Magnesium preeclamptic rats - Cairo University...Full length article Magnesium sulfate versus...
7
Full length article Magnesium sulfate versus esomeprazole impact on the neonates of preeclamptic rats Amani N. Shafik a, *, Mahmoud A. Khattab a , Ahmed H. Osman b a Department of Medical Pharmacology, Faculty of Medicine, Cairo University, Egypt b Department of Pathology, Faculty of Veterinary Medicine, Cairo University, Egypt A R T I C L E I N F O Article history: Received 15 January 2018 Received in revised form 4 May 2018 Accepted 7 May 2018 Keywords: Esomeprazole Histopathology Magnesium sulfate Preeclampsia Neonate A B S T R A C T Objective: Preeclampsia represents a major complication of pregnancy, associated with greater maternal and fetal complications. We compared the effects of esomeprazole (a proton pump inhibitor) and magnesium sulfate (MgSO4) on the deleterious effects observed on the mother and neonates in experimentally induced preeclampsia in rats. Study design: Preeclampsia was induced in pregnant rats with NG-nitro-L-arginine methyl ester (L-NAME) starting from day 10-till end of pregnancy. Pregnant rats were divided into four groups: control pregnant; untreated preeclampsia; preeclamptic rats treated with MgSO4 and preeclamptic treated with esomeprazole. Treatment was started on day 14 and continued until end of pregnancy. Systolic blood pressure, gestation duration, the total number of pups/fetal resorption, pups birth weight, and histopathology examination of the pup’s organs were recorded. Results: In comparison with the L-NAME group, the MgSO4 and esomeprazole treatment reduced the values of systolic blood pressure; MgSO4 normalized gestational duration while esomeprazole prolonged it (post-term pregnancy); both restored number of delivered pups; with no statistical differences between the numbers of died pups between the four groups studied while with esomeprazole, out of 10 pregnant females, 2 of them had complete intrauterine fetal resorption; esomeprazole normalized birth weight and histological structure of fetal liver, kidney, and brain. On the other side, MgSO4 treatment gave rise to lower than normal birth weight and minimal tissue damage. Conclusion: Esomeprazole and MgSO4 improved systolic blood pressure, prevented preterm labor and restored numbers of pups delivered and fetal weight. Esomeprazole prolonged gestational period post- term with subsequent improving reproductive outcome. © 2018 Elsevier B.V. All rights reserved. Introduction One of the most serious complications of pregnancy is Preeclampsia (PE). Fetal complications are linked to the severity of PE. Clinicians are often forced to deliverearly preeclampsia mother to prevent major maternal morbidity, but in doing so, inflict severe prematurity on the fetus. The main impact on the fetus is low nutrition as a result of uteroplacental vascular insufficiency, which leads to growth restriction. Because oxidative stress and free radicals may play roles in several neonatal diseases, a direct effect of preeclampsia on the neonatal outcome is expected [1]. Magnesium may influence blood pressure by modulating vascular tone and structure, through its effects on various biochemical reactions that control vascular contraction/dilation, growth/apoptosis, differentiation, and inflammation. Magnesium may be physiologically important in blood pressure regulation whereas changes in magnesium levels could contribute to the etiology of hypertension [2]. Although Magnesium sulfate (MgSO4) is one of the main lines of treatment for preeclampsia, and is often used to prevent the progression from preeclampsia to eclampsia, it carries risk of fetal abnormalities as it is AU TGA and US FDA pregnancy category: D [3,4]. The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine have long supported the short-term use of MgSO4 in obstetric care for appropriate conditions and durations of treatment [4]. The preeclamptic placenta releases antiangiogenic soluble fms- like tyrosine kinase 1 (sFlt-1) and soluble endoglin (sEng) into the maternal circulation. These factors cause widespread maternal endothelial dysfunction and organ injury [5]. Esomeprazole is a proton pump inhibitor, US FDA pregnancy category B, widely used to treat women with gastric reflux in * Corresponding author at: 74A Tereet el zomor, Haram, Giza, 21511, Egypt. E-mail address: [email protected] (A.N. Shafik). https://doi.org/10.1016/j.ejogrb.2018.05.004 0301-2115/© 2018 Elsevier B.V. All rights reserved. European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242 Contents lists available at ScienceDirect European Journal of Obstetrics & Gynecology and Reproductive Biology journal homepage: www.else vie r.com/locat e/e jogrb
Transcript of Magnesium preeclamptic rats - Cairo University...Full length article Magnesium sulfate versus...

Full length article
Magnesium sulfate versus esomeprazole impact on the neonates ofpreeclamptic rats
Amani N. Shafika,*, Mahmoud A. Khattaba, Ahmed H. Osmanb
aDepartment of Medical Pharmacology, Faculty of Medicine, Cairo University, EgyptbDepartment of Pathology, Faculty of Veterinary Medicine, Cairo University, Egypt
A R T I C L E I N F O
Article history:Received 15 January 2018Received in revised form 4 May 2018Accepted 7 May 2018
Keywords:EsomeprazoleHistopathologyMagnesium sulfatePreeclampsiaNeonate
A B S T R A C T
Objective: Preeclampsia represents a major complication of pregnancy, associated with greater maternaland fetal complications. We compared the effects of esomeprazole (a proton pump inhibitor) andmagnesium sulfate (MgSO4) on the deleterious effects observed on the mother and neonates inexperimentally induced preeclampsia in rats.Study design: Preeclampsia was induced in pregnant rats with NG-nitro-L-arginine methyl ester (L-NAME)starting from day 10-till end of pregnancy. Pregnant rats were divided into four groups: control pregnant;untreated preeclampsia; preeclamptic rats treated with MgSO4 and preeclamptic treated withesomeprazole. Treatment was started on day 14 and continued until end of pregnancy. Systolic bloodpressure, gestation duration, the total number of pups/fetal resorption, pups birth weight, andhistopathology examination of the pup’s organs were recorded.Results: In comparison with the L-NAME group, the MgSO4 and esomeprazole treatment reduced thevalues of systolic blood pressure; MgSO4 normalized gestational duration while esomeprazole prolongedit (post-term pregnancy); both restored number of delivered pups; with no statistical differencesbetween the numbers of died pups between the four groups studied while with esomeprazole, out of 10pregnant females, 2 of them had complete intrauterine fetal resorption; esomeprazole normalized birthweight and histological structure of fetal liver, kidney, and brain. On the other side, MgSO4 treatmentgave rise to lower than normal birth weight and minimal tissue damage.Conclusion: Esomeprazole and MgSO4 improved systolic blood pressure, prevented preterm labor andrestored numbers of pups delivered and fetal weight. Esomeprazole prolonged gestational period post-term with subsequent improving reproductive outcome.
© 2018 Elsevier B.V. All rights reserved.
Introduction
One of the most serious complications of pregnancy isPreeclampsia (PE). Fetal complications are linked to the severity ofPE.Cliniciansareoftenforcedto deliverearly preeclampsiamothertoprevent major maternal morbidity, but in doing so, inflict severeprematurity on the fetus. The main impact on the fetus is lownutrition as a result of uteroplacental vascular insufficiency, whichleads to growth restriction. Because oxidative stress and free radicalsmay play roles in several neonatal diseases, a direct effect ofpreeclampsia on the neonatal outcome is expected [1].
Magnesium may influence blood pressure by modulatingvascular tone and structure, through its effects on variousbiochemical reactions that control vascular contraction/dilation,
growth/apoptosis, differentiation, and inflammation. Magnesiummay be physiologically important in blood pressure regulationwhereas changes in magnesium levels could contribute to theetiology of hypertension [2].
Although Magnesium sulfate (MgSO4) is one of the main linesof treatment for preeclampsia, and is often used to prevent theprogression from preeclampsia to eclampsia, it carries risk of fetalabnormalities as it is AU TGA and US FDA pregnancy category: D[3,4]. The American College of Obstetricians and Gynecologists andthe Society for Maternal-Fetal Medicine have long supported theshort-term use of MgSO4 in obstetric care for appropriateconditions and durations of treatment [4].
The preeclamptic placenta releases antiangiogenic soluble fms-like tyrosine kinase 1 (sFlt-1) and soluble endoglin (sEng) into thematernal circulation. These factors cause widespread maternalendothelial dysfunction and organ injury [5].
Esomeprazole is a proton pump inhibitor, US FDA pregnancycategory B, widely used to treat women with gastric reflux in
* Corresponding author at: 74A Tereet el zomor, Haram, Giza, 21511, Egypt.E-mail address: [email protected] (A.N. Shafik).
https://doi.org/10.1016/j.ejogrb.2018.05.0040301-2115/© 2018 Elsevier B.V. All rights reserved.
European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242
Contents lists available at ScienceDirect
European Journal of Obstetrics & Gynecology andReproductive Biology
journal homepage: www.else vie r .com/ locat e/e jogrb

pregnancy. Esomeprazole decreases secretion of sFlt-1 and sEngfrom placenta and endothelial cells, also has antioxidant propertiesand strongly minimizing endothelial dysfunction [6].
If a reasonable and safe treatment was available that couldhinder the progression of preeclampsia, clinicians could safelydelay delivery and improve fetal outcome.
The purpose of this study was to compare MgSO4 andesomeprazole administered from gestational day 14 until theend of pregnancy, on the improvements in blood pressure,gestational duration and fetal outcome of preeclamptic rats.
Methods
Animals and ethics statement
Adult females Sprague Dawley albino rats, 14–16 weeks old,weighing 180–200 g were used in this study. They were housed instandard laboratory conditions under a 12 h light/dark cycle andcontrolled temperature of 22 � 3 �C, with free access to food andwater. The study was approved by Cairo University, TheInstitutional Animal Care and Use Committee (CU-IACUC) withthe approval number “CU/III/S/6/16”.
Female rat’s conception
Prior to the experiment, the rats were acclimated to laboratoryconditions for 7 days. Females were placed with males overnightand examined the next morning for the presence of sperm invaginal smears. Day 0 of pregnancy was defined as the day whenspermatozoa were found in a vaginal smear [7].
Induction of PE and experimental design
Pregnant rats were treated from day 10 to the end of pregnancywith L-NAME (L-NAME powder, Elnasr Pharmaceutical Co, Egypt,dissolved in DW) 80 mg/kg/day by oral gavage [8]. Preeclampsiaonset was evident by a significant increase in blood pressure [9].Rats were divided into four groups (ten rats per group): controlpregnant rats; untreated preeclampsia; preeclamptic rats treatedwith MgSO4 (Magnesium sulfate powder, Hikma Egypt, dissolvedin DW) 500 mg/kg/day [10] by oral gavage and preeclamptic ratstreated with esomeprazole (Esomeprazole powder, Glaxo Well-come Egypt, dissolved in polyethylene glycol 400) 3.5 mg/kg/day[11] by oral gavage. Treatment was started on day 14 and continueduntil end of pregnancy.
Measurements
Blood pressure measurement
The systolic blood pressure (SBP) of each rat in different groupswas measured 5 times; at the start of the experiment, at thegestational days 9, 14, 17 and at the end of the experiment. The SBPwas measured non-invasively using a rat tail sphygmomanometer
(Panlab, USA). The SBP for each rat was calculated as the mean of atleast 3 readings.
Gestational duration
For every pregnant female rat in each group, gestationalduration was estimated in days starting from gestational day 0 (dayof detection of sperms in vaginal smear) till the end of pregnancy.
Total number of pups/Fetal resorption
After delivery, the total number of pups (living and died) andfetal resorption for each pregnant female rat in each group wasestimated.
Pups birth weight
After delivery, pups birth weight was estimated in gram.
Histopathology examination of the pup’s organs
Pups were euthanized and their liver, kidneys, and brain tissuespecimens were fixed in 10% formol saline, then trimmed off,washed and dehydrated in ascending grades of alcohol. Thedehydrated specimens were then cleared in xylene, embedded inparaffin blocks and sectioned at 4–6 mm thick. The obtained tissuesections were deparaffinized using xylol and stained usinghematoxylin and eosin (H&E) for histopathological examinationthrough the electric light microscope [12].
Statistical analysis
Data were coded and entered using the statistical package SPSSversion 24. Data were summarized using mean and standard errorof the mean (SEM) in quantitative data and using frequency (count)and relative frequency (percentage) for categorical data.
Comparisons between groups were done using ANOVA withpost hoc test in normally distributed quantitative variables whilenon-parametric Kruskal-Wallis test and Mann-Whitney test wereused for non-normally distributed quantitative variables [13]. Forcomparison of serial measurements within each group repeatedmeasures ANOVA was used in normally distributed quantitativevariables while non-parametric Friedman test was used for thenon-normally distributed quantitative variable [14]. For comparingcategorical data, Chi-square (x2) test was performed. An exact testwas used instead when the expected frequency is less than 5 [15].P-values less than 0.05 were considered as statistically significant.
Results
Gestational duration
Gestational duration was decreased significantly in preeclamp-tic untreated rats compared to the other groups; treated with
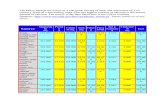
Table 1Gestational duration measured in days for every pregnant female rat (n = 10) in each group starting from gestational day 0 till the end of pregnancy.**p < 0.05: significant increase compared to untreated preeclampsia group.***p < 0.05: significant increase compared to preeclampsia group treated with MgSO4.
Groups Studied
Gestational duration (mean � SEM//days) Control pregnant Untreated preeclampsia Preeclampsia+ MgSO4 Preeclampsia+ Esomeprazole21.20 � 0.20 16.60 � 0.16* 21.10 � 0.31** 24.30 � 0.86 *,**,***
*p < 0.05: significant compared to control pregnant rats.**p < 0.05: significant increase compared to untreated preeclampsia group.***p < 0.05: significant increase compared to preeclampsia group treated with MgSO4.
A.N. Shafik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242 237

MgSO4 showed normalization of gestational duration; whilepreeclamptic rats treated with esomeprazole showed a significantincrease in gestational duration (post-term pregnancy) (Table 1).
Systolic blood pressure
In response to L-NAME, SBP started to rise significantly ongestational day 14 (4 days after induction with L-NAME) inpreeclamptic groups till the end of pregnancy (Graph 1). Therewas significant decrease (p < 0.05) in SBP values in bothpreeclamptic groups treated with MgSO4 and those treated withesomeprazole with an insignificant difference.
Total number of pups/Fetal resorption
Preeclamptic untreated rats delivered a lower number of pups;while those treated with MgSO4 and esomeprazole showed astatistically significant increase in the total number of pups withno significant difference in between and to control (Table 2).
The number of died pups was nearly the same between the fourgroups studied (Table 2).
Out of 10 pregnant females in preeclamptic group treated withesomeprazole, 2 of them had complete intrauterine fetalresorption.
Pups birth weight
Pups birth weight of untreated preeclamptic rats and thosetreated with MgSO4 was decreased significantly; While birthweights of pups delivered from preeclamptic rats treated with
esomeprazole were significantly increased compared to untreatedpreeclampsia and preeclamptic rats treated with MgSO4 (Table 3).
Histopathology examination of the pups
Pups from control pregnant mothersLight microscopic examination of neonatal livers of control
pregnant mother showed ill-defined demarcation of hepaticlobules and the inter-lobular connective tissue was poorlydeveloped. In each hepatic lobule, hepatocytes were arranged asirregular, branching and interconnected cords originating from acentral vein and go peripherally. Blood sinusoids were seen in-between the hepatic cords. The quantity of hepatocytes appearedgreater than hepatoblasts which have large nucleus basophilicwith little cytoplasm. The liver also had hematopoietic functioncharacterized by the presence of hematopoietic progenitor cellsand megakaryocyte lineage cells. Erythroblasts and Kupffer cellswithin sinusoids also were also seen (Fig. 1a).
The kidneys were bilaterally present and normal in shape in allpups of this group. On histological examination, the sagittal sectionof kidneys showed well developed cortical renal corpuscles; thesecontained loops of glomerular capillaries, surrounded by Bow-man’s capsule, having visceral and parietal layers and lined bysimple squamous epithelium, with capsular space in-between. Thecortical region also showed cross-section of proximal and distalconvoluted tubules lined by simple cuboidal epithelium. All thesestructures were embedded in the interstitium (Fig. 1b).
Brain tissue section of pups of the control group showed anincomplete development of brain architecture. The neuronal cellsappeared clear with a prominent basophilic nucleus (Fig. 1c). The
Graph 1. Mean Systolic Blood Pressure (mmHg, ANOVA)) measurements in all groups throughout gestational period (n = 10).*p < 0.05: significant increase compared to control pregnant rats# p < 0.05: significant decrease compared to untreated preeclampsia group
Table 2Total number of pups/Intra uterine Fetal resorption for each pregnant female rat (n = 10) in each grup.
(mean �SEM) Groups Studied
control pregnant Untreated preeclampsia Preeclampsia + MgSO4 Preeclampsia + Esomeprazole
Total number of pups 8.30 � 0.56 4.40 � 0.43* 7.44 � 0.29** 7.71 � 0.57**
Number of died pups 0. 0.40 � 0.22 0.80 � 0.70 0Intrauterine resorption 0 0 0 2
* p < 0.05: significant decrease compared to control pregnant rats.** p < 0.05: significant increased compared to untreated preeclampsia.
238 A.N. Shafik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242

histological findings in this group were recorded in all full-term ratoffspring and complete development of brain tissue occurredduring the first two weeks of life.
Pups from untreated preeclamptic motherNeonatal liver delivered from untreated preeclamptic mother
showed ill developed hepatic lobules with distorted hepatic cords.The hepatocytes were bloated with large, spherical droplets of fatin a focal and/or diffuse manner. The quantity of hepatoblastsappeared greater than hepatocytes. Apoptosis of hepatic cells withcomplete depletion of hematopoietic progenitor cells (Fig. 2a).
Kidneys appeared oedematous, pale and doughy. On histologi-cal examination, the sagittal section of kidney revealed illdeveloped renal corpuscles that is composed of few numbers ofcapillaries loops and surrounded by Bowman's capsule. The renaltubules showed coagulative necrosis of its epithelial lining withintact basement membrane (Fig. 2b).
Histological section of brain tissue specimens showed spon-giosis consisted of irregular clear spaces in both gray and whitematter. Neurons were shrunken and darkly stained with a smallnucleus, with a significant reduction in cell density (Fig. 2c).
Pups of preeclamptic mother treated with MgSO4The structure of hepatic parenchyma appeared resembling to
control group. The quantity of hepatocytes greater than hepato-blasts was seen. Blood spaces contained hematopoietic progenitorcells and Kupffer cells were also noticed. The hepatic lobulesshowed a fewer number of apoptotic bodies in comparison withuntreated and treated by esomeprazole groups (Fig. 3a).
Kidneys of this animal group showed a slight increase in size.The sagittal tissue section showed glomeruli with partial andvisceral layers with ill-developed glomerular tufts. The renaltubules lined by simple cuboidal epithelium. Some tubules showeddamage to its basement membrane with intra-tubular cellulardebris (Fig. 3b).
Brain tissue section appeared resembling control group withoutspongiosis and reduction of neuronal cells (Fig. 3c).
Pups of preeclamptic mother treated with esomeprazoleThe hepatic parenchyma showed many lobules with disorgani-
zation of hepatic cords with irregular blood spaces containedhematopoietic progenitor cells and Kupffer cells. Few hepatoblastsand apoptosis of few hepatocytes also were seen (Fig. 4a).
The pathological finding of renal tissue of this group revealedsimilar alterations seen in Pups of preeclamptic mother treatedwith MgSO4 (Fig. 4b).
Brain tissue section showed mild spongiosis in compared withuntreated group. Also, the neuronal cells population like controlgroup (Fig. 4c).
Discussion
The current curative treatment for preeclampsia is delivery of theplacenta as this removes the source of placental-derived factorsresponsible for the maternal organ injury. In preterm preeclampsia,clinicians are often forced to deliver the fetus preterm to save themother [16]. A treatment that quenches the severity of the maternaldisease could allow these pregnancies to safely advance to agestation where neonatal outcomes are significantly improved.
The present study reveals that L-NAME administration resultedin the increase in SBP, preterm labor, deleterious effect on the totalnumber of pups and their fetal birth weight. Placental ischemiaand hypo-perfusion were reflected in pups’ kidneys, hepatocytesand brain tissues.
Treatment with MgSO4 decreased SBP, prevented pretermlabor, and avoided the deleterious effects on the total number ofpups and fetal birth weight. Relaxation of the arterial blood vesseland the increase of placental blood flow were reflected on fetaldevelopment which appeared histologically as increase in quantityof hepatocytes than hepatoblasts and blood spaces that contained
Table 3Pups weight in gram delivered from different groups studied (n = 10).
Groups studied
control pregnant Untreated preeclampsia Preeclampsia + MgSO4 Preeclampsia +Esomeprazole
Pups Weight(mean �SEM/gm) 3.23 � 0.03 1.54 � 0.06 * 2.78 � 0.05 *,** 3.15 � 0.03 **,***
* p < 0.05: significant decrease compared to control pregnant.** p < 0.05: significant increase compared to untreated preeclampsia rats.*** p < 0.05: significant increase compared to preeclampsia rats treated with MgSO4.
Fig. 1. Tissue pathology from pups of control mother (H&Ex200).a. Hepatic tissue section showing hepatic cords and sinusoids contained erythroblasts and Kupffer cells.b. Sagittal section of kidney showing a part of the cortical region containing glomerulus within Bowman's capsule and renal tubules.c. Brain tissue showing neuronal cells appeared clear with prominent basophilic nucleus.
A.N. Shafik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242 239

Fig. 3. Tissue pathology from pups of Pre-eclamptic mother treated with MgSO4 (H&Ex200).a. Hepatic tissue section showing few number of apoptotic bodies.b. Sagittal section of kidney showing a part of the cortical region containing glomerulus within Bowman's capsule and renal tubules.c. Brain tissue showing neuronal cells appeared clear with prominent basophilic nucleus.
Fig. 4. Tissue pathology from pups of Pre-eclamptic mother treated with esomeprazole (H&Ex200).a. Hepatic tissue section showing disorganized hepatic cords with irregular blood spaces contained hematopoietic progenitor cells.b. Sagittal section of kidney showing glomeruli with partial and visceral layers with ill developed glomerular tufts.c. Brain tissue showing mild spongiosis.
Fig. 2. Tissue pathology from pups of Untreated Pre-eclamptic mother (H&Ex200).a. Hepatic tissue section showing vacuolation and apoptosis of hepatocytes.b. Sagittal section of kidney showing ill developed renal corpuscles and necrosis of renal tubules.c. Brain tissue showing spongiosis consisted of irregular clear spaces.
240 A.N. Shafik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242

active hematopoietic progenitor cells. Brain tissue sectionappeared resembling control normal group without evidence ofany damage.
The disturbance in proangiogenic and antiangiogenic factors isreported in preeclamptic pregnancies and is considered the maincause of the endothelial dysfunction. Placental ischemia andhypoperfusion decrease placental growth factor (PlGF) andproduce high concentrations of soluble vascular endothelialgrowth factor receptor-1 (sVEGFR-1), and the transmembraneglycoprotein endoglin (ENG) [17]. Increased VEGF augments nitricoxide (NO) production that was found to have an important role inthe mitogenic effect of VEGF during angiogenesis.
Nitric oxide and endothelin-1 are important endotheliumderived mediators of vascular tone. NO system may play a rolein the regulation of myometrial contractility, and that inappropri-ate synthesis of this mediator may trigger preterm delivery.Notably, the contractility of pregnant rat uterus was inhibited byNO and its precursor L-arginine [18]. NO generation would be up-regulated in myometrium and down-regulated in the cervix,assuring uterine relaxation and cervical competence, the oppositeeffects would occur during labor leading to myometrial contractionand cervical ripening. .L-NAME treatment during pregnancy in ratscauses eNOS inhibition that led to the reduction of NO whichparticipates in the cardiovascular adaptation that occurs in anormal pregnancy [19], so vasoconstriction occurs and subsequenthypertension developed, also early myometrial contraction andcervical ripening with subsequent preterm labor [20].
There are many short- and long-term consequences ofpreeclampsia to the offspring [21].; fetal health as well as itsweight, is highly compromised, leading to various degrees of fetalmorbidity, and fetal damage may be such as to cause fetal death. Inlater life, babies with intrauterine growth restriction (IGR) aremore likely to develop chronic diseases.
Magnesium is a unique calcium antagonist as it can act on mosttypes of calcium channels in vascular smooth muscle by inhibitingCa2+ influx leading to inactivation of calmodulin-dependent myosinlight chain kinase activity and decreased contraction [22,23].
Magnesium may act by stimulating the production of prosta-cyclin by endothelial cells causing vasodilation, or by inhibitingplatelet aggregation. In patients with pregnancy-induced hyper-tension [22], MgSO4 treatment significantly decreased circulatinglevels of the angiotensin-converting enzyme. These actions mayattenuate the endothelial dysfunction associated with preeclamp-sia. The endothelium appears to potentiate the vasorelaxant effectsof magnesium through the nitric oxide-cyclic GMP and cyclooxy-genase systems and prevent preterm labor [24].
In 2008, Rouse and colleagues [25] randomized MgSO4infusions or placebo in 2241 women delivered between 24 and31 weeks' gestation in a study of the effects of MgSO4 on perinataldeath and/or cerebral palsy at 2 years of age. MgSO4 therapy wasnot found to be associated with perinatal death, neonatalhypotonia, or any other neonatal morbidity. Such therapy,however, was associated with a significant reduction in cerebralpalsy, especially in infants born between 24 and 27 weeks'gestation.
Esomeprazole significantly improved SBP, prolonged thegestational duration, prevented the deleterious effect on the totalnumber of pups, fetal birth weight. The histological structure offetal vital organs appeared in normal architecture without anysignificant pathological alterations.
Onda et al. [6] induced mouse model of preeclampsia andstudied the effect of esomeprazole that was completely abrogatedan increase in blood pressure. Esomeprazole potently vasodilatedwhole maternal blood vessels and reduced blood pressure in ananimal model of preeclampsia [26].
Like sFlt-1, sENG also antagonizes endothelial receptor signal-ing by competing with full-length endoglin, decreasing its abilityto bind with its co-receptors to maintain vessel homeostasis,causing widespread maternal endothelial dysfunction and organinjury. Preeclampsia is also associated with oxidative stress.
Esomeprazole, a proton pump inhibitor decreases secretion ofsFlt-1 and sENG from primary trophoblast, placental explants fromnormal and preeclamptic pregnancies, and from 2 types of primaryendothelial cells. Esomeprazole vasodilates human vessels fromnormal and preeclamptic pregnancies and reduces blood pressure[6]. The ability of esomeprazole to dilate vessels and reduce bloodpressure may be mediated through the endothelium, perhaps byincreasing p-eNOS expression. PPIs seem to block endothelialdysfunction in vitro assays and upregulate endogenous antioxidantmolecules and decrease secretion of cytokines from placentaltissues and endothelial cells [6].
Esomeprazole showed significant improvement in reproductiveoutcome through reduction in sEng levels. Maynard et al. [27]explained that serum sEng may be a cause of the low-birth-weightbabies in multiple gestation pregnancies.
Esomeprazol has the advantages that it is available in oral formand is pregnancy category B. If esomeprazole is proven to beeffective at prolonging gestation in early onset preeclampsia withimprovement in reproductive outcome, it would be the firsttreatment option for this group of vulnerable mothers and couldplay an important role in decreasing the unfavourable outcomes.
Conclusion
Both MgSO4 and esomeprazole prevented deleterious effects ofpreeclampsia on both maternal and fetal outcome. Superior efficacywas noted with esomeprazole in prolongation of gestationalduration and increase in fetal birth weight. Further experimentaland clinical studies are recommended to evaluate the efficacy ofesomeprazole in the reduction of neonatal complications resultingfrom preeclampsia and prevention of eclampsia.
References
[1] Backes C.H., Markham K, Moorehead P, Cordero L, Nankervis CA, Giannone PJ.Maternal preeclampsia and neonatal outcomes. J Pregnancy 2011;2011:7.
[2] Adekanle DA, Adeyemo OT, Adeniyi AA, Okere RA, Jimoh AK, Adebara IO, et al.Serum magnesium levels in healthy pregnant and pre-eclamptic patients. Across-Section study. Open J Obstetr Gynecol 2014;04(09):8.
[3] Nagaria T, Mitra S, Banjare SP. Single loading low dose MgSo(4) regimen: asimple, safe and effective alternative to pritchard’s regimen for indian women.J Clin Diagn Res: JCDR 2017;11(8):QC08–12.
[4] The American College of Obstetricians and Gynecologists. Committee opinionNo 652: magnesium sulfate use in obstetrics. Obstet Gynecol 2016;127(1):e52–3.
[5] Leaños-Miranda A, Campos-Galicia I, Berumen-Lechuga MG, Molina-Pérez CJ,García-Paleta Y, Isordia-Salas I, Ramírez-Valenzuela KL. Circulating angiogenicfactors and the risk of preeclampsia in systemic lupus erythematosuspregnancies. J Rheumatol 2018 May 15:jrheum-141571..
[6] Onda K, Tong S, Beard S, Binder N, Muto M, Senadheera SN, et al. Proton pumpinhibitors decrease soluble fms-like tyrosine kinase-1 and soluble endoglinsecretion, decrease hypertension, and rescue endothelial dysfunction.Hypertension 2017;69(3):457.
[7] Shah M, Singh R, Shah R, Kakar S. An overview of the current methodologiesused for evaluation of anti-fertility agents. Asian Pac J Reprod 2016;5(3):175–8.
[8] Takiuti NH, Carvalho MHC, Kahhale S, Nigro D, Barbeiro HV, Zugaib M. Theeffect of chronic nitric oxide inhibition on vascular reactivity and bloodpressure in pregnant rats. Sao Paulo Med J 1999;117:197–204.
[9] de Souza CO, Peraçoli MTS, Weel IC, Bannwart CF, Romão M, Nakaira-TakahagiÉ, et al. Hepatoprotective and anti-inflammatory effects of silibinin onexperimental preeclampsia induced by l-NAME in rats. Life Sci 2012;91(5):159–65.
[10] Korish AA. Magnesium sulfate therapy of preeclampsia: an old tool with newmechanism of action and prospect in management and prophylaxis. Hyper-tens Res 2012;35:1005.
[11] Swamy VKM, Setty RS, Shankaraiah MM, Jyothi TM, Rajendra SV. A study ondrug-Drug interaction of esomeprazole and anti-diabetic drugs. J YoungPharm: JYP 2010;2(4):424–7.
A.N. Shafik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242 241

[12] Bancroft JD, Floyd AD, Suvarna SK. Bancroft's Theory and Practice ofHistological Techniques. 2013.
[13] Chan Y. Biostatistics 102: quantitative data–parametric & non-parametrictests. blood pressure. Singapore Med J 2003140(24.08) 79.00.
[14] Chan Y. Biostatistics 301. repeated measurement analysis. Singapore Med J2004;45:354–69.
[15] Chan Y. Biostatistics 103: qualitative data-tests of independence. SingaporeMed J 2003;44(10):498–503.
[16] Wang Y, Hao M, Sampson S, Xia J. Elective delivery versus expectantmanagement for pre-eclampsia: a meta-analysis of RCTs. Arch Gynecol Obstet2017;295(3):607–22.
[17] Harapan H, Yeni CM. The role of microRNAs on angiogenesis and vascularpressure in preeclampsia: the evidence from systematic review. Egypt J MedHum Genet 2015;16(4):313–25.
[18] George EM, Granger JP. Mechanisms and potential therapies for preeclampsia.Curr Hypertens Rep 2011;13(4):269–75.
[19] Tiboni GM, Giampietro F. Inhibition of nitric oxide synthesis causes pretermdelivery in the mouse. Hum Reprod 2000;15(8):1838–42.
[20] Dzeshka MS, Shantsila A, Lip GYH. Effects of aspirin on endothelial functionand hypertension. Curr Hypertens Rep 2016;18(11):83.
[21] Hakim J, Senterman MK, Hakim AM. Preeclampsia is a biomarker for vasculardisease in both mother and child: the need for a medical alert system. Int JPediatr 2013;2013:8.
[22] Euser AG, Cipolla MJ. Magnesium sulfate treatment for the prevention ofeclampsia: a brief review. Stroke 2009;40(4):1169–75.
[23] Altura BM, Altura BT, Carella A, Gebrewold A, Murakawa T, Nishio A. Mg2+-Ca2+ interaction in contractility of vascular smooth muscle: mg2+ versus organiccalcium channel blockers on myogenic tone and agonist-induced responsive-ness of blood vessels. Can J Physiol Pharmacol 1987;65(4):729–45.
[24] Abbassi-GhanavatiM,Alexander JM,McIntireDD,SavaniRC,LevenoKJ.Neonataleffectsof magnesium sulfate given to the mother. Am J Perinatol 2012;29(10):795–800.
[25] Rouse DJ, Hirtz DG, Thom E. A randomized, controlled trial of magnesiumsulfate for the prevention of cerebral palsy. N Engl J Med 2008;359:895–905.
[26] Powe CE, Levine RJ, Karumanchi SA. Preeclampsia, a disease of the maternalendothelium: the role of anti-angiogenic factors and implications for latercardiovascular disease. Circulation 2011123(24), doi:http://dx.doi.org/10.1161/CIRCULATIONAHA.109.853127.
[27] Maynard SE, Moore Simas TA, Bur L, Crawford SL, Solitro MJ, Meyer BA. Solubleendoglin for the prediction of preeclampsia in a high risk cohort. HypertensPregnancy 2010;29(3):330–41.
242 A.N. Shafik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 225 (2018) 236–242


















