Lunch ME Lecture ariatric Surgical Patient are - ACOFP
15
Lunch CME Lecture Bariatric Surgical Paent Care Robert F. Kushner, MD
Transcript of Lunch ME Lecture ariatric Surgical Patient are - ACOFP

Lunch CME Lecture Bariatric Surgical Patient Care
Robert F. Kushner, MD


8/6/2014
1
Bariatric Surgery Robert Kushner, MD
Professor of Medicine
Northwestern University Feinberg School of Medicine
Outline
• Prevalence, health implications and cost of severe obesity
• Clinical decision making in obesity care
• Bariatric surgery procedures
• Effectiveness and risks
• Nutritional complications and management
Classification BMI (kg/m2) Risk
Underweight <18.5 Increased Normal 18.5–24.9 Normal Overweight 25.0–29.9 Increased Obese I 30.0–34.9 High II 35.0–39.9 Very high III 40 Extremely high Additional risks:
• Large waist circumference (men >40 in; women >35 in)
• Poor aerobic fitness
• Specific races and ethnic groups
BMI-Associated Disease Risk
Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight
and Obesity in Adults—The Evidence Report. Obes Res 1998;6(suppl 2).

8/6/2014
2
Trends in
Obesity and Overweight
among US Adults, 1960-2010
Obesity and Overweight Prevalence
Fryar C, et al. http://www.cdc.gov/nchs/data/hestat/obesity_adult_09_10/obesity_adult_09_10.pdf. Accessed February 19, 2014. Flegal KM, et al. JAMA. 2012;307(5):491-497.
Prevalence of
Obesity and Overweight
in US Adults, 2009-2010
20.4%
33.3%
30.8%
6.3%
9.2%
Overweight (BMI ≥25.0-29.9)
Normal / Underweight (BMI <25.0)
Obese Class 1 (BMI ≥30.0-34.9)
Obese Class 2 (BMI <≥35.0-39.9)
Obese Class 3 (BMI ≥40.0)
40
20
0
1960- 1962
Pre
vale
nce
(%)
30
10
Obese (BMI ≥30.0 kg/m2)
Obese Class 3 (BMI ≥40.0 kg/m2)
Overweight (BMI ≥25.0-29.9 kg/m2)
25
5
35
15
1971- 1974
1976- 1980
1988- 1994
2001- 2002
2005- 2006
2009- 2010
7.3
18
6.1
0
2
4
6
8
10
12
14
16
18
20
Whitewomen
Black women Hispanicwomen
5.8 7.6
4.1
02468
101214161820
White men Black men Hispanicmen
Prevalence of Extreme Obesity
(BMI ≥ 40) by Gender and Ethnicity
Men Women
Flegal K, et al. JAMA 2012;307:491-7.
The Impact of Obesity on Health
Obesity burden largely driven by
increased risk of • Cardiovascular
diseases • Type 2 diabetes
• Certain cancers • Musculoskeletal
pain
Centers for Disease Control and Prevention. http://www.cdc.gov/VitalSigns/AdultObesity/Risk-large. html#Complications. Accessed February 19, 2014. Singh-Manoux A, et al. Neurology. 2012;79(8):755-762. Guh DP, et al. BMC Public Health. 2009;9:88. Wang YC, et al. Lancet. 2011;378(9783):815-825.
Sleep apnea
Lung disease
Asthma Pulmonary blood clots
Liver disease
Fatty liver Cirrhosis
Gallstones
Urinary
incontinence
Venous insufficiency
Inflamed veins, often with blood clots
Peripheral edema
Stroke Cognitive decline
Chronic back pain
Infertility
Arthritis
Gout
Cancer Musculoskeletal pain
Diabetes
Heart disease
Abnormal lipid profiles
High blood pressure

8/6/2014
3
Additional Yearly per Capita Healthcare and Productivity Costs Due to Obesity among
Full-Time US Employees ($2006)
All values significant (P<.05) compared to normal-weight workers. Finkelstein EA. J Occup Environ Med. 2010;52(10):971-976.
0
$2524
$4112
$7092
Ad
dit
ion
al Y
earl
y p
er C
apit
a C
ost
s
abo
ve N
orm
al-W
eigh
t Wo
rker
s ($
)
Obese Class 2 (BMI ≥35-39.9)
Obese Class 3 (BMI ≥40)
Obese Class 1 (BMI ≥30-34.9)
Women
0
$1143
$2491
8,000
6,000
4,000
3,000
2,000
1,000
7,000
5,000
Obese Class 2 (BMI ≥35-39.9)
Obese Class 3 (BMI ≥40)
Obese Class 1 (BMI ≥30-34.9)
Men
$6087
8,000
6,000
4,000
3,000
2,000
1,000
7,000
5,000
Absenteeism
Healthcare
Presenteeism
Obesity Treatment Pyramid
Surgery
Pharmacotherapy
Lifestyle Modification
Diet Physical Activity
BM
I
Co
-mo
rbid
itie
s
A Guide to Selecting Treatment
Treatment
BMI category
25-26.9 27-29.9 30-34.9 35-39.9 ≥40
Diet, physical activity,
and behavior therapy
Pharmacotherapy
Surgery
With
co-morbidity
With
co-morbidity
With
co-morbidity
+ + + +
+
+
+ +
The Practical Guide. 2000

8/6/2014
4
Factor Criteria
Weight (adults) BMI ≥ 40 kg/m2 with no comorbidities BMI ≥ 35 kg/m2 with obesity-associated comorbidity
Weight loss history Failure of previous nonsurgical attempts at weight reduction, including nonprofessional programs (e.g., Weight Watchers, Jenny Craig)
Commitment Expectation that patient will adhere to postoperative care; follow-up visits with physician(s) and team members; recommended medical management, including the use of dietary supplements; instructions regarding any recommended procedures or tests
Exclusion Reversible endocrine or other disorders that can cause obesity; current drug or alcohol abuse Uncontrolled, severe psychiatric illness Lack of comprehension of risks, benefits, expected outcomes, alternatives, and lifestyle changes required with bariatric surgery
Selection Criteria for Bariatric Surgery AACE/TOS/ASMBS Guidelines
Mechanick JI, et al. Endocr Pract. 2008;14 Suppl 1:1-83.
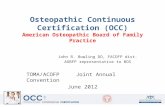
Efficacy and safety of currently available treatments
Lifestyle1 Gastric Band3
Gastric Bypass3
0% 5% 10% 15% 20% 25% 30% 35% Weight Loss
1. Jensen et al., Circulation. Published Online Nov 12, 2013. 2. Courcoulas AP et al. JAMA, November 2013 3. LABS consortium. N Engl J Med 2009;361:445-54. 4. Colman et al. N Engl J Med 2012; 367:1577-1579.
Meds + Lifestyle4
Weight loss at 3 years2 16% for gastric band
33% for bypass2
Medical Care Reducing perioperative risk
• Screen for Obstructive sleep apnea (OSA) • Polysomnogram and CPAP/BiPAP if indicated
• Deep vein thrombosis/pulmonary embolism • Preoperative DVT/PE prophylaxis
• Blood glucose control in diabetes
• Smoking cessation
• Screen for Coronary artery disease • Cardiac stress testing

8/6/2014
5
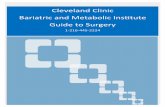
Bariatric Surgery Procedures
Laparoscopic Adjustable Gastric Band (LAGB)
Band placed at fundus is adjustable by way of its connection to a reservoir that is implanted under the skin. Injection or removal of saline into the reservoir tightens or loosens the band’s internal diameter
Roux-en-Y Gastric Bypass (RYGB) A small proximal gastric pouch is created and connected to the jejunum through a narrow (10 mm) gastrojejunostomy. “Bypass” refers to the exclusion or bypassing of the distal stomach, duodenum, and proximal jejunum.
Laparoscopic Gastric Sleeve (LGS) the stomach is restricted by stapling and dividing it vertically and removing approximately 80% of the greater curvature, leaving a slim ‘banana shaped’ remnant stomach along the lesser curvature.
How does Bariatric Surgery Work? Gut Peptides that Regulate Appetite
Murphy KG, Bloom SR. Nature 2006;444:854-859
Effect of Bariatric “Metabolic” Surgery
LAGB RYGB LGS
Mechanisms
Food intake
Ghrelin
GLP-1
Bile acids
Gut microbiota Unaltered Altered Altered
Gastric emptying
Madsbad S, et al. Lancet Diabetes Endocrinol 2014;2:152-164

8/6/2014
6
Rates of Comorbidity Reduction after Bariatric Surgery
Disease or Symptom % improvement or remission at ≤ 2y
% improvement or remission at 5-7 y
% improvement or remission at 10 y
Diabetes 72% 54% 30%
Hypertension 24% 66% 41%
Hypertriglyceridemia 62% 82% 40%
Hypercholesterolemia 22% 53% 21%
Sleep apnea 94% 66%
Fatty liver disease 84%
Stress urinary incontinence
64% resolved, 92% improved
Depression 50%
Vest AR, et al. Circ 2013;127:945-959
The Swedish Obese Subjects (SOS) study
Sjostrom L, et al. JAMA 2012;307:56-65
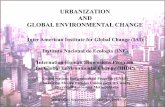
Recovery (Remission) From HTN and DM: SOS Study (Swedish Obese Subjects Study)
13% 21%
36% 34%
11% 19%
72%
0%
20%
40%
60%
80%
100%
2 years P < 0.001
10 years P = 0.001
2 years P < 0.001
10 years P = 0.02
Diabetes Hypertension
Adapted from Sjostrom L, et al. N Engl J Med. 2004;351(26):2683-2693.
21%
Control Surgery
Re
co
ve
ry

8/6/2014
7
Incidence of HTN and DM: SOS Study (Swedish Obese Subjects Study)
24% 29%
7%
24%
49% 41%
1% 0%
10%
20%
30%
40%
50%
2 years P < 0.001
10 years P = 0.0001
2 years P = 0.06
10 years P = 0.13
Diabetes Hypertension
Adapted from Sjostrom L, et al. N Engl J Med. 2004;351(26):2683-2693.
8%
60%
Control Surgery
Inc
ide
nc
e
The Swedish Obese Subjects (SOS) study Reduction in CV Mortality
Sjostrom L, et al. JAMA 2012;307:56-65
Effect of Bariatric Surgery on Type 2 Diabetes
• Increased insulin secretion
• Reduced peripheral insulin resistance
• Increased hepatic insulin sensitivity
• Increased muscle insulin sensitivity

8/6/2014
8
Meta-analysis of Randomized Controlled Trials of Bariatric Surgery Vs. Non-surgical Treatment for
Remission of T2DM
Gloy VL et al. BMJ 2013;347:f5934
Bariatric Surgery versus Intensive Medical Therapy for Diabetes
Schauer et al. NEJM 2014;370:2002-2013
Bariatric Surgery versus Intensive Medical Therapy for Diabetes
Schauer et al. NEJM 2014;370:2002-2013

8/6/2014
9
RYGB Results in Durable Remission of T2DM in Most (but not all) Patients
Retrospective cohort study of 4,434 adults who with T2DM who underwent RYGB Complete remission rates: 37% (yr 1), 63% (yr 3), 68% (yr 5) Lower remission rates predicted by poor preoperative glycemic control (HbA1c ≥6.5%), longer duration of diabetes, and receiving insulin Relapse of diabetes rates: 8% (yr 1), 22% (yr 3), 35% (yr 5). Median time to relapse was 8.3 yrs
Aterburn DE, et al. Obes Surg 2013;23:93-102
Take Home Messages: Bariatric Surgery and T2DM
• Bariatric surgery is more effective in inducing weight loss and remission of T2DM
• Remission of T2DM occurs by two main mechanisms • Increase in hepatic insulin sensitivity due to caloric restriction
(depletion of liver fat) and improved beta-cell function associated with exaggerated postprandial GLP-1 secretion, caused by altered exposure of the distal small intestine to nutrients
• A weight loss induced improvement in peripheral skeletal muscle insulin sensitivity
• 77% of patients achieve a partial or complete remission of T2DM by year 5. Of those who experience a complete remission, 35% have a relapse after a median of 8.3 years
Madsbad S, et al. Lancet Diabetes Endocrinol 2014;2:152-164; Gloy VL, et al. BMJ 2013;347:f5934; Arterburn DE, et al. Obes Surg 2013;23:93-102
The Longitudinal Assessment of Bariatric Surgery (LABS) Study
Lap Band Lap Roux-en-Y Open Roux-en-Y
Number 1198 2975 437
Age (mean) 46 ± 12.5 43.6 ± 11 45.9 ± 10.7
BMI (median) 44.1 46.9 50.9
Death in 30 days 0 6 (0.2) 9 (2.1)
DVT 3 (0.3) 12 (0.4) 5 (1.1)
Failure to be
discharged in 30 days 0 13 (0.4) 4 (0.9)
Composite endpoint*
in 30 days 12 (1.0) 143 (4.8) 34 (7.9)
*Composite endpoint: death, DVT or venous thromboembolism,
intervention or failure to be discharged within 30 days
4776 patients in 10 United States Centers 2005-2007
Flum DR, et al. N Engl J Med. 2009;361(5):445-454. Copyright © 2009 Massachusetts Medical Society.

8/6/2014
10
Perioperative Complication Rates for Roux-en-Y Gastric Bypass
Immediate Complications (Post op d 0-<3)
Early Complications (Post op d 3-30)
Late Complications (Usually beyond Post op d 30)
Mild Nausea and vomiting consequences, up to 100%; self resolving impairment in renal function, 2%
Moderate Arrhythmia without hemodynamic instability, 2%; abdominal hemorrhage or anemia without a clear source, requiring blood transfusion, 5%
Wound infection, 3%; pneumonia, 4%; nausea and vomiting requiring inpatient admission for IV repletion, 8%
Malnutrition of vitamins or minerals, up to 50%; dumping syndrome, up to 75% but clinically significant in <5%; gallstones, 2%; anastomotic ulcer, 8%; anastomotic stricture, 7%; stomal stenosis, 5%
Severe Reoperation or abdominal hemorrhage, 2%; reoperation for any reason, 6%; MI, 0.5%; unstable arrhythmia or cardiac arrest<1%
Pulmonary embolus, respiratory failure, or other potentially fatal medical complications, 0.5%
Herniation or small bowel obstruction, 4%
General overall risk of mortality to postoperative day 30, =0.3%
Vest AR, et al. Circ 2013;127:945-957
Anastomotic Ulcer
Anastomotic ulcers occur in 3-
20% of patients after RYGB
Usual presentation is epigastric
pain, but nausea and/or vomiting
may accompany pain or be the
sole presenting symptom(s)
Diagnosed via EGD
Ulcers on jejunal side (marginal
ulcers) require careful endoscopic
examination to detect
Anastomotic Stricture
Anastomotic strictures occur in 10% of
patients after RYGB
Usual presentation is vomiting or early
satiety with or without vomiting, but
abdominal pain may also present
Diagnosed via EGD
Stoma diameter usually greater than 1cm
when created
Stricture arbitrarily defined as inability to
pass standard 9mm diagnostic
gastroscope across pouch-enteric
anastomosis without resistance

8/6/2014
11
Meal Progression after Bariatric Surgery
Diet Stage Begin Fluids/food
Stage I Post op days 1 and 2 Clear liquids
Stage II Post op day 3 (discharge) Clear + protein-rich full liquids
Stage III Post op days 1-14 Soft, moist foods
Stage III, week 2 4 – 5 weeks post op Add well-cooked, soft vegetables + peeled fruit
Stage IV As hunger increases and more food is tolerated
Healthy solid food diet
AACE/TOS/ASMBS Guidelines. Obesity, 2009
Dumping Syndrome • Cause
• Carbohydrate load or liquids w/meals causing rapid dumping from pouch into jejunum
• enteroglucagon release
• Symptoms
• 10 to 15 minutes after eating: flushing, nausea, cramping,
• May have diarrhea, warm, dizzy, weak, faint, pulse, and cold sweat
Jejunum -
Duodenum
bypassed;
absorptive
area for sugar
Dumping Syndrome
>25 grams or more per serving may cause dumping in some people
• Teach slow, mindful eating
• Recommend not drinking with meals

8/6/2014
12
Clinical Presentation of Nutritional Deficiencies
Presentation Nutrient Deficiency
Anemia Iron, folate, vitamin B12, copper,
Neurological abnormality Thiamine, vitamin B12, copper, vitamin E, vitamin B6
Metabolic bone disease Vitamin D, calcium
Protein-calorie malnutrition Protein, calories
Risk of Selected Nutritional Deficiencies Resulting from Bariatric Surgery
Nutrient LAGB LGS RYGB BPD/DS
Macronutrients √√√
Thiaminea √ √ √ √
Ironb √√ √√ √
Vitamin B12 √√√ √√√ √
Vitamin D √√ √√√ √√√
Vitamin A √ √√
LAGB = Laparoscopic adjustable gastric banding; LGS = laparoscopic gastric sleeve RYGB = Roux-en-Y gastric bypass; BPD/DS = biliopancreatic bypass/duodenal switch awith persistent vomiting; bincreased with menstruation
Bariatric Surgery and Micronutrient Deficiencies
• Micronutrient deficiencies are predictable based on the surgically altered anatomy and the patient’s medical history.
• Micronutrient deficiencies are preventable by routine monitoring and prophylactic supplementation.
• All patients who undergo a malabsorptive bariatric weight loss surgery need to take vitamin and mineral supplements for their entire life.

8/6/2014
13
• Routine • CBC
• Chemistry profile
• Liver function tests
• Lipid panel
• HbA1c
• Micronutrients • Iron, TIBC, Saturation
• Ferritin
• Folate
• Vitamin B12
• 25 (OH) vitamin D
• iPTH
• DEXA scan
• *Cu, Zn, vitamin A
Nutritional Monitoring for the Bariatric Surgical Patient
*if suspect deficiency
Mechanick JI, et al. Clinical Guidelines for Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient – 2013 Update. Obesity 2013;21(S1):S1-S27
Routine Vitamin & Mineral Supplementation for RYGB Patients
a Depending on dietary calcium intake b For most menstruating women
Supplement Dosage
Multivitamin-mineral or prenatal
Calcium citrate with vitamin Da
Elemental ironb
Vitamin B12
1-2 daily
1,200-2,000 mg/day + 3000 U/day
40-65 mg/day
≥500 µg/day orally
or 1,000 µg/mo intramuscularly
Or 3,000 µg every 6 mo intramuscularly
or 500 µg every week intranasally
Mechanick JI, et al. Clinical Guidelines for Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Baiatric Surgery Patient – 2013 Update. Obesity 2013;21(S1):S1-S27
Take home Messages
• The prevalence of severe class III obesity (BMI ≥ 40) is increasing and is costly
• Bariatric surgery is indicated for a BMI ≥ 35 with co-morbidities or BMI ≥ 40, along with other weight and history criteria
• The 3 most commonly performed procedures are: LAGB, RYGB and SG
• The mechanism of action of bariatric surgery procedures are thought to be primarily metabolic
• Remission or improvement rates are seen for diabetes, hypertension, dyslipidemia, OSA and depression; and reduced mortality
• Most common long-term complications are nutritional – iron, calcium, vitamin B12, vitamin D