Maddox i npwt ab wall presentation v1.8
14
INCISIONAL NEGATIVE PRESSURE WOUND THERAPY IS ASSOCIATED WITH INCREASED WOUND PERFUSION IN ABDOMINAL WALL RECONSTRUCTION: A CASE SERIES John Maddox, MD John S Maddox MD 2 , Bryan Buckingham MD 1 , Victor Wong MD 1 , Karan Chopra MD 1 , Devinder P. Singh MD 1 1. Division of Plastic Surgery, University of Maryland School of Medicine 2. Department of General Surgery, Walter Reed National Military Medical Center
-
Upload
kchoprakaran -
Category
Documents
-
view
49 -
download
3
Transcript of Maddox i npwt ab wall presentation v1.8

INCISIONAL NEGATIVE PRESSURE WOUND THERAPY IS ASSOCIATED WITH INCREASED WOUND PERFUSION IN ABDOMINAL WALL RECONSTRUCTION: A CASE SERIES
John Maddox, MD
John S Maddox MD2, Bryan Buckingham MD1, Victor Wong MD1, Karan Chopra MD1, Devinder P. Singh MD1
1. Division of Plastic Surgery, University of Maryland School of Medicine2. Department of General Surgery, Walter Reed National Military Medical Center

Disclosures and Disclaimer
• Dr. Devinder Singh is a consultant for LifeCell Corporation/Kinetic Concepts Incorporated otherwise no disclosures for John Maddox or the remainder of the research team.
• The views expressed in this presentation are those of the author and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or U.S. Government.

Background
• Negative pressure wound therapy– initially described for use on open wounds (1,2)– improves healing and decreases the number of complications (1,2)
• Application of negative pressure dressings onto closed surgical incisions– significant reduction in wound dehiscence, surgical site infection, and
hematoma. (3)– Improved outcome in patients at high risk for surgical wound complications
after abdominal wall reconstruction. (4)
1. Morykwas et al., Ann Plast Surg. 1997; 38: 553-5622. Argenta et al., Ann Plast Surg 1997;38:563-5763. Condé-Green et al., Ann Plast Surg 2013;71:394-3974. Vargo D., Am J Surg 2012;204:1021-1024

Background
• Mechanism – Definitive mechanism of efficacy for incisional negative pressure wound
therapy (iNPWT) is not yet known • Modulation of the incisional healing environment (5)• Reduction in tension at wound margins (6) • Incisional fluid management (7)• Protected wound healing environment (8)• Changes in blood flow (7,9)
• We routinely use indocyanine green angiography for abdominal wall reconstruction
– anecdotally noted increased tissue perfusion at the wound edges.
5. Lancero et al. , Sem in Cell and Dev Biology 2013;23:987-9926. Wilkes et al., Surg Inovations 2012 ;19(1):67-757. Moues et al., Am J Surg 2011;201:544-5568. Gomoll et al., J Orthop Trauma 2006;20:705-7099. Timmers et al. Ann Plast Surg. 2005 Dec;55(6):665-71.
Hypothesis
• There is an increase in tissue perfusion with the use of incisional NPWT dressings, such as Prevena. This increase may be quantifiable using ICG angiography, and may contribute to the improved complication profile.

Materials and Methods
• Retrospective case review of 5 patients – components separation abdominal wall reconstruction for massive hernia
repair – single surgeon (Dr Devinder Singh)– reconstructed with an acellular dermal matrix on lay of the fascia. – Abdominal wounds were evaluated by ICG angiography using the SPY elite
system.– Incisional NPWT dressings were removed on post-operative day 6. – Repeat bedside ICG angiography upon removal of NPWT dressing. – Student’s T test for comparison of per and post operative fluorescence.

Results:
Patient
Change in absolute
fluorescence
P value BMI ASA Class
VHRS SSI
Wound Class
Complications
1 55.5 <0.001 28.5 1 4 Clean Cont
None
2 32.9 0.008 42 3 7 Clean Cont
DVT, PE, Wound AbscessWound Seroma
3 10.5 0.24 23 2 4 Clean Cont
None
4 20.25 <0.001 27 2 4 Clean None
5 82.1 <0.001 19.9 3 6 Clean Ileocolic anastamotic leak and intrabdominal abscess adjacent to abdominal terminus of VP shunt
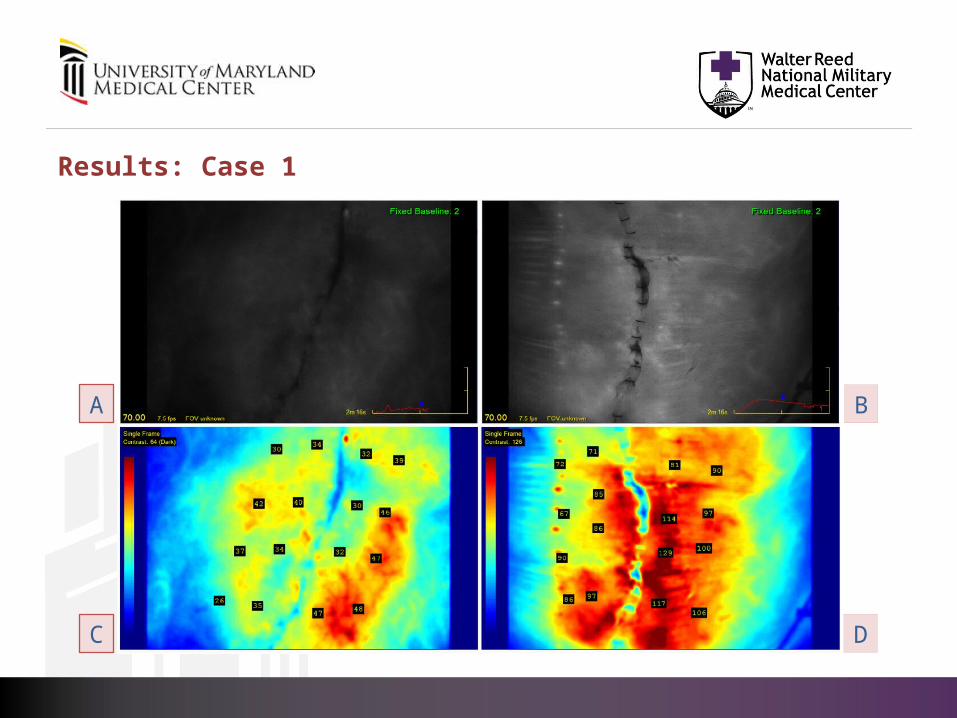
Results: Case 1
A B
C D
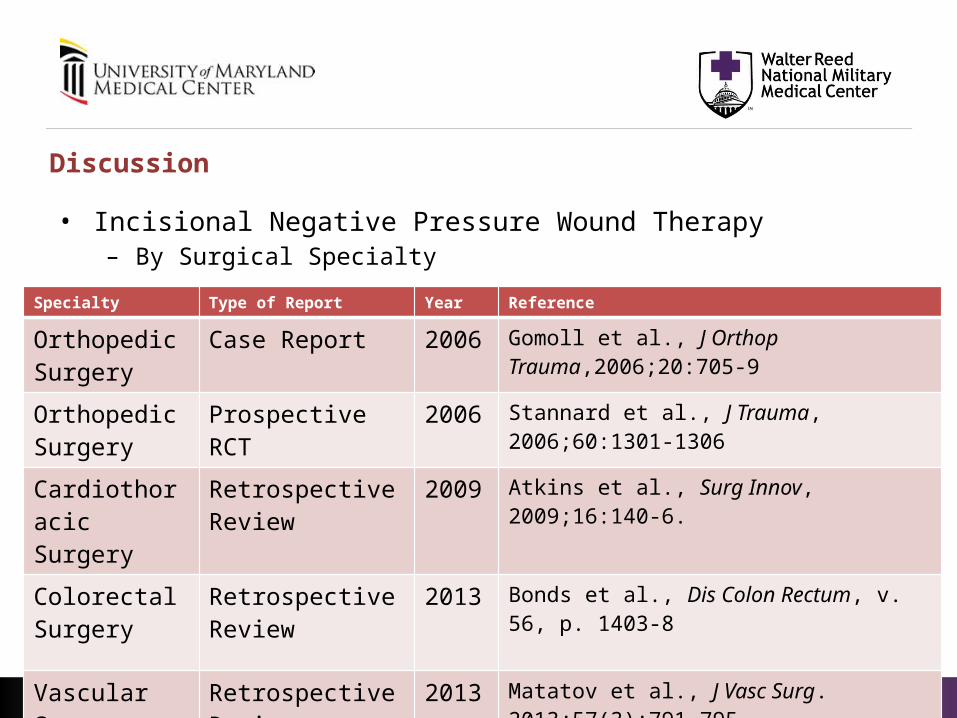
Discussion
• Incisional Negative Pressure Wound Therapy – By Surgical Specialty
Specialty Type of Report Year Reference
Orthopedic Surgery
Case Report 2006 Gomoll et al., J Orthop Trauma,2006;20:705-9
Orthopedic Surgery
Prospective RCT 2006 Stannard et al., J Trauma, 2006;60:1301-1306
Cardiothoracic Surgery
Retrospective Review
2009 Atkins et al., Surg Innov, 2009;16:140-6.
Colorectal Surgery
Retrospective Review
2013 Bonds et al., Dis Colon Rectum, v. 56, p. 1403-8
Vascular Surgery
Retrospective Review
2013 Matatov et al., J Vasc Surg. 2013;57(3):791-795

Discussion
• Recent studies and reviews report wound healing improvement• Abdominal wall reconstruction (10)
– Lower overall wound complication and dehiscence rates with iNPWT• Wound complications 22% versus 64% (p = 0.020) • Dehiscence 9% versus 39% ( p = 0.014)
• High risk lower extremity orthopedic blunt trauma (11)– Reduced infection and dehiscence rate
• Infection rate 9.9% versus 18.9% ( p = 0.049) • Dehiscence rate 8.6% versus 16.5% (p = 0.044)
• Reported improvements in edema, fluid collections within the closed incisions, and incidence of hematoma in patients treated with incisional NPWT require further study (12)
10. Condé-Green et al., Ann Plast Surg 2013;71:394-39711. Stannard et al., J Orthop Trauma 2012;26:37-4212. Ingargiola et al., Eplasty 2013;13:e49
• The mechanism by which NPWT effects the healing of open and closed wounds is believed to be multifactorial but the specific mechanisms are not fully elucidated.– Fluid model
• removal of excessive interstitial fluid containing inflammatory mediators such as matrix metalloproteinases (13)
– Mechanical model • micro and macro deformation at the wound surface causing effects similar to tissue
expansion with the release of growth factors (13)– Blood flow model
• Improvement in microvascular blood flow (14)
13. Lancero et al. Sem in Cell and Dev Biology 2013;23:987-99214. Timmers M., et. al. Ann Plast Surg. 2005 Dec;55(6):665-71.
Discussion
• Four of our five patients treated with incisional NPWT showed a statistically significant increase in absolute fluorescence measured by indocyanine green angiography (p range <0.001 to 0.008).
• Limitations and other physiologic mechanisms considered. – Retrospective uncontrolled case series
• Absolute vs relative fluorescence • No objective sampling protocol
– Early engraftment • Controlled for with matrix on lay reconstruction
– Delay phenomenon • Clinical benefit 7 – 14 days postoperatively

Conclusions
• An increase in wound edge perfusion was observed with incisional NPWT dressing use that may contribute to the improved wound healing and complication profile previously reported. Despite the limitations, this case series illustrates an intriguing observation and opens an avenue for our future plans for research.

Future directions
• A prospective randomized controlled open label study of incisional NPWT dressings and wound edge perfusion in abdominal wall reconstruction patients following massive hernia repair is in development.


















