Maintaining function in persons with chronic disabilities ... · Parkinson’s dis., CNS...
55
Maintaining function in persons with chronic disabilities by adapted physical activity programs Francesco Benvenuti Dipartimento Territorio Fragilità AUSL11 Empoli Società della Salute Valdarno Inferiore Giornata CPPS di messa in rete Promozione della salute e prevenzione nelle persone anziane: quali sfide per i Cantoni Latini? Castello Sasso Corbaro 7 febbraio 2014
-
Upload
nguyenkhanh -
Category
Documents
-
view
214 -
download
0
Transcript of Maintaining function in persons with chronic disabilities ... · Parkinson’s dis., CNS...
Maintaining function in persons with
chronic disabilities by adapted
physical activity programs
Francesco Benvenuti
Dipartimento Territorio Fragilità
AUSL11 Empoli
Società della Salute Valdarno Inferiore
Giornata CPPS di messa in rete
Promozione della salute e prevenzione
nelle persone anziane:
quali sfide per i Cantoni Latini?
Castello Sasso Corbaro
7 febbraio 2014
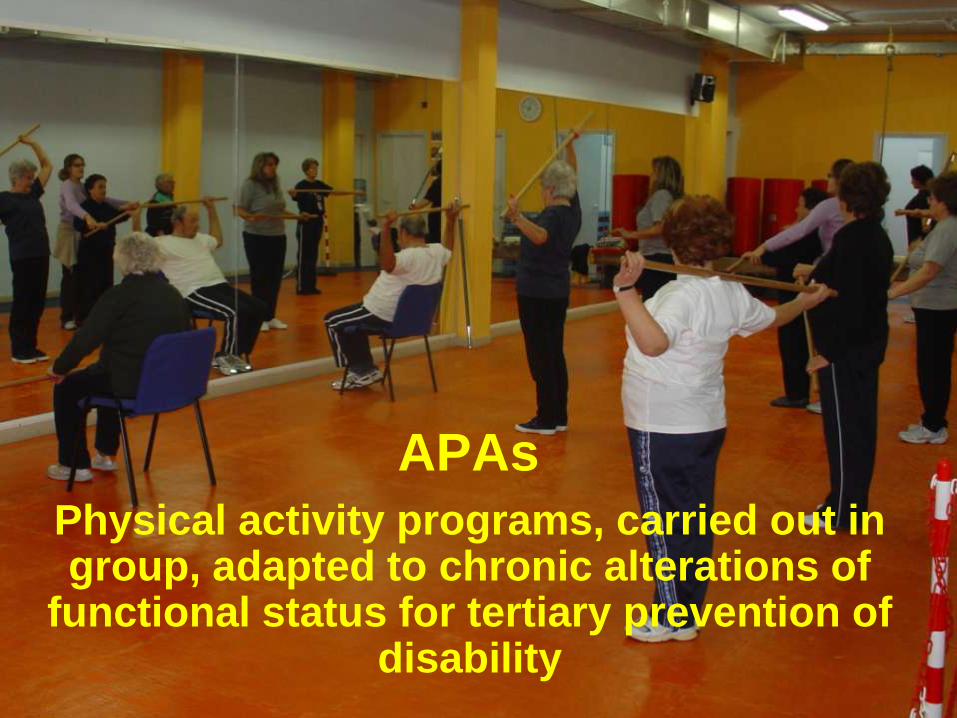
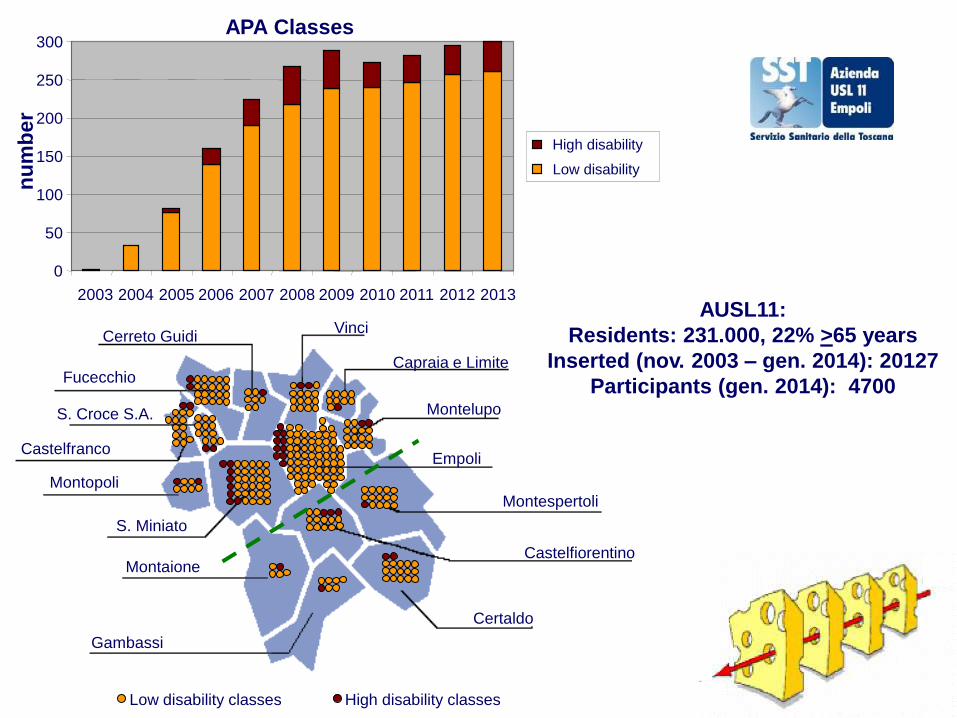
APAs
Physical activity programs, carried out in group, adapted to chronic alterations of
functional status for tertiary prevention of disability
Fucecchio
S. Croce S.A.
Castelfranco
Montopoli
S. Miniato
Gambassi
Montaione
Montelupo
Empoli
Montespertoli
Certaldo
Capraia e Limite
Cerreto Guidi Vinci
Castelfiorentino
Low disability classes High disability classes
AUSL11:
Residents: 231.000, 22% >65 years
Inserted (nov. 2003 – gen. 2014): 20127
Participants (gen. 2014): 4700
0
50
100
150
200
250
300
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
High disability
Low disability
APA Classes n
um
ber
USL1
0
50
100
150
200
250
300
2008 2009 2010 2011 2012N
UM
ER
O
USL2
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL3
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL4
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL5
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL6
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL7
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL8
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL9
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL10
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL11
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
USL12
0
50
100
150
200
250
300
2008 2009 2010 2011 2012
NU
ME
RO
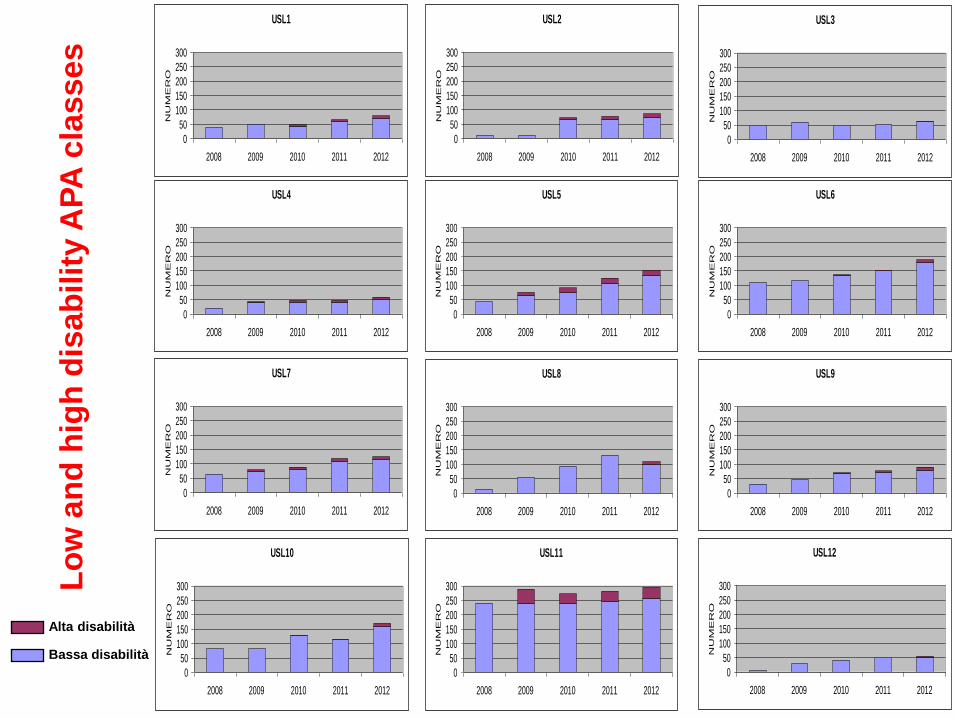
Lo
w a
nd
hig
h d
isa
bil
ity A
PA
cla
sse
s
Alta disabilità
Bassa disabilità
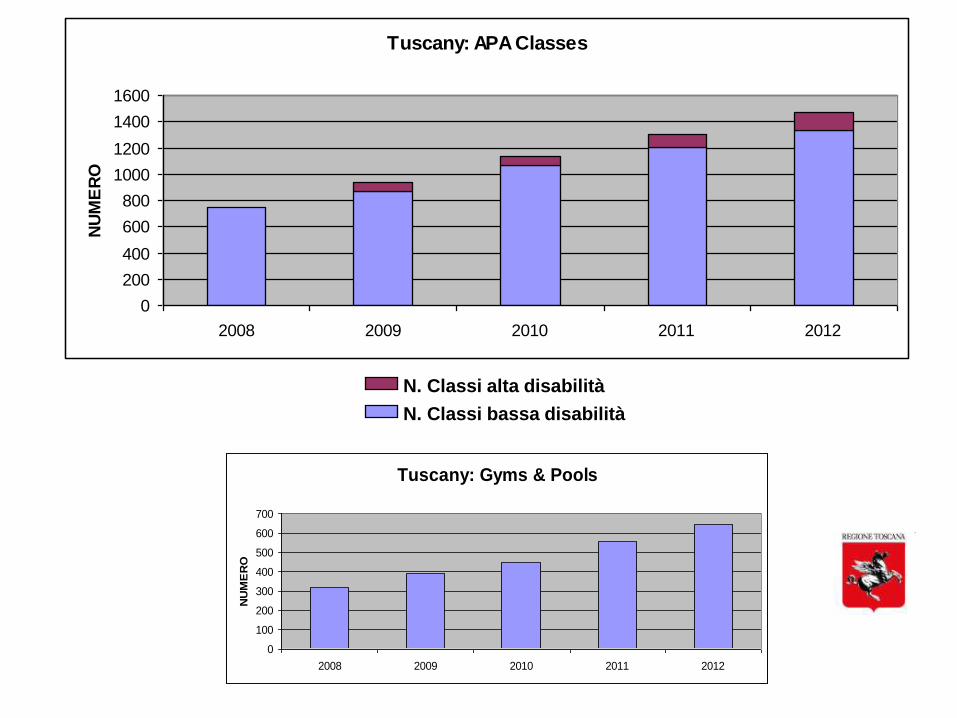
Tuscany: APA Classes
0
200
400
600
800
1000
1200
1400
1600
2008 2009 2010 2011 2012
NU
ME
RO
N. Classi alta disabilità
N. Classi bassa disabilità
Tuscany: Gyms & Pools
0
100
200
300
400
500
600
700
2008 2009 2010 2011 2012
NU
ME
RO
Implementation of physical activity
for persons with chronic disabilities
Policy steps
• Bridge theory and practice by creating exercise
opportunities (APA classes)
• Remove barriers
• Promote an organization for easy and safe
access to APA classes
• Promote collaborative environment
Implementation of physical activity
for persons with chronic disabilities
Policy steps
• Bridge theory and practice by creating
exercise opportunities (APA classes)
• Remove barriers
• Promote an organization for easy and safe
access to APA classes
• Promote collaborative environment
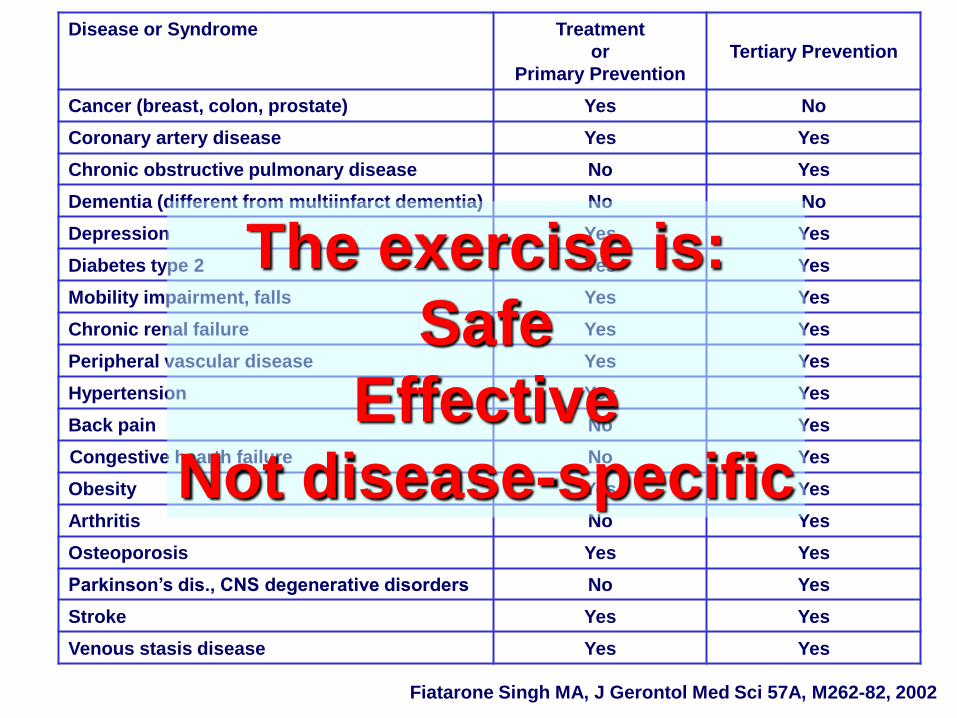
Disease or Syndrome Treatment
or
Primary Prevention
Tertiary Prevention
Cancer (breast, colon, prostate) Yes No
Coronary artery disease Yes Yes
Chronic obstructive pulmonary disease No Yes
Dementia (different from multiinfarct dementia) No No
Depression Yes Yes
Diabetes type 2 Yes Yes
Mobility impairment, falls Yes Yes
Chronic renal failure Yes Yes
Peripheral vascular disease Yes Yes
Hypertension Yes Yes
Back pain No Yes
Congestive hearth failure No Yes
Obesity Yes Yes
Arthritis No Yes
Osteoporosis Yes Yes
Parkinson’s dis., CNS degenerative disorders No Yes
Stroke Yes Yes
Venous stasis disease Yes Yes
Fiatarone Singh MA, J Gerontol Med Sci 57A, M262-82, 2002
The exercise is:
Safe
Effective
Not disease-specific
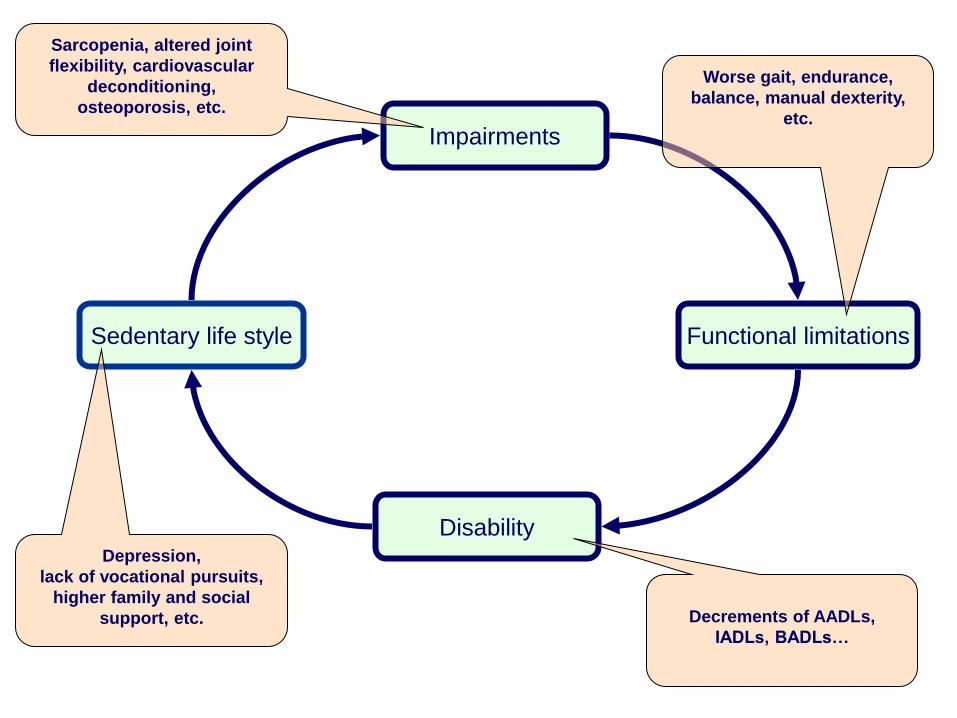
Impairments
Functional limitations
Disability
Sedentary life style
Depression,
lack of vocational pursuits,
higher family and social
support, etc.
Sarcopenia, altered joint
flexibility, cardiovascular
deconditioning,
osteoporosis, etc.
Worse gait, endurance,
balance, manual dexterity,
etc.
Decrements of AADLs,
IADLs, BADLs…

Independent
Disable
Sedentary life style
Impairments
Functional limitations
Disability
Chronic diseases converge towards common pathways!!
\
Moderate Hypomobility
Severe Hypomobility
Mild Hypomobility
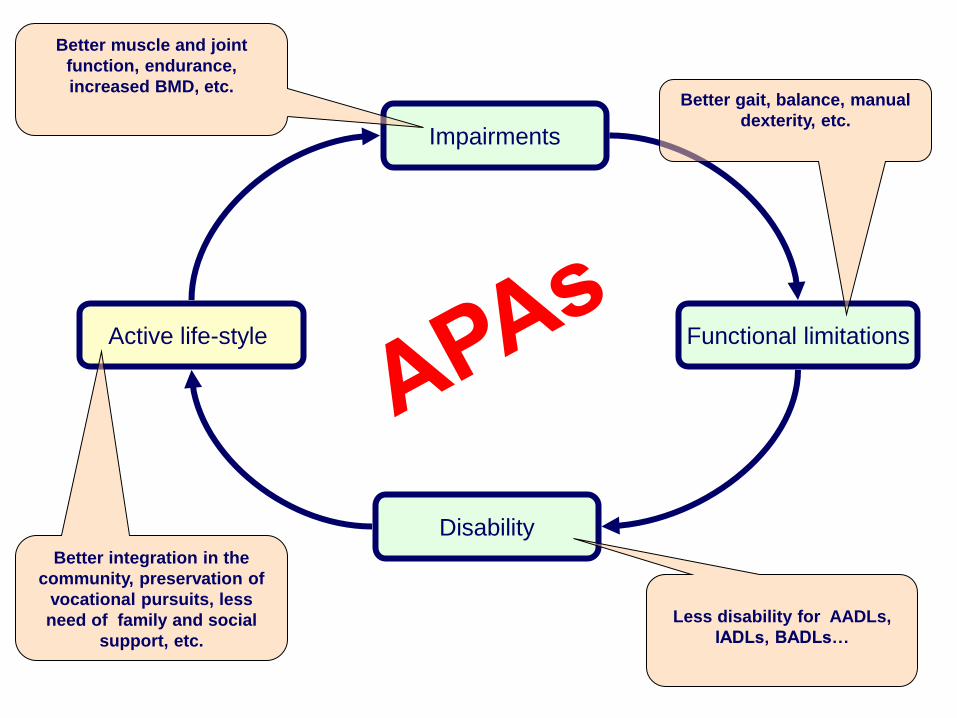
Impairments
Functional limitations
Disability
Active life-style
Better integration in the
community, preservation of
vocational pursuits, less
need of family and social
support, etc.
Better muscle and joint
function, endurance,
increased BMD, etc. Better gait, balance, manual
dexterity, etc.
Less disability for AADLs,
IADLs, BADLs…
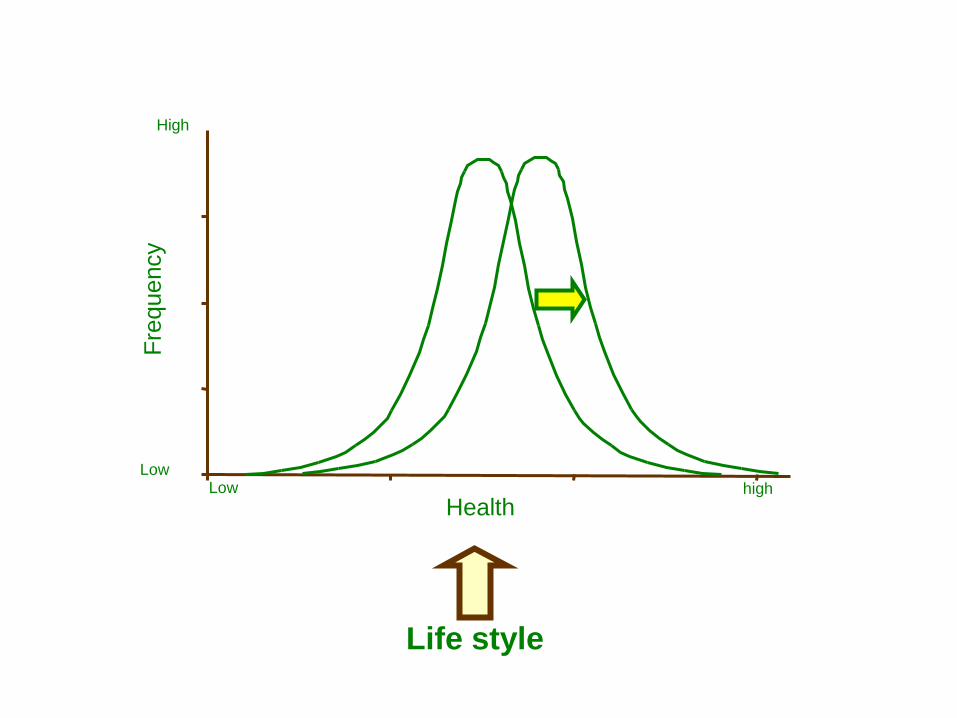
Life style
Fre
quency
Health Low high
Low
High
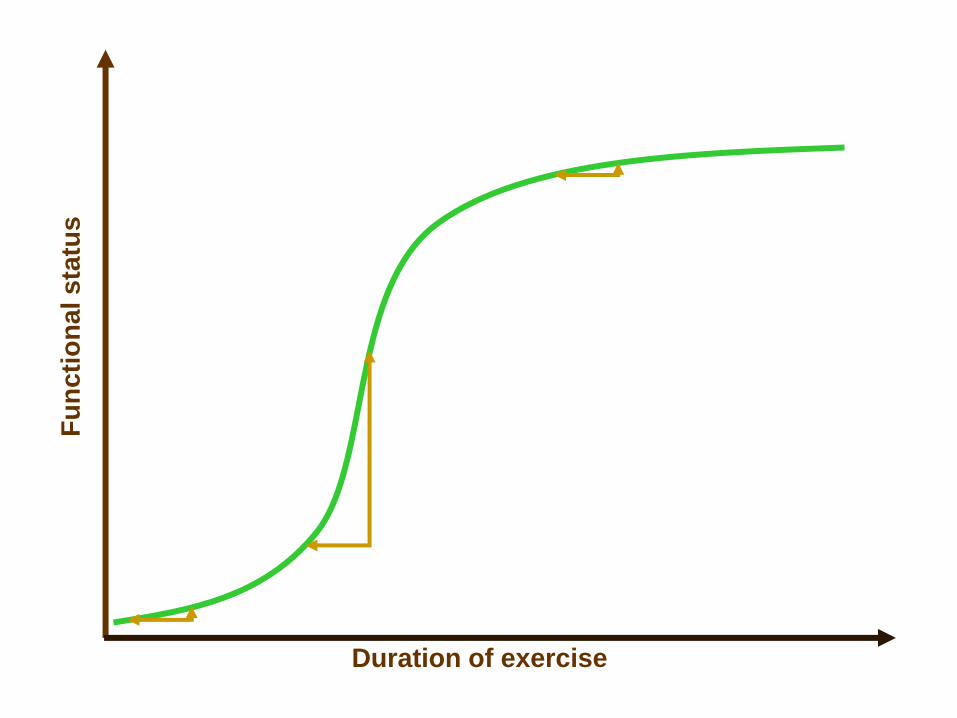
Fu
nc
tio
na
l s
tatu
s
Duration of exercise

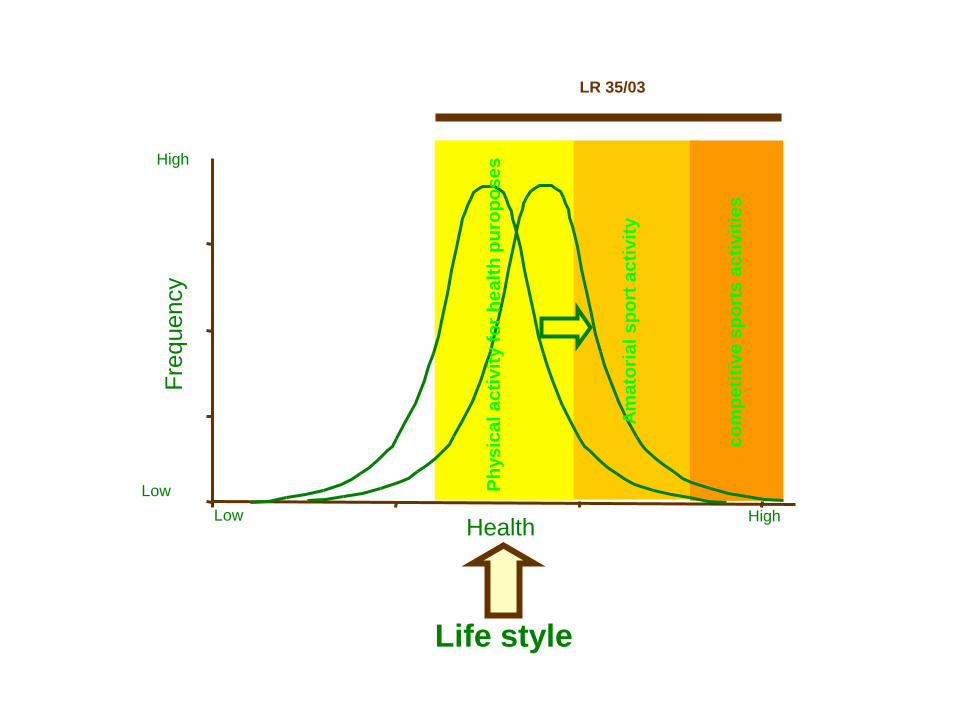
Life style
Fre
quency
Health Low High
Low
High
Ph
ys
ica
l a
cti
vit
y f
or
he
alt
h p
uro
po
se
s
LR 35/03
Am
ato
ria
l s
po
rt a
cti
vit
y
co
mp
eti
tive
sp
ort
s a
cti
vit
ies
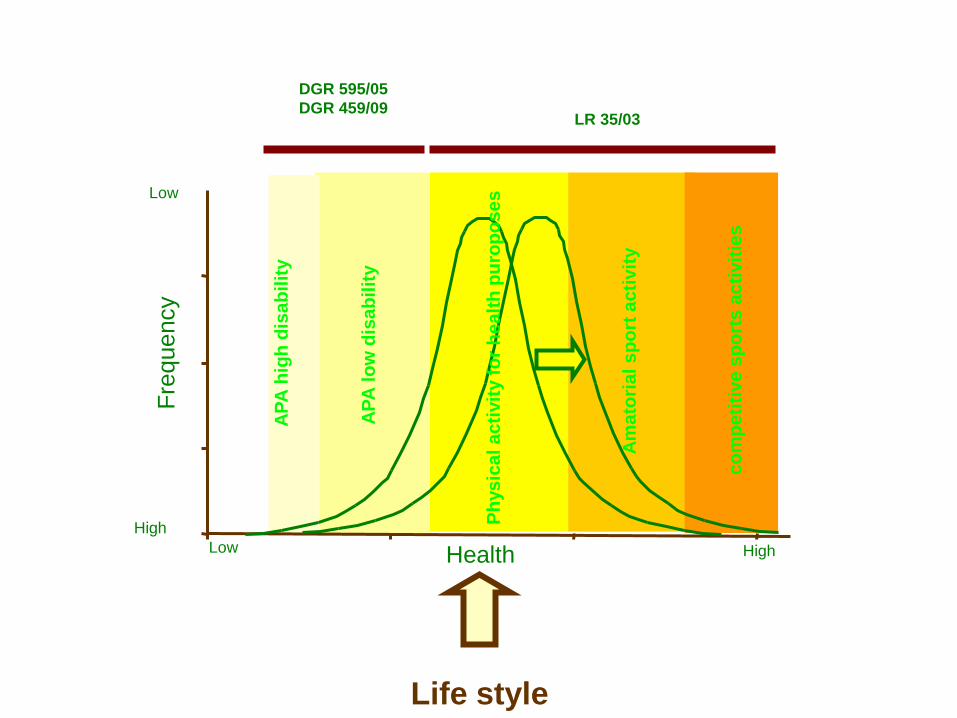
Life style
Fre
quency
Health Low High
High
Low
AP
A h
igh
dis
ab
ilit
y
Ph
ys
ica
l a
cti
vit
y f
or
he
alt
h p
uro
po
se
s
LR 35/03
DGR 595/05
DGR 459/09
AP
A l
ow
dis
ab
ilit
y
Am
ato
ria
l s
po
rt a
cti
vit
y
co
mp
eti
tive
sp
ort
s a
cti
vit
ies
Implementation of physical activity
for persons with chronic disabilities
Policy steps
• Bridge theory and practice by creating exercise
opportunities (APA classes)
• Remove barriers
• Promote an organization for easy and safe
access to APA classes
• Promote collaborative environment
Medical clearance (certification) for low intensity
leisure physical activity programs: - Useless
- Expensive
- Schizophrenic
Remove alibi (for citizens and clinicians): - follow EBM
- redirect inappropriate rehab programs to APA
FOR HYPOMOBILITY SYNDROMES AND
OSTEOPOROSIS AND CHRONIC SYNDROMES
WITH STABILIZED OUTCOMES APA
PROGRAMS ARE APPROPRIATE…..
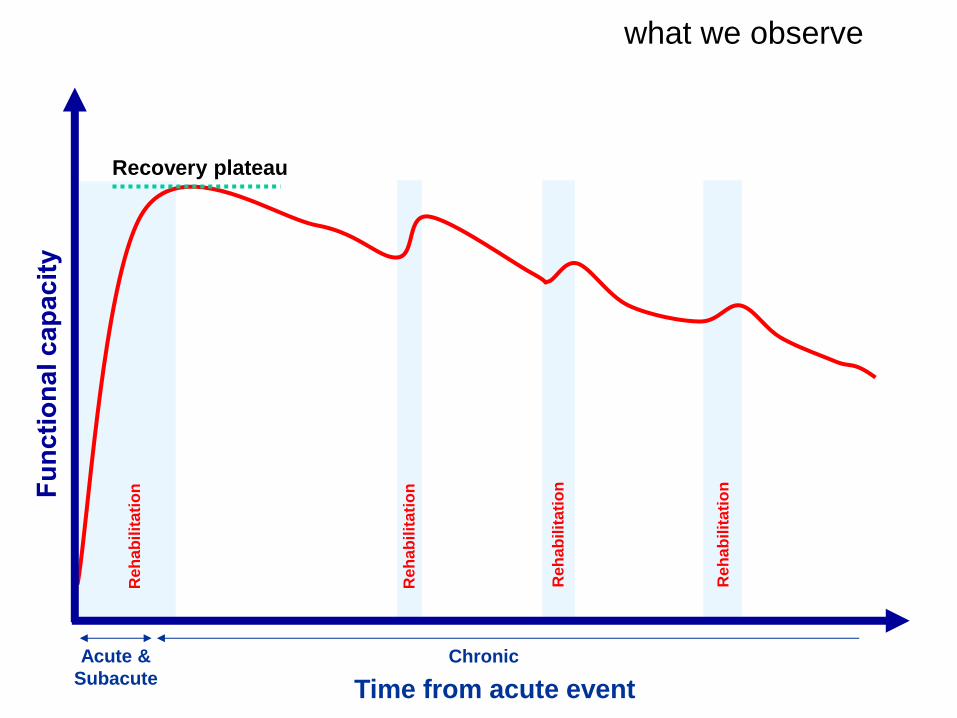
Recovery plateau
what we observe
Reh
ab
ilit
ati
on
Reh
ab
ilit
ati
on
Re
ha
bil
ita
tio
n
Reh
ab
ilit
ati
on
Time from acute event
Acute &
Subacute
Chronic
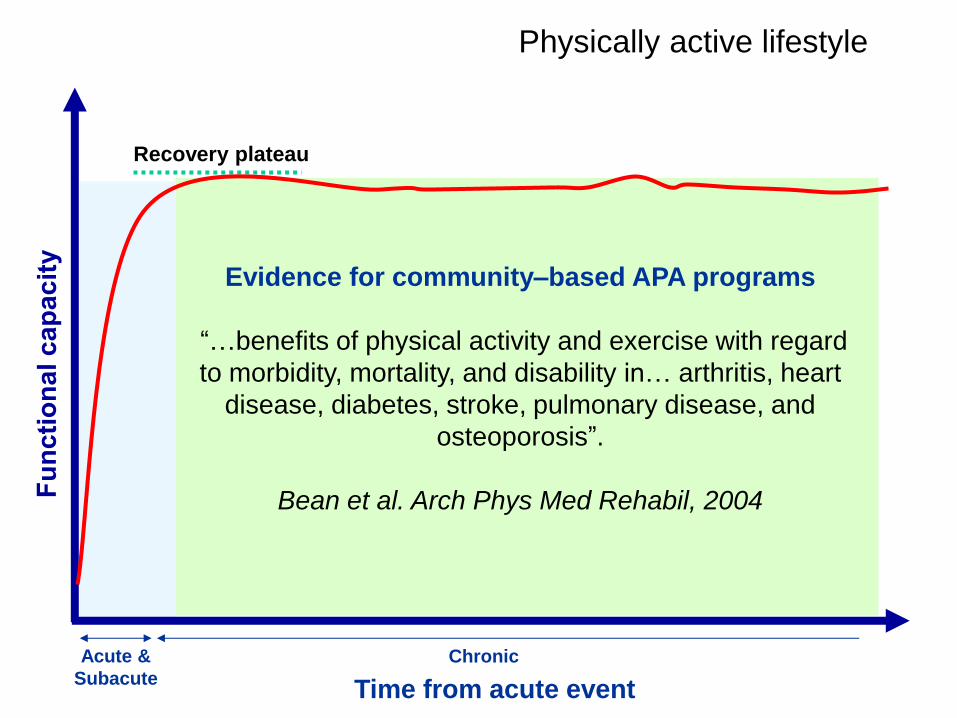
Physically active lifestyle
Recovery plateau
Time from acute event
Acute &
Subacute
Chronic
Evidence for community–based APA programs
“…benefits of physical activity and exercise with regard
to morbidity, mortality, and disability in… arthritis, heart
disease, diabetes, stroke, pulmonary disease, and
osteoporosis”.
Bean et al. Arch Phys Med Rehabil, 2004
Implementation of physical activity
for persons with chronic disabilities
Policy steps
• Bridge theory and practice by creating exercise
opportunities (APA classes)
• Remove barriers
• Promote an organization for easy and safe
access to APA classes
• Promote collaborative environment
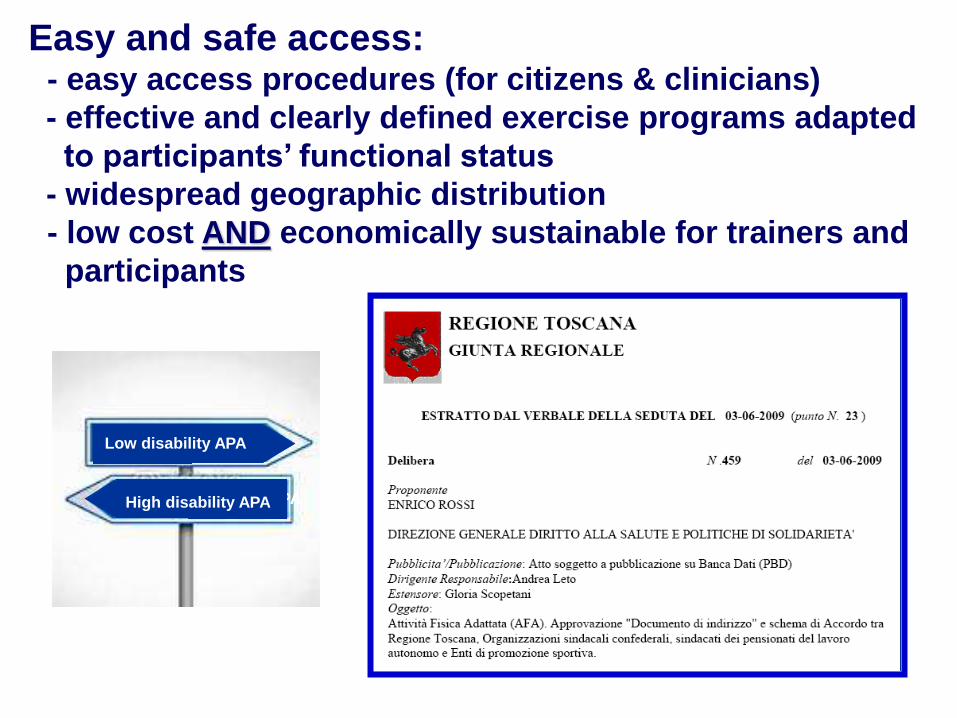
Easy and safe access: - easy access procedures (for citizens & clinicians)
- effective and clearly defined exercise programs adapted
to participants’ functional status
- widespread geographic distribution
- low cost AND economically sustainable for trainers and
participants
High disability APA
Low disability APA
High disability APA
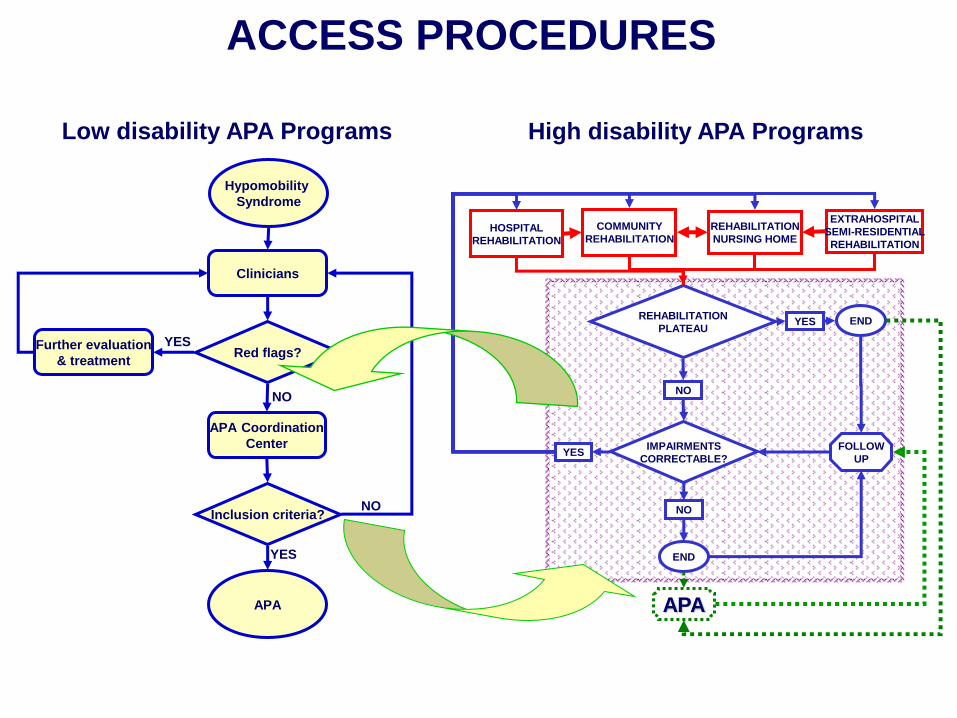
Hypomobility
Syndrome
Clinicians
Red flags? Further evaluation
& treatment
APA Coordination
Center
Inclusion criteria?
APA
YES
NO
YES
NO
REHABILITATION
PLATEAU
IMPAIRMENTS
CORRECTABLE?
HOSPITAL
REHABILITATION
COMMUNITY
REHABILITATION
REHABILITATION
NURSING HOME
EXTRAHOSPITAL
SEMI-RESIDENTIAL
REHABILITATION
YES
NO
END
NO
YES
END
APA
FOLLOW
UP
Low disability APA Programs High disability APA Programs
ACCESS PROCEDURES
Master Libri
Via Morgagni, 39/R
50134 Firenze
tel. 055/4368577
fax 055/4249446
www.usl11.toscana.it
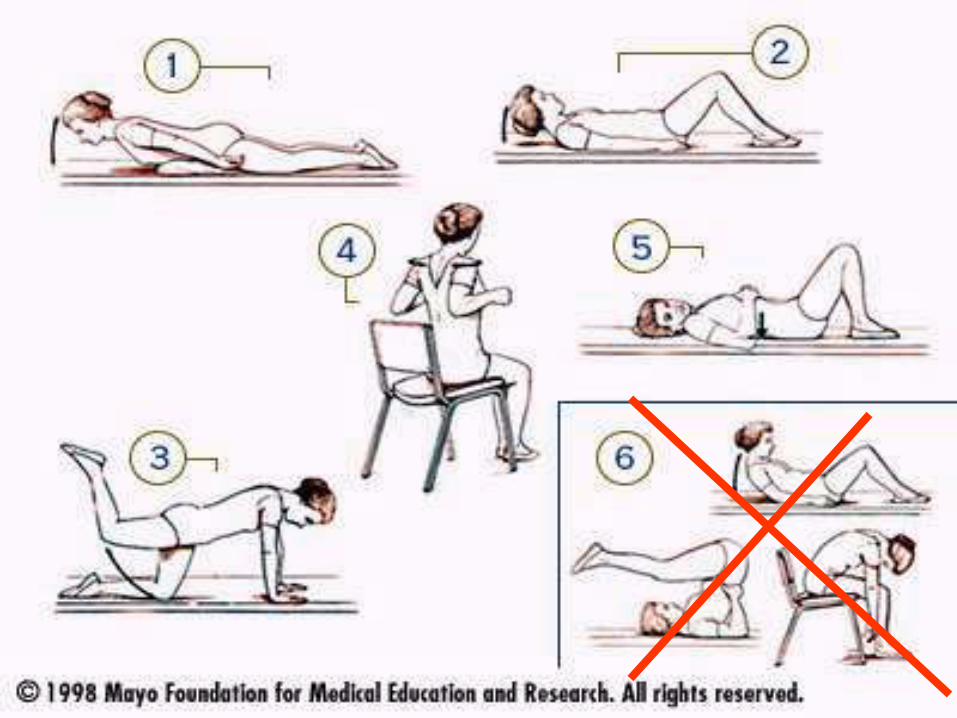
EXERCISE PROGRAM
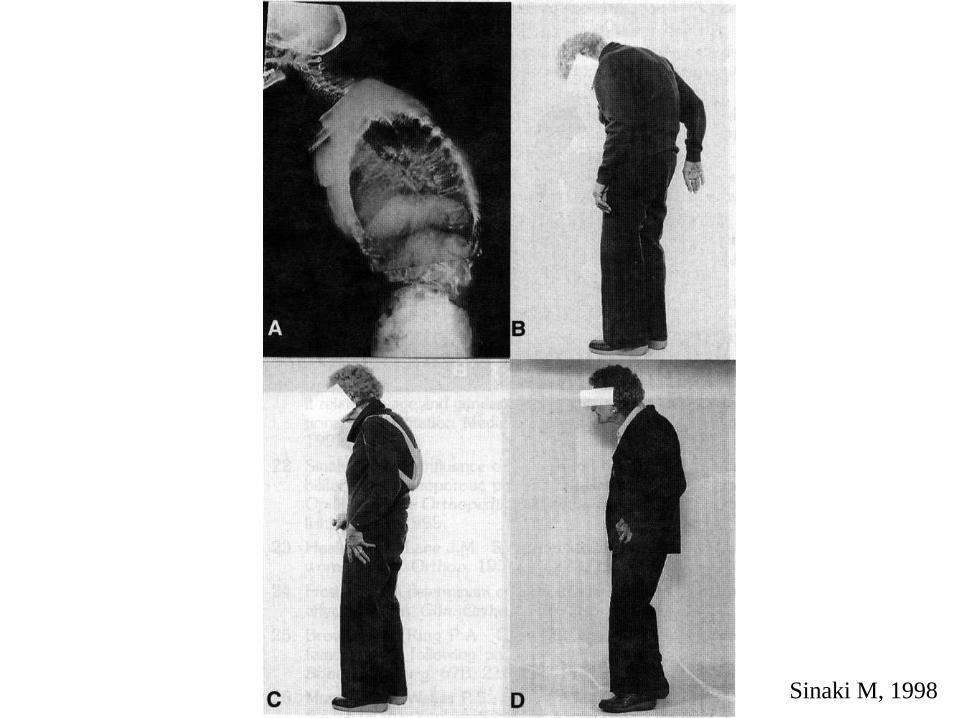
Sinaki M, 1998
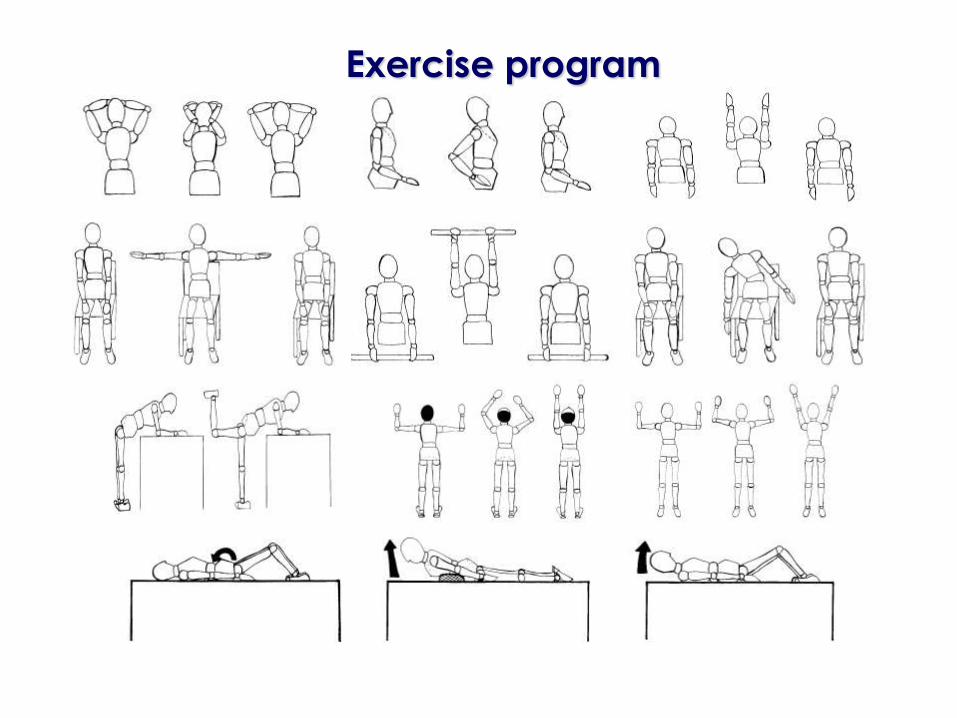
Exercise program
A&E Service contacts Fracture 5° finger left hand (2004)
*Fracture left right humerus (2005)
Fratture right wrist (2006)
Head injury (2008)
*Head injury (2010)
*Fracture D12 (2011)
*Accidents occurred during APA classes
Gym inspections
Telephone interviews
SAFETY CONTROL
40 organizations; 84 gyms/pools
Median Home-gym distance 1.1 km
GEOGRAPHIC DISTRIBUTION
≈2.20 € for 1 hour session
27 € per month for classes 3 times/week
20 € per month for classes 2 times/week
10 € / year for insurance
( ) + = 2.30 €
LOW COST AND SUSTAINABLE
Implementation of physical activity
for persons with chronic disabilities
Policy steps
• Bridge theory and practice by creating exercise
opportunities (APA classes)
• Remove barriers
• Promote an organization for easy and safe
access to APA classes
• Promote collaborative environment

Stakeholders
GPs and AUSL clinicians
Education
Reward system
Research

Clinical pathways for Chronic Care

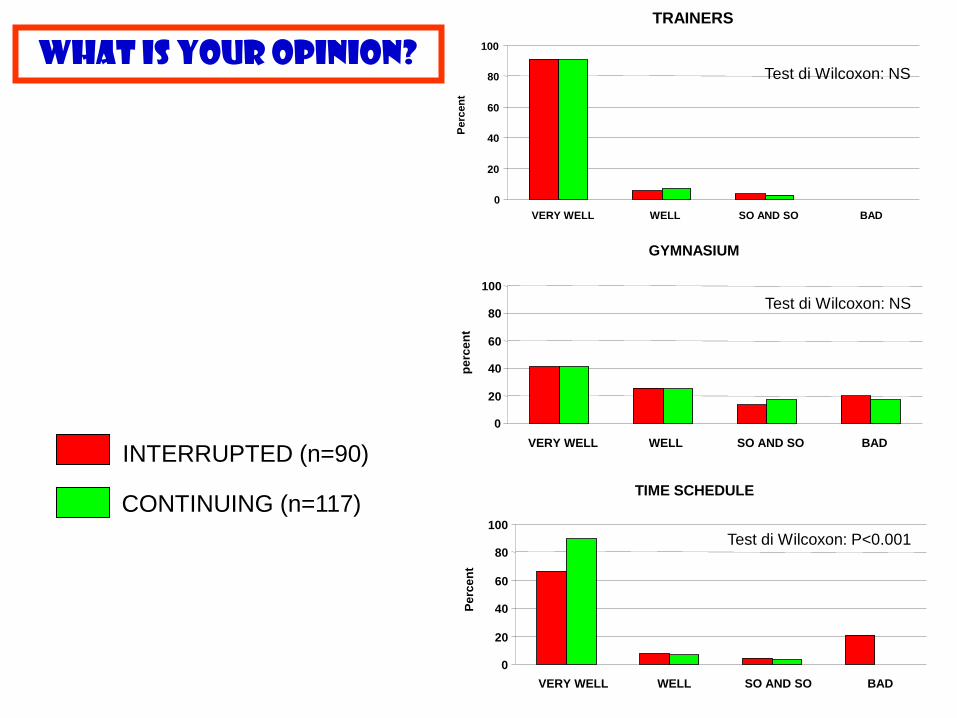
WHAT IS YOUR OPINION?
CONTINUING (n=117)
INTERRUPTED (n=90)
Test di Wilcoxon: P<0.001
Test di Wilcoxon: NS
Test di Wilcoxon: NS
TRAINERS
0
20
40
60
80
100
VERY WELL WELL SO AND SO BAD
Perc
en
t
GYMNASIUM
0
20
40
60
80
100
VERY WELL WELL SO AND SO BAD
pe
rce
nt
TIME SCHEDULE
0
20
40
60
80
100
VERY WELL WELL SO AND SO BAD
Pe
rce
nt
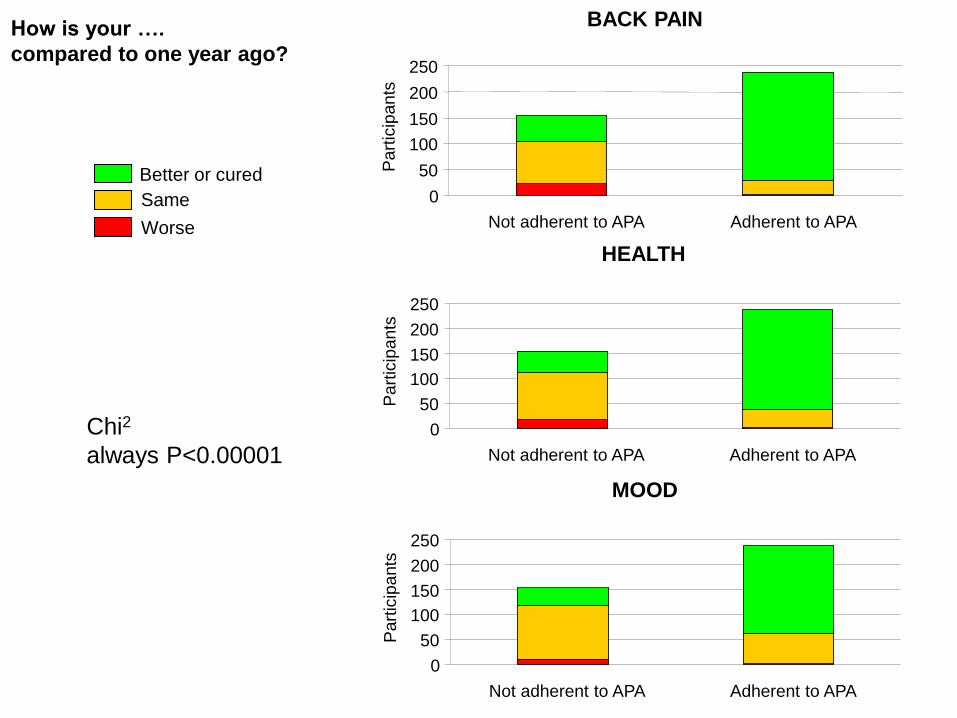
How is your ….
compared to one year ago?
Better or cured
Same
Worse
Chi2
always P<0.00001
BACK PAIN
0
50
100
150
200
250
Not adherent to APA Adherent to APA
Part
icip
ants
HEALTH
0
50
100
150
200
250
Not adherent to APA Adherent to APA
Part
icip
ants
MOOD
0
50
100
150
200
250
Not adherent to APA Adherent to APA
Part
icip
ants
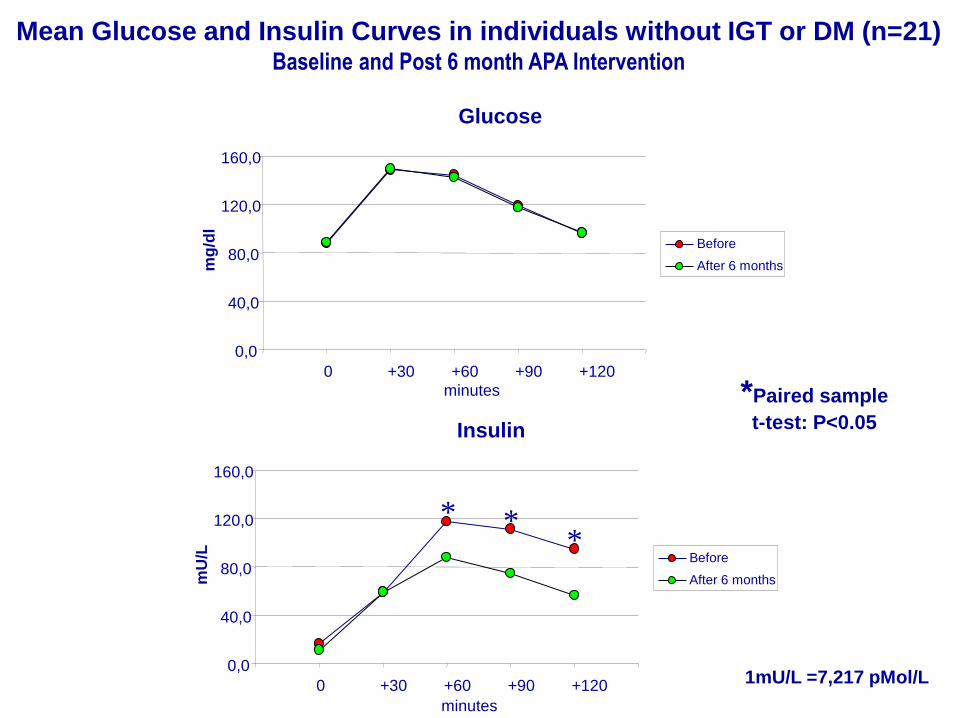
Insulin
0,0
40,0
80,0
120,0
160,0
0 +30 +60 +90 +120
mU
/L
Before
After 6 months
minutes
1mU/L =7,217 pMol/L
Mean Glucose and Insulin Curves in individuals without IGT or DM (n=21) Baseline and Post 6 month APA Intervention
* * *
*Paired sample
t-test: P<0.05
Glucose
0,0
40,0
80,0
120,0
160,0
0 +30 +60 +90 +120
mg
/dl
Before
After 6 months
minutes
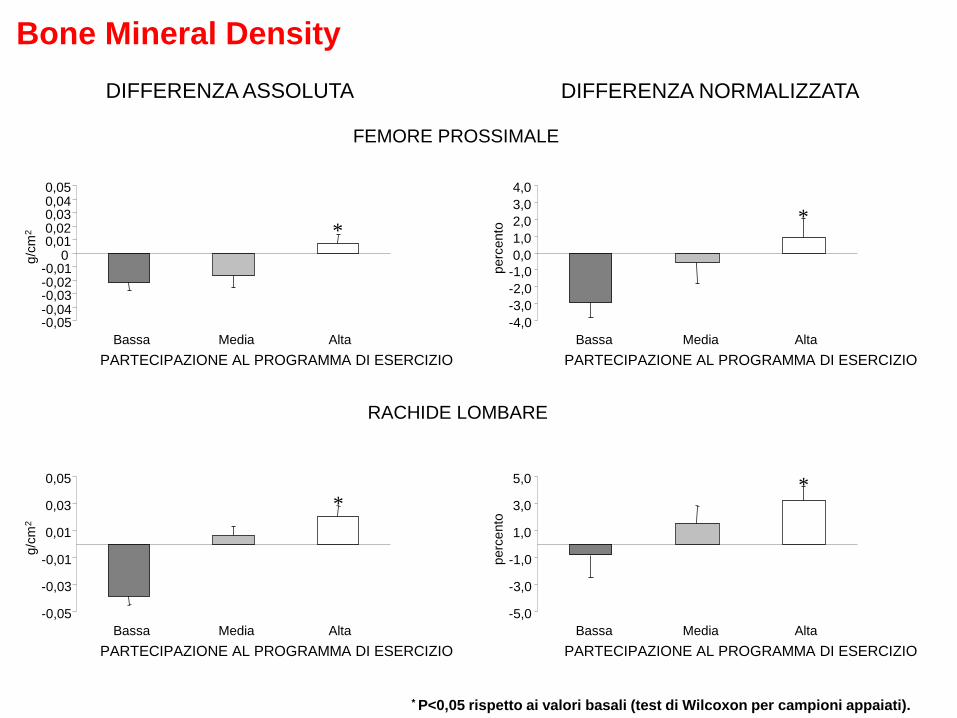
FEMORE PROSSIMALE
RACHIDE LOMBARE
-0,05 -0,04 -0,03 -0,02 -0,01
0 0,01 0,02 0,03 0,04 0,05
Bassa Media Alta
PARTECIPAZIONE AL PROGRAMMA DI ESERCIZIO
g/c
m2 *
-4,0
-3,0
-2,0
-1,0
0,0
1,0
2,0
3,0
4,0
Bassa Media Alta
PARTECIPAZIONE AL PROGRAMMA DI ESERCIZIO
perc
ento
*
-5,0
-3,0
-1,0
1,0
3,0
5,0
Bassa Media Alta
PARTECIPAZIONE AL PROGRAMMA DI ESERCIZIO
perc
ento
*
-0,05
-0,03
-0,01
0,01
0,03
0,05
Bassa Media Alta
PARTECIPAZIONE AL PROGRAMMA DI ESERCIZIO
g/c
m2
*
DIFFERENZA ASSOLUTA DIFFERENZA NORMALIZZATA
* P<0,05 rispetto ai valori basali (test di Wilcoxon per campioni appaiati).
Bone Mineral Density
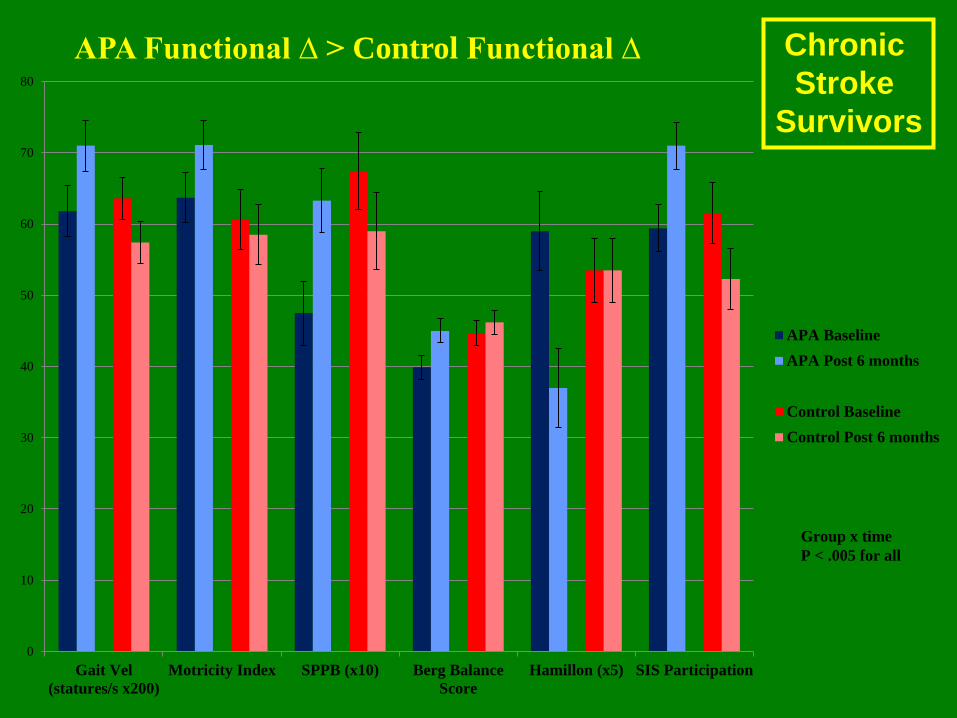
0
10
20
30
40
50
60
70
80
Gait Vel
(statures/s x200)
Motricity Index SPPB (x10) Berg Balance
Score
Hamillon (x5) SIS Participation
APA Functional ∆ > Control Functional ∆
APA Baseline
APA Post 6 months
Control Baseline
Control Post 6 months
Group x time
P < .005 for all
Chronic
Stroke
Survivors

GOALS GIVEN TO THE GENERAL DIRECTORS OF
THE 12 LOCAL HEALTH AUTHORITIES
BY TUSCANY REGION
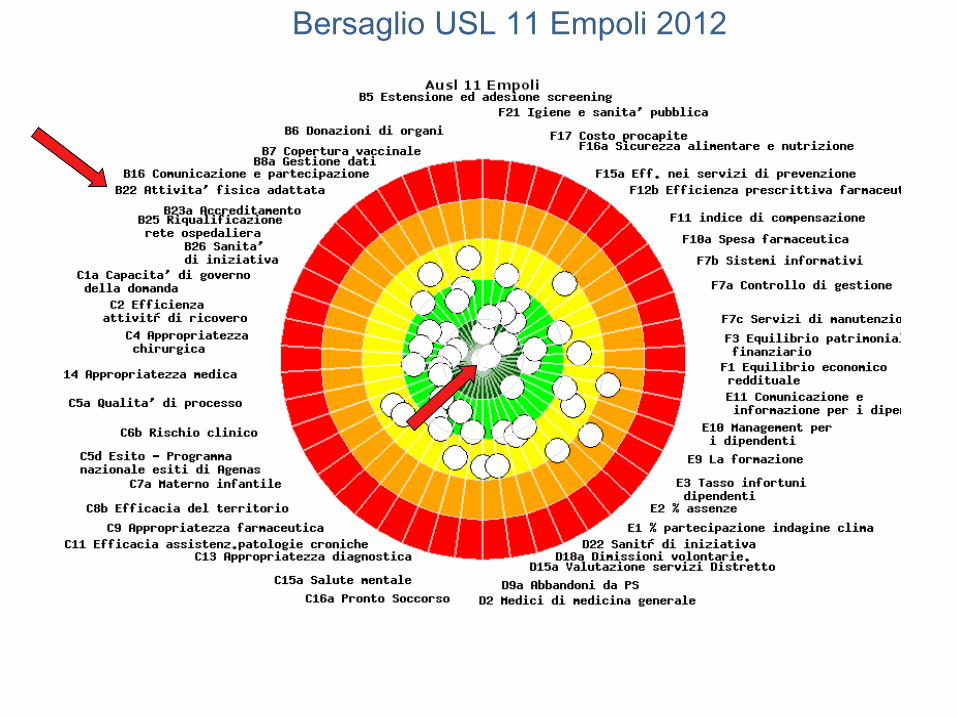
Bersaglio USL 11 Empoli 2012



Conferenza Stato Regioni ed Unificata
Citizens Conferences
APA dinners
Media
AFA day
T-shirt

Integrazione con altri programmi di salute

Punti della salute
Fare la spesa…e guadagnare salute
Integrazione con altri programmi di salute


BENESSERE DONNA

GRAZIE! [email protected]