Magnetic resonance angiography of the carotid arteries: comparison of unenhanced and contrast...
10
MAGNETIC RESONANCE Magnetic resonance angiography of the carotid arteries: comparison of unenhanced and contrast enhanced techniques Harald Kramer & Val M. Runge & John N. Morelli & Kenneth D. Williams & L. Gill Naul & Konstantin Nikolaou & Maximilian F. Reiser & Bernd J. Wintersperger Received: 12 August 2010 / Revised: 2 February 2011 / Accepted: 9 February 2011 / Published online: 9 April 2011 # European Society of Radiology 2011 Abstract Objective To compare different techniques for carotid imaging including contrast-enhanced, unenhanced and dynamic techniques to find an alternative to contrast- enhanced MRA. Methods 43 patients referred for imaging of the carotids were enrolled in this IRB-approved study. Imaging included dark-blood, time-of-flight, ECG-gated SSFP and dynamic and static contrast-enhanced MRA. Two radiologists eval- uated all datasets in terms of image quality (vessel lumen, signal homogeneity, diagnostic confidence, preferred tech- nique) on a four-point Likert-scale and in measuring the vessel area. Results Of the 43 included patients the first 8 subjects served for protocol optimisation and 4 individuals discon- tinued the examination. Thus 31 datasets served for evaluation. CE-MRA revealed best results for delineation of vessel lumen, signal homogeneity and diagnostic confidence with values of 3.61, 3.42 and 3.77. It was also rated as the most preferred technique. SSFP-MRA was rated second in all categories with values of 3.1, 2.9 and 3.11. This unenhanced technique was the only one showing non-significantly different results in quantitative analysis. Conclusion SSFP-MRA, an unenhanced form of MRA, represents an alternative to CE-MRA, particularly in patients where administration of gadolinium for CE-MRA may be contraindicated. In contrast to other techniques, SSFP-MRA serves with not significant different results compared to standard CE-MRA. Keywords MRI . MRA . Gadolinium . NSF . Unenhanced MRA Introduction Acute arterial vascular events are the leading cause of premature death in the developed world [1–3], Cerebrovas- cular events have replaced acute coronary ischaemia as the leading cause of death [4]. Because of that imaging of the supra-aortic vasculature has become a subject of great interest. Digital subtraction angiography (DSA) is still considered the gold standard, however, [5, 6], the invasive- ness of that technique, its associated risks and its dependence on ionising radiation have spurred develop- ment of non-invasive means of evaluating the supra-aortic vasculature. Vascular ultrasound, computed tomographic angiography (CTA) and magnetic resonance angiography (MRA) comprise such alternatives [7–13]. While vascular ultrasound is limited by patient body habitus and operator dependency [14], CTA and MRA are both reliable, reproducible and non-invasive means of imaging the H. Kramer (*) : K. Nikolaou : M. F. Reiser : B. J. Wintersperger Department of Clinical Radiology, University Hospitals Munich—Grosshadern Campus, Ludwig Maximilians University, Marchioninistr. 15, 81377 Munich, Germany e-mail: [email protected] V. M. Runge Department of Radiology, University of Texas Medical Branch, Galveston, TX, USA J. N. Morelli : K. D. Williams : L. G. Naul Department of Radiology, Scott and White Memorial Hospital, Temple, TX, USA B. J. Wintersperger Department of Medical Imaging, UHN, MSH and WCH, University of Toronto, Toronto, Canada Eur Radiol (2011) 21:1667–1676 DOI 10.1007/s00330-011-2110-x
-
Upload
harald-kramer -
Category
Documents
-
view
215 -
download
3
Transcript of Magnetic resonance angiography of the carotid arteries: comparison of unenhanced and contrast...
MAGNETIC RESONANCE
Magnetic resonance angiography of the carotid arteries:comparison of unenhanced and contrast enhanced techniques
Harald Kramer & Val M. Runge & John N. Morelli & Kenneth D. Williams &
L. Gill Naul & Konstantin Nikolaou & Maximilian F. Reiser & Bernd J. Wintersperger
Received: 12 August 2010 /Revised: 2 February 2011 /Accepted: 9 February 2011 /Published online: 9 April 2011# European Society of Radiology 2011
AbstractObjective To compare different techniques for carotidimaging including contrast-enhanced, unenhanced anddynamic techniques to find an alternative to contrast-enhanced MRA.Methods 43 patients referred for imaging of the carotidswere enrolled in this IRB-approved study. Imaging includeddark-blood, time-of-flight, ECG-gated SSFP and dynamicand static contrast-enhanced MRA. Two radiologists eval-uated all datasets in terms of image quality (vessel lumen,signal homogeneity, diagnostic confidence, preferred tech-nique) on a four-point Likert-scale and in measuring thevessel area.Results Of the 43 included patients the first 8 subjectsserved for protocol optimisation and 4 individuals discon-tinued the examination. Thus 31 datasets served forevaluation. CE-MRA revealed best results for delineation
of vessel lumen, signal homogeneity and diagnosticconfidence with values of 3.61, 3.42 and 3.77. It was alsorated as the most preferred technique. SSFP-MRA wasrated second in all categories with values of 3.1, 2.9 and3.11. This unenhanced technique was the only one showingnon-significantly different results in quantitative analysis.Conclusion SSFP-MRA, an unenhanced form of MRA,represents an alternative to CE-MRA, particularly inpatients where administration of gadolinium for CE-MRAmay be contraindicated. In contrast to other techniques,SSFP-MRA serves with not significant different resultscompared to standard CE-MRA.
Keywords MRI .MRA .Gadolinium . NSF. UnenhancedMRA
Introduction
Acute arterial vascular events are the leading cause ofpremature death in the developed world [1–3], Cerebrovas-cular events have replaced acute coronary ischaemia as theleading cause of death [4]. Because of that imaging of thesupra-aortic vasculature has become a subject of greatinterest. Digital subtraction angiography (DSA) is stillconsidered the gold standard, however, [5, 6], the invasive-ness of that technique, its associated risks and itsdependence on ionising radiation have spurred develop-ment of non-invasive means of evaluating the supra-aorticvasculature. Vascular ultrasound, computed tomographicangiography (CTA) and magnetic resonance angiography(MRA) comprise such alternatives [7–13]. While vascularultrasound is limited by patient body habitus and operatordependency [14], CTA and MRA are both reliable,reproducible and non-invasive means of imaging the
H. Kramer (*) :K. Nikolaou :M. F. Reiser :B. J. WinterspergerDepartment of Clinical Radiology,University Hospitals Munich—Grosshadern Campus,Ludwig Maximilians University,Marchioninistr. 15,81377 Munich, Germanye-mail: [email protected]
V. M. RungeDepartment of Radiology, University of Texas Medical Branch,Galveston, TX, USA
J. N. Morelli :K. D. Williams : L. G. NaulDepartment of Radiology, Scott and White Memorial Hospital,Temple, TX, USA
B. J. WinterspergerDepartment of Medical Imaging, UHN, MSH and WCH,University of Toronto,Toronto, Canada
Eur Radiol (2011) 21:1667–1676DOI 10.1007/s00330-011-2110-x

carotid arteries, [15]. CTA suffers from limitations such as areliance on ionising radiation [16], lack of dynamicinformation and reduced accuracy in regions of heavilyvascular calcification [17, 18]. In distinction, MRA is notimpaired by the presence of vascular calcifications, pro-vides dynamic information and allows for a detailedassessment of vascular walls because of its superior softtissue contrast [19–21].
Since the introduction of MRA in the late 1980s, varioustechniques have been described for evaluation of the carotidarteries including phase contrast (PC) and time of flight(TOF) angiography [22–26]. Image acquisition with suchtechniques may last several minutes. This limitation wasovercome with the advent of contrast-enhanced (CE) MRAin 1992 [27]. Today, CE-MRA is the technique of choicefor non-invasive, cross-sectional vascular imaging with adiagnostic accuracy of greater than 90% and specificitygreater than 95% [7, 13, 28–30]. Ongoing improvements inMR hardware and software have further spurred develop-ment of dynamic techniques such as time-resolved MRAfor evaluation of the supraaortic vessels [9, 19, 31].
With the recent discovery of Nephrogenic SystemicFibrosis (NSF) and its subsequent linkage to gadoliniumchelate contrast media administration in patients withsevere renal impairment [32–34], the use of gadoliniumchelates for the performance of CE-MRA has fallen underincreased scrutiny. The aim of the present study is thus tocompare one unenhanced approach to carotid MRA—ECG-gated steady state free precession (SSFP) MRA—withconventional CE-MRA, dynamic time-resolved CE-MRAand additional unenhanced MRA techniques.
Materials and methods
Study design and population
A total of 43 consecutive patients (mean age: 63±16 years;17 men and 24 women) were enrolled from April to July2009 in this institutional review board (IRB)-approvedstudy. All patients enrolled in this prospective cohort trialhad been referred for CE-MRA of the carotid vasculaturebased on syncope, dizziness, or the clinical suspicion ofstenosis or stroke. Written informed consent was obtainedfrom each participant.
MR imaging
All examinations were performed on a 3 Tesla, 32-channelwide bore clinical MR system (Magnetom Verio, SiemensHealthcare, Erlangen, Germany) utilising a 12-element headcoil, a 4-element neck coil and a 6-element body surfacecoil as well as portions of the 24-element spine coil. In each
patient the following distinct MRA examinations wereacquired:
& T2-weighted dark blood (DB) MRA& Time of Flight (TOF) MRA& ECG-gated SSFP MRA& Dynamic contrast-enhanced (CE) MRA& Static high-resolution CE-MRA.
Because of technical constraints related to its reliance onflow characteristics for the derivation of signal, TOF MRAwas performed in an axial orientation, covering only thecarotid bifurcation. Source images for all other techniqueswere acquired in the coronal plane.
Although dark blood and time-of-flight MRA can easilybe implemented at higher spatial resolutions, to equalise thecomparison amongst sequences, each method, with theexception of the dynamic CE-MRA, was performed at aspatial resolution of 0.9×0.9×0.9 mm3. Because of addi-tional requirements of temporal resolution with the dynamicCE-MRA technique, spatial resolution was selected to be1.1×1.1×1.1 mm3, a value providing temporal resolutionof 3.5 s/frame. CE-MRA as the most frequently usedtechniques served as the standard of reference and alltechniques were compared to this standard but also to all ofthe other techniques.
T2-weighted dark blood MRA
Although one of the first described unenhanced MRAtechniques, dark blood MRA is not routinely used forevaluation of the carotid arteries in current clinical practice,but may be utilised to further evaluate the vessel wall orconsistency of the contained plaque, and was thus includedin the study [35–37]. Detailed parameters for all utilisedsequences are given in Table 1.
TOF MRA
In distinction to dark blood techniques, gradient echo(GRE) TOF MRA sequences use only one radiofrequencyexcitation pulse, the echo being formed by reversal of thegradient magnetic field [38–40]. Sequence parameters wereoptimised for imaging the carotid arteries. Coronal slaborientation showed poor results versus the transverselyorientated slabs. The final imaging parameters utilised forall study examinations can be found in Table 1.
ECG-gated SSFP MRA (NATIVE TrueFISP—true fastimaging with steady state precession non-contrast-enhancedangiography of arteries and veins)
This ECG-gated SSFP technique is based upon thepreparation of the imaging volume with a spatially selective
1668 Eur Radiol (2011) 21:1667–1676

inversion pulse, resulting in the suppression of signal fromstationary tissue and blood initially containedwithin the imagingvolume. Blood flowing into the imaging volume exhibits thesame high signal present in conventional SSFP. High signal ofthe inflowing blood is further accentuated by the suppression ofbackground tissue signal intensity by the inversion pulse.NATIVE (Siemens Healthcare, Erlangen, Germany) TrueFISPMRA was originally implemented for imaging of the renalarteries utilising transverse slabs [41, 42]. The standardconfiguration of the inversion pulse and the imaging volumein this study is illustrated in Fig. 1. To avoid substantial flowartefacts, the technique was performed using ECG-triggeringwith the data acquisition occurring during diastole. Sequenceoptimisation showed an inversion time (TI) of 900 to 1,200 msto be optimal. If triggering was initially not well-coordinatedwith diastole, a trigger delay was utilised as shown in Fig. 2.Imaging parameters for this particular technique can be foundin Table 1.
Static CE MRA
Contrast-enhanced MRA is the technique of choice for non-invasive imaging of nearly every vascular territory [28, 43–48]. Administration of gadolinium chelate contrast agentsleads to a substantial decrease in T1 relaxation time ofblood, resulting in high intravascular signal intensity. In thisstudy a dedicated FLASH (Fast Low Angle Shot) 3D MRAsequence was utilised. Sequence parameters for CE MRAare shown in Table 1. In this study, CE MRA was theoriginal examination for which all patients were referredand served as the standard of reference.
Dynamic MRA (TWIST—time resolved angiographywith stochastic trajectories)
As the previously discussed techniques resulted only in theacquisition of static images, TWIST (Siemens Healthcare,
Erlangen, Germany) was the only technique evaluated inthis study with the capability to provide dynamic informa-tion. Like static CE-MRA, dynamic MRA utilises thesubstantial T1 relaxation produced by intravascular gado-linium chelate contrast agents to image the vasculature [9,49]. The direct link between acquisition time and spatialresolution in CE-MRA results in an inevitable trade-off
Fig. 1 Representative sagittal scout image demonstrates the typicalorientation of the acquired coronal volume (white box) relative to thespatially selective inversion pulse (grey dotted box) for ECG-gatedSSFP imaging of the carotid arteries
Table 1 Detailed sequence parameters for all the techniques utilised
DB TOF SSFP Dynamic MRA CE MRA
spatial resolution (mm3) 0.9×0.9×0.9 0.9×0.9×0.9 0.9×0.9×0.9 1.1×1.1×1.1 0.9×0.9×0.9
acquisition time (min) 5:19 2:45 a5:00 b1:07 (17) 0:18
PAT factor 2 2 2 3 3
TR/TE [ms] 1900/171 16/1.74 a1622.18/1.81 3.09/1.14 2.6/1.17
FOV [mm] 220 220 280 280 280
Slices 52 52 88 60 88
Matrix 256 256 320 256 320
BW [Hz/Px] 454 501 781 650 650
flip angle [°] 25 70 25 20
a Acquisition time for ECG-gated SSFP MRA is heart-rate-dependent, and thus TR values were also adjusted to the RR intervalb Total acquisition time for dynamic MRA is the sum of 17 consecutive timeframes
Eur Radiol (2011) 21:1667–1676 1669

between temporal and spatial resolution with this technique.Imaging with a temporal resolution of 3.5 s/frame allowedmaintenance of satisfactory SNR and CNR while providinga spatial resolution of 1.1×1.1×1.1 mm3. Image evaluationwas done in a single dataset presenting the best arterialphase. Detailed sequence information is listed in Table 1.
Contrast agent administration
In all contrast- enhanced examinations, gadobenate dime-glumine (MultiHance, Bracco, Italy) was utilized. In the
present study, a fixed volume of 14 mL was utilized forhigh-resolution CE-MRA, while a 4.5 mL fixed dose wasadministered for the dynamic examination. For accurateplanning of the static CE-MRA, an initial test bolus(1.5 mL) was used to estimate the timing of contrast agentarrival. For all examinations, the rate of administration ofcontrast agent was 1.5 mL/sec, and each injection wasfollowed by a 20 mL bolus.
Qualitative evaluation
Detailed sections of the carotid bifurcation of allacquired MRA datasets were reformatted as maximumintensity projections (MIP) (15 slices; 3 mm thickness,2 mm overlap), and displayed in a left to right, cranial tocaudal orientation allowing for in-plane evaluation of thecarotid bifurcation, including the area from the distalcommon carotid to the proximal part of the internal andexternal carotids as illustrated in Fig. 3. Right or leftcarotid artery was chosen in a randomized fashion toexclude sequence inherent influences. Images were pre-sented separately for analysis. Image quality evaluationswere performed by two independent, blinded readers withmore than 10 years of experience in MRA. To eliminatebias inherent in the given sequences, the carotid artery tobe evaluated (i.e. left or right) was chosen in a random
Fig. 2 Typical ECG waveforms demonstrate a the timing of theinversion pulse (IP) and data acquisition (DA) in the case where theRR interval is long enough to accommodate both. b To appropriatesynchronise a patient’s cardiac activity with the desired timing of theinversion pulse and data acquisition, a trigger delay (TD) may be usedbefore the inversion pulse such that data acquisition still occurs inend-diastole
Fig. 3 Reformatted 3-mm slicemaximum intensity projections(MIP) were presented for evalu-ation of image quality. Varioustechniques including a time offlight, b cardiac-gated SSFP, cdynamic CE-MRA, d static,high-resolution CE-MRA, and eT2-weighted dark bloodsequences are illustrated
1670 Eur Radiol (2011) 21:1667–1676

fashion. Image quality was assessed with respect to thefollowing criteria:
& Delineation of the vessel lumen with respect to thesurrounding tissue
& Homogeneity of the intravascular signal& Overall diagnostic confidence
Scans were rated according to these criteria on a fourpoint Likert scale. Possible assessments of the vessellumen delineation were: 1 = poor, barely visible lumenrendering the study non-diagnostic, 2 = fair, ill-definedvessel borders with suboptimal image quality for diag-nosis, 3 = good, sufficient arterial demarcation withadequate image quality for diagnosis, and 4 = excellent,sharply defined arterial borders with excellent imagequality for highly confident diagnosis. Options for ratingintravascular signal intensity were: 1 = poor, completelyinhomogeneous with no continuous signal throughout thevessel, 2 = fair, major inhomogeneities with ill-definedarterial boarders, 3 = good with some minor inhomoge-neities not influencing vessel delineation and 4 =homogeneous signal throughout the entire vessel. Diag-nostic confidence was rated as 1 = poor with no definitediagnosis possible, 2 = fair with judgment of majorchanges possible without exact grading, 3 = good withdefinite diagnosis possible and 4 = excellent with exactgrading of degree of vessel changes possible. In additionto this quality assessment, the readers were asked for
each vessel evaluated to identify the most preferredtechnique overall and to rank the other techniques.
Quantitative evaluation
Quantitative evaluation of the vessel cross-sectional areawas performed for every carotid bifurcation at threepredefined levels which were reformatted perpendicularto the course of the vessel. The levels are shown inFig. 4:
& 2 cm proximal to the bifurcation perpendicular to theCCA
& ICA origin& 2 cm distal to the bifurcation perpendicular to the ICA
Slice definitions were matched exactly for all techni-ques in each individual patient. In different sessions foreach technique, with at least 3 days in between sessionsto avoid bias, two blinded readers evaluated the vesselcross-sectional area at each slice location. To evaluate ifthere were any level-dependent differences in measure-ments which could potentially lead to differences instenosis grading, ratios between the readers’ averagemeasurements between level 3 and level 1 as well aslevel 3 and level 2 were calculated and compared amongthe various techniques. This evaluation was done to avoid thepotential drawback of only a small number of significantfindings in the evaluated population. Calculation of ratios
Fig. 4 Representative images a demonstrate the appearance of the carotid arteries utilising all the sequences evaluated at the three levels near thecarotid bifurcation (b)
Eur Radiol (2011) 21:1667–1676 1671

between different levels and comparing these ratios in differenttechniques is independent from pathologic findings.
Statistical analysis
Statistical analysis was performed utilizing a paired t-testand Bland-Altman Plots to evaluate intra- and interindivid-ual differences in measurements at each imaged level withreliability of these measurements assessed using an inter-class correlation (ICC) evaluation. An ANOVA analysiswas performed for the comparison of area ratios utilizingPASW Statistics 17.0.2 (SPSS Inc., Chicago, Illinois,USA). Results were determined to be statistically signifi-cant if the calculated p value was less than 0.05. An ICCvalue of 1 represents a perfect statistical correlation.
Results
Image quality
Of the 43 included patients, experiments in the initial8 individuals were utilized to optimize sequence parametersof the different techniques. Four individuals were excluded dueto discontinuation of the examination secondary to claustro-phobia (n=3) or technical failure of the MR System (n=1).Thus 31 datasets were evaluated. With respect to thequalitative assessment of vessel lumen delineation, the highresolution CE-MRA enabled the best lumen visualization witha mean score of 3.61±0.64, directly followed by SSFP MRAwhich achieved a mean score of 3.1±0.86. T2-weighted DBMRA, dynamic MRA and TOF MRA received average scoresof 2.89±0.77, 2.77±0.56, and 1.92±0.96, respectively. Signalintensity within the vessel was rated equally for CE-MRA(3.42±0.62) and dynamic MRA (3.42±0.59), followed bySSFP MRA, T2-weighted DB and TOF MRAwith respectivescores of 2.9±0.74, 2.68±0.62 and 2.03±0.94. Diagnosticconfidence was found to be greatest with CE-MRA, whichreceived a mean score of 3.77±0.58. SSFP was ranked secondoverall (3.11±0.87) followed by dynamic MRA, T2-weightedDB, and TOF MRAwhich were given overall scores of 3.02±0.59, 3.0±0.77 and 2.03±1 respectively.
High resolution CE-MRA was the most preferred tech-nique overall with a mean rank of 1.34±0.77, again followedby SSFP MRA (2.61±1.15). The other techniques wereranked in order: dynamic MRA, T2-weighted DB MRA andTOF MRAwith respective average ranks of 3.16±1.07, 3.44±0.9, and 4.45±0.99. CE-MRAwas deemed the overall mostpreferred technique in 79.03% of cases, with SSFP MRAbeing most preferred in 16.13% of the cases, TOF MRA in3.23%, and dynamic MRA in 1.61%. Dark blood MRAwasnever ranked as the most preferred technique. SSFP MRAmost often was judged the second most preferred technique
(37.1%) followed by dynamic MRA (30.65%), T2-weightedDB MRA (17.74%), CE-MRA (11.29) and TOF MRA(3.23%) (See Fig. 5).
Assessment of cross-sectional vessel areas
Of the 31 evaluated patients only three showed hemody-namic relevant stenoses in the evaluated area of the carotidbifurcation. Because of that no evaluation in terms of theNorth American Symptomatic Carotid EndarterectomyTrial (NASCET) criteria was done but, as mentioned inthe “Materials and methods” section, vessel area ratios atcertain levels calculated. Steady-state free precession MRAwas the only technique showing no significant differencesin cross-sectional vessel area at any level compared withthe high-resolution CE-MRA standard (Fig. 6). TOF MRAdemonstrated no significant differences in vessel areacompared with CE-MRA at levels 1 and 3, but exhibitedsignificant differences in cross-sectional area from high-resolution CE-MRA at the level of the carotid bifurcation.Both the T2-weighted dark blood MRA sequence anddynamic MRA showed significant differences at all threeevaluated levels compared with static CE-MRA. Further-more all techniques other than CE-MRA (at all levels) and
Fig. 5 Preferred MRA techniques as determined by blinded analysis.Most preferred technique is CE MRA in nearly 80% of all cases (a). TheSSFP technique was most frequently rated as 2nd most preferred in about37% of cases (b), directly followed by dynamic MRA
1672 Eur Radiol (2011) 21:1667–1676
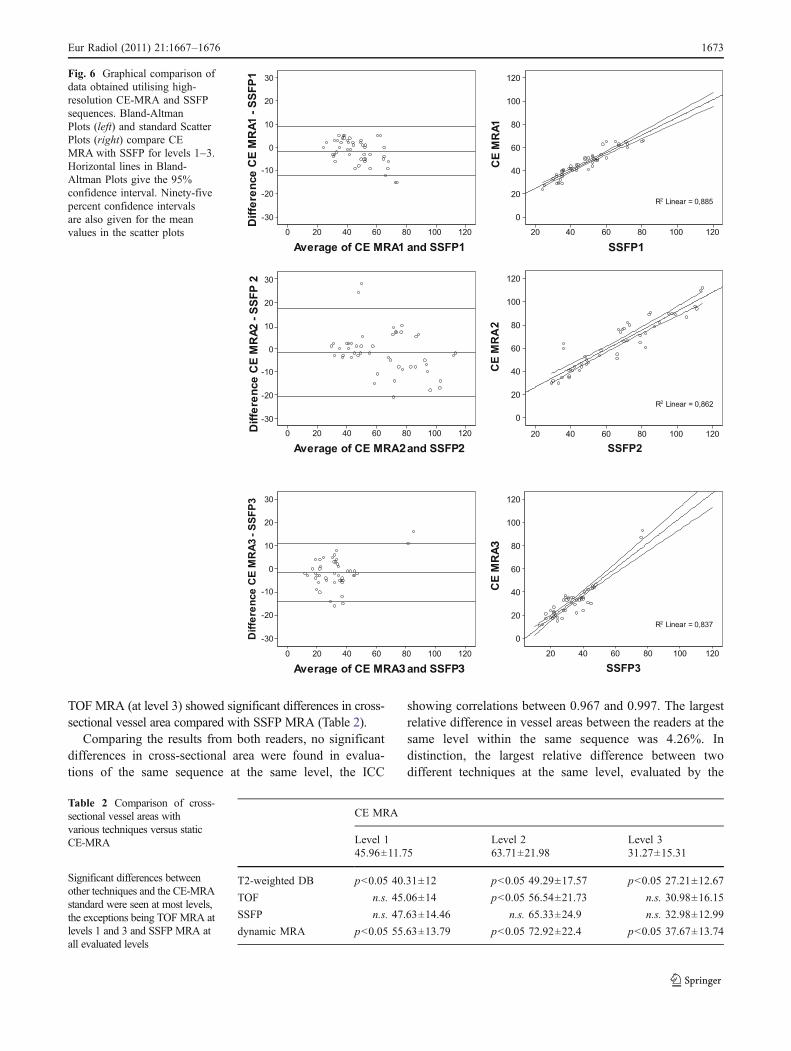
TOF MRA (at level 3) showed significant differences in cross-sectional vessel area compared with SSFP MRA (Table 2).
Comparing the results from both readers, no significantdifferences in cross-sectional area were found in evalua-tions of the same sequence at the same level, the ICC
showing correlations between 0.967 and 0.997. The largestrelative difference in vessel areas between the readers at thesame level within the same sequence was 4.26%. Indistinction, the largest relative difference between twodifferent techniques at the same level, evaluated by the
Fig. 6 Graphical comparison ofdata obtained utilising high-resolution CE-MRA and SSFPsequences. Bland-AltmanPlots (left) and standard ScatterPlots (right) compare CEMRA with SSFP for levels 1–3.Horizontal lines in Bland-Altman Plots give the 95%confidence interval. Ninety-fivepercent confidence intervalsare also given for the meanvalues in the scatter plots
CE MRA
Level 1 Level 2 Level 345.96±11.75 63.71±21.98 31.27±15.31
T2-weighted DB p<0.05 40.31±12 p<0.05 49.29±17.57 p<0.05 27.21±12.67
TOF n.s. 45.06±14 p<0.05 56.54±21.73 n.s. 30.98±16.15
SSFP n.s. 47.63±14.46 n.s. 65.33±24.9 n.s. 32.98±12.99
dynamic MRA p<0.05 55.63±13.79 p<0.05 72.92±22.4 p<0.05 37.67±13.74
Table 2 Comparison of cross-sectional vessel areas withvarious techniques versus staticCE-MRA
Significant differences betweenother techniques and the CE-MRAstandard were seen at most levels,the exceptions being TOFMRA atlevels 1 and 3 and SSFP MRA atall evaluated levels
Eur Radiol (2011) 21:1667–1676 1673

same reader was 28.29%. ANOVA analysis examining theoverall ratios between level 3 and level 1 and between level3 and level 2 revealed no significant differences among thetechniques with respect to static CE-MRA with theexception of the TOF MRA at level 2 (Table 3). However,analysis of the vessel lumen measurements at the differentlevels found results of all techniques to differ significantlyfrom high-resolution CE-MRA, with the exception of SSFPMRA.
Discussion
Due to high obtainable image quality, non-invasive techni-ques have essentially replaced conventional diagnostic cath-eter angiography for imaging the arterial vasculature.Contrast-enhanced MRA currently represents the preferredapproach for non-invasive imaging of all extracranial vascularterritories among the different possibilities for MRA [5–7,13]. The association between gadolinium chelate adminis-tration in the renally impaired and nephrogenic systemicfibrosis has raised increasing concerns about the safety ofcontrast-enhanced MR techniques [33]. CE-MRA for theevaluation of atherosclerotic vascular disease is particularlyproblematic given the high concurrent incidence of renalimpairment. Thus, there has been an increased impetus todevelop unenhanced MR techniques of comparable accuracyand efficiency to CE-MRA [50]. Numerous studies haveshown CE-MRA to be an accurate, reliable diagnostic tool inthe evaluation of stenosis degree and also in the measure-ment of cross-sectional vessel area—an important value toestablish before intervention, particularly before stenting ordeployment of other vessel prostheses [51]. While conven-tional catheter angiography remains the gold standard ofclinical reference, CE-MRA was utilised as the standard ofreference in the present investigation. Not surprisingly of alltechniques performed, CE-MRAwas rated most preferred innearly 80% of cases. The second most favoured techniquewas an unenhanced SSFP sequence, which has previouslybeen shown to produce reliable results in coronary and
thoracic MRA [52]. In terms of both vessel lumendelineation and diagnostic confidence the SSFP techniquewas rated superior to dynamic contrast-enhanced, T2-weighted DB and TOF MRA. While dynamic CE-MRAdoes allow assessment of flow dynamics, in many casesthis technique was assessed by the blinded readers ashaving a too low spatial resolution. This finding isunsurprising given the lower spatial resolution generallyutilised with this technique because of time constraintsnecessary to achieve adequate temporal resolution. Arte-facts leading to a low rating were especially prevalent inTOF MRA: because of its flow dependence, turbulencewithin the region of the carotid bifurcation often resultedin significant artefacts in this region. These led to distortedmeasurements of cross-sectional vessel area especially inat the level of the bifurcation. The present study is notwithout limitations. While SSFP MRA was the secondmost preferred technique overall by the readers, determi-nation of reader preference of CE-MRA over SSFP mayhave been somewhat overestimated given that the formeris the clinical technique most commonly employed, andthus is the technique with which the blinded readers havethe most experience and are thus most comfortable. In theevaluated cohort, there was no reliable number ofpathological findings to definitely evaluate the perfor-mance of each technique with respect to stenosis grading.Although this was a limitation, such a low incidence ofhaemodynamically significant stenoses, in the experienceof the authors, is the norm for patients referred for carotidMRA in a typical imaging centre not specialised on neuro-imaging. Because of this limitation, an alternative tool wasimplemented for assessment of the performance of eachtechnique with respect to vessel calibre: ratios werecalculated between the vessel areas in the distal ICA inrelation to the common carotid and ICA origin. As onlythe ratios were compared in this analysis, whether or not avessel stenosis was present was not of consequence to thefinal evaluation. In this analysis, TOF MRA was the onlytechnique to differ significantly from the CE-MRAstandard, showing a difference in the ratios obtained between
Table 3 Comparison of calculated ratios of vessel areas among various techniques
Level 1: Level 3 Mean ratio CE-MRA comparison Level 2: Level 3 Mean ratio CE-MRA comparison
DB T2-weighted 67.80 n.s. DB T2-weighted 56.76 n.s.
Time of Flight MRA 69.01 n.s. Time of Flight MRA 59.99 p<0.05
Cardiac-gated SSFP 71.48 n.s. Cardiac-gated SSFP 54.65 n.s.
Dynamic MRA 67.97 n.s. Dynamic MRA 54.91 n.s.
n.s. not significant
Ratios of vessel areas between the common carotid (level 1) and distal internal carotid arteries (level 3) as well as between the internal carotid arteryorigin (level 2) and distal internal carotid artery were compared among techniques. All sequences produced similar ratios with the exception of the timeof flight MRA technique, in which the ratio between level 2 and level 3 was inconsistent with the results obtained with other methods
1674 Eur Radiol (2011) 21:1667–1676

the distal internal carotid artery and the ICA origin. This findingimplies that TOF MRA would be less reliable in gradingstenoses at the origin of the ICA. Although the remainder of theresults suggest that the other techniques evaluated wouldperform similarly in the detection of stenoses, further compar-isons, particularly between SSFP MRA and CE-MRA, areessential. CE-MRA has been shown to be a reliable tool for thistype of planning with measurements acquired utilising thistechnique not differing significantly from those obtained withDSA [51]. Although comparison with DSA was not availablein this study, because of the factors previously noted, SSFPMRA was the only technique evaluated that exhibitedmeasurements of cross-sectional vessel area not significantlydifferent from those of CE-MRA. In the case of imagingpatients in renal failure the extra time required for unenhancedevaluation may be well-spent.
Conclusion
Electrocardiography-gated SSFP MRA has shown the mostaccurate results in the assessment of carotid arteryvasculature in comparison to CE-MRA in evaluation ofthe cross sectional vessel area and has been chosen as themost preferable alternative technique to CE-MRA based onits high image quality. Because of its accurate display ofvessel diameters it allows not only adequate assessment ofvessel lumen ratios—which is especially of interest withregard to stenoses’ measurements—but also the exactmeasurement of vessel dimensions allowing for adequateplanning of interventional stent therapy.
Based on given results ECG-gated SSFP MRA ought tobe considered a reliable alternative to CE-MRA techniquesin the assessment of the carotid artery vasculature allowingan accurate MR-based assessment of the carotids withoutthe need for administration of gadolinium-based contrastagents. This would be a major benefit especially in patientswith impaired renal function and a potentially elevated riskof NSF development.
Acknowledgment The authors like to thank Gary R McNeal fromSiemens Healthcare for his valuable support in the optimization processof all used sequences as well as Jilene Gendron and Vincent Mundy fortheir continuous tremendous helped during execution of all exams.
References
1. Prabhakaran P, Ajay VS, Prabhakaran D et al (2007) Globalcardiovascular disease research survey. J Am Coll Cardiol50:2322–2328
2. Reddy KS (2004) Cardiovascular disease in non-Westerncountries. N Engl J Med 350:2438–2440
3. Reddy KS, Yusuf S (1998) Emerging epidemic of cardiovasculardisease in developing countries. Circulation 97:596–601
4. Rothwell PM, Coull AJ, Silver LE et al (2005) Population-basedstudy of event-rate, incidence, case fatality, and mortality for allacute vascular events in all arterial territories (Oxford VascularStudy). Lancet 366:1773–1783
5. Remonda L, Senn P, Barth A, Arnold M, Lovblad KO, Schroth G(2002) Contrast-enhanced 3D MR angiography of the carotidartery: comparison with conventional digital subtraction angiog-raphy. AJNR Am J Neuroradiol 23:213–219
6. Sundgren PC, Sunden P, Lindgren A, Lanke J, Holtas S, LarssonEM (2002) Carotid artery stenosis: contrast-enhanced MRangiography with two different scan times compared with digitalsubtraction angiography. Neuroradiology 44:592–599
7. Anzalone N, Scomazzoni F, Castellano R et al (2005) Carotidartery stenosis: intraindividual correlations of 3D time-of-flightMR angiography, contrast-enhanced MR angiography, conven-tional DSA, and rotational angiography for detection and grading.Radiology 236:204–213
8. Boudewijn G, Vasbinder C, Nelemans PJ (2005) Accuracy ofcomputed tomographic angiography and magnetic resonanceangiography for diagnosing renal artery stenosis. Perspect VascSurg Endovasc Ther 17:180
9. Carroll TJ, Korosec FR, Petermann GM, Grist TM, Turski PA (2001)Carotid bifurcation: evaluation of time-resolved three-dimensionalcontrast-enhanced MR angiography. Radiology 220:525–532
10. Cloft HJ, Joseph GJ, Dion JE (1999) Risk of cerebralangiography in patients with subarachnoid hemorrhage, cerebralaneurysm, and arteriovenous malformation: a meta-analysis.Stroke 30:317–320
11. Kido DK, Barsotti JB, Rice LZ et al (1991) Evaluation of thecarotid artery bifurcation: comparison of magnetic resonanceangiography and digital subtraction arch aortography. Neuroradi-ology 33:48–51
12. Ross JS, Masaryk TJ, Ruggieri PM (1991) Magnetic resonanceangiography of the carotid bifurcation. Top Magn Reson Imaging3:12–22
13. Yang CW, Carr JC, Futterer SF et al (2005) Contrast-enhancedMR angiography of the carotid and vertebrobasilar circulations.AJNR Am J Neuroradiol 26:2095–2101
14. Clevert DA, Johnson T, Michaely H et al (2006) High-gradestenoses of the internal carotid artery: comparison of high-resolution contrast enhanced 3D MRA, duplex sonography andpower Doppler imaging. Eur J Radiol 60:379–386
15. Kaufmann TJ, Kallmes DF (2005) Utility of MRA and CTA in theevaluation of carotid occlusive disease. Semin Vasc Surg 18:75–82
16. Hollingworth W, Nathens AB, Kanne JP et al (2003) Thediagnostic accuracy of computed tomography angiography fortraumatic or atherosclerotic lesions of the carotid and vertebralarteries: a systematic review. Eur J Radiol 48:88–102
17. Schernthaner R, Stadler A, Lomoschitz F et al (2008) Multi-detector CT angiography in the assessment of peripheral arterialocclusive disease: accuracy in detecting the severity, number, andlength of stenoses. Eur Radiol 18:665–671
18. Bui TD, Gelfand D, Whipple S et al (2005) Comparison of CTand catheter arteriography for evaluation of peripheral arterialdisease. Vasc Endovascular Surg 39:481–490
19. Lim RP, Shapiro M, Wang EY et al (2008) 3D time-resolved MRangiography (MRA) of the carotid arteries with time-resolvedimaging with stochastic trajectories: comparison with 3D contrast-enhanced Bolus-Chase MRA and 3D time-of-flight MRA. AJNRAm J Neuroradiol 29:1847–1854
20. Nederkoorn PJ, van der Graaf Y (2009) MRA for carotid arterystenosis. Stroke 40:e77, author reply e78
21. Thurnher SA (2005) MRA of the carotid arteries. Eur Radiol 15:E11–E16
Eur Radiol (2011) 21:1667–1676 1675

22. Isoda H, Takehara Y, Isogai S et al (1998) Technique for arterial-phase contrast-enhanced three-dimensional MR angiography ofthe carotid and vertebral arteries. AJNR Am J Neuroradiol19:1241–1244
23. Wildermuth S, Debatin JF, Huisman TA, Leung DA, McKinnonGC (1995) 3D phase contrast EPI MR angiography of the carotidarteries. J Comput Assist Tomogr 19:871–878
24. Sardanelli F, Zandrino F, Parodi RC, De Caro G (1999) MRangiography of internal carotid arteries: breath-hold Gd-enhanced3D fast imaging with steady-state precession versus unenhanced2D and 3D time-of-flight techniques. J Comput Assist Tomogr23:208–215
25. Wilman AH, Huston J 3rd, Riederer SJ (1997) Three-dimensionalmagnetization-prepared time-of-flight MR angiography of thecarotid and vertebral arteries. Magn Reson Med 37:252–259
26. Buxton RB, Kerber CW, Frank LR (1993) Pulsatile flow artifactsin two-dimensional time-of-flight MR angiography: initial studiesin elastic models of human carotid arteries. J Magn ResonImaging 3:625–636
27. Marchal G, Michiels J, Bosmans H, Van Hecke P (1992) Contrast-enhanced MRA of the brain. J Comput Assist Tomogr 16:25–29
28. Nael K, Ruehm SG, Michaely HJ et al (2006) High spatial-resolution CE-MRA of the carotid circulation with parallelimaging: comparison of image quality between 2 differentacceleration factors at 3.0 Tesla. Invest Radiol 41:391–399
29. Loewe C, Schillinger M, Haumer M et al (2004) MRA versusDSA in the assessment of occlusive disease in the aortic archvessels: accuracy in detecting the severity, number, and length ofstenoses. J Endovasc Ther 11:152–160
30. Willinek WA, von Falkenhausen M, Born M et al (2005)Noninvasive detection of steno-occlusive disease of the supra-aortic arteries with three-dimensional contrast-enhanced magneticresonance angiography: a prospective, intra-individual comparativeanalysis with digital subtraction angiography. Stroke 36:38–43
31. Nokes SR (2001) Elliptic centric contrast enhanced MRAprovides high resolution, noninvasive evaluation of the carotid/vertebral arteries. J Ark Med Soc 98(83):88
32. Thomsen HS, Marckmann P, Logager VB (2007) Nephrogenicsystemic fibrosis (NSF): a late adverse reaction to some of thegadolinium based contrast agents. Cancer Imaging 7:130–137
33. Thomsen HS, Morcos SK, Dawson P (2006) Is there a causalrelation between the administration of gadolinium based contrastmedia and the development of nephrogenic systemic fibrosis(NSF)? Clin Radiol 61:905–906
34. Thomsen HS (2006) Nephrogenic systemic fibrosis: a serious lateadverse reaction to gadodiamide. Eur Radiol 16:2619–2621
35. Stivaros SM, Harris JN, Adams W, Jackson A (2009) Does blackblood MRA have a role in the assessment of intracerebralaneurysms? Eur Radiol 19:184–192
36. Potthast S, Mitsumori L, Stanescu LA, et al (2010) Measuringaortic diameter with different MR techniques: comparison ofthree-dimensional (3D) navigated steady-state free-precession(SSFP), 3D contrast-enhanced magnetic resonance angiography(CE-MRA), 2D T2 black blood, and 2D cine SSFP. J Magn ResonImaging 31:177–184
37. Tello R, Mitchell PJ, Witte DJ, Thomson KR (2003) T2 darkblood MRA for renal artery stenosis detection: preliminaryobservations. Comput Med Imaging Graph 27:11–16
38. Tanaka H, Numaguchi Y, Konno S, Shrier DA, Shibata DK, PatelU (1997) Initial experience with helical CT and 3D reconstructionin therapeutic planning of cerebral AVMs: comparison with 3D
time-of-flight MRA and digital subtraction angiography. JComput Assist Tomogr 21:811–817
39. Cronqvist M, Stahlberg F, Larsson EM, Lonntoft M, Holtas S(1996) Evaluation of time-of-flight and phase-contrast MRAsequences at 1.0 T for diagnosis of carotid artery disease. I. Aphantom and volunteer study. Acta Radiol 37:267–277
40. Dagirmanjian A, Ross JS, Obuchowski N et al (1995) Highresolution, magnetization transfer saturation, variable flip angle,time-of-flight MRA in the detection of intracranial vascularstenoses. J Comput Assist Tomogr 19:700–706
41. Herborn CU, Watkins DM, Runge VM, Gendron JM, MontgomeryML, Naul LG (2006) Renal arteries: comparison of steady-state freeprecessionMR angiography and contrast-enhancedMR angiography.Radiology 239:263–268
42. Maki JH, Wilson GJ, Eubank WB, Glickerman DJ, Pipavath S,Hoogeveen RM (2007) Steady-state free precession MRA of therenal arteries: breath-hold and navigator-gated techniques vsCE-MRA. J Magn Reson Imaging 26:966–973
43. Voth M, Haneder S, Huck K, Gutfleisch A, Schonberg SO, MichaelyHJ (2009) Peripheral magnetic resonance angiography with contin-uous table movement in combination with high spatial and temporalresolution time-resolvedMRAWith a total single dose (0.1 mmol/kg)of gadobutrol at 3.0 T. Invest Radiol 44:627–633
44. Kramer H, Zenge M, Schmitt P, Glaser C, Reiser MF, HerrmannKA (2008) Peripheral magnetic resonance angiography (MRA)with continuous table movement at 3.0 T: initial experiencecompared with step-by-step MRA. Invest Radiol 43:627–634
45. Klessen C, Hein PA, Huppertz A et al (2007) First-pass whole-body magnetic resonance angiography (MRA) using the blood-pool contrast medium gadofosveset trisodium: comparison togadopentetate dimeglumine. Invest Radiol 42:659–664
46. Nael K, Fenchel M, Krishnam M, Finn JP, Laub G, Ruehm SG(2007) 3.0 Tesla high spatial resolution contrast-enhancedmagnetic resonance angiography (CE-MRA) of the pulmonarycirculation: initial experience with a 32-channel phased array coilusing a high relaxivity contrast agent. Invest Radiol 42:392–398
47. Fenchel M, Nael K, Deshpande VS et al (2006) Renal magneticresonance angiography at 3.0 Tesla using a 32-element phased-array coil system and parallel imaging in 2 directions. InvestRadiol 41:697–703
48. Kramer U, Nael K, Laub G et al (2006) High-resolution magneticresonance angiography of the renal arteries using parallel imagingacquisition techniques at 3.0 T: initial experience. Invest Radiol41:125–132
49. Fain SB, King BF, Breen JF, Kruger DG, Riederer SJ (2001)High-spatial-resolution contrast-enhanced MR angiography of therenal arteries: a prospective comparison with digital subtractionangiography. Radiology 218:481–490
50. Kang JW, Lim TH, Choi CG, Ko GY, Kim JK, Kwon TW (2010)Evaluation of contrast-enhanced magnetic resonance angiography(MRA) using Gd-DOTA compared with time-of-flight MRA inthe diagnosis of clinically significant non-coronary arterialdisease. Eur Radiol 20:1934–1944
51. Schoenberg SO, Rieger J, Weber CH et al (2005) High-spatial-resolution MR angiography of renal arteries with integratedparallel acquisitions: comparison with digital subtraction angiog-raphy and US. Radiology 235:687–698
52. McCarthy RM, Deshpande VS, Beohar N et al (2007) Three-dimensional breathhold magnetization-prepared TrueFISP: a pilotstudy for magnetic resonance imaging of the coronary arterydisease. Invest Radiol 42:665–670
1676 Eur Radiol (2011) 21:1667–1676