
Magnesium Sulfate for Neuroprotection of Prematurity · 1 + Magnesium Sulfate for Neuroprotection...
55
+ Magnesium Sulfate for Neuroprotection of Prematurity C. David Adair, M.D. Professor and Vice-Chairman The University of Tennessee College of Medicine Department of Obstetrics & Gynecology Section on Maternal-Fetal Medicine Chattanooga, TN
Transcript of Magnesium Sulfate for Neuroprotection of Prematurity · 1 + Magnesium Sulfate for Neuroprotection...
1
+
Magnesium Sulfate for
Neuroprotection of
Prematurity
C. David Adair, M.D.
Professor and Vice-Chairman
The University of Tennessee College of Medicine
Department of Obstetrics & Gynecology
Section on Maternal-Fetal Medicine
Chattanooga, TN
+ Objectives
Define Cerebral Palsy
Review mechanisms of brain injury at neuronal level
Discuss mechanisms of MgSO4 as a potential
neuroprotective agent
Review the current literature of antenatal MgSO4
Review a suggested MgSO4 protocol
Conflict Statement
I have no real or potential conflicts
regarding the presentation of the material.
3
+ Cerebral Palsy
Definition: Global term for a hetergeneous group of
chronic, nonprogressive disabilities of the central
nervous system affecting movement and muscle
coordination.
Incidence: 2-3 children per 1,000 live births
Higher incidence in preterm infants, risk indirectly
proportional to gestational age
Incidence in VLBW ranges from 4-8%
Slightly higher incidence in males and in multiple
gestations
+ Cerebral Palsy
Risk Factors:
Preterm Birth
Damage to a developing brain
PVL, IVH
Birth Asphyxia
Hypoxia ischemic encephalopathy (HIE)
+ Early Observational Data
1980’s, studies showed decreased rates of IVH and CP in
VLBW infants born to women with preeclampsia.
Van de Bor, Leviton
Early 1990’s, it was shown that VLBW infants exposed to
MgSO4 for tocolysis also had decreased rates of IVH.
Kuban
1996 – Lower rate of CP in VLBW infants exposed MgSO4
Grether et al.
Could this be explained by exposure to MgSO4?
+ Magnesium: Functions
Essential for cellular functions
DNA transcription
Hormone receptor binding, mitochondrial oxidative phosphorylation
Gating calcium channels
Transmembrane ion flux
Adenylate cyclase regulation
Muscle contraction
Control of vasomotor tone
Cardiac excitability
Neuronal transmitter release
Anticonvulsant
Block Voltage Dependent
Ca++ Channel
NMDA receptor antagonist
+ Background: Biochemistry
Glutamate is an excitory amino acid known to play an important role
in brain injury by increasing intracellular Ca++
Increase in intracellular Ca++
Excitotoxic
Interference with enzymatic reactions
Phospholipase
Membrane phospholipid hydrolysis
Arachidonic acid cycle
Prostaglandin synthesis
Gene expression
Protein synthesis
Production of free radical
Release of Cytochrome C
+ Mechanism of Action: MgSO4
Not clearly understood, but current theories:
Magnesium is a non-competitive antagonist of the
glutamate NMDA receptor
↑ Extracellular magnesium => blocks NMDA receptor
=> inhibits intracellular calcium => block neuronal
injury
Vasodilitation of cerebral blood vessles, increasing
cerebral blood flow
Reduction of oxygen free radicals
Reduction of inflammatory cytokines
+ Current Evidence
Mittendorf (AJOG 2002)
aka MagNET
Crowther (JAMA 2003)
aka ACTOMgSO4
Magpie Trial Follow-Up Study Collaborative Group (BJOG
2007)
Marret (BJOG 2007)
aka PREMAG
Rouse (NEJM 2008)
aka BEAM
Constantine (Obstet Gynecol 2009)
Meta-analysis
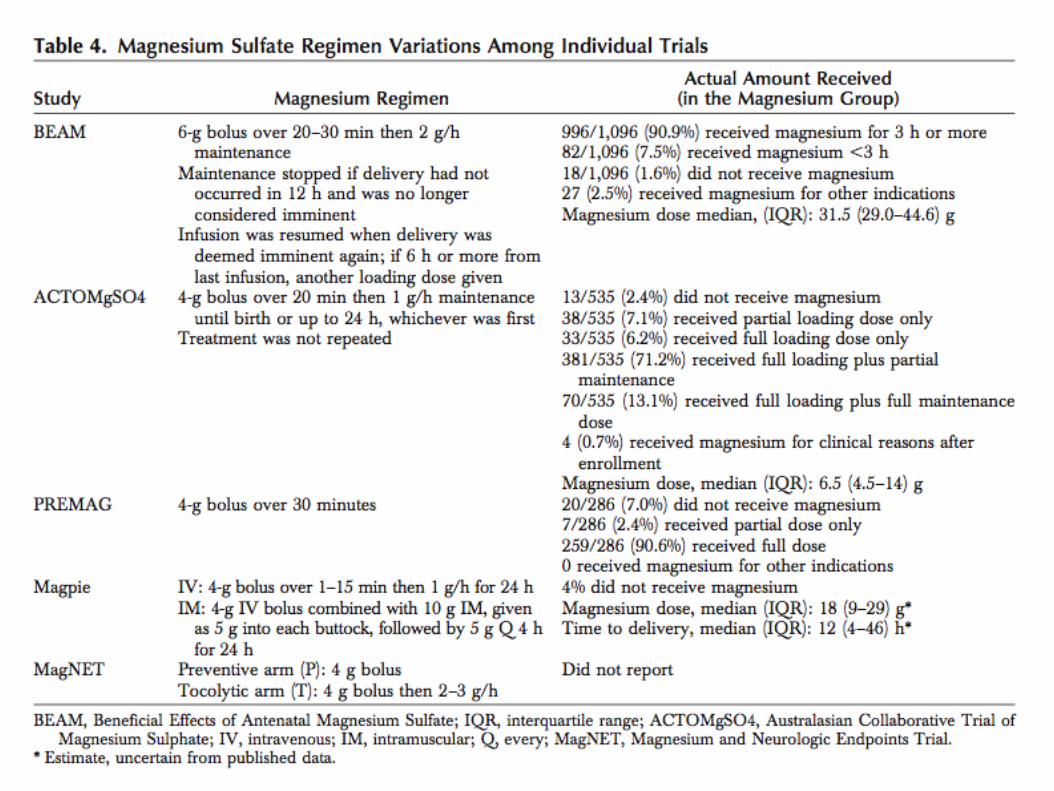
+ MagNET
Mittendorf, et al. 2002
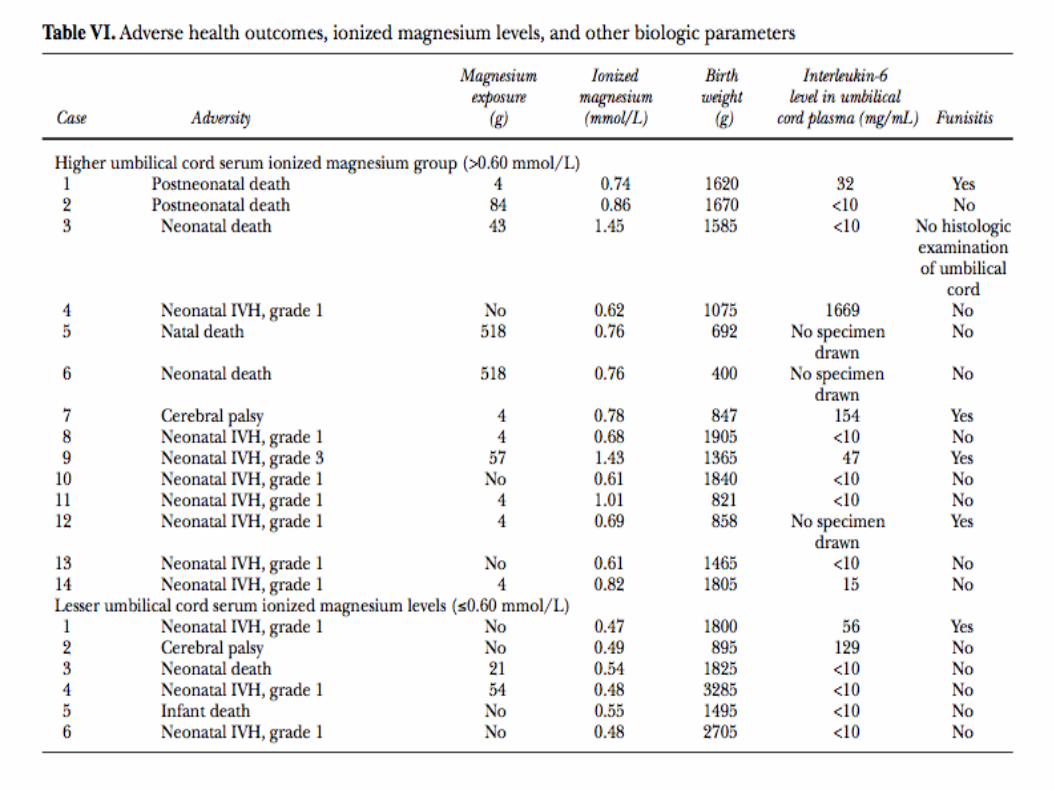
“Association between the use of antenatal magnesium
sulfate in preterm labor and adverse health outcomes in
infants” (Magnesium and Neurologic Endpoints Trial)
Objective: determine whether antenatal MgSO4
prevents adverse outcomes ( IVH/PVL/CP/Death)
149 women
Singleton or twin 24-34 weeks with PPROM or PTL
2 protocols; one which examined use for CP prevention,
the other evaluated MgSO 4 as a tocolytic
Prevention group - >4cm, received 4 gm load
+ MagNET: Outcomes
In neuroprophylaxis arm – 37% (11/30) had an adverse
event compared to 21% (6/29) of those that received
placebo.
When the 2 arms were combined, 32% of infants that
received MgSO4 had an adverse event compared to 19%
of the infants of mothers that received placebo.
The findings were not statistically significant (p=.07) yet
raised concern that MgSO4 might be harmful to
neonates.
There appeared to be a dose response relationship between
MgSO4 and adverse outcomes.
+ ACTOMgSO4
Crowther, et al. 2003. Australian Collabortive Trial of
Magnesium Sulfate Collaborative Group
“Effect of magnesium sulfate given for neuroprotection before
preterm birth”
Objective: determine effectiveness of MgSO4 given for
neuroprotection to women @ risk for preterm delivery
before 30 wks
RCT at 16 tertiary hospitals in Australia and New Zealand
1062 women, less than 30 wks gestation
Singleton/twin/triplet/quadruplet pregnancies
PPROM- 8% of patients enrolled
Birth expected within 24 hours.
4 gram load followed by 1 gram/hr x 24hrs
+ ACTOMgSO4
Primary outcome:
Rates of total pediatric mortality, CP, and the
combined outcome of death and CP at
corrected age of 2 years
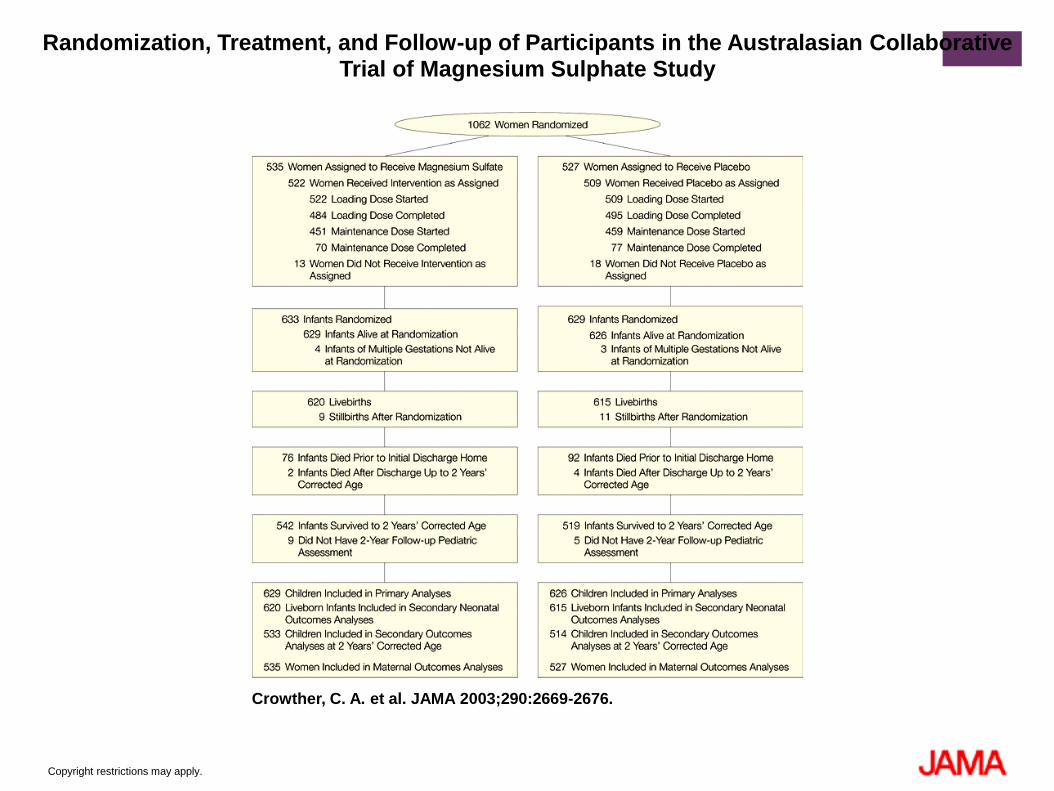
Copyright restrictions may apply.
Crowther, C. A. et al. JAMA 2003;290:2669-2676.
Randomization, Treatment, and Follow-up of Participants in the Australasian Collaborative Trial of Magnesium Sulphate Study
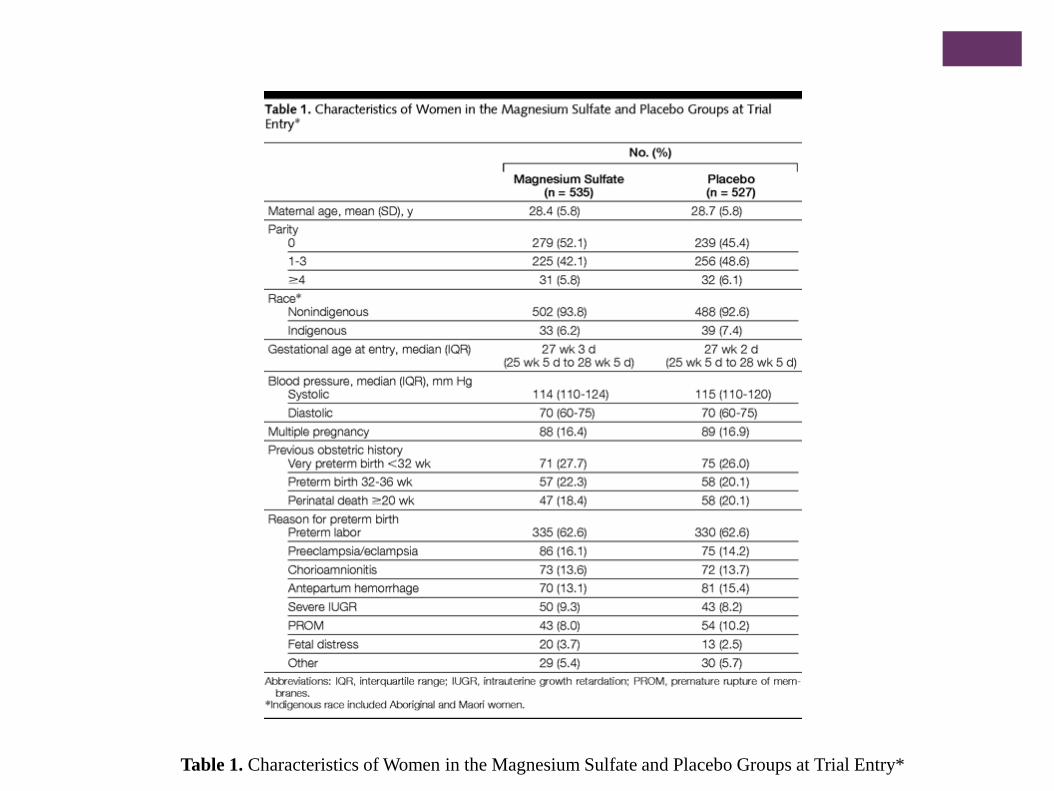
Table 1. Characteristics of Women in the Magnesium Sulfate and Placebo Groups at Trial Entry*
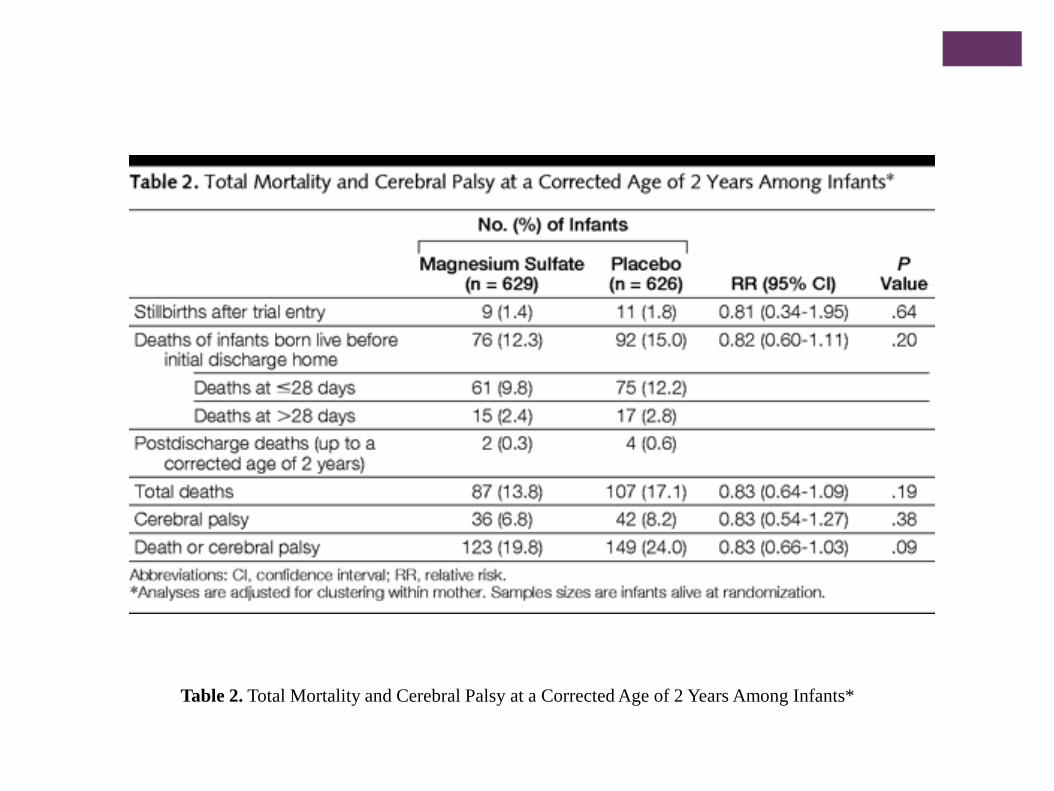
Table 2. Total Mortality and Cerebral Palsy at a Corrected Age of 2 Years Among Infants*
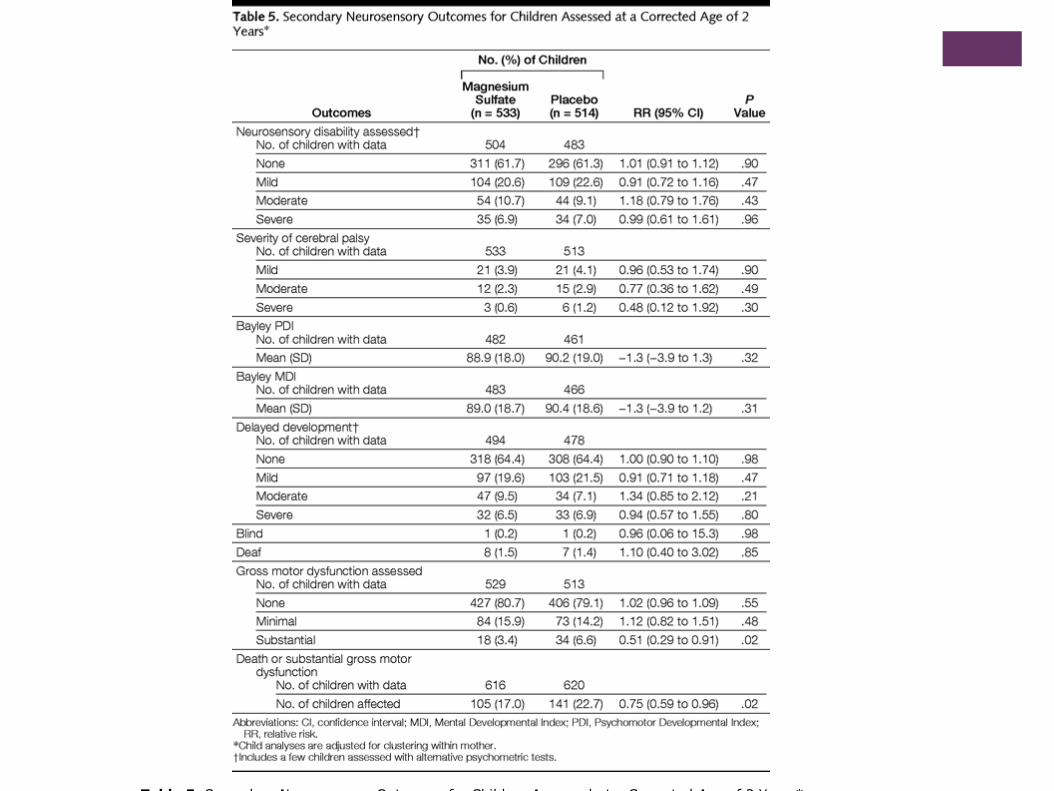
Table 5. Secondary Neurosensory Outcomes for Children Assessed at a Corrected Age of 2 Years*
+ ACTOMgSO4: Outcomes
The primary outcomes of total pediatric mortality, cerebral
palsy in survivors, and combined death or cerebral palsy
were all lower in the magnesium sulfate group, but not
statistically significant.
Stillbirth or death before age 2 was significantly less frequent
among infants of women randomized to MgSO4 group
RR 0.83, 95% CI 0.64-1.09
Substantial gross motor dysfunction was significantly less
frequent among surviving children of women randomized to
MgSO4 group
RR 0.51, 95% CI 0.29-0.91
+ Magpie
Magpie Trial Follow-up Study Collaborative Group, 2007
“The Magpie trial: a randomised trial comparing magnesium
sulfate with placebo for pre-eclampsia. Outcome for children
at 18 months”
Prospective RCT conducted at 175 hospitals in 33 countries.
Originally included 8804 women with pre-eclampsia randomized
to MgSO4 or placebo.
Concluded that risk of seizure was 58% lower in pre-eclamptic
women given MgSO4 .
Objective of the follow-up study: to assess long-term effects of in-
utero exposure to MgSO4 for children whose mothers had pre-
eclampsia
2895 of 4483 children assessed at 18 months of age for the primary
outcome of death or neurosensory disability.
+ Magpie: Outcomes
Original study – MgSO4 for women with pre-eclampsia
more than halves the risk of eclampsia and probably
reduces the risk of maternal death before discharge from
the hospital
No substantive harmful effects were apparent in the short
term, for either mother or baby.
Exposure to MgSO4 while in-utero was not associated
with a clear difference in the risk of death or disability
for children at 18 months.
+ PREMAG
Marret, et al. 2007
“Benefit of magnesium sulfate given before very preterm
birth to protect infant brain”
Objective: evaluate whether MgSO4 given to women at
risk of very-preterm birth would be neuroprotective in
preterm newborns and would prevent neonatal mortality
and severe white-matter injury.
Carried out in 18 French tertiary hospitals
Studied 573 mothers randomized to receive 4gm MgSO4
bolus or placebo
Gestational age < 33 weeks whose birth was planned or
expected within 24 hours
+ PREMAG: Outcomes
Primary outcomes: rates of severe white-matter
injury (WMI) or total mortality before hospital
discharge, and their combined outcome.
The rates of total mortality before hospital
discharge, severe WMI, and the combination of
severe WMI and/or death were all lower for the
MgSO4 group, but not statistically significant
Total mortality (9.4% vs. 10.4%; OR 0.79, 95% CI 0.44-1.44)
Severe WMI (10.0% vs. 11.7%; OR 0.78, 95% CI 0.47-1.31)
Combined (16.5% vs. 17.9%; OR 0.86, 95% CI 0.55-1.34)
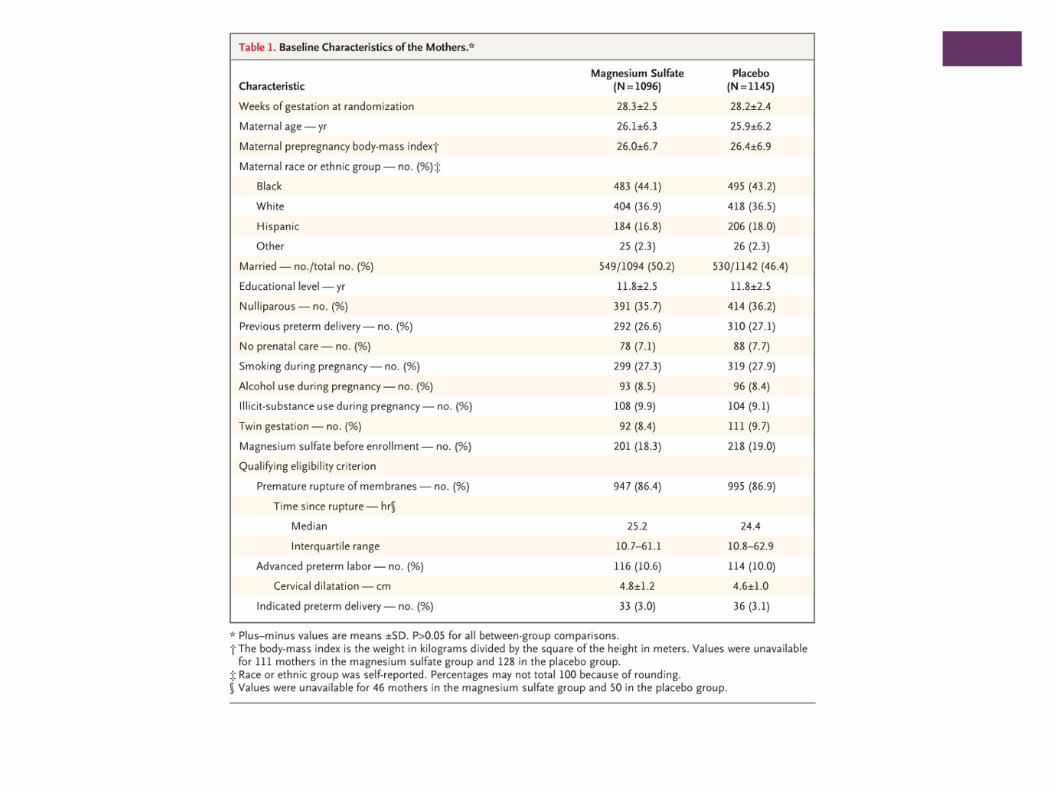
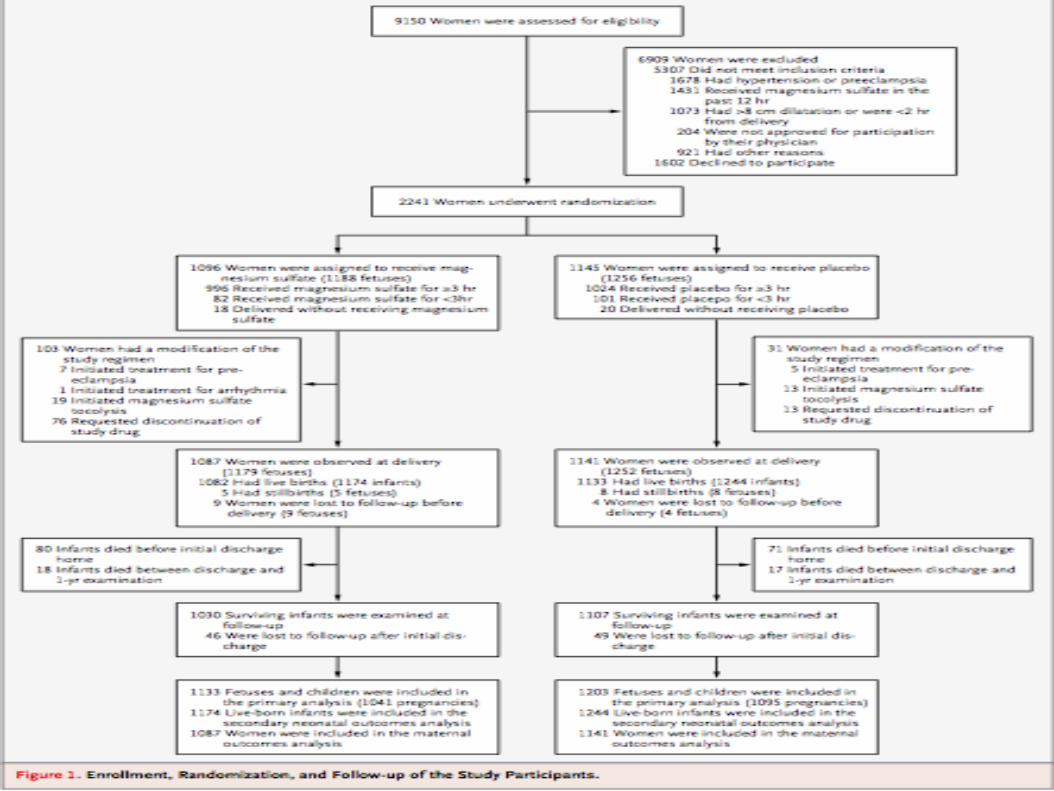
+ BEAM
Rouse, et al. 2008
“A Randomized, Controlled Trial of Magnesium Sulfate for the
Prevention of Cerebral Palsy” (Beneficial Effects of Antenatal
Magnesium Sulfate Trial)
Objective: test the hypothesis that the administration of
MgSO4 to women at high risk for early preterm delivery
would reduce the risk of CP in their children.
20 participating centers of NICHD MFMU
2241 women, singleton or twin gestations 24-31 wks.
MgSO4 administered as 6gm loading dose followed by
infusion of 2g/hr for up to 12 hours
if no delivery within 12 hours, MgSO4 was stopped, then
restarted if delivery was imminent
+ BEAM
Primary outcomes measured:
Composite of stillbirth or infant death by
1 year or moderate to severe CP at or
beyond 2 years
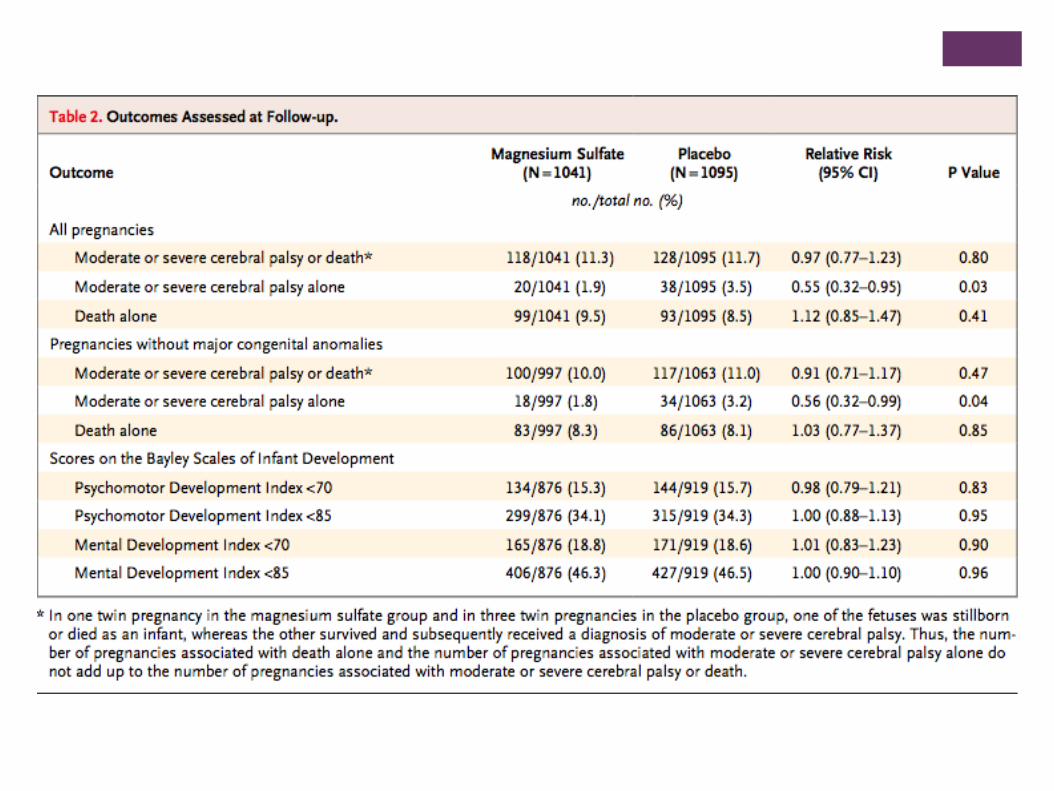
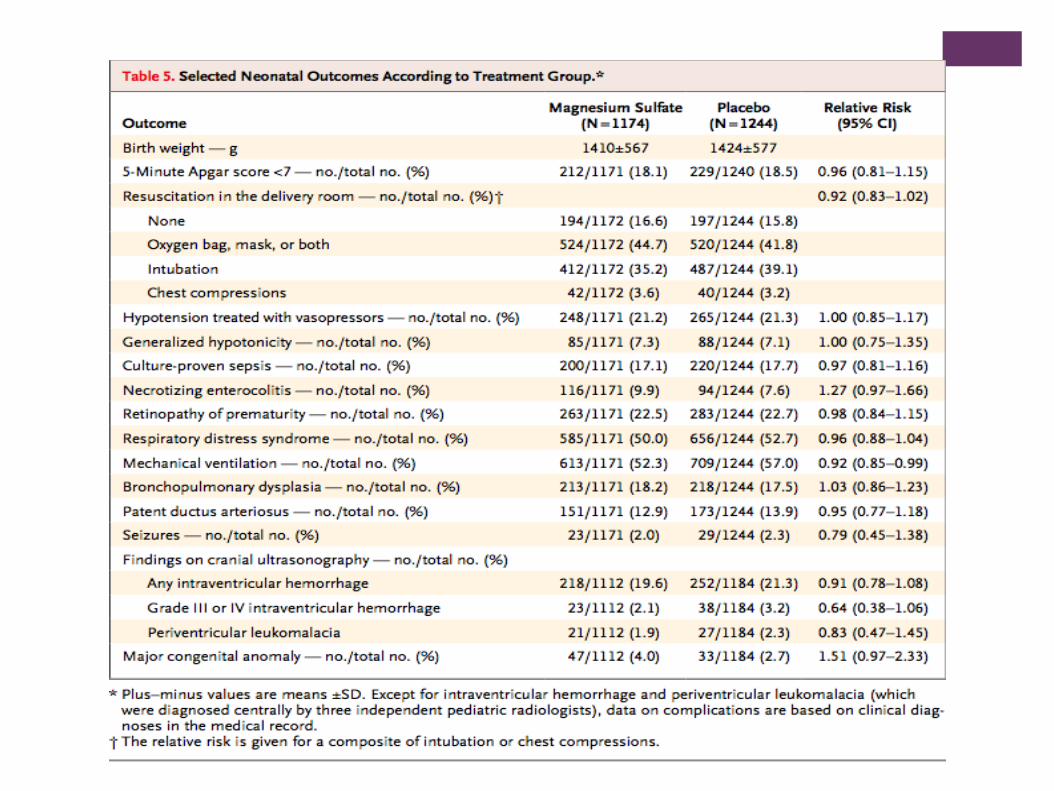
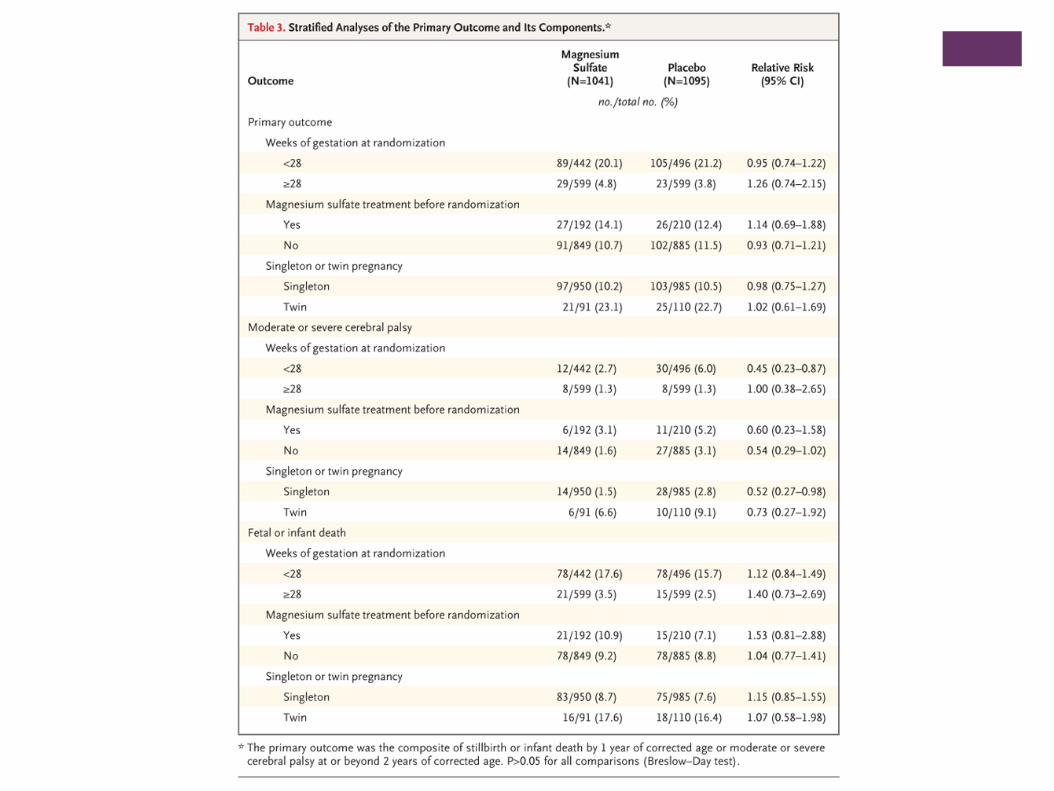
+ BEAM: Outcomes
The rate of the primary outcome was not significantly different
in the MgSO4 group and the placebo group (11.3% and
11.7%, respectively )
RR 0.97 95% CI 0.77-1.2
Prespecified secondary analysis: when mortality and CP
looked at separately, CP occurred significantly less frequently
in the MgSO4 group than the placebo group among surviving
children (1.9% vs 3.5%, respectively )
RR 0.55, 95% CI 0.32-0.95
+ Interpreting BEAM
Infants born <28 weeks had approximately same relative
risk reduction (RR 0.45, 95% CI 0.23-0.97)
Because of higher overall risk of this group, absolute risk
reduction is greater (2.7% in MgSO4 group vs. 6.1% in
placebo group)
Compared to a no difference in absolute risk if ≥28
weeks
NNT: 63 women to prevent one case of moderate to
severe CP, but 29 women to prevent one case among
infants 28 weeks or below
+ Interpreting BEAM: Criticisms
The composite outcomes are competing risk for the
outcome of interest, CP.
Infants who die before their first birthday cannot be
evaluated for CP.
How many of those infants that died at their first
birthday had CP?
Only 2 additional infants from the group who died in
those who received MgSO4 would have had to have
survived and been diagnosed with CP to lose statistical
significance
Unknown to most historians, William Tell had an older and
less fortunate son named Warren.
36
+ Meta-Analysis
Constantine M. and Weiner S., 2009
“Effects of Antenatal Exposure to Magnesium Sulfate on
Neuroprotection and Mortality in Preterm Infants: A
Meta-analysis”
Objective: To review the evidence regarding
neuroprotective effects of antenatal exposure to
MgSO4 and specifically explore the findings at
different gestational ages .
Two thresholds for analysis
Less than 32-34 wks
Less than 30 weeks
+ Meta-Analysis
Primary outcome:
Composite of perinatal/infant death or CP among
survivors
Secondary outcomes:
Death
CP
Moderate-severe CP
Combined death or moderate-severe CP
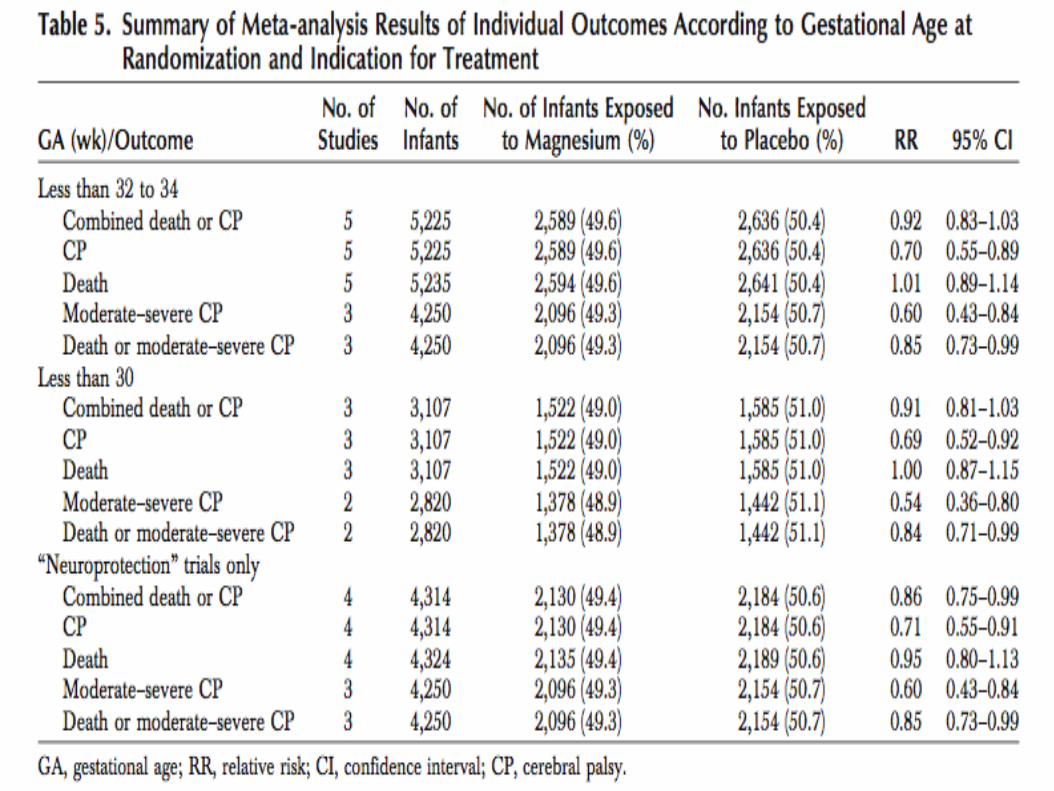
+ Meta-Analysis: Outcomes
In-utero fetal exposure to magnesium sulfate given to
women at risk of preterm delivery significantly reduced
the risk of cerebral palsy
NNT = 46 ( before 30 wks gestation )
NNT = 56 ( before 32-34 wks gestation )
No increase in the risk of perinatal or infant death
The benefit of using magnesium sulfate beyond 32-34
weeks for fetal neuroprotection is unproven.
+ Meta-Analysis
Strengths:
RCT’s specifically designed to study neuroprotective effects of
MgSO4
Reassurance of safety of MgSO4
Demonstrates beneficial effect of 32-34 wks, as well as less than 30
wks
Limitations:
MgSO4 regimen differed among trials
Dose received differed as well as timing
Differences in patient characteristics
+ The Cochrane Collaboration
Crowther, et al. 2009
“Magnesium sulphate for women at risk of
preterm birth for neuroprotection of the fetus
(Review)”
5 trials, 6145 babies were eligible for review
+ The Cochrane Collaboration:
Outcomes
MgSO4 therapy given to women at risk for preterm birth
substantially reduced:
risk of CP in their child (RR 0.68; 95% CI 0.54-0.87)
Rate if substantial gross motor dysfunction (RR 0.61; 95% CI 0.44-
0.85)
No statistically significant effect of antenatal MgSO4 therapy
on pediatric mortality
Plain language summary:
“Magnesium sulfate given to women at risk of preterm birth helps
to protect the baby’s brain and improve long-term outcomes.”
+ ACOG Committee Opinion:
Hot off the Press
“... none of the individual studies found a benefit with regard
to their primary outcome. However, the available evidence
suggests that MgSO4 given before anticipated early preterm
birth reduces the risk of CP in surviving infants.”
“Physicians electing to use MgSO4 for fetal neuroprotection
should develop specific guidelines regarding inclusion
criteria, treatment regimens, concurrent tocolysis and
monitoring in accordance with one of the larger trials.”
47
+ Protocol: Inclusion Criteria
Patients at Risk for Preterm Birth (PTB): all between 24
0/7-32 0/7 wks
Preterm Premature Rupture of Membranes (PPROM) patients with
clinical evidence of labor/imminent delivery
Preterm Labor with Advanced Cervical Dilation (ACD >4cm):
patients admitted at 24 0/7 to 32 0/7 weeks,
Anticipated, Indicated Preterm Delivery: maternal/fetal
indication(s) for preterm delivery within 2-12 hours
Should we look only at <28wks infants?
+ Protocol: Treatment Regimen
Magnesium Sulfate Administration for neuroprophylaxis
only
Initial Dose:
4 gram (gm) bolus given over 30 minutes, followed by
1 gm/hour (hr) continuous infusion x 12 hrs
Appropriate obstetric care, including delivery, should not be
delayed in order to complete 12 hrs of magnesium therapy
Note: our group uses MgSO4 as 1st line tocolytic agent at 6g
bolus to load, then titrate from 3g/hr for maintenance level x
48hr (thus we meet the minimum amount of Mg used for
neuroprophylaxis anyway)
+ Protocol: Treatment Regimen
Re-dose: (For patients who remain pregnant after the 12
hour initial infusion)
If > 6 hrs since last magnesium exposure, re-bolus with 4gm over
20-30 minutes, followed by 1gm/hr x 12 hours
If < 6hrs since last magnesium exposure, restart infusion at
1gm/hr x 12 hrs without a bolus
Typical reasons for re-dosing in the setting of PPROM
will be:
Induction
Non-reassuring fetal parameters with need for delivery suspected
Clinical suspicion for chorioamnionitis, leading to delivery
Threatened preterm labor/imminent delivery
+ Protocol: Concurrent Tocolysis
Magnesium sulfate may be used as the first-line tocolytic therapy in
patients with high clinical suspicion for imminent delivery. This
approach is aimed to avoid any delay in initiating magnesium sulfate
and to prevent concomitant exposure with calcium channel blockers
Nifedipine’s half-life is 2 hours so patients previously exposed to a
calcium channel blocker, for any indication, should be 4 hours out
from their last dose before magnesium sulfate, at any dose, is
initiated
+ References
Cahill A, Caughey A. Magnesium for neuroprophylaxis: fact or fiction? Am J Obstet
Gynecol 2009;200:590-4
Constantine M, Weiner J. Effects of Antenatal Exposure to Magnesium Sulfate on
Neuroprotection and Mortality in Preterm Infants, A Meta-analysis. Obstetrics and
Gynecology 2009;114:354-64
Crowther CA, Hiller JE, Doyle LW, Haslam RR. Effect of magnesium sulfate given for
neuroprotection before preterm birth: a randomized controlled trial. JAMA
2003;290:2669-76.
Grether JK, Nelson KB, Emery SE, Cummins SK. Prenatal and perinatal factors and
cerebral palsy in very low birth weight infants. J Pediatr 1996; 128:407-14.
Leviton A, Kuban KC, Pagano M, et al. Maternal toxemia and neonatal germinal
matrix hemorrhage in intubated infants less than 1751 grams. Obstet Gynecol 1988;
72:571-76
Magpie Trial Follow-Up Study Collaborative Group. The Magpie Trial: a randomised
trial comparing magnesium sulphate with placebo for pre-eclampsia. Outcome for
children at 18 months. BJOG 2007;114:289-99.
+ References
Marret S, Marpeau L, Zupan-Simunek V, Eurin D, Lévêque Hellot MF, et al. Magnesium
sulphate given before very-preterm birth to protect infant brain: the randomised
controlled PREMAG trial. BJOG 2007;114:310-8.
Marret S, Marpeau L, Follet-Bouhamed C, Cambonie G, Astruc D, Delaporte B, et al.
Effect ofmagnesium sulphate on mortality and neurologic morbidity of the very-
preterm new-born with two-year neurologic outcome: results of the prospective
PREMAG trial. Gynecol Obstet Fertil 2008;36:278-88.
Mittendorf R, Dambrosia J, Pryde PG, Lee KS, Gianopoulos JG, Besinger RE, et al.
Association between the use of antenatal magnesium sulfate in preterm labor and
adverse health outcomes in infants. Am J Obstet Gynecol 2002;186:1111-8.
Rouse DJ, Hirtz DG, Thom E, Varner MW, Spong CY, Mercer BM, et al. A randomized,
controlled trial of magnesium sulfate for the prevention of cerebral palsy. N Engl J
Med 2008;359:895-905
Van de Bor M, Verloove-Vanhorick SP, Brand R, et al. Incidence and prediction of
periventricular-intraventricular hemorrhage in very preterm infants. J Perinat Med
1987; 15:333-39.
+ Protocol: Consent and Monitoring
Please include the following elements in your verbal consent and
record in the patient chart that “the risks and benefits of magnesium
neuroprophylaxis were reviewed – patient accepts or declines
treatment”.
The risks for disabilities, and even death, are significant for infants
born at this early gestational age.
Recent data suggest that magnesium decreases, but does not
eliminate, the risk of cerebral palsy in children who survive. Given
this, we would like to offer you magnesium therapy.
We monitor women who receive magnesium closely to minimize
side effects of magnesium, which are commonly mild.
NICU will be informed of the use of magnesium sulfate prior to
delivery of preterm infant.