
MACRA… What is it? Why Do I Need to Be in the Know? · MACRA… What is it? Why Do I Need to Be...
74
MACRA… What is it? Why Do I Need to Be in the Know? Jim Brulé, Solutions Director - Regulatory
Transcript of MACRA… What is it? Why Do I Need to Be in the Know? · MACRA… What is it? Why Do I Need to Be...

MACRA… What is it? Why Do
I Need to Be in the Know?
Jim Brulé, Solutions Director - Regulatory

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 2
First, a word.The information contained within this presentation is intended for informational purposes only. While the information and recommendations presented in this presentation are good-faith interpretations made by Allscripts based on the publicly available information referenced within, it does not constitute legal advice or guidance. Thus, any decisions, and associated risks, made by the client pertaining to the information within this presentation are solely the responsibility and liability of the client. Clients are strongly advised that such decisions be made in consultation with their legal representatives.
The information presented within this presentation (1) should not be considered complete, exhaustive, or customized to an individual client’s needs; and (2) is subject to change due to new laws, regulations, or Department of Health and Human Services policies issued after May 18, 2016.
This presentation neither modifies any signed agreements Allscripts has with the client nor creates any Allscripts attestations, representations, warranties, guarantees or covenants related to MU or MACRA compliance, meeting MU or MACRA standards and requirements, whether Allscripts EHR software will meet new or modified requirements for certified EHR technology, or for any other matter.

Overview

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 4

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 5
“Bending the Cost Curve”

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 6
MACRA: Medicare Payment Reform• Repeals the Sustainable Growth Rate formula
– Archaic method of determining Medicare payments to providers
• Creates value-based framework for payment
– Moving directly away from volume-based payments
• Combines quality-based systems into one system
– Streamlining calculations and introduction of new measures
• Provides bonus payments
– Eligible Alternative Payment Models
MACRA: Medicare Access and CHIP Reauthorization Act | SGR: Sustainable Growth Rate

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 7
Shifting to increased quality & risk
Anticipated distribution of Medicare payments. Source: CMS
• FFS: Fee for Service
• APMs: Alternative
Payment Models
• MIPS: Merit-based
Incentive Payment
System

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 8
Two paths
QPP: Quality Payment Program | MIPS: Merit-based Incentive Payment System | APMs: Alternative Payment Models
MIPSDefault for
Medicare EPs
Advanced
APMs
QPP

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 9
Who does this affect?• Medicare Eligible Clinicians
– Physicians
– Physician assistants
– Nurse practitioners
– Clinical nurse specialists
– Certified registered nurse anesthetists
– Groups that include such clinicians
NOT
• Medicaid Eligible Professionals
• Eligible Hospitals (Medicare or Medicaid)
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 10
MIPS vs APMs• Merit-Based Incentive Payment System (MIPS)
– Default plan for all Medicare EPs
– Lower incentives; less certainty of incentive outcome
– Designed to be unattractive
• Advanced Alternative Payment Systems (APMs)
– Optional plan
– Carries higher risk, higher potential reward
• CMS anticipated initial participation:
– MIPS = 89%
– APMs = 11%
– Hoping for shift to APMs

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 11
• MACRA: Medicare Access and CHIP
Reauthorization Act
• NPRM: Notice of Proposed Rule-
Making

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 12
4/28 6/27 Oct? 11/1 1/1/17
ProposalCMS issues the
public inspection
version of the
proposed rule.
Federal Register
date: 5/9
Final RuleThis is anyone’s
guess. MU took
5+ months –
there’s not time
for that.
CommentsComments are
due to CMS by
5pm.
MeasuresThe final measures
for use in 2017
are due 11/1.
They take effect 2
months later.
QPP Active
2017 is the
performance year
for payment
adjustments in
2019.
The next 8 months

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 13
MIPS: Lower incentives, less desirable• Attempts to combine four drivers into one program:
– Quality of outcomes
– Cost of outcomes
– Use of Health IT
– Better process
• Moves the incentive/penalty bar each year based on national performance
– Participants won’t know the threshold for success until after the year is over

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 14
MIPS: Old and New Programs• Quality:
– PQRS measures (fewer required)
– VM measures (quality only)
• Cost:
– VM measures (cost only)
• Use of Health IT
– Meaningful Use measures, now called “Advancing Care Information” (ACI)
• Better process
– Clinical Practice Improvement Activities (CPIA) – New program
• PQRS: Physician Quality
Reporting System
• VM: Value-Based
Modifiers

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 15
MIPS: Integrating previous programs
Quality50%
ACI25%
CPIA15%
Cost10% • Quality: Formerly PQRS (Physician
Quality Reporting System)
• Cost: Formerly VM (Value Modifier Program)
• ACI: Advancing Care
Information, formerly MU (Meaningful Use)
• CPIA: Clinical Practice
Improvement Activities, New
Performance measurement begins in 2017;
affects payments two years later

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 16
Advanced Alternative Payment Models (APMs)• A category of payment models designed to “bend the cost curve”
• Each model is unique
• Shared characteristics:
– Assumed risk
– Some financial benefit for achieving quality
– Generally requires sharing of information across care locations
– Often creates new organizational systems for clinical and financial management
• May be actual or virtual organization

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 17
Advanced APMs: Eligible for 2017
• Medicare Shared Savings
Program—Track 2
• Medicare Shared Savings
Program—Track 3
• Next Generation ACO Model
• Comprehensive Primary Care
Plus (CPC+)
• Comprehensive ESRD Care
Model (Large Dialysis
Organization arrangement)
List will be updated by CMS annually

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 18
Surprise omissions• Medicare Shared Savings Program – Track 1
• Comprehensive Joint Replacement
• Patient Centered Medical Homes
– Only count for MIPS so far…

MIPS

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 20
MIPS: Who participates?• Medicare Eligible Clinicians (ECs):
– Physicians
– Physician assistants
– Nurse practitioners
– Clinical nurse specialists
– Certified registered nurse anesthetists
– Groups that include such clinicians
• May participate as individual or group
– Members of a group must report on identical measures/activities

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 21
MIPS scoring• Creates a composite score from performance against:
– Quality (50%) formerly PQRS and VM
– Cost (10%) formerly VM
– Use of Health IT (25%) “Advancing Care Information”, formerly MU
– Process improvements (15%) CPIA: Clinical Practice Improvement Activities
• Maintains budget neutrality (mostly)
– Sum of penalties = sum of rewards
• Rewards and Penalties are proportional to distance from performance threshold

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 22
MIPS calculation
ACI(MU)
Cost (VM)
Quality (PQRS+VM)
50
10
25
15 CPIA
ACI
Cost
Quality
ACI: Advancing Care Information | CPIA: Clinical Practice Improvement Activities
VM: Value-Based Modifiers | PQRS: Physician Quality Reporting System
MIPS Score(100 pts)
Category
CPIA

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 23
MIPS Percentages over Time
25% 25% 25%
15% 15% 15%
10% 15%30%
50% 45%30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2019 2020 2021+
ACI CPIA Cost Quality

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 24
MIPS Incentives/Penalties
-4%-5%
-7%
-9%
4%5%
7%
9%
2017 2018 2019 2020
2019 2020 2021 2022
Performance Year
Payment Year
• The more participants who do well, the lower their incentive.
• MIPS is budget neutral: total incentives must equal total penalties
• A performance threshold is set after the year closes; likely set to median score nationwide.
• Adjustments are calculated after the year closes, based on how much the individual score is above or below the performance threshold

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 25
Scenario 1
Scoring Curve
Payment Adjustments
85% of participants
+/- 1%
Many participants
doing well
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 26
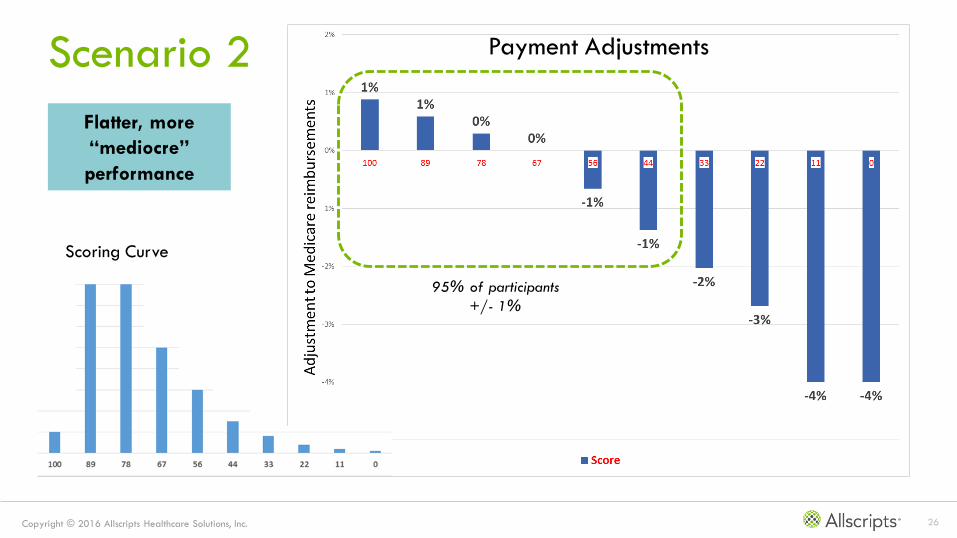
Scenario 2
Scoring Curve
Payment Adjustments
95% of participants
+/- 1%
Flatter, more
“mediocre”
performance

Composition of Scores

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 28
Scoring Strategy• There are four categories
– Quality
– Cost
– Clinical Practice Improvement Activities (CPIA)
– Advancing Care Information (ACI)
• Each has its own scoring rules
– Ways of accumulating points
– A “maximum” score that can be exceeded
– A percentage that each contributes to the MIPS score

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 29
For example:• Quality category has 8-9 measures
– Depends on practice size
• Each measure is worth up to 10 points
– Each scored proportionally based on performance
• Theoretic maximum is 90 points
• However, the most that can be contributed to MIPS is 50 points

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 30
Scoring summary
CategoryNumber of
Measures
Value of Each
Measure
Potential
Maximum
Score
Actual
Maximum
Score
Contribution to
MIPS score
Quality 8-9 10† 80-90 80-90 50%
CPIA 90 10 or 20 Hundreds 60 15%
Cost 40 10† * 10 10%
ACI – Base
ACI – Performance
ACI - PHR
6
8
3
All or nothing
10†
>0 = 1
50
80
1
100 25%
† These measures are scored proportionally; value is maximum for perfect score
* Score is based on percentage achieved for each measure selected averaged across all measures selected by CMS
131

Quality Category
Formerly PQRS (Physician Quality Reporting System)
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 32
Quality Category• Choose 6 measures to report (currently 9) (PQRS)
– Pool of hundreds of measures
– 80% of measures tailored for specialists
• CMS calculates 2-3 population measures based on claims data (no participant reporting
required) (VM)
– 2-9 clinicians = 2 measures
– >=10 clinicians = 3 measures
• Each measure is worth 10 points (proportionally)
• 1 cross-cutting measure required
• Actual maximum is 90 points
• Translates into 50% of MIPS score

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 33
Quality Measures• Individual: 273 measures – may be performed by anyone
– 18 New
– 70 Substantially Changed
– 185 Unchanged
• Cross-cutting: 10 measures – involves multiple modalities
– 3 Substantially Changed
– 7 Unchanged
• Specialty: 293 measures – tailored for specialists
– 71 Substantially Changed
– 4 New
– 218 Unchanged
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 34
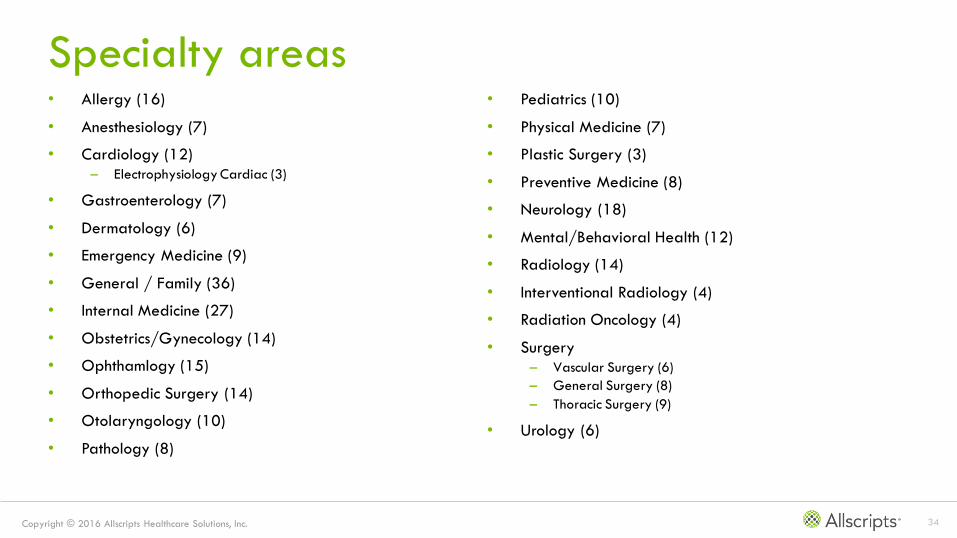
Specialty areas • Allergy (16)
• Anesthesiology (7)
• Cardiology (12)
– Electrophysiology Cardiac (3)
• Gastroenterology (7)
• Dermatology (6)
• Emergency Medicine (9)
• General / Family (36)
• Internal Medicine (27)
• Obstetrics/Gynecology (14)
• Ophthamlogy (15)
• Orthopedic Surgery (14)
• Otolaryngology (10)
• Pathology (8)
• Pediatrics (10)
• Physical Medicine (7)
• Plastic Surgery (3)
• Preventive Medicine (8)
• Neurology (18)
• Mental/Behavioral Health (12)
• Radiology (14)
• Interventional Radiology (4)
• Radiation Oncology (4)
• Surgery
– Vascular Surgery (6)
– General Surgery (8)
– Thoracic Surgery (9)
• Urology (6)

Cost Category
Formerly Value-Based Measures
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 36
Cost Category• Claims-based calculation: no reporting necessary
• 40 episode-specific measures
• Each measure worth up to 10 points
– based on cost efficiency
– 20-patient sample minimum for each measure
• Score is based on average performance across all calculated measures
• Translates into 10% of MIPS score

CPIA Category
Clinical Practice Improvement Activity

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 38
CPIA Category• 94 potential activities in 9 categories
• Each activity worth 20 or 10 points, depending on CMS
• Each activity is all or nothing
• Actual maximum is 60 points
• Translates into 15% of MIPS score
Expanded Practice
Access (4)
Population
Management (16)
Care
Coordination (14)
Beneficiary
Engagement (24)
Patient Safety and
Practice Assessment (21)
Participation in an APM,
including a PCMH
Achieving Health
Equity (5)
Emergency Preparedness
and Response (2)
Integrated Behavioral
and Mental Health (8)

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 39
Nationally recognized PCMHs
• National Committee for
Quality Assurance (NCQA)
PCMH recognition
• Accreditation Association for
Ambulatory Health Care
• The Joint Commission
Designation
• Utilization Review
Accreditation Commission
(URAC)
If a practice is part of a nationally recognized PCMH, it
automatically earns the maximum CPIA score, such as:

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 40
Different ranks of measures• High
– Worth 20 points
– High effort to implement
– Greater impact on outcomes
• Medium
– Worth 10 points
– Medium effort to implement
– Moderate impact on outcomes

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 41
Samples: Expanded Practice Access• High (20pts): Provide 24/7 access to MIPS eligible clinicians, groups, or care teams for advice
about urgent and emergent care…
• Medium (10pts): Use of telehealth services and analysis of data for quality improvement…
• Medium (10pts): Collection of patient experience and satisfaction data on access to care and
development of an improvement plan…

Advancing Care Information
Formerly “Meaningful Use”

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 50
Basic Scoring Process
Base Measures
50 points
Performance
Measures
Up to 80 points
Registry Bonus
1 point
Primary option: 11 measures
many Stage 3 measures
Alternate option: 16 measures
all Stage 2 measures
50 points, all or nothing
3 Stage 3 measures
up to 10 pts each
5 Stage 2 measures
up to 10 pts each
1 point for doing at least one
extra registry beyond
Immunization
100 points maximum

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 51
Advancing Care Information Category• Base score = 50
– 11-16 measures, all or nothing
– Yes/no or num/denom, num >= 1
• Performance score = 80
– Eight measures, up to 10 pts each
– Each measure score = (numerator/denominator) * 10
• Public Health Registry = 1
– Reporting beyond Immunization Registry
• Translates into 25% of MIPS score
– Proportional: ACI score * 0.25 = MIPS score
– >= 100 translates into 25 MIPS points

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 52
Performance Score Calculation
Objectives Patient Electronic AccessCoordination of Care Through Patient
EngagementHealth Information Exchange (HIE)
Measures Patient Access
Patient-
Specific
Education
VDTSecure
Messaging
Patient-
Generated
Health Data
Patient Care
Record
Exchange
Request /
Accept Patient
Care Record
Clinical
Information
Reconciliation
Perf
orm
an
ce R
ate
95%
65%
57%
33% 31% 38%
25% 21%
Performance
Points Earned9.5 6.5 3.3 3.1 2.5 2.1 3.8 5.7
Performance Score = 36.5 points

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 53
ACI Category Score Calculation
Base Score Performance Score Components
Tota
l Perf
orm
anc
e S
core
Pub
lic
Hea
lth
and
Clini
cal D
ata
Reg
istr
y B
onu
s Poin
t
Total
Points
Pro
tect
Pa
tient
Hea
lth
Info
rma
tion
Ob
ject
ives a
nd M
ea
sure
sPatient Electronic
Access
Coordination of Care
Through Patient
Engagement
Health Information
Exchange (HIE)
Patient
Access
Patient-
Specific
Education
VDTSecure
Messaging
Patient-
Generated
Health
Data
Patient
Care
Record
Exchange
Request /
Accept
Patient
Care
Record
Clinical
Information
Reconciliati
on
50 9.5 + 6.5 + 3.3 + 3.1 + 2.5 + 2.1 + 3.8 + 5.7 = 36.5 1 87.5
87.5 ACI points * 0.25 =
21.88 MIPS points for the ACI category

Base Score
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 55
Scoring Principles: Base Score• Worth 50 points
• All-or-nothing
• Each measure is either Yes/No or numerator >= 1
• If Protect Health Information is not achieved, entire ACI score is 0.
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 56
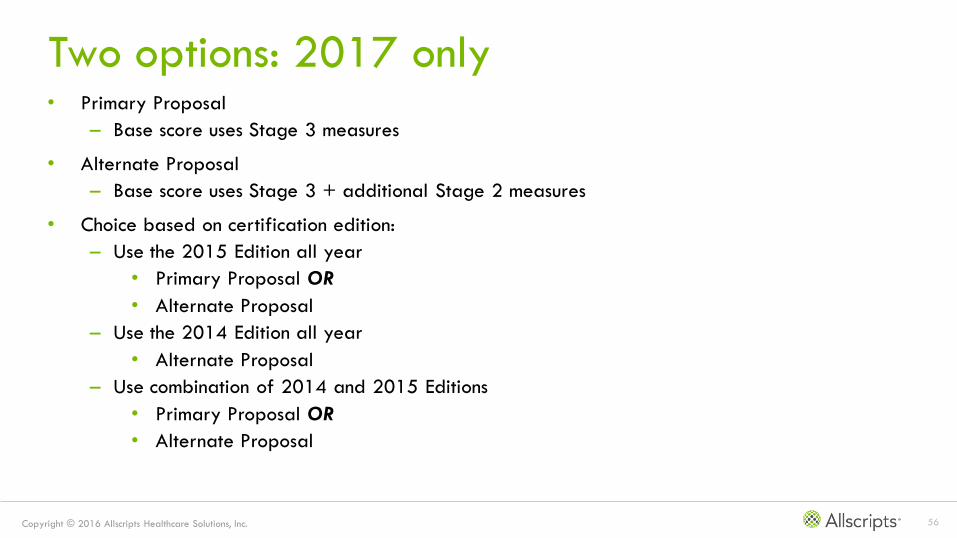
Two options: 2017 only• Primary Proposal
– Base score uses Stage 3 measures
• Alternate Proposal
– Base score uses Stage 3 + additional Stage 2 measures
• Choice based on certification edition:
– Use the 2015 Edition all year
• Primary Proposal OR
• Alternate Proposal
– Use the 2014 Edition all year
• Alternate Proposal
– Use combination of 2014 and 2015 Editions
• Primary Proposal OR
• Alternate Proposal

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 57
Primary Proposal – Base ObjectivesObjective Measure Stage 2 Stage 3
1 Protect Patient Health Information Security Risk Analysis
2 Electronic Prescribing ePrescribing
3 Patient Electronic Access Patient Access
Patient-Specific Education
4 Coordination of Care Through
Patient Engagement
View, Download or Transmit (VDT)
Secure Messaging
Patient-Generated Health Data
5 Health Information Exchange Patient Care Record Exchange
Request/Accept Patient Care Record
Clinical Information Reconciliation
6 Public Health and Clinical Data
Registry Reporting
Immunization Registry Reporting
(Optional) Syndromic Surveillance Reporting
(Optional) Electronic Case Reporting
(Optional) Public Health Registry Reporting
(Optional) Clinical Data Registry Reporting

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 58
Alternate Proposal – Base ObjectivesObjective Measure Stage 2 Stage 3
1 Protect Patient Health Information Security Risk Analysis
2 Electronic Prescribing ePrescribing
3 Clinical Decision Support (CDS) Clinical Decision Support Interactions (CDS)
Drug Interaction and Drug-Allergy Checks
4 Computerized Provider Order
Entry (CPOE)
Medication Orders
Laboratory Orders
Diagnostic Imaging Orders
5 Patient Electronic Access Patient Access
View, Download or Transmit (VDT)
6 Patient-Specific Education Patient-Specific Education
7 Secure Messaging Secure Messaging
8 Health Information Exchange Health Information Exchange
9 Medication Reconciliation Medication Reconciliation
10 Public Health Reporting Immunization Registry Reporting
Syndromic Surveillance Reporting
Specialized Registry Reporting

Performance Measures
Same for Primary and Alternative
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 60
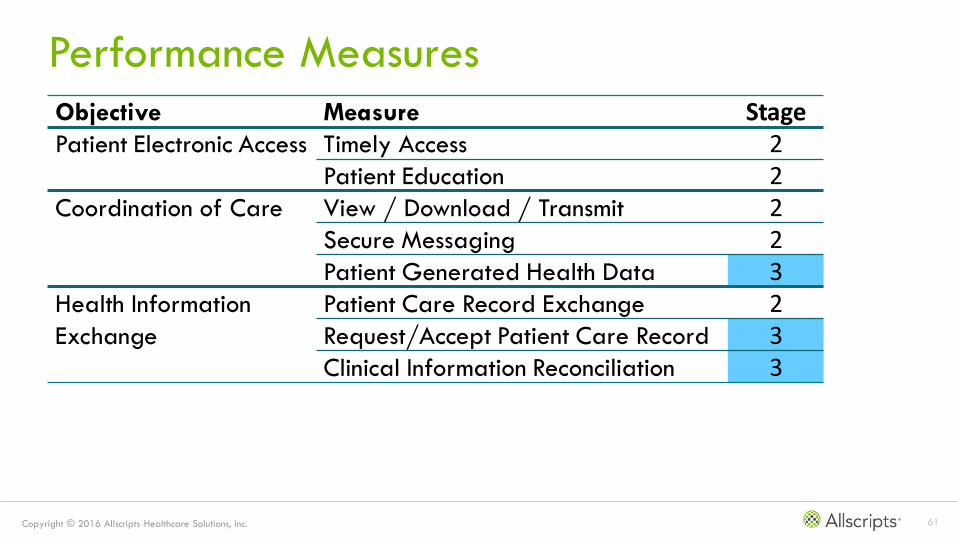
Performance Measures Method• Eight measures total
• Calculate percent achievement for each measure across each measure
• Divide each achievement percent by 10
• Maximum score is 80
• Sum all the scores
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 61
Performance Measures
Objective Measure StagePatient Electronic Access Timely Access 2
Patient Education 2Coordination of Care View / Download / Transmit 2
Secure Messaging 2Patient Generated Health Data 3
Health Information
Exchange
Patient Care Record Exchange 2Request/Accept Patient Care Record 3Clinical Information Reconciliation 3

Registry Bonus

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 63
Registry Bonus Point • May earn 1 point towards ACI score for participation in one or more extra registries
• Maximum score is 1 point, no matter how many registries
• Potential registries:
– Syndromic Surveillance
– Electronic Case Reporting
– Public Health Registry Reporting
– Clinical Data Registry Reporting

Advanced APMs

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 65
In review• APMs are a class of risk-based payment models
• Each functions in its own manner
• Incentives are in addition to FFS payments
• Only Advanced APMs qualify for QPP
– Detailed within

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 66
Requirements for Advanced APM• CMS Innovation Model or statutorily required model
• Bear more than nominal financial risk
– Advanced medical homes with 50 or fewer clinicians exempt
• Payments based on quality measures similar to MIPS
• Must use certified EHR technology

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 67
Financial Impact of APM Participation• Current incentives for APMs remain in place
• 2019-2024:
– MIPS participation waived
– 5% Medicare Part B incentive
• 2026 and forward:
– MIPS participation waived
– Higher fee schedule update

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 68
Advanced APMs• Qualify as Advanced APMs via statute:
– Medicare Shared Savings Program—Track 2
– Medicare Shared Savings Program—Track 3
– Next Generation ACO Model
– Comprehensive Primary Care Plus
– Comprehensive End Stage Renal Disease Care Model (Large Dialysis Organization
arrangement)
– Oncology Care Model Two-Sided Risk Arrangement (available in 2018)
• Note: Comprehensive Joint Replacement not included
– CMS seeking comments on how to include

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 69
Surprise omissions• Medicare Shared Savings Program – Track 1
• Comprehensive Joint Replacement
• Patient Centered Medical Homes
– Only count for MIPS so far…
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 70
Which APMs Qualify?• Will be determined by CMS by January 1 of the performance year…

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 71
Qualifying for Incentive Payments• Requires sufficient volume of payments via APMs
• May form group to reach volume
• 2019-2020, Medicare payments or patients only
• 2021 forward, may include non-Medicare
Payment Year 2019 2020 2021 2022 2023 2024+
% Payments 25% 25% 50% 50% 75% 75%
% Patients 20% 20% 35% 35% 50% 50%

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 72
Transitional Considerations• All clinicians report via MIPS in 2019 payment year
– APM participation = CPIA category
• Failure to achieve APM incentives in 2019-2020
– May opt out of APM, participate in MIPS instead
– Requires 20% of payments or 10% of patients via APM

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 73
Other APM Options• If participating in multiple APMs but no single APM performance is “qualifying,” may be assessed
to see if aggregate performance could be used
• Partial Qualifying APM: lower thresholds so no MIPS requirement, but lower bonus as well

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 74
Physician-Focused Payment Models (PFPMs)• Recommended by Physician-Focused Payment Model Technical Advisory Committee (PTAC) to HHS
• Includes physician group practices (PGPs) or individual physicians as APM entities
• Targets the quality and cost of physician services
• Don’t have to be an advanced APM
• Initially, test with Medicare as payer (third parties later)
Copyright © 2016 Allscripts Healthcare Solutions, Inc. 75
PFPM Criteria• Incentives: Pay for higher-value care
– Value over volume
– Flexibility
– Quality and cost focus (can improve both or at least one)
– Payment methodology
– Scope (broaden the APM portfolio)
– Criteria for evaluation
• Care delivery improvements
– Integration and care coordination
– Patient choice
– Patient safety
• Information enhancements
– Health IT

Transparency

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 77
Transparency via Physician Compare• Data published
– Names of clinicians in APMs
– As feasible, names and performance of APMs
– MIPS scores for clinicians
• Aggregate and individual
• Detailed per performance category
• 30-day pre-publication window for clinicians to review and submit corrections

In closing…

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 79
Questions

Copyright © 2016 Allscripts Healthcare Solutions, Inc. 80
Further information• ClientConnect: MACRA Quality Payment Program (QPP)
– https://clientconnect.allscripts.com/groups/macra/overview
• CMS QPP website:
– https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-
Based-Programs/MACRA-MIPS-and-APMs/Quality-Payment-Program.html

Thank you!


















