Long-term follow-up of the PI3Kδ inhibitor TGR-1202 … · 2019-03-18 · Long-term follow-up of...
1
Long-term follow-up of the PI3Kδ inhibitor TGR-1202 demonstrates a differentiated safety profile and high response rates in CLL and NHL: Integrated-analysis of TGR-1202 monotherapy and combined with ublituximab Howard A. Burris III, MD 1,2 , Ian W. Flinn, MD, PhD 1,2 , Matthew Lunning, DO 3 , Julie Vose, MD 3 , Nathan Fowler, MD 4 , Loretta Nastoupil, MD 4 , Susan O’Brien, MD 5 , Marshall T. Schreeder, MD 6 , Manish R. Patel, MD 2,7 , Timothy S. Fenske, MD 8 , Danielle M. Brander, MD 9 , Tanya Siddiqi, MD 10 , Christopher Flowers, MD 11 , Jan A. Burger, MD 4 , William G. Wierda, MD 4 , John G Kuhn, PharmD 12 , Peter Sportelli 13 , Hari P. Miskin, MS 13 , Michael S. Weiss 13 and Owen A. O’Connor, MD, PhD 14 1 Tennessee Oncology, PLLC, Nashville, TN; 2 Sarah Cannon Research Institute, Nashville, TN; 3 University of Nebraska Medical Center, Omaha, NE; 4 MD Anderson Cancer Center, Houston, TX; 5 University of California Irvine, Orange, CA; 6 Clearview Cancer Institute, Huntsville, AL; 7 Florida Cancer Specialists, Sarasota, FL; 8 Medical College of Wisconsin, Milwaukee, WI; 9 Duke University Medical Center, Durham, NC; 10 City of Hope National Medical Center, Duarte, CA; 11 Emory University/Winship Cancer Institute, Atlanta, GA; 12 University of Texas Health Science Center at San Antonio, San Antonio, TX; 13 TG Therapeutics, Inc., New York, NY; 14 Columbia University Medical Center, New York, NY Background PI3Kδ is highly expressed in cells of hematopoietic origin and is often upregulated in lymphoid malignancies TGR-1202 (TGR) is a next generation PI3Kδ inhibitor, with a unique structure and activity profile distinct from other PI3Kδ inhibitors in development, including: Presented at the 2016 American Society of Clinical Oncology (ASCO) Conference, June 3 – 7, 2016 Results A prolonged half-life that enables once-daily dosing A differentiated safety profile from other PI3Kδ inhibitors in development Fold-selectivity Isoform PI3Kα PI3Kβ PI3Kγ PI3Kδ TGR-1202 >1000 >50 >48 1 1 Idelalisib >300 >200 >40 1 2 IPI-145 >640 >34 >11 1 1 Flinn et al. 2009, 2 Porter et al. 2012 Demographics Safety Efficacy Conclusions TGR-1202 is well tolerated and highly active in a broad population of heavily pretreated & high-risk patients with NHL & CLL, with the addition of ublituximab to TGR-1202 exhibiting greater frequency and depth of response over TGR-1202 monotherapy Discontinuations due to adverse events have been limited (~8%); GR3/4 events most associated with PI3K delta inhibitors have been rare, including pneumonia (~5%) and pneumonitis (<1.5%), ALT/AST elevations (~3%) and colitis (<1.5%), the latter occurring with no apparent association to time on therapy Safety profile supports additional multi-drug regimens: triple therapy combinations adding novel agents to ublituximab and TGR-1202 are ongoing (including ibrutinib, bendamustine, and pembrolizumab) with additional triple therapy studies planned Marked activity observed in CLL and DLBCL being explored further in registration directed UNITY-CLL Phase 3 Study and UNITY-DLBCL Study, with UNITY-iNHL study to commence by YE 2016 Ublituximab (TG-1101, UTX) is a novel, chimeric monoclonal antibody targeting a unique epitope on the CD20 antigen, and glycoengineered to enhance affinity for all variants of FcγRIIIa receptors, thereby demonstrating greater antibody-dependent cellular cytotoxicity (ADCC) activity than rituximab and ofatumumab. Phase I trials of single agent ublituximab in patients with relapsed/refractory CLL and NHL reported impressive response rates with rapid and sustained lymphocyte depletion. Red: Amino acids contributing to ofatumumab binding Yellow: Amino acids essential for rituximab, but not ofatumumab binding Purple: Core amino acids of ublituximab epitope TGR-1202 Ublituximab Study UTX-TGR-103 (NCT02006485) is a Ph I/Ib trial evaluating the combination of ublituximab + TGR-1202 in patients with relapsed or refractory NHL and CLL. The study is divided into two parts: Phase I: 3+3 escalation evaluating Cycle 1 DLTs Phase Ib: Dose Expansion Cohort UTX Dose TGR Dose (QD) 1 900/600 mg NHL/CLL 800 mg 2 900/600 mg NHL/CLL 1200 mg 3 900 mg 400 mg (micronized) 4 900 mg 600 mg (micronized) 5 900 mg 800 mg (micronized) 6 900 mg 1000 mg (micronized) 7 900 mg 1200 mg (micronized) Expansion TGR-1202 at 800 mg, 1000 mg, and 1200 mg micronized Study Design Efficacy is assessed Week 8, and every 12 weeks thereafter. After Month 12, all patients remain on TGR-1202 single agent. Ublituximab was initially administered on Days 1, 8 and 15 of Cycles 1 & 2 and Day 1 of Cycles 4, 6, 9 & 12. The protocol was amended to use a more convenient schedule as follows: Dose Escalation Schema: Treatment Schedule: All Causality AE’s Occurring in ≥ 10% of Patients (n = 165) <8% of patients discontinued due to a TGR-1202 related AE 13% of patients had a TGR-1202 dose reduction Grade 3/4 AST/ALT increase was 3% (8% all grades), predominantly observed above the Phase 3 dose Grade 3/4 pneumonia occurred in 5% of patients (8% all grades) Two events of pneumonitis (<1.5%) were reported Two cases of colitis (<1.5%) have been reported at doses exceeding the Phase 3 dose and did not appear to be time dependent (1000 mg and 1200 mg, at 4 mos. and 24 mos., respectively, after initiating therapy). Patients Exposed to TGR-1202 at 800 Micro Type Pts (n) CR (n) PR (n) ORR n (%) SD (n) PD (n) CLL/SLL 16 2 12 14 (88%) 2 0 DLBCL 7 1 3 4 (57%) 2 1 iNHL 17 3 6 9 (53%) 6 2 Higher Doses: 1200 mg of the initial formulation, or ≥600 mg of the micronized formulation ORR in iNHL for patients treated at Higher Doses was not only greater with the combo (55%) as opposed to monotherapy (41%), but the depth of response was significantly greater with the addition of UTX (CR rate of 5% for monotherapy vs. 30% for the combo) Similarly, 3 complete responses observed in patients with DLBCL treated at Higher Doses occurred in patients receiving TGR + UTX An exploratory subset of patients with ibrutinib refractory CLL were treated with TGR + UTX and analyzed separately due to the aggressive nature of their disease A strong dose response was observed, with patients exposed to 800 mg of the micronized formulation achieving higher rates of response Best Percent Change from Baseline in Disease Burden Patients Treated at “Higher Doses” of TGR-1202 Cycle 6 Cycle 12 Cycle 1 TGR-1202 DAILY UBLITUXIMAB INFUSIONS Cycle 2 Cycle 9 Cycle 4 Cycle 3 Cycle 5 Phase 3 UNITY-CLL Study Ublituximab + TGR-1202 Obinutuzumab + Chlorambucil Ublituximab TGR-1202 RANDOMIZE (1:1:1:1) Companion study of Ublituximab + TGR-1202 Available on progression o Design, Endpoints, and Statistics agreed to via Special Protocol Assessment (SPA) o Enrolling patients with treatment naïve and previously treated CLL o Study Chair: John Gribben, MD, PhD o Clinical trials.gov #: NCT02612311 UNITY Registration Program iNHL DLBCL TGR-1202-101: TGR-1202 Monotherapy UTX-TGR-103: TGR-1202 in Combination with Ublituximab Study TGR-1202-101 (NCT01767766) is a first-in- human, Phase I study of TGR-1202 in patients with relapsed or refractory hematologic malignancies TGR-1202 dosed orally once-daily (QD) in continuous 28 Day Cycles Dose-limiting toxicities (DLTs) assessed in Cycle 1 prior to escalation Intra-patient dose escalation allowed for patients in previous cohorts following establishment of safety at higher doses 3+3 Dose Escalation Schema: Micronized TGR-1202 Dose Escalation Schema: Evaluable for Safety (n) 165 (90 Single Agent, 75 Combo with UTX) Median Age, years (range) 65 (22 - 86) Male/Female 106/59 Histology CLL 43 FL 42 DLBCL 40 MZL 11 HL 11 MCL 8 SLL 3 WM 3 T-Cell 2 HCL 1 Richter's 1 Median ECOG 1 Prior Therapies, median (range) 3 (0 - 14) Patients with ≥ 3 Prior Therapies (%) 94 (57%) Patients Refractory to Prior Therapy (%) 85 (52%) Adverse Event All Grades Grade 3/4 N % N % Diarrhea 78 47% 5 3% Nausea 74 45% 2 1% Fatigue 61 37% 5 3% Vomiting 44 27% 0 0% Neutropenia 34 21% 30 18% Cough 32 19% 0 0% Dyspnea 30 18% 6 4% Dizziness 29 18% 0 0% Headache 28 17% 2 1% Pyrexia 26 16% 2 1% Decreased appetite 26 16% 0 0% Rash 26 16% 6 4% Sinusitis 25 15% 2 1% Anemia 24 15% 9 5% Constipation 24 15% 1 1% Insomnia 23 14% 0 0% Hypokalemia 22 13% 5 3% Back pain 20 12% 1 1% Abdominal pain 18 11% 4 2% Upper respiratory infection 18 11% 0 0% Cyto- genetics # of Prior Lines Prior Therapies % SPD reduction ORR Status 11q 4 1. R-Benda 2. Ofatumumab 3. Ibrutinib 4. Ibrutinib -100% PR On Study 17p 2 1. R-Fludarabine 2. Ibrutinib -37% SD Off (PD) 17p, p53 2 1. Ibrutinib 2. Bendamustine & CAR T-cell -55% PD Off (PD) No del 5 1. FCR 2. R-Benda 3. FCR 4. Campath+R 5. Ibrutinib +25% PD Off (PD) All patients were treated with 800 mg of TGR-1202 in combination with ublituximab Ibrutinib Refractory Patients treated with TGR + UTX Phase 2b UNITY-DLBCL Study o Enrolling patients with previously treated DLBCL of all subtypes o US Study Chair: Owen A. O’Connor, MD, PhD o Ex-US Study Chair: Pier-Luigi Zinzani, MD, PhD Ublituximab + TGR-1202 TGR-1202 RANDOMIZE (1:1) 0 168 336 504 672 840 1008 1176 FL WM DLBCL DLBCL DLBCL DLBCL DLBCL DLBCL DLBCL DLBCL CLL DLBCL DLBCL FL DLBCL HL FL MCL DLBCL DLBCL FL DLBCL T-cell DLBCL DLBCL CLL CLL HL DLBCL DLBCL FL DLBCL HL DLBCL FL HL HL MCL DLBCL DLBCL FL CLL DLBCL DLBCL MCL DLBCL MCL CLL HCL HL DLBCL CLL FL CLL MCL FL FL HL FL FL FL FL FL CLL CLL DLBCL CLL FL HL DLBCL MCL DLBCL CLL MZL FL HL SLL MZL DLBCL CLL CLL MZL FL T-cell CLL HL CLL FL FL MCL DLBCL CLL CLL CLL FL SLL CLL WM FL MZL CLL FL FL FL CLL FL CLL CLL FL WM CLL FL CLL FL FL DLBCL CLL CLL CLL MZL CLL CLL/Richters FL FL HL FL CLL CLL DLBCL DLBCL FL DLBCL SLL MZL MZL MZL CLL FL CLL DLBCL MZL DLBCL CLL CLL FL FL CLL CLL CLL MCL FL CLL FL CLL DLBCL DLBCL CLL DLBCL FL MZL FL CLL MZL FL CLL Days on Study 12 cycles 24 cycles 36 cycles 6 cycles Duration on Study (n=165) Extended durations of exposure: 80 patients for 6+ cycles 43 patients for 12+ cycles 14 patients for 24+ cycles Longest patients on daily TGR-1202 for 3+ years -100% -75% -50% -25% 0% 25% 1202 Single Agent 1202 + ublituximab Overall Response Rate At Phase 3 Dose CLL/SLL -100% -75% -50% -25% 0% 25% 1202 Single Agent 1202 + ublituximab 17p/11q del -100% -75% -50% -25% 0% 25% 1202 Single Agent 1202 + ublituximab G = GCB G G G G G G G G CLL/SLL PR includes 1 patient with persistent lymphocytosis iNHL = FL & MZL
Transcript of Long-term follow-up of the PI3Kδ inhibitor TGR-1202 … · 2019-03-18 · Long-term follow-up of...

Long-term follow-up of the PI3Kδ inhibitor TGR-1202 demonstrates a differentiated safety profile and high response rates in CLL and NHL:
Integrated-analysis of TGR-1202 monotherapy and combined with ublituximabHoward A. Burris III, MD1,2, Ian W. Flinn, MD, PhD1,2, Matthew Lunning, DO3, Julie Vose, MD3, Nathan Fowler, MD4, Loretta Nastoupil, MD4, Susan O’Brien, MD5, Marshall T. Schreeder, MD6, Manish R. Patel, MD2,7, Timothy S. Fenske, MD8, Danielle M. Brander, MD9,
Tanya Siddiqi, MD10, Christopher Flowers, MD11, Jan A. Burger, MD4, William G. Wierda, MD4, John G Kuhn, PharmD12, Peter Sportelli13, Hari P. Miskin, MS13, Michael S. Weiss13 and Owen A. O’Connor, MD, PhD14
1Tennessee Oncology, PLLC, Nashville, TN; 2Sarah Cannon Research Institute, Nashville, TN; 3University of Nebraska Medical Center, Omaha, NE; 4MD Anderson Cancer Center, Houston, TX; 5University of California Irvine, Orange, CA; 6Clearview Cancer Institute, Huntsville, AL; 7Florida Cancer Specialists, Sarasota, FL; 8Medical College of Wisconsin, Milwaukee, WI;9Duke University Medical Center, Durham, NC; 10City of Hope National Medical Center, Duarte, CA; 11Emory University/Winship Cancer Institute, Atlanta, GA; 12University of Texas Health Science Center at San Antonio, San Antonio, TX; 13TG Therapeutics, Inc., New York, NY; 14Columbia University Medical Center, New York, NY
Background
PI3Kδ is highly expressed in cells of hematopoietic originand is often upregulated in lymphoid malignancies
TGR-1202 (TGR) is a next generation PI3Kδ inhibitor, witha unique structure and activity profile distinct from otherPI3Kδ inhibitors in development, including:
Presented at the 2016 American Society of Clinical Oncology (ASCO) Conference, June 3 – 7, 2016
Results
A prolonged half-life that enablesonce-daily dosing
A differentiated safety profilefrom other PI3Kδ inhibitors indevelopment
Fold-selectivity
Isoform PI3Kα PI3Kβ PI3Kγ PI3Kδ
TGR-1202 >1000 >50 >48 1
1Idelalisib >300 >200 >40 1
2IPI-145 >640 >34 >11 11Flinn et al. 2009, 2Porter et al. 2012
Demographics
Safety
Efficacy
Conclusions TGR-1202 is well tolerated and highly active in a broad population of heavily
pretreated & high-risk patients with NHL & CLL, with the addition of ublituximabto TGR-1202 exhibiting greater frequency and depth of response over TGR-1202monotherapy
Discontinuations due to adverse events have been limited (~8%); GR3/4 eventsmost associated with PI3K delta inhibitors have been rare, including pneumonia(~5%) and pneumonitis (<1.5%), ALT/AST elevations (~3%) and colitis (<1.5%), thelatter occurring with no apparent association to time on therapy
Safety profile supports additional multi-drug regimens: triple therapycombinations adding novel agents to ublituximab and TGR-1202 are ongoing(including ibrutinib, bendamustine, and pembrolizumab) with additional tripletherapy studies planned
Marked activity observed in CLL and DLBCL being explored further in registrationdirected UNITY-CLL Phase 3 Study and UNITY-DLBCL Study, with UNITY-iNHL studyto commence by YE 2016
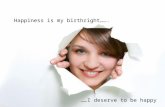
Ublituximab (TG-1101, UTX) is a novel, chimericmonoclonal antibody targeting a unique epitope on theCD20 antigen, and glycoengineered to enhance affinity forall variants of FcγRIIIa receptors, thereby demonstratinggreater antibody-dependent cellular cytotoxicity (ADCC)activity than rituximab and ofatumumab.
Phase I trials of single agent ublituximab in patients withrelapsed/refractory CLL and NHL reported impressiveresponse rates with rapid and sustained lymphocytedepletion.
Red: Amino acids contributing to
ofatumumab bindingYellow: Amino acids
essential for rituximab, but not ofatumumab bindingPurple: Core amino acids of ublituximab epitope
TGR-1202 Ublituximab
Study UTX-TGR-103 (NCT02006485) is a Ph I/Ibtrial evaluating the combination of ublituximab +TGR-1202 in patients with relapsed or refractoryNHL and CLL. The study is divided into two parts:
Phase I: 3+3 escalation evaluating Cycle 1 DLTs
Phase Ib: Dose Expansion
Cohort UTX Dose TGR Dose (QD)
1 900/600 mg NHL/CLL 800 mg
2 900/600 mg NHL/CLL 1200 mg
3 900 mg 400 mg (micronized)
4 900 mg 600 mg (micronized)
5 900 mg 800 mg (micronized)
6 900 mg 1000 mg (micronized)
7 900 mg 1200 mg (micronized)
Expansion TGR-1202 at 800 mg, 1000 mg, and 1200 mg micronized
Study Design
Efficacy is assessed Week 8, and every12 weeks thereafter. After Month 12, allpatients remain on TGR-1202 singleagent. Ublituximab was initiallyadministered on Days 1, 8 and 15 ofCycles 1 & 2 and Day 1 of Cycles 4, 6, 9 &12. The protocol was amended to use amore convenient schedule as follows:
Dose Escalation Schema:
Treatment Schedule:
All Causality AE’s Occurring in ≥ 10% of Patients (n = 165)
<8% of patients discontinued due to a TGR-1202 related AE 13% of patients had a TGR-1202 dose reduction Grade 3/4 AST/ALT increase was 3% (8% all grades), predominantly
observed above the Phase 3 dose Grade 3/4 pneumonia occurred in 5% of patients (8% all grades) Two events of pneumonitis (<1.5%) were reported Two cases of colitis (<1.5%) have been reported at doses exceeding the
Phase 3 dose and did not appear to be time dependent (1000 mg and1200 mg, at 4 mos. and 24 mos., respectively, after initiating therapy).
Patients Exposed to TGR-1202 at 800 Micro
TypePts (n)
CR(n)
PR(n)
ORRn (%)
SD(n)
PD(n)
CLL/SLL 16 2 12 14 (88%) 2 0
DLBCL 7 1 3 4 (57%) 2 1
iNHL 17 3 6 9 (53%) 6 2
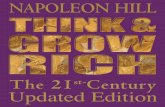
Higher Doses: 1200 mg of the initialformulation, or ≥600 mg of the micronizedformulation
ORR in iNHL for patients treated at HigherDoses was not only greater with the combo(55%) as opposed to monotherapy (41%),but the depth of response was significantlygreater with the addition of UTX (CR rate of5% for monotherapy vs. 30% for the combo)
Similarly, 3 complete responses observed inpatients with DLBCL treated at Higher Dosesoccurred in patients receiving TGR + UTX
An exploratory subset of patients withibrutinib refractory CLL were treated withTGR + UTX and analyzed separately due tothe aggressive nature of their disease
A strong dose response was observed, withpatients exposed to 800 mg of themicronized formulation achieving higherrates of response
Best Percent Change from Baseline in Disease BurdenPatients Treated at “Higher Doses” of TGR-1202
Cycle 6 Cycle 12
Cycle 1
TGR-1202 DAILY
UBLITUXIMAB INFUSIONS
Cycle 2 Cycle 9Cycle 4Cycle 3 Cycle 5
Phase 3 UNITY-CLL Study
Ublituximab + TGR-1202
Obinutuzumab
+ Chlorambucil
Ublituximab
TGR-1202
RA
ND
OM
IZE
(1:1
:1:1
)
Companion
study of
Ublituximab
+
TGR-1202
Available on
progression
o Design, Endpoints, and Statistics agreed to via Special Protocol Assessment (SPA)
o Enrolling patients with treatment naïve and previously treated CLL
o Study Chair: John Gribben, MD, PhD
o Clinical trials.gov #: NCT02612311
UNITY Registration Program
iNHLDLBCL
TGR-1202-101: TGR-1202 Monotherapy
UTX-TGR-103: TGR-1202 in Combination with Ublituximab
Study TGR-1202-101 (NCT01767766) is a first-in-human, Phase I study of TGR-1202 in patients withrelapsed or refractory hematologic malignancies TGR-1202 dosed orally once-daily (QD) in
continuous 28 Day Cycles Dose-limiting toxicities (DLTs) assessed in Cycle
1 prior to escalation Intra-patient dose escalation allowed for
patients in previous cohorts followingestablishment of safety at higher doses
3+3 Dose Escalation Schema:
Micronized TGR-1202Dose Escalation Schema:
Evaluable for Safety (n)165
(90 Single Agent, 75 Combo with UTX)
Median Age, years (range) 65 (22 - 86)Male/Female 106/59
Histology
CLL 43FL 42
DLBCL 40MZL 11HL 11
MCL 8SLL 3
WM 3T-Cell 2HCL 1
Richter's 1Median ECOG 1Prior Therapies, median (range) 3 (0 - 14)Patients with ≥ 3 Prior Therapies (%) 94 (57%)Patients Refractory to Prior Therapy (%) 85 (52%)
Adverse EventAll Grades Grade 3/4
N % N %Diarrhea 78 47% 5 3%Nausea 74 45% 2 1%Fatigue 61 37% 5 3%Vomiting 44 27% 0 0%Neutropenia 34 21% 30 18%Cough 32 19% 0 0%Dyspnea 30 18% 6 4%Dizziness 29 18% 0 0%Headache 28 17% 2 1%Pyrexia 26 16% 2 1%Decreased appetite 26 16% 0 0%Rash 26 16% 6 4%Sinusitis 25 15% 2 1%Anemia 24 15% 9 5%Constipation 24 15% 1 1%Insomnia 23 14% 0 0%Hypokalemia 22 13% 5 3%Back pain 20 12% 1 1%Abdominal pain 18 11% 4 2%Upper respiratory infection 18 11% 0 0%
Cyto-genetics
# of Prior Lines
Prior Therapies% SPD
reductionORR Status
11q 41. R-Benda2. Ofatumumab
3. Ibrutinib4. Ibrutinib
-100% PR On Study
17p 21. R-Fludarabine2. Ibrutinib
-37% SD Off (PD)
17p, p53 21. Ibrutinib2. Bendamustine & CAR T-cell
-55% PD Off (PD)
No del 51. FCR2. R-Benda3. FCR
4. Campath+R5. Ibrutinib
+25% PD Off (PD)
All patients were treated with 800 mg of TGR-1202 in combination with ublituximab
Ibrutinib Refractory Patients treated with TGR + UTX
Phase 2b UNITY-DLBCL Study
o Enrolling patients with previously treated DLBCL of all subtypes
o US Study Chair: Owen A. O’Connor, MD, PhD
o Ex-US Study Chair: Pier-Luigi Zinzani, MD, PhD Ublituximab + TGR-1202
TGR-1202
RA
ND
OM
IZE
(1:1
)
0 168 336 504 672 840 1008 1176
FL
WM
DLBCL
DLBCL
DLBCL
DLBCL
DLBCL
DLBCL
DLBCL
DLBCL
CLL
DLBCL
DLBCL
FL
DLBCL
HL
FL
MCL
DLBCL
DLBCL
FL
DLBCL
T-cell
DLBCL
DLBCL
CLL
CLL
HL
DLBCL
DLBCL
FL
DLBCL
HL
DLBCL
FL
HL
HL
MCL
DLBCL
DLBCL
FL
CLL
DLBCL
DLBCL
MCL
DLBCL
MCL
CLL
HCL
HL
DLBCL
CLL
FL
CLL
MCL
FL
FL
HL
FL
FL
FL
FL
FL
CLL
CLL
DLBCL
CLL
FL
HL
DLBCL
MCL
DLBCL
CLL
MZL
FL
HL
SLL
MZL
DLBCL
CLL
CLL
MZL
FL
T-cell
CLL
HL
CLL
FL
FL
MCL
DLBCL
CLL
CLL
CLL
FL
SLL
CLL
WM
FL
MZL
CLL
FL
FL
FL
CLL
FL
CLL
CLL
FL
WM
CLL
FL
CLL
FL
FL
DLBCL
CLL
CLL
CLL
MZL
CLL
CLL/Richters
FL
FL
HL
FL
CLL
CLL
DLBCL
DLBCL
FL
DLBCL
SLL
MZL
MZL
MZL
CLL
FL
CLL
DLBCL
MZL
DLBCL
CLL
CLL
FL
FL
CLL
CLL
CLL
MCL
FL
CLL
FL
CLL
DLBCL
DLBCL
CLL
DLBCL
FL
MZL
FL
CLL
MZL
FL
CLL
Days on Study
12 cycles 24 cycles 36 cycles6 cycles
Duration on Study (n=165)
Extended durations of exposure: 80 patients for 6+ cycles 43 patients for 12+ cycles 14 patients for 24+ cycles Longest patients on daily TGR-1202 for 3+ years
-100%
-75%
-50%
-25%
0%
25%
1202 Single Agent
1202 + ublituximab
Overall Response Rate At Phase 3 Dose
CLL/SLL
-100%
-75%
-50%
-25%
0%
25%
1202 Single Agent
1202 + ublituximab
17p/11q del
-100%
-75%
-50%
-25%
0%
25%
1202 Single Agent
1202 + ublituximab
G = GCB
GG GGGG
GG
CLL/SLL PR includes 1 patient with persistent lymphocytosis iNHL = FL & MZL