Looking Upstream for Impact - oregon.gov · JAP (10.2%) NOR (9.4%) ... somewhere and do the best we...
43
Looking Upstream for Impact: Social Determinants of Health & the Role of Health Care Reproductive health coordinators meeting – October 23, 2017 Carly Hood-Ronick MPA, MPH Oregon Primary Care Association
Transcript of Looking Upstream for Impact - oregon.gov · JAP (10.2%) NOR (9.4%) ... somewhere and do the best we...

Looking Upstream for Impact: Social Determinants of Health & the Role of
Health Care
Reproductive health coordinators meeting – October 23, 2017
Carly Hood-Ronick MPA, MPH
Oregon Primary Care Association

Session outline 2
• Review of terminology
• Role of the broader health system in promoting equity
• Relevance to the clinic
• Why this work is critical
• Questions
• Group discussion
Session goals
• Define the difference between health disparity, inequity and social determinants of health.
• Explore how systems impact health outcomes downstream.
• Hear about a national tool to screen for SDH in the clinic and WHY it’s relevant to do so.
• Further explore the clinician’s role in impacting the SDH and discuss value in your clinical setting.
3
Oregon Primary Care Association
4
Our Mission is to lead the transformation of primary care to achieve health equity for all.
Why We believe that all people, in Oregon and beyond, have the right to good health and equitable health care.
How: OPCA supports health center sustainability while working to inspire and spread innovative approaches to providing better primary care to more people at less cost.
What:We connect, build the capacity of, and advocate for community health centers across Oregon.

What are the social determinants of health?
5

Definitions
Sources: ASTHO 2000, HW2020, WHO
Health inequity
Health equity
Differences in health outcomes between groups of people that are considered preventable, unjust or unfair.
Fairness in the distribution of resources and the freedom to achieve healthy outcomes between groups with differing levels of social disadvantage.
Differences in health outcomes between groups of people.
Health disparity
Social Determinants of HealthThe social determinants of health (SDH) are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life.

0
2
4
6
8
10
12
14
16
18
1980 1983 1986 1989 1992 1995 1998 2001 2004 2007 2010 2013
US (17.1%)
FR (11.6%)
SWE (11.5%)
GER (11.2%)
NETH (11.1%)
SWIZ (11.1%)
DEN (11.1%)
NZ (11.0%)
CAN (10.7%)
JAP (10.2%)
NOR (9.4%)
AUS (9.4%)*
UK (8.8%)
Notes: GDP refers to gross domestic product. Dutch and Swiss data are for current spending only, and exclude spending on capital formation of health care providers.
Source: http://www.commonwealthfund.org/publications/issue-briefs/2015/oct/us-health-care-from-a-global-perspective OECD Health Data 2015.
Health Care Spending as a Percentage of GDP
Percent

Despite this spending…
• Source: OECD Health Data 2009

9Health and Social Care Spending as % of GDP
Notes: GDP refers to Gross Domestic ProductSource: http://www.commonwealthfund.org/publications/issue-briefs/2015/oct/us-health-care-from-a-global-perspectiveE.H. Bradley and LA Taylor, The American health Care Paradox: Why Spending More is Getting Us Less, Public Affairs, 2013.

Pop Quiz #1
What Impacts Health?
IncomeEducation
Clinical care
Insurance
Housing Neighborhood
Social support
Health behaviors
FamilyCulture
AgeDoctor
Race

What Impacts Health?
Social Determinants of Health (SDoH)

Oregon by county…
Source: http://www.countyhealthrankings.org/app/oregon/2017/overview
2017 Health Factors 2017 Health Outcomes
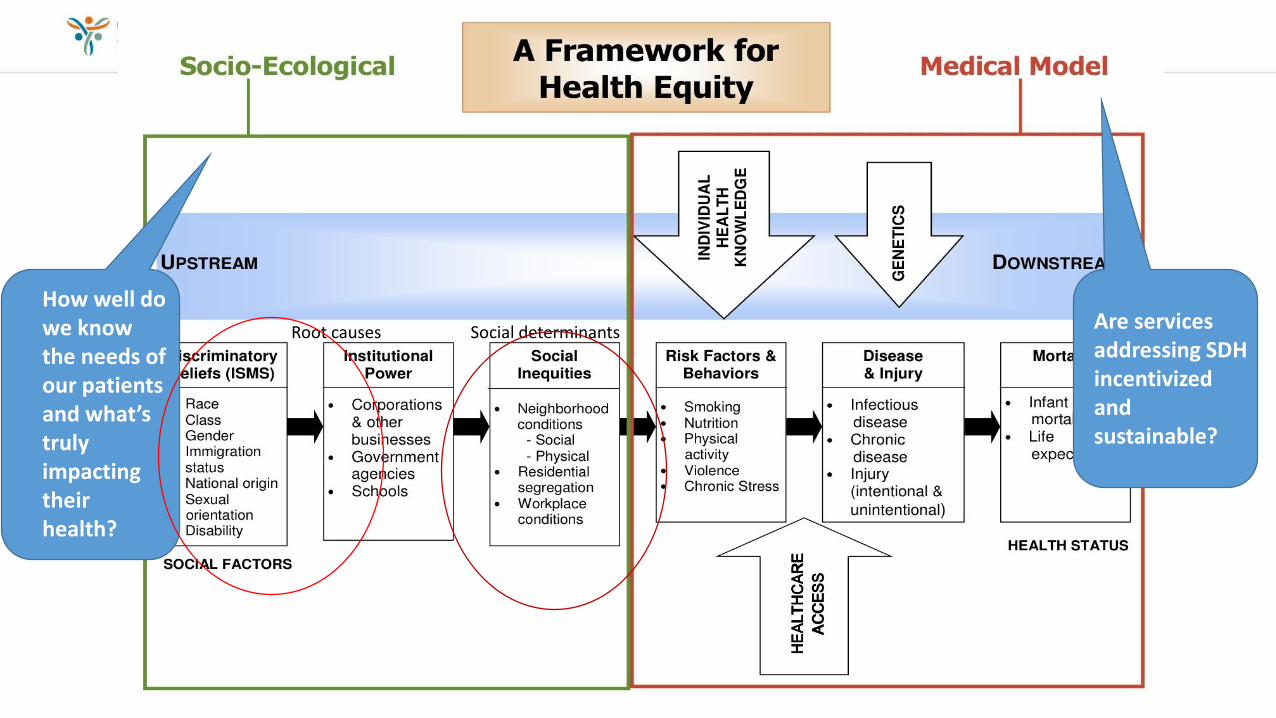
Social determinantsRoot causesAre services addressing SDH incentivized and sustainable?
How well do we know the needs of our patients and what’s truly impacting their health?

Unnatural Causes
• http://www.youtube.com/watch?feature=player_embedded&v=Btqq1yfk-9g

The 4 P’s
Source: Multnomah County Office of Diversity & Equity http://www.multco.us/sites/default/files/diversity-
equity/documents/lens_handouts-09272013.pdf

Intergenerational

Reproductive health & the cycle of poverty 17
Raised in poverty
Can’t afford an abortion
Lose pay short term (unpaid
medical leave)
Lose salary/wages
long term“For a woman who is already
struggling to make ends meet, being able to end an unintended
pregnancy is a critical component to her and her family’s ability to get out of
poverty.”
$435,049“Lost earnings of a full
time femaleworker over 40 years
due to thegender pay gap.”
Sources: National Women’s Law Center, “Employment: Fact Sheet: How the Wage Gap Hurts Women and Families,” April 2015, http:// www.nwlc.org/sites/default/ files/5.11.15_how_the_wage_gap_ hurts_women_and_families.pdf
Guttmacher Institute, “Fact Sheet: Unintended Pregnancy in the United States,” February 2015, http://www.guttmacher.org/pubs/FB-Unintended-Pregnancy-US.html

More inequality = less mobility
Higher inequality
Less
mo
bili
ty
Source: Journal of Economic Perspectives, Corak http://pubs.aeaweb.org/doi/pdfplus/10.1257/jep.27.3.79

Clinicians and the SDH
19

What impacts health?
Individual
Interpersonal
Institutions/Organizations
Community
Structures, policies, systems
Local, state, federal policies and laws to regulate/support health actions
Social networks, norms and standards
Rules, regulations, policies and informal structures
Family, peers, social networks and associations
Knowledge, attitudes, beliefs and behaviors
Largest impact
Smallest impact

Why should clinics care? 21
physicians believe that unmet social needs are leading to worse health among Americans.
physicians feel unable to address their patients health concerns caused by unmet social needs.
Social and economic
factors, 40%
Physical environment
10%
Clinical care, 20%
Health behaviors,
30%
Sources: Oregon Health Authority and Portland State University: https://www.oregon.gov/oha/pcpch/Documents/PCPCH-Program-Implementation-Report-Final-Sept-2016.pdf
RWJF 2011 http://www.rwjf.org/content/dam/web-assets/2011/11/2011-physicians--daily-life-report
Return on Investment = $13 to $1

What can clinicians do?
Meet legislator(s)
Engage with media
Be involved in local community organizing
Share SDoH with professional associations
Link patients to community services
Record social, economic patient information
Listen, empathize, connect
Source: Health Affairs Blog 2013 http://healthaffairs.org/blog/2013/02/22/the-us-health-disadvantage-and-clinicians-an-interview-with-paula-braveman/
“As a physician, I generally cannot discuss health with a patient who lives in poverty without talking about the areas where community development works: affordable housing, access to nutritious food, and safe places to play and exercise.”
~Risa Lavizzo-Mourey, MD MBAPresident and CEO, Robert Wood Johnson Foundation

Screening for social factors
23

Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences
SDH screening tool + implementation/action process
PRAPARE 24
Overall Project GoalTo create, implement/pilot test, and promote a national
standardized patient risk assessment protocol to assess and address patients’ social determinants of health (SDH)
+Assessment
Tool to Identify Needs in EHR
Protocol to Respond to
Needs

PRAPARE DOMAINS
Spanish and Chinese (Mandarin) translated versions
Find the tool at: www.nachc.org/prapare
25
Core
UDS SDH Domains Non-UDS SDH Domains (MU-3)
1. Race 10. Education
2. Ethnicity 11. Employment
3. Veteran Status 12. Material Security
4. Farmworker Status 13. Social Isolation
5. English Proficiency 14. Stress
6. Income 15. Transportation
7. Insurance 16. Housing Stability
8. Neighborhood
9. Housing Status
Optional
1. Incarceration History
3. Domestic Violence
2. Safety 4. Refugee Status
PRAPARE domains

• 16 core questions
• 9 of which already collected by health centers through federal reporting (UDS)
• All align with national initiatives
• Design
• Vetted and stakeholder engaged development process
• In the EHR to facilitate assessment & interventions (free templates)
• Common core yet flexible: • Able to make more granular and/or add questions
• Focus on standardizing the need/data, not question
• Can be used in combination with other tools/data
• Conversation starter and patient-centered
26PRAPARE is unique and feasible
PRAPARE nationally….
• Health centers and/or PCAs in every state including AK have expressed interest in PRAPARE
• Health centers in over 30 states including AK downloaded PRAPARE EHR Templates
• 600 CHCs or health systems are using PRAPARE
• National team just kicked off Train-the-Trainer Academy in August!
27
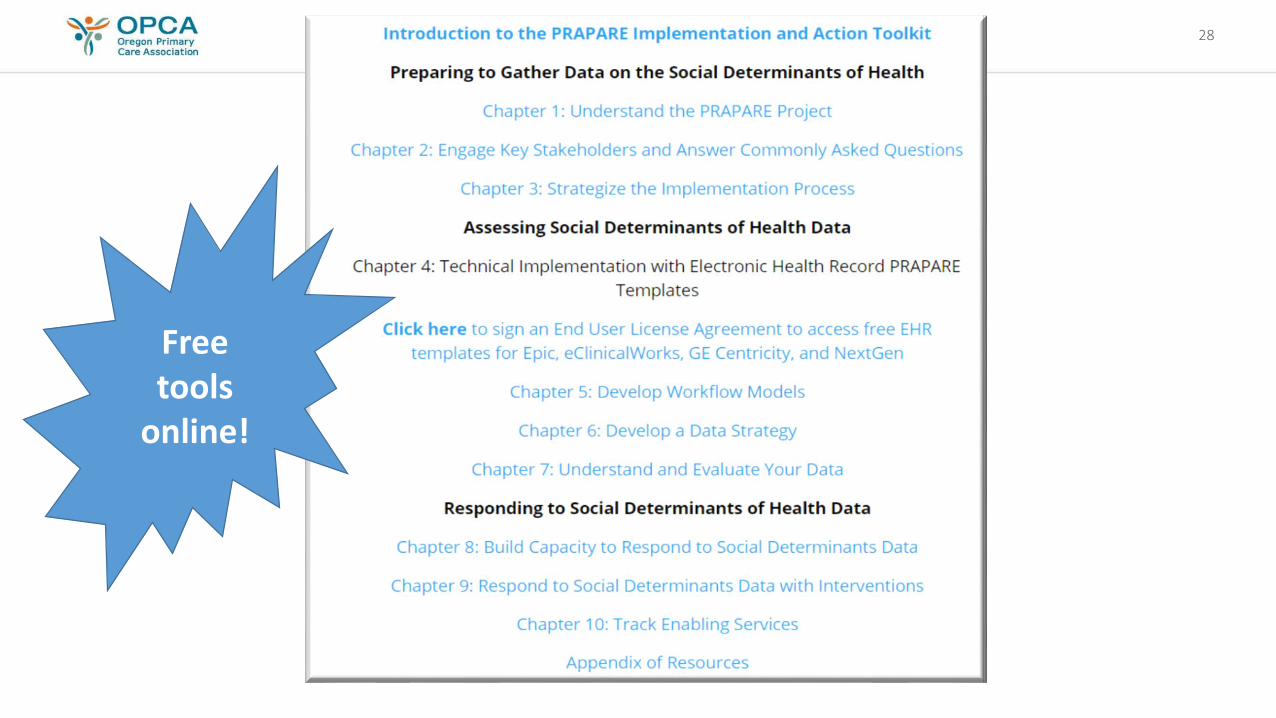
28
Free tools
online!

29Sample Workflows: A Variety of Approaches!

30

31Immediate uses for the data
Challenge: Inability to Address SDH
Solution: Message “Have to start somewhere and do the best we can with what we have. Collecting information will
help us figure out what services to provide”.
Incorporate PRAPARE into other aspects and initiatives at health
center: QI meetings, board meetings, ACO discussions so
staff see value in this work
Models to Address SDH:1) Referrals with partnerships
2) Active/Formal Collaboration of multiple agencies under one
funded mechanism3) Co-location
4) New members of the care team
Catalog current resources available to address SDH needs, both in-house and in
community (community resource guide)
Identify resources that need to be developed
and/or community partnerships that need to
be initiated or strengthened

Opportunities and other plans to use the data
Inform Care and Services:
Inform services provided in Collaborative Consortia Model and Co-Location Model
Build/strengthen partnerships with local orgs. Ex: Negotiate bulk discounts and new bus routes
with local transportation agency
Build on SDH and “Touches” work
Inform Payment
Guide work of co-located foundation to pay for non-clinical services
Inform both Medicaid and Medicare ACO
discussions and care management policies
Inform payment reform discussions with state Medicaid
agency
Inform Risk Adjustment
Create SDH risk score for risk stratification and risk adjustment
Streamline and expand care management plans
Assign weights: Put every PRAPARE
element in regression model with certain
outcome or cost
Inform APM discussions at state
level
Listening is an inherent good for patients and professionals.
33
© Oregon Primary Care Association

Why this work matters
34
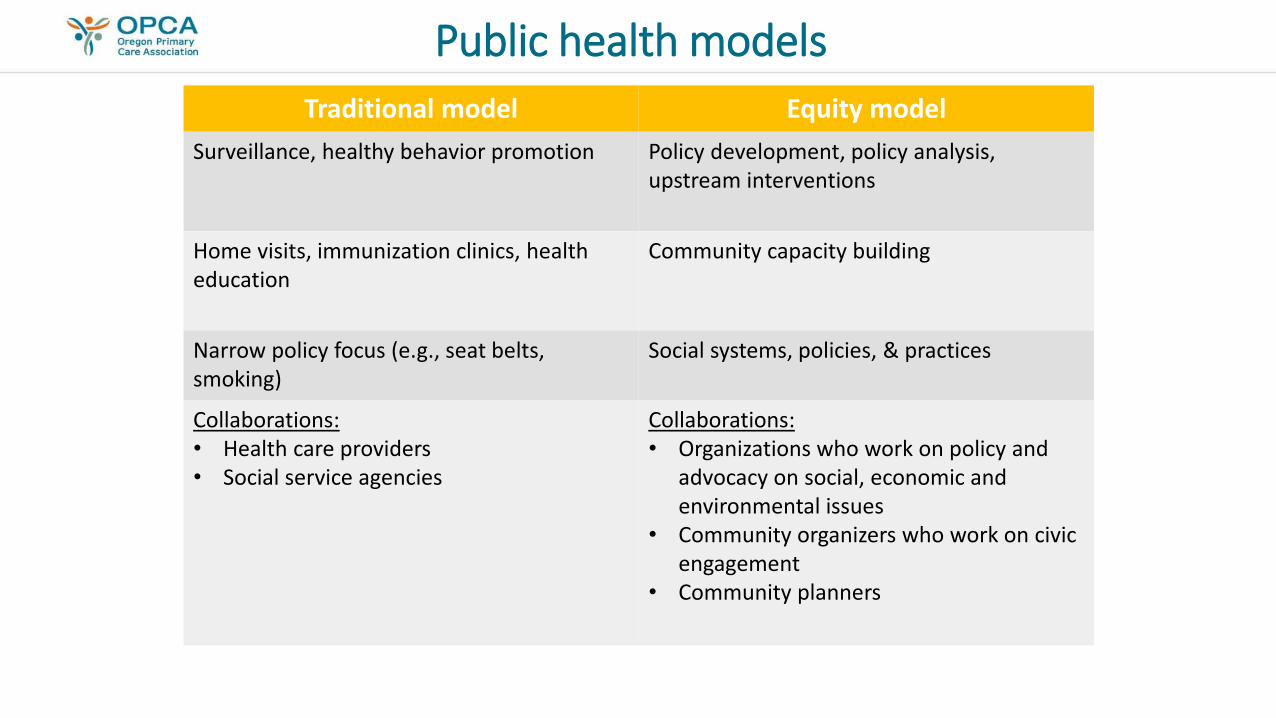
Public health models
Traditional model Equity model
Surveillance, healthy behavior promotion Policy development, policy analysis, upstream interventions
Home visits, immunization clinics, health education
Community capacity building
Narrow policy focus (e.g., seat belts, smoking)
Social systems, policies, & practices
Collaborations: • Health care providers • Social service agencies
Collaborations: • Organizations who work on policy and
advocacy on social, economic and environmental issues
• Community organizers who work on civic engagement
• Community planners

Priorities
Medical services 88%
Other 8%
Health behaviors
4%
Physical Environment 10%
Clinical care 20%
Health behaviors 30%
Socioeconomic factors 40%
What Makes Us Healthy What We Spend On Being Healthy
Source: RWJF County Health Rankings Source: Derived from information from the Boston Foundation (June 2007).
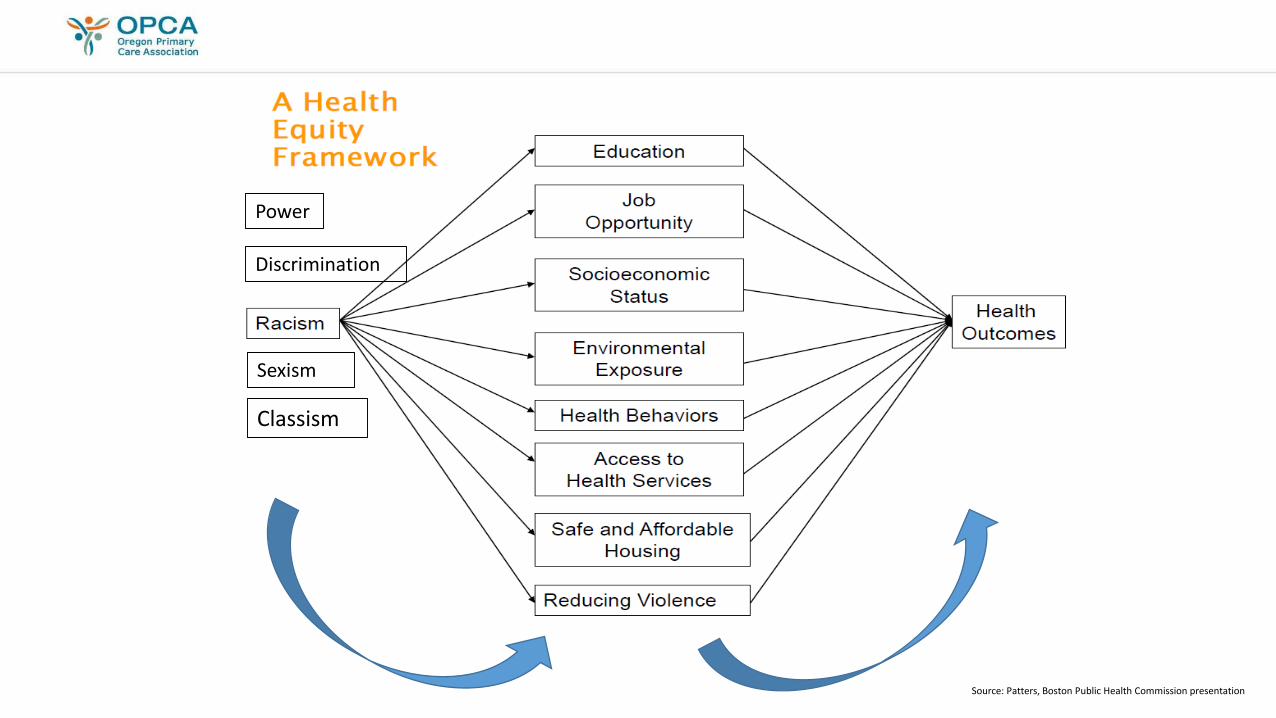
Discrimination
Sexism
Power
Source: Patters, Boston Public Health Commission presentation
Classism

Policies affect SES and SES affect health
Policies, institutions, systemsEg: Labor sphere, education sphere, social inclusion,
racism/discrimination
Health determinantsEg: Income, education, housing, childcare,
employment/vocational training, social support
Mediators of healthE.g: Lack of resources and access, constraints on
healthy behaviors, chronic stress
Health outcomes & health inequities
“Sharpening our focus on social & economic opportunity, enhancing the environments in which we live, and setting new priorities for policies and spending that optimize those conditions are our best hope for improving health…” – The Health of the States Report 2016
Source: VCU https://societyhealth.vcu.edu/media/society-health/pdf/HOTS-SummaryReport-FINAL.pdf
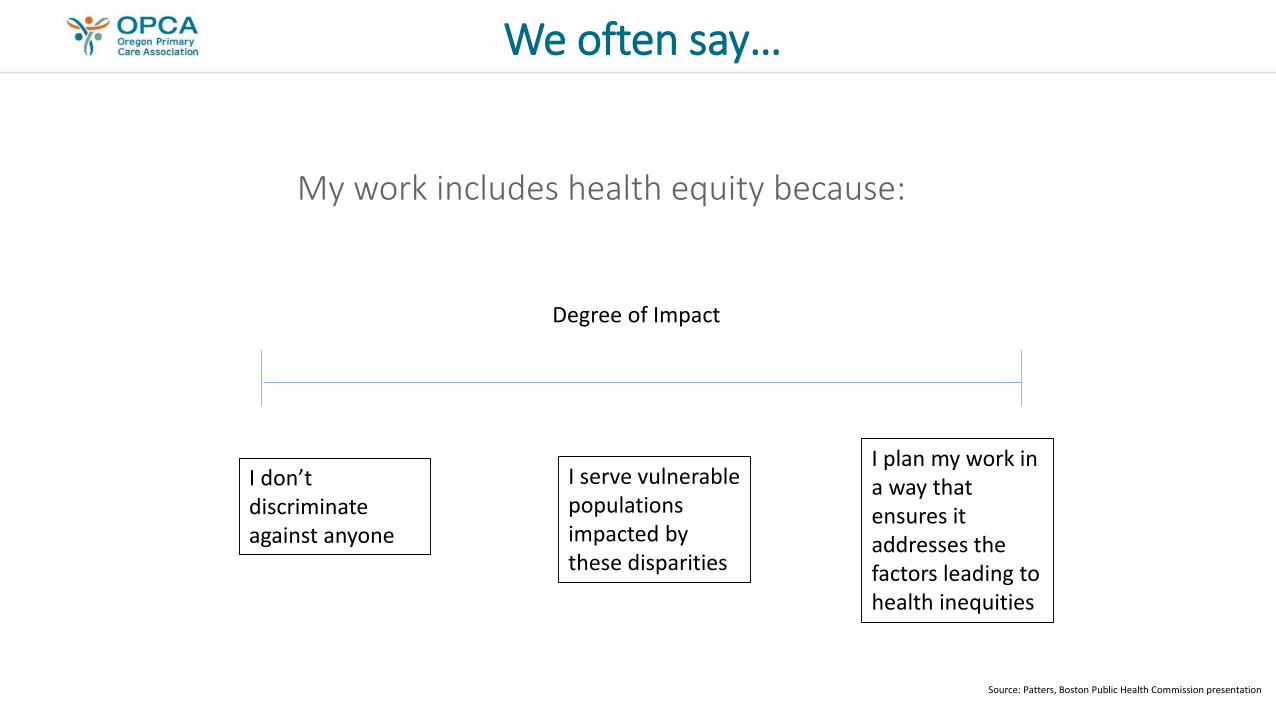
We often say…
My work includes health equity because:
Degree of Impact
I don’t discriminate against anyone
I serve vulnerable populations impacted by these disparities
I plan my work in a way that ensures it addresses the factors leading to health inequities
Source: Patters, Boston Public Health Commission presentation

How can we all get here?
Degree of Impact
I don’t discriminate against anyone
I serve vulnerable populations impacted by these disparities
I plan my work in a way that ensures it addresses the factors leading to health inequities
Source: Patters, Boston Public Health Commission presentation

Reshaping the model
Source: Braveman,P et al. The Social Determinants of Health: Coming of Age. Annual Review of Public Health 2011; 389-98.

43
Group questions
• What are the biggest social determinant of health issues impacting the patients your clinic sees?
• Why do you believe these issues exist?
• Can you see value in screening patients for their SDH?
• What might this look like in your clinical setting? Who asks the questions? Where in the visit/workflow? Is it recorded in the EHR? What do you envision doing with that data?
• What are some barriers you envision encountering?