral microvasculature. We conclude that ECM
Host candidate genes and malaria susceptibility in African populations.
LSHTM Investigators: Nuno Sepúlveda, Patrick Corran, Hugh
Reyburn, Eleanor Riley, Taane Clark & Chris Drakeley.
External Investigators/Collaborators: Alphaxard Manjurano
Mangano & David Modiamo (Sapienza University of Rome,
Italy); Bakary Maiga, Amagana Dolo, Mahamadou Thera &
Ogobara Doumbo (Malaria Research and Training Centre, Mali);
Consortium (University of Oxford, UK).
Funding:
Trust.
Malaria is a complex disease with many genetic and
variation in response to infection, progression and severity.
Several factors have a role, including parasite genetic make-up, host age, state of immunity and genetic background. Host genetic factors, including
risk. MalariaGEN has genotyped 150 candidate malaria polymorphisms across thousands of individuals from
sectional studies in Burkina Faso, Mali and Tanzania. Immunological titre data, including for IgE and MSP1, is also available. We have found strong protective effects
sectional study in Mali pinpointed the genetic (e.g. G6PD
the Fulani and Dogon, two sympatric populations differing
two association studies using data of asymptomatic individuals from Burkina Faso and Tanzania.
Malaria Centre members focus on identifying protective rather than immunopathological responses and on understanding the nature of immune memory in order to better design effective vaccines.

26 Malaria biology Malaria biology 27
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Parasite sequestration in uncomplicated and severe childhood Plasmodium falciparum malaria.
LSHTM Investigators: Aubrey Cunnington, Michael Bretscher,
Sarah Nogaro & Eleanor Riley.
External Investigators/Collaborators: Michael Walther (Medical
Funding: The Medical Research Council.
Mature red blood cell stages of Plasmodium falciparum sequester in peripheral tissues by adhering to vascular endothelium and this process is implicated in the pathogenesis of severe malaria but direct evidence is lacking.
The objective of this study was to determine whether sequestration of parasitized red blood cells differs between children with uncomplicated and severe Plasmodium falciparumcirculating-, total- and sequestered- parasite biomass, using a mathematical model based on plasma concentration of Plasmodium falciparum histidine rich protein 2. Circulating- and total-, but not sequestered-,
Gambian children with severe malaria than in those with uncomplicated malaria. Sequestered biomass estimates in children with hyperlactataemia or prostration were similar to those in uncomplicated malaria, whereas sequestered biomass was higher in patients with severe anaemia, and showed a trend to higher values in cerebral malaria and fatal cases. Blood lactate concentration correlated with circulating- and total-, but not sequestered parasite biomass.
We conclude that extensive sequestration is not a uniform requirement for severe paediatric malaria. In particular, the pathophysiology of hyperlactataemia and prostration appears to be unrelated to sequestered
mechanisms may underlie different severe malaria syndromes, and different therapeutic strategies may be required to improve survival.
The distribution of parasites in different malaria syndromes. The size of the hippopotamus represents the total parasite biomass in the human body. The proportion of the hippopotamus above or below the water-line indicates the relative proportion of circulating and sequestered parasites.
responses to malaria liver stages by genome-
LSHTM Investigators: Julius Hafalla.
External Investigators/Collaborators: Karolis Bauza & Adrian Hill
(University of Oxford, UK); Johannes Friesen & Kai Matuschewski
Funding: The Royal Society; The European Federation of
Immunological Societies; The Wellcome Trust; The Max Planck
Foundation.
CD8+ T cells mediate immunity against Plasmodium liver
of CD8+ T cells has limited our current understanding of
To identify antigenic epitopes in a stringent murine malaria immunisation model, we performed a systematic
of Plasmodium berghei
PbS20318 and PbC57BL/6 mice vaccinated by whole parasite strategies known to protect against sporozoite challenge. While both PbS20318 and Pbeffector memory phenotypes in both the spleens and livers of immunised mice, only PbCD8+ T cells exhibit in vivo cytotoxicity. Moreover, Pb Pb
development. Prime/boost vaccination with Pb
sporozoite challenge. We conclude that Pb
antigen during liver-stage infection. Together, our results underscore the presence of CD8+ T cells with divergent potencies against distinct Plasmodium liver-stage
T cells will allow interrogation of the development of immune responses against malaria liver stages.
The role of IL-27 in the immunology and immunopathology of malaria.
LSHTM Investigators
Brian de Souza, Seen-Wai Lavelle, Tovah Shaw, Kevin Couper &
Eleanor Riley.
External Investigators/Collaborators:
USA); Chris Hunter (University of Pennsylvania, USA).
Funding: The Biotechnology and Biological Sciences Research
Council;The Medical Research Council .
Successful resolution of infection requires the generation
simultaneously avoiding damage to host tissues.This balance is crucial for clinical immunity to malaria,
allowing parasitised red blood cells to be cleared whilst
to severe malaria and malaria deaths. This balance is
maintained by a suite of immunoregulatory cytokines
series of studies to investigate the role of IL-27 in malaria infection, making use of a model of malaria in mice lacking the essential IL-27 receptor molecule, WSX-1.
We have shown that IL-27/WSX-1 signalling restrains the development of pathogenic, terminally differentiated Th1 cells during infection by regulating their intrinsic responsiveness to IL-12. This process is independent of any effects of IL-10 or Foxp3. Furthermore, we have shown that IL-27 receptor signalling regulates CD4+ T cell chemotactic responses during infection and inhibits CD4+ T cell migration to the liver; and regulates memory CD4+
secondary and subsequent malaria infections. Taken together these studies have revealed a novel pathway of immunoregulation during malaria infection that may be amenable to therapeutic intervention to prevent severe disease.

26 Malaria biology Malaria biology 27
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Parasite sequestration in uncomplicated and severe childhood Plasmodium falciparum malaria.
LSHTM Investigators: Aubrey Cunnington, Michael Bretscher,
Sarah Nogaro & Eleanor Riley.
External Investigators/Collaborators: Michael Walther (Medical
Funding: The Medical Research Council.
Mature red blood cell stages of Plasmodium falciparum sequester in peripheral tissues by adhering to vascular endothelium and this process is implicated in the pathogenesis of severe malaria but direct evidence is lacking.
The objective of this study was to determine whether sequestration of parasitized red blood cells differs between children with uncomplicated and severe Plasmodium falciparumcirculating-, total- and sequestered- parasite biomass, using a mathematical model based on plasma concentration of Plasmodium falciparum histidine rich protein 2. Circulating- and total-, but not sequestered-,
Gambian children with severe malaria than in those with uncomplicated malaria. Sequestered biomass estimates in children with hyperlactataemia or prostration were similar to those in uncomplicated malaria, whereas sequestered biomass was higher in patients with severe anaemia, and showed a trend to higher values in cerebral malaria and fatal cases. Blood lactate concentration correlated with circulating- and total-, but not sequestered parasite biomass.
We conclude that extensive sequestration is not a uniform requirement for severe paediatric malaria. In particular, the pathophysiology of hyperlactataemia and prostration appears to be unrelated to sequestered
mechanisms may underlie different severe malaria syndromes, and different therapeutic strategies may be required to improve survival.
The distribution of parasites in different malaria syndromes. The size of the hippopotamus represents the total parasite biomass in the human body. The proportion of the hippopotamus above or below the water-line indicates the relative proportion of circulating and sequestered parasites.
responses to malaria liver stages by genome-
LSHTM Investigators: Julius Hafalla.
External Investigators/Collaborators: Karolis Bauza & Adrian Hill
(University of Oxford, UK); Johannes Friesen & Kai Matuschewski
Funding: The Royal Society; The European Federation of
Immunological Societies; The Wellcome Trust; The Max Planck
Foundation.
CD8+ T cells mediate immunity against Plasmodium liver
of CD8+ T cells has limited our current understanding of
To identify antigenic epitopes in a stringent murine malaria immunisation model, we performed a systematic
of Plasmodium berghei
PbS20318 and PbC57BL/6 mice vaccinated by whole parasite strategies known to protect against sporozoite challenge. While both PbS20318 and Pbeffector memory phenotypes in both the spleens and livers of immunised mice, only PbCD8+ T cells exhibit in vivo cytotoxicity. Moreover, Pb Pb
development. Prime/boost vaccination with Pb
sporozoite challenge. We conclude that Pb
antigen during liver-stage infection. Together, our results underscore the presence of CD8+ T cells with divergent potencies against distinct Plasmodium liver-stage
T cells will allow interrogation of the development of immune responses against malaria liver stages.
The role of IL-27 in the immunology and immunopathology of malaria.
LSHTM Investigators
Brian de Souza, Seen-Wai Lavelle, Tovah Shaw, Kevin Couper &
Eleanor Riley.
External Investigators/Collaborators:
USA); Chris Hunter (University of Pennsylvania, USA).
Funding: The Biotechnology and Biological Sciences Research
Council;The Medical Research Council .
Successful resolution of infection requires the generation
simultaneously avoiding damage to host tissues.This balance is crucial for clinical immunity to malaria,
allowing parasitised red blood cells to be cleared whilst
to severe malaria and malaria deaths. This balance is
maintained by a suite of immunoregulatory cytokines
series of studies to investigate the role of IL-27 in malaria infection, making use of a model of malaria in mice lacking the essential IL-27 receptor molecule, WSX-1.
We have shown that IL-27/WSX-1 signalling restrains the development of pathogenic, terminally differentiated Th1 cells during infection by regulating their intrinsic responsiveness to IL-12. This process is independent of any effects of IL-10 or Foxp3. Furthermore, we have shown that IL-27 receptor signalling regulates CD4+ T cell chemotactic responses during infection and inhibits CD4+ T cell migration to the liver; and regulates memory CD4+
secondary and subsequent malaria infections. Taken together these studies have revealed a novel pathway of immunoregulation during malaria infection that may be amenable to therapeutic intervention to prevent severe disease.

28 Malaria biology Malaria biology 29
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Analysis of antibodies to newly described Plasmodium falciparum merozoite antigens supports MSPDBL2 as a predicted target of naturally acquired immunity.
LSHTM Investigators: Kevin Tetteh,
Laura Drought & David Conway.
External Investigators/Collaborators:
Kamuyu & Kevin Marsh (Kenya
Medical Research Institute, Kenya);
Marilyne Failly & Christoph Martin (PX
Therapeutics, France).
Funding: The Wellcome Trust.
Prospective studies continue to identify malaria parasite genes showing patterns of polymorphism indicative of immune selection pressure, and such proteins require investigation.
Sixteen new recombinant protein reagents were designed to characterize three such polymorphic proteins expressed in Plasmodium falciparum schizonts and merozoites: MSPDBL1 (also
and SURFIN4.2, encoded by a member of the surface-associated interspersed (surftesting the antigenicities of these reagents by murine
analyzed naturally acquired antibody responses to the antigens in two cohorts in coastal Kenya in which the parasite was endemic (Chonyi [ ] and Ngerenya [n
antibodies increased with age. We then investigated correlations with subsequent risk of clinical malaria among children <11 years of age during 6 months follow-
region of MSPDBL2 were associated with reduced risk
remaining for the 3D7 allelic type after adjustment for individuals’ ages in years and antibody reactivity to whole-schizont extract (Chonyi, risk ratio, 0.51, and 95%
association in one cohort (Ngerenya, risk ratio, 0.53,
showed no protective associations after adjustment.
to the polymorphic region of MSPDBL2 contribute to protective immunity.
Searching for correlates of protection of the RTS,S malaria vaccine.
LSHTM Investigators: Eleanor Riley.
External Investigators/Collaborators: Michael White, Jamie
Olotu (Wellcome Trust-Kenya Medical Research Institute, Kenya);
Kent Kester & Christian Ockenhouse (Walter Reed National Military
Medical Center, USA).
Funding: The Medical Research Council; The Wellcome Trust;
Initiative.
Vaccination with the pre-erythrocytic malaria vaccine RTS,S induces high levels of antibodies and CD4+ T cells
Using a biologically-motivated mathematical model
naive adults vaccinated with RTS,S and subjected to experimental Plasmodium falciparum challenge, we
characterised the relationship between antibodies, T cell responses and protection from infection. Both anti-CSP
as immunological surrogates of protection, with RTS,S induced anti-CSP antibodies estimated to prevent 32%
is estimated to result from a 96.1% (95% CI, 93.4% –
indicating that in volunteers who developed Plasmodium falciparum infection, a small number of parasites
responsible for breakthrough blood-stage infections. These data indicate that it may not be biologically
plausible to achieve sterilising protection with this vaccine
on achieving and maintaining higher concentrations of antibodies with higher avidity.
Comparison of antibody -
sporozoite. Estimated
sporozoite (blue) with
as a function of anti-CSP antibody titres obtained using the sporozoite model. A histogram of the distribution of anti-CSP antibody titres is shown in grey.

28 Malaria biology Malaria biology 29
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Analysis of antibodies to newly described Plasmodium falciparum merozoite antigens supports MSPDBL2 as a predicted target of naturally acquired immunity.
LSHTM Investigators: Kevin Tetteh,
Laura Drought & David Conway.
External Investigators/Collaborators:
Kamuyu & Kevin Marsh (Kenya
Medical Research Institute, Kenya);
Marilyne Failly & Christoph Martin (PX
Therapeutics, France).
Funding: The Wellcome Trust.
Prospective studies continue to identify malaria parasite genes showing patterns of polymorphism indicative of immune selection pressure, and such proteins require investigation.
Sixteen new recombinant protein reagents were designed to characterize three such polymorphic proteins expressed in Plasmodium falciparum schizonts and merozoites: MSPDBL1 (also
and SURFIN4.2, encoded by a member of the surface-associated interspersed (surftesting the antigenicities of these reagents by murine
analyzed naturally acquired antibody responses to the antigens in two cohorts in coastal Kenya in which the parasite was endemic (Chonyi [ ] and Ngerenya [n
antibodies increased with age. We then investigated correlations with subsequent risk of clinical malaria among children <11 years of age during 6 months follow-
region of MSPDBL2 were associated with reduced risk
remaining for the 3D7 allelic type after adjustment for individuals’ ages in years and antibody reactivity to whole-schizont extract (Chonyi, risk ratio, 0.51, and 95%
association in one cohort (Ngerenya, risk ratio, 0.53,
showed no protective associations after adjustment.
to the polymorphic region of MSPDBL2 contribute to protective immunity.
Searching for correlates of protection of the RTS,S malaria vaccine.
LSHTM Investigators: Eleanor Riley.
External Investigators/Collaborators: Michael White, Jamie
Olotu (Wellcome Trust-Kenya Medical Research Institute, Kenya);
Kent Kester & Christian Ockenhouse (Walter Reed National Military
Medical Center, USA).
Funding: The Medical Research Council; The Wellcome Trust;
Initiative.
Vaccination with the pre-erythrocytic malaria vaccine RTS,S induces high levels of antibodies and CD4+ T cells
Using a biologically-motivated mathematical model
naive adults vaccinated with RTS,S and subjected to experimental Plasmodium falciparum challenge, we
characterised the relationship between antibodies, T cell responses and protection from infection. Both anti-CSP
as immunological surrogates of protection, with RTS,S induced anti-CSP antibodies estimated to prevent 32%
is estimated to result from a 96.1% (95% CI, 93.4% –
indicating that in volunteers who developed Plasmodium falciparum infection, a small number of parasites
responsible for breakthrough blood-stage infections. These data indicate that it may not be biologically
plausible to achieve sterilising protection with this vaccine
on achieving and maintaining higher concentrations of antibodies with higher avidity.
Comparison of antibody -
sporozoite. Estimated
sporozoite (blue) with
as a function of anti-CSP antibody titres obtained using the sporozoite model. A histogram of the distribution of anti-CSP antibody titres is shown in grey.

30 Malaria biology Malaria biology 31
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
of a malaria transmission blocking vaccine (REDMAL).
LSHTM Investigators: Sophie Jones, Teun Bousema & Chris
Drakeley.
External Investigators/Collaborators: Robert Sauerwein &
Will Roeffen (Radboud University Nijmegen Medical Centre,
Netherlands); Michael Theisen (Statens Serum Institute, Denmark);
(Kilimanjaro Christian Medical Centre, Tanzania); Daniel Dodoo
Formation sur le Paludisme, Burkina Faso).
Funding:
Malaria transmission blocking vaccine targets are sexual stage antigens which are exposed to host immunity during parasite clearance from the blood.
It is therefore anticipated that individuals living in
endemic regions will already have antibodies against the vaccine candidates, which may provide boosting to the vaccine induced immunity. The aim of this work package was to explore recognition and functionality
we have demonstrated that school aged children in 3 endemic settings have antibodies against two new recombinant transmission blocking vaccine candidates, 10C (pf pfthe majority of previous research, we found evidence of an age dependant acquisition pattern, in the site of
prevalence and transmission reducing activity at the 90%
activity of serum from vaccinated rodents to block
-
Vector biology
Malaria Transmission Consortium: molecular characterisation reveals novel malaria vectors in the western Kenyan Highlands.
LSHTM Investigators: Jennifer Stevenson, Mary Cooke, Chris
Drakeley & Jon Cox.
External Investigators/Collaborators: Brandy St. Laurent, Neil
Lobo, Puji Asih, J.D Mueller & Frank Collins (University of Notre
Dame, USA); Sam Kahindi, Elizabeth Ayoma & Robin Oriango
Prevention, Kenya); Ralph Harbach (Natural History Museum, UK).
Funding:
Transmission Consortium.
The success of mosquito-based malaria control is dependent upon susceptible bionomic traits in local malaria vectors. It is therefore crucial to have accurate and reliable methods to determine mosquito species composition.
Anopheles species was collected in the western Kenyan highlands, including mosquitoes
anopheline specimens to determine species composition. Sixteen distinct sequence
to carry Plasmodium falciparum circumsporozoite
mosquitoes not previously described as vectors in the area and demonstrated the value of using molecular
This highlights the need for accurate characterization of mosquito species and their associated behaviours for effective malaria control. Further work continues to describe the foraging behaviour of these potentially novel vectors.
Research to identify innovative new anti-mosquito vector interventions involves

30 Malaria biology Malaria biology 31
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
of a malaria transmission blocking vaccine (REDMAL).
LSHTM Investigators: Sophie Jones, Teun Bousema & Chris
Drakeley.
External Investigators/Collaborators: Robert Sauerwein &
Will Roeffen (Radboud University Nijmegen Medical Centre,
Netherlands); Michael Theisen (Statens Serum Institute, Denmark);
(Kilimanjaro Christian Medical Centre, Tanzania); Daniel Dodoo
Formation sur le Paludisme, Burkina Faso).
Funding:
Malaria transmission blocking vaccine targets are sexual stage antigens which are exposed to host immunity during parasite clearance from the blood.
It is therefore anticipated that individuals living in
endemic regions will already have antibodies against the vaccine candidates, which may provide boosting to the vaccine induced immunity. The aim of this work package was to explore recognition and functionality
we have demonstrated that school aged children in 3 endemic settings have antibodies against two new recombinant transmission blocking vaccine candidates, 10C (pf pfthe majority of previous research, we found evidence of an age dependant acquisition pattern, in the site of
prevalence and transmission reducing activity at the 90%
activity of serum from vaccinated rodents to block
-
Vector biology
Malaria Transmission Consortium: molecular characterisation reveals novel malaria vectors in the western Kenyan Highlands.
LSHTM Investigators: Jennifer Stevenson, Mary Cooke, Chris
Drakeley & Jon Cox.
External Investigators/Collaborators: Brandy St. Laurent, Neil
Lobo, Puji Asih, J.D Mueller & Frank Collins (University of Notre
Dame, USA); Sam Kahindi, Elizabeth Ayoma & Robin Oriango
Prevention, Kenya); Ralph Harbach (Natural History Museum, UK).
Funding:
Transmission Consortium.
The success of mosquito-based malaria control is dependent upon susceptible bionomic traits in local malaria vectors. It is therefore crucial to have accurate and reliable methods to determine mosquito species composition.
Anopheles species was collected in the western Kenyan highlands, including mosquitoes
anopheline specimens to determine species composition. Sixteen distinct sequence
to carry Plasmodium falciparum circumsporozoite
mosquitoes not previously described as vectors in the area and demonstrated the value of using molecular
This highlights the need for accurate characterization of mosquito species and their associated behaviours for effective malaria control. Further work continues to describe the foraging behaviour of these potentially novel vectors.
Research to identify innovative new anti-mosquito vector interventions involves

32 Malaria biology Malaria biology 33
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Malaria Transmission Consortium: Estimating
highlands: integrating sleeping patterns and vector biting times.
LSHTM Investigators: Mary Cooke, Jennifer Stevenson, Chris
Drakeley & Jon Cox.
External Investigators/Collaborators: Brandy St. Laurent, Neil
Lobo, Puji Asih, J.D Mueller & Frank Collins (University of Notre
Dame, USA); Sam Kahindi, Elizabeth Ayoma & Robin Oriango
Prevention, Kenya); Ralph Harbach (Natural History Museum, UK).
Funding:
Transmission Consortium.
This study was designed to estimate the protective
both malaria vector and human activity.Indoor and outdoor light trap collections were carried
out in a village in the highlands of western Kenya, to
calculate vector man biting rates per hour. Times of house-entry and exit and net usage of residents were captured using questionnaires to give individual hourly vector exposure indoors and outdoors. The reduction in exposure was calculated for net users and the true
Catches of Anopheles funestus and Anopheles arabiensis
peaks of activity were recorded as early as 19:30 outdoors and 18:30 indoors. Net use was calculated to reduce exposure from 1.3 bites per night to 0.63.
to bites occurs early and indoors in this area, additional control measures are needed to compliment the current protection provided by bednets and reduce the selection pressure for physiological or behavioural resistance to insecticides in the vector population.
MBR of vectors outdoors per hour, overlaid on human activity by age group.
Pan-African Malaria Vector Research Consortium (PAMVERC).
LSHTM Investigators: Mark Rowland, Richard Oxborough,
Kirby & Alex Wright.
External Investigators/Collaborators: Franklin Mosha,
Jovin Kitau, Johnson Matowo (Kilimanjaro Christian
Medical University College, Tanzania); William Kisinza,
Patrick Tungu, Robert Malima (National Institute for Medical
Research, Tanzania); Martin Akogbeto (Centre de recherche
entomologique de Cotonou, Benin).
Funding:
There is still a major lack of public health insecticides and in future we will continue evaluating promising new products at all stages from laboratory to community testing, as well as investigating resistance management strategies.
several major chemical manufacturers including
have focused on Phase 1 laboratory and Phase 2 experimental hut evaluation of novel products for the control of pyrethroid resistant mosquito populations.
Recent success stories have been the recommendation by of the indoor residual spraying insecticides pirimiphos-methyl CS, deltamethrin SC-PE. Results from
insecticides controlled malaria vectors for >6 months
formulations. We expect that some of the products we have evaluated will be used for widespread
years.
of new bi-treated mosquito nets in order to control pyrethroid-resistant malaria vectors.

32 Malaria biology Malaria biology 33
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Malaria Transmission Consortium: Estimating
highlands: integrating sleeping patterns and vector biting times.
LSHTM Investigators: Mary Cooke, Jennifer Stevenson, Chris
Drakeley & Jon Cox.
External Investigators/Collaborators: Brandy St. Laurent, Neil
Lobo, Puji Asih, J.D Mueller & Frank Collins (University of Notre
Dame, USA); Sam Kahindi, Elizabeth Ayoma & Robin Oriango
Prevention, Kenya); Ralph Harbach (Natural History Museum, UK).
Funding:
Transmission Consortium.
This study was designed to estimate the protective
both malaria vector and human activity.Indoor and outdoor light trap collections were carried
out in a village in the highlands of western Kenya, to
calculate vector man biting rates per hour. Times of house-entry and exit and net usage of residents were captured using questionnaires to give individual hourly vector exposure indoors and outdoors. The reduction in exposure was calculated for net users and the true
Catches of Anopheles funestus and Anopheles arabiensis
peaks of activity were recorded as early as 19:30 outdoors and 18:30 indoors. Net use was calculated to reduce exposure from 1.3 bites per night to 0.63.
to bites occurs early and indoors in this area, additional control measures are needed to compliment the current protection provided by bednets and reduce the selection pressure for physiological or behavioural resistance to insecticides in the vector population.
MBR of vectors outdoors per hour, overlaid on human activity by age group.
Pan-African Malaria Vector Research Consortium (PAMVERC).
LSHTM Investigators: Mark Rowland, Richard Oxborough,
Kirby & Alex Wright.
External Investigators/Collaborators: Franklin Mosha,
Jovin Kitau, Johnson Matowo (Kilimanjaro Christian
Medical University College, Tanzania); William Kisinza,
Patrick Tungu, Robert Malima (National Institute for Medical
Research, Tanzania); Martin Akogbeto (Centre de recherche
entomologique de Cotonou, Benin).
Funding:
There is still a major lack of public health insecticides and in future we will continue evaluating promising new products at all stages from laboratory to community testing, as well as investigating resistance management strategies.
several major chemical manufacturers including
have focused on Phase 1 laboratory and Phase 2 experimental hut evaluation of novel products for the control of pyrethroid resistant mosquito populations.
Recent success stories have been the recommendation by of the indoor residual spraying insecticides pirimiphos-methyl CS, deltamethrin SC-PE. Results from
insecticides controlled malaria vectors for >6 months
formulations. We expect that some of the products we have evaluated will be used for widespread
years.
of new bi-treated mosquito nets in order to control pyrethroid-resistant malaria vectors.

34 Malaria biology Malaria biology 35
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Use of indoor attractive toxic sugar baits for control of pyrethroid resistant mosquitoes.
LSHTM Investigators
Patrick Tungu, Matt Kirby, Mark Rowland & Seth Irish.
External Investigators/Collaborators: National Institute for Medical
Research (Amani Research Centre), Tanzania; Kilimanjaro Christian
Medical University College, Tanzania.
Funding:
technology taking advantage of mosquito sugar feeding behaviour, by mixing insecticide with sugar solutions.
Many agricultural insecticides are designed to kill insects that consume them, and have not been
exposure of pyrethroid-susceptible and resistant Anopheles gambiae: implications for malaria transmission control.
LSHTM Investigators
Moore.
External Investigators/Collaborators: Achille Oumbouke, Augustin
Fongnikin & Martin Akogbeto (Centre de Recherche Entomologique
de Cotonou, Benin).
Funding:
Tackling malaria vectors indoor with insecticide treated
to behavior change of vectors and build up of residual outdoor malaria.
they would not be approved for malaria control until measurable entomological end points are established to show their potential to control malaria transmission in diverse epidemiological settings including areas with high pyrethroid resistance.
used by manwould confer against pyrethroid-susceptible and resistant Anopheles gambiae bearing the knock down resistance (kdr) gene. The ability of mosquitoes
to take a subsequentblood meal after surviving the SFT space containing vapours of the SRs was evaluated using a bioassay cage containing a shaved animal.
of both pyrethroid-susceptible and resistant Anopheles gambiae
>40% protection at 65m compared to only 10% with
With either product, repellence rates of pyrethroid-susceptible Anopheles gambiae were similar to that of the resistant strain and the trends at all distance range were notdistinguishable. Pyrethroid-resistant individuals recovered from SR exposure and bloodfed sooner than their susceptible counterpart. Forty hours after exposure, between 40-60% of susceptible Anopheles gambiae were unable to bloodfeed compared to nearly 100% feeding success with resistant Anopheles gambiae.
killing no greater than 25% of both pyrethroid susceptible and resistant Anopheles gambiae at all range.
control and suggest that they would do so by creating a vector-free space, even in areas with pyrethroid
was faster in Anopheles gambiae carrying the kdr mechanism suggests possible association/interaction between the target site of pyrethroids (the sodium
antennae where SRs bind to trigger repellence.
available for mosquito to use these insecticides against pyrethroid-resistant mosquitoes. Laboratory tests showed three insecticides
effective in killing mosquitoes. These insecticidal baits were then placed in experimental huts to see if wild, pyrethroid-resistant Anopheles arabiensis and Culex quinquefasciatus
mortality was found in mosquitoes entering experimental
optimize stations in a way that might be scalable, but the
similar control to long-lasting insecticidal nets in this area.
and assessment of putative semiochemicals and blends associated with the oviposition of Anopheles gambiae sensu stricto and Anopheles arabiensis.
LSHTM Investigators: Ulrike Fillinger, Mike Okal, Manuela Herrera-
External Investigators/Collaborators: Jenny Lindh, (KTH Royal
Institute of Technology, Sweden); Steve Torr (Liverpool School of
Tropical Medicine, UK); Baldwyn Torto (International Centre of Insect
Physiology and Ecology, Kenya).
Funding: National Institute of Health.
We study the oviposition behaviour of Anopheles gambiae and Anopheles arabiensis with the aims to
for controlling and monitoring Anopheles gambiae populations.
Whilst considerable research effort continues to
its host, almost nothing is known about how gravid females locate a breeding site. We investigate oviposition behaviour in Anopheles gambiae so that
we can ‘attract and kill’ or ‘push and pull’ egg-laying vectors and their offspring.
This approach is underpinned by multi-disciplinary research to identify the visual and olfactory stimuli that cause female Anopheles gambiae to oviposit at certain sites. Such knowledge will not only allow us to identify important breeding sites and selectively treat preferred sites with novel, long-lasting and environmentally friendly larvicides but also provide a rational basis for developing oviposition traps to monitor and kill adult mosquitoes. The aim is to optimise standard methods for preparing test insects from caged colonies in order to have a large production of gravid mosquitoes for mass screening of semiochemicals. Moreover, the aim is to develop new tools and methods for implementing and analyzing oviposition bioassays designed to show substrate preferences of gravid Anopheles gambiae. and characterise putative compounds as volatile attractants and repellents or non-volatile stimulants
using electroantennogram detections coupled with gas-chromatography and putative semiochemicals tested in the developed tool box.

34 Malaria biology Malaria biology 35
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Use of indoor attractive toxic sugar baits for control of pyrethroid resistant mosquitoes.
LSHTM Investigators
Patrick Tungu, Matt Kirby, Mark Rowland & Seth Irish.
External Investigators/Collaborators: National Institute for Medical
Research (Amani Research Centre), Tanzania; Kilimanjaro Christian
Medical University College, Tanzania.
Funding:
technology taking advantage of mosquito sugar feeding behaviour, by mixing insecticide with sugar solutions.
Many agricultural insecticides are designed to kill insects that consume them, and have not been
exposure of pyrethroid-susceptible and resistant Anopheles gambiae: implications for malaria transmission control.
LSHTM Investigators
Moore.
External Investigators/Collaborators: Achille Oumbouke, Augustin
Fongnikin & Martin Akogbeto (Centre de Recherche Entomologique
de Cotonou, Benin).
Funding:
Tackling malaria vectors indoor with insecticide treated
to behavior change of vectors and build up of residual outdoor malaria.
they would not be approved for malaria control until measurable entomological end points are established to show their potential to control malaria transmission in diverse epidemiological settings including areas with high pyrethroid resistance.
used by manwould confer against pyrethroid-susceptible and resistant Anopheles gambiae bearing the knock down resistance (kdr) gene. The ability of mosquitoes
to take a subsequentblood meal after surviving the SFT space containing vapours of the SRs was evaluated using a bioassay cage containing a shaved animal.
of both pyrethroid-susceptible and resistant Anopheles gambiae
>40% protection at 65m compared to only 10% with
With either product, repellence rates of pyrethroid-susceptible Anopheles gambiae were similar to that of the resistant strain and the trends at all distance range were notdistinguishable. Pyrethroid-resistant individuals recovered from SR exposure and bloodfed sooner than their susceptible counterpart. Forty hours after exposure, between 40-60% of susceptible Anopheles gambiae were unable to bloodfeed compared to nearly 100% feeding success with resistant Anopheles gambiae.
killing no greater than 25% of both pyrethroid susceptible and resistant Anopheles gambiae at all range.
control and suggest that they would do so by creating a vector-free space, even in areas with pyrethroid
was faster in Anopheles gambiae carrying the kdr mechanism suggests possible association/interaction between the target site of pyrethroids (the sodium
antennae where SRs bind to trigger repellence.
available for mosquito to use these insecticides against pyrethroid-resistant mosquitoes. Laboratory tests showed three insecticides
effective in killing mosquitoes. These insecticidal baits were then placed in experimental huts to see if wild, pyrethroid-resistant Anopheles arabiensis and Culex quinquefasciatus
mortality was found in mosquitoes entering experimental
optimize stations in a way that might be scalable, but the
similar control to long-lasting insecticidal nets in this area.
and assessment of putative semiochemicals and blends associated with the oviposition of Anopheles gambiae sensu stricto and Anopheles arabiensis.
LSHTM Investigators: Ulrike Fillinger, Mike Okal, Manuela Herrera-
External Investigators/Collaborators: Jenny Lindh, (KTH Royal
Institute of Technology, Sweden); Steve Torr (Liverpool School of
Tropical Medicine, UK); Baldwyn Torto (International Centre of Insect
Physiology and Ecology, Kenya).
Funding: National Institute of Health.
We study the oviposition behaviour of Anopheles gambiae and Anopheles arabiensis with the aims to
for controlling and monitoring Anopheles gambiae populations.
Whilst considerable research effort continues to
its host, almost nothing is known about how gravid females locate a breeding site. We investigate oviposition behaviour in Anopheles gambiae so that
we can ‘attract and kill’ or ‘push and pull’ egg-laying vectors and their offspring.
This approach is underpinned by multi-disciplinary research to identify the visual and olfactory stimuli that cause female Anopheles gambiae to oviposit at certain sites. Such knowledge will not only allow us to identify important breeding sites and selectively treat preferred sites with novel, long-lasting and environmentally friendly larvicides but also provide a rational basis for developing oviposition traps to monitor and kill adult mosquitoes. The aim is to optimise standard methods for preparing test insects from caged colonies in order to have a large production of gravid mosquitoes for mass screening of semiochemicals. Moreover, the aim is to develop new tools and methods for implementing and analyzing oviposition bioassays designed to show substrate preferences of gravid Anopheles gambiae. and characterise putative compounds as volatile attractants and repellents or non-volatile stimulants
using electroantennogram detections coupled with gas-chromatography and putative semiochemicals tested in the developed tool box.

36 Malaria biology Malaria biology 37
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Estimating the annual entomological inoculation rate for Plasmodium falciparum transmitted by Anopheles gambiae using three sampling methods in three sites in Uganda.
LSHTM Investigators: Robert Hutchinson, Sarah
Staedke & Chris Drakeley.
External Investigators/Collaborators: Maxwell
Surveillance Project, Uganda); David Smith (Johns
Hopkins University, USA); Moses Kamya (Makerere
University,Uganda); Martin Donnelly (Liverpool School
California, USA) & Steve Lindsay (Durham University,
UK).
The Plasmodium falciparum entomological
exposure to infectious mosquitoes. It is usually interpreted as the number of Plasmodium falciparum infective bites received by an individual during a season or annually (aPfaccuracy, precision, and seasonal distribution
PfEIR in three sites in Uganda with differing levels of transmission. We compared aPfEIR estimates derived from human landing catches – the classic method for estimating biting rates – with data from CDC light traps, and with the combined catches of knock down and exit traps.
Entomological surveillance was carried out over 1 year in 2011/12 in three settings: Nagongera, Tororo District, a rural area with exceptionally high malaria transmission; Kanungu, a rural area with moderate transmission; and Jinja, a peri-urban area with low transmission. Three sampling approaches were used from randomly selected houses in each setting with monthly collections: human-landing collections, CDC light traps and paired knock down and exit traps each
with Plasmodium falciparumThe estimated aPf
PfEIR values showed strong
between sites. Estimated HBRs using human landing catches were strongly correlated with those made using CDC
patterns in the SR were discernible because either the number of sporozoite positive mosquitoes or the total number of mosquitoes caught was too low.
We found that in these settings light traps provide an alternative method for sampling indoor-resting mosquitoes to human landing catches and have the advantage that they protect individuals from being bitten during collection, are easy to use, and are not subject to collector bias.
Olfactory mechanisms underlying behavioural manipulation of mosquitoes by malaria parasites.
LSHTM Investigators
External Investigators/Collaborators: Willem Takken & Renate
Smallegange (Wageningen Uninversity, Netherlands).
Funding: The Biotechnology and Biological Sciences Research
Council.
This project aims to determine if there are differences in the behaviour and olfactory responses of Anopheles gambiae Plasmodium falciparum malaria.
If mosquitoes with the transmissible stage of malaria are more likely to seek out a host, this would affect transmission dynamics, and also possibly involve a mechanism that we could take advantage of in vector control.
Infected and uninfected mosquitoe responses to human odour will be compared in behavioural choice tests, and compared using gas-chromatogram linked
compounds which the mosquitoes respond differentially to will be investigated as possible attractants/repellents.
vectors has been accomplished, and experiments with infected mosquitoes are currently ongoing.
Oocyst infection of Anopheles gambiae with Plasmodium faliparum malaria.
-vals (solid and dashed lines respectively).

36 Malaria biology Malaria biology 37
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Estimating the annual entomological inoculation rate for Plasmodium falciparum transmitted by Anopheles gambiae using three sampling methods in three sites in Uganda.
LSHTM Investigators: Robert Hutchinson, Sarah
Staedke & Chris Drakeley.
External Investigators/Collaborators: Maxwell
Surveillance Project, Uganda); David Smith (Johns
Hopkins University, USA); Moses Kamya (Makerere
University,Uganda); Martin Donnelly (Liverpool School
California, USA) & Steve Lindsay (Durham University,
UK).
The Plasmodium falciparum entomological
exposure to infectious mosquitoes. It is usually interpreted as the number of Plasmodium falciparum infective bites received by an individual during a season or annually (aPfaccuracy, precision, and seasonal distribution
PfEIR in three sites in Uganda with differing levels of transmission. We compared aPfEIR estimates derived from human landing catches – the classic method for estimating biting rates – with data from CDC light traps, and with the combined catches of knock down and exit traps.
Entomological surveillance was carried out over 1 year in 2011/12 in three settings: Nagongera, Tororo District, a rural area with exceptionally high malaria transmission; Kanungu, a rural area with moderate transmission; and Jinja, a peri-urban area with low transmission. Three sampling approaches were used from randomly selected houses in each setting with monthly collections: human-landing collections, CDC light traps and paired knock down and exit traps each
with Plasmodium falciparumThe estimated aPf
PfEIR values showed strong
between sites. Estimated HBRs using human landing catches were strongly correlated with those made using CDC
patterns in the SR were discernible because either the number of sporozoite positive mosquitoes or the total number of mosquitoes caught was too low.
We found that in these settings light traps provide an alternative method for sampling indoor-resting mosquitoes to human landing catches and have the advantage that they protect individuals from being bitten during collection, are easy to use, and are not subject to collector bias.
Olfactory mechanisms underlying behavioural manipulation of mosquitoes by malaria parasites.
LSHTM Investigators
External Investigators/Collaborators: Willem Takken & Renate
Smallegange (Wageningen Uninversity, Netherlands).
Funding: The Biotechnology and Biological Sciences Research
Council.
This project aims to determine if there are differences in the behaviour and olfactory responses of Anopheles gambiae Plasmodium falciparum malaria.
If mosquitoes with the transmissible stage of malaria are more likely to seek out a host, this would affect transmission dynamics, and also possibly involve a mechanism that we could take advantage of in vector control.
Infected and uninfected mosquitoe responses to human odour will be compared in behavioural choice tests, and compared using gas-chromatogram linked
compounds which the mosquitoes respond differentially to will be investigated as possible attractants/repellents.
vectors has been accomplished, and experiments with infected mosquitoes are currently ongoing.
Oocyst infection of Anopheles gambiae with Plasmodium faliparum malaria.
-vals (solid and dashed lines respectively).

38 Malaria prevention Malaria prevention 39
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Malaria prevention is attainable
by protecting against the mosquito through vector control, by protect-ing against the parasite through chemoprevention, and by vaccina-tion. Malaria Centre members are active in each of these areas.
In our research on vector control, evaluation
of the impact of full versus partial intervention
coverage has been a recurrent theme. The last
few years has seen unprecedented intervention
coverage of long-lasting insecticidal-treated nets
national governments, and this is without question
the most widely accessed current form of malaria
prevention. We are involved in identifying the
cost as well as developing guidelines for deter-
mining and evaluating LLIN durability and insecti-
cide content over time by biological and chemical
tackling the vector by combined use of LLINs and
-
munity randomised trial, we have demonstrated
-
is now switching to long-lasting indoor residual
spraying formulation, pirimiphos methyl CS. We
have been determining the effectiveness of this
strategy in Tanzania, Burkina Faso and Ivory
Coast. Insecticide treated durable wall lining is
the latest in a trend to improve the residual life
of insecticide treatments on walls of houses, and
showed great potential in a multi-country trial.
-
dence to justify scaling up include larval source
-
lents. Studies on these important areas are also
presented here. For example, fundamental re-
search has emphasised the importance of maxi-
helping to settle the long-term debate over wheth-
er DDT and volatile pyrethroids work by toxicity,
repellency or a combination of actions.
The one-time spectre on the horizon, insec-
ticide resistance, is now a real presence. While
the evidence for a negative impact on malaria
control is yet to be demonstrated unequivocally,
various studies reported by our researchers are
all pointing in that direction. While LLIN remain
the primary preventive intervention it is impossible
to reverse the selection of pyrethroid resistance.
insecticide delivery a part of everyday life. The
best way to ensure this is to maintain the pipeline
of effective insecticides for nets - products we are
working in partnership with researchers and in-
dustry to develop.
In the area of chemoprevention, a number
of strategies of are being developed for different
-
ment to clear malaria parasites in school children
in Mali demonstrated success while a Kenyan
trial of school-based Intermittent Screening and
to be an ineffective intervention in low-moderate
transmission settings. In countries of seasonal
transmission such as the Sahel, seasonal malaria
SP-amodiaquine has been successfully taken to
scale in Senegal by community health workers.
comparing whether a strategy of IST in pregnancy
is non-inferior to a strategy which involves the use
IST as a potential alternative where falciparum is
highly resistant to SP. To improve the quality of
strategies for controlling malaria in pregnancy, en-
hanced district and health facility data collection
and monitoring tools are being developed and
integrated into current systems and will contribute
to a toolkit for assessing intervention coverage
and decision making in different contexts. Imple-
mentation research on the barriers to effective ac-
cess, delivery and use of interventions have high-
lighted blockages to delivery and to weaknesses
and problems in current survey techniques for
assessing coverage.
In terms of vaccines, many of our staff have
participated in the design, execution and evalua-
tion of the trials of the RTS,S candidate vaccine in
candidate vaccine (eg the prime boost vaccine

38 Malaria prevention Malaria prevention 39
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Malaria prevention is attainable
by protecting against the mosquito through vector control, by protect-ing against the parasite through chemoprevention, and by vaccina-tion. Malaria Centre members are active in each of these areas.
In our research on vector control, evaluation
of the impact of full versus partial intervention
coverage has been a recurrent theme. The last
few years has seen unprecedented intervention
coverage of long-lasting insecticidal-treated nets
national governments, and this is without question
the most widely accessed current form of malaria
prevention. We are involved in identifying the
cost as well as developing guidelines for deter-
mining and evaluating LLIN durability and insecti-
cide content over time by biological and chemical
tackling the vector by combined use of LLINs and
-
munity randomised trial, we have demonstrated
-
is now switching to long-lasting indoor residual
spraying formulation, pirimiphos methyl CS. We
have been determining the effectiveness of this
strategy in Tanzania, Burkina Faso and Ivory
Coast. Insecticide treated durable wall lining is
the latest in a trend to improve the residual life
of insecticide treatments on walls of houses, and
showed great potential in a multi-country trial.
-
dence to justify scaling up include larval source
-
lents. Studies on these important areas are also
presented here. For example, fundamental re-
search has emphasised the importance of maxi-
helping to settle the long-term debate over wheth-
er DDT and volatile pyrethroids work by toxicity,
repellency or a combination of actions.
The one-time spectre on the horizon, insec-
ticide resistance, is now a real presence. While
the evidence for a negative impact on malaria
control is yet to be demonstrated unequivocally,
various studies reported by our researchers are
all pointing in that direction. While LLIN remain
the primary preventive intervention it is impossible
to reverse the selection of pyrethroid resistance.
insecticide delivery a part of everyday life. The
best way to ensure this is to maintain the pipeline
of effective insecticides for nets - products we are
working in partnership with researchers and in-
dustry to develop.
In the area of chemoprevention, a number
of strategies of are being developed for different
-
ment to clear malaria parasites in school children
in Mali demonstrated success while a Kenyan
trial of school-based Intermittent Screening and
to be an ineffective intervention in low-moderate
transmission settings. In countries of seasonal
transmission such as the Sahel, seasonal malaria
SP-amodiaquine has been successfully taken to
scale in Senegal by community health workers.
comparing whether a strategy of IST in pregnancy
is non-inferior to a strategy which involves the use
IST as a potential alternative where falciparum is
highly resistant to SP. To improve the quality of
strategies for controlling malaria in pregnancy, en-
hanced district and health facility data collection
and monitoring tools are being developed and
integrated into current systems and will contribute
to a toolkit for assessing intervention coverage
and decision making in different contexts. Imple-
mentation research on the barriers to effective ac-
cess, delivery and use of interventions have high-
lighted blockages to delivery and to weaknesses
and problems in current survey techniques for
assessing coverage.
In terms of vaccines, many of our staff have
participated in the design, execution and evalua-
tion of the trials of the RTS,S candidate vaccine in
candidate vaccine (eg the prime boost vaccine

40 Malaria prevention Malaria prevention 41
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Vector control
long-lasting insecticidal nets.
LSHTM Investigators: Mark Rowland.
External Investigators/Collaborators:
Health Organisation, Switzerland); K Raghavendra & R Bhatt (World
Health Organisation, India).
Funding: World Health Organisation.
in 2005. Considerable experience in testing LNs has since been gained, and on monitoring the durability of LNs under operational conditions.
pyrethroid-treated LNs, LNs containing new insecticides and/or synergists are
become available for use in the near future. The revised
procedures and guidelines for testing LNs for personal protection and malaria vector control. It is intended to harmonise testing procedures in order to generate data for registration and labelling of such products by national authorities and provide a framework for industry in developing novel LN products. Currently, an LN would be expected to retain its biological activity for at least 20 standard washes under laboratory conditions and 3 years
The document describes laboratory and small- and
Evaluation of the coverage and effective use rate of long-lasting insecticidal nets after nation-wide scale up of their distribution in Benin.
LSHTM Investigators
External Investigators/Collaborators:
Control Programme, Benin).
Funding:
Agency for International Development through the President’s
In Benin, about four million long-lasting insecticide-
to prevent malaria in 2011. In contrast to a previous campaign that targeted only children under 5 years and pregnant women, this distribution campaign was conducted in order to achieve universal coverage.
This study presents the results of LLIN coverage and utilisation after the distribution campaign.
The study was a cross-sectional household survey
design. The strata represented the twelve districts covered by the national distribution campaign in 2011 and included a total of 4,800 households randomly selected
Malaria Indicator Survey Household Questionnaire was used. Data were entered using QPS software and analyzed with R 2.14.1.
Strategies for delivering insecticide-treated nets at scale for malaria control in endemic countries: a systematic review.
LSHTM Investigators: Joanna Schellenberg, Barbara Willey,
Lindsay Mangham-Jeffries & Lucy Paintain.
External Investigators/Collaborators: Josip Car (Imperial College
London, UK) .
Funding:
sectors and retail outlets, antenatal care clinics and
campaigns. Strategies that delivered insecticide-treated nets free through campaigns achieved highest usage.
Costs were comparable across strategies, with the nets being the main cost. Cost-effectiveness estimates were most sensitive to the assumed net lifespan and leakage. Common barriers to delivery included cost, stockouts of nets at distribution points, and poor logistics. Common facilitators were staff training and supervision, cooperation across departments or ministries and stakeholder involvement.
households that met the ratio one net for two persons was 77%.The proportions of individuals sleeping under LLINs
was 10% lower than in effective users from rural areas
The universal distribution campaign conducted in Benin has increased LLIN ownership and use in the community. But additional efforts are needed to improve and maintain LLIN coverage.
Malaria Centre members are conducting vector control research mainly in East and West Africa. We are working with multilateral agencies to evaluate the reach and usage of long-lasting insecticidal treated nets (LLINs) in universal coverage campaigns, the potential impact of combining indoor residual spraying campaigns with LLINs, and the potential of and constraints to less established form of vector control such as insecticide treated durable wall lining, larval source management, and topical and spatial repellent.

40 Malaria prevention Malaria prevention 41
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Vector control
long-lasting insecticidal nets.
LSHTM Investigators: Mark Rowland.
External Investigators/Collaborators:
Health Organisation, Switzerland); K Raghavendra & R Bhatt (World
Health Organisation, India).
Funding: World Health Organisation.
in 2005. Considerable experience in testing LNs has since been gained, and on monitoring the durability of LNs under operational conditions.
pyrethroid-treated LNs, LNs containing new insecticides and/or synergists are
become available for use in the near future. The revised
procedures and guidelines for testing LNs for personal protection and malaria vector control. It is intended to harmonise testing procedures in order to generate data for registration and labelling of such products by national authorities and provide a framework for industry in developing novel LN products. Currently, an LN would be expected to retain its biological activity for at least 20 standard washes under laboratory conditions and 3 years
The document describes laboratory and small- and
Evaluation of the coverage and effective use rate of long-lasting insecticidal nets after nation-wide scale up of their distribution in Benin.
LSHTM Investigators
External Investigators/Collaborators:
Control Programme, Benin).
Funding:
Agency for International Development through the President’s
In Benin, about four million long-lasting insecticide-
to prevent malaria in 2011. In contrast to a previous campaign that targeted only children under 5 years and pregnant women, this distribution campaign was conducted in order to achieve universal coverage.
This study presents the results of LLIN coverage and utilisation after the distribution campaign.
The study was a cross-sectional household survey
design. The strata represented the twelve districts covered by the national distribution campaign in 2011 and included a total of 4,800 households randomly selected
Malaria Indicator Survey Household Questionnaire was used. Data were entered using QPS software and analyzed with R 2.14.1.
Strategies for delivering insecticide-treated nets at scale for malaria control in endemic countries: a systematic review.
LSHTM Investigators: Joanna Schellenberg, Barbara Willey,
Lindsay Mangham-Jeffries & Lucy Paintain.
External Investigators/Collaborators: Josip Car (Imperial College
London, UK) .
Funding:
sectors and retail outlets, antenatal care clinics and
campaigns. Strategies that delivered insecticide-treated nets free through campaigns achieved highest usage.
Costs were comparable across strategies, with the nets being the main cost. Cost-effectiveness estimates were most sensitive to the assumed net lifespan and leakage. Common barriers to delivery included cost, stockouts of nets at distribution points, and poor logistics. Common facilitators were staff training and supervision, cooperation across departments or ministries and stakeholder involvement.
households that met the ratio one net for two persons was 77%.The proportions of individuals sleeping under LLINs
was 10% lower than in effective users from rural areas
The universal distribution campaign conducted in Benin has increased LLIN ownership and use in the community. But additional efforts are needed to improve and maintain LLIN coverage.
Malaria Centre members are conducting vector control research mainly in East and West Africa. We are working with multilateral agencies to evaluate the reach and usage of long-lasting insecticidal treated nets (LLINs) in universal coverage campaigns, the potential impact of combining indoor residual spraying campaigns with LLINs, and the potential of and constraints to less established form of vector control such as insecticide treated durable wall lining, larval source management, and topical and spatial repellent.

42 Malaria prevention Malaria prevention 43
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The useful life of bednets for malaria control in Tanzania:
Durability and insecticide resistance (ABCDR).
LSHTM Investigators: Lena Lorenz, Jason Moore
& John Bradley.
External Investigators/Collaborators: Hans
Overgaard (Norwegian University of Life Sciences,
Norway); Sarah Moore (Ifakara Health Institute,
Tanzania & Swiss Tropical and Public Health
Institute, Switzerland); William Kisinza (National
Institute for Medical Research, Tanzania).
Funding: The Research Council of Norway –
Long-lasting insecticide-treated nets
in malaria vector control in sub-Saharan
universal coverage campaigns with free or subsidised nets. However, there is only limited knowledge from a few countries of the effective life of LLINs under user conditions, an essential parameter for determining the operational and cost-effectiveness of this strategy.
Durability and insecticide resistance
prospective design to investigate LLIN durability by measuring attrition,
degradation in Tanzania following World
methodologies. LLINs from national net campaigns between 2009 and 2011 were evaluated retrospectively and data on net use, net loss and net disposal is being analysed and shared with the national malaria control programme.
approved LLIN products and are being followed up after 12, 24, 30 and 36 months to compare the performance of the LLIN brands in vivo.
We are also developing a GIS-based network to understand potential spatial reasons for net loss and deterioration and to monitor insecticide resistance.
The data collected will be of importance to policy makers and vector control specialists both in Tanzania and the
malaria control.
Walking or waiting? Topologies of the breeding ground in malaria control.LSHTM Investigators: Ann Kelly.
External Investigators/Collaborators: Javier Lezaun
(University of Oxford, UK).
accumulation of stagnant water where disease-carrying insects lay their eggs. Since the turn of the
transmission, these aquatic habitats have been a key object of epidemiological research and public health intervention against the disease. Yet the breeding ground can be incorporated into a number of different topologies, each implying a different spatialization of malaria and a distinct imagination of what kind of
of malaria control in Dar es Salaam, Tanzania, illuminates an essential tension between what we characterise as territorial and bionomic approaches to the breeding ground—that is, between control strategies premised on treating all mosquito habitats within a given region, and those that prioritise certain sites on the basis of their position within ecological networks. Each topology localises the breeding ground by reference to a distinct set of relations, and thus advances an idiosyncratic understanding of what sort of research is worthwhile conducting and what kinds of intervention are sustainable. The multiple ways in which the breeding ground can become an
topology as an infra-logic of public health, and makes explicit the politics implicit in efforts to bring different orders of the local to scale.

42 Malaria prevention Malaria prevention 43
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The useful life of bednets for malaria control in Tanzania:
Durability and insecticide resistance (ABCDR).
LSHTM Investigators: Lena Lorenz, Jason Moore
& John Bradley.
External Investigators/Collaborators: Hans
Overgaard (Norwegian University of Life Sciences,
Norway); Sarah Moore (Ifakara Health Institute,
Tanzania & Swiss Tropical and Public Health
Institute, Switzerland); William Kisinza (National
Institute for Medical Research, Tanzania).
Funding: The Research Council of Norway –
Long-lasting insecticide-treated nets
in malaria vector control in sub-Saharan
universal coverage campaigns with free or subsidised nets. However, there is only limited knowledge from a few countries of the effective life of LLINs under user conditions, an essential parameter for determining the operational and cost-effectiveness of this strategy.
Durability and insecticide resistance
prospective design to investigate LLIN durability by measuring attrition,
degradation in Tanzania following World
methodologies. LLINs from national net campaigns between 2009 and 2011 were evaluated retrospectively and data on net use, net loss and net disposal is being analysed and shared with the national malaria control programme.
approved LLIN products and are being followed up after 12, 24, 30 and 36 months to compare the performance of the LLIN brands in vivo.
We are also developing a GIS-based network to understand potential spatial reasons for net loss and deterioration and to monitor insecticide resistance.
The data collected will be of importance to policy makers and vector control specialists both in Tanzania and the
malaria control.
Walking or waiting? Topologies of the breeding ground in malaria control.LSHTM Investigators: Ann Kelly.
External Investigators/Collaborators: Javier Lezaun
(University of Oxford, UK).
accumulation of stagnant water where disease-carrying insects lay their eggs. Since the turn of the
transmission, these aquatic habitats have been a key object of epidemiological research and public health intervention against the disease. Yet the breeding ground can be incorporated into a number of different topologies, each implying a different spatialization of malaria and a distinct imagination of what kind of
of malaria control in Dar es Salaam, Tanzania, illuminates an essential tension between what we characterise as territorial and bionomic approaches to the breeding ground—that is, between control strategies premised on treating all mosquito habitats within a given region, and those that prioritise certain sites on the basis of their position within ecological networks. Each topology localises the breeding ground by reference to a distinct set of relations, and thus advances an idiosyncratic understanding of what sort of research is worthwhile conducting and what kinds of intervention are sustainable. The multiple ways in which the breeding ground can become an
topology as an infra-logic of public health, and makes explicit the politics implicit in efforts to bring different orders of the local to scale.

44 Malaria prevention Malaria prevention 45
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A simple colorimetric test for the rapid detection of type 2-pyrethroids on bed nets.
LSHTM Investigators: Harparkash Kaur.
External Investigators/Collaborators: Tunis Eggelte (University of
Amsterdam, Amsterdam, Netherlands).
Funding: The London School of Hygiene & Tropical Medicine
Insecticide treated nets are major modes of intervention,
amount of insecticide deposit on bed nets is essential for quality control.
Currently such information can only be provided by laboratory based high tech methods such as gas chromatography and high performance liquid
bioassays where insecticide susceptible strains of mosquitoes are exposed to the bed nets. They are technically demanding to perform and require skilled staff with access to laboratory and insectary facilities.
test part of the net is placed over the tube and the cap is pushed tightly to seal the net. The test tube is turned upside down so that the solution is in contact with the net for 10 minutes. Solution D is then added to stop the reaction and the pink/red colour formed estimates the amount of deltamethrin. The test is performed in situ and does not damage the net. Field evaluations of the prototype are underway in Bioko – Equatorial Guinea.
Indoor residual spraying in combination with insecticide treated nets compared to insecticide treated nets alone for protection against malaria: a cluster randomised trial in Tanzania.
LSHTM Investigators: Philippa West, Natacha Protopopoff
Alexandra Wright, Mark Rowland & Immo Kleinschmidt.
External Investigators/Collaborators: Franklin Mosha (Kilimanjaro
Christian Medical College, Moshi, Tanzania); William Kisinza &
Tanzania); Robinson Tigererwa (Department of Health, Tanzania).
Funding: United States Agency for International Development.
This cluster randomised trial showed that deploying
compared to using ITNs alone. The size of the added protection may depend on ITN use and on local vector ecology.
Fifty clusters were randomly allocated to ITNs only or ITNs and IRS. Dwellings in the ITN+IRS arm were sprayed with two rounds of bendiocarb in 2012. Plasmodium falciparum infection prevalence (Pf
Combined use of indoor residual spraying and long-lasting insecticidal nets for malaria reduction in endemic rural Tanzania.
LSHTM Investigators: Natacha Protopopoff, Philippa West,
Alexandra Wright, Immo Kleinschmidt & Mark Rowland.
External Investigators/Collaborators: Frank Mosha & Reginald
Kavishe (Kilimanjaro Christian Medical Colleges, Tanzania); Robert
Malima & William Kisinza (National Institute for Medical Research,
Tanzania).
Funding: President’s Malaria Initiative.
Numerous studies have shown that llong-lasting
is less certain is the added value of combining both or whether LLIN can substitute for IRS.
This study aims to evaluate the impact of combining IRS and LLINs compared to LLINs alone on malaria prevalence through a two-arm cluster randomised trial. The study is being carried out in Muleba district to the
in children 0.5-14, determined in three cross-sectional household surveys, and Entomological inoculation rate were compared between study arms.
IRS coverage was approximately 90%. ITN use ranged from 36-50%. Mean PfPR was 13% in the ITN+IRS arm and 26% in the ITN only arm, odds
effect was observed in the peak transmission season, six
ITN users were additionally protected if their houses were sprayed. Mean monthly entomological inoculation rate
added protection from combining IRS and ITNs compared to ITNs alone. The effect is likely to be attributable to IRS providing added protection to ITN users as well as compensating for inadequate ITN use. Policy makers should consider deploying IRS in combination with ITNs to control transmission if local ITN strategies on their own
for malaria control programmes to evaluate the cost effectiveness of deploying the combination.
west of Lake Victoria in Tanzania. The control villages
and the intervention villages LLIN and indoor residual spraying. Three household and prevalence cross-sectional surveys have been undertaken in children aged 6 months to 14 years and monthly entomology collection completed. IRS coverage in the intervention arm was 90%. 85% of households owned at least one insecticide
from 36 to 50%. Malaria prevalence was 13% in the
Anopheles gambiae
randomised trial that provides evidence that IRS, when
protection against malarial infection compared to ITN use alone.

44 Malaria prevention Malaria prevention 45
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A simple colorimetric test for the rapid detection of type 2-pyrethroids on bed nets.
LSHTM Investigators: Harparkash Kaur.
External Investigators/Collaborators: Tunis Eggelte (University of
Amsterdam, Amsterdam, Netherlands).
Funding: The London School of Hygiene & Tropical Medicine
Insecticide treated nets are major modes of intervention,
amount of insecticide deposit on bed nets is essential for quality control.
Currently such information can only be provided by laboratory based high tech methods such as gas chromatography and high performance liquid
bioassays where insecticide susceptible strains of mosquitoes are exposed to the bed nets. They are technically demanding to perform and require skilled staff with access to laboratory and insectary facilities.
test part of the net is placed over the tube and the cap is pushed tightly to seal the net. The test tube is turned upside down so that the solution is in contact with the net for 10 minutes. Solution D is then added to stop the reaction and the pink/red colour formed estimates the amount of deltamethrin. The test is performed in situ and does not damage the net. Field evaluations of the prototype are underway in Bioko – Equatorial Guinea.
Indoor residual spraying in combination with insecticide treated nets compared to insecticide treated nets alone for protection against malaria: a cluster randomised trial in Tanzania.
LSHTM Investigators: Philippa West, Natacha Protopopoff
Alexandra Wright, Mark Rowland & Immo Kleinschmidt.
External Investigators/Collaborators: Franklin Mosha (Kilimanjaro
Christian Medical College, Moshi, Tanzania); William Kisinza &
Tanzania); Robinson Tigererwa (Department of Health, Tanzania).
Funding: United States Agency for International Development.
This cluster randomised trial showed that deploying
compared to using ITNs alone. The size of the added protection may depend on ITN use and on local vector ecology.
Fifty clusters were randomly allocated to ITNs only or ITNs and IRS. Dwellings in the ITN+IRS arm were sprayed with two rounds of bendiocarb in 2012. Plasmodium falciparum infection prevalence (Pf
Combined use of indoor residual spraying and long-lasting insecticidal nets for malaria reduction in endemic rural Tanzania.
LSHTM Investigators: Natacha Protopopoff, Philippa West,
Alexandra Wright, Immo Kleinschmidt & Mark Rowland.
External Investigators/Collaborators: Frank Mosha & Reginald
Kavishe (Kilimanjaro Christian Medical Colleges, Tanzania); Robert
Malima & William Kisinza (National Institute for Medical Research,
Tanzania).
Funding: President’s Malaria Initiative.
Numerous studies have shown that llong-lasting
is less certain is the added value of combining both or whether LLIN can substitute for IRS.
This study aims to evaluate the impact of combining IRS and LLINs compared to LLINs alone on malaria prevalence through a two-arm cluster randomised trial. The study is being carried out in Muleba district to the
in children 0.5-14, determined in three cross-sectional household surveys, and Entomological inoculation rate were compared between study arms.
IRS coverage was approximately 90%. ITN use ranged from 36-50%. Mean PfPR was 13% in the ITN+IRS arm and 26% in the ITN only arm, odds
effect was observed in the peak transmission season, six
ITN users were additionally protected if their houses were sprayed. Mean monthly entomological inoculation rate
added protection from combining IRS and ITNs compared to ITNs alone. The effect is likely to be attributable to IRS providing added protection to ITN users as well as compensating for inadequate ITN use. Policy makers should consider deploying IRS in combination with ITNs to control transmission if local ITN strategies on their own
for malaria control programmes to evaluate the cost effectiveness of deploying the combination.
west of Lake Victoria in Tanzania. The control villages
and the intervention villages LLIN and indoor residual spraying. Three household and prevalence cross-sectional surveys have been undertaken in children aged 6 months to 14 years and monthly entomology collection completed. IRS coverage in the intervention arm was 90%. 85% of households owned at least one insecticide
from 36 to 50%. Malaria prevalence was 13% in the
Anopheles gambiae
randomised trial that provides evidence that IRS, when
protection against malarial infection compared to ITN use alone.

46 Malaria prevention Malaria prevention 47
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Combining organophosphate treated wall linings and long-lasting insecticidal nets for improved control of pyrethroid resistant Anopheles gambiae.
LSHTM Investigators: Corine Ngufor & Mark Rowland.
External Investigators/Collaborators: Emile Tchicaya & Benjamin
Sagnon N’Fale (Centre National de Recherche et de Formation sur
le Paludisme, Burkina Faso); Roch Dabire (Centre Muraz, Burkina
(Liverpool School of Tropical Medicine, UK).
Funding: European Union through the AvecNet project.
which can be produced in a long-lasting format. Non-pyrethroid versions could be used in combination with long-lasting insecticidal nets for improved control and management of insecticide resistant vector populations.
Experimental hut trials were carried out in Valley
pirimiphos methyl treated DL and NWH either alone or in combination with long-lasting insecticide-treated nets
Anopheles gambiae. Comparison was made with pyrethroid DL. Mosquitoes were genotyped for kdr and ace-1R resistant genes
to investigate the insecticide resistance management potential of the combination.
The overall kdr and ace-1R allele frequencies were 0.95 and 0.01 respectively. Mortality with p-methyl DL and NWH alone was higher than with pyrethroid DL alone
p-methyl DL or NWH with LLINs reduced biting rates
huts. Mosquitoes bearing the ace-1R gene were more
whereas all resistant and susceptible genotypes were killed by the combination.
P-methyl DL and NWH outperformed pyrethroid DL. Combining p-methyl DL and NWH with LLINs could
a vector population which is resistant to pyrethroids but susceptible to organophosphates. There was evidence that the single intervention would select kdr and ace-1R resistance genes and the combination intervention might select less strongly. Technology to bind organophosphates to plastic wall lining would be worth developing.
Multicentre studies of insecticide-treated durable wall lining in Africa and Southeast
LSHTM Investigators: Louisa Messenger, Mark Rowland & Immo
Kleinschmidt.
External Investigators/Collaborators: Abrahan Arnez (Medical
Louise Larsen (Technical Institute of Denmark, Denmark); Nathan P
Miller, The MENTOR Initiative, Angola); Adedapo Adeogun (Nigerian
Institute of Medical Research, Nigeria).
Funding:
insecticide is gradually released from an aesthetically attractive wall lining material to provide vector control for several years.
and household acceptability of DL, compared to conventional IRS in a variety of operational settings.
This study was conducted in 220 households over
was assessed using were gathered from focus group
containing questions relating to installation, exposure reactions, entomology, indoor environment, aesthetics
using bioassay tests.
The deltamethrin DL demonstrated little to no
study, supported by minimal loss of insecticide content.
bioactivity by 6 months and full loss after 12 months. The majority of participants in DL households perceived reductions in mosquito density and biting, but no changes
wanted to retain the DL, 73% cited protective reasons, 20% expressed a desire to keep theirs for decoration and 7% valued both assets equally. In Nigeria, a dichotomy between rural and urban respondents emerged. Rural participants favoured wall adornments and accepted DL because of its perceived decorative value and
preferred minimal wall decoration and rejected the DL based upon objections to its aesthetics and installation feasibility.
Just as long-lasting insecticidal nets overcame several of the technical and operational constraints associated with conventionally treated nets, this study demonstrated the potential of DL to sustain user compliance and overcome the operational challenges associated with IRS. The high level of acceptability
communities as the ideal target consumer group for DL. The poorer compliance among urban households suggests that DL would not be readily adopted or sustained in these areas. If DL is as well received in other rural areas it could overcome some of the logistical constraints associated with spray campaigns and has the potential to become a long-lasting alternative to IRS in malaria endemic areas.
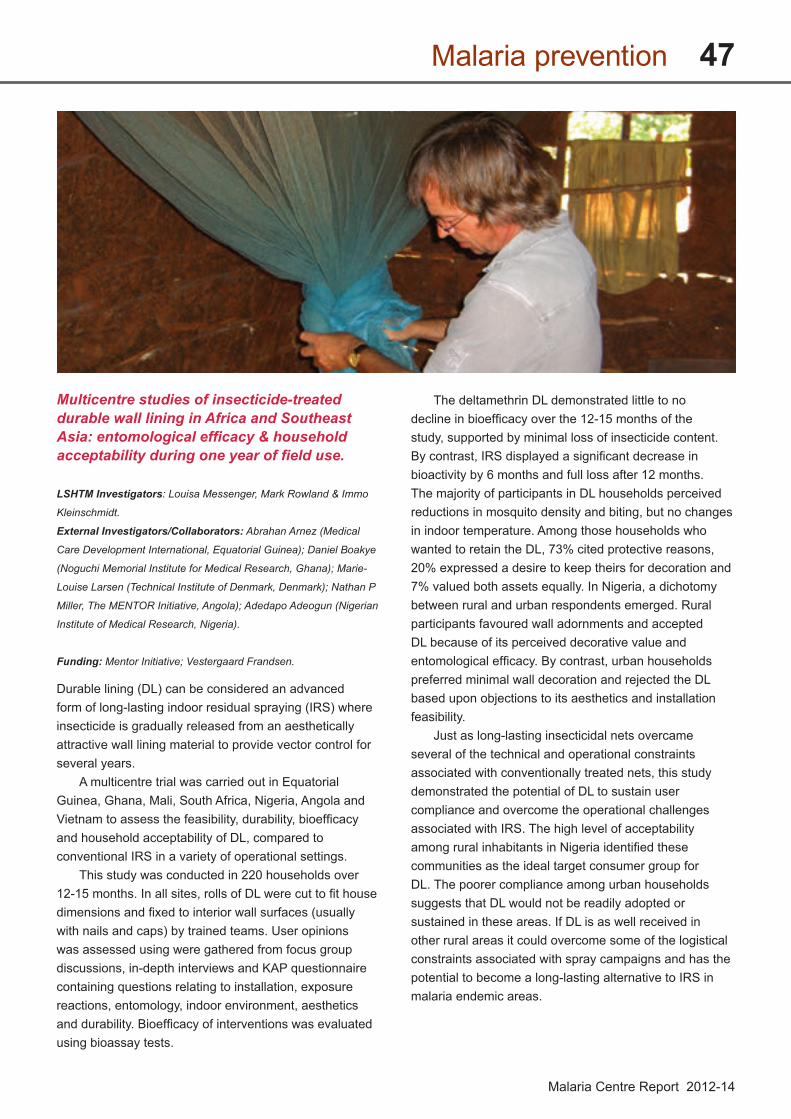
46 Malaria prevention Malaria prevention 47
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Combining organophosphate treated wall linings and long-lasting insecticidal nets for improved control of pyrethroid resistant Anopheles gambiae.
LSHTM Investigators: Corine Ngufor & Mark Rowland.
External Investigators/Collaborators: Emile Tchicaya & Benjamin
Sagnon N’Fale (Centre National de Recherche et de Formation sur
le Paludisme, Burkina Faso); Roch Dabire (Centre Muraz, Burkina
(Liverpool School of Tropical Medicine, UK).
Funding: European Union through the AvecNet project.
which can be produced in a long-lasting format. Non-pyrethroid versions could be used in combination with long-lasting insecticidal nets for improved control and management of insecticide resistant vector populations.
Experimental hut trials were carried out in Valley
pirimiphos methyl treated DL and NWH either alone or in combination with long-lasting insecticide-treated nets
Anopheles gambiae. Comparison was made with pyrethroid DL. Mosquitoes were genotyped for kdr and ace-1R resistant genes
to investigate the insecticide resistance management potential of the combination.
The overall kdr and ace-1R allele frequencies were 0.95 and 0.01 respectively. Mortality with p-methyl DL and NWH alone was higher than with pyrethroid DL alone
p-methyl DL or NWH with LLINs reduced biting rates
huts. Mosquitoes bearing the ace-1R gene were more
whereas all resistant and susceptible genotypes were killed by the combination.
P-methyl DL and NWH outperformed pyrethroid DL. Combining p-methyl DL and NWH with LLINs could
a vector population which is resistant to pyrethroids but susceptible to organophosphates. There was evidence that the single intervention would select kdr and ace-1R resistance genes and the combination intervention might select less strongly. Technology to bind organophosphates to plastic wall lining would be worth developing.
Multicentre studies of insecticide-treated durable wall lining in Africa and Southeast
LSHTM Investigators: Louisa Messenger, Mark Rowland & Immo
Kleinschmidt.
External Investigators/Collaborators: Abrahan Arnez (Medical
Louise Larsen (Technical Institute of Denmark, Denmark); Nathan P
Miller, The MENTOR Initiative, Angola); Adedapo Adeogun (Nigerian
Institute of Medical Research, Nigeria).
Funding:
insecticide is gradually released from an aesthetically attractive wall lining material to provide vector control for several years.
and household acceptability of DL, compared to conventional IRS in a variety of operational settings.
This study was conducted in 220 households over
was assessed using were gathered from focus group
containing questions relating to installation, exposure reactions, entomology, indoor environment, aesthetics
using bioassay tests.
The deltamethrin DL demonstrated little to no
study, supported by minimal loss of insecticide content.
bioactivity by 6 months and full loss after 12 months. The majority of participants in DL households perceived reductions in mosquito density and biting, but no changes
wanted to retain the DL, 73% cited protective reasons, 20% expressed a desire to keep theirs for decoration and 7% valued both assets equally. In Nigeria, a dichotomy between rural and urban respondents emerged. Rural participants favoured wall adornments and accepted DL because of its perceived decorative value and
preferred minimal wall decoration and rejected the DL based upon objections to its aesthetics and installation feasibility.
Just as long-lasting insecticidal nets overcame several of the technical and operational constraints associated with conventionally treated nets, this study demonstrated the potential of DL to sustain user compliance and overcome the operational challenges associated with IRS. The high level of acceptability
communities as the ideal target consumer group for DL. The poorer compliance among urban households suggests that DL would not be readily adopted or sustained in these areas. If DL is as well received in other rural areas it could overcome some of the logistical constraints associated with spray campaigns and has the potential to become a long-lasting alternative to IRS in malaria endemic areas.

48 Malaria prevention Malaria prevention 49
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
(Aquatain) and the insect growth regulator pyriproxifen (Sumilarv) for the control of immature Anopheles gambiae and Anopheles arabiensis.
LSHTM Investigators: Ulrike Fillinger, Oscar Mbare & Steve
Lindsay.
External Investigators/Collaborators: Bryson Ndenga (Kenya
Medical Research Institute, Kenya).
Funding: National Institute of Health; Sumitomo Chemical Ltd.
mosquito life cycle, but for the past 50 years efforts have focused almost exclusively on the control of host-seeking adults.
The opportunity provided by integrated vector
on a single intervention through sound integration of complimentary alternatives such as larval source
sustainability of available insecticides and country
are typically built around treatment of all aquatic habitats, irrespective of their productivity, and larvicides need to be applied weekly. For improving the cost-effectiveness of LSM it is important to:
space and time
to reduce the number of applications made
be incorporated into resistance management schemes
that are both potentially effective and long-lasting:
the possibility of auto-dissemination of pyriproxifen by gravid mosquitoes and a number of cage bioassays to test physiological impact of insecticides on fertility and fecundity.
Rationalising mosquito larval source management to develop a cost-effective tool for integrated vector management against malaria vectors in the western Kenya highlands.
LSHTM Investigators: Ulrike Fillinger & Oscar Mbare.
External Investigators/Collaborators: Bryson Ndenga (Kenya
Medical Research Institute, Kenya); Stefan Dongus (Ifakara Health
Institute, Tanzania); Hilary Ranson (Liverpool School of Tropical
Medicine, UK).
Funding: European Union Seventh Framework Programme;
Sumitomo Chemical.
source management highlights the potential of this method in reducing malaria transmission especially in areas where larval habitats are focal and accessible, i.e. in highland areas.
Costs per person protected for implementing larval control programs at scale are estimated in the same range as indoor residual spraying programmes
and higher cost-effectiveness is likely for areas where targeting the intervention in time would be feasible and where high population density could be protected by the intervention; however there is a lack of empirical evidence to support this suggestion. Rationalising of this strategy
to date, is that the intervention is typically built around treatment of all aquatic habitats all year round in short re-application cycles. This pilot study was designed to investigate the insect growth regulator, pyriproxyfen, for its potential residual control of immature malaria vectors and to compare the technical feasibility and potential impact on malaria transmission of time-targeted (March-
of this insecticide in the western Kenya Highlands, the most highly populated area in Kenya with localised larval habitats. Data from this pilot trial will provide the necessary information to design a large scale randomised controlled trial.
Mosquito larval source management for controlling malaria.
LSHTM Investigators: Lucy Tusting, Ulrike Fillinger, Christian
Bottomley & Steve Lindsay.
External Investigators/Collaborators: Julie Thwing (Centers for
Disease Control and Prevention, USA); David Sinclair (Liverpool
and Prevention, USA); Kimberley Bonner (Princeton University,
Princeton, USA).
Funding:
of malaria vector control that targets mosquito larvae as they mature in aquatic habitats, for example by larviciding or draining land.
We carried out a Cochrane Review to evaluate the effectiveness of LSM for controlling malaria. We screened
eligible for inclusion. In two cluster-randomised controlled
and rural India and rural Kenya, results were inconsistent.
the Gambia River, larviciding by ground teams did not
larviciding reduced parasite prevalence by almost 90%
and-after trials in Greece, India, the Philippines, and Tanzania, LSM reduced parasite prevalence by two-thirds
another policy option, alongside long-lasting insecticide-treated nets and indoor residual spraying for malaria
proportion of larval habitats can be targeted. Further research is needed to evaluate whether larval source
larval habitats are more extensive.
Do topical repellents divert mosquitoes within a community? Health equity implications of topical repellents as a mosquito bite prevention tool.
LSHTM Investigators: Onyango Sangoro.
External Investigators/Collaborators: Marta Maia, Max Thele,
Emmanuel Simfukwe & Sarah Moore (Ifakara Health Institute,
Tanzania); Elizabeth Turner (Duke University, USA).
Repellents do not kill mosquitoes-they simply reduce human-vector contact. Thus it is possible that individuals who do not use repellents but dwell close to repellent users experience more bites than otherwise. The objective of this study was to measure if diversion occurs from households that use repellents to those that do not use repellents.
The study was performed in three Tanzanian villages
insecticide-treated nets. Three coverage scenarios were investigated: complete coverage (all households
crossover study design was used and coverage scenarios
were rotated weekly over a period of ten weeks. The placebo lotion was randomly allocated to households in the incomplete coverage scenario. The level of compliance was reported to be close to 100%. Mosquito densities were measured through aspiration of resting mosquitoes. Data were analysed using negative binomial regression models.
Repellent-users had consistently fewer mosquitoes in their dwellings. In villages where everybody had been given 15%-DEET, resting mosquito densities were fewer than half that of households in the no coverage scenario
a village where 80% of the households used 15%-DEET were likely to have over four-times more mosquitoes
dwellings in comparison to households in a village where nobody uses repellent.
There is evidence that high coverage of repellent use
incomplete coverage evidence suggests that mosquitoes are diverted from households that use repellent to those that do not. Therefore, if repellents are to be considered for vector control, strategies to maximise coverage are required.

48 Malaria prevention Malaria prevention 49
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
(Aquatain) and the insect growth regulator pyriproxifen (Sumilarv) for the control of immature Anopheles gambiae and Anopheles arabiensis.
LSHTM Investigators: Ulrike Fillinger, Oscar Mbare & Steve
Lindsay.
External Investigators/Collaborators: Bryson Ndenga (Kenya
Medical Research Institute, Kenya).
Funding: National Institute of Health; Sumitomo Chemical Ltd.
mosquito life cycle, but for the past 50 years efforts have focused almost exclusively on the control of host-seeking adults.
The opportunity provided by integrated vector
on a single intervention through sound integration of complimentary alternatives such as larval source
sustainability of available insecticides and country
are typically built around treatment of all aquatic habitats, irrespective of their productivity, and larvicides need to be applied weekly. For improving the cost-effectiveness of LSM it is important to:
space and time
to reduce the number of applications made
be incorporated into resistance management schemes
that are both potentially effective and long-lasting:
the possibility of auto-dissemination of pyriproxifen by gravid mosquitoes and a number of cage bioassays to test physiological impact of insecticides on fertility and fecundity.
Rationalising mosquito larval source management to develop a cost-effective tool for integrated vector management against malaria vectors in the western Kenya highlands.
LSHTM Investigators: Ulrike Fillinger & Oscar Mbare.
External Investigators/Collaborators: Bryson Ndenga (Kenya
Medical Research Institute, Kenya); Stefan Dongus (Ifakara Health
Institute, Tanzania); Hilary Ranson (Liverpool School of Tropical
Medicine, UK).
Funding: European Union Seventh Framework Programme;
Sumitomo Chemical.
source management highlights the potential of this method in reducing malaria transmission especially in areas where larval habitats are focal and accessible, i.e. in highland areas.
Costs per person protected for implementing larval control programs at scale are estimated in the same range as indoor residual spraying programmes
and higher cost-effectiveness is likely for areas where targeting the intervention in time would be feasible and where high population density could be protected by the intervention; however there is a lack of empirical evidence to support this suggestion. Rationalising of this strategy
to date, is that the intervention is typically built around treatment of all aquatic habitats all year round in short re-application cycles. This pilot study was designed to investigate the insect growth regulator, pyriproxyfen, for its potential residual control of immature malaria vectors and to compare the technical feasibility and potential impact on malaria transmission of time-targeted (March-
of this insecticide in the western Kenya Highlands, the most highly populated area in Kenya with localised larval habitats. Data from this pilot trial will provide the necessary information to design a large scale randomised controlled trial.
Mosquito larval source management for controlling malaria.
LSHTM Investigators: Lucy Tusting, Ulrike Fillinger, Christian
Bottomley & Steve Lindsay.
External Investigators/Collaborators: Julie Thwing (Centers for
Disease Control and Prevention, USA); David Sinclair (Liverpool
and Prevention, USA); Kimberley Bonner (Princeton University,
Princeton, USA).
Funding:
of malaria vector control that targets mosquito larvae as they mature in aquatic habitats, for example by larviciding or draining land.
We carried out a Cochrane Review to evaluate the effectiveness of LSM for controlling malaria. We screened
eligible for inclusion. In two cluster-randomised controlled
and rural India and rural Kenya, results were inconsistent.
the Gambia River, larviciding by ground teams did not
larviciding reduced parasite prevalence by almost 90%
and-after trials in Greece, India, the Philippines, and Tanzania, LSM reduced parasite prevalence by two-thirds
another policy option, alongside long-lasting insecticide-treated nets and indoor residual spraying for malaria
proportion of larval habitats can be targeted. Further research is needed to evaluate whether larval source
larval habitats are more extensive.
Do topical repellents divert mosquitoes within a community? Health equity implications of topical repellents as a mosquito bite prevention tool.
LSHTM Investigators: Onyango Sangoro.
External Investigators/Collaborators: Marta Maia, Max Thele,
Emmanuel Simfukwe & Sarah Moore (Ifakara Health Institute,
Tanzania); Elizabeth Turner (Duke University, USA).
Repellents do not kill mosquitoes-they simply reduce human-vector contact. Thus it is possible that individuals who do not use repellents but dwell close to repellent users experience more bites than otherwise. The objective of this study was to measure if diversion occurs from households that use repellents to those that do not use repellents.
The study was performed in three Tanzanian villages
insecticide-treated nets. Three coverage scenarios were investigated: complete coverage (all households
crossover study design was used and coverage scenarios
were rotated weekly over a period of ten weeks. The placebo lotion was randomly allocated to households in the incomplete coverage scenario. The level of compliance was reported to be close to 100%. Mosquito densities were measured through aspiration of resting mosquitoes. Data were analysed using negative binomial regression models.
Repellent-users had consistently fewer mosquitoes in their dwellings. In villages where everybody had been given 15%-DEET, resting mosquito densities were fewer than half that of households in the no coverage scenario
a village where 80% of the households used 15%-DEET were likely to have over four-times more mosquitoes
dwellings in comparison to households in a village where nobody uses repellent.
There is evidence that high coverage of repellent use
incomplete coverage evidence suggests that mosquitoes are diverted from households that use repellent to those that do not. Therefore, if repellents are to be considered for vector control, strategies to maximise coverage are required.

50 Malaria prevention Malaria prevention 51
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
--
tions provides a disease exposure free tech-
LSHTM Investigators: Onyango Sangoro.
External Investigators/Collaborators: Dickson Lweitojera, Emma-
nuel Simfukwe, Hassan Ngonyani, Edgar Mbeyela, Daniel Lugiko,
Japhet Kihonda, Marta Maia & Sarah Moore (Ifakara Health Institute,
Tanzania).
Before topical repellents can be employed as interven--
volunteers, are the main methods used for assessing the
However, laboratory tests are not representative of real life conditions under which repellents are used and
-ease. There is, therefore, a need to develop methods to
minimizing volunteer exposure to disease. -
compared to a placebo lotion in a 200 sq m (10 m x 20
Anopheles arabiensisagainst wild malaria vectors and nuisance-biting mosqui-toes. The average percentage protection against biting
used to determine relative risk of being bitten when wear-ing either of these repellents compared to the placebo.
15% DEET repellent after four hours of mosquito collec-
DEET in ethanol after four hours was 71.29% (CI 61.77-
applied mosquito repellents, thereby avoiding risks of exposure to mosquito-borne pathogens, associated with
An experimental hut study to quantify the ef-fect of DichloroDiphenylTrichloroethane (DDT) and airborne pyrethroids on entomological parameters of malaria transmission.
LSHTM Investigators: Sheila Ogoma & Lena Lorenz.
External Investigators/Collaborators: Hassan Ngonyani, Robert
Sangusangu, Mohammed Kitumbukile, Masoudi Kilalangongono,
Emmanuel Simfukwe, Anton Mseka, Edgar Mbeyela, Deogratius
Roman, Jason Moore, Katharina Kreppel Marta Maia & Sarah Moore
(Ifakara Health Institute, Tanzania).
Current malaria vector control programmes rely on insec-ticides with rapid contact toxicity. However, spatial repel-lents can also be applied to reduce man-vector contact, which might ultimately impact malaria transmission. The aim of this study was to quantify effects of airborne pyre-throids from coils and DDT used an indoor residual spray
transmission. -
pared to DDT on house entry, exit and indoor feeding be-haviour of Anopheles gambiae sensu lato were measured
-comes were deterrence - reduction in house entry of mos-
quitoes; irritancy or excito-repellency - induced premature exit of mosquitoes; blood feeding inhibition and effect on
and DDT reduced human vector contact through deter-rence by 38%, 30% and 8%, respectively and induced half of the mosquitoes to leave huts before feeding (56%,
than three quarters of mosquitoes in the DDT hut did not feed, almost none laid eggs and 67%, 72% and 70% of all
DDT huts, respectively had died after 24 hours.This study highlights that airborne pyrethroids and
DDT affect a range of anopheline mosquito behaviours that are important parameters in malaria transmission, namely deterrence, irritancy/excito-repellency and blood-
-cant toxicity and reduced mosquito fecundity that affect mosquito densities and, therefore, provide community protection against diseases for both users and non-users.
-lar effects on deterrence, irritancy and feeding inhibition. Therefore, it is suggested that airborne pyrethroids, if delivered in suitable formats, may complement existing mainstream vector control tools.
Insecticide resistance
Loss of household protection with insecticide treated nets against pyrethroid-resistant Anopheles gambiae.
LSHTM Investigators
& Mark Rowland.
External Investigators/Collaborators: Martin Akogbeto (The
Entomological Research Center of Cotonou, Benin).
Funding: London School of Hygiene & Tropical Medicine, Curtis
Foundation.
Pyrethroid resistance is becoming widespread in nopheles gambiae, coinciding with expansion of
To investigate whether nets in-use are still protective, household trials were undertaken in northern and Southern Benin where Anopheles gambiae is susceptible and resistant to pyrethroids respectively. Rooms were
blood-feeding and survival rates before and after the nets were treated with pyrethroid.
Sleeping under an ITN at the resistant location was no more protective than sleeping under an untreated net
Distribution and Spread of Pyrethroid and DichloroDiphenylTrichloroethane (DDT) Resistance among the Anopheles gambiae complex in Tanzania.
LSHTM Investigators: Mark Rowland & Natacha Protopopoff.
External Investigators/Collaborators: Bilali Kabula, Patrick
Tungu, Robert Malima, Stephen Magesa & William Kisinza (The
National Institute for Medical Research, Tanzania); Franklin Mosha
(Kilimanjaro Christian Medical Centre, Tanzania).
Funding: The United States Agency for International Development.
The development of insecticide resistance is a threat
annual surveys of resistance in 14 sentinel site. The report the 2011 National Survey is compared
to the situations in 2004 and 2010. Anopheles gambiae was resistant to pyrethroids in Muleba, Muheza, Moshi
Anopheles gambiae is becoming resistant to pyrethoids and DDT in several parts of Tanzania. This coincided with scaling up of vector control measures. Resistance may impair the effectiveness of these interventions and therefore demands close monitoring and adoption of a resistance management strategy.
at the susceptible location decreased by 66% the odds
ITNs provide little or no protection once the mosquitoes become resistant and the netting holed. Resistance presents a grave threat to malaria control strategy based on ITN.
With universal coverage of vector control interventions, selection of resistance to insecticide in the mosquito vector is following close behind. Strategies of combining insecticides are being evaluated for their potential to control malaria transmitted by insecticide resistant populations.

50 Malaria prevention Malaria prevention 51
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
--
tions provides a disease exposure free tech-
LSHTM Investigators: Onyango Sangoro.
External Investigators/Collaborators: Dickson Lweitojera, Emma-
nuel Simfukwe, Hassan Ngonyani, Edgar Mbeyela, Daniel Lugiko,
Japhet Kihonda, Marta Maia & Sarah Moore (Ifakara Health Institute,
Tanzania).
Before topical repellents can be employed as interven--
volunteers, are the main methods used for assessing the
However, laboratory tests are not representative of real life conditions under which repellents are used and
-ease. There is, therefore, a need to develop methods to
minimizing volunteer exposure to disease. -
compared to a placebo lotion in a 200 sq m (10 m x 20
Anopheles arabiensisagainst wild malaria vectors and nuisance-biting mosqui-toes. The average percentage protection against biting
used to determine relative risk of being bitten when wear-ing either of these repellents compared to the placebo.
15% DEET repellent after four hours of mosquito collec-
DEET in ethanol after four hours was 71.29% (CI 61.77-
applied mosquito repellents, thereby avoiding risks of exposure to mosquito-borne pathogens, associated with
An experimental hut study to quantify the ef-fect of DichloroDiphenylTrichloroethane (DDT) and airborne pyrethroids on entomological parameters of malaria transmission.
LSHTM Investigators: Sheila Ogoma & Lena Lorenz.
External Investigators/Collaborators: Hassan Ngonyani, Robert
Sangusangu, Mohammed Kitumbukile, Masoudi Kilalangongono,
Emmanuel Simfukwe, Anton Mseka, Edgar Mbeyela, Deogratius
Roman, Jason Moore, Katharina Kreppel Marta Maia & Sarah Moore
(Ifakara Health Institute, Tanzania).
Current malaria vector control programmes rely on insec-ticides with rapid contact toxicity. However, spatial repel-lents can also be applied to reduce man-vector contact, which might ultimately impact malaria transmission. The aim of this study was to quantify effects of airborne pyre-throids from coils and DDT used an indoor residual spray
transmission. -
pared to DDT on house entry, exit and indoor feeding be-haviour of Anopheles gambiae sensu lato were measured
-comes were deterrence - reduction in house entry of mos-
quitoes; irritancy or excito-repellency - induced premature exit of mosquitoes; blood feeding inhibition and effect on
and DDT reduced human vector contact through deter-rence by 38%, 30% and 8%, respectively and induced half of the mosquitoes to leave huts before feeding (56%,
than three quarters of mosquitoes in the DDT hut did not feed, almost none laid eggs and 67%, 72% and 70% of all
DDT huts, respectively had died after 24 hours.This study highlights that airborne pyrethroids and
DDT affect a range of anopheline mosquito behaviours that are important parameters in malaria transmission, namely deterrence, irritancy/excito-repellency and blood-
-cant toxicity and reduced mosquito fecundity that affect mosquito densities and, therefore, provide community protection against diseases for both users and non-users.
-lar effects on deterrence, irritancy and feeding inhibition. Therefore, it is suggested that airborne pyrethroids, if delivered in suitable formats, may complement existing mainstream vector control tools.
Insecticide resistance
Loss of household protection with insecticide treated nets against pyrethroid-resistant Anopheles gambiae.
LSHTM Investigators
& Mark Rowland.
External Investigators/Collaborators: Martin Akogbeto (The
Entomological Research Center of Cotonou, Benin).
Funding: London School of Hygiene & Tropical Medicine, Curtis
Foundation.
Pyrethroid resistance is becoming widespread in nopheles gambiae, coinciding with expansion of
To investigate whether nets in-use are still protective, household trials were undertaken in northern and Southern Benin where Anopheles gambiae is susceptible and resistant to pyrethroids respectively. Rooms were
blood-feeding and survival rates before and after the nets were treated with pyrethroid.
Sleeping under an ITN at the resistant location was no more protective than sleeping under an untreated net
Distribution and Spread of Pyrethroid and DichloroDiphenylTrichloroethane (DDT) Resistance among the Anopheles gambiae complex in Tanzania.
LSHTM Investigators: Mark Rowland & Natacha Protopopoff.
External Investigators/Collaborators: Bilali Kabula, Patrick
Tungu, Robert Malima, Stephen Magesa & William Kisinza (The
National Institute for Medical Research, Tanzania); Franklin Mosha
(Kilimanjaro Christian Medical Centre, Tanzania).
Funding: The United States Agency for International Development.
The development of insecticide resistance is a threat
annual surveys of resistance in 14 sentinel site. The report the 2011 National Survey is compared
to the situations in 2004 and 2010. Anopheles gambiae was resistant to pyrethroids in Muleba, Muheza, Moshi
Anopheles gambiae is becoming resistant to pyrethoids and DDT in several parts of Tanzania. This coincided with scaling up of vector control measures. Resistance may impair the effectiveness of these interventions and therefore demands close monitoring and adoption of a resistance management strategy.
at the susceptible location decreased by 66% the odds
ITNs provide little or no protection once the mosquitoes become resistant and the netting holed. Resistance presents a grave threat to malaria control strategy based on ITN.
With universal coverage of vector control interventions, selection of resistance to insecticide in the mosquito vector is following close behind. Strategies of combining insecticides are being evaluated for their potential to control malaria transmitted by insecticide resistant populations.

52 Malaria prevention Malaria prevention 53
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Global project on the implications of insecticide resistance.
Testing local mosquitos for insecticide resistance, Chhattisgarh, India.
An online tool for mapping insecticide resistance in major Anopheles vectors of human malaria parasites and review of resistance status for the Afrotropical region.
LSHTM Investigators
External Investigators/Collaborators:
Control and Prevention, Kenya & Maseno University, Maseno,
Ndungo & Patrick Chege (Esri Eastern Africa, Kenya); Richard Hunt
(University of the Witwatersrand, South Africa); Nabie M Bayoh
Prevention, Kenya); Riann Christian & Maureen Coetzee (University
of the Witwatersrand, South Africa; The National Health Laboratory
Service, South Africa).
Funding: President’s Malaria Initiative; The United States Agency
for International Development.
are facing increasing insecticide resistance in the major anopheline vectors.
In order to preserve or prolong the effectiveness of the main malaria vector interventions, up-to-date and easily accessible insecticide resistance data that are interpretable at operationally-relevant scales are critical. Here in we introduce and demonstrate the usefulness of an online mapping tool, IR Mapper.
literature was performed and Anopheles insecticide
susceptibility and resistance mechanisms data were extracted and added to a database after a two-level
exploration and projection of these data.Literature searches yielded a total of 4,084
susceptibility data points for 1,505 populations, and 2,097 resistance mechanisms data points for 1,000 populations of Anopheles collected via recommended World Health
abundant for populations of Anopheles gambiae, and
were more commonly used in susceptibility assays (51.1
and organophosphates. Between 2001 and 2012, there was a clear increase in prevalence and distribution
Anopheles gambiae to pyrethroids (from 41 to 87% of the mosquito populations
were widespread. For Anopheles funestus, relatively few populations were tested, although in 2010–2012 resistance was reported in 50% of 10 populations tested. Maps are provided to illustrate the use of IR Mapper and the distribution of insecticide resistance in malaria vectors
LSHTM Investigators: Immo Kleinschmidt & John Bradley.
External Investigators/Collaborators: World Health
Organization
Liverpool School of Tropical Medicine, UK;
Federal Ministry of Health, Sudan; Malaria Control
Kenya Medical Research Institute, Kenya; National Malaria
Control Programme, Kenya; National Malaria Control
Programme, Benin; The Entomological Research Center of
Benin; National University of Benin, Benin; National
Malaria Control Programme, Cameroon; , Organisation de
Centrale, Benin; India: Organisation de Coordination pour la
Institute for Medical Research, India; Ministry of Health, India;
Family Welfare, Chhattisgarh Directorate of Health Services,
India.
Funding: World
Health Organization
This study assesses the impact that insecticide resistance has on the effectiveness of malaria vector control tools long-lasting insecticide-treated nets
In two countries this is done by cluster randomised trials of universal coverage LLINs versus universal coverage LLINs in combination with IRS, with levels of insecticide resistance of the main vector balanced between the two study arms. In each cluster resistance to the insecticide used on LLINs is monitored, and malaria incidence is estimated from
the duration of the study. In three countries, clusters are established and malaria vector mosquitoes in each cluster assessed for resistance to the insecticide used. Cohorts of children recruited for follow-up and estimation of malaria incidence. Resistance impact will be assessed from the ratio of incidence rates in clusters with high compared to those with low resistance. Resistance mechanisms will be determined in subsets of study clusters.

52 Malaria prevention Malaria prevention 53
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Global project on the implications of insecticide resistance.
Testing local mosquitos for insecticide resistance, Chhattisgarh, India.
An online tool for mapping insecticide resistance in major Anopheles vectors of human malaria parasites and review of resistance status for the Afrotropical region.
LSHTM Investigators
External Investigators/Collaborators:
Control and Prevention, Kenya & Maseno University, Maseno,
Ndungo & Patrick Chege (Esri Eastern Africa, Kenya); Richard Hunt
(University of the Witwatersrand, South Africa); Nabie M Bayoh
Prevention, Kenya); Riann Christian & Maureen Coetzee (University
of the Witwatersrand, South Africa; The National Health Laboratory
Service, South Africa).
Funding: President’s Malaria Initiative; The United States Agency
for International Development.
are facing increasing insecticide resistance in the major anopheline vectors.
In order to preserve or prolong the effectiveness of the main malaria vector interventions, up-to-date and easily accessible insecticide resistance data that are interpretable at operationally-relevant scales are critical. Here in we introduce and demonstrate the usefulness of an online mapping tool, IR Mapper.
literature was performed and Anopheles insecticide
susceptibility and resistance mechanisms data were extracted and added to a database after a two-level
exploration and projection of these data.Literature searches yielded a total of 4,084
susceptibility data points for 1,505 populations, and 2,097 resistance mechanisms data points for 1,000 populations of Anopheles collected via recommended World Health
abundant for populations of Anopheles gambiae, and
were more commonly used in susceptibility assays (51.1
and organophosphates. Between 2001 and 2012, there was a clear increase in prevalence and distribution
Anopheles gambiae to pyrethroids (from 41 to 87% of the mosquito populations
were widespread. For Anopheles funestus, relatively few populations were tested, although in 2010–2012 resistance was reported in 50% of 10 populations tested. Maps are provided to illustrate the use of IR Mapper and the distribution of insecticide resistance in malaria vectors
LSHTM Investigators: Immo Kleinschmidt & John Bradley.
External Investigators/Collaborators: World Health
Organization
Liverpool School of Tropical Medicine, UK;
Federal Ministry of Health, Sudan; Malaria Control
Kenya Medical Research Institute, Kenya; National Malaria
Control Programme, Kenya; National Malaria Control
Programme, Benin; The Entomological Research Center of
Benin; National University of Benin, Benin; National
Malaria Control Programme, Cameroon; , Organisation de
Centrale, Benin; India: Organisation de Coordination pour la
Institute for Medical Research, India; Ministry of Health, India;
Family Welfare, Chhattisgarh Directorate of Health Services,
India.
Funding: World
Health Organization
This study assesses the impact that insecticide resistance has on the effectiveness of malaria vector control tools long-lasting insecticide-treated nets
In two countries this is done by cluster randomised trials of universal coverage LLINs versus universal coverage LLINs in combination with IRS, with levels of insecticide resistance of the main vector balanced between the two study arms. In each cluster resistance to the insecticide used on LLINs is monitored, and malaria incidence is estimated from
the duration of the study. In three countries, clusters are established and malaria vector mosquitoes in each cluster assessed for resistance to the insecticide used. Cohorts of children recruited for follow-up and estimation of malaria incidence. Resistance impact will be assessed from the ratio of incidence rates in clusters with high compared to those with low resistance. Resistance mechanisms will be determined in subsets of study clusters.

54 Malaria prevention Malaria prevention 55
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
High level resistance in Anopheles gambiae to pyrethroid insecticides and reduced susceptibility to bendiocarb in North-Western Tanzania.
LSHTM Investigators
Wright, Philippa West, Immo Kleinschmidt & Mark
Rowland.
External Investigators/Collaborators: Johnson
Matowo, Reginald Kavishe, Robert Kaaya & Franklin
Mosha (Kilimanjaro Christian Medical Centre, Tanzania);
Robert Malima & William Kisinza, (The National Institute
for Medical Research, Tanzania).
Funding: President’s Malaria Initiative; The United
States Agency for International Development.
To control malaria, long lasting insecticide-
Tanzania. The main threat to these measures is the selection of insecticide resistance.
To monitor the rapidly evolving situation, the resistance status of Anopheles gambiae to different insecticides were investigated in North West Tanzania, an area that has been subject to several rounds of pyrethroid IRS since 2006.
Collections of mosquitoes were exposed to diagnostic dosages of pyrethroid and
resistance test kits and samples analysed for resistance mechanisms using real time PCR.
80% were Anopheles gambiae and 20% Anopheles arabiensis. No fewer than 60% were resistant in any survey. The kdr-eastern variant was present in 97% of Anopheles gambiae but was absent in Anopheles arabiensis. Anopheles gambiae also showed reduced susceptibility to the carbamate insecticide, bendiocarb.
Anopheles gambiae has developed a high frequency of resistance to pyrethroids
Unlike in coastal Tanzania, where the ratio of Anopheles gambiae to Anopheles arabiensis has decreased in response to vector control, Anopheles gambiae persists at high frequency in north-western Tanzania, probably due to selection of pyrethroid resistance, and this trend is likely to arise in other areas as resistance spreads or is subject to local selection from IRS or LLINs.
Use of indoor residual spraying and long-lasting insecticidal nets with synergist for control of malaria transmitted by pyrethroid resistant vectors in endemic Tanzania.
LSHTM Investigators: Natacha Protopopoff, Alexandra Wright,
Immo Kleinschmidt & Mark Rowland.
External Investigators/Collaborators: Frank Mosha & Reginald
Kavishe (Kilimanjaro Christian Medical Colleges, Tanzania); Robert
Malima & William Kisinza (National Institute for Medical Research,
Tanzania).
Funding: The Medical Research Council; The Wellcome Trust; The
UK Department for International Development.
The massive scale-up of vector control measures has
prevention and vector control tools are long-lasting
Both rely on pyrethroid insecticides either to provide a repellent barrier between humans and mosquitoes
or to kill mosquitoes before they can transmit malaria. With the huge efforts being taken to provide universal coverage of LLINs to those at risk there is, unfortunately, enormous selection pressure on mosquitoes to develop resistance to pyrethroids. Resistance is now occurring in most countries and some forms appear to be so strong that vector mosquitoes survive contact and continue to transmit malaria. In the present trial we will evaluate a new types of LLIN that incorporate a chemical synergist that knocks out the resistance mechanism so the LLIN continues to protect and long-lasting non-pyrethroid insecticides that can be sprayed on walls and provide control for almost a year compared to standard LLIN
will be randomly allocated to 4 different interventions; 1/the standard LLIN, 2/ new LLIN, 3/combination standard LLIN and IRS with the long lasting insecticide and 4/ IRS with the new type of LLIN. The impact of the intervention on malaria prevalence and transmission, entomological inoculation rate and the selection of resistance will be evaluated for 2 years.
Olyset Duo® (a pyriproxyfen and permethrin mixture net): an experimental hut trial against pyrethroid resistant Anopheles gambiae and Culex quinquefasciatus in southern Benin.
LSHTM Investigators
Rowland.
External Investigators/Collaborators: Akogbeto Martin (Centre de
Recherches Entomologiques de Cotonou, Benin).
Funding:
control of pyrethroid resistant malaria vectors are urgently
reduces the fecundity and fertility of adult female mosquitoes.
mixture LN containing pyriproxyfen and permethrin, was evaluated in experimental huts in southern Benin against pyrethroid resistant Anopheles gambiae and Culex quinquefasciatus.
fed Anopheles gambiae from the control hut was 37%
laid eggs. The tunnel test results were consistent with the
resistant Culex quinquefasciatus although mortality rates
surviving blood-fed Culex quinquefasciatus. with the PPF-treated nets.
personal protection and killing of pyrethroid resistant Anopheles gambiae, and sterilized surviving blood-fed mosquitoes. Mixing pyrethroid and pyriproxyfen on a LN shows potential for malaria control and management of pyrethroid resistant vectors by preventing further selection of pyrethroid resistant phenotypes.

54 Malaria prevention Malaria prevention 55
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
High level resistance in Anopheles gambiae to pyrethroid insecticides and reduced susceptibility to bendiocarb in North-Western Tanzania.
LSHTM Investigators
Wright, Philippa West, Immo Kleinschmidt & Mark
Rowland.
External Investigators/Collaborators: Johnson
Matowo, Reginald Kavishe, Robert Kaaya & Franklin
Mosha (Kilimanjaro Christian Medical Centre, Tanzania);
Robert Malima & William Kisinza, (The National Institute
for Medical Research, Tanzania).
Funding: President’s Malaria Initiative; The United
States Agency for International Development.
To control malaria, long lasting insecticide-
Tanzania. The main threat to these measures is the selection of insecticide resistance.
To monitor the rapidly evolving situation, the resistance status of Anopheles gambiae to different insecticides were investigated in North West Tanzania, an area that has been subject to several rounds of pyrethroid IRS since 2006.
Collections of mosquitoes were exposed to diagnostic dosages of pyrethroid and
resistance test kits and samples analysed for resistance mechanisms using real time PCR.
80% were Anopheles gambiae and 20% Anopheles arabiensis. No fewer than 60% were resistant in any survey. The kdr-eastern variant was present in 97% of Anopheles gambiae but was absent in Anopheles arabiensis. Anopheles gambiae also showed reduced susceptibility to the carbamate insecticide, bendiocarb.
Anopheles gambiae has developed a high frequency of resistance to pyrethroids
Unlike in coastal Tanzania, where the ratio of Anopheles gambiae to Anopheles arabiensis has decreased in response to vector control, Anopheles gambiae persists at high frequency in north-western Tanzania, probably due to selection of pyrethroid resistance, and this trend is likely to arise in other areas as resistance spreads or is subject to local selection from IRS or LLINs.
Use of indoor residual spraying and long-lasting insecticidal nets with synergist for control of malaria transmitted by pyrethroid resistant vectors in endemic Tanzania.
LSHTM Investigators: Natacha Protopopoff, Alexandra Wright,
Immo Kleinschmidt & Mark Rowland.
External Investigators/Collaborators: Frank Mosha & Reginald
Kavishe (Kilimanjaro Christian Medical Colleges, Tanzania); Robert
Malima & William Kisinza (National Institute for Medical Research,
Tanzania).
Funding: The Medical Research Council; The Wellcome Trust; The
UK Department for International Development.
The massive scale-up of vector control measures has
prevention and vector control tools are long-lasting
Both rely on pyrethroid insecticides either to provide a repellent barrier between humans and mosquitoes
or to kill mosquitoes before they can transmit malaria. With the huge efforts being taken to provide universal coverage of LLINs to those at risk there is, unfortunately, enormous selection pressure on mosquitoes to develop resistance to pyrethroids. Resistance is now occurring in most countries and some forms appear to be so strong that vector mosquitoes survive contact and continue to transmit malaria. In the present trial we will evaluate a new types of LLIN that incorporate a chemical synergist that knocks out the resistance mechanism so the LLIN continues to protect and long-lasting non-pyrethroid insecticides that can be sprayed on walls and provide control for almost a year compared to standard LLIN
will be randomly allocated to 4 different interventions; 1/the standard LLIN, 2/ new LLIN, 3/combination standard LLIN and IRS with the long lasting insecticide and 4/ IRS with the new type of LLIN. The impact of the intervention on malaria prevalence and transmission, entomological inoculation rate and the selection of resistance will be evaluated for 2 years.
Olyset Duo® (a pyriproxyfen and permethrin mixture net): an experimental hut trial against pyrethroid resistant Anopheles gambiae and Culex quinquefasciatus in southern Benin.
LSHTM Investigators
Rowland.
External Investigators/Collaborators: Akogbeto Martin (Centre de
Recherches Entomologiques de Cotonou, Benin).
Funding:
control of pyrethroid resistant malaria vectors are urgently
reduces the fecundity and fertility of adult female mosquitoes.
mixture LN containing pyriproxyfen and permethrin, was evaluated in experimental huts in southern Benin against pyrethroid resistant Anopheles gambiae and Culex quinquefasciatus.
fed Anopheles gambiae from the control hut was 37%
laid eggs. The tunnel test results were consistent with the
resistant Culex quinquefasciatus although mortality rates
surviving blood-fed Culex quinquefasciatus. with the PPF-treated nets.
personal protection and killing of pyrethroid resistant Anopheles gambiae, and sterilized surviving blood-fed mosquitoes. Mixing pyrethroid and pyriproxyfen on a LN shows potential for malaria control and management of pyrethroid resistant vectors by preventing further selection of pyrethroid resistant phenotypes.

56 Malaria prevention Malaria prevention 57
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Mosquito nets treated with a mixture of the insecticides chlorfenapyr and alphacypermethrin control pyrethroid resistant Anopheles gambiae and Culex quinquefasciatus mosquitoes in West Africa.
LSHTM Investigators
Rowland.
External Investigators/Collaborators: Andreas Kudom, Pelagie
Boko & Abibathou Odjo (Centre de Recherche Entomologique
Consortium, UK).
Funding:
The effectiveness of insecticide treated nets is under
selection of pyrethroid resistance in Anopheles gambiae mosquitoes.
To maintain progress against malaria it is necessary to identify alternative residual insecticides for mosquito nets. Mixtures of pyrethroid and insecticides with novel mode of action provide scope for both improved control and management of resistance through concurrent exposure to unrelated insecticides.
The pyrrole chlorfenapyr and the pyrethroid alphacypermethrin were tested individually and as a mixture on mosquito nets in an experimental hut trial in southern Benin against pyrethroid resistant Anopheles
gambiae and Culex quinquefasciatus mosquitoes. The nets were deliberately holed to simulate the effect of wear and tear.
The nets treated with the mixture of chlorfenapyr 200mg/m2 and alphacypermethrin 25mg/m2 killed a proportion of Anopheles gambiae (77%, 95%CI:
nets treated with the mixture reduced mosquito biting and blood-feeding rates to the same level as the alphacypermethrin treated net, whereas the chlorfenapyr
mortality and blood feeding inhibition between treatments was observed among Culex quinquefasciatus to that seen among Anopheles gambiae, although the effects were
applied at 100mg/m2 had an effect similar to the mixture with chlorfenapyr at 200mg/m2.
The effectiveness of Iinsecticide treated nets against pyrethroid resistant mosquitoes was restored by the mixture: the alphacypermethrin component reduced human-vector contact while the chlorfenapyr controlled pyrethroid-resistant mosquitoes. The complementary action of these unrelated insecticides demonstrates that the mixture has potential for preventing malaria transmission in areas compromised by the spread of pyrethroid resistance.
Malaria prevention in schoolchildren: a cluster-randomised trial in schools in Mali.
LSHTM Investigators: Sian Clarke, Saba Rouhani, Rebecca Jones
& Simon Brooker.
External Investigators/Collaborators: Natalie Roschnik, Seybou
Diarra & Bamadio Modibo (Save the Children, Mali); Moussa Sacko,
Renion Saye & Diahara Traore (Ministry of Health, Mali); Matthew
Jukes (Room to Read, UK); Josselin Thuillez (Centre d’economie de
la Sorbonne, France).
Funding: Save the Children; The Wellcome Trust.
School-aged children are rarely targeted by malaria control, yet the prevalence of malaria infection in this age group often exceeds that seen in younger children and the consequences for health and school performance have yet to be fully investigated.
This cluster-randomised trial examined the impact of a teacher-led malaria control programme in schools in Mali which combined participatory education activities to promote the use of insecticide treated nets, with a single annual antimalarial treatment to clear malaria parasites from the blood at the end of the transmission season. The trial was conducted in 80 schools, with 40 schools randomised to receive the intervention.
The prevalence of malaria infection and anaemia in
to control schools. These differences were sustained until
Future work in Mali will examine the effect of malaria control on health and child development in pre-school children, with a focus on effects on cognitive foundation skills for early literacy.
Teachers administering an annual treatment to clear malaria infections in schoolchildren in Mali.
ChemopreventionWe are currently seeking to generate knowledge on the health impact, cost, feasibility and acceptability of chemoprevention and screening and treatment strategies in a number of target populations including children, school children and pregnant women.

56 Malaria prevention Malaria prevention 57
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Mosquito nets treated with a mixture of the insecticides chlorfenapyr and alphacypermethrin control pyrethroid resistant Anopheles gambiae and Culex quinquefasciatus mosquitoes in West Africa.
LSHTM Investigators
Rowland.
External Investigators/Collaborators: Andreas Kudom, Pelagie
Boko & Abibathou Odjo (Centre de Recherche Entomologique
Consortium, UK).
Funding:
The effectiveness of insecticide treated nets is under
selection of pyrethroid resistance in Anopheles gambiae mosquitoes.
To maintain progress against malaria it is necessary to identify alternative residual insecticides for mosquito nets. Mixtures of pyrethroid and insecticides with novel mode of action provide scope for both improved control and management of resistance through concurrent exposure to unrelated insecticides.
The pyrrole chlorfenapyr and the pyrethroid alphacypermethrin were tested individually and as a mixture on mosquito nets in an experimental hut trial in southern Benin against pyrethroid resistant Anopheles
gambiae and Culex quinquefasciatus mosquitoes. The nets were deliberately holed to simulate the effect of wear and tear.
The nets treated with the mixture of chlorfenapyr 200mg/m2 and alphacypermethrin 25mg/m2 killed a proportion of Anopheles gambiae (77%, 95%CI:
nets treated with the mixture reduced mosquito biting and blood-feeding rates to the same level as the alphacypermethrin treated net, whereas the chlorfenapyr
mortality and blood feeding inhibition between treatments was observed among Culex quinquefasciatus to that seen among Anopheles gambiae, although the effects were
applied at 100mg/m2 had an effect similar to the mixture with chlorfenapyr at 200mg/m2.
The effectiveness of Iinsecticide treated nets against pyrethroid resistant mosquitoes was restored by the mixture: the alphacypermethrin component reduced human-vector contact while the chlorfenapyr controlled pyrethroid-resistant mosquitoes. The complementary action of these unrelated insecticides demonstrates that the mixture has potential for preventing malaria transmission in areas compromised by the spread of pyrethroid resistance.
Malaria prevention in schoolchildren: a cluster-randomised trial in schools in Mali.
LSHTM Investigators: Sian Clarke, Saba Rouhani, Rebecca Jones
& Simon Brooker.
External Investigators/Collaborators: Natalie Roschnik, Seybou
Diarra & Bamadio Modibo (Save the Children, Mali); Moussa Sacko,
Renion Saye & Diahara Traore (Ministry of Health, Mali); Matthew
Jukes (Room to Read, UK); Josselin Thuillez (Centre d’economie de
la Sorbonne, France).
Funding: Save the Children; The Wellcome Trust.
School-aged children are rarely targeted by malaria control, yet the prevalence of malaria infection in this age group often exceeds that seen in younger children and the consequences for health and school performance have yet to be fully investigated.
This cluster-randomised trial examined the impact of a teacher-led malaria control programme in schools in Mali which combined participatory education activities to promote the use of insecticide treated nets, with a single annual antimalarial treatment to clear malaria parasites from the blood at the end of the transmission season. The trial was conducted in 80 schools, with 40 schools randomised to receive the intervention.
The prevalence of malaria infection and anaemia in
to control schools. These differences were sustained until
Future work in Mali will examine the effect of malaria control on health and child development in pre-school children, with a focus on effects on cognitive foundation skills for early literacy.
Teachers administering an annual treatment to clear malaria infections in schoolchildren in Mali.
ChemopreventionWe are currently seeking to generate knowledge on the health impact, cost, feasibility and acceptability of chemoprevention and screening and treatment strategies in a number of target populations including children, school children and pregnant women.

58 Malaria prevention Malaria prevention 59
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Impact of intermittent screening and treatment for malaria among school children in Kenya.
LSHTM Investigators: Simon Brooker, Katherine Halliday, Elizabeth
Allen, Caroline Jones, Thomas Drake, Lindsay Mangham & Kara
Hanson.
External Investigators/Collaborators: Matthew Jukes (Harvard
Research Institute, Kenya); Elizabeth Turner (Duke University, USA);
Hellen Inyega (University of Nairobi, Kenya); Kiambo Njagi (Ministry
of Public Health and Sanitation, Kenya); Margaret Dubeck (College
of Charleston, USA).
Funding: International Initiative for Impact Evaluation; Development
Impact Evaluation Initiative of the World Bank, The Wellcome Trust &
Partnership for Child Development.
School-based malaria control is recognized as an important potential component of integrated school-health packages.
on the health and education of school children in a low-moderate transmission setting in south coast, Kenya.
The intervention, screening once a term by health
treatment, for those positive for malaria parasiteamia, with artemether-lumefantrine, was delivered to children in 51 randomly selected primary schools with another 50 serving as control schools.
During the 2-year study period, 17.5% of children screened were RDT-positive. However, no difference was observed in the prevalence of anaemia at 12 or 24 months between children in intervention and control groups, nor was there any effect on malaria parasitaemia
based IST in this context to be relatively expensive at US$6.61 per child screened. While a qualitative stakeholder analysis indicated school-based IST to be widely acceptable, consideration of the various roles of teachers and health workers and use of simpler regimen anti-malarial drugs is important. This evaluation showed that IST is not an effective intervention in low-moderate malaria transmission settings. However, school screenings using RDTs could provide an operationally
for targeted community control.
‘School-based treatment with artemisinin-based combination therapy to reduce transmission’ (START): evaluation of the community impact of intermittent preventive treatment for malaria in Ugandan children: a cluster randomised trial.
LSHTM Investigators: Sarah Staedke, Chris Drakeley, Chi Eziefula
& Clare Chandler.
External Investigators/Collaborators:
(University of California, UK); Steve Lindsay (Durham University,
Funding:
schoolchildren for malaria on malaria transmission at the community level in Jinja, Uganda.
school and the 100 nearest households, will be included in the trial; half will be randomised to the IPT intervention,
will be administered to schoolchildren monthly during one school year.
The evaluation will include:
after the intervention
end of the school year
implementation of the intervention;
In addition, we will conduct a qualitative study concurrently with the main trial. The primary outcome of the trial is the prevalence of parasitaemia in community
The baseline surveys will begin in February 2014 and the intervention will be delivered during the 2014 school year.
Extending the age range for seasonal malaria chemoprevention (SMC): effectiveness of SMC in children under 10 years of age delivered through the district health service in Senegal.
LSHTM Investigators: Badara Cisse, Catherine Pitt, Matthew Cairns, Colin Sutherland, Brian
External Investigators/Collaborators: El Hadj Ba, Jean-François Trape, Cheikh Sokhna
Funding:
Children under 5 years of age living in areas of seasonal transmission in the Sahel are recommended to receive seasonal malaria chemoprevention
transmission season, to prevent malaria. The purpose of this study was to evaluate the feasibility of delivering SMC
on a large scale by district health staff using community health workers, its safety and effectiveness, in Senegal. SMC was introduced in three districts
system was established to record all deaths and all malaria cases diagnosed at health facilities, and a pharmacovigilance system was established to detect adverse drug reactions. Coverage of SMC was independently assessed
documented courses of SMC had been administered by health workers. High coverage of three courses of treatment was achieved, and no serious adverse events attributable to the intervention were detected, despite a high
effectiveness of SMC in reducing malaria incidence in treated children, with a random effect to account for variation in incidence between health posts. To determine whether SMC was able to reduce malaria transmission, incidence of malaria in age groups too old to receive SMC, was compared between health posts in which SMC was delivered to children, and health posts without SMC, using random-effects Poisson regression.
Where SMC was delivered, the number of malaria cases in children under
age groups was reduced in areas where SMC was delivered to children, by 29%
SMC is recommended for children under <5yrs of age, but in some areas the age distribution of disease burden may justify extending this age limit, as has been done in Senegal. SMC with Sulfadoxine-Pyrimethamine plus
older children. Pharmacovigilance should be maintained in areas where SMC is implemented, and provision for strengthening national pharmacovigilance systems should therefore be included in plans for SMC implementation. When provided for a wider age range with high coverage, SMC may have an effect in reducing malaria transmission, and our results were consistent with such an effect.

58 Malaria prevention Malaria prevention 59
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Impact of intermittent screening and treatment for malaria among school children in Kenya.
LSHTM Investigators: Simon Brooker, Katherine Halliday, Elizabeth
Allen, Caroline Jones, Thomas Drake, Lindsay Mangham & Kara
Hanson.
External Investigators/Collaborators: Matthew Jukes (Harvard
Research Institute, Kenya); Elizabeth Turner (Duke University, USA);
Hellen Inyega (University of Nairobi, Kenya); Kiambo Njagi (Ministry
of Public Health and Sanitation, Kenya); Margaret Dubeck (College
of Charleston, USA).
Funding: International Initiative for Impact Evaluation; Development
Impact Evaluation Initiative of the World Bank, The Wellcome Trust &
Partnership for Child Development.
School-based malaria control is recognized as an important potential component of integrated school-health packages.
on the health and education of school children in a low-moderate transmission setting in south coast, Kenya.
The intervention, screening once a term by health
treatment, for those positive for malaria parasiteamia, with artemether-lumefantrine, was delivered to children in 51 randomly selected primary schools with another 50 serving as control schools.
During the 2-year study period, 17.5% of children screened were RDT-positive. However, no difference was observed in the prevalence of anaemia at 12 or 24 months between children in intervention and control groups, nor was there any effect on malaria parasitaemia
based IST in this context to be relatively expensive at US$6.61 per child screened. While a qualitative stakeholder analysis indicated school-based IST to be widely acceptable, consideration of the various roles of teachers and health workers and use of simpler regimen anti-malarial drugs is important. This evaluation showed that IST is not an effective intervention in low-moderate malaria transmission settings. However, school screenings using RDTs could provide an operationally
for targeted community control.
‘School-based treatment with artemisinin-based combination therapy to reduce transmission’ (START): evaluation of the community impact of intermittent preventive treatment for malaria in Ugandan children: a cluster randomised trial.
LSHTM Investigators: Sarah Staedke, Chris Drakeley, Chi Eziefula
& Clare Chandler.
External Investigators/Collaborators:
(University of California, UK); Steve Lindsay (Durham University,
Funding:
schoolchildren for malaria on malaria transmission at the community level in Jinja, Uganda.
school and the 100 nearest households, will be included in the trial; half will be randomised to the IPT intervention,
will be administered to schoolchildren monthly during one school year.
The evaluation will include:
after the intervention
end of the school year
implementation of the intervention;
In addition, we will conduct a qualitative study concurrently with the main trial. The primary outcome of the trial is the prevalence of parasitaemia in community
The baseline surveys will begin in February 2014 and the intervention will be delivered during the 2014 school year.
Extending the age range for seasonal malaria chemoprevention (SMC): effectiveness of SMC in children under 10 years of age delivered through the district health service in Senegal.
LSHTM Investigators: Badara Cisse, Catherine Pitt, Matthew Cairns, Colin Sutherland, Brian
External Investigators/Collaborators: El Hadj Ba, Jean-François Trape, Cheikh Sokhna
Funding:
Children under 5 years of age living in areas of seasonal transmission in the Sahel are recommended to receive seasonal malaria chemoprevention
transmission season, to prevent malaria. The purpose of this study was to evaluate the feasibility of delivering SMC
on a large scale by district health staff using community health workers, its safety and effectiveness, in Senegal. SMC was introduced in three districts
system was established to record all deaths and all malaria cases diagnosed at health facilities, and a pharmacovigilance system was established to detect adverse drug reactions. Coverage of SMC was independently assessed
documented courses of SMC had been administered by health workers. High coverage of three courses of treatment was achieved, and no serious adverse events attributable to the intervention were detected, despite a high
effectiveness of SMC in reducing malaria incidence in treated children, with a random effect to account for variation in incidence between health posts. To determine whether SMC was able to reduce malaria transmission, incidence of malaria in age groups too old to receive SMC, was compared between health posts in which SMC was delivered to children, and health posts without SMC, using random-effects Poisson regression.
Where SMC was delivered, the number of malaria cases in children under
age groups was reduced in areas where SMC was delivered to children, by 29%
SMC is recommended for children under <5yrs of age, but in some areas the age distribution of disease burden may justify extending this age limit, as has been done in Senegal. SMC with Sulfadoxine-Pyrimethamine plus
older children. Pharmacovigilance should be maintained in areas where SMC is implemented, and provision for strengthening national pharmacovigilance systems should therefore be included in plans for SMC implementation. When provided for a wider age range with high coverage, SMC may have an effect in reducing malaria transmission, and our results were consistent with such an effect.

60 Malaria prevention Malaria prevention 61
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Maximising the impact of chemoprevention on the malaria burden in children in areas of seasonal transmission.
LSHTM Investigators: Matthew Cairns.
External Investigators/Collaborators:
College London); Harry Tagbor (Kwame Nkrumah University of
Funding: The Medical Research Council.
a short rainy season, monthly courses of antimalarial drugs can prevent malaria in children very effectively.
This approach, called seasonal malaria
where malaria is transmitted for a larger part of the year. However, the impact in such areas is not well understood.
existing treatment regimens for long-acting artemisinin-
further malaria infections for several weeks. This may
transmission because repeated malaria attacks are likely to occur close together in time.
trial in Kumasi, Ghana, reanalysis of trial data and mathematical modelling
quantifying the burden of repeated malaria attacks and the heterogeneity in malaria risk in different epidemiological settings
to be advantageous, estimate the population at risk and the public health impact.
The costs of delivering seasonal malaria chemoprevention to children under ten at scale in Central Senegal.
LSHTM Investigators: Catherine Pitt, Badara Cisse & Paul Milligan.
External Investigators/Collaborators: Mouhamed N’Diaye &
(Institut de Recherche pour le Developpement, Dakar, Senegal);
Lesong Conteh (Imperial College London, UK).
Funding:
Preliminary results from this study were presented
contributed to its policy recommendation in March 2012 that SMC be given to children in areas of seasonal
costs of delivering SMC in a population of approximately
175,000 children aged 3 to 120 months in 45 health posts across four districts of central Senegal in 2010.
travelled door-to-door in pairs to administer sulphadoxine-pyramethamine and amodiaquine tablets over the course of several days in each of the three main months of the malaria season. We found that the costs were lower than in most previous studies of SMC, which can be attributed in part to economies of scale, as this was a much larger study than any previously conducted, as well as to the Ministry of Health’s leading role in implementation and the economies of scope achieved in extending the usual age range of SMC from children under 5 to children under 10. The SMC tablets themselves and the incentive payments
informed implementation of SMC in Senegal and several
A trial of intermittent screening and treatment as an alternative to intermittent preventive treatment with sulfadoxine-pyrimethamine for the control of malaria in pregnancy.
LSHTM Investigators: Matthew Cairns, Daniel Chandramohan,
External Investigators/Collaborators: Sheick Coulibaly
(University of Ouagadougou, Burkina Faso); John Williams
(University of Bamako, Mali); Kalifa Bojang (Medical Research
of Copenhagen, Denmark); Feiko ter Kuile (Liverpool School of
Tropical Medicine, UK).
Funding: The European & Developing Countries Clinical Trials
Partnership.
determine whether intermittent screening and treatment
infection of the placenta in pregnant women who slept under an insecticide treated bed net.
IST involved intermittent screening using a rapid diagnostic test at scheduled antenatal clinic visits and treatment of those who tested positive for maalaria with arthemether lumefantrine. Women in the standard SP-IPTp arm received two or three courses of SP in the second and third trimester. 5354 women were randomised into one of the two study arms . The prevalence of LBW was 15.1% in women in the IPT-SP group and 15.6% among those in the IST group. The mean haemoglobin concentration at the last clinic attendance before delivery was 10.97g/dL (SD 1.3g/
to IPTp-SP in preventing LBW and maternal anaemia according to criteria established prior to the trial. Thus IST is a potential alternative approach to control of malaria in pregnancy which may be especially valuable in areas where Plasmodium falciparum is highly resistant to SP.
Malaria knowledge and utilisation of chemoprophylaxis in the UK population and in UK passengers departing to malaria-endemic areas.LSHTM Investigators: Ron Behrens & Neal Alexander.
Funding: Sigma Tau Pharmaceutical.
The burden of imported malaria is predominantly
chemoprophylaxis is recognised as the most important factor. Understanding the reasons for failure was the basis of this study to explore whether knowledge and risk perception.
Two face-to-face questionnaire surveys were conducted; a survey of individuals representative of the UK population and a departure lounge survey of passengers departing to malarious regions.
had previously travelled to a malarious area. Five-hundred departing passengers were interviewed, of which 56% VFR’s and 42% were travelling to West
who had previously travelled or were travelling (63.8
similar in individuals who had and had not sought pre-travel advice and travellers using and not using chemoprophylaxis. Despite similar high knowledge
of malaria in the three groups, chemoprophylaxis
Malaria knowledge, perceived threat, travel experience, and quality of pre-travel advice appear unrelated to the use of chemoprophylaxis in passengers. Reducing malaria in VFR travellers will require strategies other than improving malaria knowledge and enhancing malaria risk awareness.
60 Malaria prevention Malaria prevention 61
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Maximising the impact of chemoprevention on the malaria burden in children in areas of seasonal transmission.
LSHTM Investigators: Matthew Cairns.
External Investigators/Collaborators:
College London); Harry Tagbor (Kwame Nkrumah University of
Funding: The Medical Research Council.
a short rainy season, monthly courses of antimalarial drugs can prevent malaria in children very effectively.
This approach, called seasonal malaria
where malaria is transmitted for a larger part of the year. However, the impact in such areas is not well understood.
existing treatment regimens for long-acting artemisinin-
further malaria infections for several weeks. This may
transmission because repeated malaria attacks are likely to occur close together in time.
trial in Kumasi, Ghana, reanalysis of trial data and mathematical modelling
quantifying the burden of repeated malaria attacks and the heterogeneity in malaria risk in different epidemiological settings
to be advantageous, estimate the population at risk and the public health impact.
The costs of delivering seasonal malaria chemoprevention to children under ten at scale in Central Senegal.
LSHTM Investigators: Catherine Pitt, Badara Cisse & Paul Milligan.
External Investigators/Collaborators: Mouhamed N’Diaye &
(Institut de Recherche pour le Developpement, Dakar, Senegal);
Lesong Conteh (Imperial College London, UK).
Funding:
Preliminary results from this study were presented
contributed to its policy recommendation in March 2012 that SMC be given to children in areas of seasonal
costs of delivering SMC in a population of approximately
175,000 children aged 3 to 120 months in 45 health posts across four districts of central Senegal in 2010.
travelled door-to-door in pairs to administer sulphadoxine-pyramethamine and amodiaquine tablets over the course of several days in each of the three main months of the malaria season. We found that the costs were lower than in most previous studies of SMC, which can be attributed in part to economies of scale, as this was a much larger study than any previously conducted, as well as to the Ministry of Health’s leading role in implementation and the economies of scope achieved in extending the usual age range of SMC from children under 5 to children under 10. The SMC tablets themselves and the incentive payments
informed implementation of SMC in Senegal and several
A trial of intermittent screening and treatment as an alternative to intermittent preventive treatment with sulfadoxine-pyrimethamine for the control of malaria in pregnancy.
LSHTM Investigators: Matthew Cairns, Daniel Chandramohan,
External Investigators/Collaborators: Sheick Coulibaly
(University of Ouagadougou, Burkina Faso); John Williams
(University of Bamako, Mali); Kalifa Bojang (Medical Research
of Copenhagen, Denmark); Feiko ter Kuile (Liverpool School of
Tropical Medicine, UK).
Funding: The European & Developing Countries Clinical Trials
Partnership.
determine whether intermittent screening and treatment
infection of the placenta in pregnant women who slept under an insecticide treated bed net.
IST involved intermittent screening using a rapid diagnostic test at scheduled antenatal clinic visits and treatment of those who tested positive for maalaria with arthemether lumefantrine. Women in the standard SP-IPTp arm received two or three courses of SP in the second and third trimester. 5354 women were randomised into one of the two study arms . The prevalence of LBW was 15.1% in women in the IPT-SP group and 15.6% among those in the IST group. The mean haemoglobin concentration at the last clinic attendance before delivery was 10.97g/dL (SD 1.3g/
to IPTp-SP in preventing LBW and maternal anaemia according to criteria established prior to the trial. Thus IST is a potential alternative approach to control of malaria in pregnancy which may be especially valuable in areas where Plasmodium falciparum is highly resistant to SP.
Malaria knowledge and utilisation of chemoprophylaxis in the UK population and in UK passengers departing to malaria-endemic areas.LSHTM Investigators: Ron Behrens & Neal Alexander.
Funding: Sigma Tau Pharmaceutical.
The burden of imported malaria is predominantly
chemoprophylaxis is recognised as the most important factor. Understanding the reasons for failure was the basis of this study to explore whether knowledge and risk perception.
Two face-to-face questionnaire surveys were conducted; a survey of individuals representative of the UK population and a departure lounge survey of passengers departing to malarious regions.
had previously travelled to a malarious area. Five-hundred departing passengers were interviewed, of which 56% VFR’s and 42% were travelling to West
who had previously travelled or were travelling (63.8
similar in individuals who had and had not sought pre-travel advice and travellers using and not using chemoprophylaxis. Despite similar high knowledge
of malaria in the three groups, chemoprophylaxis
Malaria knowledge, perceived threat, travel experience, and quality of pre-travel advice appear unrelated to the use of chemoprophylaxis in passengers. Reducing malaria in VFR travellers will require strategies other than improving malaria knowledge and enhancing malaria risk awareness.

62 Malaria prevention Malaria prevention 63
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Using routine data to assess and improve the delivery of interventions to control malaria in pregnancy.
LSHTM Investigators: Jayne Webster, Jane Bruce & Lucy Paintain.
External Investigators/Collaborators: Jenny Hill (Liverpool School
of Tropical Medicine, UK); Kassoum Kayentao, Sory Diawara &
Samba Diarra (Malaria Research and Training Centre, Mali); Fady
Toure (Le Programme National de Lutte contre le Paludisme, Mali);
Balla Diarra (Baraoueli District team), Eric Onyango, Meghna
for Disease Control and Prevention, Kenya); Titus Kwambai & Tom
Arunga (Kisumu East Subcounty Health Management Team, Kenya)
& Dickens Onyango (County epidemiologist).
Funding:
Malaria in Pregnancy Consortium.
The aim of the study is to develop and evaluate an enhanced district and facility level data monitoring system for the ongoing evaluation of the delivery of malaria in pregnancy interventions.
Current data collection practices relating to
treatment, insecticide treated nets and malaria case management in pregnant women were assessed.
was collected and collated at the facility level and at the district level. In-depth interviews were used to determine the drivers of effective routine data collection at the facility and district levels.
routine data collection/monitoring tools integrated into the
district level. Data completeness and accuracy is currently assessed through quarterly data auditing and compared with completeness and accuracy of reporting on priority indicators at baseline.
Sustainability of the use of the enhanced monitoring as developed will depend to an extent upon its perceived utility and acceptability by those involved in its use. This will be assessed through in-depth interviews with health providers at the facility and district levels.
the development of routine monitoring modules for a toolkit for assessing coverage of malaria in pregnancy interventions, and a decision tool which will drive which
Field testing baseline household survey data collection using tablet PCs, Khunti district, Jharkhand, India.
Identifying and quantifying the major barriers to the scale-up and use of interventions for the control of malaria in pregnancy.
LSHTM Investigators: Jayne Webster & Jane Bruce.
External Investigators/Collaborators: Jenny Hill & Feiko ter Kuile
(Liverpool School of Tropical Medicine, UK); Kassoum Kayentao,
Sory Diawara & Samba Diarra (Malaria Research and Training
Centre, Mali); Stephanie Dellicour, Meghna Desai & Peter Ouma
Prevention, Kenya).
Funding:
Pregnancy Consortium.
In order to support global efforts to scale-up malaria control interventions greater attention must be given to implementation research in order to understand the obstacles to progress at the level of local decision makers.In this study we have provided evidence on the barriers to effective access, delivery and use of intermittent prevent treatment and long lasting insecticide-treated nets in one district of each of Mali and Kenya. Findings have highlighted blockages in delivery of preventative interventions, methodological anomalies in the way in which we are currently assessing coverage of interventions, and the strengths and weaknesses of survey techniques in providing information for programme
delivery and use of case management of malaria in pregnancy is ongoing and will be completed in 2014.
SToP MiP Indonesia: implementation research and cost effectiveness studies.
LSHTM Investigators: Jayne Webster & Jane Bruce.
External Investigators/Collaborators: Feiko ter Kuile, Rukhsana
Ahmed & Jenny Hill, (Liverpool School of Tropical Medicine, UK);
Din Syafruddin, Puji Bud Asih & Rintis Noviyanti (Eijkman Institute
for Molecular Biology, Indonesia) & Jeanne Poespoprodjo (Timika
Research Facility, Indonesia).
Funding:
Council; The Department for International Development; The
Wellcome Trust via Liverpool School of Tropical Medicine.
This research is a sub-study running alongside a trial
effective than the current strategy of single screening
by long lasting insecticide treated nets in areas with relatively low Plasmodium falciparum and Plasmodium vivax transmission in Indonesia. The current status of the SSTp-DHP programme in Papua and Sumba will be evaluated using quantitative and qualitative techniques. The feasibility, acceptability and cost effectiveness of the alternate strategies will then be assessed for the context
acceptability of changing from a test and treat strategy to one of intermittent preventive treatment.

62 Malaria prevention Malaria prevention 63
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Using routine data to assess and improve the delivery of interventions to control malaria in pregnancy.
LSHTM Investigators: Jayne Webster, Jane Bruce & Lucy Paintain.
External Investigators/Collaborators: Jenny Hill (Liverpool School
of Tropical Medicine, UK); Kassoum Kayentao, Sory Diawara &
Samba Diarra (Malaria Research and Training Centre, Mali); Fady
Toure (Le Programme National de Lutte contre le Paludisme, Mali);
Balla Diarra (Baraoueli District team), Eric Onyango, Meghna
for Disease Control and Prevention, Kenya); Titus Kwambai & Tom
Arunga (Kisumu East Subcounty Health Management Team, Kenya)
& Dickens Onyango (County epidemiologist).
Funding:
Malaria in Pregnancy Consortium.
The aim of the study is to develop and evaluate an enhanced district and facility level data monitoring system for the ongoing evaluation of the delivery of malaria in pregnancy interventions.
Current data collection practices relating to
treatment, insecticide treated nets and malaria case management in pregnant women were assessed.
was collected and collated at the facility level and at the district level. In-depth interviews were used to determine the drivers of effective routine data collection at the facility and district levels.
routine data collection/monitoring tools integrated into the
district level. Data completeness and accuracy is currently assessed through quarterly data auditing and compared with completeness and accuracy of reporting on priority indicators at baseline.
Sustainability of the use of the enhanced monitoring as developed will depend to an extent upon its perceived utility and acceptability by those involved in its use. This will be assessed through in-depth interviews with health providers at the facility and district levels.
the development of routine monitoring modules for a toolkit for assessing coverage of malaria in pregnancy interventions, and a decision tool which will drive which
Field testing baseline household survey data collection using tablet PCs, Khunti district, Jharkhand, India.
Identifying and quantifying the major barriers to the scale-up and use of interventions for the control of malaria in pregnancy.
LSHTM Investigators: Jayne Webster & Jane Bruce.
External Investigators/Collaborators: Jenny Hill & Feiko ter Kuile
(Liverpool School of Tropical Medicine, UK); Kassoum Kayentao,
Sory Diawara & Samba Diarra (Malaria Research and Training
Centre, Mali); Stephanie Dellicour, Meghna Desai & Peter Ouma
Prevention, Kenya).
Funding:
Pregnancy Consortium.
In order to support global efforts to scale-up malaria control interventions greater attention must be given to implementation research in order to understand the obstacles to progress at the level of local decision makers.In this study we have provided evidence on the barriers to effective access, delivery and use of intermittent prevent treatment and long lasting insecticide-treated nets in one district of each of Mali and Kenya. Findings have highlighted blockages in delivery of preventative interventions, methodological anomalies in the way in which we are currently assessing coverage of interventions, and the strengths and weaknesses of survey techniques in providing information for programme
delivery and use of case management of malaria in pregnancy is ongoing and will be completed in 2014.
SToP MiP Indonesia: implementation research and cost effectiveness studies.
LSHTM Investigators: Jayne Webster & Jane Bruce.
External Investigators/Collaborators: Feiko ter Kuile, Rukhsana
Ahmed & Jenny Hill, (Liverpool School of Tropical Medicine, UK);
Din Syafruddin, Puji Bud Asih & Rintis Noviyanti (Eijkman Institute
for Molecular Biology, Indonesia) & Jeanne Poespoprodjo (Timika
Research Facility, Indonesia).
Funding:
Council; The Department for International Development; The
Wellcome Trust via Liverpool School of Tropical Medicine.
This research is a sub-study running alongside a trial
effective than the current strategy of single screening
by long lasting insecticide treated nets in areas with relatively low Plasmodium falciparum and Plasmodium vivax transmission in Indonesia. The current status of the SSTp-DHP programme in Papua and Sumba will be evaluated using quantitative and qualitative techniques. The feasibility, acceptability and cost effectiveness of the alternate strategies will then be assessed for the context
acceptability of changing from a test and treat strategy to one of intermittent preventive treatment.

64 Malaria prevention Malaria prevention 65
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Effective and safe interventions for prevention of malaria in pregnancy in India: an assessment of burden of malaria in pregnancy, implementability of a screening strategy and barriers to scaling up interventions.
LSHTM Investigators: Daniel Chandramohan, Jayne Webster, Irene
External Investigators/Collaborators:
Mishra, Anupkumar Anvikar & B Shahi (National Malaria Research
Institute, India); Feiko ter Kuile (Liverpool School of Tropical
Medicine, UK).
Funding:
Pregnancy Consortium.
The current strategy for control of malaria in pregnancy
they report any sign or symptom suggestive for malaria.The current status of the SSTp-DHP programme in
Papua and Sumba will be evaluated using quantitative and qualitative techniques. The feasibility, acceptability and cost effectiveness of the alternate strategies will then be assessed for the context of both islands.
This strategy is probably inadequate to reduce the
burden of MiP because a substantial proportion of MiP cases remain asymptomatic. The aim of this study is to
component of the study is a cluster randomised controlled trial with two arms. Women in the IST arm are screened
arm are tested for malaria only if they have any sign or symptom of malaria. The primary outcome is placental
women have been enrolled by March 2014. The trIal is expected tobe completed by June 2015.
In a second component of the study, RDT based IST was implemented at pilot scale in a sub-district in
evaluate the implementability of IST including: a pre-post intervention household survey, health facility survey, focus group discussions, in-depth interviews and a costing study.
Economic analysis and evaluations for the Malaria in Pregnancy Consortium.
LSHTM Investigators: Kara Hanson, Silke Fernandes & Jayne
Webster.
External Investigators/Collaborators: Elisa Sicuri (Barcelona
Patrick Walker (Imperial College London, UK); Feiko ter Kuile &
Jenny Hill (Liverpool School of Tropical Medicine, UK).
Funding:
Pregnancy Consortium.
Sitting within the Public Health Impact activity of the
the economics contributions are:
prevention and case management interventions
interventions
Fieldwork was conducted over the course of the past 4 years in 11 countries located in 4 continents and is anticipated to end in early 2015. Data were collected using a variety of methods, including cross-sectional household and facility surveys, exit surveys
building on a recent meta-analysis of clinical trials found
cost-effective compared with two doses of SP. In 2014-15 we will focus our efforts on further data analysis, building cost effectiveness models of Intermittent Screening and
with intermittent preventive treatment and a model of the economic burden of MiP. This analysis will support the development of a map identifying those settings where ISTp may be a more appropriate strategy for preventing the consequences of malaria in pregnancy.
the age of 18 months. Twelve months after vaccination, -
cated and severe malaria was approximately 50% in chil-dren vaccinated when aged 5-17 months but less when it was given to infants aged 6-12 weeks at the same time as routine Expanded Program on Immunization vaccines. Further analysis undertaken 18 months after vaccination showed that protection had been sustained in the older group of children but had waned substantially in infants.
all centres regardless of the level of malaria transmission.
2014 when the majority of trial subjects will have been followed for 3-4 years. It is expected that a decision on registration of the vaccine will be made in 2015 and, if this
guidelines on its use shortly afterwards.
vaccine (257049)(RTS,S/AS01) against malaria disease caused by Plasmodium falciparum in infants and children in Africa.
LSHTM Investigators: Daniel Chandramohan, Chris Drakeley, Brian
External Investigators/Collaborators: The RTS,S Clinical Trials
Partnership.
Funding:
advanced malaria vaccine and is currently being evalu-ated in a phase three trial being conducted in 11 centres
-cruited and randomised to receive three doses of RTS,S/
regimen against plasmodium falciparum ma-laria infection in Senegalese adults.
LSHTM Investigators: Badara Cisse.
External Investigators/Collaborators:
-
nostou, Nick Edwards, Babatunde Imoukhuede, Rachel Roberts,
Funding: The European and Developing Countries Clinical Trials
Extensive pre-clinical data indicate that protective im-munity to the liver-stage of malaria can be conferred by
been recently demonstrated in Kenya and it is important -
tween 2012 & 2013, we ran a phase IIb, controlled, single blinded, randomised vaccine trial in Guediawaye. The main objectives were to assess the safety, immunogenic-
We randomly allocated 120 healthy male adult vol-unteers to vaccination with either the vaccine candidate, or verorab as control. Immunogenicity was measured by
--
mia and conducted intensive PCR monitoring to identify new Plasmodium falciparum infections over an eight week follow-up period. Vaccine related adverse events were mild to moderate in intensity with 1 serious adverse event in the control group not related to the intervention.
-
days later as measured by Elispot. Peak immunogenicity was shown 7 days after the boost and was high at a geo-metric mean of 1266 Spots per million PBMCs (95% CI
dose vectored vaccination approach targeting the liver-stage of malaria shows promise as a candidate malaria vaccine.
Vaccine developmentSeveral of our staff have participated in the design, execution and evaluation of RTS,S candidate vaccine trials as well as a trial of a prime boost vaccine candidate in Senegal.

64 Malaria prevention Malaria prevention 65
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Effective and safe interventions for prevention of malaria in pregnancy in India: an assessment of burden of malaria in pregnancy, implementability of a screening strategy and barriers to scaling up interventions.
LSHTM Investigators: Daniel Chandramohan, Jayne Webster, Irene
External Investigators/Collaborators:
Mishra, Anupkumar Anvikar & B Shahi (National Malaria Research
Institute, India); Feiko ter Kuile (Liverpool School of Tropical
Medicine, UK).
Funding:
Pregnancy Consortium.
The current strategy for control of malaria in pregnancy
they report any sign or symptom suggestive for malaria.The current status of the SSTp-DHP programme in
Papua and Sumba will be evaluated using quantitative and qualitative techniques. The feasibility, acceptability and cost effectiveness of the alternate strategies will then be assessed for the context of both islands.
This strategy is probably inadequate to reduce the
burden of MiP because a substantial proportion of MiP cases remain asymptomatic. The aim of this study is to
component of the study is a cluster randomised controlled trial with two arms. Women in the IST arm are screened
arm are tested for malaria only if they have any sign or symptom of malaria. The primary outcome is placental
women have been enrolled by March 2014. The trIal is expected tobe completed by June 2015.
In a second component of the study, RDT based IST was implemented at pilot scale in a sub-district in
evaluate the implementability of IST including: a pre-post intervention household survey, health facility survey, focus group discussions, in-depth interviews and a costing study.
Economic analysis and evaluations for the Malaria in Pregnancy Consortium.
LSHTM Investigators: Kara Hanson, Silke Fernandes & Jayne
Webster.
External Investigators/Collaborators: Elisa Sicuri (Barcelona
Patrick Walker (Imperial College London, UK); Feiko ter Kuile &
Jenny Hill (Liverpool School of Tropical Medicine, UK).
Funding:
Pregnancy Consortium.
Sitting within the Public Health Impact activity of the
the economics contributions are:
prevention and case management interventions
interventions
Fieldwork was conducted over the course of the past 4 years in 11 countries located in 4 continents and is anticipated to end in early 2015. Data were collected using a variety of methods, including cross-sectional household and facility surveys, exit surveys
building on a recent meta-analysis of clinical trials found
cost-effective compared with two doses of SP. In 2014-15 we will focus our efforts on further data analysis, building cost effectiveness models of Intermittent Screening and
with intermittent preventive treatment and a model of the economic burden of MiP. This analysis will support the development of a map identifying those settings where ISTp may be a more appropriate strategy for preventing the consequences of malaria in pregnancy.
the age of 18 months. Twelve months after vaccination, -
cated and severe malaria was approximately 50% in chil-dren vaccinated when aged 5-17 months but less when it was given to infants aged 6-12 weeks at the same time as routine Expanded Program on Immunization vaccines. Further analysis undertaken 18 months after vaccination showed that protection had been sustained in the older group of children but had waned substantially in infants.
all centres regardless of the level of malaria transmission.
2014 when the majority of trial subjects will have been followed for 3-4 years. It is expected that a decision on registration of the vaccine will be made in 2015 and, if this
guidelines on its use shortly afterwards.
vaccine (257049)(RTS,S/AS01) against malaria disease caused by Plasmodium falciparum in infants and children in Africa.
LSHTM Investigators: Daniel Chandramohan, Chris Drakeley, Brian
External Investigators/Collaborators: The RTS,S Clinical Trials
Partnership.
Funding:
advanced malaria vaccine and is currently being evalu-ated in a phase three trial being conducted in 11 centres
-cruited and randomised to receive three doses of RTS,S/
regimen against plasmodium falciparum ma-laria infection in Senegalese adults.
LSHTM Investigators: Badara Cisse.
External Investigators/Collaborators:
-
nostou, Nick Edwards, Babatunde Imoukhuede, Rachel Roberts,
Funding: The European and Developing Countries Clinical Trials
Extensive pre-clinical data indicate that protective im-munity to the liver-stage of malaria can be conferred by
been recently demonstrated in Kenya and it is important -
tween 2012 & 2013, we ran a phase IIb, controlled, single blinded, randomised vaccine trial in Guediawaye. The main objectives were to assess the safety, immunogenic-
We randomly allocated 120 healthy male adult vol-unteers to vaccination with either the vaccine candidate, or verorab as control. Immunogenicity was measured by
--
mia and conducted intensive PCR monitoring to identify new Plasmodium falciparum infections over an eight week follow-up period. Vaccine related adverse events were mild to moderate in intensity with 1 serious adverse event in the control group not related to the intervention.
-
days later as measured by Elispot. Peak immunogenicity was shown 7 days after the boost and was high at a geo-metric mean of 1266 Spots per million PBMCs (95% CI
dose vectored vaccination approach targeting the liver-stage of malaria shows promise as a candidate malaria vaccine.
Vaccine developmentSeveral of our staff have participated in the design, execution and evaluation of RTS,S candidate vaccine trials as well as a trial of a prime boost vaccine candidate in Senegal.

66 Treatment of malaria Treatment of malaria 67
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Malaria Centre members continue to investigate how best to treat malaria, responding to shifting and localised dynamics in parasitological, epidemiological, systemic and political economic contexts.
2012-14 across a range of issues in malaria
treatment, grappling with how interventions
interact with a variety of contextual
methods.
Malaria treatment studies within the Malaria
Centre include attention to antimalarial drugs
effectiveness; strong focus on how antimalarials
are used and how best to support access and
appropriate use through different programmes;
and emphasis on wider case management
questions, with a keen interest in the use of
targeting of antimalarial drugs.
These studies have been carried out across
a range of contexts – in different countries
on different health care providers, including
community volunteers, private retailers and
school teachers as well as formal health facilities.
In so-doing, these studies have contributed to
an increased evidence base of the effects of
different programmes to improve antimalarial
and diagnostic use across a variety of settings.
The studies also explicitly investigate and aim to
antimalarial and diagnostic use, for example
in the context of patients taking antiretroviral
drugs for HIV, or where patients may have
is unreliable, or where knowledge of local
epidemiology of malaria-like illnesses is poor.
Through a lens of research on malaria treatment,
this collection of studies therefore goes beyond
a perspective of drugs as a simple solution,
to investigate how best to implement these in
complex and varied situations of health care
seeking and health care delivery.
To address these topics of research,
the Malaria Centre’s strengths in multiple
disciplines, and interdisciplinary working, are
powerfully displayed. Many of the studies
operate through teams of investigators from
different backgrounds who contribute different
understanding malaria treatment, designing
interventions to support access and use of
biomedical tools, and evaluating interventions to
make a robust contribution to the evidence base
in a way amenable for use by policy makers and
programme managers.
In the studies presented in this section,
answers to research questions have been
conceptual frameworks and modelling allow us
to learn from previous experience and predict
future scenarios; surveys and qualitative studies
of existing situations allow us to learn where
needs are greatest and how best to intervene, as
well as providing a platform for evaluation; and
intervention trials allow us to test solutions in a
implementation research.
These studies provide strong evidence on
a range of questions around how best to treat
malaria across a range of settings with different
biological, infrastructural and social scenarios.
Taken together, they show the importance of
interdisciplinary work and integration of malaria
care seeking and health care systems. This set
of studies represents a substantial contribution
to national and global policy and programme
making.
66 Treatment of malaria Treatment of malaria 67
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Malaria Centre members continue to investigate how best to treat malaria, responding to shifting and localised dynamics in parasitological, epidemiological, systemic and political economic contexts.
2012-14 across a range of issues in malaria
treatment, grappling with how interventions
interact with a variety of contextual
methods.
Malaria treatment studies within the Malaria
Centre include attention to antimalarial drugs
effectiveness; strong focus on how antimalarials
are used and how best to support access and
appropriate use through different programmes;
and emphasis on wider case management
questions, with a keen interest in the use of
targeting of antimalarial drugs.
These studies have been carried out across
a range of contexts – in different countries
on different health care providers, including
community volunteers, private retailers and
school teachers as well as formal health facilities.
In so-doing, these studies have contributed to
an increased evidence base of the effects of
different programmes to improve antimalarial
and diagnostic use across a variety of settings.
The studies also explicitly investigate and aim to
antimalarial and diagnostic use, for example
in the context of patients taking antiretroviral
drugs for HIV, or where patients may have
is unreliable, or where knowledge of local
epidemiology of malaria-like illnesses is poor.
Through a lens of research on malaria treatment,
this collection of studies therefore goes beyond
a perspective of drugs as a simple solution,
to investigate how best to implement these in
complex and varied situations of health care
seeking and health care delivery.
To address these topics of research,
the Malaria Centre’s strengths in multiple
disciplines, and interdisciplinary working, are
powerfully displayed. Many of the studies
operate through teams of investigators from
different backgrounds who contribute different
understanding malaria treatment, designing
interventions to support access and use of
biomedical tools, and evaluating interventions to
make a robust contribution to the evidence base
in a way amenable for use by policy makers and
programme managers.
In the studies presented in this section,
answers to research questions have been
conceptual frameworks and modelling allow us
to learn from previous experience and predict
future scenarios; surveys and qualitative studies
of existing situations allow us to learn where
needs are greatest and how best to intervene, as
well as providing a platform for evaluation; and
intervention trials allow us to test solutions in a
implementation research.
These studies provide strong evidence on
a range of questions around how best to treat
malaria across a range of settings with different
biological, infrastructural and social scenarios.
Taken together, they show the importance of
interdisciplinary work and integration of malaria
care seeking and health care systems. This set
of studies represents a substantial contribution
to national and global policy and programme
making.

68 Treatment of malaria Treatment of malaria 69
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The ACT Consortium: a research consortium to optimise the delivery of effective anti-malarial treatment.
Drug studies
Fake artemisinin-based combination therapies –where are they?
LSHTM Investigators: Harparkash Kaur.
External Investigators/Collaborators: Facundo Fernandez
Prevention USA).
Funding:
Consortium.
Reports of ad hocthat up to 50% of the artesunate monotherpy sold
monotherapies and artemisinin-based combination
where the predominant species is the potentially fatal Plasmodium falciparum. Resource poor countries do not
to inspect and police the drug supply.
public and private healthcare providers in Rwanda,
database, the packages scanned and, tablets weighed and measured, followed with qualitative (mass
environmental impact, we are investigating the ageing of
studies, with quantitative analysis carried out at regular intervals. Characterisation of the degradation products is underway.
varying sample collections methods, have been analysed and most have been found to contain the stated active
in the samples between the three collaborating bio analytical laboratories (London School of Hygiene and Tropical Medicine, Georgia Technical School of Chemistry
Counterfeit, medicinal products.
Antimalarial drug samples.
Malaria centre members carry out research related to malaria diagnosis and treatment
effectiveness modelling.
LSHTM Investigators: Evelyn Ansah, Katia Bruxwoort,
Matthew Cairns, Clare Chandler, Daniel Chandramohan, Sian
Harparkash Kaur, Sham Lal, Toby Leslie, Seth Owusu-Agyei,
Hugh Reyburn, Mark Rowland, David Schellenberg, Sarah
Staedke , Rebecca Thomson, Jayne Webster, Christopher
External Investigators/Collaborators: US Centres for
Disease Control and Prevention,USA; College of Medicine,
University of Malawi, Malawi; College of Medicine, University
Institute of Technology, USA; Health Protection and Research
Organisation, Afghanistan; Healthnet, Afghanistan; Ifakara
Health Institute, Tanzania; Karolinska Institutet, Sweden;
Kilimanjaro Christian Medical Centre, Tanzania; Kintampo
Tropical Medicine, UK; Makerere University, Uganda; Merlin,
Afghanistan; National Malaria Control Programme, Cambodia;
National Institute for Medical Research, Tanzania; National
Malaria Control Programme, Tanzania; Ministry of Health,
Kampala, Uganda; University of California, San Francisco,
USA; University of Cape Town, South Africa; University of
Funding:
an international research collaboration aiming to maximise the public health impact of artemisinin-
quality, policy-driven, multidisciplinary operational research. We work on 25 projects in 10 countries and with partners worldwide, using a variety of study of methods to address research questions about:
for those who most need them
through the deployment of rapid diagnostic tests
sub-standard and counterfeit artemisinin drugs
conditions, especially in high risk groups and when used in combination with other drugs.
We conduct formative research, cluster randomised trials, cohort and descriptive studies, and impact evaluation, as well as economic and anthropological assessments

68 Treatment of malaria Treatment of malaria 69
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The ACT Consortium: a research consortium to optimise the delivery of effective anti-malarial treatment.
Drug studies
Fake artemisinin-based combination therapies –where are they?
LSHTM Investigators: Harparkash Kaur.
External Investigators/Collaborators: Facundo Fernandez
Prevention USA).
Funding:
Consortium.
Reports of ad hocthat up to 50% of the artesunate monotherpy sold
monotherapies and artemisinin-based combination
where the predominant species is the potentially fatal Plasmodium falciparum. Resource poor countries do not
to inspect and police the drug supply.
public and private healthcare providers in Rwanda,
database, the packages scanned and, tablets weighed and measured, followed with qualitative (mass
environmental impact, we are investigating the ageing of
studies, with quantitative analysis carried out at regular intervals. Characterisation of the degradation products is underway.
varying sample collections methods, have been analysed and most have been found to contain the stated active
in the samples between the three collaborating bio analytical laboratories (London School of Hygiene and Tropical Medicine, Georgia Technical School of Chemistry
Counterfeit, medicinal products.
Antimalarial drug samples.
Malaria centre members carry out research related to malaria diagnosis and treatment
effectiveness modelling.
LSHTM Investigators: Evelyn Ansah, Katia Bruxwoort,
Matthew Cairns, Clare Chandler, Daniel Chandramohan, Sian
Harparkash Kaur, Sham Lal, Toby Leslie, Seth Owusu-Agyei,
Hugh Reyburn, Mark Rowland, David Schellenberg, Sarah
Staedke , Rebecca Thomson, Jayne Webster, Christopher
External Investigators/Collaborators: US Centres for
Disease Control and Prevention,USA; College of Medicine,
University of Malawi, Malawi; College of Medicine, University
Institute of Technology, USA; Health Protection and Research
Organisation, Afghanistan; Healthnet, Afghanistan; Ifakara
Health Institute, Tanzania; Karolinska Institutet, Sweden;
Kilimanjaro Christian Medical Centre, Tanzania; Kintampo
Tropical Medicine, UK; Makerere University, Uganda; Merlin,
Afghanistan; National Malaria Control Programme, Cambodia;
National Institute for Medical Research, Tanzania; National
Malaria Control Programme, Tanzania; Ministry of Health,
Kampala, Uganda; University of California, San Francisco,
USA; University of Cape Town, South Africa; University of
Funding:
an international research collaboration aiming to maximise the public health impact of artemisinin-
quality, policy-driven, multidisciplinary operational research. We work on 25 projects in 10 countries and with partners worldwide, using a variety of study of methods to address research questions about:
for those who most need them
through the deployment of rapid diagnostic tests
sub-standard and counterfeit artemisinin drugs
conditions, especially in high risk groups and when used in combination with other drugs.
We conduct formative research, cluster randomised trials, cohort and descriptive studies, and impact evaluation, as well as economic and anthropological assessments

70 Treatment of malaria Treatment of malaria 71
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Surveillance approaches to detect the quality of antimalarial drugs in Senegal.
LSHTM Investigators: Mirza Lalani, Harparkash Kaur, Sian Clarke
& Jayne Webster.
External Investigators/Collaborators: Aminata Dior Ndiaye (Uni-
versity of Cheikh Anta Diop, Senegal).
Funding:
Fund.
The aim of this study was to establish the perceptions of stakeholders relating to their institutional roles and responsibilities for assuring the quality of drugs and the perceived strengths and weaknesses of the drug quality surveillance system in Senegal.
In-depth qualitative interviews were conducted with key stakeholders; representatives of the surveillance sys-tem authorities and treatment providers in the regulated public and private health sectors. The interview guide focussed on two main aspects; system context including challenges faced and institutional roles and responsibili-
increase the risk of poor quality antimalarials in Senegal. Within this a health systems lens was applied allowing for inductive expansion of emergent themes relating to the six building blocks of health systems.
Preliminary analysis of the data indicates that all stakeholders perceive that the system operates effectively
authorities and between authorities and treatment pro-viders is perceived to be a problem. Perceptions of the quality of antimalarials are related to their cost, country of
-ditions and the informal drug sector are seen as the two main risk factors for poor quality antimalarials in Senegal.
Stringent drug regulation and a secure drug supply
the quality of antimalarials available Senegal. However a lack of funding, issues of governance, inadequate human resource and an absence of monitoring of the informal sector (due to concerns that acknowledgment would le-
that has been made by national authorities and external partners in assuring drug quality in Senegal.
sub-study focussing on one component of a drug quality surveillance system - drug quality analysis is in progress. Data collection was undertaken at the Laboratoire Natio-nale de Contrôle des Medicaments in Dakar, Senegal. The sub-study focussed on the practical utility and per-ceptions of usefulness of a drug quality screening test the
Use of artemether-lumefantrine in the treatment of asymptomatic malaria in HIV-positive and HIV-negative Nigerian adults.
LSHTM Investigators: Ifeyinwa Nwogo Chijioke-Nwauche, Mary
Oguike, Khalid Beshir, Harparkash Kaur & Colin Sutherland.
External Investigators/Collaborators: Chijioke Nwauche (Univer-
sity of Port Harcourt, Nigeria).
Funding: Rivers State Sustainable Development Agency; the MA-
LACTRES Consortium.
in the treatment of asymptomatic-malaria in HIV-positive and HIV-negative Nigerian adults.
Plasmodium falciparum and the use of medication for HIV management
-mether-lumefantrine and antiretroviral drugs
-mether-lumefantrine and other antimalarial drugs
-ymptomatic infections completely, as judged by post hoc PCR. HIV-positive people on nevirapine harbour higher concentrations of peripheral blood lumefantrine on day 7 post-treatment, and were also more likely to harbour par-asitaemia before and after treatment. There was a strong selection for the N allele in those with PCR-detectable parasitaemia at day 3. This allele has previ-
T was observed especially in the HIV-positive group, indicating that CQ resistant parasites are common in this setting. Primary diagnosis of parasite infections was performed locally by
a high rate of false positives, and thus over-estimation of the number of malaria infections. Future studies will be carried out to include children and pregnant women in a
will be carried out at multiple sites around Port Harcourt
need to invest in equipment and training of personnel for improved quality of malaria diagnosis.
artemisinin-based combination therapies in four endemic sites in Africa – the WANECAM Consortium.
LSHTM Investigators: Colin Sutherland & Khalid Beshir.
External Investigators/Collaborators: West African Network for
Clinical trials of AntiMalarial drugs; Malaria Research and Training
et de Formation sur le Paludisme, Burkina Faso; Institut de Re-
-
-
nard, France; Karolinska Institutet, Sweden; University of Heidelberg
Funding: European and Developing Countries Clinical Trials Part-
nership Programme through the West African Network for Clinical
trials of AntiMalarial drugs.
To overcome the challenge of frequent sampling and lack of microscopic sensitivity, we have developed a rapid and
-
We have recently shown that the presence of persis--
cantly associated with presence of gametocyte on day-7, infectiousness to mosquitoes and recrudescent parasites 28- or 42-days after treatment in Kenyan children (Beshir
infectivity was a step in the development of resistance to the old anti-malarial drugs chloroquine and sulphadoxine pyrimethamine.
-ing qPCR.
treatment arms
clearance and gametocyte carriage, infectivity to mos-quito and recurrent parasitemia
episode-1 and episode-2
clearance and candidate molecular markers (pfcrt and
technique, and in analysis of trial data
Khalid Beshir on his visit to Abdoulaye Djimde’s laboratory in Mali and staff who received training on measurement of malaria parasitemia using quantitative real-time PCR.
Modelling the cost-effectiveness of options for the radical cure of Plasmodium vivax.
LSHTM Investigators
External Investigators/Collaborators:
Thailand).
Funding:
Plasmodium vivax causes a huge burden of disease Plasmodium falciparum, it
forms hypnozoites which can cause repeated relapses. The only class of drugs effective against hypnozoites is 8-aminoquinolones however, these have the potential to cause life-threatening haemolysis in patients with G6PD
The aim of this project is to examine the cost-effectiveness of adding an 8-aminoquinolone with or
cure of symptomatic infection with Plasmodium vivax.We used a combination of a decision tree model with
Markov cycle, to model the cost-effectiveness of different strategies managing symptomatic patients ie with and without an 8-aminoquinolone, and with and without prior
The model results are very sensitive to key uncertainties such as the level of adherence to primaquine and the likelihood of heamolysis in patients. However, when adherence levels were high, in most scenarios treatment with an 8-aminoquinolone with prior G6PD testing came out as the most cost-effective option.

70 Treatment of malaria Treatment of malaria 71
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Surveillance approaches to detect the quality of antimalarial drugs in Senegal.
LSHTM Investigators: Mirza Lalani, Harparkash Kaur, Sian Clarke
& Jayne Webster.
External Investigators/Collaborators: Aminata Dior Ndiaye (Uni-
versity of Cheikh Anta Diop, Senegal).
Funding:
Fund.
The aim of this study was to establish the perceptions of stakeholders relating to their institutional roles and responsibilities for assuring the quality of drugs and the perceived strengths and weaknesses of the drug quality surveillance system in Senegal.
In-depth qualitative interviews were conducted with key stakeholders; representatives of the surveillance sys-tem authorities and treatment providers in the regulated public and private health sectors. The interview guide focussed on two main aspects; system context including challenges faced and institutional roles and responsibili-
increase the risk of poor quality antimalarials in Senegal. Within this a health systems lens was applied allowing for inductive expansion of emergent themes relating to the six building blocks of health systems.
Preliminary analysis of the data indicates that all stakeholders perceive that the system operates effectively
authorities and between authorities and treatment pro-viders is perceived to be a problem. Perceptions of the quality of antimalarials are related to their cost, country of
-ditions and the informal drug sector are seen as the two main risk factors for poor quality antimalarials in Senegal.
Stringent drug regulation and a secure drug supply
the quality of antimalarials available Senegal. However a lack of funding, issues of governance, inadequate human resource and an absence of monitoring of the informal sector (due to concerns that acknowledgment would le-
that has been made by national authorities and external partners in assuring drug quality in Senegal.
sub-study focussing on one component of a drug quality surveillance system - drug quality analysis is in progress. Data collection was undertaken at the Laboratoire Natio-nale de Contrôle des Medicaments in Dakar, Senegal. The sub-study focussed on the practical utility and per-ceptions of usefulness of a drug quality screening test the
Use of artemether-lumefantrine in the treatment of asymptomatic malaria in HIV-positive and HIV-negative Nigerian adults.
LSHTM Investigators: Ifeyinwa Nwogo Chijioke-Nwauche, Mary
Oguike, Khalid Beshir, Harparkash Kaur & Colin Sutherland.
External Investigators/Collaborators: Chijioke Nwauche (Univer-
sity of Port Harcourt, Nigeria).
Funding: Rivers State Sustainable Development Agency; the MA-
LACTRES Consortium.
in the treatment of asymptomatic-malaria in HIV-positive and HIV-negative Nigerian adults.
Plasmodium falciparum and the use of medication for HIV management
-mether-lumefantrine and antiretroviral drugs
-mether-lumefantrine and other antimalarial drugs
-ymptomatic infections completely, as judged by post hoc PCR. HIV-positive people on nevirapine harbour higher concentrations of peripheral blood lumefantrine on day 7 post-treatment, and were also more likely to harbour par-asitaemia before and after treatment. There was a strong selection for the N allele in those with PCR-detectable parasitaemia at day 3. This allele has previ-
T was observed especially in the HIV-positive group, indicating that CQ resistant parasites are common in this setting. Primary diagnosis of parasite infections was performed locally by
a high rate of false positives, and thus over-estimation of the number of malaria infections. Future studies will be carried out to include children and pregnant women in a
will be carried out at multiple sites around Port Harcourt
need to invest in equipment and training of personnel for improved quality of malaria diagnosis.
artemisinin-based combination therapies in four endemic sites in Africa – the WANECAM Consortium.
LSHTM Investigators: Colin Sutherland & Khalid Beshir.
External Investigators/Collaborators: West African Network for
Clinical trials of AntiMalarial drugs; Malaria Research and Training
et de Formation sur le Paludisme, Burkina Faso; Institut de Re-
-
-
nard, France; Karolinska Institutet, Sweden; University of Heidelberg
Funding: European and Developing Countries Clinical Trials Part-
nership Programme through the West African Network for Clinical
trials of AntiMalarial drugs.
To overcome the challenge of frequent sampling and lack of microscopic sensitivity, we have developed a rapid and
-
We have recently shown that the presence of persis--
cantly associated with presence of gametocyte on day-7, infectiousness to mosquitoes and recrudescent parasites 28- or 42-days after treatment in Kenyan children (Beshir
infectivity was a step in the development of resistance to the old anti-malarial drugs chloroquine and sulphadoxine pyrimethamine.
-ing qPCR.
treatment arms
clearance and gametocyte carriage, infectivity to mos-quito and recurrent parasitemia
episode-1 and episode-2
clearance and candidate molecular markers (pfcrt and
technique, and in analysis of trial data
Khalid Beshir on his visit to Abdoulaye Djimde’s laboratory in Mali and staff who received training on measurement of malaria parasitemia using quantitative real-time PCR.
Modelling the cost-effectiveness of options for the radical cure of Plasmodium vivax.
LSHTM Investigators
External Investigators/Collaborators:
Thailand).
Funding:
Plasmodium vivax causes a huge burden of disease Plasmodium falciparum, it
forms hypnozoites which can cause repeated relapses. The only class of drugs effective against hypnozoites is 8-aminoquinolones however, these have the potential to cause life-threatening haemolysis in patients with G6PD
The aim of this project is to examine the cost-effectiveness of adding an 8-aminoquinolone with or
cure of symptomatic infection with Plasmodium vivax.We used a combination of a decision tree model with
Markov cycle, to model the cost-effectiveness of different strategies managing symptomatic patients ie with and without an 8-aminoquinolone, and with and without prior
The model results are very sensitive to key uncertainties such as the level of adherence to primaquine and the likelihood of heamolysis in patients. However, when adherence levels were high, in most scenarios treatment with an 8-aminoquinolone with prior G6PD testing came out as the most cost-effective option.

72 Treatment of malaria Treatment of malaria 73
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
ivermectin to prevent malaria transmission after treatment: a double-blind, randomised clinical trial.
LSHTM Investigators: Teun Bousema & Chris Drakeley.
External Investigators/Collaborators:
Edith Bougouma, Issa Nebie, Maurice San Ouattara, Sodiomon
Sirima (Centre National de Recherche et de Formation sur le
Sauerwein (Radboud University Medical Center, Netherlands);
Kevin Kobylinski (Walter Reed Army Institute of Research, USA);
Lawrence Fleckenstein (University of Iowa, USA) & Hannah Slater,
Thomas Churcher (Imperial College London, UK).
Funding: The Radboud University Medical Center; The Bill &
by Novartis.
asexual malaria parasites and immature gametocytes but does not prevent post-treatment malaria transmission.
killing mosquitoes that take blood meals from IVM treated humans. In a double-blinded placebo-controlled trial, 120
asymptomatic Plasmodium falciparum parasite carriers were randomised to receive artemether-lumefantrine
feeding was performed 1, 3, and 7 days after initiation of treatment to determine Anopheles gambiae and Anopheles funestus survival and infection rates. IVM resulted in a 4 to 7-fold increased mortality in mosquitoes
levels were positively associated with body mass index
until 7 days after a single dose of IVM (hazard rate ratio
evidence that IVM reduced Plasmodium infection rates among surviving mosquitoes, the mosquitocidal effect
reductions in the patients contribution to transmission
respectively. We conclude that IVM can be safely given
malaria transmission by reducing the lifespan of feeding mosquitoes. Future work should aim to maximise the duration of the mosquitocidal effect.
-
Community-based case managementA key area of our work focuses on understanding and evaluating interventions to improve case management of malaria and the use of artemisinin-based combination therapy in the community (private retail outlets, community health workers and schools) as well as evaluation of the Affordable Medicines Facility for malaria.
Village Malaria Worker Access to Treatment (VIMWAT) study.
LSHTM Investigators
Edith Patouillard & Tom Drake.
External Investigators/Collaborators: Chea Nguon & Poly Teng
(National Malaria Control Programme, Cambodia).
Funding: Clinton Health Access Initiative; The Department for
through the ACT Consortium.
In Cambodia the national malaria control programme
in 2004. VMWs are community volunteers who perform
malaria cases with artemisinin-based combination
In selected villages, VMWs have an expanded role to diagnose and treat acute respiratory infections and
diarrhoea with antibiotics or oral rehydration salts and Zinc respectively for children under 5 years.
effectiveness and cost of the VMW programme in delivering prompt access to appropriate diagnosis and
in children. In Kampot province, 1,152 households in villages with malaria only VMWs, expanded role VMWs or no VMWs were followed up over 6 months in order to capture information on illnesses experienced and health seeking behaviour. Total annual programme costs were calculated from 2004 to 2010.
The number of reported suspected malaria episodes
the selected province However for individuals who did report suspected malaria, those from villages with VMWs were more likely to receive appropriate diagnosis with a blood test, than in villages without VMWs.

72 Treatment of malaria Treatment of malaria 73
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
ivermectin to prevent malaria transmission after treatment: a double-blind, randomised clinical trial.
LSHTM Investigators: Teun Bousema & Chris Drakeley.
External Investigators/Collaborators:
Edith Bougouma, Issa Nebie, Maurice San Ouattara, Sodiomon
Sirima (Centre National de Recherche et de Formation sur le
Sauerwein (Radboud University Medical Center, Netherlands);
Kevin Kobylinski (Walter Reed Army Institute of Research, USA);
Lawrence Fleckenstein (University of Iowa, USA) & Hannah Slater,
Thomas Churcher (Imperial College London, UK).
Funding: The Radboud University Medical Center; The Bill &
by Novartis.
asexual malaria parasites and immature gametocytes but does not prevent post-treatment malaria transmission.
killing mosquitoes that take blood meals from IVM treated humans. In a double-blinded placebo-controlled trial, 120
asymptomatic Plasmodium falciparum parasite carriers were randomised to receive artemether-lumefantrine
feeding was performed 1, 3, and 7 days after initiation of treatment to determine Anopheles gambiae and Anopheles funestus survival and infection rates. IVM resulted in a 4 to 7-fold increased mortality in mosquitoes
levels were positively associated with body mass index
until 7 days after a single dose of IVM (hazard rate ratio
evidence that IVM reduced Plasmodium infection rates among surviving mosquitoes, the mosquitocidal effect
reductions in the patients contribution to transmission
respectively. We conclude that IVM can be safely given
malaria transmission by reducing the lifespan of feeding mosquitoes. Future work should aim to maximise the duration of the mosquitocidal effect.
-
Community-based case managementA key area of our work focuses on understanding and evaluating interventions to improve case management of malaria and the use of artemisinin-based combination therapy in the community (private retail outlets, community health workers and schools) as well as evaluation of the Affordable Medicines Facility for malaria.
Village Malaria Worker Access to Treatment (VIMWAT) study.
LSHTM Investigators
Edith Patouillard & Tom Drake.
External Investigators/Collaborators: Chea Nguon & Poly Teng
(National Malaria Control Programme, Cambodia).
Funding: Clinton Health Access Initiative; The Department for
through the ACT Consortium.
In Cambodia the national malaria control programme
in 2004. VMWs are community volunteers who perform
malaria cases with artemisinin-based combination
In selected villages, VMWs have an expanded role to diagnose and treat acute respiratory infections and
diarrhoea with antibiotics or oral rehydration salts and Zinc respectively for children under 5 years.
effectiveness and cost of the VMW programme in delivering prompt access to appropriate diagnosis and
in children. In Kampot province, 1,152 households in villages with malaria only VMWs, expanded role VMWs or no VMWs were followed up over 6 months in order to capture information on illnesses experienced and health seeking behaviour. Total annual programme costs were calculated from 2004 to 2010.
The number of reported suspected malaria episodes
the selected province However for individuals who did report suspected malaria, those from villages with VMWs were more likely to receive appropriate diagnosis with a blood test, than in villages without VMWs.

74 Treatment of malaria Treatment of malaria 75
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Independent evaluation of the Affordable Medicines Facility – malaria (AMFm).
LSHTM Investigators: Barbara Willey, Sarah Tougher, Andrea
Mann, Rebecca Thomson, Sergio Torres Rueda, Didier Diallo, Katia
External Investigators/Collaborators: ICF-International;
ACTwatch; Population Services International, Kenya; Ifakara Health
Health Research Centre, Kenya; Centre de Recherche pour le
Recherches sur les Populations Africaines, Niger.
Funding:
Consortium.
Medicines Facility – malaria to increase the access and use of quality-assured artemisinin-based combination
factory gate price subsidies, and supporting interventions such as communications campaigns. We conducted an evaluation of the programme to estimate its impact
Ghana, Kenya, Madagascar, Niger, Nigeria, Uganda, and
Data included nationally representative baseline and endline surveys of public and private sector outlets stocking antimalarials, and key informant interviews and document reviews to record contextual factors and the implementation process.
In all pilots except Niger and Madagascar, there
were seen in the PFP sector in six pilots, ranging from
where it was not minimal at baseline. We concluded that subsidies combined with
supporting interventions can be eff ective in rapidly improving availability, price, and market share of
Mystery clients and drug cocktails.
LSHTM Investigators
Mikhael Dsouza.
External Investigators/Collaborators: Facundo Fernandez &
& Ouk Rada (National Malaria control programme, Cambodia).
Funding:
Consortium.
In Cambodia, as in other countries in Southeast asia, it is common practice for patients seeking treatment for fever to be sold little packets containing a colourful combination of different tablets and capsules. However, the content of these “drug cocktails” is largely unknown.
This study aimed to identify the contents of these drug cocktails through a mystery client study where
to drug shops and pharmacies, seeking treatment for
an experienced pharmacist. Two hundred and ten providers were visited from
whom 191 drug cocktails were bought. The median
of tablets were for symptomatic relief (anti-pyretic, anti-
commonly found, as were antimalarials and occasionally steroids. This has important implications both for individual patients and public health in terms of the inappropriate use of antimicrobials and drug resistance.
An economic analysis of the Affordable Medicines Facility - malaria (AMFm).
LSHTM Investigators: Sarah Tougher, Kara Hanson & Catherine
External Investigators/Collaborators:
Poyer, Julius Njogu, Illah Evance, Meghan Littrell, & Desmond
Chavasse (ACTwatch & Population Services International); Jennifer
Anyanti & Ekundayo Arogundade (Society for Family Health); Perter
Buyungo & Henry Kaula (PACE, Uganda).
Funding:
sector, subsidies for artemisinin-based combination
endemic countries, have been implemented in a number
other treatments. The largest initiative of this type was the
was implemented at a national scale in eight pilots in seven countries from 2010-2013.
share in six of the eight pilots. However, little is known about the causes of inter- and intra- country variations in performance, or the equity impact of the programme.
This study uses existing outlet and household survey data to establish the impact of market structure on performance of markets for antimalarials in three
to model provider decisions to stock and set prices for subsidized medicines, as these aspects of provider behavior are critical to a subsidy programme’s success. The household survey data will be used to assess the
Evidence from this study will be available in 2014,
and the types of supporting interventions and their targeting that are most appropriate.

74 Treatment of malaria Treatment of malaria 75
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Independent evaluation of the Affordable Medicines Facility – malaria (AMFm).
LSHTM Investigators: Barbara Willey, Sarah Tougher, Andrea
Mann, Rebecca Thomson, Sergio Torres Rueda, Didier Diallo, Katia
External Investigators/Collaborators: ICF-International;
ACTwatch; Population Services International, Kenya; Ifakara Health
Health Research Centre, Kenya; Centre de Recherche pour le
Recherches sur les Populations Africaines, Niger.
Funding:
Consortium.
Medicines Facility – malaria to increase the access and use of quality-assured artemisinin-based combination
factory gate price subsidies, and supporting interventions such as communications campaigns. We conducted an evaluation of the programme to estimate its impact
Ghana, Kenya, Madagascar, Niger, Nigeria, Uganda, and
Data included nationally representative baseline and endline surveys of public and private sector outlets stocking antimalarials, and key informant interviews and document reviews to record contextual factors and the implementation process.
In all pilots except Niger and Madagascar, there
were seen in the PFP sector in six pilots, ranging from
where it was not minimal at baseline. We concluded that subsidies combined with
supporting interventions can be eff ective in rapidly improving availability, price, and market share of
Mystery clients and drug cocktails.
LSHTM Investigators
Mikhael Dsouza.
External Investigators/Collaborators: Facundo Fernandez &
& Ouk Rada (National Malaria control programme, Cambodia).
Funding:
Consortium.
In Cambodia, as in other countries in Southeast asia, it is common practice for patients seeking treatment for fever to be sold little packets containing a colourful combination of different tablets and capsules. However, the content of these “drug cocktails” is largely unknown.
This study aimed to identify the contents of these drug cocktails through a mystery client study where
to drug shops and pharmacies, seeking treatment for
an experienced pharmacist. Two hundred and ten providers were visited from
whom 191 drug cocktails were bought. The median
of tablets were for symptomatic relief (anti-pyretic, anti-
commonly found, as were antimalarials and occasionally steroids. This has important implications both for individual patients and public health in terms of the inappropriate use of antimicrobials and drug resistance.
An economic analysis of the Affordable Medicines Facility - malaria (AMFm).
LSHTM Investigators: Sarah Tougher, Kara Hanson & Catherine
External Investigators/Collaborators:
Poyer, Julius Njogu, Illah Evance, Meghan Littrell, & Desmond
Chavasse (ACTwatch & Population Services International); Jennifer
Anyanti & Ekundayo Arogundade (Society for Family Health); Perter
Buyungo & Henry Kaula (PACE, Uganda).
Funding:
sector, subsidies for artemisinin-based combination
endemic countries, have been implemented in a number
other treatments. The largest initiative of this type was the
was implemented at a national scale in eight pilots in seven countries from 2010-2013.
share in six of the eight pilots. However, little is known about the causes of inter- and intra- country variations in performance, or the equity impact of the programme.
This study uses existing outlet and household survey data to establish the impact of market structure on performance of markets for antimalarials in three
to model provider decisions to stock and set prices for subsidized medicines, as these aspects of provider behavior are critical to a subsidy programme’s success. The household survey data will be used to assess the
Evidence from this study will be available in 2014,
and the types of supporting interventions and their targeting that are most appropriate.

76 Treatment of malaria Treatment of malaria 77
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A cost-consequences analysis of the Affordable Medicines Facility - malaria (AMFm).
LSHTM Investigators: Fiona Cianci, Daniel Cobos, Sarah Tougher,
Funding:
In 2010 the Global Fund launched national scale
assured artemisinin-based combination therapies
involved manufacturer price negotiations, factory gate price subsidies, and supporting interventions such as
Communicating the Affordable Medicines Facility - malaria (AMFm) message: exploring the effect of communication and training
awareness and knowledge related to a multi-country anti-malarial subsidy intervention.
LSHTM Investigators
Mann, Rebecca Thomson, Sergio Torres Rueda, Didier Diallo, Katia
External Investigators/Collaborators:
Arnold, Ruilin Ren & Abdinasir Amin (ICF International, USA); The
Johanes, Charles Festo & Admirabilis Kalolella (Ifakara Health
Institute, Tanzania); Idrissa Kourgueni, Moctar Seydou & Oumarou
Malam (Institut National de la Statistique, Niger); John Amuasi,
Samuel Blay Nguah & Daniel Ansong (Komfo Anokye Teaching
Population and Health Research Center, Kenya); Mark Taylor
(Trnava University, Slovakia); Salif Ndiaye (Centre de Recherche
for Neglected Diseases initiative, Switzerland); Catherine Adegoke
(Phar-Mark Consultants, Nigeria).
Funding:
Central and ACTwatch surveys in three countries.
or territories, subsidized quality-assured artemisinin
campaigns to support implementation and promote appropriate anti-malarial use. This project reports private
of appropriate malaria treatment, based on nationally representative surveys of outlets stocking anti-malarials
Based on data from over 19,500 outlets, results show that in four of eight settings, where communication campaigns were implemented for 5–9 months, 76%-94%
80% awareness of the correct recommended retail price
remaining four settings where communication campaigns were implemented for three months or less, levels were substantially lower. In six of eight settings, increases
uncomplicated malaria were seen; and in three of these the levels of knowledge achieved at endline were over 80%.
The results support the interpretation that, in addition
communication campaigns may have contributed to
communications campaigns. We conducted a cost-consequences analysis of
Nigeria and Madagascar. Data were collected in the
secretariat in Geneva. Cost data were collected through
Consequences data were collated through literature review.
Results will be available in late 2014, providing
the consequences in terms of a range of outcomes, and
in other settings.
School-based programme of malaria diagnosis and treatment in Malawi.
LSHTM Investigators: Simon Brooker, Katherine Halliday, Stefan
Witek-McManus, Elizabeth Allen & Rebecca Jones.
External Investigators/Collaborators: Don Mathanga (Malaria
Alert Centre, College of Medicine, Malawi); Doreen Ali & John Sande
(National Malaria Control Programme, Ministry of Health, Malawi);
Reuben Mwenda (Health Technical Support Services-Diagnostics,
Ministry of Health, Malawi); Charles Mazinga (Ministry of Education,
Science and Technology, Malawi); Austin Mtali & Tiyese Chimuna
(Save the Children International, Malawi); Natalie Roschnik (Save
the Children International, USA).
Funding: International Initiative for Impact Evaluation & Save the
Children Sponsorship funds.
With increasing levels of attendance, schools present a credible and pragmatic opportunity to improve the access of school children to timely diagnosis and treatment of clinical malaria, increasingly recognised as a major
evaluating the impact of a programme of teacher-based diagnosis and treatment for uncomplicated malaria on primary school attendance in 58 schools in Zomba, Malawi.
The pilot programme, implemented by the National Malaria control Programme in conjunction with Save the Children, involves training teachers in 29 randomly
artemether-lumefantrine to treat uncomplicated malaria.
the programme is ongoing in the schools with oversight
Researchers at the London School of Hygiene &
evaluating the programme, with ongoing monitoring of attendance throughout the school year. Secondary
nested process evaluation employing mixed methods will evaluate the cost effectiveness, feasibility and community acceptability of the school-based programme
Investigating the determinants of demand for antimalarial medicines in Benin, Nigeria, Uganda and Zambia.
LSHTM Investigators: Benjamin Palafox & Kara Hanson.
Funding: The Economic and Social Research Council
By 2008, all malaria endemic countries had adopted
particularly among children under 5 years of age for whom presumptive treatment continues to be widely accepted and practised where access to diagnostic testing is limited. Price is a critical barrier to their wider
prices including the national-level subsidy programme,
Maximising the impact of these investments and
requires an understanding of how responsive demand is to price and other determinants. To do this, we are using econometric demand models to analyse the determinants
of antimalarial choice in Benin, Madagascar, Uganda and Zambia. We are also examining changes in treatment seeking behaviour over time, making use of multiple rounds of household survey data.
In each country, data were collected through nationally representative surveys of households that experienced a recent paediatric febrile episode. This was complemented by survey data from all possible public and private sources of antimalarial medicines in the
artemisinin monotherapies, non-artemisinin therapies, and no treatment. The range of determinants being studied include the price of various treatment components
76 Treatment of malaria Treatment of malaria 77
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A cost-consequences analysis of the Affordable Medicines Facility - malaria (AMFm).
LSHTM Investigators: Fiona Cianci, Daniel Cobos, Sarah Tougher,
Funding:
In 2010 the Global Fund launched national scale
assured artemisinin-based combination therapies
involved manufacturer price negotiations, factory gate price subsidies, and supporting interventions such as
Communicating the Affordable Medicines Facility - malaria (AMFm) message: exploring the effect of communication and training
awareness and knowledge related to a multi-country anti-malarial subsidy intervention.
LSHTM Investigators
Mann, Rebecca Thomson, Sergio Torres Rueda, Didier Diallo, Katia
External Investigators/Collaborators:
Arnold, Ruilin Ren & Abdinasir Amin (ICF International, USA); The
Johanes, Charles Festo & Admirabilis Kalolella (Ifakara Health
Institute, Tanzania); Idrissa Kourgueni, Moctar Seydou & Oumarou
Malam (Institut National de la Statistique, Niger); John Amuasi,
Samuel Blay Nguah & Daniel Ansong (Komfo Anokye Teaching
Population and Health Research Center, Kenya); Mark Taylor
(Trnava University, Slovakia); Salif Ndiaye (Centre de Recherche
for Neglected Diseases initiative, Switzerland); Catherine Adegoke
(Phar-Mark Consultants, Nigeria).
Funding:
Central and ACTwatch surveys in three countries.
or territories, subsidized quality-assured artemisinin
campaigns to support implementation and promote appropriate anti-malarial use. This project reports private
of appropriate malaria treatment, based on nationally representative surveys of outlets stocking anti-malarials
Based on data from over 19,500 outlets, results show that in four of eight settings, where communication campaigns were implemented for 5–9 months, 76%-94%
80% awareness of the correct recommended retail price
remaining four settings where communication campaigns were implemented for three months or less, levels were substantially lower. In six of eight settings, increases
uncomplicated malaria were seen; and in three of these the levels of knowledge achieved at endline were over 80%.
The results support the interpretation that, in addition
communication campaigns may have contributed to
communications campaigns. We conducted a cost-consequences analysis of
Nigeria and Madagascar. Data were collected in the
secretariat in Geneva. Cost data were collected through
Consequences data were collated through literature review.
Results will be available in late 2014, providing
the consequences in terms of a range of outcomes, and
in other settings.
School-based programme of malaria diagnosis and treatment in Malawi.
LSHTM Investigators: Simon Brooker, Katherine Halliday, Stefan
Witek-McManus, Elizabeth Allen & Rebecca Jones.
External Investigators/Collaborators: Don Mathanga (Malaria
Alert Centre, College of Medicine, Malawi); Doreen Ali & John Sande
(National Malaria Control Programme, Ministry of Health, Malawi);
Reuben Mwenda (Health Technical Support Services-Diagnostics,
Ministry of Health, Malawi); Charles Mazinga (Ministry of Education,
Science and Technology, Malawi); Austin Mtali & Tiyese Chimuna
(Save the Children International, Malawi); Natalie Roschnik (Save
the Children International, USA).
Funding: International Initiative for Impact Evaluation & Save the
Children Sponsorship funds.
With increasing levels of attendance, schools present a credible and pragmatic opportunity to improve the access of school children to timely diagnosis and treatment of clinical malaria, increasingly recognised as a major
evaluating the impact of a programme of teacher-based diagnosis and treatment for uncomplicated malaria on primary school attendance in 58 schools in Zomba, Malawi.
The pilot programme, implemented by the National Malaria control Programme in conjunction with Save the Children, involves training teachers in 29 randomly
artemether-lumefantrine to treat uncomplicated malaria.
the programme is ongoing in the schools with oversight
Researchers at the London School of Hygiene &
evaluating the programme, with ongoing monitoring of attendance throughout the school year. Secondary
nested process evaluation employing mixed methods will evaluate the cost effectiveness, feasibility and community acceptability of the school-based programme
Investigating the determinants of demand for antimalarial medicines in Benin, Nigeria, Uganda and Zambia.
LSHTM Investigators: Benjamin Palafox & Kara Hanson.
Funding: The Economic and Social Research Council
By 2008, all malaria endemic countries had adopted
particularly among children under 5 years of age for whom presumptive treatment continues to be widely accepted and practised where access to diagnostic testing is limited. Price is a critical barrier to their wider
prices including the national-level subsidy programme,
Maximising the impact of these investments and
requires an understanding of how responsive demand is to price and other determinants. To do this, we are using econometric demand models to analyse the determinants
of antimalarial choice in Benin, Madagascar, Uganda and Zambia. We are also examining changes in treatment seeking behaviour over time, making use of multiple rounds of household survey data.
In each country, data were collected through nationally representative surveys of households that experienced a recent paediatric febrile episode. This was complemented by survey data from all possible public and private sources of antimalarial medicines in the
artemisinin monotherapies, non-artemisinin therapies, and no treatment. The range of determinants being studied include the price of various treatment components

78 Treatment of malaria Treatment of malaria 79
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Introducing rapid diagnostic tests in drug shops to improve the targeting of malaria treatment.
LSHTM Investigators: Sian
Clarke, Kristian Hansen, Clare
Chandler & Sham Lal.
External Investigators/
Collaborators: Anthony Mbonye
(Ministry of Health, Kampala,
Uganda); Pascal Magnussen
(University of Copenhagen,
Denmark).
Funding: The Wellcome Trust; The
through the ACT Consortium.
conducted in 59 registered drug shops in Uganda to assess the feasibility of introducing rapid diagnostic
shops in order to promote the rational and correct use of artemisinin-based
drugs when managing cases of malaria.
Drug shop vendors were also trained on malaria case
rectal artesunate pre-referral treatment, and when to refer. The trial compared treatment practices in shops trained to base malaria treatment on an RDT test result with the current approach of treating patients based solely on their symptoms, To examine whether RDTs improved targeting of
patient determined by expert microscopy on a research blood slide collected at the time of drug shop visit.The study found that the vast majority of patients accepted purchasing a rapid diagnostic test, and that over 85%
qualitative evaluation conducted alongside the trial found diagnostic testing was popular with both patients and providers, and fundamentally transformed the perception and role of drug shops.
Pictorial job aid used by drug shop vendors to guide treatment for drug shops in Uganda.
Use of rapid diagnostic tests in Uganda to improve malaria treatment in the community.
LSHTM Investigators: Sian Clarke, Kristian Hansen, Clare
Chandler & Sham Lal.
External Investigators/Collaborators: Richard Ndyomugyenyi
(National Malaria Control Programme, Uganda); Pascal Magnussen
(Univeristy of Copenhagen, Denmark).
Funding:
Consortium.
This randomised trial aims to assess whether the use of rapid diagnostic tests by community health workers
managing cases of malaria in the community. The trial compared home-based management of
malaria based on the results of rapid diagnostic tests
based solely on their symptoms, in two areas of high
were also trained on malaria case management including
to refer. To determine whether use of RDTs improved
by CHWs were evaluated against the malaria parasite infection status of the patient as detected by expert microscopy on a research blood slide collected at the time of consultation.
Early analysis suggests that over 85% of the community medicine distributors complied with the results of rapid diagnostic tests. The community were also aware that not all fever is caused by malaria, which increased
Introducing rapid diagnostic tests into the private health sector: a cost-effectiveness analysis among registered drug shops in Mukono district, Uganda.
LSHTM Investigators: Kristian Hansen, Sian Clarke & Sham Lal.
External Investigators/Collaborators: Anthony Mbonye (Ministry
of Health, Kampala, Uganda); Pascal Magnussen (University of
Copenhagen, Denmark).
Funding:
through the ACT Consortium.
It is common in Uganda for people to seek treatment for malaria in private drug shops where parasitological diagnosis to guide malaria treatment is not usually
to perform and have high accuracy, these tests could feasibly be offered in drug shops.
a cluster-randomised trial in Mukono district, Uganda, where drug shops were randomised either to prescribe
perspective incorporating provider costs (training,
health care seeking for malaria treatment. Preliminary results suggest that the total cost of providing malaria services in drug shops with access to RDT diagnosis was at least 15% higher than in drug shops providing presumptive diagnosis. However, the share of appropriately treated fever patients was much higher in RDT drug shops compared to drug shops with
the incremental cost of replacing presumptive diagnosis by RDT diagnosis in drug shops could therefore still be as low as US$2-3 per additional patient appropriately treated.

78 Treatment of malaria Treatment of malaria 79
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Introducing rapid diagnostic tests in drug shops to improve the targeting of malaria treatment.
LSHTM Investigators: Sian
Clarke, Kristian Hansen, Clare
Chandler & Sham Lal.
External Investigators/
Collaborators: Anthony Mbonye
(Ministry of Health, Kampala,
Uganda); Pascal Magnussen
(University of Copenhagen,
Denmark).
Funding: The Wellcome Trust; The
through the ACT Consortium.
conducted in 59 registered drug shops in Uganda to assess the feasibility of introducing rapid diagnostic
shops in order to promote the rational and correct use of artemisinin-based
drugs when managing cases of malaria.
Drug shop vendors were also trained on malaria case
rectal artesunate pre-referral treatment, and when to refer. The trial compared treatment practices in shops trained to base malaria treatment on an RDT test result with the current approach of treating patients based solely on their symptoms, To examine whether RDTs improved targeting of
patient determined by expert microscopy on a research blood slide collected at the time of drug shop visit.The study found that the vast majority of patients accepted purchasing a rapid diagnostic test, and that over 85%
qualitative evaluation conducted alongside the trial found diagnostic testing was popular with both patients and providers, and fundamentally transformed the perception and role of drug shops.
Pictorial job aid used by drug shop vendors to guide treatment for drug shops in Uganda.
Use of rapid diagnostic tests in Uganda to improve malaria treatment in the community.
LSHTM Investigators: Sian Clarke, Kristian Hansen, Clare
Chandler & Sham Lal.
External Investigators/Collaborators: Richard Ndyomugyenyi
(National Malaria Control Programme, Uganda); Pascal Magnussen
(Univeristy of Copenhagen, Denmark).
Funding:
Consortium.
This randomised trial aims to assess whether the use of rapid diagnostic tests by community health workers
managing cases of malaria in the community. The trial compared home-based management of
malaria based on the results of rapid diagnostic tests
based solely on their symptoms, in two areas of high
were also trained on malaria case management including
to refer. To determine whether use of RDTs improved
by CHWs were evaluated against the malaria parasite infection status of the patient as detected by expert microscopy on a research blood slide collected at the time of consultation.
Early analysis suggests that over 85% of the community medicine distributors complied with the results of rapid diagnostic tests. The community were also aware that not all fever is caused by malaria, which increased
Introducing rapid diagnostic tests into the private health sector: a cost-effectiveness analysis among registered drug shops in Mukono district, Uganda.
LSHTM Investigators: Kristian Hansen, Sian Clarke & Sham Lal.
External Investigators/Collaborators: Anthony Mbonye (Ministry
of Health, Kampala, Uganda); Pascal Magnussen (University of
Copenhagen, Denmark).
Funding:
through the ACT Consortium.
It is common in Uganda for people to seek treatment for malaria in private drug shops where parasitological diagnosis to guide malaria treatment is not usually
to perform and have high accuracy, these tests could feasibly be offered in drug shops.
a cluster-randomised trial in Mukono district, Uganda, where drug shops were randomised either to prescribe
perspective incorporating provider costs (training,
health care seeking for malaria treatment. Preliminary results suggest that the total cost of providing malaria services in drug shops with access to RDT diagnosis was at least 15% higher than in drug shops providing presumptive diagnosis. However, the share of appropriately treated fever patients was much higher in RDT drug shops compared to drug shops with
the incremental cost of replacing presumptive diagnosis by RDT diagnosis in drug shops could therefore still be as low as US$2-3 per additional patient appropriately treated.

80 Treatment of malaria Treatment of malaria 81
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Perceptions and impact of introducing rapid diagnostic tests in drug shops in Uganda.
LSHTM Investigators: Clare Chandler, Eleanor Hutchinson, Sian
Clarke, Kristian Hansen & Sham Lal.
External Investigators/Collaborators: Anthony Mbonye (Ministry
of Health, Kampala, Uganda); Pascal Magnussen (University of
Copenhagen, Denmark).
Funding:
through the ACT Consortium.
This research study was conducted alongside a trial in which workers in drug shops were trained to carry out
were perceived and used by the local constituents of the trial.
Twenty one focus group discussions were carried out with clients, drug shop vendors and local health facility staff. While RDTs were valued as diagnostic tools they also had unintended consequences. The availability of RDTs was interpreted as a marker of quality care, raising the overall status of drug shops in the local health care system and enabling drug shops appear to offer services similar to primary health care centres. Drug shop vendors used RDTs to demonstrate biomedical skill and increase
seller. The system of referral was largely unsuccessful in its attempt to establish a professional link between the formal health system and the drug shops.Drug shop in Mukono district, Uganda.
The role of rapid diagnostic tests for Malaria for the targeting of artemisinin-based combination therapies at community level: a cluster randomized controlled trial in Ghana.
LSHTM Investigators: Christopher Whitty.
External Investigators/Collaborators:
Funding:
Foundation through the Malaria Capacity Development Consortium.
We conducted a cluster randomized trial in the Dangme West District of Ghana among clients reporting to a chemical shop complaining of fever or requesting an
antimalarial. Shops were randomly allocated to standard practice or dispensing informed by rapid diagnostic test
double-read research slides. The proportion of slide negative clients, who received any antimalarial was
control arm, received appropriate treatment based on double-read research slide results.
Introducing rapid diagnostic tests into com-munity-based management of malaria: a cost-effectiveness analysis among community medicine distributors in two areas of high and low transmission in Uganda.
LSHTM Investigators: Kristian Hansen, Sian Clarke & Sham Lal.
External Investigators/Collaborators: Richard Ndyomugyenyi
(Ministry of Health, Kampala, Uganda); Pascal Magnussen (Univer-
sity of Copenhagen, Denmark).
Funding: -
tion through the ACT Consortium.
Treatment of malaria by trained community members has been seen as a way of increasing access to health care in remote and underserved areas. Rapid diagnostic tests
-agnosis in remote locations where community members with limited training may be able to perform RDTs and
The inSCALE Project: Integrated Community Case Management of Common Childhood Dis-eases: Mozambique and Uganda.
LSHTM Investigators -
sall, Frida Kasteng & Seyi Soremekun.
External Investigators/Collaborators: James Tibenderana (Ma-
laria Consortium Africa, Uganda); Sylvia Meek & Karin Kallander
(University of London Institute of Child Health, UK).
Funding:
Programmes involved in the integrated community case management of malaria, diarrhoea and pneumonia
health care for hard-to-reach communities. iCCM pro-
trained to diagnose and treat malaria, diarrhoea and pneumonia and to carry out preventative health activities. In order to minimise the common problems of poor super-vision and motivation, and the low retention rates that can occur in CHW programmes, a partnership of academics and public health practitioners at the London School of Hygiene & Tropical Medicine, University College London and the Malaria Consortium have designed two innova-tive intervention packages aimed at strengthening CHW
The project will evaluate the impact of providing CHWs with mobile phones and accessories (‘technology
treat accordingly.-
side a cluster-randomised trial to assess the impact of introducing RDTs to improve malaria diagnosis and treat-
sub-counties with contrasting transmission in Rukungiri District, Uganda. Costs were collected from a societal perspective. Provider costs incorporated the cost of com-munity sensitisation, training of CMDs, development of training material, allowances for CMDs and the commod-
cost was captured through interviews with a sample of patients treated by CMDs incorporating household cost of treatment-seeking for fever including the direct costs of transport, diagnosis and drugs and opportunity cost of lost time. Finally, while CMDs were unpaid volunteers, the extent of time utilised by CMDs was estimated through
of data collected is ongoing.
coverage of appropriately treated children with malaria, diarrhoea and pneumonia in Uganda and Mozambique. The interventions have been successfully implemented
-ogy intervention a total of 100 CHW supervisors and 1400
accessories to aid them in their work through digital as-sistance with diagnosis, receipt of regular motivational messages and feedback, and through free communica-
880 CHWs in Uganda are involved in the setting up and running of village health clubs which are open to all com-munity members to help raise the awareness in the com-munity of the CHW programme and to mobilise members to solve local health problems.The impact of both these additions to the iCCM programme will be assessed af-
comparison with CHWs in areas with routine iCCM in a cluster-randomised controlled design. In addition to de-termining the impact on the coverage of children who are appropriately treated for malaria, diarrhoea and pneumo-nia, we will also assess the effects of the interventions on CHW motivation, performance and retention. Information on implementation and running costs, and on the cost-effectiveness of the interventions will also be collected and analysed in order to provide complete and informed policy advice to government and academic stakeholders post-evaluation.

80 Treatment of malaria Treatment of malaria 81
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Perceptions and impact of introducing rapid diagnostic tests in drug shops in Uganda.
LSHTM Investigators: Clare Chandler, Eleanor Hutchinson, Sian
Clarke, Kristian Hansen & Sham Lal.
External Investigators/Collaborators: Anthony Mbonye (Ministry
of Health, Kampala, Uganda); Pascal Magnussen (University of
Copenhagen, Denmark).
Funding:
through the ACT Consortium.
This research study was conducted alongside a trial in which workers in drug shops were trained to carry out
were perceived and used by the local constituents of the trial.
Twenty one focus group discussions were carried out with clients, drug shop vendors and local health facility staff. While RDTs were valued as diagnostic tools they also had unintended consequences. The availability of RDTs was interpreted as a marker of quality care, raising the overall status of drug shops in the local health care system and enabling drug shops appear to offer services similar to primary health care centres. Drug shop vendors used RDTs to demonstrate biomedical skill and increase
seller. The system of referral was largely unsuccessful in its attempt to establish a professional link between the formal health system and the drug shops.Drug shop in Mukono district, Uganda.
The role of rapid diagnostic tests for Malaria for the targeting of artemisinin-based combination therapies at community level: a cluster randomized controlled trial in Ghana.
LSHTM Investigators: Christopher Whitty.
External Investigators/Collaborators:
Funding:
Foundation through the Malaria Capacity Development Consortium.
We conducted a cluster randomized trial in the Dangme West District of Ghana among clients reporting to a chemical shop complaining of fever or requesting an
antimalarial. Shops were randomly allocated to standard practice or dispensing informed by rapid diagnostic test
double-read research slides. The proportion of slide negative clients, who received any antimalarial was
control arm, received appropriate treatment based on double-read research slide results.
Introducing rapid diagnostic tests into com-munity-based management of malaria: a cost-effectiveness analysis among community medicine distributors in two areas of high and low transmission in Uganda.
LSHTM Investigators: Kristian Hansen, Sian Clarke & Sham Lal.
External Investigators/Collaborators: Richard Ndyomugyenyi
(Ministry of Health, Kampala, Uganda); Pascal Magnussen (Univer-
sity of Copenhagen, Denmark).
Funding: -
tion through the ACT Consortium.
Treatment of malaria by trained community members has been seen as a way of increasing access to health care in remote and underserved areas. Rapid diagnostic tests
-agnosis in remote locations where community members with limited training may be able to perform RDTs and
The inSCALE Project: Integrated Community Case Management of Common Childhood Dis-eases: Mozambique and Uganda.
LSHTM Investigators -
sall, Frida Kasteng & Seyi Soremekun.
External Investigators/Collaborators: James Tibenderana (Ma-
laria Consortium Africa, Uganda); Sylvia Meek & Karin Kallander
(University of London Institute of Child Health, UK).
Funding:
Programmes involved in the integrated community case management of malaria, diarrhoea and pneumonia
health care for hard-to-reach communities. iCCM pro-
trained to diagnose and treat malaria, diarrhoea and pneumonia and to carry out preventative health activities. In order to minimise the common problems of poor super-vision and motivation, and the low retention rates that can occur in CHW programmes, a partnership of academics and public health practitioners at the London School of Hygiene & Tropical Medicine, University College London and the Malaria Consortium have designed two innova-tive intervention packages aimed at strengthening CHW
The project will evaluate the impact of providing CHWs with mobile phones and accessories (‘technology
treat accordingly.-
side a cluster-randomised trial to assess the impact of introducing RDTs to improve malaria diagnosis and treat-
sub-counties with contrasting transmission in Rukungiri District, Uganda. Costs were collected from a societal perspective. Provider costs incorporated the cost of com-munity sensitisation, training of CMDs, development of training material, allowances for CMDs and the commod-
cost was captured through interviews with a sample of patients treated by CMDs incorporating household cost of treatment-seeking for fever including the direct costs of transport, diagnosis and drugs and opportunity cost of lost time. Finally, while CMDs were unpaid volunteers, the extent of time utilised by CMDs was estimated through
of data collected is ongoing.
coverage of appropriately treated children with malaria, diarrhoea and pneumonia in Uganda and Mozambique. The interventions have been successfully implemented
-ogy intervention a total of 100 CHW supervisors and 1400
accessories to aid them in their work through digital as-sistance with diagnosis, receipt of regular motivational messages and feedback, and through free communica-
880 CHWs in Uganda are involved in the setting up and running of village health clubs which are open to all com-munity members to help raise the awareness in the com-munity of the CHW programme and to mobilise members to solve local health problems.The impact of both these additions to the iCCM programme will be assessed af-
comparison with CHWs in areas with routine iCCM in a cluster-randomised controlled design. In addition to de-termining the impact on the coverage of children who are appropriately treated for malaria, diarrhoea and pneumo-nia, we will also assess the effects of the interventions on CHW motivation, performance and retention. Information on implementation and running costs, and on the cost-effectiveness of the interventions will also be collected and analysed in order to provide complete and informed policy advice to government and academic stakeholders post-evaluation.

82 Treatment of malaria Treatment of malaria 83
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Optimal price subsidies for appropriate malaria testing and treatment behaviour.
LSHTM Investigators: Kristian Hansen.
External Investigators/Collaborators: Tine Hjernø Lesner & Lars
Peter Østerdal (University of Southern Denmark, Denmark).
Funding:
Consortium.
Malaria continues to be a serious public health problem
do not receive an effective antimalarial while at the same time a large proportion of people receiving treatment for malaria does not suffer from malaria.
proposed to subsidise artemisinin-based combination
effective antimalarial available. Such a scheme
recommends that all individuals suspected of having malaria should receive a parasitological test before
research project is investigating what may be the optimal
cheaper, less effective antimalarials, a model describing health-seeking behaviour of customers with suspected malaria was developed. Preliminary results in the form of numerical simulations of this model suggest that a more optimal use of funds would be to redirect some of the
Interventions to improve community case management of malaria in sub-Saharan Africa: a systematic review.
LSHTM Investigators: Lucy Paintain, Barbara Willey, David
Schellenberg & Jayne Webster .
External Investigators/Collaborators:
Ngashi Ngongo & Alyssa Sharkey (UNICEF, USA)
Funding: UNICEF.
In total, 33 papers covering a total of 36 studies in 15
alone, 16 of these by presumptive diagnosis and 11 by
malaria CCM integrated with other basic health services.
Six main strategies emerged from the review as being important determinants of the success of malaria CCM for children:
packaging of medicines in appropriate doses
to health facility level
Due to the multi-faceted nature of many of the
directly link outcomes to individual components of the intervention. Nevertheless, all of these strategies play some part in the success of a community health worker programme and their impact if implemented in combination is likely to be greater.
Village malaria workers and the management of malaria and childhood illnesses in rural Cambodia: knowledge, perceptions, and preferences of caregivers.
LSHTM Investigators
External Investigators/Collaborators: Chea Nguon (National
Malaria Control Programme, Cambodia).
Funding: The Department for International Development through
Consortium.
trained and deployed to diagnose suspected malaria
patients to the nearest public health facility. In addition, VMWs in selected villages have also been trained to provide treatment for diarrhoea and acute respiratory
The VMW programme continues to expand but questions remain about the way in which the scaling up of interventions should be implemented and how utilisation of VMWs can be increased.
This qualitative study aimed to understand the community’s health seeking practices in one province in Cambodia. In 2013, eighty in-depth interviews were carried out with carers of children, village authorities, malaria workers, and mobile and migrant workers,
reveal tensions, limitations and opportunities that should be considered in the scaling-up of the VMW programme.
Commumnity Health Worker walking through mud with his motorcycle.Patient undergoing a rapid diagnostic test for malaria.

82 Treatment of malaria Treatment of malaria 83
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Optimal price subsidies for appropriate malaria testing and treatment behaviour.
LSHTM Investigators: Kristian Hansen.
External Investigators/Collaborators: Tine Hjernø Lesner & Lars
Peter Østerdal (University of Southern Denmark, Denmark).
Funding:
Consortium.
Malaria continues to be a serious public health problem
do not receive an effective antimalarial while at the same time a large proportion of people receiving treatment for malaria does not suffer from malaria.
proposed to subsidise artemisinin-based combination
effective antimalarial available. Such a scheme
recommends that all individuals suspected of having malaria should receive a parasitological test before
research project is investigating what may be the optimal
cheaper, less effective antimalarials, a model describing health-seeking behaviour of customers with suspected malaria was developed. Preliminary results in the form of numerical simulations of this model suggest that a more optimal use of funds would be to redirect some of the
Interventions to improve community case management of malaria in sub-Saharan Africa: a systematic review.
LSHTM Investigators: Lucy Paintain, Barbara Willey, David
Schellenberg & Jayne Webster .
External Investigators/Collaborators:
Ngashi Ngongo & Alyssa Sharkey (UNICEF, USA)
Funding: UNICEF.
In total, 33 papers covering a total of 36 studies in 15
alone, 16 of these by presumptive diagnosis and 11 by
malaria CCM integrated with other basic health services.
Six main strategies emerged from the review as being important determinants of the success of malaria CCM for children:
packaging of medicines in appropriate doses
to health facility level
Due to the multi-faceted nature of many of the
directly link outcomes to individual components of the intervention. Nevertheless, all of these strategies play some part in the success of a community health worker programme and their impact if implemented in combination is likely to be greater.
Village malaria workers and the management of malaria and childhood illnesses in rural Cambodia: knowledge, perceptions, and preferences of caregivers.
LSHTM Investigators
External Investigators/Collaborators: Chea Nguon (National
Malaria Control Programme, Cambodia).
Funding: The Department for International Development through
Consortium.
trained and deployed to diagnose suspected malaria
patients to the nearest public health facility. In addition, VMWs in selected villages have also been trained to provide treatment for diarrhoea and acute respiratory
The VMW programme continues to expand but questions remain about the way in which the scaling up of interventions should be implemented and how utilisation of VMWs can be increased.
This qualitative study aimed to understand the community’s health seeking practices in one province in Cambodia. In 2013, eighty in-depth interviews were carried out with carers of children, village authorities, malaria workers, and mobile and migrant workers,
reveal tensions, limitations and opportunities that should be considered in the scaling-up of the VMW programme.
Commumnity Health Worker walking through mud with his motorcycle.Patient undergoing a rapid diagnostic test for malaria.

84 Treatment of malaria Treatment of malaria 85
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Facility-based case management
Barriers to effectiveness: artemisinin-based combination therapies and health systems.
LSHTM Investigators: Bhargavi Rao & David Schellenberg plus
-
becca Thomson).
External Investigators/Collaborators:
Lucy Okell (Imperial College London, UK).
Funding:
through the ACT Consortium.
--
pered by weak health systems and a poorly controlled
-sion model to include dimensions of access to sources of
in order to estimate the impact of overcoming health sys-tems barriers on malaria mortality and transmission risk. We parameterised out model using data from 3 different
We found that systems interventions resulted in
proportionately greater clinical impact than epidemiologi-cal, with the greatest relative impact at low transmission settings. Modelling policies such as the rollout of rapid
prevalence despite reducing treatment of non-malarial
uncomplicated malaria and reducing transmission. How-ever investment would be required across case manage-ment in the private sector to improve the quality of care delivered. The impact of packages of systems interven-tions was highly dependent on existing health systems provision and population references as well as epidemi-
-prove progress towards targets set by Roll Back malaria or to approach elimination.
Future work will include including considerations of cost-effectiveness, synergies with other control interven-tions and modelling appropriate treatment for NMFI. We
-ments at a local level and consider the application of this model in unstable and elimination settings.
IMPACT2: evaluating policies in Tanzania to improve malaria diagnosis and treatment.
LSHTM Investigators
Rebecca Thomson & Matthew Cairns.
External Investigators/Collaborators: Patrick Kachur, Denise
Roth Allen & Melissa Briggs (US Centers for Disease Control and
Prevention, USA); Salim Abdulla, Admirabilis Kalolella, Charles
Festo, Boniface Johanes, Happy Nchimbi & Clarence Mkoba
(Ifakara Health Institute, Tanzania).
Funding:
Consortium.
This set of evaluation studies assesses the effectiveness of two policies implemented by the government of Tanzania to improve the accessibility and targeting of malaria treatment.
Quantitative surveys and qualitative methods were used in public health facilities, antimalarial outlets and households to assess the impact of these initiatives on treatment availability, affordability, targeting and use. The effect of text message reminders targeted at drug shop
dispensers to improve patients’ adherence to treatment was studied as part of a cluster randomised controlled trial.
The study has highlighted some key implications for policy:
appropriateness of antimalarial provision in public facilities. However, public sector stockouts of drugs and diagnostics are a key challenge for successful implementation of malaria control
subsidies are an effective way to improve availability, reduce price and increase market share of quality
shops, further investigation is required of steps to improve quality of care in these outlets
and private outlets, but the text message reminder intervention did not improve adherence among private sector clients, highlighting the need for further intervention development
We carry out a number of studies in health facilities including several large randomised control trials of interventions aimed at improving malaria diagnosis and treatment through health facilities in Africa and Asia.
Mobilize Against Malaria: interventions to im-prove the delivery of rtemisinin-based com-bination therapies in Ghana, Kenya and Sen-egal.
LSHTM Investigators: Jayne Webster, Caroline Jones, Jane Bruce,
Lucy Paintain, Alexandra Hyde & Manuela Claite.
External Investigators/Collaborators: Kwame Adogboba, Nana
Enyimayew, Sofo Ali, Kwadwo Koram & David Ofori-Adjei (Health
Diallo (IntraHealth Senegal).
Funding:
and 20012 by partners in Ghana, Kenya and Senegal. The aim of the programme was to reduce malaria morbid-ity and mortality through the implementation of different models of delivery of artemisinin-based combination ther-apies through retail, public and community sectors.
The study has demonstrated the viability of improved
and maintaining community-run health huts in Senegal and tested the effectiveness of health worker training and mass communications in Kenya.
Cross cutting issues emerging from the opportunity of having conducted evaluations across three delivery mod-els in three sectors of three countries are in process and will be completed in 2014
Health worker carries out malaria rapid diagnostic test with child in Tanzania.

84 Treatment of malaria Treatment of malaria 85
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Facility-based case management
Barriers to effectiveness: artemisinin-based combination therapies and health systems.
LSHTM Investigators: Bhargavi Rao & David Schellenberg plus
-
becca Thomson).
External Investigators/Collaborators:
Lucy Okell (Imperial College London, UK).
Funding:
through the ACT Consortium.
--
pered by weak health systems and a poorly controlled
-sion model to include dimensions of access to sources of
in order to estimate the impact of overcoming health sys-tems barriers on malaria mortality and transmission risk. We parameterised out model using data from 3 different
We found that systems interventions resulted in
proportionately greater clinical impact than epidemiologi-cal, with the greatest relative impact at low transmission settings. Modelling policies such as the rollout of rapid
prevalence despite reducing treatment of non-malarial
uncomplicated malaria and reducing transmission. How-ever investment would be required across case manage-ment in the private sector to improve the quality of care delivered. The impact of packages of systems interven-tions was highly dependent on existing health systems provision and population references as well as epidemi-
-prove progress towards targets set by Roll Back malaria or to approach elimination.
Future work will include including considerations of cost-effectiveness, synergies with other control interven-tions and modelling appropriate treatment for NMFI. We
-ments at a local level and consider the application of this model in unstable and elimination settings.
IMPACT2: evaluating policies in Tanzania to improve malaria diagnosis and treatment.
LSHTM Investigators
Rebecca Thomson & Matthew Cairns.
External Investigators/Collaborators: Patrick Kachur, Denise
Roth Allen & Melissa Briggs (US Centers for Disease Control and
Prevention, USA); Salim Abdulla, Admirabilis Kalolella, Charles
Festo, Boniface Johanes, Happy Nchimbi & Clarence Mkoba
(Ifakara Health Institute, Tanzania).
Funding:
Consortium.
This set of evaluation studies assesses the effectiveness of two policies implemented by the government of Tanzania to improve the accessibility and targeting of malaria treatment.
Quantitative surveys and qualitative methods were used in public health facilities, antimalarial outlets and households to assess the impact of these initiatives on treatment availability, affordability, targeting and use. The effect of text message reminders targeted at drug shop
dispensers to improve patients’ adherence to treatment was studied as part of a cluster randomised controlled trial.
The study has highlighted some key implications for policy:
appropriateness of antimalarial provision in public facilities. However, public sector stockouts of drugs and diagnostics are a key challenge for successful implementation of malaria control
subsidies are an effective way to improve availability, reduce price and increase market share of quality
shops, further investigation is required of steps to improve quality of care in these outlets
and private outlets, but the text message reminder intervention did not improve adherence among private sector clients, highlighting the need for further intervention development
We carry out a number of studies in health facilities including several large randomised control trials of interventions aimed at improving malaria diagnosis and treatment through health facilities in Africa and Asia.
Mobilize Against Malaria: interventions to im-prove the delivery of rtemisinin-based com-bination therapies in Ghana, Kenya and Sen-egal.
LSHTM Investigators: Jayne Webster, Caroline Jones, Jane Bruce,
Lucy Paintain, Alexandra Hyde & Manuela Claite.
External Investigators/Collaborators: Kwame Adogboba, Nana
Enyimayew, Sofo Ali, Kwadwo Koram & David Ofori-Adjei (Health
Diallo (IntraHealth Senegal).
Funding:
and 20012 by partners in Ghana, Kenya and Senegal. The aim of the programme was to reduce malaria morbid-ity and mortality through the implementation of different models of delivery of artemisinin-based combination ther-apies through retail, public and community sectors.
The study has demonstrated the viability of improved
and maintaining community-run health huts in Senegal and tested the effectiveness of health worker training and mass communications in Kenya.
Cross cutting issues emerging from the opportunity of having conducted evaluations across three delivery mod-els in three sectors of three countries are in process and will be completed in 2014
Health worker carries out malaria rapid diagnostic test with child in Tanzania.

86 Treatment of malaria Treatment of malaria 87
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
REACT Cameroon: cost-effectiveness of interventions to support the introduction of malaria rapid diagnostic tests in Cameroon.
LSHTM Investigators
Jefferies, Bonnie Cundill & Clare Chandler.
External Investigators/Collaborators: Wilfred Mbacham, Olivia
Obinna Onwujekwe (University of Nigeria, Nigeria).
Funding:
Consortium.
This 3-arm cluster randomised trial aims to support the use of rapid diagnostic tests and adherence to their results in Cameroon.
We worked with the Ministry of Health to design basic and enhanced rapid diagnostic test training courses. Both trainings explained how to use the test and how to treat uncomplicated malaria. The enhanced course contained additional interactive methods – such as drama and problem solving exercises – to encourage health workers
to test for malaria and to prescribe treatment based on the results.
We have published papers that describe problems in malaria case management: malaria testing was available but under-used and many health workers prefer to prescribe an antimalarial even if the malaria test has a negative result.
In addition, we are submitting effectiveness and cost-
being prepared, including one that describes the process of designing and implementing the interventions.
provide an important basis for comparison across different
well as different treatment seeking practices by ethnic and socioeconomic groups. Perhaps most interesting, these intervention trials will allow comparison between sites where currently microscopy testing is widely available
Card games as part of training to use malaria rapid diagnostic tests.
REACT Nigeria: costs and effects of strategies to improve malaria diagnosis and treatment in Nigeria.
LSHTM Investigators
Jefferies, Bonnie Cundill & Clare Chandler.
External Investigators/Collaborators: Obinna Onwujekwe,
BSC Uzochukwu, Ogo Ibe, Emmanuel Nwala, Eloka Uchegbu &
Chinelo Enemuo (University of Nigeria, Nigeria); Wilfred Mbacham
Funding:
Consortium.
This cluster randomised trial aims to assist Nigerian policy-makers in deciding which types of provider and community interventions should support the roll-out of rapid diagnostic tests in Nigeria, especially in the private sector which is a major source of malaria treatment in the country.
Working with the state malaria control programme,
selected public health centres, pharmacies and drug stores. In the control arm, the tests were supplied and providers were shown how they should be used. In the
provider intervention arm, rapid diagnostic tests were also supplied and providers received two-day training and monthly support visits. In the third arm, the provider intervention was supplemented by a school-based programme to raise community awareness about malaria, RDTs and artemisinin-based combination therapies as the recommended antimalarial.
The research team have published papers that describe problems in malaria case management: malaria testing was available but under-used and many health workers prefer to prescribe an antimalarial even if the malaria test has a negative result. We also published a study protocol. In addition, the team is conducting the
provide an important basis for comparison across different
and different treatment seeking practices by ethnic and socioeconomic groups. Perhaps most interesting, these intervention trials will allow comparison between sites where currently microscopy testing is widely available
Comparing adherence to artemisinin-based combination therapies for the treatment of uncomplicated malaria in Freetown, Sierra Leone.
LSHTM Investigators: Kristin Banek, Clare Chandler, Toby Leslie,
Daniel Chandramohan & Sarah Staedke.
External Investigators/Collaborators: Samuel Juana Smith, Anitta
Kamara & Musa Sillah Kanu (National Malaria Control Programme,
Sierra Leone).
Funding: This study was primarily self-funded. Amodiaquine-
Fund through the National Malaria Control Program. Equipment
Scholarship. Kristin Banek is supported by an American Association
of University Women Dissertation Fellowship.
Increasing access to and targeting of artemisinin-based
ensure adequate treatment outcomes, health worker and patient/caregiver adherence to treatment guidelines is essential.
This was an open-labelled randomised controlled study conducted in two public health facilities in urban Freetown, Sierra Leone with the aim to measure and compare the level of provider compliance with malaria treatment guidelines and patient/caregiver adherence to
facilities for the treatment of fever were randomised to
of prescription. Health worker compliance to treatment guidelines were assessed through direct observation and interviews. Caregivers’ adherence to the prescribed drugs and factors associated with adherence were assessed though short exit interviews at the health facility and during follow-up at their home on day four post-prescription.
The study took place between July 2013 and January
inclusion criteria and were enrolled in the study, of which
on-going and results are expected to be available by late 2014.

86 Treatment of malaria Treatment of malaria 87
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
REACT Cameroon: cost-effectiveness of interventions to support the introduction of malaria rapid diagnostic tests in Cameroon.
LSHTM Investigators
Jefferies, Bonnie Cundill & Clare Chandler.
External Investigators/Collaborators: Wilfred Mbacham, Olivia
Obinna Onwujekwe (University of Nigeria, Nigeria).
Funding:
Consortium.
This 3-arm cluster randomised trial aims to support the use of rapid diagnostic tests and adherence to their results in Cameroon.
We worked with the Ministry of Health to design basic and enhanced rapid diagnostic test training courses. Both trainings explained how to use the test and how to treat uncomplicated malaria. The enhanced course contained additional interactive methods – such as drama and problem solving exercises – to encourage health workers
to test for malaria and to prescribe treatment based on the results.
We have published papers that describe problems in malaria case management: malaria testing was available but under-used and many health workers prefer to prescribe an antimalarial even if the malaria test has a negative result.
In addition, we are submitting effectiveness and cost-
being prepared, including one that describes the process of designing and implementing the interventions.
provide an important basis for comparison across different
well as different treatment seeking practices by ethnic and socioeconomic groups. Perhaps most interesting, these intervention trials will allow comparison between sites where currently microscopy testing is widely available
Card games as part of training to use malaria rapid diagnostic tests.
REACT Nigeria: costs and effects of strategies to improve malaria diagnosis and treatment in Nigeria.
LSHTM Investigators
Jefferies, Bonnie Cundill & Clare Chandler.
External Investigators/Collaborators: Obinna Onwujekwe,
BSC Uzochukwu, Ogo Ibe, Emmanuel Nwala, Eloka Uchegbu &
Chinelo Enemuo (University of Nigeria, Nigeria); Wilfred Mbacham
Funding:
Consortium.
This cluster randomised trial aims to assist Nigerian policy-makers in deciding which types of provider and community interventions should support the roll-out of rapid diagnostic tests in Nigeria, especially in the private sector which is a major source of malaria treatment in the country.
Working with the state malaria control programme,
selected public health centres, pharmacies and drug stores. In the control arm, the tests were supplied and providers were shown how they should be used. In the
provider intervention arm, rapid diagnostic tests were also supplied and providers received two-day training and monthly support visits. In the third arm, the provider intervention was supplemented by a school-based programme to raise community awareness about malaria, RDTs and artemisinin-based combination therapies as the recommended antimalarial.
The research team have published papers that describe problems in malaria case management: malaria testing was available but under-used and many health workers prefer to prescribe an antimalarial even if the malaria test has a negative result. We also published a study protocol. In addition, the team is conducting the
provide an important basis for comparison across different
and different treatment seeking practices by ethnic and socioeconomic groups. Perhaps most interesting, these intervention trials will allow comparison between sites where currently microscopy testing is widely available
Comparing adherence to artemisinin-based combination therapies for the treatment of uncomplicated malaria in Freetown, Sierra Leone.
LSHTM Investigators: Kristin Banek, Clare Chandler, Toby Leslie,
Daniel Chandramohan & Sarah Staedke.
External Investigators/Collaborators: Samuel Juana Smith, Anitta
Kamara & Musa Sillah Kanu (National Malaria Control Programme,
Sierra Leone).
Funding: This study was primarily self-funded. Amodiaquine-
Fund through the National Malaria Control Program. Equipment
Scholarship. Kristin Banek is supported by an American Association
of University Women Dissertation Fellowship.
Increasing access to and targeting of artemisinin-based
ensure adequate treatment outcomes, health worker and patient/caregiver adherence to treatment guidelines is essential.
This was an open-labelled randomised controlled study conducted in two public health facilities in urban Freetown, Sierra Leone with the aim to measure and compare the level of provider compliance with malaria treatment guidelines and patient/caregiver adherence to
facilities for the treatment of fever were randomised to
of prescription. Health worker compliance to treatment guidelines were assessed through direct observation and interviews. Caregivers’ adherence to the prescribed drugs and factors associated with adherence were assessed though short exit interviews at the health facility and during follow-up at their home on day four post-prescription.
The study took place between July 2013 and January
inclusion criteria and were enrolled in the study, of which
on-going and results are expected to be available by late 2014.

88 Treatment of malaria Treatment of malaria 89
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Cost-effectiveness analysis of introducing rapid diagnostic tests for malaria diagnosis as compared to microscopy and presumptive diagnosis in public health centres in Ghana.
LSHTM Investigators: Kristian Hansen, Christopher Whitty &
External Investigators/Collaborators: Evelyn Ansah & Michael
Funding:
Consortium.
The present research project assessed the cost-effectiveness of introducing malaria rapid diagnostic tests
which is a rural area of Ghana. In one setting, the population had access to a health
centre with a microscope and suspected malaria patients
were randomly assigned to a diagnosis by either an RDT or a microscopy and subsequent treatment by health centre staff. In the other setting, the population had access to health centres without a microscope and suspected malaria patients were randomly assigned to diagnosis by an RDT or based on clinical signs. Cost of offering diagnostic services and outpatient services in three public health centres was collected as well as the household cost of treatment-seeking. It was found that the introduction of RDTs increased the proportion of patients who were correctly treated in relation to treatment with antimalarials, from 42% to 65% at an incremental societal
patient in the setting where malaria diagnosis was currently presumptive. In the setting where the health centre had a microscope, there was no advantage to replacing microscopy by RDT as the cost and proportion of correctly treated patients were similar.
Comparative cost-effectiveness of malaria rapid diagnostic tests, microscopy and presumptive diagnosis in public health centres in Afghanistan.
LSHTM Investigators
& Mark Rowland.
External Investigators/Collaborators: Ismail Mayan, Nader
Mohammed & Asif Alokozai (Health Protection and Research
Organisation, Afghanistan); Mohammed Anwar (HealthNet TPO,
Jalalabad, Afghanistan); Sayed Bakhtash (Merling, Kunduz,
Afghanistan).
Funding:
Consortium.
The study was conducted within a randomised trial of three different approaches to malaria diagnosis. The
for malaria and the control arms were either microscopy or clinical diagnosis based on signs and symptoms alone. We enrolled around 6000 patients in the study and assessed the proportion of patients with fever who were appropriately treated for malaria.
appropriate malaria drug, and those with no malaria not receiving any antimalarial drug. We also examined the use of antibiotics and other treatments.
costs of each approach to identify which approach was the most cost-effective. These included costs to the health service (including training, staff time, commodities,
Initial analysis indicates that RDTs are cost-effective when compared to microscopy or clinical diagnosis in low and moderate transmission settings. The result will
roll out RDTs.
Training Afghan health workers on the use of malaria rapid diagnostic tests. Photo: Sayed Bakhtash.
Strategies for expanding access to quality malaria diagnosis in south-central Asia where malaria incidence is low.
LSHTM Investigators: Mark Rowland, Toby Leslie, Chris Whitty &
Amy Mikhail.
External Investigators/Collaborators: Ismail Mayan (Health
Protection and Research Organization, Afghanistan) Nader
Mohammed & Anwar Hasanzai (HealthNet-TPO, Afghanistan);
Sayed Habib Baktash (Medical Emergency Relief International,
Afghanistan).
Funding:
Consortium.
Diagnosis is unavailable in most places where fever is common, so clinicians cannot distinguish the symptoms of malaria from other causes of fever. This results in a huge
overtreatment of malaria. We conducted a series of studies to test how effective
different diagnostic and treatment methods are under
treating malaria.First, we tested the accuracy of a rapid test that can
distinguish the two malaria species and accurately identify negative patients. We found that one brand was the most accurate, and this was subsequently introduced as the
We then conducted two randomised trials, one in clinics and one amongst community health workers, comparing the use of rapid diagnostic tests and microscopy. These studies will provide robust evidence for the most effective diagnostic tool, and allow both clinicians and community health workers to apply malaria treatments according to diagnostic results.
Health worker carries out parasitological diagnosis of malaria in Afghanistan.

88 Treatment of malaria Treatment of malaria 89
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Cost-effectiveness analysis of introducing rapid diagnostic tests for malaria diagnosis as compared to microscopy and presumptive diagnosis in public health centres in Ghana.
LSHTM Investigators: Kristian Hansen, Christopher Whitty &
External Investigators/Collaborators: Evelyn Ansah & Michael
Funding:
Consortium.
The present research project assessed the cost-effectiveness of introducing malaria rapid diagnostic tests
which is a rural area of Ghana. In one setting, the population had access to a health
centre with a microscope and suspected malaria patients
were randomly assigned to a diagnosis by either an RDT or a microscopy and subsequent treatment by health centre staff. In the other setting, the population had access to health centres without a microscope and suspected malaria patients were randomly assigned to diagnosis by an RDT or based on clinical signs. Cost of offering diagnostic services and outpatient services in three public health centres was collected as well as the household cost of treatment-seeking. It was found that the introduction of RDTs increased the proportion of patients who were correctly treated in relation to treatment with antimalarials, from 42% to 65% at an incremental societal
patient in the setting where malaria diagnosis was currently presumptive. In the setting where the health centre had a microscope, there was no advantage to replacing microscopy by RDT as the cost and proportion of correctly treated patients were similar.
Comparative cost-effectiveness of malaria rapid diagnostic tests, microscopy and presumptive diagnosis in public health centres in Afghanistan.
LSHTM Investigators
& Mark Rowland.
External Investigators/Collaborators: Ismail Mayan, Nader
Mohammed & Asif Alokozai (Health Protection and Research
Organisation, Afghanistan); Mohammed Anwar (HealthNet TPO,
Jalalabad, Afghanistan); Sayed Bakhtash (Merling, Kunduz,
Afghanistan).
Funding:
Consortium.
The study was conducted within a randomised trial of three different approaches to malaria diagnosis. The
for malaria and the control arms were either microscopy or clinical diagnosis based on signs and symptoms alone. We enrolled around 6000 patients in the study and assessed the proportion of patients with fever who were appropriately treated for malaria.
appropriate malaria drug, and those with no malaria not receiving any antimalarial drug. We also examined the use of antibiotics and other treatments.
costs of each approach to identify which approach was the most cost-effective. These included costs to the health service (including training, staff time, commodities,
Initial analysis indicates that RDTs are cost-effective when compared to microscopy or clinical diagnosis in low and moderate transmission settings. The result will
roll out RDTs.
Training Afghan health workers on the use of malaria rapid diagnostic tests. Photo: Sayed Bakhtash.
Strategies for expanding access to quality malaria diagnosis in south-central Asia where malaria incidence is low.
LSHTM Investigators: Mark Rowland, Toby Leslie, Chris Whitty &
Amy Mikhail.
External Investigators/Collaborators: Ismail Mayan (Health
Protection and Research Organization, Afghanistan) Nader
Mohammed & Anwar Hasanzai (HealthNet-TPO, Afghanistan);
Sayed Habib Baktash (Medical Emergency Relief International,
Afghanistan).
Funding:
Consortium.
Diagnosis is unavailable in most places where fever is common, so clinicians cannot distinguish the symptoms of malaria from other causes of fever. This results in a huge
overtreatment of malaria. We conducted a series of studies to test how effective
different diagnostic and treatment methods are under
treating malaria.First, we tested the accuracy of a rapid test that can
distinguish the two malaria species and accurately identify negative patients. We found that one brand was the most accurate, and this was subsequently introduced as the
We then conducted two randomised trials, one in clinics and one amongst community health workers, comparing the use of rapid diagnostic tests and microscopy. These studies will provide robust evidence for the most effective diagnostic tool, and allow both clinicians and community health workers to apply malaria treatments according to diagnostic results.
Health worker carries out parasitological diagnosis of malaria in Afghanistan.

90 Treatment of malaria Treatment of malaria 91
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The effectiveness of interventions delivered at scale to improve the delivery of health services by front-line workers in low-income countries: a systematic review.
LSHTM Investigators: Barbara Willey, Joanna Schellenberg,
Lindsay Mangham-Jeffries & Lucy Paintain.
External Investigators/Collaborators: Josip Car (Imperial College
London, UK).
Funding: The Department for International Development.
The aim of this study was to identify evidence for the effectiveness of interventions to strengthen national health service delivery in countries with low and lower-middle incomes. The focus was on supply-side interventions to improve the ability of front-line workers to deliver health services, including treatment of malaria,
and evidence from evaluations of interventions delivered at scale.
In total, 21 papers covering 12 studies were included, eight of which had a malaria focus. The evidence base for
for survival impact was limited to two studies of IMCI; both found weak evidence of a positive effect on under-5
Between-study heterogeneity precluded meta-analysis. However, studies which strengthened other elements of the health service delivery in addition to technical guidance, as well as community mobilisation and interventions at the health sector policy and strategic management level showed more consistent improvement on quality of care and counselling than those using technical guidance alone.
Availability of evidence from a systematic review of the effectiveness of supply-side interventions to improve health services in low and middle income countries.
evaluating the impact of an intervention implemented in public health centres on management of malaria and health outcomes of children using a cluster-randomised design in Tororo, Uganda.
LSHTM Investigators: Sarah Staedke & Clare Chandler.
External Investigators/Collaborators: Moses Kamya (Makerere
California, San Francisco, USA).
Funding:
Consortium.
The PRIME study was designed to evaluate the impact of an intervention delivered at public health centres in Tororo, Uganda.
Twenty lower-level public health centres were included in this cluster-randomised trial; 10 were randomly assigned to the intervention and 10 to control. The intervention had four components including:
evaluation, was also conducted alongside the main
understanding about why the PRIME intervention is effective, or not.
Formative research was done in 2009-2010. The
Evaluation activities were conducted from 2010 to 2013. The PRIME intervention was implemented
successfully, although not all health workers received the training. The intervention appeared to improve malaria case management, communication between health workers and patients, and patient satisfaction with care.
impact on health outcomes of community children. Introducing RDTs did not appear to change treatment of malaria or fever outcomes in this very high malaria transmission setting.
Health workers receive training to use malaria rapid diagnostic tests.

90 Treatment of malaria Treatment of malaria 91
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
The effectiveness of interventions delivered at scale to improve the delivery of health services by front-line workers in low-income countries: a systematic review.
LSHTM Investigators: Barbara Willey, Joanna Schellenberg,
Lindsay Mangham-Jeffries & Lucy Paintain.
External Investigators/Collaborators: Josip Car (Imperial College
London, UK).
Funding: The Department for International Development.
The aim of this study was to identify evidence for the effectiveness of interventions to strengthen national health service delivery in countries with low and lower-middle incomes. The focus was on supply-side interventions to improve the ability of front-line workers to deliver health services, including treatment of malaria,
and evidence from evaluations of interventions delivered at scale.
In total, 21 papers covering 12 studies were included, eight of which had a malaria focus. The evidence base for
for survival impact was limited to two studies of IMCI; both found weak evidence of a positive effect on under-5
Between-study heterogeneity precluded meta-analysis. However, studies which strengthened other elements of the health service delivery in addition to technical guidance, as well as community mobilisation and interventions at the health sector policy and strategic management level showed more consistent improvement on quality of care and counselling than those using technical guidance alone.
Availability of evidence from a systematic review of the effectiveness of supply-side interventions to improve health services in low and middle income countries.
evaluating the impact of an intervention implemented in public health centres on management of malaria and health outcomes of children using a cluster-randomised design in Tororo, Uganda.
LSHTM Investigators: Sarah Staedke & Clare Chandler.
External Investigators/Collaborators: Moses Kamya (Makerere
California, San Francisco, USA).
Funding:
Consortium.
The PRIME study was designed to evaluate the impact of an intervention delivered at public health centres in Tororo, Uganda.
Twenty lower-level public health centres were included in this cluster-randomised trial; 10 were randomly assigned to the intervention and 10 to control. The intervention had four components including:
evaluation, was also conducted alongside the main
understanding about why the PRIME intervention is effective, or not.
Formative research was done in 2009-2010. The
Evaluation activities were conducted from 2010 to 2013. The PRIME intervention was implemented
successfully, although not all health workers received the training. The intervention appeared to improve malaria case management, communication between health workers and patients, and patient satisfaction with care.
impact on health outcomes of community children. Introducing RDTs did not appear to change treatment of malaria or fever outcomes in this very high malaria transmission setting.
Health workers receive training to use malaria rapid diagnostic tests.

92 Treatment of malaria Treatment of malaria 93
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Targeting artemisinin-based combination therapiy drugs to patients with a positive result with a malaria rapid diagnostic test in Ghana.
LSHTM Investigators: Daniel Chandramohan, Jayne Webster &
Jane Bruce.
External Investigators/Collaborators: Seth Owusu-Agyei & Frank
Funding:
In this study we have tested the effects of providing
patients who had a positive result in a rapid diagnostic test.
This approach could improve the treatment of malaria, as well as support health services to better
example is pneumonia, which is often misdiagnosed as malaria in children. Finally, this system could also reduce the use of anti-malarials and the risk of developing drug resistance.
We have assessed the accuracy of rapid diagnostic tests and the outcomes of treatment based on rapid diagnostic test results in 32 health facilities. The team conducted interviews with health providers to understand their diagnostic and treatment decisions, as well as exit
presenting fever to assess their satisfaction with the treatment received.
This study has made it possible for us to know with greater certainty the effect of restricting antimalarial to
how frequently they will get malaria or anaemia, and how this will impact on the prescriptions of other drugs.
A health worker performs malaria rapid diagnostic test.
Targeting artemisinin-based combination therapy drugs in Tanzania: the TACT trial.
LSHTM Investigators: Hugh Reyburn, Christopher Whitty & Clare
Chandler.
External Investigators/Collaborators: Renata Mandike (Malaria
Control Programme, Tanzania); Hilda Mbakilwa, (Joint Malaria
Programme, Tanzania); Raimos Olomi (Kilimanjaro Christian Medical
Centre, Tanzania); Steven Magesa (National Institute for Medical
Research, Tanzania).
Funding:
Consortium.
Because of their accuracy, rapid diagnostic tests are a potential cost-effective solution for malaria overdiagnosis. However, this method only works if health professionals
Training to improve use of malaria diagnostic tools, Tanzania.
are trained and supervised.
that may be useful in improving both the management of malaria cases and the treatment of other diseases that also cause fever. The control group of facilities received rapid diagnostic tests and basic training in how to use
at the workplace, messages from senior staff and monthly
workers and community members with the same package as well as a community-based intervention to modify the expectations of patients.

92 Treatment of malaria Treatment of malaria 93
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Targeting artemisinin-based combination therapiy drugs to patients with a positive result with a malaria rapid diagnostic test in Ghana.
LSHTM Investigators: Daniel Chandramohan, Jayne Webster &
Jane Bruce.
External Investigators/Collaborators: Seth Owusu-Agyei & Frank
Funding:
In this study we have tested the effects of providing
patients who had a positive result in a rapid diagnostic test.
This approach could improve the treatment of malaria, as well as support health services to better
example is pneumonia, which is often misdiagnosed as malaria in children. Finally, this system could also reduce the use of anti-malarials and the risk of developing drug resistance.
We have assessed the accuracy of rapid diagnostic tests and the outcomes of treatment based on rapid diagnostic test results in 32 health facilities. The team conducted interviews with health providers to understand their diagnostic and treatment decisions, as well as exit
presenting fever to assess their satisfaction with the treatment received.
This study has made it possible for us to know with greater certainty the effect of restricting antimalarial to
how frequently they will get malaria or anaemia, and how this will impact on the prescriptions of other drugs.
A health worker performs malaria rapid diagnostic test.
Targeting artemisinin-based combination therapy drugs in Tanzania: the TACT trial.
LSHTM Investigators: Hugh Reyburn, Christopher Whitty & Clare
Chandler.
External Investigators/Collaborators: Renata Mandike (Malaria
Control Programme, Tanzania); Hilda Mbakilwa, (Joint Malaria
Programme, Tanzania); Raimos Olomi (Kilimanjaro Christian Medical
Centre, Tanzania); Steven Magesa (National Institute for Medical
Research, Tanzania).
Funding:
Consortium.
Because of their accuracy, rapid diagnostic tests are a potential cost-effective solution for malaria overdiagnosis. However, this method only works if health professionals
Training to improve use of malaria diagnostic tools, Tanzania.
are trained and supervised.
that may be useful in improving both the management of malaria cases and the treatment of other diseases that also cause fever. The control group of facilities received rapid diagnostic tests and basic training in how to use
at the workplace, messages from senior staff and monthly
workers and community members with the same package as well as a community-based intervention to modify the expectations of patients.

94 Malaria moving forward Malaria moving forward 95
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Malaria Centre members are actively involved in research to set future priorities for malaria control and development.
The role of surveillance, monitoring and evalua-
-
sential to improved malaria control and eventual
number of metrics have been used to measure
the intensity of malaria transmission including
the revitalisation of the approach of using serol-
ogy to gain insights into the dynamics of malaria
various measures and a study from Uganda eval-
uates operational experience of using different
approaches. Malaria Centre members also rec-
ognise the increasing importance of school-age
-
other approach to assessing malaria transmission
which are resistant to the currently recommended
importance of surveillance for drug resistance and
a framework for decision-making to improve ma-
laria control in the context of resistance.
There is growing appreciation of the importance
of sub-patent malaria infections – that is infections
which are below the detectable limit of conven-
– as a pool for the reservoir of malaria transmis-
sion. Work in the Philippines and Burkina Faso
has attempted to understand the extent to which
sub-patent infections contribute to transmission.
The recognition in recent years that Plasmodium
knowlesi
has lead to extensive epidemiological studies in
Malaysia and the use of mathematical model-
transmission.
-
neous nature of its transmission becomes in-
creasingly apparent. Understanding how to iden-
tify foci of transmission is important for targeting
control activities. Malaria control in boarder areas
is a particular challenge and operational studies
involving cross-border transmission control have
been conducted in Namibia, informed by studies
of population movement based on data from mo-
bile phones.
-
ingly apparent that non-malaria considerations
will impact the effectiveness and acceptability of
control strategies. The roll-out of RDTs means
alike have to accept that not all fevers are due to
malaria. It becomes important to identify the non-
malaria causes of fever and to understand how
targeted malaria control likely to improve.
The importance for effective malaria control
of development of whole economies is becom-
ing clear through macro-economic modeling. The
challenge of eliminating malaria, even on a small
island, is being captured through operational re-
search in Bioko Island. Malaria is recognised as
a cause of poverty but also a result of poverty.
Malaria Centre members are also evaluating the
extent to which socio-economic development can
be considered an intervention against malaria and
are taking a multi-sectoral approach to framing
control of this disease.
The last decade has seen major gains in ma-
laria control, leading to increased coverage of key
interventions and a corresponding decrease in
the incidence of malaria disease and death. How-
ever, these changes have not been consistent
across different settings, and the role of socio-
economic development in shaping disease bur-
den remains clear. The future of malaria control
therefore requires a multi-sectoral and focalized
approach to intervention, which can be guided
by careful observation of changes and hot spots
in disease transmission. The roll-out of RDTs
and mobile telephony sets the scene for step-
improves, it will become increasingly important to
understand the utility of novel markers of malaria
transmission through surveillance and response
systems. It will be important to understand the
broad economic health and social determinants
this information is transmitted to key policy mak-
ers at global and national levels.

94 Malaria moving forward Malaria moving forward 95
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Summary
Malaria Centre members are actively involved in research to set future priorities for malaria control and development.
The role of surveillance, monitoring and evalua-
-
sential to improved malaria control and eventual
number of metrics have been used to measure
the intensity of malaria transmission including
the revitalisation of the approach of using serol-
ogy to gain insights into the dynamics of malaria
various measures and a study from Uganda eval-
uates operational experience of using different
approaches. Malaria Centre members also rec-
ognise the increasing importance of school-age
-
other approach to assessing malaria transmission
which are resistant to the currently recommended
importance of surveillance for drug resistance and
a framework for decision-making to improve ma-
laria control in the context of resistance.
There is growing appreciation of the importance
of sub-patent malaria infections – that is infections
which are below the detectable limit of conven-
– as a pool for the reservoir of malaria transmis-
sion. Work in the Philippines and Burkina Faso
has attempted to understand the extent to which
sub-patent infections contribute to transmission.
The recognition in recent years that Plasmodium
knowlesi
has lead to extensive epidemiological studies in
Malaysia and the use of mathematical model-
transmission.
-
neous nature of its transmission becomes in-
creasingly apparent. Understanding how to iden-
tify foci of transmission is important for targeting
control activities. Malaria control in boarder areas
is a particular challenge and operational studies
involving cross-border transmission control have
been conducted in Namibia, informed by studies
of population movement based on data from mo-
bile phones.
-
ingly apparent that non-malaria considerations
will impact the effectiveness and acceptability of
control strategies. The roll-out of RDTs means
alike have to accept that not all fevers are due to
malaria. It becomes important to identify the non-
malaria causes of fever and to understand how
targeted malaria control likely to improve.
The importance for effective malaria control
of development of whole economies is becom-
ing clear through macro-economic modeling. The
challenge of eliminating malaria, even on a small
island, is being captured through operational re-
search in Bioko Island. Malaria is recognised as
a cause of poverty but also a result of poverty.
Malaria Centre members are also evaluating the
extent to which socio-economic development can
be considered an intervention against malaria and
are taking a multi-sectoral approach to framing
control of this disease.
The last decade has seen major gains in ma-
laria control, leading to increased coverage of key
interventions and a corresponding decrease in
the incidence of malaria disease and death. How-
ever, these changes have not been consistent
across different settings, and the role of socio-
economic development in shaping disease bur-
den remains clear. The future of malaria control
therefore requires a multi-sectoral and focalized
approach to intervention, which can be guided
by careful observation of changes and hot spots
in disease transmission. The roll-out of RDTs
and mobile telephony sets the scene for step-
improves, it will become increasingly important to
understand the utility of novel markers of malaria
transmission through surveillance and response
systems. It will be important to understand the
broad economic health and social determinants
this information is transmitted to key policy mak-
ers at global and national levels.

96 Malaria moving forward Malaria moving forward 97
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
On the estimation of malaria transmission intensity using serology data.
LSHTM Investigators: Nuno Sepúlveda &
Chris Drakeley.
Funding: The Wellcome Trust.
Malaria transmission intensity is typi-cally assessed by parasite preva-lence or entomological infection rate.
seroprevalence data of parasite spe-
catalytic models.In this modelling approach, the
individuals become seropositive upon parasite exposure and may revert to a seronegative state after parasite clearance. The rate by which individuals convert to a sero-positive state is of particular interest for epidemiologists because it can be used as a proxy of the underly-ing malaria transmission intensity. This project aims to perform power calculations using different reverse catalytic models and study designs. We are particularly interested in de-termining the minimum sample size required to:
with a given precision-
laria transmission occurred in the past or
disease dynamics after an interven-tion
We also aim to correct the es-timates for putative biases while maintaining other good statistical properties, such as consistency and low mean square error.
Measuring changes in Plasmodium falciparum transmission: precision, accuracy and costs of metrics.
LSHTM Investigators: Lucy Tusting, Chris Drakeley & Teun
Bousema.
External Investigators/Collaborators: David Smith (Johns Hopkins
Bloomberg School of Public Health, USA); Diadier Diallo (PATH
Funding:
Reliable methods to evaluate the effect of interventions and control programmes on malaria transmission are needed.
To help guide the design of trials to evaluate transmission-reducing interventions, this project assessed
evaluating their accuracy, precision and methods and costs of collection. We also reviewed the nonlinear
transmission: the entomological inoculation rate, force of infection, sporozoite rate, parasite rate and the basic reproductive number, R0. We found that although the entomological inoculation rate is widely considered the gold standard metric of malaria transmission, and may be necessary for measuring changes in transmission in highly endemic areas, it has limited precision and accuracy and more standardised collection methods are needed. In areas of low transmission, parasite rate, seroconversion rates and molecular metrics including
Programme for Resistance, Immunology, Surveillance and Modeling of Malaria in Uganda (PRISM): malaria transmission, infection and disease at three sites with varied transmission intensity in Uganda: implications for malaria control.
LSHTM Investigators: Sarah Staedke & Chris Drakeley.
External Investigators/Collaborators:
California, San Francisco, USA); Moses Kamya, Harriet Mayanja-
Kizza, Samuel Nsobya & Fred Wabwire-Mangen (Makerere
University, Uganda); David Smith & Andy Tatem (University of
Florida, USA); Martin Donnelly (Liverpool School of Tropical
Medicine, UK); Steve Lindsay (Durham University, UK).
Funding: USA National Institutes of Health.
This project aims to address the complexity of interactions between the mosquito vector, malaria parasite, and human host.
sub-counties of interest to provide a sampling frame for comprehensive surveillance activities. In each sub-county, 100 houses were randomly selected for measures of malaria transmission, infection and disease over a 2-year period. For transmission, the entomological inoculation
CDC light traps. Cohorts of children aged 0.5-11 years received all care from study clinics open 7 days/week
with routine blood smears done every 3 months and passive surveillance for malaria for measures of infection
of malaria were promptly treated with an artemisinin-
across the 3 sites with estimated EIRs of 3, 32, and 299 infected bites per person year for Jinja, Kanungu and Tororo respectively.
Parasite prevalence was 8.8% in Jinja, 15.0% in
differences when comparing the 1st and 2nd years of observation. The incidence of malaria per person year was 0.48 in Jinja, 1.67 in Kanungu and 3.52 in Tororo with
met criteria for complicated disease and there were no
excellent with only 3 episodes required rescue therapy within 3 days and 31 required repeat therapy within
until 2017, and continue to utilise samples collected for immunology and resistance projects
Surveillance, monitoring and evaluation
A. Proportion of tests that rejected the single force-of-infection reverse catalytic model using an age-adjusted cross-sectional
Effective surveillance, monitoring and evaluation (SME) is required to monitor progress with control and to inform the targeting of resources to where they are most needed. Malaria Centre members are actively engaged in a range of activities to improve SME.

96 Malaria moving forward Malaria moving forward 97
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
On the estimation of malaria transmission intensity using serology data.
LSHTM Investigators: Nuno Sepúlveda &
Chris Drakeley.
Funding: The Wellcome Trust.
Malaria transmission intensity is typi-cally assessed by parasite preva-lence or entomological infection rate.
seroprevalence data of parasite spe-
catalytic models.In this modelling approach, the
individuals become seropositive upon parasite exposure and may revert to a seronegative state after parasite clearance. The rate by which individuals convert to a sero-positive state is of particular interest for epidemiologists because it can be used as a proxy of the underly-ing malaria transmission intensity. This project aims to perform power calculations using different reverse catalytic models and study designs. We are particularly interested in de-termining the minimum sample size required to:
with a given precision-
laria transmission occurred in the past or
disease dynamics after an interven-tion
We also aim to correct the es-timates for putative biases while maintaining other good statistical properties, such as consistency and low mean square error.
Measuring changes in Plasmodium falciparum transmission: precision, accuracy and costs of metrics.
LSHTM Investigators: Lucy Tusting, Chris Drakeley & Teun
Bousema.
External Investigators/Collaborators: David Smith (Johns Hopkins
Bloomberg School of Public Health, USA); Diadier Diallo (PATH
Funding:
Reliable methods to evaluate the effect of interventions and control programmes on malaria transmission are needed.
To help guide the design of trials to evaluate transmission-reducing interventions, this project assessed
evaluating their accuracy, precision and methods and costs of collection. We also reviewed the nonlinear
transmission: the entomological inoculation rate, force of infection, sporozoite rate, parasite rate and the basic reproductive number, R0. We found that although the entomological inoculation rate is widely considered the gold standard metric of malaria transmission, and may be necessary for measuring changes in transmission in highly endemic areas, it has limited precision and accuracy and more standardised collection methods are needed. In areas of low transmission, parasite rate, seroconversion rates and molecular metrics including
Programme for Resistance, Immunology, Surveillance and Modeling of Malaria in Uganda (PRISM): malaria transmission, infection and disease at three sites with varied transmission intensity in Uganda: implications for malaria control.
LSHTM Investigators: Sarah Staedke & Chris Drakeley.
External Investigators/Collaborators:
California, San Francisco, USA); Moses Kamya, Harriet Mayanja-
Kizza, Samuel Nsobya & Fred Wabwire-Mangen (Makerere
University, Uganda); David Smith & Andy Tatem (University of
Florida, USA); Martin Donnelly (Liverpool School of Tropical
Medicine, UK); Steve Lindsay (Durham University, UK).
Funding: USA National Institutes of Health.
This project aims to address the complexity of interactions between the mosquito vector, malaria parasite, and human host.
sub-counties of interest to provide a sampling frame for comprehensive surveillance activities. In each sub-county, 100 houses were randomly selected for measures of malaria transmission, infection and disease over a 2-year period. For transmission, the entomological inoculation
CDC light traps. Cohorts of children aged 0.5-11 years received all care from study clinics open 7 days/week
with routine blood smears done every 3 months and passive surveillance for malaria for measures of infection
of malaria were promptly treated with an artemisinin-
across the 3 sites with estimated EIRs of 3, 32, and 299 infected bites per person year for Jinja, Kanungu and Tororo respectively.
Parasite prevalence was 8.8% in Jinja, 15.0% in
differences when comparing the 1st and 2nd years of observation. The incidence of malaria per person year was 0.48 in Jinja, 1.67 in Kanungu and 3.52 in Tororo with
met criteria for complicated disease and there were no
excellent with only 3 episodes required rescue therapy within 3 days and 31 required repeat therapy within
until 2017, and continue to utilise samples collected for immunology and resistance projects
Surveillance, monitoring and evaluation
A. Proportion of tests that rejected the single force-of-infection reverse catalytic model using an age-adjusted cross-sectional
Effective surveillance, monitoring and evaluation (SME) is required to monitor progress with control and to inform the targeting of resources to where they are most needed. Malaria Centre members are actively engaged in a range of activities to improve SME.

98 Malaria moving forward Malaria moving forward 99
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
endemicity in Pará state, Brazil.
LSHTM Investigators: Nuno Sepúlveda, Patrick Corran, Eleanor
Riley & Chris Drakeley.
External Investigators/Collaborators: Maristela Cunha
(Universidade Federal do Pará, Brazil).
Funding: The Wellcome Trust.
Parasite prevalence or entomologic infection rate are typically used to assess malaria transmission on a given study area.
to different parasite antigens as a way of assessing past or recent malaria exposure. This approach has been successfully used to monitor Plasmodium falciparum transmission dynamics. To test whether the same approach could be applied to Plasmodium vivax
epidemiology, we collected serology data on ~1,330
region, where Plasmodium vivax infections predominate. In each site, we found parasite prevalences less than 5.0%. Conversely the seroprevalences to Plasmodium vivax antigens or to Plasmodium falciparum antigens vary considerably across sites (e.g, 19.6% in Belém to 77.5% in Goianésia do Pará for Plasmodium vivax
Brazilian Ministry of Public Health. When we analysed the data with the reverse catalytic models, we found statistical evidence for a change in Plasmodium falciparum transmission in sites close to Jacareacanga and occurred around 30 years ago. We concluded that, irrespective of the malaria species, serological data could detect not only heterogeneity of the sites in terms of malaria endemicity but also putative temporal changes in disease dynamics
Malaria in school-aged children in areas of highly seasonal transmission: epidemiological risk, disease burden and strategies for control.
LSHTM Investigators: Sian Clarke, Daniel Chandramohan, Badara
Cisse, Saba Rouhani, Rebecca Jones & Simon Brooker.
External Investigators/Collaborators: Jean-Francois Trape
& Cheikh Sokna (Institut de recherche pour le developpement,
Anta Diop, Senegal); Malick Sembene, Aliou Dia & Khady Diallo
(Division of School Health, Ministry of Education, Senegal); Fatou
Ba Fall (National Malaria Conbtrol Programme, Ministry of Health,
Senegal); Natalie Roschnik, Seybou Diarra & Bamadio Modibo
(Save the Children, Mali); Moussa Sacko & Renion Saye (National
Institute for Public Health Research, Ministry of Health, Mali);
Diahara Traore (National Malaria Control Programme, Ministry of
Health, Mali); Matthew Jukes (Room to Read, UK); Josselin Thuillez
(Centre d’economie de la Sorbonne, France).
Funding: The Wellcome Trust & Save the Children.
The risk of malaria is greatest in early childhood and most research and control has focussed on young children. There is now increasing evidence that malaria can also
adversely affect schoolchildren, though the consequences for health and school performance have yet to be fully investigated.
To characterise the epidemiological burden and impact of malaria in school-aged children living in areas
series of studies were conducted in Senegal and Mali between 2010 and 2014. Epidemiological investigations were undertaken across a range of transmission settings including low-moderate seasonal, intense seasonal and intense year-round transmission. The incidence of clinical attacks, prevalence of asymptomatic infections, anaemia and cognitive function were examined in children aged 6 months to 14 years, including children below school age and children enrolled in primary school. Randomised trials in schools examined the impact of intermittent parasite clearance on malaria, anaemia and cognitive performance. The research is intended to inform the development of malaria control strategies for school-aged children in areas of highly seasonal transmission.
Future work will also examine the effects of malaria control on child development in pre-school children, with a focus on cognitive foundation skills for early literacy.
Reliability of school surveys in estimating geographic variation in malaria transmission in the western Kenyan Highlands.
LSHTM Investigators
Jonathan Cox.
External Investigators/Collaborators:
of Notre Dame, USA) & Chrispin Owaga, Elizabeth Marube,
Wycliffe Odongo, Albert Okoth, Pauline China & Robin Oriango
Prevention, Kenya).
Funding:
Malaria Transmission Consortium.
School surveys provide an operational approach to assess malaria transmission through parasite prevalence however, there is limited evidence on how well these estimates compare to those from the surrounding community.
Concurrent school and community cross-sectional surveys were conducted in 46 school/community clusters
36.4% of school children sampled resided within 600 m of their school with the mean distance of 793 m (IQR:
consistently higher than those from community surveys
the school population was restricted to those residing
seroconversion rates were similar between school and
prevalence rates measured during school surveys have been directly compared to those in the surrounding community. Ultimately, school-based estimates can be used as a reliable indicator of malaria transmission intensity in the wider community and may provide a basis for identifying priority areas for malaria control and be used to measure or monitor changes in transmission intensity.

98 Malaria moving forward Malaria moving forward 99
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
endemicity in Pará state, Brazil.
LSHTM Investigators: Nuno Sepúlveda, Patrick Corran, Eleanor
Riley & Chris Drakeley.
External Investigators/Collaborators: Maristela Cunha
(Universidade Federal do Pará, Brazil).
Funding: The Wellcome Trust.
Parasite prevalence or entomologic infection rate are typically used to assess malaria transmission on a given study area.
to different parasite antigens as a way of assessing past or recent malaria exposure. This approach has been successfully used to monitor Plasmodium falciparum transmission dynamics. To test whether the same approach could be applied to Plasmodium vivax
epidemiology, we collected serology data on ~1,330
region, where Plasmodium vivax infections predominate. In each site, we found parasite prevalences less than 5.0%. Conversely the seroprevalences to Plasmodium vivax antigens or to Plasmodium falciparum antigens vary considerably across sites (e.g, 19.6% in Belém to 77.5% in Goianésia do Pará for Plasmodium vivax
Brazilian Ministry of Public Health. When we analysed the data with the reverse catalytic models, we found statistical evidence for a change in Plasmodium falciparum transmission in sites close to Jacareacanga and occurred around 30 years ago. We concluded that, irrespective of the malaria species, serological data could detect not only heterogeneity of the sites in terms of malaria endemicity but also putative temporal changes in disease dynamics
Malaria in school-aged children in areas of highly seasonal transmission: epidemiological risk, disease burden and strategies for control.
LSHTM Investigators: Sian Clarke, Daniel Chandramohan, Badara
Cisse, Saba Rouhani, Rebecca Jones & Simon Brooker.
External Investigators/Collaborators: Jean-Francois Trape
& Cheikh Sokna (Institut de recherche pour le developpement,
Anta Diop, Senegal); Malick Sembene, Aliou Dia & Khady Diallo
(Division of School Health, Ministry of Education, Senegal); Fatou
Ba Fall (National Malaria Conbtrol Programme, Ministry of Health,
Senegal); Natalie Roschnik, Seybou Diarra & Bamadio Modibo
(Save the Children, Mali); Moussa Sacko & Renion Saye (National
Institute for Public Health Research, Ministry of Health, Mali);
Diahara Traore (National Malaria Control Programme, Ministry of
Health, Mali); Matthew Jukes (Room to Read, UK); Josselin Thuillez
(Centre d’economie de la Sorbonne, France).
Funding: The Wellcome Trust & Save the Children.
The risk of malaria is greatest in early childhood and most research and control has focussed on young children. There is now increasing evidence that malaria can also
adversely affect schoolchildren, though the consequences for health and school performance have yet to be fully investigated.
To characterise the epidemiological burden and impact of malaria in school-aged children living in areas
series of studies were conducted in Senegal and Mali between 2010 and 2014. Epidemiological investigations were undertaken across a range of transmission settings including low-moderate seasonal, intense seasonal and intense year-round transmission. The incidence of clinical attacks, prevalence of asymptomatic infections, anaemia and cognitive function were examined in children aged 6 months to 14 years, including children below school age and children enrolled in primary school. Randomised trials in schools examined the impact of intermittent parasite clearance on malaria, anaemia and cognitive performance. The research is intended to inform the development of malaria control strategies for school-aged children in areas of highly seasonal transmission.
Future work will also examine the effects of malaria control on child development in pre-school children, with a focus on cognitive foundation skills for early literacy.
Reliability of school surveys in estimating geographic variation in malaria transmission in the western Kenyan Highlands.
LSHTM Investigators
Jonathan Cox.
External Investigators/Collaborators:
of Notre Dame, USA) & Chrispin Owaga, Elizabeth Marube,
Wycliffe Odongo, Albert Okoth, Pauline China & Robin Oriango
Prevention, Kenya).
Funding:
Malaria Transmission Consortium.
School surveys provide an operational approach to assess malaria transmission through parasite prevalence however, there is limited evidence on how well these estimates compare to those from the surrounding community.
Concurrent school and community cross-sectional surveys were conducted in 46 school/community clusters
36.4% of school children sampled resided within 600 m of their school with the mean distance of 793 m (IQR:
consistently higher than those from community surveys
the school population was restricted to those residing
seroconversion rates were similar between school and
prevalence rates measured during school surveys have been directly compared to those in the surrounding community. Ultimately, school-based estimates can be used as a reliable indicator of malaria transmission intensity in the wider community and may provide a basis for identifying priority areas for malaria control and be used to measure or monitor changes in transmission intensity.

100 Malaria moving forward Malaria moving forward 101
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Analysis of multiplicity of infection and clonal diversity in paired human blood and mosquito oocyst samples from Burkina Faso.
LSHTM Investigators
Drakeley.
External Investigators/Collaborators: Kerstin Lanke & Will
Stone (Radboud University Nijmegen Medical Center, Nijmegen,
et de Formation sur le Paludisme, Burkina Faso).
Funding:
The aim of the project was to investigate the clonal diversity and the number of clones that are transmitted when a mosquito takes a blood meal from an individual infected with Plasmodium falciparum malaria.
to the clones found in mosquito midguts.
We recorded 4 different outcomes:
various combinations of matching clones detected in the
various combinations of different clones (not present in
The work is ongoing and we are now planning to test samples from the 4th outcome for recombination using a cloning and sequencing strategy. In addition, we also have data on asexual parasite density, gametocytaemia and number of oocysts in the midgut. Further analysis is needed to understand the relevance of clonal diversity and number in transmission from humans to the mosquito vector.
Bioko Island Malaria Control Project.
LSHTM Investigators: Immo Kleinschmidt, Chris Drakeley, Colin
Sutherland, Andrea Rehman, John Bradley & Jo Lines.
External Investigators/Collaborators: Christopher Schwabe
(Medical Care Development International); Michel Slotman (Texas
A&M University, USA); Janet Hemingway (Liverpool School of
Consortium).
Funding: Marathon Oil Company through Medical Care
Development International.
Comprehensive malaria control measures were introduced in Bioko, Equatorial Guinea, in 2004. The
rate , malaria related disease burden, child mortality and sero-positivity to malarial antigens have been observed. These reductions have been uneven and marked by substantial variation in prevalence of infection between
island. In a programmatic setting, a number of questions
related to malaria control and elimination are being investigated. These include evaluation of:
uniformly applied interventions
conversion, insecticide treated net and indoor residual
kdr gene in Anopheles gambiae on the effectiveness of pyrethroid based vector control
community participation
durability and utilization
Identifying Anopheles breeding sites, Bioko Island.
100 Malaria moving forward Malaria moving forward 101
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Analysis of multiplicity of infection and clonal diversity in paired human blood and mosquito oocyst samples from Burkina Faso.
LSHTM Investigators
Drakeley.
External Investigators/Collaborators: Kerstin Lanke & Will
Stone (Radboud University Nijmegen Medical Center, Nijmegen,
et de Formation sur le Paludisme, Burkina Faso).
Funding:
The aim of the project was to investigate the clonal diversity and the number of clones that are transmitted when a mosquito takes a blood meal from an individual infected with Plasmodium falciparum malaria.
to the clones found in mosquito midguts.
We recorded 4 different outcomes:
various combinations of matching clones detected in the
various combinations of different clones (not present in
The work is ongoing and we are now planning to test samples from the 4th outcome for recombination using a cloning and sequencing strategy. In addition, we also have data on asexual parasite density, gametocytaemia and number of oocysts in the midgut. Further analysis is needed to understand the relevance of clonal diversity and number in transmission from humans to the mosquito vector.
Bioko Island Malaria Control Project.
LSHTM Investigators: Immo Kleinschmidt, Chris Drakeley, Colin
Sutherland, Andrea Rehman, John Bradley & Jo Lines.
External Investigators/Collaborators: Christopher Schwabe
(Medical Care Development International); Michel Slotman (Texas
A&M University, USA); Janet Hemingway (Liverpool School of
Consortium).
Funding: Marathon Oil Company through Medical Care
Development International.
Comprehensive malaria control measures were introduced in Bioko, Equatorial Guinea, in 2004. The
rate , malaria related disease burden, child mortality and sero-positivity to malarial antigens have been observed. These reductions have been uneven and marked by substantial variation in prevalence of infection between
island. In a programmatic setting, a number of questions
related to malaria control and elimination are being investigated. These include evaluation of:
uniformly applied interventions
conversion, insecticide treated net and indoor residual
kdr gene in Anopheles gambiae on the effectiveness of pyrethroid based vector control
community participation
durability and utilization
Identifying Anopheles breeding sites, Bioko Island.

102 Malaria moving forward Malaria moving forward 103
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Tracking Resistance to Artemisinins Collaboration.
LSHTM Investigators
External Investigators/Collaborators: Elizabeth Ashley & Nick
White (Mahidol Oxford Research Unit, Thailand); Siv Sovannaroth,
Malaria Control Programme, Cambodia); Ric Fairhust, & Chanaki
Amaratunga (National Institutes of Health, USA); Sethavudh
Kaewviset & Sasithon Pukrittayakamee (Mahidol University,
Thailand); Abdul Faiz (Chittagong Medical School, Bangladesh);
Khin Maung Lwin and Francois Nosten (Shoklo Malaria Research
Unit, Thailand); Olugbenga Mokuolu (University of Ilorin Teaching
Hospital, Nigeria).
Funding: The Department for International Development.
is a multi-country multi-disciplinary collaboration. The
was completed in 2013 after recruiting a total of 1241
of spread of artemisinin resistance.
The School team was responsible for a range of studies exploring the demand, use and quality of antimalarial drugs and the implications for the development and control of drug resistance. Patients enrolled in the clinical studies in 9 sites participated in an additional study aimed a collecting additional behavioural and epidemiological data. In addition the locations of their homes and likely places of transmission were mapped.
Cambodia, Laos, Thailand, Myanmar and Nigeria for
Consortium drug quality project. Finally, in Cambodia structured and in-depth
interviews were carried out with communities at risk including mobile and migrant workers, in order to understand their demand for and use of fever treatments and to identify possible interventions for improving the use of antimalarial medicines.
Malaria, drug resistance and mobile and migrants population in Cambodia: a framework of planning.
LSHTM Investigators
External Investigators/Collaborators: Chea Nguon & Char Meng
Chuor (National Malaria Control Programme, Cambodia) & Sara
Canavati & Arantxa Roca (Malaria Consortium).
Funding: The Department for International Development .
The movement of populations in malaria-endemic areas poses a major threat to the spread of artemisinin
activities are simultaneously a high risk group for malaria and a “hard to reach” population.
We have developed the parasite multiplication factor
and populated it with activities conducted by population in
seasonal workers; construction/mine workers; forest workers; security personnel and visitors and four related indices: a vulnerability index, a forest/exposure index, an access index and a summary malaria risk index. The PMF also suggests relevant packages of interventions
The National Malaria Control Programme and other stakeholders were directly engaged in the development of the framework to maximize the relevance and utility of the framework. Challenges remain in the need to adapt research results, their complexity and the dynamic aspects of MMP to be combined with the need of a clear and relatively static strategy for programmatic and implementation purposes.
Sub-patent malaria, a challenge to diagnostics for malaria elimination in Mindanao islands, the Philippines.
LSHTM Investigators
Sutherland.
External Investigators/Collaborators: Judeline Dimalibot
(University of the Philippines Los Banos, Philippines); Christine
Candari (Philippines National Malaria Control Program, Philippines);
Fatima Pir Allian (Sinhaya Sinkawman, Philippines); Sukarno Asri &
Funding: Ford Foundation International Fellowships Program;
Chadwick Trust; University of the Philippines System Doctoral
Studies Fund; Philippine Council for Health Research and
Development.
We focused on three endemic provinces of Sarangani, South Cotabato and Tawi-Tawi in Mindanao islands,
which are aiming for continued reduction in malaria cases to achieve the Philippines’ goal of malaria elimination by 2020. In these provinces we screened malaria infection in 2595 individuals using microscopy and/or rapid diagnostic
and serological screening of exposure to P. falciparum and Plasmodium vivax infections.
Using the nested PCR assay as the gold standard,
pLDH-based RDT failed to diagnose subpatent P. falciparum and P. vivax infections in these provinces. We will complement our PCR diagnoses with serological data to locate residual transmission foci. The presence of subpatent malaria in Sarangani, South Cotabato and Tawi-Tawi recommends a review of existing policies on
adopting a more sensitive molecular method that can be deployed in these transmission settings.

102 Malaria moving forward Malaria moving forward 103
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Tracking Resistance to Artemisinins Collaboration.
LSHTM Investigators
External Investigators/Collaborators: Elizabeth Ashley & Nick
White (Mahidol Oxford Research Unit, Thailand); Siv Sovannaroth,
Malaria Control Programme, Cambodia); Ric Fairhust, & Chanaki
Amaratunga (National Institutes of Health, USA); Sethavudh
Kaewviset & Sasithon Pukrittayakamee (Mahidol University,
Thailand); Abdul Faiz (Chittagong Medical School, Bangladesh);
Khin Maung Lwin and Francois Nosten (Shoklo Malaria Research
Unit, Thailand); Olugbenga Mokuolu (University of Ilorin Teaching
Hospital, Nigeria).
Funding: The Department for International Development.
is a multi-country multi-disciplinary collaboration. The
was completed in 2013 after recruiting a total of 1241
of spread of artemisinin resistance.
The School team was responsible for a range of studies exploring the demand, use and quality of antimalarial drugs and the implications for the development and control of drug resistance. Patients enrolled in the clinical studies in 9 sites participated in an additional study aimed a collecting additional behavioural and epidemiological data. In addition the locations of their homes and likely places of transmission were mapped.
Cambodia, Laos, Thailand, Myanmar and Nigeria for
Consortium drug quality project. Finally, in Cambodia structured and in-depth
interviews were carried out with communities at risk including mobile and migrant workers, in order to understand their demand for and use of fever treatments and to identify possible interventions for improving the use of antimalarial medicines.
Malaria, drug resistance and mobile and migrants population in Cambodia: a framework of planning.
LSHTM Investigators
External Investigators/Collaborators: Chea Nguon & Char Meng
Chuor (National Malaria Control Programme, Cambodia) & Sara
Canavati & Arantxa Roca (Malaria Consortium).
Funding: The Department for International Development .
The movement of populations in malaria-endemic areas poses a major threat to the spread of artemisinin
activities are simultaneously a high risk group for malaria and a “hard to reach” population.
We have developed the parasite multiplication factor
and populated it with activities conducted by population in
seasonal workers; construction/mine workers; forest workers; security personnel and visitors and four related indices: a vulnerability index, a forest/exposure index, an access index and a summary malaria risk index. The PMF also suggests relevant packages of interventions
The National Malaria Control Programme and other stakeholders were directly engaged in the development of the framework to maximize the relevance and utility of the framework. Challenges remain in the need to adapt research results, their complexity and the dynamic aspects of MMP to be combined with the need of a clear and relatively static strategy for programmatic and implementation purposes.
Sub-patent malaria, a challenge to diagnostics for malaria elimination in Mindanao islands, the Philippines.
LSHTM Investigators
Sutherland.
External Investigators/Collaborators: Judeline Dimalibot
(University of the Philippines Los Banos, Philippines); Christine
Candari (Philippines National Malaria Control Program, Philippines);
Fatima Pir Allian (Sinhaya Sinkawman, Philippines); Sukarno Asri &
Funding: Ford Foundation International Fellowships Program;
Chadwick Trust; University of the Philippines System Doctoral
Studies Fund; Philippine Council for Health Research and
Development.
We focused on three endemic provinces of Sarangani, South Cotabato and Tawi-Tawi in Mindanao islands,
which are aiming for continued reduction in malaria cases to achieve the Philippines’ goal of malaria elimination by 2020. In these provinces we screened malaria infection in 2595 individuals using microscopy and/or rapid diagnostic
and serological screening of exposure to P. falciparum and Plasmodium vivax infections.
Using the nested PCR assay as the gold standard,
pLDH-based RDT failed to diagnose subpatent P. falciparum and P. vivax infections in these provinces. We will complement our PCR diagnoses with serological data to locate residual transmission foci. The presence of subpatent malaria in Sarangani, South Cotabato and Tawi-Tawi recommends a review of existing policies on
adopting a more sensitive molecular method that can be deployed in these transmission settings.

104 Malaria moving forward Malaria moving forward 105
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Characterisation of the cryptic reservoir of malaria infections: a study from Burkina Faso.
LSHTM Investigators
Bousema.
External Investigators/Collaborators:
(Centre National de Recherche et de Formation sur le Paludisme,
Burkina Faso) & Robert Sauerwein & Adrian Luty (Radboud
university medical center, Netherlands).
Funding: Netherlands Organization for Higher Education in the
Man-to-mosquito malaria transmission depends on the presence of mature gametocytes in the peripheral blood; however only a small proportion of infected individuals have patent gametocytes.
The contribution of infections with subpatent gametocytes to onward malaria transmission is unknown. In this study, we assessed the importance of this cryptic reservoir of infections. Infectiousness of 130 individuals living in a malaria endemic area in Burkina Faso was determined at the start/peak of transmission season and in the subsequent dry season by membrane feeding
were ~3 times more infectious than individuals with subpatent gametocytes. Throughout the study, most infectious individuals had subpatent gametocytes. Most infected mosquitoes fed on blood with submicroscopic
mosquito infections in the community but at least 15% of
that submicroscopic gametocytes are a major source of mosquito infection and that all ages contribute to the infectious reservoir.
submicroscopic gametocytes to malaria transmission during the transition between dry and wet season and to
vector exposure in natural populations.
Infectiousness by season, age and gametocyte status. The stacked bars represent the total population in each age group and at each time
microscopy; hatched bars indicate the proportion of individuals who
bars indicate the proportion of individuals who do not infect mosquitoes
Border malaria and approaches to local elimination in Namibia.
LSHTM Investigators: Immo Kleinschmidt.
External Investigators/Collaborators:
Sturrock (The University of California, San Francisco, USA); Davis
Mumbengegwi (University of Namibia, Namibia) & Stark Katokele
(National Malaria Program, Namibia).
Funding:
Malaria incidence has declined to low levels in Namibia, and the country has set 2020 as the target for malaria elimination. Many of the residual cases occur in the
Malaria transmission may be associated with
to determine risk factors for malaria, including cross-border travel, intervention coverage and compliance, and local factors that may be linked to transmission of malaria. By mapping cases and controls, and testing for sub-patent infections and antibody seroconversions in the neighbourhood of each case and each control, the study will investigate the existence of any hotspots of transmission.
which will evaluate targeted parasite and vector control in the neighbourhood of cases.
Quantifying travel behaviour for infectious disease research: A comparison of data from surveys and mobile phones.
LSHTM Investigators
Drakeley & Jonathan Cox.
External Investigators/Collaborators: Amy Wesolowski (Carnegie
Mellon University, USA.; Nathan Eagle & Caroline Buckee (Harvard
School of Public Health, USA); Jennifer Stevenson (Kenya Medical
Kenya & Johns Hopkins Bloomberg School of Public Health, USA);
Chrispin Owaga & Elizabeth Marube (Kenya Medical Research
Funding:
Transmission Consortium.
Human travel impacts the spread of infectious diseases across spatial and temporal scales, with broad implications for the biological and social sciences.
obtain, particularly in low-income countries.Travel survey data provide detailed demographic
information, but sample sizes are often small and travel histories are hard to validate. Mobile phone records can provide vast quantities of spatio-temporal travel data, but vary in spatial resolution and explicitly do not include individual information in order to protect the privacy of subscribers. We have compared and contrasted both
sources of data over the same time period in a rural area of Kenya. Mobile phone records reporting an order
indicates that people with phones are more likely to travel and the primary motivation for traveling is visiting family
broad travel patterns, distinguish regional differences in travel, and are able to identify the main routes of malaria importation. Ultimately, each data source provides different insights that can be combined to form a more detailed picture of travel in low-income settings to understand the spread of infectious diseases.

104 Malaria moving forward Malaria moving forward 105
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Characterisation of the cryptic reservoir of malaria infections: a study from Burkina Faso.
LSHTM Investigators
Bousema.
External Investigators/Collaborators:
(Centre National de Recherche et de Formation sur le Paludisme,
Burkina Faso) & Robert Sauerwein & Adrian Luty (Radboud
university medical center, Netherlands).
Funding: Netherlands Organization for Higher Education in the
Man-to-mosquito malaria transmission depends on the presence of mature gametocytes in the peripheral blood; however only a small proportion of infected individuals have patent gametocytes.
The contribution of infections with subpatent gametocytes to onward malaria transmission is unknown. In this study, we assessed the importance of this cryptic reservoir of infections. Infectiousness of 130 individuals living in a malaria endemic area in Burkina Faso was determined at the start/peak of transmission season and in the subsequent dry season by membrane feeding
were ~3 times more infectious than individuals with subpatent gametocytes. Throughout the study, most infectious individuals had subpatent gametocytes. Most infected mosquitoes fed on blood with submicroscopic
mosquito infections in the community but at least 15% of
that submicroscopic gametocytes are a major source of mosquito infection and that all ages contribute to the infectious reservoir.
submicroscopic gametocytes to malaria transmission during the transition between dry and wet season and to
vector exposure in natural populations.
Infectiousness by season, age and gametocyte status. The stacked bars represent the total population in each age group and at each time
microscopy; hatched bars indicate the proportion of individuals who
bars indicate the proportion of individuals who do not infect mosquitoes
Border malaria and approaches to local elimination in Namibia.
LSHTM Investigators: Immo Kleinschmidt.
External Investigators/Collaborators:
Sturrock (The University of California, San Francisco, USA); Davis
Mumbengegwi (University of Namibia, Namibia) & Stark Katokele
(National Malaria Program, Namibia).
Funding:
Malaria incidence has declined to low levels in Namibia, and the country has set 2020 as the target for malaria elimination. Many of the residual cases occur in the
Malaria transmission may be associated with
to determine risk factors for malaria, including cross-border travel, intervention coverage and compliance, and local factors that may be linked to transmission of malaria. By mapping cases and controls, and testing for sub-patent infections and antibody seroconversions in the neighbourhood of each case and each control, the study will investigate the existence of any hotspots of transmission.
which will evaluate targeted parasite and vector control in the neighbourhood of cases.
Quantifying travel behaviour for infectious disease research: A comparison of data from surveys and mobile phones.
LSHTM Investigators
Drakeley & Jonathan Cox.
External Investigators/Collaborators: Amy Wesolowski (Carnegie
Mellon University, USA.; Nathan Eagle & Caroline Buckee (Harvard
School of Public Health, USA); Jennifer Stevenson (Kenya Medical
Kenya & Johns Hopkins Bloomberg School of Public Health, USA);
Chrispin Owaga & Elizabeth Marube (Kenya Medical Research
Funding:
Transmission Consortium.
Human travel impacts the spread of infectious diseases across spatial and temporal scales, with broad implications for the biological and social sciences.
obtain, particularly in low-income countries.Travel survey data provide detailed demographic
information, but sample sizes are often small and travel histories are hard to validate. Mobile phone records can provide vast quantities of spatio-temporal travel data, but vary in spatial resolution and explicitly do not include individual information in order to protect the privacy of subscribers. We have compared and contrasted both
sources of data over the same time period in a rural area of Kenya. Mobile phone records reporting an order
indicates that people with phones are more likely to travel and the primary motivation for traveling is visiting family
broad travel patterns, distinguish regional differences in travel, and are able to identify the main routes of malaria importation. Ultimately, each data source provides different insights that can be combined to form a more detailed picture of travel in low-income settings to understand the spread of infectious diseases.

106 Malaria moving forward Malaria moving forward 107
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
period.
Which factors increase the risk for acquiring Plasmodium knowlesi malaria in Sabah, Malaysia.
LSHTM Investigators: Christopher Drakeley, Jon Cox & Kimberly
Fornace.
External Investigators/Collaborators:
Australia); Timothy William (Sabah Department of Health, Malaysia).
Funding: The Biotechnology and Biological Sciences Research
Council; The Economic and Social Research Council; The Medical
Research Council; The Natural Environment Research Council.
Human malaria due to the simian parasite Plasmodium knowlesi
Pk transmission has been linked to factors such as individual forest and seasonal
rainfall, detailed environmental, behavioural and genetic risk factors have not been systematically evaluated.
This population-based case control study aims to detect and describe factors which predispose individuals to Pk symptomatic infection in Sabah, Malaysia. Three controls from the same village will be matched for each case detected. Cases and controls will be interviewed on demographics, malaria history and prevention activities, travel history and movement patterns and interactions with macaques. Blood sampling will be done for PCR
cases and 508 controls have been recruited to date and enrolment is expected to continue through early 2015.
Transmission and control of Plasmodium knowlesi: a mathematical modelling study.
LSHTM Investigators: Christopher Drakeley.
External Investigators/Collaborators: Natsuko Imai, Michael
Plasmodium knowlesi is a zoonotic malaria but now
humans come into increasing contact with the reservoir
deforestation, assessing the potential for a shift from zoonotic to sustained Plasmodium knowlesi transmission between humans is of major importance.
developed, taking into account the three areas (forest,
occur. Latin hypercube sampling of model parameters was utilised to identify parameter sets consistent with plausible prevalence in macaques and humans inferred from observed data. We then explore the consequences of increasing human-macaque contact in the farm, the likely impact of rapid treatment, and the use of long-
spread of this emerging infection.
transmission being sustained by the macaque population with spill over infections in the human population and with
The extent to which macaques forage for food in the farms had a non-linear relationship with human infection prevalence, with the highest prevalence occurring when
frequently to the forest where they experience higher contact with vectors and hence sustain transmission.
sustained human to human transmission in the absence of macaques, although with a low human reproduction
rapid treatment provide personal protection to humans with maximal estimated reductions in human prevalence of 42% and 95%, respectively.
This model simulates conditions where Plasmodium knowlesi transmission may occur and the potential impact of control measures. Predictions suggest that
the risk of infection in humans, but they must be actively implemented if Plasmodium knowlesi is to be controlled. More data to better parameterise models is needed.
Schematic distribution of forest, farm, villages, and the movement of macaques and humans between the 3 areas, and the hypothesised transmission cycle of Plasmodium knowlesi in Malaysia and Southeast Asia. Adapted from the yellow fever transmission cycle observed in Africa.

106 Malaria moving forward Malaria moving forward 107
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
period.
Which factors increase the risk for acquiring Plasmodium knowlesi malaria in Sabah, Malaysia.
LSHTM Investigators: Christopher Drakeley, Jon Cox & Kimberly
Fornace.
External Investigators/Collaborators:
Australia); Timothy William (Sabah Department of Health, Malaysia).
Funding: The Biotechnology and Biological Sciences Research
Council; The Economic and Social Research Council; The Medical
Research Council; The Natural Environment Research Council.
Human malaria due to the simian parasite Plasmodium knowlesi
Pk transmission has been linked to factors such as individual forest and seasonal
rainfall, detailed environmental, behavioural and genetic risk factors have not been systematically evaluated.
This population-based case control study aims to detect and describe factors which predispose individuals to Pk symptomatic infection in Sabah, Malaysia. Three controls from the same village will be matched for each case detected. Cases and controls will be interviewed on demographics, malaria history and prevention activities, travel history and movement patterns and interactions with macaques. Blood sampling will be done for PCR
cases and 508 controls have been recruited to date and enrolment is expected to continue through early 2015.
Transmission and control of Plasmodium knowlesi: a mathematical modelling study.
LSHTM Investigators: Christopher Drakeley.
External Investigators/Collaborators: Natsuko Imai, Michael
Plasmodium knowlesi is a zoonotic malaria but now
humans come into increasing contact with the reservoir
deforestation, assessing the potential for a shift from zoonotic to sustained Plasmodium knowlesi transmission between humans is of major importance.
developed, taking into account the three areas (forest,
occur. Latin hypercube sampling of model parameters was utilised to identify parameter sets consistent with plausible prevalence in macaques and humans inferred from observed data. We then explore the consequences of increasing human-macaque contact in the farm, the likely impact of rapid treatment, and the use of long-
spread of this emerging infection.
transmission being sustained by the macaque population with spill over infections in the human population and with
The extent to which macaques forage for food in the farms had a non-linear relationship with human infection prevalence, with the highest prevalence occurring when
frequently to the forest where they experience higher contact with vectors and hence sustain transmission.
sustained human to human transmission in the absence of macaques, although with a low human reproduction
rapid treatment provide personal protection to humans with maximal estimated reductions in human prevalence of 42% and 95%, respectively.
This model simulates conditions where Plasmodium knowlesi transmission may occur and the potential impact of control measures. Predictions suggest that
the risk of infection in humans, but they must be actively implemented if Plasmodium knowlesi is to be controlled. More data to better parameterise models is needed.
Schematic distribution of forest, farm, villages, and the movement of macaques and humans between the 3 areas, and the hypothesised transmission cycle of Plasmodium knowlesi in Malaysia and Southeast Asia. Adapted from the yellow fever transmission cycle observed in Africa.

108 Malaria moving forward Malaria moving forward 109
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A cluster-randomised trial of targetted control to eliminate malaria in central Senegal: study design and acceptability of the interventions.
LSHTM Investigators: Badara Cisse, Clare Flach, Matt Cairns,
External Investigators/Collaborators: Abdoulaye Diallo, Fassiath
Tairou, Ousmane Sy, Jean-Louis Ndiaye, Tidiane Ndoye, Lansana
Diop, Senegal); El-Hadj Ba & Cheikh Sokhna (Institut de Recherche
Funding: The Wellcome Trust; The Medical Research Council;
The Department for International Development Clinical Trials
Control and Elimination Partnership in Africa.
The purpose of this trial is to evaluate the extent to which a targetted malaria control strategy combining
chemotherapy, delivered by district health staff to villages reporting clinical cases, can reduce the transmission of malaria, in a region where scaling up of control measures has been effective in reducing the incidence of malaria.
The trial will also determine whether, as part of this strategy, chemotherapy should be delivered to all
The unit of randomisation is the health post and the population of approximately 10,000 people that it serves. 40 health posts were randomized, 15 to receive targeted
Interventions are delivered over two years, the primary outcomes are the incidence of malaria in the second year and the prevalence of parasitaemia just after the main peak period of transmission in the second year. To assess effects on transmission, incidence in non-targetted areas in each cluster will be compared. In intervention
reported the previous year. In 30 clusters, all households in hotspot villages were targetted to receive IRS with
were screened using a malaria rapid diagnostic test
coverage was topped-up by providing persons diagnosed with malaria with a LLIN.Results will be available in 2015.
Identifying and characterising foci of malaria transmission in potential malaria elimination settings in rural Senegal.
LSHTM Investigators
Milligan.
External Investigators/Collaborators: Ernest Faye, El hadj Ba, El Hadj Diouf,
Funding: The Malaria Capacity Development Consortium.
programmes in Senegal is threatened by resistance to insecticides.We determined the effectiveness of LLIN use by the individual
and in the local community in reducing the incidence of malaria.
the district of Fatick, central Senegal, in an area covered by a
uncomplicated malaria presenting at health posts in the district
study. For each case, one or two controls of the same age group, selected by random sampling from the DSS listing for the district, were recruited concurrently if a malaria rapid diagnostic test was negative. For cases and controls, and members of their households and of surrounding households, bednet use and approximate age was recorded after inspecting sleeping places. Information about bednet use was also obtained for all households in the district when visited in demographic surveillance rounds from January to December 2011. Conditional logistic regression was used to estimate the rate ratio associated with use of LLIN, and with the level of local coverage of LLINs in the community grouped by quintiles, adjusted for potential confounding factors including distance to health facility, socio-economic status, and distance to mosquito breeding sites.
540 malaria case-control pairs were recruited. Sleeping under an LLIN, and local coverage of LLINs, were independently associated with reduced malaria incidence. Malaria incidence for individuals in communities with coverage in the upper quintile (>81% of persons
LLINs remain effective in central Senegal but high coverage is required to maximise impact. LLIN distribution programmes should target communities with low coverage.
Bio assays on LLINs of 12 to 15 months of use show strong correlation between level of malaria transmission and mosquitos mortality rates after exposition to LLINs.
The project also allowed an extension of the malaria surveillance initiated in 2008 in central Senegal where malaria transmission remains patchy with many communities free of clinical cases over 5 years of follow-up.

108 Malaria moving forward Malaria moving forward 109
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
A cluster-randomised trial of targetted control to eliminate malaria in central Senegal: study design and acceptability of the interventions.
LSHTM Investigators: Badara Cisse, Clare Flach, Matt Cairns,
External Investigators/Collaborators: Abdoulaye Diallo, Fassiath
Tairou, Ousmane Sy, Jean-Louis Ndiaye, Tidiane Ndoye, Lansana
Diop, Senegal); El-Hadj Ba & Cheikh Sokhna (Institut de Recherche
Funding: The Wellcome Trust; The Medical Research Council;
The Department for International Development Clinical Trials
Control and Elimination Partnership in Africa.
The purpose of this trial is to evaluate the extent to which a targetted malaria control strategy combining
chemotherapy, delivered by district health staff to villages reporting clinical cases, can reduce the transmission of malaria, in a region where scaling up of control measures has been effective in reducing the incidence of malaria.
The trial will also determine whether, as part of this strategy, chemotherapy should be delivered to all
The unit of randomisation is the health post and the population of approximately 10,000 people that it serves. 40 health posts were randomized, 15 to receive targeted
Interventions are delivered over two years, the primary outcomes are the incidence of malaria in the second year and the prevalence of parasitaemia just after the main peak period of transmission in the second year. To assess effects on transmission, incidence in non-targetted areas in each cluster will be compared. In intervention
reported the previous year. In 30 clusters, all households in hotspot villages were targetted to receive IRS with
were screened using a malaria rapid diagnostic test
coverage was topped-up by providing persons diagnosed with malaria with a LLIN.Results will be available in 2015.
Identifying and characterising foci of malaria transmission in potential malaria elimination settings in rural Senegal.
LSHTM Investigators
Milligan.
External Investigators/Collaborators: Ernest Faye, El hadj Ba, El Hadj Diouf,
Funding: The Malaria Capacity Development Consortium.
programmes in Senegal is threatened by resistance to insecticides.We determined the effectiveness of LLIN use by the individual
and in the local community in reducing the incidence of malaria.
the district of Fatick, central Senegal, in an area covered by a
uncomplicated malaria presenting at health posts in the district
study. For each case, one or two controls of the same age group, selected by random sampling from the DSS listing for the district, were recruited concurrently if a malaria rapid diagnostic test was negative. For cases and controls, and members of their households and of surrounding households, bednet use and approximate age was recorded after inspecting sleeping places. Information about bednet use was also obtained for all households in the district when visited in demographic surveillance rounds from January to December 2011. Conditional logistic regression was used to estimate the rate ratio associated with use of LLIN, and with the level of local coverage of LLINs in the community grouped by quintiles, adjusted for potential confounding factors including distance to health facility, socio-economic status, and distance to mosquito breeding sites.
540 malaria case-control pairs were recruited. Sleeping under an LLIN, and local coverage of LLINs, were independently associated with reduced malaria incidence. Malaria incidence for individuals in communities with coverage in the upper quintile (>81% of persons
LLINs remain effective in central Senegal but high coverage is required to maximise impact. LLIN distribution programmes should target communities with low coverage.
Bio assays on LLINs of 12 to 15 months of use show strong correlation between level of malaria transmission and mosquitos mortality rates after exposition to LLINs.
The project also allowed an extension of the malaria surveillance initiated in 2008 in central Senegal where malaria transmission remains patchy with many communities free of clinical cases over 5 years of follow-up.

110 Malaria moving forward Malaria moving forward 111
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
national humanitarian assistance is greatest but also during chronic emergencies when there is no fully rec-ognised government but opportunity for providing more comprehensive assistance improves. The handbook
-tors with practical advice on designing and implement-ing measures in both man-made and natural disasters. The handbook is organised into ten chapters covering coordination and ad-vocacy, assessment and operational plan-ning, surveillance outbreak response, diagnosis and case management, ap-proaches for vector control and personal protection, commu-nity and refugee par-ticipation, monitoring and evaluation, and operational research to improve the effectiveness of prevention and treat-ment in humanitarian emergencies.
Malaria control and development
Methodological development of whole-economy modelling of infectious disease: Plasmodium falciparum malaria control in Africa.
LSHTM Investigators: Richard Smith, Marcus Keogh-Brown,
Michael Bretscher & Chris Drakeley.
External Investigators/Collaborators: Henning Tarp Jensen
(University of Copenhagen, Denmark).
Funding: Medical Research Council Methodology.
to develop epidemiological models of malaria, and to estimate cost-effectiveness of interventions and malaria control. However, interactions between malaria, demographic characteristics and the national economy have received little attention. Many economic studies of malaria take a partial equilibrium approach which
interventions.
takes an economy-wide approach to estimating full
capture many important economic aspects of population health including morbidity and mortality effects on labour supply, long-term cognitive effects of child morbidity, and public budget implications of prevention, treatment, and basic care for the sick and dying. Existing applications of
Malaria, but do not capture interaction or feedback effects between epidemiology, demographics and the economy.
model of malaria transmission which captures multiplicity
simulation framework for Ghana and for Tanzania has been produced and policy simulations will soon be implemented.
Socioeconomic development as an intervention against malaria.
LSHTM Investigators: Lucy Tusting, Barbara Willey, Richard Smith
& Steve Lindsay.
External Investigators/Collaborators: Hmooda Toto Kafy
(National Malaria Control Programme, Sudan); Henry Lucas & John
Thompson (Institute of Development Studies, UK).
Funding: The Department for International Development.
Future progress in malaria control may be hampered by the development of resistance to drugs and insecticides and by the contraction of aid budgets. Historically, control
This project aimed to assess whether socioeconomic development can contribute to malaria control. We
did a systematic review and meta-analysis to assess whether the risk of malaria in children aged 0–15 years
reviewed, 20 met the criteria for inclusion in the qualitative analysis, and 15 of these reported the necessary data for inclusion in the meta-analysis. The odds of malaria infection were higher in the poorest children than in the
existing malaria control efforts, increased investment in interventions to support socioeconomic development is warranted, since such interventions could prove highly effective and sustainable against malaria in the long term.
Malaria control in humanitarian emergencies: an inter-
LSHTM Investigators: Natasha Howard, Mark Rowland &
Toby Leslie.
External Investigators/Collaborators: A writing committee of
malaria experts coordinated by Jose Nkuni, Natasha Howard
and Abraham Mnzava produced the draft of this second ver-
sion.
Funding: The World Health Organisation.
This second edition is a comprehensive interagency manual on how to control malaria in countries af-
authorship by staff at the School who have broad experience of working in emergencies the handbook represents a thorough review of the literature and knowledge gained during the last decade. The struc-
an additional chapter on humanitarian coordination.
best practices, improvements in technologies, avail-ability of new tools, and changes in World Health
The interagency handbook is designed to set out malaria control responses in humanitarian emergen-cies, in both the acute phase when reliance on inter-
Malaria Centre members are evaluating the role of events and interventions beyond the health sector in shaping malaria risks and responses.

110 Malaria moving forward Malaria moving forward 111
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
national humanitarian assistance is greatest but also during chronic emergencies when there is no fully rec-ognised government but opportunity for providing more comprehensive assistance improves. The handbook
-tors with practical advice on designing and implement-ing measures in both man-made and natural disasters. The handbook is organised into ten chapters covering coordination and ad-vocacy, assessment and operational plan-ning, surveillance outbreak response, diagnosis and case management, ap-proaches for vector control and personal protection, commu-nity and refugee par-ticipation, monitoring and evaluation, and operational research to improve the effectiveness of prevention and treat-ment in humanitarian emergencies.
Malaria control and development
Methodological development of whole-economy modelling of infectious disease: Plasmodium falciparum malaria control in Africa.
LSHTM Investigators: Richard Smith, Marcus Keogh-Brown,
Michael Bretscher & Chris Drakeley.
External Investigators/Collaborators: Henning Tarp Jensen
(University of Copenhagen, Denmark).
Funding: Medical Research Council Methodology.
to develop epidemiological models of malaria, and to estimate cost-effectiveness of interventions and malaria control. However, interactions between malaria, demographic characteristics and the national economy have received little attention. Many economic studies of malaria take a partial equilibrium approach which
interventions.
takes an economy-wide approach to estimating full
capture many important economic aspects of population health including morbidity and mortality effects on labour supply, long-term cognitive effects of child morbidity, and public budget implications of prevention, treatment, and basic care for the sick and dying. Existing applications of
Malaria, but do not capture interaction or feedback effects between epidemiology, demographics and the economy.
model of malaria transmission which captures multiplicity
simulation framework for Ghana and for Tanzania has been produced and policy simulations will soon be implemented.
Socioeconomic development as an intervention against malaria.
LSHTM Investigators: Lucy Tusting, Barbara Willey, Richard Smith
& Steve Lindsay.
External Investigators/Collaborators: Hmooda Toto Kafy
(National Malaria Control Programme, Sudan); Henry Lucas & John
Thompson (Institute of Development Studies, UK).
Funding: The Department for International Development.
Future progress in malaria control may be hampered by the development of resistance to drugs and insecticides and by the contraction of aid budgets. Historically, control
This project aimed to assess whether socioeconomic development can contribute to malaria control. We
did a systematic review and meta-analysis to assess whether the risk of malaria in children aged 0–15 years
reviewed, 20 met the criteria for inclusion in the qualitative analysis, and 15 of these reported the necessary data for inclusion in the meta-analysis. The odds of malaria infection were higher in the poorest children than in the
existing malaria control efforts, increased investment in interventions to support socioeconomic development is warranted, since such interventions could prove highly effective and sustainable against malaria in the long term.
Malaria control in humanitarian emergencies: an inter-
LSHTM Investigators: Natasha Howard, Mark Rowland &
Toby Leslie.
External Investigators/Collaborators: A writing committee of
malaria experts coordinated by Jose Nkuni, Natasha Howard
and Abraham Mnzava produced the draft of this second ver-
sion.
Funding: The World Health Organisation.
This second edition is a comprehensive interagency manual on how to control malaria in countries af-
authorship by staff at the School who have broad experience of working in emergencies the handbook represents a thorough review of the literature and knowledge gained during the last decade. The struc-
an additional chapter on humanitarian coordination.
best practices, improvements in technologies, avail-ability of new tools, and changes in World Health
The interagency handbook is designed to set out malaria control responses in humanitarian emergen-cies, in both the acute phase when reliance on inter-
Malaria Centre members are evaluating the role of events and interventions beyond the health sector in shaping malaria risks and responses.

112 Malaria moving forward Malaria moving forward 113
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Mapping causes of non-malarial fever in Africa and Asia.
LSHTM Investigators
Schellenberg.
External Investigators/Collaborators: Heidi Hopkins & David Bell
Funding:
Consortium.
The successful introduction of malaria rapid tests into routine health services is challenged by the lack of lo-cal knowledge of the probability of alternative causes of febrile illness. To address this we searched databases of peer reviewed publications to identify studies that had
described the prevalence of infection among patients with undifferentiated fever.
papers met criteria of blood culture or csf series in undif-
Both sets of data suggest a large variation in quality be-
for laboratory or antibiotic sensitivity data. It is hoped to -
malarial Resistance Network and that this will be used by public health authorities. The longer term future and link-age with other mapping initiatives is under discussion.
Future priorities
Knowing insects: hosts, vectors and companions of science.
The contribution of the Malaria Centre to policy making for malaria treatment and control.
LSHTM Investigators: Ann Kelly
External Investigators/Collaborators: Noemi Tousignant
(University of Cambridge, UK); Uli Beisel (Bayreuth University,
Researchers at the School carried out social analy-sis of insects as disease vectors in Tanzania, The Gambia, Senegal and Ghana. Reading insects not simply as vectors of disease, but equally as hosts, vectors and companions of science, their work opens up the epistemic, biopolitical and social dimensions of human–insect connections. By parsing these inter-sections, they suggest we can begin to understand the kinds of knowledge made possible and elusive by insects’ capacity to connect and carry, inscribe and destabilize, disgust and inspire. Thinking with insects allows us to re-examine how life produces
-cal, institutional and experimental relations. Studying both insect and disease control programmes and the diverse kinds of knowledge scientists make with and through insects has led these researchers to explore the different ways in which insect-mediated science shapes understandings of the natural and social
world. While insects are studied predominantly to know, manipulate and transform the natural world in order to minimise diseases, insects also resist
-laria control policies, Kelly and Beisel have further-more excavated “neglected malarias”, the kinds of malaria control practices that fall outside of much of contemporary global health policy. Critiquing the predominant rationale of malaria elimination, they chart malaria as the outcome of a complex rela-tional exchange of unpredictable proximities. In this understanding malaria control is not a war to be won, but a moving target. They underline that ma-
for putting more emphasis on modest practices of control. Techniques that are place-sensitive and re-quire precise and continuous effort; techniques that do not understand malaria in an integrated, over-arching socio-ecological model, but that instead
mosquito-parasite entanglements.
of infectious diseases, including malaria. The way
prevention of malaria was reorganised recently. In
was established and an open competition held for places on this committee. Meetings of the committee are open and its discussions and conclusions are reported with a few months of each meeting in the
control. TEGs and ERGs are tasked with gather-ing and reviewing the evidence that could support a change in policy and presenting this information to
-mendations for the introduction of seasonal malaria chemoprevention in appropriate epidemiological situ-ations, increasing the number of doses of intermittent preventive treatment during pregnancy and lowering the dose of primaquine given to kill gametocytes.
Members of the Malaria Centre contribute to several aspects of the policy-making process. Brian
ERG on malaria in pregnancy, David Schellenberg chairs the TEG on surveillance, monitoring and evalu-ation and Peter Smith chaired an ERG on measuring the burden of malaria. Jo Lines and Mark Rowland are members of the TEG that addresses issues in Vector Control such as the use of new insecticides and insecticide treated materials. The setting of stan-
work is supported by Mark Rowland.
out a plan to accelerate progress in malaria control in the period 2015-2030. The Roll Back Malaria Partner-ship is preparing a supportive action plan to ensure that the technical strategy is implemented and to sus-tain advocacy and funding for malaria control. Several members of the Malaria Centre have contributed to the development of both of these key documents.
Ensuring that research conducted by members of the School helps to inform policy is a key part of the activities of the Malaria Centre.
It is important to understand the political economics of malaria control efforts, and mem-bers of the Malaria Centre actively participate in shaping these efforts, working to ensure

112 Malaria moving forward Malaria moving forward 113
London School of Hygiene & Tropical Medicine Malaria Centre Report 2012-14
Mapping causes of non-malarial fever in Africa and Asia.
LSHTM Investigators
Schellenberg.
External Investigators/Collaborators: Heidi Hopkins & David Bell
Funding:
Consortium.
The successful introduction of malaria rapid tests into routine health services is challenged by the lack of lo-cal knowledge of the probability of alternative causes of febrile illness. To address this we searched databases of peer reviewed publications to identify studies that had
described the prevalence of infection among patients with undifferentiated fever.
papers met criteria of blood culture or csf series in undif-
Both sets of data suggest a large variation in quality be-
for laboratory or antibiotic sensitivity data. It is hoped to -
malarial Resistance Network and that this will be used by public health authorities. The longer term future and link-age with other mapping initiatives is under discussion.
Future priorities
Knowing insects: hosts, vectors and companions of science.
The contribution of the Malaria Centre to policy making for malaria treatment and control.
LSHTM Investigators: Ann Kelly
External Investigators/Collaborators: Noemi Tousignant
(University of Cambridge, UK); Uli Beisel (Bayreuth University,
Researchers at the School carried out social analy-sis of insects as disease vectors in Tanzania, The Gambia, Senegal and Ghana. Reading insects not simply as vectors of disease, but equally as hosts, vectors and companions of science, their work opens up the epistemic, biopolitical and social dimensions of human–insect connections. By parsing these inter-sections, they suggest we can begin to understand the kinds of knowledge made possible and elusive by insects’ capacity to connect and carry, inscribe and destabilize, disgust and inspire. Thinking with insects allows us to re-examine how life produces
-cal, institutional and experimental relations. Studying both insect and disease control programmes and the diverse kinds of knowledge scientists make with and through insects has led these researchers to explore the different ways in which insect-mediated science shapes understandings of the natural and social
world. While insects are studied predominantly to know, manipulate and transform the natural world in order to minimise diseases, insects also resist
-laria control policies, Kelly and Beisel have further-more excavated “neglected malarias”, the kinds of malaria control practices that fall outside of much of contemporary global health policy. Critiquing the predominant rationale of malaria elimination, they chart malaria as the outcome of a complex rela-tional exchange of unpredictable proximities. In this understanding malaria control is not a war to be won, but a moving target. They underline that ma-
for putting more emphasis on modest practices of control. Techniques that are place-sensitive and re-quire precise and continuous effort; techniques that do not understand malaria in an integrated, over-arching socio-ecological model, but that instead
mosquito-parasite entanglements.
of infectious diseases, including malaria. The way
prevention of malaria was reorganised recently. In
was established and an open competition held for places on this committee. Meetings of the committee are open and its discussions and conclusions are reported with a few months of each meeting in the
control. TEGs and ERGs are tasked with gather-ing and reviewing the evidence that could support a change in policy and presenting this information to
-mendations for the introduction of seasonal malaria chemoprevention in appropriate epidemiological situ-ations, increasing the number of doses of intermittent preventive treatment during pregnancy and lowering the dose of primaquine given to kill gametocytes.
Members of the Malaria Centre contribute to several aspects of the policy-making process. Brian
ERG on malaria in pregnancy, David Schellenberg chairs the TEG on surveillance, monitoring and evalu-ation and Peter Smith chaired an ERG on measuring the burden of malaria. Jo Lines and Mark Rowland are members of the TEG that addresses issues in Vector Control such as the use of new insecticides and insecticide treated materials. The setting of stan-
work is supported by Mark Rowland.
out a plan to accelerate progress in malaria control in the period 2015-2030. The Roll Back Malaria Partner-ship is preparing a supportive action plan to ensure that the technical strategy is implemented and to sus-tain advocacy and funding for malaria control. Several members of the Malaria Centre have contributed to the development of both of these key documents.
Ensuring that research conducted by members of the School helps to inform policy is a key part of the activities of the Malaria Centre.
It is important to understand the political economics of malaria control efforts, and mem-bers of the Malaria Centre actively participate in shaping these efforts, working to ensure

Publications 2012-14 115
Malaria Centre Report 2012-14
114 Publications 2012-14
London School of Hygiene & Tropical Medicine
Adu-Gyasi, D., Adams, M., Amoako, S.,
Mahama, E., Nsoh, M., Amenga-Etego,
-
laria parasite density: assumed white blood
-
ate measure in Central Ghana. Malaria
Journal, 11, 238.
among HIV seropositve clinic attendants
12, 382.
Adams, M., Dosoo, D., Dery, D., Wilson,
Agyei, S.
Plasmodium falciparum infections among
asymptomatic residents in the middle belt
of Ghana. Malaria Journal, 12, 22.
Allan, R., Howard, N., Lines, J., Mac-
donald, M., Maes, P., Mnzava, A., Nkuni,
J., Renshaw, M. & Rowland, M.
Chapter 7 Prevention. In: Howard, N. &
humanitarian emergencies: an interagency
Allan, R., Howard, N., Macdonald, M.,
Maes, P., Renshaw, M. & Rowland, M.
and associated routine monitoring. In: n:
-
laria control in humanitarian emergencies:
Allen, E., Chandler, C., Mandimika, N.,
Evaluating harm associated with anti-
malarial drugs: a survey of methods used
by clinical researchers to elicit, assess and
record participant-reported adverse events
and related data. Malaria Journal, 12:325.
Allen, E., Mushi, A., Massawe, I., Vester-
gaard, L., Lemnge, M., Staedke, S.,
process of eliciting adverse event, medical
history and concomitant medication reports
in antimalarial and antiretroviral interaction
trials. BMC Medical Research Methodology,
13, 140.
Amambua-Ngwa, A., Park, D., Volkman,
P., Van Tyne, D., Ndiaye, D., Wirth, D.,
Conway, D., Neafsey, D. & Schaffner, S.
Signatures of Selection in a Deep Sample
Malaria Parasites. Molecular Biology and
M., Gomez-Escobar, N., Stewart, L.,
Deerhake, M., Cheeseman, I., Newbold,
Population genomic scan for candidate
signatures of balancing selection to guide
antigen characterization in malaria para-
sites. Plos Genetics, 8, e1002992.
Das, A., Hamade, P., Howard, N., Moham-
6 Case management. Malaria control in
Ansah, E., Epokor, M., Whitty, C., Yeung,
-
Malaria Diagnosis as Compared to Micros-
copy and Presumptive Diagnosis in Central
and Peripheral Public Health Facilities in
Medicine and Hygiene, 89, 724-36.
middle-income countries: a systematic lit-
erature review. Health Policy and Planning,
16: doi: 10.1093/heapol/czu034.
-
-
no, J.
Plasmodium falciparum Circumsporozoite
Protein Likely Due to Protein-Protein Inter-
A., Dodoo, T., Mahama, E., Amoako, N.,
Chandramohan, D. -
laria and the Risk of Malaria in Infants in a
Infectious Diseases, 208, 1504-1513.
Assefa, S., Preston, M., Campino, S.,
infection using parasite deep sequencing
Athrey, G., Hodges, T., Reddy, M.,
-
schmidt, I., Caccone, A. & Slotman, M.
malaria mosquitoes: large impact of vector
control. Plos Genetics, 8, e1003097.
Maslen, G., Mangano, V., Alcock, D., Ma-
-
D.
Plasmodium falciparum Diversity Using
Next-Generation Sequence Data. Plos
Auburn, S., Marfurt, J., Maslen, G.,
Campino, S., Ruano Rubio, V., Manske,
-
-
-
D. & Price, R. -
tion of Plasmodium vivax Field Isolates for
High-Throughput Whole Genome Sequenc-
-
vura, M., Delmini, R., Amenga-Etego,
D.
combination therapy to test positive malaria
in a high-transmission setting in Ghana - a
cluster-randomised trial. Tropical Medicine
& International Health, 2013; 18:74-74.
& Webster, J.
diagnostic test-based management of Ma-
-
-
D. -
ia and treatment outcomes for malaria and
-
Molyneux, M., Taylor, T., Ndila, C., Pe-
D., Andrews, R., Edkins, S., Gray, E.,
J., Spencer, C. & ¶, M. G. E. N.
Imputation-based meta-analysis of severe
malaria in three african populations. PloS
Genetics, 9, e1003509.
Chandramohan, D.
to artemisinin-based combination therapy
for the treatment of malaria: a systematic
review of the evidence. Malaria Journal,
13, 7.
-
buguzi, C., Diliberto, D., Taaka, L., Chan-
dler, C. & Staedke, S.
case management of malaria: exploring
support, capacity and motivation of commu-
nity medicine distributors in Uganda. Health
Policy and Planning. 0:czu033v1-czu033
-
-
tion Therapy: Challenges and Perspectives
e1001590.
-
laria knowledge and utilization of chemo-
prophylaxis in the UK population and in UK
passengers departing to malaria-endemic
areas. Malaria Journal, 12, 461.
S., Abdulla, S. & Ghani, A. -
cacy of RTS,S malaria vaccines: individual-
participant pooled analysis of phase 2
data. The Lancet Infectious Diseases, 13,
319-27.
epidemiological analysis of febrile malaria
in Coastal Kenya showing hotspots within
hotspots. Elife, 3, e02130.
-
haire, A., Arinaitwe, M., Adriko, M., Mwe-
Sutherland, C. & Stothard, J. -
tection of persistent Plasmodium spp. infec-
tions in Ugandan children after artemether-
lumefantrine treatment. Parasitology, 1-11.
Crump, J.
Transmission Intensity in Tanzania. Clinical
Infectious Diseases, 58, 638-647.
& Dinglasan, R.
mosquito feeding assays be used for evalu-
ating transmission-blocking interventions?
Drakeley, C.
for falciparum malaria. The Lancet Infec-
tious Diseases, 14, 677.
Drakeley, C. & Cox, J.
of hotspot-targeted interventions on malaria
transmission: study protocol for a cluster-
randomized controlled trial. Trials, 14, 36.
Vargas, D., Monti, F., Ela, C., Riloha, M.
-
lence of malaria infection in children living
in houses with window screening or closed
eaves on bioko island, equatorial Guinea.
-
anti, M., Nugraheni, D., Widyastuti, A.,
Lobo, N., Hawley, W., Cook, J. & Drake-
ley, C. -
dium falciparum transmission intensity us-
ing serological cohort data from Indonesian
schoolchildren. Malaria Journal, 12, 21.
-
of Malaria Parasitemia and Purchase of
Thompson, E., Sebastian, S., Volkmann,
Phosphoinositide Metabolism Links cGMP-
Dependent Protein Kinase G to Essential
Ca2+ Signals at Key Decision Points in the
Life Cycle of Malaria Parasites. PloS Biol-
ogy, 12, e1001806.
Publications 2012-14 115
Malaria Centre Report 2012-14
114 Publications 2012-14
London School of Hygiene & Tropical Medicine
Adu-Gyasi, D., Adams, M., Amoako, S.,
Mahama, E., Nsoh, M., Amenga-Etego,
-
laria parasite density: assumed white blood
-
ate measure in Central Ghana. Malaria
Journal, 11, 238.
among HIV seropositve clinic attendants
12, 382.
Adams, M., Dosoo, D., Dery, D., Wilson,
Agyei, S.
Plasmodium falciparum infections among
asymptomatic residents in the middle belt
of Ghana. Malaria Journal, 12, 22.
Allan, R., Howard, N., Lines, J., Mac-
donald, M., Maes, P., Mnzava, A., Nkuni,
J., Renshaw, M. & Rowland, M.
Chapter 7 Prevention. In: Howard, N. &
humanitarian emergencies: an interagency
Allan, R., Howard, N., Macdonald, M.,
Maes, P., Renshaw, M. & Rowland, M.
and associated routine monitoring. In: n:
-
laria control in humanitarian emergencies:
Allen, E., Chandler, C., Mandimika, N.,
Evaluating harm associated with anti-
malarial drugs: a survey of methods used
by clinical researchers to elicit, assess and
record participant-reported adverse events
and related data. Malaria Journal, 12:325.
Allen, E., Mushi, A., Massawe, I., Vester-
gaard, L., Lemnge, M., Staedke, S.,
process of eliciting adverse event, medical
history and concomitant medication reports
in antimalarial and antiretroviral interaction
trials. BMC Medical Research Methodology,
13, 140.
Amambua-Ngwa, A., Park, D., Volkman,
P., Van Tyne, D., Ndiaye, D., Wirth, D.,
Conway, D., Neafsey, D. & Schaffner, S.
Signatures of Selection in a Deep Sample
Malaria Parasites. Molecular Biology and
M., Gomez-Escobar, N., Stewart, L.,
Deerhake, M., Cheeseman, I., Newbold,
Population genomic scan for candidate
signatures of balancing selection to guide
antigen characterization in malaria para-
sites. Plos Genetics, 8, e1002992.
Das, A., Hamade, P., Howard, N., Moham-
6 Case management. Malaria control in
Ansah, E., Epokor, M., Whitty, C., Yeung,
-
Malaria Diagnosis as Compared to Micros-
copy and Presumptive Diagnosis in Central
and Peripheral Public Health Facilities in
Medicine and Hygiene, 89, 724-36.
middle-income countries: a systematic lit-
erature review. Health Policy and Planning,
16: doi: 10.1093/heapol/czu034.
-
-
no, J.
Plasmodium falciparum Circumsporozoite
Protein Likely Due to Protein-Protein Inter-
A., Dodoo, T., Mahama, E., Amoako, N.,
Chandramohan, D. -
laria and the Risk of Malaria in Infants in a
Infectious Diseases, 208, 1504-1513.
Assefa, S., Preston, M., Campino, S.,
infection using parasite deep sequencing
Athrey, G., Hodges, T., Reddy, M.,
-
schmidt, I., Caccone, A. & Slotman, M.
malaria mosquitoes: large impact of vector
control. Plos Genetics, 8, e1003097.
Maslen, G., Mangano, V., Alcock, D., Ma-
-
D.
Plasmodium falciparum Diversity Using
Next-Generation Sequence Data. Plos
Auburn, S., Marfurt, J., Maslen, G.,
Campino, S., Ruano Rubio, V., Manske,
-
-
-
D. & Price, R. -
tion of Plasmodium vivax Field Isolates for
High-Throughput Whole Genome Sequenc-
-
vura, M., Delmini, R., Amenga-Etego,
D.
combination therapy to test positive malaria
in a high-transmission setting in Ghana - a
cluster-randomised trial. Tropical Medicine
& International Health, 2013; 18:74-74.
& Webster, J.
diagnostic test-based management of Ma-
-
-
D. -
ia and treatment outcomes for malaria and
-
Molyneux, M., Taylor, T., Ndila, C., Pe-
D., Andrews, R., Edkins, S., Gray, E.,
J., Spencer, C. & ¶, M. G. E. N.
Imputation-based meta-analysis of severe
malaria in three african populations. PloS
Genetics, 9, e1003509.
Chandramohan, D.
to artemisinin-based combination therapy
for the treatment of malaria: a systematic
review of the evidence. Malaria Journal,
13, 7.
-
buguzi, C., Diliberto, D., Taaka, L., Chan-
dler, C. & Staedke, S.
case management of malaria: exploring
support, capacity and motivation of commu-
nity medicine distributors in Uganda. Health
Policy and Planning. 0:czu033v1-czu033
-
-
tion Therapy: Challenges and Perspectives
e1001590.
-
laria knowledge and utilization of chemo-
prophylaxis in the UK population and in UK
passengers departing to malaria-endemic
areas. Malaria Journal, 12, 461.
S., Abdulla, S. & Ghani, A. -
cacy of RTS,S malaria vaccines: individual-
participant pooled analysis of phase 2
data. The Lancet Infectious Diseases, 13,
319-27.
epidemiological analysis of febrile malaria
in Coastal Kenya showing hotspots within
hotspots. Elife, 3, e02130.
-
haire, A., Arinaitwe, M., Adriko, M., Mwe-
Sutherland, C. & Stothard, J. -
tection of persistent Plasmodium spp. infec-
tions in Ugandan children after artemether-
lumefantrine treatment. Parasitology, 1-11.
Crump, J.
Transmission Intensity in Tanzania. Clinical
Infectious Diseases, 58, 638-647.
& Dinglasan, R.
mosquito feeding assays be used for evalu-
ating transmission-blocking interventions?
Drakeley, C.
for falciparum malaria. The Lancet Infec-
tious Diseases, 14, 677.
Drakeley, C. & Cox, J.
of hotspot-targeted interventions on malaria
transmission: study protocol for a cluster-
randomized controlled trial. Trials, 14, 36.
Vargas, D., Monti, F., Ela, C., Riloha, M.
-
lence of malaria infection in children living
in houses with window screening or closed
eaves on bioko island, equatorial Guinea.
-
anti, M., Nugraheni, D., Widyastuti, A.,
Lobo, N., Hawley, W., Cook, J. & Drake-
ley, C. -
dium falciparum transmission intensity us-
ing serological cohort data from Indonesian
schoolchildren. Malaria Journal, 12, 21.
-
of Malaria Parasitemia and Purchase of
Thompson, E., Sebastian, S., Volkmann,
Phosphoinositide Metabolism Links cGMP-
Dependent Protein Kinase G to Essential
Ca2+ Signals at Key Decision Points in the
Life Cycle of Malaria Parasites. PloS Biol-
ogy, 12, e1001806.

Publications 2012-14 117
Malaria Centre Report 2012-14
116 Publications 2012-14
London School of Hygiene & Tropical Medicine
-
& Snow, R.
coinfection and its sources of heterogeneity
-
tious Diseases, 205, 841-52.
-
chur, S., Goodman, C. & Schellenberg,
D.
Message Reminders to Retail Staff in Tan-
Lumefantrine: Effect on Dispenser Knowl-
Journal of Tropical Medicine and Hygiene,
pii: 14-0126.
& Schellenberg, D.
take malaria treatment: a systematic review
of the literature on adherence to antima-
-
mara, S., Takken, W., Carnevale, P. & Al-
lan, R.
Sheeting for Emergency Malaria Prevention
and Shelter among Displaced Populations:
-
Journal of Tropical Medicine and Hygiene,
87, 242-50.
Milligan, P.
complete protection in malaria cohort stud-
ies. Malaria Journal, 12, 355.
Cairns, M., Roca-Feltrer, A., Garske, T.,
Wilson, A., Diallo, D., Milligan, P., Ghani,
the potential public health impact of sea-
children. Nature Communications, 3, 881.
J., Conway, D. & Della Torre, A.
triggered by habitat discontinuities across
a riverine landscape. Molecular Ecology,
23:18, 4574–4589.
-
Indian monsoon. Nature Climate Change,
3, 502-507.
-
Dürrheim, D.
of malaria vector control using routine sur-
veillance data in Zambia: implications for
monitoring and evaluation. Malaria Journal,
11, 437.
V. -
aging lab results, you are managing the
patient’: How the enactment of malaria at
health facilities in Cameroon compares with
74, 1528-35.
Chandler, C., Meta, J., Ponzo, C., Nasu-
A. & Reyburn, H.
of effective behaviour change interventions
to support the use of malaria rapid diagnos-
tic tests by Tanzanian clinicians. Implemen-
tation Science, 9, 83.
C.
imported falciparum malaria in the United
Kingdom over 20 years: an observational
study. British Medical Journal (Clinical re-
J.
determine the safety of the topical insect
Parasites and Vectors, 7, 173.
S. & Lindsay, S.
Randomised Controlled Trial of the Insect
Chico, R., Mayaud, P., Ariti, C., Mabey,
D., Ronsmans, C. & Chandramohan, D.
transmitted and reproductive tract infec-
-
quito infection from Plasmodium falciparum
gametocyte density and estimating the res-
ervoir of infection. Elife, 2, e00626.
Clarke, S., Ly, A., Ndiaye, J., Fall, F., Dial-
children: epidemiology, disease burden
and control approaches in areas of highly
seasonal transmission. Tropical Medicine
152-152.
Clemente, A., Fadigati, G., Caporale, R.,
Marchese, D., Castronovo, G., Sannella,
A., Severini, C., Verra, F., Garaci, E., Coz-
zolino, F. & Torcia, M.
-
es by Plasmodium falciparum Schizont
Extracts: Role of Myeloid Dendritic Cells
in Effector and Regulatory Functions of
-
nity, 81, 1842-1851.
Collins, C., Hackett, F., Strath, M., Penzo,
cGMP-dependent Protein Kinase Regulates
Discharge and Egress. Plos Pathogens, 9.
Committee, W. M. P. A. & Secretariat
-
Journal, 12, 213.
Cox, S., Nweneka, C., Doherty, C., Ful-
ford, A., Moore, S. & Prentice, A.
Randomised controlled trial of weekly
chloroquine to re-establish normal erythron
-
malarial anaemia. British Medical Journal,
Crawley, J., Sismanidis, C., Goodman,
T. V. -
tive treatment for malaria during infancy
on serological responses to measles and
other vaccines used in the Expanded Pro-
randomised controlled trials. Lancet, 380,
1001-10.
Craft, J., Shin, C., Fleckenstein, L.,
-
view of pyronaridine anti-malarial properties
and product characteristics. Malaria Jour-
nal, 11, 270.
S., Riley, E. & Walther, M. -
parison of parasite sequestration in uncom-
plicated and severe childhood plasmodium
falciparum malaria. The Journal of infection,
Cunnington, A., De Souza, J., Walther,
M. & Riley, E. -
sistance to Salmonella through heme- and
heme oxygenase-dependent dysfunctional
granulocyte mobilization. Nature Medicine,
18, 120-7.
Takem, E., Riley, E. & Walther, M.
Prolonged Neutrophil Dysfunction after
Plasmodium falciparum Malaria Is Related
-
duction. Journal of Immunology (Baltimore,
Md, 189, 5336-46.
Cunnington, A., Riley, E. & Walther, M.
Plasmodium falciparum malaria. The Jour-
nal of Infectious Diseases.
Strengthening the policy setting process
for global malaria control and elimination.
Malaria Journal, 11, 28.
Da Silva Santos, S., Clark, T., Campino,
-
Investigation of host candidate malaria-
associated risk/protective SNPs in a Brazil-
e36692.
-
bazi, E., Nabukeera, D., Ssemmondo,
E., Gonahasa, S., Tumwebaze, P., Dilib-
erto, D., Maiteki-Sebuguzi, C., Staedke,
S. & Drakeley, C.
the WST8/1-methoxy-PMS enzymatic as-
say in Uganda. Malaria Journal, 12, 210.
De Savigny, D., Webster, J., Agyepong,
-
ducing vouchers for malaria prevention in
Ghana and Tanzania: context and adoption
of innovation in health systems. Health
Policy and Planning, 27, 32-43.
De Souza, J.
against malaria after vaccination. Parasite
S. & Nefzi, A.
cytotoxic activities of chiral triamines. Bio-
organic & Medicinal Chemistry Letters, 23,
4579-4582.
-
ma, T. & Sutherland, C.
detection of Plasmodium falciparum, P.
malariae, P. ovale curtisi and P. ovale wal-
Ghanaian school-children. International
Journal for Parasitology-Drugs and Drug
Resistance, 3, 45-50.
-
J., Sene, P., Ahouidi, A., Dieye, T., Gaye,
-
-
I., Gomis, J., Mather, F., Sissako, A., Di-
-
R., Duraisingh, M., Muskavitch, M.,
D’alessandro, U., Conway, D., Volkman,
Drakeley, C. & Lines, J.
long haul: 20 years of malaria surveillance.
The Lancet Infectious Diseases, 14, 445-
446.
Mukabana, W., Lindsay, S. & Fillinger, U.
Teo, Y., Thai, C., Hang, N., Jeffreys, A.,
-
rar, J., Phu, N., Hien, T. & Consortium, M.
are associated with severe malaria in the
Vietnamese. Genes and Immunity, 13,
503-8.
drug quality assessment. Tropical Medicine
& International Health, 2013; 18:21-22.
El Chaar, M., Atwal, S., Freimanis, G.,
-
irradiation. Transfusion, 53, 3174-83.
El Chaar, M., Atwal, S., Freimanis, G.,
-
land, C. & Allain, J.

Publications 2012-14 117
Malaria Centre Report 2012-14
116 Publications 2012-14
London School of Hygiene & Tropical Medicine
-
& Snow, R.
coinfection and its sources of heterogeneity
-
tious Diseases, 205, 841-52.
-
chur, S., Goodman, C. & Schellenberg,
D.
Message Reminders to Retail Staff in Tan-
Lumefantrine: Effect on Dispenser Knowl-
Journal of Tropical Medicine and Hygiene,
pii: 14-0126.
& Schellenberg, D.
take malaria treatment: a systematic review
of the literature on adherence to antima-
-
mara, S., Takken, W., Carnevale, P. & Al-
lan, R.
Sheeting for Emergency Malaria Prevention
and Shelter among Displaced Populations:
-
Journal of Tropical Medicine and Hygiene,
87, 242-50.
Milligan, P.
complete protection in malaria cohort stud-
ies. Malaria Journal, 12, 355.
Cairns, M., Roca-Feltrer, A., Garske, T.,
Wilson, A., Diallo, D., Milligan, P., Ghani,
the potential public health impact of sea-
children. Nature Communications, 3, 881.
J., Conway, D. & Della Torre, A.
triggered by habitat discontinuities across
a riverine landscape. Molecular Ecology,
23:18, 4574–4589.
-
Indian monsoon. Nature Climate Change,
3, 502-507.
-
Dürrheim, D.
of malaria vector control using routine sur-
veillance data in Zambia: implications for
monitoring and evaluation. Malaria Journal,
11, 437.
V. -
aging lab results, you are managing the
patient’: How the enactment of malaria at
health facilities in Cameroon compares with
74, 1528-35.
Chandler, C., Meta, J., Ponzo, C., Nasu-
A. & Reyburn, H.
of effective behaviour change interventions
to support the use of malaria rapid diagnos-
tic tests by Tanzanian clinicians. Implemen-
tation Science, 9, 83.
C.
imported falciparum malaria in the United
Kingdom over 20 years: an observational
study. British Medical Journal (Clinical re-
J.
determine the safety of the topical insect
Parasites and Vectors, 7, 173.
S. & Lindsay, S.
Randomised Controlled Trial of the Insect
Chico, R., Mayaud, P., Ariti, C., Mabey,
D., Ronsmans, C. & Chandramohan, D.
transmitted and reproductive tract infec-
-
quito infection from Plasmodium falciparum
gametocyte density and estimating the res-
ervoir of infection. Elife, 2, e00626.
Clarke, S., Ly, A., Ndiaye, J., Fall, F., Dial-
children: epidemiology, disease burden
and control approaches in areas of highly
seasonal transmission. Tropical Medicine
152-152.
Clemente, A., Fadigati, G., Caporale, R.,
Marchese, D., Castronovo, G., Sannella,
A., Severini, C., Verra, F., Garaci, E., Coz-
zolino, F. & Torcia, M.
-
es by Plasmodium falciparum Schizont
Extracts: Role of Myeloid Dendritic Cells
in Effector and Regulatory Functions of
-
nity, 81, 1842-1851.
Collins, C., Hackett, F., Strath, M., Penzo,
cGMP-dependent Protein Kinase Regulates
Discharge and Egress. Plos Pathogens, 9.
Committee, W. M. P. A. & Secretariat
-
Journal, 12, 213.
Cox, S., Nweneka, C., Doherty, C., Ful-
ford, A., Moore, S. & Prentice, A.
Randomised controlled trial of weekly
chloroquine to re-establish normal erythron
-
malarial anaemia. British Medical Journal,
Crawley, J., Sismanidis, C., Goodman,
T. V. -
tive treatment for malaria during infancy
on serological responses to measles and
other vaccines used in the Expanded Pro-
randomised controlled trials. Lancet, 380,
1001-10.
Craft, J., Shin, C., Fleckenstein, L.,
-
view of pyronaridine anti-malarial properties
and product characteristics. Malaria Jour-
nal, 11, 270.
S., Riley, E. & Walther, M. -
parison of parasite sequestration in uncom-
plicated and severe childhood plasmodium
falciparum malaria. The Journal of infection,
Cunnington, A., De Souza, J., Walther,
M. & Riley, E. -
sistance to Salmonella through heme- and
heme oxygenase-dependent dysfunctional
granulocyte mobilization. Nature Medicine,
18, 120-7.
Takem, E., Riley, E. & Walther, M.
Prolonged Neutrophil Dysfunction after
Plasmodium falciparum Malaria Is Related
-
duction. Journal of Immunology (Baltimore,
Md, 189, 5336-46.
Cunnington, A., Riley, E. & Walther, M.
Plasmodium falciparum malaria. The Jour-
nal of Infectious Diseases.
Strengthening the policy setting process
for global malaria control and elimination.
Malaria Journal, 11, 28.
Da Silva Santos, S., Clark, T., Campino,
-
Investigation of host candidate malaria-
associated risk/protective SNPs in a Brazil-
e36692.
-
bazi, E., Nabukeera, D., Ssemmondo,
E., Gonahasa, S., Tumwebaze, P., Dilib-
erto, D., Maiteki-Sebuguzi, C., Staedke,
S. & Drakeley, C.
the WST8/1-methoxy-PMS enzymatic as-
say in Uganda. Malaria Journal, 12, 210.
De Savigny, D., Webster, J., Agyepong,
-
ducing vouchers for malaria prevention in
Ghana and Tanzania: context and adoption
of innovation in health systems. Health
Policy and Planning, 27, 32-43.
De Souza, J.
against malaria after vaccination. Parasite
S. & Nefzi, A.
cytotoxic activities of chiral triamines. Bio-
organic & Medicinal Chemistry Letters, 23,
4579-4582.
-
ma, T. & Sutherland, C.
detection of Plasmodium falciparum, P.
malariae, P. ovale curtisi and P. ovale wal-
Ghanaian school-children. International
Journal for Parasitology-Drugs and Drug
Resistance, 3, 45-50.
-
J., Sene, P., Ahouidi, A., Dieye, T., Gaye,
-
-
I., Gomis, J., Mather, F., Sissako, A., Di-
-
R., Duraisingh, M., Muskavitch, M.,
D’alessandro, U., Conway, D., Volkman,
Drakeley, C. & Lines, J.
long haul: 20 years of malaria surveillance.
The Lancet Infectious Diseases, 14, 445-
446.
Mukabana, W., Lindsay, S. & Fillinger, U.
Teo, Y., Thai, C., Hang, N., Jeffreys, A.,
-
rar, J., Phu, N., Hien, T. & Consortium, M.
are associated with severe malaria in the
Vietnamese. Genes and Immunity, 13,
503-8.
drug quality assessment. Tropical Medicine
& International Health, 2013; 18:21-22.
El Chaar, M., Atwal, S., Freimanis, G.,
-
irradiation. Transfusion, 53, 3174-83.
El Chaar, M., Atwal, S., Freimanis, G.,
-
land, C. & Allain, J.
Publications 2012-14 119
Malaria Centre Report 2012-14
118 Publications 2012-14
London School of Hygiene & Tropical Medicine
of Plasmodium Falciparum-Infected Whole
Blood With Mirasol. Vox Sanguinis, 103,
137-137.
Exploring health providers’ and community
perceptions and experiences with malaria
tests in South-East Nigeria: a critical step
towards appropriate treatment. Malaria
Journal, 11, 368.
Wanzira, H., Mpimbaza, A., Nsobya, S.,
White, N., Webb, E., Staedke, S. & Drake-
ley, C.
clearance of Plasmodium falciparum game-
tocytes in children with uncomplicated ma-
laria in Uganda: a randomised, controlled,
double-blind, dose-ranging trial. The Lancet
Infectious Diseases.14:2, 130 - 139.
Eziefula, A., Gosling, R., Hwang, J.,
I. A. D.
transmission. Malaria Journal, 11, 360.
Hallett, R., Vennerstrom, J., Duong, S.,
Ringwald, P., Wellems, T., Plowe, C. &
Dondorp, A.
-
ties, and Public Health Implications. The
Hygiene, 87, 231-241.
Fancony, C., Gamboa, D., Sebastiao,
Y., Hallett, R., Sutherland, C., Sousa-
Figueiredo, J. & Nery, S.
pfcrt and pfmdr1 Genotypes of Plasmodium
falciparum Cocirculate with P. malariae, P.
56, 5271-5277.
Community perceptions of a malaria vac-
cine in the Kintampo districts of Ghana.
Malaria Journal, 12, 156.
N., De Souza, J., Grady, L., Saris, C.,
signalling regulates memory CD4+ T cell
populations and suppresses rapid in-
malaria infection. Infection and Immunity,
M., Riley, E. & Walther, M.
thaw lysates of P. falciparum-infected red
blood cells induce differentiation of func-
tionally competent regulatory T cells from
memory T cells. European Journal of Im-
parasite epigenetics: when virulence and
romance collide. Cell Host & Microbe, 16,
148-50.
Franco, A., Gomes, M., Rowland, M.,
Coleman, P. & Davies, C. -
trolling Malaria Using Livestock-Based
Gadalla, N., Abdallah, T., Atwal, S.,
Sutherland, C. & Adam, I. -
tion of pfdhfr/pfdhps alleles and declining
artesunate/sulphadoxine-pyrimethamine ef-
years after deployment in eastern Sudan.
Malaria Journal, 12, 255.
Gatton, M., Chitnis, N., Churcher, T.,
Donnelly, M., Ghani, A., Godfray, H.,
Gould, F., Hastings, I., Marshall, J.,
Ranson, H., Rowland, M., Shaman, J.
& Lindsay, S.
-
1218-1230.
Gaudart, J., Huiart, L., Milligan, P., Thie-
baut, R. & Giorgi, R. -
ibility issues in science, is P value really the
only answer? Proceedings of the National
Gayer, M., Golaz, A., Howard, N. & Schil-
peroord, M. -
nation. In: Howard, N. & Clements-Hunt,
-
book, 2nd Edition. Geneva: World Health
Gayer, M., Golaz, A., Howard, N. & Schil-
peroord, M. -
ment and operational planning. In: oward,
-
Lietman, T. -
mycin Distribution on Malaria Parasitemia
during the Low-Transmission Season in
-
Etego, L., Anyorigiya, T., Hodgson, A.,
D. -
moglobin C and haemoglobin S and the
dynamics of the evolutionary response to
malaria in Kassena-Nankana District of
Ghumra, A., Semblat, J., Ataide, R.,
M., Amambua-Ngwa, A., Walther, M.,
Virulent Malaria Parasites. Plos Pathogens,
8, e1002665.
Plasmodium infection, anaemia and mos-
quito net use among school children across
different settings in Kenya. Tropical Medi-
cine & International Health, 17, 858-70.
-
S.
in Malaria School Surveys in Kenya:
Does their Under-performance Matter for
Journal of Tropical Medicine and Hygiene,
C. & Chiodini, P.
malaria prevention advice to Public Health
England, Malaria Reference Labora-
Travel Medicine and Infectious Disease,
vaccination to global health: past, present
and future. Philosophical Transactions of
the Royal Society of London Series B, Bio-
consortium approach to malaria research
and capacity development. Tropical Medi-
much to do. Lancet, 383, 1703-4.
Grigg, M., William, T., Drakeley, C., Jelip,
Factors that are associated with the risk
of acquiring Plasmodium knowlesi malaria
in Sabah, Malaysia: a case-control study
e006004.
G., Renia, L., De Souza, J. & Riley, E.
-
hibitory Pathways Independently Regulate
Host Resistance to Plasmodium-induced
8, e1002504.
-
modium falciparum, anaemia and cogni-
tive and educational performance among
school children in an area of moderate
malaria transmission: baseline results of
a cluster randomized trial on the coast of
Kenya. Tropical Medicine & International
Health, 17, 532-549.
-
Impact of Intermittent Screening and Treat-
ment for Malaria among School Children in
Medicine, 11, e1001594.
& Comm, S.
New England Journal of Medicine, 366,
765-766.
-
sen, P. & Clarke, S. -
to Prevent Malaria in Pregnancy in an area
of low transmission in Uganda. Interna-
tional Health, 4, 38-46.
& Yeung, S.
for a rapid malaria diagnostic test and
artemisinin-based combination therapy
from private drug shops in Mukono district,
Uganda. Health Policy and Planning, 28,
185-96.
Matowo, N., Lorenz, L., Devine, G. &
its potential use in malaria control. Para-
sites & Vectors, 6: :144.
-
-
murine immune memory. Parasite Immunol-
ogy, 36, 199-206.
Hemingway, J., Vontas, J., Poupardin,
R., Raman, J., Lines, J., Schwabe, C.,
Country-level operational implementation of
the Global Plan for Insecticide Resistance
Management. Proceedings of the National
Hendriksen, I., Maiga, D., Lemnge, M.,
Mtove, G., Gesase, S., Reyburn, H.,
Lindegardh, N., Day, N., Von Seidlein,
L., Dondorp, A., Tarning, J. & White, N.
pharmacodynamic properties of intramus-
cular quinine in Tanzanian children with
Gesase, S., Reyburn, H., Lemnge, M.,
Lindegardh, N., Day, N., Von Seidlein,
L., White, N., Dondorp, A. & Tarning, J.
with severe malaria: implications for a prac-
tical dosing regimen. Clinical Pharmacology
and Therapeutics, 93, 443-50.
Directional selection at the pfmdr1, pfcrt,
pfubp1 and pfap2mu loci of Plasmodium
falciparum in Kenyan children treated with
pii: jiu358.
Herrera-Varela, M., Lindh, J., Lindsay, S.
& Fillinger, U. -
lato - a push-pull system. Malaria Journal,
13, 133.

Publications 2012-14 119
Malaria Centre Report 2012-14
118 Publications 2012-14
London School of Hygiene & Tropical Medicine
of Plasmodium Falciparum-Infected Whole
Blood With Mirasol. Vox Sanguinis, 103,
137-137.
Exploring health providers’ and community
perceptions and experiences with malaria
tests in South-East Nigeria: a critical step
towards appropriate treatment. Malaria
Journal, 11, 368.
Wanzira, H., Mpimbaza, A., Nsobya, S.,
White, N., Webb, E., Staedke, S. & Drake-
ley, C.
clearance of Plasmodium falciparum game-
tocytes in children with uncomplicated ma-
laria in Uganda: a randomised, controlled,
double-blind, dose-ranging trial. The Lancet
Infectious Diseases.14:2, 130 - 139.
Eziefula, A., Gosling, R., Hwang, J.,
I. A. D.
transmission. Malaria Journal, 11, 360.
Hallett, R., Vennerstrom, J., Duong, S.,
Ringwald, P., Wellems, T., Plowe, C. &
Dondorp, A.
-
ties, and Public Health Implications. The
Hygiene, 87, 231-241.
Fancony, C., Gamboa, D., Sebastiao,
Y., Hallett, R., Sutherland, C., Sousa-
Figueiredo, J. & Nery, S.
pfcrt and pfmdr1 Genotypes of Plasmodium
falciparum Cocirculate with P. malariae, P.
56, 5271-5277.
Community perceptions of a malaria vac-
cine in the Kintampo districts of Ghana.
Malaria Journal, 12, 156.
N., De Souza, J., Grady, L., Saris, C.,
signalling regulates memory CD4+ T cell
populations and suppresses rapid in-
malaria infection. Infection and Immunity,
M., Riley, E. & Walther, M.
thaw lysates of P. falciparum-infected red
blood cells induce differentiation of func-
tionally competent regulatory T cells from
memory T cells. European Journal of Im-
parasite epigenetics: when virulence and
romance collide. Cell Host & Microbe, 16,
148-50.
Franco, A., Gomes, M., Rowland, M.,
Coleman, P. & Davies, C. -
trolling Malaria Using Livestock-Based
Gadalla, N., Abdallah, T., Atwal, S.,
Sutherland, C. & Adam, I. -
tion of pfdhfr/pfdhps alleles and declining
artesunate/sulphadoxine-pyrimethamine ef-
years after deployment in eastern Sudan.
Malaria Journal, 12, 255.
Gatton, M., Chitnis, N., Churcher, T.,
Donnelly, M., Ghani, A., Godfray, H.,
Gould, F., Hastings, I., Marshall, J.,
Ranson, H., Rowland, M., Shaman, J.
& Lindsay, S.
-
1218-1230.
Gaudart, J., Huiart, L., Milligan, P., Thie-
baut, R. & Giorgi, R. -
ibility issues in science, is P value really the
only answer? Proceedings of the National
Gayer, M., Golaz, A., Howard, N. & Schil-
peroord, M. -
nation. In: Howard, N. & Clements-Hunt,
-
book, 2nd Edition. Geneva: World Health
Gayer, M., Golaz, A., Howard, N. & Schil-
peroord, M. -
ment and operational planning. In: oward,
-
Lietman, T. -
mycin Distribution on Malaria Parasitemia
during the Low-Transmission Season in
-
Etego, L., Anyorigiya, T., Hodgson, A.,
D. -
moglobin C and haemoglobin S and the
dynamics of the evolutionary response to
malaria in Kassena-Nankana District of
Ghumra, A., Semblat, J., Ataide, R.,
M., Amambua-Ngwa, A., Walther, M.,
Virulent Malaria Parasites. Plos Pathogens,
8, e1002665.
Plasmodium infection, anaemia and mos-
quito net use among school children across
different settings in Kenya. Tropical Medi-
cine & International Health, 17, 858-70.
-
S.
in Malaria School Surveys in Kenya:
Does their Under-performance Matter for
Journal of Tropical Medicine and Hygiene,
C. & Chiodini, P.
malaria prevention advice to Public Health
England, Malaria Reference Labora-
Travel Medicine and Infectious Disease,
vaccination to global health: past, present
and future. Philosophical Transactions of
the Royal Society of London Series B, Bio-
consortium approach to malaria research
and capacity development. Tropical Medi-
much to do. Lancet, 383, 1703-4.
Grigg, M., William, T., Drakeley, C., Jelip,
Factors that are associated with the risk
of acquiring Plasmodium knowlesi malaria
in Sabah, Malaysia: a case-control study
e006004.
G., Renia, L., De Souza, J. & Riley, E.
-
hibitory Pathways Independently Regulate
Host Resistance to Plasmodium-induced
8, e1002504.
-
modium falciparum, anaemia and cogni-
tive and educational performance among
school children in an area of moderate
malaria transmission: baseline results of
a cluster randomized trial on the coast of
Kenya. Tropical Medicine & International
Health, 17, 532-549.
-
Impact of Intermittent Screening and Treat-
ment for Malaria among School Children in
Medicine, 11, e1001594.
& Comm, S.
New England Journal of Medicine, 366,
765-766.
-
sen, P. & Clarke, S. -
to Prevent Malaria in Pregnancy in an area
of low transmission in Uganda. Interna-
tional Health, 4, 38-46.
& Yeung, S.
for a rapid malaria diagnostic test and
artemisinin-based combination therapy
from private drug shops in Mukono district,
Uganda. Health Policy and Planning, 28,
185-96.
Matowo, N., Lorenz, L., Devine, G. &
its potential use in malaria control. Para-
sites & Vectors, 6: :144.
-
-
murine immune memory. Parasite Immunol-
ogy, 36, 199-206.
Hemingway, J., Vontas, J., Poupardin,
R., Raman, J., Lines, J., Schwabe, C.,
Country-level operational implementation of
the Global Plan for Insecticide Resistance
Management. Proceedings of the National
Hendriksen, I., Maiga, D., Lemnge, M.,
Mtove, G., Gesase, S., Reyburn, H.,
Lindegardh, N., Day, N., Von Seidlein,
L., Dondorp, A., Tarning, J. & White, N.
pharmacodynamic properties of intramus-
cular quinine in Tanzanian children with
Gesase, S., Reyburn, H., Lemnge, M.,
Lindegardh, N., Day, N., Von Seidlein,
L., White, N., Dondorp, A. & Tarning, J.
with severe malaria: implications for a prac-
tical dosing regimen. Clinical Pharmacology
and Therapeutics, 93, 443-50.
Directional selection at the pfmdr1, pfcrt,
pfubp1 and pfap2mu loci of Plasmodium
falciparum in Kenyan children treated with
pii: jiu358.
Herrera-Varela, M., Lindh, J., Lindsay, S.
& Fillinger, U. -
lato - a push-pull system. Malaria Journal,
13, 133.

Publications 2012-14 121
Malaria Centre Report 2012-14
120 Publications 2012-14
London School of Hygiene & Tropical Medicine
Hill, J., D’mello-Guyett, L., Hoyt, J., Van
for the Case Management of Malaria during
Smith, H. & Webster, J.
affecting the delivery, access, and use of
interventions to prevent malaria in preg-
review and meta-analysis. PLoS Medicine,
10, e1001488.
-
-
Effectiveness of antenatal clinics to deliver
intermittent preventive treatment and insec-
ticide treated nets for the control of malaria
in pregnancy in mali: a household survey.
P. & Lindsay, S.
Mosquito House Entry in the Lao PDR.
Hopkins, H., Gonzalez, I., Polley, S.,
Angutoko, P., Ategeka, J., Asiimwe, C.,
Sensitive Detection of Malaria Parasitemia
in a Malaria-Endemic Setting: Performance
-
The Journal of Infectious Diseases, 208,
645-652.
The role of cGMP signalling in regulating
life cycle progression of Plasmodium. Mi-
crobes and Infection / Institut Pasteur.
Hopp, C., Flueck, C., Solyakov, L., Tobin,
Functional Characterisation of the Plasmo-
dium falciparum cGMP-Dependent Protein
-
ingu, J., Dekker, D., Leach, A., Moris, P.,
Cohen, J., Vekemans, J., Villafana, T.,
Seidlein, L. & Riley, E.
NK Cell Responses after Immunization of
Malaria Vaccine. Journal of Immunology
(Baltimore, Md, 188, 5054-62.
Horowitz, A. & Riley, E.
of human NK cells by Plasmodium-infected
red blood cells. Methods in Molecular Biol-
Howard, N. & Clements-Hunt, A.
Malaria control in humanitarian emergen-
-
tion.
Chea, N., Yok, S., Top, S., Ros, S., So-
phal, U., Thompson, M., Mellor, S., Ariey,
Duong, S., Newman, R. & Menard, D.
Malaria Parasite Carriers and Contain Drug
Resistant P. falciparum, Pailin, Cambodia.
-
G.
the proportion of human exposure to ma-
laria vector populations occurring indoors in
-
Imai, N., White, M., Ghani, A. & Drake-
ley, C.
Modelling Study. PLoS Neglected Tropical
Diseases, 8, e2978.
M. & Cameron, M.
nonanal-trimethylamine lure for collection of
in gravid traps. Journal of Medical Entomol-
ogy, 50, 619-23.
Jallow, M., Casals-Pascual, C., Acker-
M., Sisay-Joof, F., Usen, S., Abubakar, I.,
Clinical features of severe malaria associ-
ated with death: a 13-year observational
Jaramillo Ramirez, G., Logan, J., Loza-
Reyes, E., Stashenko, E. & Moores, G.
e48698.
Jarvis, J., Coltart, C., Pule, M., Chiodini,
P. & Doherty, T.
and severe delayed haemolysis. Lancet,
382, 180.
Magesa, S.
of Tanzania. Tropical Medicine & Interna-
tional Health, 19:3.
-
Protopopoff, N., Magesa, S., Mosha,
spread of pyrethroid and DDT resistance
Tanzania. Medical and Veterinary Entomol-
commitment tosexual development in ma-
laria parasites. Nature, 507, 248–252.
-
he, R., Perlmann, H., Takeo, S., Tsuboi,
Drakeley, C.
Distribution of Plasmodium vivax Infections
-
Alegana, V., Nyandigisi, A., Pandit, J.,
Fegan, G., Todd, J., Snow, R. & Good-
man, C.
malarial subsidy programme on the quality
of service provision of artemisinin-based
combination therapy in Kenya: a cluster-
randomized, controlled trial. Malaria Jour-
nal, 12.
-
burn, H., Agbenyega, T., Taylor, T.,
Epilepsia, 54, 990-1001.
-
sion patterns in Navrongo demographic
surveillance site, northern Ghana. Malaria
Journal, 12, 63.
-
J., Roper, C. & Alifrangis, M.
Surveillance of artemether-lumefantrine as-
sociated Plasmodium falciparum multidrug
resistance protein-1 gene polymorphisms in
Tanzania. Malaria Journal, 13, 264.
Naidoo, I., Roper, C., Mulokozi, A.,
Macarthur, J., Luntamo, M., Ashorn,
Intermittent Preventive Therapy for Malaria
During Pregnancy Using 2 vs 3 or More
Doses of Sulfadoxine-Pyrimethamine and
-
594-604.
S., Snow, R. & Goodman, C.
Understanding the Impact of Subsidizing
Focus Group Discussions in Rural Kenya.
hosting vectors. The Journal of the Royal
or Waiting? Topologies of the Breeding
Ground in Malaria Control. Science as Cul-
ture, 22, 86-107.
-
-
wanyi, A., Smith, E., Somi, M., Lyimo, T.,
artemisinin-based combination treatment
prevalence in Tanzania: an observational
study. Malaria Journal, 11, 140.
H., Magesa, S., Mosha, F., Rowland, M.
& Logan, J. -
perimental hut evaluation of a long-lasting
insecticide treated blanket for protection
against mosquitoes. Parasites and Vectors,
7, 129.
indicators for eliminating malaria transmis-
sion. Biology Letters, 8, 874-877.
Staedke, S. & Chandler, C. -
proving access to health care for malaria
-
tracts patients. Malaria Journal, 11.
Lauinger, I., Vivas, L., Perozzo, R.,
Pham, D., Esguerra, C., Crawford, A.,
Maes, L. & Tasdemir, D.
of Lichen Secondary Metabolites against
Plasmodium Liver Stage Parasites with
Natural Products, 76, 1064-1070.
Leslie, T., Mikhail, A., Mayan, I., Cundill,
& Rowland, M.
tests to improve treatment of malaria and
other febrile illnesses: patient randomised
effectiveness trial in primary care clinics in
-
-
for treatment policy in the region. Malaria
Journal, 12, 230.
-
bining malaria vector control interventions:
some trial design issues. Pathogens and
global health, 107, 1-4.
S., Hashim, R., Maxwell, C., Chandramo-
han, D. & Gosling, R.
among Young Children and Mosquito Vec-
tor Numbers? Evidence from Korogwe,
Plenderleith, L., Malenke, J., Sunda-
raraman, S., Ramirez, M., Crystal, P.,
Locatelli, S., Esteban, A., Mouacha, F.,
S., Sanz, C., Morgan, D., Gonder, M.,
Muller, M., Piel, A., Stewart, F., Wilson,

Publications 2012-14 121
Malaria Centre Report 2012-14
120 Publications 2012-14
London School of Hygiene & Tropical Medicine
Hill, J., D’mello-Guyett, L., Hoyt, J., Van
for the Case Management of Malaria during
Smith, H. & Webster, J.
affecting the delivery, access, and use of
interventions to prevent malaria in preg-
review and meta-analysis. PLoS Medicine,
10, e1001488.
-
-
Effectiveness of antenatal clinics to deliver
intermittent preventive treatment and insec-
ticide treated nets for the control of malaria
in pregnancy in mali: a household survey.
P. & Lindsay, S.
Mosquito House Entry in the Lao PDR.
Hopkins, H., Gonzalez, I., Polley, S.,
Angutoko, P., Ategeka, J., Asiimwe, C.,
Sensitive Detection of Malaria Parasitemia
in a Malaria-Endemic Setting: Performance
-
The Journal of Infectious Diseases, 208,
645-652.
The role of cGMP signalling in regulating
life cycle progression of Plasmodium. Mi-
crobes and Infection / Institut Pasteur.
Hopp, C., Flueck, C., Solyakov, L., Tobin,
Functional Characterisation of the Plasmo-
dium falciparum cGMP-Dependent Protein
-
ingu, J., Dekker, D., Leach, A., Moris, P.,
Cohen, J., Vekemans, J., Villafana, T.,
Seidlein, L. & Riley, E.
NK Cell Responses after Immunization of
Malaria Vaccine. Journal of Immunology
(Baltimore, Md, 188, 5054-62.
Horowitz, A. & Riley, E.
of human NK cells by Plasmodium-infected
red blood cells. Methods in Molecular Biol-
Howard, N. & Clements-Hunt, A.
Malaria control in humanitarian emergen-
-
tion.
Chea, N., Yok, S., Top, S., Ros, S., So-
phal, U., Thompson, M., Mellor, S., Ariey,
Duong, S., Newman, R. & Menard, D.
Malaria Parasite Carriers and Contain Drug
Resistant P. falciparum, Pailin, Cambodia.
-
G.
the proportion of human exposure to ma-
laria vector populations occurring indoors in
-
Imai, N., White, M., Ghani, A. & Drake-
ley, C.
Modelling Study. PLoS Neglected Tropical
Diseases, 8, e2978.
M. & Cameron, M.
nonanal-trimethylamine lure for collection of
in gravid traps. Journal of Medical Entomol-
ogy, 50, 619-23.
Jallow, M., Casals-Pascual, C., Acker-
M., Sisay-Joof, F., Usen, S., Abubakar, I.,
Clinical features of severe malaria associ-
ated with death: a 13-year observational
Jaramillo Ramirez, G., Logan, J., Loza-
Reyes, E., Stashenko, E. & Moores, G.
e48698.
Jarvis, J., Coltart, C., Pule, M., Chiodini,
P. & Doherty, T.
and severe delayed haemolysis. Lancet,
382, 180.
Magesa, S.
of Tanzania. Tropical Medicine & Interna-
tional Health, 19:3.
-
Protopopoff, N., Magesa, S., Mosha,
spread of pyrethroid and DDT resistance
Tanzania. Medical and Veterinary Entomol-
commitment tosexual development in ma-
laria parasites. Nature, 507, 248–252.
-
he, R., Perlmann, H., Takeo, S., Tsuboi,
Drakeley, C.
Distribution of Plasmodium vivax Infections
-
Alegana, V., Nyandigisi, A., Pandit, J.,
Fegan, G., Todd, J., Snow, R. & Good-
man, C.
malarial subsidy programme on the quality
of service provision of artemisinin-based
combination therapy in Kenya: a cluster-
randomized, controlled trial. Malaria Jour-
nal, 12.
-
burn, H., Agbenyega, T., Taylor, T.,
Epilepsia, 54, 990-1001.
-
sion patterns in Navrongo demographic
surveillance site, northern Ghana. Malaria
Journal, 12, 63.
-
J., Roper, C. & Alifrangis, M.
Surveillance of artemether-lumefantrine as-
sociated Plasmodium falciparum multidrug
resistance protein-1 gene polymorphisms in
Tanzania. Malaria Journal, 13, 264.
Naidoo, I., Roper, C., Mulokozi, A.,
Macarthur, J., Luntamo, M., Ashorn,
Intermittent Preventive Therapy for Malaria
During Pregnancy Using 2 vs 3 or More
Doses of Sulfadoxine-Pyrimethamine and
-
594-604.
S., Snow, R. & Goodman, C.
Understanding the Impact of Subsidizing
Focus Group Discussions in Rural Kenya.
hosting vectors. The Journal of the Royal
or Waiting? Topologies of the Breeding
Ground in Malaria Control. Science as Cul-
ture, 22, 86-107.
-
-
wanyi, A., Smith, E., Somi, M., Lyimo, T.,
artemisinin-based combination treatment
prevalence in Tanzania: an observational
study. Malaria Journal, 11, 140.
H., Magesa, S., Mosha, F., Rowland, M.
& Logan, J. -
perimental hut evaluation of a long-lasting
insecticide treated blanket for protection
against mosquitoes. Parasites and Vectors,
7, 129.
indicators for eliminating malaria transmis-
sion. Biology Letters, 8, 874-877.
Staedke, S. & Chandler, C. -
proving access to health care for malaria
-
tracts patients. Malaria Journal, 11.
Lauinger, I., Vivas, L., Perozzo, R.,
Pham, D., Esguerra, C., Crawford, A.,
Maes, L. & Tasdemir, D.
of Lichen Secondary Metabolites against
Plasmodium Liver Stage Parasites with
Natural Products, 76, 1064-1070.
Leslie, T., Mikhail, A., Mayan, I., Cundill,
& Rowland, M.
tests to improve treatment of malaria and
other febrile illnesses: patient randomised
effectiveness trial in primary care clinics in
-
-
for treatment policy in the region. Malaria
Journal, 12, 230.
-
bining malaria vector control interventions:
some trial design issues. Pathogens and
global health, 107, 1-4.
S., Hashim, R., Maxwell, C., Chandramo-
han, D. & Gosling, R.
among Young Children and Mosquito Vec-
tor Numbers? Evidence from Korogwe,
Plenderleith, L., Malenke, J., Sunda-
raraman, S., Ramirez, M., Crystal, P.,
Locatelli, S., Esteban, A., Mouacha, F.,
S., Sanz, C., Morgan, D., Gonder, M.,
Muller, M., Piel, A., Stewart, F., Wilson,
Publications 2012-14 123
Malaria Centre Report 2012-14
122 Publications 2012-14
London School of Hygiene & Tropical Medicine
A., Sutherland, C., Nolder, D., Hart, J.,
-
E., Delaporte, E., Carter, R., Culleton, R.,
Shaw, G., Rayner, J., Peeters, M., Hahn,
malaria parasite Plasmodium vivax. Nature
Communications, 5, 3346.
Liu, Y., Auburn, S., Cao, J., Trimarsanto,
structure of Plasmodium vivax in Central
China. Malaria Journal, 13, 262.
Tine, R., Abiola, A., Ndiaye, M., Ndiaye,
J., Ndiaye, D., Sokhna, C., Gomis, J.,
Cairns, M., Hallett, R., Sutherland, C. &
markers of drug resistance in an area of
seasonal malaria chemoprevention in chil-
dren in Senegal. Malaria Journal, 12, 137.
C., Seeholzer, L., Mseka, A., Simfukwe,
Moore, S.
directional movement of mosquitoes to ol-
factory cues. Parasites and Vectors, 6, 131.
Lover, A. & Coker, R.
Effect of Geographic Location on Epidemi-
ology of Plasmodium vivax Malaria. Emerg-
ing Infectious Diseases, 19, 1058-65.
Lover, A. & Coker, R. -
ing the relationship between sporozoite
dose and incubation period in Plasmodium
vivax malaria: a systematic re-analysis.
Parasitology, 141, 859-868.
Lubell, Y., White, L., Varadan, S., Drake,
T., Yeung, S., Cheah, P., Maude, R., Don-
dorp, A., Day, N., White, N. & Parker, M.
primaquine to reduce falciparum malaria
transmission in asymptomatic populations.
PLoS Medicine, 11, e1001704.
-
nasar, D., Durrheim, D., Seocharan,
-
schmidt, I.
779-83.
-
we, E., Turner, E. & Moore, S.
Topical Repellents Divert Mosquitoes within
a Community? - Health Equity Implications
of Topical Repellents as a Mosquito Bite
Tapily, A., Campino, S., Sepulveda, N.,
-
Receptor IIa- H131R polymorphism and
malaria susceptibility in sympatric ethnic
groups, Fulani and Dogon of Mali. Scandi-
Tapily, A., Campino, S., Sepulveda, N.,
Risley, P., Silva, N., Corran, P., Rockett,
-
phisms in sympatric ethnic groups differing
8, e75675.
Malima, R., Tungu, P., Mwingira, V., Max-
& Rowland, M.
long-lasting insecticidal net Interceptor LN:
laboratory and experimental hut studies
against anopheline and culicine mosquitoes
in northeastern Tanzania. Parasites and
Vectors, 6, 296.
-
preference for the treatment of uncompli-
cated malaria? Social Science & Medicine
Ambebila, J., Lele, A., Metoh, T., Ndive,
J. & Mbacham, W. -
lence and treatment of febrile patients at
health facilities and medicine retailers in
Cameroon. Tropical Medicine & Interna-
tional Health, 17, 330-42.
Mtove, G., Wangai, H., Sepulveda, N.,
M., Riley, E., Reyburn, H. & Drakeley, C.
-
phisms and severe malaria in a tanzanian
Auburn, S., Almagro-Garcia, J., Maslen,
Amaratunga, C., Fairhurst, R., Socheat,
D., Nosten, F., Imwong, M., White, N.,
Sanders, M., Anastasi, E., Alcock, D.,
Ruano-Rubio, V., Jyothi, D., Amenga-
Etego, L., Hubbart, C., Jeffreys, A.,
Mangano, V., Modiano, D., Tan, J., Fer-
dig, M., Amambua-Ngwa, A., Conway, D.,
Takala-Harrison, S., Plowe, C., Rayner,
-
kowski, D.
falciparum diversity in natural infections by
deep sequencing. Nature, 487, 375-9.
Marks, M., Armstrong, M., Suvari, M.,
-
inghan, G. & Doherty, J.
imported falciparum malaria among adults
requiring intensive care: a retrospective
study at the hospital for tropical diseases,
London. BMC Infectious Diseases, 13, 118.
Matowo, N., Moore, J., Mapua, S., Mad-
-
a new odour-baited device to explore op-
tions for luring and killing outdoor-biting
malaria vectors: a report on design and
Box. Parasites & Vectors, 6:137.
Mbacham, W., Mangham-Jefferies, L.,
Ambebila, J., Nkwescheu, A., Forsah-
Achu, D., Ndiforchu, V., Tchekountouo,
Wiseman, V.
clinician training to improve adherence to
malaria treatment guidelines: a cluster-
randomised trial in two areas of Cameroon.
Lancet Global Health, 2, E346-E358.
evaluation of lethal and sub-lethal effects of
slow release pyriproxyfen granules (Sumi-
Malaria Journal, 12: 94.
Mbogo, G., Nankoberanyi, S., Tukwa-
Tappero, J., Staedke, S., Dorsey, G.,
Temporal Changes in Prevalence of Mo-
Resistance in a High Malaria Transmission
61.
Treatment of fevers prior to introducing
rapid diagnostic tests for malaria in regis-
tered drug shops in Uganda. Malaria Jour-
nal, 12:131.
Menaca, A., Pell, C., Manda-Taylor, L.,
Chatio, S., Afrah, N., Were, F., Hodgson,
Pool, R.
their relevance for the prevention and con-
trol of malaria during pregnancy in Ghana,
-
parative qualitative study. Malaria Journal,
12, 257.
Amambua-Ngwa, A., Gomez-Escobar, N.,
Walther, M., Conway, D. & Duraisingh,
M.
Virulence Gene Expression in Severe Plas-
modium falciparum Malaria. The Journal of
Infectious Diseases, 205, 1593-600.
Messenger, L., Matias, A., Manana, A.,
Rowland, M.
of insecticide-treated durable wall lining in
358.
Messenger, L., Miller, N., Adeogun, A.,
Awolola, T. & Rowland, M.
development of insecticide-treated durable
wall lining for malaria control: insights from
Nigeria. Malaria Journal, 11, 332.
Mills, A.
low- and middle-income countries. The
New England Journal of Medicine, 370,
552-7.
Mills, A. -
San Diego: Elsevier.
Mills, A. & Hsu, J.
in Low- and Middle-Income Countries:
Financing, Payment, and Provision. In:
Economics. San Diego: Elsevier.
Mimche, P., Thompson, E., Taramelli, D.
& Vivas, L.
non-opsonic phagocytosis of Plasmodium
falciparum through up-regulation of CD36
surface expression on monocytes/macro-
-
-
S., Sreng, S., Anderson, J., Duong, S.,
Nguon, C., Chuor, C., Saunders, D., Se,
Y., Lon, C., Fukuda, M., Amenga-Etego,
L., Hodgson, A., Asoala, V., Imwong, M.,
Ringwald, P., Ariey, F., Dolecek, C., Hien,
-
ers, M., Hubbart, C., Maslen, G., Ruano-
D., Dondorp, A., Plowe, C., Fairhurst, R.
-
tions of artemisinin-resistant Plasmodium
falciparum in Cambodia. Nature Genetics,
45, 648-55.
Lusingu, J., Drakeley, C., Fay, M., Long,
C. & Vekemans, J. -
gested human antibodies induced by RTS,
Plasmodium falciparum oocyst formation
and sporogony in mosquitoes. Malaria
Journal, 13, 263.
Mobegi, V., Duffy, C., Amambua-Ngwa,
-
-
way, D.
selection on the malaria parasite Plasmo-
of differing infection endemicity. Molecular
Satoguina, J., Nwakanma, D., Amambua-

Publications 2012-14 123
Malaria Centre Report 2012-14
122 Publications 2012-14
London School of Hygiene & Tropical Medicine
A., Sutherland, C., Nolder, D., Hart, J.,
-
E., Delaporte, E., Carter, R., Culleton, R.,
Shaw, G., Rayner, J., Peeters, M., Hahn,
malaria parasite Plasmodium vivax. Nature
Communications, 5, 3346.
Liu, Y., Auburn, S., Cao, J., Trimarsanto,
structure of Plasmodium vivax in Central
China. Malaria Journal, 13, 262.
Tine, R., Abiola, A., Ndiaye, M., Ndiaye,
J., Ndiaye, D., Sokhna, C., Gomis, J.,
Cairns, M., Hallett, R., Sutherland, C. &
markers of drug resistance in an area of
seasonal malaria chemoprevention in chil-
dren in Senegal. Malaria Journal, 12, 137.
C., Seeholzer, L., Mseka, A., Simfukwe,
Moore, S.
directional movement of mosquitoes to ol-
factory cues. Parasites and Vectors, 6, 131.
Lover, A. & Coker, R.
Effect of Geographic Location on Epidemi-
ology of Plasmodium vivax Malaria. Emerg-
ing Infectious Diseases, 19, 1058-65.
Lover, A. & Coker, R. -
ing the relationship between sporozoite
dose and incubation period in Plasmodium
vivax malaria: a systematic re-analysis.
Parasitology, 141, 859-868.
Lubell, Y., White, L., Varadan, S., Drake,
T., Yeung, S., Cheah, P., Maude, R., Don-
dorp, A., Day, N., White, N. & Parker, M.
primaquine to reduce falciparum malaria
transmission in asymptomatic populations.
PLoS Medicine, 11, e1001704.
-
nasar, D., Durrheim, D., Seocharan,
-
schmidt, I.
779-83.
-
we, E., Turner, E. & Moore, S.
Topical Repellents Divert Mosquitoes within
a Community? - Health Equity Implications
of Topical Repellents as a Mosquito Bite
Tapily, A., Campino, S., Sepulveda, N.,
-
Receptor IIa- H131R polymorphism and
malaria susceptibility in sympatric ethnic
groups, Fulani and Dogon of Mali. Scandi-
Tapily, A., Campino, S., Sepulveda, N.,
Risley, P., Silva, N., Corran, P., Rockett,
-
phisms in sympatric ethnic groups differing
8, e75675.
Malima, R., Tungu, P., Mwingira, V., Max-
& Rowland, M.
long-lasting insecticidal net Interceptor LN:
laboratory and experimental hut studies
against anopheline and culicine mosquitoes
in northeastern Tanzania. Parasites and
Vectors, 6, 296.
-
preference for the treatment of uncompli-
cated malaria? Social Science & Medicine
Ambebila, J., Lele, A., Metoh, T., Ndive,
J. & Mbacham, W. -
lence and treatment of febrile patients at
health facilities and medicine retailers in
Cameroon. Tropical Medicine & Interna-
tional Health, 17, 330-42.
Mtove, G., Wangai, H., Sepulveda, N.,
M., Riley, E., Reyburn, H. & Drakeley, C.
-
phisms and severe malaria in a tanzanian
Auburn, S., Almagro-Garcia, J., Maslen,
Amaratunga, C., Fairhurst, R., Socheat,
D., Nosten, F., Imwong, M., White, N.,
Sanders, M., Anastasi, E., Alcock, D.,
Ruano-Rubio, V., Jyothi, D., Amenga-
Etego, L., Hubbart, C., Jeffreys, A.,
Mangano, V., Modiano, D., Tan, J., Fer-
dig, M., Amambua-Ngwa, A., Conway, D.,
Takala-Harrison, S., Plowe, C., Rayner,
-
kowski, D.
falciparum diversity in natural infections by
deep sequencing. Nature, 487, 375-9.
Marks, M., Armstrong, M., Suvari, M.,
-
inghan, G. & Doherty, J.
imported falciparum malaria among adults
requiring intensive care: a retrospective
study at the hospital for tropical diseases,
London. BMC Infectious Diseases, 13, 118.
Matowo, N., Moore, J., Mapua, S., Mad-
-
a new odour-baited device to explore op-
tions for luring and killing outdoor-biting
malaria vectors: a report on design and
Box. Parasites & Vectors, 6:137.
Mbacham, W., Mangham-Jefferies, L.,
Ambebila, J., Nkwescheu, A., Forsah-
Achu, D., Ndiforchu, V., Tchekountouo,
Wiseman, V.
clinician training to improve adherence to
malaria treatment guidelines: a cluster-
randomised trial in two areas of Cameroon.
Lancet Global Health, 2, E346-E358.
evaluation of lethal and sub-lethal effects of
slow release pyriproxyfen granules (Sumi-
Malaria Journal, 12: 94.
Mbogo, G., Nankoberanyi, S., Tukwa-
Tappero, J., Staedke, S., Dorsey, G.,
Temporal Changes in Prevalence of Mo-
Resistance in a High Malaria Transmission
61.
Treatment of fevers prior to introducing
rapid diagnostic tests for malaria in regis-
tered drug shops in Uganda. Malaria Jour-
nal, 12:131.
Menaca, A., Pell, C., Manda-Taylor, L.,
Chatio, S., Afrah, N., Were, F., Hodgson,
Pool, R.
their relevance for the prevention and con-
trol of malaria during pregnancy in Ghana,
-
parative qualitative study. Malaria Journal,
12, 257.
Amambua-Ngwa, A., Gomez-Escobar, N.,
Walther, M., Conway, D. & Duraisingh,
M.
Virulence Gene Expression in Severe Plas-
modium falciparum Malaria. The Journal of
Infectious Diseases, 205, 1593-600.
Messenger, L., Matias, A., Manana, A.,
Rowland, M.
of insecticide-treated durable wall lining in
358.
Messenger, L., Miller, N., Adeogun, A.,
Awolola, T. & Rowland, M.
development of insecticide-treated durable
wall lining for malaria control: insights from
Nigeria. Malaria Journal, 11, 332.
Mills, A.
low- and middle-income countries. The
New England Journal of Medicine, 370,
552-7.
Mills, A. -
San Diego: Elsevier.
Mills, A. & Hsu, J.
in Low- and Middle-Income Countries:
Financing, Payment, and Provision. In:
Economics. San Diego: Elsevier.
Mimche, P., Thompson, E., Taramelli, D.
& Vivas, L.
non-opsonic phagocytosis of Plasmodium
falciparum through up-regulation of CD36
surface expression on monocytes/macro-
-
-
S., Sreng, S., Anderson, J., Duong, S.,
Nguon, C., Chuor, C., Saunders, D., Se,
Y., Lon, C., Fukuda, M., Amenga-Etego,
L., Hodgson, A., Asoala, V., Imwong, M.,
Ringwald, P., Ariey, F., Dolecek, C., Hien,
-
ers, M., Hubbart, C., Maslen, G., Ruano-
D., Dondorp, A., Plowe, C., Fairhurst, R.
-
tions of artemisinin-resistant Plasmodium
falciparum in Cambodia. Nature Genetics,
45, 648-55.
Lusingu, J., Drakeley, C., Fay, M., Long,
C. & Vekemans, J. -
gested human antibodies induced by RTS,
Plasmodium falciparum oocyst formation
and sporogony in mosquitoes. Malaria
Journal, 13, 263.
Mobegi, V., Duffy, C., Amambua-Ngwa,
-
-
way, D.
selection on the malaria parasite Plasmo-
of differing infection endemicity. Molecular
Satoguina, J., Nwakanma, D., Amambua-

Publications 2012-14 125
Malaria Centre Report 2012-14
124 Publications 2012-14
London School of Hygiene & Tropical Medicine
Ngwa, A. & Conway, D.
genetic structure of Plasmodium falciparum
across a region of diverse endemicity in
F., Alifrangis, M., Reyburn, H., Roper, C.
-
quine resistance marker, Pfcrt-K76T muta-
tion ten years after chloroquine withdrawal
in Tanzania. Malaria Journal, 12, 415.
Medical Journal, 103, 801-6.
Moore, S., Mordue Luntz, A. & Logan, J.
73.
Hill, N. & And Cameron, M.
Malaria in China: Use of Personal Protec-
tion by Minority Populations. BMC Public
Health 8:344.
Moorthy, V., Newman, R., Duclos, P.,
-
The Lancet Infectious Diseases, 13, 280-
282.
Hung, N., Coosemans, M., D’alessandro,
U. & Mills, A.
of Long-Lasting Insecticide-Treated Ham-
mocks in Preventing Malaria in South-Cen-
-
ling, R.
Plasmodium falciparum infection: implica-
tions for detection of hotspots with imper-
fect diagnostics. Malaria Journal, 12:221.
Sutherland, C., Gadalla, N., Atwal, S.,
D. & Gosling, R.
a comparison of spatial statistical methods
to predict prospective malaria infections.
Malaria Journal, 13, 53.
Moyes, C., Henry, A., Golding, N., Huang,
-
Plasmodium knowlesi Reservoir. PLoS Ne-
glected Tropical Diseases, 8, e2780.
-
-
vation for providing intermittent preventive
treatment of malaria during pregnancy in
Tanzania: evidence from two rural districts.
Malaria Journal 11:48.
-
Felger, I.
to understanding the epidemiology of Plas-
modium falciparum malaria in Papua New
Guinean children. Proceedings of the Na-
-
aging malaria in tuberculosis patients on
-
sessing the risk of QT prolongation. The
International Journal of Tuberculosis and
Lung Disease, 16, 144-149.
-
land, M.
-
permethrin Control Pyrethroid Resistant
-
9, e87710.
N’guessan, R. & Rowland, M.
Indoor residual spraying for prevention of
malaria. The Lancet Infectious Diseases,
12:8, 581 - 582.
an update for physicians. Infectious Dis-
-
Reyburn, H.
-
ted to the Hospital with Febrile Illness in
Naidoo, I. & Roper, C.
‘partially resistant’, ‘fully resistant’, and ‘su-
per resistant’ malaria. Trends in Parasitol-
ogy, 29:10, 505–515.
Jayaraman, J., Traherne, J., Elliott, A.,
-
in a Ugandan population. Immunogenetics,
65, 765-775.
-
fett, A. & Mirembe, F. -
-
spective Cohort Study at Mulago Hospital,
Treatment With Dihydroartemisinin-Piper-
aquine on Malaria in Ugandan Schoolchil-
Trial. Clinical Infectious Diseases, 58,
1404-1412.
S.
Infection and Cognition among Primary
Schoolchildren in a High Malaria Trans-
Journal of Tropical Medicine and Hygiene,
Alifrangis, M. -
malarial Drug Resistance after Intermit-
tent Preventive Treatment of Infants and
Journal of Tropical Medicine and Hy-
-
& Schellenberg, D.
case management in malaria: review and
perspectives after four years of operational
experience in Saraya district, south-east
Senegal. Malaria Journal, 12, 240.
Ndibazza, J., Webb, E., Lule, S., Mpair-
Akurut, H., Muhangi, L., Magnussen, P.,
-
sociations between maternal helminth and
malaria infections in pregnancy and clinical
malaria in the offspring: a birth cohort in
entebbe, Uganda. The Journal of Infectious
Diseases, 208, 2007-16.
-
ported malaria-related healthcare services
malaria chemoprophylaxis reduce imported
Malaria Journal, 12, 238.
Ngufor, C., N’guessan, R., Fagbohoun,
Rowland, M. -
Experimental Hut Trial against Pyrethroid
quinquefasciatus in Southern Benin. Plos
N’fale, S., Dabire, R., Johnson, P., Ran-
son, H. & Rowland, M.
Long-lasting Insecticidal Nets for Improved
Nielsen, C., White, M., Goodier, M. &
Riley, E.
CD57 Expression on Human NK Cells and
Relevance to Disease. Frontiers in Immu-
nology, 4, 422.
events resulting from use of drugs with
sulphonamide-containing anti-malarials and
incidence and household costs from three
districts with routine demographic surveil-
lance systems in rural Tanzania. Malaria
Journal, 12: 236.
H., Niyazi, H., Smith, V., Chiodini, P. &
Sutherland, C.
study of malaria in British travellers: Plas-
modium ovale wallikeri and Plasmodium
-
ration of latency. British Medical Journal
Nwakanma, D., Duffy, C., Amambua-
M., Drakeley, C., Sutherland, C., Mil-
resistance in an endemic population over
a 25-year period with resulting genomic
evidence of selection. The Journal of Infec-
Nwakanma, D., Neafsey, D., Jawara,
M., Adiamoh, M., Lund, E., Rodrigues,
Awolola, T., Muskavitch, M. & Conway,
D.
Genetics, 193, 1221-31.
Phou, M., Dysoley, L., Yeung, S., Allen,
H. & Littrell, M. -
cestor that knock us out” and other tales.
-
ment in Cambodia. Malaria Journal, 11,
335.
& Johnson, J.
of Plasmodium infections by conventional
microscopy and the impact of remedial
-
laria Journal, 12, 113.
-
-
& Montgomery, J.
scans provide evidence of adaptive evolu-
tion in Malawian Plasmodium falciparum
isolates. The Journal of Infectious Diseas-
es, pii: jiu349.
-
sitological evaluation of the heterogeneity
of malaria infection in the Gambia. Malaria
Journal, 12, 222.

Publications 2012-14 125
Malaria Centre Report 2012-14
124 Publications 2012-14
London School of Hygiene & Tropical Medicine
Ngwa, A. & Conway, D.
genetic structure of Plasmodium falciparum
across a region of diverse endemicity in
F., Alifrangis, M., Reyburn, H., Roper, C.
-
quine resistance marker, Pfcrt-K76T muta-
tion ten years after chloroquine withdrawal
in Tanzania. Malaria Journal, 12, 415.
Medical Journal, 103, 801-6.
Moore, S., Mordue Luntz, A. & Logan, J.
73.
Hill, N. & And Cameron, M.
Malaria in China: Use of Personal Protec-
tion by Minority Populations. BMC Public
Health 8:344.
Moorthy, V., Newman, R., Duclos, P.,
-
The Lancet Infectious Diseases, 13, 280-
282.
Hung, N., Coosemans, M., D’alessandro,
U. & Mills, A.
of Long-Lasting Insecticide-Treated Ham-
mocks in Preventing Malaria in South-Cen-
-
ling, R.
Plasmodium falciparum infection: implica-
tions for detection of hotspots with imper-
fect diagnostics. Malaria Journal, 12:221.
Sutherland, C., Gadalla, N., Atwal, S.,
D. & Gosling, R.
a comparison of spatial statistical methods
to predict prospective malaria infections.
Malaria Journal, 13, 53.
Moyes, C., Henry, A., Golding, N., Huang,
-
Plasmodium knowlesi Reservoir. PLoS Ne-
glected Tropical Diseases, 8, e2780.
-
-
vation for providing intermittent preventive
treatment of malaria during pregnancy in
Tanzania: evidence from two rural districts.
Malaria Journal 11:48.
-
Felger, I.
to understanding the epidemiology of Plas-
modium falciparum malaria in Papua New
Guinean children. Proceedings of the Na-
-
aging malaria in tuberculosis patients on
-
sessing the risk of QT prolongation. The
International Journal of Tuberculosis and
Lung Disease, 16, 144-149.
-
land, M.
-
permethrin Control Pyrethroid Resistant
-
9, e87710.
N’guessan, R. & Rowland, M.
Indoor residual spraying for prevention of
malaria. The Lancet Infectious Diseases,
12:8, 581 - 582.
an update for physicians. Infectious Dis-
-
Reyburn, H.
-
ted to the Hospital with Febrile Illness in
Naidoo, I. & Roper, C.
‘partially resistant’, ‘fully resistant’, and ‘su-
per resistant’ malaria. Trends in Parasitol-
ogy, 29:10, 505–515.
Jayaraman, J., Traherne, J., Elliott, A.,
-
in a Ugandan population. Immunogenetics,
65, 765-775.
-
fett, A. & Mirembe, F. -
-
spective Cohort Study at Mulago Hospital,
Treatment With Dihydroartemisinin-Piper-
aquine on Malaria in Ugandan Schoolchil-
Trial. Clinical Infectious Diseases, 58,
1404-1412.
S.
Infection and Cognition among Primary
Schoolchildren in a High Malaria Trans-
Journal of Tropical Medicine and Hygiene,
Alifrangis, M. -
malarial Drug Resistance after Intermit-
tent Preventive Treatment of Infants and
Journal of Tropical Medicine and Hy-
-
& Schellenberg, D.
case management in malaria: review and
perspectives after four years of operational
experience in Saraya district, south-east
Senegal. Malaria Journal, 12, 240.
Ndibazza, J., Webb, E., Lule, S., Mpair-
Akurut, H., Muhangi, L., Magnussen, P.,
-
sociations between maternal helminth and
malaria infections in pregnancy and clinical
malaria in the offspring: a birth cohort in
entebbe, Uganda. The Journal of Infectious
Diseases, 208, 2007-16.
-
ported malaria-related healthcare services
malaria chemoprophylaxis reduce imported
Malaria Journal, 12, 238.
Ngufor, C., N’guessan, R., Fagbohoun,
Rowland, M. -
Experimental Hut Trial against Pyrethroid
quinquefasciatus in Southern Benin. Plos
N’fale, S., Dabire, R., Johnson, P., Ran-
son, H. & Rowland, M.
Long-lasting Insecticidal Nets for Improved
Nielsen, C., White, M., Goodier, M. &
Riley, E.
CD57 Expression on Human NK Cells and
Relevance to Disease. Frontiers in Immu-
nology, 4, 422.
events resulting from use of drugs with
sulphonamide-containing anti-malarials and
incidence and household costs from three
districts with routine demographic surveil-
lance systems in rural Tanzania. Malaria
Journal, 12: 236.
H., Niyazi, H., Smith, V., Chiodini, P. &
Sutherland, C.
study of malaria in British travellers: Plas-
modium ovale wallikeri and Plasmodium
-
ration of latency. British Medical Journal
Nwakanma, D., Duffy, C., Amambua-
M., Drakeley, C., Sutherland, C., Mil-
resistance in an endemic population over
a 25-year period with resulting genomic
evidence of selection. The Journal of Infec-
Nwakanma, D., Neafsey, D., Jawara,
M., Adiamoh, M., Lund, E., Rodrigues,
Awolola, T., Muskavitch, M. & Conway,
D.
Genetics, 193, 1221-31.
Phou, M., Dysoley, L., Yeung, S., Allen,
H. & Littrell, M. -
cestor that knock us out” and other tales.
-
ment in Cambodia. Malaria Journal, 11,
335.
& Johnson, J.
of Plasmodium infections by conventional
microscopy and the impact of remedial
-
laria Journal, 12, 113.
-
-
& Montgomery, J.
scans provide evidence of adaptive evolu-
tion in Malawian Plasmodium falciparum
isolates. The Journal of Infectious Diseas-
es, pii: jiu349.
-
sitological evaluation of the heterogeneity
of malaria infection in the Gambia. Malaria
Journal, 12, 222.

Publications 2012-14 127
Malaria Centre Report 2012-14
126 Publications 2012-14
London School of Hygiene & Tropical Medicine
-
draogo, A., Ghani, A. & Drakeley, C.
of submicroscopic malaria infections and
their relevance for control. Nature Commu-
nications, 3, 1237.
-
-
ferring Mutations in Plasmodium falciparum
57:9, 4595-4598.
-
lock, M., Sangusangu, R., Ligamba, G.,
Russell, T. & Moore, S. -
responses of disease-transmitting mos-
quitoes to indoor interventions: the Ifakara
-
noglobulin-like receptors and falciparum
malaria in southwest Nigeria. Human Im-
-
ventive treatment for malaria in pregnancy
Journal, 11, 82.
delivery of intermittent preventive treatment
-
ence of provider factors. Malaria Journal,
11, 317.
A., Edwards, T., Fegan, G., Molyneux, S.
& Goodman, C.
of patient charges at primary care facilities
in Kenya: implications of low adherence
to user fee policy for users and facility
revenue. Health Policy and Planning: doi:
10.1093/heapol/czu026.
-
Malaria Cases with or without Laboratory
Diagnosis: The Experience in a District
doi:10.1371/journal.pone.0058107.
I. & Slotman, M. -
Bioko Island, Equatorial Guinea. Parasites
and Vectors, 5, 253.
Feston, E., Matowo, J., Mosha, F. & Row-
land, M.
-
plication of micro-encapsulated pirimiphos-
13, 37.
Fragile Gains: The Need to Maintain Cover-
age with Long-Lasting Insecticidal Nets for
Malaria Control and Likely Implications of
-
Chavasse, D. -
vate sector antimalarial distribution chains:
a cross-sectional mixed methods study in
9, e93763.
Pates, H., Curtis, C. & Takken, W.
Hybridization studies to modify the host
and Veterinary Entomology, 28, 68-74.
-
Comparative analysis of two methods for
measuring sales volumes during malaria
medicine outlet surveys. Malaria Journal,
12, 311.
F., Alonso, P., Tanner, M., Mshinda, H.,
Roper, C. & Schellenberg, D.
community-randomised evaluation of the
effect of IPTi on anti-malarial drug resis-
tance in southern Tanzania. The Journal of
Infectious Diseases, 207, 848-59.
-
L.
of malaria in children: a qualitative study of
community perceptions and recommenda-
7, e32900.
E., Armstrong, M., Gray, C., Perkins, M.,
Y., Mori, Y., Chiodini, P. & Sutherland,
C.
Imported Malaria. The Journal of Infectious
Diseases, 208, 637-44.
Prentice, A. & Cox, S.
malaria interactions: research needs from
Prentice, A., Verhoef, H. & Cerami, C.
Preston, M., Campino, S., Assefa, S.,
Ngwa, A., Stewart, L., Conway, D.,
-
ley, C., Fairhurst, R., Sutherland, C.,
Roper, C. & Clark, T.
organellar genome polymorphisms identi-
falciparum strains. Nature Communica-
tions, 5, 4052.
Egwang, T., Corran, P., Ronca, R., Arcà,
a cohort exposed to intense malaria trans-
mission in northern Uganda. Parasite Im-
Protopopoff, N., Matowo, J., Malima, R.,
F. & Rowland, M.
-
biae to pyrethroid insecticides and reduced
susceptibility to bendiocarb in north-west-
ern Tanzania. Malaria Journal, 12, 149.
Pullan, R., Gitonga, C., Mwandawiro, C.,
-
ing the relative contribution of parasitic
infections and nutrition for anaemia among
school-aged children in Kenya: a subna-
tional geostatistical analysis. British Medi-
Rao, V., Schellenberg, D. & Ghani, A.
-
ers to successful malaria treatment. Trends
in Parasitology, 29, 164-180.
-
schmidt, I., Ridl, F., Powell, J., Caccone,
A. & Slotman, M. -
-
ventions in Continental Equatorial Guinea.
Rehman, A., Mann, A., Schwabe, C.,
Reddy, M., Roncon Gomes, I., Slotman,
M., Yellott, L., Matias, A., Caccone, A.,
continental region, Equatorial Guinea. Ma-
laria Journal, 12, 154.
Reynolds, J., Mangesho, P., Lemnge, M.,
Vestergaard, L. & Chandler, C.
in the project they really care for us’: Mean-
ing and experiences of participating in a
-
laria and HIV in Tanzanian adults. Global
Reynolds, J., Wood, M., Mikhail, A.,
Chandler, C. & Leslie, T.
Qualitative Health Research, 23, 579-91.
Riley, E. & Grencis, R.
Immunology embraces 21st century pub-
lishing: moving to online-only publication.
Parasite Immunology, 36, 1-2.
-
Aide, P., Lanaspa, M., Aponte, J., Mache-
Macete, E., Alonso, P., Abdulla, S., Salim,
A., Mtoro, A., Hamad, A., Mutani, P., Tan-
ner, M., Tinto, H., D’alessandro, U., Sorg-
-
-
E., Chandramohan, D., Greenwood,
E., Malle, L., Lemnge, M., Theander, T.,
Drakeley, C., Ansong, D., Agbenyega, T.,
J., Sylverken, J., Sambian, D., Sarfo, A.,
Agyekum, A., Martinson, F., Hoffman,
-
J., Guerra, Y., Jongert, E., Lapierre, D.,
D., Sillman, M. & Vansadia, P.
-
Journal of Medicine, 367, 2284-95.
Saeed, S., Carter, V., Tremp, A. & Des-
sens, J.
controls temporal expression of the Plas-
modium berghei LCCL protein complex.
Molecular and Biochemical Parasitology,
189, 38-42.
Sawa, P., Shekalaghe, S., Drakeley, C.,
L., Schallig, H., Sauerwein, R., Hallett,
-
Randomized Trial. The Journal of Infectious
Diseases, 207, 1637-1645.
-
keeto, S., Sserwanga, A., Staedke, S.,
-
mya, M. & Dorsey, G.
prescription practices among outpatients
setting of a health facility-based sentinel
site surveillance system in Uganda. Malaria
Journal, 12.
Sepúlveda, N., Campino, S., Assefa,
S., Sutherland, C., Pain5, A. & Clark, T.
approach to detecting copy number varia-
tion in sequence coverage data. BMC Ge-
nomics, 14, 128.

Publications 2012-14 127
Malaria Centre Report 2012-14
126 Publications 2012-14
London School of Hygiene & Tropical Medicine
-
draogo, A., Ghani, A. & Drakeley, C.
of submicroscopic malaria infections and
their relevance for control. Nature Commu-
nications, 3, 1237.
-
-
ferring Mutations in Plasmodium falciparum
57:9, 4595-4598.
-
lock, M., Sangusangu, R., Ligamba, G.,
Russell, T. & Moore, S. -
responses of disease-transmitting mos-
quitoes to indoor interventions: the Ifakara
-
noglobulin-like receptors and falciparum
malaria in southwest Nigeria. Human Im-
-
ventive treatment for malaria in pregnancy
Journal, 11, 82.
delivery of intermittent preventive treatment
-
ence of provider factors. Malaria Journal,
11, 317.
A., Edwards, T., Fegan, G., Molyneux, S.
& Goodman, C.
of patient charges at primary care facilities
in Kenya: implications of low adherence
to user fee policy for users and facility
revenue. Health Policy and Planning: doi:
10.1093/heapol/czu026.
-
Malaria Cases with or without Laboratory
Diagnosis: The Experience in a District
doi:10.1371/journal.pone.0058107.
I. & Slotman, M. -
Bioko Island, Equatorial Guinea. Parasites
and Vectors, 5, 253.
Feston, E., Matowo, J., Mosha, F. & Row-
land, M.
-
plication of micro-encapsulated pirimiphos-
13, 37.
Fragile Gains: The Need to Maintain Cover-
age with Long-Lasting Insecticidal Nets for
Malaria Control and Likely Implications of
-
Chavasse, D. -
vate sector antimalarial distribution chains:
a cross-sectional mixed methods study in
9, e93763.
Pates, H., Curtis, C. & Takken, W.
Hybridization studies to modify the host
and Veterinary Entomology, 28, 68-74.
-
Comparative analysis of two methods for
measuring sales volumes during malaria
medicine outlet surveys. Malaria Journal,
12, 311.
F., Alonso, P., Tanner, M., Mshinda, H.,
Roper, C. & Schellenberg, D.
community-randomised evaluation of the
effect of IPTi on anti-malarial drug resis-
tance in southern Tanzania. The Journal of
Infectious Diseases, 207, 848-59.
-
L.
of malaria in children: a qualitative study of
community perceptions and recommenda-
7, e32900.
E., Armstrong, M., Gray, C., Perkins, M.,
Y., Mori, Y., Chiodini, P. & Sutherland,
C.
Imported Malaria. The Journal of Infectious
Diseases, 208, 637-44.
Prentice, A. & Cox, S.
malaria interactions: research needs from
Prentice, A., Verhoef, H. & Cerami, C.
Preston, M., Campino, S., Assefa, S.,
Ngwa, A., Stewart, L., Conway, D.,
-
ley, C., Fairhurst, R., Sutherland, C.,
Roper, C. & Clark, T.
organellar genome polymorphisms identi-
falciparum strains. Nature Communica-
tions, 5, 4052.
Egwang, T., Corran, P., Ronca, R., Arcà,
a cohort exposed to intense malaria trans-
mission in northern Uganda. Parasite Im-
Protopopoff, N., Matowo, J., Malima, R.,
F. & Rowland, M.
-
biae to pyrethroid insecticides and reduced
susceptibility to bendiocarb in north-west-
ern Tanzania. Malaria Journal, 12, 149.
Pullan, R., Gitonga, C., Mwandawiro, C.,
-
ing the relative contribution of parasitic
infections and nutrition for anaemia among
school-aged children in Kenya: a subna-
tional geostatistical analysis. British Medi-
Rao, V., Schellenberg, D. & Ghani, A.
-
ers to successful malaria treatment. Trends
in Parasitology, 29, 164-180.
-
schmidt, I., Ridl, F., Powell, J., Caccone,
A. & Slotman, M. -
-
ventions in Continental Equatorial Guinea.
Rehman, A., Mann, A., Schwabe, C.,
Reddy, M., Roncon Gomes, I., Slotman,
M., Yellott, L., Matias, A., Caccone, A.,
continental region, Equatorial Guinea. Ma-
laria Journal, 12, 154.
Reynolds, J., Mangesho, P., Lemnge, M.,
Vestergaard, L. & Chandler, C.
in the project they really care for us’: Mean-
ing and experiences of participating in a
-
laria and HIV in Tanzanian adults. Global
Reynolds, J., Wood, M., Mikhail, A.,
Chandler, C. & Leslie, T.
Qualitative Health Research, 23, 579-91.
Riley, E. & Grencis, R.
Immunology embraces 21st century pub-
lishing: moving to online-only publication.
Parasite Immunology, 36, 1-2.
-
Aide, P., Lanaspa, M., Aponte, J., Mache-
Macete, E., Alonso, P., Abdulla, S., Salim,
A., Mtoro, A., Hamad, A., Mutani, P., Tan-
ner, M., Tinto, H., D’alessandro, U., Sorg-
-
-
E., Chandramohan, D., Greenwood,
E., Malle, L., Lemnge, M., Theander, T.,
Drakeley, C., Ansong, D., Agbenyega, T.,
J., Sylverken, J., Sambian, D., Sarfo, A.,
Agyekum, A., Martinson, F., Hoffman,
-
J., Guerra, Y., Jongert, E., Lapierre, D.,
D., Sillman, M. & Vansadia, P.
-
Journal of Medicine, 367, 2284-95.
Saeed, S., Carter, V., Tremp, A. & Des-
sens, J.
controls temporal expression of the Plas-
modium berghei LCCL protein complex.
Molecular and Biochemical Parasitology,
189, 38-42.
Sawa, P., Shekalaghe, S., Drakeley, C.,
L., Schallig, H., Sauerwein, R., Hallett,
-
Randomized Trial. The Journal of Infectious
Diseases, 207, 1637-1645.
-
keeto, S., Sserwanga, A., Staedke, S.,
-
mya, M. & Dorsey, G.
prescription practices among outpatients
setting of a health facility-based sentinel
site surveillance system in Uganda. Malaria
Journal, 12.
Sepúlveda, N., Campino, S., Assefa,
S., Sutherland, C., Pain5, A. & Clark, T.
approach to detecting copy number varia-
tion in sequence coverage data. BMC Ge-
nomics, 14, 128.

Publications 2012-14 129
Malaria Centre Report 2012-14
128 Publications 2012-14
London School of Hygiene & Tropical Medicine
C. & Clark, T.
of Multiple Imputation Based on Chained
Equations in Tackling Missing Data of the
-
ics, 78, 277-89.
Fe
a complementary age grading and species
-
tors. Parasites and Vectors, 3:49.
Yadeta, D., Ruiz Carrascal, D. & Pascual,
M.
Incidence in Highlands of Ethiopia and
1154-1158.
L. & Ghani, A.
of adding Ivermectin to a mass treatment
intervention to reduce malaria transmission:
a modelling study. The Journal of Infectious
Diseases, pii: jiu351.
Smallegange, R., Van Gemert, G., Van De
Sauerwein, R. & Logan, J.
Infected Mosquitoes Express Enhanced
e63602.
Smith, D., Perkins, T., Tusting, L., Scott,
T. & Lindsay, S. -
tion regulation and larval source manage-
ment in heterogeneous environments. Plos
Smith Paintain, L., Awini, E., Addei, S.,
Manyei, A., Yayemain, D., Rusamira, E.,
Mangham-Jefferies, L.
of a universal long-lasting insecticidal net
effectiveness of distribution and hang-up
activities. Malaria Journal, 13, 71.
J., Schellenberg, D. & Ngongo, N.
Community Health Workers and Stand-
Staedke, S., Chandler, C., Diliberto, D.,
Maiteki-Sebuguzi, C., Nankya, F., Webb,
PRIME trial protocol: evaluating the impact
of an intervention implemented in public
health centres on management of malaria
and health outcomes of children using a
cluster-randomised design in Tororo, Ugan-
da. Implementation Science, 8, 114.
-
bach, R., Cox, J. & Drakeley, C.
Novel vectors of malaria parasites in the
Western highlands of kenya. Emerging
Infectious Diseases, 18, 1547-9.
Stevenson, J., Stresman, G., Gitonga, C.,
-
Cox, J.
in estimating geographic variation in ma-
laria transmission in the Western kenyan
Nets for Control of Pyrethroid-Resistant
-
sase, S., Hashim, R., Gosling, R., Car-
neiro, I., Chandramohan, D., Theander,
Drakeley, C.
Detect Variation in Exposure to Malaria
e40170.
Stone, W., Churcher, T., Graumans,
-
ment of Plasmodium falciparum transmis-
sion in the standard membrane feeding as-
say using transgenic parasites expressing
GFP-luciferase. The Journal of Infectious
Diseases, doi: 10.1093/infdis/jiu271.
Stone, W., Eldering, M., Van Gemert,
Graumans, W., Roeffen, W., Drakeley, C.,
relevance and applicability of oocyst preva-
lence as a read-out for mosquito feeding
Sturrock, H., Hsiang, M., Cohen, J.,
& Gosling, R. -
atic malaria infections: active surveillance
in control and elimination. PloS Medicine,
10, e1001467.
malarial serine protease SUB1 plays an es-
sential role in parasite liver stage develop-
ment. Plos Pathogens, 9, e1003811.
Takala-Harrison, S., Clark, T., Jacob,
A., Fukuda, M., Nosten, F., Noedl, H.,
Tyner, S., Saunders, D., Socheat, D., Ari-
ey, F., Phyo, A., Starzengruber, P., Fueh-
Flegg, J., Arze, C., Cerqueira, G., Silva,
J., Ricklefs, S., Porcella, S., Stephens,
Plowe, C.
with delayed clearance of Plasmodium
falciparum following artemisinin treatment
-
Takala-Harrison, S., Jacob, C., Arze, C.,
Cummings, M., Silva, J., Dondorp, A.,
Fukuda, M., Hien, T., Mayxay, M., No-
Tyner, S., Saunders, D., Ariey, F., Mer-
-
D., White, N., Ringwald, P. & Plowe, C.
-
modium falciparum artemisinin resistance
Infectious Diseases, pii: jiu491.
Takem, E., Affara, M., Amambua-Ngwa,
Clifford, C., Taal, M., Sowe, M., Suso,
P., Mendy, A., Mbaye, A., Drakeley, C. &
D’alessandro, U.
Malaria Transmission with School Surveys:
Takem EN, Affara M, Amambua-Ngwa
-
tecting Foci of Malaria Transmission with
-
journal.pone.0067108.
Juma, E., Logedi, J., Nyandigisi, A.,
Mulenga, M., Mbacham, W., Roper, C.,
Guerin, P., Dalessandro, U. & Snow., R.
-
for enhanced wide coverage malaria drug
resistance surveillance and response sys-
888–896.
Tanomsing, N., Imwong, M., Sutherland,
C., Dolecek, C., Hien, T., Nosten, F., Day,
N., White, N. & Snounou, G. -
genotyping of Plasmodium ovale curtisi
and Plasmodium ovale wallikeri. Journal of
Clinical Microbiology, 51, 4213-6.
-
committee. Malaria Journal, 12, 362.
-
Mathanga, D., Mårtensson, A., Ngasala,
A., Moormann, A., Vulule, J., Doumbo,
& Juliano, J.
Plasmodium falciparum artemisinin resis-
molecular epidemiologic study. The Journal
of Infectious Diseases: doi: 10.1093/infdis/
jiu467.
Temu, E., Coleman, M., Abilio, A. &
of Malaria in Zambezia, Mozambique: The
Protective Effect of IRS versus Increased
Risks Due to Pig-Keeping and House Con-
G., Drought, L., Failly, M., Martin, C.,
of antibodies to newly described Plasmodi-
um falciparum merozoite antigens supports
MSPDBL2 as a predicted target of naturally
acquired immunity. Infection and Immunity,
-
ment of a Transgenic Plasmodium berghei
cGMP-Dependent Protein Kinase, a Novel
e96923.
Theisen, M., Roeffen, W., Singh, S.,
Andersen, G., Amoah, L., Van De Vegte-
-
egiel, M., Christiansen, M. & Sauerwein,
R.
candidate targeting both transmission and
asexual parasite life-cycle stages. Vaccine,
-
maprasad, A., Nwakanma, D., Fischer,
Journal of Proteome Research, 12, 1211-
1222.
-
schmidt, I., Ye, Y., Mann, A., Ren, R., Wil-
& Goodman, C. -
-
let and Household Surveys before and after
South-west burkina faso: comparison of
active and passive case detection methods.
-
-
ogbeto, M. -
age and effective use rate of long-lasting
insecticidal nets after nation-wide scale up
of their distribution in Benin. Parasites and
Vectors. 2013; 6: 265.
Souza, J., Liu, F., Riley, E. & Rabinovich,
G.

Publications 2012-14 129
Malaria Centre Report 2012-14
128 Publications 2012-14
London School of Hygiene & Tropical Medicine
C. & Clark, T.
of Multiple Imputation Based on Chained
Equations in Tackling Missing Data of the
-
ics, 78, 277-89.
Fe
a complementary age grading and species
-
tors. Parasites and Vectors, 3:49.
Yadeta, D., Ruiz Carrascal, D. & Pascual,
M.
Incidence in Highlands of Ethiopia and
1154-1158.
L. & Ghani, A.
of adding Ivermectin to a mass treatment
intervention to reduce malaria transmission:
a modelling study. The Journal of Infectious
Diseases, pii: jiu351.
Smallegange, R., Van Gemert, G., Van De
Sauerwein, R. & Logan, J.
Infected Mosquitoes Express Enhanced
e63602.
Smith, D., Perkins, T., Tusting, L., Scott,
T. & Lindsay, S. -
tion regulation and larval source manage-
ment in heterogeneous environments. Plos
Smith Paintain, L., Awini, E., Addei, S.,
Manyei, A., Yayemain, D., Rusamira, E.,
Mangham-Jefferies, L.
of a universal long-lasting insecticidal net
effectiveness of distribution and hang-up
activities. Malaria Journal, 13, 71.
J., Schellenberg, D. & Ngongo, N.
Community Health Workers and Stand-
Staedke, S., Chandler, C., Diliberto, D.,
Maiteki-Sebuguzi, C., Nankya, F., Webb,
PRIME trial protocol: evaluating the impact
of an intervention implemented in public
health centres on management of malaria
and health outcomes of children using a
cluster-randomised design in Tororo, Ugan-
da. Implementation Science, 8, 114.
-
bach, R., Cox, J. & Drakeley, C.
Novel vectors of malaria parasites in the
Western highlands of kenya. Emerging
Infectious Diseases, 18, 1547-9.
Stevenson, J., Stresman, G., Gitonga, C.,
-
Cox, J.
in estimating geographic variation in ma-
laria transmission in the Western kenyan
Nets for Control of Pyrethroid-Resistant
-
sase, S., Hashim, R., Gosling, R., Car-
neiro, I., Chandramohan, D., Theander,
Drakeley, C.
Detect Variation in Exposure to Malaria
e40170.
Stone, W., Churcher, T., Graumans,
-
ment of Plasmodium falciparum transmis-
sion in the standard membrane feeding as-
say using transgenic parasites expressing
GFP-luciferase. The Journal of Infectious
Diseases, doi: 10.1093/infdis/jiu271.
Stone, W., Eldering, M., Van Gemert,
Graumans, W., Roeffen, W., Drakeley, C.,
relevance and applicability of oocyst preva-
lence as a read-out for mosquito feeding
Sturrock, H., Hsiang, M., Cohen, J.,
& Gosling, R. -
atic malaria infections: active surveillance
in control and elimination. PloS Medicine,
10, e1001467.
malarial serine protease SUB1 plays an es-
sential role in parasite liver stage develop-
ment. Plos Pathogens, 9, e1003811.
Takala-Harrison, S., Clark, T., Jacob,
A., Fukuda, M., Nosten, F., Noedl, H.,
Tyner, S., Saunders, D., Socheat, D., Ari-
ey, F., Phyo, A., Starzengruber, P., Fueh-
Flegg, J., Arze, C., Cerqueira, G., Silva,
J., Ricklefs, S., Porcella, S., Stephens,
Plowe, C.
with delayed clearance of Plasmodium
falciparum following artemisinin treatment
-
Takala-Harrison, S., Jacob, C., Arze, C.,
Cummings, M., Silva, J., Dondorp, A.,
Fukuda, M., Hien, T., Mayxay, M., No-
Tyner, S., Saunders, D., Ariey, F., Mer-
-
D., White, N., Ringwald, P. & Plowe, C.
-
modium falciparum artemisinin resistance
Infectious Diseases, pii: jiu491.
Takem, E., Affara, M., Amambua-Ngwa,
Clifford, C., Taal, M., Sowe, M., Suso,
P., Mendy, A., Mbaye, A., Drakeley, C. &
D’alessandro, U.
Malaria Transmission with School Surveys:
Takem EN, Affara M, Amambua-Ngwa
-
tecting Foci of Malaria Transmission with
-
journal.pone.0067108.
Juma, E., Logedi, J., Nyandigisi, A.,
Mulenga, M., Mbacham, W., Roper, C.,
Guerin, P., Dalessandro, U. & Snow., R.
-
for enhanced wide coverage malaria drug
resistance surveillance and response sys-
888–896.
Tanomsing, N., Imwong, M., Sutherland,
C., Dolecek, C., Hien, T., Nosten, F., Day,
N., White, N. & Snounou, G. -
genotyping of Plasmodium ovale curtisi
and Plasmodium ovale wallikeri. Journal of
Clinical Microbiology, 51, 4213-6.
-
committee. Malaria Journal, 12, 362.
-
Mathanga, D., Mårtensson, A., Ngasala,
A., Moormann, A., Vulule, J., Doumbo,
& Juliano, J.
Plasmodium falciparum artemisinin resis-
molecular epidemiologic study. The Journal
of Infectious Diseases: doi: 10.1093/infdis/
jiu467.
Temu, E., Coleman, M., Abilio, A. &
of Malaria in Zambezia, Mozambique: The
Protective Effect of IRS versus Increased
Risks Due to Pig-Keeping and House Con-
G., Drought, L., Failly, M., Martin, C.,
of antibodies to newly described Plasmodi-
um falciparum merozoite antigens supports
MSPDBL2 as a predicted target of naturally
acquired immunity. Infection and Immunity,
-
ment of a Transgenic Plasmodium berghei
cGMP-Dependent Protein Kinase, a Novel
e96923.
Theisen, M., Roeffen, W., Singh, S.,
Andersen, G., Amoah, L., Van De Vegte-
-
egiel, M., Christiansen, M. & Sauerwein,
R.
candidate targeting both transmission and
asexual parasite life-cycle stages. Vaccine,
-
maprasad, A., Nwakanma, D., Fischer,
Journal of Proteome Research, 12, 1211-
1222.
-
schmidt, I., Ye, Y., Mann, A., Ren, R., Wil-
& Goodman, C. -
-
let and Household Surveys before and after
South-west burkina faso: comparison of
active and passive case detection methods.
-
-
ogbeto, M. -
age and effective use rate of long-lasting
insecticidal nets after nation-wide scale up
of their distribution in Benin. Parasites and
Vectors. 2013; 6: 265.
Souza, J., Liu, F., Riley, E. & Rabinovich,
G.

Publications 2012-14 131
Malaria Centre Report 2012-14
130 Publications 2012-14
London School of Hygiene & Tropical Medicine
R., Goodman, C., Mann, A., Ren, R., Wil-
-
S., Nguah, S., Seydou, M., Taylor, M.,
Rueda, S., Wamukoya, M., Arnold, F. &
availability, price, and market share of qual-
ity-assured artemisinin-based combination
therapies in seven countries: a before-and-
after analysis of outlet survey data. Lancet,
380, 1916-26.
Tougher, S., Ye, Y., Goodman, C., Arnold,
-
thors’ reply. Lancet, 381, 1095-6.
-
-
severe malaria in a Malian population. Plos
-
& Molez, J.
Policies and Child Mortality in Senegal:
Reaching Millennium Development Goal 4.
The Journal of Infectious Diseases, 205,
672-679.
Tremp, A., Carter, V., Saeed, S. & Des-
sens, J. -
modium zoites is uncoupled from tensile
strength. Molecular Microbiology, 89, 552-
64.
population in KwaZulu-Natal negates the
need for policies to prevent malaria in preg-
103, 172-5.
Drakeley, C.
in Plasmodium falciparum Transmission:
Tusting, L., Thwing, J., Sinclair, D.,
-
tomley, C. & Lindsay, S.
larval source management for controlling
malaria. Cochrane Database Syst Rev, 8,
CD008923.
-
intervention against malaria: a systematic
review and meta-analysis. Lancet, 382,
963-72.
treatment and insecticide-treated nets for
the control of malaria during pregnancy in
analysis of national survey data, 2009-11.
The Lancet Infectious Diseases, 13, 1029-
42.
-
-
& Sutherland, C.
Plasmodium falciparum isolates from UK
travellers: in vitro drug sensitivity, clonality
and drug resistance markers. Malaria Jour-
nal, 12, 320.
Venkatesan, M., Gadalla, N., Stepniews-
Moriera, C., Price, R., Mårtensson, A.,
Rosenthal, P., Dorsey, G., Sutherland,
-
-
berg, G., Grivoyannis, A., Hamour, S.,
-
ras, P., Malmberg, M., Mwai, L., Ngasala,
Sibley, C. -
modium falciparum Chloroquine Resistance
Transporter and Multidrug Resistance 1
Journal of Tropical Medicine and Hygiene,
pii: 14-0031.
Villegas-Mendez, A., De Souza, J.,
Lavelle, S., Gwyer Findlay, E., Shaw, T.,
-
ceptor Signalling Restricts the Formation of
Pathogenic, Terminally Differentiated Th1
Cells during Malaria Infection by Repress-
ing IL-12 Dependent Signals. Plos Patho-
gens, 9, e1003293.
Villegas-Mendez, A., Greig, R., Shaw, T.,
De Souza, J., Gwyer Findlay, E., Stum-
?-Producing CD4+ T Cells Promote Ex-
perimental Cerebral Malaria by Modulating
Villegas-Mendez, A., Gwyer Findlay, E.,
De Souza, J., Grady, L., Saris, C., Lane,
to the Liver during Malaria Infection by
Repressing Chemokine-Independent Path-
Von Seidlein, L., Auburn, S., Espino,
A., Vestergaard, L., Green, J., Domingo,
G., Yeung, S. & Price, R.
of key knowledge gaps in glucose-6-phos-
with regard to the safe clinical deployment
of 8-aminoquinoline treatment regimens: a
workshop report. Malaria Journal, 12, 112.
Ranson, H., Lindsay, S., Lengeler, C.,
Hamon, N., Mclean, T. & Hemingway, J.
and adoption of new vector control tools.
-
Ghani, A. -
dent immunity to placental malaria. Nature
Communications, 4:1609.
-
dazzi, I., Cunnington, A., Deininger, S.,
Takem, E., Ebonyi, A., Weis, S., Walton,
R., Rowland-Jones, S., Sirugo, G., Wil-
liams, S. & Conway, D.
levels are associated with severe malaria
in Gambian children. Plos Pathogens, 8,
e1002579.
J., Tivura, M., Delmini, R., Amenga-
Agyei, S.
health centres of rural Ghana. Malaria Jour-
nal, 13, 261.
Diawara, S., Abathina, A., Haiballa, A.,
-
tion of malaria in pregnancy with intermit-
tent preventive treatment and insecticide
treated nets in mali: a quantitative health
8, e67520.
West, P., Protopopoff, N., Rowland, M.,
Cumming, E., Rand, A., Drakeley, C.,
Malaria risk factors in north west Tanzania:
the effect of spraying, nets and wealth. Plos
& Ghani, A. -
against Plasmodium falciparum Infection.
A. -
sponse to Plasmodium falciparum infection
White, M., Nielsen, C., Mcgregor, R.,
Riley, E. & Goodier, M.
subsets during recall responses to vaccine
antigens. Immunology, 142, 140-150.
Whitty, C., Chiodini, P. & Lalloo, D.
-
ported malaria in non-endemic countries.
British Medical Journal (Clinical research
Car, J. & Schellenberg, J. -
gies for delivering insecticide-treated nets
at scale for malaria control: a systematic
-
zation, 90, 672-684E.
-
-
gueni, I., Amuasi, J., Ren, R., Wamukoya,
M., Rueda, S., Taylor, M., Seydou, M.,
-
sage: exploring the effect of communication
and training interventions on private for-
related to a multi-country anti-malarial sub-
sidy intervention. Malaria Journal, 13, 46.
C. & Mbacham, W. -
tiveness analysis of provider interventions
to improve health worker practice in provid-
ing treatment for uncomplicated malaria in
Cameroon: a study protocol for a random-
ized controlled trial. Trials, 13, 4.
Withers-Martinez, C., Suarez, C., Fulle,
-
and function of a pan-malaria drug target.
International Journal for Parasitology, 42,
597-612.
I., Mzilahowa, T., Irving, H., Ndula, M.,
Hemingway, J. -
throid resistance on operational malaria
control in Malawi. Proceedings of the Na-
Yindom, L., Forbes, R., Aka, P., Janha,
& Walther, M. -
globulin-like receptors and malaria caused
by Plasmodium falciparum in The Gambia.
J., Malishee, A., Stevenson, J., Sulisty-
awati, Collins, F. & Madey, G.
Based Geo-Tagged Malaria-Related Survey
Azindow, I., Amenga-Etego, S., Tchum,
Agyei, S.
on malaria incidence in infants and young
children in Ghana: a randomized trial.

Publications 2012-14 131
Malaria Centre Report 2012-14
130 Publications 2012-14
London School of Hygiene & Tropical Medicine
R., Goodman, C., Mann, A., Ren, R., Wil-
-
S., Nguah, S., Seydou, M., Taylor, M.,
Rueda, S., Wamukoya, M., Arnold, F. &
availability, price, and market share of qual-
ity-assured artemisinin-based combination
therapies in seven countries: a before-and-
after analysis of outlet survey data. Lancet,
380, 1916-26.
Tougher, S., Ye, Y., Goodman, C., Arnold,
-
thors’ reply. Lancet, 381, 1095-6.
-
-
severe malaria in a Malian population. Plos
-
& Molez, J.
Policies and Child Mortality in Senegal:
Reaching Millennium Development Goal 4.
The Journal of Infectious Diseases, 205,
672-679.
Tremp, A., Carter, V., Saeed, S. & Des-
sens, J. -
modium zoites is uncoupled from tensile
strength. Molecular Microbiology, 89, 552-
64.
population in KwaZulu-Natal negates the
need for policies to prevent malaria in preg-
103, 172-5.
Drakeley, C.
in Plasmodium falciparum Transmission:
Tusting, L., Thwing, J., Sinclair, D.,
-
tomley, C. & Lindsay, S.
larval source management for controlling
malaria. Cochrane Database Syst Rev, 8,
CD008923.
-
intervention against malaria: a systematic
review and meta-analysis. Lancet, 382,
963-72.
treatment and insecticide-treated nets for
the control of malaria during pregnancy in
analysis of national survey data, 2009-11.
The Lancet Infectious Diseases, 13, 1029-
42.
-
-
& Sutherland, C.
Plasmodium falciparum isolates from UK
travellers: in vitro drug sensitivity, clonality
and drug resistance markers. Malaria Jour-
nal, 12, 320.
Venkatesan, M., Gadalla, N., Stepniews-
Moriera, C., Price, R., Mårtensson, A.,
Rosenthal, P., Dorsey, G., Sutherland,
-
-
berg, G., Grivoyannis, A., Hamour, S.,
-
ras, P., Malmberg, M., Mwai, L., Ngasala,
Sibley, C. -
modium falciparum Chloroquine Resistance
Transporter and Multidrug Resistance 1
Journal of Tropical Medicine and Hygiene,
pii: 14-0031.
Villegas-Mendez, A., De Souza, J.,
Lavelle, S., Gwyer Findlay, E., Shaw, T.,
-
ceptor Signalling Restricts the Formation of
Pathogenic, Terminally Differentiated Th1
Cells during Malaria Infection by Repress-
ing IL-12 Dependent Signals. Plos Patho-
gens, 9, e1003293.
Villegas-Mendez, A., Greig, R., Shaw, T.,
De Souza, J., Gwyer Findlay, E., Stum-
?-Producing CD4+ T Cells Promote Ex-
perimental Cerebral Malaria by Modulating
Villegas-Mendez, A., Gwyer Findlay, E.,
De Souza, J., Grady, L., Saris, C., Lane,
to the Liver during Malaria Infection by
Repressing Chemokine-Independent Path-
Von Seidlein, L., Auburn, S., Espino,
A., Vestergaard, L., Green, J., Domingo,
G., Yeung, S. & Price, R.
of key knowledge gaps in glucose-6-phos-
with regard to the safe clinical deployment
of 8-aminoquinoline treatment regimens: a
workshop report. Malaria Journal, 12, 112.
Ranson, H., Lindsay, S., Lengeler, C.,
Hamon, N., Mclean, T. & Hemingway, J.
and adoption of new vector control tools.
-
Ghani, A. -
dent immunity to placental malaria. Nature
Communications, 4:1609.
-
dazzi, I., Cunnington, A., Deininger, S.,
Takem, E., Ebonyi, A., Weis, S., Walton,
R., Rowland-Jones, S., Sirugo, G., Wil-
liams, S. & Conway, D.
levels are associated with severe malaria
in Gambian children. Plos Pathogens, 8,
e1002579.
J., Tivura, M., Delmini, R., Amenga-
Agyei, S.
health centres of rural Ghana. Malaria Jour-
nal, 13, 261.
Diawara, S., Abathina, A., Haiballa, A.,
-
tion of malaria in pregnancy with intermit-
tent preventive treatment and insecticide
treated nets in mali: a quantitative health
8, e67520.
West, P., Protopopoff, N., Rowland, M.,
Cumming, E., Rand, A., Drakeley, C.,
Malaria risk factors in north west Tanzania:
the effect of spraying, nets and wealth. Plos
& Ghani, A. -
against Plasmodium falciparum Infection.
A. -
sponse to Plasmodium falciparum infection
White, M., Nielsen, C., Mcgregor, R.,
Riley, E. & Goodier, M.
subsets during recall responses to vaccine
antigens. Immunology, 142, 140-150.
Whitty, C., Chiodini, P. & Lalloo, D.
-
ported malaria in non-endemic countries.
British Medical Journal (Clinical research
Car, J. & Schellenberg, J. -
gies for delivering insecticide-treated nets
at scale for malaria control: a systematic
-
zation, 90, 672-684E.
-
-
gueni, I., Amuasi, J., Ren, R., Wamukoya,
M., Rueda, S., Taylor, M., Seydou, M.,
-
sage: exploring the effect of communication
and training interventions on private for-
related to a multi-country anti-malarial sub-
sidy intervention. Malaria Journal, 13, 46.
C. & Mbacham, W. -
tiveness analysis of provider interventions
to improve health worker practice in provid-
ing treatment for uncomplicated malaria in
Cameroon: a study protocol for a random-
ized controlled trial. Trials, 13, 4.
Withers-Martinez, C., Suarez, C., Fulle,
-
and function of a pan-malaria drug target.
International Journal for Parasitology, 42,
597-612.
I., Mzilahowa, T., Irving, H., Ndula, M.,
Hemingway, J. -
throid resistance on operational malaria
control in Malawi. Proceedings of the Na-
Yindom, L., Forbes, R., Aka, P., Janha,
& Walther, M. -
globulin-like receptors and malaria caused
by Plasmodium falciparum in The Gambia.
J., Malishee, A., Stevenson, J., Sulisty-
awati, Collins, F. & Madey, G.
Based Geo-Tagged Malaria-Related Survey
Azindow, I., Amenga-Etego, S., Tchum,
Agyei, S.
on malaria incidence in infants and young
children in Ghana: a randomized trial.

Members 133
Malaria Centre Report 2012-14
132 Members
London School of Hygiene & Tropical Medicine
Members
Central Services
Anne Mills:
Health Economics and Policy
Diseases
Dawn Britten:
Paul Lansdell:
Sue Passarelli:
Ranjan Ramasamy: Distance Learning
Module Reviewer
Claire Rogers: Head of Teaching and
Julie Tucker:
Emma Victory:
Cheryl Whitehorn:
John Williams: Clinical Scientist
Department of Clinical Research
Robin Bailey: Professor of Tropical
Medicine, Professor Consultant Physician
in Infectious Diseases and Tropical
Medicine, Hospital for Tropical Diseases
Ron Behrens: Senior Lecturer & Research
Degree co-ordinator
Michael Brown: Senior lecturer in
infectious diseases and tropical medicine
Bianca DSouza: Manager, ACT
Consortium
Peter Chiodini: Honorary Professor
Alison Elliott: Professor of Tropical
Medicine
Chris Drakeley
Malaria Centre Director Professor of Infection and Immunity
Steering Committee
David Baker: Reader in Parasite Molecular
Biology
Amit Bhasin: Manager, Malaria Capacity
Development Consortium
Clare Chandler: Lecturer in Social Science
Daniel Chandramohan: Professor of
Public Health
Brian Greenwood: Professor of Clinical
Tropical Medicine
Immo Kleinschmidt: Reader in
Epidemiology
Paul Milligan: Reader in Epidemiology and
Medical Statistics
Eleanor Riley: Professor of Immunology
David Schellenberg: Professor of Malaria
& International Health, ACT Consortium
Director, MCDC Deputy Director
Mark Rowland: Professor of Medical
Entomology and Malaria Control
Colin Sutherland: Head of Department
of Immunology and Infection, Reader in
Parasitology
Peter Godfrey-Faussett: Professor of
International Health (Currently seconded to
UNAIDS)
Heidi Hopkins: Consultant SCALE
Coordinator, ACT Consortium
Benjamin Judkewitz: Sir Henry Wellcome
Postdoctoral Fellow
Harparkash Kaur: Lecturer of
Pharmacology
David Mabey: Professor of Communicable
Diseases
Naiela Malik:
Research and Control Technician
Alexandra Miller: Programme Manager
Behzad Nadjm: Lecturer
Paul Newton: Honorary Senior Lecturer
Seth Owusu-Agyei: Research Fellow
Sarah Staedke: Senior Lecturer
Rebecca Tremain: PA to ACT Consortium
Director
Catherine Goodman
Malaria Centre Deputy Director Senior Lecturer in Health Economics and Policy
Dalia Iskander
Malaria Centre Coordinator
Karen Williams
Malaria Centre Coordinator
Philippe Verstraete: Assistant Manager,
ACT Consortium
Christopher Whitty: Professor of public &
International Health
Department of Disease Control
Patricia Aiyenuro: Research Assistant
Helen Allwood: Assistant Manager,
Malaria Capacity Development Consortium
David Bradley: Professor
Simon Brooker: Professor of
Epidemiology
Jane Bruce: Lecturer
Mary Cameron: Senior Lecturer
Ilona Carneiro: Lecturer, Distance
Learning Tutor Public Health
Matthew Chico: Lecturer of Maternal,
Newborn and Child Health
Badara Cisse: Lecturer in Epidemiology
Manuela Claite: Overseas Project
Coordinator
Sian Clarke: Senior Lecturer in Malaria
Research and Control
Frank Cox:
Jonathan Cox: Senior Lecturer
Diadier Diallo: Lecturer
Caterina Fanello: Honorary Lecturer
Ulrike Fillinger: Research Fellow Medical
Entomology & Malaria Control
Caroline Jones: Senior Lecturer
Mojca Kristan: Research Fellow
Matt Kirby: Lecturer of Medical
Entomology
Sham Lal: Research Fellow
Toby Leslie: Lecturer, ACT Consortium
Steve Lindsay: Professor of Public Health
Entomology
Jo Lines: Reader in Malaria Control &
James Logan: Senior Lecturer in Medical
arctec
Lena Lorenz: Research Fellow in Medical
Entomology
Caroline Lynch: Lecturer Programme
Design and Evaluation
Tanya Marchant: Senior Lecturer
Debora Miranda: Technical
Hazel Mccullough: Professional
Development and Educational
Advisor,Malaria Capacity Development
Consortium
Sarah Moore: Lecturer in Medical
Entomology Corine Ngufor: Research
Assistant in Medical Entomology
Raphael N’Guessan: Research Fellow in
Medical Entomology
Terri O’Halloran: Overseas Project
Administrator
Richard Oxborough: Research Fellow
Lucy Paintain: Lecturer
Rachel Pullan: Lecturer
Hugh Reyburn: Senior Lecturer in Clinical
Epidemiology
Ailie Robinson: Research Assistant
Joanna Schellenberg: Head of
Deapartment of Department of Disease
Control; Reader in Epidemiology &
International Health
Wolf-Peter Schmidt: Lecturer in
Epidemiology
Karen Slater:
Nina Stanczyk: Research Fellow
Jennifer Stevenson: Research Fellow
Harry Tagbor: Clinical Lecturer, MiP Trial
Coordinator
Lien Tran: Project Administrator, Malaria
Capacity Development Consortium
Jayne Webster: Senior Lecturer
Khalid Beshir: Research Fellow
Teun Bousema: Senior Lecturer
Michael Bretscher:
Fellow
Hollie Burrell-Saward: Research Assistant
Rebekah Burrow:
Patrick Corran: Honorary Senior Lecturer
Simon Croft: Professor of Parasitology
Aubrey Cunnington:
Research Fellow
Rebecca Dabbs:
Brian deSouza: Honorary Senior Lecturer,
Module Organizer for Distance learning
Hazel Dockrell: Professor of Immunology
Elizabeth Downe: Project Administrator
Kimberley Fornace: Research Fellow
Matt Gibbins: Research Assistant
Bronner Goncalves: Research Fellow
Julius Hafalla: Senior Lecturer in
Immunology, Royal Society University
Research Fellow
Tom Hall: Research Assistant
Helena Helmby: Senior Lecturer
Lou Herman:
Mary Oguike: Research Fellow
Carolyn Stanley: Laboratory Manager
Geoff Targett: Emeritus Professor of
Immunology of Parasitic Diseases
Don Van Schalkwyk: Research Fellow
Department of Pathogen Molecular
Biology
Samuel Assefa: Research Fellow in
Mike Blackman: Professor
Paul Bowyer: Research Fellow
David Conway: Professor of Biology
Johannes Dessens: Senior Lecturer in
Parasite Cell Biology
Craig Duffy: Research Fellow
Christian Flueck: Research Fellow
John Kelly: Professor of Molecular
Biology, Head of Department of Pathogen
Molecular Biology
Michael Miles: Professor of Medical
Protozoology
Debbie Nolder:
in Molecular Diagnostics
Mark Preston: Research Fellow
Cally Roper: Senior Lecturer in Malaria
Lindsay Stewart: Laboratory Technician
Kevin Tetteh: Lecturer
Eloise Thompson:
Annie Tremp: Research Assistant
David Warhurst: Emeritus Professor of
Protozoan Chemotherapy

Members 133
Malaria Centre Report 2012-14
132 Members
London School of Hygiene & Tropical Medicine
Members
Central Services
Anne Mills:
Health Economics and Policy
Diseases
Dawn Britten:
Paul Lansdell:
Sue Passarelli:
Ranjan Ramasamy: Distance Learning
Module Reviewer
Claire Rogers: Head of Teaching and
Julie Tucker:
Emma Victory:
Cheryl Whitehorn:
John Williams: Clinical Scientist
Department of Clinical Research
Robin Bailey: Professor of Tropical
Medicine, Professor Consultant Physician
in Infectious Diseases and Tropical
Medicine, Hospital for Tropical Diseases
Ron Behrens: Senior Lecturer & Research
Degree co-ordinator
Michael Brown: Senior lecturer in
infectious diseases and tropical medicine
Bianca DSouza: Manager, ACT
Consortium
Peter Chiodini: Honorary Professor
Alison Elliott: Professor of Tropical
Medicine
Chris Drakeley
Malaria Centre Director Professor of Infection and Immunity
Steering Committee
David Baker: Reader in Parasite Molecular
Biology
Amit Bhasin: Manager, Malaria Capacity
Development Consortium
Clare Chandler: Lecturer in Social Science
Daniel Chandramohan: Professor of
Public Health
Brian Greenwood: Professor of Clinical
Tropical Medicine
Immo Kleinschmidt: Reader in
Epidemiology
Paul Milligan: Reader in Epidemiology and
Medical Statistics
Eleanor Riley: Professor of Immunology
David Schellenberg: Professor of Malaria
& International Health, ACT Consortium
Director, MCDC Deputy Director
Mark Rowland: Professor of Medical
Entomology and Malaria Control
Colin Sutherland: Head of Department
of Immunology and Infection, Reader in
Parasitology
Peter Godfrey-Faussett: Professor of
International Health (Currently seconded to
UNAIDS)
Heidi Hopkins: Consultant SCALE
Coordinator, ACT Consortium
Benjamin Judkewitz: Sir Henry Wellcome
Postdoctoral Fellow
Harparkash Kaur: Lecturer of
Pharmacology
David Mabey: Professor of Communicable
Diseases
Naiela Malik:
Research and Control Technician
Alexandra Miller: Programme Manager
Behzad Nadjm: Lecturer
Paul Newton: Honorary Senior Lecturer
Seth Owusu-Agyei: Research Fellow
Sarah Staedke: Senior Lecturer
Rebecca Tremain: PA to ACT Consortium
Director
Catherine Goodman
Malaria Centre Deputy Director Senior Lecturer in Health Economics and Policy
Dalia Iskander
Malaria Centre Coordinator
Karen Williams
Malaria Centre Coordinator
Philippe Verstraete: Assistant Manager,
ACT Consortium
Christopher Whitty: Professor of public &
International Health
Department of Disease Control
Patricia Aiyenuro: Research Assistant
Helen Allwood: Assistant Manager,
Malaria Capacity Development Consortium
David Bradley: Professor
Simon Brooker: Professor of
Epidemiology
Jane Bruce: Lecturer
Mary Cameron: Senior Lecturer
Ilona Carneiro: Lecturer, Distance
Learning Tutor Public Health
Matthew Chico: Lecturer of Maternal,
Newborn and Child Health
Badara Cisse: Lecturer in Epidemiology
Manuela Claite: Overseas Project
Coordinator
Sian Clarke: Senior Lecturer in Malaria
Research and Control
Frank Cox:
Jonathan Cox: Senior Lecturer
Diadier Diallo: Lecturer
Caterina Fanello: Honorary Lecturer
Ulrike Fillinger: Research Fellow Medical
Entomology & Malaria Control
Caroline Jones: Senior Lecturer
Mojca Kristan: Research Fellow
Matt Kirby: Lecturer of Medical
Entomology
Sham Lal: Research Fellow
Toby Leslie: Lecturer, ACT Consortium
Steve Lindsay: Professor of Public Health
Entomology
Jo Lines: Reader in Malaria Control &
James Logan: Senior Lecturer in Medical
arctec
Lena Lorenz: Research Fellow in Medical
Entomology
Caroline Lynch: Lecturer Programme
Design and Evaluation
Tanya Marchant: Senior Lecturer
Debora Miranda: Technical
Hazel Mccullough: Professional
Development and Educational
Advisor,Malaria Capacity Development
Consortium
Sarah Moore: Lecturer in Medical
Entomology Corine Ngufor: Research
Assistant in Medical Entomology
Raphael N’Guessan: Research Fellow in
Medical Entomology
Terri O’Halloran: Overseas Project
Administrator
Richard Oxborough: Research Fellow
Lucy Paintain: Lecturer
Rachel Pullan: Lecturer
Hugh Reyburn: Senior Lecturer in Clinical
Epidemiology
Ailie Robinson: Research Assistant
Joanna Schellenberg: Head of
Deapartment of Department of Disease
Control; Reader in Epidemiology &
International Health
Wolf-Peter Schmidt: Lecturer in
Epidemiology
Karen Slater:
Nina Stanczyk: Research Fellow
Jennifer Stevenson: Research Fellow
Harry Tagbor: Clinical Lecturer, MiP Trial
Coordinator
Lien Tran: Project Administrator, Malaria
Capacity Development Consortium
Jayne Webster: Senior Lecturer
Khalid Beshir: Research Fellow
Teun Bousema: Senior Lecturer
Michael Bretscher:
Fellow
Hollie Burrell-Saward: Research Assistant
Rebekah Burrow:
Patrick Corran: Honorary Senior Lecturer
Simon Croft: Professor of Parasitology
Aubrey Cunnington:
Research Fellow
Rebecca Dabbs:
Brian deSouza: Honorary Senior Lecturer,
Module Organizer for Distance learning
Hazel Dockrell: Professor of Immunology
Elizabeth Downe: Project Administrator
Kimberley Fornace: Research Fellow
Matt Gibbins: Research Assistant
Bronner Goncalves: Research Fellow
Julius Hafalla: Senior Lecturer in
Immunology, Royal Society University
Research Fellow
Tom Hall: Research Assistant
Helena Helmby: Senior Lecturer
Lou Herman:
Mary Oguike: Research Fellow
Carolyn Stanley: Laboratory Manager
Geoff Targett: Emeritus Professor of
Immunology of Parasitic Diseases
Don Van Schalkwyk: Research Fellow
Department of Pathogen Molecular
Biology
Samuel Assefa: Research Fellow in
Mike Blackman: Professor
Paul Bowyer: Research Fellow
David Conway: Professor of Biology
Johannes Dessens: Senior Lecturer in
Parasite Cell Biology
Craig Duffy: Research Fellow
Christian Flueck: Research Fellow
John Kelly: Professor of Molecular
Biology, Head of Department of Pathogen
Molecular Biology
Michael Miles: Professor of Medical
Protozoology
Debbie Nolder:
in Molecular Diagnostics
Mark Preston: Research Fellow
Cally Roper: Senior Lecturer in Malaria
Lindsay Stewart: Laboratory Technician
Kevin Tetteh: Lecturer
Eloise Thompson:
Annie Tremp: Research Assistant
David Warhurst: Emeritus Professor of
Protozoan Chemotherapy

Members 135
Malaria Centre Report 2012-14
134 Members
London School of Hygiene & Tropical Medicine
Health
Department of Infectious Disease
Epidemiology
Neal Alexander: Reader in Medical
Statistics and Epidemiology
John Bradley: Research Fellow
Matthew Cairns: Lecturer in Epidemiology
Taane Clark:
Epidemiology and Statistics
Simon Cousens: Professor of
Epidemiology and Medical Statistics
Bonnie Cundill: Lecturer in Medical
Statistics & Epidemiology
John Edmunds: Dean of Faculty;
Professor
Clare Flach: Research Fellow
Paul Fine: Professor of Communicable
Disease Epidemiology
Neil French: Reader in Infectious Disease
Epidemiology
David Heymann: Chair of the Health
Protection Agency
DiTanna GianLuca: Lecturer in Medical
Statistics & Epidemiology
Baptiste Leurent: Lecturer in Medical
Statistics and Epidemiology
Andrea Mann: Distance Learning Tutor,
MSc Epidemiology (Distance Learning)
Joshua Mendelsohn: Research Fellow
Maureen OLeary: Research Fellow
Nuno Sepulveda: Research Fellow in
Susana Scott : Lecturer
Peter Smith: Professor of Tropical
Epidemiology
Paul Snell: Data Manager, ACT
Consortium
Emily Webb: Senior Lecturer in
Epidemiology and Medical Statistics
Intervention Research
Paula Dominguez-Salas: Research Fellow
of Public Health Nutrition
Seyi Soremekun: Lecturer of
Epidemiology
Hans Verhoef: Senior Lecturer
Department of Population Health
Richard Mutemwa: Research Fellow
Jani Puradiredja: Research Fellow
Jim Todd: Reader Applied Biostatistics
Department of Medical Statistics
Diana Elbourne: Professor of Healthcare
Evaluation
Richard Smith: Dean of Faculty;
Professor of Health System Economics
Development
Uli Beisel: Postdoctoral Research Fellow
Richard Coker: Professor of Public Health
Eleanor Grieve: Research Fellow in Health
Economics
Senior Lecturer in Health
Economics
Philippe Guyant: Research Fellow Project
Manager
Kristian Hansen: Lecturer in Health
Economics
Kara Hanson: Reader in Health System
Economics
Natasha Howard:
Eleanor Hutchinson: Research Fellow
Frida Kasteng: Research Fellow in Health
Economics
Ann Kelly: Honorary Lecturer in
Anthropology
Marcus Keogh-Brown: Lecturer
Harriet Lawford: Research Fellow
Marco Liverani: Lecturer in Health Policy
Lindsay Mangham-Jefferies: Lecturer in
Health Economics
Benjamin Palafox: Research Fellow in
Pharmaceutical Policy & Economics
Edith Patouillard: Lecturer in Health
Economics and Systems Analysis
Catherine Pitt: Lecturer in Health
Economics
Andreia Santos: Lecturer
Annemarie terVeen: Distance Learning
Lecturer in Infectious & Tropical Diseases;
Sergio TorresRueda: Research Fellow
Sarah Tougher: Research Fellow in
Pharmaceutical Policy & Economics
Barbara Willey: Lecturer in Epidemiology
Shunmay Yeung: Senior Lecturer
Nayantara Wijayanandana: Research
Fellow Epidemiology
Department of Health Services Research
Andreia Santos: Lecturer in Health
Economics
Department of Non-communicable
Disease Epidemiology
Lorna Gibson: Lecturer
Dorothea Nitsch: Senior Lecturer (Clinical)
Research degree studentsI Ifeyinwa Aniebo
Harvey Aspeling-Jones
El Hadj Ba
Kristin Banek
Katia Bruxvoort
Vanessa Chen-Hussey
Ifeyinwa Chijioke-Nwauche
Bianca D’Souza
Mary Grace Dacuma
Deborah DiLiberto
Bismarck Dinko
Paul Divis
Laura Drought
Christina Due
Chi Eziefula
Kimberly Fornace
Matt Gibbins
Bronner Goncalves
Katherine Halliday
Luke Harman
Gisela Henriques
Lou Herman
Manuela Herrera-Varela
Lauren Hutchinson
Natasha Howard
Sophie Jones
Ronnie Kasirye
Sham Lal
Mirza Lalani
Marie Lamy
Inke Lubis
Jenny Luchavez
Zawadi Mageni
Oscar Mbare
Louisa Messenger
Lee Murray
Inbarani Naidoo
Corine Ngufor
Enesia Ngulube
Enesia Ngulube
Mike Okal
Richard Oxborough
Benjamin Palafox
Bhargavi Rao
Joanna Reynolds
Ailie Robinson
Maha Saeed
Gillian Stresman
Asia Sophia-Wolf
Ebako Takem
Katherine Theiss-Nyland
Eloise Thompson
Samuel Thorburn
Sarah Tougher
Patrick Tungu
Lucy Tusting
Philippa West
John Williams
Issaka Zongo
MCDC linked PhD stu-dents
Gifty Antwi
Jovin Kitau
Johnson Matowo
Jacklin Mosha
Joaniter Nankabirwa
Youssoupha Ndiaye
Juliet Ndibazza
Harold Ocholla
Joseph Osarfo
Alberta Amu Quartey
To mark the centenary of World War One, and inspired by LSHTM’s summer exhibition Improving Health in War Time, this year’s World Mosquito Day celebrations focused on Sir Ronald Ross’s contribution to the War Effort in his role as Consulting Physician in tropical diseases.

Members 135
Malaria Centre Report 2012-14
134 Members
London School of Hygiene & Tropical Medicine
Health
Department of Infectious Disease
Epidemiology
Neal Alexander: Reader in Medical
Statistics and Epidemiology
John Bradley: Research Fellow
Matthew Cairns: Lecturer in Epidemiology
Taane Clark:
Epidemiology and Statistics
Simon Cousens: Professor of
Epidemiology and Medical Statistics
Bonnie Cundill: Lecturer in Medical
Statistics & Epidemiology
John Edmunds: Dean of Faculty;
Professor
Clare Flach: Research Fellow
Paul Fine: Professor of Communicable
Disease Epidemiology
Neil French: Reader in Infectious Disease
Epidemiology
David Heymann: Chair of the Health
Protection Agency
DiTanna GianLuca: Lecturer in Medical
Statistics & Epidemiology
Baptiste Leurent: Lecturer in Medical
Statistics and Epidemiology
Andrea Mann: Distance Learning Tutor,
MSc Epidemiology (Distance Learning)
Joshua Mendelsohn: Research Fellow
Maureen OLeary: Research Fellow
Nuno Sepulveda: Research Fellow in
Susana Scott : Lecturer
Peter Smith: Professor of Tropical
Epidemiology
Paul Snell: Data Manager, ACT
Consortium
Emily Webb: Senior Lecturer in
Epidemiology and Medical Statistics
Intervention Research
Paula Dominguez-Salas: Research Fellow
of Public Health Nutrition
Seyi Soremekun: Lecturer of
Epidemiology
Hans Verhoef: Senior Lecturer
Department of Population Health
Richard Mutemwa: Research Fellow
Jani Puradiredja: Research Fellow
Jim Todd: Reader Applied Biostatistics
Department of Medical Statistics
Diana Elbourne: Professor of Healthcare
Evaluation
Richard Smith: Dean of Faculty;
Professor of Health System Economics
Development
Uli Beisel: Postdoctoral Research Fellow
Richard Coker: Professor of Public Health
Eleanor Grieve: Research Fellow in Health
Economics
Senior Lecturer in Health
Economics
Philippe Guyant: Research Fellow Project
Manager
Kristian Hansen: Lecturer in Health
Economics
Kara Hanson: Reader in Health System
Economics
Natasha Howard:
Eleanor Hutchinson: Research Fellow
Frida Kasteng: Research Fellow in Health
Economics
Ann Kelly: Honorary Lecturer in
Anthropology
Marcus Keogh-Brown: Lecturer
Harriet Lawford: Research Fellow
Marco Liverani: Lecturer in Health Policy
Lindsay Mangham-Jefferies: Lecturer in
Health Economics
Benjamin Palafox: Research Fellow in
Pharmaceutical Policy & Economics
Edith Patouillard: Lecturer in Health
Economics and Systems Analysis
Catherine Pitt: Lecturer in Health
Economics
Andreia Santos: Lecturer
Annemarie terVeen: Distance Learning
Lecturer in Infectious & Tropical Diseases;
Sergio TorresRueda: Research Fellow
Sarah Tougher: Research Fellow in
Pharmaceutical Policy & Economics
Barbara Willey: Lecturer in Epidemiology
Shunmay Yeung: Senior Lecturer
Nayantara Wijayanandana: Research
Fellow Epidemiology
Department of Health Services Research
Andreia Santos: Lecturer in Health
Economics
Department of Non-communicable
Disease Epidemiology
Lorna Gibson: Lecturer
Dorothea Nitsch: Senior Lecturer (Clinical)
Research degree studentsI Ifeyinwa Aniebo
Harvey Aspeling-Jones
El Hadj Ba
Kristin Banek
Katia Bruxvoort
Vanessa Chen-Hussey
Ifeyinwa Chijioke-Nwauche
Bianca D’Souza
Mary Grace Dacuma
Deborah DiLiberto
Bismarck Dinko
Paul Divis
Laura Drought
Christina Due
Chi Eziefula
Kimberly Fornace
Matt Gibbins
Bronner Goncalves
Katherine Halliday
Luke Harman
Gisela Henriques
Lou Herman
Manuela Herrera-Varela
Lauren Hutchinson
Natasha Howard
Sophie Jones
Ronnie Kasirye
Sham Lal
Mirza Lalani
Marie Lamy
Inke Lubis
Jenny Luchavez
Zawadi Mageni
Oscar Mbare
Louisa Messenger
Lee Murray
Inbarani Naidoo
Corine Ngufor
Enesia Ngulube
Enesia Ngulube
Mike Okal
Richard Oxborough
Benjamin Palafox
Bhargavi Rao
Joanna Reynolds
Ailie Robinson
Maha Saeed
Gillian Stresman
Asia Sophia-Wolf
Ebako Takem
Katherine Theiss-Nyland
Eloise Thompson
Samuel Thorburn
Sarah Tougher
Patrick Tungu
Lucy Tusting
Philippa West
John Williams
Issaka Zongo
MCDC linked PhD stu-dents
Gifty Antwi
Jovin Kitau
Johnson Matowo
Jacklin Mosha
Joaniter Nankabirwa
Youssoupha Ndiaye
Juliet Ndibazza
Harold Ocholla
Joseph Osarfo
Alberta Amu Quartey
To mark the centenary of World War One, and inspired by LSHTM’s summer exhibition Improving Health in War Time, this year’s World Mosquito Day celebrations focused on Sir Ronald Ross’s contribution to the War Effort in his role as Consulting Physician in tropical diseases.