
M. Wirth Department of Urology, Technical University of Dresden Adjuvant or Salvage Radiotherapy...
105
M. Wirth Department of Urology, Technical University of Dresden Adjuvant or Salvage Radiotherapy after Radical Prostatectomy
-
Upload
megan-todd -
Category
Documents
-
view
227 -
download
2
Transcript of M. Wirth Department of Urology, Technical University of Dresden Adjuvant or Salvage Radiotherapy...
M. Wirth
Department of Urology, Technical University of Dresden
Adjuvant or Salvage Radiotherapy after Radical
Prostatectomy
Adjuvant or Salvage Radiotherapy after Radical Prostatectomy:
Background

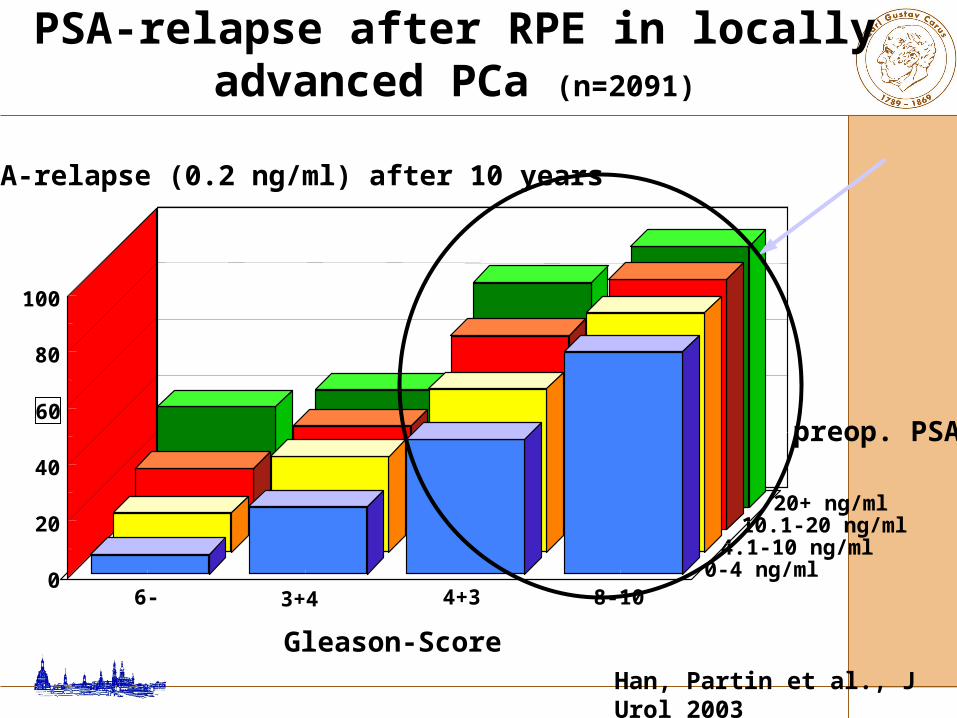
6- 3+4 4+3 8-100
20
40
60
80
100
0-4 ng/ml4.1-10 ng/ml
10.1-20 ng/ml20+ ng/ml
% PSA-relapse (0.2 ng/ml) after 10 years
Gleason-ScoreHan, Partin et al., J Urol 2003
PSA-relapse after RPE in locally advanced PCa (n=2091)
preop. PSA
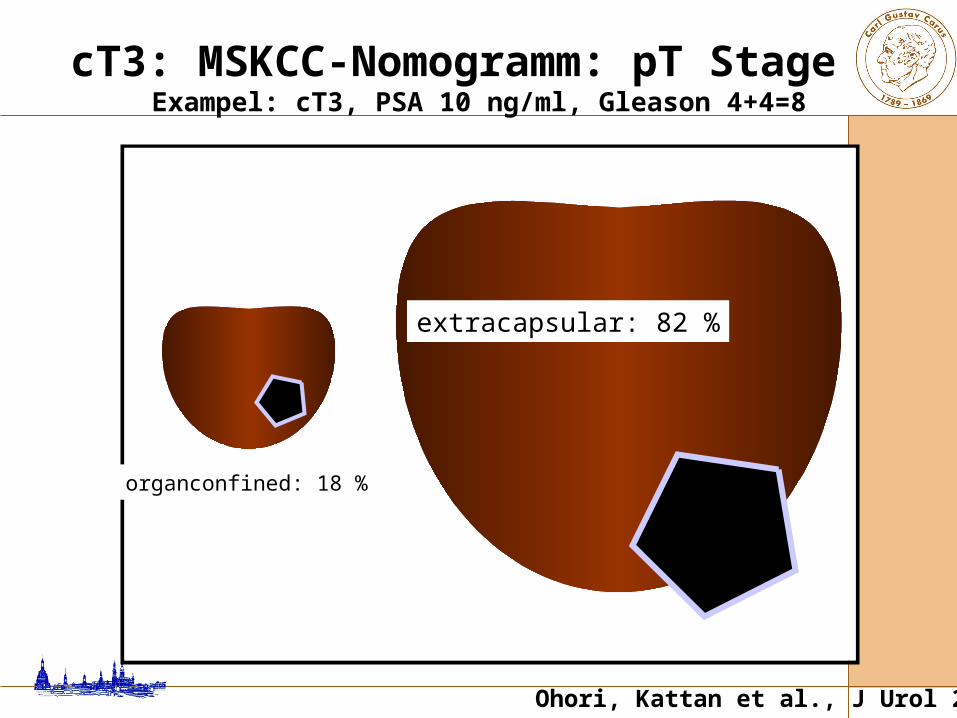
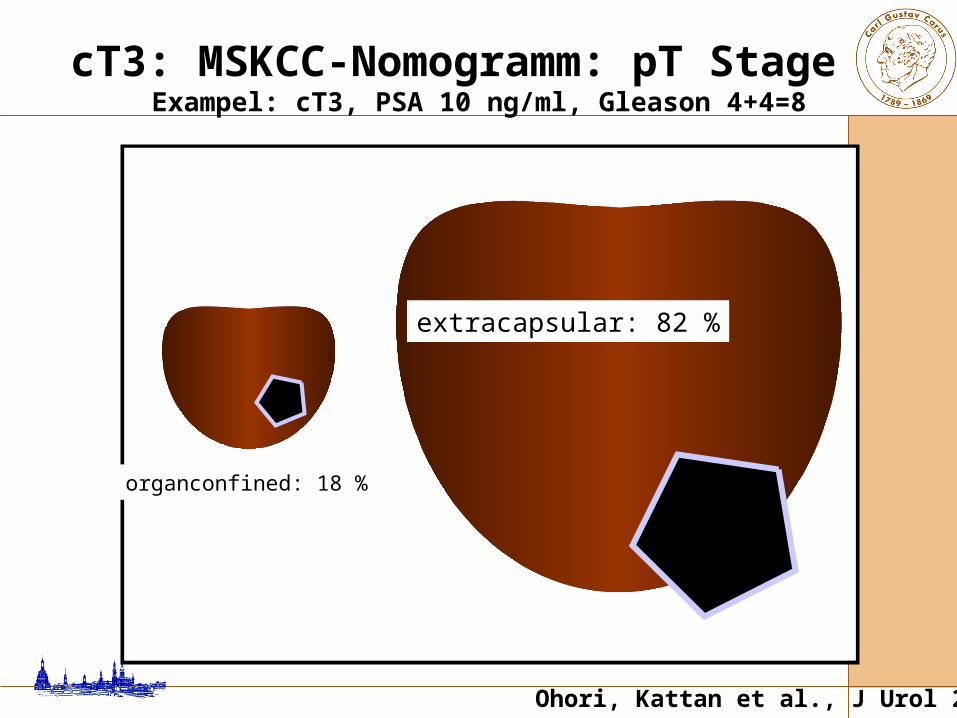
organconfined: 18 %
extracapsular: 82 %
cT3: MSKCC-Nomogramm: pT Stage Exampel: cT3, PSA 10 ng/ml, Gleason 4+4=8
Ohori, Kattan et al., J Urol 2004
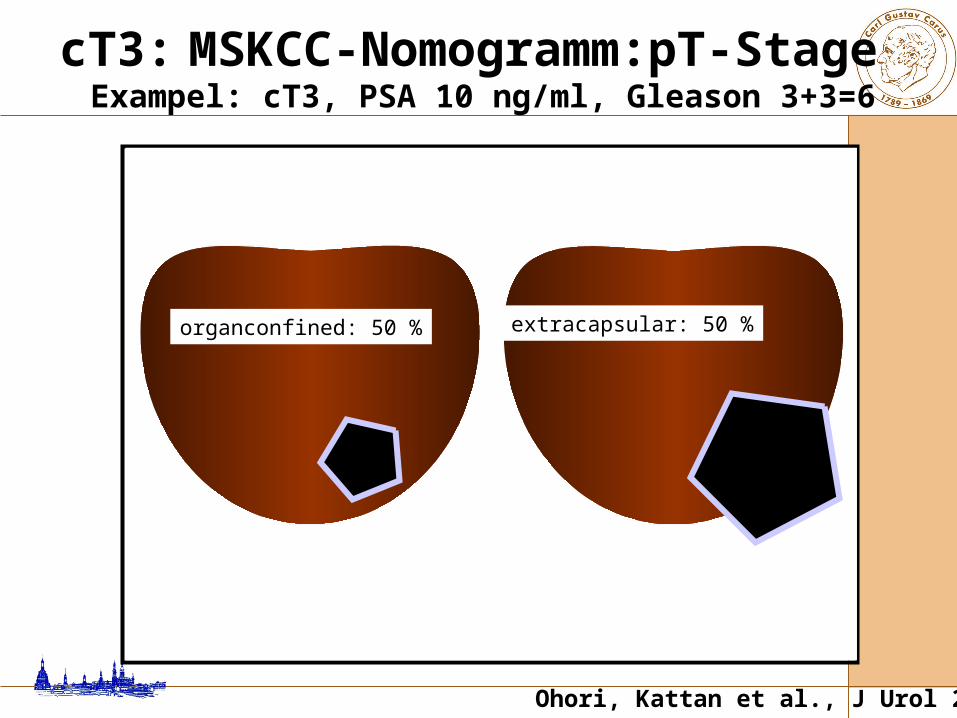
cT3: MSKCC-Nomogramm:pT-Stage Exampel: cT3, PSA 10 ng/ml, Gleason 3+3=6
Ohori, Kattan et al., J Urol 2004
organconfined: 50 % extracapsular: 50 %
Adjuvant or Salvage Radiotherapy after Margin Positive Radical Prostatectomy
• Patients with R1 after RPE are at an increased risk of biochemical, local and distant failure [1].
• With R1, the risk of biochemical recurrence may supersede 50 % after 10-years [2].
• The associated 10-year local recurrence rate accounts for narrowly 30 % [2].
1 EAU guidelines 2008; 2 Pfitzenmaier et al., BJU Int 2008

Adjuvant Radiotherapy vs. Wait-and-see
after Radical Prostatectomy

randomised controlled trial pT3 or positive margins, pN0 age < 76 years, WHO perf. status 0-1
wait-and-see (n=503) vs.
irradition (60 Gy) within 16 w. after RPE (n=502)
Bolla et al., Lancet 2005
Wait-and-see vs. immediate postoperative radiotherapy - EORTC trial 22911 (n=1005)
age 65 y. (61-69) PSA: 12.4 ng/ml (7.2-20.3) PSA: 3 weeks after RPE, before RTX
0.2 (0.0-0.3) median FU 5 y. biochemical and clinical progression free
survival significantly improved after ART overall survival with trend towards
improvement after ART, but not (yet?) significant
Bolla et al., Lancet 2005
wait-and-see vs. immediate postoperative radiotherapy - EORTC trial 22911 (n=1005)

EORTC trial 22911 (n=1005) clinical progression free survival
Bolla et al., Lancet 2005
Clinical progression-free survival

EORTC trial 22911 (n=1005) biochemical progression free survival
Bolla et al., Lancet 2005
PSA progression-free survival
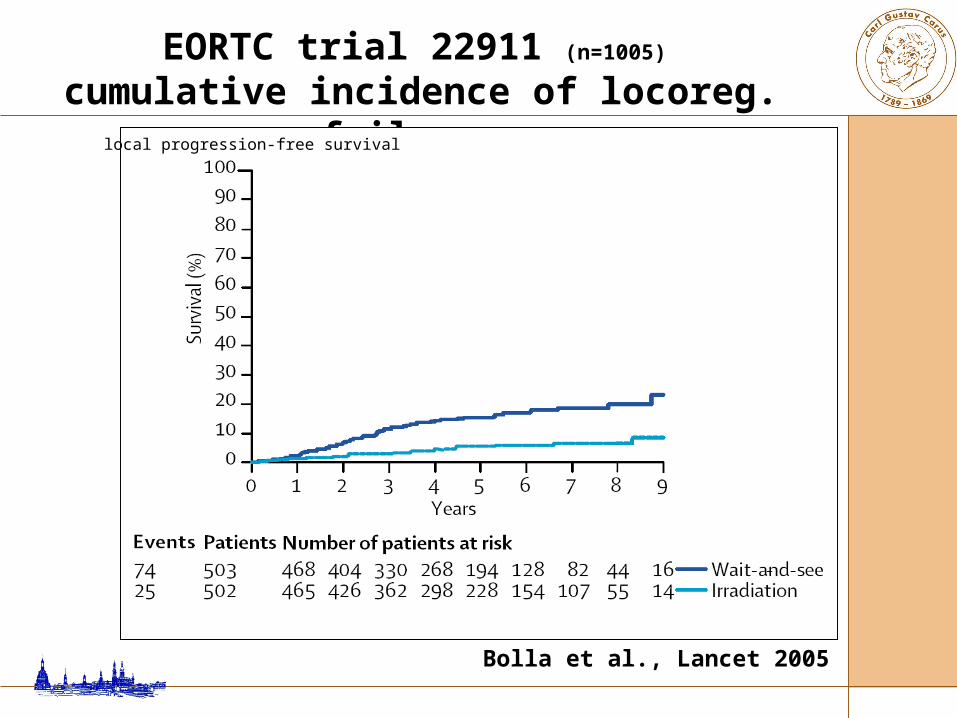
EORTC trial 22911 (n=1005)
cumulative incidence of locoreg. failure
Bolla et al., Lancet 2005
local progression-free survival

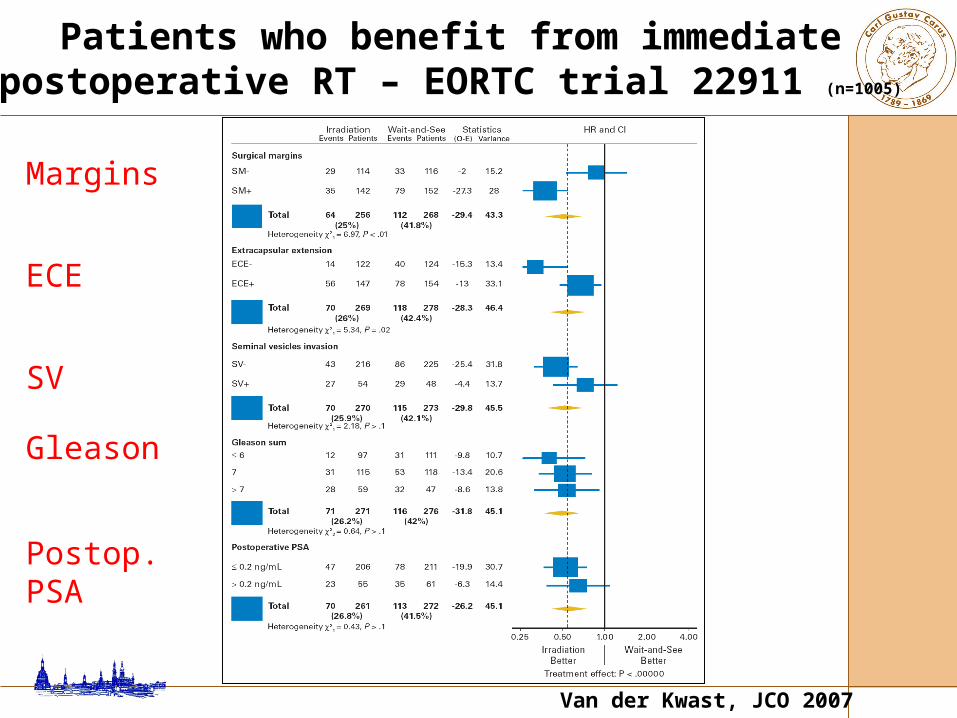
Patients who benefit from immediate postoperative RT – EORTC trial 22911 (n=1005)
Van der Kwast, JCO 2007
Patients who benefit from immediate postoperative RT – EORTC trial 22911 (n=1005)
Van der Kwast, JCO 2007
Margins
ECE
SV
Gleason
Postop. PSA

Patients who benefit from immediate postoperative RT – EORTC trial 22911 (n=1005)
Van der Kwast, JCO 2007

Patients who benefit from immediate postoperative RT – EORTC trial 22911 (n=1005)
Van der Kwast, JCO 2007
control arm
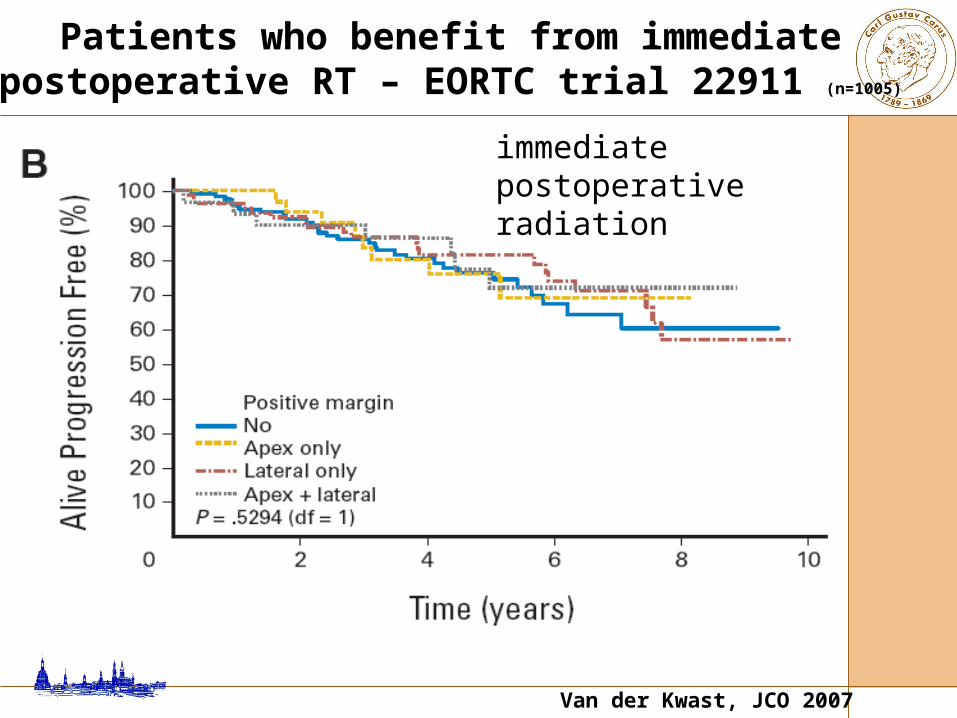
Patients who benefit from immediate postoperative RT – EORTC trial 22911 (n=1005)
Van der Kwast, JCO 2007
immediate postoperative radiation

EORTC trial 22911 (n=1005) cumulative incidence of late complications
Bolla et al., Lancet 2005
Late complications

Randomised controlled trial clinical T1/T2 preoperatively pT3 or positive margins, N0 M0 WHO perf. status 0-2
Wait-and-see (n=211) vs. Irradition (60-64 Gy, n=214)
Thompson et al., J Urol 2009
Adjuvant RTX for T3N0M0 PCA – randomised SWOG trial 8794 (n=425)
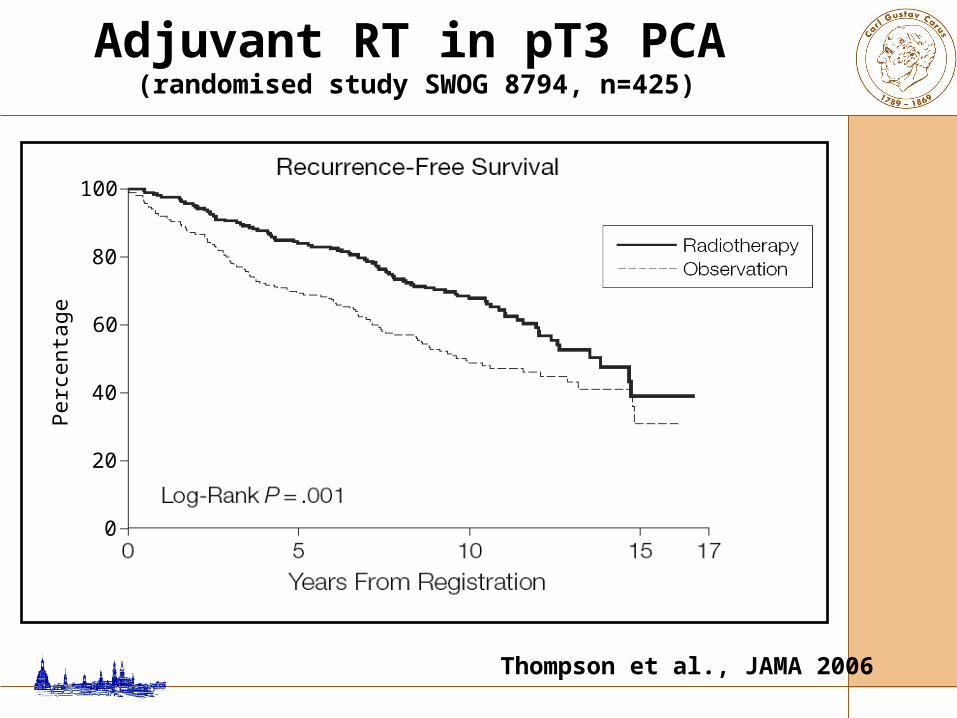
Adjuvant RT in pT3 PCA (randomised study SWOG 8794, n=425)
Thompson et al., JAMA 2006
100
60
80
40
20
0
Per
cent
age

Thompson et al., J Urol 2009
Adjuvant RTX for T3N0M0 PCA – randomised SWOG trial 8794 (n=425)
Overall survival p=0.023
Thompson et al., J Urol 2009
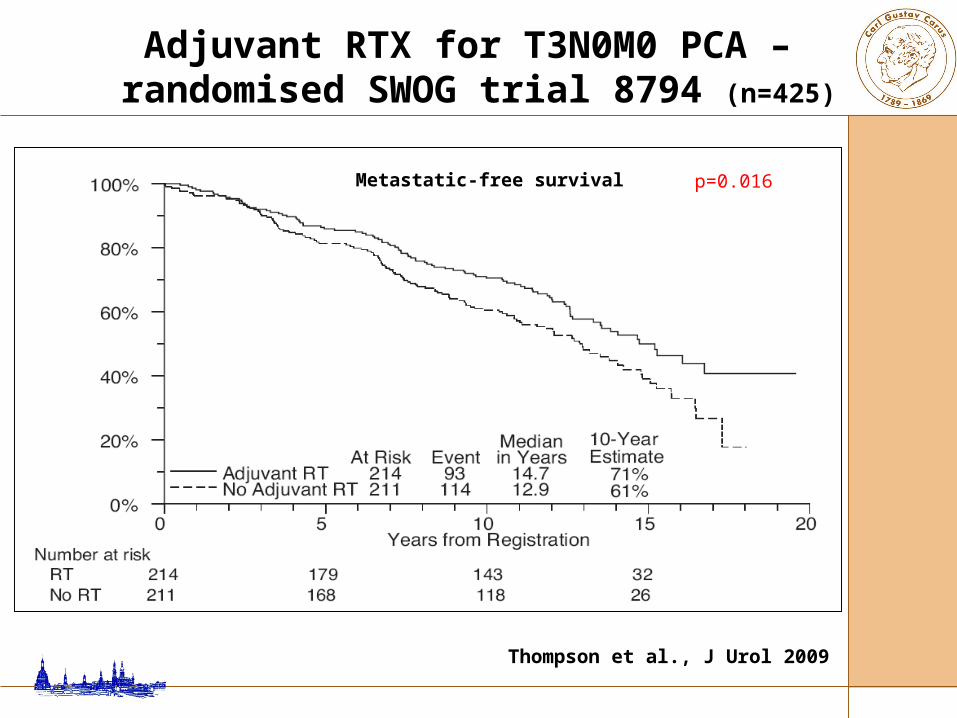
Adjuvant RTX for T3N0M0 PCA – randomised SWOG trial 8794 (n=425)
Metastatic-free survival p=0.016

Thompson et al., J Urol 2009
Adjuvant RTX for T3N0M0 PCA – randomised SWOG trial 8794 (n=425)
Metastatic-free survival, PSA < / > 0.2 p=0.03

Thompson et al., J Urol 2009
Adjuvant RTX for T3N0M0 PCA – randomised SWOG trial 8794 (n=425)
Summary

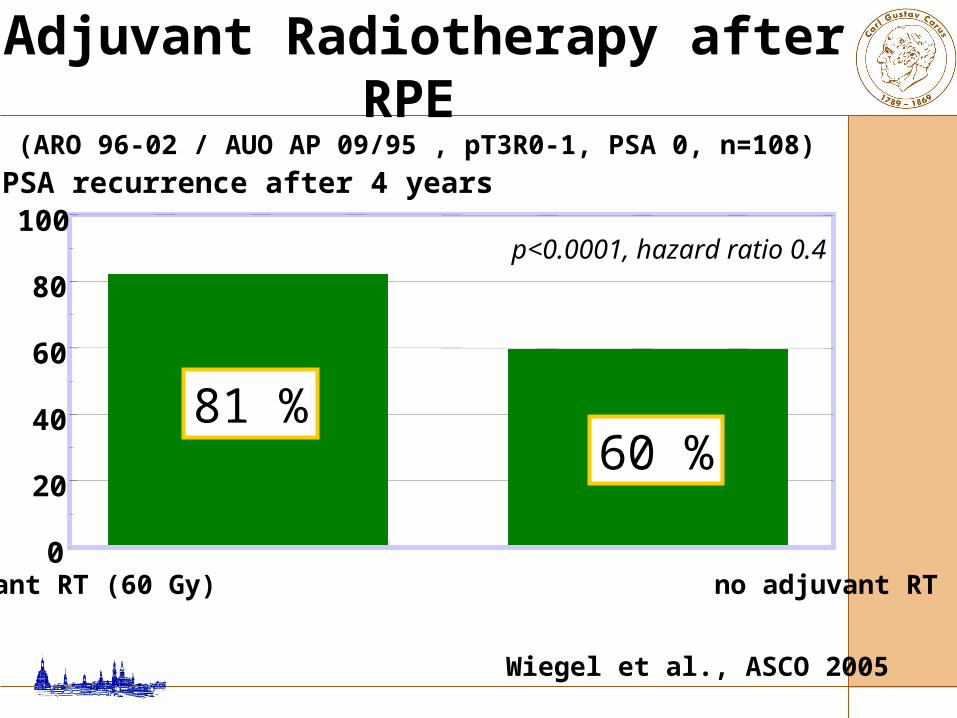
Wiegel et al., ASCO 2005 [in press as full article: J Clin Oncol 2009]
adjuvant RT (60 Gy) no adjuvant RT
Adjuvant radiotherapy after RPE (ARO 96-02 / AUO AP 09/95 , pT3R0-1, PSA 0, n=108)
% PSA recurrence after 4 years
0
20
40
60
80
100p<0.0001, hazard ratio 0.4
81 %60 %
Bottke and Wiegel, Urol Int 2007
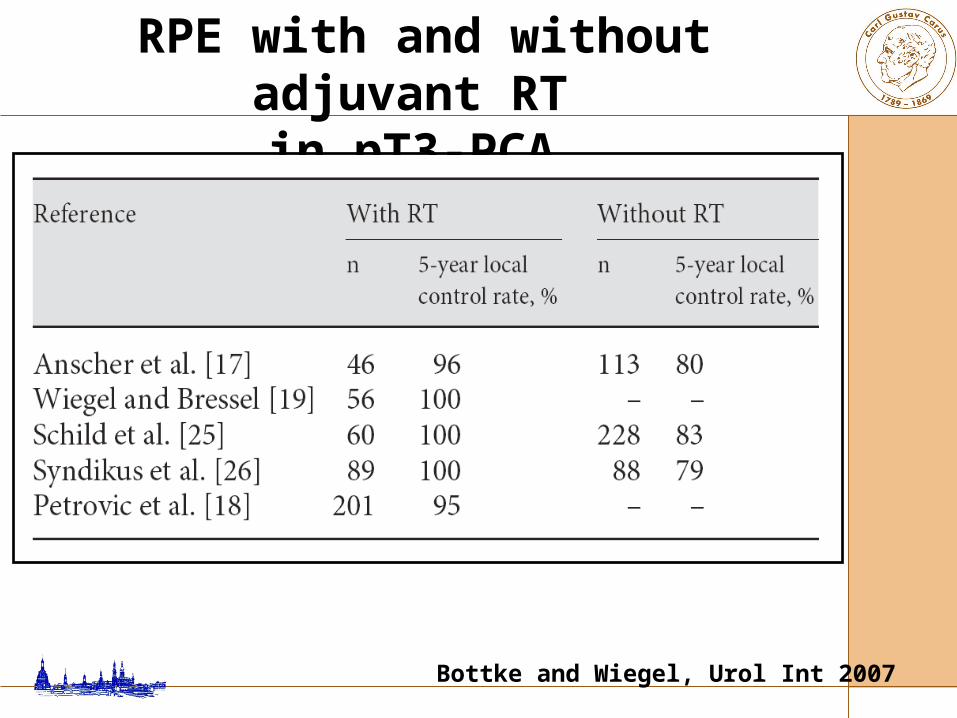
RPE with and without adjuvant RT in pT3-PCA
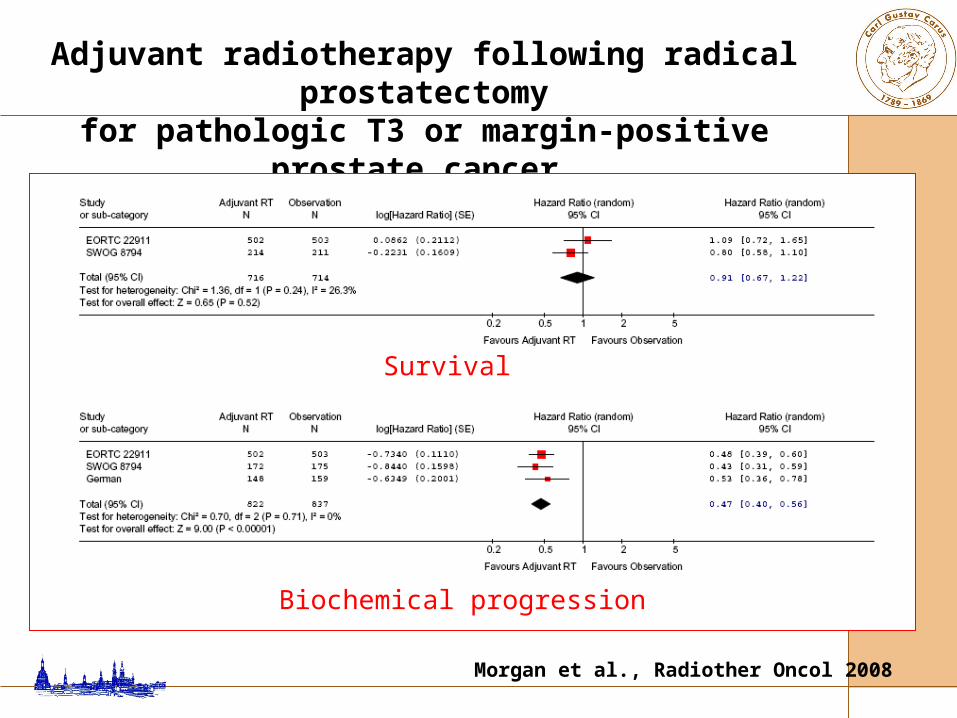
Morgan et al., Radiother Oncol 2008
Adjuvant radiotherapy following radical prostatectomyfor pathologic T3 or margin-positive prostate cancer
A systematic review and meta-analysis
Survival
Biochemical progression

Salvage Radiotherapy vs. Observation
at PSA Failure after Radical Prostatectomy
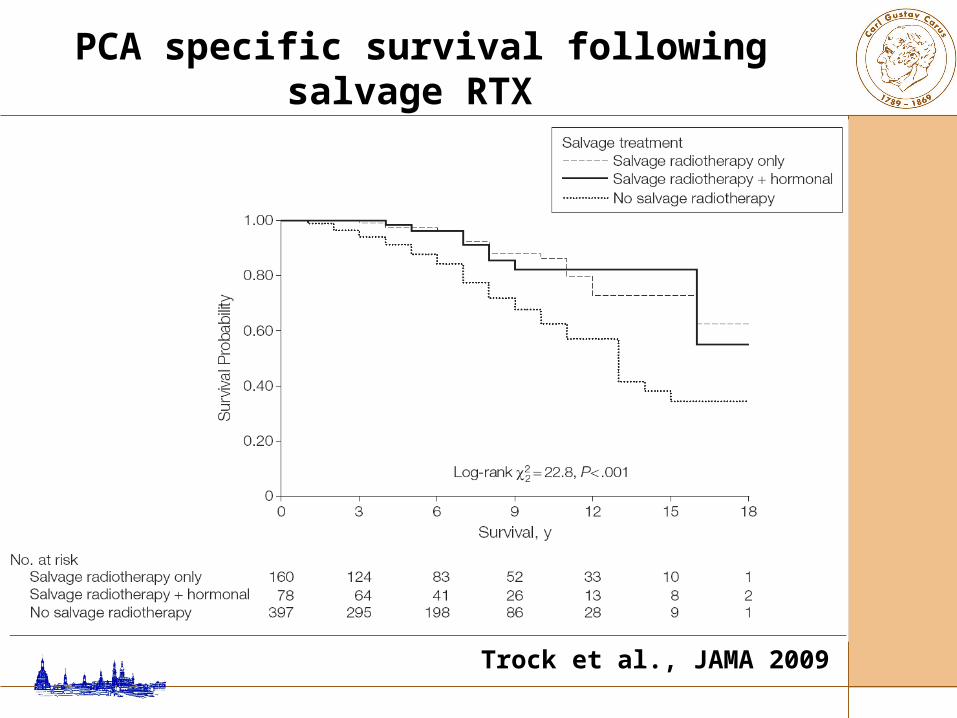
no salvage treatment (n=397) vs. salvage radiotherapy (n=160) vs. salvage radiotherapy + HT (n=78)
significant increase of PC-specific survival for both SRT (HR 0.32, p<0.001) and SRT+HT (HR 0.34, p=0.003)
improvement limited to patients with - PSA-doubling time < 6 month - SRT within 2 y. after recurrence
Trock et al., JAMA 2009
PCA specific survival following salvage RTX vs observation after RPE – survival

PCA specific survival following salvage RTX vs. observation after RPE – survival
Trock et al., JAMA 2009
PCA specific survival
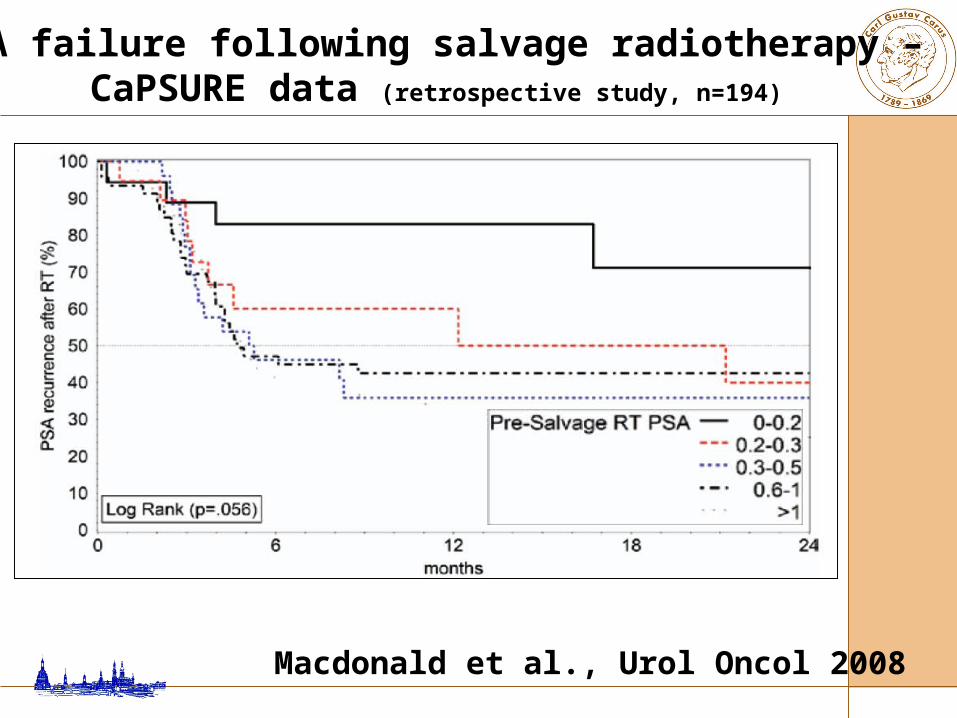
PSA failure following salvage radiotherapy – CaPSURE data (retrospective study, n=194)
Macdonald et al., Urol Oncol 2008
0 20 40 60 80 100
time / months
0,0
0,2
0,4
0,6
0,8
1,0
p b
ne
d
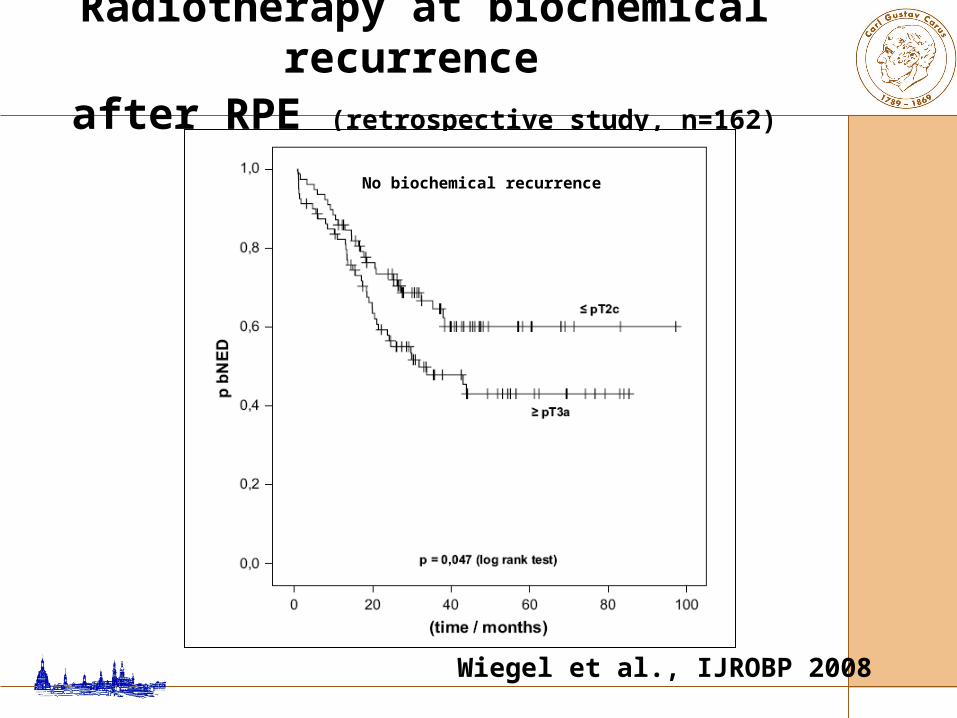
PSA ≤ 0,5 ng/ml
PSA ≥ 0,5 ng/ml
p = 0,031 (log rank test)
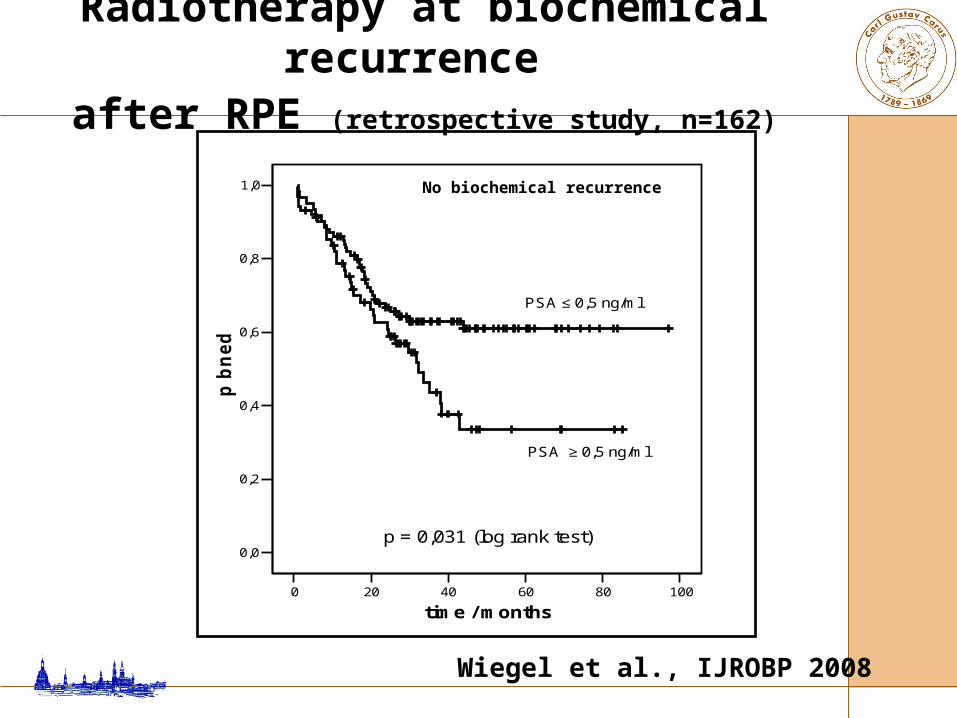
Radiotherapy at biochemical recurrence after RPE (retrospective study, n=162)
Wiegel et al., IJROBP 2008
No biochemical recurrence
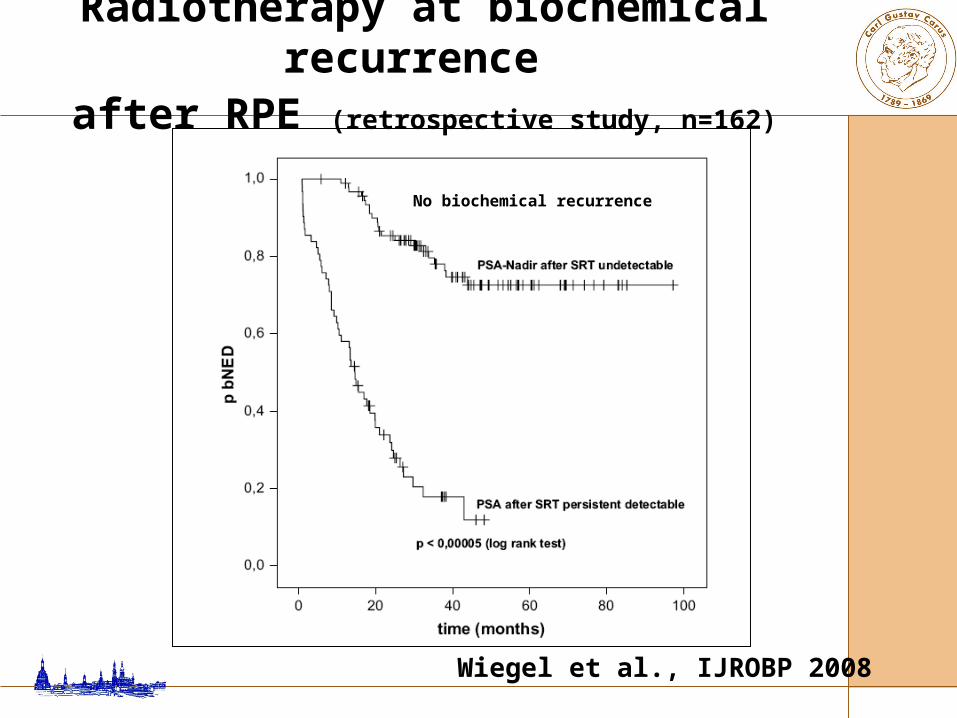
Radiotherapy at biochemical recurrence after RPE (retrospective study, n=162)
Wiegel et al., IJROBP 2008
No biochemical recurrence
Radiotherapy at biochemical recurrence after RPE (retrospective study, n=162)
Wiegel et al., IJROBP 2008
No biochemical recurrence

Salvage RTX at PSA progression: long-term efficacyLiterature review
Bottke and Wiegel, Urologe 2008
35-54 %
Arguments pro delayed radiotherapy for positive surgical margins
• Questionable survival advantage for immediate adjuvant RTX
• Sparing of side effects and costs in about 50 % of patients
• Improved risk stratification by monitoring of PSA value and PSA kinetics
• High rate of disease control with timely applied salvage therapy
Adjuvant vs. Salvage Radiotherapy after Radical Prostatectomy

Adjuvant vs. Salvage Radiotherapy Matched-control analysis (n=192)
Trabulsi et al., Urology 2008
Five-year freedom from biochemical failure from end of RT

Adjuvant vs. Salvage Radiotherapy Matched-control analysis (n=192)
Trabulsi et al., Urology 2008
Five-year freedom from biochemical failure from end of surgery

Adjuvant and Salvage RTX after RPE Biochemical failure free survival
Jereczek-Fossa, IntJRadOncol 2008
Adjuvant RT
Salvage RT
n=410

Adjuvant and Salvage RTX after RPE Grade 2 or greater rectal and urinary toxicity
Jereczek-Fossa, IntJRadOncol 2008
n=410
Adjuvant RT
Salvage RT

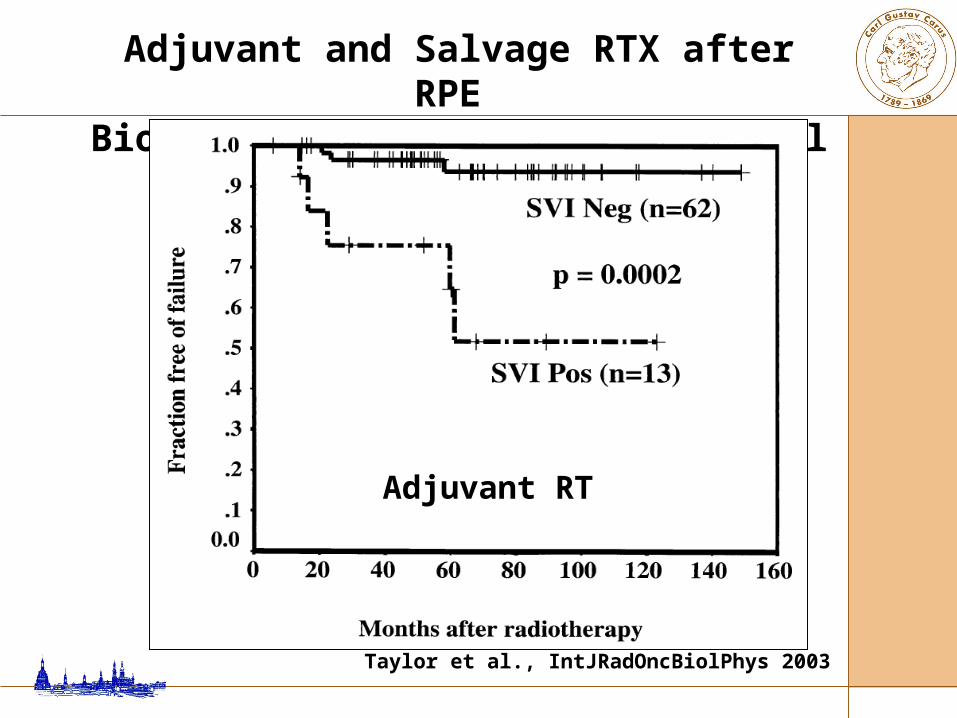
Adjuvant and Salvage RTX after RPE Biochemical failure free survival
Taylor et al., IntJRadOncBiolPhys 2003
Adjuvant and Salvage RTX after RPE Biochemical failure free survival
Taylor et al., IntJRadOncBiolPhys 2003
Adjuvant RT
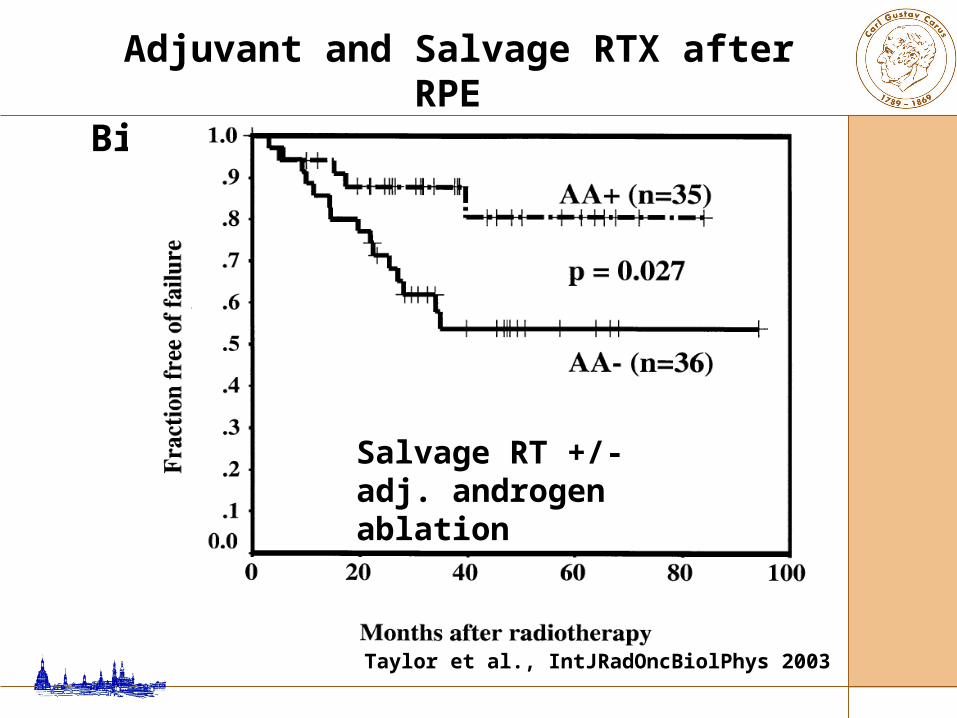
Adjuvant and Salvage RTX after RPE Biochemical failure free survival
Taylor et al., IntJRadOncBiolPhys 2003
Salvage RT +/- adj. androgen ablation

Adjuvant RTX for pN+ disease?

Da Pozzo et al., Eur Urol 2009
Conclusions: This study is the first to report a significant protective role for adjuvant RT in BCR-free survival and CSS of node-positive patients.

Adjuvant RTX for pN+ disease (retrospective study, n=250)
Da Pozzo et al., Eur Urol 2009
No biochemical failure

Adjuvant RTX for pN+ disease (retrospective study, n=250)
Da Pozzo et al., Eur Urol 2009
PCA-specific survival
p<0.0001
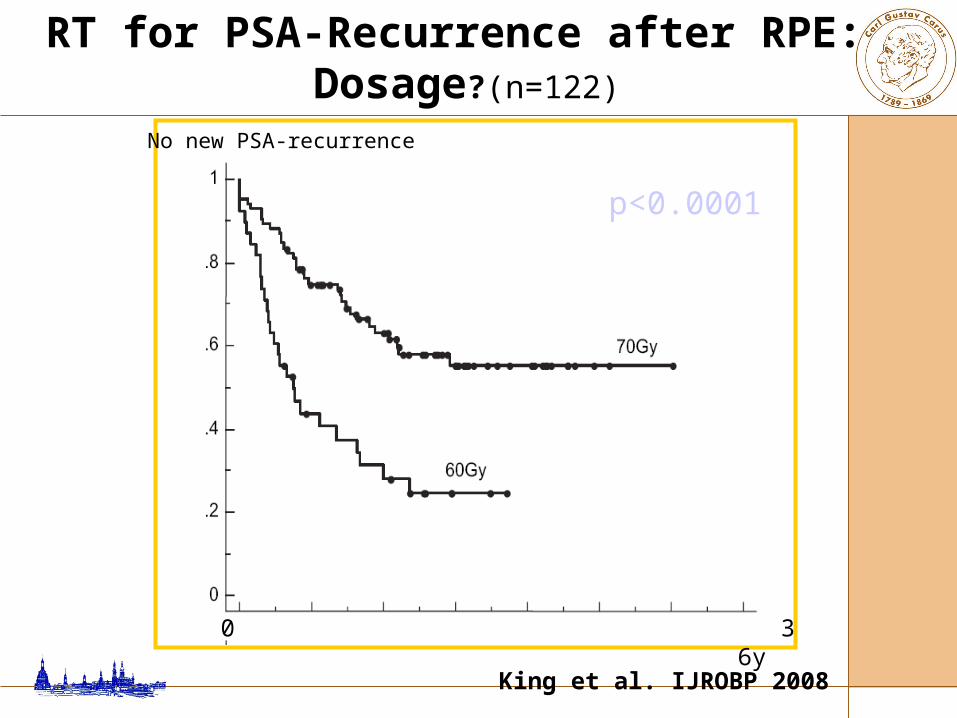
RT for PSA-Recurrence after RPE: Dosage?(n=122)
0 3 6y
No new PSA-recurrence
King et al. IJROBP 2008
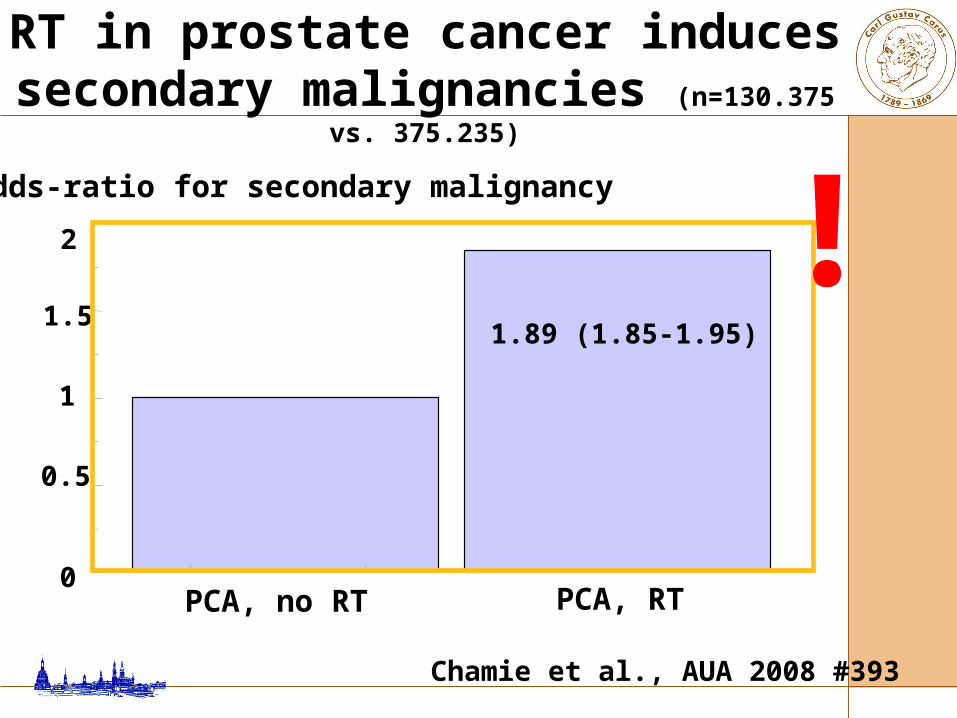
Chamie et al., AUA 2008 #393
RT in prostate cancer induces secondary malignancies (n=130.375 vs. 375.235)
PCA, no RT0
1.5
0.5
odds-ratio for secondary malignancy
1
2
1.89 (1.85-1.95)
PCA, RT
!

Risk stratification?
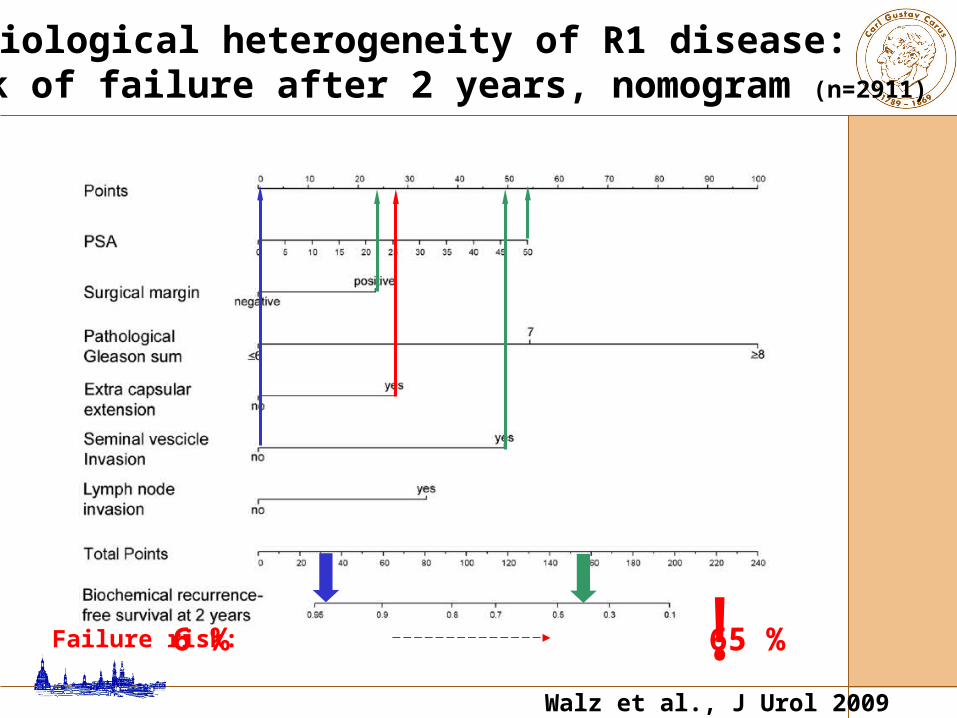
6 % 65 % !
Biological heterogeneity of R1 disease: risk of failure after 2 years, nomogram (n=2911)
Walz et al., J Urol 2009
Failure risk:
• definite evidence for adjuvant RTX for margin-positive disease is still pending
• patients should be informed on the significance of the presently available results from randomized trial
• stratification by recurrence risk is a plausible but not yet proven concept to select patients
• with “temporarily delayed” RTX at PSA relapse, early onset is needed to maintain the chance of durable remission
Summary
Adjuvant hormonal therapy?

Prospective randomised study: flutamide vs. control after RPE in pT3-4 pN0 (n=309)
0 100 200 300 400 500 6000
20
40
60
80
100
weeks after RPE
recurrence-free survival [%]
log-rank-Test, p=0.0041
0 100 200 300 400 500 6000
20
40
60
80
100survival [%]
log-rank-Test, p=0.92
Flutamide, n=152
control, n=157
Wirth et al., Eur Urol 2004

EPC program: objective progression (prospective randomised trial, n=8116, FU 7.4 y)
McLeod et al., BJU Int 2006

McLeod et al., BJU Int 2006
EPC program: overall survival (prospective randomised trial, n=8116, FU 7.4 y)
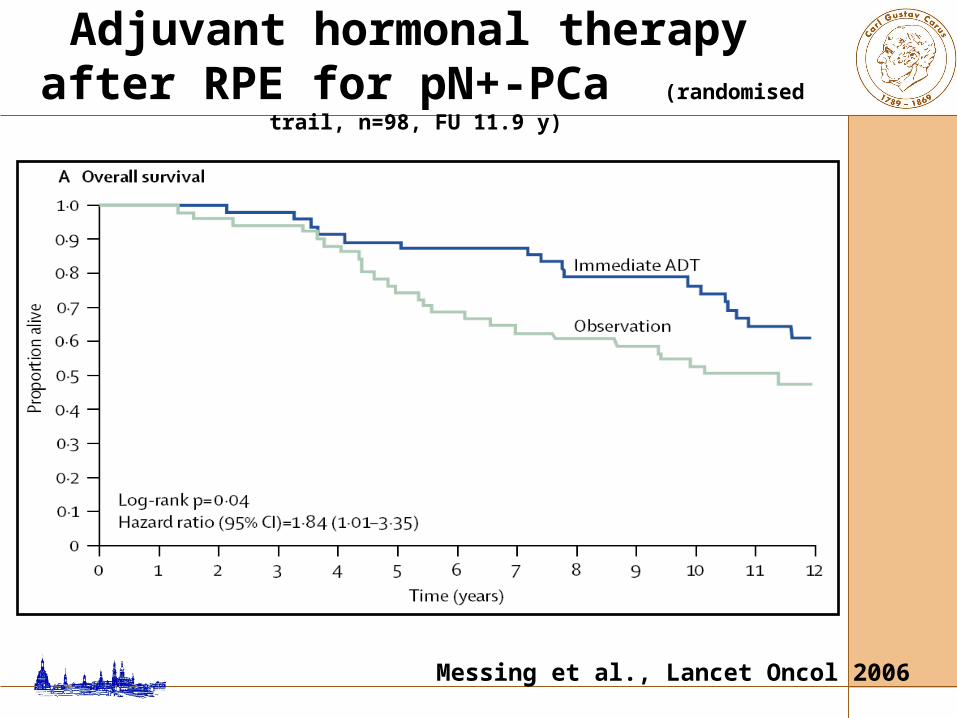
Adjuvant hormonal therapy after RPE for pN+-PCa (randomised trail, n=98, FU 11.9 y)
Messing et al., Lancet Oncol 2006
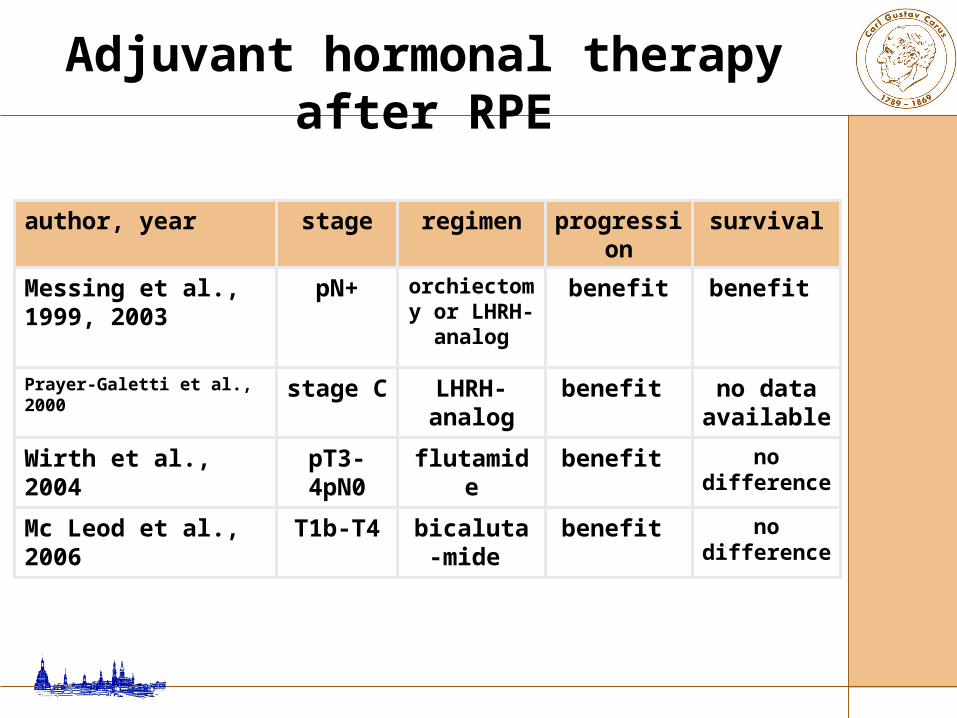
no difference
benefit flutamidepT3-4pN0
Wirth et al., 2004
no difference
benefit bicaluta-mide
T1b-T4Mc Leod et al., 2006
no data available
benefit LHRH- analog
stage CPrayer-Galetti et al., 2000
benefit benefitorchiectomy or LHRH-
analog
pN+Messing et al., 1999, 2003
survivalprogressionregimenstageauthor, year
Adjuvant hormonal therapy after RPE



BACKUP

M. Wirth Klinik und Poliklinik für Urologie
Adjuvant or Salvage Radiotherapy after Radical
Prostatectomy
6- 3+4 4+3 8-100
20
40
60
80
100
0-4 ng/ml4.1-10 ng/ml
10.1-20 ng/ml20+ ng/ml
% PSA-relapse (0.2 ng/ml) after 10 years
Gleason-ScoreHan, Partin et al., J Urol 2003
PSA-relapse after RPE in locally advanced PCa (n=2091)
preop. PSA
organconfined: 18 %
extracapsular: 82 %
cT3: MSKCC-Nomogramm: pT Stage Exampel: cT3, PSA 10 ng/ml, Gleason 4+4=8
Ohori, Kattan et al., J Urol 2004

cT3: MSKCC-Nomogramm:pT-Stage Exampel: cT3, PSA 10 ng/ml, Gleason 3+3=6
Ohori, Kattan et al., J Urol 2004
organconfined: 50 % extracapsular: 50 %
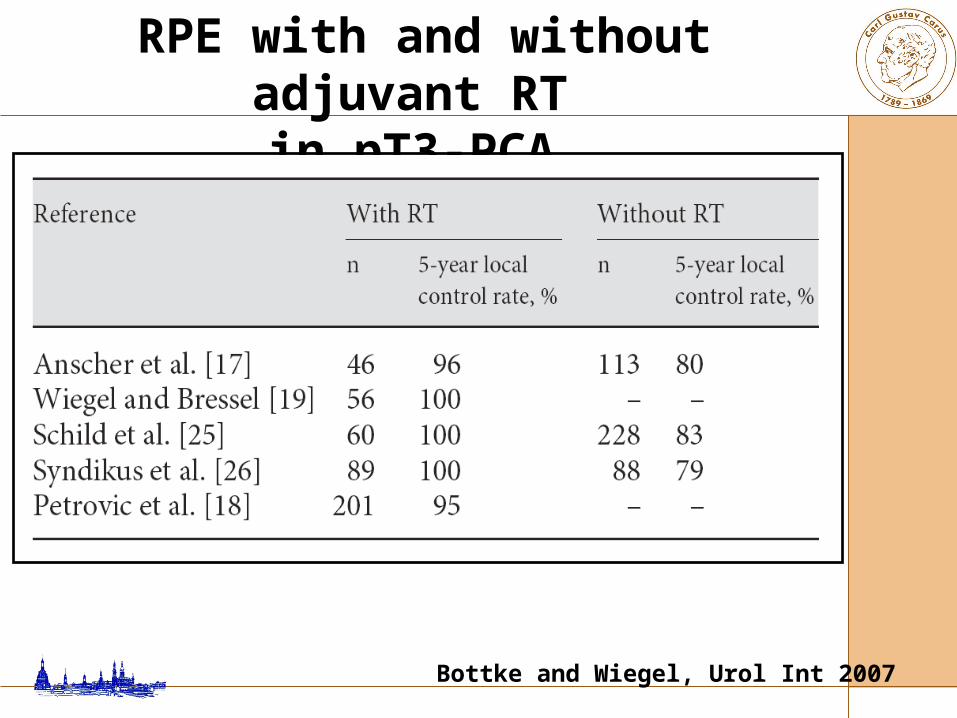
Bottke and Wiegel, Urol Int 2007
RPE with and without adjuvant RT in pT3-PCA
Randomised controlled trial clinical T1/T2 preoperatively pT3 or positive margins, N0 M0 WHO perf. status 0-2
Wait-and-see (n=211) vs. Irradition (60-64 Gy, n=214)
Thompson et al., JUrol 2009
Adjuvant RTX for T3N0M0 PCA – SWOG 8794
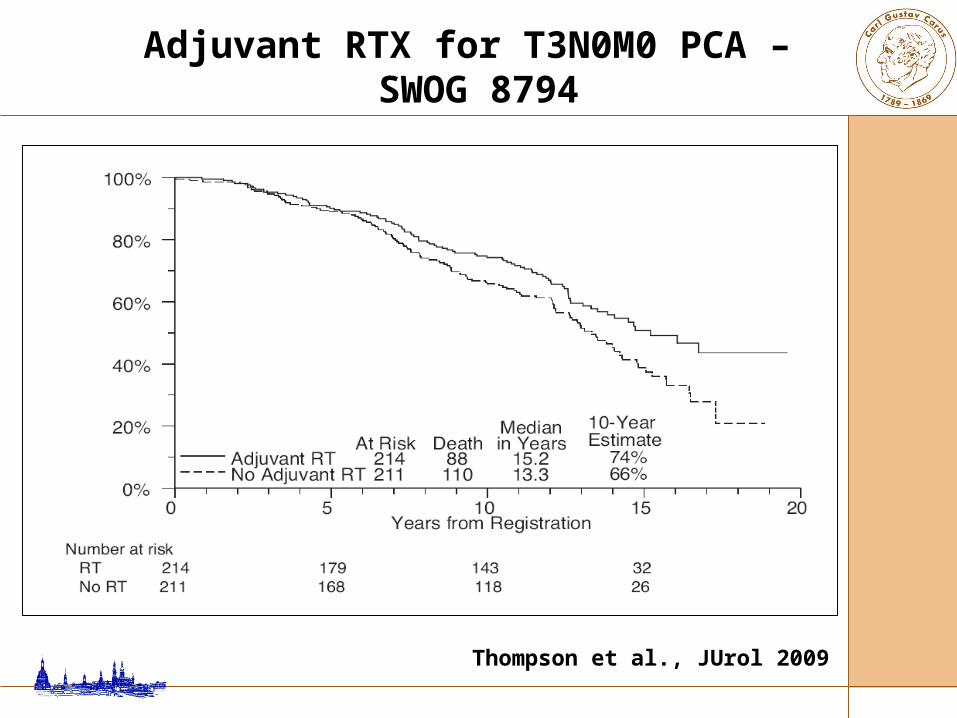
Thompson et al., JUrol 2009
Adjuvant RTX for T3N0M0 PCA – SWOG 8794

Randomised controlled trial pT3 or positive margins, pN0 age < 76 years, WHO perf. status 0-1
Wait-and-see (n=503) vs.
Irradiation (60 Gy) within 16 w. after RPE (n=502)
Bolla et al., Lancet 2005
wait-and-see vs. immediate postoperative radiotherapy - EORTC trial 22911

Age 65 y. (61-69) PSA: 12.4 ng/ml (7.2-20.3) PSA: 3 weeks after RPE, before RTX
0.2 (0.0-0.3) median FU 5 y. biochemical and clinical progression free
survival significantly improved after ART overall survival with trend towards
improvement after ART, but not (yet?) significant
Bolla et al., Lancet 2005
wait-and-see vs. immediate postoperative radiotherapy - EORTC trial 22911

EORTC trial 22911 clinical progression free survival
Bolla et al., Lancet 2005

EORTC trial 22911 biochemical progression free survival
Bolla et al., Lancet 2005
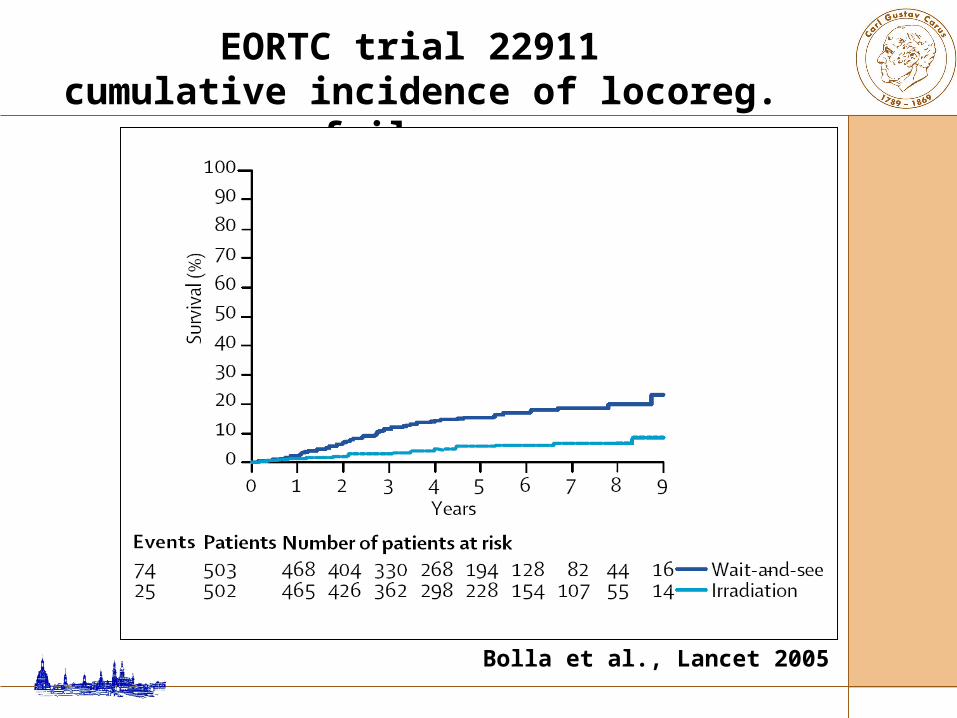
EORTC trial 22911 cumulative incidence of locoreg. failure
Bolla et al., Lancet 2005
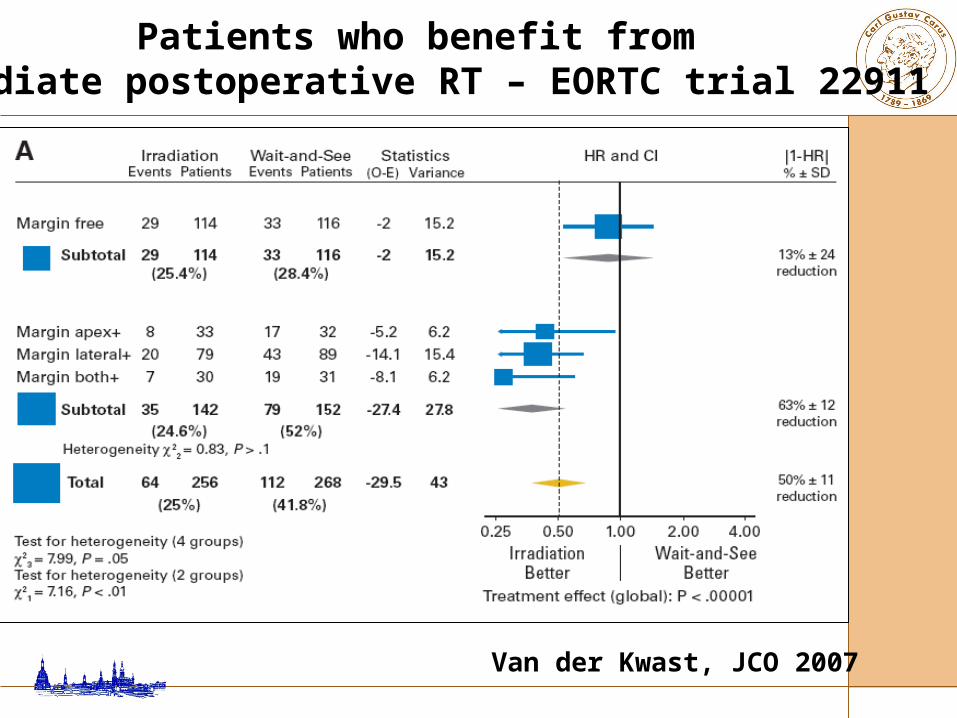
Patients who benefit from immediate postoperative RT – EORTC trial 22911
Van der Kwast, JCO 2007
Wiegel et al., ASCO 2005
adjuvant RT (60 Gy) no adjuvant RT
Adjuvant Radiotherapy after RPE (ARO 96-02 / AUO AP 09/95 , pT3R0-1, PSA 0, n=108)
% PSA recurrence after 4 years
0
20
40
60
80
100p<0.0001, hazard ratio 0.4
81 %60 %
PSA Recurrence after RPE:
Salvage Radiotherapy vs. Observation

Salvage radiotherapy within 2 years of biochemical recurrence was associated with a significant increase in CaP–specific survival among men with a PSA doubling time <6 months, independent of pathological stage or Gleason score.
JAMA 2008
PCA specific survival following salvage RTX vs observation after RPE – survival
Trock et al., JAMA 2009

no salvage treatment (n=397) vs. salvage radiotherapy (n=160) vs. salvage radiotherapy + HT (n=78)
significant increase of PC-specific survival for both SRT (HR 0.32, p<0.001) and SRT+HT (HR 0.34, p=0.003)
improvement limited to patients with - PSA-doubling time < 6 month - SRT within 2 y. after recurrence
Trock et al., JAMA 2009
PCA specific survival following salvage RTX vs observation after RPE – survival
PSA Recurrence after RPE:
Salvage Radiotherapy vs. Observation:
Timing?

Radiotherapy for PSA-Recurrence (n=1540)
Stephenson et al., JCO 2007
bis 0.5 ng/ml
0.51-1.0 ng/ml
1.01-1.50 ng/ml1.51+ ng/ml

PSA Failure following Salvage Radiotherapy – CaPSURE data
Macdonald et al., UrolOncolSemOrigInv 2008

Adjuvant Radiotherapy or after PSA-Recurrence (n=162)
Wiegel et al., IJROBP 2009

Adjuvant and Salvage RTX after RPE Biochemical failure free survival
Jereczek-Fossa, IntJRadOncolBiolPhys 2008
Adjuvant RT
Salvage RT

Adjuvant and Salvage RTX after RPE Biochemical failure free survival
Taylor et al., IntJRadOncBiolPhys 2003

p<0.0001
RT for PSA-Recurrence after RPE: Dosage?(n=122)
0 3 6 Jahre
No new PSA-recurrence
King et al. IJROBP 2008
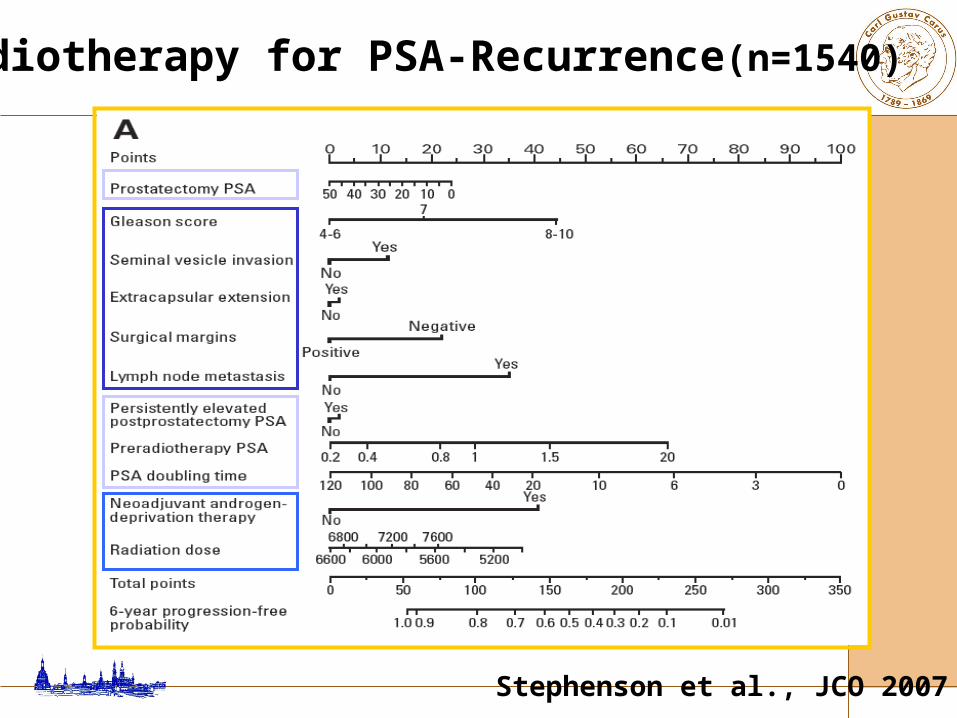
Radiotherapy for PSA-Recurrence(n=1540)
Stephenson et al., JCO 2007
• adjuvant and Salvage-RT after RPE both improve recurrance free survival and offer a second chance of cure
• adjuvant RT should be considered in patients with positive margins
Summary (I)

• Salvage-RT should be performed at a low PSA-level << 1.0 ng/ml
• postoperative RT has a limited effect on patients with pN+
• optimal radiation dose unclear
Summary (II)

BACKUP
• adjuvant and salvage-RT after RPE both improve recurrance free survival and offer a second chance of cure
• adjuvant RT should be considered in patients with positive margins
Summary (I)

• salvage-RT should be performed at a low PSA-level << 1.0 ng/ml
• postoperative RT has a limited effect on patients with pN+
• optimal radiation dose unclear
Summary (II)
Radiotherapy + HT vs. hormonal Therapy alone

Thompson et al., JAMA 2006
Adjuvant RT in pT3 PCA (randomised study SWOG 8794, n=425)
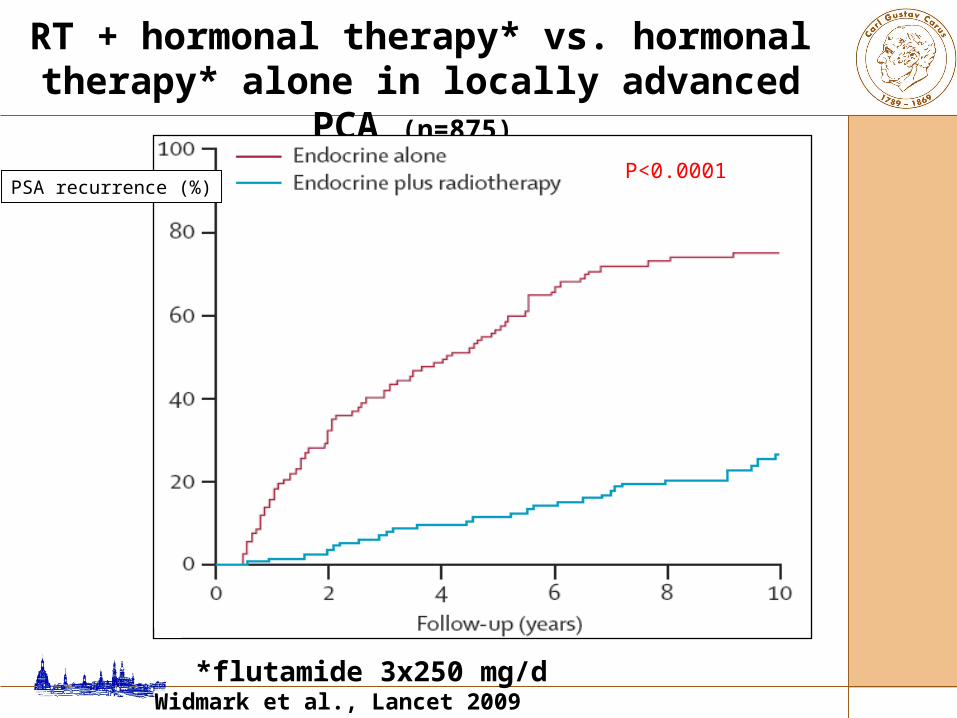
RT + hormonal therapy* vs. hormonal therapy* alone in locally advanced PCA (n=875)
*flutamide 3x250 mg/d Widmark et al., Lancet 2009
P<0.0001PSA recurrence (%)
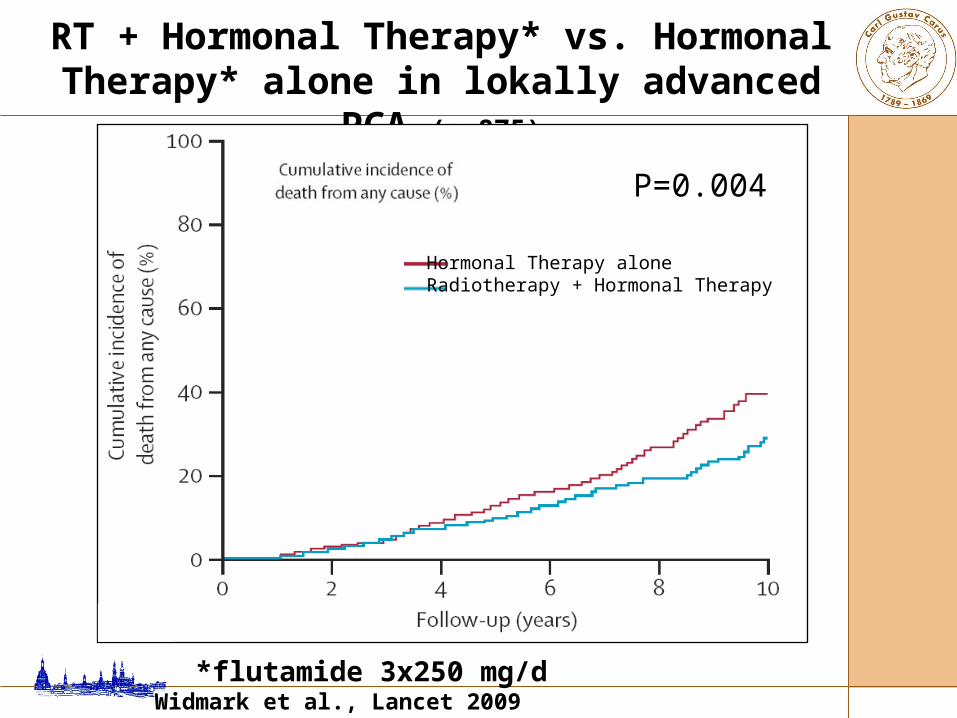
RT + Hormonal Therapy* vs. Hormonal Therapy* alone in lokally advanced PCA (n=875)
P=0.004
Hormonal Therapy alone Radiotherapy + Hormonal Therapy
*flutamide 3x250 mg/d Widmark et al., Lancet 2009

Adjuvant HT* after RT in organ confined high risk tumor *6 mo., n=206
D‘Amico et al., JAMA 2008

Short vs. long* adjuvant ADT after RT*3 years vs. 6 months
Bolla et al., ASCO 2007
Overall survival
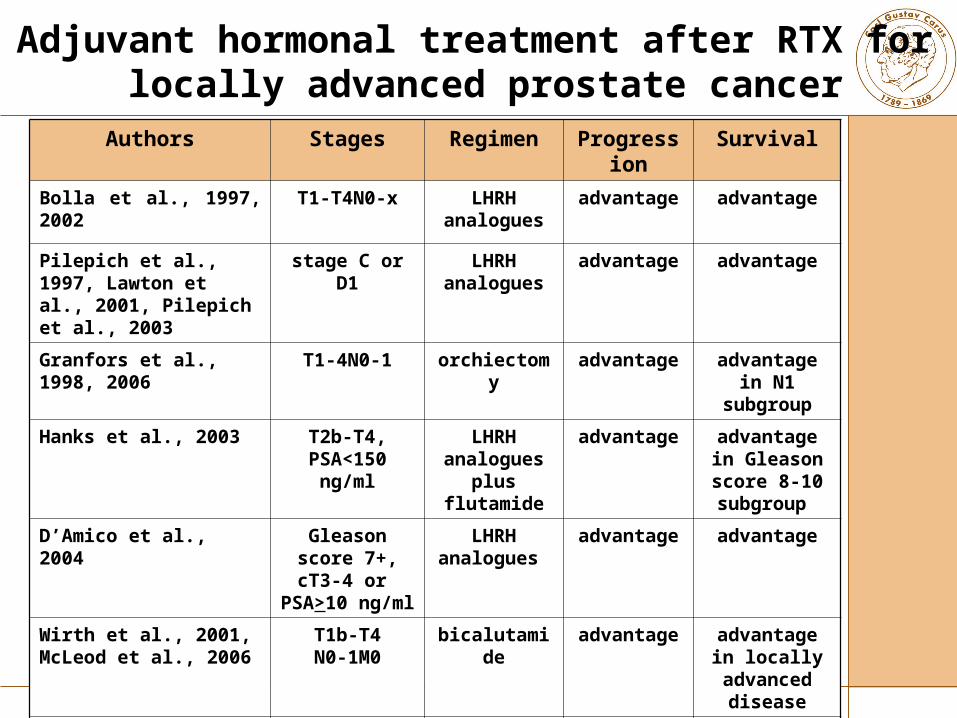
Authors Stages Regimen Progression Survival
Bolla et al., 1997, 2002 T1-T4N0-x LHRH analogues
advantage advantage
Pilepich et al., 1997, Lawton et al., 2001, Pilepich et al., 2003
stage C or D1 LHRH analogues
advantage advantage
Granfors et al., 1998, 2006 T1-4N0-1 orchiectomy advantage advantage in N1 subgroup
Hanks et al., 2003 T2b-T4, PSA<150 ng/ml
LHRH analogues plus
flutamide
advantage advantage in Gleason score 8-10 subgroup
D’Amico et al., 2004 Gleason score 7+, cT3-4 or
PSA>10 ng/ml
LHRH analogues
advantage advantage
Wirth et al., 2001,McLeod et al., 2006
T1b-T4N0-1M0
bicalutamide advantage advantage in locally
advanced disease
D’Amico et al., 2006 Localized or locally advanced, PSA velocity
>2ng/ml/y
Not specified advantage advantage
Adjuvant hormonal treatment after RTX for locally advanced prostate cancer
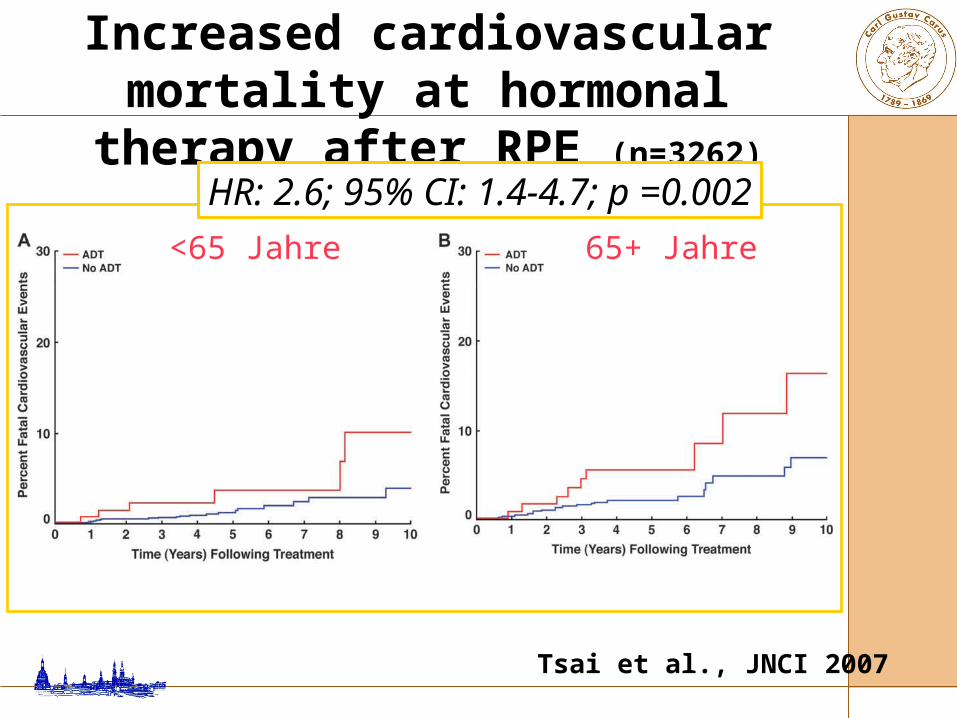
Increased cardiovascular mortality at hormonal therapy after RPE (n=3262)
Tsai et al., JNCI 2007
<65 Jahre 65+ Jahre
HR: 2.6; 95% CI: 1.4-4.7; p =0.002

D‘Amico et al., JAMA 2008
Negative consequences of androgen suppression in men
with comorbidities and RT in high-risk PCA (randomised trial, n=206)

After RPE adjuvant hormonal therapy is not necessary!
After radiotherapy an adjuvant hormonal therapy
is recommended(side effects!) for at least 3
years.
• good results after RPE
• adjuvant / early RT after RPE improves recurrance free survival and offers a second chance of cure
• neoadjuvant hormonal therapy after RPE not necessary
Summary (I)

• adjuvant hormonal therapy after RPE is not necessary – no survival benefit
• radiotherapy + hormonal therapy is recommended
• best concept of hormonal therapy adjuvant to radiotherapy is unclear
Summary (II)


















