Lung Cancer Updates 2018 · • NE, not estimable; NR, not reported. • 1. Gandhi L, ... 476 377...
82
8/19/2018 1 Lung Cancer Updates 2018 Edward S. Kim, M.D., FACP Chair, Solid Tumor Oncology and Investigational Therapeutics Donald S. Kim Distinguished Chair for Cancer Research Medical Director, Clinical Trials Office Levine Cancer Institute Charlotte, NC
Transcript of Lung Cancer Updates 2018 · • NE, not estimable; NR, not reported. • 1. Gandhi L, ... 476 377...
8/19/2018
1
Lung Cancer Updates 2018
Edward S. Kim, M.D., FACP
Chair, Solid Tumor Oncology and Investigational Therapeutics
Donald S. Kim Distinguished Chair for Cancer Research
Medical Director, Clinical Trials Office
Levine Cancer Institute
Charlotte, NC
8/19/2018
2
L E V I N E C A N C E R I N S T I T U T E
Organizations
8/19/2018
3
L E V I N E C A N C E R I N S T I T U T E
NSCLC: A Major Public Health Problem
• Estimated 1.6 million deaths each year worldwide from lung cancer
• In 2015:
• Estimated 221,200 new cases of lung cancer expected to be diagnosed in US
• 158,000 Americans expected to die from lung cancer
• Leading cause of cancer-related deaths in US men and women
• More deaths from lung cancer than breast, prostate, colon, liver, melanoma, and kidney cancers combined
• Need for better thought out, patient-driven studies
Torre LA, et al. CA Cancer J Clin. 2015;65(2):87-108.Siegel RL, et al. CA Cancer J Clin. 2015;65(1):5-29.
8/19/2018
4
L E V I N E C A N C E R I N S T I T U T E
Importance of Clinical Trials

8/19/2018
5
L E V I N E C A N C E R I N S T I T U T E
Must Allow More Patients to Participate

8/19/2018
6
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
7
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
8
L E V I N E C A N C E R I N S T I T U T E
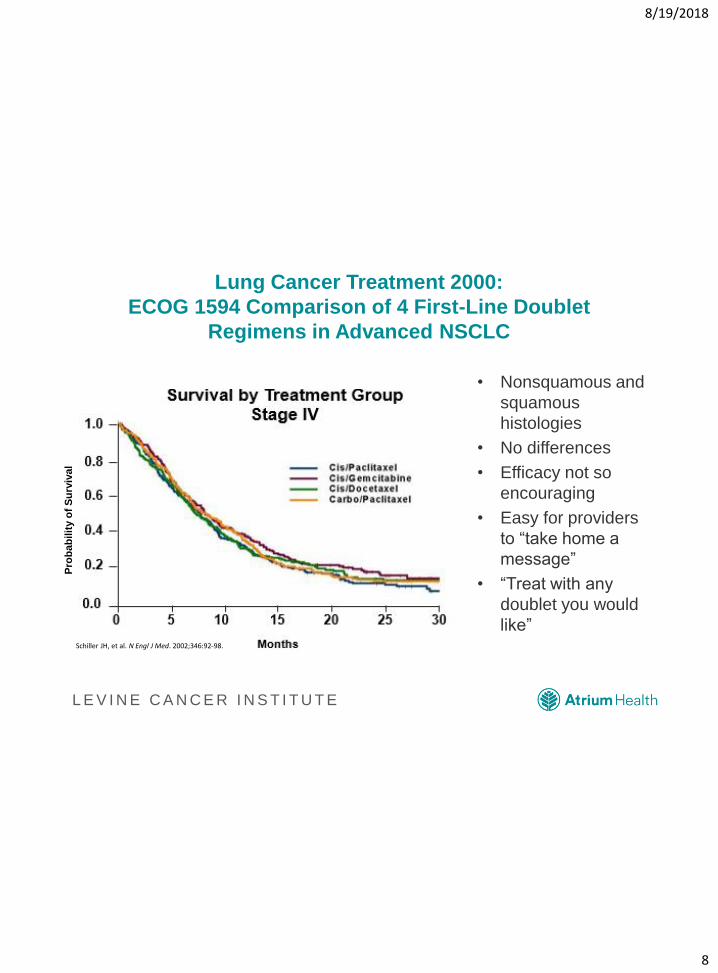
Lung Cancer Treatment 2000:
ECOG 1594 Comparison of 4 First-Line Doublet
Regimens in Advanced NSCLC
• Nonsquamous and
squamous
histologies
• No differences
• Efficacy not so
encouraging
• Easy for providers
to “take home a
message”
• “Treat with any
doublet you would
like”Schiller JH, et al. N Engl J Med. 2002;346:92-98.
Pro
bab
ilit
y o
f S
urv
ival
8/19/2018
9
L E V I N E C A N C E R I N S T I T U T E
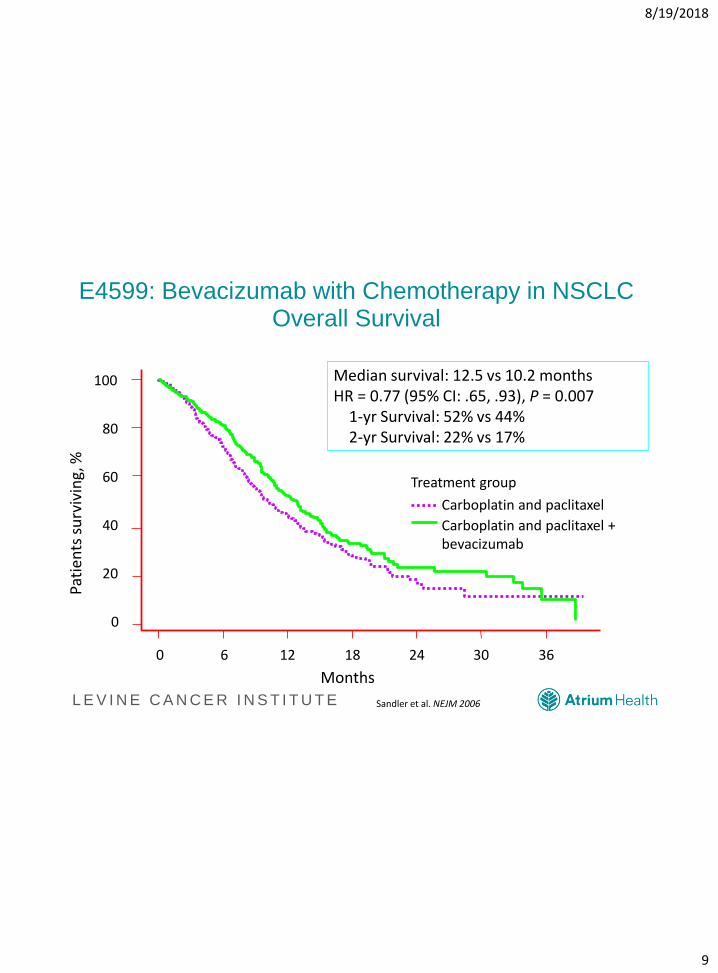
E4599: Bevacizumab with Chemotherapy in NSCLCOverall Survival
0 6 12 18 24 30 36
0
20
40
60
80
100
Months
Carboplatin and paclitaxel
Carboplatin and paclitaxel + bevacizumab
Treatment group
Median survival: 12.5 vs 10.2 monthsHR = 0.77 (95% CI: .65, .93), P = 0.007
1-yr Survival: 52% vs 44%2-yr Survival: 22% vs 17%
Pati
ents
su
rviv
ing,
%
Sandler et al. NEJM 2006
8/19/2018
10
L E V I N E C A N C E R I N S T I T U T E
NSCLC Drug Approvals/Indications: 2015 - Present
• Alectinib
• Necitumumab
• Nivolumab
• Osimertinib
• Gefitinib
• Ramucirumab
• Atezolizumab
• Ceritinib
• Brigatinib
• Pembrolizumab
– PD-L1 + (1st, 2nd line)
– MSI-H or dMMR solid
tumors
– NSCLC (Carboplatin
+ Pemetrexed)
• Crizotinib (ROS1)
• Dabrafenib, Trametinib
• Durvalumab
8/19/2018
11
8/19/2018 11
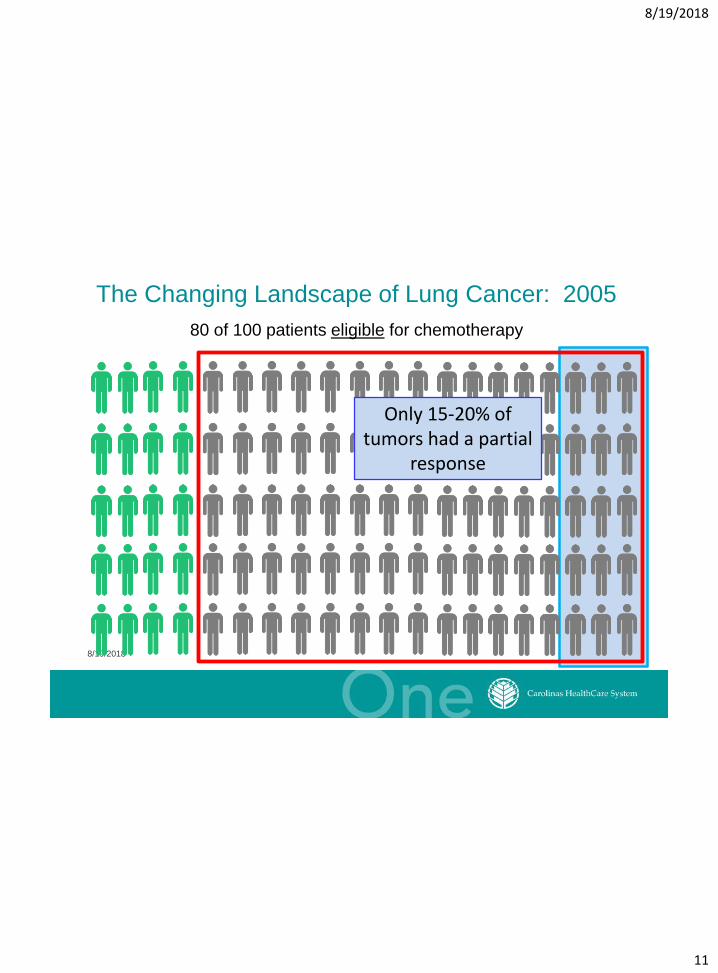
The Changing Landscape of Lung Cancer: 2005
80 of 100 patients eligible for chemotherapy
Only 15-20% of tumors had a partial
response
8/19/2018
12
8/19/2018 12
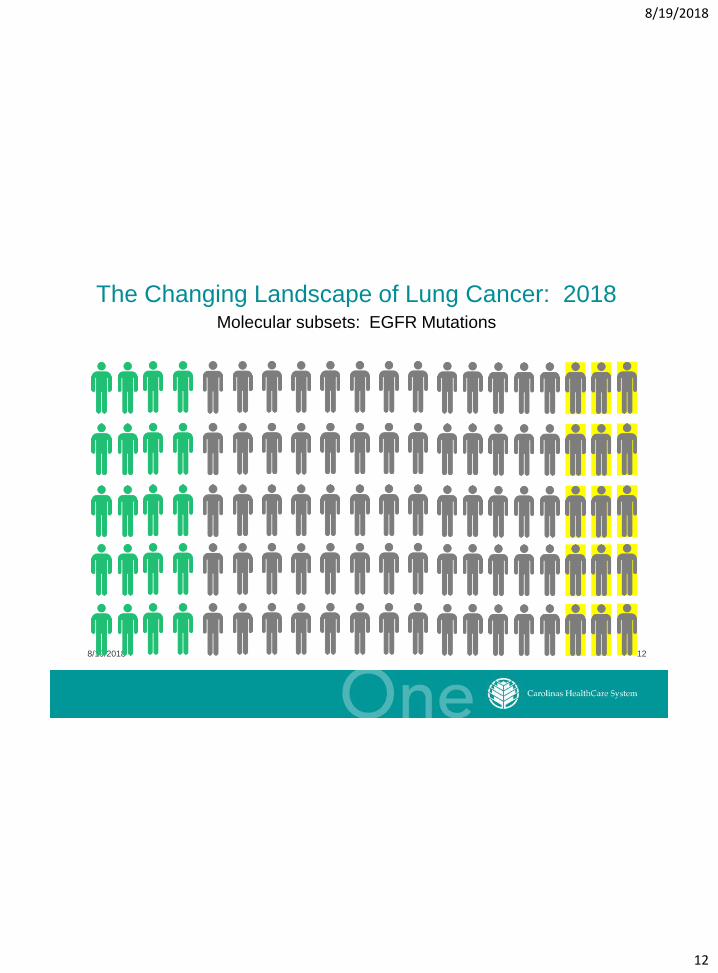
Molecular subsets: EGFR Mutations
The Changing Landscape of Lung Cancer: 2018
8/19/2018
13
8/19/2018 13
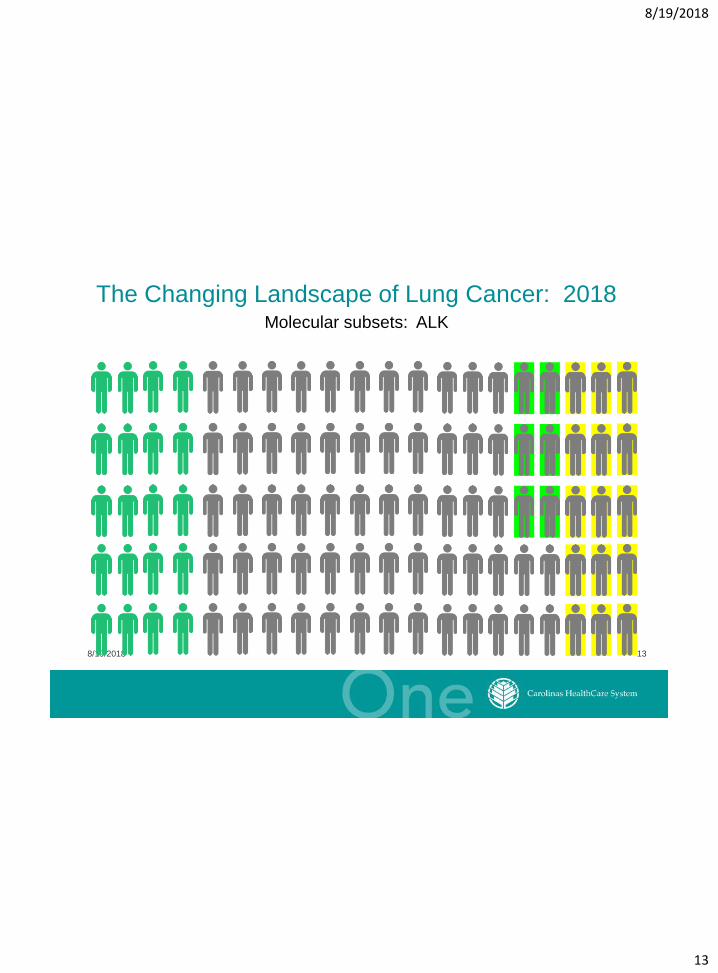
Molecular subsets: ALK
The Changing Landscape of Lung Cancer: 2018
8/19/2018
14
8/19/2018 14
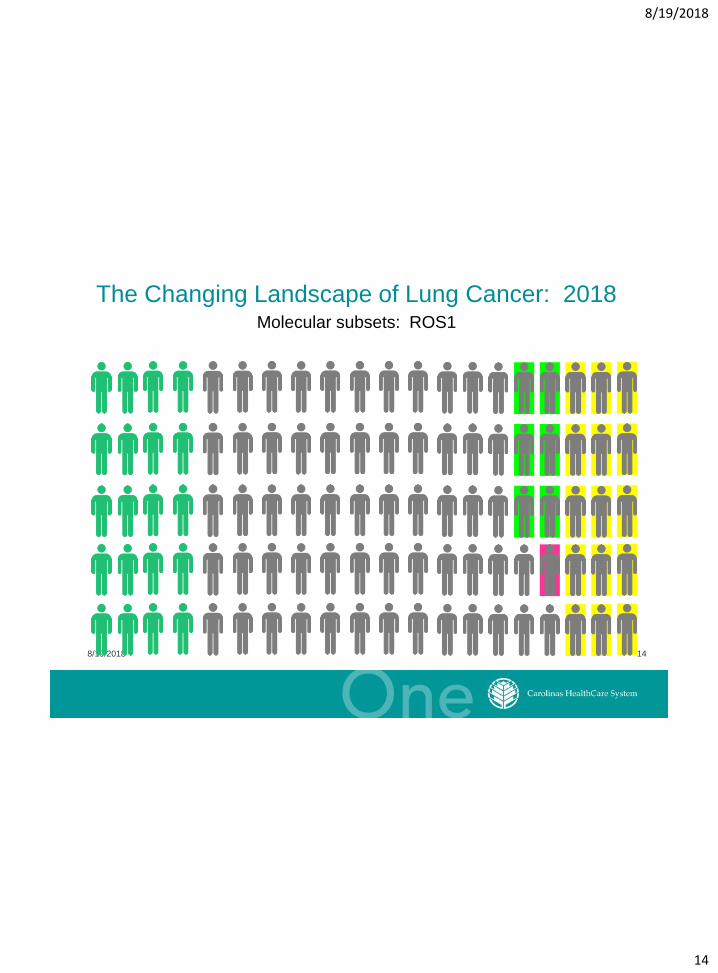
Molecular subsets: ROS1
The Changing Landscape of Lung Cancer: 2018
8/19/2018
15
8/19/2018 15
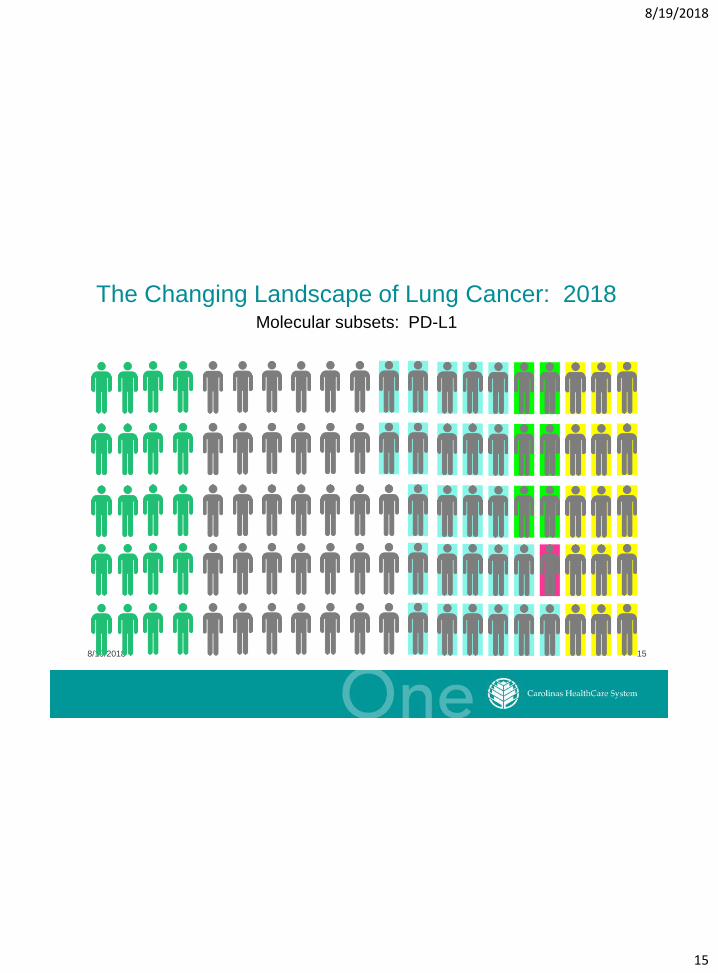
Molecular subsets: PD-L1
The Changing Landscape of Lung Cancer: 2018
8/19/2018
16
8/19/2018 16
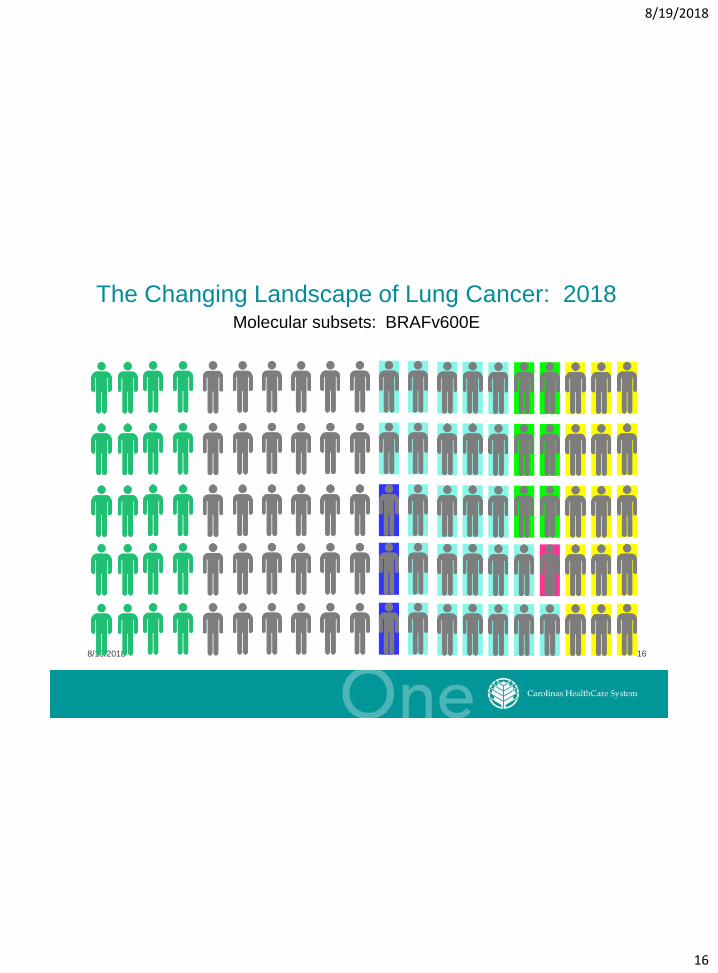
Molecular subsets: BRAFv600E
The Changing Landscape of Lung Cancer: 2018
8/19/2018
17
8/19/2018 17
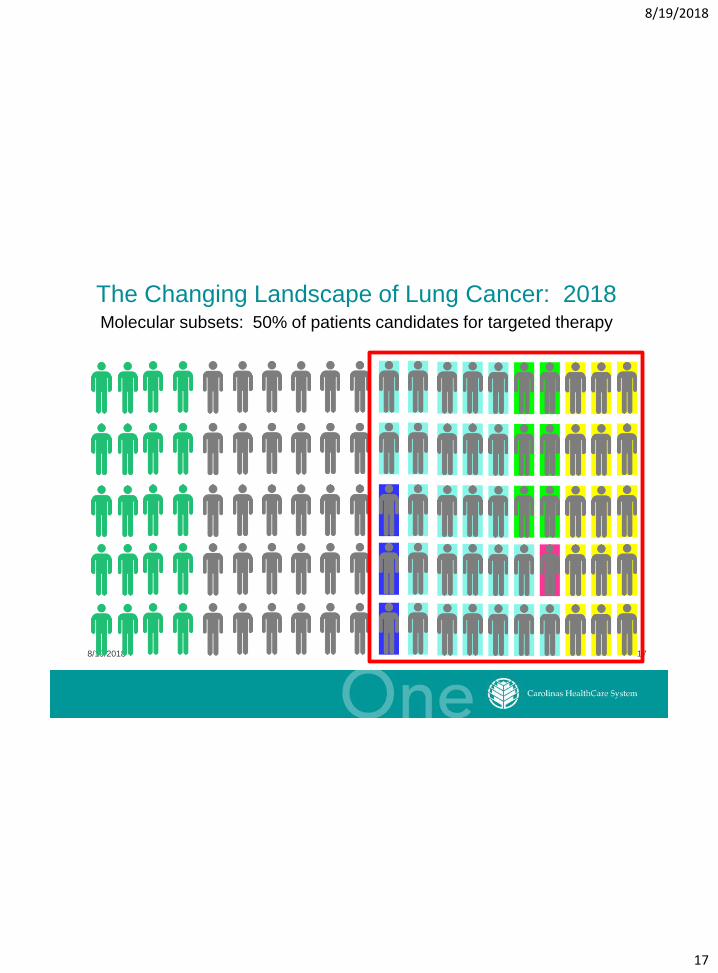
Molecular subsets: 50% of patients candidates for targeted therapy
The Changing Landscape of Lung Cancer: 2018
8/19/2018
18
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
19
L E V I N E C A N C E R I N S T I T U T E
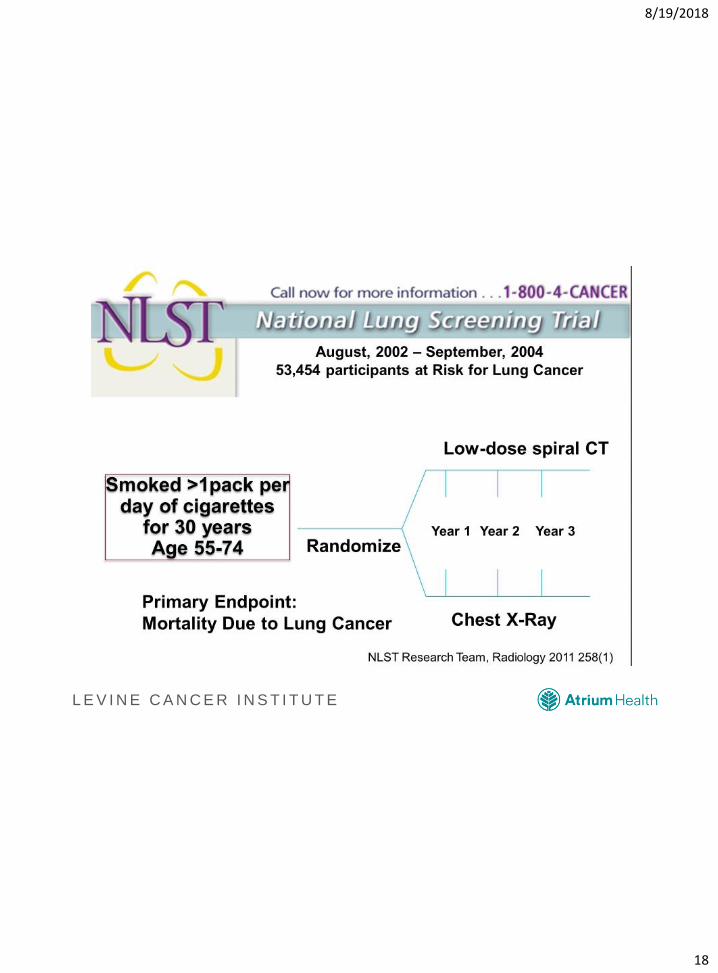
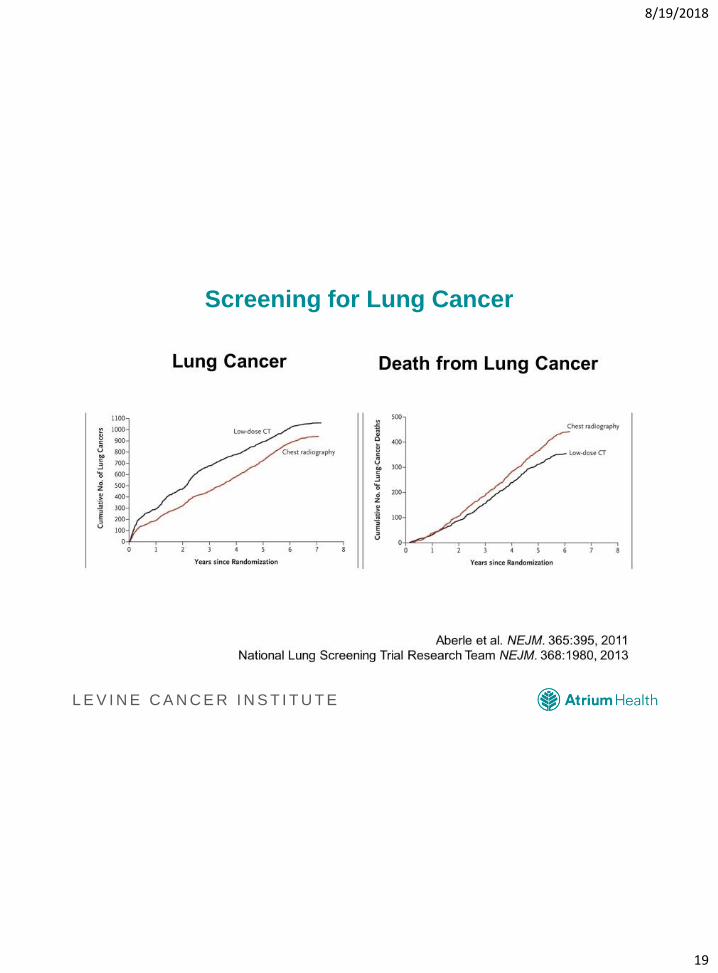
Screening for Lung Cancer

8/19/2018
20
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
21
L E V I N E C A N C E R I N S T I T U T E
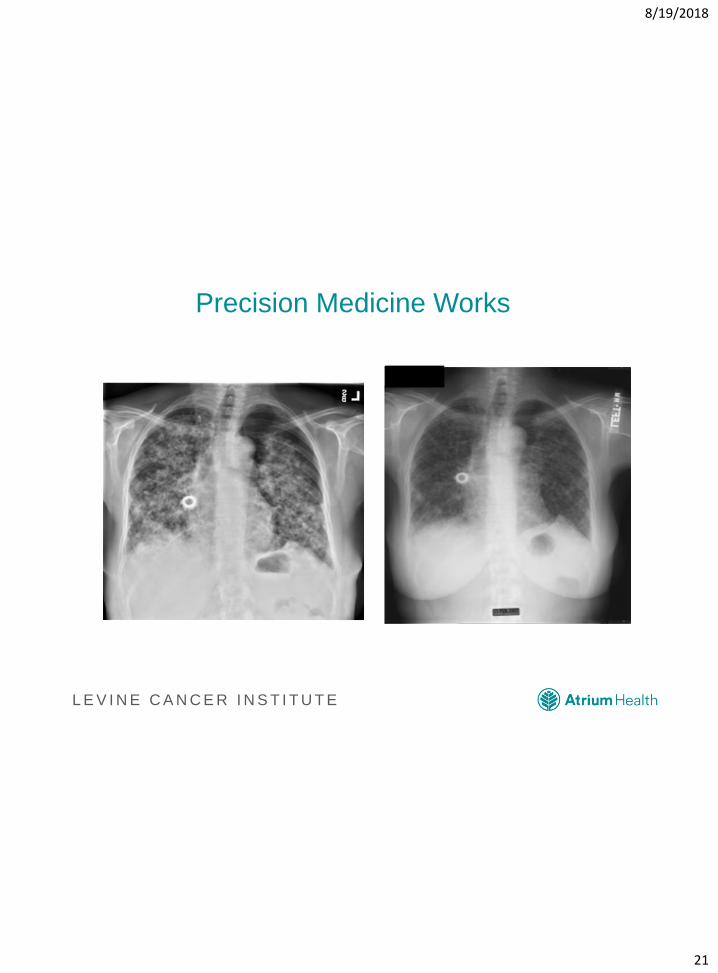
Precision Medicine Works
Precision Medicine Works
8/19/2018
22
L E V I N E C A N C E R I N S T I T U T E
Biomarker Recommendations: Practical
Applications
• EGFR
• BRAF
• ALK
• ROS1
• PD-L1
• EGFR T790M
8/19/2018
23
L E V I N E C A N C E R I N S T I T U T E
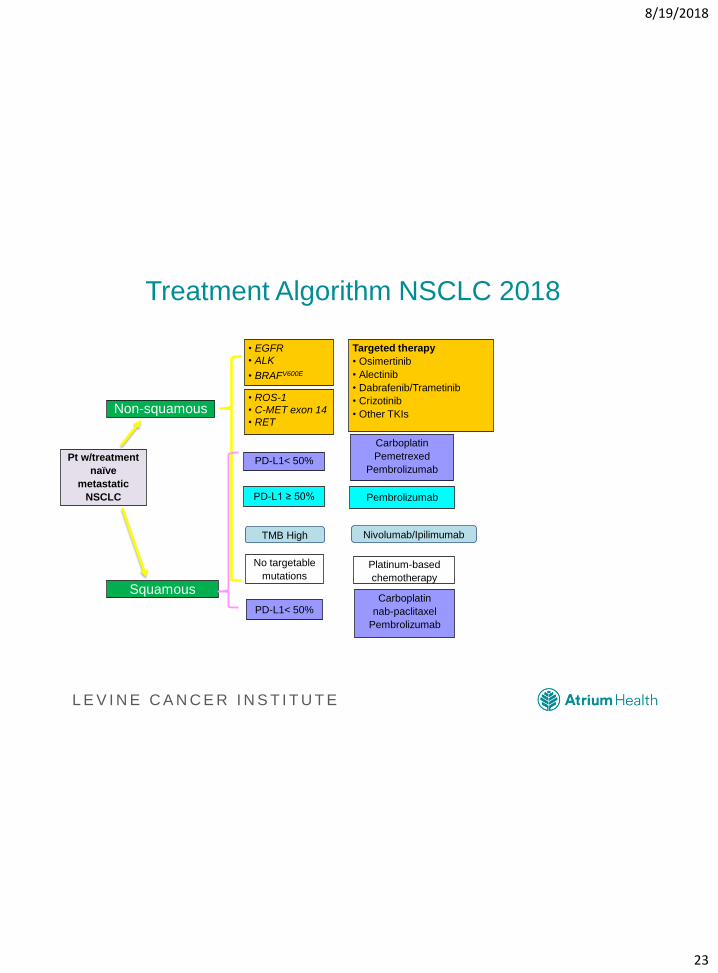
Treatment Algorithm NSCLC 2018
PD-L1< 50%Carboplatin
nab-paclitaxel
Pembrolizumab
No targetable
mutations
PD-L1< 50%
Platinum-based
chemotherapy
Squamous
Pt w/treatment
naïve
metastatic
NSCLC
Non-squamous
• EGFR
• ALK
• BRAFV600E
Targeted therapy
• Osimertinib
• Alectinib
• Dabrafenib/Trametinib
• Crizotinib
• Other TKIs
• ROS-1
• C-MET exon 14
• RET
PD-L1 ≥ 50% Pembrolizumab
Carboplatin
Pemetrexed
Pembrolizumab
Nivolumab/IpilimumabTMB High
8/19/2018
24
L E V I N E C A N C E R I N S T I T U T E
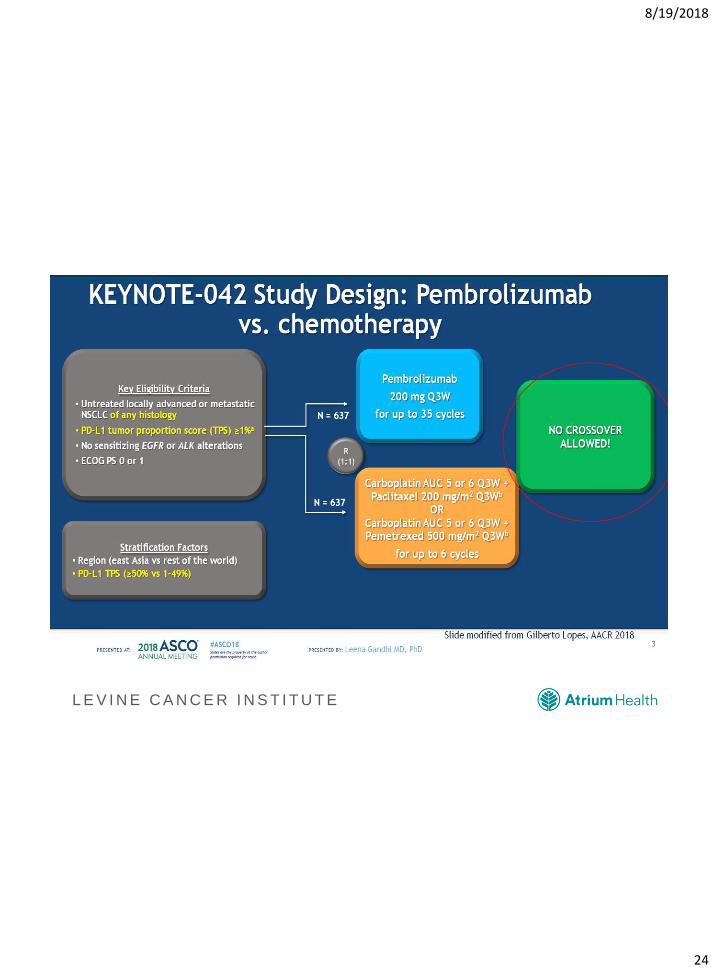
KEYNOTE-042 Study Design: Pembrolizumab vs. chemotherapy
8/19/2018
25
L E V I N E C A N C E R I N S T I T U T ELopes, ASCO 2018
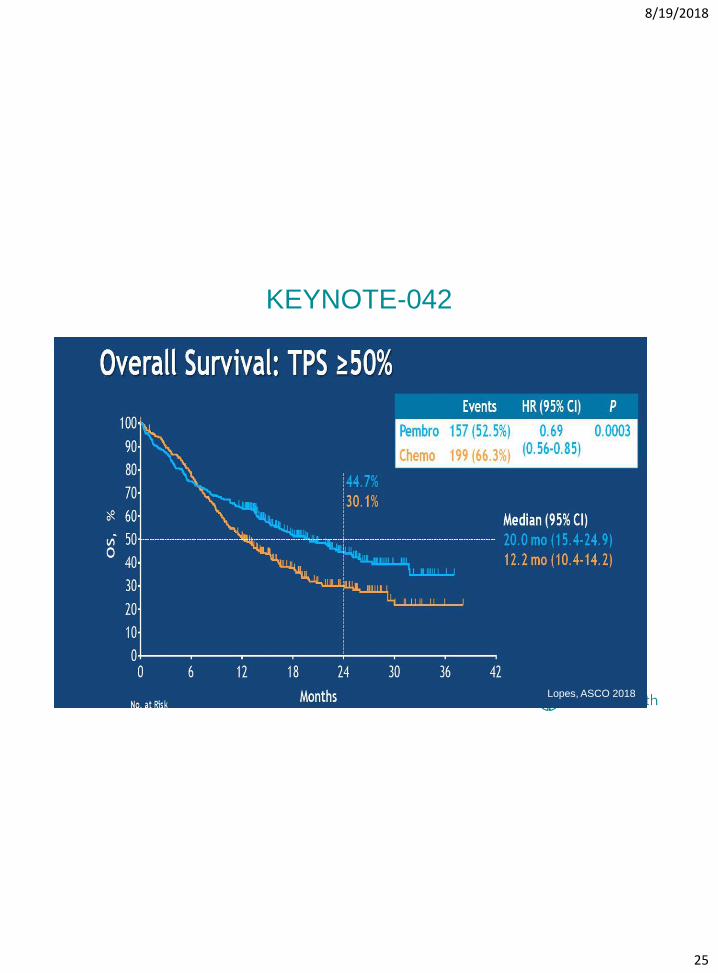
KEYNOTE-042
8/19/2018
26
L E V I N E C A N C E R I N S T I T U T E
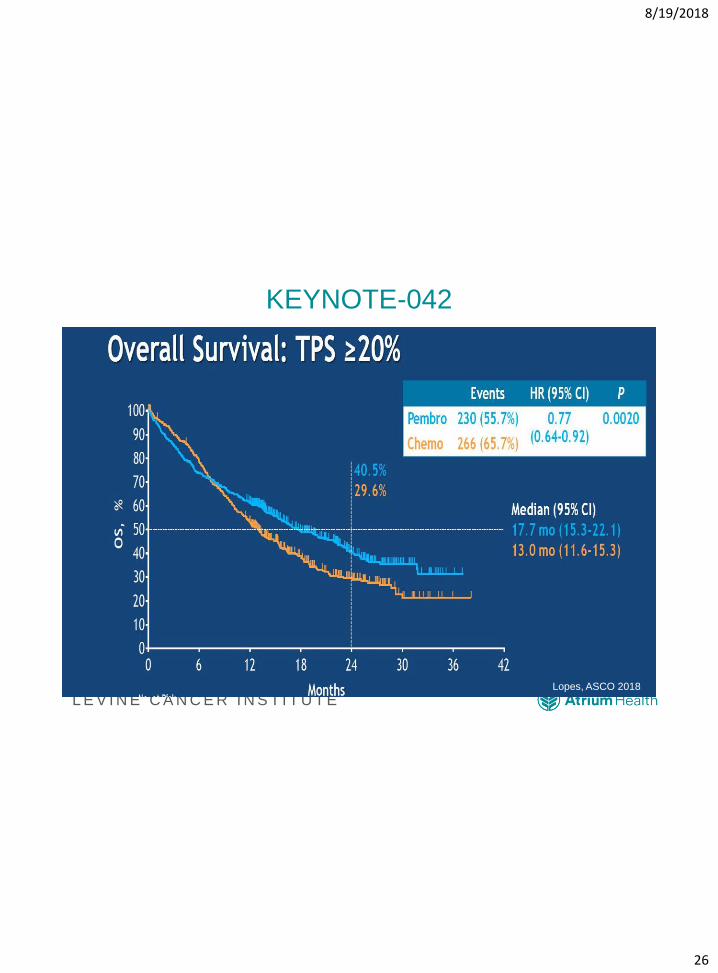
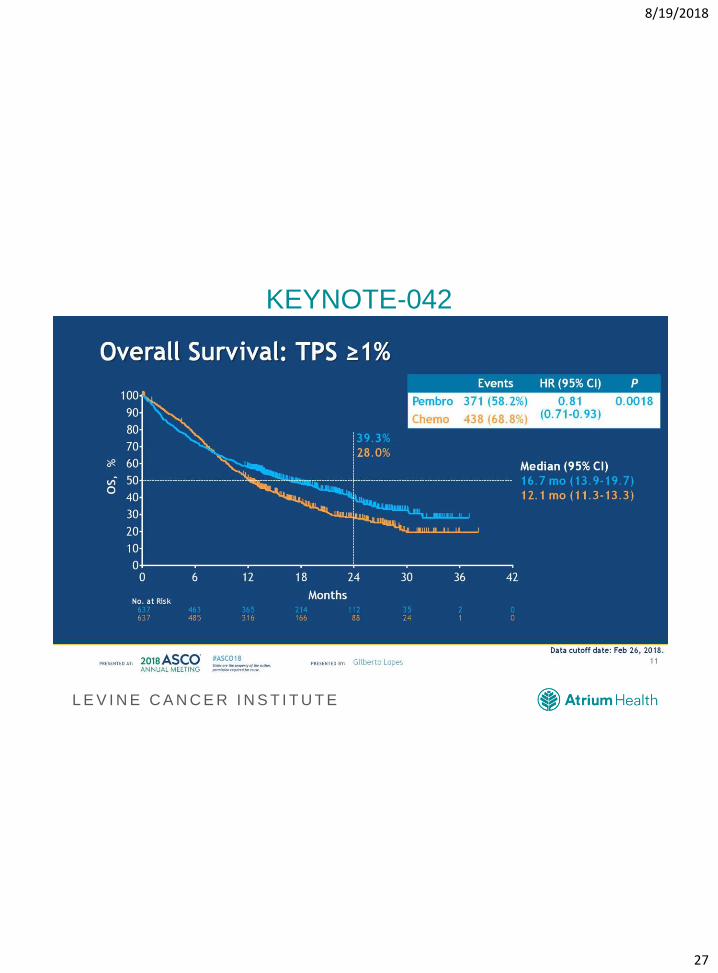
KEYNOTE-042
Lopes, ASCO 2018
8/19/2018
27
L E V I N E C A N C E R I N S T I T U T E
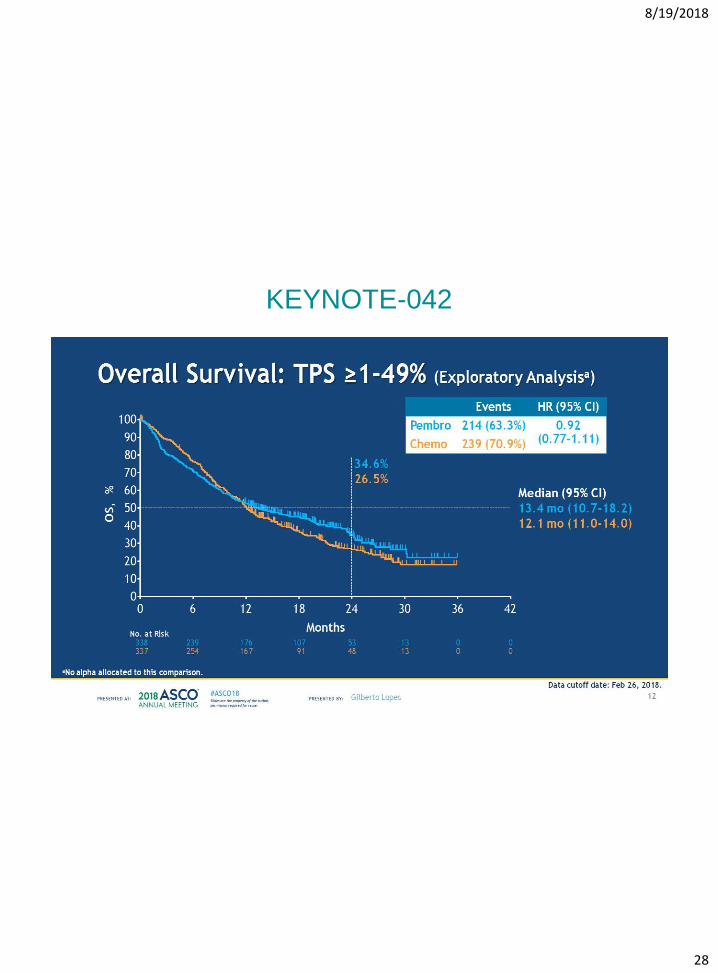
KEYNOTE-042
8/19/2018
28
L E V I N E C A N C E R I N S T I T U T E
KEYNOTE-042
8/19/2018
29
L E V I N E C A N C E R I N S T I T U T E
Implications of KEYNOTE-042
• Single agent Pembrolizumab has activity in PD-L1 + lung
cancer
• PD-L1 ≥ 50% continue single agent
• Consider the response rates
• Fit patients should be considered for combination
chemotherapy (KEYNOTE-189)
• Medically less fit patients should be given single agent
8/19/2018
30
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
31
L E V I N E C A N C E R I N S T I T U T E
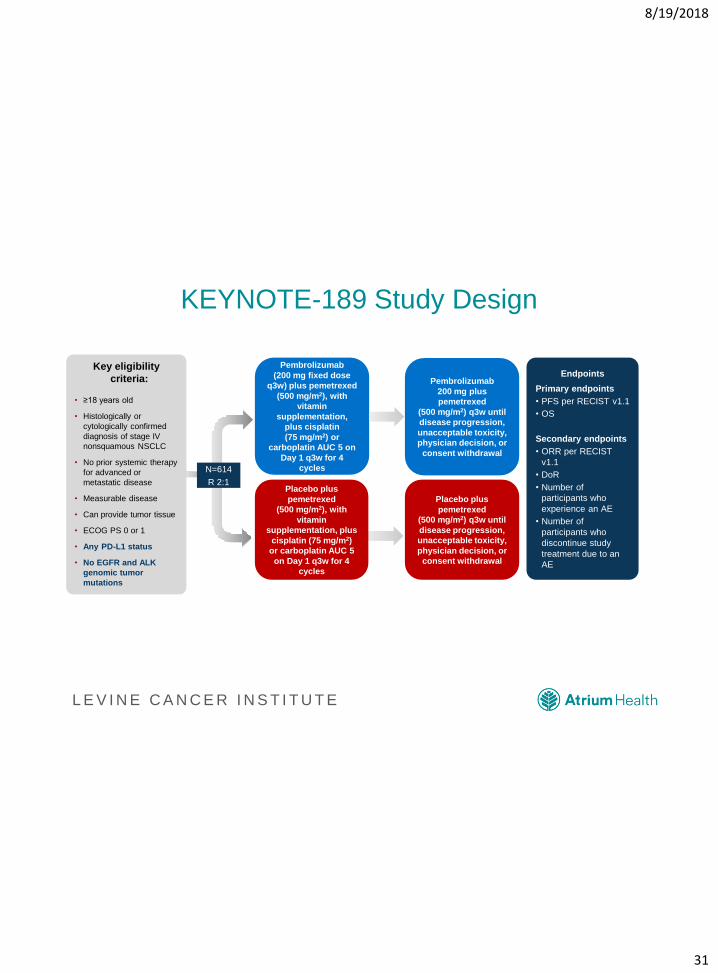
KEYNOTE-189 Study Design
31
Pembrolizumab
(200 mg fixed dose
q3w) plus pemetrexed
(500 mg/m2), with
vitamin
supplementation,
plus cisplatin
(75 mg/m2) or
carboplatin AUC 5 on
Day 1 q3w for 4
cycles
Placebo plus
pemetrexed
(500 mg/m2), with
vitamin
supplementation, plus
cisplatin (75 mg/m2)
or carboplatin AUC 5
on Day 1 q3w for 4
cycles
Endpoints
Primary endpoints
• PFS per RECIST v1.1
• OS
Secondary endpoints
• ORR per RECIST
v1.1
• DoR
• Number of
participants who
experience an AE
• Number of
participants who
discontinue study
treatment due to an
AE
Key eligibility
criteria:
• ≥18 years old
• Histologically or
cytologically confirmed
diagnosis of stage IV
nonsquamous NSCLC
• No prior systemic therapy
for advanced or
metastatic disease
• Measurable disease
• Can provide tumor tissue
• ECOG PS 0 or 1
• Any PD-L1 status
• No EGFR and ALK
genomic tumor
mutations
N=614
R 2:1
Pembrolizumab
200 mg plus
pemetrexed
(500 mg/m2) q3w until
disease progression,
unacceptable toxicity,
physician decision, or
consent withdrawal
Placebo plus
pemetrexed
(500 mg/m2) q3w until
disease progression,
unacceptable toxicity,
physician decision, or
consent withdrawal
8/19/2018
32
L E V I N E C A N C E R I N S T I T U T E
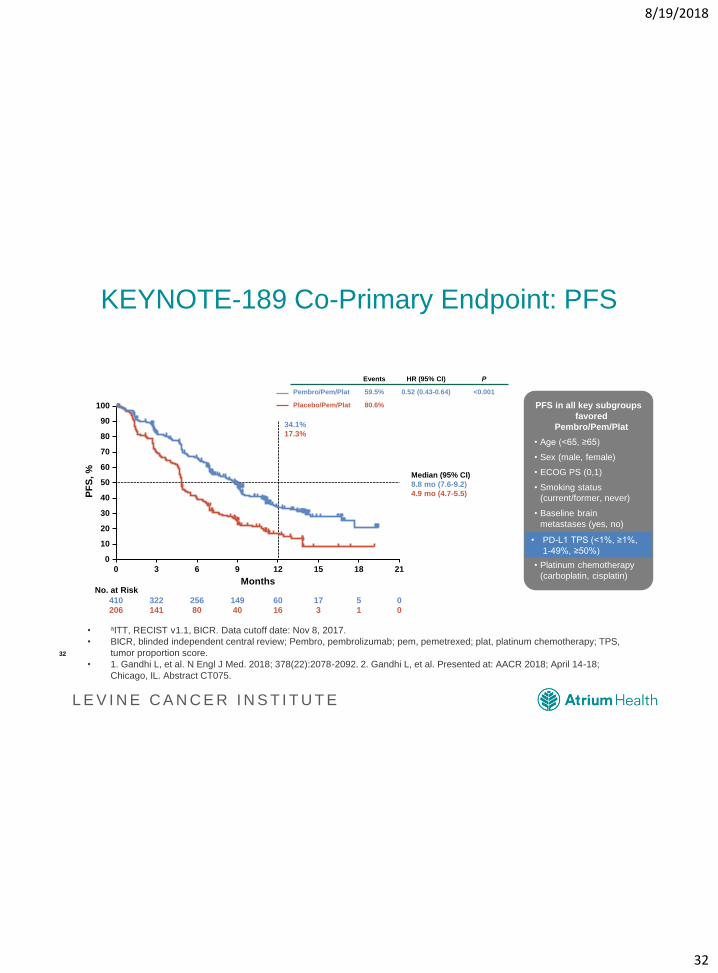
KEYNOTE-189 Co-Primary Endpoint: PFS
• aITT, RECIST v1.1, BICR. Data cutoff date: Nov 8, 2017.
• BICR, blinded independent central review; Pembro, pembrolizumab; pem, pemetrexed; plat, platinum chemotherapy; TPS,
tumor proportion score.
• 1. Gandhi L, et al. N Engl J Med. 2018; 378(22):2078-2092. 2. Gandhi L, et al. Presented at: AACR 2018; April 14-18;
Chicago, IL. Abstract CT075.
PFS in all key subgroups
favored
Pembro/Pem/Plat
• Age (<65, ≥65)
• Sex (male, female)
• ECOG PS (0,1)
• Smoking status
(current/former, never)
• Baseline brain
metastases (yes, no)
• PD-L1 TPS (<1%, ≥1%,
1-49%, ≥50%)
• Platinum chemotherapy
(carboplatin, cisplatin)
• PD-L1 TPS (<1%, ≥1%,
1-49%, ≥50%)
Events HR (95% CI) P
Pembro/Pem/Plat 59.5% 0.52 (0.43-0.64) <0.001
Placebo/Pem/Plat 80.6%
34.1%
17.3%
Median (95% CI)
8.8 mo (7.6-9.2)
4.9 mo (4.7-5.5)
100
80
90
70
60
40
30
10
50
20
0
0 3 6 9 12 15 21
Months
410
No. at Risk
206
322
141
256
80
149
40
60
16
17
3
18
5
1
0
0
PF
S,
%
32
8/19/2018
33
L E V I N E C A N C E R I N S T I T U T E
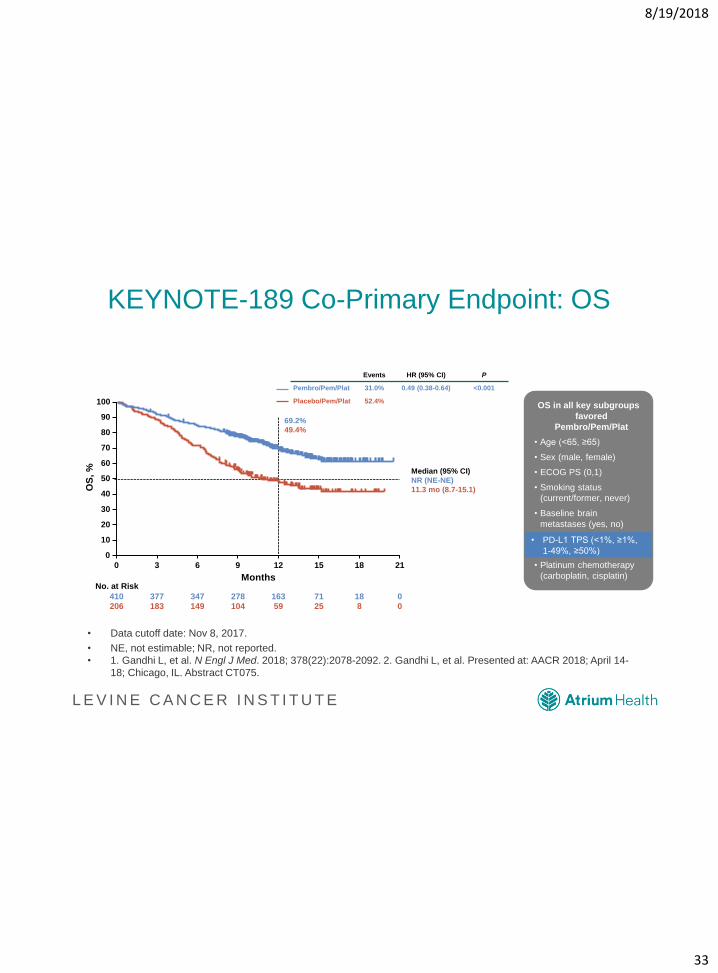
KEYNOTE-189 Co-Primary Endpoint: OS
• Data cutoff date: Nov 8, 2017.
• NE, not estimable; NR, not reported.
• 1. Gandhi L, et al. N Engl J Med. 2018; 378(22):2078-2092. 2. Gandhi L, et al. Presented at: AACR 2018; April 14-
18; Chicago, IL. Abstract CT075.
33
OS in all key subgroups
favored
Pembro/Pem/Plat
• Age (<65, ≥65)
• Sex (male, female)
• ECOG PS (0,1)
• Smoking status
(current/former, never)
• Baseline brain
metastases (yes, no)
• PD-L1 TPS (<1%, ≥1%,
1-49%, ≥50%)
• Platinum chemotherapy
(carboplatin, cisplatin)
• PD-L1 TPS (<1%, ≥1%,
1-49%, ≥50%)
Events HR (95% CI) P
Pembro/Pem/Plat 31.0% 0.49 (0.38-0.64) <0.001
Placebo/Pem/Plat 52.4%
69.2%
49.4%
Median (95% CI)
NR (NE-NE)
11.3 mo (8.7-15.1)OS
, %
100
80
90
70
60
40
30
10
50
20
0
0 3 6 9 12 15 21
Months
410
No. at Risk
206
377
183
347
149
278
104
163
59
71
25
18
18
8
0
0
8/19/2018
34
L E V I N E C A N C E R I N S T I T U T E
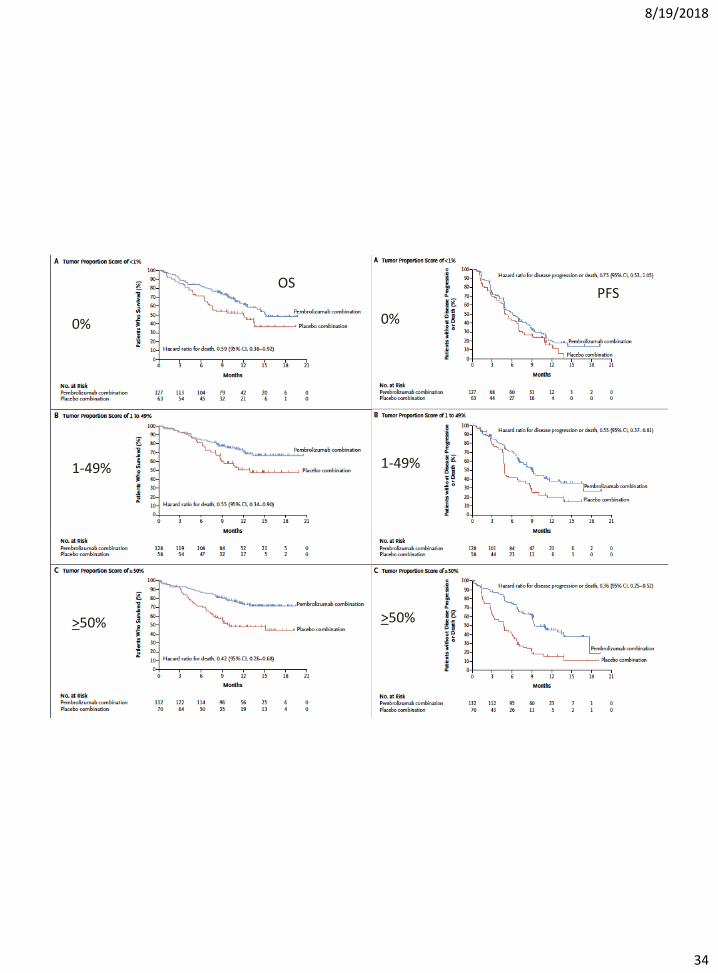
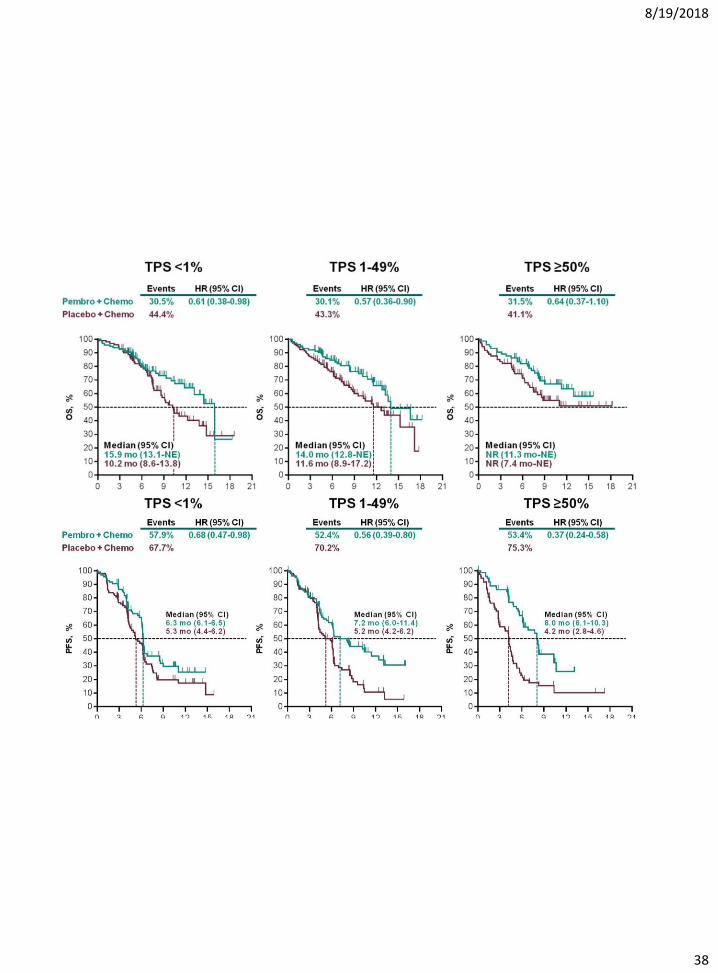
PFS
0%
OS
1-49%
>50%
0%
1-49%
>50%
8/19/2018
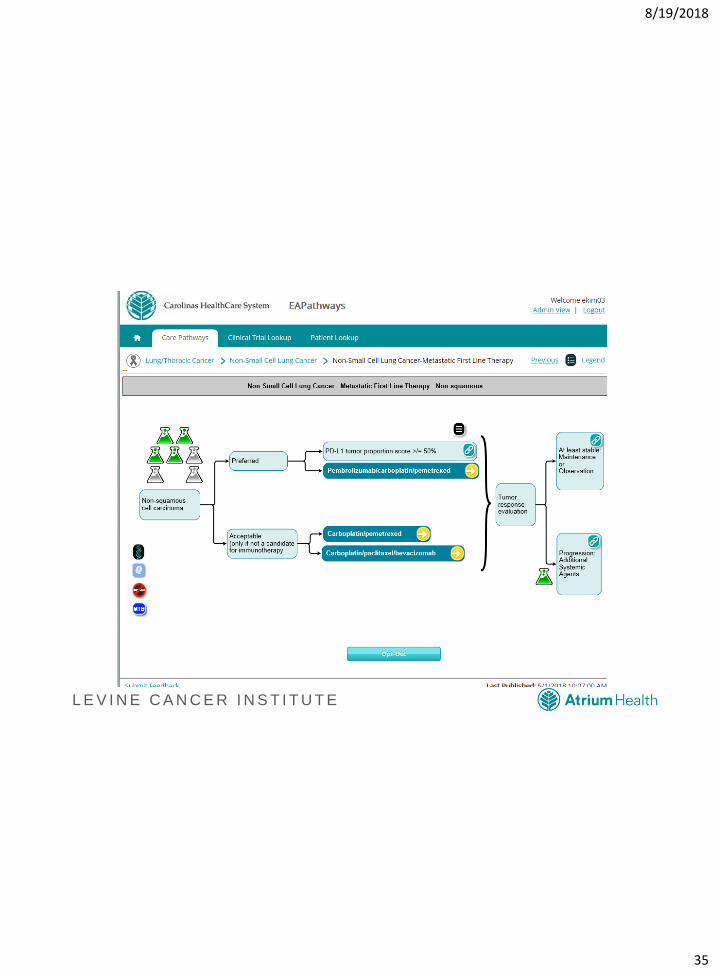
35
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
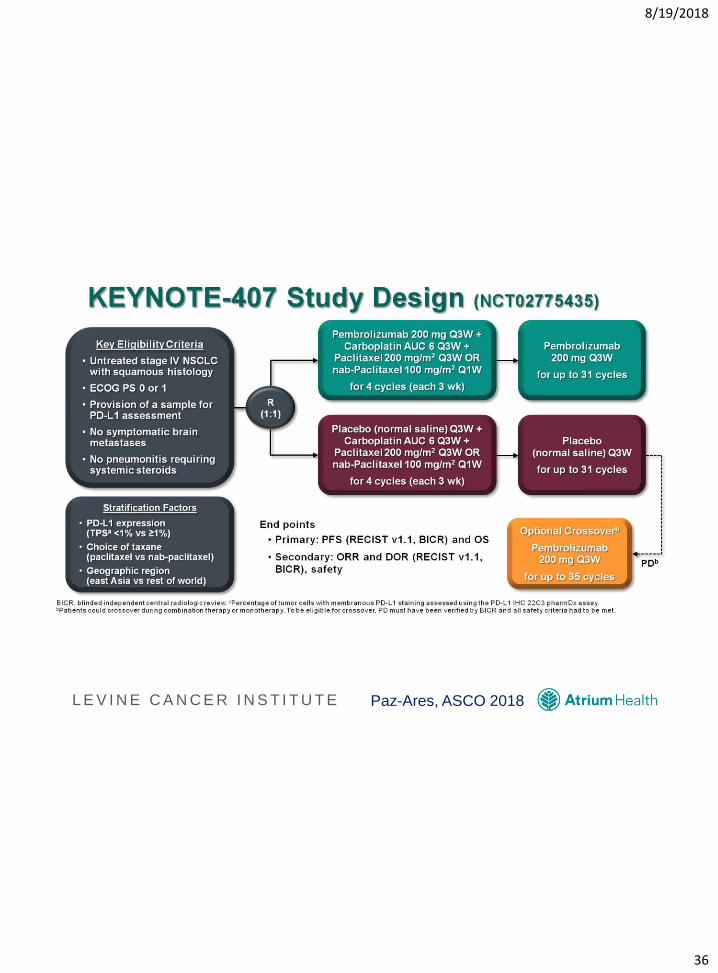
36
L E V I N E C A N C E R I N S T I T U T E Paz-Ares, ASCO 2018
8/19/2018
37
L E V I N E C A N C E R I N S T I T U T E
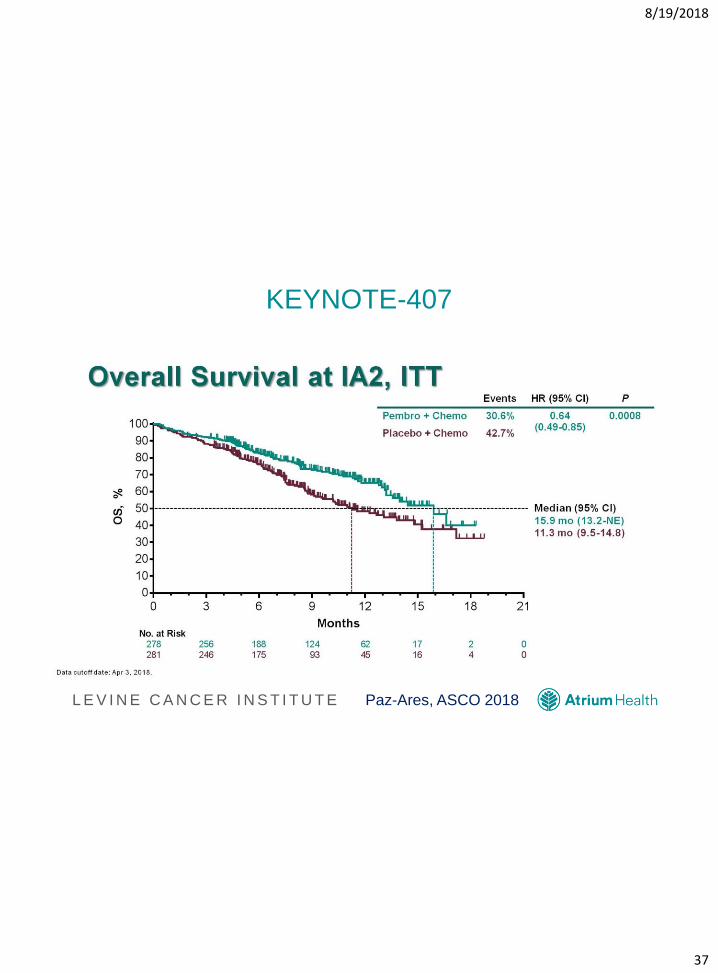
KEYNOTE-407
Paz-Ares, ASCO 2018
8/19/2018
38
L E V I N E C A N C E R I N S T I T U T E
Overall Survival at IA2, ITT
Presented By Luis Paz-Ares at 2018 ASCO Annual Meeting
8/19/2018
39
L E V I N E C A N C E R I N S T I T U T E
Implications of KEYNOTE-407
• New standard of care in the treatment of patients with
squamous cell lung cancer
• No steroids with nab-paclitaxel
8/19/2018
40
L E V I N E C A N C E R I N S T I T U T E
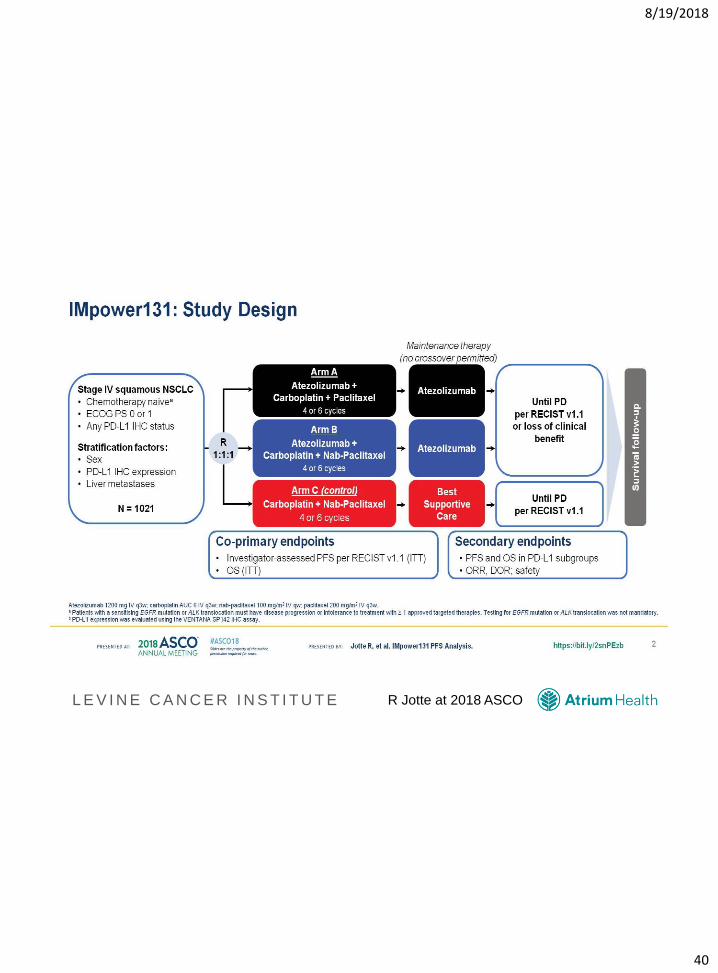
IMpower131: Study Design
R Jotte at 2018 ASCO
8/19/2018
41
L E V I N E C A N C E R I N S T I T U T E
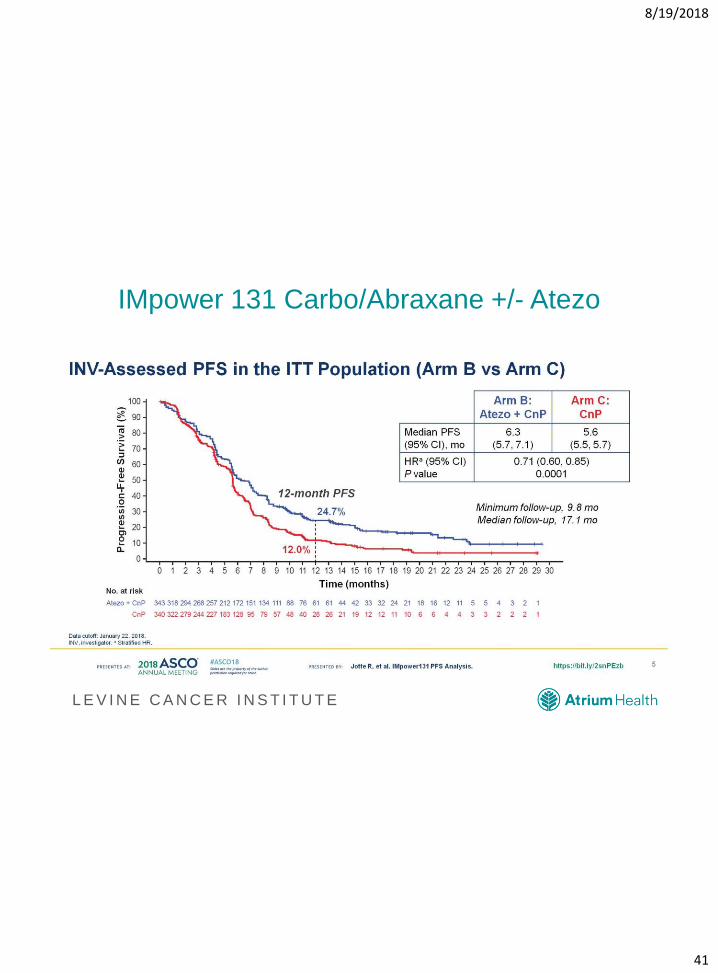
IMpower 131 Carbo/Abraxane +/- Atezo
8/19/2018
42
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
43
L E V I N E C A N C E R I N S T I T U T E
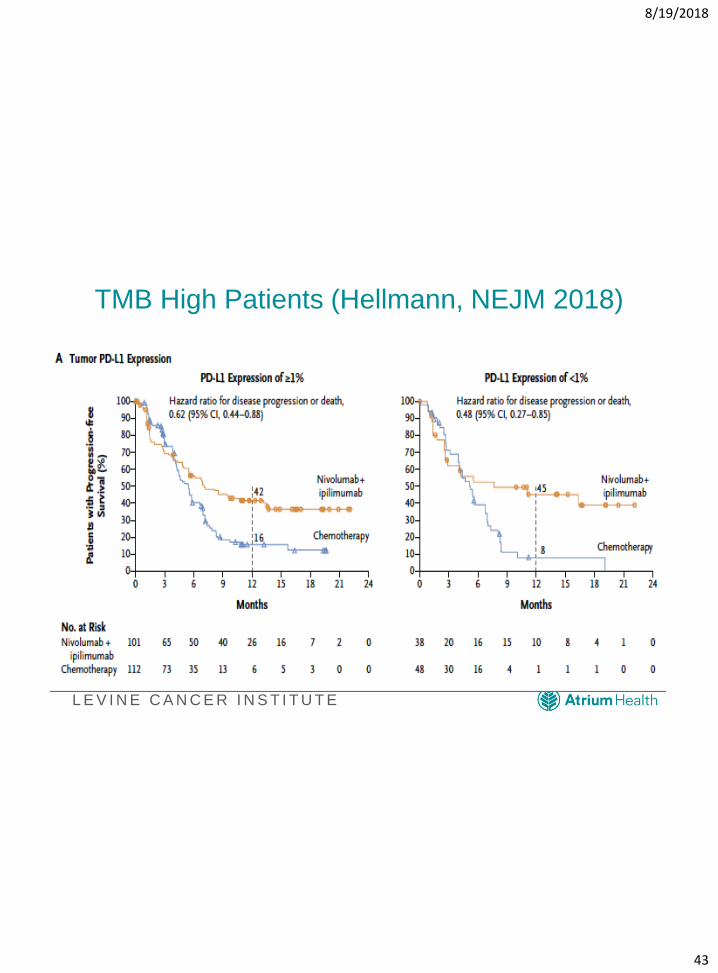
TMB High Patients (Hellmann, NEJM 2018)
8/19/2018
44
L E V I N E C A N C E R I N S T I T U T E
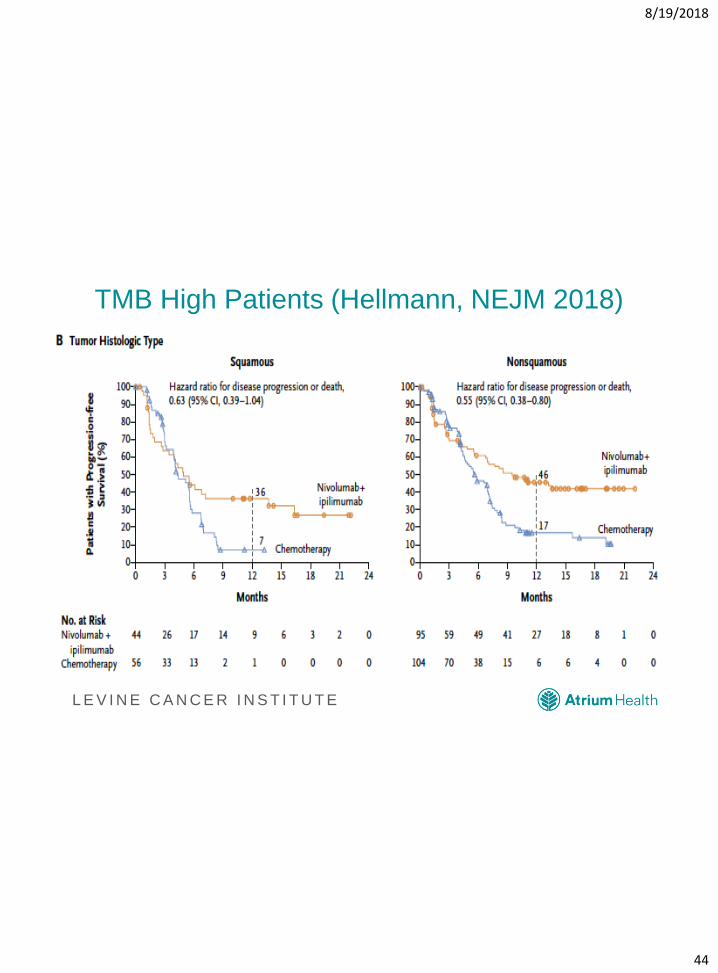
TMB High Patients (Hellmann, NEJM 2018)
8/19/2018
45
L E V I N E C A N C E R I N S T I T U T E
TMB in Lung Cancer
• Tumor Mutational Burden is an interesting marker
• Will it be like MSI-H?
• Still trying to find best clinical fit
– Ipi-Nivo
– Dual markers?
– Logistics
8/19/2018
46
L E V I N E C A N C E R I N S T I T U T E
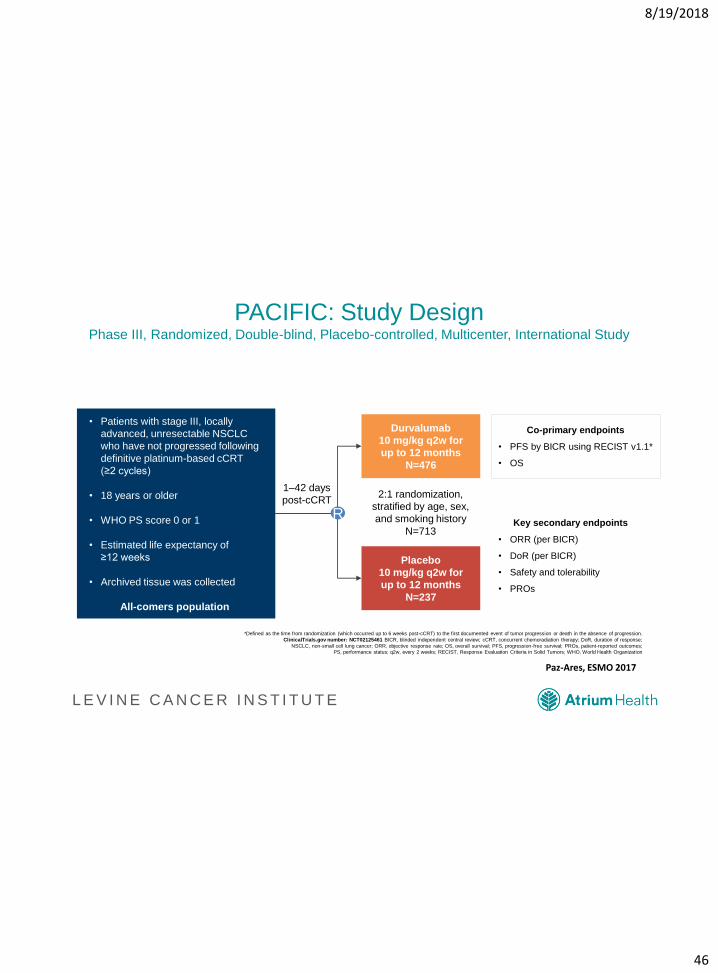
PACIFIC: Study DesignPhase III, Randomized, Double-blind, Placebo-controlled, Multicenter, International Study
*Defined as the time from randomization (which occurred up to 6 weeks post-cCRT) to the first documented event of tumor progression or death in the absence of progression.
ClinicalTrials.gov number: NCT02125461 BICR, blinded independent central review; cCRT, concurrent chemoradiation therapy; DoR, duration of response;
NSCLC, non-small cell lung cancer; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; PROs, patient-reported outcomes;
PS, performance status; q2w, every 2 weeks; RECIST, Response Evaluation Criteria in Solid Tumors; WHO, World Health Organization
• Patients with stage III, locally
advanced, unresectable NSCLC
who have not progressed following
definitive platinum-based cCRT
(≥2 cycles)
• 18 years or older
• WHO PS score 0 or 1
• Estimated life expectancy of
≥12 weeks
• Archived tissue was collected
All-comers population
Durvalumab
10 mg/kg q2w for
up to 12 months
N=476
Placebo
10 mg/kg q2w for
up to 12 months
N=237
2:1 randomization,
stratified by age, sex,
and smoking history
N=713Key secondary endpoints
• ORR (per BICR)
• DoR (per BICR)
• Safety and tolerability
• PROs
Co-primary endpoints
• PFS by BICR using RECIST v1.1*
• OS
R
1–42 days
post-cCRT
Paz-Ares, ESMO 2017
8/19/2018
47
L E V I N E C A N C E R I N S T I T U T E
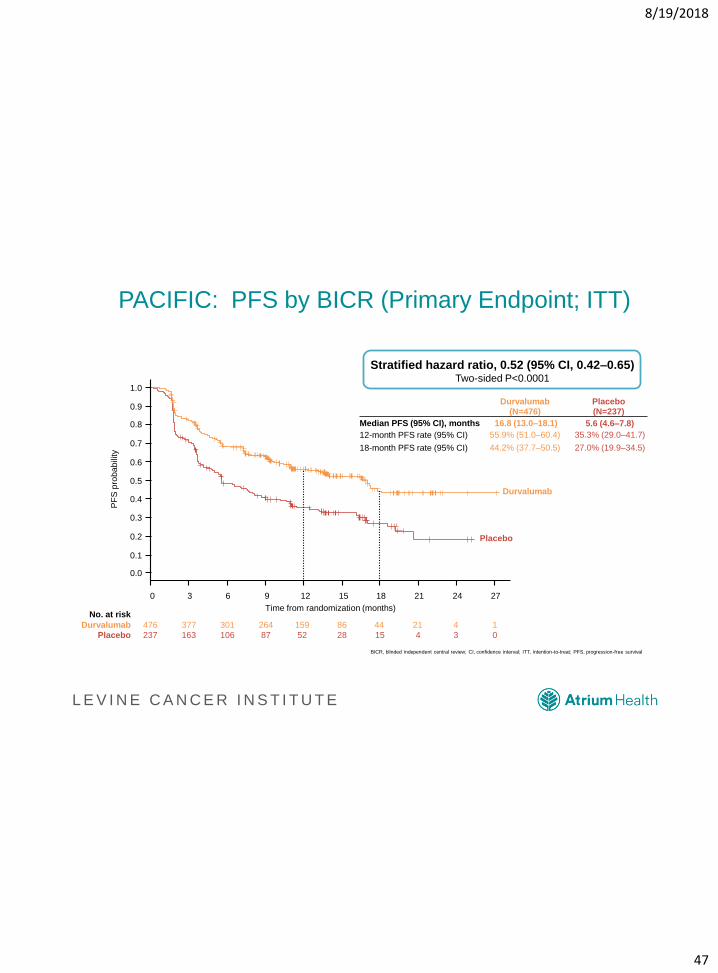
PACIFIC: PFS by BICR (Primary Endpoint; ITT)
PF
S p
robabili
ty
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 3 6 9 12 15 18 21 24 27
Time from randomization (months)
Placebo
Durvalumab
476 377 301 264 159 86 44 21 4
237 163 106 87 52 28 15 4 3
1
0
No. at risk
Durvalumab
Placebo
Durvalumab(N=476)
Placebo(N=237)
Median PFS (95% CI), months 16.8 (13.0–18.1) 5.6 (4.6–7.8)
12-month PFS rate (95% CI) 55.9% (51.0–60.4) 35.3% (29.0–41.7)
18-month PFS rate (95% CI) 44.2% (37.7–50.5) 27.0% (19.9–34.5)
BICR, blinded independent central review; CI, confidence interval; ITT, intention-to-treat; PFS, progression-free survival
Stratified hazard ratio, 0.52 (95% CI, 0.42–0.65)Two-sided P<0.0001
8/19/2018
48
L E V I N E C A N C E R I N S T I T U T E
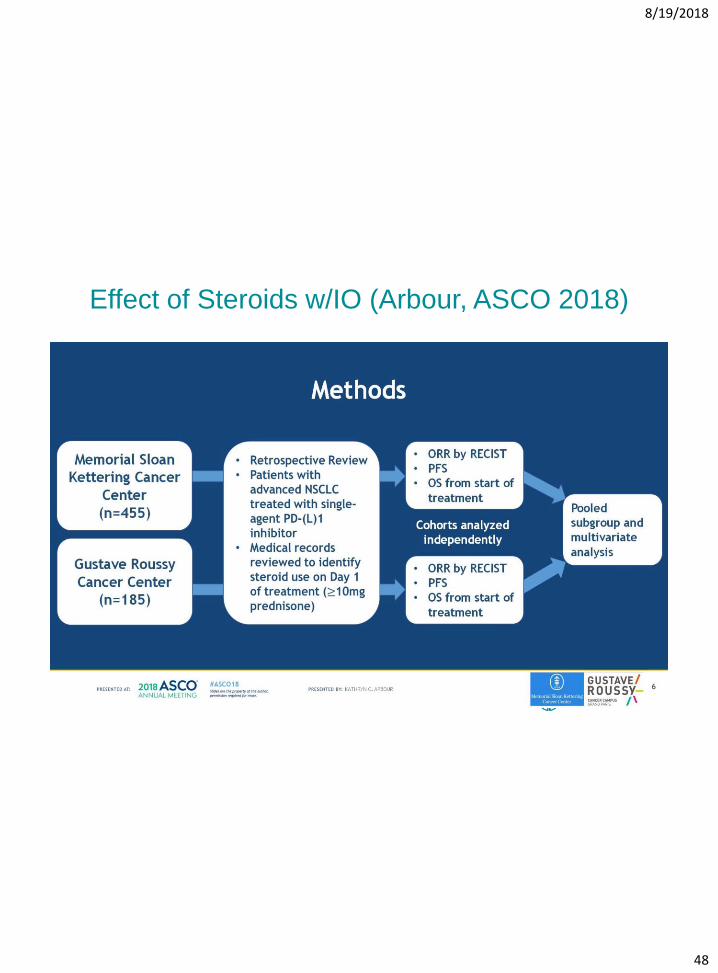
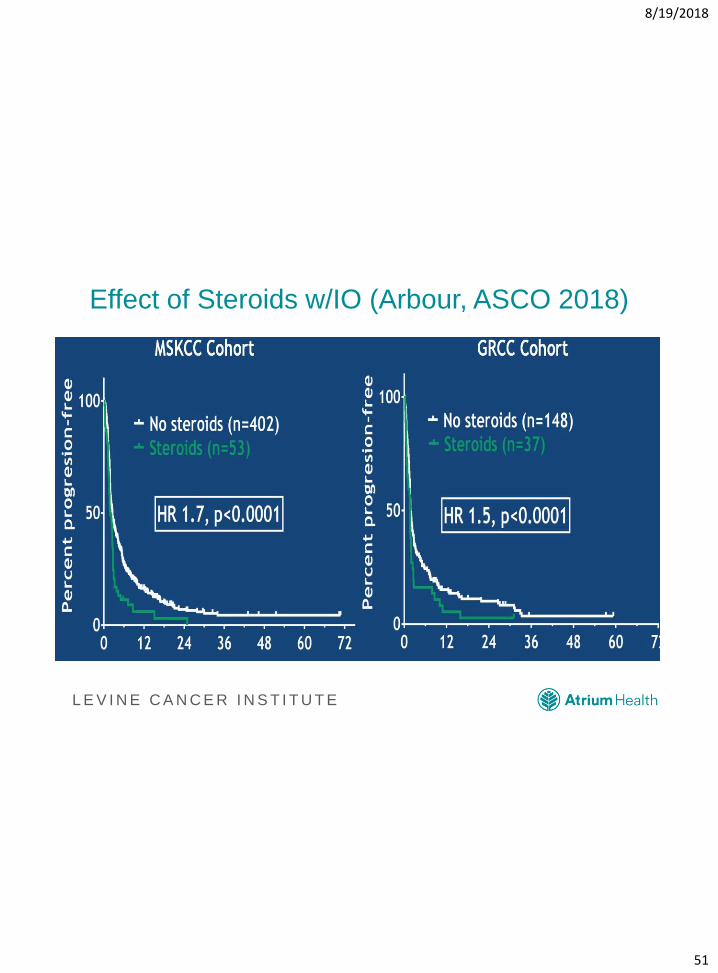
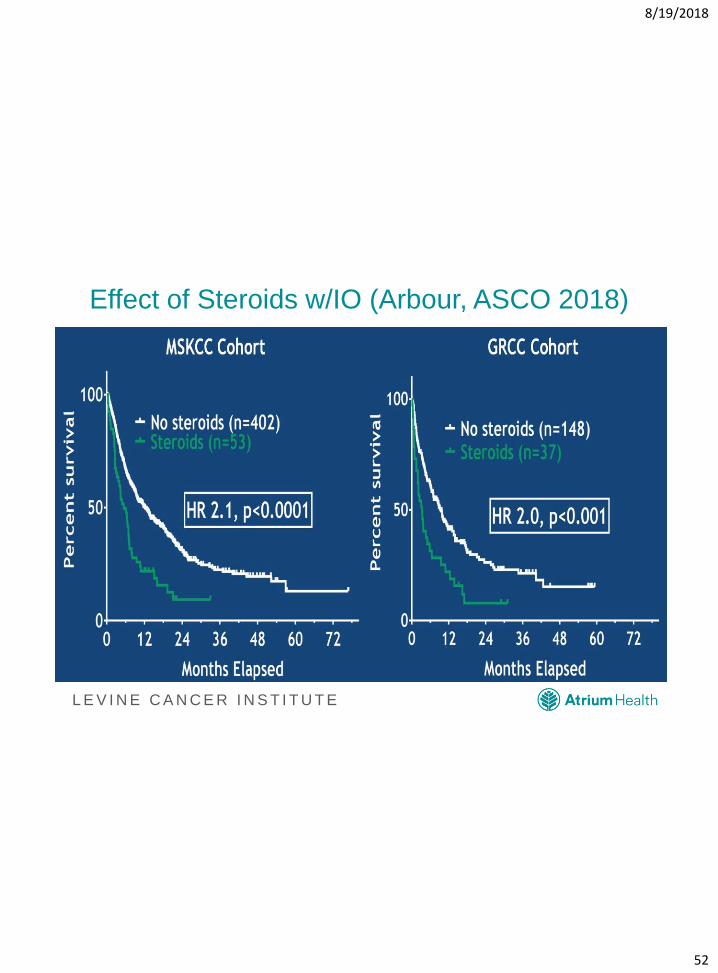
Effect of Steroids w/IO (Arbour, ASCO 2018)
8/19/2018
49
L E V I N E C A N C E R I N S T I T U T E
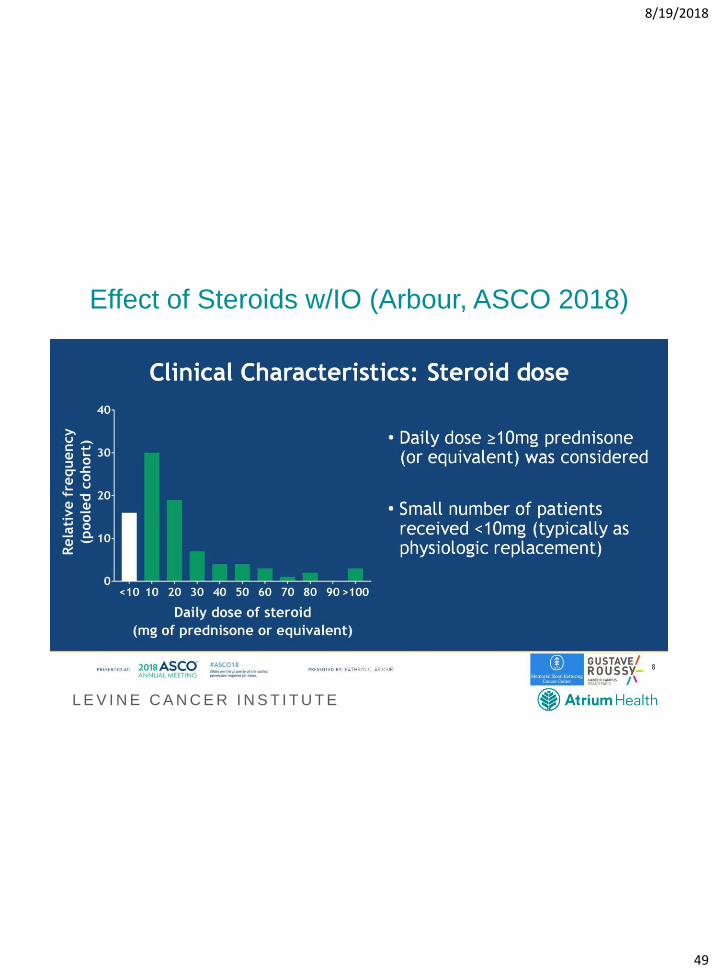
Effect of Steroids w/IO (Arbour, ASCO 2018)
8/19/2018
50
L E V I N E C A N C E R I N S T I T U T E
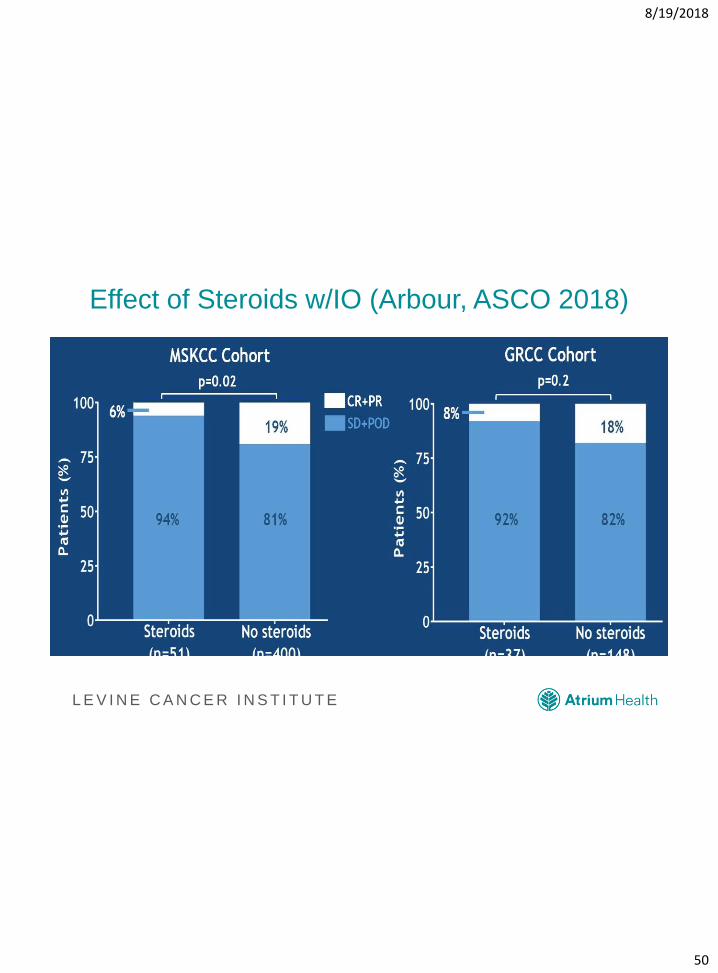
Effect of Steroids w/IO (Arbour, ASCO 2018)
8/19/2018
51
L E V I N E C A N C E R I N S T I T U T E
Effect of Steroids w/IO (Arbour, ASCO 2018)
8/19/2018
52
L E V I N E C A N C E R I N S T I T U T E
Effect of Steroids w/IO (Arbour, ASCO 2018)
8/19/2018
53
L E V I N E C A N C E R I N S T I T U T E
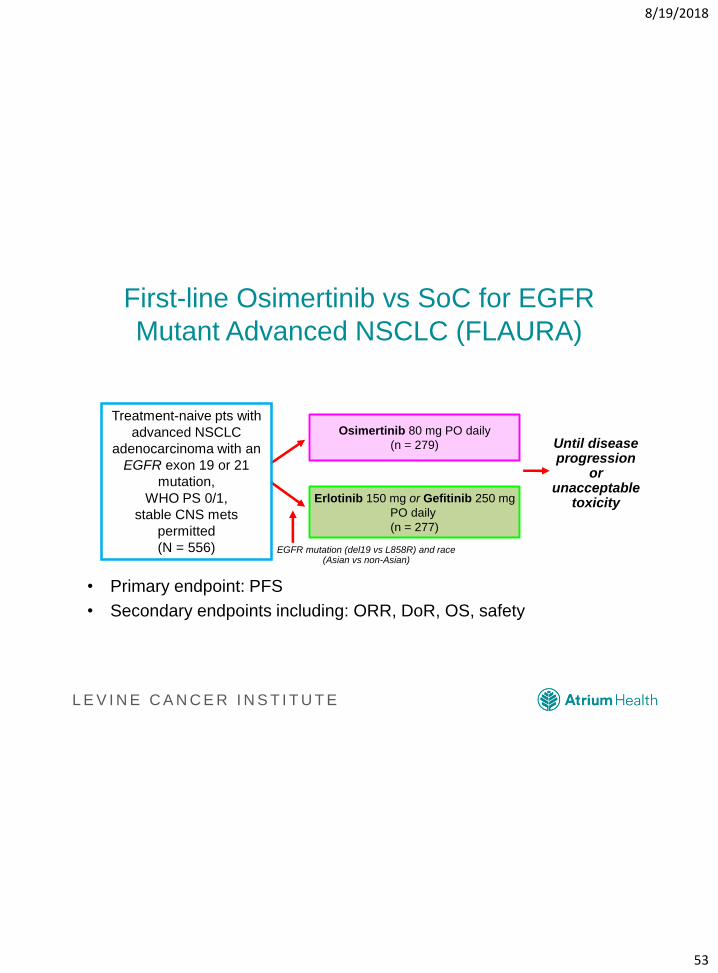
First-line Osimertinib vs SoC for EGFR
Mutant Advanced NSCLC (FLAURA)
• Primary endpoint: PFS
• Secondary endpoints including: ORR, DoR, OS, safety
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
Treatment-naive pts with
advanced NSCLC
adenocarcinoma with an
EGFR exon 19 or 21
mutation,
WHO PS 0/1,
stable CNS mets
permitted
(N = 556)
Osimertinib 80 mg PO daily
(n = 279)
Erlotinib 150 mg or Gefitinib 250 mg
PO daily
(n = 277)
Until disease progression
or unacceptable
toxicity
EGFR mutation (del19 vs L858R) and race (Asian vs non-Asian)
8/19/2018
54
L E V I N E C A N C E R I N S T I T U T E
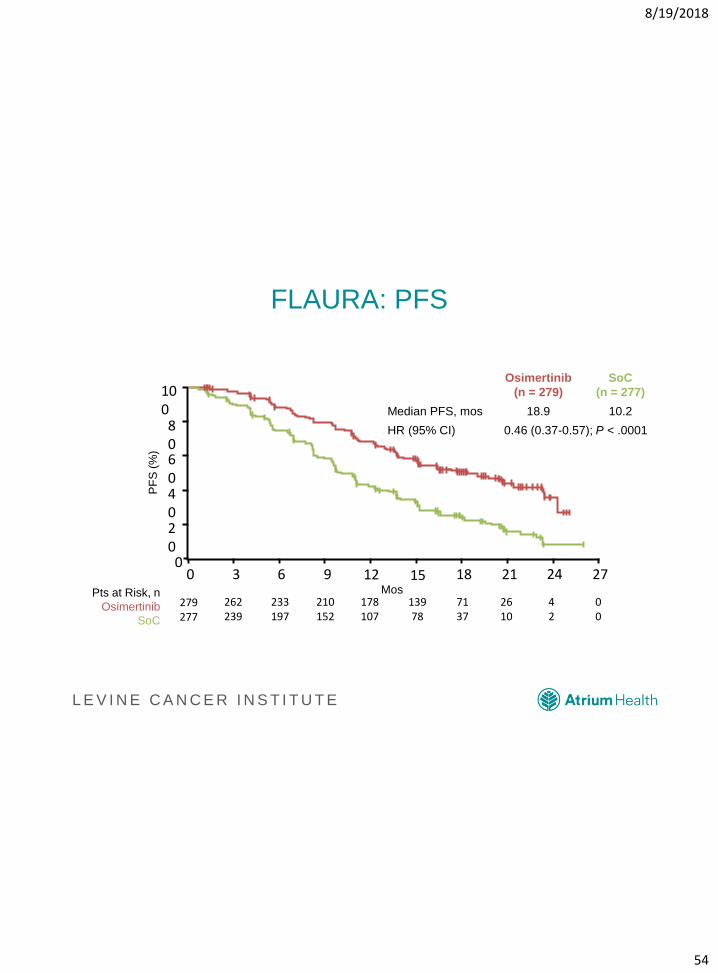
FLAURA: PFS
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
PF
S (
%)
MosPts at Risk, n
Osimertinib
SoC
100806040200
0 6 9 2112 18 24 27
279277
262239
233197
210152
13978
7137
2610
00
153
178107
42
Osimertinib
(n = 279)
SoC
(n = 277)
Median PFS, mos 18.9 10.2
HR (95% CI) 0.46 (0.37-0.57); P < .0001
8/19/2018
55
L E V I N E C A N C E R I N S T I T U T E
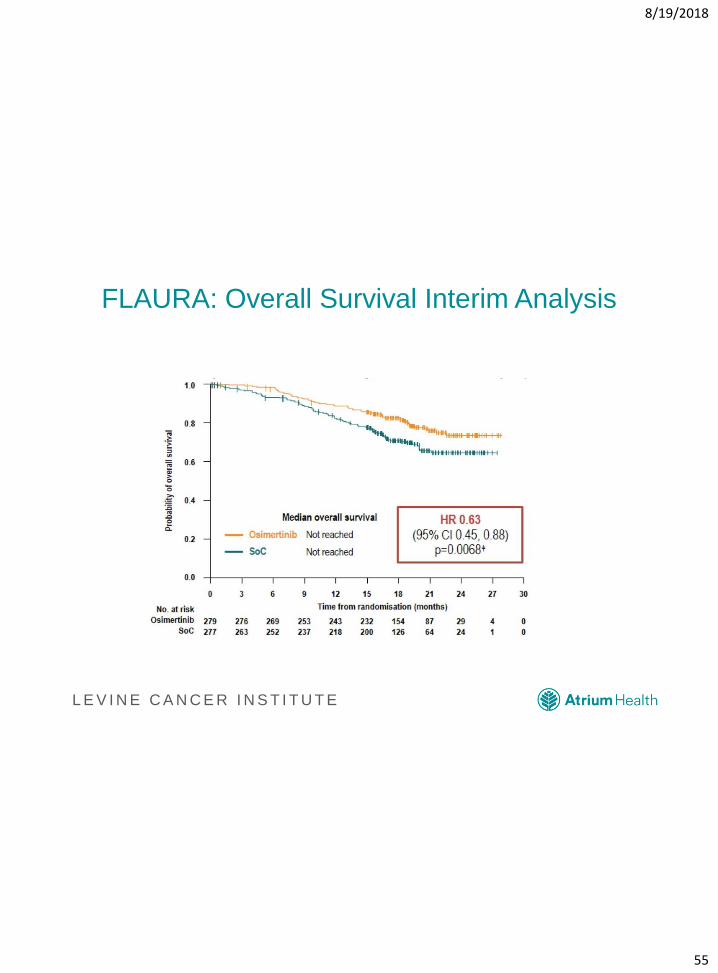
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
FLAURA: Overall Survival Interim Analysis
8/19/2018
56
L E V I N E C A N C E R I N S T I T U T E
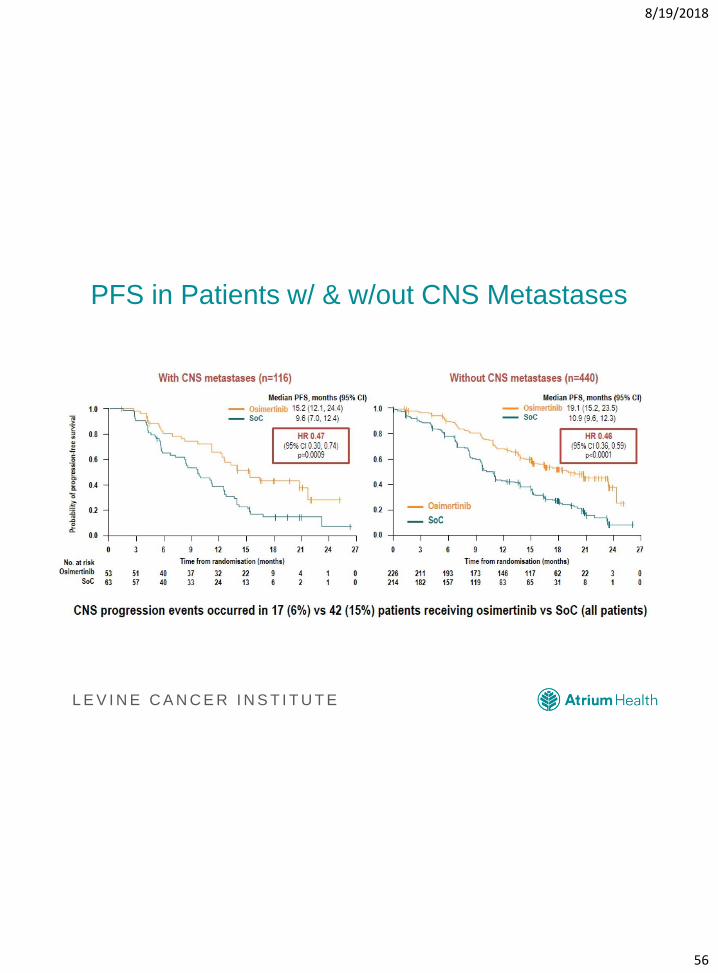
PFS in Patients w/ & w/out CNS Metastases
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
8/19/2018
57
8/19/2018 60
Resistance to Third Generation EGFR TKIs
Thress KS, et al. Nat Med. 2015;21(6):560-562.
8/19/2018
58
L E V I N E C A N C E R I N S T I T U T E
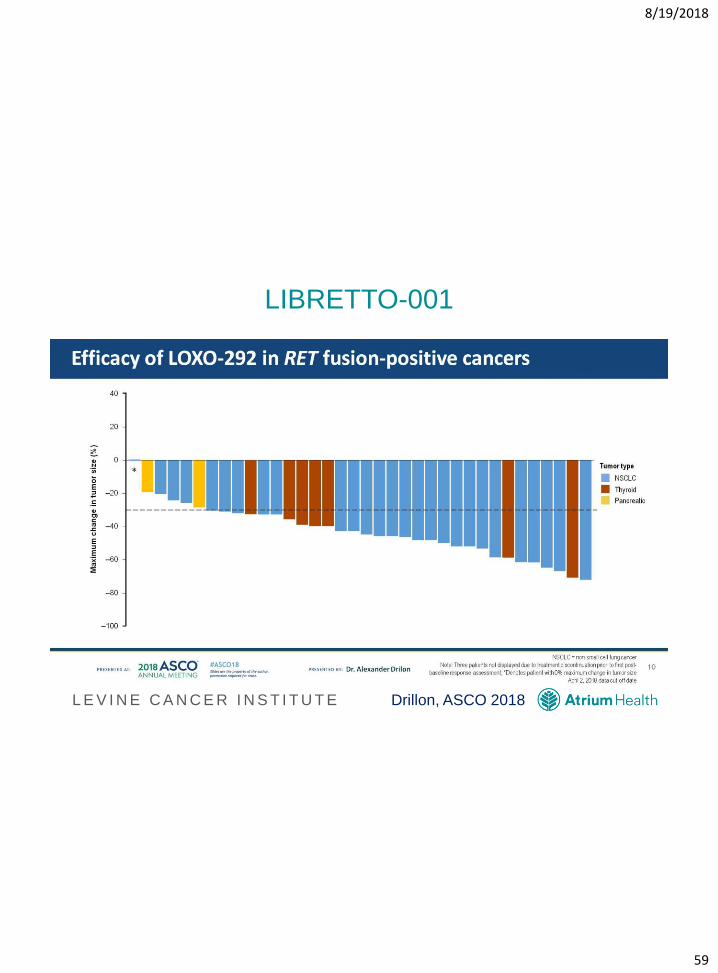
• Other Targeted Therapy
8/19/2018
59
L E V I N E C A N C E R I N S T I T U T E
LIBRETTO-001
Drillon, ASCO 2018
8/19/2018
60
L E V I N E C A N C E R I N S T I T U T E
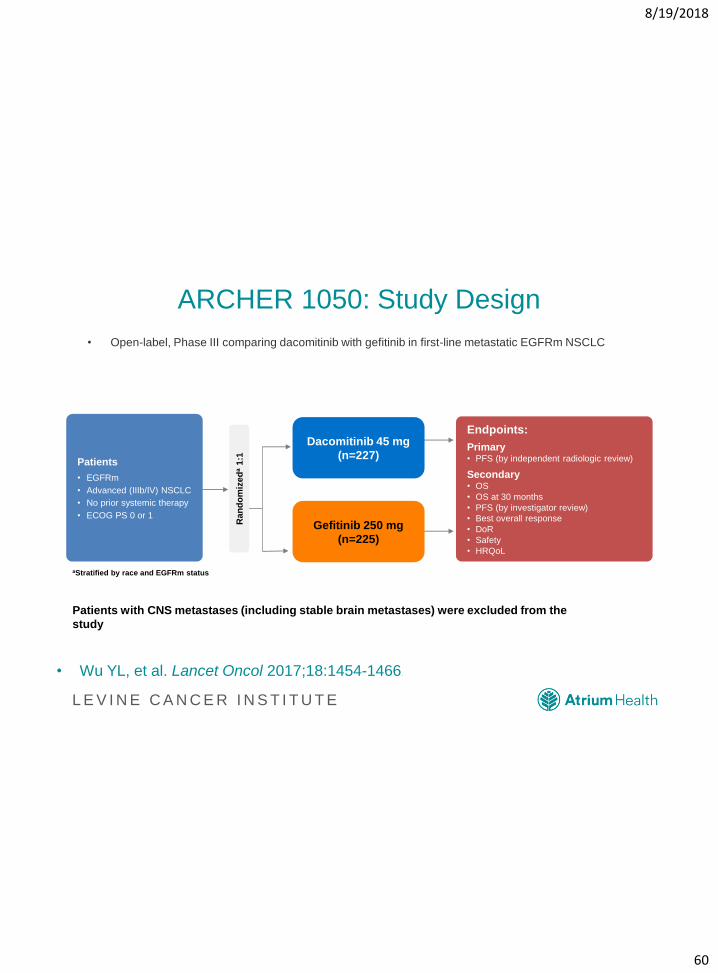
ARCHER 1050: Study Design
• Open-label, Phase III comparing dacomitinib with gefitinib in first-line metastatic EGFRm NSCLC
• Wu YL, et al. Lancet Oncol 2017;18:1454-1466.
63
Patients
• EGFRm
• Advanced (IIIb/IV) NSCLC
• No prior systemic therapy
• ECOG PS 0 or 1
Endpoints:
Primary• PFS (by independent radiologic review)
Secondary• OS
• OS at 30 months
• PFS (by investigator review)
• Best overall response
• DoR
• Safety
• HRQoL
Patients with CNS metastases (including stable brain metastases) were excluded from the
study
aStratified by race and EGFRm status
Ra
nd
om
ize
da
1:1
Dacomitinib 45 mg
(n=227)
Gefitinib 250 mg
(n=225)
8/19/2018
61
L E V I N E C A N C E R I N S T I T U T E
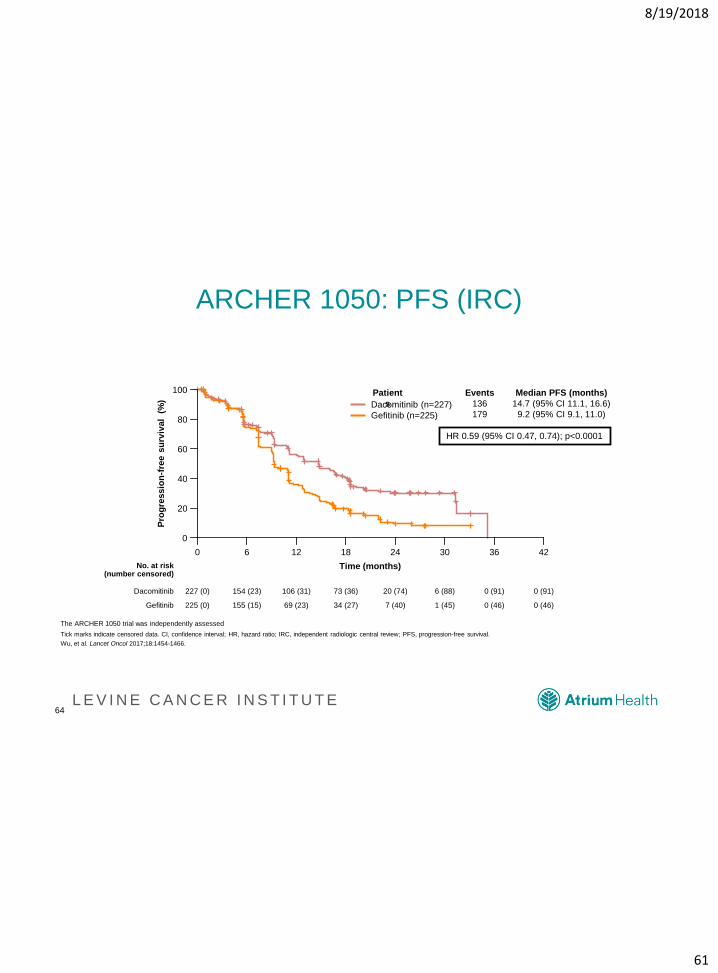
ARCHER 1050: PFS (IRC)
64
HR 0.59 (95% CI 0.47, 0.74); p<0.0001
Dacomitinib (n=227)
Gefitinib (n=225)
Median PFS (months)
14.7 (95% CI 11.1, 16.6)
9.2 (95% CI 9.1, 11.0)
Pro
gre
ss
ion
-fre
e s
urv
ival
(%
)
100
80
60
40
20
0
0 6 12 18 24 30 42
Gefitinib
Dacomitinib
No. at risk(number censored)
Time (months)
36
227 (0) 154 (23) 106 (31) 73 (36) 20 (74) 6 (88) 0 (91)0 (91)
225 (0) 155 (15) 69 (23) 34 (27) 7 (40) 1 (45) 0 (46)0 (46)
Events
136
179
Patient
s
The ARCHER 1050 trial was independently assessed
Tick marks indicate censored data. CI, confidence interval; HR, hazard ratio; IRC, independent radiologic central review; PFS, progression-free survival.
Wu, et al. Lancet Oncol 2017;18:1454-1466.
8/19/2018
62
L E V I N E C A N C E R I N S T I T U T E
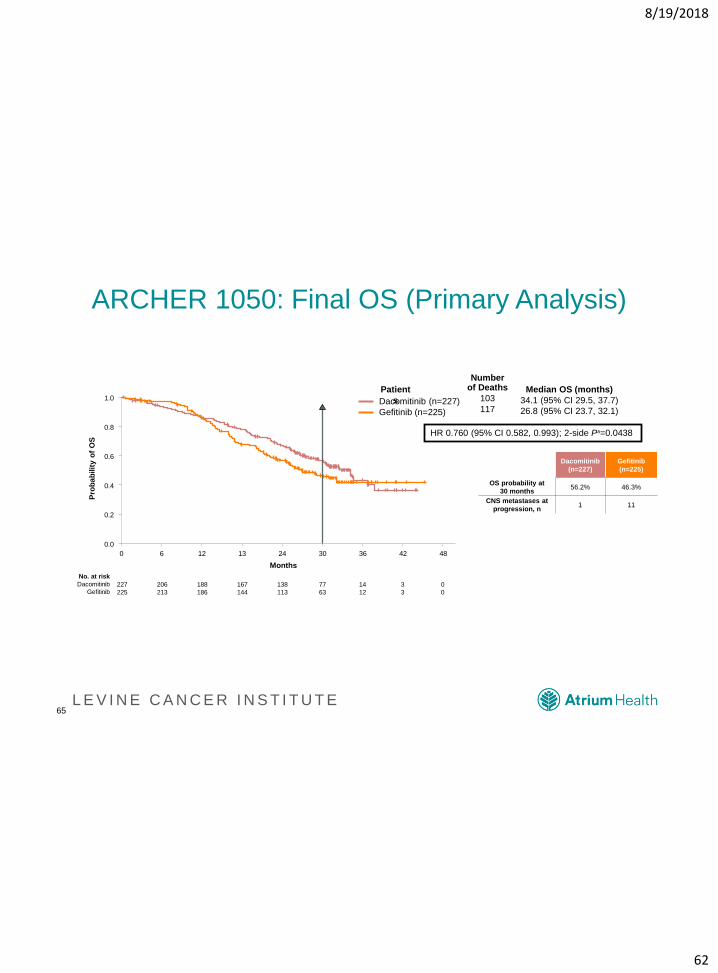
ARCHER 1050: Final OS (Primary Analysis)
65
227
225
206
213
188
186
167
144
138
113
77
63
14
12
3
3
0
0
No. at risk
Dacomitinib
Gefitinib
Dacomitinib
(n=227)
Gefitinib
(n=225)
OS probability at
30 months56.2% 46.3%
CNS metastases at
progression, n1 11
Pro
ba
bilit
y o
f O
S
Months
0 6 12 13 24 30 36 42 48
1.0
0.8
0.6
0.4
0.2
0.0
HR 0.760 (95% CI 0.582, 0.993); 2-side Pa=0.0438
Dacomitinib (n=227)
Gefitinib (n=225)
Median OS (months)
34.1 (95% CI 29.5, 37.7)
26.8 (95% CI 23.7, 32.1)
Numberof Deaths
103
117
Patient
s
8/19/2018
63
L E V I N E C A N C E R I N S T I T U T E
Poziotinib
• EGFR exon20 insertions (affecting 2% of NSCLCs) have
demonstrated resistance to current EGFR TKIs (PFS 2
months, RR <20% to other therapies)
• Poziotinib is an oral, quinazoline-based pan-HER
inhibitor
• Preliminary results of phase II trial
– 8 of 11 patients (73%) demonstrated partial response (ranging
from 30 to 50% tumor reduction)
– 6 of 11 patients required dose reduction (rash, diarrhea)
8/19/2018
64
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
65
L E V I N E C A N C E R I N S T I T U T E
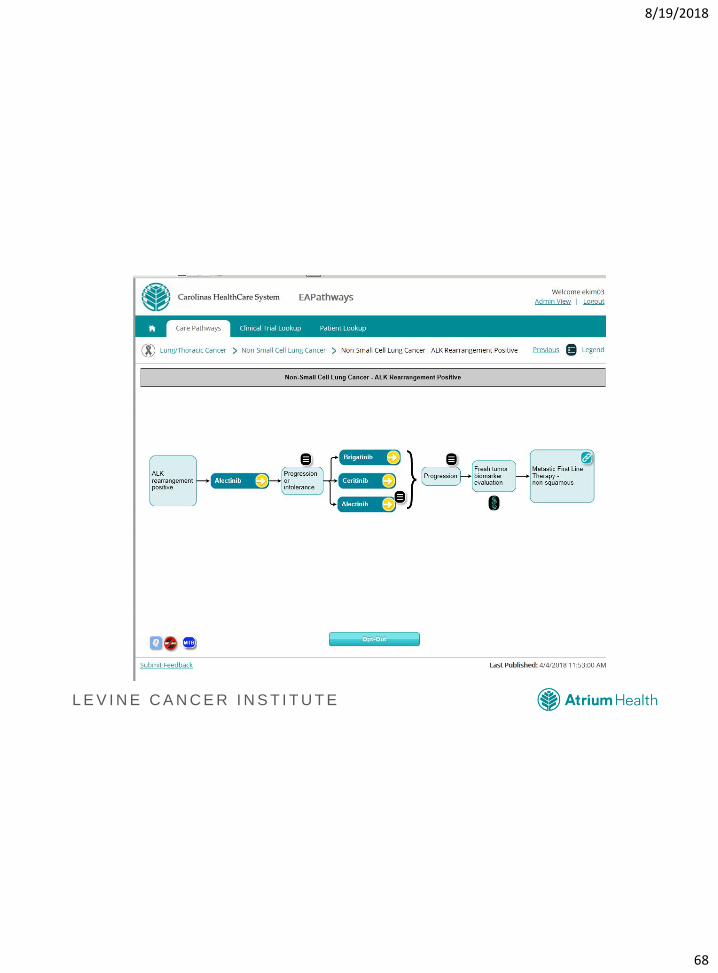
ALK Targeted Therapy Updates
FIRST-LINE
• Crizotinib: mPFS 10.9 months
• Ceritinib: mPFS 16.6 months
• Alectinib: mPFS 25.7 months
NEXT-LINE
• Crizotinib: mPFS 7.7 months
• Ceritinib: mPFS 5.4 months
• Alectinib: mPFS 8.9 months
• Brigatinib: mPFS 12.9
months
• Lorlatinib
• Ensartinib
8/19/2018
66
L E V I N E C A N C E R I N S T I T U T E
ALEX: Results In CNS
• Alectinib reduced the risk for CNS progression by 84%
compared with crizotinib (HR, 0.16; 95% CI, 0.10-0.28;
p<0.0001).
• The 12-month cumulative rate of CNS progression was
9.4% vs 41.4%.
• CNS ORR = 81% vs 50% (CR rate 38% vs 5%)
8/19/2018
67
L E V I N E C A N C E R I N S T I T U T E
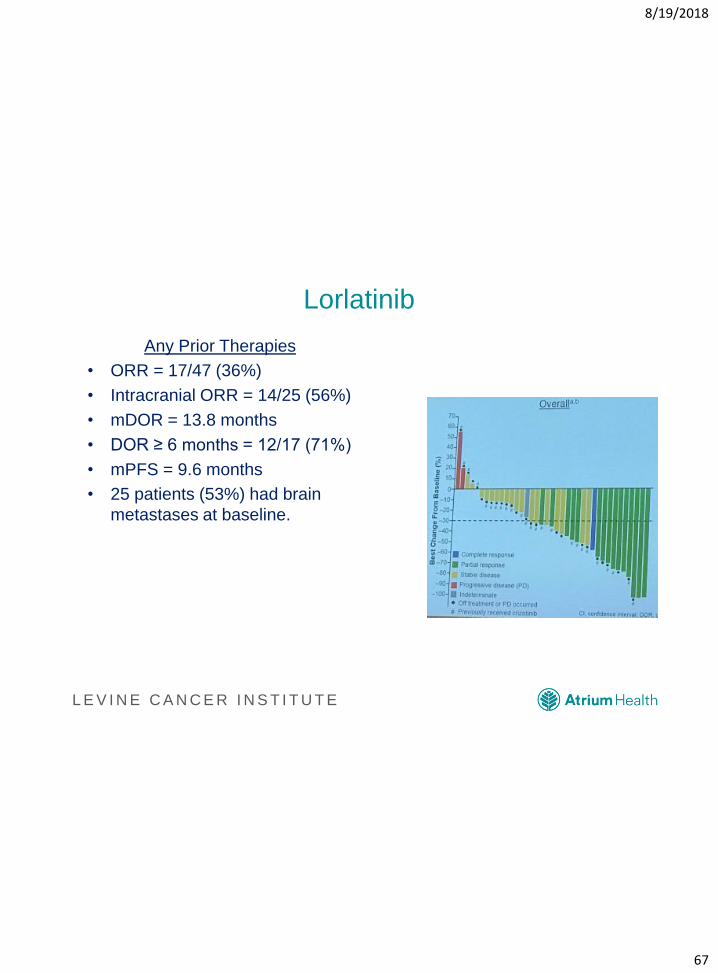
Lorlatinib
Any Prior Therapies
• ORR = 17/47 (36%)
• Intracranial ORR = 14/25 (56%)
• mDOR = 13.8 months
• DOR ≥ 6 months = 12/17 (71%)
• mPFS = 9.6 months
• 25 patients (53%) had brain
metastases at baseline.
Solomon, et al. IASLC 18th WCLC; 2017, Japan.
8/19/2018
68
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
69
L E V I N E C A N C E R I N S T I T U T E
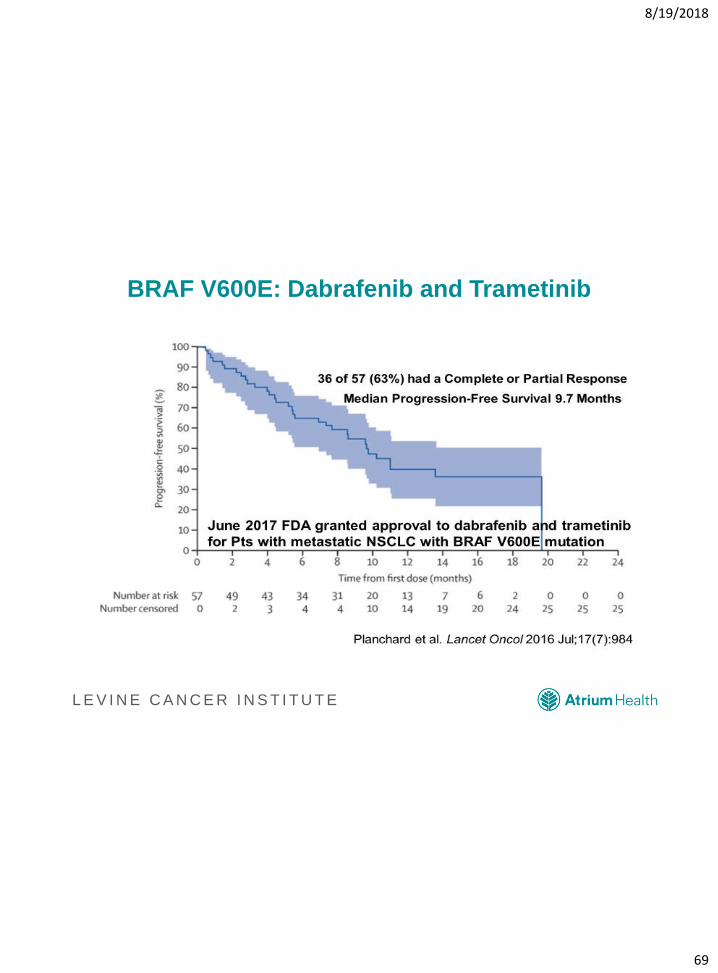
BRAF V600E: Dabrafenib and Trametinib
8/19/2018
70
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
71
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
72
L E V I N E C A N C E R I N S T I T U T E
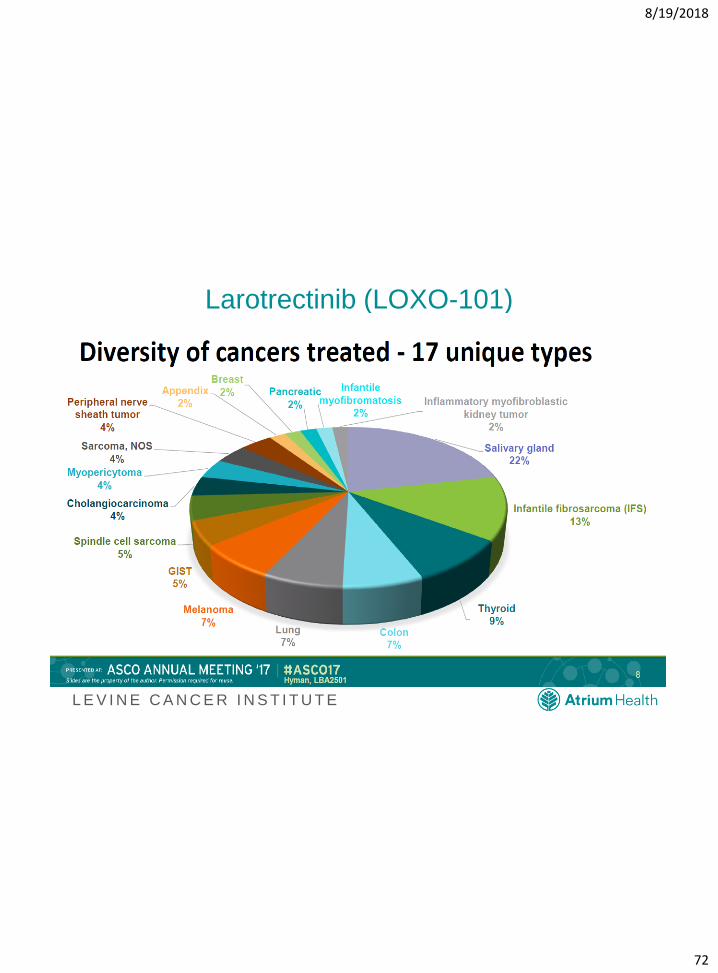
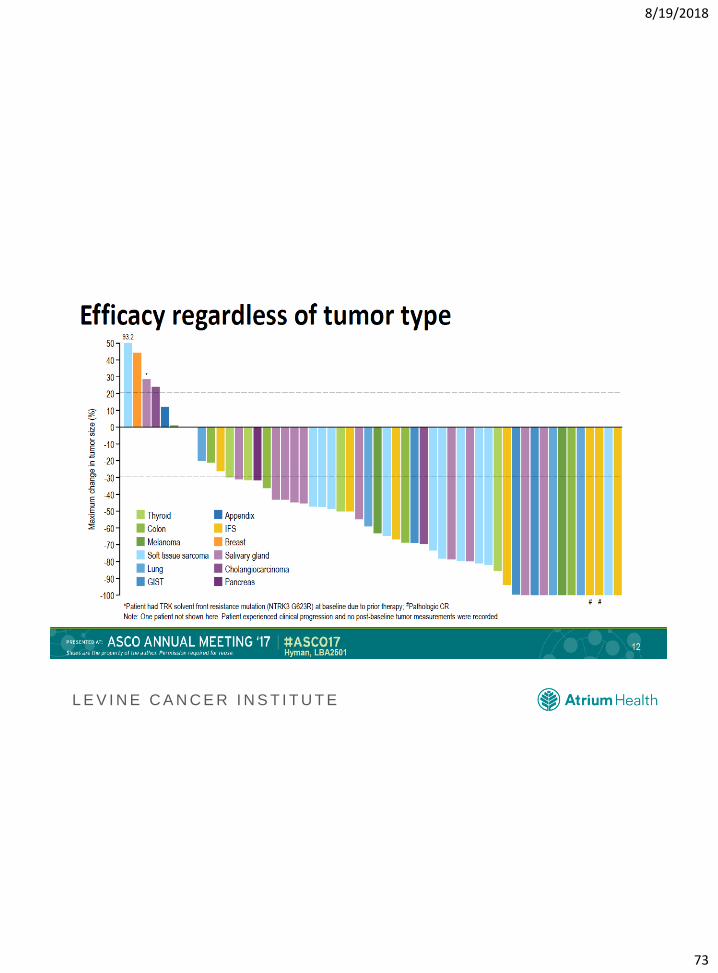
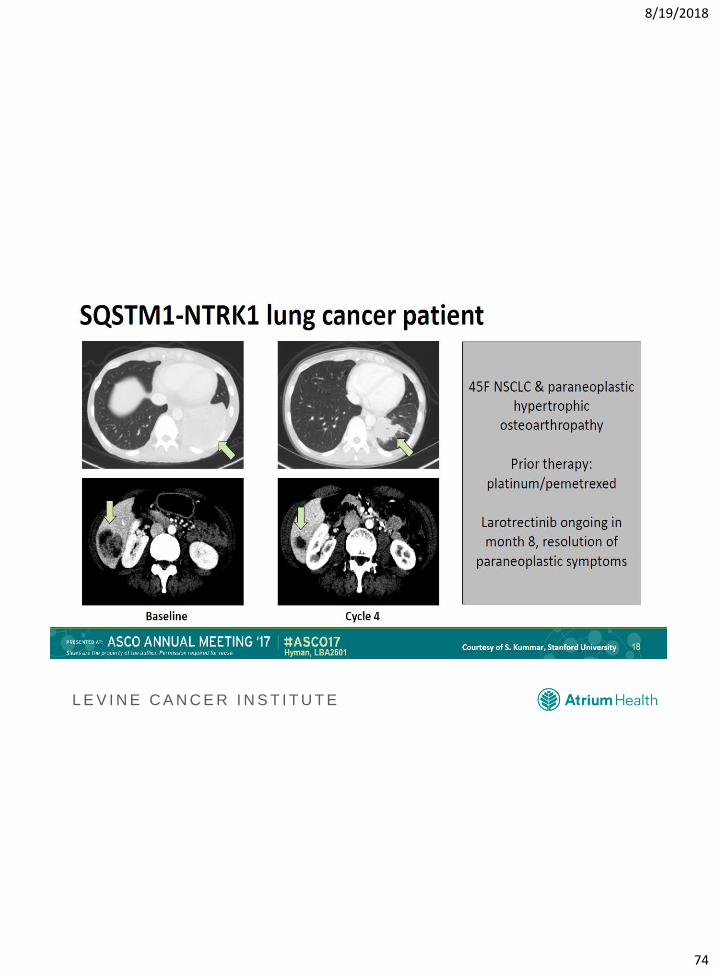
Larotrectinib (LOXO-101)
8/19/2018
73
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
74
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
75
L E V I N E C A N C E R I N S T I T U T E
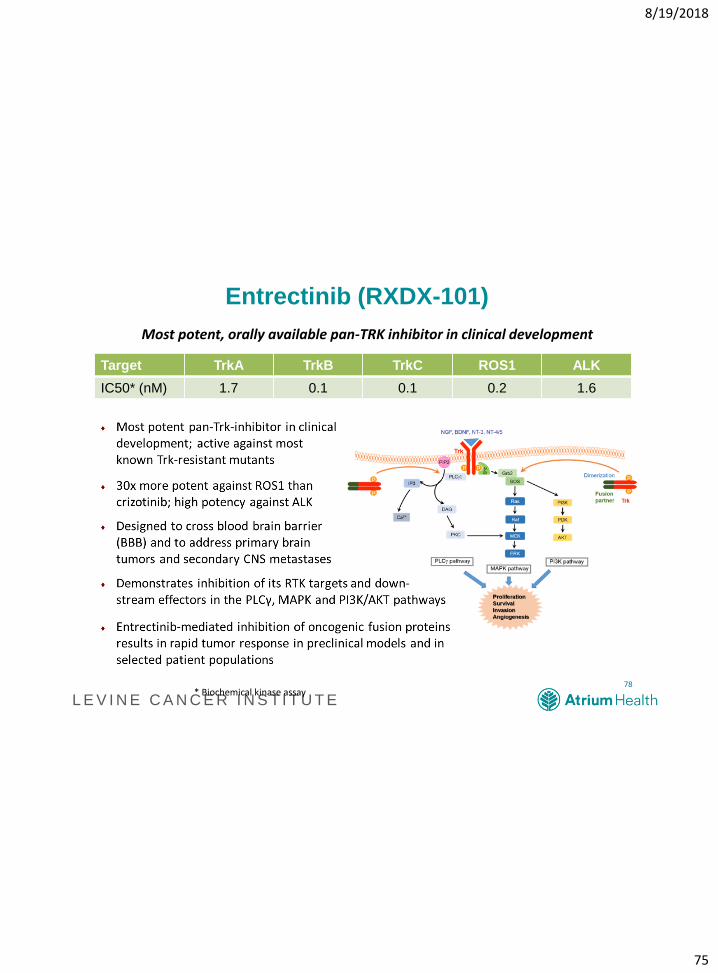
Entrectinib (RXDX-101)
Target TrkA TrkB TrkC ROS1 ALK
IC50* (nM) 1.7 0.1 0.1 0.2 1.6
78* Biochemical kinase assay
Most potent, orally available pan-TRK inhibitor in clinical development
8/19/2018
76
L E V I N E C A N C E R I N S T I T U T E
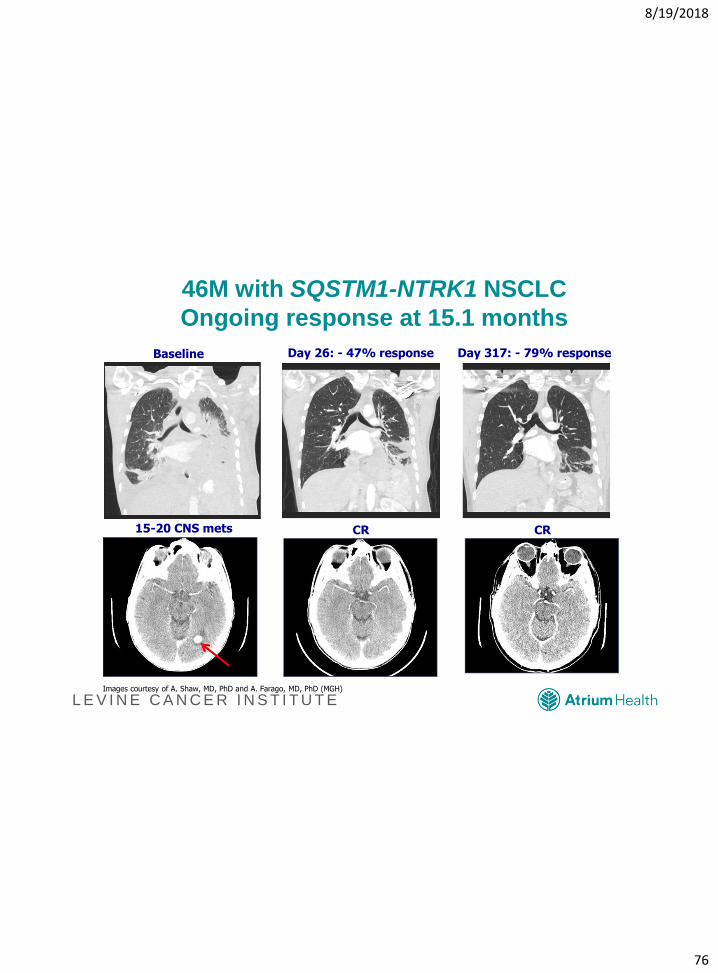
46M with SQSTM1-NTRK1 NSCLC
Ongoing response at 15.1 months
Baseline Day 26: - 47% response Day 317: - 79% response
15-20 CNS mets CR CR
Images courtesy of A. Shaw, MD, PhD and A. Farago, MD, PhD (MGH)
8/19/2018
77
L E V I N E C A N C E R I N S T I T U T E
Levine Cancer Institute
Carolinas HealthCare System
• Started with 3 community practices
• 25 Locations
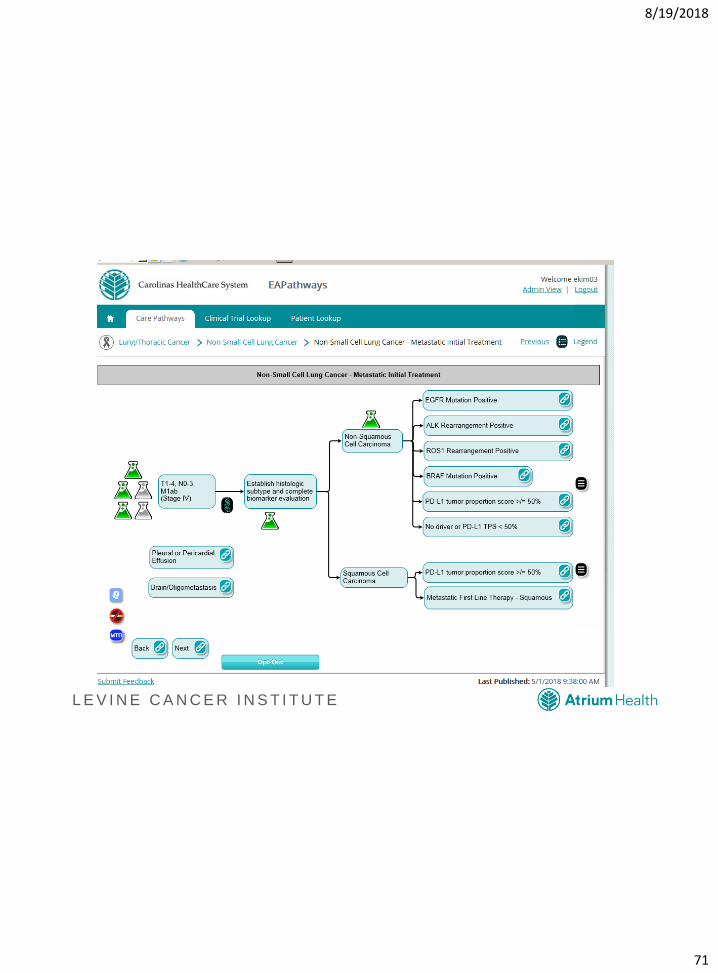
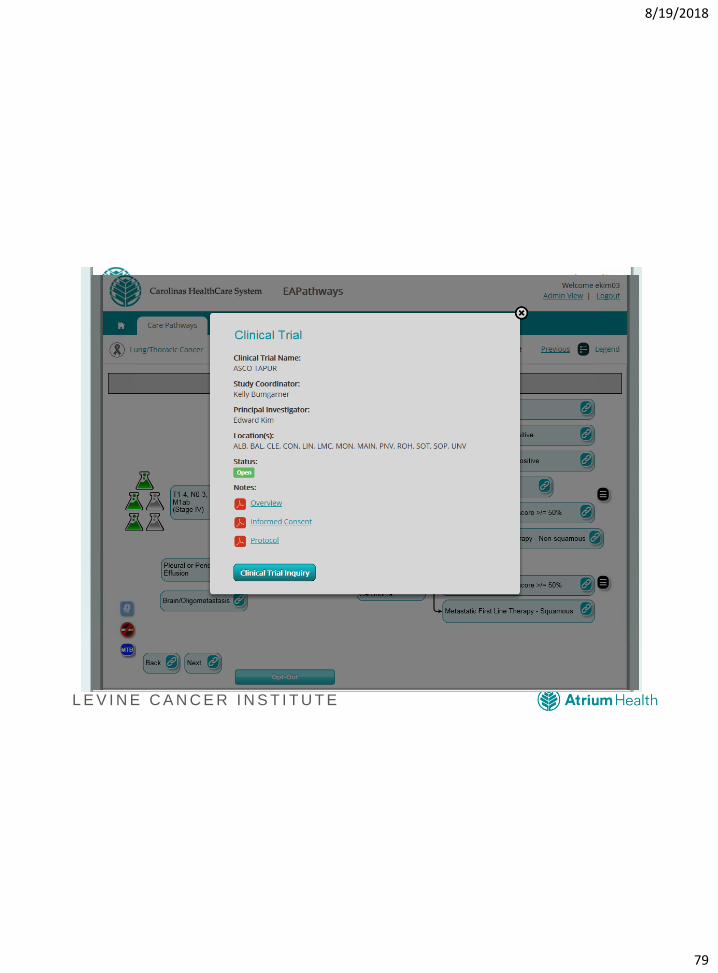
• EAPathways
• Multi-Site Phase I Unit
• Bone Marrow Transplant Unit
• Biostatistics Department
• Biospecimen Repository
• Patient Navigation
• Supportive Oncology Department
• Integrative Medicine
• Senior Oncology
• >100 Providers
• >400 Clinical Trials
• CAR-T cellular therapy performed
Derek Raghavan, MD
President, Levine Cancer
Institute
8/19/2018
78
L E V I N E C A N C E R I N S T I T U T E
Targeted Agent and Profiling Utilization
Registry (TAPUR) Study
• Pragmatic phase 2 study with FDA-approved, targeted
agents
• 60-70% match rates
• Incorporates general and drug-specific eligibility criteria
• Adopted ASCO-Friends Eligibility Criteria
8/19/2018
79
L E V I N E C A N C E R I N S T I T U T E
8/19/2018
80
L E V I N E C A N C E R I N S T I T U T E
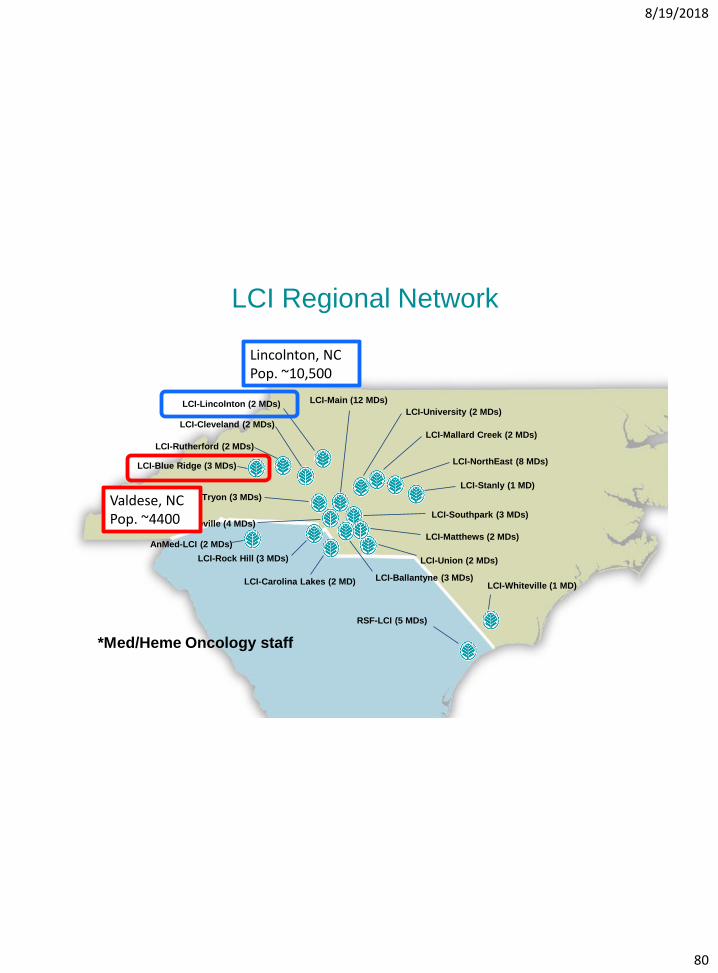
LCI Regional Network
LCI-Cleveland (2 MDs)
LCI-NorthEast (8 MDs)
LCI-Main (12 MDs)
LCI-Union (2 MDs)
LCI-Pineville (4 MDs)
LCI-University (2 MDs)
LCI-Ballantyne (3 MDs)
LCI-Rock Hill (3 MDs)
LCI-Mallard Creek (2 MDs)
LCI-South Tryon (3 MDs)
LCI-Southpark (3 MDs)
LCI-Matthews (2 MDs)
LCI-Carolina Lakes (2 MD)
LCI-Stanly (1 MD)
AnMed-LCI (2 MDs)
RSF-LCI (5 MDs)
LCI-Rutherford (2 MDs)
LCI-Blue Ridge (3 MDs)
LCI-Whiteville (1 MD)
LCI-Lincolnton (2 MDs)
*Med/Heme Oncology staff
Valdese, NCPop. ~4400
Lincolnton, NCPop. ~10,500
8/19/2018
81
L E V I N E C A N C E R I N S T I T U T E
Current State of Lung Cancer 2018
• Biomarker assessment as important as
histology
• Adequate tissue at diagnosis essential
• Less chemotherapy 1st line paradigm evolving
• Multiple TKI therapy
• Immunotherapy
• Sequencing
• Patient is the most precious resource

8/19/2018
82
L E V I N E C A N C E R I N S T I T U T E
The Fight Against Lung Cancer