Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future

of 110
-
Upload
ashley-swearingen -
Category
Documents
-
view
218 -
download
0
Transcript of Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
1/110
Jun 2012
Lot to Lo:How Americas Health andObesity Crisis Threatensour Economic Future
Halth PgamNutrition and Physical Activity Initiative
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
2/110
Halth PgamNutrition and Physical Activity Initiative
BPC would like to thank the Robert Wood Johnson Foundation, the W.K. Kellogg
Foundation, and the Stuart Family Foundation or their generous support o the
Nutrition and Physical Activity Initiative.
D i s c L a i m e r
This report is the product o the Bipartisan Policy Centers Nutrition and Physical
Activity Initiative (NPAI). The ndings and recommendations expressed herein are
solely those o NPAI and do not necessarily represent the views or opinions o the
Bipartisan Policy Center, its ounders or its board o directors.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
3/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
Bruce Knight
Senior Advisor
Former Undersecretary or Marketing
and Regulatory Programs, USDA
Robin Schepper
Senior Advisor
Former Executive Director, Lets Move!
Matt Levy, MD, MPH
Advisor
Division Chie, Community Pediatrics,
Georgetown University Hospital
Health Policy Fellow 2010-2011, RWJF
Marika Tatsutani
Lead Writer and Editor
Nutrition and Physical Activity Initiative
STAFF MeMberS
Lisel Loy
Director, Nutrition and Physical
Activity Initiative
Leah Ralph
Policy Analyst
Amelia Shister
Administrative Assistant
Co-CHAirS
Dan Glickman
Senior Fellow, Bipartisan Policy Center;
Former Secretary o Agriculture;
Former Representative rom Kansas
Mike Leavitt
Chairman, Leavitt Partners;
Former Governor o Utah;
Former Secretary o Health and
Human Services
Donna E. Shalala
President o the University o Miami;
Former Secretary o Health and
Human Services
Ann M. Veneman
Former Executive Director o UNICEF;
Former Secretary o Agriculture
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
4/110
Halth PgamNutrition and Physical Activity Initiative
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
5/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
Executive Summary . . . . . . . . . . . . . . . . . . . . 5
Chapter 1: Introduction . . . . . . . . . . . . . . . .19
Chapter 2: Americas Health Crisis . . . . . . . . 23
Chapter 3: Healthy Families . . . . . . . . . . . . . 31
Diet and Physical Activity Guidelines . . . . . . . . . . . . . 32
Nutrition Assistance Programs . . . . . . . . . . . . . . . . . . 34
Breastfeeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Chapter 4: Healthy Schools . . . . . . . . . . . . . 41
Chapter 5: Healthy Workplaces . . . . . . . . . . 49
Case Study: Department of Defense Initiatives . . 54
Chapter 6: Healthy Communities . . . . . . . . . . 61
Community-based, Prevention-focused health care . . . 61
Large Institutions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Community Programs and the Built Environment . . . . . 78
Chapter 7: Cross-Cutting Recommendations . . . 83
Public Awareness and Marketing . . . . . . . . . . . . . . . . 83
Food and Farm Policy . . . . . . . . . . . . . . . . . . . . . . . . . 86
Information Sharing and Analysis . . . . . . . . . . . . . . . . 89
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . 92
List of Acronyms . . . . . . . . . . . . . . . . . . . . . 94
Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
Acknowledgements . . . . . . . . . . . . . . . . . . 102
Table of Contents
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
6/110
Halth PgamNutrition and Physical Activity Initiative
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
7/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
Our nation is in the midst o a public health crisis so proound
that is it undermining our national well-being, our economic
competitiveness and even our long-term national security. Fully
two-thirds o Americans are overweight or obese. One-third o
American children are overweight or obese. And among children
under the age o six, nearly one in ve is overweight or obese.I
Obese people are ar more likely to develop chronic diseaseslike diabetes, hypertension, asthma, heart disease and cancer.
Obese children are more likely to have one or more risk actors
or cardiovascular disease, to be prediabetic (i.e., at high risk or
developing diabetes), and to suer rom bone and joint problems,
sleep apnea, and social and psychological problems such as
stigmatization and poor sel-esteem. They are also very likely to
become obese adults.
In short, obesity is the most urgent public health problem in
America today. It is a primary reason why lie expectancy in
large parts o the United States is already several years lower
than in other advanced countries around the world. For millions
o Americans, it means many more years even decades
o sharply reduced quality o lie. More broadly, the costs o
obesity and chronic disease have become a major drag on our
economy. Escalating health care costs are themain driver o our
spiraling national debt, and obesity-related illness comprises an
increasingly large share o our massive health costs. The obesity
crisis is thereore not just a health crisis, but a major contributor
to our scal crisis. At home, individuals and amilies struggle with
the consequences and costs o obesity and disease on a daily
basis. But or our nation as a whole, the impacts o Americas
obesity epidemic jeopardize our global competitiveness and
national security, directly undermining our ability to cut the
ederal debt, prepare and sustain a highly productive workorce,
maintain our military strength, and compete eectively in the
global economy.
Turning the tide o this epidemic is challenging or several
reasons. First, changing behavior is never easy, particularly when
that behavior is rooted in much deeper changes in the way many
Americans live, work, play and eat. Second, public resources
to implement new policies and programs are constrained as
never beore. Given these twin challenges, the importance o
responsibility and leadership in combating obesity and chronic
disease cannot be overemphasized. Both are clearly needed
at the level o individuals and parents, who ultimately make the
decisions and set the examples that infuence not only their
own health but that o uture generations. But responsibility andleadership are also needed at the level o communities and key
institutions, including government. These institutions shape the
environment in which individual and amily decisions get made
and they can help bring about the broader changes needed
to ensure that all Americansincluding especially vulnerable
citizenshave access to inormation and options that support
and encourage healthy choices.
The Bipartisan Policy Center (BPC) launched its Nutrition and
Physical Activity Initiative based in large part on our concern
about the national debt and the clear role that escalating health
care costs play in our nations looming scal emergency. Obesity
and chronic disease are a critically important piece o this puzzle.
In searching or solutions, we have ocused on those areas that
we believe hold the most promise to bring about change on
the scale and within the timerame needed to respond to the
enormous scal, social, economic, and public health threat they
present. We recognize that eective responses to the current
epidemic will require action and change on the part o individuals
and amilies, as well as action and change on the part o a wide
variety o interests and organizations: large companies, advocacy
groups, community leaders, health proessionals, business
groups, and oundations, not to mention local, state and ederal
government. Success is only possible i all these entities work
together and bring creativity, innovation and ocused commitment
to the eort.
The good news is that we are already seeing an enormous
convergence o attention and initiative in this area. Many
important ideas are being tried some o them out o economic
or other necessity and oten with limited resources rom
healthier menus in Army mess halls to improved school lunch
Executive Summary
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
8/110
exutv suy
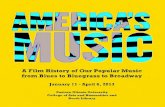
Source: Derived rom inormation rom the Boston Foundation (June 2007).
ACCESS TO CARE 10%
GENETICS 20%
SERVICESMEDICAL
OTHER 8%
HEALTHY BEHAVIORS
HEALTHY BEHAVIORS 4%
ENVIRONMENT 20%
What Makes
Us Healthy
What We Spend
On Being Healthy+
88%
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
9/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
programs and community-based preventive care services. This
report makes specic recommendations aimed at building on the
most promising eorts, with the benet o insights gained rom a
year o intensive research and outreach to groups and individuals
who are already working in all kinds o settings and in many
dierent ways to promote healthy nutrition and physical activity.
This Executive Summary, like the main report, is organizedto refect our broad categories or targets or action: amilies,
schools, workplaces, and communities. A th category o cross-
cutting recommendations addresses public awareness, ood and
arm policy, and inormation sharing.
Halthy Famls
For most people, healthy patterns o diet and physical activity
begin at home. Parents and caregivers, in particular, have a
strong infuence on what children eat and how active they are. In
act, recent studies indicate that the general health and obesityo parents is a powerul indicator or the health outcomes o
children. Moreover, these infuences start very early: a growing
body o research indicates that nutrition during the rst thousand
days starting during pregnancy and continuing to age two
plays a signicant role in determining an individuals health,
not only later in childhood but over his or her entire lietime.
BPCs recommendations or healthy amilies ocus on increasing
awareness o ederal diet and physical activity guidelines, aligning
ederal nutrition assistance programs with dietary guidelines, and
promoting breasteeding or the rst six months o an inants lie.
Healthy Families Recommendation #1: HHS and
USDA should extend federal guidelines for diet
and physical activity to all children under six and
enhance public awareness and understanding of
these guidelines.
Existing dietary guidelines, which are developed by the U.S.
Departments o Health and Human Services (HHS) and
Agriculture (USDA), apply to children and adults ages two and
up; current physical activity guidelines start at age six. Given the
importance o establishing healthy patterns or diet and activity
in very young children we recommend that HHS and USDA take
the ollowing specic actions:
Develop, implement and promote national dietary guidelines
or the rst thousand days, covering pregnant women and
children up to two years old;
Similarly, develop national physical activity guidelines or
children under six years old; and
Support these guidelines by developing an eective national
strategy or disseminating this inormation and educating
parents about the benets o rst oods and physical activity,
particularly or populations that are most at risk or poor
nutrition and health.
Healthy Families Recommendation #2: USDA should
ensure that all its nutrition assistance programsreect and support federal dietary guidelines.
The USDAs Food and Nutrition Service (FNS) operates 15
ederal nutrition assistance programs that together serve millions
o the nations most vulnerable citizens, including many o the
populations most at risk or poor nutrition, obesity and related
chronic diseases. Because these programs touch nearly one in
our Americans annually, they provide a critical opportunity or
educating people about the connections between diet, physical
activity and health. The major ederal ood programs include
the National School Lunch and School Breakast Programs, the
Special Supplemental Nutrition Program or Women, Inants and
Children (WIC) program, the Supplemental Nutrition Assistance
Program (SNAP), and the Child and Adult Care Food Program
(CACFP). To promote better childhood nutrition and health
through these programs, we recommend that HHS and USDA
take several steps to: (a) align messaging and education about
nutrition through these programs, particularly as they aect
pregnant women, new mothers, inants and young children;
(b) provide technical training to states and local USDA sta to
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
10/110
exutv suy
that a national program be established to publicly recognize
businesses that demonstrate best practices in providing lactation
accommodations.
Halthy Schls
Because most children spend signicant amounts o time in
school or in childcare acilities outside the home, these settings
aord an important opportunity to infuence the health and
liestyle choices o the next generation. Studies also nd a
direct link between nutrition and physical activity and improved
perormance in school. For these reasons, opportunities to
promote better health through nutrition and physical activity in
school have received considerable attention rom policymakers,
health experts, and other stakeholders. The Healthy Hunger-Free
Kids Act passed by Congress in 2010 required USDA to update
nutrition standards or oods and beverages served in schools,
including oods and beverages sold through vending machinesand school stores. This was the rst update in 15 years. The
legislation also calls on schools to strengthen their wellness
policies to look at the overall health o students.
Historically, less attention has been given to nutrition and health
in childcare settings or preschool-aged (as opposed to school-
aged) children, but here too a growing number o initiatives and
programs have been launched in recent years. For example,
USDA is moving to update Child and Adult Care Food Program
(CACFP) meal guidelines, which apply to ood served in childcare
settings (among other venues). For schools and preschools, the
primary challenge at present is to scale up successul programs
and ully implement policy changes that have already been
introduced, including the Healthy Hunger-Free Kids Act.
Healthy Schools Recommendation #1: Childcare
providers should improve nutrition and physical
activity opportunities for preschool-aged children.
Nationwide, 12 million U.S. children under the age o six are in
childcare and, o these, 1.9 million are cared or in a amily day
improve program implementation and eectiveness; (c) conduct
research to gain a better understanding o program participation,
utilization and impacts; and (d) increase awareness o program
benets.
Healthy Families Recommendation #3: All key
institutions including hospitals, workplaces,communities, government and insurance providers
should support and promote breastfeeding with the
goal of substantially increasing U.S. breastfeeding
rates for the rst six months of an infants life.
Breasteeding is enormously benecial or both mother and child.
And or the child, these benets are long lasting: research nds
that breasted inants have improved health outcomes later in
lie, including lower rates o obesity and chronic disease.II A 2010
study published by the American Academy o Pediatrics ound
that i 90 percent o new mothers in the United States breasted
exclusively or six months, this change alone could deliver health
care cost savings on the order o $13 billion annually.III
Today, roughly three-quarters o new mothers in the United
States start outbreasteeding, but that rate drops o sharply once
mothers and inants leave the hospital: by three months, only 35
percent o inants are exclusively breasted and at six months,
the gure is less than 15 percent.IV And while not all mothers
breasteed, or those who do, institutional, amily and community
support can make the dierence between sustaining this practice
versus not. To support and promote breasteeding, hospitals
should ollow baby riendly practices, including discouragingthe use o ormula except where medically necessary, tracking
and reporting their maternity care practices, and providing ollow-
up support or breasteeding ater new mothers leave the hospital.
Both hospitals and the ederal WIC program should ollow the
World Health Organizations Code o Marketing o Breast Milk
Substitutes, which aims to limit unwarranted exposure to breast
milk substitutes and related advertising. Finally, employers have
an important role to play in providing nursing breaks and a private
place or mothers to express breast milk. We also recommend
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
11/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
School gardens are an example o the kind o project that has
been shown to be highly eective as a teaching tool, that does
not require a very large commitment o resources, and that lends
itsel well to partnerships with outside organizations. Schools
should also look to outside sources o unding and support using
models such as the Alliance or a Healthier Generations Healthy
Schools Program, which provides technical assistance to helpparticipating schools improve ood quality and physical education
programs. This eort is similar to the USDAs Healthier U.S.
Schools Challenge, which provides small monetary incentives to
schools that meet rigorous standards or ood quality, participation
in meal programs, physical activities, and nutrition education.
Healthy Schools Recommendation #4: Federal, state
and local governments, along with private partners,
should explore all available avenues to increase
quality physical activity in schools.
Specically, schools should require 60 minutes o physical activity
per day as an integral part o their wellness policies. Children
spend much o their day in school and oten also participate
in ater-school programs, and promoting physical activity in
the school environment is critical to supporting physical and
mental tness in students. Given the unding challenges many
schools ace, all available options should be explored, including
but certainly not limited to physical education classes. Options
requently exist that are simple and not costly. Partnering
with other public and private institutions, incorporating health
inormation in school curricula, and innovating to maximize
returns rom existing resources will be critical to successullyimplementing these recommendations.
Halthy Wkplacs
For many Americans, the workplace is second only to home in
terms o time spent and impact on liestyle choices. Fortunately,
growing numbers o employers are seeing the connection
between healthier workers and healthier prots. This is because
obesity and chronic disease are strongly linked to lower employee
care setting.V While strides have been made to improve nutrition
and provide more opportunities or physical activity in school,
childcare and preschool settings are another critical area or
intervention. A growing body o research indicates that waiting
until kindergarten is too late. By age ve, one in ve children
is already overweight or obese. Given the importance o early
intervention, we must ensure that early childhood environmentsprovide the strongest start possible, including access to nutritious
ood and regular physical activity.
Healthy Schools Recommendation #2: Schools
should improve food and nutrition education by
aggressively implementing the Healthy Hunger-Free
Kids Act.
To assist states and school districts in implementing the above
recommendation, USDA should compile existing resources,
and supplement them where necessary, to establish a national
clearinghouse o tools and inormation. We also recommend that
the Centers or Disease Control (CDC) and the Department o
Education explore how they can provide resources to assist with
education and other elements o the transition.
For their part, states should develop implementation plans, with
a ocus on training and other support necessary or successul
implementation, to help schools aggressively embrace Healthy
Hunger-Free Kids Act requirements. Particular attention needs
to be paid to the training and technical assistance needs o small
and rural school districts where barriers to implementation have
typically been higher.
Healthy Schools Recommendation #3: Schools
should improve nutrition and physical activity
offerings, in partnership with the private sector.
Given current budget constraints at the ederal, state and local
levels, schools and school districts will have to innovate and
work with the private sector to expand the resources available to
support nutrition and physical activity in schools and to prioritize
the use o existing resources to achieve maximum benets.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
12/110
exutv suy
The ederal governments Oce o Personnel and Management
(OPM) currently spends $40 billion per year covering health care
costs or ederal employees. But because all employee-related
medical and pharmacy claims are paid centrally through OPM,
individual departments or agencies have no way o tracking their
particular health care costs. This reduces accountability as well
as incentives to promote employee health or disease prevention.Options or changing current practice so as to make department
or agency heads accountable or, or at least aware o, employee
health costs should be explored as a rst step toward modeling
leadership on the issue o workplace wellness in the ederal
government. Federal investments in data collection and tracking
to substantiate the benets achieved through dierent workplace
wellness demonstrations will be well justied i they point the way
toward replicable approaches that reduce costs and improve
perormance, not just in the ederal workorce but or rms and
their employees throughout the economy.
The U.S. Department o Deense (DoD) is providing particularly
strong leadership in this arena and has several initiatives
underway to improve health among service members and military
amilies. For example, the Army launched the Soldier Fueling
Initiative when it ound that attrition rates were higher among
new recruits because many o them had lower bone density
levels, incurred more injuries, and suered rom deciencies in
calcium, iron and various other vitamins and nutrients compared
to previous recruit cohorts. This initiative combines enhanced
physical education and training with healthier ood choices
and an inormation/awareness campaign to emphasize the
importance o good nutrition or soldier perormance. DoD has
worked with dietitians to improve ood oerings at military dining
acilities more broadly but it could do even more to promote
nutrition and physical activity, both on base through military
hospitals, schools and childcare centers and o base in
communities with a high proportion o military amilies. Because
our national security depends on a t and high-perorming
military, DoD is an employer with a particularly critical charge.
It also has the capacity, infuence and organization to change
productivity, higher rates o absenteeism and presenteeism
(when people are present, but not working eectively), and
higher health care costs. O course, employers are also uniquely
positioned to infuence workorce health, particularly since they
bear such a large share o employee health care costs (currently,
60 percent o Americans are insured through an employment-
based plan).VI Increasingly, research is nding positive, and insome cases quite dramatic, returns on employer investments
in workplace wellness.VII These programs also deliver less
measurable but still important (and valuable) benets, in terms o
improved employee satisaction and retention.
Healthy Workplaces Recommendation #1: CDC, in
partnership with private companies, should develop
a database of exemplary workplace wellness
programs with a rigorous cost/benet analysis to
help scale up existing best practices in both the
private sector and within government. The SmallBusiness Administration (SBA) should provide support
here.
A registry o workplace wellness and health promotion initiatives
that could be readily accessed by a variety o stakeholders would
put the workplace wellness movement on more solid ooting and
help employers identiy proven strategies and program designs
that are well-suited to their industry, size and organizational
structure. Additional steps that would support employer
investments in workplace wellness include developing tools and
resources to analyze the costs and impacts o wellness programs,
providing resources or pilot programs and program evaluations,and supporting certication and accreditation programs as a way
to lower barriers to participation and accelerate the dissemination
o best practices.
Healthy Workplaces Recommendation #2: The
federal government should both scale up successful
workplace wellness programs and continue
exploring innovative approaches.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
13/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
settings. Demand or these services already exists, but so ar
the supply o providers has not caught up. Third, we need
mechanisms to enable public and private reimbursement
or health conditions and services that are oten not covered
under the existing system.
Healthy Communities Recommendation #1:Nutrition and physical activity training should be
incorporated in all phases of medical education
medical schools, residency programs,
credentialing processes and continuing
education requirements.
Proessionals throughout the health care system are uniquely
positioned to inorm and motivate Americans on the subjects
o nutrition and physical activity. Americans see medical
proessionals nurses in particular as a trusted source o
inormation, and health care providers are the number one
go-to resource or parents who are concerned about their
childs weight. But the medical education and licensing
system in the United States is not currently set up to ensure
that health proessionals have the incentive and expertise
to deliver messages about weight, chronic disease, diet
and physical activity not only eectively but consistently. On
the contrary, the consensus among medical organizations
and experts is that nutrition education at all levels o
health training (undergraduate, post-graduate, ellowship,
licensing and board certication, and continuing education)
is uneven at best and oten inadequate. The goal o this
recommendation is to inuse the education and training oall health proessionals with nutrition and physical activity
inormation and behavioral methodologies or tools (such as
motivational interviewing), and to make basic competency
in these areas an integral part o certication and continuing
education requirements. Achieving this goal will require
leading expert organizations to partner in developing a
comprehensive national strategy and standards or nutrition
and physical activity education across the continuum o the
health proession.
business as usual in ways that aect the rest o government,
as well as institutions in our larger society. By applying many o
the tools described in this report rom supporting breasteeding
at maternity hospitals to providing healthier ood choices and
recognizing the important role o schools and amilies DoD
has an opportunity to substantially enhance the health and
perormance o service members and their amilies, while at thesame time leading the way or the rest o the country.
Halthy Cmmunts
Along with home, school and workplace, community plays a
central role in the liestyle choices that infuence peoples health
outcomes. Their local community is where most Americans
access the goods and services on which they rely, rom the
grocery store to the doctors oce; it is also where most o us
go to play, worship, recreate, eat out and be entertained. This
chapter discusses a wide-ranging set o recommendations,all o which are rooted in the community, broadly dened. For
organizational purposes, we divide this chapter into three major
subtopics: health care services, large institutions, and the built
environment.
1. Community-based, Prevention-focused Health Care
Rising health care costs have prompted growing interest in
disease prevention as a more eective and ultimately less
expensive way to keep Americans healthy. Good diet and an
active liestyle are clearly central to an approach that avors
promoting wellness and preventing disease over a model
that ocuses on treating health problems only ater they arise.
Our recommendations target three kinds o interventions that
are necessary to support the shit to a prevention-ocused
health care system. First, health care proessionals must be
better trained to provide care that addresses issues o diet,
physical activity, wellness and disease prevention. Second,
the base o available care resources and care providers
must be broadened to include non-traditional providers
who can deliver services in non-clinical, community-based
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
14/110
exutv suy
wellness-ocused approach to health care. An example o
this approach is being pioneered by UnitedHealth Group
(UHG) and the YMCA, which have partnered to implement
a diabetes prevention program in which UHG reimburses
the YMCA or education, counseling and weight-loss services
according to perormance-based metrics (not simple
participation rates). Similarly, the ederal government isexamining potential ways to increase coverage or preventive
services through programs such as Medicare, Medicaid and
the Childrens Health Insurance Program (CHIP). Further
demonstration projects, whether public or private, are needed
to provide data on what works. We should reward those
services and providers who demonstrate the capacity to bend
the cost curve.
2. Large Institutions
Large institutions such as hospitals and universities, sports
and entertainment venues, hotels, and large government
departments or agencies (DoD, or example) serve meals to
thousands o people on a daily basis. A single major retailer
such as Walmart may sell ood to millions o customers
each day. These entities, private and public, have enormous
purchasing power and can leverage major changes in
the ood supply chain, both in terms o what kind o ood
is produced and in terms o where and how the ood is
distributed. As in schools and workplaces, interest in healthy
ood and wellness on the part o large institutions has been on
the rise in recent years. Innovative programs and partnerships
have been multiplying and there are a growing number osuccess stories to be considered and possibly emulated.
Several large hospitals, major retailers, universities, restaurant
and hotel chains, and large government agencies have
launched promising initiatives in recent years to improve
menu oerings and promote healthier ood choices.
Healthy Communities Recommendation #2: Non-
clinical, community-based care is a critical tool
in preventing obesity and chronic disease. We
need to train and deploy a prevention workforce
to deliver this kind of preventive care.
Recognizing that or many people, contact with traditionalhealth care proessionals such as doctors and nurses is
limited or sporadic, we recommend engaging a wider base
o resources and person-to-person interactions to deliver
messages about health and infuence liestyle behaviors.
Recent initiatives suggest that community health workers,
health coaches, dietitians and nutritionists, lactation
consultants, and others can be eective in working with
individuals and groups to change awareness and habits
around diet, physical activity and other health-relevant
behaviors. And their interventions, whether provided in
collaboration with a health proessional or not, can be
more cost eective than the same services delivered by a
traditionally trained doctor or nurse practitioner.VIII Expanding
this trained, community-based prevention workorce
and nding ways to reimburse or its services would oer
multiple benets by improving health outcomes, reducing
health care costs, and creating new job opportunities.
Standardized training programs and curricula are needed to
tap this potential.
Healthy Communities Recommendation #3:
Public and private insurers should structure
incentives to reward effective, community-based, prevention-oriented services that
have demonstrated capacity to reduce costs
signicantly over time.
Because many community-based, preventive health care
services are not currently covered by either public or private
insurers, creating new reimbursement mechanisms or
reorming existing ones to cover these types o services
is critical to realizing the potential benets o a broader,
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
15/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
Healthy Communities Recommendation #6: Local
governments should leverage existing resources
and infrastructure assets to expand opportunities
for physical activity.
In communities that lack sae, adequate places or children,
youth and adults to exercise and play, or where schools donthave the acilities to support physical activity programs, joint
use agreements provide a mechanism to enable the shared
use o public acilities. Typically, this type o agreement would
be struck between two government entities, such as a school
district and a city or county. Joint use agreements have
been successully used in a number o locales to expand
the sport and recreational opportunities available to students
and members o the community. A variety o other low-cost
options and public-private partnerships have also been used
to promote healthy activity at the community levela good
example are the various walking initiatives, such as Everybody
Walk and Get Fit, that have been launched in neighborhoods
and at schools across America.
Healthy Communities Recommendation #7: Families
and local governments should make creative use of
technology to increase physical activity.
Modern technologies, including video games, mobile
phones and computers, are oten viewed as a major driver
behind todays more sedentary, less healthy liestyles.
Ater all, American children spend, on average, more than
seven hours a day in ront o a screen. Yet, given that thesetechnologies have become an inescapable and, or many
people, indispensable part o daily lie, we believe it is time
to rerame the debate. Opportunities to develop games that
require or encourage the user to be physically active are
expanding rapidly. Some such games already exist and others
are being developed. Newer ideas include linking pedometers
and accelerometers to games and prizes, using geo-cashing
and other geographic digital games to encourage kids to go
outside, and using social media to share inormation about
Healthy Communities Recommendation #4:
Large, private-sector institutions should procure
and serve healthier foods, using their signicant
market power to shift food supply chains and
make healthier options more available and cost-
competitive.
Healthy Communities Recommendation #5:
Public-sector institutions should continue to
lead by example, promoting healthy foods
and physical tness as a means to enhance
employee performance, both in the military and
within the civilian workforce.
3. Community Programs and the Built Environment
Community programs and the built environment play an
important role in supporting (or discouraging) a healthy level
o regular physical activity. In many parts o America, the builtenvironment refects and reinorces an automobile-centered
way o lie. Resource-strapped towns and cities have cut
back on recreational programs and acilities. And only those
with extra time and means have the option to join a health
club or gym. In some areas, its hard even or children to be
active; schools dont oer sports and activities, parks and
playgrounds may be inadequate or non-existent, and simply
playing outside may be too dangerous because o trac
or crime or both. In sum, considerable empirical evidence
exists to suggest that where people live and work has a much
greater impact on their health than their interactions with thehealth care sector or their genetic makeup. And while these
social determinants o health do have some correlation to
income levels, they aect all Americans living in all kinds o
communities. Our recommendations or promoting more
active liestyles at the community level ocus on three specic
areas o opportunity: (1) leveraging existing resources, (2)
utilizing technology in innovative ways, and (3) changing the
built environment over time.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
16/110
exutv suy
many advertising messages including particularly those
directed to children continue to promote unhealthy
oods. At the same time, research shows that many people
have diculty interpreting the health-related claims that
are oten used to market ood, either as part o ood
packaging or in advertisements.
In sum, more can and should be done to communicate
clear, consistent messages about the importance
o healthy diet and physical activity and to provide
consumers with the inormation to make healthier choices.
Expanded eorts in this realm should make use o new
advertising and media outlets, including not just TV, print,
radio and the internet, but also new and emerging social
media, kid-directed games, product packaging, and digital
media advertising.
Public Awareness and Marketing
Recommendation #1: The food industry should
adopt uniform standards for what constitutes
better for you foods using the Institute of
Medicine Phase 2 report as a starting point and
making sure industry standards are aligned with
the U.S. Dietary Guidelines.
We also call or an independent entity to monitor and evaluate
the impact the industrys voluntary Facts up Front proposal
is having on consumer choice, with the goal o measuring
whether consumers are using this inormation to change their
purchasing and consumption behaviors.
Public Awareness and Marketing
Recommendation #2: The Ad Council or similar
organizations should coordinate a multi-media
campaign to promote healthy diet and physical
activity, funded by leading private sector
companies in collaboration with federal agencies.
For both the nutrition and physical activity aspects o the
campaign, high prole and infuential messengers are
physical activity options (such as mobile apps that provide
inormation about good recreation or walking options).
Healthy Communities Recommendation #8: Local
governments should use the planning process
to change the built environment in ways that
promote active living.
Growing numbers o cities and towns are using the planning
process and zoning codes to shape the built environment in
ways that promote walking and bicycling, help residents stay
connected, and improve quality o lie. In many cases, mayors
and county and city council representatives are working with
architects and designers and with planning, transportation
and public health departments to create healthier buildings,
streets, and urban spaces based on the latest academic
research and best practices. As an alternative to imposing
new requirements, some cities have removed or changed
old zoning codes that work against the goal o encouraging
healthier, more active living. Other cities have incorporated
physical activity guidelines into their construction codes and
adopted policies that support outdoor play and exercise.
These include oering incentives to designers and developers
to build in ways that encourage walking, bicycling, and active
transportation and recreation.
Css-Cuttng rcmmndatns
1. Public Awareness and Marketing
The ood industry spends billions o dollars each year
marketing products to American consumers. According to the
Institute o Medicine (IOM), as much as $10 billion per year
is spent just to market ood specically to children. A number
o large ood and beverage companies, both individually and
in some cases as part o a larger initiative, have recently made
voluntary commitments to reduce their marketing to children,
and/or sought to improve the nutritional quality o their
product oerings. While these eorts are to be applauded, too
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
17/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
We recommend taking specic actions, including: reviewing
existing government policies or opportunities to eliminate
barriers that may reduce the supply and increase the cost
o healthy oods; authorizing a generic ruit and vegetable
promotion board; improving transportation and distribution
systems to make resh produce more available and
aordable; and exploring ways to incentivize healthier oodchoices through ederal nutrition assistance programs.
Food and Farm Policy Recommendation #2: USDA
should identify and pursue further opportunities to
promote health and nutrition through its nutrition
assistance programs.
Federal nutrition assistance programs, like SNAP, WIC
and CACFP, reach millions o the nations most vulnerable
individuals and amilies each year including many people
at high risk or obesity and chronic disease. We recommend
continued support or these programs coupled with increased
eorts to align program guidelines and incentives with ederal
dietary guidelines. We also recommend urther research and
analysis to better understand the impacts o these programs
on dietary choices and health in the recipient population and
to inorm relevant policy debates going orward, such as the
current debate about whether certain ood items should be
excluded rom the SNAP program.
Food and Farm Policy Recommendation #3:
Congress should continue sustained support for
relevant research by ofces of USDA.
Research conducted by the USDAs Agricultural Research
Service (ARS), the National Institute o Food and Agriculture
(NIFA), and Economic Research Service (ERS) is valuable
to ensure that policymakers, stakeholders and the public
continue to have robust, up-to-date inormation on the
impacts o ood and arm policies.
critical. We recommend involving celebrities, athletes
and other public gures who resonate with audiences
and have the ability to inspire change.
Public Awareness and Marketing Recommendation
#3: Food retailers should adopt in-store marketing
and product placement strategies to promote thepurchase of healthier, lower calorie products.
Public Awareness and Marketing Recommendation
#4: States and localities should continue to innovate
and experiment with ways to change the prole of
foods in the marketplace.
As part o ongoing eorts in this area, additional inormation
generated by states and localities about the impact that
dierent state policies and local ordinances are having
on ood choices, portion sizes and other actors or the
general population and or children in particular would bea useul contribution to existing research in the eld.
2. Food and Farm Policy
Agriculture is a major sector o the U.S. economy and one
in which government decisions subsidies and incentives,
trade policies, etc. play a major role. Historically, arm and
agriculture policies were, at most, tangentially infuenced by
considerations o diet, nutrition and health. This has begun to
change. Growing awareness o the costs and impacts o high
rates o obesity and chronic disease in America are prompting
a broader look at our entire ood supply chain and at the
policies and programs that, along with consumer preerence,
determine what oods appear on grocery store shelves and,
ultimately, on our plates.
Food and Farm Policy Recommendation #1: USDA, in
collaboration with other stakeholders, should identify
and address barriers to increasing the affordability
and accessibility of fruits, vegetables and legumes.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
18/110
exutv suy
Cnclusn
While the statistics on obesity and chronic disease are truly
alarming, numbers alone cannot convey the ull human and
social costs o the health crisis we conront today in America.
The problem is clear and its impact on our uture both in
terms o the health, productivity and well-being o the currentgeneration and generations to come, and in terms o the
prosperity, competitiveness and scal integrity o our nation as a
whole is hard to overstate. Turning the tide o this epidemic will
require leadership, rst and oremost. All sectors o society must
be engaged and all must take responsibility rom individuals
and amilies to communities, institutions and government.
Together, our challenge will be to dene and implement policies,
strategies, incentives and actions that, by encouraging and
supporting healthy behaviors, can begin to slow and even
reverse the trajectory we are on. The complexity o the problem
demands a diversity o solutions; whats required is not a newtop-down program or a vast expenditure o public resources, but
a multiplicity o smaller steps and changes, at all levels o society,
that collectively translate to lasting, large-scale shits over time.
Results will rarely be quick, but progress must be steady. And as
we strive to reduce obesity, improve health, and slow the runaway
growth o health care costs in America, continued research and
data collection will be critical to inorm our eorts and make sure
we are investing in those strategies we know will work.
In this report, BPC has ocused on areas and opportunities
or intervention that we believe hold particular promise, both
because they can have a signicant impact and because
they can be implemented within existing rameworks and
structures. The good news is that many powerul examples
and inspiring programs are already underway. To achieve the
goal o signicantly reducing obesity and chronic disease in
America within the next generation, we must build on what is
already working, expand the reach o good programs, and greatly
accelerate the pace o change. The problem is complex but we
know at least some o the solutions. Now it is time to get to work.
3. Information Sharing and Analysis
One o the greatest challenges or all parties interested
in promoting healthy diet, physical activity, wellness, and
preventive care is accessing the wealth o data and ideas that
is being generated in this realm. From understanding what
programs are working well to what the latest research cantell us, there is an enormous need or better ways to share
knowledge and learn rom dierent eorts. Time and again,
as BPC reached out to dierent stakeholders we learned
about important, innovative, sometimes low-cost or even
cost-neutral programs that have achieved desired results
but are not widely known. And despite some eorts to pull
together some o this inormation, no central repository exists
or systematically collecting, organizing and disseminating
research, data and best practices or combating obesity and
chronic disease. Also needed are ongoing public-private
eorts to rigorously evaluate the costs and impacts o specic
public health interventions. Given the scale o the challenges
and current scal and political constraints, it will be critical
to demonstrate that prevention-based approaches can yield
tangible results.
Information-sharing recommendation #1: CDC
and HHS should continue robust efforts to collect
and disseminate information on food, physical
activity and health including information on the
social determinants of health and future costs
and Congress should continue to support these
monitoring and information-gathering functions.
Information-sharing recommendation #2:
Public- and private-sector organizations active
in this eld should partner to establish a national
clearinghouse on health-related nutrition and
physical activity initiatives. The clearinghouse
should provide links to further resources, technical
assistance, coordination and partnership
opportunities, and up-to-date research ndings.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
19/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
Notes
I. Ogden, Cynthia, Ph.D., and Margaret Carroll, M.S.P.H. Prevalence o Obesity
Among Children and Adolescents: United States Trends 1963-1965 Through
2007-2008. CDC.gov. Centers or Disease Control and Prevention, 4 June
2010. Retrieved rom http://www.cdc.gov/nchs/data/hestat/obesity_child_07_08/
obesity_child_07_08.htm
II. U.S. Department o Health and Human Services, Oce o the Surgeon General.
The Surgeon Generals Call to Action to Support Breasteeding. Washington, DC,
2011 P.1.
III. Bartick, Melissa, and Arnold Reinhold. The Burden o Suboptimal Breasteeding
in the United States: A Pediatric Cost Analysis.Pediatricsvol. 125 No. 5. 2010.
IV. Breasteeding Report Card 2011, United States: Outcome Indicators.CDC.gov.
Centers or Disease Control and Prevention, 1 August 2011. Retrieved romhttp://
www.cdc.gov/breasteeding/data/reportcard2.htm
V. Mulligan, Gail M., DeeAnn Brimhall, Jerry West, and Christopher Chapman.Child
Care and Early Education Arrangements o Inants, Toddlers and Preschoolers.
U.S. Department o Education. National Center or Education Statistics, National
Household Education Surveys Program, 2005 P. 4. Laughlin, Lynda. Whos
Minding the Kids? Child Care Arrangements: Spring 2005/Summer 2006.
Census.gov. U.S. Census Bureau, Aug. 2010. P. 2. Retrieved romhttp://www.
census.gov/prod/2010pubs/p70-121.pd
VI. Baicker, Katherine, David Cutler, and Zirui Song. Workplace Wellness Programs
Can Generate Savings. Health Aairs. February 2010.
VII. Ibid. See also Berry, Leonard L., Ann M. Mirabito, and William B. Baun. Whatsthe Hard Return on Employee Wellness Programs? Harvard Business Review.
VIII. Shearer, Gail, M.P.P. Issue Brie: Prevention Provisions in the Aordable
Care Act. APHA.org. American Public Health Association, Oct. 2010 P.4.
Retrieved rom http://www.apha.org/NR/rdonlyres/763D7507-2CC3-4828-AF84-
1010EA1304A4/0/FinalPreventionACAWeb.pd
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
20/110
Halth PgamNutrition and Physical Activity Initiative
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
21/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
Our nation is in the midst o a health crisis. Fully two-thirds o Americans are overweight
or obese. One-third o American children are overweight or obese. And among children
under the age o six, nearly one in ve is overweight or obese.1 Fewer than 20 percent o
Americans meet ederal guidelines or a healthy level o regular physical activity.2 Chronic,
debilitating, expensive and oten lethal diseases such as diabetes and hypertension aect
millions o people, at younger and younger ages, and are especially prevalent in low-income
and minority communities.
The consequences o this crisis threaten not only the day-to-day well-being and quality-
o-lie o millions o Americans, but the uture prosperity and security o our country as
a whole. Chronic diseases linked to obesity, poor nutrition and a lack o physical activity
are major drivers o todays runaway health care costs. Already, these costs are crowding
out other critical investments and orcing lose-lose choices on households, businesses
and the government alike. At risk in the long run is not just the scal integrity o the U.S.
government, but the American peoples ability to grapple with challenges on multiple ronts.
Chronic poor health aects everything rom the academic perormance o U.S. students, to
the productivity o U.S. workers and the readiness o the U.S. military.
Behind these trends lie many changes, large and small, in the way Americans live, work,
eat and play. Compared to our parents and grandparents, most o us spend more time in
ront o computer or television screens and more time in the car. We are more likely to work
in sedentary occupations, less likely to live in neighborhoods where we can walk to work or
to the grocery store, and less likely to have time to prepare home-cooked ood or sit down
or amily meals. In low-income communities, kids may lack sae places to play outside and
Chapt 1: Introduction
Rates of obesity (BMI 30)
in the U.S. population
increased strikingly over
the last 30 years, more than
doubling for adults and
more than tripling for
children.
0
10
20
30
40
50
In 1972, 5% of
children and
14.5%of adults
were obese.
By 2008, 17% of
children and
34.3% of adults
were obese.
Percentage
ofU.
S.
Population
Sources: Centers or Disease Control and Prevention, National Center or Health Statistics (June 2010); Lets Move White
House Task Force on Childhood Obesity Report to the President (May 2010).
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
22/110
chpt 1: intoduton
local stores may not stock resh ruits and vegetables. Everywhere, ast-prepared oods
many o them laden with ats and sugar are available in abundance and at prices
that make them cheaper per calorie than healthier options. Everywhere, a barrage o
advertising makes us crave the oods that we can least aord to eat. In this environment,
eating well, staying active, and maintaining a healthy weight is an uphill struggle or
many i not most Americans. And despite a media culture that celebrates being thin and
physically t, millions o Americans are losing the battle or long-term wellness many othem rom a young age.
Changing this picture indeed, merely shiting the odds presents an enormous
challenge. The actors involved are numerous, complex and rooted in the social,
economic, cultural and demographic realities o our time. No easy policy prescriptions
exist because solutions to the problem depend on choices about diet and physical
activity that are ultimately personal; they come down to the messages parents send their
kids, the decisions people make in the supermarket aisle, and everyones willingness
and ability to look out or his or her own health. But it is equally critical to recognize
that individual choices take place in a context and are powerully shaped by a host o
external infuences. That means government and other institutions have an important
role to play in ensuring that all citizens have at least the inormation and the opportunity
to pursue a healthy liestyle. Put simply, it shouldnt be more dicult in 21st century
America to eat well and stay active than to do the opposite. And or too many people in
too many places especially those in low-income and minority communities healthy
options are either out o reach or simply not available.
To turn the tide on Americas obesity and chronic disease epidemic, all sectors o society,
rom employers and government agencies to schools, health care providers and the
ood industry, will have to work together to support and encourage healthy choices.
Inormation, incentives and access to better ood and physical activity options can be
powerul tools or broad-based change and all o them must be brought to bear. The
stakes are high and the need or action is urgent not just to avoid crippling healthcare costs in the uture but to ensure that Americas workorce remains one o the most
productive and competitive in the world.
The Bipartisan Policy Center (BPC) launched its Nutrition and Physical Activity Initiative
in 2011 to explore potential levers or change in the ght against obesity and chronic
disease in America. The initiative is led by our ormer U.S. cabinet secretaries and
brings together a wide range o experts, policymakers and stakeholders. This report
reviews the challenges our nation conronts today in terms o nutrition, physical activity
and health; it also identies best practices, highlights specic success stories, and
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
23/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
advances a set o concrete policy recommendations designed to address these issues
rom multiple angles.
Throughout, our ocus is on specic actions that could be taken to reduce current
rates o obesity and chronic disease, and thereby ease the nancial strains and loss o
longevity and productivity that are the ultimate consequences o our deepening national
health crisis. These recommendations refect insights gained rom a year o intensiveresearch and outreach to experts and stakeholders who are actively addressing health
issues rom the perspective o nutrition and physical activity. An enormous amount o
good work is being done in this area and success stories abound rom an innovative
eort to help U.S. servicemen and women make healthier choices in Army mess halls to
school lunch programs that have improved the quality o ood being oered to children
while also reducing costs. But scaling up these success stories will be challenging,
especially when many o the major players including schools, cities and counties
lack the resources to expand promising programs. Moreover, policies that aim to
change behavior are oten intrinsically hard to implement. BPCs goal with this initiative
is not to duplicate or repeat eorts that are already working. Rather, it is to explore how
individuals, government and the private sector can build on the best o these eorts
with a combination o behavior changes, targeted interventions and policy reorms that,
over time, will have a lasting impact on the health o the American people and the uture
strength and security o our nation as a whole.
This report is organized as ollows: Chapter II provides background and context on
Americas current crisis o obesity and chronic disease, elaborating on several o the
points and themes raised in this introduction. Subsequent chapters (Chapters III
through VI) outline our recommendations. They are organized according to the level
(or unit) o society that is primarily being addressed in each case, recognizing that
these distinctions are not always clear cut and that, given the nature o the topic, some
overlap across dierent categories or target audiences is inevitable. We begin with
healthy amilies, which are the rst line o deense in ensuring that healthy attitudesand patterns o behavior with respect to ood and physical activity are established early
and passed on to the next generation. Additional chapters ocus on schools, which oer
some o the most important opportunities to reach young people outside the home; the
workplace, where most adults spend a large portion o their waking hours; and nally,
the community, which provides the setting in which most o the activities o daily lie
rom buying ood and accessing health care services to socializing, moving to school
and work, and engaging in recreational activities occur. A th category o cross-cutting
recommendations is covered in Chapter VII.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
24/110
Halth PgamNutrition and Physical Activity Initiative
1990 2010
No data
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
25/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
By several measures, obesity is already the single largest
threat to public health in America today. According to
the American Cancer Society, obesity is now responsible
or roughly as many cases o cancer as smoking.3 It also
aects a ar larger number o people; as we noted in the
introduction, well over hal the U.S. population two-
thirds o adults and one-third o children and adolescents is obese or overweight. Obesity is not only extremely
prevalent, it has alarming consequences or peoples
health. A 2001 study ound that obese people had a
67 percent higher chance o suering rom conditions
like diabetes, hypertension, asthma, heart disease and
cancer than normal-weight people o the same age and
social demographic.4 Obese people also spent much
more on medical services 36 percent more, on average,
than normal-weight individuals. In sum, obesity is a
major reason why nearly hal the U.S. population today
about 145 million people in total suers rom one ormore chronic diseases.5 These impacts are borne by all
segments o society, but they disproportionately aect low-
income households and communities o color.6 And the
resulting health care costs aect us all.
For children, the immediate and long-term eects o obesity
can be particularly devastating. In the short term, according
to the Centers or Disease Control and Prevention (CDC),
obese children are more likely to have one or more risk
actors or cardiovascular disease, to be prediabetic (i.e.,
at high risk or developing diabetes), and to suer rom
bone and joint problems, sleep apnea, and social andpsychological problems such as stigmatization and poor
sel-esteem.7 In act, due to the rapid increase in the number
o diabetic children, a disease that was once called adult
onset diabetes has now been renamed Type 2 diabetes. In
the longer run, obese children are much more likely to be
obese adults with all the costs and impacts this implies not
only in terms o contracting expensive and debilitating adult
chronic diseases but in terms o quality o lie and the ability
to realize their personal and proessional potential.
Fraction of U.S. Population that Is Overweight or Obese
100
90
80
70
60
50
40
30
20
10
0
Percent
Year
1960
-196
2
1963
-196
6
1966
-197
0
1971
-197
4
1976
-198
0
1988
-199
4
1999
-200
0
2003
-200
4
Overweight including obese, 20-74 years
Overweight but not obese, 20-74 years
Obese, 20-74 years Overweight, 6-11 years
Overweight,12-19 years
Todays crisis o obesity and chronic disease is alarming
in part because it emerged so rapidly: over little more
than the span o a single generation. Prior to 1960, rates
o obesity in the U.S. population were relatively stable
(around 13 percent); between 1960 and 1980 they
increased moderately but stayed well below 20 percent.
Since 1980, however, the percentage o Americans
who are overweight or obese has grown dramatically; in
addition, much o this increase has been concentrated in
the obese category, which grew by 61 percent between
1991 and 2000.8 Today 35.7 percent o Americans (more
than 78 million)9 are considered obese (within the latter
category, roughly nine million people are considered
Chapt 2: Americas Health Crisis
Source: Centers or Disease Control and Prevention, National Center or Health
Statistics (2006). Data rom National Health and Nutrition Examination Survey.
Today 35.7 percent of Americans(more than 78 million) areconsidered obese.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
26/110
chpt 2: a Hlth c
severely obese).10 Roughly another third o the adult
population is considered overweight. In act, the U.S.
has the highest rates o obesity among 33 o the worlds
wealthiest countries.11 Current trends in childhood obesity
are especially worrisome, given the high correlation
between childhood and adult obesity and the longer-termimplications o a lietime o obesity. Overall, the incidence
o childhood obesity more than tripled in the United
States over the past 30 years: between 1980 and 2008,
the percentage o children aged six to 11 years who were
obese increased rom seven percent to nearly 20 percent,
while the percentage o adolescents aged 12 to 19 years
who were obese increased rom ve percent to 18 percent.
An important aspect o obesity and chronic disease is that
the prevalence o both is not evenly distributed across
the population. According to the CDC, non-Hispanic
blacks have the highest rates o obesity (44.1 percent)
compared with Mexican Americans (39.3 percent),
all Hispanics (37.9 percent) and non-Hispanic whites(32.6 percent). The relationship between socioeconomic
status and obesity is more complex. Among women,
the prevalence o obesity declines with higher income,
whereas the same is not necessarily true or men (among
non-Hispanic black and Mexican-American men, or
example, the prevalence o obesity actually increases with
higher income).Thus while there is a connection between
obesity and poverty, the act is that most obese people in
the United States are not low-income. On the contrary,
Diagnosed Diabetes Amoung Adults Age 20 Years and Older,
By Race/Ethnicity, 2007-2009
Billions
of2009
U.
S.
Dollars
Percent with Diagnosed Diabetes
Source: 2011 National Diabetes Fact Sheet. Centers for Disease Control and Prevention.
0
5
10
15
20
8%8%7%
12%
13%
16%
White,
Non-HispanicOverall Hispanic
Black,
Non-HispanicAsian
American
Indian/Alaska
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
27/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
among both men and women, most obese adults in this
country are non-Hispanic whites with income at or above
130 percent o the poverty level.12 Just as important,
rates o obesity have been rising in recent years or all
ethnic groups, at all income levels, and in all categories
o educational attainment. The epidemic, in other words,
is unevenly distributed but it is aecting everyone. Andthough there is some evidence that the rate o increase in
obesity has begun to slow in recent years, the problem is
still growing in terms o numbers o adults and, perhaps
more importantly, childrenaected. Indeed, among some
groups (boys aged nine to 19, or example) the rate o
increase in obesity still appears be accelerating.13
As we noted in the introduction, there are many reasons
or the sharp increase in obesity in the U.S. population
over the last 30 years, and we are only beginning to
gain a sophisticated understanding o the role played
by dierent genetic, environmental and liestyle actors.
Recent research, or example, suggests that inadequate
sleep may be linked to weight gain and related chronic
health conditions.14 Researchers are also looking closely
at changes in the American diet and at the role o specic
oods. Sugar, or example, has been at the center o a
vigorous debate about whether it is disproportionately
responsible or the increase in obesity and chronic
disease seen over the last several decades. In the 1950s,
Americans consumed on average 110 pounds o sugar
per person per year. By 2000, this gure had increased
to more than 150 pounds per year, with much o thisincreased consumption coming in the orm o sweetened
beverages. Most public health experts agree that urther
research is needed to ully understand the role that sugar
in its dierent orms, including sucrose and high-ructose
corn syrup, plays in weight gain and chronic disease.15
Available data, meanwhile, conrm broad and striking
shits in both the eating habits and physical activity levels
o Americans over the last 30 to 40 years. Between 1977
and 1995, the percentage o meals eaten away rom home
nearly doubled, rom 16 to 29 percent, and the percentage
o meals eaten at ast ood restaurants specically
tripled rom three to nine percent.16 Data rom the
U.S. Department o Agriculture indicate that Americans
average daily caloric intake increased by 24.5 percent,
or about 530 calories, between 1970 and 2000.17 Evenas caloric intake has grown, there is broad anecdotal and
some empirical evidence that physical activity levels have
declined. A recent study that looked at the connection
between occupational physical activity and obesity ound
that in the early 1960s, almost hal the private-sector jobs
in the U.S. required at least moderate-intensity physical
activity. This compares to ewer than 20 percent o
current jobs demanding this level o energy expenditure.18
Meanwhile, despite a modest increase in the percentage
o adults who reported engaging in regular physical activity
between 2001 and 2005, the latest available CDC data stillindicate that less than hal the adult U.S. population meets
recommended guidelines or physical activity. Reliable
inormation on physical activity19 among children is harder
to nd, but the available data point to (1) a clear decline
in physical activity as kids enter adolescence and (2) large
amounts o time spent in ront o television or computer
screens. A study by the Kaiser Family Foundation ound
that todays eight- to 18-year-olds spend an average o
seven hours and 38 minutes per day (more than 53 hours
a week) using entertainment media.20
I the reasons behind obesity are varied and complex,so are its many costs and consequences not just or
individuals but or society as a whole. Numerous studies
have looked at the impacts o obesity, and the literature
on this subject is growing daily. Rather than attempt an
exhaustive summary in this short overview, we cite a ew
key ndings rom recent work.21 A 2010 article on the
economic costs o obesity in America reviews ndings in
our categories: direct medical costs, productivity costs,
transportation costs, and human capital costs. Productivity
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
28/110
chpt 2: a Hlth c
costs include the costs o absenteeism, presenteeism
(when people are at work, but are not as productive as
they could be), disability, and premature mortality related
to obesity; transportation costs include the additional ueluse and environmental impact associated with transporting
heavier people; and human capital costs include adverse
impacts on educational attainment (including both quantity
and quality o schooling).
O these costs, direct medical cost is the metric that has
received the most attention. CDC has estimated that
spending on medical care or obesity-related illnesses
in America totals $147 billion per year.22 A more recent
estimate puts the gure as high as $190 billion annually.23
Another recent study by the Campaign to End Obesity
ound that i indirect costs are included, the annual cost is
close to $300 billion.24 The annual direct cost o childhood
obesity in America has been estimated at $14.3 billion, and
this gure would be much higher i it accounted or the highprobability that obese children will become obese adults.25
The very high cost o managing and treating many o the
chronic diseases associated with obesity helps to explain
the magnitude o these cost impacts. Diabetes is a good
example. According to one study, the annual cost o
treating a case o diagnosed diabetes averages $6,649
per year; or undiagnosed cases and prediabetes, annual
costs per case average $1,744 and $443.26 Another
study ound that expected lietime medical care costs
or patients who have one or more o ve weight-related
chronic diseases were 20 percent higher or people who
are overweight, 50 percent higher or people who are
obese, and nearly double or people who are severely
obese.27 And while many o these costs are borne by the
private sector, obesity also accounts or a growing burden
on public spending. A study using data rom 1998 and
2006 concluded that in the absence o obesity, Medicare
spending would be 8.5 percent lower and Medicaid
spending would be 11.8 percent lower.28
Interest in these gures is not merely academic. An
increasingly urgent debate is underway about theimplications o recent explosive growth in U.S. health care
spending, both in terms o the nations overall economic
outlook and in terms o impacts on the ederal decit and
debt. Again, the numbers are startling. As a percent o
GDP (gross domestic product), overall spending on health
care in America doubled between 1980 and 2010, rom
nine to 18 percent. Today, nearly one in every ve dollars
generated by the U.S. economy is going to health care
and expenditures are still growing.29 Multiple reasons
U.S. National Health Spending, 1965-2010
Billions
ofDellars
$3,000
$2,500
$2,000
$1,500
$1,000
$500
$0
65 70 75 80 85 90 95 00 05 10
Out of Pocket
Private Insurance
Medicare
Medicaid
Other Third-Party Payers
Source: Centers or Medicare and Medicaid Services, National HealthExpenditure Accounts (2011).
...expected lifetime medical care costsfor patients who have one or more ofve weight-related chronic diseaseswere 20 percent higher for people
who are overweight, 50 percenthigher for people who are obese, andnearly double for people who areseverely obese.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
29/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
have been advanced to explain the rapid escalation in
overall U.S. health care spending rom the increasing
sophistication o technology and greater use o prescription
drugs to administrative costs and the aging o the
population. But the rising incidence o chronic diseases,
many o them obesity-related, is clearly an important
part o the picture and likely plays a role in the act that
America, despite substantially higher per capita spending
on health care, lags well behind other wealthy developednations in terms o key health outcomes.30
I rising health care costs are a concern or the economy
as a whole, they amount to nothing short o a ticking
time bomb or the ederal budget. This is because costs
or Medicare and Medicaid the two major government-
provided health insurance programs have emerged
as the dominant drivers o Americas rapidly mounting
debt.31 Already, these two programs account or more than
Health Care Costs are the Primary Driver of the Debt
Source: Congressional Budget Office (August 2011).
%o
fGDP
Year
Health Care Spending
Discretionary Spending (Defense and Nondefense)
Other Mandatory Programs
Social Security
2021 2031 2041 20512011
0%
2%
4%
6%
8%
10%
12%
14%
...the combined cost of [Medicare andMedicaid] can be expected to nearlydouble to just over $1.3 trillion by2020. If that were to occur, federalexpenditures for these two programsalone would exceed current federalspending on all defense and non-defense discretionary programs.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
30/110
chpt 2: a Hlth c
one-th (21 percent) o ederal spending with combined
outlays exceeding $750 billion per year in FY2010 and
2011. Meanwhile, the Center or Medicare and Medicaid
Services has projected that the combined cost o these
programs can be expected to nearly double to just
over $1.3 trillion by 2020. I that were to occur, ederal
expenditures or these two programs alone would exceedcurrent ederal spending on all deense and non-deense
discretionary programs.
Dealing with the nations budget problems is obviously a
much bigger policy discussion; rising health care costs
arent the only driver (increased enrollment and expanded
eligibility account or much o the projected growth in
Medicare and Medicaid spending, or example) and
there is broad agreement that entitlement reorm will be
necessary to put the U.S. Treasury back on stable ooting.
By the same token, obesity and obesity-related chronic
disease arent the only drivers o growth in U.S. health care
costs; here too, many actors are in play. But reducing the
prevalence o obesity in America and avoiding some o
its costly consequences is surely a signicant part o the
answer to managing our nations daunting economic and
health care challenges going orward.
When BPC launched its Nutrition and Physical Activity
Initiative, we were prepared to nd that a great deal was
already going on in this realm. Nonetheless, we were
taken aback by the sheer number and variety o initiatives
currently underway. Many important ideas are being tried,some o them out o economic or other necessity and
oten with limited resources. But the good news is that
innovation, inspiration and leadership in the ght against
obesity and chronic disease are emerging at all levels o
government and civil society, including non-governmental
organizations and private companies. This report and our
recommendations do not try to capture all the potentially
promising ideas that are out there, nor do we want to ocus
on suggestions that others have already put orward or are
trying to implement. Rather, our aim has been to approach
the challenge rom multiple angles, seeking points o
leverage where specic actions have the potential to bring
about large-scale change. Naturally, this has led to a
ocus on especially vulnerable, disproportionately aected
populations (including children, low-income households,
and communities o color); on institutions with the potential
to infuence large numbers o people, rom schools and
large employers, to health care providers and the military;
and ultimately on policies that shape our ood and health
environment in not always obvious but powerul ways.
In selecting among different ideas and
recommendations, we applied six basic criteria:
1. Hold promise or signicant real-world impact, among large
numbers o people and particularly vulnerable groups
2. Address the disparate impacts o obesity and chronic
disease on dierent segments o the population
3. Emphasize incentives to encourage healthier choices and
behaviors
4. Build on existing successes that have demonstrated results
and lend themselves to replication
5. Require action rom an identiable decision maker, whether
in the private and NGO sectors, or in ederal, state, local or
tribal government
6. Can be measured using progress metrics to ensure
accountability
Current rates of obesity threaten toblight not only the life prospects ofmillions of individual Americans, butthe future prosperity and security of
our nation as a whole.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
31/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
In sum, obesity in America clearly constitutes a major
health crisis but it is also much more than that. For
reasons discussed in this chapter and throughout this
report, the dimensions o the crisis are economic, social,
scal and political, as well as medical. Current rates o
obesity threaten to blight not only the lie prospects o
millions o individual Americans, but the uture prosperityand security o our nation as a whole. Fortunately, this
threat is now getting a lot o attention. Researchers,
businesses, the medical community, policymakers
and health advocates share a sense o urgency about
improving our understanding o obesity and nding
more eective strategies to combat it. Their combined
eorts provide grounds or optimism that we can take
action to reduce obesity in America more thoughtully,
systematically and successully than we have in the past.
Doing so will require leadership rom all sectors o society,
greater awareness, a ocused policy commitment at all
levels o government, and some up-ront investment
o public and private resources. None o the above will
come easily, particularly in the context o a still-ragile
economy and intense budget pressure at the ederal,state and local level. Nonetheless, all Americans should
be able to unite behind the recognition that it is easier,
better and ultimately less costly to prevent obesity and
chronic disease than to resign ourselves to living with the
consequences.
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
32/110
Halth PgamNutrition and Physical Activity Initiative
-
7/31/2019 Lots to Lose: How America's Health and Obesity Crisis Threatens our Economic Future
33/110
Lot to Lo: How a Hlth nd Obty c Thtn ou eono Futu
For most people, healthy patterns o diet and physical
activity begin at home. Parents and caregivers, in
particular, have a strong inluence on what children
eat and how active they are. In act, recent studies
indicate that the general health and obesity o parents
is a powerul indicator or the health outcomes o
children.32 Moreover, these inluences start very early;a growing body o research indicates that nutrition
during the irst thousand days o a childs lie starting
during pregnancy and continuing to age two plays a
signiicant role in determining that individuals health,
not only later in childhood but over his or her entire
lietime.Recent reports suggest that obesity during
pregnancy can be a risk actor or developing obesity,
diabetic, and cardiovascular diseases in the newborn
later in lie.33
Unortunately, the data indicate that obesity in early
childhood is already a major problem in the U.S. One
in ive American children is overweight or obese by age
six.34 According to the CDC, approximately 12.5 million
Americ