Mako Robotic-Arm Assisted System: A Clinical and Economic ... · The Mako Robotic-Arm Assisted...
20
Mako Robotic-Arm Assisted System: A Clinical and Economic Analysis for Health Plans and Providers.
Transcript of Mako Robotic-Arm Assisted System: A Clinical and Economic ... · The Mako Robotic-Arm Assisted...
DRAFT INTERNAL PURPOSES ONLY
Mako Robotic-Arm Assisted System: A Clinical and Economic Analysis for Health Plans and Providers.
DRAFT INTERNAL PURPOSES ONLY
1
About this document
This document, prepared by Baker Tilly, LLP at the request of Stryker, presents health plans and
providers with clinical and economic information supporting the Mako Robotic-Arm Assisted System
(‘Mako’) as a safe and effective surgical tool that surgeons can use to help achieve greater accuracy
of component placement and enhance patient satisfaction during hip and knee arthroplasty
procedures. Moreover, this document supports Mako’s use within current standard-of-care
treatment protocols and reimbursement parameters.
The studies relied on in this document are of varying design, ranging from large randomized
controlled trials (RCTs) to single-surgeon studies and cadaver studies. As a result of variations in
study design, the robustness of the data arising from different studies may vary. The document
includes descriptions of studies relied upon and published sources are cited throughout. We
encourage you to consult the cited publications.
Executive reimbursement statement:
Many payers consider the robotic surgical system a tool or technique that is “integral to the primary
procedure.” This policy is employed by payers in the U.S. such as UnitedHealthcare and Humana.a
Moreover, some payers state that “[s]uch matters are left to the discretion of the surgeon.”a
Recommended approach, or reimbursement statement, if necessary:
“Robotic-Arm Assisted Systems are integral to the primary surgical procedures (e.g., hip and knee
arthroplasties), and as such, these systems are available for surgeons to use at their discretion
within existing reimbursement parameters.”
a Policies in place as of April 18, 2016.
2
Purpose:
The purpose of this report is to provide clinical and economic evidence of the Mako Robotic-Arm
Assisted System (‘Mako’) to support coverage and adoption of this technology. Mako is an assistive
tool that is ancillary to the primary procedure and is designed to enhance the surgical outcome.
Mako has demonstrated value to surgeons, patients, hospitals, and payers through clinical and
operational benefits. For example, studies have shown surgeons using Mako for assistance in
unicompartmental knee arthroplasty (UKA) have demonstrated the following value when compared
to non-robotic UKA and/or total knee arthroplasty (TKA) that do not include the Mako Robotic-Arm
Assisted System:
More accurate implant placement1-3
Lower early post-operative pain4
Reduced average length of stay for the index procedure5
Reduced revision rates at 24 months6-8
Legend:
ALOS: Average Length of Stay
PMPM: Per Member Per Month
TKA: Total Knee Arthroplasty
THA: Total Hip Arthroplasty
UKA: Unicompartmental Knee Arthroplasty
CJR: Comprehensive Care for Joint Replacement
IPSAF: Inpatient Standard Analytical File
OPSAF: CMS Medicare Outpatient Standard Analytical File
3
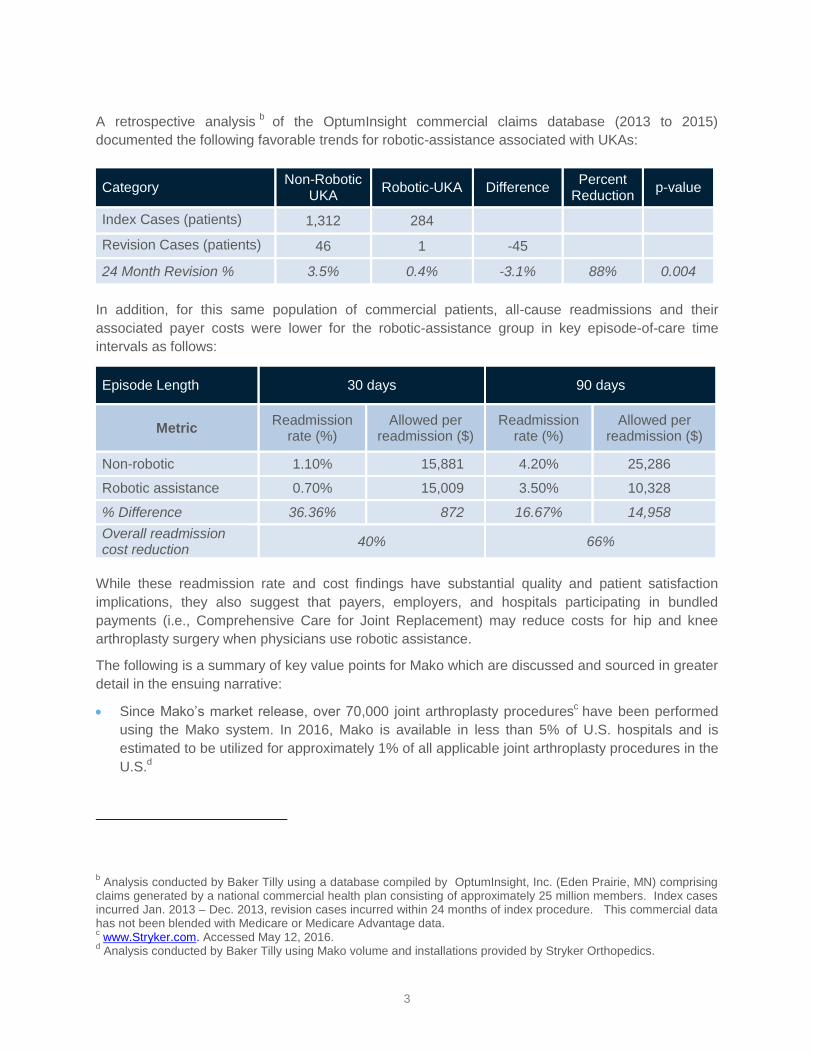
A retrospective analysisb of the OptumInsight commercial claims database (2013 to 2015)
documented the following favorable trends for robotic-assistance associated with UKAs:
Category Non-Robotic
UKA Robotic-UKA Difference
Percent Reduction
p-value
Index Cases (patients) 1,312 284
Revision Cases (patients) 46 1 -45
24 Month Revision % 3.5% 0.4% -3.1% 88% 0.004
In addition, for this same population of commercial patients, all-cause readmissions and their
associated payer costs were lower for the robotic-assistance group in key episode-of-care time
intervals as follows:
Episode Length 30 days 90 days
Metric Readmission
rate (%) Allowed per
readmission ($) Readmission
rate (%) Allowed per
readmission ($)
Non-robotic 1.10% 15,881 4.20% 25,286
Robotic assistance 0.70% 15,009 3.50% 10,328
% Difference 36.36% 872 16.67% 14,958
Overall readmission cost reduction
40% 66%
While these readmission rate and cost findings have substantial quality and patient satisfaction
implications, they also suggest that payers, employers, and hospitals participating in bundled
payments (i.e., Comprehensive Care for Joint Replacement) may reduce costs for hip and knee
arthroplasty surgery when physicians use robotic assistance.
The following is a summary of key value points for Mako which are discussed and sourced in greater
detail in the ensuing narrative:
Since Mako’s market release, over 70,000 joint arthroplasty proceduresc have been performed
using the Mako system. In 2016, Mako is available in less than 5% of U.S. hospitals and is
estimated to be utilized for approximately 1% of all applicable joint arthroplasty procedures in the
U.S.d
b Analysis conducted by Baker Tilly using a database compiled by OptumInsight, Inc. (Eden Prairie, MN) comprising
claims generated by a national commercial health plan consisting of approximately 25 million members. Index cases incurred Jan. 2013 – Dec. 2013, revision cases incurred within 24 months of index procedure. This commercial data has not been blended with Medicare or Medicare Advantage data. c www.Stryker.com. Accessed May 12, 2016.
d Analysis conducted by Baker Tilly using Mako volume and installations provided by Stryker Orthopedics.
4
Over 30 published peer-reviewed studies have reported favorable outcomes with the use of
robotic-arm assistance.
A Level 1 randomized controlled trial has demonstrated UKAs with robotic-arm assistance had
more accurate implant placement 4,9
and less early post-operative pain than non-robotic UKAs.4,9
For total hip arthroplasty (THA), the use of the Mako Total Hip application has demonstrated
more accurate component positioning,10-12
which may lead to greater range-of-motion, reduced
soft-tissue damage, decreased bone-to-bone impingement, and enhanced stability.11
Mako can be used in all surgical facility types including ambulatory surgical centers, community
hospitals, and large academic centers. This means that payers can potentially benefit from
patients seeking care at lower cost, but high quality, ambulatory surgical centers and community
hospitals.
Mako facilitates enhanced precision4,9
and enables surgeons to perform technically challenging
UKA procedures. Several studies have shown that meaningful subsets of patients treated with
TKA may have been candidates for UKAs.13-15
Moreover, a 2011 study that reviewed surgeries
performed by seven (7) clinicians at the same tertiary site found 21% of cases treated with a
TKA could have been treated with a UKA.13
Note: UKA with robotic-arm assistance has shown a significantly lower adverse event rate
(less than 1%) than that of non-robotic UKAs (3.5%) in a retrospective analysis of
commercial claims (OptumInsight commercial claims database 2013 to 2015). UKA with
robotic-arm assistance also drives lower index and revision procedure costs when
compared to non-robotic UKAs and/or TKAs (OptumInsight commercial claims database
2013 to 2015).
To the extent UKA candidates are currently undergoing TKAs,13 -15
and the use of robotic-arm
assistance can allow surgeons to perform UKAs when appropriate in a lower cost outpatient
setting, the use of Mako may lead to savings for payers. In an analysis of the OptumInsight
commercial claim database (2013 to 2015) with the following conservative assumptions, Mako
has the potential to deliver a potential savings of $0.02 to $0.05 Per Member Per Month
(PMPM).
o Five to twelve percent (5-12%) of procedures are switched from TKA ($30,982) to
robotic-arm assisted UKA ($30,398),
o Ten percent (10%) migration from an inpatient setting to hospital outpatient,
o Reduced readmissions per the study described herein,
o Industry-standard utilization and cost growth projection to 2020.
Note: If, as seen in the 2011 study referenced above,13
21% of UKA candidates were treated
with a UKA where robotic-arm assistance was used, the savings can increase to $0.09
PMPM. Furthermore, if a 20% migration from inpatient to hospital outpatient is realized, savings
can increase to $0.30 PMPM by 2020.
5
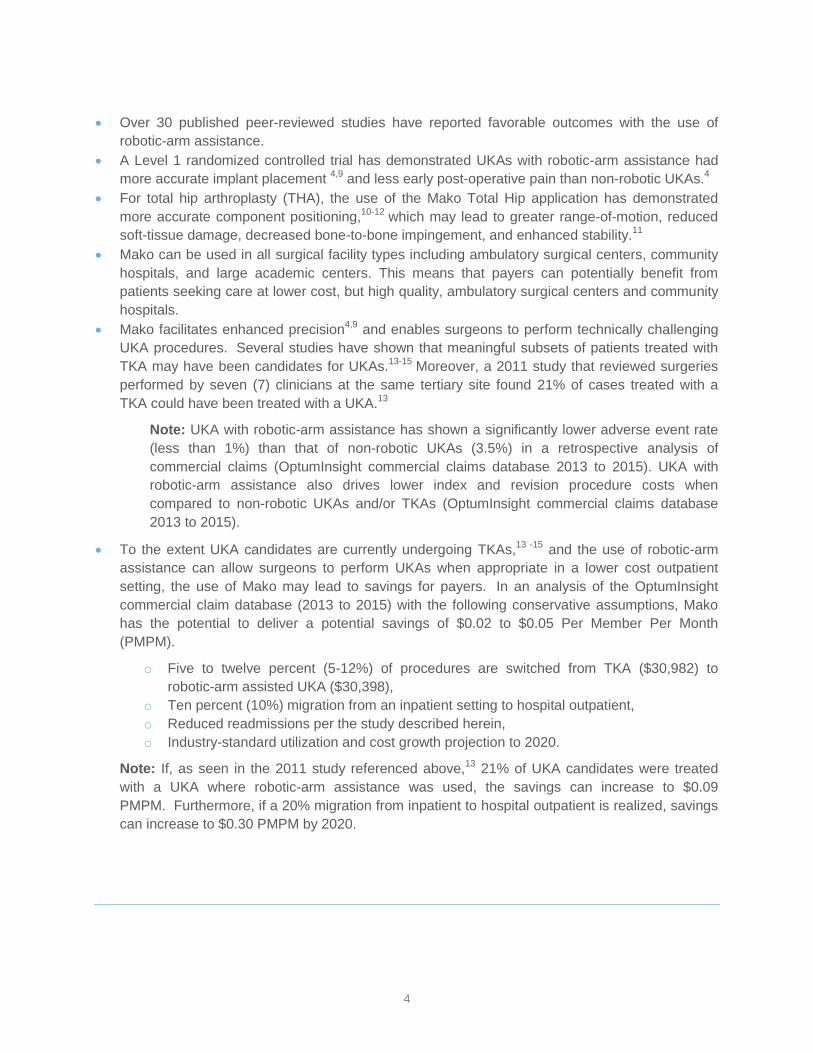
Introduction:
The Mako Robotic-Arm Assisted System
The Mako Robotic-Arm Assisted System allows surgeons to treat painful knee and hip conditions
with reproducible precision and more accurate implant alignment.2,3
It allows surgeons to optimize
current and proven standard surgical approaches for joint arthroplasty. The robotic technology
facilitates more accurate component placement1-3,16,19
and helps to eliminate unnecessary variation
in the surgical process across surgeons.4
The Mako System’s ability to enable surgical and implant
placement accuracy begins with patient-specific pre-operative planning. Pre-operative planning is an
Enhanced planning
Patient-specific pre-operative plan enables
accurate implant sizing and positioning.1-3,16,17
Functional positioning
Surgeon-controlled intra-operative adjustments can be made
to optimize implant placements.45
6
essential prerequisite for the success of many orthopedic procedures. Emerging evidence to date
suggests that pre-operative planning may be an effective means of favorably influencing the
outcomes of orthopedic procedures.20 Mako’s pre-operative, computer-assisted 3D planning allows
surgeons to evaluate the bone structure, alignment, and joint space as well as the surrounding
tissue, so that the surgeon can plan the patient-specific orientation for the implant, select the
appropriate size implant, balance the soft-tissue and ensure proper alignment.21
In the operating room, the robotic-arm system provides real-time data to the surgeon, allowing
continuous assessment of ligament tension and range-of-motion during implant placement and
articulation. Mako technology allows the surgeon to make intra-operative adjustments, as needed,
to optimize joint implant placement.21
In addition, the real-time data collected through Mako
technology enables the surgeon to avoid transection of vital structures, which has shown to reduce
blood loss. The decrease in blood loss associated with Mako may be attributed to a number of
factors including a smaller incision, decreased soft-tissue trauma, and conservative reaming for hip
arthroplasty.18
These benefits potentially eliminate the need for routine post-operative hemoglobin
monitoring and post-procedure blood transfusions, all factors which could lengthen the patient’s
hospitalization.22
Importantly, by using real-time data, surgeons are able to refine the surgical plan
intra-operatively to achieve soft-tissue balance, resulting in patients who are more likely to forget
their artificial joint in daily life.23
The Mako Robotic-Arm Assisted System was released in 2006 for use during partial knee
arthroplasty surgery and in 2010 for total hip arthroplasty surgery (Mako plans to have a market
release in 2017 for total knee arthroplasty). To date, approximately 70,000 patients or 1% of those
receiving a partial knee or hip arthroplasty procedure in the United States have received the benefit
of Mako robotic assistance. Over 30 studies summarizing the results of procedures performed with
the Mako System, including several randomized trials, have been published in peer-reviewed
journals. Results from many of these studies have reported that Mako is associated with enhanced
clinical outcomes.4,18
Key studies are highlighted in this document. A full bibliography is available
upon request.
Burden of Disease: The Cost of Osteoarthritis is Unsustainable without Treatment
Changes
Osteoarthritis, the most common form of arthritis, affects more people than any other joint disease
and is the most widespread cause of walking-related disability in people over the age of 65 years.24-
26 Osteoarthritis has been estimated to affect nearly 27 million adults in the United States.
27 Among
adults 60 years and older in the United States, an estimated 37.4% have osteoarthritis.28
Due to the
aging population and increasing trends in joint injury, the number of affected adults with
osteoarthritis is expected to increase by about 50% over the next 20 years (with the caveat that past
projections have underestimated future burden).29
The morbidity associated with osteoarthritis is considerable:
80% of individuals report limitations of movement,
25% of those have difficulty performing major activities of daily living.30
While osteoarthritis-related symptoms such as physical pain affect patients’ quality of life, the burden
of osteoarthritis extends far beyond that, to encompass the social and personal aspects of everyday
functionality.31

7
The economic burden of osteoarthritis in the United States is estimated to be more than $60 billion
per year, with job-related costs reaching as much as $13 billion per year.24
As the fourth-most
common cause for hospitalization, a diagnosis of osteoarthritis is attributed to approximately 12
million ambulatory care visits and 85,000 emergency room visits per year.32
Osteoarthritis is the leading indication for joint arthroplasty surgery, which is expected to grow
exponentially. By 2030, demand for knee arthroplasty is projected to grow by 673% or to 9.6
procedures per 1,000, while the demand for primary total hip arthroplasty is estimated to grow by
174% or to 1.6 procedures per 1,000. As the number of primary procedures increases, so will the
number of joint revision procedures.33
This trend demands that providers and payers collaborate to
manage this segment of the population.33
Joint Arthroplasty - Treatment Complications and Adverse Events
Joint replacement or arthroplasty is most often performed for painful arthritis that limits activities of
daily living and the pain is not relieved by medications or other conservative therapies. Joint
arthroplasty has been performed with favorable outcomes over the past several decades and is a
proven medical advancement in the field of orthopedic surgery.34
That said, a revision procedure
may be necessary due to an ineffective primary joint procedure.35
This can be due to infection
involving the joint, bone loss in the structures supporting the prosthesis, fracture, loosening of the
implant, among others.36
The risk of an ineffective primary procedure may also be affected by patient
factors such as age, weight, activity level, rehabilitation compliance, and the presence of co-
morbidities, as well as by the surgical technique. Complications associated with the surgical
procedure can include incorrect ligament balancing, poor cement technique, and malrotation of
implant parts. Major perioperative adverse events are reported in under 7.5% of patients and most
often become manifest within four days following the implant procedure.22,37
Clinical Studies
Partial Knee Arthroplasty (PKA) with Robotic-Arm Assistance
For patients who are appropriate candidates for a partial knee arthroplasty (PKA)/unicompartmental
knee arthroplasty (UKA), Mako technology can help to preserve healthy ligaments to maintain
stability and control. Partial knee arthroplasty for patients with osteoarthritis isolated to only 1 or 2
compartments makes it possible for the surgeon to “save” (i.e., avoid cutting) the anterior cruciate
ligament (ACL) and posterior cruciate ligament (PCL), as well as healthy bone and tissue.
Minimizing tissue disruption may reduce recovery time, thereby reducing the risk of complications,
hospital days, and associated costs.38,39
Traditional, non-robotic partial knee procedures, however,
are technically challenging and difficult to perform with accuracy, which is why surgeons tend to
perform total knee procedures on potential UKA candidates.2
One major limitation of a non-robotic UKA procedure is the high failure rate associated with
inaccurate placement of the implant due, in part, to a restricted visual field. Successful UKA requires
proper placement of components in multiple planes, where even the slightest abnormality in implant
depth can cause complications.1 As discussed below, Mako Robotic-Arm assisted procedures may
help to overcome the technical challenges associated with non-robotic UKA procedures.
8
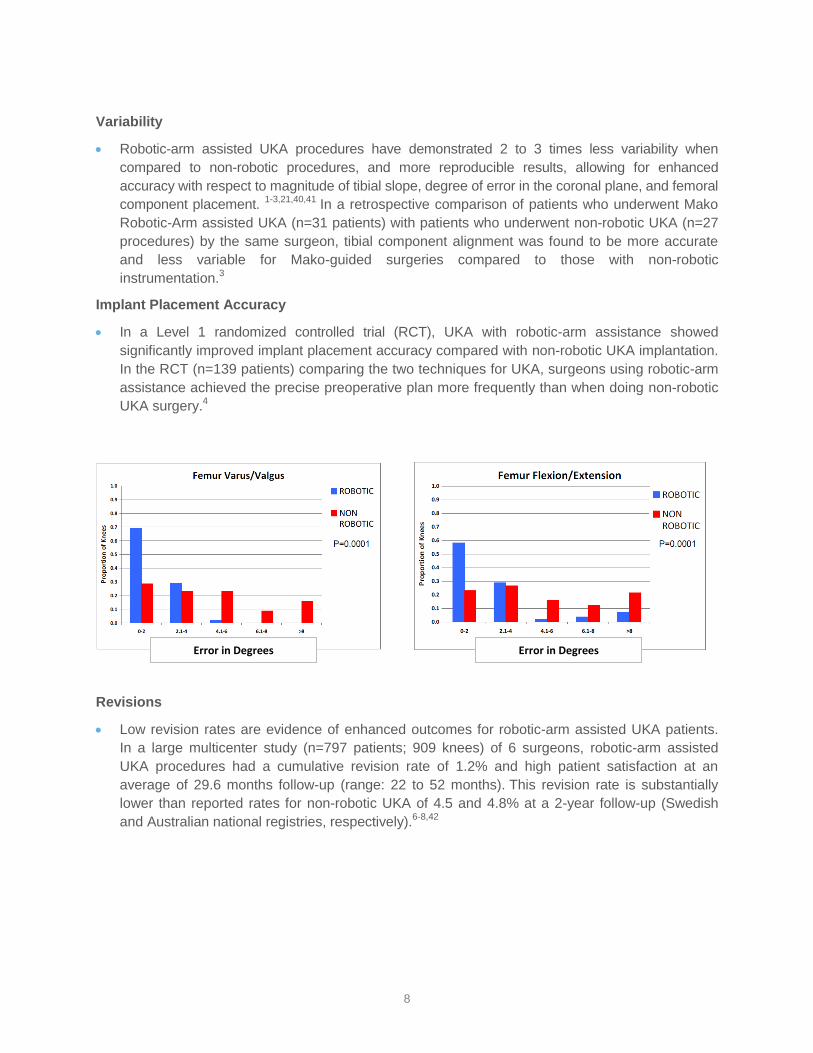
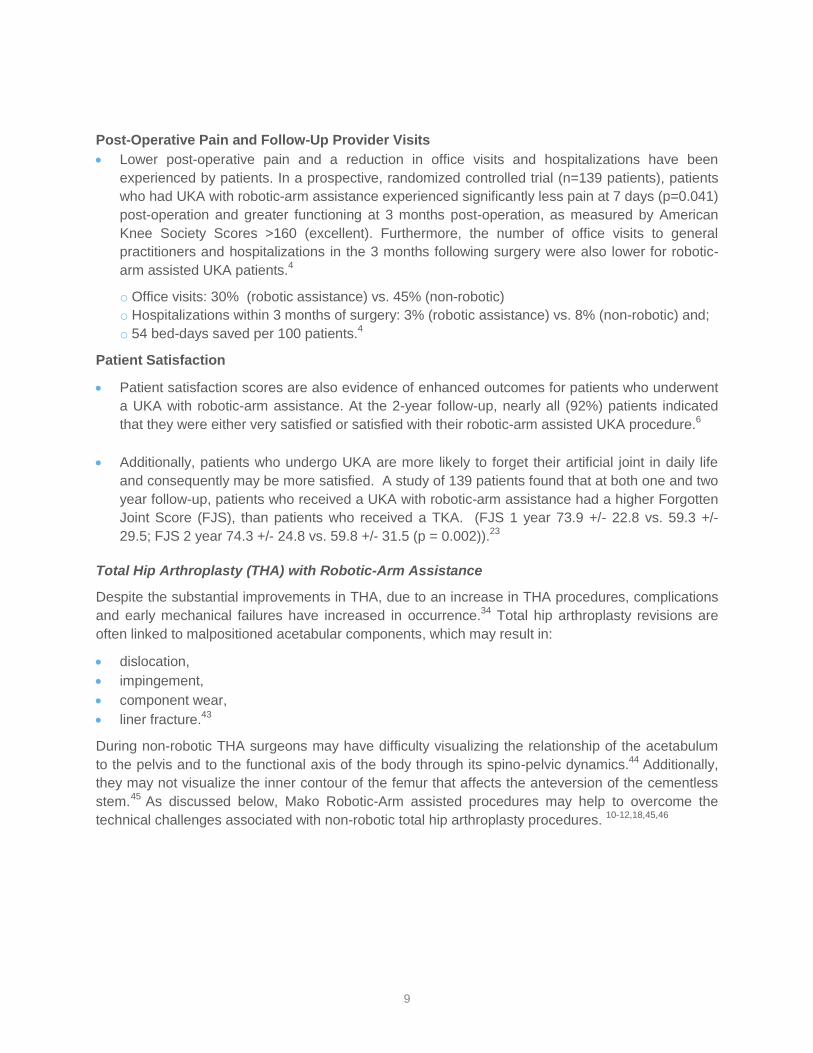
Variability
Robotic-arm assisted UKA procedures have demonstrated 2 to 3 times less variability when
compared to non-robotic procedures, and more reproducible results, allowing for enhanced
accuracy with respect to magnitude of tibial slope, degree of error in the coronal plane, and femoral
component placement. 1-3,21,40,41
In a retrospective comparison of patients who underwent Mako
Robotic-Arm assisted UKA (n=31 patients) with patients who underwent non-robotic UKA (n=27
procedures) by the same surgeon, tibial component alignment was found to be more accurate
and less variable for Mako-guided surgeries compared to those with non-robotic
instrumentation.3
Implant Placement Accuracy
In a Level 1 randomized controlled trial (RCT), UKA with robotic-arm assistance showed
significantly improved implant placement accuracy compared with non-robotic UKA implantation.
In the RCT (n=139 patients) comparing the two techniques for UKA, surgeons using robotic-arm
assistance achieved the precise preoperative plan more frequently than when doing non-robotic
UKA surgery.4
Revisions
Low revision rates are evidence of enhanced outcomes for robotic-arm assisted UKA patients.
In a large multicenter study (n=797 patients; 909 knees) of 6 surgeons, robotic-arm assisted
UKA procedures had a cumulative revision rate of 1.2% and high patient satisfaction at an
average of 29.6 months follow-up (range: 22 to 52 months). This revision rate is substantially
lower than reported rates for non-robotic UKA of 4.5 and 4.8% at a 2-year follow-up (Swedish
and Australian national registries, respectively).6-8,42
Error in Degrees Error in Degrees
9
Post-Operative Pain and Follow-Up Provider Visits
Lower post-operative pain and a reduction in office visits and hospitalizations have been
experienced by patients. In a prospective, randomized controlled trial (n=139 patients), patients
who had UKA with robotic-arm assistance experienced significantly less pain at 7 days (p=0.041)
post-operation and greater functioning at 3 months post-operation, as measured by American
Knee Society Scores >160 (excellent). Furthermore, the number of office visits to general
practitioners and hospitalizations in the 3 months following surgery were also lower for robotic-
arm assisted UKA patients.4
o Office visits: 30% (robotic assistance) vs. 45% (non-robotic)
o Hospitalizations within 3 months of surgery: 3% (robotic assistance) vs. 8% (non-robotic) and;
o 54 bed-days saved per 100 patients.4
Patient Satisfaction
Patient satisfaction scores are also evidence of enhanced outcomes for patients who underwent
a UKA with robotic-arm assistance. At the 2-year follow-up, nearly all (92%) patients indicated
that they were either very satisfied or satisfied with their robotic-arm assisted UKA procedure.6
Additionally, patients who undergo UKA are more likely to forget their artificial joint in daily life
and consequently may be more satisfied. A study of 139 patients found that at both one and two
year follow-up, patients who received a UKA with robotic-arm assistance had a higher Forgotten
Joint Score (FJS), than patients who received a TKA. (FJS 1 year 73.9 +/- 22.8 vs. 59.3 +/-
29.5; FJS 2 year 74.3 +/- 24.8 vs. 59.8 +/- 31.5 (p = 0.002)).23
Total Hip Arthroplasty (THA) with Robotic-Arm Assistance
Despite the substantial improvements in THA, due to an increase in THA procedures, complications
and early mechanical failures have increased in occurrence.34
Total hip arthroplasty revisions are
often linked to malpositioned acetabular components, which may result in:
dislocation,
impingement,
component wear,
liner fracture.43
During non-robotic THA surgeons may have difficulty visualizing the relationship of the acetabulum
to the pelvis and to the functional axis of the body through its spino-pelvic dynamics.44
Additionally,
they may not visualize the inner contour of the femur that affects the anteversion of the cementless
stem.45
As discussed below, Mako Robotic-Arm assisted procedures may help to overcome the
technical challenges associated with non-robotic total hip arthroplasty procedures. 10-12,18,45,46
10
Dislocations
Patients have experienced a reduction in dislocations with robot-assisted THA. In a recent study
evaluating patients undergoing posterior-approach total hip arthroplasty, individuals undergoing
robotic-arm assisted THA experienced significantly fewer dislocations at 6 months compared to
those undergoing non-robotic THA (P<0.001).18
Based on data prospectively collected on primary THAs, using robotic-arm assistance during
THA reduced early dislocation rates compared to conventional THA.18,45
In this analysis, data
were reviewed for all THAs (n=200) conducted consecutively by one surgeon at a single
institution in 2011 and 2012. Results included:
o Lower dislocation rates—likely stemming from enhanced accuracy for both acetabular
abduction (AAB) and acetabular anteversion (AAV) in the patient group receiving robotic-
arm assisted surgery compared with non-robotic THA (0% vs 3%, p<0.05).18 ,45
o Reduced blood loss in the patient group receiving robotic-arm assisted surgery
compared to non-robotic THA (p-value <0.0001). 18 ,45
o Higher modified Harris Hip scores and UCLA activity level at one year in the patient
group receiving robotic-arm assisted surgery compared with non-robotic THA. 18 ,45
Implant Stability
Preservation of acetabular bone during primary THA is important to implant stability and
longevity. Eccentric or excessive acetabular reaming may result in many complications that lead
to subsequent THA revisions.46
In a matched-pair controlled study, robotic-arm assisted THA
allowed for the use of smaller acetabular cups in relation to the patient’s femoral head size
compared to conventional THA. The use of smaller acetabular cups resulted in greater
preservation of bone stock which supports implant stability and has been shown to help prevent
dislocation.46
Acetabular Cup Implantation
Optimal positioning of the acetabular component promotes the long-term success of total hip
arthroplasty by reducing the rate of adverse outcomes, such as component wear and dislocation,
and ultimately a reduction in admissions and revisions. Robotic-arm assistance has
demonstrated a significantly greater percent of acetabular components placed in both
Lewinnek’s and Callanan’s safe zones.11
Recent studies have demonstrated that optimal
acetabular cup implantation in non-robotic cases is achieved less frequently than originally
believed.18,45
Orientation of the acetabular cup influences the risk of post-operative complications
following THA. Studies suggest that the optimal anteversion ranges from 0 to 30° and acceptable
inclination ranges from 30 to 50°.43
Cup angles that occur outside these optimal ranges increase
the risk of complications such as impingement, increased wear at bearing surfaces, and hip
dislocation.48
Furthermore, the amount of surgical experience does not appear to affect proper
cup orientation.4849
A recent study revealed that the acetabular cup was positioned in an ideal range only 50% of the
time during traditionally performed procedures (non-robotic).43
11
In a study comparing non-robotic and robotic alignment techniques, 50 Mako Robotic-Arm
assisted THAs were matched to historical non-robotic THAs conducted between 2008 and
2012.11
One hundred percent (100%) of the Mako Robotic-Arm assisted THAs were placed
within an acceptable range for anteversion and inclination vs. only 80% (40/50) of the manually
aligned and implanted THAs. Similarly, 92% of the Mako Robotic-Arm assisted THAs were within
another generally accepted range (Callanan) vs. only 62% of non-robotic THAs.11
In a multicenter study (n=119 Mako Robotic-Arm assisted THA cases), planned cup placement
was compared with cup orientation post-operatively. In 95% of cases, cup placements were
recorded to be within 5° of the surgical plan, demonstrating that Mako Robotic-Arm assistance
provides surgeons with improved measures to facilitate patient-specific planning.12
In a 2015 multicenter study (n=1,980, 228 Mako Robotic-Arm Assisted and 1,752 non-robotic
THA procedures), robotic-arm assistance resulted in a significantly greater percent of
components placed within a recommended range than conventional, x-ray, and fluoroscopic
modalities (p <0.05).10
Clinical Efficacy Summary
In summary, the use of Mako in both UKA and THA procedures has demonstrated enhanced clinical
outcomes and durability through more accurate component positioning/alignment, bone
preservation, and the potential for decreased blood loss. This has led to revision rates lower than
previously reported in historic registry data, as well as higher patient satisfaction scores. Moreover,
many of the technical challenges and increased adverse events associated with non-robotic UKA
and THA have been shown to be reduced with the use of robotic-arm assistance.
The Economics of Mako
Joint disease, affecting 13.9% of adults aged 25 years and older, is associated with an extremely
high economic burden. More than 600,000 patients in the U.S. had a primary knee arthroplasty
surgery in 2010, or 1.9 per 1,000, and as previously mentioned, by 2030 this demand is projected to
increase over 600% to 9.6 procedures per 1,000. The demand for primary total hip arthroplasty is
estimated to grow by 174% to 1.6 procedures per 1,000.
Robotic-arm assistance enables surgeons performing UKAs to reduce variability, achieve more
accurate placement, and reduce revisions, as previously indicated (3.5% vs 0.4%, p=.004, Source:
OptumInsight claims data). It is important to note that a revision joint arthroplasty is much more
complicated and more costly than the initial operation. The following are results of an analysis of the
Medicare population in the U.S. (CMS IPSAF and OPSAF, 2012 to 2014):
The average cost of a revision following a non-robotic primary knee replacement was greater
than $39,000;
A revision subsequent to a robotic arm-assisted primary knee arthroplasty surgery was $22,941,
40% less expensive than a revision following a non-robotic knee arthroplasty procedure;
This represents a significant cost savings (over $16,000 per procedure).

12
Moreover, in the OptumInsight commercial population, robotic assistance is associated with lower
all-cause readmission rates for UKA procedures within 30 days (over 36% lower) and 90 days (over
16% lower). These reduced readmission rates, in addition to the lower average cost per readmission
for robotic-arm assisted UKA procedures, translates to:
40% lower readmission costs @ 30 days
66% lower readmission costs @ 90 days
Managing Costs for Patients Requiring Knee Arthroplasty by Incorporating Mako
Robotic-Arm
The PMPM spend for primary joint arthroplasty and associated readmissions (including revisions) is
approximately $3.50 to $4.00 PMPM in a typical commercial population, a significant line item that
Mako can assist in managing. Importantly, demographic trends project increases in osteoarthritis
and joint arthroplasty at levels that will require all stakeholders to consider tools like Mako. Such
tools can facilitate increased opportunity to provide patients with the right procedure (specific to their
joint disease) at the right time, within an episode of care that utilizes services that potentially reduce
UKA revision rates as well as subsequent TKA rates.
In a Medicare population (CMS IPSAF and OPSAF, 2012 to 2014), the cost of revision surgery
subsequent to a robotic arm-assisted knee arthroplasty procedure is 40% less expensive than a
revision following a non-robotic knee arthroplasty procedure ($22,941 for robotic-arm assisted vs.
$39,165 for non-robotic). Additionally, in the Medicare population (CMS IPSAF, 2012 to 2014) the
average length of stay was 1.1 days shorter for a revision surgery subsequent to a robotic arm-
assisted knee arthroplasty procedure than a revision following a non-robotic knee arthroplasty
procedure (2.2 vs. 3.3 days). Note: See Appendix for commercial and Medicare claims analysis
methodology.
Robotic-Arm Assistance Can Change the Trajectory of Surgical Joint Interventionse
Robotic-arm assistance may allow surgeons to perform UKAs in some patients who traditionally
would have undergone a TKA, thereby resulting in a change in practice patterns and surgical setting
with a favorable cost impact (robotic UKAs cost $500 less than TKAs on average in a commercial
population). To the extent that approximately 5 to 21% of UKA candidates are undergoing TKAs13,14
in an inpatient setting, robotic-arm assistance can facilitate more accurate alignment with less
variation, a reduction in readmissions (notably revisions), as well as a shift to an outpatient setting,
leading to potential savings of $0.02 to $0.09 PMPM by 2020 in a typical commercial population
(OptumInsight data 2013 to 2015). Furthermore, if a 20% migration from inpatient to hospital
outpatient is realized, savings can increase to $0.30 PMPM by 2020.
e Analysis conducted by Baker Tilly using a database compiled by OptumInsight, Inc. (Eden Prairie, MN) comprising
claims generated by a national commercial health plan consisting of approximately 25 million members. Index cases incurred Jan. 2013 – Dec. 2013, revision cases incurred within 24 months of index procedure. This commercial data has not been blended with Medicare or Medicare Advantage data.

13
The economic benefits are noteworthy. A review of commercial 2014 data showed an ALOS of 1.8
days for UKA with robotic-arm assistance versus 2.9 days for TKA. Moreover, as previously stated,
from the OptumInsight data analysis, the rate of revision following a UKA with robotic-arm assistance
is significantly lower than that of a non-robotic UKA (0.4% vs 3.5%, p=.004) in a large commercial
data set.e Additionally, a recent study showed using robotic-arm assistance in UKA procedures is
cost effective compared with non-robotic UKAs providing additional quality-adjusted life years
(QALY) and reduced costs in high volume centers.49
Impact on Innovative Reimbursement Models
April 1, 2016 commenced the Medicare Comprehensive Care Joint Replacement (CJR) model in the
U.S., otherwise known as bundled payments. Under CJR, participation is mandatory for 791
hospitals in 67 geographic areas. These hospitals are accountable for the quality and total Medicare
cost of care provided to Medicare fee-for-service beneficiaries for lower extremity joint arthroplasty
procedures and recovery within 90 days post hospital discharge. Similarly, commercial payers and
employers have been implementing bundled payments with hospitals on hip and knee arthroplasty
surgeries. For example, The Connecticut Joint Replacement Institute at St. Francis Hospital has
rolled out a bundled payment program with ConnectiCare, the Mayo Clinic implemented a bundled
payment for knee arthroplasty surgeries covered by Florida Blue, and Johns Hopkins participates in
the Employers Centers for Excellence Network which offers bundled payments to large U.S.
employers such as Walmart and Lowe’s.50
The quality and cost benefits described in this value summary may improve a hospital’s performance
in these bundled payment episodes, by potentially reducing those costs associated with
complications and adverse events as well as potentially improving quality composite scores for a
participating hospital. This projected improvement in quality and cost may further reduce the
episode cost for payers and employers.
Payer Coverage Considerations
The majority of payers consider robotic-arm assistance integral to the primary joint arthroplasty
surgical procedure and not separately or additionally reimbursed. Surgical procedures completed
with robotic-arm assistance should be consistent with existing payer coverage policies and current
payer contract rates for the primary surgical procedure. For example, as previously stated, the
UnitedHealthcare and Humana reimbursement policies on Robotic-Assisted Surgery do not provide
for additional reimbursement. However, the lack of incremental reimbursement should not prohibit
surgeons from using their professional discretion in deploying robotic-arm assistance.
Conclusion
Robotic-arm assistance is an innovative, cost effective solution for payers. The Mako Robotic-Arm
Assisted System enables surgeons to treat knee and hip conditions with greater predictability4,6,7,11
by allowing for more accurate component placement and reproducibility of both partial knee
arthroplasty and total hip arthroplasty. This technology can also have a positive impact on patients
by potentially reducing post-operative pain,4 decreasing adverse events,
6-8 and enhancing their
satisfaction with the joint replacement procedure.6
14
With all factors pointing to an increase in the prevalence of joint arthroplasties, it is important to
identify technologies to help mitigate rising costs and reduce the overall economic burden of
osteoarthritis. Allowing surgeons access to this important safe and effective operating room
technology gives surgeons a valuable tool to potentially enhance outcomes, mitigate adverse
events,6-8
and enhance the patient experience.
15
APPENDIX:
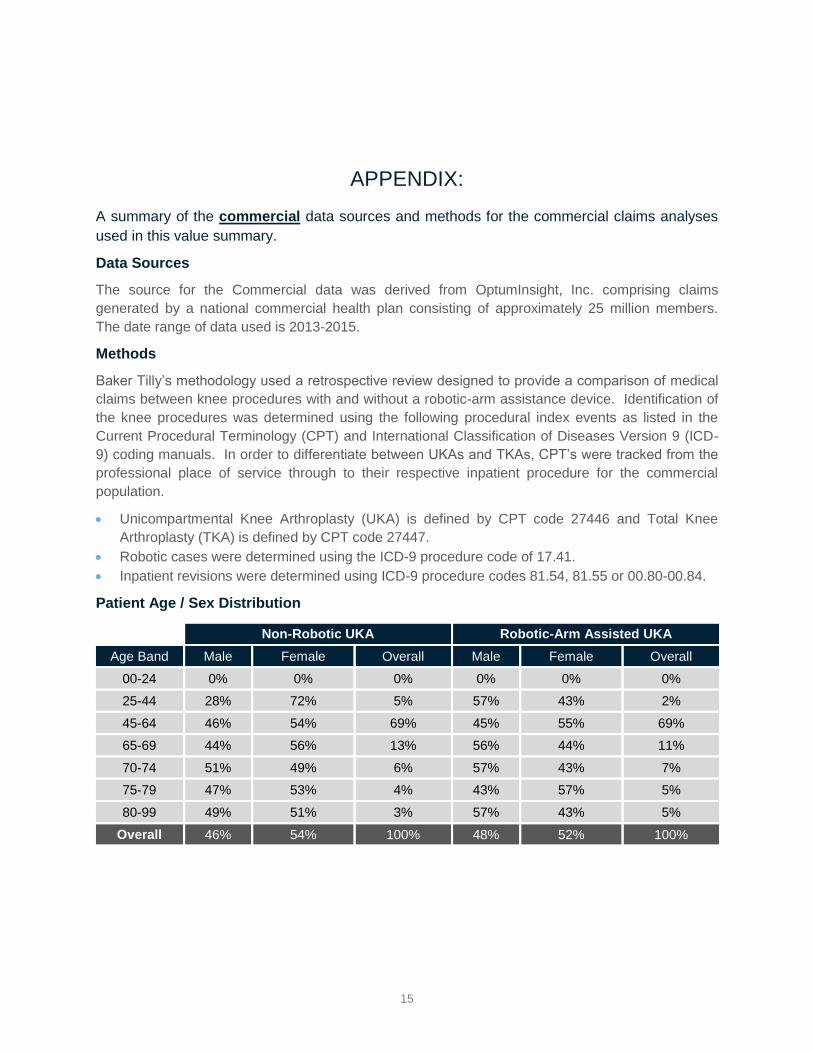
A summary of the commercial data sources and methods for the commercial claims analyses
used in this value summary.
Data Sources
The source for the Commercial data was derived from OptumInsight, Inc. comprising claims
generated by a national commercial health plan consisting of approximately 25 million members.
The date range of data used is 2013-2015.
Methods
Baker Tilly’s methodology used a retrospective review designed to provide a comparison of medical
claims between knee procedures with and without a robotic-arm assistance device. Identification of
the knee procedures was determined using the following procedural index events as listed in the
Current Procedural Terminology (CPT) and International Classification of Diseases Version 9 (ICD-
9) coding manuals. In order to differentiate between UKAs and TKAs, CPT’s were tracked from the
professional place of service through to their respective inpatient procedure for the commercial
population.
Unicompartmental Knee Arthroplasty (UKA) is defined by CPT code 27446 and Total Knee
Arthroplasty (TKA) is defined by CPT code 27447.
Robotic cases were determined using the ICD-9 procedure code of 17.41.
Inpatient revisions were determined using ICD-9 procedure codes 81.54, 81.55 or 00.80-00.84.
Patient Age / Sex Distribution
Non-Robotic UKA Robotic-Arm Assisted UKA
Age Band Male Female Overall Male Female Overall
00-24 0% 0% 0% 0% 0% 0%
25-44 28% 72% 5% 57% 43% 2%
45-64 46% 54% 69% 45% 55% 69%
65-69 44% 56% 13% 56% 44% 11%
70-74 51% 49% 6% 57% 43% 7%
75-79 47% 53% 4% 43% 57% 5%
80-99 49% 51% 3% 57% 43% 5%
Overall 46% 54% 100% 48% 52% 100%
16
A summary of the Medicare data sources and methods for the Medicare claims analyses used
in this value summary.
Data Sources
The Medicare data was derived from the Medicare Inpatient Standard Analytical File (IPSAF) and
the Medicare Outpatient Standard Analytical File (OPSAF) for calendar years 2012-2014.
Methods
Baker Tilly’s methodology used a retrospective review designed to provide a comparison of medical
claims between knee procedures with and without a robotic-arm assistance device. Identification of
the knee procedures was determined using the following procedural index events as listed in the
Current Procedural Terminology (CPT) and International Classification of Diseases Version 9 (ICD-
9) coding manuals.
ICD-9 procedure code 81.54 with either DRG 461, 462, 469 or 470 was used to determine knee
procedures.
Robotic cases were determined using the ICD-9 procedure code of 17.41.
Inpatient revisions were determined using ICD-9 procedure codes 81.54, 81.55 or 00.80-00.84.
Outpatient revisions were determined using CPT codes 27486 or 27487.

17
References
1Dunbar NJ, Roche MW, Park BH, Branch SH, Conditt MA, Banks SA. Accuracy of dynamic tactile-guided
unicompartmental knee arthroplasty. J Arthroplasty. 2012;27(5):803-808,e1.
2Lonner JH. Robotic arm–assisted unicompartmental arthroplasty. Seminars in Arthroplasty. 2009;20(1):15-22.
3Lonner JH, John TK, Conditt MA. Robotic arm-assisted UKA improves tibial component alignment: a pilot
study. Clin Orthop Relat Res. 2010;468(1):141-146.
4Blyth M, Jones B, MacLean A, Anthony I, Rowe P. Accuracy of UKA implant positioning and early clinical
outcomes in a RCT comparing robotic assisted and manual surgery. In: Proceedings 13th Annual Computer Assisted Orthopedic Surgery Meeting; June 12-15, 2013; Orlando, FL, USA. (Blyth/Jones 2013b).
5Augart M, Plate JF, Seyler TM, et al. Improving outcomes of lateral UKA with robotic assisted surgery. In:
Proceedings 13th Annual meeting Computer Assisted Orthopedic Surgery; June 18-21, 2014; Milan, Italy.
6Coon T, Roche M, Buechel F,et al. Short to mid term survivorship of robotic arm assisted UKA: a multicenter
Study. In: Proceedings Annual Pan Pacific Orthopaedic Congress; July 16-19, 2014; Kona, HI.
7The Swedish Knee Arthroplasty Registry. Annual Report 2012. Department of Orthopaedics; Skåne University
Hospital; Lund, Sweden.
8Australian Orthopaedic Association National Joint Replacement Registry. Annual Report. Adelaide:AOA; 2013.
9Bell S, Anthony I, Jones B, MacLean A, et al. Improved accuracy of component positioning with robotoc-
assisted unicompartmental knee arthroplasty. J Bone Joint Surg Am. 2016;98:627-635.
10Domb BG, et al. Accuracy of component positioning in 1980 total hip arthroplasties: a comparative analysis
by surgical technique and mode of guidance. J Arthroplasty. 2015 December 30(12):2208-2218.
11Domb BG, Bitar YFE, Sadik AY, Stake CE, Botser IB. Comparison of robotic-assisted and conventional
acetabular cup placement in THA: a matched-pair controlled study. Clin Orthop Relat Res. 2013;472(1):329-336.
12Elson L, Dounchis J, Illgren R, Marchand R, et al. Precision of acetabular cup placement in robotic integrated
total hip arthroplasty. Hip International. 2015; 25(6):531-536.
13Arno S, Maffei D, Walker PS, Schwarzkopf R, Desai P, Steiner GC. Retrospective analysis of total knee
arthroplasty cases for visual, histological, and clinical eligibility of unicompartmental knee arthroplasties. J Arthroplasty. 2011;26(8):1396-1403.
14Ghomrawi HM, Eggman AA, Pearle AD. Effect of age on cost effectiveness of unicompartmental knee
arthroplasty compared with total knee arthroplasty in the U.S. J Bone Joint Surg Am. 2015;97:396-402.
15Ritter M, Faris P, Thong A, Davis K, Meding J, Berend M. Intra-operative findings in varus osteoarthritis of the
knee. An analysis of pre-operative alignment in potential candidates for unicompartmental arthroplasty. J Bone Joint Surg Br. 2004; 86(1):43-47.
16Jerabek SA, Carroll KM, Maratt JD, Mayman DJ, Padgett DE. Accuracy of cup positioning and achieving
desired hip length and offset following robotic THA. Poster presented at: 14th Annual Computer Assisted Orthopedic Surgery Meeting, June 18-21, 2014, Milan, Italy.
17Esposito CI, Lipman J, Carroll KM, Jerabek SA, Mayman SA, Padgett DE. Acetabular component cup
placement using a haptically guided robotic technology in total hip arthroplasty. 16th EFFORT Congress, May
28-30, 2015, Prague, Czech Republic.
18Illgen RL, Bukowski BR, Abiola R. Outcomes after primary total hip arthroplasty: manual compared with
robotic assisted techniques. 44th Annual Advances in Arthroplasty; Cambridge, MA. October 7-10 2014.
18
19Nawabi DH, Conditt MA, Ranawat AS, et al. Haptically guided robotic technology in total hip arthroplasty: a
cadaveric investigation. Proceedings of the Institution of Mechanical Engineers, Journal of Engineering in Medicine. 2012;2273(3, pt h):302-309.
20Atesok K, Galos D, Jazrawi LM, Egol KA. Preoperative planning in orthopaedic surgery. Bulletin of the
Hospital for Joint Diseases. 2015;73(4):257-268. 12p.
21Plate JF, Mofidi A, Mannava S, et al. Achieving accurate ligament balancing using robotic-assisted
unicompartmental knee arthroplasty. Adv Orthop. 2013;1-6.
22Parvizi J, Mui A, Purtill JJ, Sharkey PF, Hozack WJ, Rothman RH. Total joint arthroplasty: when do fatal or
near-fatal complications occur? J Bone Joint Surg Am. 2007;89:27-32.
23Zuiderbaan H, va der List J, Khamaisy S, et al. Unicompartmental knee arthroplasty versus total knee
arthroplasty: which type of artificial joint do patients forget? Knee Surg Sports Traumatol Arthrosc. 2015 November;1-6, 21.
24Buckwalter JA, Saltzman C, Brown T. The impact of osteoarthritis. Clin Orthop Relat Res. 2004;427:S6-S15.
25Felson DT. Osteoarthritis: new insights. The disease and its risk factors. Ann Intern Med. 2000;133(8, pt
1):635-646.
26Leopold SS. Minimally invasive total knee arthroplasty for osteoarthritis. N Engl J Med. 2009;360(17):1749-
1758.
27Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic
conditions in the United States. Arthritis Rheum. 2007;58(1, pt 2):26-35.
28Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: arthritis data
from the Third National Health and Nutrition Examination Survey 1991-94. J Rheumatol. 2006;33(11):2271-2279.
29 Hunter D, Schofield D, Callander E. The individual and socioeconomic impact of osteoarthritis. Nature
Reviews Rheumatology. 2014; 10:437-441.
30Barbour KE, Helmick CG, Theis KA, et al. Prevalence of doctor-diagnosed arthritis and arthritis-attributable
activity limitation-United States, 2010-2012. Morb Mortal Wkly. Rep. 2013;62(44):869-873.
31Carr AJ. Beyond disability: measuring the social and personal consequences of osteoarthritis. Osteoarthritis
and Cartilage. 1999;7(2):230-238.
32Murphy L, Hemlock CG. The impact of osteoarthritis in the United States; a population-health perspective: A
population-based review of the fourth most common cause of hospitalization in U.S. adults. Orthop Nurs. 2012;31(2):85-91.
33Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in
the United States from 2005 to 2030. Bone Joint Surg Am. 2007 April;89(4)780-785. doi: 10.2106/JBJS.F.00222.
34Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, Berry DJ. The epidemiology of revision total hip arthroplasty in
the United States. J Bone Joint Surg Am. 2009;91(1):128-133. doi: 10.2106/JBJS.H.00155.
35Novitas LCD for total hip and knee arthroplasty citing the American Academy of Orthopaedic Surgeons
(AAOS) and the American Association of Hip and Knee Surgeons (AAHKS). Model Coverage Determination: Total Joint Arthroplasty.
36Callaghan JJ, O’Rourke MR, Saleh KJ. Why knees fail: lessons learned. J Arthroplast. 2004;19(4):31-34.
37Ng VY, Lustenberger D, Hoang K, et al. Preoperative risk stratification and risk reduction for total joint
reconstruction: AAOS exhibit selection. J Bone Joint Surg Am. 2013;95:e191-15.

19
38White RE, Allman JK, Trauger JA, Dales BH. Clinical comparison of the midvastus and medial parapatellar
surgical approaches. Clin Orthop Relat Res. 1999;367:117-12275.
39Tria AJ, Coon TM. Minimal incision total knee arthroplasty. Clin Orthop Relat Res. 2003;416:185-190.
40Blyth M, Smith J, Jones B, MacLean A, Anthony I, Rowe P. A CT based comparison of accuracy of
unicompartmental knee arthroplasty (UKA) implant positioning with and without the aid of robotic surgical assistance. 13
th Annual CAOS Meeting, June 12-15, 2013, Orlando, FL, USA. (Blyth/Jones 2013a).
41 Citak M, Suero EM, Citak M, et al. Unicompartmental knee arthroplasty: is robotic technology more accurate
than conventional technique? The Knee. 2013;20(4):268-271.
42Coon T, Roche M, Pearle A, Dounchis J, Borus T, Buechel F, Bhowmik-Stoker M, Conditt M. Short to Mid
Term Survivorship of Robotic-Arm Assisted Unicompartmental Knee Arthroplasty; EFFORT 2016 Poster; 1-3 June; Geneva.
43 Callanan MC, Jarrett B, Bragdon CR, et al. The John Charnley Award: risk factors for cup malpositioning:
quality improvement through a joint registry at a tertiary hospital. Clin Orthop Relat Res. 2010;469(2):319-329
44 Lazennac JY, Boyer P, Gorin M, Catone Y, Rosseau MA. Acetabular anteversion with CT in supine,
simulated standing, and sitting positions in a THA patient population. Clin Orthop Relat Res. 2011; 469:1103-1109. doi 10.1007/s11999-010-1732-7.
45Illgen R. Robotic assisted THA: reduce outliers and predictable outcomes. 43rd Annual Course: Advances in
Arthroplasty; October 22-25, 2013; Cambridge, MA. (Illgen 2013b)
46Suarez-Ahedo C, Gui C, Martin TJ, Stake CE, et al. Preservation of acetabular bone stock in total hip
arthroplasty using conventional vs. robotic techniques, A Matched-Pair Controlled Study. In: Preceedings World Arthroplasty Congress; April 15-18, 2015; Paris, France.
47Malik A, Maheshwari A, Dorr LD. Impingement with Total Hip Replacement. J Bone Joint Surg Am.
2007;89:1832-1842.
48Reize P, Geiger EV, Suckel A, Rudert M, Wulker N. Influence of surgical experience on accuracy of
acetabular cup positioning in total hip arthroplasty. Am J Orthop. 2008;37(7):360-363.
49Moschetti WE, Konopka JF, Genuario JW, Rubash HE. Can robot-assisted unicompartmental knee
arthroplasty be cost effective? a markov decision analysis. J Arthroplasty. November 2015.
50Tomsic, M. “How Lowe’s Saves Money While Offering Employees Free Surgeries.” WFAE. March 2015.
MKOSYM-WP-3_11184