Maintaining Clinical Exposure Following Mandated 2011 Residency … · Maintaining Clinical...
21
1 Maintaining Clinical Exposure Following Mandated 2011 Residency Program Redesign A retrospective review of programmatic changes of the Internal Medicine Residency at Johns Hopkins Bayview Medical Center Jonathon Thorp, M.D., M.B.A, Senior Resident, Internal Medicine
Transcript of Maintaining Clinical Exposure Following Mandated 2011 Residency … · Maintaining Clinical...

1
Maintaining Clinical Exposure
Following Mandated 2011 Residency
Program RedesignA retrospective review of programmatic changes of the Internal
Medicine Residency at Johns Hopkins Bayview Medical Center
Jonathon Thorp, M.D., M.B.A,
Senior Resident, Internal Medicine

Disclosures
• None
2

Presentation Objectives
1. Briefly review the historical context of the 2011
duty hour changes.
2. Explain how we applied the duty hour rules to
our internal medicine program.
3. Review the impact of these changes on volume
and types of patients seen by PGY1 trainees.
3
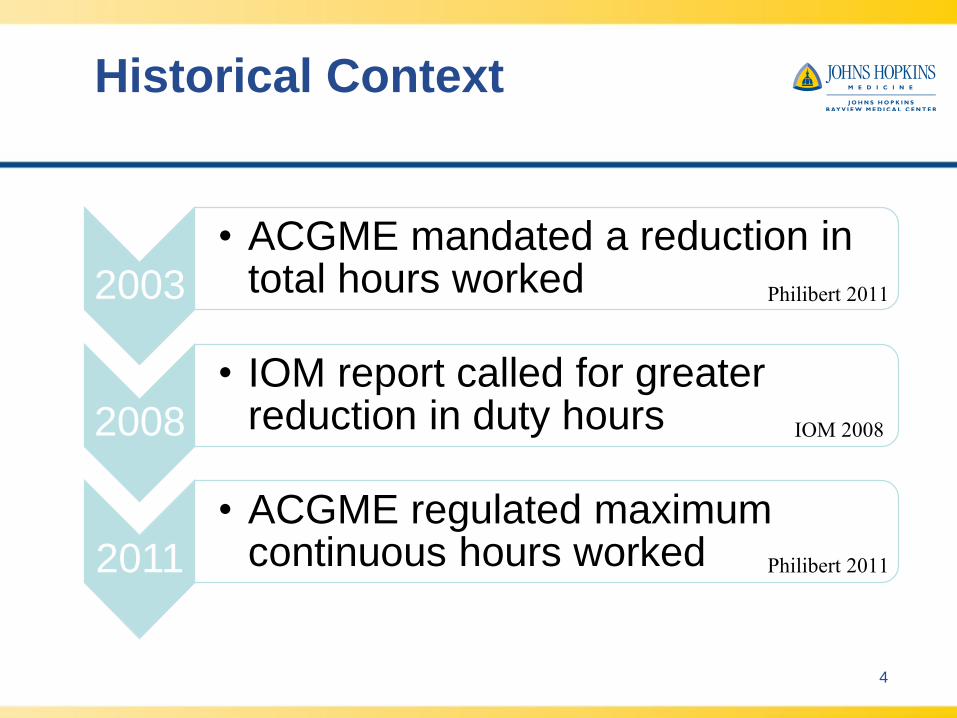
Historical Context
2003
• ACGME mandated a reduction in total hours worked
2008
• IOM report called for greater reduction in duty hours
2011
• ACGME regulated maximum continuous hours worked
4
IOM 2008
Philibert 2011
Philibert 2011

Continuous Hours Worked
• Pre-2011 • Post-2011
5
24
Hours
16
Hours
‡ didactic activities, transfer of patient care, outpatient clinics
+ 6‡
Hours

Types of Redesigns
6
Workload Compression
Workload Reduction

Program Redesign
2006
• Aliki Initiative
• Curriculum: patient centered care and safe transitions of care
2009/10
• Resident Review Oversight Committee
• Goal: increase continuity and improve team based care
2011 & Current
• Application of Duty Hours
• Increased ambulatory & general acute care medicine
• Decreased critical care time & elective
7
Study Design
• IRB approved
• Retrospective Analysis
• Data sources:
– Electronic Medical Record (i.e. Meditech)
– Administrative Billing Data (e.g. morality
data, case mix index)
– Program data (e.g. Demographic
information and training scores)
8
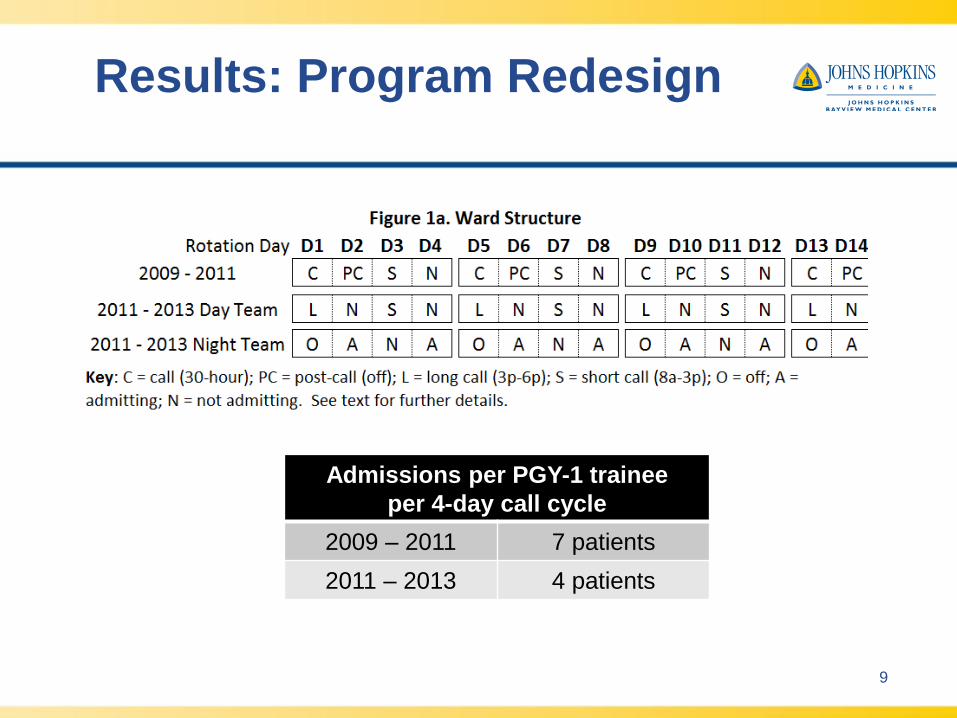
Results: Program Redesign
9
Admissions per PGY-1 trainee
per 4-day call cycle
2009 – 2011 7 patients
2011 – 2013 4 patients

Results: Program Redesign
10
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
160.00
180.00
No
. D
ays ±
Std
. D
ev.
Days on Service
Wards Critical Care Ambulatory Elective Vacation
All groups: P=0.00
Pre-2011
Post-2011

Variable2009-2011 2011-2013
P Valuemean (std. dev.) mean (std. dev.)
Total Inpatient
Encounters561.61 (63.43) 585.37 (125.92) 0.37
Unique Encounters 266.65 (36.58) 269.77 (62.16) 0.82
Unique & New
Encounters181.72 (25.45) 157.47 (40.47) 0.00
Follow up notes 379.89 (51.20) 427.90 (91.83) 0.02
Results: Inpatient Encounters
11

Results: Outpatient
Encounters
12
Variable2009-2011 2011-2013
P Valuemean (std. dev.) mean (std. dev.)
Outpatient Appointments
Scheduled 99.29 (5.03) 112.77 (18.42) 0.00
Attended 56.98 (6.59) 64.80 (10.85) 0.00

Results: Patient
Characteristics
13
Variable2009-2011 2011-2013
P Valuemean (std. dev.) mean (std. dev.)
Quality Data
Case Mix Index
(CMI)1.51 (0.081) 1.54 (0.11) 0.31
30-day Readmission
Rate0.22 (0.023) 0.19 (0.022) 0.00
30-day Mortality
Rate0.064 (0.012) 0.062 (0.016) 0.59
Average Length of
Stay8.48 (0.66) 9.28 (0.98) 0.00

Workload Reduction
• Better educational outcomes
• Improved trainee satisfaction
• Increased conference attendance
• Decreased duty hour violations
• Reduced 30-day hospital readmissions
• Increased bedside interprofessional
rounds
April 29, 2015 14
Gonzalo 2014, McMahon 2010, O’Connor 2011, Record 2011, Thanarajasingam 2012

Preliminary outcomes of
mandated reforms
15
30-day Mortality
30-day Readmission Rates
Surgical Morbidity & Mortality
Trainee Exam Scores
No D
iffe
rence
Patel 2014
Patel 2014, Block 2014
Rajaram 2014
Rajaram 2014

Limitations
• Objective educational outcomes are still in
data collection and analysis phase
• Encounter location may not be accurate if
note type was entered incorrectly
• Design did not allow for measurement of
face-to-face clinical time (e.g. time-motion
study)
• No inclusion of measures of burnout or
trainee fatigue 16

Discussion
17
1. Increased ambulatory & general acute care medicine
rotations
2. Created and integrated a night team member into
acute care medicine teams
3. Despite lowering admission caps, total, unique, and
follow-up encounters were essentially unchanged
4. PGY-1 trainees cared for similar types of patients pre-
and post-duty hour reform

References
• Block L, Jarlenski M, Wu A, et al. (2014). “Inpatient Safety Outcomes Following the 2011 Residency Work-
Hour Reform. Journal of Hospital Medicine, 9:347-352.
• Institute of Medicine (2008). Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. 15 Dec 2008.
Web. Accessed 11 Jan 2015. http://www.iom.edu/Reports/2008/Resident-Duty-Hours-Enhancing-Sleep-
Supervision-and-Safety.aspx
• McMahon GT, Katz JT, Thorndike ME, et al. “Evaluation of a redesign initiative in an internal-medicine
residency.” NEJM 2010; 362(14):1304-1311.
• O’Connor AB, Lang VJ, Bordley DR. (2011). Restructuring an inpatient resident service to improve
outcomes for residents, students, and patients. Acad Med, 86(12): 1500-1507.
• Patel MS, Volpp KG, Small DS, et al. (2014). Association of the 2011 ACGME resident duty hour reforms
with mortality and readmissions among hospitalized Medicare patients. JAMA, 312(22):2364-73.
• Philibert, I., Amis, S. (Eds.). (2011). The ACGME 2011 duty hour standards: enhancing quality of care,
supervision, and resident professional development. Chicago, IL: ACGME.
• Rajaram R, Chung JW, Jones AT, et al. (2014). Association of the 2011 ACGME resident duty hour reform
with general surgery patient outcomes and with resident examination performance. JAMA, 312(22):2374-
84.
• Record JD, Rand C, Christmas C, et al. (2011). Reducing heart failure readmissions by teaching patient-
centered care to internal medicine residents. Arch Internal Med, 171(9): 858-859.
• Thanarajasingam U, McDonald FS, Halvorsen AJ, et al. (2012) “Service census caps and unit-based
admissions: resident workload, conference attendance, duty hour compliance, and patient safety.” Mayo
Clin Proc., 87(4):320-327
18

Acknowledgements
• Colleen Christmas, MD
• Khalil Ghanem, MD
• Melissa Dattalo, MD
19

Questions Thank you for your attention!
20

21