How public policy could enable Knowledge Based Economy: The Tunisian Healthcare case study
Upload
posy-meltonCategory
view
215download
1
Long-term clinical service strategy
How healthcare could be provided in the future for local communities
How healthcare could be provided in the future for local communities
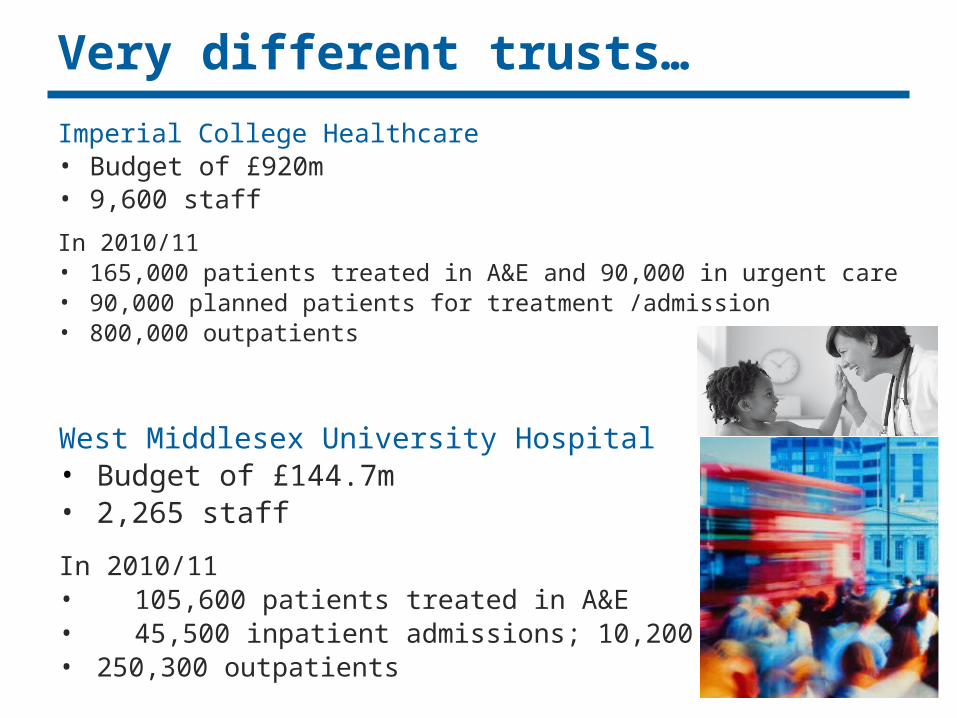
Imperial College Healthcare• Budget of £920m• 9,600 staff
In 2010/11• 165,000 patients treated in A&E and 90,000 in urgent care• 90,000 planned patients for treatment /admission• 800,000 outpatients
Very different trusts…
West Middlesex University Hospital• Budget of £144.7m• 2,265 staff
In 2010/11• 105,600 patients treated in A&E• 45,500 inpatient admissions; 10,200 operations• 250,300 outpatients
West Middlesex University Hospital• Budget of £144.7m• 2,265 staff
In 2010/11• 105,600 patients treated in A&E• 45,500 inpatient admissions; 10,200 operations• 250,300 outpatients

ICHT: OverviewICHT serves patients across NW London, including Brent, Ealing, Hammersmith and Fulham, Hounslow, Kensington and Chelsea, and Westminster. It also draws in patients from across London and nationally, particularly for specialist services
• Major acute trust with full 24/7 A&E at Charing X and St Mary’s. Secondary A&E at Hammersmith. A major teaching hospital
• Full range of general medical and surgical sub-specialties with around 5,000 births/yr at both St Mary’s and Queen Charlotte
• An Academic Health Science Centre, with Imperial college, and the biggest biomedical research centre in the country
• One of the lowest mortality ratios in the country
• Specialist services include:• Hyper Acute Stroke Unit (8 in London), cancer centre (Charing Cross)
• Major trauma (4 in London), arterial surgery, surgical innovation centre (St M)
• Cardiothoracic services, renal medicine and transplants (Hammersmith)
ICHT serves patients across NW London, including Brent, Ealing, Hammersmith and Fulham, Hounslow, Kensington and Chelsea, and Westminster. It also draws in patients from across London and nationally, particularly for specialist services
• Major acute trust with full 24/7 A&E at Charing X and St Mary’s. Secondary A&E at Hammersmith. A major teaching hospital
• Full range of general medical and surgical sub-specialties with around 5,000 births/yr at both St Mary’s and Queen Charlotte
• An Academic Health Science Centre, with Imperial college, and the biggest biomedical research centre in the country
• One of the lowest mortality ratios in the country
• Specialist services include:• Hyper Acute Stroke Unit (8 in London), cancer centre (Charing Cross)
• Major trauma (4 in London), arterial surgery, surgical innovation centre (St M)
• Cardiothoracic services, renal medicine and transplants (Hammersmith)

WMUH: Overview
Broadly serves patients from London Borough’s of Hounslow & Richmond Upon Thames
• District General Hospital – full range of services, 24 hour A&E, critical care, emergency surgery and urgent medicine and paediatrics
• Queen Mary Maternity Unit which includes Natural Birth Centre – circa 5,000 births per annum
• State of the art buildings and facilities (PFI buildings opened 2003)
• Designated stroke and trauma units
• Community based services – outreach dermatology & sexual health
Broadly serves patients from London Borough’s of Hounslow & Richmond Upon Thames
• District General Hospital – full range of services, 24 hour A&E, critical care, emergency surgery and urgent medicine and paediatrics
• Queen Mary Maternity Unit which includes Natural Birth Centre – circa 5,000 births per annum
• State of the art buildings and facilities (PFI buildings opened 2003)
• Designated stroke and trauma units
• Community based services – outreach dermatology & sexual health

But similarities in…
• High quality services and performance (e.g. low mortality)
• Shared services e.g. teaching, renal dialysis (provided at WMUH by ICHT); around 20 joint appointments
• Patient catchment
• The financial and clinical challenge
• A vision to…
– maintain and improve clinical outcomes for patients
– improve the patient experience
– gain value for money for taxpayers
– secure their future and develop more locally appropriate services by becoming a Foundation Trust. This would enable greater local accountability and surpluses to be reinvested

The sites – ICHT and WMUH
West Middlesex Hospital• Queen Mary Maternity Unit (Modern PFI site)
ICHT:
• Charing Cross
• Hammersmith
• Queen Charlotte’s and Chelsea
• St Mary’s
• Western Eye
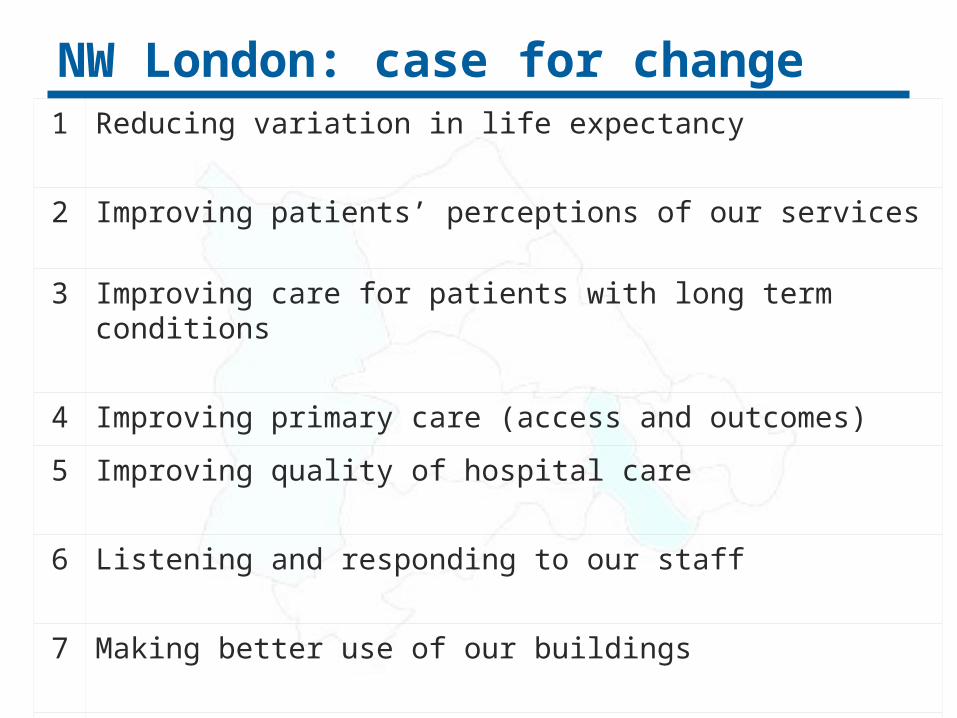
NW London: case for change1 Reducing variation in life expectancy
2 Improving patients’ perceptions of our services
3 Improving care for patients with long term conditions
4 Improving primary care (access and outcomes)
5 Improving quality of hospital care
6 Listening and responding to our staff
7 Making better use of our buildings
8 Achieving £1bn of savings

NW London: case for change1 Reducing variation in life expectancy
- Life expectancy differs by 14 years between communities three miles apart
2 Improving patients’ perceptions of our services- ICHT and WMUH patient satisfaction is below the national average
3 Improving care for patients with long term conditions- More outpatients and care moving out of hospitals. This is better for patients
4 Improving primary care (access and outcomes)
5 Improving quality of hospital care - Need for more specialisation and shorter lengths of stay
6 Listening and responding to our staff- Training, flexible working, career development etc
7 Making better use of our buildings- Better use of WMUH. Old buildings at St Mary’s, Hammersmith and W Eye
8 Achieving £1bn of savings
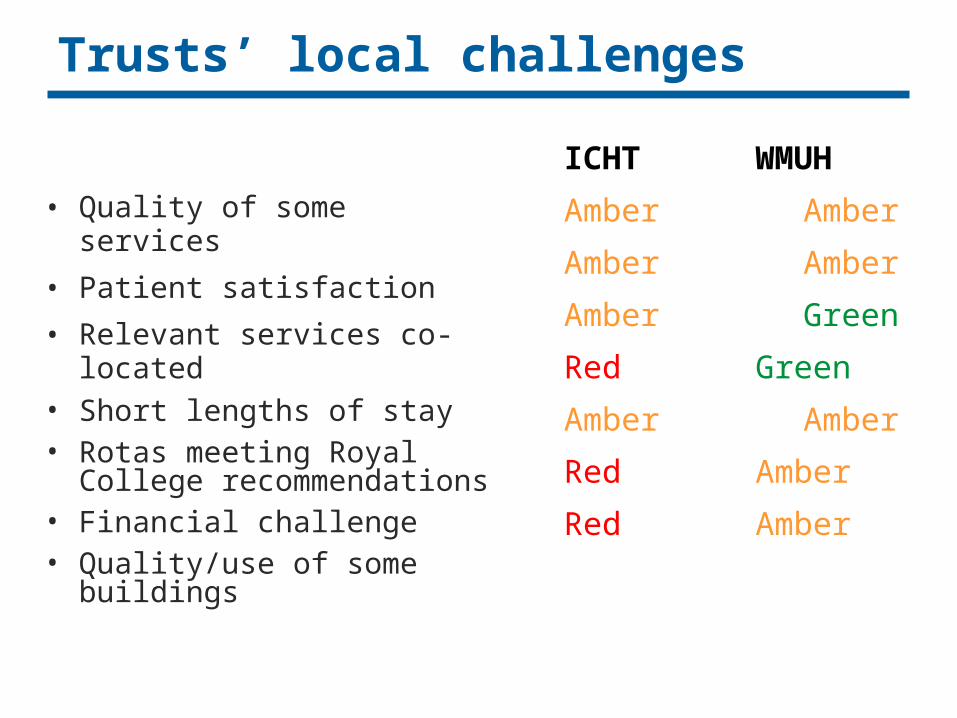
Trusts’ local challenges
• Quality of some services
• Patient satisfaction
• Relevant services co-located• Short lengths of stay• Rotas meeting Royal
College recommendations• Financial challenge• Quality/use of some
buildings
ICHT WMUH
Amber Amber
Amber Amber
Amber Green
Red Green
Amber Amber
Red Amber
Red Amber
ICHT WMUH
Amber Amber
Amber Amber
Amber Green
Red Green
Amber Amber
Red Amber
Red Amber

Financial history
ICHT2008/09
• Surplus: £12m2009/10
• Surplus: £9m2010/11
• Savings delivered: £39m• Surplus: £5.15m
2011/12• £100m savings required• Savings plan: £70m
Financial history
ICHT2008/09
• Surplus: £12m2009/10
• Surplus: £9m2010/11
• Savings delivered: £39m• Surplus: £5.15m
2011/12• £100m savings required• Savings plan: £70m
WMUH • Deficit : £3.5m
• Deficit : £5.5m
• Savings delivered £9.4m• Surplus: £104k
• £12.2m savings required• Savings plan: £12.2m
WMUH • Deficit : £3.5m
• Deficit : £5.5m
• Savings delivered £9.4m• Surplus: £104k
• £12.2m savings required• Savings plan: £12.2m

Financial case for change
• A triple whammy…
• NW London health economy required to make £1billion savings by 2015
• Commissioners are buying more care in the community and not in hospital settings
• Reductions in education and research funding
• ICHT did not make the level of recurrent savings required last year

What are the trusts doing?
• Cost improvement plans to make better use of theatres, reduce lengths of stay, reduce the number of people not attending appointments, reducing unnecessary follow-up appointments
• Outreach working in the community e.g. diabetes and respiratory care. Looking at the use of telemedicine
• Invested £millions in improving the patient environment (buildings, décor etc)
• Developed new services e.g. Hyper Acute Stroke Centre and the Major Trauma Centre
• Reconfigured services e.g. breast surgery and oncology moved to Charing Cross; cardiothoracic services moved to Hammersmith
• However…

“If the NHS is to cope with the financial pressures it is going to face under any government without resorting to indiscriminate and damaging service and staffing cuts, large-scale planned service redesign and reconfiguration based on clinical evidence will have to be at the heart of the strategy.”[1]
Letter to the Guardian, April 2010. Academy of Medical Royal Colleges, Royal College of Physicians, Royal College General Practitioners, NHS Confederation, Royal College of Obstetricians and Gynaecologists, Royal College of Paediatrics & Child Health, Royal College of Psychiatrists, Royal College of Anaesthetists, Royal College of Physicians, Royal College of Radiologists, Royal College of Ophthalmologists, Faculty of Public Health Medicine, Faculty of Pharmaceutical Medicine, Faculty of Occupational Health

Opportunity 1: Specialisation
Greater specialisation would lead to improved healthcare
– Successes in stroke, major trauma, heart attacks
– Evidence for cancer and other specialties
Bilimoria DJ et al., Directing Surgical Quality Improvement Initiatives: comparison of peri-operative mortality and long term survival for cancer surgery, Journal of Oncology, 2008, 26:28
Bilimoria DJ et al., Directing Surgical Quality Improvement Initiatives: comparison of peri-operative mortality and long term survival for cancer surgery, Journal of Oncology, 2008, 26:28

Opportunity 2: Role of consultantsConsultant-delivered services lead to better quality diagnoses, decision-making, patient outcomes and safety. For the best outcomes for patients, there should be consultants on site 24/7
– Studies1[show that babies born during the day have a greater survival rate than those born at weekends or night (when consultants are less likely to be present)
– Better supervision of staff and the presence of a more experienced doctor at the time of a complication in pregnancy could prevent more than three-quarters of serious problems in childbirth. Royal colleges recommend labour wards with more than 5,000 births should provide 24/7 consultant presence2. Queen Charlotte’s and St Mary’s have consultants present for around 60 hours a week, WMUH for around 96 hours which is compliant but will need investment for over 5,000 babies
– Royal colleges also recommend increased consultant presence in urgent care of (and surgery on) children and adults
1 Pasupathy et al, Time of birth and risk of neonatal death at term: retrospective cohort study, July 2010 and de Graaf J et al. Increased adverse perinatal outcome of hospital delivery at night. BJOG 20102 Royal College of Obstetrics and Gynaecologists, The Future Role of the Consultant, Dec 2005

Opportunity 3: Separating care
Patients benefit from separating planned and urgent surgery and increased day surgery
“Separating elective care from emergency pressures can, if well planned, resourced and managed reduce cancellations, achieve a more predictable workflow, provide excellent training opportunities, increase senior supervision of complex/emergency cases, and therefore improve the quality of care delivered to patients…minimise patient inconvenience and maximise productivity for the Trust…(and) hospital-acquired infections can be reduced.”
Royal College of Surgeons1
Day surgery minimises the amount of time that patients spend in hospital. This has been shown to aid recovery and minimise the risk of infections. Just as importantly, patients like this type of care2
1 Separating emergency and elective surgical care: Recommendations for practice, 20072 Naftalin N.J., Habiba M.A: Keeping patients out of hospital. Patients like it. BMJ 2000

Opportunity 4: Co-located care
There are a number of specialties that would be best located next to one another because:
• patients often have more than one disease – e.g. patients with liver disease and other pancreatic or intestinal problems;
• there needs to be joint working and learning between the specialists – for instance paediatrics (care of children), neonatal (care of newborn babies), maternity and gynaecology (women’s diseases – especially the reproductive system);
• the specialists involved are required to treat more than one type of patient, for instance surgeons operating on arteries and
those operating on nerves are needed to treat patients with arterial disease or neurological problems but they are also often needed to treat patients who have been involved in a serious accident.

Opportunity 5: Integrated care
A more integrated, accessible health service would improve patient safety, care and experiences
– Local initiatives to move care into the community at both trusts are working well. Fulham Centre for Health (at Charing Cross) now cares for 42,000 patients a year compared with the 32,000 in A&E. Urgent Care Centre opening at WMUH later this year
– Successful integrated care partnership across NW London
– The partnership of the Academic Health Science Centre has introduced new diagnostics, therapies and techniques:
• Largest community-based preventative cardiology programme in the country, with NHS Westminster
• Developing a new test that can diagnose TB more accurately than ever before

In essence
• The status quo is not sustainable
• If we do not change our approach to delivering care now, we will miss an opportunity to tackle the
inequalities that currently exist and ensure our patients and residents continue to receive high-quality, sustainable care
• If we do not act now we cannot rely on taxpayers to subsidise our health economy

A joint clinical strategy
To ensure the required large-scale service redesign is based on clinical evidence, an understanding of patients and their needs, and can be delivered within budget, the trusts are developing a joint clinical strategy
The work is being led by senior clinicians who have been asked to consider how the trusts could provide the best healthcare for local people. Assessments of the various opportunities will be made by looking at:
• clinical safety and quality
• patient impact
• financial impact
• strategic fit (how do the options relate to other trusts’ plans, to research and training potential etc)
• integrated care potential (ability to improve the patient pathway)?

What will the strategy do?
• The draft strategy (due to be published by the end of the year) will set out a number of clinical assumptions, co-dependencies and options. These will then be published and stakeholders and the public will be invited to comment
• This will enable the trust to develop a programme of change to improve the health of the local population and healthcare by:
– informing the development of any public consultation if service change is proposed
– support the development of other business cases if there is a requirement for major capital investment
– be used to develop an implications paper for WMUH
• A case for change will be published in the next few weeks (based on the content of this slide pack) [