MAJOR DEPRESSION IN CHILDREN - University of Cape Town · DEPRESSION in Children and Adolescents Dr...
48
DEPRESSION in Children and Adolescents Dr Wendy Vogel. Child & Adolescent Psychiatrist, Division of Child and Adolescent Psychiatry, Red Cross War Memorial Children’s Hospital and University of Cape Town. 1
Transcript of MAJOR DEPRESSION IN CHILDREN - University of Cape Town · DEPRESSION in Children and Adolescents Dr...

DEPRESSION
in Children and Adolescents Dr Wendy Vogel. Child & Adolescent Psychiatrist,
Division of Child and Adolescent Psychiatry,
Red Cross War Memorial Children’s Hospital and University of Cape Town.
1

DEPRESSION
“Depressive disorders are often familial
recurrent illnesses associated with
increased psychosocial morbidity and
mortality. Early identification and
treatment may reduce the
impact…Evidence supported treatment
interventions have emerged…” J.Am Acad of Child adolesc. Psychiatry 46:11 Nov 2007
Depression refers to MDD and Dysthymia
2

EPIDEMIOLOGY
1-2 % in children (aged 6-12 years)
2-5% in adolescents (aged 13-18 years)
during childhood m:f ratio 1:1
during adolescence m:f ratio 1:2
3

Environmental factors
Family conflict
Bullying
Abuse
Poor support
Increased evidence of stressful life event in 12 months prior to onset
Death of a caregiver
Divorce
Birth of a sibling
4

Environmental factors
Acquired physical illness or injury
Developmental challenges
Co-morbidity (anxiety,ADHD,ASD)
Medical conditions
NOTE: The effect of these stressors also
depends on the child’s negative
attributional styles for interpreting and
coping with stress, support and genetic
factors
5

CLINICAL PRESENTATION:
2/52 changed mood
Depressed/irritable
Loss of interest
Changes in appetite
Weight changes
Sleep changes
Activity levels change
Concentration decreases
Energy level changes
Self-esteem is low
Motivation poor
6

CLINICAL PRESENTATION:
Wishing to be dead
Suicidal attempts or ideation
Exaggerated guilt
Feeling hopeless
Clinical picture similar to adults but
differences attributed to child’s physical,
emotional, cognitive and social development
Dysthymia: chronic condition lasting for a year
7

Clinical features: pre-school
under 6 years
Apathy
Food refusal
Miserable
Crying
Rocking
8

Clinical features: middle school
6-12 years
Somatization
Low self- worth
Poor school
performance
Anxiety
Irritable, Bored,
Sad,
Angry
Sleep & Appetite
changes
A.D.H.D-like
Apathy
Withdrawn
Temper outbursts
9

Clinical features:
adolescents Melancholia
Conduct problems
Suicide attempts
Functional impairments
Atypical presentation
10

CO-MORBIDITY
40 – 90% have other psychiatric disorders
20 – 50% have two or more co-morbidities
Dysthymia: 30-80%
ASD
Anxiety: 30-80%
Disruptive Disorders: 10 – 80%
Substance Use disorders: (20-30%)
These may predate MDD
Risk of early pregnancy
11

DEPRESSED CHILDREN
MULTIPLE PROBLEMS
Educational failure
Impaired psychosocial function
Co-morbid disorders
High family psychopathology
Risk of suicide (hx of attempts, co-morbid
conditions, impulsivity and aggression, lethal weapons,
exposure to negative events)
12

ASSESSMENT:
• Interview parents & child & family
• Collateral (school, others)
• Psychiatric interview with M.S.E.
• Physical exam: (TFT)
• Review medical & psychiatric hx
• Family medical & psychiatric hx
• Rating scales
• Psychological assessment
• Assess severity and impairment
• Assess safety (and safety plan)
• Assess required level of care
13

CONSIDER:
Potential co-morbidities
Social, educational and family context
Quality of relationships
Social network for positive or negative impact
Always ask about substance use, bullying, abuse, self harm, suicidal
ideation
Opportunity for privacy/confidentiality
Consider cultural and family values
Consent
Child protection
Consider the parents’ mental health
14

TREATMENT:
Therapeutic Alliance/rapport/confidentiality
Psycho-education. Give written information.
Give advice about self help groups , leaflets
Evidence based research on Rx is sparse
Treat co-morbid diagnosis, social & educational problems, NB bullying
Offer CBT , IPT or short-term family Rx
Consider parents’ psychopathology and refer
Use CDI or MFQ to monitor progress
15

16
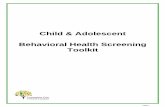
Mood and Feelings Questionnaire--
1. I felt awful or unhappy.
2. I didn't enjoy anything at all.
3. I was less hungry than usual.
4. I ate more than usual.
5. I felt too tired I just sat around and did nothing.
6. I was moving and walking more slowly than usual
7. I was very restless.
8. I felt I was no good anymore.
9. I blamed myself for things that weren't my fault.
10. It was hard for me to make up my mind.
11. I felt grumpy and upset with my parents.

TREATMENT
Medication plus psychotherapy is best
combination (although mixed evidence)
AACAP vs NICE guidelines
Opinion is divided as to whether to start
with psychotherapy first
Mild depression may respond to
supportive psychotherapy only. Period of
watchful waiting. Discuss lifestyle
17

TREATMENT
TADS Study (March et al Arch Gen Psych Vol 64 (No 10) Oct 2007)
(March & Vitiello Am J Psychiatry 166: Oct 2009)
ADAPT Study (Goodyer et al, Health Technol Assess 2008;12 1-60)
TORDIA Study (Brent et al, JAMA 2008;299(8):901-913)
NICE GUIDELINES/AACAP Practice
parameters
18

TADS STUDY
TADS matters : mod to severe range of illness
Combined treatment (CBT plus fluoxetine) significantly accelerates benefits (at 12 weeks)
Treating patients longer makes a big difference in medical benefits (at 36 weeks)
Need 6-9 months treatment
Adding CBT to Fluoxetine minimises suicidal ideation and Rx emergent suicidal events
19

TADS STUDY
Longer term treatment provides
sustained benefit once treatment is
discontinued
Combined treatment is cost effective in
the long run
20

ADAPT Study
Brief (2 week) psycho educational
intervention may be effective in a
proportion of pts with moderate to
severe depression
SSRI (Fluoxetine) together with active
clinical care (ACC) is treatment of choice
if non responsive
21

ADAPT Study
For non responsive adolescents, the
addition of CBT to Fluoxetine plus active
clinical care
does not improve outcome or confer
protective effects against adverse events.
SSRIs ( fluoxetine) are not likely to result
in harmful effects
After 7 months of active Rx 10% will
have no response ie Rx resistent
22

ADAPT Study
No evidence of protective effect of CBT
on suicidality
Fluoxetine plus Active clinical care is
important not fluoxetine alone
How did TADS respond?
ADAPT : sicker pts, ACC good, CBT not.
23

TORDIA STUDY
• MDD non responsive after 2 months on an SSRI were switched to a second DIFFERENT SSRI, or venlafaxine or either arm plus CBT.
• Combination medication plus CBT was superior.
• No difference between second SSRI and venlafaxine except for CVS side effects so they recommended changing to second SSRI and CBT
24

25
SIDE EFFECTS
Common side effects:
Headaches
GI/Stomachaches/nausea
diarrhea
Sedation/insomnia
Sweating
Sexual side effects
Tremor
Diastolic hypertension
Uncommon side effects:
Activation
Bipolar switching
Suicidality
Serotonin syndrome
Bleeding

NICE GUIDELINES/AACAP
MILD DEPRESSION
PSYCHO-EDUCATION: written and web
• 2 week period of watchful waiting (up to 4/52)
• If continues with no suicidal ideation or co-morbidity offer psychological therapies for 2-3 months
Individual supportive psychotherapy
Group CBT
Guided self help
Family involvement //+- role of school
DONOT use anti depressants
26

NICE GUIDELINES/AACAP
MODERATE TO SEVERE DEPRESSION
CBT/IPT/Family Therapy for ? 3 months
If no response look at additional factors (family discord
etc)
MEDICATION
Fluoxetine for 12 to 18 year olds
Cautiously consider Fluoxetine for 5-11 year olds
(evidence not established)
Start low and go slow
Adequate doses for long periods
If unresponsive, family Rx or individual Rx (30)
27

INFORMANT
ALWAYS check outcomes with child and
adolescent
Family /caregiver feedback
School feedback
NB CONFIDENTIALITY ISSUES
Note most studies are with
adolescents..very few with children..so
adapt CBT/IPT/psychodynamic and family
Rx
28

ABC of CBT
Affect identification and regulation
Behaviour activation
Cognitive restructuring
29

AFFECT IDENTIFICATION
Psychoeducation about feelings and
depression
Co-existing feelings
Linking feelings to events
Hierarchy of feelings/ events
Mood thermometer
Triggers for strong negative affect
Patterns for reacting to negative affect
30

AFFECT REGULATION TOOLS
Relaxation exercises
Take a deep breath
Time out Chill
Distraction
Talk about feelings
Diary
Ask for help
Imagery
31

Behaviour activation
Pleasant activity scheduling
In vivo exercises ( using imagery)
Pre and post mood check
Positive self talk
Externalise distressing thoughts
Concretise the relationship between thoughts and mood
Thinking outside the box
32

33
IMAGERY

INTERPERSONAL THERAPY (IPT)
IPT is a brief time limited Rx based on the premise that depression occurs in the context of relationships regardless of origins in biology or genetics. The IPT model identifies 4 areas of relationship difficulties:
Grief
Conflict in significant relationships
Difficulties adapting to changes in relationships or life circumstances
Difficulties from social isolation
12-16 week treatment
34

PSYCHODYNAMIC
PSYCHOTHERAPY
Case based literature and clinical experience suggesting that psychodynamic therapy can address a broad range of co-morbidities..need more rigorous studies
Most cases in clinical practice have multiple factors requiring multi-modal treatment approach with a combination of CBT,IPT, individual psychodynamic, family therapy, school interventions and medication.
35

PHASES OF Rx
Acute: Rx if no response to active monitoring for 6 to 12 weeks aim for remission
Continuation: All who have responded to Rx, continue Rx for 6 to 9 months aim to consolidate remission & prevent relapse
Maintenance: YP who are at high risk of recurrence (family hx MDD, multiple episodes, severe and complicated MDD) for 1- 2 years; aim to prevent recurrence.
36

TIDY project
Consider stressors
Consider seeing the young person alone
Ask the transitional question
General psychiatric screening questions
Screen for depression (ask core
symptoms)
To diagnose depression
Impairment
37

TIDY PROJECT
TREATING DEPRESSION After making a diagnosis
Give feedback
Name it
Describe it ie link symptoms
Link to known stressors
Give information about depression
Give leaflet
38

TIDY PROJECT
TREATING DEPRESSION • Promote coping strategies
• Mobilise help
• Identify confidante
• Activity scheduling with self re-enforcement
• Give positive re-enforcement
• Reminder: It is usually self-limiting
• Invite back
• Need for referral
39

CHALLENGES
Time
Lack of therapists
Self train
Nurse practitioners
School support staff
40

DEPRESSED PARENTS
Role of depressed mother
• PND has negative effect on caregiving
which affected language development
(greater risk in lower se groups)
Role of depressed father
• Children whose fathers were chronically
depressed were at greater risk of
emotional & behavioural problems • Alan Stein
41

SELF HELP GROUPS
South African Depression and Anxiety
Group
Gardens: 0824441952
Athlone:0798149634
BOOKS
42

DCAP REFERRAL
All children under 13 years:
All adolescents over 13 years:
Non responsive to Rx
Actively suicidal with recurrent risk
Manic episodes
Psychosis
SAD
Family hx of BMD/Psychosis
Co-morbid psychiatric conditions
Side effects ( agitation/suicidality) from SSRI
43

DCAP REFERRAL
Division of Child and Adolescent Psychiatry
Red Cross War Memorial Children’s Hospital &
UCT
Referral form
46 Sawkins Road, Rondebosch 7700
Tel. (021) 685 4103 Fax (021) 685 4107
Tel. (021) 685 5116 Fax (021) 689 1343
44

Where is further information available?
NICE guideline:
◦ www.nice.org.uk/cg028niceguideline Information for the public
◦ www.nice.org.uk/cg028publicinfo
◦ Practice Parameters for the Assessment and
treatment of Children and Adolescents with
Depressive Disorders. J.Am.Acad. Child and
Adolesc. Psychiatry 46:11 Nov 2007.S
45
33

THANK YOU for your attention!
46

CASE STUDY:
6 year old boy
Catatonic
Depressed mood
Children’s Home
Mother in jail
47

CASE STUDY:
9 year old boy
Referred for ADHD
Irritable ,disruptive in class
Poor sleeper
Apathy and lethargic
FAMILY HISTORY
48