Major Trauma Patient Document - hscboard.hscni.net · Major Trauma Patient Document The scribe must...
44
Major Trauma Patient Document The scribe must complete pages 1-5 and Drug Page The Team Leader is responsible for checking the entire document OPEN FRACTURES - PLEASE COMPLETE ORTHOPLASTIC OPEN FRACTURES PRO FORMA Use addressograph - otherwise write in capitals Surname: ________________________________________ First names: ______________________________________ DOB: ____________________________________________ Health and Care No._______________________________ Date: ________________________ Arrival time: ________________________ ED Consultant: ______________________________________________ Present: Yes No Name: ___________________________________________________ Team Leader: _________________________________________ Grade: ____________________ Scribe: _______________________________________________ Speciality Name Grade Arrival time Nurse ED A nurse: ____________________ Anaesthetics B nurse: ____________________ General surgery C nurse: ____________________ Orthopaedics Runner: ____________________ Cardiothoracic Please ensure each page is completed in full NI Major Trauma Network | September 2018 1
-
Upload
nguyencong -
Category
Documents
-
view
220 -
download
0
Transcript of Major Trauma Patient Document - hscboard.hscni.net · Major Trauma Patient Document The scribe must...

Major Trauma Patient Document
The scribe must complete pages 1-5 and Drug Page
The Team Leader is responsible forchecking the entire document
OPEN FRACTURES - PLEASE COMPLETE ORTHOPLASTIC OPEN FRACTURES PRO FORMA
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Date: ________________________ Arrival time: ________________________
ED Consultant: ______________________________________________
Present: Yes No Name: ___________________________________________________
Team Leader: _________________________________________ Grade: ____________________
Scribe: _______________________________________________
Speciality Name GradeArrival time Nurse
EDA nurse: ____________________
AnaestheticsB nurse: ____________________
General surgeryC nurse: ____________________
OrthopaedicsRunner: ____________________
Cardiothoracic
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 1

NI Major Trauma Network | September 20182
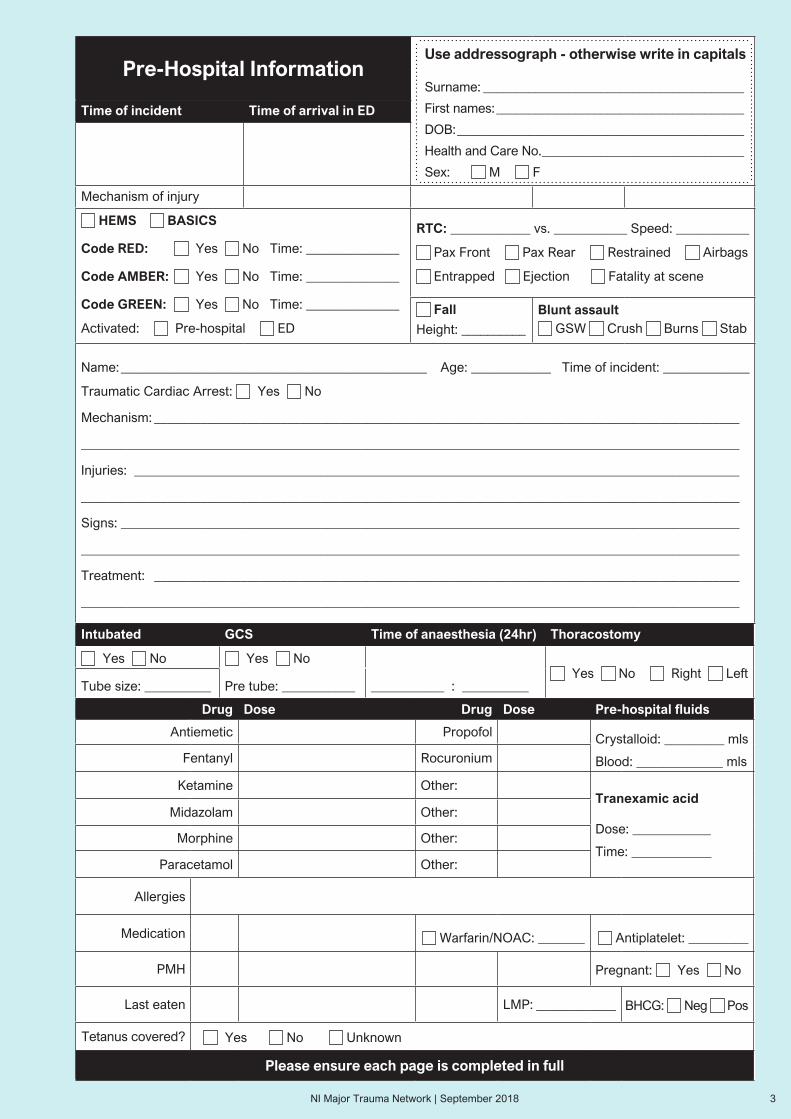
Pre-Hospital Information
Time of incident Time of arrival in ED
Mechanism of injury
HEMS BASICS
Code RED: Yes No Time: ______________
Code AMBER: Yes No Time: ______________
Code GREEN: Yes No Time: ______________
Activated: Pre-hospital ED
RTC: ____________ vs. ___________ Speed: ___________
Pax Front Pax Rear Restrained Airbags
Entrapped Ejection Fatality at scene
Fall
Height: __________
Blunt assault GSW Crush Burns Stab
Name: ______________________________________________ Age: ____________ Time of incident: _____________
Traumatic Cardiac Arrest: Yes No
Mechanism: ________________________________________________________________________________________
___________________________________________________________________________________________________
Injuries: ___________________________________________________________________________________________
___________________________________________________________________________________________________
Signs: _____________________________________________________________________________________________
___________________________________________________________________________________________________
Treatment: ________________________________________________________________________________________
___________________________________________________________________________________________________
Drug Dose Drug Dose Pre-hospital fluids
Antiemetic Propofol Crystalloid: _________ mls
Blood: _____________ mlsFentanyl Rocuronium
Ketamine Other:Tranexamic acid
Dose: ____________
Time: ____________
Midazolam Other:
Morphine Other:
Paracetamol Other:
Allergies
Medication Warfarin/NOAC: _______ Antiplatelet: _________
PMH Pregnant: Yes No
Last eaten LMP: ____________ BHCG: Neg Pos
Tetanus covered? Yes No Unknown
Please ensure each page is completed in full
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Intubated GCS Time of anaesthesia (24hr) Thoracostomy
Yes No Yes No Yes No Right Left
Tube size: __________ Pre tube: ___________ ___________ : __________
NI Major Trauma Network | September 2018 3
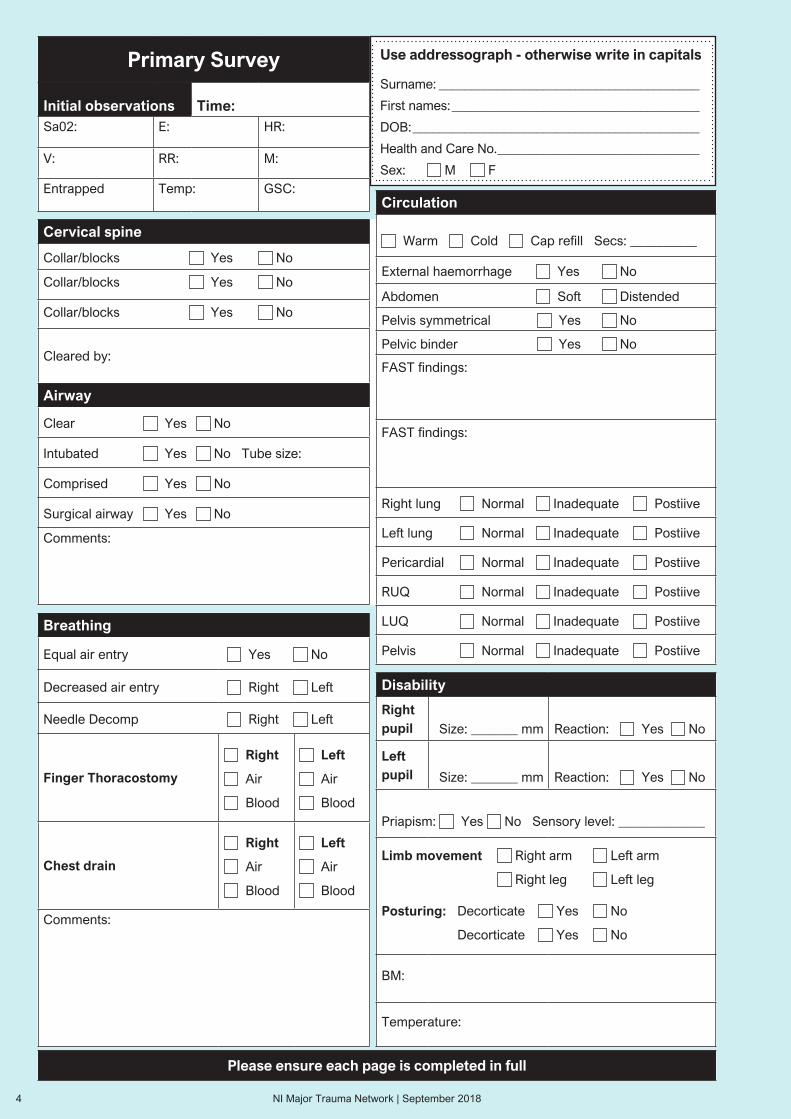
Primary Survey
Initial observations Time:Sa02: E: HR:
V: RR: M:
Entrapped Temp: GSC:
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Cervical spine
Collar/blocks Yes No
Collar/blocks Yes No
Collar/blocks Yes No
Cleared by:
Airway
Clear Yes No
Intubated Yes No Tube size:
Comprised Yes No
Surgical airway Yes No
Comments:
Breathing
Equal air entry Yes No
Decreased air entry Right Left
Needle Decomp Right Left
Finger Thoracostomy
Right
Air
Blood
Left
Air
Blood
Chest drain
Right
Air
Blood
Left
Air
Blood
Comments:
Disability
Rightpupil Size: _______ mm Reaction: Yes No
Leftpupil Size: _______ mm Reaction: Yes No
Priapism: Yes No Sensory level: _____________
Limb movement Right arm Left arm
Right leg Left leg
Posturing: Decorticate Yes No
Decorticate Yes No
BM:
Temperature:
Circulation
Warm Cold Cap refill Secs: __________
External haemorrhage Yes No
Abdomen Soft Distended
Pelvis symmetrical Yes No
Pelvic binder Yes No
FAST findings:
FAST findings:
Right lung Normal Inadequate Postiive
Left lung Normal Inadequate Postiive
Pericardial Normal Inadequate Postiive
RUQ Normal Inadequate Postiive
LUQ Normal Inadequate Postiive
Pelvis Normal Inadequate Postiive
Please ensure each page is completed in full
NI Major Trauma Network | September 20184

Trauma Chronology
Body region findings
Plain films (tick)
Time:_____________ CXR PXR C-SPINE
eFAST
Time:_____________
Clinician name: ____________________
Clinician grade/training: _____________
Result: ________________________________
______________________________________
IV access: Yes No Site1: ___________ Site2: __________
Site3: ___________ Site4: __________
IO access: Yes No Site1: ___________ Site2: __________
Site3: ___________ Site4: __________
Whole body CT Head Spine Chest Abdomen and pelvis Other:
Airway+C Spine ____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Breathing ____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Circulation ____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Disability ____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Exposure ____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 5
ED Injury Summary
Performed by:____________________________________
Signature:______________________ Date: ____________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
eFAST
Head
Max Fax
Neck
Chest
Abdomen
Pelvis
Upper limbs
Lower limbs
Log roll/back
Rectal
ECG
Other
Time of death: Admitting Consultant:
Disposal: Signature of Team Leader:
NI Major Trauma Network | September 20186

Secondary SurveyPlease indicate location of all injuries
and interventions
Signature: _______________________ Date: __________
Interventions
Collar Yes No
Tracheal tube Yes No
Chest drainage Yes No Left Right
Pelvic splint Yes No
Traction splint Yes No Left Right
IV accesS Site1: ________ Site2: ____________
Yes No Site3: ________ Site4: ____________
IO access Site1: ________ Site2: ____________
Yes No Site3: ________ Site4: ____________
Central line Yes No Left Right
Arterial line Yes No Left Right
Urine catheter Yes No
Pop backslab Yes No Left Right
Comments:
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
NI Major Trauma Network | September 2018 7

Secondary Survey
Performed by:____________________________________
Signature:______________________ Date: ____________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Body Region FindingsHead None
Max Fax None
Neck None
Chest None
Abdomen None
Pelvis None
Upper limbs None
Lower limbs None
Log roll/back None
Rectal None
ECG None
Other None
Please ensure each page is completed in full
NI Major Trauma Network | September 20188

Team Leader’s notes
Date:______________________ Time: _________________
Consultant: ______________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 9

Team Leader’s notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201810

Nursing notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 11
Nursing notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201812

Anaesthetic notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Anaesthetics have reviewed the patient and feel there is no further involvement and are signing off.We are happy to review patient on request
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 13
Anaesthetic notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201814
General Surgery notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
General Surgeons have reviewed the patient and feel there is no further involvement and are signing off.We are happy to review patient on request
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 15
General Surgery notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201816

Orthoplastic Open Fracture Pathway
• Indications - Open fractures of Long bones, Hindfoot or Midfoot• Open fractures require timely MDT input, follow BOAST Open
Fractures Standards• All open fractures must be reported to TARN; accurate completion
of proforma is mandatory.
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Injury Description
Wound Characteristics (Size, location, dept etc)
________________________________________________
________________________________________________
________________________________________________
________________________________________________
Heavily Contaminated (Sewage, Agricultural, Aquatic, Blast)
Wound Photography Yes No
Wound Dressing
Time: ______ : ______
Type: ___________________________________________
Wound Splintage________________________________________________________________________________________________
Imaging X-Ray CT ]Findings________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
IV ANTIBIOTICS [< 1 hour from injury achieved ]Agent: __________________________________________
Time Given: ______ : ______ Date Given: ___________
Tetaus Administered
Allergies___________ Significant Co-Morbidities ______
________________________________________________
________________________________________________
Smoker Occupation: _________________________
Clinical Assessment
Vascular Status
CRT ___________ Secs
Distal Pulses Clinically Palpable Doppler
Locations Present ________________________________
Post Splintage Re-check _______________________
SUSPECTED VASCULAR INJURY
Neurological Status
Sensory ________________________________________
Motor __________________________________________
Post Splintage Re-check __________________________
SUSPECTED NEUROLOGICAL INJURY
SUSPECTED COMPARTMENT SYNDROME
Specialist Referral
Orthopaedic Team
Name/Grade ____________________________________
Consultant ______________________________________
Time ____________ : ___________
Plastics Team
Name/Grade ____________________________________
Consultant ______________________________________
Time ____________ : ___________
Combined Orthoplastics Reconstructive Plan
Yes No Not recorded
Date of Injury ___________/___________/ ___________
Mechanism: HIGH ENERGY
________________________________________________
________________________________________________
________________________________________________
_______________________ Local ED Transfer From________________________________________________Limb involved: ___________________________________
Isolated Open Fracture: Yes No
Completed by: ________________ Grade ________ Date _______ / _______ / _______ Time: _______ : _______
NI Major Trauma Network | September 2018 17

Orthoplastic Open Fracture Pathway
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Orthoplastic Injury Initial Management
Debridement and Stabilisation within 24 hours: Yes No
Definitive Soft Tissue Coverage: Yes No
Procedure:
________________________________________________
________________________________________________
________________________________________________
Date: _____ / _____ / ______ Time: ______ : ______
Stabilisation: Temporary / Permanent
Grade of anaesthetist: ____________________________
Grade of Seniour Orthopaedic Surgeon: ____________
Grade of Senior Plastic Surgeon: __________________
Grade of Assisting Surgeons: _____________________
Location of Surgery: DGH / MTC / OPU
Gustillo-Anderson Classification: ___________(if appropriate)
Peri-operative Antibiotics:
Trust protocol / BAPRAS guidelines met:
Yes No
Agent: _________________________________________
Time: _____ : _____
Definitive Reconstructive Management
OPCS Code 1. Fracture _____________________________________2. Soft Tissue ___________________________________
Procedure:
________________________________________________
________________________________________________
_________________ Location: _____________________
Date: __________________________________________
Antibiotics Therapy: ______________________________
Time: ______ : ______
Grade of anaesthetist: ____________________________
Grade and Speciality of Surgeon: __________________
Second Surgeon: ________________________________
Supervising Surgeon Present:
Yes No Not recorded
AO Classification: _______________________________
Alternative Classification System: __________________
Return to Theatre: Yes No Not recorded
Indication: ______________________________________
Deep Tissue Samples:
Yes No Not recorded
Isolated Organism: ______________________________
Additional Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
Isolation Open Fracture: Yes No
Additional injuries:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
Injuries Requiring MTC treatment:
Head injury: ____________________________________
Spinal injury: ____________________________________
Thoracic injury: __________________________________
Pelvic injury: ____________________________________
NI Major Trauma Network | September 201818
Orthopaedic notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Orthopaedics have reviewed the patient and feel there is no further involvement and are signing off.We are happy to review patient on request
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 19

Orthopaedic notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201820

Cardiothoracic notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Cardiothoracic have reviewed the patient and feel there is no further involvement and are signing off.We are happy to review patient on request
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 21
Cardiothoracic notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201822

Burn assessment form
Referral: Acute Post-acute Reconst Rehab
Date: _____________ Time: ______________
T /F from: ______________ Via: NIAS Private
Seen by: ___________ Consultant _____________
Nature of Burn: Scale Oil Flame Flash Chemical Contact Electrical % TBSA: __________
Date of Burn: ______ / ______ / ______ Time of Burn ______ : ______
Predisposing Factors: Age Occupation Alcohol Social
Place of Burn: Indoors Outdoors Rescued by: ________________________________________________
First Aid given: _______________________________ Burn in percentage of total BSA: ____________ (see overleaf)
Additional injuries: ___________________________________________________________________________________
____________________________________________________________________________________________________
Pt Wt: __________ Kg Allergies: __________ Medication: __________ PMH: __________ Last meal: __________
Airway
C-Spine clear Yes NoSupraglottic inhal injury: Nose/Mouth Burn: Yes No Nose/Mouth soot: Yes NoStained sputum: Yes NoEpiglottic inhal injury: Hoarseness Yes No Stridor: Yes NoInfraglottic inhal injury: Go to breathing
Circulation
Attach 02 Pulse: ___________ BP: ___________ No. of IV lines: __________ Urinary catheter Yes No
Lymbs escharotomy: Yes No details: _______________________________ Go to fluids
Breathing
Attach 02 Normal chest expansion: Yes No Dyspnoea: Yes No Stridor: Yes No
Added breath sounds: Yes No Resp rate: CHest escharotomy Yes No
Disability
GCS: _______/15 Pupils normal Yes No
Exposure / environment Temp: __________ Clothes/jewellery off: Yes No Warmer: Yes No
Tetanus toxoid: Yes No Corneal injury: Yes No
Laryngoscopy: Direct Indirect by Dr: ________________ Findings: Uvula Epiglottis Cords Oedema
Intubation: Yes No by Dr: ___________________ Size of tube: ________ Position at teeth: __________cm
Investigations (order as required): Direct U+E Gp and hold ABG CoHb CXR
ECG Wound culture
Checklist: Direct IV fluids (see overleaf) Urinary catheter Warmer Tetanus cover Analgesia Antibiotics (one dose of flucloxacillin)
Dressing Theatre required: Yes No ICU required: Yes No Photograph: Yes No
Outcome and additional notes:
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 23

Burn assessment form Cont’d
Fluid Resuscitation Required: Yes No
% Total Body Surface Area (TBSA): ____________
Weight of patient: ___________ kg
Parkland Formula: %TBSA burn x weight in kg x 4mls of Hartmann’s solution (Normal saline in children)
(Half of total fluid requirement in first 8 hours from time of burn and half in following 16 hours)
Resuscitation started: Date: ______ / ______ / ______ Time: ______ : ______ Any bolus given: ___________mls
Maintenance fluid added: Yes No (children 24 hour requirements: 100mls/kg/15t 10kg, 50mls/kg/next 10kg,
20mls/kg/remainder body wt)
Urinary Catheter passed: Yes No Initial volume passed: ___________mls
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Region %
Head
Neck
Ant. Trunk
Post. Trunk
Right Arm
Left Arm
Buttocks
Genitalia
Right Leg
Left Leg
Ignore simple erythema
Superficial
Deep
Relative percentage of body surface area affected by age
Area Age
0 1 5 10 15 Adult
A = 1/2 of head 9 1/2 8 1/2 6 1/2 5 1/2 4 1/2 3 1/2
B = 1/2 of thight 2 3/4 3 1/4 4 4 1/2 4 1/2 4 3/4
C = 1/2 of one lower leg 2 1/2 2 1/2 2 3/4 3 3 1/4 3 1/2
Please ensure each page is completed in full
A
2
2 2
2
1½1½
A
2 2
1½1½
1
1
BR L L RB B B
C
1¾ 1¾ 1¾ 1¾
1½1½ 1½1½
13
C C C
A
2
2 2
2
1½1½
A
2 2
1½1½
1
1
BR L L RB B B
C
1¾ 1¾ 1¾ 1¾
1½1½ 1½1½
13
C C C
NI Major Trauma Network | September 201824
Burns/Plastics notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Burns/Plastics have reviewed the patient and feel there is no further involvement and are signing off.We are happy to review patient on request
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 25

Burns/Plastics notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201826

Specialty notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 27

Specialty notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201828
Miscellaneous notes
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 29

Miscellaneous notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201830

Results page
Results
Time
HB
WCC
PLTS
INR
PPT
APPT
NA
K
Urea
Crea
Gluc
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 31

Affix Arterial Blood Gas Here
Results page
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 201832

Radiology notes
Date:______________________ Time: _________________
Consultant:_______________________________________
Print name:______________________________________
Brain
Mass effect
Inta axial blood
Extra axial collection
___________________________________________________________
___________________________________________________________
___________________________________________________________
___________________________________________________________
Thorax
Large pneumothorax
Major vascular injury
Pericardial effusion
Pleural collection
Major lung insult
___________________________________________________________
___________________________________________________________
___________________________________________________________
___________________________________________________________
___________________________________________________________
Peritoneal cavity
Free fluid Free air Extravasation
Major abnormality
Liver Spleen Kidneys
Adrenals Pancreas Bowel
___________________________________________________________
___________________________________________________________
___________________________________________________________
___________________________________________________________
___________________________________________________________
Skeletal
Spinal alignment
Pelvic integrity
___________________________________________________________
___________________________________________________________
___________________________________________________________
Transfer Destination
Theatre
Trauma bed
Ward (state speciality)
Interventional Radiology
ED
___________________________________________________________
___________________________________________________________
___________________________________________________________
___________________________________________________________
___________________________________________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 33

Radiology notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201834

Trauma Team Debrief
1. Contact (team leader starts session)
2. State Event (state what just happened in the room)
3. Appreciation/Thanks (state gratitude to staff)
4. Gather thoughts and feelings (discuss emotions)
5. Support services (state support available)
6. Facilitate (organise if needed extra support for staff members)
Please ensure each page is completed in full
Georgia-May Swales 2015Head of Psychological Services Dr Sarah Meekin 9063 6608 Adult Psychological Service Miss Bridie McElhill 9056 6199
NI Major Trauma Network | September 2018 35

Trauma Team Debrief continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201836

Next day MDT Ward Round
Date:______________________ Time: _________________
Consultant:____________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 37

Next day MDT Ward Round continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201838

Prescribed Drugs
Drugs Dose Route Date Time Drs Given by Date Time
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 39

Prescribed Drugs continued
Drugs Dose Route Date Time Drs Given by Date Time
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 201840
Trauma Ward Notes
Date:______________________ Time: _________________
Consultant: ______________________________________
Print name: ______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Use addressograph - otherwise write in capitals
Surname: ________________________________________
First names: ______________________________________
DOB: ____________________________________________
Health and Care No. _______________________________
Sex: M F
Please ensure each page is completed in full
NI Major Trauma Network | September 2018 41

Please ensure each page is completed in full
Trauma Ward notes continued
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature: _________________________________________ Date: _________________________
Please ensure each page is completed in full
NI Major Trauma Network | September 201842

URGENT TRAUMA TRANSFER FORM
PATIENT DETAILS
Name:
HRC No:
DOB:
NOK Details:
TRANSFER DETAILS
Receiving
Hospital: HDU/ICU
Xray Theatre
Ward ED
STAFF ACCEPTING PATIENT
Name:
Position:
Receiving Location Contact No:
REASON FOR TRANSFER
Ongoing assessment Imaging Surgery Critical Care
BACKGROUND
Allergies: No Yes
Meds Given:
Tetanus
Infection Status: No Yes
RELEVANT PMH & MEDICATIONS
Anticoagulation: No Yes
INVESTIGATIONS
Imaging on Bloods on ECRPACS
WBCT _______________
CXR ________________
WORKING DIAGNOSIS
1.
2.
3.
4.
STATUS PRE-TRANSFER
[A] FM Grade:
Trache/Cric I III
ETT II IV
Tube size/length:
[B] Chest Drain Unclamped
Yes ABG Pre-transfer
No
[C] ECG O2 sats
NIBP ETCO2
PIVC x 2
CVC Yes No
Art Yes No
Inotroples Yes No
[D] (Pre-intubation) (Pre-Transfer)
Pupils R L GCS M
size E
V
If Ventilated TV PIP
PEEP Type Ventilator
ESCORT
Dr Nurse Paramedic
Name:
Reg No:
Position:
Signature:
Time Departure Time Arrival
DETAILS TRANSFER
Clinical
Equipment
Organised
____15
____15
____4
Social Care Board
NI Major Trauma Network | September 2018 43

250
240
230
220
210
200
190
180
170
160
150
140
130
120
110
90
80
70
60
50
40
30
SpO2
Fi O2
ETCO2
Drugs
Fluids
Time (24hrs)
40˙C
32˙C
BP
HR
•
READY TO GO!
Patient
Airway safe
TXA
ETT secured
Established ventilator
ABG pre transfer
HR, BP stable
No obvious blood loss
IV access
Cervical spine protected
No pneumothorax
Fractures stabilised
Secured to trolley
Wrapped to prevent heat loss
Lines secure
Staff
Handover appropriate
Money
Phone
Equipment
Transfer bag complete
Fluids
Drugs
Bag Valve Mask
Sufficien O2 supply
Suction
Organisation
Trauma documentation
Other medical notes
NOK aware
Receiving unit aware pre departure
NI Major Trauma Network | September 201844