Low level laser therapy (LLLT) is the application of light ...
26
BIPHASIC DOSE RESPONSE IN LOW LEVEL LIGHT THERAPY Ying-Ying Huang Wellman Center for Photomedicine, Massachusetts General Hospital, Boston, MA; Department of Dermatology, Harvard Medical School, Boston, MA; Aesthetic and Plastic Center of Guangxi Medical University, Nanning, P.R. China Aaron C.-H. Chen Wellman Center for Photomedicine, Massachusetts General Hospital, Boston, MA; Boston University School of Medicine, Graduate Medical Sciences, Boston, MA James D. Carroll THOR Photomedicine Ltd, 18A East Street, Chesham, HP5 1HQ, UK Michael R. Hamblin Wellman Center for Photomedicine, Massachusetts General Hospital, Boston, MA; Department of Dermatology, Harvard Medical School, Boston, MA; Harvard-MIT Division of Health Sciences and Technology, Cambridge, MA The use of low levels of visible or near infrared light for reducing pain, inflammation and edema, promoting healing of wounds, deeper tissues and nerves, and preventing cell death and tissue damage has been known for over forty years since the invention of lasers. Despite many reports of positive findings from experiments conducted in vitro, in animal models and in randomized controlled clinical trials, LLLT remains controversial in main- stream medicine. The biochemical mechanisms underlying the positive effects are incom- pletely understood, and the complexity of rationally choosing amongst a large number of illumination parameters such as wavelength, fluence, power density, pulse structure and treatment timing has led to the publication of a number of negative studies as well as many positive ones. A biphasic dose response has been frequently observed where low levels of light have a much better effect on stimulating and repairing tissues than higher levels of light. The so-called Arndt-Schulz curve is frequently used to describe this biphasic dose response. This review will cover the molecular and cellular mechanisms in LLLT, and describe some of our recent results in vitro and in vivo that provide scientific explanations for this biphasic dose response. 1. INTRODUCTION 1.1. Brief history Low level laser therapy (LLLT) is the application of light (usually a low power laser or LED in the range of 1mW – 500mW) to a pathology to promote tissue regeneration, reduce inflammation and relieve pain. The light is typically of narrow spectral width in the red or near infrared Dose-Response (Prepress) Formerly Nonlinearity in Biology, Toxicology, and Medicine Copyright © 2009 University of Massachusetts ISSN: 1559-3258 DOI: 10.2203/dose-response.09-027.Hamblin Address correspondence to Professor Michael R. Hamblin, BAR 414, Wellman Center for Photomedicine, Massachusetts General Hospital, 40 Blossom Street, Boston, MA 02114; Phone: 617-726-6182, Fax: 617-726-8566, E-mail: [email protected]
Transcript of Low level laser therapy (LLLT) is the application of light ...

BIPHASIC DOSE RESPONSE IN LOW LEVEL LIGHT THERAPY
Ying-Ying Huang � Wellman Center for Photomedicine, Massachusetts GeneralHospital, Boston, MA; Department of Dermatology, Harvard Medical School,Boston, MA; Aesthetic and Plastic Center of Guangxi Medical University, Nanning,P.R. China
Aaron C.-H. Chen � Wellman Center for Photomedicine, Massachusetts GeneralHospital, Boston, MA; Boston University School of Medicine, Graduate MedicalSciences, Boston, MA
James D. Carroll � THOR Photomedicine Ltd, 18A East Street, Chesham, HP51HQ, UK
Michael R. Hamblin � Wellman Center for Photomedicine, MassachusettsGeneral Hospital, Boston, MA; Department of Dermatology, Harvard MedicalSchool, Boston, MA; Harvard-MIT Division of Health Sciences and Technology,Cambridge, MA
� The use of low levels of visible or near infrared light for reducing pain, inflammationand edema, promoting healing of wounds, deeper tissues and nerves, and preventing celldeath and tissue damage has been known for over forty years since the invention of lasers.Despite many reports of positive findings from experiments conducted in vitro, in animalmodels and in randomized controlled clinical trials, LLLT remains controversial in main-stream medicine. The biochemical mechanisms underlying the positive effects are incom-pletely understood, and the complexity of rationally choosing amongst a large number ofillumination parameters such as wavelength, fluence, power density, pulse structure andtreatment timing has led to the publication of a number of negative studies as well as manypositive ones. A biphasic dose response has been frequently observed where low levels oflight have a much better effect on stimulating and repairing tissues than higher levels oflight. The so-called Arndt-Schulz curve is frequently used to describe this biphasic doseresponse. This review will cover the molecular and cellular mechanisms in LLLT, anddescribe some of our recent results in vitro and in vivo that provide scientific explanationsfor this biphasic dose response.
1. INTRODUCTION
1.1. Brief history
Low level laser therapy (LLLT) is the application of light (usually alow power laser or LED in the range of 1mW – 500mW) to a pathology topromote tissue regeneration, reduce inflammation and relieve pain. Thelight is typically of narrow spectral width in the red or near infrared
Dose-Response (Prepress)Formerly Nonlinearity in Biology, Toxicology, and MedicineCopyright © 2009 University of MassachusettsISSN: 1559-3258DOI: 10.2203/dose-response.09-027.Hamblin
Address correspondence to Professor Michael R. Hamblin, BAR 414, Wellman Center forPhotomedicine, Massachusetts General Hospital, 40 Blossom Street, Boston, MA 02114; Phone:617-726-6182, Fax: 617-726-8566, E-mail: [email protected]
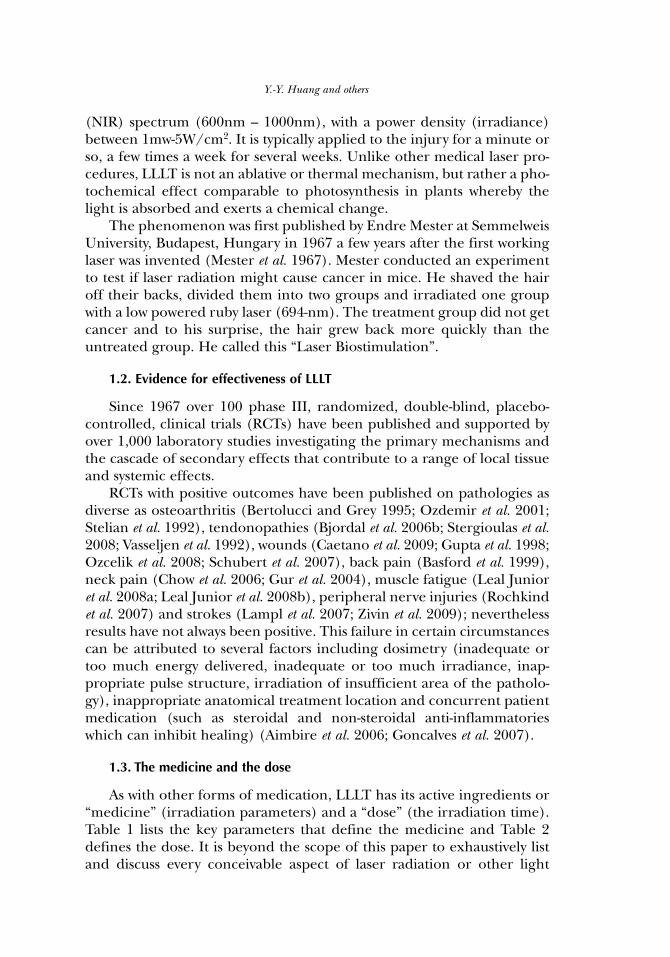
(NIR) spectrum (600nm – 1000nm), with a power density (irradiance)between 1mw-5W/cm2. It is typically applied to the injury for a minute orso, a few times a week for several weeks. Unlike other medical laser pro-cedures, LLLT is not an ablative or thermal mechanism, but rather a pho-tochemical effect comparable to photosynthesis in plants whereby thelight is absorbed and exerts a chemical change.
The phenomenon was first published by Endre Mester at SemmelweisUniversity, Budapest, Hungary in 1967 a few years after the first workinglaser was invented (Mester et al. 1967). Mester conducted an experimentto test if laser radiation might cause cancer in mice. He shaved the hairoff their backs, divided them into two groups and irradiated one groupwith a low powered ruby laser (694-nm). The treatment group did not getcancer and to his surprise, the hair grew back more quickly than theuntreated group. He called this “Laser Biostimulation”.
1.2. Evidence for effectiveness of LLLT
Since 1967 over 100 phase III, randomized, double-blind, placebo-controlled, clinical trials (RCTs) have been published and supported byover 1,000 laboratory studies investigating the primary mechanisms andthe cascade of secondary effects that contribute to a range of local tissueand systemic effects.
RCTs with positive outcomes have been published on pathologies asdiverse as osteoarthritis (Bertolucci and Grey 1995; Ozdemir et al. 2001;Stelian et al. 1992), tendonopathies (Bjordal et al. 2006b; Stergioulas et al.2008; Vasseljen et al. 1992), wounds (Caetano et al. 2009; Gupta et al. 1998;Ozcelik et al. 2008; Schubert et al. 2007), back pain (Basford et al. 1999),neck pain (Chow et al. 2006; Gur et al. 2004), muscle fatigue (Leal Junioret al. 2008a; Leal Junior et al. 2008b), peripheral nerve injuries (Rochkindet al. 2007) and strokes (Lampl et al. 2007; Zivin et al. 2009); neverthelessresults have not always been positive. This failure in certain circumstancescan be attributed to several factors including dosimetry (inadequate ortoo much energy delivered, inadequate or too much irradiance, inap-propriate pulse structure, irradiation of insufficient area of the patholo-gy), inappropriate anatomical treatment location and concurrent patientmedication (such as steroidal and non-steroidal anti-inflammatorieswhich can inhibit healing) (Aimbire et al. 2006; Goncalves et al. 2007).
1.3. The medicine and the dose
As with other forms of medication, LLLT has its active ingredients or“medicine” (irradiation parameters) and a “dose” (the irradiation time).Table 1 lists the key parameters that define the medicine and Table 2defines the dose. It is beyond the scope of this paper to exhaustively listand discuss every conceivable aspect of laser radiation or other light
Y.-Y. Huang and others
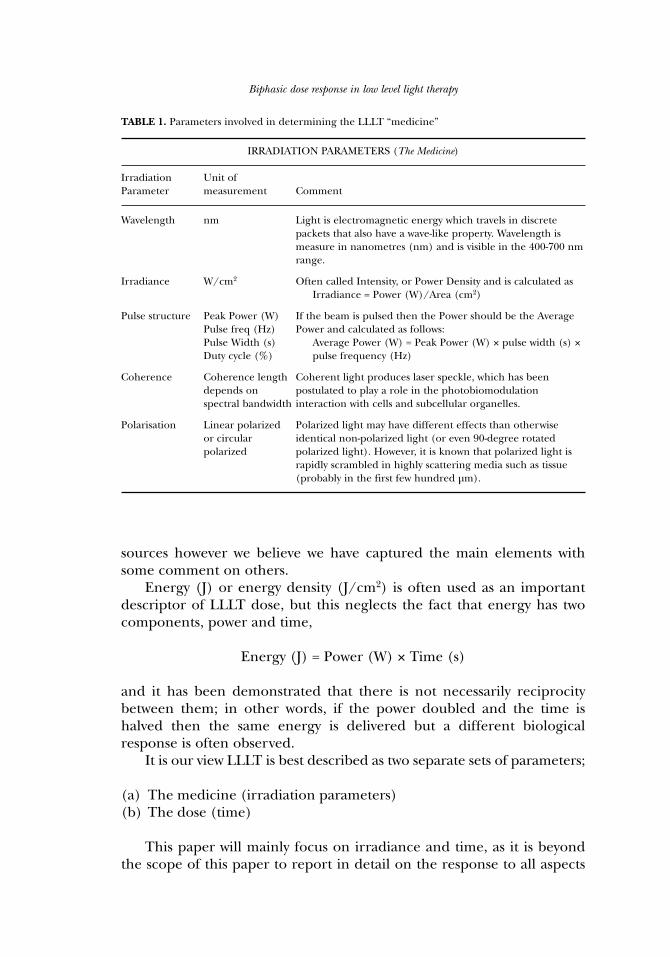
sources however we believe we have captured the main elements withsome comment on others.
Energy (J) or energy density (J/cm2) is often used as an importantdescriptor of LLLT dose, but this neglects the fact that energy has twocomponents, power and time,
Energy (J) = Power (W) × Time (s)
and it has been demonstrated that there is not necessarily reciprocitybetween them; in other words, if the power doubled and the time ishalved then the same energy is delivered but a different biologicalresponse is often observed.
It is our view LLLT is best described as two separate sets of parameters;
(a) The medicine (irradiation parameters)(b) The dose (time)
This paper will mainly focus on irradiance and time, as it is beyondthe scope of this paper to report in detail on the response to all aspects
Biphasic dose response in low level light therapy
TABLE 1. Parameters involved in determining the LLLT “medicine”
IRRADIATION PARAMETERS (The Medicine)
Irradiation Unit of Parameter measurement Comment
Wavelength nm Light is electromagnetic energy which travels in discrete packets that also have a wave-like property. Wavelength is measure in nanometres (nm) and is visible in the 400-700 nm range.
Irradiance W/cm2 Often called Intensity, or Power Density and is calculated asIrradiance = Power (W)/Area (cm2)
Pulse structure Peak Power (W) If the beam is pulsed then the Power should be the Average Pulse freq (Hz) Power and calculated as follows:Pulse Width (s) Average Power (W) = Peak Power (W) × pulse width (s) ×Duty cycle (%) pulse frequency (Hz)
Coherence Coherence length Coherent light produces laser speckle, which has been depends on postulated to play a role in the photobiomodulation spectral bandwidth interaction with cells and subcellular organelles.
Polarisation Linear polarized Polarized light may have different effects than otherwise or circular identical non-polarized light (or even 90-degree rotated polarized polarized light). However, it is known that polarized light is
rapidly scrambled in highly scattering media such as tissue (probably in the first few hundred µm).
laser radiation listed in the “medicine” table; however there is evidence toshow that different wavelengths, pulses, coherence, polarization havesome effect on the magnitude of biomodulation (see sections 3 and 4).
2. MECHANISMS OF LOW LEVEL LIGHT THERAPY.
2.1. Cellular Chromophores and First Law of Photobiology
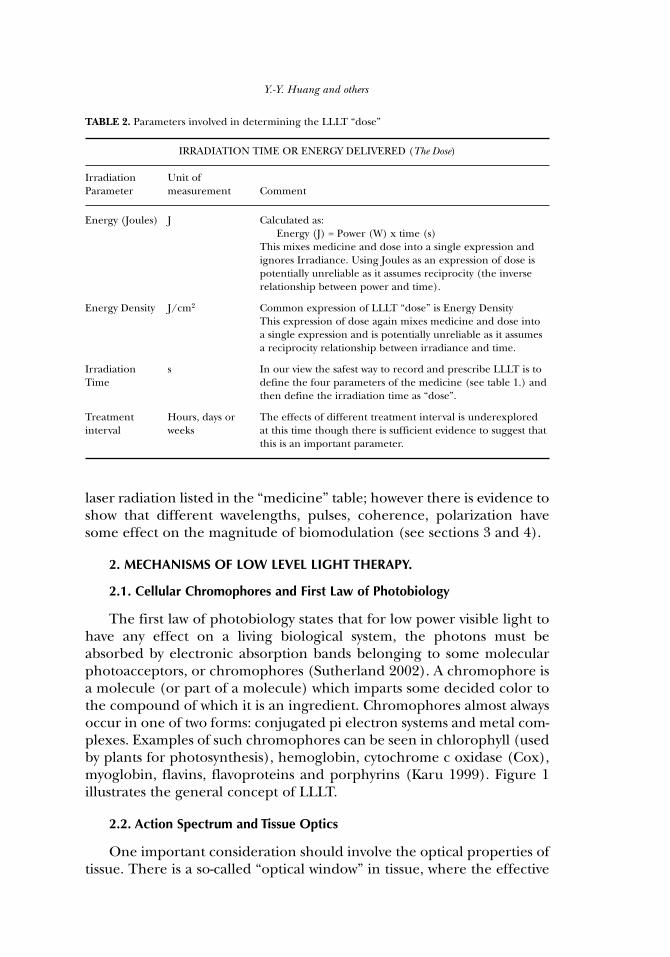
The first law of photobiology states that for low power visible light tohave any effect on a living biological system, the photons must beabsorbed by electronic absorption bands belonging to some molecularphotoacceptors, or chromophores (Sutherland 2002). A chromophore isa molecule (or part of a molecule) which imparts some decided color tothe compound of which it is an ingredient. Chromophores almost alwaysoccur in one of two forms: conjugated pi electron systems and metal com-plexes. Examples of such chromophores can be seen in chlorophyll (usedby plants for photosynthesis), hemoglobin, cytochrome c oxidase (Cox),myoglobin, flavins, flavoproteins and porphyrins (Karu 1999). Figure 1illustrates the general concept of LLLT.
2.2. Action Spectrum and Tissue Optics
One important consideration should involve the optical properties oftissue. There is a so-called “optical window” in tissue, where the effective
Y.-Y. Huang and others
TABLE 2. Parameters involved in determining the LLLT “dose”
IRRADIATION TIME OR ENERGY DELIVERED (The Dose)
Irradiation Unit of Parameter measurement Comment
Energy (Joules) J Calculated as: Energy (J) = Power (W) x time (s)
This mixes medicine and dose into a single expression and ignores Irradiance. Using Joules as an expression of dose is potentially unreliable as it assumes reciprocity (the inverse relationship between power and time).
Energy Density J/cm2 Common expression of LLLT “dose” is Energy DensityThis expression of dose again mixes medicine and dose into a single expression and is potentially unreliable as it assumes a reciprocity relationship between irradiance and time.
Irradiation s In our view the safest way to record and prescribe LLLT is to Time define the four parameters of the medicine (see table 1.) and
then define the irradiation time as “dose”.
Treatment Hours, days or The effects of different treatment interval is underexplored interval weeks at this time though there is sufficient evidence to suggest that
this is an important parameter.
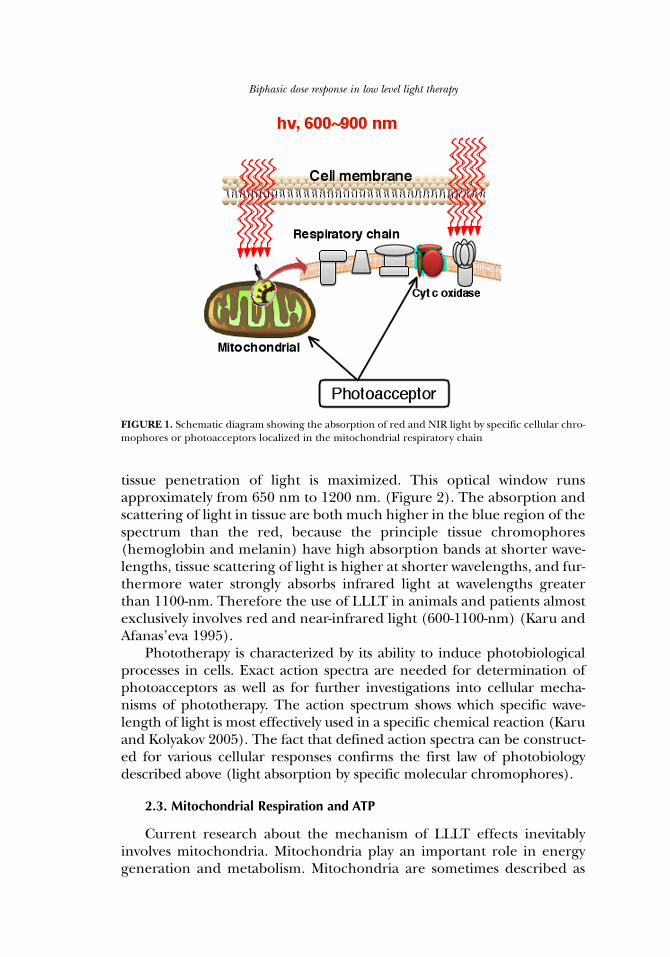
tissue penetration of light is maximized. This optical window runsapproximately from 650 nm to 1200 nm. (Figure 2). The absorption andscattering of light in tissue are both much higher in the blue region of thespectrum than the red, because the principle tissue chromophores(hemoglobin and melanin) have high absorption bands at shorter wave-lengths, tissue scattering of light is higher at shorter wavelengths, and fur-thermore water strongly absorbs infrared light at wavelengths greaterthan 1100-nm. Therefore the use of LLLT in animals and patients almostexclusively involves red and near-infrared light (600-1100-nm) (Karu andAfanas’eva 1995).
Phototherapy is characterized by its ability to induce photobiologicalprocesses in cells. Exact action spectra are needed for determination ofphotoacceptors as well as for further investigations into cellular mecha-nisms of phototherapy. The action spectrum shows which specific wave-length of light is most effectively used in a specific chemical reaction (Karuand Kolyakov 2005). The fact that defined action spectra can be construct-ed for various cellular responses confirms the first law of photobiologydescribed above (light absorption by specific molecular chromophores).
2.3. Mitochondrial Respiration and ATP
Current research about the mechanism of LLLT effects inevitablyinvolves mitochondria. Mitochondria play an important role in energygeneration and metabolism. Mitochondria are sometimes described as
Biphasic dose response in low level light therapy
FIGURE 1. Schematic diagram showing the absorption of red and NIR light by specific cellular chro-mophores or photoacceptors localized in the mitochondrial respiratory chain
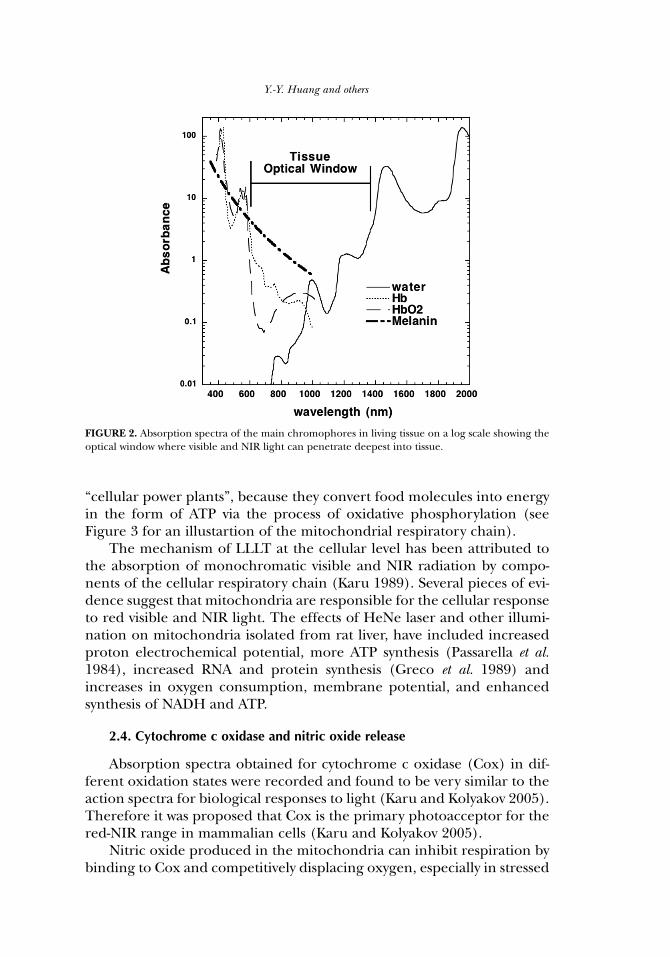
“cellular power plants”, because they convert food molecules into energyin the form of ATP via the process of oxidative phosphorylation (seeFigure 3 for an illustartion of the mitochondrial respiratory chain).
The mechanism of LLLT at the cellular level has been attributed tothe absorption of monochromatic visible and NIR radiation by compo-nents of the cellular respiratory chain (Karu 1989). Several pieces of evi-dence suggest that mitochondria are responsible for the cellular responseto red visible and NIR light. The effects of HeNe laser and other illumi-nation on mitochondria isolated from rat liver, have included increasedproton electrochemical potential, more ATP synthesis (Passarella et al.1984), increased RNA and protein synthesis (Greco et al. 1989) andincreases in oxygen consumption, membrane potential, and enhancedsynthesis of NADH and ATP.
2.4. Cytochrome c oxidase and nitric oxide release
Absorption spectra obtained for cytochrome c oxidase (Cox) in dif-ferent oxidation states were recorded and found to be very similar to theaction spectra for biological responses to light (Karu and Kolyakov 2005).Therefore it was proposed that Cox is the primary photoacceptor for thered-NIR range in mammalian cells (Karu and Kolyakov 2005).
Nitric oxide produced in the mitochondria can inhibit respiration bybinding to Cox and competitively displacing oxygen, especially in stressed
Y.-Y. Huang and others
FIGURE 2. Absorption spectra of the main chromophores in living tissue on a log scale showing theoptical window where visible and NIR light can penetrate deepest into tissue.
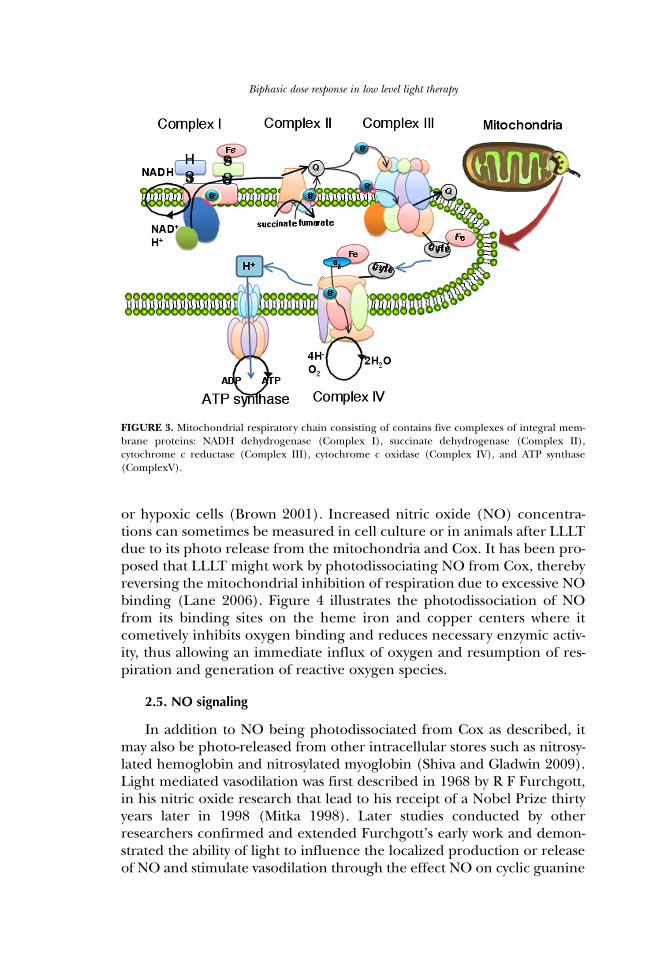
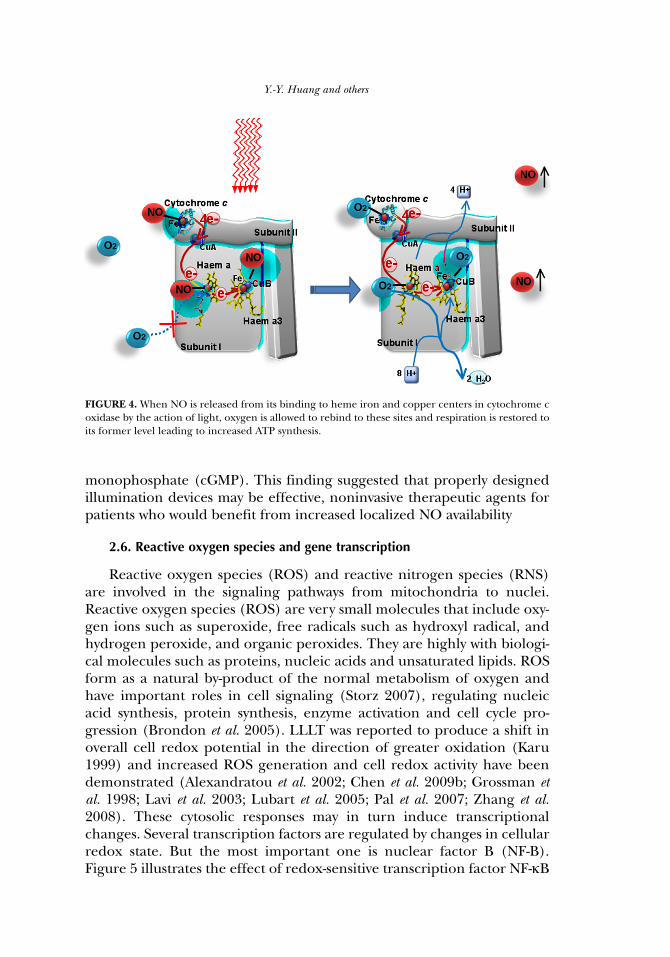
or hypoxic cells (Brown 2001). Increased nitric oxide (NO) concentra-tions can sometimes be measured in cell culture or in animals after LLLTdue to its photo release from the mitochondria and Cox. It has been pro-posed that LLLT might work by photodissociating NO from Cox, therebyreversing the mitochondrial inhibition of respiration due to excessive NObinding (Lane 2006). Figure 4 illustrates the photodissociation of NOfrom its binding sites on the heme iron and copper centers where itcometively inhibits oxygen binding and reduces necessary enzymic activ-ity, thus allowing an immediate influx of oxygen and resumption of res-piration and generation of reactive oxygen species.
2.5. NO signaling
In addition to NO being photodissociated from Cox as described, itmay also be photo-released from other intracellular stores such as nitrosy-lated hemoglobin and nitrosylated myoglobin (Shiva and Gladwin 2009).Light mediated vasodilation was first described in 1968 by R F Furchgott,in his nitric oxide research that lead to his receipt of a Nobel Prize thirtyyears later in 1998 (Mitka 1998). Later studies conducted by otherresearchers confirmed and extended Furchgott’s early work and demon-strated the ability of light to influence the localized production or releaseof NO and stimulate vasodilation through the effect NO on cyclic guanine
Biphasic dose response in low level light therapy
FIGURE 3. Mitochondrial respiratory chain consisting of contains five complexes of integral mem-brane proteins: NADH dehydrogenase (Complex I), succinate dehydrogenase (Complex II),cytochrome c reductase (Complex III), cytochrome c oxidase (Complex IV), and ATP synthase(ComplexV).
monophosphate (cGMP). This finding suggested that properly designedillumination devices may be effective, noninvasive therapeutic agents forpatients who would benefit from increased localized NO availability
2.6. Reactive oxygen species and gene transcription
Reactive oxygen species (ROS) and reactive nitrogen species (RNS)are involved in the signaling pathways from mitochondria to nuclei.Reactive oxygen species (ROS) are very small molecules that include oxy-gen ions such as superoxide, free radicals such as hydroxyl radical, andhydrogen peroxide, and organic peroxides. They are highly with biologi-cal molecules such as proteins, nucleic acids and unsaturated lipids. ROSform as a natural by-product of the normal metabolism of oxygen andhave important roles in cell signaling (Storz 2007), regulating nucleicacid synthesis, protein synthesis, enzyme activation and cell cycle pro-gression (Brondon et al. 2005). LLLT was reported to produce a shift inoverall cell redox potential in the direction of greater oxidation (Karu1999) and increased ROS generation and cell redox activity have beendemonstrated (Alexandratou et al. 2002; Chen et al. 2009b; Grossman etal. 1998; Lavi et al. 2003; Lubart et al. 2005; Pal et al. 2007; Zhang et al.2008). These cytosolic responses may in turn induce transcriptionalchanges. Several transcription factors are regulated by changes in cellularredox state. But the most important one is nuclear factor B (NF-B).Figure 5 illustrates the effect of redox-sensitive transcription factor NF-κB
Y.-Y. Huang and others
FIGURE 4. When NO is released from its binding to heme iron and copper centers in cytochrome coxidase by the action of light, oxygen is allowed to rebind to these sites and respiration is restored toits former level leading to increased ATP synthesis.
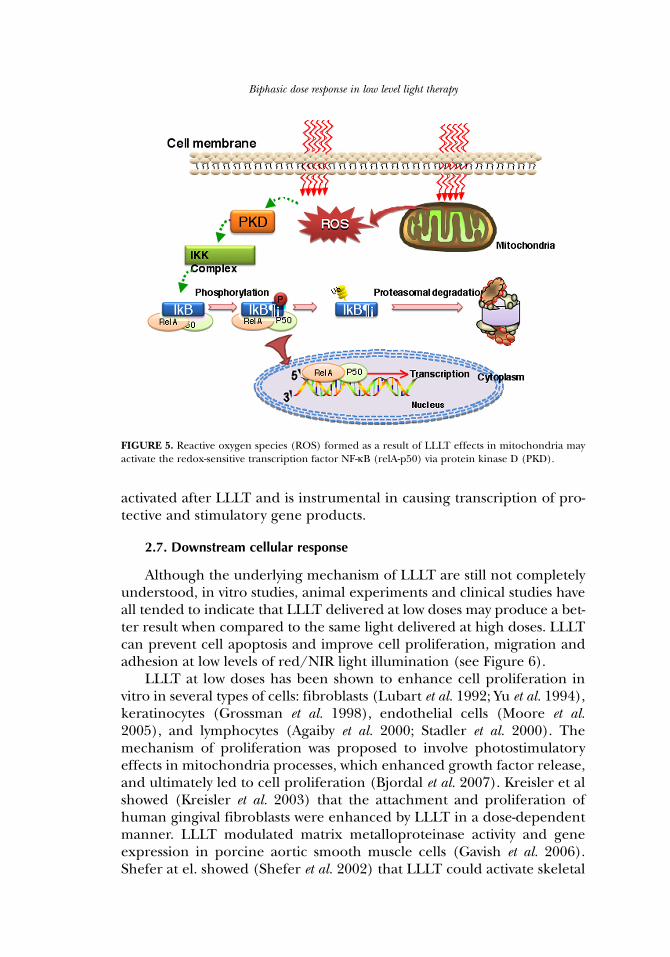
activated after LLLT and is instrumental in causing transcription of pro-tective and stimulatory gene products.
2.7. Downstream cellular response
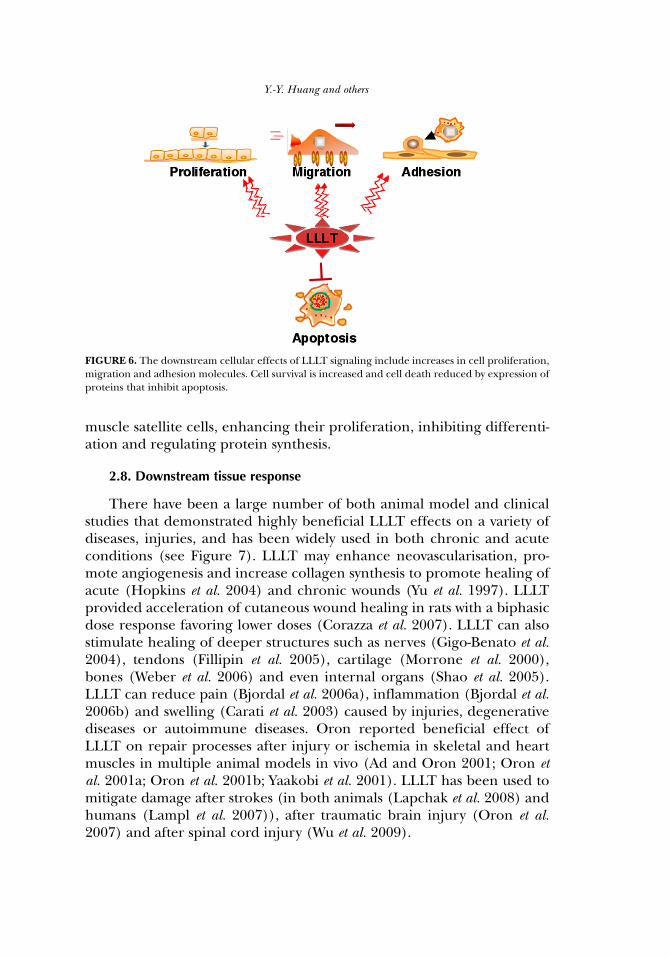
Although the underlying mechanism of LLLT are still not completelyunderstood, in vitro studies, animal experiments and clinical studies haveall tended to indicate that LLLT delivered at low doses may produce a bet-ter result when compared to the same light delivered at high doses. LLLTcan prevent cell apoptosis and improve cell proliferation, migration andadhesion at low levels of red/NIR light illumination (see Figure 6).
LLLT at low doses has been shown to enhance cell proliferation invitro in several types of cells: fibroblasts (Lubart et al. 1992; Yu et al. 1994),keratinocytes (Grossman et al. 1998), endothelial cells (Moore et al.2005), and lymphocytes (Agaiby et al. 2000; Stadler et al. 2000). Themechanism of proliferation was proposed to involve photostimulatoryeffects in mitochondria processes, which enhanced growth factor release,and ultimately led to cell proliferation (Bjordal et al. 2007). Kreisler et alshowed (Kreisler et al. 2003) that the attachment and proliferation ofhuman gingival fibroblasts were enhanced by LLLT in a dose-dependentmanner. LLLT modulated matrix metalloproteinase activity and geneexpression in porcine aortic smooth muscle cells (Gavish et al. 2006).Shefer at el. showed (Shefer et al. 2002) that LLLT could activate skeletal
Biphasic dose response in low level light therapy
FIGURE 5. Reactive oxygen species (ROS) formed as a result of LLLT effects in mitochondria mayactivate the redox-sensitive transcription factor NF-κB (relA-p50) via protein kinase D (PKD).
muscle satellite cells, enhancing their proliferation, inhibiting differenti-ation and regulating protein synthesis.
2.8. Downstream tissue response
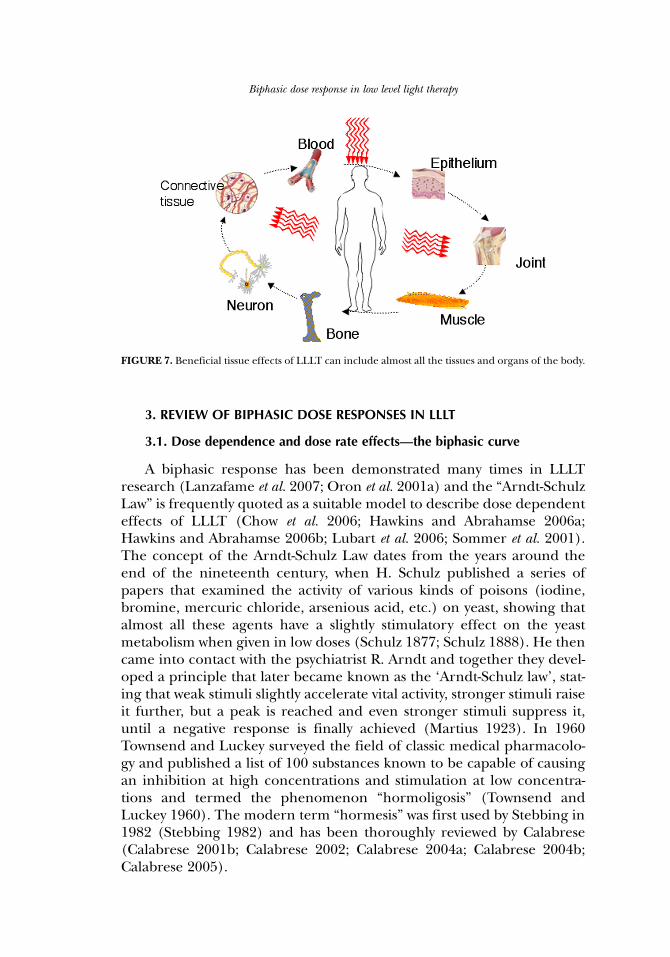
There have been a large number of both animal model and clinicalstudies that demonstrated highly beneficial LLLT effects on a variety ofdiseases, injuries, and has been widely used in both chronic and acuteconditions (see Figure 7). LLLT may enhance neovascularisation, pro-mote angiogenesis and increase collagen synthesis to promote healing ofacute (Hopkins et al. 2004) and chronic wounds (Yu et al. 1997). LLLTprovided acceleration of cutaneous wound healing in rats with a biphasicdose response favoring lower doses (Corazza et al. 2007). LLLT can alsostimulate healing of deeper structures such as nerves (Gigo-Benato et al.2004), tendons (Fillipin et al. 2005), cartilage (Morrone et al. 2000),bones (Weber et al. 2006) and even internal organs (Shao et al. 2005).LLLT can reduce pain (Bjordal et al. 2006a), inflammation (Bjordal et al.2006b) and swelling (Carati et al. 2003) caused by injuries, degenerativediseases or autoimmune diseases. Oron reported beneficial effect ofLLLT on repair processes after injury or ischemia in skeletal and heartmuscles in multiple animal models in vivo (Ad and Oron 2001; Oron etal. 2001a; Oron et al. 2001b; Yaakobi et al. 2001). LLLT has been used tomitigate damage after strokes (in both animals (Lapchak et al. 2008) andhumans (Lampl et al. 2007)), after traumatic brain injury (Oron et al.2007) and after spinal cord injury (Wu et al. 2009).
Y.-Y. Huang and others
FIGURE 6. The downstream cellular effects of LLLT signaling include increases in cell proliferation,migration and adhesion molecules. Cell survival is increased and cell death reduced by expression ofproteins that inhibit apoptosis.
3. REVIEW OF BIPHASIC DOSE RESPONSES IN LLLT
3.1. Dose dependence and dose rate effects—the biphasic curve
A biphasic response has been demonstrated many times in LLLTresearch (Lanzafame et al. 2007; Oron et al. 2001a) and the “Arndt-SchulzLaw” is frequently quoted as a suitable model to describe dose dependenteffects of LLLT (Chow et al. 2006; Hawkins and Abrahamse 2006a;Hawkins and Abrahamse 2006b; Lubart et al. 2006; Sommer et al. 2001).The concept of the Arndt-Schulz Law dates from the years around theend of the nineteenth century, when H. Schulz published a series ofpapers that examined the activity of various kinds of poisons (iodine,bromine, mercuric chloride, arsenious acid, etc.) on yeast, showing thatalmost all these agents have a slightly stimulatory effect on the yeastmetabolism when given in low doses (Schulz 1877; Schulz 1888). He thencame into contact with the psychiatrist R. Arndt and together they devel-oped a principle that later became known as the ‘Arndt-Schulz law’, stat-ing that weak stimuli slightly accelerate vital activity, stronger stimuli raiseit further, but a peak is reached and even stronger stimuli suppress it,until a negative response is finally achieved (Martius 1923). In 1960Townsend and Luckey surveyed the field of classic medical pharmacolo-gy and published a list of 100 substances known to be capable of causingan inhibition at high concentrations and stimulation at low concentra-tions and termed the phenomenon “hormoligosis” (Townsend andLuckey 1960). The modern term “hormesis” was first used by Stebbing in1982 (Stebbing 1982) and has been thoroughly reviewed by Calabrese(Calabrese 2001b; Calabrese 2002; Calabrese 2004a; Calabrese 2004b;Calabrese 2005).
Biphasic dose response in low level light therapy
FIGURE 7. Beneficial tissue effects of LLLT can include almost all the tissues and organs of the body.
In the context of LLLT the increasing “stimulus” may be irradiationtime or increased irradiance. This non-linear effect contradicts theBunsen-Roscoe rule of reciprocity (which was originally formulated forvisual detection of light by photoreceptors (Brindley 1952)), which pre-dicts that if the products of exposure time in seconds and irradiance inmW/cm2 are equal, i.e. the energy density is the same, then the changesin biological endpoint will be equal. This inverse linear relationshipbetween irradiance and time has frequently failed in LLLT research(Karu and Kolyakov 2005; Lubart et al. 2006).
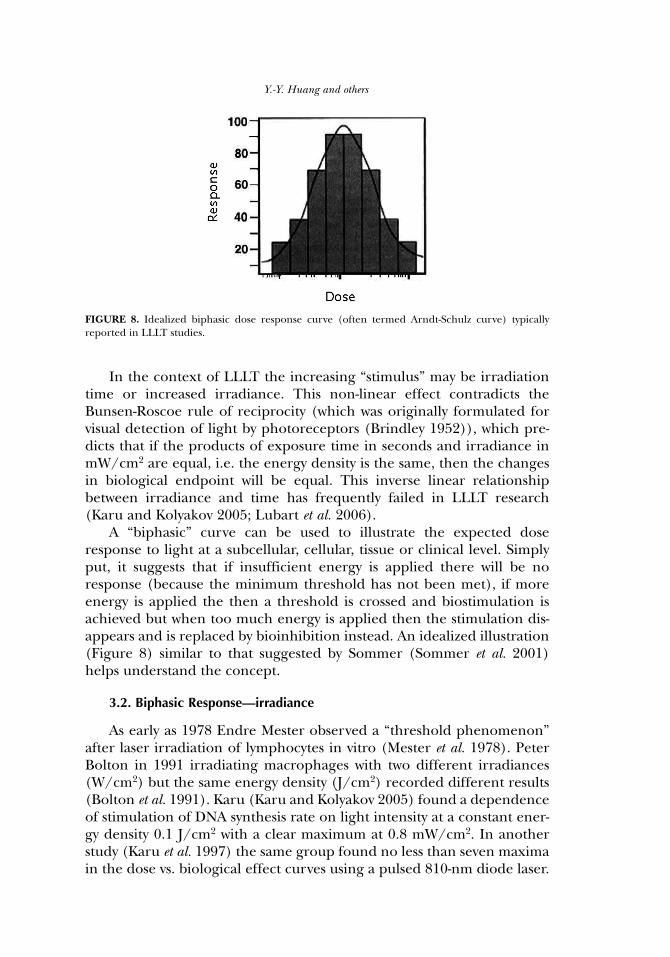
A “biphasic” curve can be used to illustrate the expected doseresponse to light at a subcellular, cellular, tissue or clinical level. Simplyput, it suggests that if insufficient energy is applied there will be noresponse (because the minimum threshold has not been met), if moreenergy is applied the then a threshold is crossed and biostimulation isachieved but when too much energy is applied then the stimulation dis-appears and is replaced by bioinhibition instead. An idealized illustration(Figure 8) similar to that suggested by Sommer (Sommer et al. 2001)helps understand the concept.
3.2. Biphasic Response—irradiance
As early as 1978 Endre Mester observed a “threshold phenomenon”after laser irradiation of lymphocytes in vitro (Mester et al. 1978). PeterBolton in 1991 irradiating macrophages with two different irradiances(W/cm2) but the same energy density (J/cm2) recorded different results(Bolton et al. 1991). Karu (Karu and Kolyakov 2005) found a dependenceof stimulation of DNA synthesis rate on light intensity at a constant ener-gy density 0.1 J/cm2 with a clear maximum at 0.8 mW/cm2. In anotherstudy (Karu et al. 1997) the same group found no less than seven maximain the dose vs. biological effect curves using a pulsed 810-nm diode laser.
Y.-Y. Huang and others
FIGURE 8. Idealized biphasic dose response curve (often termed Arndt-Schulz curve) typicallyreported in LLLT studies.
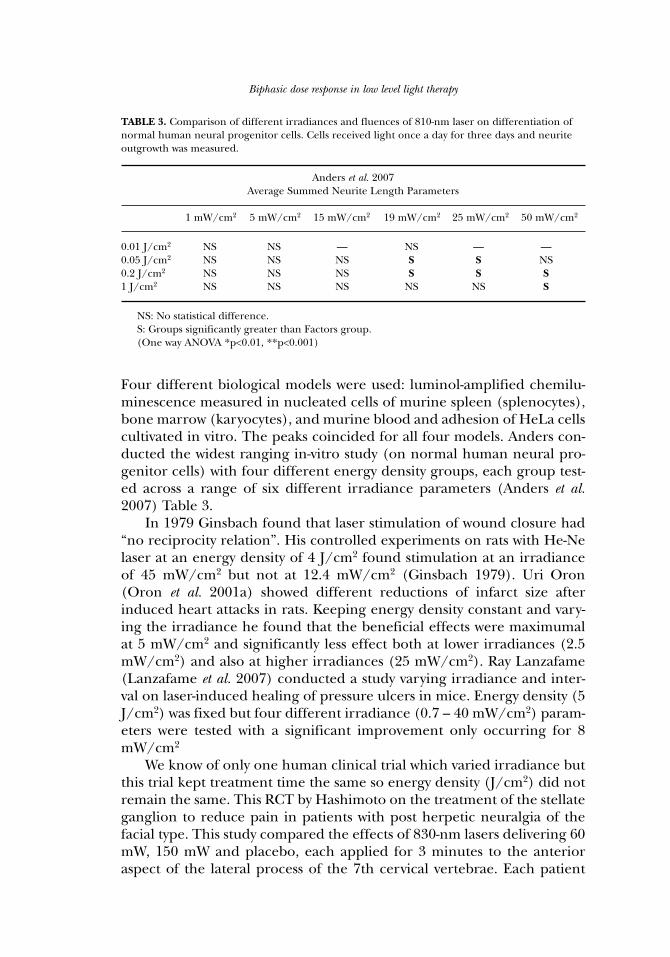
Four different biological models were used: luminol-amplified chemilu-minescence measured in nucleated cells of murine spleen (splenocytes),bone marrow (karyocytes), and murine blood and adhesion of HeLa cellscultivated in vitro. The peaks coincided for all four models. Anders con-ducted the widest ranging in-vitro study (on normal human neural pro-genitor cells) with four different energy density groups, each group test-ed across a range of six different irradiance parameters (Anders et al.2007) Table 3.
In 1979 Ginsbach found that laser stimulation of wound closure had“no reciprocity relation”. His controlled experiments on rats with He-Nelaser at an energy density of 4 J/cm2 found stimulation at an irradianceof 45 mW/cm2 but not at 12.4 mW/cm2 (Ginsbach 1979). Uri Oron(Oron et al. 2001a) showed different reductions of infarct size afterinduced heart attacks in rats. Keeping energy density constant and vary-ing the irradiance he found that the beneficial effects were maximumalat 5 mW/cm2 and significantly less effect both at lower irradiances (2.5mW/cm2) and also at higher irradiances (25 mW/cm2). Ray Lanzafame(Lanzafame et al. 2007) conducted a study varying irradiance and inter-val on laser-induced healing of pressure ulcers in mice. Energy density (5J/cm2) was fixed but four different irradiance (0.7 – 40 mW/cm2) param-eters were tested with a significant improvement only occurring for 8mW/cm2
We know of only one human clinical trial which varied irradiance butthis trial kept treatment time the same so energy density (J/cm2) did notremain the same. This RCT by Hashimoto on the treatment of the stellateganglion to reduce pain in patients with post herpetic neuralgia of thefacial type. This study compared the effects of 830-nm lasers delivering 60mW, 150 mW and placebo, each applied for 3 minutes to the anterioraspect of the lateral process of the 7th cervical vertebrae. Each patient
Biphasic dose response in low level light therapy
TABLE 3. Comparison of different irradiances and fluences of 810-nm laser on differentiation ofnormal human neural progenitor cells. Cells received light once a day for three days and neuriteoutgrowth was measured.
Anders et al. 2007Average Summed Neurite Length Parameters
1 mW/cm2 5 mW/cm2 15 mW/cm2 19 mW/cm2 25 mW/cm2 50 mW/cm2
0.01 J/cm2 NS NS — NS — —0.05 J/cm2 NS NS NS S S NS0.2 J/cm2 NS NS NS S S S1 J/cm2 NS NS NS NS NS S
NS: No statistical difference. S: Groups significantly greater than Factors group. (One way ANOVA *p<0.01, **p<0.001)

had three treatments (one treatment, three consecutive days), each treat-ment was with a different laser or placebo. The study was properly blind-ed and randomized. There was a significant difference in skin tempera-ture of the forehead and in recorded pain scores. The greatest improve-ments were for the 150mW laser (Hashimoto et al. 1997).
There have been several systematic reviews and meta analyses of RCTsand these have revealed some irradiance dependant effects: Bjordal pub-lished a review of LLLT for chronic joint disorders and identified 14 RCTsof suitable methodological quality, 4 of which failed to report a significanteffect because the irradiance was either too high or too low, and/or deliv-ered insufficient energy, the remaining eight studies all produced positiveeffects (Bjordal et al. 2003). Tumilty reviewed 25 LLLT RCTs oftendinopathies,13 of which (55%) failed to produce a positive outcome,all of these negative/inconclusive studies that recorded irradiance (orcould subsequently be established) had delivered an irradiance in excessof the guidelines set by the World Association for Laser Therapy(www.walt.nu) (Tumilty et al. 2009).
3.3. Biphasic Response—time or energy density
Again, Peter Bolton’s study mentioned in 3.2 above had an energydensity aspect showing a different response for each of the irradiancesused. For the 400mW/cm2 study he found increasing energy density from2.4 J/cm2 to 7.2 J/cm2 increased fibroblast proliferation, in the 800mW/cm2 group increasing energy density from 2.4 J/cm2 to 7.2 J/cm2
decreased fibroblast proliferation (Bolton et al. 1991). Anders’ study alsomentioned in 3.2 above looked at four energy density groups, and for theirradiance parameters that produced significant results increasing energydensity increased neurite length (Anders et al. 2007) Table 3. Yamaura andcolleagues found a biphasic dose response in MTT activity in rheumatoidarthritis synoviocytes after 810-nm laser with a peak at 8 J/cm2 and lesseffect at lower and higher fluences (Yamaura et al. 2009). Loevschall meas-ured human oral mucosal fibroblast cell proliferation by incorporation oftritiated thymidine after varying fluences of 812-nm laser delivered at 4.5mW/cm2 and found a biphasic dose response with a distinct peak at 0.45J/cm2 (Loevschall and Arenholt-Bindslev 1994). Another study (al-Watbanand Andres 2001) looked at chinese hamster ovary and human fibroblastproliferation after various fluences of He-Ne laser delivered at a constantirradiance of 1.25 mW/cm2. Again they found a clear biphasic doseresponse with a peak at 0.18 J/cm2. Zhang et al (Zhang et al. 2003) founda biphasic dose response in human fibroblast cell numbers after treatmentwith varying fluences of 628-nm light, with a maximum increase of 30%after 0.88 J/cm2 and an actual reduction appearing at 9 J/cm2. Brondonand colleagues (Brondon et al. 2005) found that two treatments per day
Y.-Y. Huang and others

caused a bigger increase than 1 or 4 treatments per day measuring prolif-eration index in human HEP-2 and murine L-929 cell lines. They used a670 nm light emitting diode device with an irradiance of 10 mW /cm2 andeach single treatment was 5 J/cm2 and the course was stopped after 50J/cm2 had been given (at 10, 5 or 2.5 days).
Lopes-Martins showed a biphasic response to LLLT on the number ofmononuclear cells that accumulate in pleural cavity after carrageenaninjection. The results showed neutrophil influx mice treated with threedifferent laser fluencies at 1, 2.5 & 5 J/cm2) with 2.5 having the greatesteffect (Lopes-Martins et al. 2005).
As stated in 3.2 above, Hashimoto reported on the laser treatment ofthe stellate ganglion to reduce pain in patients with post herpetic neu-ralgia of the facial type. The study compared the effects of 830-nm lasersdelivering 60mW, 150mW and placebo, The greatest improvements werefor the 150mW laser (Hashimoto et al. 1997). Again as stated in 3.2 above,there have been several systematic reviews and meta analyses of RCTs andthese revealed some energy density dependant effects (Bjordal et al. 2003;Tumilty et al. 2009).
3.4. Beam measurement reporting errors
One notable aspect of the dose rate (W/cm2) studies is the wide vari-ation of “optimal” irradiances in vitro studies as they range from 1-800mW/cm2 in just the few papers referenced in this review. If the primaryphoto acceptor is cytochrome C oxidase as postulated here, then whywould so many authors arrive at different conclusions for optimal param-eters in vitro, should it not be the same for all of them?
Explanations may include, the slightly different wavelengths used orsensitivity due the redox state of mitochondia in the target cells (Tafurand Mills 2008), but we consider that the greater contributor may be laserbeam measurement problems. It may be a surprise to non-physicists thatdiode laser beams are not inherently round, and even if circularizinglenses are used to correct this, then the beam intensity distribution is nothomogeneous. Laser beams are brighter (higher irradiance) in the mid-dle and weaker towards the edge. Cells in the centre of a culture well willbe exposed to considerably higher irradiances than those on the periph-ery. Because the edge of a laser beam is hard to define and find this couldmean that irradiance calculations are significantly different betweenresearch centers. Agreement on beam measurement and reporting ofintensity distribution is needed to reduce these inconsistencies. This isimportant not only for in vitro studies but also in vivo and clinical trials asreporting of irradiance is just as important though we accept that tissuescattering diffuses the beam probably making non-homogenous sourcesless critical to clinical effectiveness.
Biphasic dose response in low level light therapy
4. BIPHASIC LLLT DOSE RESPONSE STUDIES IN OUR LABORATORY
4.1. In vitro activation of NF-κB
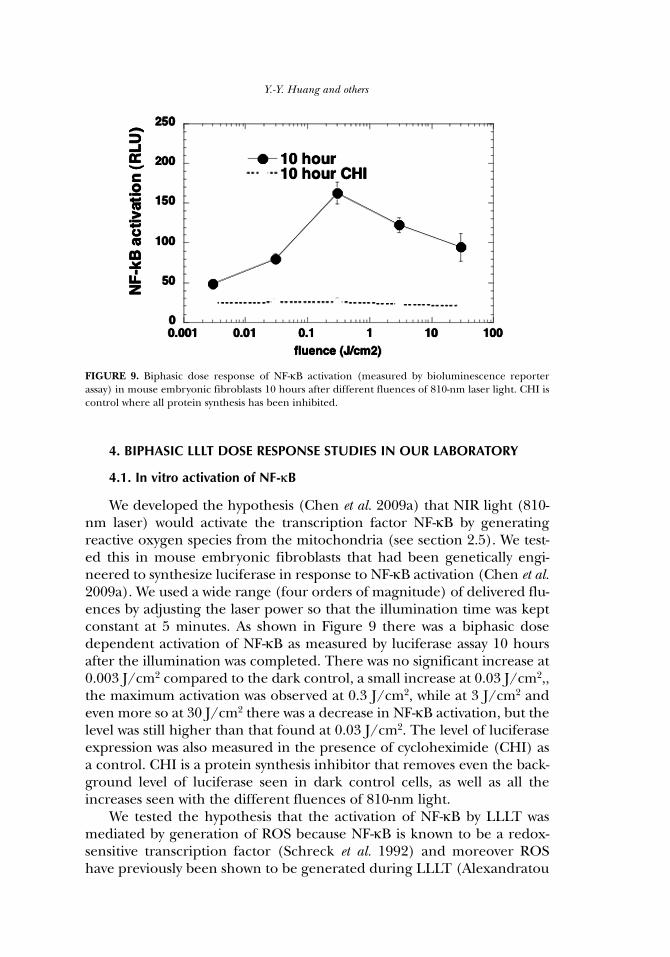
We developed the hypothesis (Chen et al. 2009a) that NIR light (810-nm laser) would activate the transcription factor NF-κB by generatingreactive oxygen species from the mitochondria (see section 2.5). We test-ed this in mouse embryonic fibroblasts that had been genetically engi-neered to synthesize luciferase in response to NF-κB activation (Chen et al.2009a). We used a wide range (four orders of magnitude) of delivered flu-ences by adjusting the laser power so that the illumination time was keptconstant at 5 minutes. As shown in Figure 9 there was a biphasic dosedependent activation of NF-κB as measured by luciferase assay 10 hoursafter the illumination was completed. There was no significant increase at0.003 J/cm2 compared to the dark control, a small increase at 0.03 J/cm2,,the maximum activation was observed at 0.3 J/cm2, while at 3 J/cm2 andeven more so at 30 J/cm2 there was a decrease in NF-κB activation, but thelevel was still higher than that found at 0.03 J/cm2. The level of luciferaseexpression was also measured in the presence of cycloheximide (CHI) asa control. CHI is a protein synthesis inhibitor that removes even the back-ground level of luciferase seen in dark control cells, as well as all theincreases seen with the different fluences of 810-nm light.
We tested the hypothesis that the activation of NF-κB by LLLT wasmediated by generation of ROS because NF-κB is known to be a redox-sensitive transcription factor (Schreck et al. 1992) and moreover ROShave previously been shown to be generated during LLLT (Alexandratou
Y.-Y. Huang and others
FIGURE 9. Biphasic dose response of NF-κB activation (measured by bioluminescence reporterassay) in mouse embryonic fibroblasts 10 hours after different fluences of 810-nm laser light. CHI iscontrol where all protein synthesis has been inhibited.
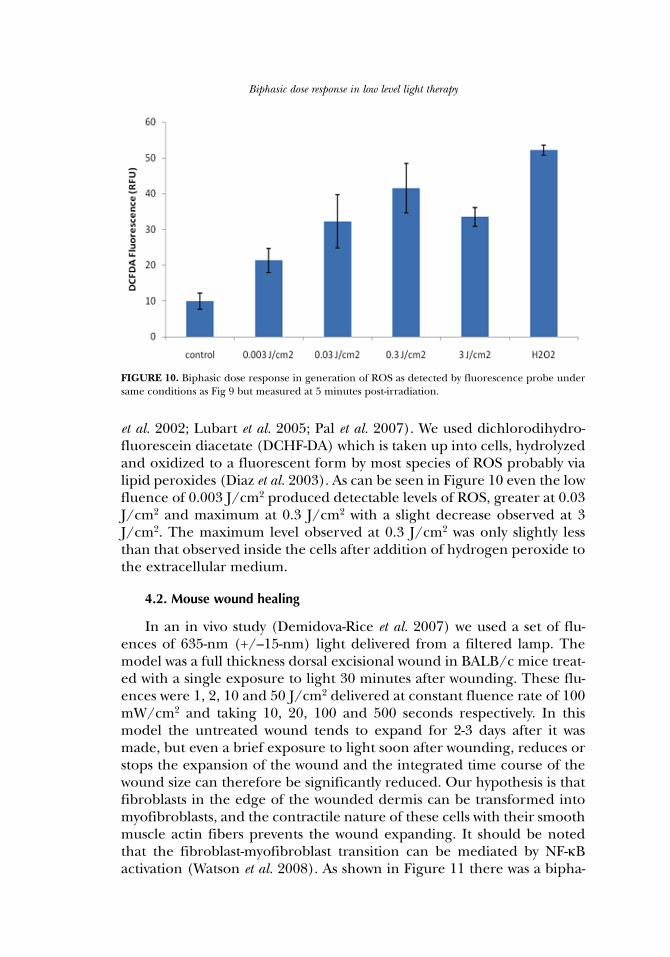
et al. 2002; Lubart et al. 2005; Pal et al. 2007). We used dichlorodihydro-fluorescein diacetate (DCHF-DA) which is taken up into cells, hydrolyzedand oxidized to a fluorescent form by most species of ROS probably vialipid peroxides (Diaz et al. 2003). As can be seen in Figure 10 even the lowfluence of 0.003 J/cm2 produced detectable levels of ROS, greater at 0.03J/cm2 and maximum at 0.3 J/cm2 with a slight decrease observed at 3J/cm2. The maximum level observed at 0.3 J/cm2 was only slightly lessthan that observed inside the cells after addition of hydrogen peroxide tothe extracellular medium.
4.2. Mouse wound healing
In an in vivo study (Demidova-Rice et al. 2007) we used a set of flu-ences of 635-nm (+/–15-nm) light delivered from a filtered lamp. Themodel was a full thickness dorsal excisional wound in BALB/c mice treat-ed with a single exposure to light 30 minutes after wounding. These flu-ences were 1, 2, 10 and 50 J/cm2 delivered at constant fluence rate of 100mW/cm2 and taking 10, 20, 100 and 500 seconds respectively. In thismodel the untreated wound tends to expand for 2-3 days after it wasmade, but even a brief exposure to light soon after wounding, reduces orstops the expansion of the wound and the integrated time course of thewound size can therefore be significantly reduced. Our hypothesis is thatfibroblasts in the edge of the wounded dermis can be transformed intomyofibroblasts, and the contractile nature of these cells with their smoothmuscle actin fibers prevents the wound expanding. It should be notedthat the fibroblast-myofibroblast transition can be mediated by NF-κBactivation (Watson et al. 2008). As shown in Figure 11 there was a bipha-
Biphasic dose response in low level light therapy
FIGURE 10. Biphasic dose response in generation of ROS as detected by fluorescence probe undersame conditions as Fig 9 but measured at 5 minutes post-irradiation.
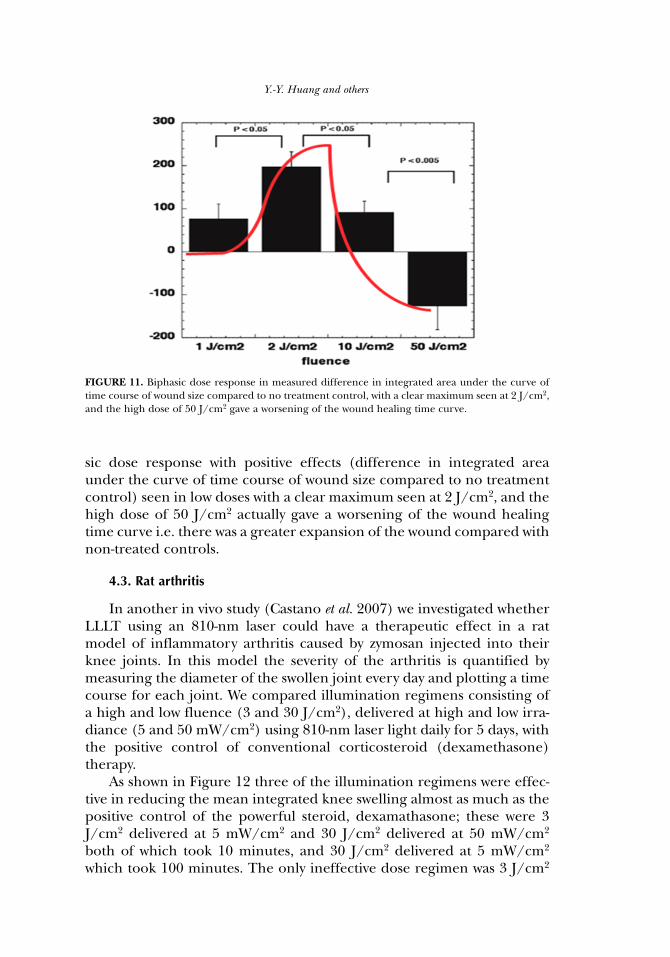
sic dose response with positive effects (difference in integrated areaunder the curve of time course of wound size compared to no treatmentcontrol) seen in low doses with a clear maximum seen at 2 J/cm2, and thehigh dose of 50 J/cm2 actually gave a worsening of the wound healingtime curve i.e. there was a greater expansion of the wound compared withnon-treated controls.
4.3. Rat arthritis
In another in vivo study (Castano et al. 2007) we investigated whetherLLLT using an 810-nm laser could have a therapeutic effect in a ratmodel of inflammatory arthritis caused by zymosan injected into theirknee joints. In this model the severity of the arthritis is quantified bymeasuring the diameter of the swollen joint every day and plotting a timecourse for each joint. We compared illumination regimens consisting ofa high and low fluence (3 and 30 J/cm2), delivered at high and low irra-diance (5 and 50 mW/cm2) using 810-nm laser light daily for 5 days, withthe positive control of conventional corticosteroid (dexamethasone)therapy.
As shown in Figure 12 three of the illumination regimens were effec-tive in reducing the mean integrated knee swelling almost as much as thepositive control of the powerful steroid, dexamathasone; these were 3J/cm2 delivered at 5 mW/cm2 and 30 J/cm2 delivered at 50 mW/cm2
both of which took 10 minutes, and 30 J/cm2 delivered at 5 mW/cm2
which took 100 minutes. The only ineffective dose regimen was 3 J/cm2
Y.-Y. Huang and others
FIGURE 11. Biphasic dose response in measured difference in integrated area under the curve oftime course of wound size compared to no treatment control, with a clear maximum seen at 2 J/cm2,and the high dose of 50 J/cm2 gave a worsening of the wound healing time curve.
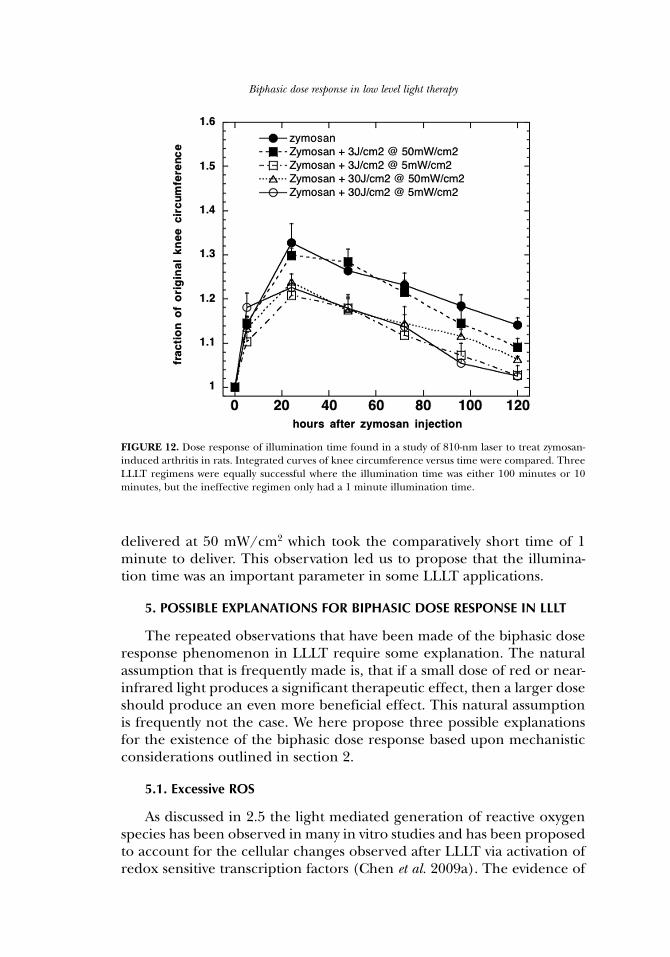
delivered at 50 mW/cm2 which took the comparatively short time of 1minute to deliver. This observation led us to propose that the illumina-tion time was an important parameter in some LLLT applications.
5. POSSIBLE EXPLANATIONS FOR BIPHASIC DOSE RESPONSE IN LLLT
The repeated observations that have been made of the biphasic doseresponse phenomenon in LLLT require some explanation. The naturalassumption that is frequently made is, that if a small dose of red or near-infrared light produces a significant therapeutic effect, then a larger doseshould produce an even more beneficial effect. This natural assumptionis frequently not the case. We here propose three possible explanationsfor the existence of the biphasic dose response based upon mechanisticconsiderations outlined in section 2.
5.1. Excessive ROS
As discussed in 2.5 the light mediated generation of reactive oxygenspecies has been observed in many in vitro studies and has been proposedto account for the cellular changes observed after LLLT via activation ofredox sensitive transcription factors (Chen et al. 2009a). The evidence of
Biphasic dose response in low level light therapy
FIGURE 12. Dose response of illumination time found in a study of 810-nm laser to treat zymosan-induced arthritis in rats. Integrated curves of knee circumference versus time were compared. ThreeLLLT regimens were equally successful where the illumination time was either 100 minutes or 10minutes, but the ineffective regimen only had a 1 minute illumination time.
ROS mediated activation of NF-κB in MEF cells presented in 4.1 providesadditional support for this hypothesis (Chen et al. 2009a). It is well-accept-ed that ROS can have both beneficial and harmful effects (Huang andZheng 2006). Hydrogen peroxide is often used to kill cells in vitro (Imlay2008). Other ROS such as singlet oxygen (Klotz et al. 2003) and hydroxylradicals (Pryor et al. 2006) are thought to be harmful even at low con-centrations. The concept of biphasic dose response in fact is well estab-lished in the field of oxidative stress (Day and Suzuki 2005). If the gener-ation of ROS can be shown to be dose dependent on the delivered ener-gy fluence this may provide an explanation for the stimulation and inhi-bition observed with low and high light fluences.
5.2. Excessive NO
The other mechanistic hypothesis that is put forward to explain thecellular effects of LLLT relates to the photolysis of nitrosylated proteinsthat releases free NO (see section 2.6). Again the literature has manypapers that discuss the so-called two-faced or “Janus” molecule NO(Anggard 1994; Lane and Gross 1999). NO can be either protective orharmful depending on the dose and particularly on the cell or tissue typewhere it is generated (Calabrese 2001a).
5.3. Activation of a cytotoxic pathway
The third hypothesis to explain the biphasic dose response of LLLTis the idea that the protective and stimulatory effects of light occur at lowdoses, but there is an additional pathway that leads to damaging effects oflight that only occurs at high doses, and effectively overwhelms the ben-eficial effects of low doses of light. Work from South China NormalUniversity provides some support for this hypothesis. Low doses of LLLTwere found to phosphorylate hepatocyte growth factor receptor (c-Met),and initiate signaling via cyclic AMP and Jun kinase and Src (Gao andXing 2009). By contrast, high dose LLLT was found to induce apoptosisvia a mitochondrial caspase-3 pathway and cytochrome c release wasattributed to opening of the mitochondrial permeability transition porecaused by high-level intracellular reactive oxygen species (ROS) genera-tion (Wu et al. 2009). A secondary signaling pathway through Bax activa-tion was observed (Wu et al. 2009).
6. SUMMARY AND CONCLUSION
LLLT delivered at low doses tends to work better than the same wave-length delivered at high levels, which illustrates the basic concept of bipha-sic dose response or hormesis (Calabrese 2001b). In general, fluences ofred or NIR as low as 3 or 5 J/cm2 will be beneficial in vivo, but a large dose
Y.-Y. Huang and others

like 50 or 100 J/cm2 will lose the beneficial effect and may even becomedetrimental. The molecular and cellular mechanisms LLLT suggest thatphotons are absorbed by the mitochondria; they stimulate more ATP pro-duction and low levels of ROS, which then activates transcription factors,such as NF-κB, to induce many gene transcript products responsible forthe beneficial effects of LLLT. ROS are well known to stimulate cellularproliferation of low levels, but inhibit proliferation and kill cells at highlevels. Nitric oxide is also involved in LLLT, and may be photo-releasedfrom its binding sites in the respiratory chain and elsewhere. It is possiblethat NO release in low amounts by low dose light may be beneficial, whilehigh levels released by high dose LLLT may be damaging. The third pos-sibility is that LLLT may activate transcription factors, upregulating pro-tective proteins which are anti-apoptotic, and generally promote cell sur-vival. In contrast, it is entirely possible that different transcription factorsand cell-signaling pathways, that promote apoptosis, could be activatedafter higher light exposure. We believe that further advances in the mech-anistic understanding of LLLT will continue to be made in the nearfuture. These advances will lead to greater acceptance of LLLT in main-stream medicine and may lead to LLLT being used for serious diseasessuch as stroke, heart attack and degenerative brain diseases. Neverthelessthe concept of biphasic dose response or LLLT hormesis (low levels oflight are good for you, while high levels are bad for you) will remain.
ACKNOWLEDGMENTS
Research in the Hamblin laboratory is supported by the US NIH(grants R01CA/AI838801 and R01AI050875 to MRH).
REFERENCES
Ad N and Oron U. 2001. Impact of low level laser irradiation on infarct size in the rat followingmyocardial infarction. Int J Cardiol 80:109-16.
Agaiby AD, Ghali LR, Wilson R, and Dyson M. 2000. Laser modulation of angiogenic factor produc-tion by T-lymphocytes. Lasers Surg Med 26:357-63.
Aimbire F, Albertini R, Pacheco MT, Castro-Faria-Neto HC, Leonardo PS, Iversen VV, Lopes-MartinsRA, and Bjordal JM. 2006. Low-level laser therapy induces dose-dependent reduction ofTNFalpha levels in acute inflammation. Photomed Laser Surg 24:33-7.
al-Watban FA and Andres BL. 2001. The effect of He-Ne laser (632.8 nm) and Solcoseryl in vitro.Lasers Med Sci 16:267-75.
Alexandratou E, Yova D, Handris P, Kletsas D, and Loukas S. 2002. Human fibroblast alterationsinduced by low power laser irradiation at the single cell level using confocal microscopy.Photochem Photobiol Sci 1:547-52.
Anders J, Romanczyk T, Moges H, Ilev I, Waynant R, and Longo L. 2007. Light Interaction WithHuman Central Nervous System Progenitor Cells. NAALT conference proceedings. 2007
Anggard E. 1994. Nitric oxide: mediator, murderer, and medicine. Lancet 343:1199-206.Basford JR, Sheffield CG, and Harmsen WS. 1999. Laser therapy: a randomized, controlled trial of
the effects of low-intensity Nd:YAG laser irradiation on musculoskeletal back pain. Arch PhysMed Rehabil 80:647-52.
Bertolucci LE and Grey T. 1995. Clinical analysis of mid-laser versus placebo treatment of arthralgicTMJ degenerative joints. Cranio 13:26-9.
Biphasic dose response in low level light therapy
Bjordal JM, Couppe C, Chow RT, Tuner J, and Ljunggren EA. 2003. A systematic review of low levellaser therapy with location-specific doses for pain from chronic joint disorders. Aust J Physiother49:107-16.
Bjordal JM, Johnson MI, Iversen V, Aimbire F, and Lopes-Martins RA. 2006a. Photoradiation in acutepain: a systematic review of possible mechanisms of action and clinical effects in randomizedplacebo-controlled trials. Photomed Laser Surg 24:158-68.
Bjordal JM, Johnson MI, Lopes-Martins RA, Bogen B, Chow R, and Ljunggren AE. 2007. Short-termefficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials. BMC Musculoskelet Disord 8:51.
Bjordal JM, Lopes-Martins RA, and Iversen VV. 2006b. A randomised, placebo controlled trial of lowlevel laser therapy for activated Achilles tendinitis with microdialysis measurement of peri-tendinous prostaglandin E2 concentrations. Br J Sports Med 40:76-80; discussion 76-80.
Bolton P, Young S, and Dyson M. 1991. Macrophage responsiveness to light therapy with varyingpower and energy densities. Laser Ther 3:6-9.
Brindley GS. 1952. The Bunsen-Roscoe law for the human eye at very short durations. J Physiol118:135–139.
Brondon P, Stadler I, and Lanzafame RJ. 2005. A study of the effects of phototherapy dose intervalon photobiomodulation of cell cultures. Lasers Surg Med 36:409-13.
Brown GC. 2001. Regulation of mitochondrial respiration by nitric oxide inhibition of cytochrome coxidase. Biochim Biophys Acta 1504:46-57.
Caetano KS, Frade MA, Minatel DG, Santana LA, and Enwemeka CS. 2009. Phototherapy ImprovesHealing of Chronic Venous Ulcers. Photomed Laser Surg
Calabrese EJ. 2001a. Nitric oxide: biphasic dose responses. Crit Rev Toxicol 31:489-501.Calabrese EJ. 2001b. The future of hormesis: where do we go from here? Crit Rev Toxicol 31:637-48.Calabrese EJ. 2002. Hormesis: changing view of the dose-response, a personal account of the history
and current status. Mutat Res 511:181-9.Calabrese EJ. 2004a. Hormesis: a revolution in toxicology, risk assessment and medicine. EMBO Rep
5 Spec No:S37-40.Calabrese EJ. 2004b. Hormesis: from marginalization to mainstream: a case for hormesis as the
default dose-response model in risk assessment. Toxicol Appl Pharmacol 197:125-36.Calabrese EJ. 2005. Hormetic dose-response relationships in immunology: occurrence, quantitative
features of the dose response, mechanistic foundations, and clinical implications. Crit RevToxicol 35:89-295.
Carati CJ, Anderson SN, Gannon BJ, and Piller NB. 2003. Treatment of postmastectomy lymphede-ma with low-level laser therapy: a double blind, placebo-controlled trial. Cancer 98:1114-22.
Castano AP, Dai T, Yaroslavsky I, Cohen R, Apruzzese WA, Smotrich MH, and Hamblin MR. 2007.Low-level laser therapy for zymosan-induced arthritis in rats: Importance of illumination time.Lasers Surg Med 39:543-50.
Chen AC-H, Arany PR, Huang Y-Y, Tomkinson EM, Saleem T, Yull FE, Blackwell TS, and HamblinMR. (2009a). Low level laser therapy activates NF-κB via generation of reactive oxygen speciesin mouse embryonic fibroblasts. In Mechanisms for Low-Light Therapy IV, Hamblin, M.R.,Anders, J.J. & Waynant, R.W. (eds), Vol. 7165. pp. doi: 10.1117/12.809605. The InternationalSociety for Optical Engineering, Bellingham, WA, : San Jose.
Chen AC-H, Arany PR, Huang YY, Tomkinson EM, Saleem T, Yull FE, Blackwell TS, and Hamblin MR.2009b. Low level laser therapy activates NF-κB via generation of reactive oxygen species inmouse embryonic fibroblasts. Proc SPIE in press:
Chow RT, Heller GZ, and Barnsley L. 2006. The effect of 300 mW, 830 nm laser on chronic neck pain:a double-blind, randomized, placebo-controlled study. Pain 124:201-10.
Corazza AV, Jorge J, Kurachi C, and Bagnato VS. 2007. Photobiomodulation on the angiogenesis ofskin wounds in rats using different light sources. Photomed Laser Surg 25:102-6.
Day RM and Suzuki YJ. 2005. Cell proliferation, reactive oxygen and cellular glutathione. DoseResponse 3:425-42.
Demidova-Rice TN, Salomatina EV, Yaroslavsky AN, Herman IM, and Hamblin MR. 2007. Low-levellight stimulates excisional wound healing in mice. Lasers Surg Med 39:706-15.
Diaz G, Liu S, Isola R, Diana A, and Falchi AM. 2003. Mitochondrial localization of reactive oxygenspecies by dihydrofluorescein probes. Histochem Cell Biol 120:319-25.
Y.-Y. Huang and others
Fillipin LI, Mauriz JL, Vedovelli K, Moreira AJ, Zettler CG, Lech O, Marroni NP, and Gonzalez-Gallego J. 2005. Low-level laser therapy (LLLT) prevents oxidative stress and reduces fibrosis inrat traumatized Achilles tendon. Lasers Surg Med 37:293-300.
Gao X and Xing D. 2009. Molecular mechanisms of cell proliferation induced by low power laser irra-diation. J Biomed Sci 16:4.
Gavish L, Perez L, and Gertz SD. 2006. Low-level laser irradiation modulates matrix metalloproteinaseactivity and gene expression in porcine aortic smooth muscle cells. Lasers Surg Med 38:779-86.
Gigo-Benato D, Geuna S, de Castro Rodrigues A, Tos P, Fornaro M, Boux E, Battiston B, andGiacobini-Robecchi MG. 2004. Low-power laser biostimulation enhances nerve repair after end-to-side neurorrhaphy: a double-blind randomized study in the rat median nerve model. LasersMed Sci 19:57-65.
Ginsbach G. 1979. Laser induced stimulation of woundhealing in bad healing wounds. Proc Laser '79Opto Elektronics Conf Munich. IPC Science and Technology Press Guildford UK 5.
Goncalves WL, Souza FM, Conti CL, Cirqueira JP, Rocha WA, Pires JG, Barros LA, and Moyses MR.2007. Influence of He-Ne laser therapy on the dynamics of wound healing in mice treated withanti-inflammatory drugs. Braz J Med Biol Res 40:877-84.
Greco M, Guida G, Perlino E, Marra E, and Quagliariello E. 1989. Increase in RNA and protein synthesisby mitochondria irradiated with helium-neon laser. Biochem Biophys Res Commun 163:1428-34.
Grossman N, Schneid N, Reuveni H, Halevy S, and Lubart R. 1998. 780 nm low power diode laserirradiation stimulates proliferation of keratinocyte cultures: involvement of reactive oxygenspecies. Lasers Surg Med 22:212-8.
Gupta AK, Filonenko N, Salansky N, and Sauder DN. 1998. The use of low energy photon therapy(LEPT) in venous leg ulcers: a double-blind, placebo-controlled study. Dermatol Surg 24:1383-6.
Gur A, Sarac AJ, Cevik R, Altindag O, and Sarac S. 2004. Efficacy of 904 nm gallium arsenide low levellaser therapy in the management of chronic myofascial pain in the neck: a double-blind andrandomize-controlled trial. Lasers Surg Med 35:229-35.
Hashimoto K, Kemmotsu O, Otsuka H, Numazawa R, and Ohta Y. 1997. Efficacy of laser irradiationon the area near the stellate ganglion is dose-dependent: a double-blind crossover placebo-con-trolled study. Laser Therapy 7:5.
Hawkins D and Abrahamse H. 2006a. Effect of multiple exposures of low-level laser therapy on thecellular responses of wounded human skin fibroblasts. Photomed Laser Surg 24:705-14.
Hawkins DH and Abrahamse H. 2006b. The role of laser fluence in cell viability, proliferation, andmembrane integrity of wounded human skin fibroblasts following helium-neon laser irradia-tion. Lasers Surg Med 38:74-83.
Hopkins JT, McLoda TA, Seegmiller JG, and David Baxter G. 2004. Low-level laser therapy facili-tates superficial wound healing in humans: a triple-blind, sham-controlled study. J Athl Train39:223-229.
Huang SS and Zheng RL. 2006. Biphasic regulation of angiogenesis by reactive oxygen species.Pharmazie 61:223-9.
Imlay JA. 2008. Cellular defenses against superoxide and hydrogen peroxide. Annu Rev Biochem77:755-76.
Karu T. 1989. Laser biostimulation: a photobiological phenomenon. J Photochem Photobiol B 3:638-40.Karu T. 1999. Primary and secondary mechanisms of action of visible to near-IR radiation on cells. J
Photochem Photobiol B 49:1-17.Karu TI and Afanas'eva NI. 1995. Cytochrome c oxidase as the primary photoacceptor upon laser
exposure of cultured cells to visible and near IR-range light. Dokl Akad Nauk 342:693-5.Karu TI and Kolyakov SF. 2005. Exact action spectra for cellular responses relevant to phototherapy.
Photomed Laser Surg 23:355-61.Karu TI, Pyatibrat LV, and Ryabykh TP. 1997. Nonmonotonic behavior of the dose dependence of
the radiation effect on cells in vitro exposed to pulsed laser radiation at lambda = 820 nm.Lasers Surg Med 21:485-92.
Klotz LO, Kroncke KD, and Sies H. 2003. Singlet oxygen-induced signaling effects in mammaliancells. Photochem Photobiol Sci 2:88-94.
Kreisler M, Christoffers AB, Willershausen B, and d'Hoedt B. 2003. Effect of low-level GaAlAs laserirradiation on the proliferation rate of human periodontal ligament fibroblasts: an in vitrostudy. J Clin Periodontol 30:353-8.
Biphasic dose response in low level light therapy

Lampl Y, Zivin JA, Fisher M, Lew R, Welin L, Dahlof B, Borenstein P, Andersson B, Perez J, CaparoC, Ilic S, and Oron U. 2007. Infrared Laser Therapy for Ischemic Stroke: A New TreatmentStrategy. Results of the NeuroThera Effectiveness and Safety Trial-1 (NEST-1). Stroke
Lane N. 2006. Cell biology: power games. Nature 443:901-3.Lane P and Gross SS. 1999. Cell signaling by nitric oxide. Semin Nephrol 19:215-29.Lanzafame RJ, Stadler I, Kurtz AF, Connelly R, Peter TA, Sr., Brondon P, and Olson D. 2007.
Reciprocity of exposure time and irradiance on energy density during photoradiation onwound healing in a murine pressure ulcer model. Lasers Surg Med 39:534-42.
Lapchak PA, Han MK, Salgado KF, Streeter J, and Zivin JA. 2008. Safety profile of transcranial near-infrared laser therapy administered in combination with thrombolytic therapy to embolized rab-bits. Stroke 39:3073-8.
Lavi R, Shainberg A, Friedmann H, Shneyvays V, Rickover O, Eichler M, Kaplan D, and Lubart R.2003. Low energy visible light induces reactive oxygen species generation and stimulates anincrease of intracellular calcium concentration in cardiac cells. J Biol Chem 278:40917-22.
Leal Junior EC, Lopes-Martins RA, Baroni BM, De Marchi T, Taufer D, Manfro DS, Rech M, DannaV, Grosselli D, Generosi RA, Marcos RL, Ramos L, and Bjordal JM. 2008a. Effect of 830 nm low-level laser therapy applied before high-intensity exercises on skeletal muscle recovery in ath-letes. Lasers Med Sci
Leal Junior EC, Lopes-Martins RA, Vanin AA, Baroni BM, Grosselli D, De Marchi T, Iversen VV, andBjordal JM. 2008b. Effect of 830 nm low-level laser therapy in exercise-induced skeletal musclefatigue in humans. Lasers Med Sci
Loevschall H and Arenholt-Bindslev D. 1994. Effect of low level diode laser irradiation of human oralmucosa fibroblasts in vitro. Lasers Surg Med 14:347-54.
Lopes-Martins RA, Albertini R, Martins PS, Bjordal JM, and Faria Neto HC. 2005. Spontaneous effectsof low-level laser therapy (650 nm) in acute inflammatory mouse pleurisy induced byCarrageenan. Photomed Laser Surg 23:377-81.
Lubart R, Eichler M, Lavi R, Friedman H, and Shainberg A. 2005. Low-energy laser irradiation pro-motes cellular redox activity. Photomed Laser Surg 23:3-9.
Lubart R, Lavi R, Friedmann H, and Rochkind S. 2006. Photochemistry and photobiology of lightabsorption by living cells. Photomed Laser Surg 24:179-85.
Lubart R, Wollman Y, Friedmann H, Rochkind S, and Laulicht I. 1992. Effects of visible and near-infrared lasers on cell cultures. J Photochem Photobiol B 12:305-10.
Martius F. 1923. Das Amdt-Schulz Grandgesetz. Munch Med Wschr 70:1005-1006.Mester E, Nagylucskay S, Waidelich W, Tisza S, Greguss P, Haina D, and Mester A. 1978. Effects of
direct laser radiation on human lymphocytes. Arch Dermatol Res 263:241-5.Mester E, Szende. B. and Tota, J.G. 1967. Effect of laser on hair growth of mice. Kiserl Orvostud
19:628-631.Mitka M. 1998. 1998 NObel Prize winners are announced: three discoverers of nitric oxide activity.
Jama 280:1648.Moore P, Ridgway TD, Higbee RG, Howard EW, and Lucroy MD. 2005. Effect of wavelength on low-
intensity laser irradiation-stimulated cell proliferation in vitro. Lasers Surg Med 36:8-12.Morrone G, Guzzardella GA, Torricelli P, Rocca M, Tigani D, Brodano GB, Fini M, and Giardino R.
2000. Osteochondral lesion repair of the knee in the rabbit after low-power diode Ga-Al-As laserbiostimulation: an experimental study. Artif Cells Blood Substit Immobil Biotechnol 28:321-36.
Oron A, Oron U, Streeter J, de Taboada L, Alexandrovich A, Trembovler V, and Shohami E. 2007.low-level laser therapy applied transcranially to mice following traumatic brain injury signifi-cantly reduces long-term neurological deficits. J Neurotrauma 24:651-6.
Oron U, Yaakobi T, Oron A, Hayam G, Gepstein L, Rubin O, Wolf T, and Ben Haim S. 2001a.Attenuation of infarct size in rats and dogs after myocardial infarction by low-energy laser irra-diation. Lasers Surg Med 28:204-11.
Oron U, Yaakobi T, Oron A, Mordechovitz D, Shofti R, Hayam G, Dror U, Gepstein L, Wolf T,Haudenschild C, and Haim SB. 2001b. Low-energy laser irradiation reduces formation of scartissue after myocardial infarction in rats and dogs. Circulation 103:296-301.
Ozcelik O, Cenk Haytac M, Kunin A, and Seydaoglu G. 2008. Improved wound healing by low-levellaser irradiation after gingivectomy operations: a controlled clinical pilot study. J ClinPeriodontol 35:250-4.
Y.-Y. Huang and others
Ozdemir F, Birtane M, and Kokino S. 2001. The clinical efficacy of low-power laser therapy on painand function in cervical osteoarthritis. Clin Rheumatol 20:181-4.
Pal G, Dutta A, Mitra K, Grace MS, Romanczyk TB, Wu X, Chakrabarti K, Anders J, Gorman E,Waynant RW, and Tata DB. 2007. Effect of low intensity laser interaction with human skinfibroblast cells using fiber-optic nano-probes. J Photochem Photobiol B 86:252-61.
Passarella S, Casamassima E, Molinari S, Pastore D, Quagliariello E, Catalano IM, and Cingolani A.1984. Increase of proton electrochemical potential and ATP synthesis in rat liver mitochondriairradiated in vitro by helium-neon laser. FEBS Lett 175:95-9.
Pryor WA, Houk KN, Foote CS, Fukuto JM, Ignarro LJ, Squadrito GL, and Davies KJ. 2006. Free radi-cal biology and medicine: it's a gas, man! Am J Physiol Regul Integr Comp Physiol 291:R491-511.
Rochkind S, Leider-Trejo L, Nissan M, Shamir MH, Kharenko O, and Alon M. 2007. Efficacy of 780-nm laser phototherapy on peripheral nerve regeneration after neurotube reconstruction pro-cedure (double-blind randomized study). Photomed Laser Surg 25:137-43.
Schreck R, Albermann K, and Baeuerle PA. 1992. Nuclear factor kappa B: an oxidative stress-respon-sive transcription factor of eukaryotic cells (a review). Free Radic Res Commun 17:221-37.
Schubert MM, Eduardo FP, Guthrie KA, Franquin JC, Bensadoun RJ, Migliorati CA, Lloid CM,Eduardo CP, Walter NF, Marques MM, and Hamdi M. 2007. A phase III randomized double-blind placebo-controlled clinical trial to determine the efficacy of low level laser therapy for theprevention of oral mucositis in patients undergoing hematopoietic cell transplantation. SupportCare Cancer 15:1145-54.
Schulz H. 1877. Uber die Theorie der Arzneimittelwirkung. Virchows Archiv 108:423--434.Schulz H. 1888. Uber Hefegiste. Pflügers Archiv Gesammte Physiologie 42:517-541.Shao XH, Yang YP, Dai J, Wu JF, and Bo AH. 2005. Effects of He-Ne laser irradiation on chronic
atrophic gastritis in rats. World J Gastroenterol 11:3958-61.Shefer G, Partridge TA, Heslop L, Gross JG, Oron U, and Halevy O. 2002. Low-energy laser irradia-
tion promotes the survival and cell cycle entry of skeletal muscle satellite cells. J Cell Sci115:1461-9.
Shiva S and Gladwin MT. 2009. Shining a light on tissue NO stores: near infrared release of NO fromnitrite and nitrosylated hemes. J Mol Cell Cardiol 46:1-3.
Sommer AP, Pinheiro AL, Mester AR, Franke RP, and Whelan HT. 2001. Biostimulatory windows inlow-intensity laser activation: lasers, scanners, and NASA's light-emitting diode array system. JClin Laser Med Surg 19:29-33.
Stadler I, Evans R, Kolb B, Naim JO, Narayan V, Buehner N, and Lanzafame RJ. 2000. In vitro effects oflow-level laser irradiation at 660 nm on peripheral blood lymphocytes. Lasers Surg Med 27:255-61.
Stebbing AR. 1982. Hormesis; the stimulation of growth by low levels of inhibitors. Sci Tot Environ22:213-234.
Stelian J, Gil I, Habot B, Rosenthal M, Abramovici I, Kutok N, and Khahil A. 1992. Improvement ofpain and disability in elderly patients with degenerative osteoarthritis of the knee treated withnarrow-band light therapy. J Am Geriatr Soc 40:23-6.
Stergioulas A, Stergioula M, Aarskog R, Lopes-Martins RA, and Bjordal JM. 2008. Effects of low-levellaser therapy and eccentric exercises in the treatment of recreational athletes with chronicachilles tendinopathy. Am J Sports Med 36:881-7.
Storz P. 2007. Mitochondrial ROS--radical detoxification, mediated by protein kinase D. Trends CellBiol 17:13-8.
Sutherland JC. 2002. Biological effects of polychromatic light. Photochem Photobiol 76:164-70.Tafur J and Mills PJ. 2008. Low-intensity light therapy: exploring the role of redox mechanisms.
Photomed Laser Surg 26:323-8.Townsend JF and Luckey TD. 1960. Hormoligosis in pharmacology. J Am Med Assoc 173:44-48.Tumilty S, Munn J, McDonough S, Hurley DA, Basford JR, and Baxter GD. 2009. Low Level Laser
Treatment of Tendinopathy: A Systematic Review with Meta-analysis Photomed Laser SurgAhead of print:
Vasseljen O, Jr., Hoeg N, Kjeldstad B, Johnsson A, and Larsen S. 1992. Low level laser versus placeboin the treatment of tennis elbow. Scand J Rehabil Med 24:37-42.
Watson MR, Wallace K, Gieling RG, Manas DM, Jaffray E, Hay RT, Mann DA, and Oakley F. 2008. NF-kappaB is a critical regulator of the survival of rodent and human hepatic myofibroblasts. JHepatol 48:589-97.
Biphasic dose response in low level light therapy
Weber JB, Pinheiro AL, de Oliveira MG, Oliveira FA, and Ramalho LM. 2006. Laser therapy improveshealing of bone defects submitted to autologous bone graft. Photomed Laser Surg 24:38-44.
Wu S, Xing D, Gao X, and Chen WR. 2009. High fluence low-power laser irradiation induces mito-chondrial permeability transition mediated by reactive oxygen species. J Cell Physiol 218:603-11.
Yaakobi T, Shoshany Y, Levkovitz S, Rubin O, Ben Haim SA, and Oron U. 2001. Long-term effect oflow energy laser irradiation on infarction and reperfusion injury in the rat heart. J Appl Physiol90:2411-9.
Yamaura M, Yao M, Yaroslavsky I, Cohen R, Smotrich M, and Kochevar IE. 2009. Low level lighteffects on inflammatory cytokine production by rheumatoid arthritis synoviocytes. Lasers SurgMed 41:282-90.
Yu W, Naim JO, and Lanzafame RJ. 1994. The effect of laser irradiation on the release of bFGF from3T3 fibroblasts. Photochem Photobiol 59:167-70.
Yu W, Naim JO, and Lanzafame RJ. 1997. Effects of photostimulation on wound healing in diabeticmice. Lasers Surg Med 20:56-63.
Zhang J, Xing D, and Gao X. 2008. Low-power laser irradiation activates Src tyrosine kinase throughreactive oxygen species-mediated signaling pathway. J Cell Physiol 217:518-28.
Zhang Y, Song S, Fong CC, Tsang CH, Yang Z, and Yang M. 2003. cDNA microarray analysis of geneexpression profiles in human fibroblast cells irradiated with red light. J Invest Dermatol 120:849-57.
Zivin JA, Albers GW, Bornstein N, Chippendale T, Dahlof B, Devlin T, Fisher M, Hacke W, Holt W,Ilic S, Kasner S, Lew R, Nash M, Perez J, Rymer M, Schellinger P, Schneider D, Schwab S,Veltkamp R, Walker M, and Streeter J. 2009. Effectiveness and safety of transcranial laser thera-py for acute ischemic stroke. Stroke 40:1359-64.
Y.-Y. Huang and others









![Low Level Laser (Light) Therapy (LLLT) for Cosmetic Medicine ......Low Level Laser (Light) Therapy (LLLT) for Cosmetic Medicine and Dermatology Mossum K. Sawhney [1] and Michael R.](https://static.fdocuments.in/doc/165x107/60324a44e0ded43d400877e7/low-level-laser-light-therapy-lllt-for-cosmetic-medicine-low-level-laser.jpg)