Lymphoma: Treatment Updates
52
New Therapies for Lymphoma: An ASCO/ICML Update F B Hagemeister, MD Professor of Medicine Department of Lymphoma and Myeloma M D Anderson Cancer Center Bangkok 28 August 2015
Transcript of Lymphoma: Treatment Updates

New Therapies for Lymphoma: An ASCO/ICML Update
F B Hagemeister, MDProfessor of Medicine
Department of Lymphoma and MyelomaM D Anderson Cancer Center
Bangkok 28 August 2015

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

GCB and ABC DLBCLs: Two Different Mechanisms for Malignant Change
BCL-2 translocation Apoptosis
miR-17-92 mTOR amplification ActivationPTEN deletionING1 deletionMDM2 gain or Genomic amp InstabilityP53 mutation
MYC translocation
BCL-2 amplification ApoptosisNFK-B activation Apoptosis IL-6, IL-10 STAT3 IRF4 Essential 19Q gain Regulatory or amp SPIB Network Trisomy 3 FOXP1 Del ink4A-ARF Senescense Genomic InstabilityAID Switch TranslocationsMYC amp
GCB ABC
GCB Cell
PlasmablastPlasma Cell

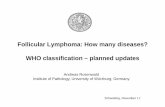
ADCC Activity with Rituximab Improves When Patients Are Given Vitamin D
Bittenbring et al. JCO 10: 3242-3428, 2014.
• Vitamin D levels tested at diagnosis of DLBCL• “Low” level: 8.4 + 3 ng/ml• Pts achieved 40.6 +13.6 ng/ml after given Vit D• ADCC activity tested before/after Vit D given

Effect of Vitamin D3 Levels on Results for Patients Receiving R-CHOP-14
Prop
ortio
n Pr
ogre
ssio
n Fr
ee
Prop
ortio
n A
live
Bittenbring et al. JCO 10: 3242-3428, 2014.
Prop
ortio
n A
live
Prop
ortio
n Ev
ent F
ree
Results from RICOVER-60 (Training Cohort)
Results from RICOVER-noRTh (Validation Cohort)

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

Novel Drugs for Aggressive NHLs?Agent Comment
ABT-199 Platelets-sparing BCL-2 inhibitor
BET Bromodomain Inhibitors Down regulators of MYC transcription
CAR-T cells T cell killing of CD-19 positive NHLs
Aurora kinase inhibitors Kinase needed for survival of MYC
mTOR inhibitors mTOR pathway important in MYC drive
Ixasomib (proteasome inhibitor) Inhibits MYC at n-molar concentrations
PI3K inibhitors Loss of PTEN leads to PI3K activation and increased MYC
SIRT4 protein Inhibits glutamine metabolism in MYC driven tumors
Inhibitors of mitochondrial peptide deformylase
In tumor models, cause apoptosis in MYC driven tumors by depolarizing mitochondrial membnrane

BV for Relapsed/Refractory CD30 Positive DLBCL
• 118 patients with DLBCL, Med prior TXs = 2, tested for CD30 by visual IHC and computer assisted method, all had elevated soluble CD30 blood levels
• Dose: 1.8 mg/kg q 3 wk with or without rituximab• CD30U = Undetected, but mRNA CD30 similar to those with
CD30 + cells
Smith et al. ICML-13, 2015, # 91.
CD30 + CD30U
Feature BV + R, # (%) BV, # (%) BV, # (%)
Refractory last TX 10 (63) 40 (82) 37 (70)
% CD30 Expression ND 37 2
CR 2 (15) 9 (19) 5 (10)
PR 4 (31) 11 (23) 8 (16)
Med PFS, Mo (Max) 2.4 (12+) 4 (24+) 1.4 (12.2+)

Lenalidomide + Rituximab for Ref/Rel DLBCL
Group No. of Pt. ORR CRR ReferenceUS 49 (various
histology)35% 12% Wiernik
2008
Italian 23 DLBCL 35% 4% Zinzani 2011
International 217 DLBCL 35% 13% Witzig 2011
Retrospective from 4 sites
40 DLBCLGCB 23
Non-GCB 179%
53%4%
24%
Hernandez-Illizaliturri
2011

Ibrutinib for Relapsed/Refractory DLBCL: Responses by Molecular Phenotype
Wilson et al. ASH, 2012.

Phase I CUDC-907, a Dual PI3K/HDAC Inhibitor for Ref/Rel NHL and Myeloma
• 51 patients enrolled, 41 evaluable for response• Dose: 3X3 escalation, with both frequency and dose given,
30-120 mg and 2 x wk, 3 x wk, 5 x wk• DLT in 3 = Diarrhea, hyperglycemia • 4/41 objective responses ( 1 CR, 3 PR, all in DLBCLs)
Younes et al. ICML-13, 2015, # 80.
Schedule Dose No. Pts Tumor Regression, # (%)
QD 30-60 10 3 (38)
BIW 60-150 12 7 (58)
TIW 60-150 15 5 (38)
5 x wk 60 14 4 (50)

PD-1 is Inactivated by PD-L1 and PD-L2 on Tumor Cells
• PD-1 is a protein on T-Cells that dampens the normal immune response
• Tumor cells can evade normal T-cell attack• Inactivate T-cell function by activation of PD-1 via PD-L1 and PD-L2
present on lymphoma cells
• T-Cells are “exhausted”• Cannot attack tumor cells• Inactivation is reversible

Phase I Nivolumab (BMS-936558) for Rel/Ref Lymphoid Malignancies
Lesokhin et al. ASH 2014 # 291
Resp
All B 29
FL 10
DLCL 11
All T 23
MF 13
PTCL 5
MM 27
PMBL 2
%OR 28 40 36 17 15 40 0 0
%CR 7 10 9 0 0 0 0 0
%PR 21 30 27 17 15 40 0 0
%SD 48 60 27 43 69 0 67 100
Ongoing studies in DLBCL and FL

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

Phase II Lenalidomide Plus R-CHOP for Patients with Untreated DLBCL
• 64 pts: Med age 65, 53% IPI 4-5. • Doses: Lenalidomide 25 mg qd,, d 1-10, plus R-CHOP-21 X 6 Support: PegFilgrastin day 2, aspirin prophylaxis• 60 evaluable pts compared with 87 historical pts treated with R-CHOP from same center• Result: ORR-98%, CR-80%. 2 yr EFS-59%, 2 yr OS- 78%.• By Hans Criteria:
• Conclude: Lenalidomide may erase the differences seen with R-CHOP by improving the results for non-GCB subtypes.
R-CHOP R2-CHOP
Feature GCB Non-GCB P GCB Non-GCB P
2 Yr PFS 64 28 <0.001 59 60 0.83
2 yr OS 78 46 <0.001 75 83 0.61
Nowakowski et al. JCO 32: 5s, 2014 (abst 8520).

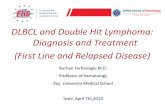
R-CHOP Compared with R2-CHOP for GCB and Non-GCB DLBCLs: PFS and OS Results
Nowakowski et al. JCO 33: 251-258, 2014.
Results with R-CHOP2 Yr PFS: G-64%; Non-G-28% 2 Yr PFS: G-59%; Non-G-60%
Results with R2-CHOP
P = 0.08P<0.001
2 Yr OS: G-76%; Non-G-82% 2 Yr OS: G-74%; Non-G-46%
P = 0.61P<0.001
GCBGCB
GCB GCB
Non-GCB Non-GCB
Non-GCBNon-GCB

Phase I Ibrutinib with R-CHOP for Patients with B-Cell NHLs
Dosing: R-CHOP standard doses, plus Ibrutinib at 280, 420, 560 mg daily
ORR = 100%, CR = 69%, PR = 31%
Responses at all dose levels, MTD not reached
Toxicities: ANC-77%, PLT -65%, and vomiting -59%
The basis of a trial of Ibrutinib-R-CHOP vs R-CHOP-placebo for pts with non-GCB subtype
Younes et al, ASCO 2013 # 8502.
Response DLBCL (N=8)
MCL (N=5)
FL (N=4)
Total (N=17)*
CR 2 4 1 7PR 2 1 2 5

Other Studies in DLBCL 2015UK R-CHOP + Bortezomib (REMoDL-B, up to 900 pt!)
– 2nd similar trial in US– Based on Ph 2 BR-CHOP, 95% CR, 4 yr PFS 58%
Intnl R-CHOP + Ibrutinib– Only for Non-GCB type by Hans Criteria– Based on Ph 1-2 IR-CHOP, 18 pt, 83% CR
R-CHOP + Maint Everolimus vs R-CHOP, 600 pt– Completed, not reported– Based on Ph 2 ER-CHOP, 3 yr PFS 76%– Alliance PH 1-2 R-CHOP + E also final to report
Furman et al. Cancer 116: 5432-5436, 2010. Younes et al. Lancet Oncol 15: 1019-1026, 2014. Micaleff et al. Blood
118: 4053-4061, 2011.

GOYA Phase III G-CHOP vs R-CHOP for Untreated CD20+ DLBCL: Study Design
Rituximab CHOP
GA101 CHOPPreviously untreated CD20
DLBCL (N=1400)
R
Primary endpoint:● PFS (investigator-
assessed)● TTNLT● Safety● QOL● Resource utilization
Secondary endpoints:● OS● Response rates● EFS● DFS● DOR
http://www.clinicaltrials.gov/ct2/show/NCT01287741 as of 09/01/13.
GA101=1000 mg d1, d8, d15 cycle 1; d1 cycles 2-8 q21d; rituximab 375 mg/m2 on d1 q21d cycles 1-8; CHOP=q21d 6-8 cycles

Phase II Randomized Dose BV + R-CHOP for Advanced Untreated DLBCL
• 51 patients: IPI 3 in 62%, IPI 4-5 in 38%.– ECOG 2 – 28%, Stage IV – 70%.
• Dose: 1.2 vs 1.8 mg/kg q 3 wk plus R-CHOP vs R-CHOP alone, reduced to 1.2 early on due to neuropathy with 1.8.• Gr 3-4 AEs: FN 27%, ANC 25%, HGB 24%
– All Gr PN: 38% at 1.2 mg/kg, 77% at 1.8 mg/kg.
• CR rates: ABC=GCB (69% vs 65%), but CD30 pos > CD30 neg (92% vs 69%). No PD for CD30+ with med f/u 5 mo.
Bartlett et al. ASCO 2015, Abst 8506.
Response 1.2 mg/kgN (%)
1.8 mg/kgN (%)
Total N (%)
CR 19 (66) 15 (68) 34 (67)PR 4 (14) 3 (14) 7 (14)PD 2 (7) 3 (14) 5 (10)

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

MYC Rearrangement (MYC-R) in DLBCL: DHL or DEL?
• In general, R positivity infers an inferior prognosis– R-CHOP therapy is inadequate, with < 12 mo OS
• High MYC protein expression without MYC-R has also been identified (alternate mechanism)– DLBCL with high MYC (>40%) and BCL-2 (50-70%)
protein expression by IHC = Double Expressor DLBCL (DEL)
– Also has a poor prognosis with R-CHOP• Should the approach to therapy be the same for
both DHLs and DELs?– Majority of DHL = GCB DLBCL– Majority of DEL = ABC DLBCL

R-CHOP-21 or Variants for DHLs
Author No. Pts
Therapy % MYC-R
%DHLs (BCL-2-R)
Outcome
Klapper 177 CHOP or CHOEP
8 NR OS worse for MYC-R
Barrans 303 R-CHOP 14 11 2 yr OS 35% (MYC-R) vs 61% (MYC-N)
Savage 135 R-CHOP 9 5 5 yr OS 33% (MYC-R) vs 72% (MYC-N)
Cunningham 1080 R-CHOP 14 or 21
6 3 No differences in 2 yr OS for MRC-R or N
MYC-R = Rearranged; MYC-N = Not rearranged

OtherTrials of Intensive Therapy for DHLsAuthor No.
PtsTherapy(% Pts)
Outcome (Mo, Median)
Comments
Petrich 311 R-CHOP -32R-HCVAD-21R-EPOCH-21R-CODOX-14
OS=22, PFS=10.9PFS 7.8 R-CHOP
vs 26.6 Other (p=0.001)
Med F/U=23 moNo OS diff among
intensive TXs; OS not affected by SCT
Oki 129 R-CHOP-44R-HCVAD-26R-EPOCH-22
2 yr EFS= 33%CR rates: 20% vs
70% vs 68%
OS better with R-EPOCH vs R-CHOP
(p=0.057); no benefit with SCT; 13% CNS
Johnson 54 CHOP-43R-CHOP-20
OS: R-CHOP=15 mo
CHOP=5 mo
BCL-2 Protein negative cases
favorable
Li 56 R-CHOP-39RHCVAD-59
OS: 19 mo Neither SCT nor intensive therapy made OS better
Petrich. Blood 124: 2354-2361, 2014. Oki. Br J Haematol 166: 891-901, 2014. Johnson. JCO 30: 3452-3459, 2012. Li. Adv Anat Path 20: 315-326, 2013.

Double Hit DLBCL in 100 MDACC Patients: A Retrospective Analysis
• CR rates: All 59%, CHOP + R 49%, EPOCH + R 50%, HCVAD + R 60% (P=NS). • 3 Year PFS (All pt) = 32%, OS = 41%. No diff by chemo regimen
Oki et al. ASH 2013 #1776 Dunleavy et al. ASH 2013 Hu et al, Blood 122: 2014
PFS by Therapy Regimen OS by Therapy Regimen
Similar results for DA-EPOCH-R from NCI., and R-CHOP consortium data.

Double Hit DLBCL in 100 MDACC Patients: A Retrospective Analysis
• SCT performed in 19 of 59 CRs• 3 Yr PFS: SCT 66%, None 45%. OS: SCT 67%, None 62%
Oki et al. ASH 2013 #1776.
PFS By SCT or None OS by SCT or None
But for 15 CRs after EPOCH + R, PFS = 100% (SCT in 8)

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell



New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

Ibrutinib Monotherapy in Relapsed/ Refractory FL: Max Tumor Vol Reduction
Bartlett NL, et al. ASH 2014. Abstract 800.
60
20
-20
-60
-100
Tum
or S
ize
(% C
hang
e in
SP
D F
rom
Bas
elin
e)
CRPRSDPD
72% of pts had reductionin tumor volume
Individual Pts

Phase 2 Idelalisib for 125 Alkylator-Rituximab Ref iNHL: Nodal Response and PFS Results
-100
-75
-25
0
-50a
+25
+50
Individual Patients (N=125)
SP
D o
f M
easu
red
Lym
ph
No
des,
Best
% C
han
ge f
rom
Baselin
e
•90% had improvement in lymphadenopathy•57% had ≥50% decrease from baselineGopal et al. ASH 2013 #85 .
Median PFS = 11.4 monthsMaximum Nodal Response
Historical Control:Bendamustine: DOR 10mo
53% ORR

Phase I IPI-145 (PI3K , Inhibitor) for NHLs and HL: Clinical Activity
Horwitz et al. ASCO 2012.

Phase I Ublituximab, TGR-1202, and Ibrutinib for Relapsed B-Cell NHLs
• Background– Ublituximab: A glycoengineered anti-CD20 MAB against
a unique epitope on CD20.– TGR-1202: A highly active oral PI3K inhibitor (Burris
2014). • TX: UTX-900 mg d 1,8,15 cycles 1-2, then q 2 mo
– TGR-400-1200 mg + Ibrutinib 420 (CLL) or 560 (NHL) QD• 12 pts, could have had Ibru or Idela; any # prior txs
– AEs (Gr 1-2): 30% diarrhea, constipation, fatigue, no DLT– Response: OR-75%, all iNHL or MCL
• Phase II study planned.
Fowler et al. ASCO 2015, Abst 2801. Nastoupil et al. ICML-13 2015, # 106.

Phase IIa Anti-CD19 Antibody (MOR208) for Rel/Ref NHLS
• Fc engineered humanized monoclonal antibody directed against CD19
• 89 patients, previously received rituximab, not candidates for SCT; Med prior therapies – 2.
• Dose 12 mg/kg IV weekly for 2, 28 day cycles• Gr 3-4 AEs: Non-hematologic in 30 pts (34%)• Hematologic Gr 3-4 events in 8 (9%)
Jurczak et al. ASCO 2015 Abst 8500.
Best Resp (N, %)
DLBCL (N=35)
FL (N=34)
MCL (N=12)
iNHL (N=11)
Total (N=92)
CR 2 (6) 2 (6) 0 2 (18) 6 (7)
PR 7 (20) 7 (21) 0 1 (9) 15 (16)
SD 5 (14) 17 (50) 6 (50) 4 (36) 32 (35)
Med DoR 2.6 (DLBCL), 7.7 (FL). Longest resp 62 and 67 wks. Combination trials planned.

Phase II Obinutuzumab for Relapsed or Refractory iNHL: Gauguin Study
Salles et al. JCO 31: 2920-2926, 2013.
Response Rates Progression Free Survival

GADOLIN Phase III Safety and Efficacy of G-Benda vs SA Benda for R-Refractory iNHL
G: 1000 mg d1, d8, d15 cycle 1; d1 cycles 2-6 q28daBendamustine: 90 mg/m2 d2, d3 cycle 1; d1, d2 cycles 2-6 q28d; bBendamustine: 120 mg/m2 on d1, d2 cycles 1-6 q28d
Bendamustineb
CR/PR/SD
Maintenance G
q2m 2 yearsG Bendamustinea
Rituximab-refractory iNHL (N=360)
R
Primary endpoint:● PFS
Secondary endpoints:● OS● Response rates
Sehn et al. ASCO 2015 Abst 8502; Cheson et al ICML-13, 2015, #123.

Phase III G-Benda vs SA Benda for R-Refractory iNHL: Pathology and Prior R Type
19.6 22.3
80.4 77.7
0
20
40
60
80
100
G-B(n=194)
B(n=202)
R-chemotherapycombination*
R-monotherapy
FL, follicular lymphoma; MZL, marginal zone lymphoma including extranodal, nodal and splenic; SLL, small lymphocytic lymphoma; WM, Waldenström macroglobulinemia.
Patie
nts
(%)
79.9 82.2
13.9 9.4
0
20
40
60
80
100
G-B(n=194)
B(n=202)
WDSLLMZLFL
Rituximab-refractory type
* Includes patients with relapse within 6 months of last dose of rituximab
Patie
nts
(%)
6.2 7.90.5
Lymphoma subtype
Sehn et al. ASCO 2015 Abst 8502; Cheson et al ICML-13, 2015, #123.
WM

Phase III G-Benda vs SA Benda for R-Refractory iNHL: Response Rates
End-of-induction response (IRF) Best overall response to 12 months (IRF)
69.2 63.078.7 76.7
Patie
nts
(%)
Patie
nts
(%)
• 19 patients still in induction (G-B, n=6; B, n=13)
11.7 18.59.0
9.010.1 9.5
58.0 50.8
11.2 12.2
0
20
40
60
80
100
G-Bn=188*
Bn=189*
G-Bn=188*
Bn=189*
Sehn et al. ASCO 2015 Abst 8502; Cheson et al ICML-13, 2015, #123.
Patients still in induction therapy are excluded from analysis. Patients with end of induction response > 60 days shown as missing. Best overall response excludes patients who have not yet had response analysis.

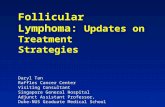
GADOLIN Trial: Investigator-Assessed PFSInvestigator-assessed PFS G-B (n=194) B (n=202)
Events, n 77 (40%) 115 (57%)Median PFS, months (95% CI) 29.2 (20.2–NR) 14.0 (11.7–16.0)Stratified HR (95% CI) 0.52 (0.39–0.70) Log-rank p-value p<0.0001
1.0
0.8
0.6
0.4
0.2
0 6 12 18 24 30 36 42 48 54Time (months)
Pro
babi
lity
of P
FS
0.0
194202
157150
10889
7746
5128
2715
75
22
11
No. at riskG-B
B
14.0 29.2
Median follow-up: 21 months
Sehn et al. ASCO 2015 Abst 8502; Cheson et al ICML-13, 2015, #123.
GB
B

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

GALLIUM Phase III CT vs R + CT Followed by G or R Maint for Untreated Advanced iNHL
68
G:1000 mg d1, d8, d15 cycle 1; d1 cycles 2-8 q21d or cycles 2-6 q28d; CT=CHOP (6 cycles q21d), CVP (8 cycles q21d) or benda (6 cycles q28d); Rituximab 375 mg/m2 on d1 cycles 2-8 q21d aFL: Each site chooses CHOP, CVP, or benda. Non-FL: CHOP, CVP, or benda selected on a patient-by-patient basis
Maintenance Rq2m 2 years
Maintenance Gq2m 2 years
Rituximab + CTa
CRPRSD
GA101 + CTaPreviously untreated advanced iNHL (N=1400)
R
Primary endpoint:● PFS (investigator
assessed) in FL patients
Secondary endpoints:● PFS● ITT (investigator and IRC
assessed)● Response rates● OS● EFS
● Safety● DFS● DOR● PROs● Resource utilization
http://www.clinicaltrials.gov/ct2/show/NCT01332968 as of 09/01/13.

R2 for Untreated FL: Response by Tumor Burden and Molecular Features
By GELF Criteria (N=46)High Tumor Burden (N=22, 48%) Low Tumor Burden (N=24, 52%)
SD PR CR/CRu ORR SD PR CR/CRu ORR0 1 (5%) 21(95%) 100% 1(4%) 4(17%) 19 (79%) 96%
By Bulk of Disease (N=46) Bulky (N=13, 28%) Non-Bulky (N=33, 72%)
SD PR CR/CRu ORR SD PR CR/CRu ORR
0 1(8%) 12(92%) 100% 1(3%) 4 (12%) 28 (85%) 97%
Fowler et al. ASH 2012, abst 901.
Molecular Response (N=44 Evaluable, Marrow and Blood) PCR Positive PCR Negative
PRETREATMENT 17(41%) 26(59%)POST CYCLE 3 5(11%) 39(89%)POST CYCLE 6 2(5%) 42(95%)


New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

Phase II Rituximab, Bendamustine, Cytarabine (R-BAC) for MCL > 60 Years
• 57 patients, med age 71 (61-79), stage III-IV-91%,High MIPI in 45%, Blastoid in 9%.
• 91% received 4, 63% received 6 cycles• Gr 3-4 ANC in 49%, PLT in 52% of cycles, FN in 6%• Results: Med F/U 18 mo; ORR-96%, CR-93%.• Projected 2 yr PFS and OS: 83% and 91%.
Visco et al. ICML-13, 2015, # 59. Albertsson Linblad et al. ICML-13, 2015, # 60.
Lenalidomide, Bendamustine, Rituximab (LenBenRit) for MCL > 65
• 51 patients, med age 72, stages II-IV
• Doses: Len-10 mg d 1-14, Ben-90/m2 d1-2, Rituximab d1
• Med F/U 31 mo: ORR-91%, CR-78%. Med PFS-42 mo, OS-53 mo.
• Infection in 21/51 patients, and 12 deaths 3 due to toxicity

R-DHAP and SCT + R Maintenance for MCL Under 66 Years: The LYMA trial
• 299 patients, Med age 57. MIPI-Low in 53%, Intermeidate in 27%, High in 19%.
• TX: 4 cycles of R-DHAP followed by R-BEAM and ASCT for CR/PRs; MR given q 2 mo X 3 yrs for CR/PRs after ASCT.
• 257 (86%) went to ASCT; CR rates before and after ASCT were 81% and 93%.
• Overall 3 Yr PFS and OS are 75% and 83%.
Le Gouill et al. ICML-13, 2015, #61.
3 Yr Result
MR N=119 W+W N=120 P value
EFS 88 73 0.006OS 93 86 0.72

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

AutoSCT vs AlloSCT for Newly Diagnosed PTCL
Author Pt Ind Chemo AutoSCT 3 Yr PFS 3 Yr OSd’Amore 166 CHOEP14x6 BEAM 48 56Reimer 83 CHOP21x4-6,
Dexa-BEAMHdCy-TBI 36 48
Schmitz et al. ASCO 2015, Abst 8507. Schmitz et al. ICML-13, 2015, # 33. d’Amore et al. JCO 2012. Reimer et al. JCO 2009.
• Background
• Treatment Plan
4 CHOEP-14 N=30
DHAP N=19
SC Harvest N=24
4 CHOEP-14 N=28
DHAP N=18
AlloSCT N=13
AutoSCT N=23
5No Donor

Auto vs AlloSCT After Induction Chemotherapy for PTCL
• Pathology included any mature T-Cell NHL excluding Anaplastic CD30 Positive NHL
• ECOG PS 0-3, Any Stage except Stage I and aaIPI=0• 38% could not go to SCT due to PD with induction • 21/36 randomized patients died; 12 of NHL (7 post
auto, 6 post allo), and 4 in the allo arm died of GVH or late infection
• For ITT analysis: 1 yr EFS=41%, OS=69%.• Study closed due to futility.
Schnitz et al. ICM:L-13, # 33. Schmitz et al. ASCO 2015, Abst 8507.

New Therapies for Lymphoma: An ASCO/ICML Update
• Aggressive NHLs– Novel Drugs– Initial Therapy– Management of Double Hit Lymphomas
• Indolent NHLs– Novel Drugs– Initial Therapy
• Other NHLs– MCL– T-Cell

New Therapies for Lymphoma: An ASCO/ICML Update
F B Hagemeister, MDProfessor of Medicine
Department of Lymphoma and MyelomaM D Anderson Cancer Center
Bangkok 28 August 2015