
Lynne Colagiovanni, former Consultant Nurse, and Jane ...
8
Protouch Protouch 350 Ambidextrous Examination Gloves 100PCS Ref: Size Large 350 Ambidextrous Examination Gloves Ref: Size Large 100PCS 60 - 59 - 58 - 5 7 - 5 6 - 5 5 - 54 - 5 3 - 52 - 5 1 - 5 0 - 49 - 4 8 - 47 - 4 6 - 45 - 44 - 43 - 4 2 - 4 1 - 4 0 - 3 9 - 3 8 - 3 7 - 3 6 - 3 5 - 34 - 33 - 32 - 31 - 30 29 - 2 8 - 27 - 2 6 - 2 5 - 2 4 - 2 3 - 2 2 - 2 1 - 2 0 - 19 - 18 - 1 7 - 1 6 - 15 - 14 - 1 3 - 1 2 - L u b r i ca t i n g J e l l y / F o r P r o f e s s i o n a l a n d H o s p i t a l U s e 5 . 0 g m ( 0 . 1 7 o z ) S t e r i l e G e l e e l a brif i a n t e / P o u r u s a g e p r o f e s s i o n a l e t e n m i l l e u h o s p i t a l i e r S t e r i l e R S t e r i l e S c h m i e r ga l l e r i e / F u r A r z t - u n d K r a s k e r s c h a u s g e r b r a u c h S t e r i l e G e l a t i n a la b r i f i c a n t e / P r r u s o m e d i c o e d o s p e d a l i e r o S t e r i l e P a s t a m et a l i e / V o o r P r o f e s s i o n e l G e b r u i k e n G e b r u i k i n Z i e k e n h u i z e n E s t e r i l G e l l u b r i c a n t e / P a r a U s o P r o f e s s i o n a l y H o s p i t a l a r i o Lubricating Jelly / For Professional and Hospital Use 5.0gm (0.17 oz) Sterile Gelee labrifiante/ Pour usage professional et en milleu hospitalier Sterile R Sterile Schmiergallerie/ Fur Arzt-und Kraskerschausgerbrauch Sterile Gelatina labrificante/ Prr uso medico ed ospedaliero Sterile Pasta met alie/ Voor Professionel Gebruik en Gebruik in Ziekenhuizen Esteril Gel lubricante/ Para Uso Professional y Hospitalario pH 3.0 3.5 4.0 4.5 5.0 5.5 6.0 LOT Expiry date Store cool and dry. (15 - 25 °C) Place 2-3 drops of aspirate onto the test zones. Allow any excess aspirate on the indicator strip to run off onto a paper towel. Within 20 to 60 seconds read off the corresponding pH. HC771304 SEP 2023 pH strips Non-sterile gloves Apron Box of tissues Glass of water or squash and straw (if appropriate) Lubricant according to local policy Water for flushing tube (type will depend on local guidelines) Nasogastric feeding tube Receiver/vomit bowl Nasogastric tubes used for feeding must be radio-opaque throughout their length and have externally visible centimetre markings (NPSA, 2011). Always follow local policies and guidelines, where these exist. These pages show the ENFit ® connector, as per the ISO standard (GEDSA, 2017). pH paper or strips must bear the CE mark, which confirms that they comply with European Union legislation, and have been manufactured specifically for the purpose of testing human gastric aspirate. Suitable hypoallergenic tape 0 1 2 0 3 0 4 0 5 0 6 0 0 1 2 0 3 0 4 0 50 6 0 50/60-mL enteral syringe Pen (to mark tube if needed) Feeding via a fine-bore nasogastric feeding tube is a common method of providing short-term nutritional support, usually to patients in acute hospital settings, although it can also be used for community and care home patients who require longer-term feeding. The benefit of this type of feeding tube is that it can be inserted easily and quickly at the patient’s bedside. Indications for insertion of a nasogastric feeding tube include: • Those with an unsafe swallow, for example as a result of stroke, motor neurone disease or head injury; • Altered level of consciousness, as in ventilated patients; • To supplement oral intake. Contraindications include basilar skull fractures, facial injuries and oesophageal obstruction (Sigmon & An, 2021). Discuss cases such as these with the nutrition support team as you may need to consider other methods of tube insertion. Risks associated with the insertion of fine-bore nasogastric feeding tubes include inadvertent placement into the lungs and/or displacement from the stomach leading to aspiration of the feed, fluids or medication. When deciding to insert a nasogastric feeding tube, it is important to consider the anticipated risks and benefits for the individual patient. Gain consent from the patient, and clearly document the decision and rationale for insertion of a nasogastric feeding tube in the patient’s medical notes. Healthcare professionals should complete competency-based training before carrying out the insertion of a nasogastric feeding tube (NPSA, 2011). It is essential that you confirm the position of the tube before introducing any feed, fluid or medication (NPSA, 2012). Administering feed, fluid or medication via a nasogastric tube that is found to be in the lung is known as a “never event”. This can lead to aspiration pneumonia and potentially serious harm to the patient. Never events can also have serious consequences for the healthcare professionals involved (Williams & McDavid, 2012). Confirmation of the nasogastric feeding tube position is usually determined by collecting gastric aspirate via the tube and testing it with pH paper (or sticks). In order to indicate correct placement of the tube, the pH reading must lie between 1 and 5.5 (NPSA, 2011). However, always follow local guidance. These pages also include a troubleshooting guide that you can use if an aspirate cannot be obtained or if the aspirate has a pH of greater than 5.5. Page 1 of 8 Nutrition Adults Inserting a fine-bore nasogastric feeding tube Lynne Colagiovanni, former Consultant Nurse, and Jane Fletcher, Lead Nurse for Nutrition, Queen Elizabeth Hospital, University Hospitals Birmingham NHS Foundation Trust ©2021 Clinical Skills Limited. All rights reserved Equipment Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person. Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution. Gather the equipment that you will need. Check the expiry dates on the packaging. Introduce yourself to the patient and discuss the procedure with them, clearly explaining the risks and benefits.
Transcript of Lynne Colagiovanni, former Consultant Nurse, and Jane ...

Protouch
Protouch
350Ambidextrous
Examination Gloves
100PCS
Ref:Size Large
350AmbidextrousExamination Gloves Ref:
Size Large
100PCS
6 0 - 5 9- 5 8
-5 7
-
5 6
-
5 5-
5 4-
53
-5
2-
51-
50-
49
-
48
-47
-46
-45-44-43-42
-41
-
40
-39
-38
-3
7-
36
-35
-3 4
-
3 3
-
32-
31-
302 9 - 28 - 2 7
-2 6
-2 5
-24
-2
3-
22
-2
1-
20-
19-
18
-
17-
16-15-14-13-12
-
Lubricating Jelly / For Professional and Hospital Use 5.0gm (0.17 oz)Sterile Gelee labrifiante / Pour usage professional et en milleu hospitalier
Sterile R
Sterile Schmiergallerie / Fur Arzt-und KraskerschausgerbrauchSterile Gelatina labrificante / Prr uso medico ed ospedalieroSterile Pasta met alie / Voor Professionel Gebruik en Gebruik in ZiekenhuizenEsteril Gel lubricante / Para Uso Professional y Hospitalario
Lubricating Jelly / For Professional and Hospital Use 5.0gm (0.17 oz)Sterile Gelee labrifiante / Pour usage professional et en milleu hospitalier
Sterile R
Sterile Schmiergallerie / Fur Arzt-und KraskerschausgerbrauchSterile Gelatina labrificante / Prr uso medico ed ospedalieroSterile Pasta met alie / Voor Professionel Gebruik en Gebruik in ZiekenhuizenEsteril Gel lubricante / Para Uso Professional y Hospitalario
pH 3
.0
3.5
4
.0
4.5
5
.0
5.5
6
.0
LOT Expiry date
Store cool and dry. (15 - 25 °C) Place 2-3 drops of aspirate onto the test zones.
Allow any excess aspirate on the indicator strip to run off onto a paper towel.
Within 20 to 60 seconds read off the corresponding pH.
HC771304 SEP 2023
pH strips
Non-sterile gloves
Apron
Box of tissues
Glass of water or squash and straw (if appropriate)
Lubricant according to local policy
Water for flushing tube (type will depend on local guidelines)
Nasogastric feeding tube
Receiver/vomit bowl
Nasogastric tubes used for feeding must be radio-opaque throughout their length and have externally visible centimetre markings (NPSA, 2011). Always follow local policies and guidelines, where these exist. These pages show the ENFit® connector, as per the ISO standard (GEDSA, 2017).
pH paper or strips must bear the CE mark, which confirms that they comply with European Union legislation, and have been manufactured specifically for the purpose of testing human gastric aspirate.
Suitable hypoallergenic tape
01 20 30 40 50 60
01 2 0 3 0 4 0 5 0 6 0
50/60-mL enteral syringe
Pen (to mark tube if needed)
Feeding via a fine-bore nasogastric feeding tube is a common method of providing short-term nutritional support, usually to patients in acute hospital settings, although it can also be used for community and care home patients who require longer-term feeding. The benefit of this type of feeding tube is that it can be inserted easily and quickly at the patient’s bedside.
Indications for insertion of a nasogastric feeding tube include:• Those with an unsafe swallow, for example as a result of stroke, motor
neurone disease or head injury;• Altered level of consciousness, as in ventilated patients;• To supplement oral intake.
Contraindications include basilar skull fractures, facial injuries and oesophageal obstruction (Sigmon & An, 2021). Discuss cases such as these with the nutrition support team as you may need to consider other methods of tube insertion.
Risks associated with the insertion of fine-bore nasogastric feeding tubes include inadvertent placement into the lungs and/or displacement from the stomach leading to aspiration of the feed, fluids or medication.
When deciding to insert a nasogastric feeding tube, it is important to consider the anticipated risks and benefits for the individual patient. Gain consent from the patient, and clearly document the decision and rationale for insertion of a nasogastric feeding tube in the patient’s medical notes.
Healthcare professionals should complete competency-based training before carrying out the insertion of a nasogastric feeding tube (NPSA, 2011). It is essential that you confirm the position of the tube before introducing any feed, fluid or medication (NPSA, 2012). Administering feed, fluid or medication via a nasogastric tube that is found to be in the lung is known as a “never event”. This can lead to aspiration pneumonia and potentially serious harm to the patient. Never events can also have serious consequences for the healthcare professionals involved (Williams & McDavid, 2012).
Confirmation of the nasogastric feeding tube position is usually determined by collecting gastric aspirate via the tube and testing it with pH paper (or sticks). In order to indicate correct placement of the tube, the pH reading must lie between 1 and 5.5 (NPSA, 2011). However, always follow local guidance. These pages also include a troubleshooting guide that you can use if an aspirate cannot be obtained or if the aspirate has a pH of greater than 5.5.
Page 1 of 8
NutritionAdults
Inserting a fine-bore nasogastric feeding tubeLynne Colagiovanni, former Consultant Nurse, and Jane Fletcher, Lead Nurse for Nutrition,
Queen Elizabeth Hospital, University Hospitals Birmingham NHS Foundation Trust
©2021 Clinical Skills Limited. All rights reserved
Equipment
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Gather the equipment that you will need. Check the expiry dates on the packaging. Introduce yourself to the patient and discuss the procedure with them, clearly explaining the risks and benefits.

Nutrition
Adults
Inserting a fine-bore nasogastric feeding tube Page 2
Gain the patient’s consent Provide a vomit bowl
Position the patientAgree a signal
Perform hand hygiene and put on PPE Check the guidewire
You must gain consent before inserting a nasogastric feeding tube. Document verbal consent and details of the discussion in the patient’s notes. If you think that the patient lacks the capacity to consent to the procedure, carry out a capacity assessment (Mental Capacity Act, 2005) before making and documenting a best-interest decision.
Explain to the patient that the procedure may make them gag, and provide them with a vomit bowl.
You may wish to involve a colleague to assist you in supporting the patient. Help the patient to sit in a semi-upright position in a bed or chair, supported with pillows behind the head (Shaw et al., 2020). Make sure that the patient’s head is flexed slightly forward as this reduces the risk of tracheal intubation (Mensforth & Nightingale, 2001).
You and the patient should agree on a signal to indicate that the patient would like you to pause or stop the procedure. As you do not want the patient to speak to you while you are passing the tube, the signal could be to lift a hand.
If there is a guidewire, first make sure that it moves freely within the tube to avoid snagging on removal, and that it is firmly engaged in the tube.
Page 2 of 8
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Decontaminate your hands with soap and water or using an alcohol-based hand sanitiser, and put on an apron and gloves (Loveday et al., 2014).

0 + 2 + 4 + 6 + 8 + 10 + 12 + 14 + 16 + 18
54 +52
+50
+48
+46
+44
+42
+40
+38
+36
+34
+32
+30
+28
+26
+24
+22
+20
+18
+16
+14
+12
+
80+
78+
76+
74+
72+
70+
68+
66+
64+
62+
--60
+58
+56
+
14 +
12 +
pH 3
.0
3.5
4
.0
4.5
5
.0
5.5
6
.0
LOT Expiry date
Store cool and dry. (15 - 25 °C) Place
2-3 d
rops o
f asp
irate
onto
the te
st zo
nes.
Allow
any e
xces
s asp
irate
on th
e ind
icator
strip
to ru
n off o
nto a
pape
r towe
l.Wi
thin 2
0 to 6
0 sec
onds
read
off th
e corr
espo
nding
pH.
HC771304 SEP 14
01 20 30 40 50 60
80+78+76+74+72+70
+
68+
66
+
64+
62+
-
Lubricating Jelly/ For Professional and Hospital Use
5.0gm (0.17 oz)
Sterile Gelee labrifiante / Pour usage professional et en milleu hospitalier
Sterile RSterile Schmiergallerie / Fur Arzt-und Kraskerschausgerbrauch
Sterile Gelatina labrificante / Prr uso medico ed ospedaliero
Sterile Pasta met alie / Voor Professionel Gebruik en Gebruik in Ziekenhuizen
Esteril Gel lubricante / Para Uso Professional y Hospitalario
0 +
2 + 4 + 6 + 8 + 10 + 12 + 14 + 16 + 18 + 20 + 22 + 24 + 26 + 28 + 30 + 32 + 34 + 36 + 38 + 40 + 42 + 44 + 46 + 48 + 50
4 + 52+
50+
48+
46+
44+
42+
40+
38+
36+
34+
32+
30+
28+
26+
24+
22+
20+
18+
16+
14+ -- 12
80+
78+
76+
74+
72+
70+
68+
66+
64+
62+
--60
+58
+
56+
14 + 12
Nutrition
Adults
Inserting a fine-bore nasogastric feeding tube Page 3
Measure the tube: (a) Nose to earlobe (b) Earlobe to xiphisternum
Lubricate the tube Insert the tube: (a)
(b) Dealing with obstructions (c) Encourage swallowing
Use the NEX (nose to earlobe to xiphisternum) measurement as a guide to the correct tube length. First measure the distance from the nose to the earlobe, holding the distal tip (exit port) of the tube at the tip of the nose.
Then measure from the earlobe to two finger-widths below the xiphisternum. Note the nearest centimetre marking on the tube; this is a guide to how far you will need to insert the tube. Some evidence supports adding 10 cm to this measurement (Fan et al., 2019); follow local policy.
If the tube has a side port, close it. Lubricate the tube according to the manufacturer’s guidelines and local policy. Some lubricants may affect the pH reading; follow local policy regarding choice of lubricant.
Ask the patient which nostril they would prefer you to use; check the nostril for patency. Insert the tube into the chosen nostril and advance straight backwards along the floor of the nose to the nasopharynx (approximately 8 to 10 cm). Keep reassuring the patient as it can be an uncomfortable procedure.
As the tube moves down into the nasopharynx, ask the patient (if appropriate) to swallow water or squash through a straw. Encourage patients who are unable to drink to mimic the action of swallowing if possible.
Page 3 of 8
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
If you feel an obstruction, try rotating the tube and gently move it in a slightly different direction. If you are still unable to pass the tube, try the other nostril. If you are unable to pass the tube after three attempts, you must stop and seek help from specialist staff.

80+
78
+76 + 74 + 72
+70
+68
+66
+64
+62
+60
+58
+56
+102030405060
30+
28+
26+
24+
22+ 20 + 18 + 16 +
14
+12
+
60
+
59
+58
+57
+56
+5
5+
54
+
5 3+ 5 2 + 5 1 - 5 0
4 44 5 +
80 + 78
+76
+74
+72
+70
+68
+66
+64
+62
+
60+
58
1 02 03 04 05 06 0
pH 3
.0
3.5
4
.0
4.5
5
.0
5.5
6
.0
LOT Expiry date
Store cool and dry. (15 - 25 °C) Place
2-3 d
rops o
f asp
irate
onto
the te
st zo
nes.
Allow
any e
xces
s asp
irate
on th
e ind
icator
strip
to ru
n off o
nto a
pape
r towe
l.Wi
thin 2
0 to 6
0 sec
onds
read
off th
e corr
espo
nding
pH.
HC771304 SEP 2023
10
20
30
40
50
60
pH 3.0 3.5 4.0 4.5 5.0 5.5 6.0
LOT Expiry date
Store cool and dry. (15 - 25 °C)
Place 2-3 drops of aspirate onto the test zones.Allow any excess aspirate on the indicator strip to run off onto a paper towel.
Within 20 to 60 seconds read off the corresponding pH.
HC
771304 SEP 2023
Nutrition
Adults
Inserting a fine-bore nasogastric feeding tube Page 4
(d) Encourage patient to tuck their chin down (e) Advance the tube
Check the position of the tube: (a) (b) Slowly aspirate a small amount of fluid
Deposit aspirate onto a pH strip Read the pH value
Swallowing closes the glottis, encouraging the tube to pass into the oesophagus (Shaw et al., 2020). For patients who are unable to swallow or mimic swallowing, sometimes encouraging them to tuck their chin down may aid placement by providing airway protection (Pauloski, 2008).
As the patient swallows, advance the tube until you reach the mark you noted or made on the tube. Leave the guidewire in place until you have confirmed the correct position, as this makes manipulation of the tube easier should it need to be repositioned. Follow local policy.
Do not introduce any water or feed into the tube until you have confirmed the correct position (NPSA, 2012). Ask the patient (if they are able) to hold the tube close to the nostril. The aim is to prevent unnecessary movement of the tube, which can be uncomfortable. Open the appropriate port on the end of the tube and attach a 50/60-mL enteral syringe to the port. Do not use a smaller syringe, as it will create stronger suction, with the risk that the tube will collapse or cause gastric biopsy (Boeykens et al., 2014; Fletcher, 2011).
Slowly aspirate fluid. You need only a small amount, about 1 mL. Remove the syringe from the port and close the end of the port (see inset).
Deposit one to two drops of aspirate onto pH paper or a pH strip, ensuring that you cover all the test pads. Read the result within the time period specified on the product packaging: a pH of between 1 and 5.5 indicates that the tube is unlikely to be in the lungs but does not definitively confirm gastric placement. Therefore, always follow local guidelines regarding acceptable pH.
If you cannot obtain any aspirate, or the aspirate is above pH 5.5 (or the value set by local policy), follow the troubleshooting process described on page 7. If this is either unsuccessful or inappropriate, then an X-ray and confirmation by a competent healthcare professional is advisable to check that the tube is correctly positioned.
Page 4 of 8
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
80+ 78
+76
+74
+72
+70
+68
+66
+64
+62
+60
+58
+56
+
1 02 03 04 05 06 0
80
+7
8+
76+
7 4+
7 2+
7 0+
6 8
+
6
70+ 6 8
+
6 6
+
6 4
+
6 2+
6 0+
5 8+
5 6+
5 4+
5 2+
5 0 +4 8
+
Patient Notes ? X
OK Cancel
General Notes
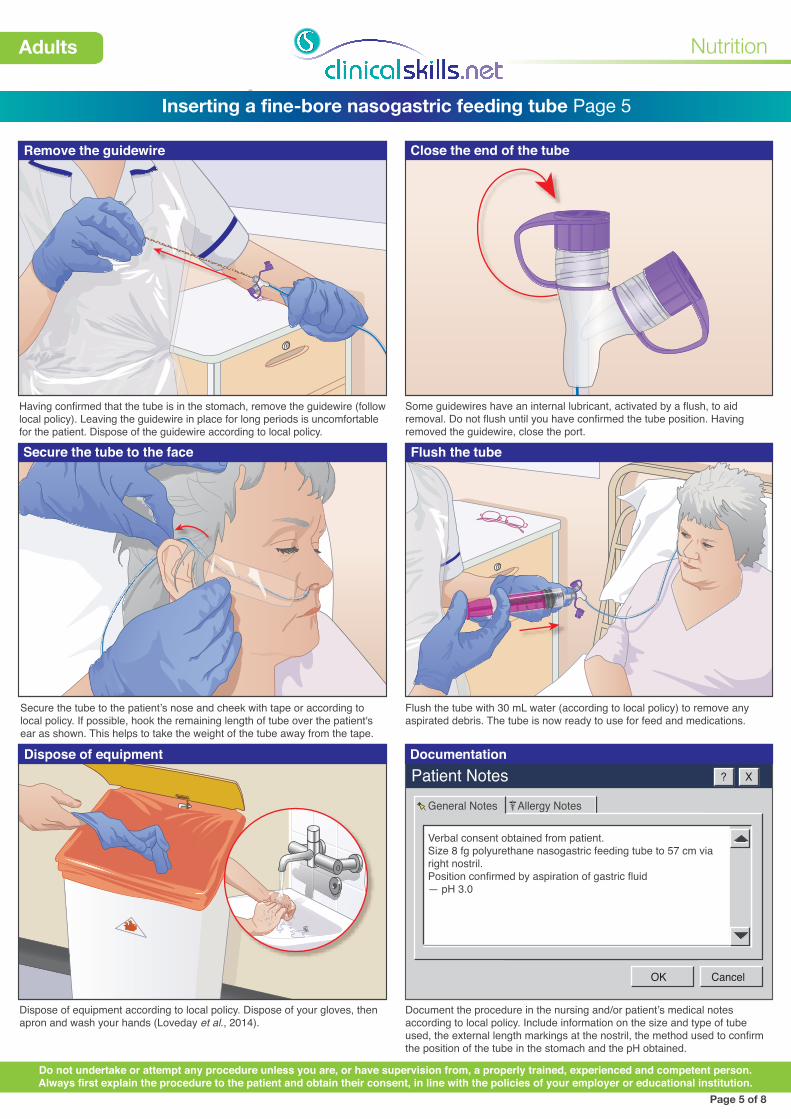
Verbal consent obtained from patient.Size 8 fg polyurethane nasogastric feeding tube to 57 cm via right nostril.Position confirmed by aspiration of gastric fluid— pH 3.0
Allergy Notes
Nutrition
Adults
Inserting a fine-bore nasogastric feeding tube Page 5
Remove the guidewire Close the end of the tube
Secure the tube to the face Flush the tube
Dispose of equipment Documentation
Having confirmed that the tube is in the stomach, remove the guidewire (follow local policy). Leaving the guidewire in place for long periods is uncomfortable for the patient. Dispose of the guidewire according to local policy.
Some guidewires have an internal lubricant, activated by a flush, to aid removal. Do not flush until you have confirmed the tube position. Having removed the guidewire, close the port.
Secure the tube to the patient’s nose and cheek with tape or according to local policy. If possible, hook the remaining length of tube over the patient's ear as shown. This helps to take the weight of the tube away from the tape.
Flush the tube with 30 mL water (according to local policy) to remove any aspirated debris. The tube is now ready to use for feed and medications.
Dispose of equipment according to local policy. Dispose of your gloves, then apron and wash your hands (Loveday et al., 2014).
Page 5 of 8
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Document the procedure in the nursing and/or patient’s medical notes according to local policy. Include information on the size and type of tube used, the external length markings at the nostril, the method used to confirm the position of the tube in the stomach and the pH obtained.

2 9-
2 8-
27-
26
-25
-24
2 4-
23-
22- 2 1
-2
0-
19
-18
-17-16-
2 9-
2 8-
27-
26
-25
-24
-23
2 9 -
28
-2
7-
26
-25
-
280
+
78+
76+
74+ 72 + 70 + 68 + 66 + 64 + 62 +
60+
58+ 56 + 54 + 52 + 50 + 48 + 44
+ 42+
40+
70
+6
8+
6 6+
6 4+
6 2+
6 0+
80+
78+
76+
74+
72+
70+
68+
66+
64
+62
+-- 60 + 58 + 56 +
10
20
30
40
50
60
1 02 03 04 05 06 0
8 0+
7 8+
7 6+
7 4+
7 2+
7 0
+
6 8
+
66+
6 4
+
6 2
70+ 6 8
+
6 6
+
6 4
+
6 2+
6 0+
5 8+
5 6+
5 4+
5 2+
5 0 +4 8
+
Nutrition
Adults
Inserting a fine-bore nasogastric feeding tube Page 6
Remove the nasogastric tube: (a) (b) Remove the tube quickly and gently
(c) Dispose of equipment and document removal Difficulty obtaining aspirate: (a) Alter patient's position
(b) Try injecting air into the tube (c) Withdraw or advance the tube
Removal of a nasogastric tube may be uncomfortable and stimulate a gag reflex. Explain this to the patient. Help the patient to sit in a comfortable upright position. Provide the patient with a receiver/vomit bowl and tissues in case they retch on removal. Decontaminate your hands and put on an apron and gloves. Carefully remove the adherent tape that is securing the nasogastric tube.
Gently pull on the tube until you have removed it completely from the patient’s nostril. It will be more comfortable for the patient if you do this fairly quickly.
Ensure that the patient is comfortable. Dispose of equipment according to local policy. Dispose of your gloves and apron and wash your hands (Loveday et al., 2014). Document removal of the tube in the patient’s notes.
If you are unable to obtain aspirate, try these strategies. If possible, turn the patient onto their left side. Altering the patient’s position may allow the tip of the nasogastric tube to move into the pool of gastric fluid.
If aspirate still cannot be obtained, inject 10 mL of air into the tube with a 50/60-mL enteral syringe. This may remove any debris from the tube and may dislodge the tip of the tube from the gastric mucosa allowing aspiration. (Note that the aim of this procedure is not to test whether the tube is in the stomach: do not carry out auscultation of air to confirm the tube position, as this method is unreliable and against National Patient Safety Agency [NPSA] guidelines.)
If still unable to obtain aspirate, gently withdraw or advance the tube by 10 to 20 cm. The tube may not be far enough into the stomach for the tip to reach the gastric pool or, alternatively, may be coiled within the stomach. If still unable to obtain aspirate, you may need to confirm the position of the tube on an X-ray, according to local policy.
Page 6 of 8
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.

Nutrition
Adults
Inserting a fine-bore nasogastric feeding tube Page 7
Troubleshooting flow diagram
Page 7 of 8
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
A pH of between 1 and 5.5 reliably confirms that the tube is not in the lung, but does not confirm gastric placement (the tip could lie in the oesophagus, with a higher risk of aspiration). If there is any concern, confirm the position of the tube with an X-ray checked by a healthcare professional who has undergone competency-based training. The NPSA (2011) recommends that where pH readings are borderline, a second competent person checks the reading or retests the aspirate. Therefore a second competent person should check the reading or retest the aspirate if the first reading is 5.0 or 5.5.
When confirming the position of a nasogastric tube in adults:
1. Consider whether the patient is taking an acid-inhibiting medication.
2. For a tube that is already inserted, check for signs that the tube might have become displaced; note the centimetre marking at the nostril, measure tube length and compare with the figures in the patient’s notes. If possible, check that the tube is not coiled at the back of the patient's throat.
3. Aspirate with a 50/60-mL enteral syringe. You will need approximately 1 mL of fluid. Test the aspirate on pH paper.
One option is to repass or replace the tube and then again attempt to confirm its position in the stomach. Alternatively, check the tube’s position with an X-ray, confirmed by a competent person.
START FEEDYou must document the length of the tube at the nostril and the pH result, or the result of the X-ray confirming gastric position.
Aspirate obtained?
NO
Aspirate obtained:Check pH and
proceed according to the result
Still no aspirate
DO NOT FEEDYES
Try each of the techniques below and attempt to aspirate again after each one:
1. Turn the patient onto their left side.
2. Inject 10 mL of air into the tube using a 50/60-mL syringe.
3. Advance or withdraw the tube by 10–20 cm.
4. Wait for 15–30 minutes and try to obtain aspirate again.
5. Give mouth care to patients who are “nil by mouth”, to stimulate gastric acid secretion.
pH 6.0 or aboveDO NOT FEED
pH 5.5or below
Try to obtain aspirate again after 1 hour
pH 6.0 or aboveDO NOT FEEDpH 5.5 or below

Patient Notes ? X
OK Cancel
General Notes
Verbal consent obtained from patient.Size 8 fg PUR nasogastric feeding tube to 57 cm via right nostril.Gastric aspirate pH 6.0.Patient is taking proton pump inhibitors.Chest x-ray obtained. See medical notes for documentation confirming position.
Allergy Notes
Document evidence of the correct position
Do not use the tube until there is clear documentation from the competent clinician interpreting the X-ray, describing the position of the tube and that it is safe to use.
The tube follows the line of the left bronchus
The tube lies in the left lower lobe of the lung
The tube fails to cross the diaphragm in the midline
28AMITRIPTYLINE25mgTABLETS
Take ONE at NIGHT
MrB.LOCK 21.MAY/23*10003KEEP OUT OF REACH OF CHILDREN
123 HIGH STREETA. POTHECARY
KEEP OUT OF REACH OFCHILDREN
romycin Tablets 250mgo be taken FOUR times dailyallow whole, do not chewplete the prescribed course
KEEP OUT OF REACH OF
CHILDREN
rythromycin Tablets 250mg
NE to be taken FOUR times daily
Swallow whole, do not chew
omplete the prescribed course
The tube does not follow the line of a bronchus
The tube descends in a straight line to below the diaphragm
Check that the X-ray is for the correct patient, and that it is the most recent film for that patient
The tube is not kinked or coiled
The tube crosses the diaphragm in the midline and its tip sits below the diaphragm
Nutrition
Adults
Inserting a fine-bore nasogastric feeding tube Page 8
Unable to obtain aspirate of pH of 5.5 or below: (a) (b) Check the patient’s medication
(c) Consider chest X-ray to confirm position (d) X-ray showing an incorrectly positioned tube
If you can obtain aspirate but the pH is too high, check whether the patient has recently received fluid or food, or is taking medication that may affect the gastric pH (see right). If so, wait an hour to allow the stomach to empty and the pH to fall, aspirate and test again.
Check whether the patient is on any medication that may alter the gastric pH, for example antacids, H2 antagonists and proton pump inhibitors. If so, it may not be possible to get a pH of 5.5 or below. Follow local policy.
If still unable to obtain an aspirate pH of 5.5 or below, consider confirming the position of the tube on a chest X-ray, according to local policy. A doctor who has undergone competency-based training should review the X-ray, document the position of the tube in the patient’s notes, and state whether it is safe to use for feeding. If the tube is correctly positioned (as shown above), feeding can commence (NPSA, 2011).
Page 8 of 8
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Change date to 23 please


















