Long-Term Care Updates - Creighton University
6
By Daniel Kerner, PharmD October/November 2015 Long-Term Care Updates www.creighton.edu/pharmerica A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main classifications of strokes: hemorrhagic stroke, ischemic stroke, and transient ischemic attack (TIA). A hemorrhagic stroke occurs when a blood vessel ruptures leading to bleeding in the brain. An ischemic stroke occurs when the blood supply to the brain is reduced or interrupted and the brain is deprived of vital oxygen and nutrients. Within a matter of minutes, brain cells are damaged and begin die. A TIA, also known as a mini-stroke, occurs when signs and symptoms of brain ischemia are present but clear within 24 hours. 1 In the U.S., around 795,000 people suffer from stroke each year, with 129,000 events resulting in death. Further, stroke is the leading cause of long-term disability in the United States. 2 Six months following a stroke, 26% of patients aged 65 years or older are dependent in their activities of daily living and 46% have cognitive deficits. 3 The following article will summarize and synthesize clinical practice guidelines for stroke prevention from the American Medical Directors Association (AMDA), American Heart Association/American Stroke Association (AHA/ASA), and American College of Chest Physicians (ACCP). While these guidelines provide significant evidence-based guidance on the prevention of stroke, patient-specific factors and clinician judgement should ultimately dictate an appropriate care plan. AMDA Clinical Practice Guideline In 2011, AMDA published guidelines for Stroke Management in the Long-Term Care Setting. The guidelines identify several modifiable risk factors for stroke (see Table 1). By identifying and treating these risk factors, the chance of a first-time or recurrent stroke is reduced. 1 AMDA cites one study suggesting that patients can lower their five-year cumulative risk of recurrent stroke by 80% by initiating antihypertensive medications, aspirin, a statin, exercise, and dietary adjustments. The 80% risk reduction translates to a number needed to treat of
Transcript of Long-Term Care Updates - Creighton University
By Daniel Kerner, PharmD
October/November 2015
Long-Term Care Updates
www.creighton.edu/pharmerica
A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or
damage to brain cells. There are three main classifications of strokes: hemorrhagic stroke,
ischemic stroke, and transient ischemic attack (TIA). A hemorrhagic stroke occurs when a
blood vessel ruptures leading to bleeding in the brain. An ischemic stroke occurs when the
blood supply to the brain is reduced or interrupted and the brain is deprived of vital oxygen
and nutrients. Within a matter of minutes, brain cells are damaged and begin die. A TIA, also
known as a mini-stroke, occurs when signs and symptoms of brain ischemia are present but
clear within 24 hours.1 In the U.S., around 795,000 people suffer from stroke each year,
with 129,000 events resulting in death. Further, stroke is the leading cause of long-term
disability in the United States.2 Six months following a stroke, 26% of patients aged 65 years
or older are dependent in their activities of daily living and 46% have cognitive deficits.3
The following article will summarize and synthesize clinical practice guidelines for stroke
prevention from the American Medical Directors Association (AMDA), American Heart
Association/American Stroke Association (AHA/ASA), and American College of Chest
Physicians (ACCP). While these guidelines provide significant evidence-based guidance on
the prevention of stroke, patient-specific factors and clinician judgement should ultimately
dictate an appropriate care plan.
AMDA Clinical Practice Guideline
In 2011, AMDA published guidelines for Stroke Management in the Long-Term Care Setting.
The guidelines identify several modifiable risk factors for stroke (see Table 1). By identifying
and treating these risk factors, the chance of a first-time or recurrent stroke is reduced.1
AMDA cites one study suggesting that patients can lower their five-year cumulative risk of
recurrent stroke by 80% by initiating antihypertensive medications, aspirin, a statin, exercise,
and dietary adjustments. The 80% risk reduction translates to a number needed to treat of
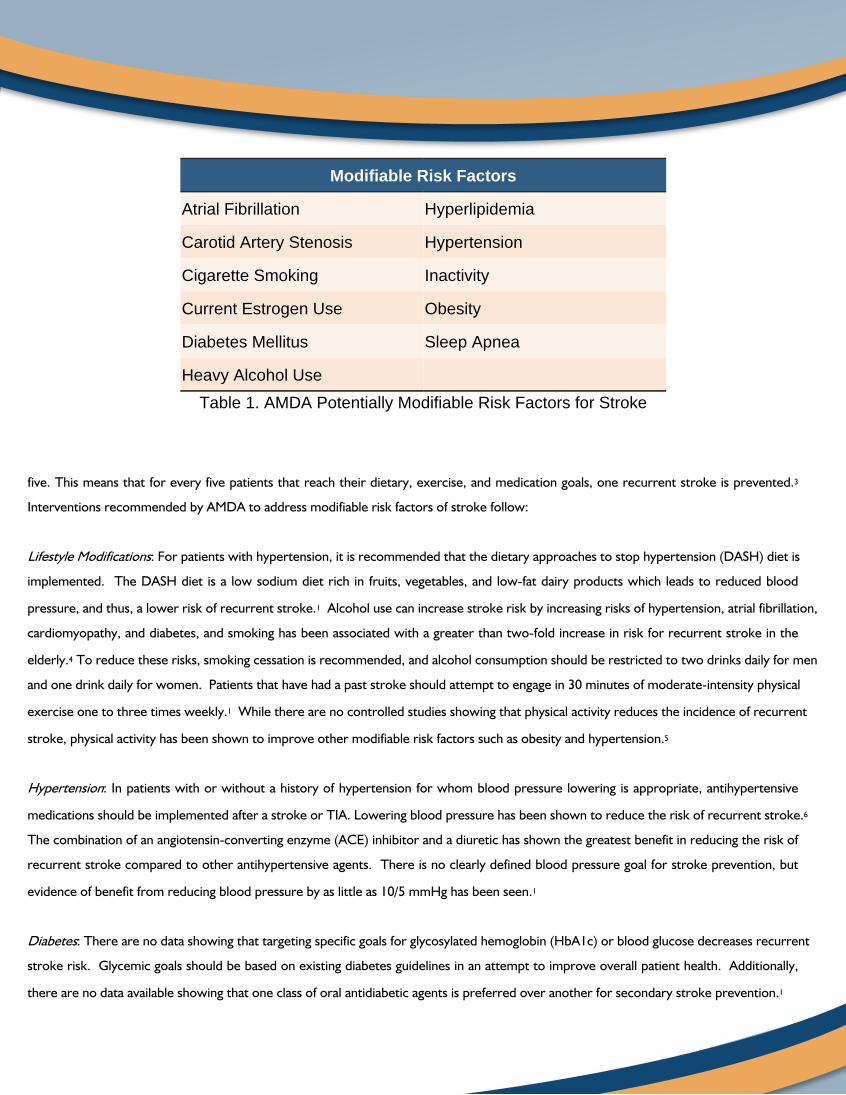
Table 1. AMDA Potentially Modifiable Risk Factors for Stroke
five. This means that for every five patients that reach their dietary, exercise, and medication goals, one recurrent stroke is prevented.3
Interventions recommended by AMDA to address modifiable risk factors of stroke follow:
: For patients with hypertension, it is recommended that the dietary approaches to stop hypertension (DASH) diet is
implemented. The DASH diet is a low sodium diet rich in fruits, vegetables, and low-fat dairy products which leads to reduced blood
pressure, and thus, a lower risk of recurrent stroke.1 Alcohol use can increase stroke risk by increasing risks of hypertension, atrial fibrillation,
cardiomyopathy, and diabetes, and smoking has been associated with a greater than two-fold increase in risk for recurrent stroke in the
elderly.4 To reduce these risks, smoking cessation is recommended, and alcohol consumption should be restricted to two drinks daily for men
and one drink daily for women. Patients that have had a past stroke should attempt to engage in 30 minutes of moderate-intensity physical
exercise one to three times weekly.1 While there are no controlled studies showing that physical activity reduces the incidence of recurrent
stroke, physical activity has been shown to improve other modifiable risk factors such as obesity and hypertension.5
: In patients with or without a history of hypertension for whom blood pressure lowering is appropriate, antihypertensive
medications should be implemented after a stroke or TIA. Lowering blood pressure has been shown to reduce the risk of recurrent stroke.6
The combination of an angiotensin-converting enzyme (ACE) inhibitor and a diuretic has shown the greatest benefit in reducing the risk of
recurrent stroke compared to other antihypertensive agents. There is no clearly defined blood pressure goal for stroke prevention, but
evidence of benefit from reducing blood pressure by as little as 10/5 mmHg has been seen.1
: There are no data showing that targeting specific goals for glycosylated hemoglobin (HbA1c) or blood glucose decreases recurrent
stroke risk. Glycemic goals should be based on existing diabetes guidelines in an attempt to improve overall patient health. Additionally,
there are no data available showing that one class of oral antidiabetic agents is preferred over another for secondary stroke prevention.1
Modifiable Risk Factors
Atrial Fibrillation Hyperlipidemia
Carotid Artery Stenosis Hypertension
Cigarette Smoking Inactivity
Current Estrogen Use Obesity
Diabetes Mellitus Sleep Apnea
Heavy Alcohol Use
: The AMDA guidelines cite a meta-analysis of statin therapy that showed reduction of low-density lipoprotein cholesterol (LDL-C) with
statins reduces the incidence of stroke.1 The AMDA guidelines agree with the current American College of Cardiology/American Heart
Association (ACC/AHA) guidelines recommending that patients 75 years or less with a prior stroke be started on a high-intensity statin, which
produces a greater than 50% decrease in LDL-C. Patients greater than 75 years with a prior stroke should take a moderate-intensity statin,
which produces a 30-50% decrease in LDL-C.7
: For all patients with a prior TIA or thrombotic stroke not caused by a cardioembolism, antiplatelet therapy is
recommended. For every 40 patients receiving antiplatelet therapy, one nonfatal stroke is prevented. Antiplatelet medications that can be
used for recurrent stroke prevention include 50-325 mg aspirin daily, aspirin 25 mg/extended-release dipyridamole 200 mg twice daily, or
clopidogrel 75 mg daily. These agents have shown similar efficacy as antiplatelet monotherapy, and combination therapy has shown no added
benefit for stroke prevention.1
: To prevent stroke in patients with atrial fibrillation, anticoagulation is recommended. The AMDA guidelines maintain that
anticoagulation with warfarin is the gold standard for stroke prevention in patients with atrial fibrillation. While warfarin is more effective than
dabigatran for preventing stroke, it is associated with higher incidence of life-threatening hemorrhagic complications and requires more
frequent monitoring. Therefore, dabigatran may be more appropriate for some patients.1 Due to the date of approval, apixaban, edoxaban,
and rivaroxaban are not addressed in the AMDA guidelines.
: In addition to optimizing medication therapy as stated above, a carotid endarterectomy (CEA) is recommended in
patients with greater than 70% stenosis. For patients that have 50% to 69% stenosis, CEA may be an option based on patient preference and
suitability for surgery. Surgery is not recommended for patients with less than 50% stenosis. Carotid artery stenting may be a less invasive
alternative to CEA.1
: Estrogen with or without a progestin can increase the risk of stroke. Estrogen therapy should be
discontinued in patients recovering from a stroke.1
AHA/ASA Guidelines
The AHA and ASA published updated guidelines for the prevention of stroke in patients with stroke and TIA in 2014. The purpose of these
guidelines was to provide comprehensive, evidence-based recommendations for the prevention of future stroke in those that have previously
experienced an ischemic stroke or TIA.4 These guidelines were an update of the 2011 AHA/ASA statement on secondary stroke prevention.5
The AHA/ASA guidelines differentiate between non-modifiable and modifiable risk factors for stroke. Non-modifiable risk factors include
older age, low birth weight, race/ethnicity, and genetic factors that cannot be controlled in the prevention of stroke. AHA/ASA does not offer
recommendations to counteract these non-modifiable risk factors. However, the guidelines provide several recommendations for modifiable
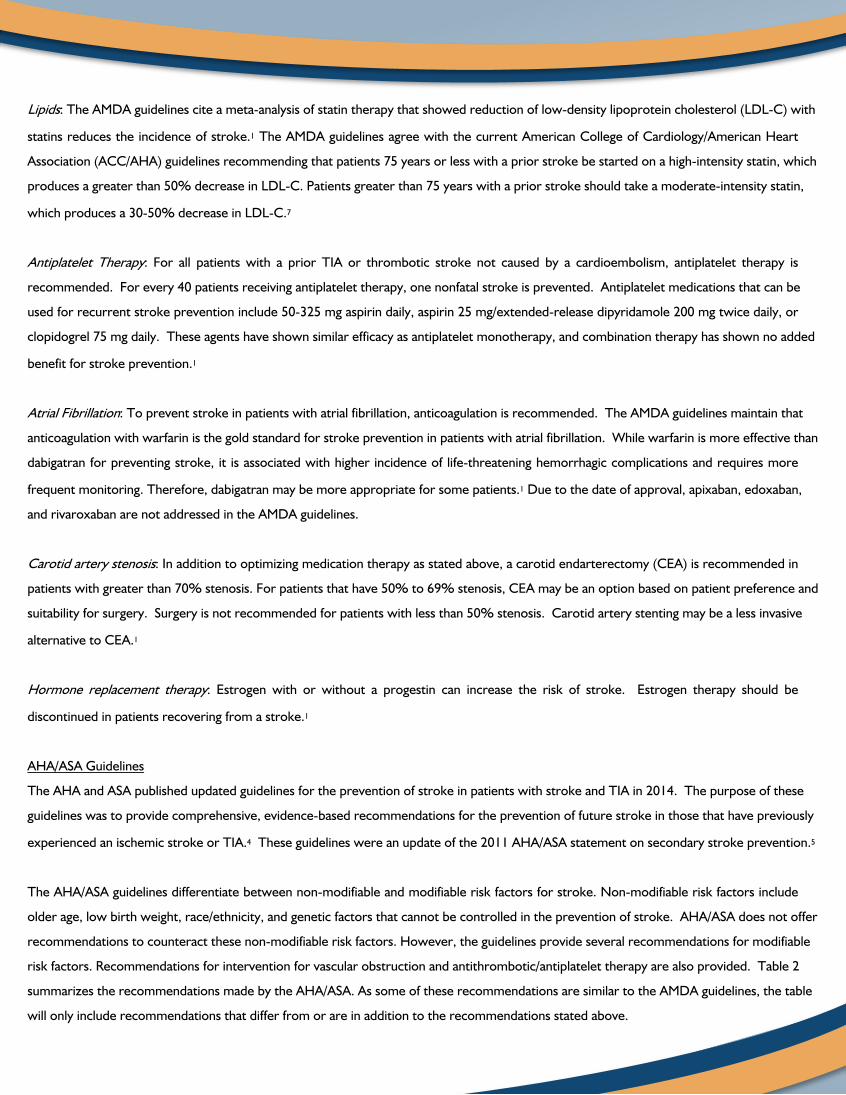
risk factors. Recommendations for intervention for vascular obstruction and antithrombotic/antiplatelet therapy are also provided. Table 2
summarizes the recommendations made by the AHA/ASA. As some of these recommendations are similar to the AMDA guidelines, the table
will only include recommendations that differ from or are in addition to the recommendations stated above.
Table 2. AHA/ASA Recommendations for Prevention of Stroke in Patients with Stroke and TIA4
Section Recommendations
Diet and Nutrition
● Single vitamin or multivitamin supplementation is not recommended as this has not shown aproven benefit in secondary stroke prevention.
● To lower the stroke risk associated with elevated blood pressure, patients with a history of strokeor TIA should reducer sodium intake to less than 2.4 g/day. Greater blood pressure reductionmay be seen with sodium intake reduction to <1.5 g/day.
● A Mediterranean diet, which consists of fruits, vegetables, whole grains, low-fat dairy products,poultry, fish, legumes, nuts, and olive oil has also shown to decrease blood pressure.
Hypertension
● For patients with stroke or TIA, not previously treated for hypertension, and with a bloodpressure ≥140/90 mmHg, antihypertensive therapy should be initiated within the first few dayspost-stroke to prevent recurrent stroke.
● For patients that have had a stroke or TIA and have been previously treated for hypertension,blood pressure lowering therapy should be resumed after the first several days post-stroke.
Atrial Fibrillation
● To prevent recurrent stroke in atrial fibrillation patients that cannot take oral anticoagulants,aspirin monotherapy is recommended. Dual therapy of clopidogrel and aspirin has also shownbenefit in secondary stroke prevention.
● Oral anticoagulation should be initiated within 14 days of the onset of neurological symptoms formost patients following a stroke or TIA. This may be delayed in instances of hemorrhagic risk,such as a large infarct, uncontrolled hypertension, or hemorrhage tendency.
Sleep Apnea
● A sleep study may be warranted in patients following a stroke or TIA due to the high prevalenceof sleep apnea in this population.
● Treatment with continuous positive airway pressure (CPAP) has shown to reduce recurrentstroke risk in patients with sleep apnea following a stroke or TIA.
IntracranialAtherosclerosis
● Ninety day treatment with clopidogrel 75 mg/day plus aspirin may be warranted to reducerecurrent stroke risk in patients suffering from stroke or TIA within 30 days of severe stenosis(70%-99%) of a major intracranial artery.
● Systolic blood pressure should be maintained at <140 mmHg and a high-intensity statin therapyshould be initiated for patients with a stroke or TIA due to 50% to 99% stenosis of a majorintracranial artery.
● For patients with a stroke or TIA due to moderate stenosis (50%-69%) of a major intracranialartery, the periprocedural risk of angioplasty or stenting outweighs the benefit of decreasing thelow rate of recurrent stroke and is not recommended.
Hypercoagulation ● If anticoagulation therapy is not administered in patients with abnormal findings on coagulationtesting, antiplatelet therapy is recommended to reduce the risk of recurrent stroke.
Sickle Cell Disease● Reducing hemoglobin S to <30% of total hemoglobin via chronic blood transfusions has shown
to significantly decrease the rate or recurrent stroke in patients with sickle cell disease and priorstroke or TIA.
Prosthetic Heart Valve
● For patients with a history of stroke or TIA prior to the insertion of a mechanical aortic valve,warfarin therapy is recommended with an INR target of 2.5 (range, 2.0-3.0).
● For patients with a history of stroke or TIA prior to the insertion of a mechanical mitral valve,warfarin therapy is recommended with an INR target of 3.0 (range, 2.5-3.5).
● For low bleeding risk patients with a history of stroke or TIA prior to the insertion of a mechanicalaortic or mitral valve, the addition of aspirin 75-100 mg/day to warfarin therapy is recommended.
● For patients with a history of stroke or TIA prior to the insertion of a bioprosthetic aortic or mitralvalve that are not indicated for anticoagulation therapy beyond 3 to 6 months from the valveplacement, long-term therapy with aspirin 75-100 mg/day is preferred over long-termanticoagulation due to decreased risk of thromboembolism in these patients.
ACCP Guidelines
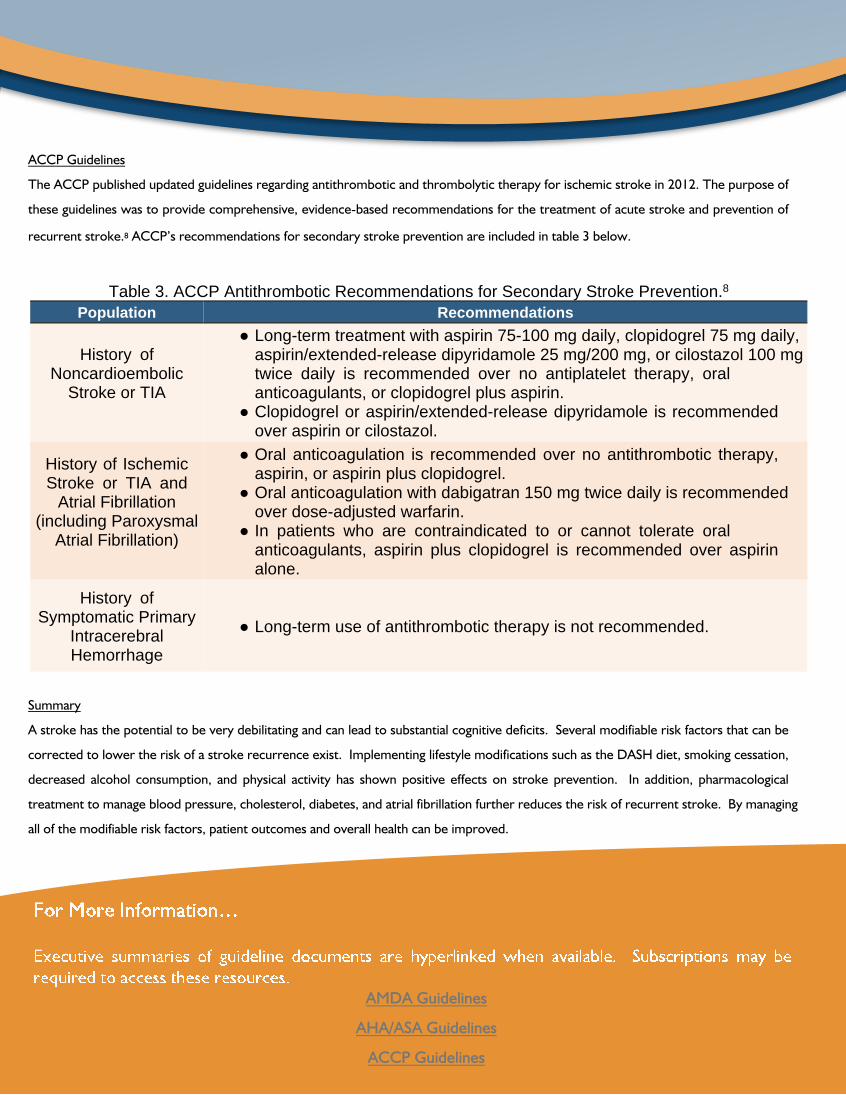
The ACCP published updated guidelines regarding antithrombotic and thrombolytic therapy for ischemic stroke in 2012. The purpose of
these guidelines was to provide comprehensive, evidence-based recommendations for the treatment of acute stroke and prevention of
recurrent stroke.8 ACCP’s recommendations for secondary stroke prevention are included in table 3 below.
Table 3. ACCP Antithrombotic Recommendations for Secondary Stroke Prevention.8
Summary
A stroke has the potential to be very debilitating and can lead to substantial cognitive deficits. Several modifiable risk factors that can be
corrected to lower the risk of a stroke recurrence exist. Implementing lifestyle modifications such as the DASH diet, smoking cessation,
decreased alcohol consumption, and physical activity has shown positive effects on stroke prevention. In addition, pharmacological
treatment to manage blood pressure, cholesterol, diabetes, and atrial fibrillation further reduces the risk of recurrent stroke. By managing
all of the modifiable risk factors, patient outcomes and overall health can be improved.
Population Recommendations
History ofNoncardioembolic
Stroke or TIA
● Long-term treatment with aspirin 75-100 mg daily, clopidogrel 75 mg daily,aspirin/extended-release dipyridamole 25 mg/200 mg, or cilostazol 100 mgtwice daily is recommended over no antiplatelet therapy, oralanticoagulants, or clopidogrel plus aspirin.
● Clopidogrel or aspirin/extended-release dipyridamole is recommendedover aspirin or cilostazol.
History of IschemicStroke or TIA and
Atrial Fibrillation(including Paroxysmal
Atrial Fibrillation)
● Oral anticoagulation is recommended over no antithrombotic therapy,aspirin, or aspirin plus clopidogrel.
● Oral anticoagulation with dabigatran 150 mg twice daily is recommendedover dose-adjusted warfarin.
● In patients who are contraindicated to or cannot tolerate oralanticoagulants, aspirin plus clopidogrel is recommended over aspirinalone.
History ofSymptomatic Primary
IntracerebralHemorrhage
● Long-term use of antithrombotic therapy is not recommended.

1. American Medical Directors Association. Stroke Management in the Long-Term Care Setting Clinical Practice Guide-line. Columbia, MD: AMDA 2011
2. American Heart Association and American Stroke Association. Heart Disease and Stroke States – At-A-Glance.http://www.heart.org/idc/groups/ahamah-public/@wcm/@sop/@smd/documents/downloadable/ucm_470704.pdf.Dallas, TX: AHA 2015.
3. Meschia JF, Bushnell C, Boden-Albala B, et al. Guidelines for the primary prevention of stroke: A statement for health-care professionals from the American Heart Association/ American Stroke Association. 2014;45(12):3754-832.
4. Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transientischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Asso-ciation. 2014;45(7):2160-236.
5. Furie KL, Kasner SE, Adams RJ, et al. Guidelines for the prevention of stroke in patients with stroke and transient isch-emic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Associa-tion. 2011;42(1):227-76.
6. Rashid P, Leonardi-Bee J, Bath P. Blood pressure reduction and secondary prevention of stroke and other vascularevents: A systematic review. 2003;34(11):2741-8.
7. Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of bloodcholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College ofCardiology/American Heart Association Task Force on Practice Guidelines. 2014;129(25 Suppl 2):S1-45.
8. Lansberg MG, O’Donnell MJ, Khatri P, et al. Antithrombotic and thrombolytic therapy for ischemic stroke: Antithrom-botic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical prac-tice guidelines. 2012;141(2 Suppl):e601S-36S.
http://creighton.edu/pharmerica


















