Textbook of Forensic Medicine and Toxicology Principles and Practice 5e

Introduction to principles of toxicology and riskassessment
SEAC TrainingHelsinki, 29-30/06/2009
Kimmo LouekariUnit B4, Evaluation
Disclaimer: This presentation does not represent ECHA’s position on the issues covered nor is it based on expert consultation within ECHA. The presentation includes an introduction to
some of the basic concepts of toxicology and risk assessment. It is also a preliminary suggestion of the author on how results of risk assessment process could be used for the
Human Impact Assessment under the restriction processes of REACH.
Introduction
• Paracelsus: “…dose makes a poison”, – Examples:
• 60 µg/day of cadmium may causes a kidney failure after long-term exposure,
• “The current recommendations to reduce salt intake to 5 grams per day (i.e. 5000 000 ug/day) will lower blood pressure” (Cochrane reviews).
– Dose is usually given as mg or µg per kilogram of body weight per day

Introduction (2)
• In hazard assessment the aim is – to describe the intrinsic properties (toxicity) of
chemicals. Understanding the intrinsic hazardous properties can be based on animal or in vitro tests, on human data, e.g. clinical cases or epidemiological studies, and on non-testing methods
– to estimate how much of the chemical is necessary to produce the toxic response in human (or to obtain DNEL. i.e. a safe level)
• It is necessary to understand the toxic properties of a chemical to ensure that it can be used safely.

Distinction of hazard and risk
• Hazard refers to the intrinsic toxic properties of the substance/chemical
• Risk refers to the likelihood that there will be toxic effects in the human population
• Risk can not be assessed without data on the exposure of the relevant populations
In REACH, toxicity data and exposure data are combined in Exposure Scenarios

Distinction between risk assessment (RA) and human impact assessment (HIA) – some preliminary thoughts (1)
The starting point of RA is that • There is scientific evidence, often based on animal data,
that a specific effect may occur The outcome of the RA can be • A crude estimate of the likely hood or/and severity of the
effect or• RCR or margin of safety.
e.g. 5 cases of specific cancer may occur in 1 Million exposed persons (the DMEL, level of exposure and number of exposed people are considered there)
• Dose response curve with respective NOAEL and LOAEL
• Qualitative effects sensitisation or skin corrosion may occur in a specific use scenario

Distinction between RA and HIA (2)
In HIA we ask • How many people are affected• How much will the effect (cancer, skin corrosion) reduce
their quality of life (NB. Reversibility of an effect)• What would be the societal and economic costs of the
overall effect• How should the health impact be valued
However, note that physical/health impact (RAC) and the following other, e.g. monetary evaluation (SEAC) should be distinct.
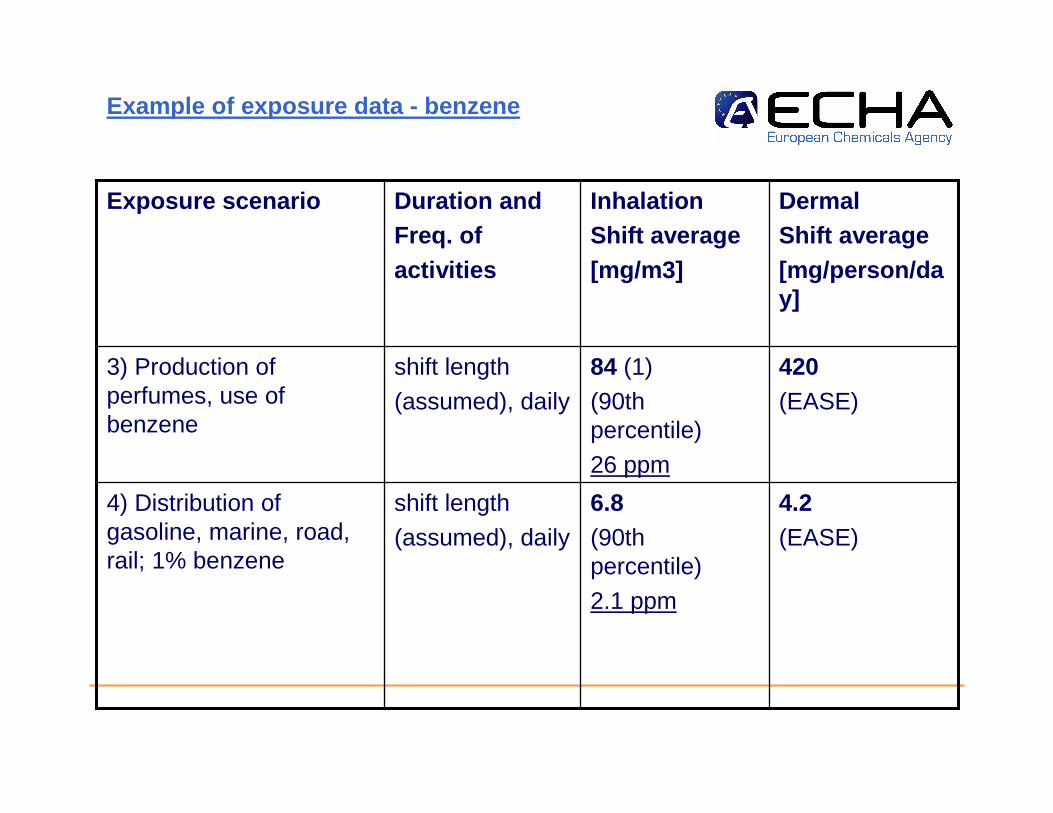
Example of exposure data - benzene
4.2 (EASE)
6.8(90th percentile)
2.1 ppm
shift length
(assumed), daily
4) Distribution of gasoline, marine, road, rail; 1% benzene
420 (EASE)
84 (1)
(90th percentile)
26 ppm
shift length
(assumed), daily
3) Production of perfumes, use of benzene
DermalShift average[mg/person/day]
InhalationShift average[mg/m3]
Duration andFreq. ofactivities
Exposure scenario
Health effects and RC of benzene
• “…an average exposure of 1 ppm over a working lifetime of 45 years resulted in estimations which span several orders of magnitude. From 1.6 – 3.1 cases per thousand exposed individuals to a range of 0.02 – 0.036 cases per thousand. (Two meta-analysis based on epi data)

Toxic effects covered in regulatory testing and in REACH
• Acute toxicity, irritation/corrosion, sensitisation, repeated dose toxicity, toxicity to reproduction, genotoxicity/mutagenicity, carcinogenicity,
• Local/systemic effects (systemic means: distributed by circulation)
• Acute/chronic effects– Local and acute: e.g. acids and bases on the skin or
in the eye cause irritation or corrosion; – Systemic and chronic: e.g. long-term exposure to
benzene increases the cancer risk

Toxicokinetics
• There is no specific information requirement in REACH• The available information has to be used in the CSA• Covers absorption (skin, g-i- system, lungs), distribution,
metabolism and excretion (urine, faeces etc.) of chemicals.
• supports the identification and understanding of – most relevant route of exposure and – bioavailability – detoxification of chemicals, mainly in liver and– determination of the half-life of chemicals i.e. whether a chemical
should be considered accumulative of not.

How is toxicity identified/tested
• Animal testing, e.g. 90day repeated dose toxicity study where gross pathology, organs, growth, blood and urine parameters etc are studies. Organ toxicity and/ or general systemic toxicity can often be observed
• In vitro testing: for skin and eye irritation/corrosion and genotoxicity testing, possible for some other endpoint in future
• Human evidence: comes mainly from clinical reports, poisoning cases, epidemiological data, or from worker health surveys
• QSAR, read-across and categories: QSAR modelling tools better suited for some toxic endpoints (e.g. mutagenicity) than for the others,

Animal (in vivo) studies
• Mostly used for effect assessment for human health;
• “More or less” good models for humans;
• Different species and strains;
• EU Annex V Guidance, OECD guidance,…

In vitro studies• Results from in vitro test may fully or partly replace an in vivo
test if:- validated according to internationally agreed validation
principles,- results adequate for C&L, RA.
• The use of results from in vitro methods that have not yet been scientifically validated (“suitable studies”) depends on whether such study indicates certain dangerous property and on the potential risk identified.
• In vitro studies• Genotoxicity/Cytotoxicity
• Dermal absorption
• Irritation (skin – eye), phototoxicity
• Cellular metabolism/mechanism of action
• Macromolecular binding
• Sperm motility/Embryo culture

• Analytical epidemiological studiesRelationship between human exposure and effects: biological effects marker, early signs of chronic effects, disease occurrence or mortality
• case control, cohort, cross sectional studies
• Descriptive epidemiological studies (examine differences in disease rates in relation to differences in temporal and environmental conditions )
• Case reports (particular effects after exposure; often single exposure; misuse of the substance)
• Controlled studies in human volunteers
���� Ethical considerations!
Meta-analysis
Human data

(Q)SARs
Results obtained from valid (Q)SARs may indicate the presence or absence of a certain dangerous property. Results of (Q)SARs may be used instead of testing when the conditions in Annex XI (1.3) are met:
- Established scientific validity- Substance within the applicability domain- Results adequate for C&L and RA- Adequate and reliable documentation
Not well developed/validated in relation to mammalian toxicity (skin sensitization, mutagenicity, skin irritation/corrosion);
Well developed (Q)SARs for phys-chem properties relevant for effect assessment for human health

There are many types of effect data
EndpointInformation:
Annexes V-IX
(Q)SARs
Read Across
In-vitro
Waiving:• technical• exposure
Existinginformation
TESTING
Last resort

Effect Assessment (1)
• Assessment of the inherent properties – potential to cause harm
• Objectives:– Determine Classification and Labelling– Derive levels of exposure to the substance above
which humans should not be exposed – Derived No-effect Levels (DNELs)

Effect assessment (2)Involves• Selection of the key study, for each endpoint to be
evaluated• Assessment of the human/biological relevance and
severity of the effects observe e.g. – reversible/irreversible, – adaptive or harmful/adverse – consideration of the toxicokinetics
• Evaluation of the dose-response
Is done by industry, and
checked by the Agency for 5% of the dossiers within the compliance check

Dose response relationship
• If an experiment is well done, there should be a relation between dose and the effect/response, i.e. with increased dose/concentration the effect increases, i.e. more of the exposure animals have the effects or the effect becomes more severe
• If dose response relationship can not be seen, it may be the it was a chance finding or artifact, then the study data usually can not be alone used for risk assessment

Reversibility of the effect
• Normally, reversible effect are regarded as less severe than irreversible ones.
• In some tests, there is a follow-up period to observe whether the animal recover in time, e.g. irritation/corrosion studies and acute toxicity studies (e.g. 7 days).
• Reversibility depends e.g. on the regenerative and repair capacity of cells and sub-cellular structures; e.g. epithelial cell of gastro intestinal tract have high regenerative capacity, whereas nerve cells of adults have completely lost this capacity.
• Covalent binding of a genotoxic substance with DNA, cancer and damage of central nervous system are considered irreversible

DNEL=Derived No Effect Level
• Is calculated by dividing the NOAEL/dose descriptor by the assessment factor
• For example if NOAEL from a reproduction toxicity study (reduced fertility/sperm count) would be 150 mg/kg (of body weight of experimental
animal) and assessment factor would be 1000, DNEL is 150 µg/kg/b.w (for human).

DNEL (2)
• DNEL is needed fro risk characterization (RC)• In RC, DNEL is directly compared with the
exposure level of the relevant human population• For example if workers exposure in cleaning
work is 100 µg/kg (normally derived from inhalation exposure
• Risk characterization ratio would be 100/150, which is 0.66, i.e below 1
• Thus, it could be concluded and the use of the substance in that scenario is safe

Assessment factors in DNEL
Aim to cover • Interspecies (between animal and human) and
intraspecies (among humans)• Severity of the effect • Sensitivity of the human (sub-)populations (e.g.
children, pregnant women)• Quality of the data• Extrapolation from shorter test to chronic exposure A specific DNEL might be named e.g. as worker-DNEL
long-term for dermal route

Basic assessment factors
Interspecies variation
Intraspecies variation
10 10
kinetics kineticsdynamics dynamics

Implications to the HIA and SEA
• When RCR is close to 1 and especially when it is above it, there may be health consequences
• Uncertainties in the risk assessment and especially the size of the sub-population exposure should then be analysed carefully
• This may have been done by the applicant of authorisation already or it may require more close examination by RAC and SEAC
• Combination of 1. CMR effect, 2. high RCR and 3. large size of exposure population (and/or wide spread uses) would be the ”worst scenario”

NOAEL=No Observed AdverseEffect Level
• May be obtained from any toxicity study where different dose levels have been applied
• E.g. Dose levels of 10, 150, 500 mg/kg may have been used in a repro study – In case 500 mg/kg caused decreased fertility in the reproduction
toxicity study then 150 mg/kg would be NOAEL
• The effect is supposed to be adverse; e.g. irreversible organ damage, skin corrosion or cancer are adverse effects, whereas mild irritation of skin or transient change of liver enzyme levels are considered less adverse.

NOAEL (2)
• NOAEL normally is not obtained from irritation/corrosion, mutagenicity or sensitisation study
• In reproduction toxicity study and repeated dose toxicity study, when there is an adverse effect it should always be possible to obtain a NOAEL or LOAEL

DMEL
• Especially genotoxic carcinogens are considered to have no effect threshold; thus NOAEL can not be set.
• This implies that exposure needs to be minimised leading to very strict controls and setting of DMEL, Derived Minimal Effect Level
• whereas non-genotoxic carcinogenicity is thought to be a threshold effect and thus, DNEL can be obtained

DMEL (2)
• Starting point of DMEL derivation can be e.g. T25 which is a dose that causes the tumour incidence in exposure am anal to increase by 25% and compared to the control animals
• To obtain DMEL, T25 is divided by every high assessment factor

DMEL (3)
• The philosophy behind high assessment factor is the linear extrapolation and acceptable of small statistical risk, i.e. if the number of exposed people is not tens or hundreds of millions, the risk might be only statistical. i.e. there would be no cancer cases associated with the exposure to the chemical

RCR
Operationalconditions
Measurements modeling
Exposure estimate
Data set
Toxicity data
Assessment factors
DNEL
Exposure assessment Effects assessment
Risk characterization
Data evaluation
Risk Assessment Process
TGD
IUCLID5 EUSES,ECETOC TRA

Information requirements (1)
• Depend on the amount of substance manufactured or imported.
• Information submitted to ECHA in registration should enable classification and labeling as well as risk assessment

Information requirements (2)
• For example, at the 1-10 t/a level, data on irritation/corrosion, sensitisation, mutagenicity (only the Ames test) and acute oral toxicity
• At higher levels, the information requirement for repeated dose toxicity and on reproduction toxicity are set
• At the highest tonnage, i.e. above 1000 t/a, data which enables full assessment of repeated dose toxicity (up to chronic toxicity), reproduction toxicity (up to two generation reproduction toxicity test) and mutagenicity has to be provided.

An example of qualitative grading of the risk level, based on R-phrases and level of exposure BS 8800
High riskHigh riskMedium riskHigh
High riskMedium riskLow riskModerate
Medium riskLow riskLow riskLow
extreme harmasthma, intoxications,
carcinogenesis e.g.
R35, R41, R42,
moderate harm, Irreversible effects are possible, skin sensitisation, skin or eye corrosion, e.g.
R34, R43, R48
slight harmIrritation or other
transient mild effect, e.g. R20, R21, R36
Hazard categories of the health effects (R-phrases)Level of exposure based on a questionnaire

Restriction process
• When a MS CA justifies the restriction proposal, it mayneed to, depending on the specific case– Proceed from the RA to HIA, in order to point out the public
health consequences of the current non-restricted use(s) and show the benefits of the restriction
– Revise the toxicological evaluation (e.g. DNEL) or the exposure assessment to demonstrate the there is an uncontrolled or unmanaged risk, associated with specific uses/products and thereby with specific Exposure Scenario(s)
– Provide an estimate of the size of the sub-population exposed to the substance. For that purpose, information of the market share/penetration, use pattern may be relevant
•

Uncertainties
• Assessment factors are partly regulatory assumptions rather that scientific, AFs may be over- or under-protective– Especially interspecies differences can be substantial, e.g.
different/lacking mechanisms,
• Only those health effects can be observed for with there are testing/information requirement; low tonnage testing is very crude– There are e.g. immunotoxic and developmental neurotoxic
effects which may go unidentified even at higher tonnage
• Most of in vitro methods and QSAR tools are not yet robust enough.













![TOXICOLOGY CENTRE SELF-ASSESSMENT DOCUMENT Assessment_Report... · toxicopathology, inorganic biogeochemistry [later changed to analytical toxicology], and contaminant fate ... Toxicology](https://static.fdocuments.in/doc/165x107/5b42ffd97f8b9ab15f8b94bd/toxicology-centre-self-assessment-document-assessmentreport-toxicopathology.jpg)

![[a. Barile Frank] Principles of Toxicology Testing(BookFi.org)](https://static.fdocuments.in/doc/165x107/552b0be84a795931588b4569/a-barile-frank-principles-of-toxicology-testingbookfiorg.jpg)