LSU HEALTH CARE SERVICES DIVISION QUARTERLY HEALTH EFFECTIVENESS MEETING BATON ROUGE, SEPTEMBER 18,...
50
LSU HEALTH CARE SERVICES DIVISION QUARTERLY HEALTH EFFECTIVENESS MEETING BATON ROUGE, SEPTEMBER 18, 2007
-
Upload
jaren-burgamy -
Category
Documents
-
view
215 -
download
1
Transcript of LSU HEALTH CARE SERVICES DIVISION QUARTERLY HEALTH EFFECTIVENESS MEETING BATON ROUGE, SEPTEMBER 18,...

LSU HEALTH CARE SERVICES DIVISIONQUARTERLY HEALTH EFFECTIVENESS MEETING
BATON ROUGE, SEPTEMBER 18, 2007

THOUGHTS FROM
OKLAHOMA
Michael Lapolla, College of Public HealthJohn Gaudet, Bedlam Alliance
September 18, 2007
ABOUT MEDICAL HOMES - AND MORE

MIKE LAPOLLA
OUR THOUGHTSFROM HIGH ALTITUDES

OUR HEALTH CARE “DUST BOWL”

CAUSES
CHALLENGES
COMMUNITY RESPONSE

THECAUSES

MEDICARE AND MEDICAIDResponded well concerning physician production – but poorly concerning Medicaid administration and policy. The state (and the nation) was still learning how to deal with federal programs and how to maximize patient care reimbursements. Emphasis on larger enrollments and smaller payments. Abuse led to PPS and DRG in the 1980’s.
1960’s

OIL BOOM MASKS PROBLEMSState DHS (next slide) suffocates all other health policy players. Dedicated state sales tax. State Health Department rendered inert – university (OU) “teaching hospital” a shambles – the concept of a dynamic Health Sciences Center is still a vision. About 170 county commissioners sent to federal prison (there are only 231 in the state), Oil boom is underway full-speed – things “ain’t too bad”.
1970’s

+
HUEY LONG J. EDGAR HOOVER
OIL BUST EXPOSES PROBLEMSThe state is both broke and shocked. LER dies; Medicaid and DHS left disarray with no institutional memory. Academic Health Center Teaching Hospital (now under DHS) “beyond repair”. Any federal (matching) Medicaid opportunities, such as DSH, are foregone. Health policy issues just emerging. Still in generally blissful ignorance - cannot see storm clouds.
1980’s
EMERGING FROM DARKNESSEconomy recovers. Legislature is starting to change and turnover (term limits/no new taxes). Good ole boys on the way out. State creates a Health Care Authority. Privatizes the only public hospital in the state. Begins to take advantage of Medicaid – but it is way too late. The “uninsured” are noticed – the concept of a “safety net” emerges. Starting to realize we have big problems.
1990’s

SEEING THE LIGHTRealized that we missed the boat on Medicaid – “too bad – so sad”. Medicaid DSH frozen. Some states are big winners (Louisiana) – some states are still at the starting gate (Oklahoma). Communities cannot solely rely upon the state and feds. Now what?
Let’s review the past 15 years.
NOW

STATE OF OKLAHOMAMissed FQHC opportunitiesMissed Medicaid DSH opportunitiesIgnored State of State Health warningsDismissed United Health rankings
Health Care Authority rises from chaosPrivatized state’s only public hospital
1992-2007

TULSA COMMUNITYNew Medical School identity and leadershipStart of the Bedlam AlliancePhilanthropy awakened and enablingGood-to-Great philosophy engagedRegional Strategic Health PlanCommunity respondingSchool of Community Medicine
2002-2007

THECHALLENGES
CAUSED BY GENERATIONS OF NEGLECT

OKLAHOMA AND NATIONAL
18.1
19.9
20.1
18.6
18.2
22.0
23.6
17.8
19.2
17.0
17.7
18.3
16.4
18.9
18.3
17.3
20.4
19.9
18.5
12.9
13.4
13.6
13.9
14.1
15.0
15.315.2
15.4
15.6
16.1
16.3
14.5
14.2
14.6
15.2
15.615.7
15.9
10
15
20
25
1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
25%
20%
15%
10%
OKLAHOMA UNINSURED
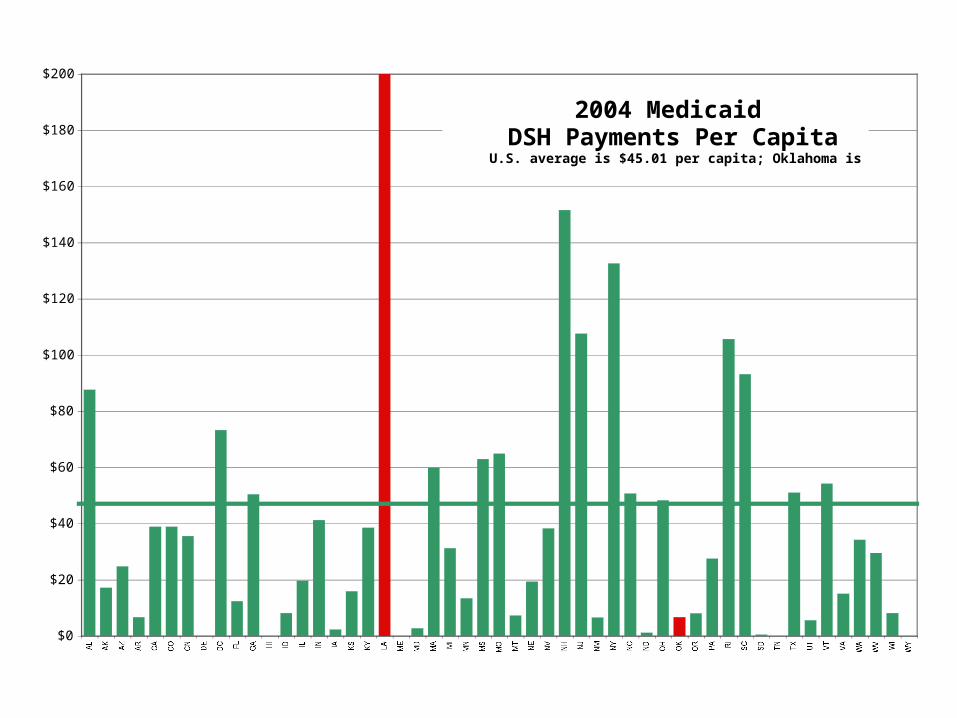
$0
$20
$40
$60
$80
$100
$120
$140
$160
$180
$200
AL AK AZ AR CA CO CN DE DC FL GA HI ID IL IN IA KS KY LA ME MD MA MI MN MS MO MT NE NV NH NJ NM NY NC ND OH OK OR PA RI SC SD TN TX UT VT VA WA WV WI WY
2004 MedicaidDSH Payments Per Capita
U.S. average is $45.01 per capita; Oklahoma is $6.67

LA OK LA OK
Hospital $ 930m $ 407m $ 205 $ 117
DSH $ 911m $ 23m $ 201 $ 7
Nursing Home $ 594m $ 463m $ 131 $ 133
Managed Care $ 0 $ 171m $ 0 $ 49
Drugs $ 945m $ 417m $ 208 $ 120
FQHC $ 9m $ 5m $ 2 $ 1
Indian $ 6m $ 62m $ 1 $ 18
Other $ 1,700m $ 1,000m $ 372 $ 294
TOTAL $ 5.1B $ 2.6B $ 1,120 $ 737
MEDICAID 2004
PER CAPITATOTAL DOLLARS

Metropolitan Safety NetsPublicHospital
Comp Med Sch
MedicaidDSH
FocusedHospital
State FQHC
Jacksonville University Yes Yes Yes No Jacksonville
Rochester University Yes Yes Yes Yes Rochester
Grand Rapids No No Yes Yes No Grand Rapids
Oklahoma City University Yes Yes Yes No Oklahoma City
Louisville University Yes Yes Yes Yes Louisville
Richmond District Yes Yes Yes Yes Richmond
Greenville District Yes Yes Yes No Greenville
Dayton No Yes Yes Yes No Dayton
Fresno County No Yes Yes Yes Fresno
Birmingham State Yes Yes Yes Yes Birmingham
Honolulu Public Yes Alternate Yes Yes Honolulu
Albany University Yes Yes Yes Yes Albany
Tucson University Yes Yes Yes No Tucson
Tulsa No No No No No Tulsa
Syracuse State Yes Yes Yes Yes Syracuse
Omaha University Yes Yes Yes No Omaha
“Tulsa (and Wichita) are the only two major metro areas (of the 80 largest) in the nation lacking all traditional infrastructure, financing mechanisms and organizational tools for providing coordinated and focused safety net services. Both have community-based med schools.”
OU College of Public Health study for the Oklahoma Secretary of Health, April 2005

350,000
300,000
250,000
200,000
150,000
100,000
50,000
0
346,976
130,494
40,000 Primary90,000 Specialty
31,199
46,320
101,661
37,300
SE
RV
ED
BY
SA
FE
TY
NE
TU
NS
ER
VE
D
ER
Oth
erC
linic
sM
ajor
Clin
ics
Fre
eC
linic
s
TU
LS
A M
ET
RO

4444
40
4546
44
4140
4141
383939
3231
3030
0
5
10
15
20
25
30
35
40
45
50
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
OKLAHOMAUnited Health Foundation
America’s Health Rankings – 2006

HEART DISEASE

MENTAL HEALTH NEEDS

National Average
1,029
1,011
1979AGE ADJUSTED DEATH RATES
THE TEN STATES WITH THE HIGHEST RATES Source: Centers for Disease Control. Graphic: OU College of Public Health

National Average
946
801
2004AGE ADJUSTED DEATH RATES
THE TEN STATES WITH THE HIGHEST RATES Source: Centers for Disease Control. Graphic: OU College of Public Health

OklahomaA State of Health?
“We are the ONLY state where our age-adjusted death rates became WORSE through the 1990s and into this century.”
“If we had the same adjusted death rate as the nation, we would have about 3,700 fewer people dying each year.”
Oklahoma State Board of Health “2006 State of the State’s Health” Graphic: University of Oklahoma College of Public Health. Data Source: U.S. Centers for Disease Control and Prevention
AGE ADJUSTED DEATH RATE
U.S
OK

700
800
900
1,000
1,100
1,200
1979 1984 1989 1994 1999 2004
LA
US
OKOKLAHOMAFROM THE NATIONAL AVERAGE TO LOUISIANA
AGE ADJUSTED DEATH RATES

While the death rate of most U.S. residents is declining, that of Tulsans is not – and the trend is going in the wrong directionUnited States
Tulsa County
1980 1990 2000
1,000
950
900
850
800
1,100
AIMING HIGHERThe Commonwealth Fund
Results from a State Scorecard on Health System Performance

OK
COMMONWEALTH FUND State Scorecard Summary of Health System Performance

OUR EMBARASSMENT
“When you are 50th – how do you defend the status quo?”
50th

COMMUNITYRESPONSES

KIM HOLLANDOKLAHOMA INSURANCE COMMISSIONER
INITIATIVES FOR OKLAHOMA

AN OKLAHOMA CHATCHOOSING HEALTHPLAN ALL TOGETHER
© University of Michigan; courtesy of Sacramento Healthcare Decisions (SHD)

Oklahoma Employer/EmployeePartnership for Insurance Coverage
PREMIUM SHARING15% EMPLOYEE – 25% EMPLOYER – 20% STATE – 40% FEDERAL


HIDC

HEALTH FOR OKLAHOMANS INFORMATION FOR POLICYMAKERSOHI
OKLAHOMA HEALTH INSTITUTE

GERRY CLANCY, MDPRESIDENT, OU-TULSA
INITIATIVES FOR TULSA
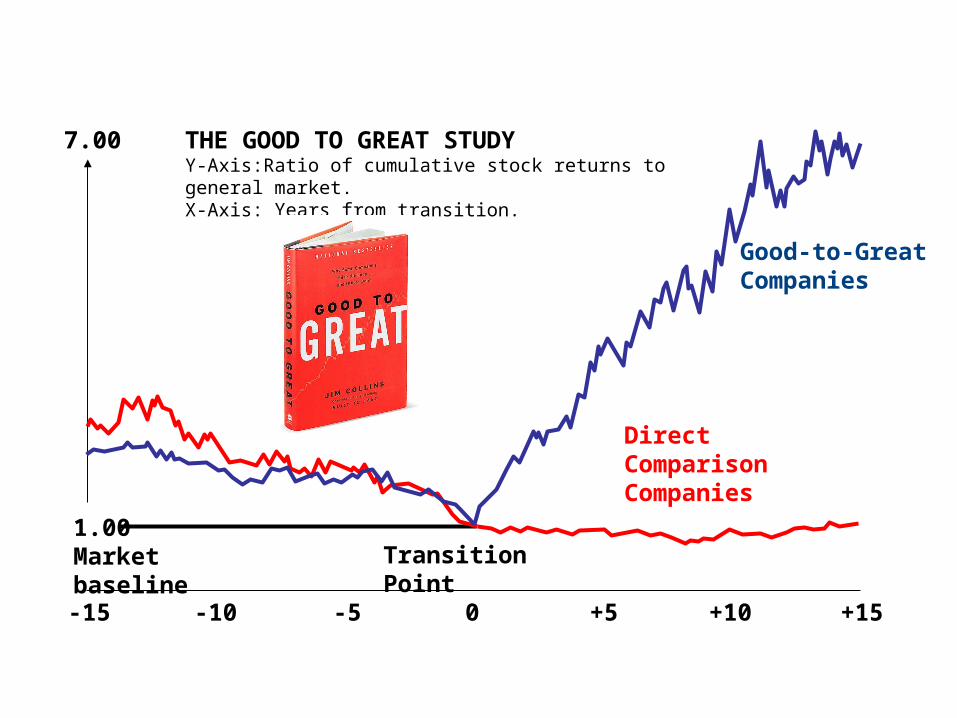
THE GOOD TO GREAT STUDYY-Axis:Ratio of cumulative stock returns to general market.X-Axis: Years from transition.
-15 -10 -5 0 +5 +10 +15
Good-to-GreatCompanies
DirectComparisonCompanies
1.00Market baseline Transition Point
7.00

This begs the question, “what could the University of Oklahoma College of Medicine, Tulsa do to become a great medical school?”
One answer is to lead a long-term strategy to successfully improve the health status of the entire Tulsa metropolitan region.
COLLEGE OFMEDICINE-TULSA
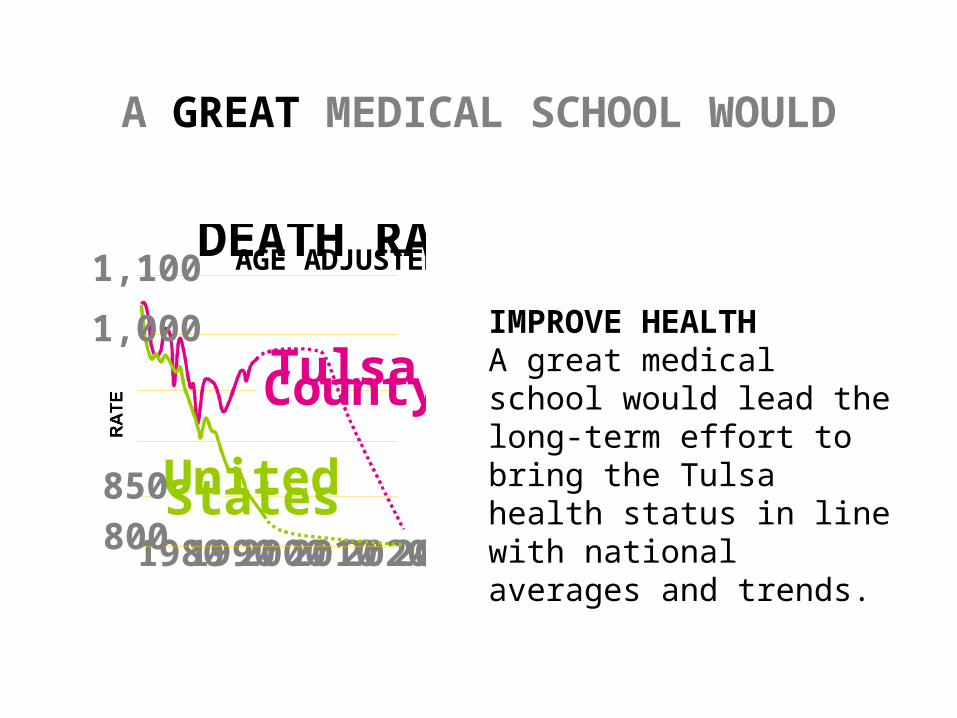
TulsaCounty
198019902000201020202030
DEATH RATES AGE ADJUSTED
UnitedStates800
1,100
RATE
1,000
850
A GREAT MEDICAL SCHOOL WOULD
IMPROVE HEALTHA great medical school would lead the long-term effort to bring the Tulsa health status in line with national averages and trends.
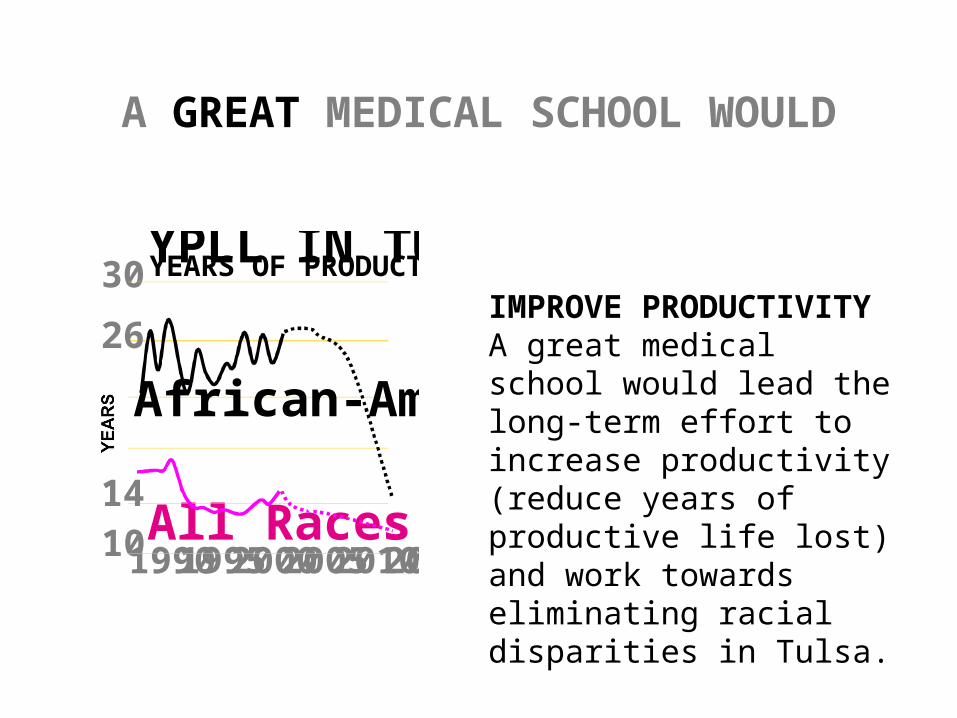
All Races19901995200020052010201510
30YPLL IN TULSA COUNTY YEARS OF PRODUCTIVE LIFE LOST PER DEATH
YEARSAfrican-American
26
14
IMPROVE PRODUCTIVITYA great medical school would lead the long-term effort to increase productivity (reduce years of productive life lost) and work towards eliminating racial disparities in Tulsa.
A GREAT MEDICAL SCHOOL WOULD

925989 995
1,486
HIGHESTMID-HIGHMID-LOWLOWESTHOUSEHOLD INCOMES
AGE-ADJUSTED DEATH RATES
OFFSET POVERTY
A great medical school would lead the effort to bring better health status to those in poverty, especially children.
A GREAT MEDICAL SCHOOL WOULD

CONTINUUM OF HEALTH SERVICES
Prenatal CareLive Birth
PrimaryDisease
PreventionTreatment of
Acute Disease
TertiaryDisease
PreventionRehabilitative
Care
End of LifeHealthPromotion
Diagnosisof Disease
SecondaryDisease
Prevention
Treatment ofChronic Illness
Long TermCare
PalliativeCare
INSTITUTIONSHOSPITALS - NURSING HOMES
REHABILTATION CENTERS
PRIMARY CARESAFETY NET CLINICS & PROVIDERS
HEALTHPLEXSPECIALTY OUTPATIENT SERVICE
BY REFERRAL

CREATING THE NATION’S FIRST
SCHOOL OFCOMMUNITY MEDICINEA PLATFORM TO IMPROVE THE HEALTH STATUS OF THE TULSA REGION
GERRY CLANCY, MD, PRESIDENT, OU-TULSAMICHAEL LAPOLLA, OU COLLEGE OF PUBLIC HEALTH

… will blend the education and practice of public health with medical education to produce community-oriented and jointly credentialed physicians who will influence personal and population health.
SCHOOL OFCOMMUNITY MEDICINE

COMMUNITY PHILANTHROPY


NOW - FROM THE TREETOPS
THE BEDLAM ALLIANCEJohn Gaudet