One-lung ventilation via tracheostomy and left endobronchial ...
LUNG PROTECTIVE VENTILATION FOR THE NEONATEACTIVE HUMIDIFICATION AND RESPIRATORY GAS CONDITIONING
Our lungs function best when the inspired air has a temperature of 37 °C at 100 % relative humidity by the time it reaches the lungs. During normal inspiration, the air is conditioned to these optimal levels during its passage through the upper respiratory tract.
During mechanical ventilation the supplied air is typically cold and dry which can lead to diverse problems for the patient:
In order to support the natural airway defense, preserve sufficient gas exchange and conserve the infant's energy, effective humidification and heating of respiratory gases are essential.
Humidity is the amount of water vapor held in air or any other gas.
The temperature affects humidity in a way that warm gas holds more water vapor than a cold gas.
Relative humidity describes the amount of water vapor contained in the air compared to its maximum capacity to hold water. The maximal air humidity increases with rising temperatures.
The dew point is the temperature where gas is saturated (i.e. relative humidity = 100 %). If the dew point is exceeded, condensation sets in. Relative humidity of 100 % indicates that the dew point temperature is equal to current temperature and the air is fully saturated.
HUMIDITY EXPLAINED IN A NUTSHELL
HOW ACTIVE HUMIDIFICATION WORKS
HOW TO AVOID CONDENSATION DURING ACTIVE HUMIDIFICATION
KEY BENEFITS OF ACTIVE HUMIDIFICATION IN VENTILATION OF NEONATES
WHAT YOU NEED
Drying out of mucosa and hypothermia, resulting in viscous mucusSlowdown of the mucociliary transport system (contaminants aren't removed)Higher infection risk Impairment of surfactant activityHigher risk of air trapping, hyperinflation and atelectasisPossible degradation of gas exchange due to changes in lung compliance andairway patency Increased airway workload
Possible consequences of mechanical ventilation using cold and dry gas1,8
36mg/L
30 °C
30mg/L
32mg/L
34mg/L
38mg/L
40mg/L
42mg/L
44mg/L
31 °C 32 °C 33 °C 34 °C 35 °C 36 °C 37 °C
Active humidification aims to externally warm and humidify the inhaled air to avoid the harmful effects of inspiring cold and dry gas.
?
HUMIDITIY COMPENSATION (HC MODE):
The HC mode is designed to ensure enough humidity output during ventilation. If too little energy is transmitted to the gas, the device increases the chamber set point in steps of 0,5 °C up to 3 °C.The HC mode is only available in the Fisher & Paykel MR850.
Invasive mode: target 37 °C / 44 mg H₂O / LNon-invasive mode: target 34 °C / 32 mg H₂O / L
c°
Absolute humidity is the total mass of water vapor in a given volume of gas. It is measured in mg/L air.mg/L
4 Epithelium cell layer5 Submucosal glan6 Goblet cell
1
2
3
4
6
Mucociliary Transport System
1 Mucus2 Aqueous layer3 Cilia
5
The cold and dry medical gas is warmed and humidified to optimal conditions in the humidifier chamber.
The heating wire further increases the temperature to make up for temperature losses occurring in the unheated tube between the Y-piece and the patient (~-1 °C per 10 cm).
If the expiratory limb is unheated, the exhaled air will cool down. The capacity to hold water is decreased compared to the water vapor from the exhaled air. The vapor exceeds its dew point and condensate will occur.
The rain out is collected in a water trap that shall be placed at the lowest point to prevent the water from flowing towards patient or device.
Keeping the temperature at or above 37 °C helps to avoid condensate in the inspiratory limb, which would result in higher resistance and increased work of breathing.
The patient inspires gas at optimal conditions.
c°
Energy is directed to the growth and development of the infant
Optimal Humidity
Optimized Airway Defense
Optimized Ventilation
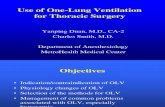
Baseline Heated Humidification
10 minsRoom Air
20
12 315
10
5
0
19 3
Work of Breathing
Wor
k of
Bre
athi
ng (
gm-c
m/k
g)
Baseline
CompliancemL/cm H₂O/kg
Ventilation of stable pre-term intubated infant (previously on humidification)
1.12 0.94 P < 0.005
RTFcm H₂O/L/kg
37 71 P < 0.005
WOBgm-cm/kg
12 19 P < 0.005
After P Value
HEATED CIRCUIT:
The better the air humidity is sustained, the less condensate occurs in the system. Optimally, use a double heated circuit, that preserves the temperature over its whole length. VentStar Helix circuits enable a more uniform heat distribution.
SOURCES:1) Williams R, Rankin N, Smith T, Galler D, Seakins P. Relationship between the humidity and temperature of inspired gas
and the function of the airway mucosa. Critical Care Medicine 1996; 24(11):1920-1929.2) Greenspan J, Wolfson M,Shaffer T. Airway responsiveness to low inspired gas temperature in pre-term neonates. Journal
of Pediatrics 1991; 118(3):443-5.3) Tarnow-Mordi W, Reid E, Griffiths P, Wilkinson A. Low inspired gas temperature and respiratory complications in very
low birthweight infants. Journal of Pediatrics 1989; 114(3):438-42.4) Morán I, Bellapart J, Vari A. Mancebo J. Heat and moisture exchangers and heated humidifiers in acute lung injury/acute
respiratory distress syndrome patients. Effects on respiratory mechanics and gas exchange. Intensive Care Medicine 2006; 32(4):524-31.
5) Scott DH, Fraser S, Willson P, Drummond GB, Baillie JK. Passage of pathogenic microorganisms through breathing system filters used in anaesthesia and intensive care. Anaesthesia. 2010: 65(7):670-3
6) Williams R, Rankin N, Smith T, Galler D, Seakins P. Relationship between the humidity and temperature of inspired gas and the function of the airway mucosa. Critical Care Medicine 1996; 24(11): 1920-1929
7) Girault C, Breton L, Richard J, Tamion F, Vandelet P, Aboab J, et al. Mechanical effects of airway humidification devices in difficult to wean patients. Critical Care Medicine 2003; 31(5):1306-11
8) Ryan SN, Rankin N, Meyer E, Williams R (2002) Energy balance in the intubated human airway is an indicator ofoptimal gas conditioning. Crit Care Med 30:355–361
For more information, visitwww.draeger.com/neonatal-ventilation and download also our Humidification Troubleshooting Guideline.
LUNG PROTECTIVE VENTILATION
Lung function will improve with the delivery of optimal humidity. A decrease in humidity will increase the incidence of pneumothorax and the need for supplemental oxygen.
c°
Neonatal ventilator Dräger Babylog
Humidifier F&P MR850
Humidification chamber
Breathing circuit
Temperature sensor cover
Water bag
PDF-
9430
1
2
3
4
5
6
1 2
3
4
56
Prevent long-term damages to the lung41.Reduce infection risks with natural breathing mechanism5 2.
Improve efficient gas exchange63.Decrease work of breathing and thus increase patient comfort and therapy tolerance74.
Insp.Exp.
EFFECT OF 10 MINUTES MECHANICAL VENTILATION WITHOUT HUMIDIFICATION2
▸▸▸▸▸▸
▸