Lower Extremity Fxnl Anatomy SD Dx 2017(1)nevadaosteopathic.org/attachments/article/57/OMM_Lower...
79
Lower Extremity Functional Anatomy and Somatic Dysfunction Eric Toder, DO Dept of OMM Touro University Nevada November 7, 2017
Transcript of Lower Extremity Fxnl Anatomy SD Dx 2017(1)nevadaosteopathic.org/attachments/article/57/OMM_Lower...

Lower ExtremityFunctional Anatomy and Somatic Dysfunction
Eric Toder, DODept of OMM
Touro University NevadaNovember 7, 2017

General Outline
• Landmarks
• Neurological Exam
• Hip, Knee, Tibia, Fibula, Ankle, Foot– Anatomy and ROM
• Lower Extremity Somatic Dysfunction
• Additional Orthopedic Special Tests– for the Hip, Knee, Ankle, Foot
ObjectivesOn a written exam, the student will:
• Identify the application of the following special tests (including the interpretation of a positive test):
- Hip: Straight Leg Test, Patrick (FABERE), Thomas, Ober, Trendelenburg Test
- Knee: Patellar Grind Test, Bulge/Ballottement tests, Apleys and McMurray tests, Anterior/ posterior drawer, and Lachmans test, Varus/ Valgus test
- Ankle: Ankle drawer test
On a written and practical exam, the student will:
• Identify physiologic motion and somatic dysfunction for the following joints :
- Tibia (Femorotibial Joint) – External/Internal Rotation
- Fibular Head (Proximal Tibiofibular Joint) – Anterior/Posterior
- Talus (Tibiotalar Joint) – Anterior/Posterior
- Calcaneus (Talocalcaneal Joint, Subtalar Joint) – Inversion/Eversion
- Cuboid and Navicular – Inversion/Eversion (“dropped”)

Landmarks• Greater Trochanter
• Lateral and Medial Femoral condyles
• Patella
• Popliteal Fossa
• Tibial Tuberosity
• Lateral Fibular Head
• Lateral and Medial Malleolus
• Calcaneus
• Proximal head of the 5th metatarsal
• Navicular

Innervation of the Lower ExtremityThe innervation to the lower extremity
is from spinal cord levels L1-S3Sympathetics to the lower extremity is
from T10-L2
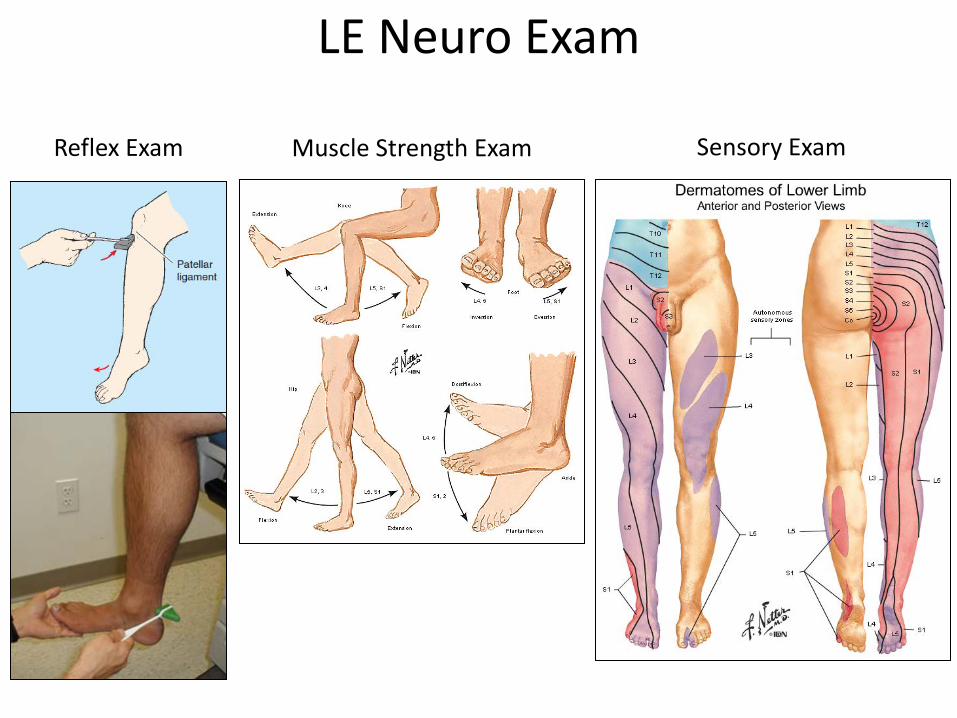
LE Neuro Exam
Sensory ExamMuscle Strength ExamReflex Exam
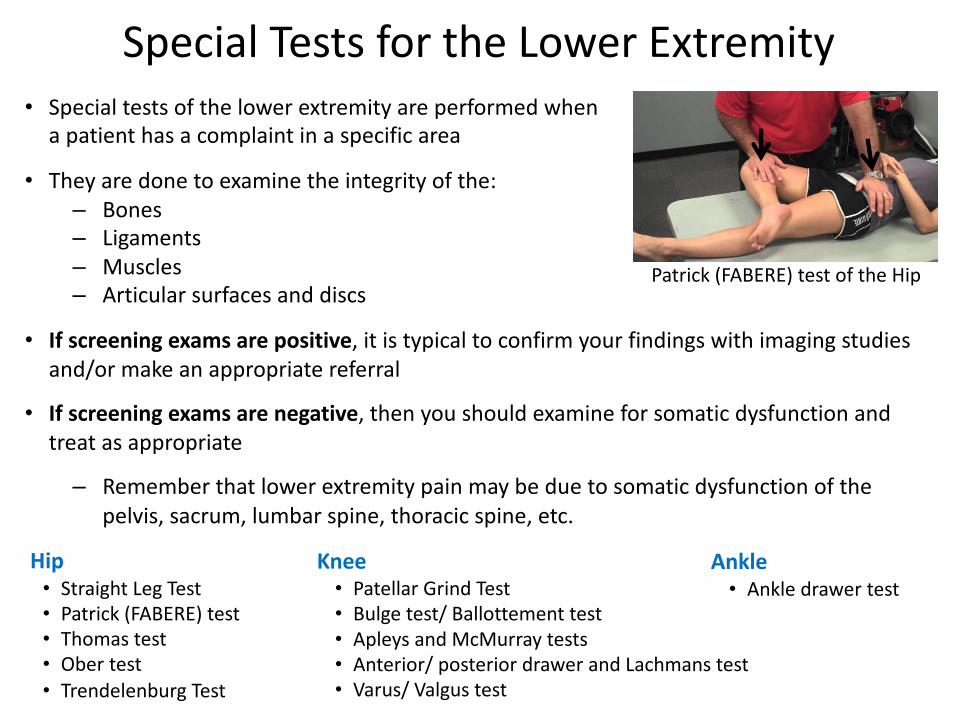
Special Tests for the Lower Extremity• Special tests of the lower extremity are performed when
a patient has a complaint in a specific area
• They are done to examine the integrity of the:– Bones– Ligaments– Muscles– Articular surfaces and discs
• If screening exams are positive, it is typical to confirm your findings with imaging studies and/or make an appropriate referral
• If screening exams are negative, then you should examine for somatic dysfunction and treat as appropriate
– Remember that lower extremity pain may be due to somatic dysfunction of the pelvis, sacrum, lumbar spine, thoracic spine, etc.
Hip• Straight Leg Test• Patrick (FABERE) test• Thomas test• Ober test• Trendelenburg Test
Ankle • Ankle drawer test
Knee• Patellar Grind Test• Bulge test/ Ballottement test• Apleys and McMurray tests• Anterior/ posterior drawer and Lachmans test• Varus/ Valgus test
Patrick (FABERE) test of the Hip

HipAnatomy and ROM

Ball and socket synovial joint
Femoroacetabular Joint(Hip or Os Coxae)
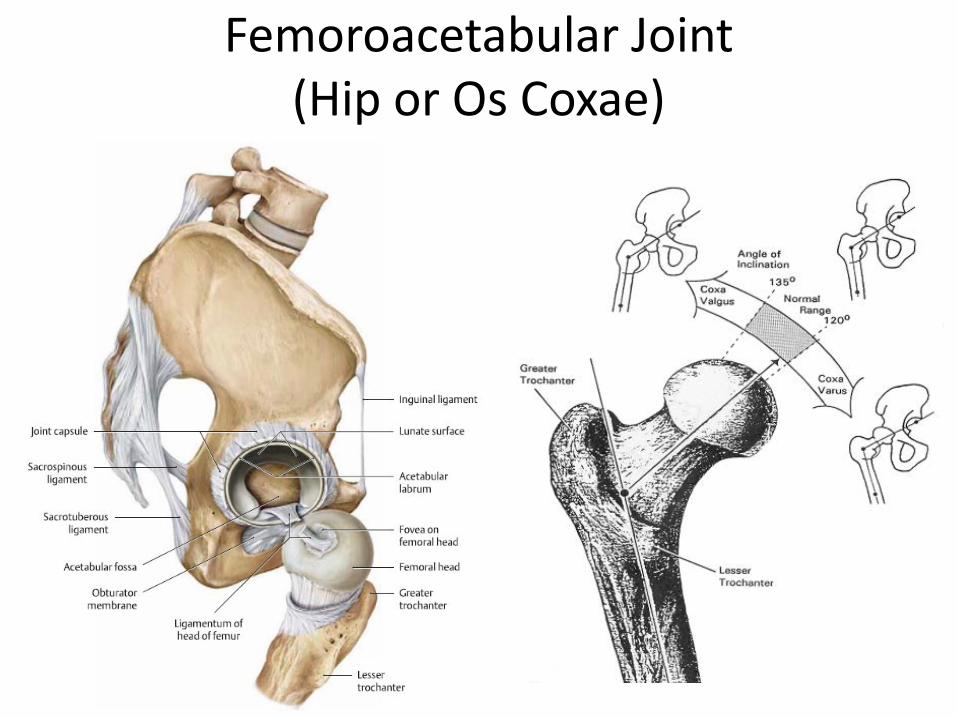
Femoroacetabular Joint(Hip or Os Coxae)
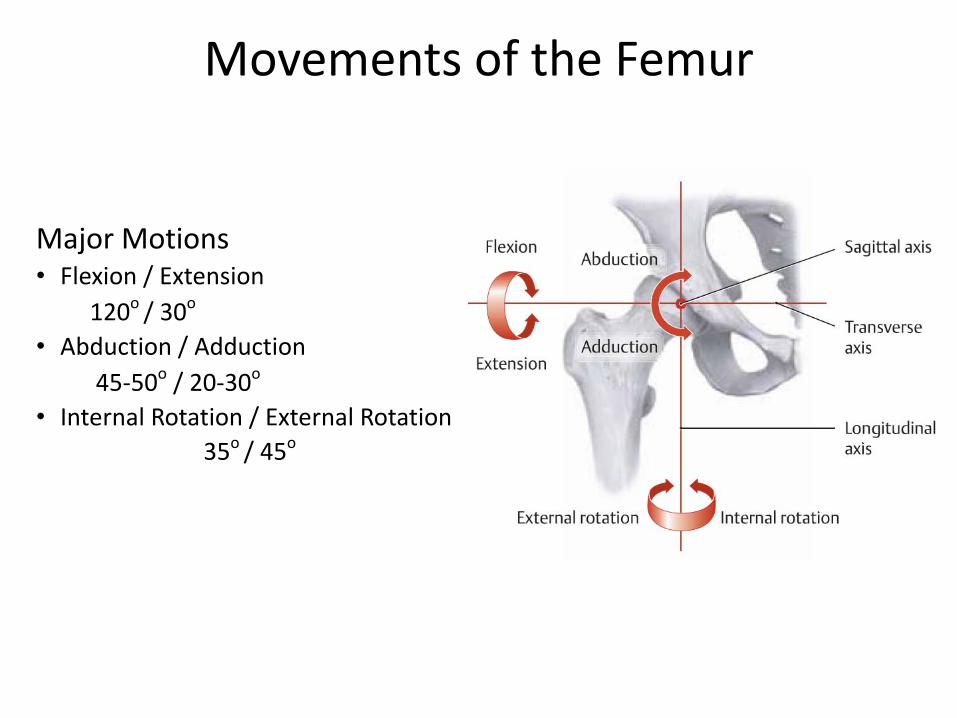
Major Motions• Flexion / Extension
120o / 30o
• Abduction / Adduction45-50o / 20-30o
• Internal Rotation / External Rotation 35o / 45o
Movements of the Femur
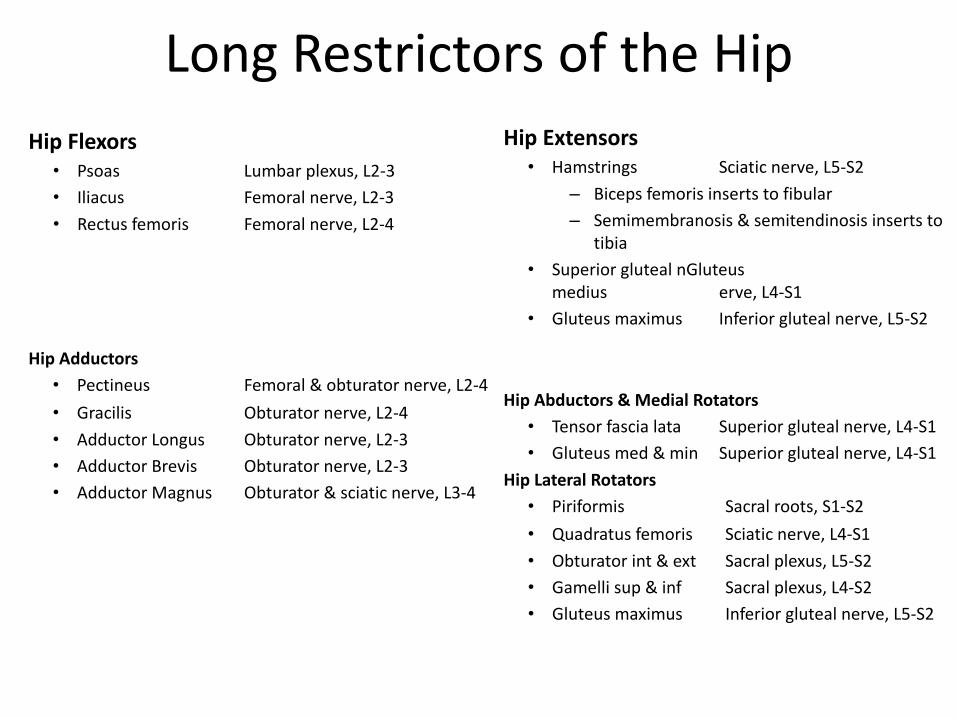
Long Restrictors of the HipHip Flexors
• Psoas Lumbar plexus, L2-3• Iliacus Femoral nerve, L2-3 • Rectus femoris Femoral nerve, L2-4
Hip Adductors• Pectineus Femoral & obturator nerve, L2-4• Gracilis Obturator nerve, L2-4• Adductor Longus Obturator nerve, L2-3• Adductor Brevis Obturator nerve, L2-3• Adductor Magnus Obturator & sciatic nerve, L3-4
Hip Extensors• Hamstrings Sciatic nerve, L5-S2
– Biceps femoris inserts to fibular– Semimembranosis & semitendinosis inserts to
tibia• Superior gluteal nGluteus
medius erve, L4-S1• Gluteus maximus Inferior gluteal nerve, L5-S2
Hip Abductors & Medial Rotators• Tensor fascia lata Superior gluteal nerve, L4-S1• Gluteus med & min Superior gluteal nerve, L4-S1
Hip Lateral Rotators• Piriformis Sacral roots, S1-S2• Quadratus femoris Sciatic nerve, L4-S1• Obturator int & ext Sacral plexus, L5-S2• Gamelli sup & inf Sacral plexus, L4-S2• Gluteus maximus Inferior gluteal nerve, L5-S2
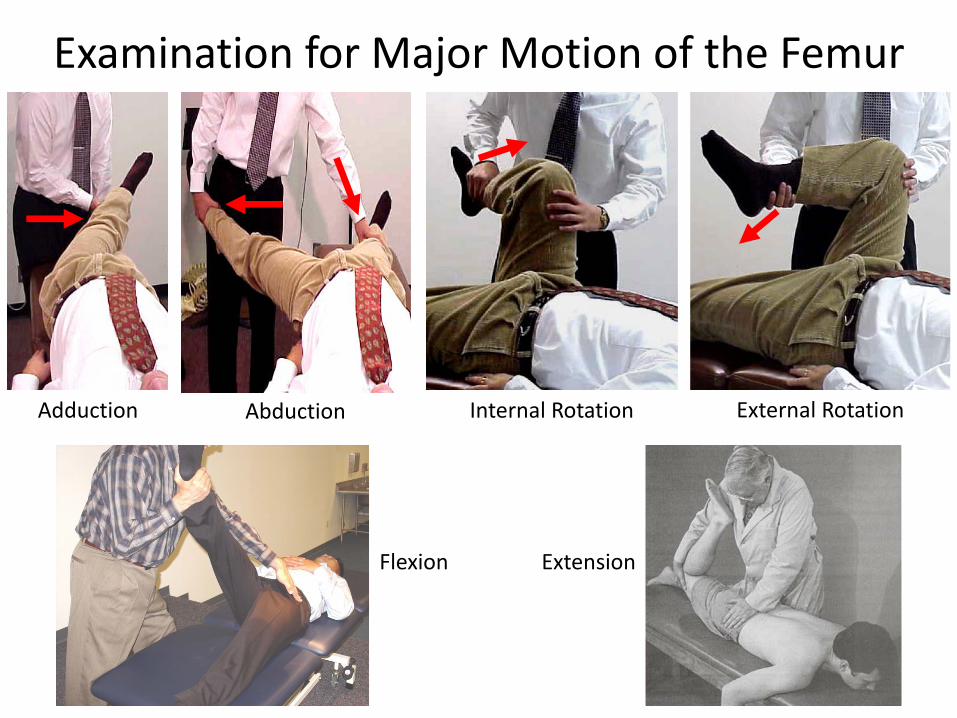
Examination for Major Motion of the Hip Joint• Active range of motion for the hip is often evaluated just by observing the
patient walking and changing position
• Passive range of motion:– Patient supine– Move the lower extremity into:
• Flexion• Abduction• Adduction
– Flex the hip and knee to 90 degrees then move the lower extremity into:• External rotation• Internal rotation
– Patient is prone to test hip extension
Adduction
Examination for Major Motion of the Femur
External RotationInternal RotationAbduction
Flexion Extension
KneeAnatomy and ROM

Femorotibial Joint “Knee or Genu”• Structural
- Femur- Tibia
• Femoral condyles- Medial/lateral
• Tibial plateau- Double condylar, complex synovial articulation- Semilunar cartilages (menisci)
• Multiple ligaments- Cruciate Ligaments (ACL/PCL)- Collateral Ligaments (Medial/Lateral)
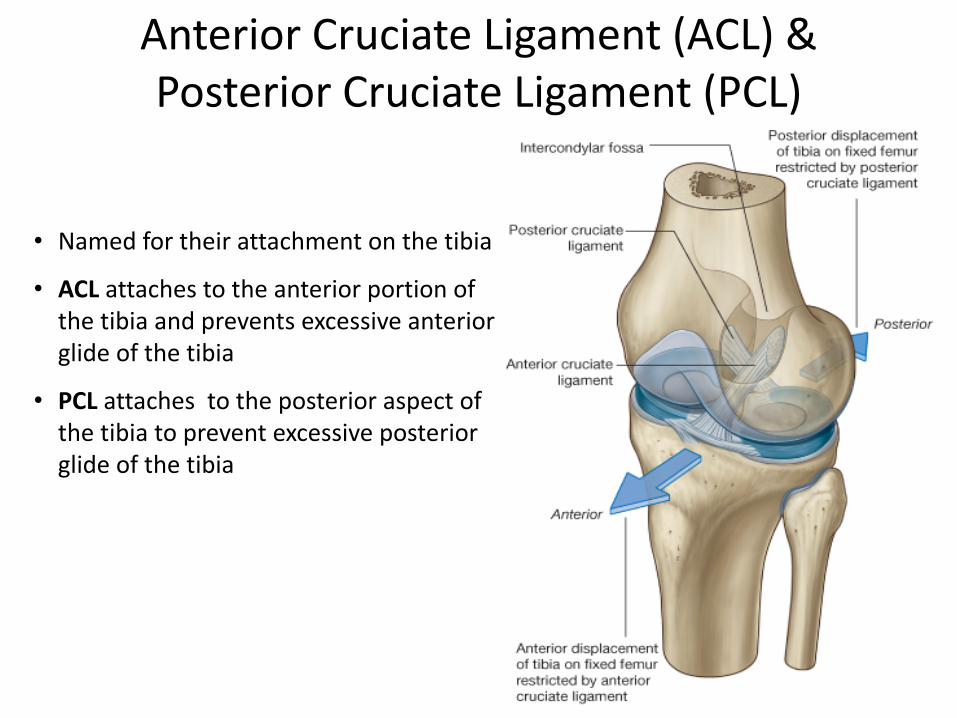
Anterior Cruciate Ligament (ACL) &Posterior Cruciate Ligament (PCL)
• Named for their attachment on the tibia
• ACL attaches to the anterior portion of the tibia and prevents excessive anterior glide of the tibia
• PCL attaches to the posterior aspect of the tibia to prevent excessive posterior glide of the tibia

Femorotibial Motion• Normal knee flexion range is
from 0 to 135 degrees.• Normal knee extension is from
0 to 15 degrees.• During extension movement,
the larger articular surface of the medial joint surface allows for external rotation of the tibia.
• As the knee returns to flexion this results in internal rotation of the tibia
This is called the “screw home” motion of the knee in non-weightbearing. Extension externally rotates tibia on femur
Hoppenfeld, Stanley. Physical Examination of the Spine and Extremities
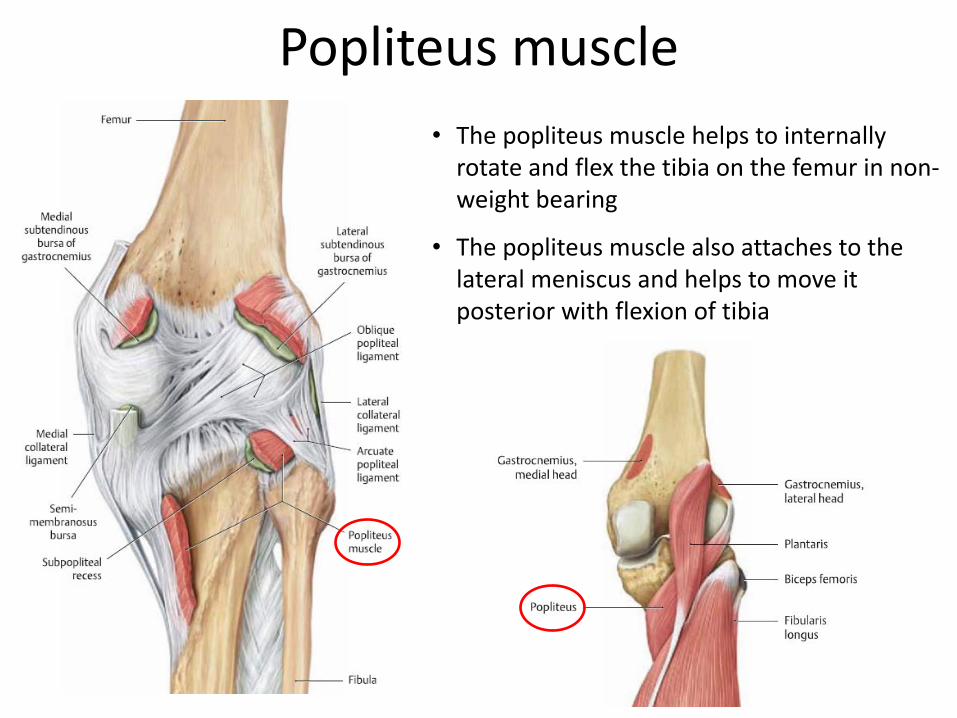
Popliteus muscle • The popliteus muscle helps to internally
rotate and flex the tibia on the femur in non-weight bearing
• The popliteus muscle also attaches to the lateral meniscus and helps to move it posterior with flexion of tibia
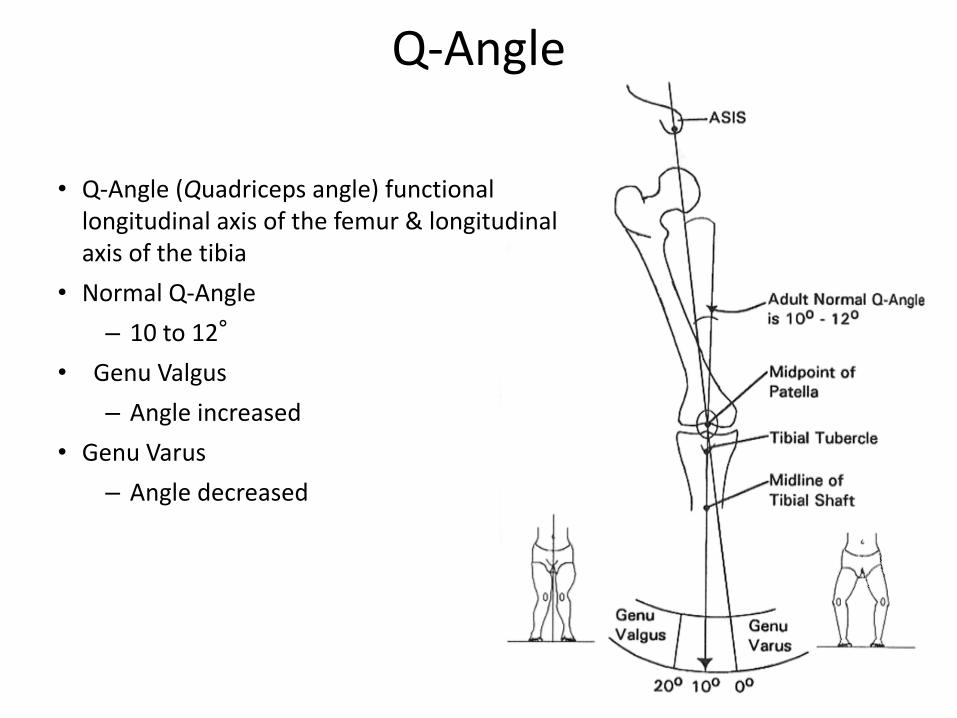
Q-Angle
• Q-Angle (Quadriceps angle) functional longitudinal axis of the femur & longitudinal axis of the tibia
• Normal Q-Angle– 10 to 12°
• Genu Valgus– Angle increased
• Genu Varus– Angle decreased

Muscles of Major Knee MotionKnee Flexors
• Biceps femoris Sciatic nerve, L5-S2• Semimembranosus Sciatic nerve, L5-S2• Semitendinosus Sciatic nerve, L5-S2• Gracilis Obturator nerve, L2-L3• Sartorius Femoral nerve, L2-L3• Gastrocnemius Tibial nerve, S1-S2• Popliteus Tibial nerve, L4-S1• Tensor fascia lata Superior gluteal nerve, L4-L5 (at 45-145 hip flexion)
Knee Extensors• Rectus femoris Femoral nerve, L2-L4• Vastus lateralis Femoral nerve, L2-L4• Vastus medialis Femoral nerve, L2-L4• Vastus intermedius Femoral nerve, L2-L4• Tensor fascia lata Superior gluteal nerve, L4-L5 (at 0-30 hip flexion)
Muscles of Minor Knee MotionInternal rotation of flexed leg (non-weight bearing)
• Popliteus Tibial nerve, L4-L5• Semimembranosus Sciatic nerve, L5-S2• Semitendinosus Sciatic nerve, L5-S2• Sartorius Femoral nerve, L2-L3• Gracilis Obturator nerve, L2-L3
External rotation of flexed leg (non-weight bearing)• Biceps Femoris Sciatic nerve, L5-S2

Tibia & FibulaAnatomy and ROM

Tibia & Fibula – Anatomy
Proximal Tibiofibular Joint– Synovial joint separate from knee
Interosseous Membrane– Fibrous connective tissue between tibia and fibula– Allows sharing of compressive forces & movements – May develop Somatic dysfunction
Distal Tibiofibular Joint– Syndesmosis joint– Allows fibula to move laterally from tibia allowing room
for the talus– Dorsiflexion increases width for talus
FibularHead
Lateral Maleolus
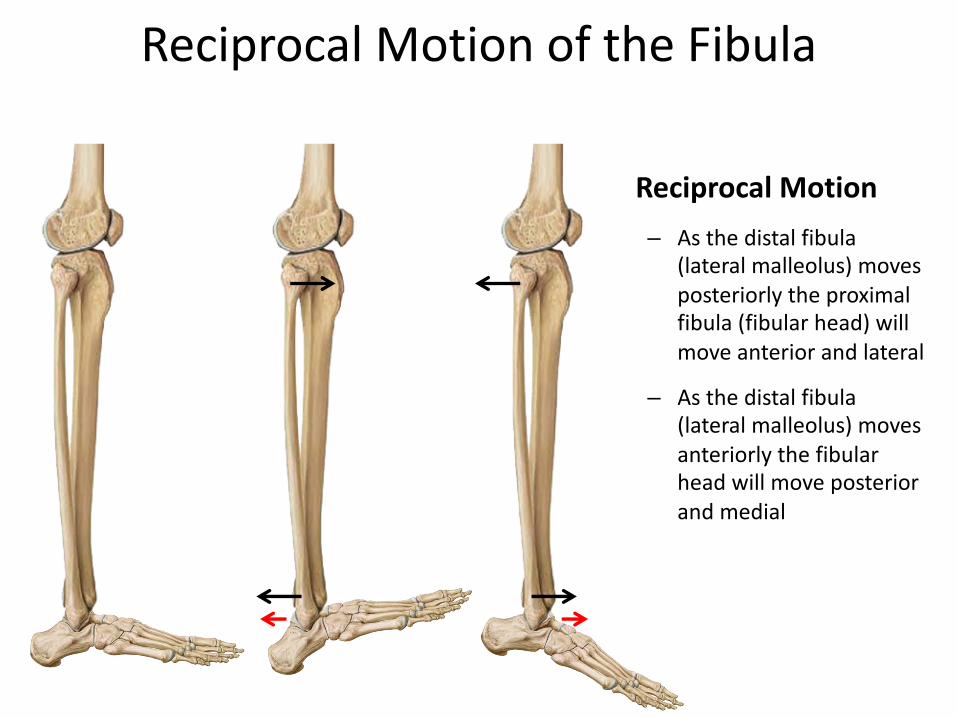
Reciprocal Motion– As the distal fibula
(lateral malleolus) moves posteriorly the proximal fibula (fibular head) will move anterior and lateral
– As the distal fibula (lateral malleolus) moves anteriorly the fibular head will move posterior and medial
Reciprocal Motion of the Fibula

AnkleAnatomy and ROM

Ankle & Foot ROM
• Dorsiflexion: 20°• Plantar flexion: 50°
• Inversion: 5°• Eversion: 5°
• Abduction: 10°• Adduction: 20°

Muscles of Ankle MotionAnkle Dorsiflexors
• Extensor digitorum longus Deep fibular nerve, L4-S1• Extensor hallucis longus Deep fibular nerve, L4-S1• Fibularis tertius Deep fibular nerve, L4-S1• Tibialis anterior Deep fibular nerve, L4-L5
Ankle Plantar Flexors• Fibularis longus & brevis Superficial fibular nerve, L5-S2• Flexor digitorum longus Tibial nerve, S1-S3• Flexor hallucis longus Tibial nerve, S1-S3• Gastrocnemius Tibial nerve, S1-S2• Plantaris Tibial nerve, S1-S2• Soleus Tibial nerve, S1-S2• Tibialis posterior Tibial nerve, L4-L5

The ankle has two joints1. Tibiotalar (ankle mortise)
• “True ankle joint”
2. Talocalcaneal (Subtalar) • Main shock absorber
Ankle
Coronal Section
Talus
Tibia
Calcaneus
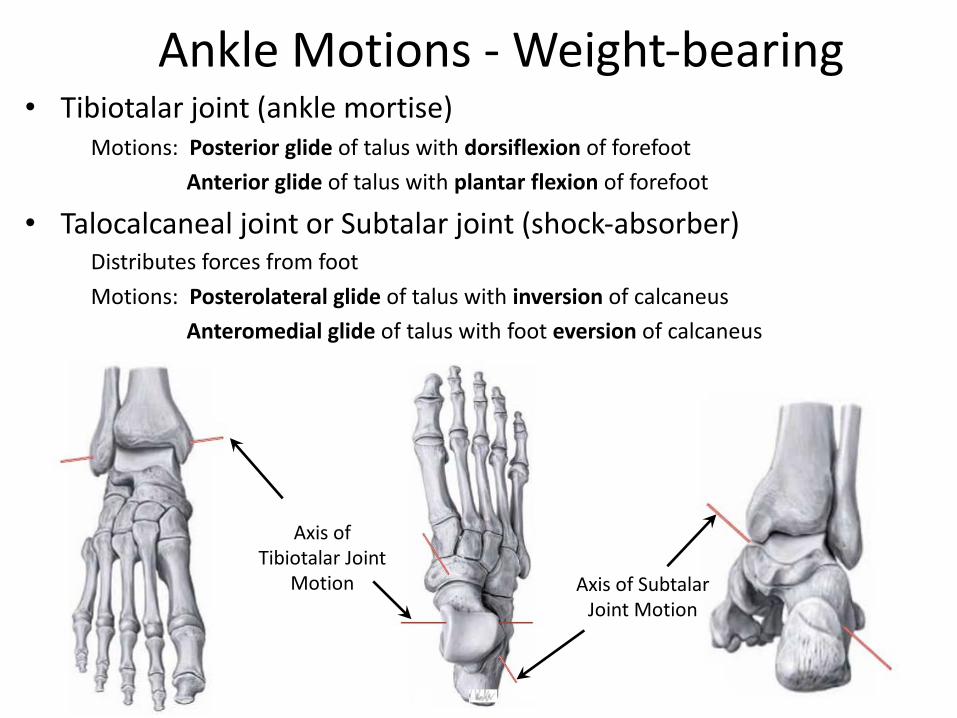
Ankle Motions - Weight-bearing• Tibiotalar joint (ankle mortise)
Motions: Posterior glide of talus with dorsiflexion of forefootAnterior glide of talus with plantar flexion of forefoot
• Talocalcaneal joint or Subtalar joint (shock-absorber)Distributes forces from footMotions: Posterolateral glide of talus with inversion of calcaneus
Anteromedial glide of talus with foot eversion of calcaneus
Axis of SubtalarJoint Motion
Axis of Tibiotalar Joint
Motion

Biomechanics of the Foot and Ankle
YouTube Videohttps://www.youtube.com/watch?v=7SK_O-NuFr4
Rod depicting the rotational axis of the Subtalar Joint
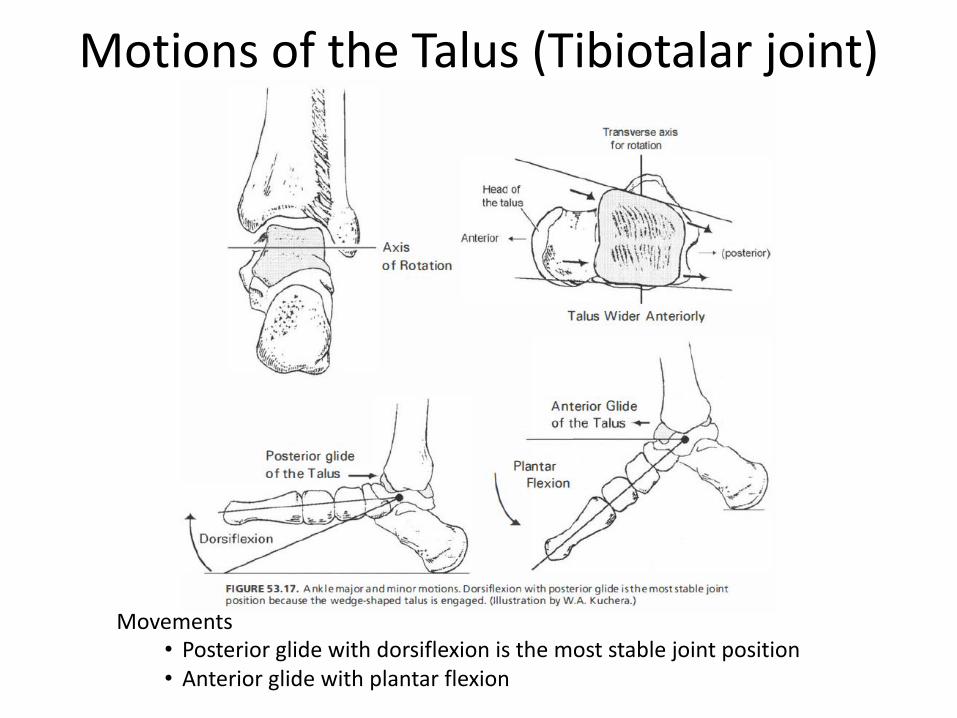
Motions of the Talus (Tibiotalar joint)
Movements• Posterior glide with dorsiflexion is the most stable joint position• Anterior glide with plantar flexion

Ankle Ligaments
• Lateral– Anterior talofibular– Calcaneofibular– Posterior talofibular
• Medial– Posterior tibiotalar– Tibiocalcaneal– Tibionavicular– Anterior tibiotalar
Deltoid Ligament
Lateral
Medial

Inversion Sprain– 80% of all ankle sprains– Ligament Involvement
• Anterior talofibular ligament• Posterior talofibular ligament• Calcanofibular ligament
– Inversion Sprain Nomenclature• First-degree-the integrity of the
ligament is undisturbed• Second-degree-partial tearing and
moderate laxity and instability• Third degree-complete disruption of
ligaments and total instability
Ankle SprainsAnterior TaloFibularAlways Tears First
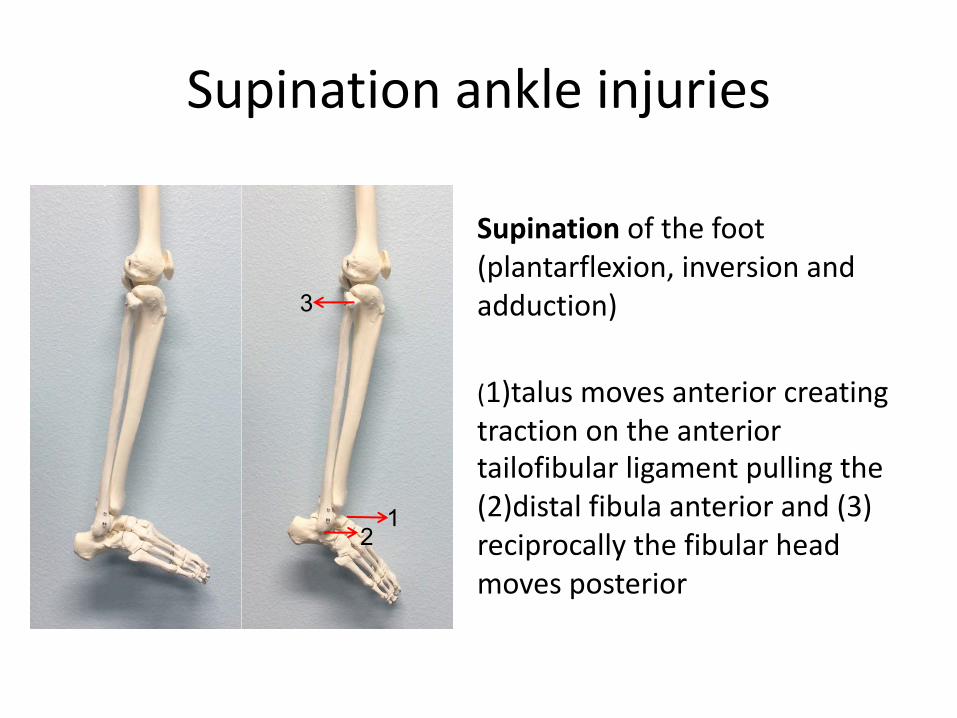
Supination ankle injuries
Supination of the foot (plantarflexion, inversion and adduction)
(1)talus moves anterior creating traction on the anterior tailofibular ligament pulling the (2)distal fibula anterior and (3) reciprocally the fibular head moves posterior
3
12

FootAnatomy and ROM

Foot
Thieme Atlas of Anatomy; General Anatomy and Musculoskeletal System, 1st ed, 2010
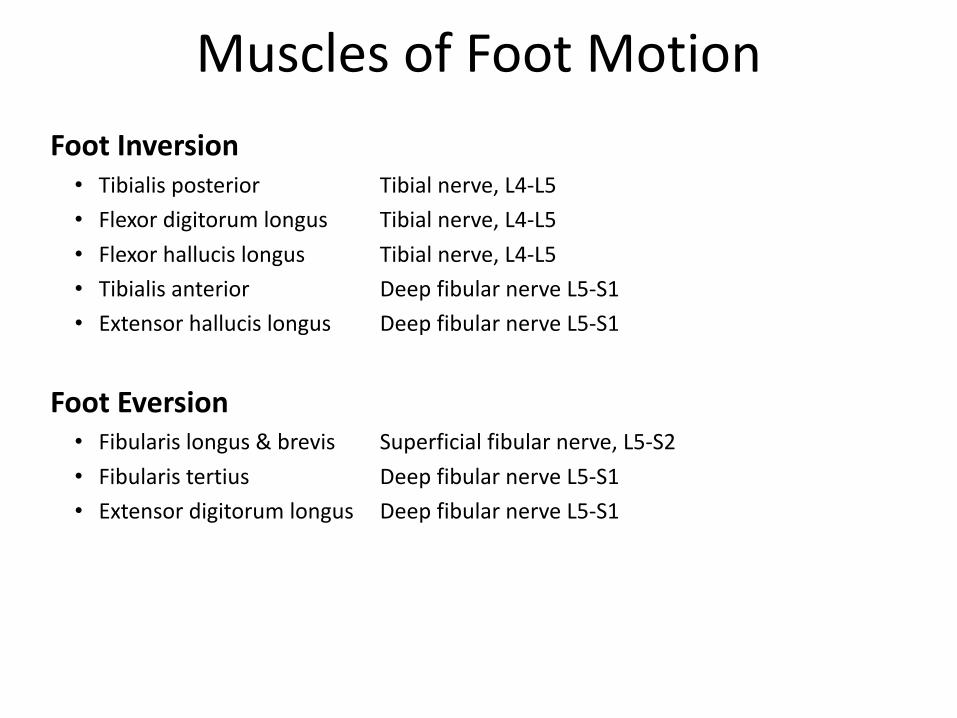
Muscles of Foot MotionFoot Inversion
• Tibialis posterior Tibial nerve, L4-L5• Flexor digitorum longus Tibial nerve, L4-L5• Flexor hallucis longus Tibial nerve, L4-L5• Tibialis anterior Deep fibular nerve L5-S1• Extensor hallucis longus Deep fibular nerve L5-S1
Foot Eversion• Fibularis longus & brevis Superficial fibular nerve, L5-S2• Fibularis tertius Deep fibular nerve L5-S1 • Extensor digitorum longus Deep fibular nerve L5-S1

Foot Motions
Inversion and Eversion Only Supination and PronationIn non-weight bearing
Adduction +Plantar Flexion +
Inversion = Supination
We ADD PLANTs IN SoUP
Abduction +Dorsiflexion +
Eversion = Pronation

Ligaments and Tendons of Plantar foot
FibularisLongus
TibialisPosterior
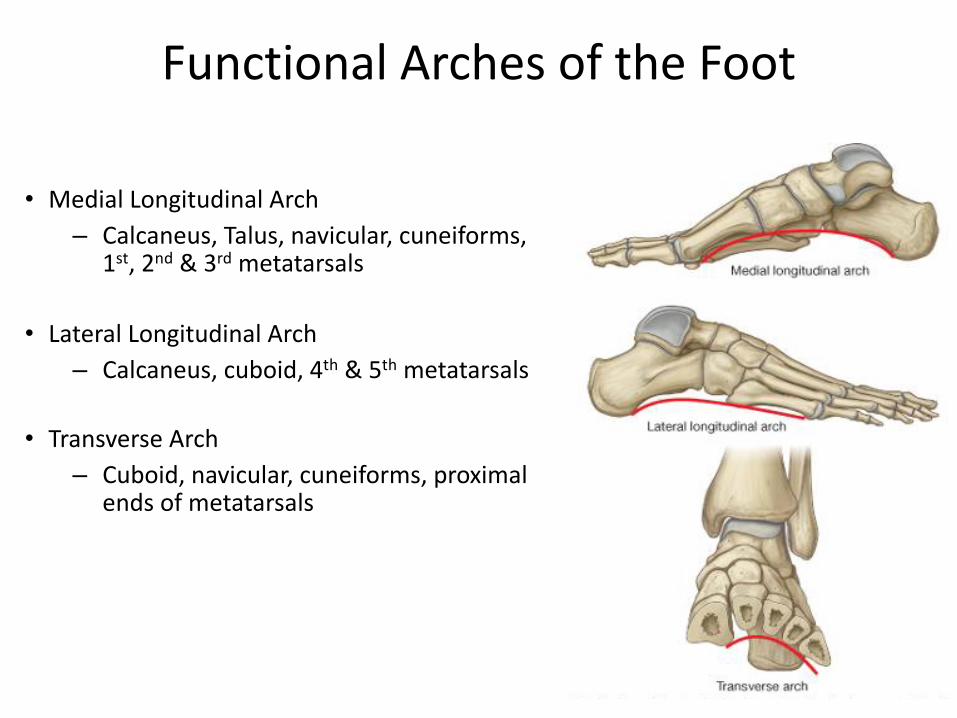
Functional Arches of the Foot
• Medial Longitudinal Arch– Calcaneus, Talus, navicular, cuneiforms,
1st, 2nd & 3rd metatarsals
• Lateral Longitudinal Arch– Calcaneus, cuboid, 4th & 5th metatarsals
• Transverse Arch– Cuboid, navicular, cuneiforms, proximal
ends of metatarsals

Plantar Fascia
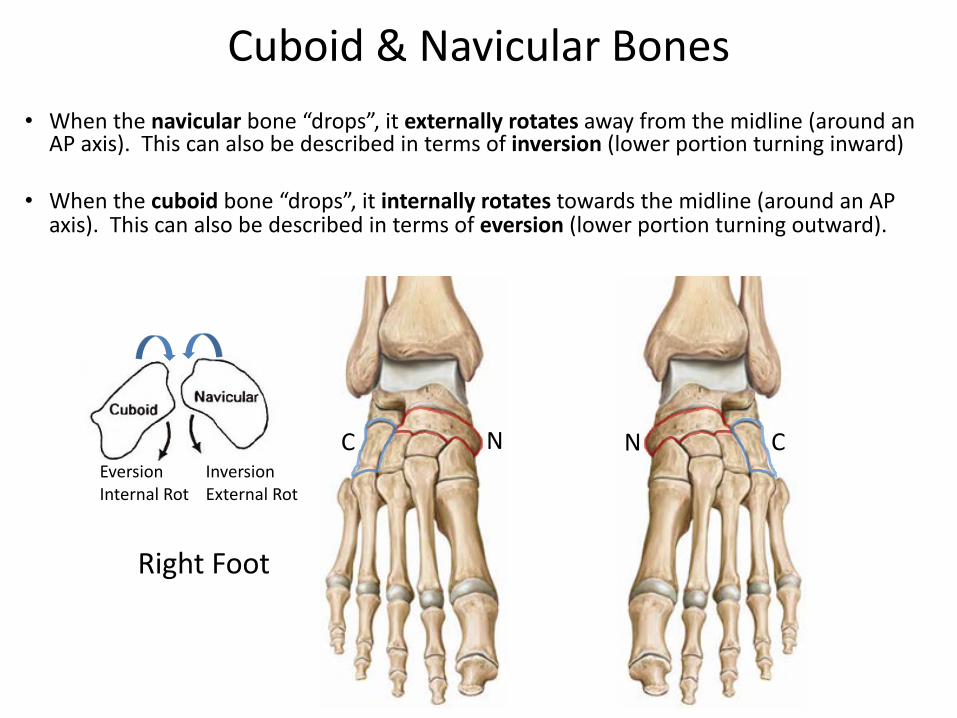
Cuboid & Navicular Bones• When the navicular bone “drops”, it externally rotates away from the midline (around an
AP axis). This can also be described in terms of inversion (lower portion turning inward)
• When the cuboid bone “drops”, it internally rotates towards the midline (around an AP axis). This can also be described in terms of eversion (lower portion turning outward).
InversionExternal Rot
EversionInternal Rot
Right Foot
C N N C

Pes Planus and Pes Cavus
Pes Planus (Flat Foot)• Longitudinal & transverse arches fall• Subtalar axis more horizontal• More loose feeling foot
Pes Cavus (High Arch)• Higher Longitudinal & transverse arches• Subtalar axis more vertical• More rigid feeling foot
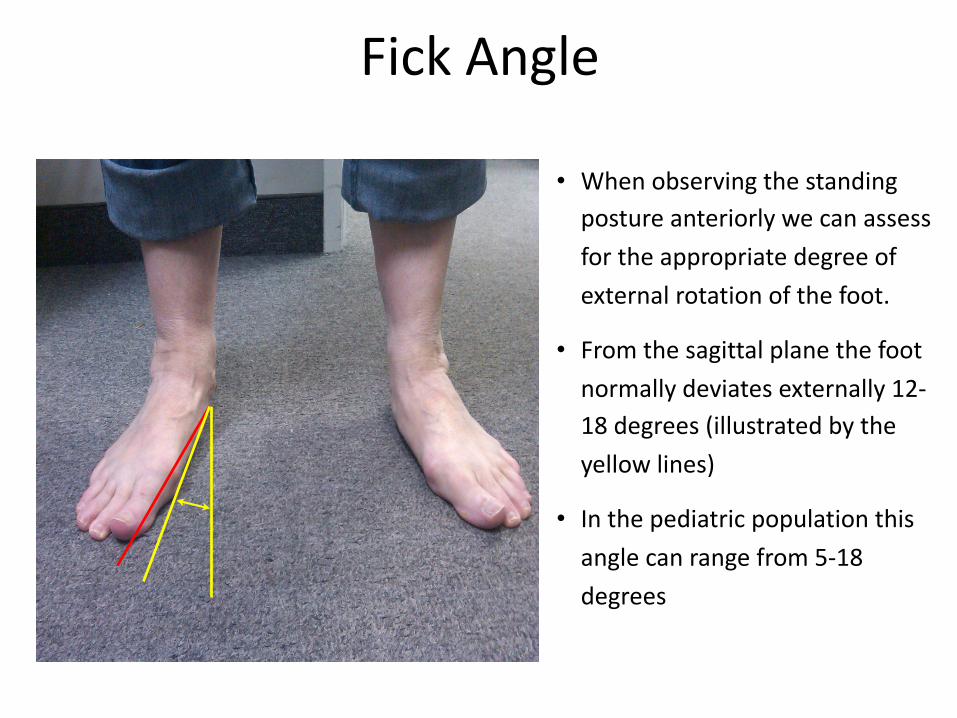
Fick Angle
• When observing the standing posture anteriorly we can assess for the appropriate degree of external rotation of the foot.
• From the sagittal plane the foot normally deviates externally 12-18 degrees (illustrated by the yellow lines)
• In the pediatric population this angle can range from 5-18 degrees
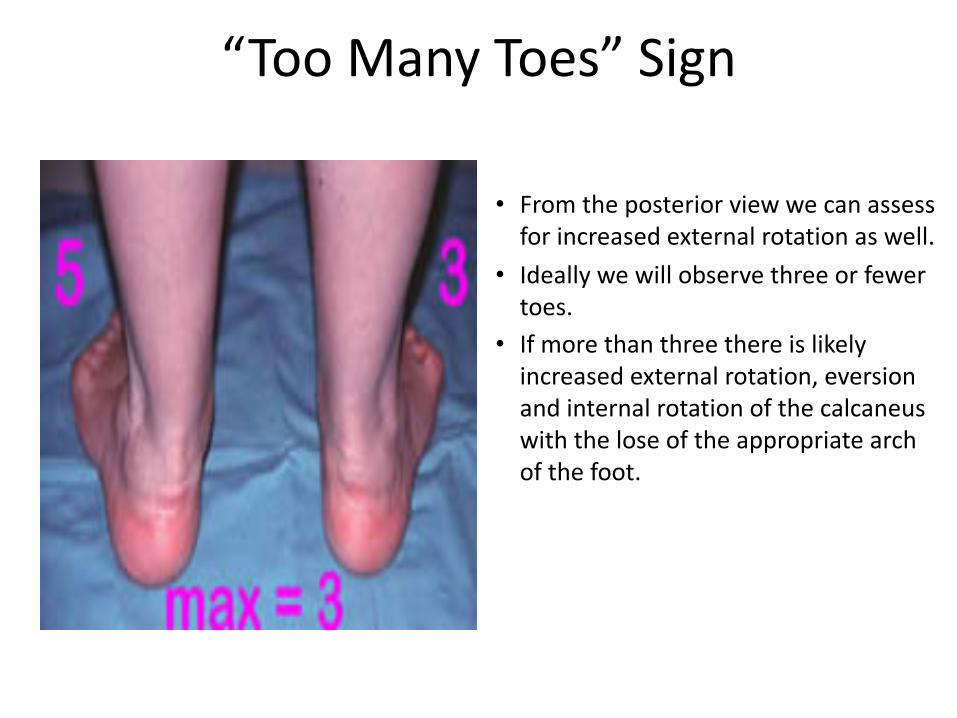
“Too Many Toes” Sign
• From the posterior view we can assess for increased external rotation as well.
• Ideally we will observe three or fewer toes.
• If more than three there is likely increased external rotation, eversion and internal rotation of the calcaneus with the lose of the appropriate arch of the foot.
Lower ExtremitySomatic Dysfunction
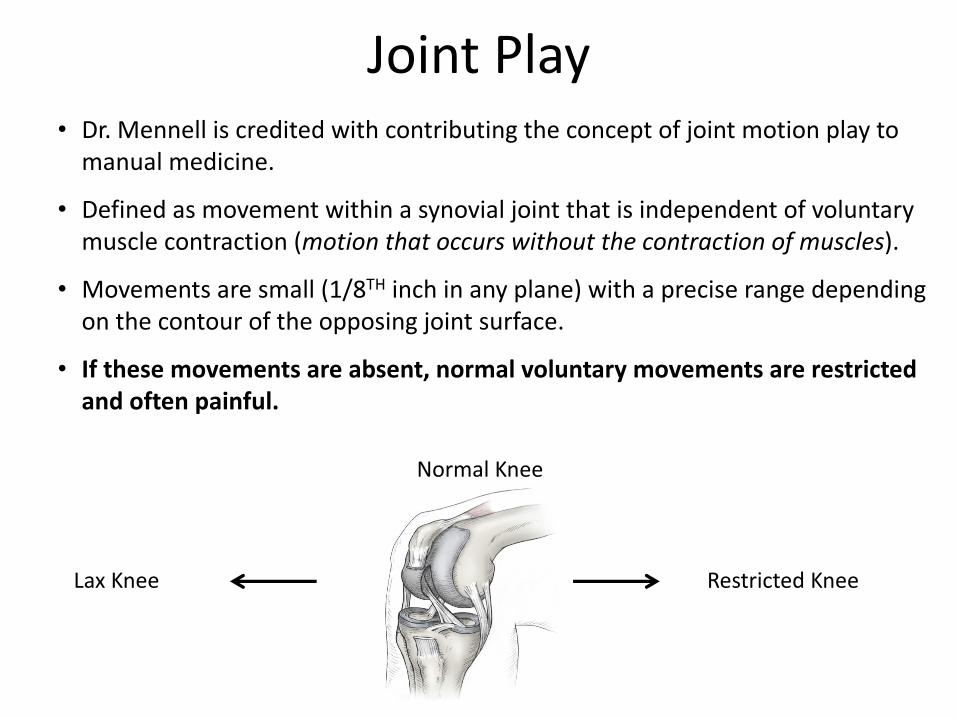
Joint Play• Dr. Mennell is credited with contributing the concept of joint motion play to
manual medicine.
• Defined as movement within a synovial joint that is independent of voluntary muscle contraction (motion that occurs without the contraction of muscles).
• Movements are small (1/8TH inch in any plane) with a precise range depending on the contour of the opposing joint surface.
• If these movements are absent, normal voluntary movements are restricted and often painful.
Normal Knee
Lax Knee Restricted Knee

Hip (Femoroacetabular Joint)• Adduction, Abduction, Extension, Flexion,
Internal rotation, External rotationTibia (Femorotibial Joint)
• External rotation• Internal rotation
Fibular Head (Proximal Tibiofibular Joint)• Anterior or posterior
Talus (Tibiotalar Joint) • Anterior or posterior
Calcaneus (Talocalcaneal Joint, Subtalar Joint)• Inversion or eversion
Cuboid and Navicular• Inversion or eversion (“dropped”)
Joint Motion andSomatic Dysfunction Diagnosis
Will be covered next week

Screening Test: Squat Test Assesses Functional mobility of:• Hip Flexion
– Hips posteriorly rotate near bottom of squat compensatory Lumbar Spinal Flexionnoted (as seen in picture) may indicate muscular tightness
– Gluteus Maximus– Adductor Magnus
– Thighs contact with abdomen relative to depth of squat • Knee Flexion
– Calf contact with hamstrings relative to depth of squat • Ankle Dorsal Flexion
– Heels raise from floor or weight shifted to forefoot near bottom of squat may indicate tight Soleus
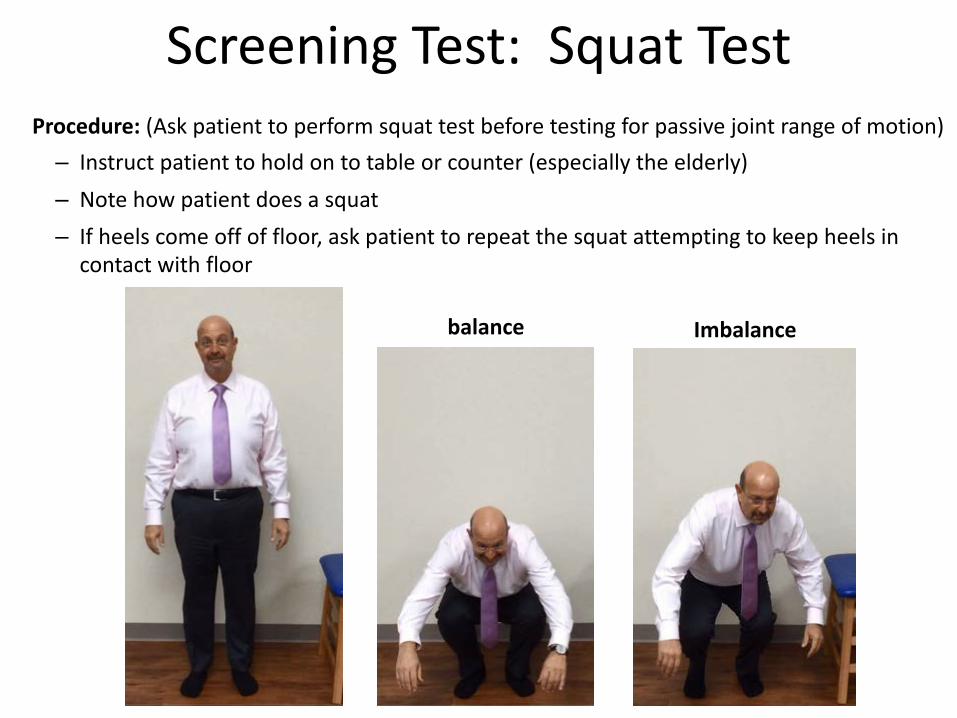
Screening Test: Squat Test Procedure: (Ask patient to perform squat test before testing for passive joint range of motion)
– Instruct patient to hold on to table or counter (especially the elderly)– Note how patient does a squat– If heels come off of floor, ask patient to repeat the squat attempting to keep heels in
contact with floor
Imbalancebalance
TibiaSomatic Dysfunction

• Patient seated with legs hanging off the table.• Physician’s hand on the knee rests on the distal femur while monitoring the tibia with the
fingers.• Physician’s other hand holds the foot into dorsiflexion, to close pack the ankle joint, while
rotating the leg into internal and external rotation.
Tibia - Internally/Externally RotatedSomatic Dysfunction
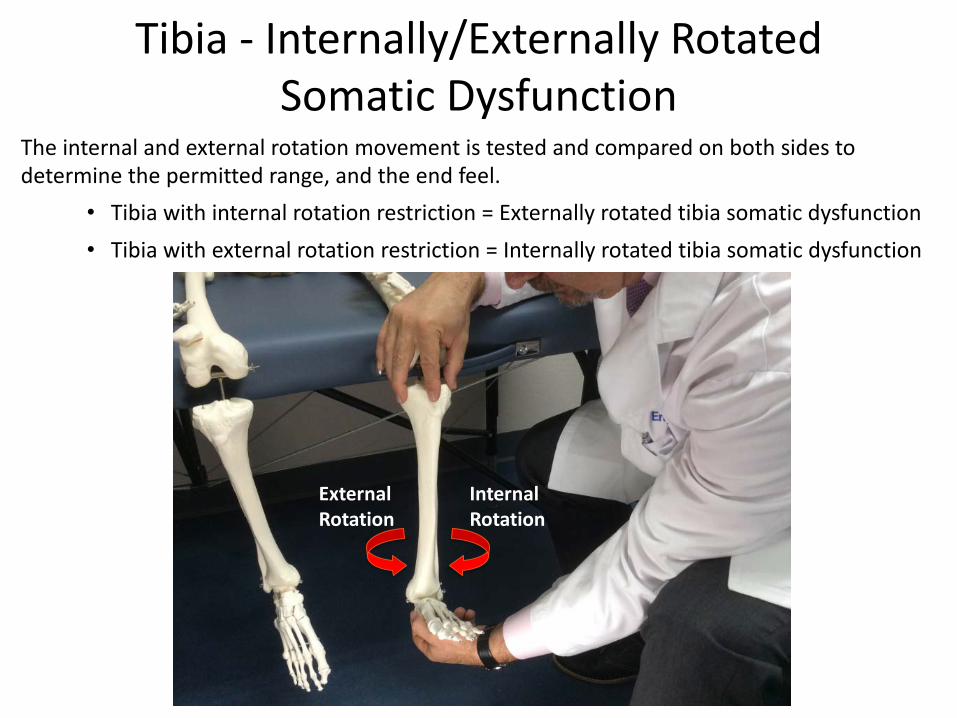
The internal and external rotation movement is tested and compared on both sides to determine the permitted range, and the end feel.
• Tibia with internal rotation restriction = Externally rotated tibia somatic dysfunction • Tibia with external rotation restriction = Internally rotated tibia somatic dysfunction
Tibia - Internally/Externally RotatedSomatic Dysfunction
Internal Rotation
External Rotation
FibulaSomatic Dysfunction

• Fibular head dysfunctions are common and often occur in recurrent ankle sprains.
• Fibular head dysfunction is checked by gliding the fibular head posteriorly (and slightly medially) and anteriorly (and slightly laterally). This may be performed seated or supine.
***In grasping the fibular head, care must be taken to avoid putting pressure on the common fibular nerve, which lies directly behind the fibular head.
• If Anterolateral glide feels more restricted:– Diagnosis is “Posterior Fibular Head”
• If Posteromedial glide feels more restricted:– Diagnosis is “Anterior Fibular Head”
Fibular Head – Anterior/PosteriorSomatic Dysfunction
(anterior)
A/L
P/M
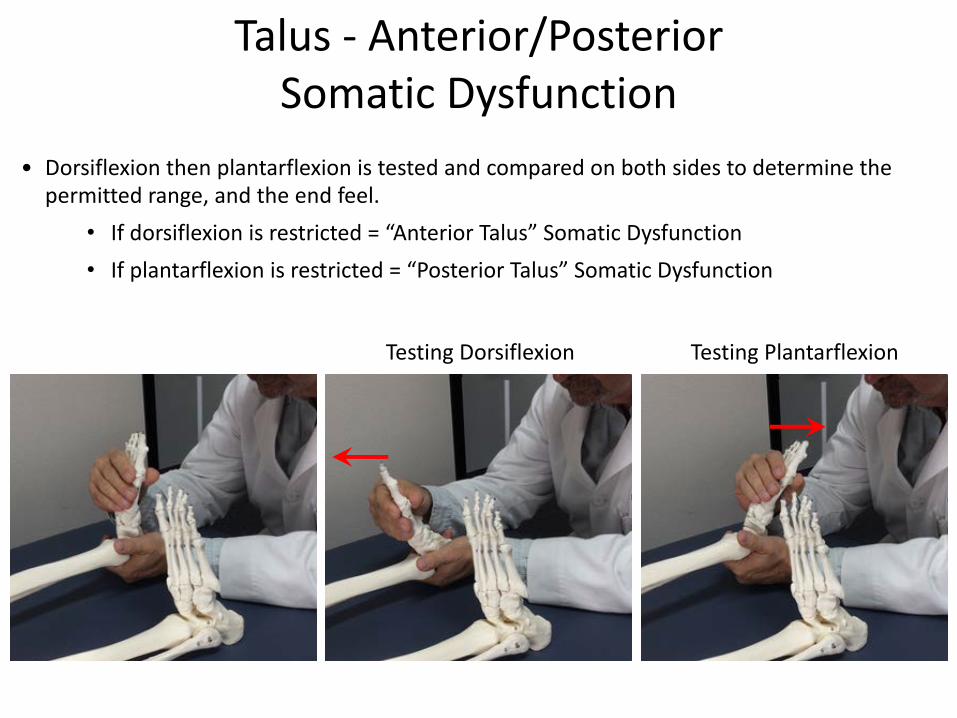
Talus - Anterior/PosteriorSomatic Dysfunction
• Dorsiflexion then plantarflexion is tested and compared on both sides to determine the permitted range, and the end feel.
• If dorsiflexion is restricted = “Anterior Talus” Somatic Dysfunction • If plantarflexion is restricted = “Posterior Talus” Somatic Dysfunction
Testing PlantarflexionTesting Dorsiflexion
Calcaneus, Navicular, Cuboid
Somatic Dysfunction
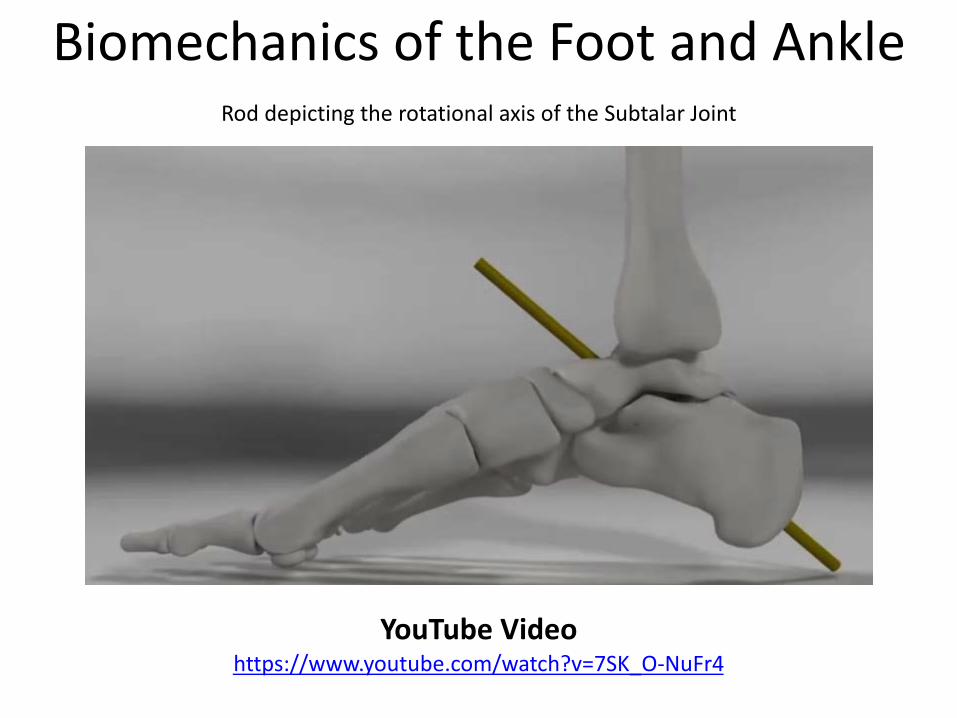
Biomechanics of the Foot and Ankle
YouTube Videohttps://www.youtube.com/watch?v=7SK_O-NuFr4
Rod depicting the rotational axis of the Subtalar Joint
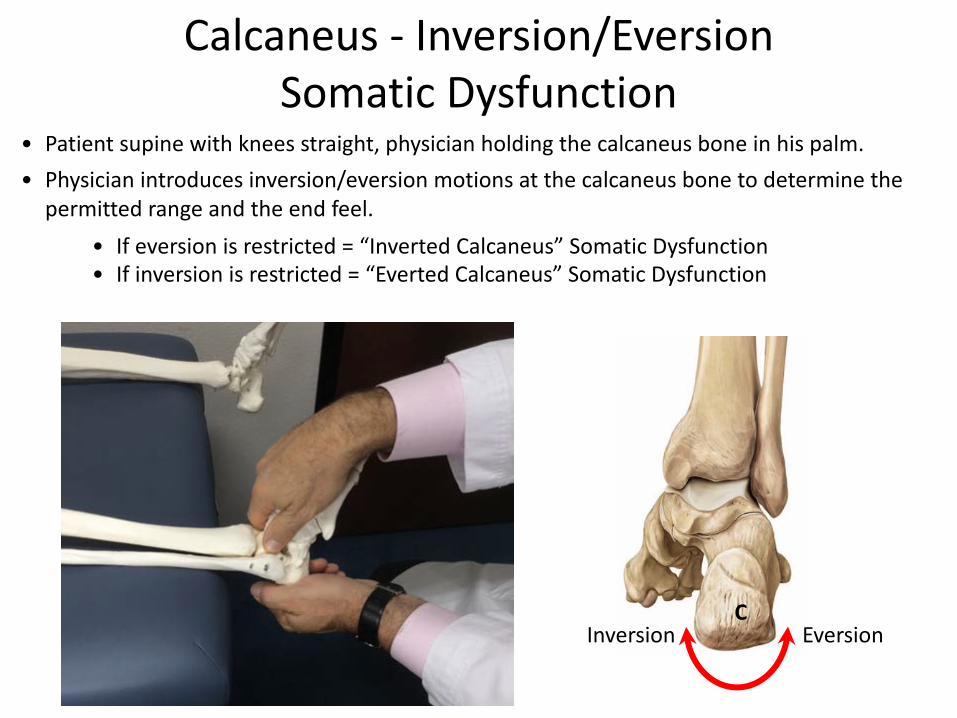
Calcaneus - Inversion/EversionSomatic Dysfunction
• Patient supine with knees straight, physician holding the calcaneus bone in his palm.• Physician introduces inversion/eversion motions at the calcaneus bone to determine the
permitted range and the end feel.• If eversion is restricted = “Inverted Calcaneus” Somatic Dysfunction • If inversion is restricted = “Everted Calcaneus” Somatic Dysfunction
InversionC
Eversion
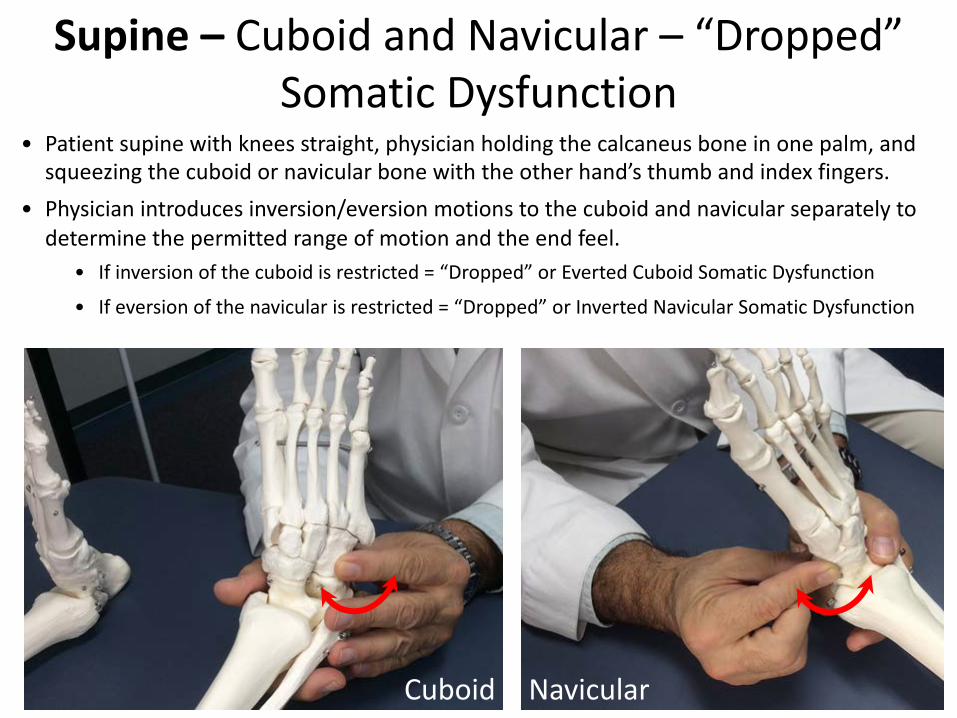
Supine – Cuboid and Navicular – “Dropped”Somatic Dysfunction
• Patient supine with knees straight, physician holding the calcaneus bone in one palm, and squeezing the cuboid or navicular bone with the other hand’s thumb and index fingers.
• Physician introduces inversion/eversion motions to the cuboid and navicular separately to determine the permitted range of motion and the end feel.
• If inversion of the cuboid is restricted = “Dropped” or Everted Cuboid Somatic Dysfunction
• If eversion of the navicular is restricted = “Dropped” or Inverted Navicular Somatic Dysfunction
Cuboid Navicular

• Patient prone with leg to be diagnosed hanging off the table with knee flexed to 90 degrees.• Physician places his two thumbs almost together at the cuboid-navicular junction. • While pressing inferior and lateral, the physician tests the cuboid’s ability to invert. While
pressing inferior and medial, the physician tests the navicular’s ability to evert.• If inversion of the cuboid is restricted = “Dropped” or Everted Cuboid Somatic Dysfunction
• If eversion of the navicular is restricted = “Dropped” or Inverted Navicular Somatic Dysfunction
Prone – Cuboid and Navicular – “Dropped”Somatic Dysfunction
TestingCuboid
Testing Navicular
C N
Inferior View
Lower ExtremitySpecial Tests
Hip• Straight Leg Test• Patrick (FABERE) test• Thomas test• Ober test• Trendelenburg Test
Ankle • Ankle drawer test
Knee• Patellar Grind Test• Bulge test/ Ballottement test• Apleys and McMurray tests• Anterior/ posterior drawer
and Lachmans test• Varus/ Valgus test

HipSpecial Tests

Straight Leg Raise Test (Lasegue’s)• Assessment for sciatic nerve compression• Normal straight leg raise ~90°• Nerve root pain between 35-70°(will be in the sciatic nerve distribution all
the way down the leg or in the low back) • Further pain after 70ᵒ may be:
• Hamstring pain (in the posterior thigh) • Joint pain (SI or facet joint)
• At the point where the patient feels pain, lower the leg slightly and dorsiflex the foot. This will stretch the sciatic nerve, reproducing sciatic pain.

Patrick (FABERE) Test• Flexion• ABduction• External Rotation• Extension - is added as physician places hand on knee and opposite ASIS
***A positive test is when there is decreased range of motion or pain in the femoroacetabular joint indicating joint dysfunction
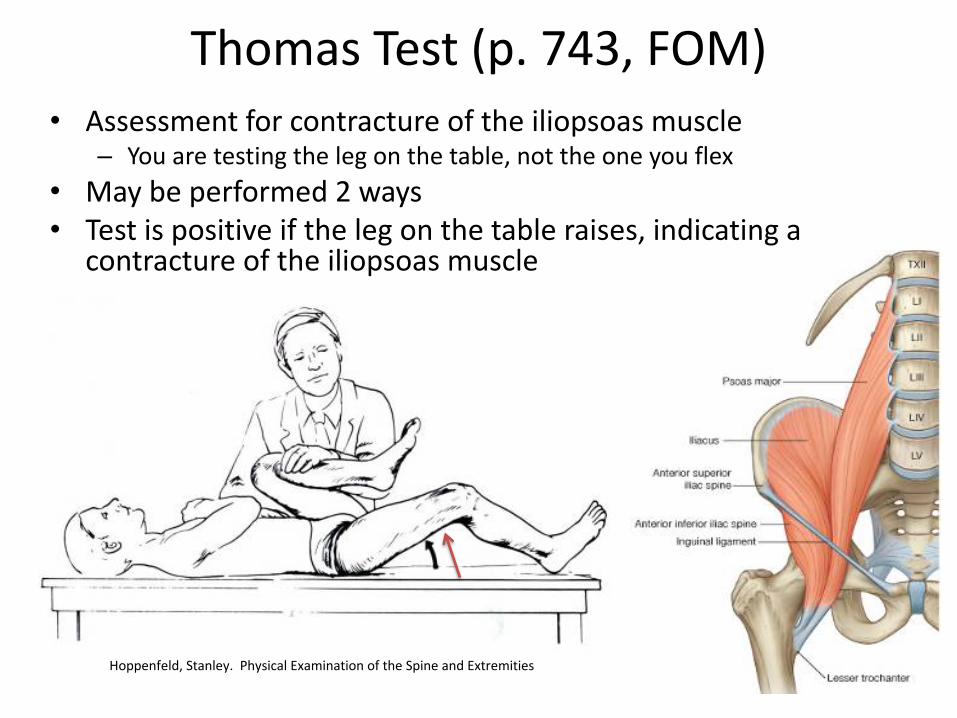
Thomas Test (p. 743, FOM)• Assessment for contracture of the iliopsoas muscle
– You are testing the leg on the table, not the one you flex• May be performed 2 ways• Test is positive if the leg on the table raises, indicating a
contracture of the iliopsoas muscle
Hoppenfeld, Stanley. Physical Examination of the Spine and Extremities

Ober Test• Assessment for contracture of
iliotibial band or tensor fascia lata
• If leg remains abducted, the test is positive
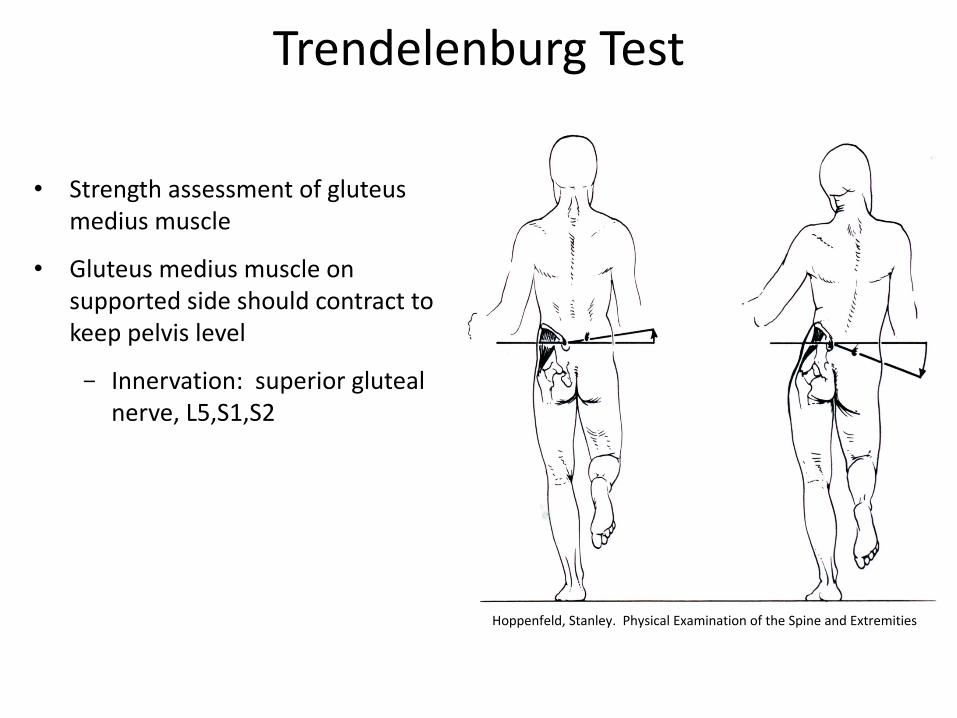
Trendelenburg Test
• Strength assessment of gluteus medius muscle
• Gluteus medius muscle on supported side should contract to keep pelvis level
- Innervation: superior gluteal nerve, L5,S1,S2
Hoppenfeld, Stanley. Physical Examination of the Spine and Extremities

KneeSpecial Tests

Patellar Grind Test
• Assessment of posterior patellar articulatory surface– Positive test for
chondromalacia patella– A grinding or gritty
sensation (crepitus) indicating chondromalacia patella

Bulge Test & Ballottement TestPositive test:
– Visual and palpable fluid indicating joint effusion
FOM, 3rd EdBallottement test
Ballottement test
Bulge test

ApleyCompression/Distraction Tests
• Compression– Assessment of torn meniscus– Compression with internal or
external rotation
• Distraction– Assessment for integrity of the
collateral ligaments– Traction with internal or
external rotation
Hoppenfeld, Stanley. Physical Examination of the Spine and Extremities

McMurray TestAssessment for lateral and medial meniscal tears
• Medial meniscus
– One hand holds the foot and the other hand holds around the anterior part of the knee with the thumb palpating the lateral joint line and at least one finger palpating the medial joint line.
– The knee is fully flexed, the foot is turned outward (to externally rotate the tibia), and the tibia is abducted (genu valgus). The knee is then extended to test the medial meniscus.
• Lateral meniscus
– The knee is fully flexed, the foot is turned inward (to internally rotate the tibia), and the tibia is adducted (genu varus). The knee is then extended to test the lateral meniscus.
• A positive test is indicated by eliciting a palpable/audible click accompanied by pain
• See FOM figure 53.13 p.793
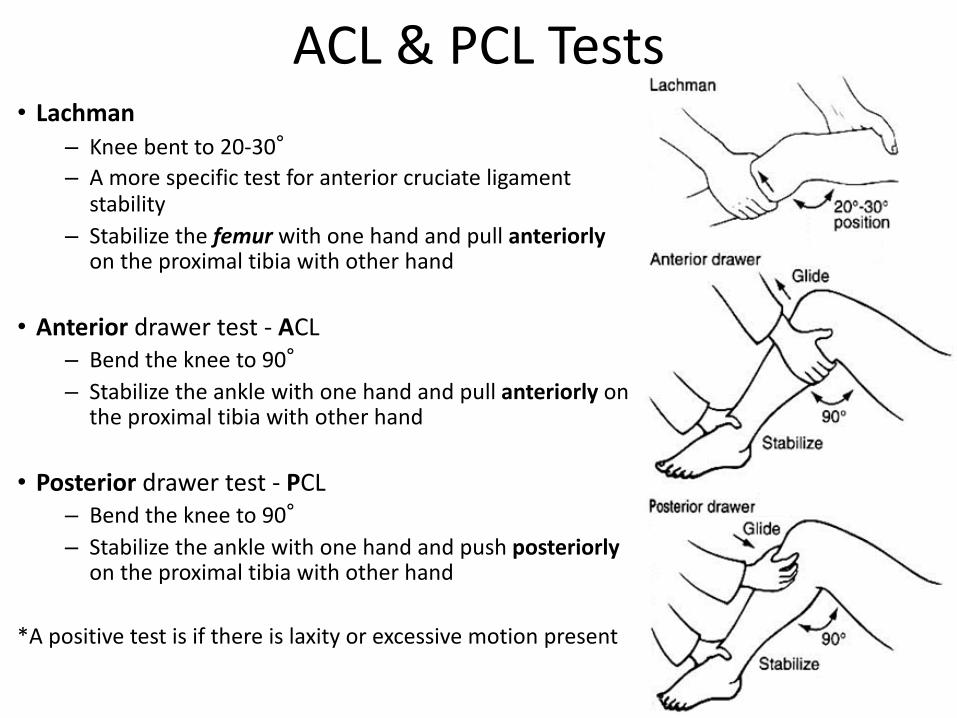
ACL & PCL Tests• Lachman
– Knee bent to 20-30°– A more specific test for anterior cruciate ligament
stability– Stabilize the femur with one hand and pull anteriorly
on the proximal tibia with other hand
• Anterior drawer test - ACL– Bend the knee to 90°– Stabilize the ankle with one hand and pull anteriorly on
the proximal tibia with other hand
• Posterior drawer test - PCL– Bend the knee to 90°– Stabilize the ankle with one hand and push posteriorly
on the proximal tibia with other hand
*A positive test is if there is laxity or excessive motion present

Valgus/Varus Test• Tests Medial and Lateral Collateral Ligaments • Pt supine, knee flexed to 15 degrees• Stabilize the distal tibia with one hand and add a
medial or lateral force with the other hand• Positive test = gapping (maybe pain) felt on
either side of knee joint
Example: Valgus Stress Test

AnkleSpecial Tests
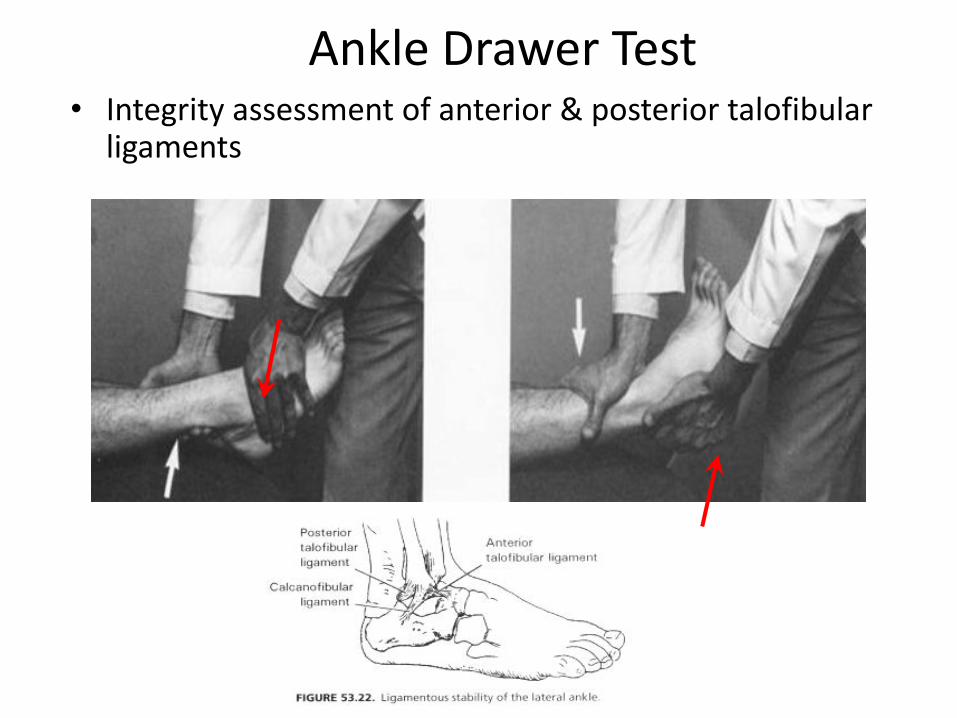
Ankle Drawer Test• Integrity assessment of anterior & posterior talofibular
ligaments

References
• FOM, pp. 784 - 818
• Thieme Atlas of Anatomy; General Anatomy and Musculoskeletal System, 1st ed, 2010
• Hoppenfeld, Stanley. Physical Examination of the Spine and Extremities.
• UNTHSC-TCOM, Department of Osteopathic Manipulative Medicine, 2003-2004 powerpoint lecture materials
• Greenman, Phillip E., Principles of Manual Medicine
• Magee, David J., Orthopedic Physical Assessment