LUNG ABSCESS ETIOLOGY, PATHOPHYSIOLOGY & MANAGEMENT – NEIL BARRY.
24
LUNG ABSCESS ETIOLOGY, PATHOPHYSIOLOGY & MANAGEMENT – NEIL BARRY
-
Upload
randell-reed -
Category
Documents
-
view
234 -
download
4
Transcript of LUNG ABSCESS ETIOLOGY, PATHOPHYSIOLOGY & MANAGEMENT – NEIL BARRY.

LUNG ABSCESSETIOLOGY, PATHOPHYSIOLOGY & MANAGEMENT – NEIL BARRY

Definition
• A lung abscess is a localised collection of pus within the lung that leads to formation of a cavity, usually with a thick wall.
• Abscesses occur most commonly when microbial infection causes necrosis of the lung parenchyma, forming 1 or more cavities.
• Communication of such cavities with the bronchial tree results in a cough productive of purulent sputum and the presence of air-fluid levels.
• Commonly associated with aspiration of oral secretions.

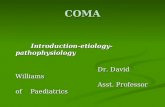
LARGE RIGHT LOWER LOBE ABSCESS DEMONSTRATING A CAVITY THAT CONTAINS AN AIR-FLUID LEVEL.

ETIOLOGY:
▪ Lung abscess is usually a polymicrobial infection. Anaerobic bacteria are abundant in the gingival crevices, particularly in the presence of periodontal disease, and are major pathogens
Most Common
infections caused by aerobic bacteria (streptococcus
pneumoniae, streptococcus pyogenes, staphylococus aereus,
klebsiella pneumonie, pseodomonas aeruginosa, proteus
vulgaris, escherichia coli, neisseria meningitidis, haemophillus
influenzae)

ETIOLOGY:
infections caused by anaerobic bacteria (clostridium hystoliticum, bacteroides fragilis).
Mixed (aerobic and anaerobic bacteria) infections ( observed pretty frequently)
mycotic infections - infrequent cases, found usually in chronic abscesses
caused by protozoa (entamoeba histolytica) diagnosed extremely rarely in our climatic zone

Pathophysiology
▪ Lung abscess commonly occurs in patients with a predisposition to gastric content aspiration due to altered consciousness. E.g. as a result of surgery- opioid use.
▪ Aspiration of gastric contents can also result from dysphagia associated with neurological or esophageal disease.
▪ Common causes of gastric content aspiration include seizures, stroke, neurological bulbar dysfunction, drug overdose, and general anesthesia
▪ Other causes include dental or oropharyngeal surgery (especially tonsillectomy in the sitting position) and esophageal diseases (stricture, malignancy, and reflux).

Pathophysiology
▪ Nasogastric and endotracheal tubes that interfere with normal anatomical barriers predispose to aspiration of oropharyngeal fluid.
▪ Aspiration of contaminated oropharyngeal secretions results in necrotising infection that follows a segmental distribution limited by the pleura.
▪ The resultant cavity is usually solitary, with a thick, fibrous wall at its periphery. Expansion to the pleural space is uncommon. As gastric content aspiration usually occurs in the supine position, in aspiration-related lung abscess lesions are found in the right lung and in the dependent portions of the lungs (i.e., posterior segment of the right upper lobe and superior segments of both lower lobes).

Pathophysiology
▪ Other processes that may result in lung abscess include infection distal to an obstructing tumour or foreign body, secondary infection of an infarct related to a pulmonary embolus, and septic embolisation from right-sided (e.g., tricuspid valve) bacterial endocarditis or peripheral septic thrombophlebitis
▪ irect expansion through the diaphragm of a liver amoebic abscess may result in an amoebic lung abscess, which typically occurs in the right lower lobe.
▪ Nearly 50% of lung abscesses occurring in adults >50 years of age are associated with lung tumours, and preceding pneumonia is reported in 17% to 40% of cases.

Management-
▪ These can be followed by surgical intervention
Bronchoscopy
Step 2Chest Physiotherapy
Step 1Empirical IV antibiotics

Management – Chest Physiotherapy
▪ Placing patients with a large lung abscess in the lateral decubitus position with the abscess side down could prevent sudden discharge of abscess content causing asphyxiation or spread of infection to other lung segments.
▪ Chest physiotherapy and postural drainage may improve clearance of purulent and necrotic abscess contents.
▪ Plurulent: consisting of, containing, or discharging pus
▪ Necrotic: a form of cell injury that results in the premature death of cells in living tissue.

▪ The goals of CPT are to move bronchial secretions to the central airways via gravity,
▪ external manipulation of the chest,
▪ and to eliminate secretions by cough or aspiration with a catheter.
▪ Improved mobilization of bronchial secretions contributes to improved ventilation-perfusion matching and the normalization of the functional residual capacity.

Chest Physiotherapy
▪ Turning is the rotation of the body about its long axis.
▪ This is usually done in conjunction with procedures designed to aid patient comfort and skin care.
▪ However, attention to chest position and deliberate region-specific positioning is usually needed to effect secretion mobilization.
▪ Postural drainage is the positioning of the patient and bed in such a way as to have the carina inferior to a lung segment to be drained.
▪ The targeted lung segment is as nearly perpendicular to the ground as possible.
▪ The aim is to move secretions from peripheral to more central airways for elimination. The duration is usually 3 to 15 minutes per segment depending on the properties of the secretions.

Chest Physiotherapy
▪ Percussion may also be referred to as cupping or clapping.
▪ These names describe the manual rhythmic striking of the thorax over a lung segment which is being drained.
▪ The theory is that this energy is transmitted through the chest wall to the lung and is able to dislodge secretions adhering to lung tissue.

Chest Physiotherapy
▪ Vibration is the placement of hands along the ribs in the direction of expiratory movement of the chest.
▪ A small rapid vibration (tremor) and slight pressure is applied during exhalation to accentuate this phase of the respiratory cycle.
▪ The maneuver mimics the forced exhalation of a cough.
▪ A vigorous form of this manual vibration combined with positive pressure ventilation is called an "artificial cough".
▪ This is used as an assistive technique for sputum removal in paralyzed patients on ventilators.
▪ Mechanical devices used to perform vibration differ from the manual method in that the mechanical device is continuously applied during both inspiration and exhalation.

Chest Physiotherapy
▪ When the spontaneous cough is inadequate to mobilize secretions, directed cough techniques may be employed.
▪ Directed cough techniques are deliberate maneuvers that are taught, supervised, and monitored.
▪ The Forced Expiratory Technique, or "huff cough," and manually assisted cough are two such maneuvers.

Chest Physiotherapy: Contraindications and Precautions
▪ Appropriate precautions include:
▪ the immediate availability of functional suction equipment, emergency airway
▪ equipment, and oxygen therapy equipment
▪ Adrenergic bronchodilators in solution and metered dose inhalers should be available in case of significant bronchospasm during treatment.

▪ The absence of an acceptable cough may render application of CPT less effective.
▪ Diligence in coaching the patient to an effective cough as well as timely suctioning of the trachea are essential to performing good CPT.
▪ Instruction in proper cough technique prior to therapy may decrease the risk of decompensation in case of pulmonary hemorrhage or mobilization of copious secretions.

Chest Physiotherapy
▪ Adverse Reactions and Interventions
▪ Hypoxemia: Administer higher concentrations of oxygen before and during therapy if the patient has a potential or history of falling arterial oxygen saturation
▪ Increases in Intracranial Pressure: Patients at risk for neurological status changes (i.e., patients with clotting or bleeding abnormalities) must be closely monitored. Assess the patient frequently for his/her tolerance of the therapy, especially for acute onset or worsening headache

▪ Acute hypotension during therapy: An acute fall in the blood pressure must be heated by a return of the patient to an appropriate rest position.
▪ Pain or Injury to Muscles, Ribs or Spine: Coordination of CPT with pain medication administration may serve to lessen the pain in patients.
▪ Pulmonary Hemorrhage: stop therapy immediately
▪ Vomiting and/or Aspiration: The Trendelenberg position is contraindicated in patients clearly at risk of aspiration.

Chest Physiotherapy
▪ Trendelenburg position

Assessment of Outcome
▪ Change in Sputum Production
▪ Change in Breath Sounds
▪ Subjective Change Reported by Patient
▪ Improved Quality of Sleep
▪ Change in Vital Signs
▪ Change in the Chest Radiograph
▪ Change in Gas Exchange
▪ Change in Lung Mechanics

Summary
▪ Circumscribed collection of pus in the lung that leads to cavity formation, usually with an air-fluid level visible on Chest radiography.
▪ Aspiration of gastric contents is the most common causative factor.
▪ Mixed microbial flora, including anaerobic bacteria and microaerophilic streptococci, are involved in the formation of abscesses related to the aspiration of gastric contents.
▪ Fever associated with a productive cough and putrid expectoration is a common clinical manifestation.
▪ Diagnosis is based on radiological findings revealing cavitation with an air-fluid level. Documenting anaerobic infection is usually difficult.
▪ Treatment options include antimicrobial agents against aerobic and anaerobic bacteria, given alone or in combination, and chest physiotherapy
▪ Image-guided percutaneous drainage or surgical resection is reserved for patients not responding to antimicrobial treatment.

References
▪ Bartlett JG. Anaerobic bacterial infections of the lung. Chest. 1987;91:901-909.Wang JL, Chen KY, Fang CT, et al. Changing bacteriology of adult community-acquired lung abscess in Taiwan: Klebsiella pneumoniae versus anaerobes. Clin Infect Dis. 2005;40:915-922.Bartlett JG. Anaerobic bacterial infections of the lung and pleural space. Clin Infect Dis. 1993;16(suppl 4):S248-S255.Hirshberg B, Sklair-Levi M, Nir-Paz R, et al. Factors predicting mortality of patients with lung abscess. Chest. 1999;115:746-750.Allewelt M, Schuler P, Bolcskei PL, et al; Study Group on Aspiration Pneumonia. Ampicillin + sulbactam vs clindamycin +/- cephalosporin for the treatment of aspiration pneumonia and primary lung abscess. Clin Microbiol Infect. 2004;10:163-170.http://clinicalcenter.nih.gov/ccmd/cctrcs/pdf_docs/Bronchial%20Hygiene/01-ChestPhysiotherapy.pdf ( 2014-10-12)

Click icon to add picture