
Work in progress Naomi Fulop London School Of Hygiene & Tropical Medicine
Upload
hoangkhanhCategory
view
215download
0
London School
of Hygiene & Tropical Medicine
MSc. Public Health
A Health Policy Report How could changes of case definitions, ascertainment procedures, and diagnostic and registration conventions have impacted on reductions in the prevalence of leprosy in India, reported over the last decade (taking
the state of Jharkhand as a case study)?
August 2008
LSHTM Candidate Number 470127
Word Count: 9953
LSHTM Candidate Number 470127 2
Acknowledgements
I would like to thank Karen Lock for all her understanding and support,
and express my heartfelt appreciation for all her advice and comments
which were always spot-on, throughout the development and completion
of this project. Also I would like to thank Professors Paul Fine and Diana
Lockwood for their guidance and time.
Lastly, I would also like to thank those who generously gave their time to
be interviewed as well as those who made these interviews possible.

LSHTM Candidate Number 470127 3
Table of Contents
GLOSSARY & ABBREVIATIONS .....................................................................................................5 EXECUTIVE SUMMARY ....................................................................................................................6 1 INTRODUCTION.........................................................................................................................9
1.1 HISTORY ................................................................................................................................9 1.2 CLASSIFICATION.....................................................................................................................9 1.3 TREATMENT .........................................................................................................................10 1.4 CURRENT SITUATION ...........................................................................................................10 1.5 LEPROSY CONTROL PROGRAMMES IN INDIA ........................................................................13 1.6 LEPROSY PREVALENCE IN INDIA: WHAT IS THE TRUE PICTURE?...........................................14
2 AIMS & OBJECTIVES..............................................................................................................16 2.1 AIM ......................................................................................................................................16 2.2 OBJECTIVES..........................................................................................................................16
3 METHODOLOGY .....................................................................................................................17 3.1 LITERATURE REVIEW ...........................................................................................................17
3.1.1 Selection Criteria............................................................................................................17 3.1.2 Search Strategy for Identification of Studies ..................................................................17 3.1.3 Methods of the Review....................................................................................................18
3.2 SEMI-STRUCTURED INTERVIEWS ..........................................................................................19 3.2.1 Topic Guide ....................................................................................................................20 3.2.2 Selection of interviewees.................................................................................................20 3.2.3 Data Extraction and Thematic Analysis .........................................................................21
4 RESULTS & FINDINGS............................................................................................................22 4.1 LITERATURE REVIEW ...........................................................................................................22
4.1.1 Results of Search Strategy ..............................................................................................22 4.1.2 Findings from the review ................................................................................................22
4.2 SEMI-STRUCTURED INTERVIEWS ..........................................................................................33 4.2.1 Leprosy Elimination Programme....................................................................................33 4.2.2 Case detection.................................................................................................................33 4.2.3 Case diagnosis................................................................................................................35 4.2.4 Case validation ...............................................................................................................36 4.2.5 Case registration ............................................................................................................36 4.2.6 Range/Types of cases......................................................................................................37 4.2.7 Case treatment................................................................................................................38 4.2.8 Case cure ........................................................................................................................38 4.2.9 Prevalence data ..............................................................................................................39 4.2.10 Case reductions and leprosy as a public health problem ..........................................39 4.2.11 Vertical VS Integrated................................................................................................40 4.2.12 Improvements, limitations and shortcomings.............................................................42 4.2.13 Stigma ........................................................................................................................43
5 DISCUSSION ..............................................................................................................................44 6 LIMITATIONS...........................................................................................................................48 7 CONCLUSIONS & RECOMMENDATIONS .........................................................................50
7.1 CONCLUSIONS ......................................................................................................................50 7.2 RECOMMENDATIONS ............................................................................................................51

LSHTM Candidate Number 470127 4
APPENDIX 1: ANONYMISED COPY OF FINAL REVISED PROTOCOL ................................54 APPENDIX 2: ANONYMISED COPY OF RISK ASSESSMENT FORM.....................................58 APPENDIX 3: ANONYMISED COPY OF LSHTM ETHICS APPROVAL LETTER ................61 APPENDIX 4: LITERATURE REVIEW SEARCH STRATEGY..................................................67 APPENDIX 5: SEMI-STRUCTURED TOPIC GUIDE....................................................................70 APPENDIX 6: CODING SCHEME FOR INTERVIEW ANALYSIS.............................................74 REFERENCES .....................................................................................................................................75

LSHTM Candidate Number 470127 5
Glossary & Abbreviations
ANCDR- Annual New Case Detection Rates; proxy indicator for leprosy incidence ANM- Auxiliary Nurse Midwife; a type of peripheral health worker at village and
block level in India BI- Bacteriological Index; a logarithmic-scaled measure of density of M. Leprae in
the dermis (skin) CBR- Community Based Rehabilitation; a type of rehabilitation approach GHS- General Healthcare Services IEC- Information, Education & Communication MB- Multibacillary; meaning many bacteria (M. Leprae), a type of leprosy
classification with a BI > 2 MDT- Multi-Drug Therapy MHW- Multi-Purpose Health Worker; another type of peripheral health worker at
village and block level in India MLEC- Modified Leprosy Elimination Campaign NCDR- New Case Detection Rates NGO- Non-Governmental Organisation NLEP- National Leprosy Eradication Programme; the Indian governments’ health
programme for leprosy PB- Paucibacillary; meaning less (paucity) of bacteria (M. Leprae), a type of leprosy
classification with a BI< 2 PHC- Primary Health Centre; the main health service at block level in India PR- Prevalence Rate RFT- Release From Treatment ROM- Rifampicin, Ofloxacin & Minocycline; the regimen for single lesion leprosy SER- Socio-Economic Rehabilitation; another type of rehabilitation approach WHO- World Health Organisation
LSHTM Candidate Number 470127 6
Executive Summary
Background
In 1991 the World Health Assembly (WHA) passed a resolution to “eliminate leprosy
as a public health problem” by the year 20001. Elimination was defined in this context
as a reduction in prevalence to below 1 per 10,000 population. India achieved
elimination in December 2005 following a dramatic fall in prevalence, particularly
between the years 2000-2005.
Although some states like Jharkhand, as per Government of India figures continue to
have prevalence above 1 per 10,000 the rapid and drastic fall in prevalence seen
nationally in India has been greeted with scepticism by some in scientific and NGO
community- and international queries about what has actually happened2,3. One theory
is that changes to the diagnostic, surveillance and reporting procedures are creating
‘data artefacts’ that are obscuring the true picture of leprosy prevalence and control in
India.
Aims of the project
This paper is a health policy report aimed at gaining insight into the relationship
between the steep fall of leprosy prevalence reported in India and changes to the
diagnostic, surveillance and reporting procedures being followed, looking at the
Indian state of Jharkhand as a case study.
LSHTM Candidate Number 470127 7
Methods
The research is based on a review of published and unpublished literature and semi-
structured interviews of key staff involved in the delivery of leprosy control services
in the Indian state of Jharkhand, to gain understanding on the issues related to
assessment of prevalence.
Key Findings
While there is no doubt that significant strides have been made towards reducing the
prevalence of leprosy in India, key findings confirm that repeated changes by WHO
and the National Leprosy Eradication Programme (NLEP) to case definitions,
diagnostic conventions (from skin smears to lesion counting), duration & types of
treatment (MB-MDT duration, ROM therapy, accompanied MDT), prevalence
calculations (from period to point prevalence), case detection methods (from active
detection to voluntary reporting), registration conventions, RFT (release from
treatment) protocols, programme structures (from vertical to integrated approaches),
and ineffective coverage and awareness initiatives have had direct and indirect
impacts on the prevalence figures of leprosy in India, obscuring the true extent of the
actual reductions in disease prevalence.
Conclusions
While a more detailed analysis would be required to fully understand the extent of the
impact of these diagnostic, surveillance and treatment changes, this research
underscores the danger of a repeating what happenned with tuberculosis and malaria,
which in the 1960’s were pronounced defeated, only to re-emerge now as global
emergencies4.

LSHTM Candidate Number 470127 8
The paper suggests policy amendments and new policy initiatives to the National
Leprosy Eradication Programme, and recommends reinstating some past policies and
practices that have gathered a considerable evidence-base of effectiveness, to address
the future challenges of leprosy as a public health problem in India.

LSHTM Candidate Number 470127 9
1 Introduction
Globally and especially in India, leprosy prevalence has fallen dramatically in the last
decade. That a disease as old as humankind itself has been ‘eliminated’ particularly by
efforts in this millennium, needs to be examined critically before it is accepted as fact.
1.1 History
Leprosy is probably the oldest disease
known to mankind. The word leper
comes from the Greek word ‘lepid’
meaning scaly. In India, leprosy is
known since ancient times as ‘kustha
roga’ and attributed to punishment or
curse from God.
Figure 1: Leprosy, demarcated skin lesions
Modern-day leprosy dates from 1873 when Hansen of Norway discovered
Mycobacterium leprae (M. leprae), the bacterial pathogen that causes leprosy. For
long years, there was no effective remedy for leprosy. The introduction of sulphone
drugs in 1943 marked the beginning of a new era of case-finding and domiciliary
treatment. The decade of 1980s witnessed a change in the strategy of leprosy control
from DDS (Dapsone) monotherapy to multidrug therapy (MDT), due to widespread
emergence of dapsone resistant strains of M. leprae.
1.2 Classification
Several classifications for leprosy exist, i.e. the Madrid5, Ridley-Jopling6 and the
Indian7 classifications; based on clinical, bacteriological, immunological and

LSHTM Candidate Number 470127 10
histological states of patients. Broadly speaking, the disease manifests in two polar
forms, the lepromatous and tuberculoid forms lying at the two ends of a spectrum that
includes borderline and indeterminate forms. Cases are commonly described as being
either Multibacillary or Paucibacillary. Multibacillary (lepromatous) leprosy is
considered more severe while Paucibacillary (tuberculoid) leprosy is relatively less
severe.
1.3 Treatment
Originally WHO recommended Multibacillary cases to be treated with MDT for 24
months or until the smear became negative (generally 5 years). Subsequently the
acceptable course was reduced by WHO to 12 months, a change that remains
especially controversial in the absence of supporting clinical trials8. Paucibacillary
cases are given MDT for 6 months9 .
1.4 Current Situation
In 1991 the World Health Assembly (WHA) passed a resolution to “eliminate leprosy
as a public health problem” by the year 2000, elimination defined in this context as a
reduction in prevalence to below 1 per 10,000 population. WHO states that this has
now been accomplished10. In December 2005 India announced it had achieved
elimination, according to the National Leprosy Eradication Programme data11.

LSHTM Candidate Number 470127 11
Figure 2: Trends in Leprosy Prevalence12
In India between 1996 and 2000 leprosy prevalence fell from 5.9 to 5.3 per 10,000
population, a 10% reduction of 0.6 per 10,000 population over 5 years. From 2000 to
2006, the prevalence fell from 5.3 to 0.8 per 10,000 population, a staggering 85%
reduction of 4.5 per 10,000 population over the next five years. WHO explained that
the fall in prevalence was due to improvements in the management of cases, very low
rates of relapse, high cure rates, absence of drug resistance and shorter duration of
treatment with MDT13. As of March 2008, only six States/ Union Territories remain
with prevalence over 1 per 10,000 population; these are D&N Haveli, Chhattisgarh,
Jharkhand, Bihar, Chandigarh & West Bengal11.
LSHTM Candidate Number 470127 12
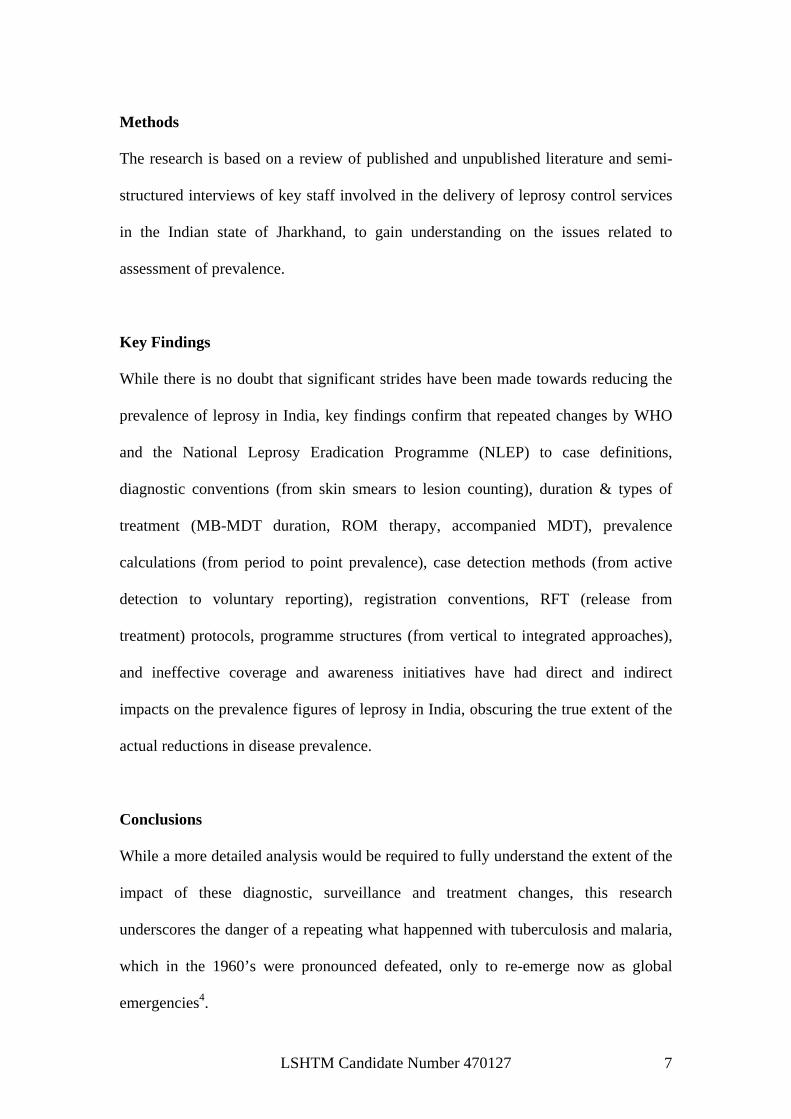
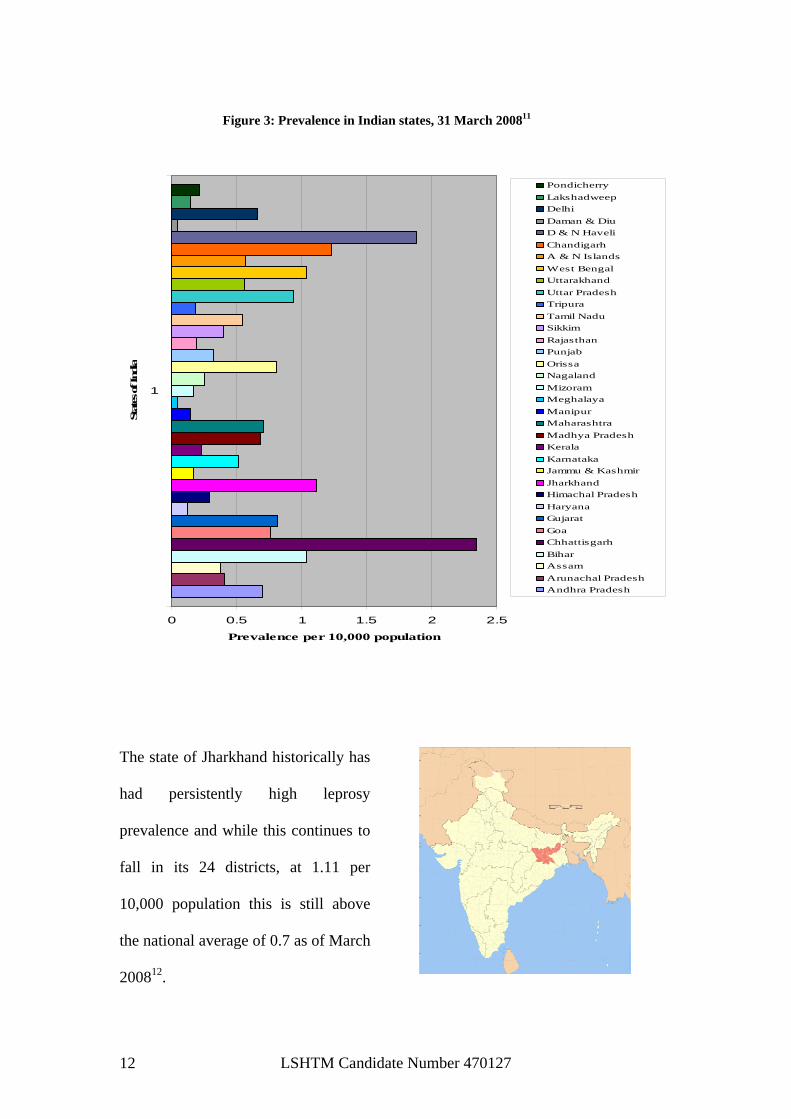
Figure 3: Prevalence in Indian states, 31 March 200811
0 0.5 1 1.5 2 2.5
1
Stat
es of I
ndia
Prevalence per 10,000 population
PondicherryLakshadweepDelhiDaman & DiuD & N HaveliChandigarhA & N IslandsWest BengalUttarakhandUttar PradeshTripuraTamil NaduSikkimRajasthanPunjabOrissaNagalandMizoramMeghalayaManipurMaharashtraMadhya PradeshKeralaKarnatakaJammu & KashmirJharkhandHimachal PradeshHaryanaGujaratGoaChhattisgarhBiharAssamArunachal PradeshAndhra Pradesh
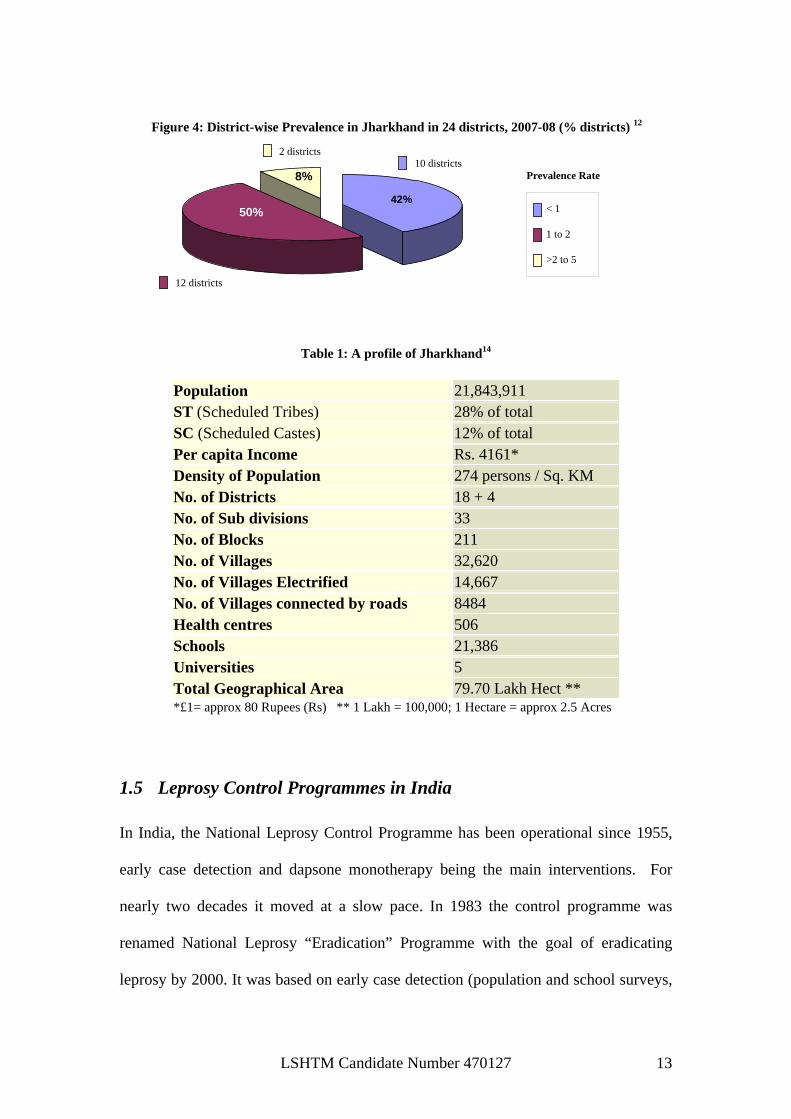
The state of Jharkhand historically has
had persistently high leprosy
prevalence and while this continues to
fall in its 24 districts, at 1.11 per
10,000 population this is still above
the national average of 0.7 as of March
200812.
LSHTM Candidate Number 470127 13
Figure 4: District-wise Prevalence in Jharkhand in 24 districts, 2007-08 (% districts) 12
42%50%
8%
< 1
1 to 2
>2 to 5
Prevalence Rate
12 districts
10 districts 2 districts
Table 1: A profile of Jharkhand14
Population 21,843,911 ST (Scheduled Tribes) 28% of total. SC (Scheduled Castes) 12% of total Per capita Income Rs. 4161* Density of Population 274 persons / Sq. KM No. of Districts 18 + 4 No. of Sub divisions 33 No. of Blocks 211 No. of Villages 32,620 No. of Villages Electrified 14,667 No. of Villages connected by roads 8484 Health centres 506 Schools 21,386 Universities 5 Total Geographical Area 79.70 Lakh Hect **
*£1= approx 80 Rupees (Rs) ** 1 Lakh = 100,000; 1 Hectare = approx 2.5 Acres
1.5 Leprosy Control Programmes in India
In India, the National Leprosy Control Programme has been operational since 1955,
early case detection and dapsone monotherapy being the main interventions. For
nearly two decades it moved at a slow pace. In 1983 the control programme was
renamed National Leprosy “Eradication” Programme with the goal of eradicating
leprosy by 2000. It was based on early case detection (population and school surveys,

LSHTM Candidate Number 470127 14
contact examination and voluntary referral), short term multi-drug therapy, health
education, ulcer and deformity care and rehabilitation activities. An appraisal in 1997
indicated that while overall progress was satisfactory, it was uneven in some states.
To address this, the Modified Leprosy Elimination Campaign (MLEC) was launched,
which included short term orientation training in leprosy to health staff, increasing
public awareness and house-to-house case detection for a period of six days. The first
of five such MLEC rounds was conducted in 1997-98 and the fifth in 2003-0415.
Currently the strategy of the National Leprosy Eradication Programme includes11:
• Decentralization of NLEP to States & Districts
• Integration of leprosy services with General Health Care System (GHS)
• Leprosy Training of GHS functionaries
• Early diagnosis & prompt MDT, through routine and special efforts
• Information Education and Communication (IEC) using Local & Mass Media
for reduction of Stigma & Discrimination.
• Prevention of Disability & Medical Rehabilitation.
• Monitoring & Periodic Evaluation
• Inter-sectoral collaboration
• Monitoring & Evaluation
1.6 Leprosy Prevalence in India: What is the true picture?
While the reported reductions worldwide and especially in India are laudable
achievements, such drastic reductions have left many in the scientific and NGO
community sceptical about what has actually happened. One theory is that changes to
the diagnostic, surveillance and reporting procedures are creating ‘data artefacts’ that
are obscuring the true picture of leprosy prevalence and control in India1-3.

LSHTM Candidate Number 470127 15
The 11th August 2006 WHO Weekly Epidemiological Report (Table 5) indicates that
since 2002, annual case detection in India decreased from 473,658 to 161,457; a 66%
decline of 312,201. Over the same 3 years global figures reduced from 620,638 to
296,499; a 52% decline of 324,139. Thus a staggering 96% of the global decline
(312,201/ 324,139) is accounted for by India. Such figures lend themselves towards
disbelief and scepticism16.
Declaring that leprosy has been eliminated from a country has very serious
implications. A Government making such a declaration may disband its control
programmes and disperse skilled staff. Uncertainties are generated as to who will
provide drug treatment once elimination is achieved, who will train primary health
care workers once vertical programmes become ‘integrated’, what plans will exist for
the long-term care of patients with nerve damage, deformities and disabilities. There
is the danger of a repeat of what happenned with tuberculosis and malaria, which in
the 1960’s were pronounced defeated, only to re-emerge now as global emergencies3.

LSHTM Candidate Number 470127 16
2 Aims & Objectives
2.1 Aim
To explore the role played by changes to definitions, ascertainment procedures, and
diagnostic and registration conventions in the reported reduction in prevalence of
leprosy in India over the last decade. Recommendations will address issues related to
the assessment of leprosy prevalence.
2.2 Objectives
• To gain understanding about the change in leprosy prevalence in India over the past
decade.
• To explore changes in diagnosis and reporting surveillance systems in India over
the same period.
• To understand how the diagnostic and reporting systems for leprosy are currently
organised in India, using the state of Jharkhand as a case study.
• Draw conclusions about the possible relationship between changes of case
definitions, ascertainment procedures, and diagnostic and registration conventions
(etc) and the dramatic reported reductions in leprosy rates.

LSHTM Candidate Number 470127 17
3 Methodology
Given the complexity of the research question, a much larger scale research project
would be required to fully explore all relevant issues in depth. This rapid assessment
of the key issues is based on a literature review and semi-structured interviews of key
informants involved in leprosy work on the ground in Jharkhand.
3.1 Literature Review
3.1.1 Selection Criteria The research question called for the exploration of the significance of changes in
diagnosis, reporting and surveillance systems and the prevalence of leprosy in India.
In the time available, a systematic literature review was difficult in the absence of a
single study design that could address all these concepts, with no specific participants,
interventions or outcomes (PICO criteria). Therefore the inclusion criteria for this
review were relevance by title to the concepts of the research question, relevance in
relation to India and/or Jharkhand and relevance by time period (1997-2007).
3.1.2 Search Strategy for Identification of Studies Initially EMBASE & EMBASE Classic were searched. The results were then limited
by the criteria mentioned above, resulting in the initial list of studies. The same search
strategy was used to search MEDLINE, 1950 to July Week 5 2008. The EMBASE
results were matched to MEDLINE’s and new studies were identified. The Web of
Science, CINAHL and TRIP databases were subsequently searched. Internet searches
for non-peer reviewed literature was undertaken of UNAIDS, WHO, World Bank,
National Leprosy Eradication Programme (India), Ministry of Health & Family
Welfare (India), Google scholar, and non-governmental agencies (ILEP, Italian

LSHTM Candidate Number 470127 18
Association Amici di Raoul Follereau – AIFO, Leprosy Mission, Lepra) websites.
Online archives of the International Journal of Leprosy and Other Mycobacterial
Diseases (till ’05), Leprosy Review & Indian Journal of Dermatology, Venereology &
Leprology were searched (1997-2007). Further manual searching was undertaken
from the Indian Journal of Leprosy 1997-2007. Reference lists in the extracted articles
were also assessed.
Based on the research question, search terms were generated based on the following
major key terms: ‘leprosy’ (keyword, MeSH, other synonyms), ‘Hansen’s disease’
(key word, MeSH), ‘Case defin$’, ‘case finding’, ‘case detection’, ‘case diagnosis’,
‘new case$ or new case$ defin$ or new case$ diagnos$’, ‘registration$ or registration
convention$ or registration protocol$ or registration procedure$’, ‘India/ or Leprosy
Control/ or Leprosy/ or Health Program/ or Prevalence/ or Mycobacterium Leprae/’,
‘India’, ‘Jharkhand’ and so on. The search terms were combined using ‘and’/ ‘or’
where relevant. The search was then limited by year (1997 – 2007), humans and
English language. The actual search strategy is included as appendix 4.
3.1.3 Methods of the Review
Study Identification
The search results were reviewed based on the study titles, for general relevance to
one or more of the terms leprosy, prevalence, elimination, eradication, diagnosis,
registration, case finding/ case detection/ surveillance, India and/or Jharkhand in
various combinations and synonyms. Studies that did not contain any combination of
these or related terms in the title were discarded.
LSHTM Candidate Number 470127 19
Study Inclusion
Abstracts of the studies identified above were obtained and reviewed for eligibility in
terms of the selection criteria mentioned earlier. Emphasis was on relevance, time
period (’97 to ’07) and Indian context. Articles that did not have abstracts or where
the objectives or relevance were unclear, were withheld till further clarity could be
gained by reading the full text. The full texts of the included studies were obtained.
Studies that had been withheld thus far were excluded based on reviewing the full
text.
Data Extraction & Analysis
The selected studies were reviewed and any data relevant to the concepts of the
research question in any combination were extracted, collated and analysed for
associations between changes of case definitions, ascertainment procedures,
diagnostic and registration conventions (etc) and reductions in leprosy prevalence.
Analysis using validated instruments for assessing quality of studies and data
extraction was not possible, given the nature of the research question.
3.2 Semi-structured Interviews
The literature review was undertaken prior to the semi-structured interviews; so that
its preliminary findings could inform the topic guide for the semi-structured
interviewing. The purpose of the interviews was to understand from individuals
involved in leprosy control programmes in India about how the diagnostic and
reporting systems actually worked in practise and what changes had occurred between
1997 and 2007, specifically in Jharkhand.

LSHTM Candidate Number 470127 20
3.2.1 Topic Guide
Based on the findings from the literature review, a topic guide was drafted. This was
piloted with a sample of MSc PH students from London School of Hygiene and
Tropical Medicine and further modifications were made. It was then tested for cultural
and contextual appropriateness with colleagues from India and the study version was
finalised. This is included in appendix 5.
3.2.2 Selection of interviewees
The intention was to interview 10 individuals. Interviews were planned for one month
over December 2007. The number of interviews was based on an estimation of what
seemed feasible for the MSc project, and how many interviews would be required to
gain sufficient information on the context of leprosy control in India. Professionals in
the field of leprosy elimination locally in Jharkhand from NGO & Government
settings (General Health Services or specialized leprosy services), directly involved in
diagnosis and case finding were sought for interviews.
Identification and recruitment of interviewees at first instance was done through
contact with a regional level co-ordinator of leprosy elimination activities in a district
of Jharkhand as well as the lead of a key local general health provider in the region.
This enabled the researcher to visit some of the leprosy centres and interview
professionals.
The semi-structured interviews were undertaken following the topic guide (appendix
5) after securing informed and written consent, and recorded either by a digital audio
recorder or by scribing.

LSHTM Candidate Number 470127 21
3.2.3 Data Extraction and Thematic Analysis
The interviews were transcribed into English. They were then analysed using the
techniques of thematic analysis. Based on the initial interview, a preliminary coding
scheme was generated based on the original key themes from the interview guide.
This was modified in terms of categories and sub-categories as the coding of the
subsequent interviews progressed and new themes emerged, in an iterative process.
The final coding scheme (appendix 6) was generated and the coded extracts of the
various interviews collated under the identified themes. This collated data was then
scrutinized, compared within and across data sets, and analysed, resulting in further
modifications to the coding scheme and the eventual generation of the results.

LSHTM Candidate Number 470127 22
4 Results & Findings
4.1 Literature Review
4.1.1 Results of Search Strategy
A total of 30 articles were identified that met the inclusion criteria and were reviewed.
These papers were located from the following sources. The EMBASE & EMBASE
Classic search yielded 573 articles. After limiting this result to English language,
humans & 1997-2007, 327 articles resulted. Screening these articles for general
relevance by title and year (1997-2007) narrowed down results to 52 articles. Reading
the abstracts of these articles narrowed down the results to 24 articles of which 11
articles were found relevant to the research question after reading the full text.
MEDLINE search (1980 – 2007 Week 11) using the same search strategy as for
EMBASE yielded the same articles. Searches of Web of Science, CINAHL and TRIP
databases also did not identify any new articles. Further searches of UNAIDS, WHO,
World Bank, National Leprosy Eradication Programme (India), Ministry of Health &
Family Welfare (India), Google scholar and non-governmental agencies (ILEP,
Leprosy Review, Leprosy Mission) websites identified 5 further articles. Manual
searching of the Indian Journal of Leprosy archives (1997-2007) yielded 14 possible
articles of which 7 were included. Searching the references of all included articles
identified 7 further papers.
4.1.2 Findings from the review
A report in the British Journal of Medicine in 200517 stated that doctors in India were
expressing concern about health authorities playing down the number of leprosy

LSHTM Candidate Number 470127 23
patients in a bid to declare leprosy eliminated from India as a public health problem.
Elimination targets would allegedly be met through “artful manipulation” of the
definition of leprosy and “avoiding active case detection”. The Principal of the
Christian Medical College in Vellore, Tamil Nadu was quoted saying that new cases
were emerging almost unabated and yet they had explicit warnings against being
overenthusiastic in case detection.
4.1.2.1 How has prevalence been distorted?
What appears to emerge from the literature is that repeated changes of definitions,
ascertainment procedures, and diagnostic and registration conventions, by both WHO
and the National Leprosy Eradication Programme significantly distorted the true
reductions to leprosy prevalence in India, adversely affecting the ability of the
scientific community to monitor what actually happened2.
Particularly over the last decade, WHO has made several changes to leprosy policies
and guidelines that were adopted by the NLEP and have had major impacts on
prevalence data of India. Additionally, NLEP itself implemented operational practises
and policies that further compounded these inaccuracies and distortions.
4.1.2.2 How did WHO guidelines and policies affect prevalence in India?
a. By changing the way prevalence is calculated
Changing period prevalence to point prevalence: At the start of the elimination
programme, year prevalence was used to report the number of registered patients.
Later WHO advised that this should be changed to point prevalence to include only
those patients on the registers as of 31st December of the year, resulting in a marked
decline in the numbers registered and an automatic decrease in prevalence18. This
LSHTM Candidate Number 470127 24
especially affected PB cases which form 90% of cases in India, since these are treated
either by ROM or 6 month MDT and are presumably no longer on the registers by the
end of the year.
b. By changing the definition of a case
WHO defined a “case” of leprosy as a person showing clinical signs of leprosy, with
or without bacteriological confirmation of the diagnosis, and who has not yet
completed a full course of treatment with MDT19. This definition was adopted by
NLEP in India and resulted in only patients currently on MDT being included in the
prevalence count, effectively excluding patients with ongoing complications or
disabilities4,20.
c. By changing diagnostic classifications
Generally an accepted criterion for the diagnosis of leprosy was positive findings for
any two of the following three criteria 8,21:
I. Loss of sensation in a skin lesion to light touch
II. Enlarged nerve among all palpable peripheral nerves
III. Positive skin smear
The slit-skin smear was key to estimating bacterial load and classifying patients, for
treatment purposes, as multibacillary or paucibacillary. According to some experts
this was the weakest link in implementation of the MDT programme22,23. The advent
of HIV/AIDS and poor quality control on slit-skin smears shifted the focus to clinical
classification of PB & MB cases24,25,26.
WHO (WHO expert committee, 7th report, 1998)27 decided that counting skin lesions
would be no less sensitive than counting bacilli in a skin smear:
I. Paucibacillary single lesion case defined as a patient with one skin lesion

LSHTM Candidate Number 470127 25
II. Paucibacillary, 2 – 5 lesions
III. Multibacillary, more than 5 lesions
Neurological assessments and slit skin smears do not contribute to this
classification18. Neuritic leprosy, which accounts for a significant proportion of
leprosy in the Indian subcontinent28,29,30 manifests with neural signs and/or symptoms,
without any clinically evident skin involvement31. Such cases are very likely to be
missed using the above classification32,33,34,35.
The WHO document states that in 70% of patients, diagnosis can be made by a single
sign: an anaesthetic skin patch. In 2002 an evidence based group convened by the
International Leprosy Association, found that the other 30% are multibacillary
patients, who are more likely to be infectious and to develop nerve damage4,36.
d. By changing treatment durations and regimens
In 1998, the WHO expert committee on Leprosy concluded that the duration of the
MDT regimen for MB leprosy could be shortened to 12 months (from 24 months). It
was even suggested that all leprosy patients should be treated for only 6 months
despite the lack of scientific evidence to support this18,37. By shortening the treatment
duration for MB-MDT from 24 to 12 months, the number of MB registrations halved,
thus improving statistics and excluding large numbers of MB cases from point
prevalence data18,38.
Further, on the basis of field trials and clinical studies WHO decided that a single
dose combination of rifampicin- ofloxacin- minocycline (ROM) was an acceptable
and cost-effective alternative regimen for the treatment of single lesion PB
leprosy18,27. ROM therapy improved statistics in India, a country with a relatively high

LSHTM Candidate Number 470127 26
proportion of single lesion cases and 90% PB cases. This effectively wiped out the
group from the prevalence data18.
A case is considered cured once the therapy is completed regardless of the
bacteriological load. There were no definite data establishing that 1 year MB-MDT
treatment would be sufficient to prevent relapses; in fact, there were some indications
that patients with high number of bacilli (a BI of 4-6) might relapse39. Moreover, it
could be expected that the number of leprosy reactions in the year after RFT would
increase, leading to more disability in the so-called ‘cured’ patients8,40,41.
In 2002, WHO proposed a new treatment called ‘accompanied MDT’42, whereby
patients are given all the medicines for the full 6 or 12 month course of treatment at
their first visit, with the proviso that someone close to the patient will take
responsibility for helping the patient complete the course of treatment. This is a
curious reversal of policy, where for the ten years prior to this the strength of the
leprosy programme lay in the monthly supervision of medication, which also meant
that nerve damage was picked up early and health education could be ongoing4.
4.1.2.3 How did operational practises and policies of NLEP affect prevalence?
a. ROM Therapy from 1998 – 2002
Single dose treatment for single lesion paucibacillary patients; through ROM therapy
was introduced in January 199843 and was in vogue for about five years till 2002.
These cases never came into prevalence data since they received only a single dose
treatment. They should have been counted as new cases44.

LSHTM Candidate Number 470127 27
b. Changing from active case detection to voluntary reporting
Official guidelines launched in March 2005 recommended that the state should stop
actively searching for cases and register only those with confirmed diagnosis45.
Earlier in January 2005, in the South East Regional meeting of National leprosy
programme managers46 it was decided that every leprosy case detected by primary
health care workers was to be confirmed as leprosy by a special team at the district
level. This approach of 100% validation was adopted from 2005. Various methods of
active case detection were to be discontinued and case detection was to be taken up by
voluntary reporting. These decisions affected case detection enormously with 100%
validation rarely feasible and a significant proportion of cases never getting examined
for confirmation44.
c. Underdetection & Underdiagnosis
While increasing attention was being given to ‘overdetection’, ‘underdetection’ was
being ignored, perhaps because it was difficult to estimate and less appealing to
programme managers and therefore had no apparent mandate47. The few sample
surveys conducted using traditional methods48 or Lot Quality Assurance Sampling
(LQAS)49 have revealed sample prevalence 4-5 times higher than recorded
prevalence. Even after five LECs and with reasonably effective MDT service, the
extent of underdetection is very high50. Underdiagnosis is more likely in borderline
lepromatous and lepromatous leprosy because of low degree of suspicion. These are
the cases that are likely to transmit infection in the community47.
In several high endemic states such as Bihar, the decline in prevalence is dramatic.
Deliberate under-detection of cases during the year 2003-04 by the over-zealous staff
due to pressure at all levels to achieve elimination by 2005 could have contributed to
LSHTM Candidate Number 470127 28
the steep decline in the PR51. In fact, there was a report from a reputed NGO with
credible leadership that several new cases in an endemic district under its support
were not reported during the first quarter of 200551,52.
Cases are missed on account of non-coverage of certain areas or population groups
(working men, difficult to reach areas, tribal populations, people below poverty line
etc.)53. Marginalisation on account of gender and poverty, inaccessibility to health
services, opportunity costs, disabilities and stigma were some known factors that
influence case detection activities54.
d. Changing from vertical to integrated programmes
The integration of leprosy programmes into the general health services, moving away
from the erstwhile vertical programmes, has resulted in widening health care
networks, bringing diagnosis and treatment services closer to the patient38 and more
workers involved in the diagnosis and treatment of leprosy18. But these advantages
have been nullified by lack of staff at PHC’s and not enough health centres. E.g. in
Bihar there is 1 health centre for every 200,000 population, in contrast with South
India, where there is 1 for every 30,000 population38,55. Lack of proper trained and
specialised staff, compounded with lack of consensus over case definitions, absence
of common standards for instrumentation and procedures related to sensory testing of
anaesthetic patches has resulted in over and under diagnosis of cases56. In 2004, inter-
observer variation for diagnosis was estimated at 50% and validation of diagnosis
conducted in various places revealed wrong diagnosis ranging between 10 & 30 %56. )

LSHTM Candidate Number 470127 29
e. Target setting
Targets provide an inescapable sense of urgency among health workers44. In the
NLEP the targets were of two kinds; the first target was to detect at least a minimum
specified number of cases and the other was in respect to marching towards
elimination by year 2000, pre-fixing prevalence figures for the year44. To achieve the
goal of elimination by the year 2000, targets were prepared after committing to the
goal of elimination57 and projections were made on such targets. Setting targets was
eventually considered counterproductive to the assessment of surveillance data and
was discontinued by the Government of India58.
f. Excluding data
Data from private health practitioners and dermatologists that serve large segments of
the population are not included in official prevalence data. NGO’s and private
practitioners that are not part of the governments elimination programme may serve a
significant segment of society and their patients are not included in official
figures38,59.
g. Masking sub-national high prevalences
In large countries such as India, national averages do not mean anything. Severe
problems in some high prevalence states can easily be masked and averaged out by
well-performing low prevalence states60. Prevalence at sub-national levels, provided
sub-national populations are sufficiently large, is of greater relevance60.
LSHTM Candidate Number 470127 30
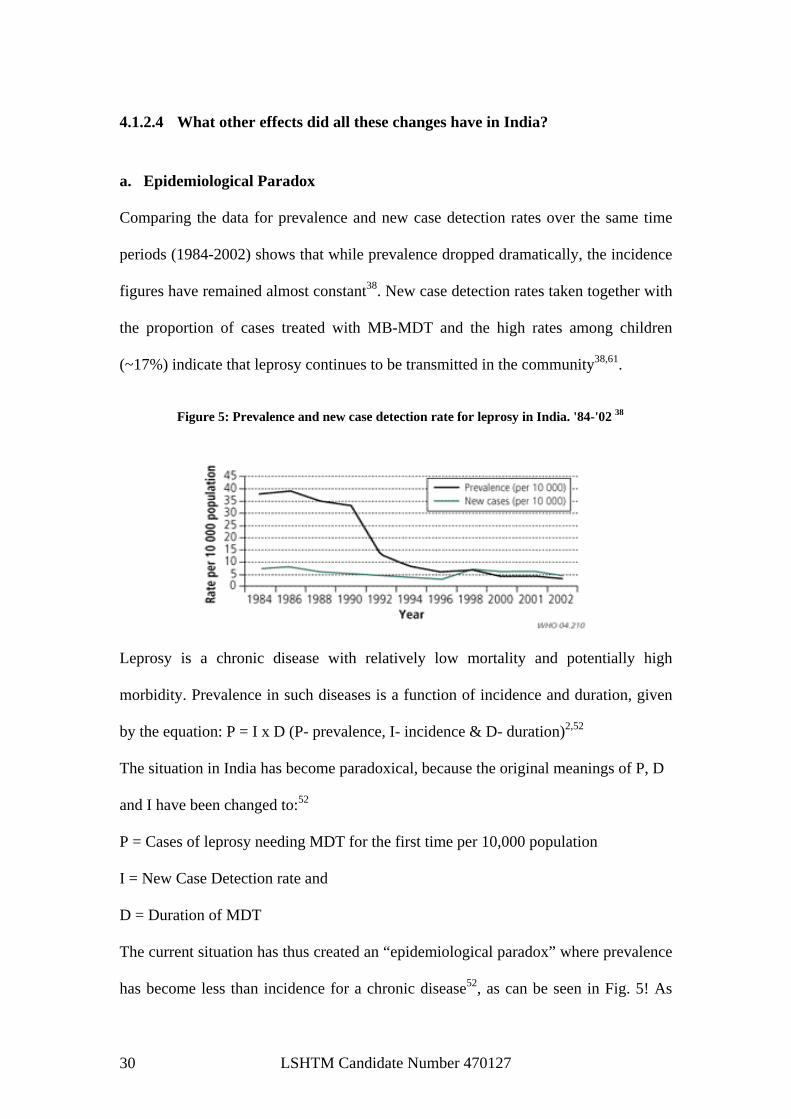
4.1.2.4 What other effects did all these changes have in India?
a. Epidemiological Paradox Comparing the data for prevalence and new case detection rates over the same time
periods (1984-2002) shows that while prevalence dropped dramatically, the incidence
figures have remained almost constant38. New case detection rates taken together with
the proportion of cases treated with MB-MDT and the high rates among children
(~17%) indicate that leprosy continues to be transmitted in the community38,61.
Leprosy is a chronic disease with relatively low mortality and potentially high
morbidity. Prevalence in such diseases is a function of incidence and duration, given
by the equation: P = I x D (P- prevalence, I- incidence & D- duration)2,52
The situation in India has become paradoxical, because the original meanings of P, D
and I have been changed to:52
P = Cases of leprosy needing MDT for the first time per 10,000 population
I = New Case Detection rate and
D = Duration of MDT
The current situation has thus created an “epidemiological paradox” where prevalence
has become less than incidence for a chronic disease52, as can be seen in Fig. 5! As
Figure 5: Prevalence and new case detection rate for leprosy in India. '84-'02 38

LSHTM Candidate Number 470127 31
durations of MDT got reduced from life-long treatment, to 10 years to 2 years to 1
year, and now for only 6 months, the prevalence rate reflects largely this diminishing
factor52,20.
b. Social Stigma and case detection
Due to prevailing negative perceptions of leprosy and social stigma, persons
suspecting leprosy delay seeking effective treatment till irreversible symptoms
develop. By then, the disease would have spread within the body and would also have
been transmitted to contacts. It is obvious that drugs alone can never solve a public
health problem, such as leprosy, due to public attitudes and health behavior
conditioned by massive prejudices, inadequate knowledge & several socioeconomic
factors in accessing MDT or anti-reactional drugs, etc62,63. This has been further
exacerbated by the implementation of voluntary reporting as a method for case
detection and dismantling specialist leprosy infrastructure through integration.
c. Reduced government spending on an ‘eliminated’ disease
With elimination declared, resources are becoming limited in relation to leprosy work
in India. Field workers say new cases are emerging continuously but there are not
enough resources to help them. A leprosy expert in Osmania Medical College,
Hyderabad said that trained leprosy workers are being diverted for HIV work or as
multi-purpose health workers. He claimed that India would soon lose trained leprosy
personnel and track of the disease and it would become a simmering problem like
malaria59.

LSHTM Candidate Number 470127 32
4.1.2.5 Alternative explanation for reductions in prevalence
Some WHO experts are saying that the dramatic reductions in India were mainly due
to the minimization of operational factors, such as wrong diagnosis, re-registration of
cases, delayed treatment completion, overtreatment etc. Better treatment compliance
rates and regular updating of registers were also identified as important contributory
factors64. Re-registration of old or cured cases as new patients, ranging between 33-
82%53 has been observed.
Some researchers say that because leprosy eradication was administered as a vertical
programme and was poorly integrated into general heath services, this hindered case
detection and treatment. The social stigma associated with being seen, and easily
identified and labelled by the community, while taking treatment from special leprosy
centres acted as a deterrent to voluntary reporting31.
4.1.2.6 WHO Elimination Hypothesis: Eradication or Elimination?
The idea of elimination was based on the hypothesis that at a prevalence of less than 1
per 10,000 population, transmission of leprosy in the community would be
interrupted. The International Leprosy Association’s Technical Forum noted that there
was little evidence to support this hypothesis65. Leprosy has a long incubation period
from 2 – 20 years66; newly diagnosed patients may have transmitted the disease to
others in their family or community long before their disease is detected38. Eradication
would imply that a disease reaches zero prevalence and zero transmission, which is
improbable with the disease characteristics of leprosy52.

LSHTM Candidate Number 470127 33
4.2 Semi-structured interviews
4.2.1 Leprosy Elimination Programme
Guidelines, policies and targets
All the informants said that guidelines and policies were disseminated from national
level down through states to districts, blocks and villages. One informant said that
about ten years ago skin smears were done to confirm cure before patients were
released from treatment (RFT) and this changed to RFT once the MDT course was
completed adding “it was the government policy… it keeps changing any time…”
This concurs with the literature review findings, the implication being that at the most
a case would remain registered for 12 months, after which it would no longer be
included in prevalence data, regardless of the actual cure status.
All informants maintained that the government did not set any targets. NGOs set their
own targets in relation to rehabilitation work according to the mandates of their
funding agencies.
Campaigns
One informant said that the government had conducted an awareness campaign
(BLAC- block level awareness campaign) recently, prior to which one had been done
four years ago, which coincides with the last (fifth) MLEC (Modified Leprosy
Elimination Campaign) in 2003-04. Another said that NGO’s have been involved in
IEC activities for many years, using individual, group and mass level approaches.
4.2.2 Case detection “…though the survey is over now but still we are doing the survey because we believe
that there is a lot of hidden cases…”

LSHTM Candidate Number 470127 34
“…though they (government) are asking help from us, they are involving us also but
our party is… umm… totally off doing survey… because nowadays whatever case we
are finding by any means, it will be treated as voluntary reporting…”
“…the reason was government accepted that… umm… it is a leprosy free area so no
further detection is necessary. But there are two things, number one… umm… I think
that this is arbitrarily deterred… and number two who can say that within this ten
years further cases won’t come up?...”
“INT: I see…. so, you do not do case detection officially….
ANS: No…”
Four out of five informants said that NGO’s no longer undertook active case detection,
at least in official capacity. One reason offered was that any cases they detected were
treated by the government as voluntary reporting, so there was no recognition for this
work. While one informant maintained that the peripheral health workers still did door-
to-door surveys and also said there had been no changes over the years to the way case
detection was done, the rest said that in general active case detection had been stopped;
three of them stating that NGO’s had stopped since 2001. This is interesting because
the literature review findings revealed that active case detection had officially stopped
as per NLEP guidelines since March 2005. If NGO’s had ceased active detection since
2001, this would have had a significant impact on case finding and subsequent
prevalence data between 2001 and 2005, particularly since Jharkhand is highly
endemic for leprosy. However unofficially they still did this through school surveys
and village meetings as they believed there were a lot of hidden cases in the
community, even though their efforts were not subsequently acknowledged.

LSHTM Candidate Number 470127 35
4.2.3 Case diagnosis “ANS: But now there is no such thing as a relapsed case… they are calling them old
cases and treating them…
INT: That means these cases are not appearing on the register…
ANS: No… they are not appearing on the register…”
“Around 1982 when MDT was introduced, MB and PB was used. In those days smears
were done and doctors who were scientifically inclined did biopsies. This stopped
afterwards.”
All informants maintained that provisional diagnosis through the detection of cardinal
signs of leprosy was routinely done by peripheral health workers (Anganwadi
workers, ANM’s & MHW’s) as well as by NGO’s during school and village
meetings. The suspected cases were referred to the PHC for confirmation. This is in
line with findings from the literature review.
All informants said that cases were diagnosed by the medical officer at the PHC
through clinical examination for patches and nerve enlargement and no skin smears
were taken to confirm the diagnosis.
Two informants said that smears to confirm diagnosis had been done till 2000, being
stopped at the time the programme was integrated into general health services after
which diagnosis was done by clinical examination alone. This is in agreement with the
findings from the literature review. One informant appeared to not know if smears had
been used in the past to diagnose cases, even though this informant had been working
in the leprosy field for a considerable time at a senior level. Three informants said that
till as recently as 2006-07, NGOs had been involved in case detection, diagnosis,
registration and treatment of leprosy cases in their designated districts/ blocks.
LSHTM Candidate Number 470127 36
While relapsed cases, like new cases needed to be registered, one informant said that
the approach taken by PHC’s was to consider them as old cases and therefore not
register them. This would impact on prevalence data quite significantly, as in endemic
states such as Jharkhand there would be a significant number of relapsed cases.
While one informant said that overdiagnosis happened in the past but was now very
rare after validation started, others were unable to comment on this.
4.2.4 Case validation Three informants said that case validation and quality assurance was undertaken by
the DLO. This was started in 2003-04 and was done by a multi-disciplinary validation
team, comprising the DLO and representatives from WHO and NGO’s, that visits
block PHC’s fairly frequently at pre-arranged times. The literature review showed
that a 100% validation approach was adopted since March 200544. If case validation
was indeed carried out since 2003-04, then the high prevalences in Jharkhand since
then cannot be put down to overdiagnosis or re-registration as alternative views of
prevalence decreases suggest64. If one added to the equation the fact that active case
detection by NGO’s ceased in 2001 and officially by NLEP in 2005, then there is a
much higher likelihood of under rather than over detection and diagnosis.
4.2.5 Case registration
Informants said that cases were registered at PHC level if the medical officer was
satisfied that the case was new. Relapsed cases were regarded as old cases and
although they were provided treatment, they were not registered. NGO’s no longer
registered cases. Further they said that registered cases were taken off the prevalence
register once they were released from treatment (RFT) - six months for PB cases and
12 months for MB cases, regardless of bacterial load. Re-registration was not

LSHTM Candidate Number 470127 37
common and occurred when a case already registered in one district, migrated to
another and claims to be a new case.
This corroborates findings from the literature review that changes to the RFT (release
from treatment) protocols artificially reduced prevalence.
4.2.6 Range/Types of cases “INT: ….and have you seen children…with leprosy…?
ANS: Yes absolutely, it happens a lot…”
Most informants said that majority of cases of leprosy were PB (Paucibacillary), with
one informant making the observation that in places where literacy, education and
awareness were greater more PB cases were observed, while areas with less
education, awareness and hygiene had more MB cases. One informant said that MB
cases were more common.
While all informants agreed that in general all types of cases had reduced, they said
that in children leprosy continued unabated with relatively little change to the
numbers seen, making up around 10-15% of the cases according to one informant.
Most children with leprosy had a positive family history for leprosy although one
informant was quick to point out that this need not be the case. In the pre-MDT era
deformities were very common but now the deformity rate had come down.
Deformities were mostly of grade 2 (visible deformity/ damage present in hands and
feet and severe visual impairment).
The fact that leprosy continues unabated in children, with a positive family history of
leprosy in most cases, is evidence of continued active transmission of leprosy in the
region and underscores that there are major shortcomings in early case detection.

LSHTM Candidate Number 470127 38
4.2.7 Case treatment
All informants maintained that there was no longer any single lesion ROM therapy.
The duration of treatment for PB cases was 6 months to be completed in 9 months, for
MB cases 12 months to be completed in 18 months. An informant said that from 1986
till 1996 MB cases were treated with 24 months of MDT. In the past NGO’s were
closely involved in detection, diagnosis, treatment and registration of cases but now
only the government health services did this. This corroborates literature review
findings.
Informants said that once cases were diagnosed and registered at the PHC, it provided
the first months MDT. Subsequent months of MDT are provided by peripheral health
workers, who monitored the cases for improvements and signs of reactions or
complications, which if present resulted in the case being referred back to the PHC for
further management. This appears to be a variant form of ‘accompanied MDT’
advocated by WHO in 20024 and contrasts with ‘supervised MDT’ that was
recommended earlier. This arrangement has a high possibility of delayed treatment
completion, overtreatment, poor treatment compliance rates, failure to detect
complications or reactions, relapses and less opportunity for health education.
4.2.8 Case cure
Informants were of the view that with completion of the full prescribed course of
MDT the assumption was that the patient is cured. One informant said this is
considered ‘100% cured’. Treatment completion results in patient being ‘released
from treatment’ or ‘RFT’, which is done at the PHC once the medical officer is
satisfied that no complications or reactions are in evidence. The case is removed from
the prevalence register. Till 1996 smears were done to determine if cases were cured.
LSHTM Candidate Number 470127 39
The literature review revealed that there was no definite data establishing that 1 year
MB-MDT treatment would be sufficient to prevent relapses; in fact, there were some
indications that the patients with high number of bacilli (a BI of 4-6) might relapse39.
Moreover, it could be expected that the number of leprosy reactions in the year after
RFT would increase, leading to more disability in the so-called ‘cured’ patients8,40,41.
To regard completion of MDT course as evidence of 100% cure is inaccurate and this
definition of a cured case exacerbates the endemicity of leprosy in India.
4.2.9 Prevalence data
Informants said that prevalence was calculated as the total balance of cases under
treatment in an area divided by the total population of that area, multiplied by 10,000
to give the prevalence per 10,000 population. It was calculated monthly at every block
PHC. Each block reported to the district (DLO) and from all the districts, the data went
to the state (SLO). One informant said that prevalence was calculated by randomly
surveying a thousand people in an area to find how many of them had leprosy, giving
the prevalence per thousand population. Earlier the denominator was per 1000
population, but this was changed to per 10,000. Only one informant seemed certain
about the way prevalence was calculated.
4.2.10 Case reductions and leprosy as a public health problem
“I would say that leprosy is still a public health problem. Particularly awareness issues.
In middle class families there is a lot of stigma associated with leprosy, even though it
is much less than before. General health workers do not have much training in relation
to leprosy particularly on the course duration. Training on leprosy needs to be more
detailed to multi-purpose health worker level.”

LSHTM Candidate Number 470127 40
All respondents said that the prevalence of leprosy had been greatly reduced. NGOs
had a key role to play in this. However respondents felt that there were a lot of hidden
cases and also that unless the social stigma of the disease was removed one could not
say leprosy was eliminated. One respondent felt that there had not been significant
reductions in prevalence locally. Most respondents maintained that it was still a public
health issue, due to the presence of hidden cases, the challenges of SER/CBR and
social stigma.
4.2.11 Vertical VS Integrated
While one respondent felt that the integrated system worked better, another felt it
could have been introduced later because unless social stigma was tackled and the
barriers created by the absence of social acceptance of the disease removed,
integration was counter-productive. In the erstwhile vertical model there were
specialised leprosy centres to which patients came for dressings, physiotherapy and
treatment. Many of these were shut down as recently as two-three months ago and
subsequently the patients were reluctant to visit the general health services due to the
fear of social ostracism.
“First you remove the social stigma. Socially acceptance must be beyond on
government level or do some machinery… put some machinery then only you can
realise. Generalism is what…when there is a social acceptance is there. As long as
you don’t have acceptance of leprosy patient in the society, so how can you generalise
this?”
“…social acceptance must be there for leprosy is integrated. If you declare
integrated… government generalised the cases, it doesn’t have meaning. Because
LSHTM Candidate Number 470127 41
when leprosy is a stigma, unless and until you remove the social obstacles, no
integration is there. Integration start from the social obstacles first… then to your
medicine part and hospital part… many thing can be done, many thing has to be done,
specially for the deformity cases.”
“… If you have seen Calcutta based newspapers… I have read two-three months
earlier, so many leprosy hospitals… those who are set out for leprosy only… either
they have stopped because all the doctors, staffs… those who are deputed for the
leprosy patients, they have withdrawn… they have deputed some other hospitals…
that hospital has been closed or building is this there because integration is there. So
leprosy patient having ulcer or deformity, those…those who are used to come that
hospital…they are feeling little hesitant…they are not attending to general hospital…
not attending general hospital. So this is practical… practically we have seen.” …
One informant said that in the vertical programme there was improved networking
between NGO’s and the government, with better trained, knowledgeable and
experienced staff and consequently better care. But the social stigma extended to
those workers involved in leprosy work themselves, compounded by the existence of
separate leprosy wards in general hospitals.
The integrated approach resulted in increased capacity for leprosy work and many
patients felt less stigmatised going to a general health service for leprosy. Staff
attitudes towards leprosy patients also improved with greater understanding,
sympathy and openness. Because peripheral health workers could do home visits for
any number of reasons, many families felt less stigmatised. Lack of specialised,
experienced staff and the lack of training used to be a problem but this is apparently
no longer the case.

LSHTM Candidate Number 470127 42
Some informants said that the programme was still vertical in many places, with little
real integration. Earlier, when there was a vertical set-up, more patients were
registered as the case detection and diagnosis was better. Now due to the distances a
patient had to travel to get the closest PHC, many cases remained unregistered and
untreated for a long time, resulting in greater severity and complications while
transmitting the infection to the community. Despite the increased numbers of staff
involved in leprosy work at the periphery through integration, the patient had to still
visit the PHC at first instance for confirmation, registration and treatment before the
peripheral workers could extend support locally.
4.2.12 Improvements, limitations and shortcomings
One respondent felt that it was necessary to incentivise case detection at the
periphery, in order to find hidden cases. In pulse polio drives apparently peripheral
workers are told that if they brought in a certain number of cases they would get a
cash bonus. Others said there was a lot of room for improvement in IEC, campaigning
and public awareness initiatives. This could be tied in with the ongoing government
campaign, the total literacy mission. A lot more work was needed in the rehabilitation
of leprosy patients with disabilities and deformities both medically and socially.
Survey and active case detection were still very important, as many cases of leprosy
were not coming forward voluntarily due to stigma and also lack of awareness about
leprosy.
“So...that survey or say your reaching to this people is very essential. It won’t be
proper to expect particularly in this area where their literacy rate is very poor that they
will just come forward and disclose that they are having this sort of things. Neither

LSHTM Candidate Number 470127 43
they can detect…uhh…the disease…if at all they can detect…out of that stigma or the
fear or the some sort of shame they can’t disclose.”
“Voluntarily they cannot come forward….so we have to reach out to them.”
“And if we take it granted that who will have the disease and they will come forward
in this Indian context, or in the context of this region… umm… it is too much to
expect.”
4.2.13 Stigma
All respondents said that social stigma prevented patients from going to general health
services. Stigma hampered with rehabilitation work and placed severe limitations on
the occupational opportunities of leprosy patients in addition to those already
experienced by them on account of deformities and disabilities. They said that one
could not say a patient of leprosy was cured or that leprosy was eliminated unless
stigma was removed. Integration too would always remain incomplete unless stigma
and other barriers to access were addressed.
“So ultimately they have taken medicine but while their social status… you cannot
say we are cured… ultimately stigmatized is there… social acceptance is not there…
so until and unless you put a patient in that level where he can move here and there,
he or she can earn his butter and… bread and butter… then treatment is not cured, so
far NGO sense of concern is there. So far medical is concerned you have taken…
given medicine, it’s cured. But we feel until and unless you develop that person in his
previous life it’s not completed.”
LSHTM Candidate Number 470127 44
5 Discussion It is evident from the literature review that numerous changes to case definitions,
ascertainment procedures, and diagnostic and registration conventions over the last
two decades have directly or indirectly impacted on leprosy prevalence. Findings
from the semi-structured interviews corroborate these findings locally in Jharkhand.
The prevalence of leprosy in India has most definitely declined, but the true extent
remains unclear. The fact that in 2003 the Indian Council for Medical Research found
leprosy prevalence in Agra 40 times higher than official figures67 and the few sample
surveys that have been conducted through traditional methods48 and Lot Quality
Assurance Sampling (LQAS)49 revealed sample prevalence 4-5 times higher than
recorded prevalence, underscores this ambiguity.
Apart from the issue of whether or not prevalence has reached “elimination” levels in
a country that has almost 80% of the global burden of leprosy38,68, the whole
elimination hypothesis itself, that prevalence under 1 per 10,000 population interrupts
the transmission of leprosy in a population, is highly contested65. Perhaps the
elimination concept has now served its purpose and might even become detrimental to
public health2. The elimination rhetoric has come close to eliminating leprosy
research2,69. Funders and young researchers are not attracted to an officially
“eliminated” disease and there is little active research on the subject despite our
continued ignorance about its natural history2.
LSHTM Candidate Number 470127 45
While prevalence dropped dramatically, the incidence figures have remained almost
constant38. New case detection rates taken together with the proportion of cases
treated with MB-MDT and the high rates among children (~17%) indicate that leprosy
continues to be transmitted in the community38,61. The impact of MDT on prevalence
and case detection trends across India was earlier examined in a workshop conducted
by the Indian Association of Leprologists in Chennai, in 199370. It observed that in the
face of rapid decline in prevalence following MDT, NCDR remained quite steady.
NCDRs for several countries clearly demonstrated that MDT did not result in a
precipitous decline in NCDR71. Thus prevalence reductions could not be attributed
directly to MDT per se. Unchanged levels of new case detection could be explained
by intensive case finding in some states, but examination of state-level data did not
support such a hypothesis53. Hence even in the absence of active case finding
strategies such a level of decline is not convincing.
Prevalence figures have been influenced by changes to case definitions whereby a
case is only a case so long as it is being treated with MDT. Once the treatment is
completed, the case is considered cured which when married to the WHO
recommended convention of MDT lasting 12 months only (in MB cases and 6 months
for PB cases) and changing from period to point prevalence18, results in many cases
being excluded from prevalence data regardless of their true status4,20. From 1998 to
2002 a substantial proportion of cases never made it into prevalence or incidence data
on account of single dose ROM therapy for single lesion paucibacillary cases, which
is particularly common in India43,44.

LSHTM Candidate Number 470127 46
Findings from the literature review and the interviews underline the role of social
stigma in the reluctance of leprosy patients to seek treatment and care. Two changes
in the leprosy programme, switching from a vertical to an integrated leprosy
programme and the cessation of active case detection in preference for voluntary
reporting, have further compounded this situation as individuals fearing social
ostracism and marginalisation are hardly likely to come forward voluntarily, that too
to a general health care system. Marginalisation on account of gender and poverty,
inaccessibility to health services, opportunity costs, disabilities and stigma are some
known factors that influence case detection activities54.
In 2003 WHO opined that the ‘case detection trends in India are not showing any
appreciable decline and there is no clear explanation for the persistence of this
situation in spite of the highly specialised and expensive vertical programme in
operation for close to 50 years’72. For political leaders achievement of leprosy
elimination has been and is a highly attractive objective, besides having one problem
less in their portfolio60. Perhaps this explains, to some extent the complex political
and economic realities in which the leprosy eradication programme sits and the
urgency to reach so-called ‘elimination’?
An alternative explanation for the reductions is that they were mainly due to the
minimization of operational factors, such as wrong diagnosis, re-registration of cases,
delayed treatment completion, overtreatment etc.; and better treatment compliance
rates and regular updating of registers were also important contributory factors64.
Others say that leprosy has a strongly committed constituency, which is not easy to
dismantle irrespective of the size of the problem, with this constituency lobbying and

LSHTM Candidate Number 470127 47
working towards sustaining the remaining anti-leprosy activities60. The subtext is that
such a constituency would want to demonstrate that leprosy is still not eliminated, in
order to remain viable as many vested interests, livelihoods and jobs were at stake.

LSHTM Candidate Number 470127 48
6 Limitations
As mentioned earlier, the aim was to obtain 10 interviews but ultimately 5 were
possible. It took considerable time to find informants prepared to be speak on record
(a lot was said off the record but this cannot be included in the research). Predictably
the initial informants were from non-governmental settings. Representatives from the
government involved directly in the local leprosy eradication programme (District
Civil Surgeon, District Leprosy Officer and others) were identified, contacted and
they even discussed issues off the record. Eventually they agreed to be interviewed for
the project, but during fieldwork they were all transferred en-mass to another district
with other officials replacing them. Apparently it is the policy of the government to
transfer district leprosy teams within a year with practically no notice, to other
districts to curb corruption. This left insufficient time during the fieldwork in India to
contact new government interviewees. Ideally 10 interviews or more would have
greater validity and representativeness, although it should be noted that there was a
considerable degree of coherence of responses, suggesting it was unlikely that
additional interviews would have identified significantly different themes. .
The nature of the research question meant that a systematic literature review was not
possible in this instance. With greater time and resources, more grey literature could
have been obtained and more articles that provided possible alternative explanations
to the hypothesis unearthed.
This research merely scratches the surface of what is a complex and difficult question.
More detailed and extensive research is required to fully answer it. One possible line

LSHTM Candidate Number 470127 49
of analysis is co-relating the volume of the chemotherapy drugs (supplied for free
through WHO by the Nippon Foundation) consumed over a period of time to
prevalence within a particular region or country, to possibly give a better idea of
prevalence than official prevalence data itself.

LSHTM Candidate Number 470127 50
7 Conclusions & Recommendations
7.1 Conclusions
Declaring a disease eliminated from a country has very serious implications. Despite
more than 20 years of MDT, leprosy has not been eradicated. Leprosy patients are
highly infectious and M.Leprae can remain viable outside the human host for many
months. The mean incubation period of lepromatous disease is 10 years. These factors
make it difficult to completely eradicate the disease21 and there is no evidence that the
global initiative has lead to the disappearance of infection or disease from any
population2. Perhaps we are failing to understand some important aspect of the
disease’s natural history2.
With elimination declared, resources are becoming scarce for the continued efforts
necessary to keep this enigmatic disease at bay. Integration has resulted in the loss of
skilled and experienced leprosy workers and the lack of training to general health staff
has further compounded the situation. Cessation of active case detection will continue
to contribute to a rise in hidden cases. In the absence of effective IEC, campaigning
and public awareness initiatives, voluntary reporting will not be effective in new case
detection.
Social stigma in relation to leprosy is ingrained in society. Fear of social ostracism
and discrimination discourage patients from accessing services or even being
diagnosed. Socio-economic rehabilitation of leprosy cases is greatly hampered by this.
LSHTM Candidate Number 470127 51
Ignoring the reality of the problem will not make it go away. Declarations of
elimination on paper do not magically rid a country of a disease. Much to the
contrary, it is possible the leprosy will re-emerge as a major health issue unless it is
addressed according to the ground realities.
7.2 Recommendations
Reinstating active case detection
While it is an expensive proposition to re-implement active detection all over India,
this should be done in regions that continue to demonstrate high prevalence of
leprosy. Jharkhand is a case in point where the prevalence is above the national
average with 12 districts having prevalences between 1 & 2 and 2 districts having
prevalences between 2 and 5, yet there is no active case detection. Hidden cases that
are missed because of voluntary reporting will eventually resurface at later more
complicated stages, having transmitted the infection to many others by then. A cost-
effectiveness analysis of re-implementing active case detection would undoubtedly
reveal that the costs of managing such cases later far exceed any cost considerations
of re-implementing active case detection now.
Surveillance
Surveillance must be undertaken in an integrated setting using clinically relevant
indicators. The number of new cases will drop as a result of integration and it is
critical to establish whether patients with leprosy are being missed by the surveillance
system47. These areas should use active case finding.

LSHTM Candidate Number 470127 52
Effective IEC, campaigning and public awareness initiatives
Effective awareness campaigns will uncover more hidden cases, dispel many myths
and misconceptions and also help to counter the stigma attached with leprosy. It will
help SER programmes and sign-post local services to leprosy patients. The frequency,
duration and coverage of campaigns need to be improved. Tying in leprosy awareness
campaigns with the total literacy mission is an effective way forward.
Training general health staff
Since the programme is integrated into general health services, continued training and
refresher training need to be made mandatory for all medical staff. Such workshops
must include modules on attitudes and values and challenging stigma.
Parallel vertical programmes
It is clear from the evidence of this report, that the leprosy programme is not fully
integrated into general health services in many areas. The advantages of integrated
services have been nullified by lack of staff at PHC’s and not enough health centres.
E.g. in Bihar there is 1 health centre for every 200,000 population, in contrast with
South India, where there is 1 for every 30,000 population38,55. In such regions,
maintaining specialist leprosy initiatives in partnership with local NGO’s till such a
time that capacity issues of general health services are resolved would best serve the
interests of those afflicted with this disease.

LSHTM Candidate Number 470127 53
Incentivising case detection at peripheral health worker level
Innovative schemes to motivate peripheral health workers to find leprosy cases should
be piloted in high prevalence districts/ blocks. If this is found effective then it should
be extended to other high prevalence districts/ blocks.
Confirming cure by skin smears
HIV/AIDS and poor quality control on slit-skin smears not withstanding, it is
essential particularly in multibacillary cases to confirm cure by bacteriological load as
opposed to RFT after MDT course completion. Ideally this should apply to diagnosis
as well, but it is better to overdiagnose leprosy than to release from treatment leprosy
patients that are still infectious and liable to relapse. Poor quality control of smears is
addressed through better training, providing standardised equipment and standardised
procedure protocols.
Moving away from elimination rhetoric
The national leprosy eradication programme must recognise the limitations of an
elimination (& prevalence)-centric focus, particularly since there is no evidence to
support the WHO elimination hypothesis65. The elimination concept has run its course
and served its purpose. The programme must focus on new case detection rates,
disability rates, proportion of new cases that are children and proportion of MB cases
instead, as these provide are more accurate assessment of active disease transmission.
More emphasis should be placed on the socio-economic rehabilitation of leprosy
cases.

LSHTM Candidate Number 470127 54
Appendix 1: Anonymised copy of final revised protocol
LONDON SCHOOL OF HYGIENE & TROPICAL MEDICINE MSc Public Health Project Protocol 2006-2007 CANDIDATE NAME: XXXXXXX MSc Public Health Stream name………MSc. Public Health General If you are a Half-time student please indicate whether this is your 1st or 2nd year of study
PROJECT TYPE: (please indicate which type of project you intend to undertake, i.e. Health Policy Report or Literature Review or Research Project)
Health Policy Report TITLE OF PROJECT: How could changes of case definitions, ascertainment procedures, and diagnostic and registration conventions have impacted on reductions in the prevalence of leprosy in India, reported over the last decade (taking the state of Jharkhand as a case study)? BACKGROUND: (i.e. why this topic is of interest/relevance. If your project involves work with a specific organisation, please give details) In 1991 the World Health Assembly (WHA) passed a resolution to “eliminate leprosy as a public health problem” by the year 2000, elimination defined in this context as a reduction in prevalence to below 1 per 10,000 population. India achieved elimination in December 2005; according to the National Leprosy Eradication Programme data (‘Current Leprosy Situation in India as on March 2006’, National Leprosy Eradication Programme). This was achieved following a dramatic fall in prevalence, particularly between the years 2000-2005. Although some states like Jharkhand, as per Government of India figures continue to have prevalence above 1 per 10,000 such drastic reductions have left many in the scientific and NGO community sceptical about what has actually happened (‘Leprosy: what is being “eliminated”?’ Professor Paul Fine; WHO International Bulletin, Volume 85/1/06-039206; Professor Paul Fine & Dr. Diana Lockwood, personal communication). One theory is that changes to the diagnostic, surveillance and reporting procedures are creating ‘data artefacts’ that are obscuring the true picture of leprosy prevalence and control in India. This research is aimed at gaining insight into the co-relationship between this steep

LSHTM Candidate Number 470127 55
fall in prevalence and changes to the diagnostic, surveillance and reporting procedures being followed, looking at the Indian state of Jharkhand as a case study. AIMS: Make recommendations to the Government of India, based on the findings about the role played by changes to definitions, ascertainment procedures, and diagnostic and registration conventions in the reported reduction in prevalence of leprosy in India over the last decade. Recommendations will address issues related to the assessment of leprosy prevalence. OBJECTIVES: • To gain understanding about the change in leprosy prevalence in India over the
past decade. • To understand how the diagnostic and reporting system actually works in practise,
in India, informed by the interviews to be conducted in India. • To explore changes in diagnosis, reporting and surveillance systems in India over
the same period. • Draw conclusions about the possible relationship between changes of case
definitions, ascertainment procedures, and diagnostic and registration conventions (etc) and the dramatic reported reductions in leprosy rates.
METHODOLOGY: (please note that methods of literature review should be detailed and specific)
Phase 1: Reviewing the literature Initially the research will take the form of reviewing the literature available to shed light on the reasons for the drastic changes in prevalence rates reported in India over the past decade. The review will seek to inform the research about the various factors purported to contribute to the elimination of leprosy in India, and whether similar trends and factors have contributed to reductions in other countries. Further, the review will provide insight into role played by changes to definitions, ascertainment procedures, and diagnostic and registration conventions in the reported reduction in prevalence of leprosy in India over the last decade The search strategy for this review will be to break down the research question into concepts and frame search items. This will be followed by bibliographical database searches for each of the search items and subsequent combined searches. The search items for this review could be: ‘case definitions’, ‘surveillance OR case finding’, ‘diagnosis OR case confirmation’, ‘case registration OR reporting’, ‘prevalence’, ‘leprosy OR Hansen’s Disease’, ‘India OR Jharkhand’, ‘reduction OR elimination OR control’, ‘reasons’, ‘policy changes’ etc, and search combinations thereof. Grey literature searches will involve free text terms and concepts. The databases that will be searched include Cochrane Library, WHO weekly Epidemiological Record, Pub Med, Medline, EMBASE, CAB Direct, IBSS, SIGLE, TRIP database, Development databases etc. Grey literature from the Government of India as well as NGO’s working in India will be included in the review. Grey literature will be sought through internet search engines as well as specific NGO websites (Leprosy Mission, Lepra, Damien Foundation, Nippon Foundation, ILEP etc.), Government of India NLEP website, CAB Direct, IBSS, SIGLE, Google search engine etc. Data will also be directly sought from agencies working in India.

LSHTM Candidate Number 470127 56
Literature will also be searched directly from the LSHTM library and other medical libraries. Articles will be selected from the search results and other sources, based on the formulated eligibility criteria, such as year of publication, geographical location, language(s) and specific subject material. After quality assessment, data extraction and synthesis will be undertaken followed by report writing and recommendations. The objectives of the study may not be answerable through a single line of questioning. It may well be necessary to pursue multiple lines of enquiry, each tailored to meet the specific requirements of the objective they are linked to (i.e. case definitions & diagnostic conventions, registration and reporting procedures, ascertainment procedures, leprosy prevalence etc.), as any single search may not provide a clear picture or adequate data. The data thus gathered will be collated to provide an overall view of what is actually going on. Phase 2: Qualitative Research Through semi-structured interviews of key people in the field of leprosy internationally as well as locally on the ground in Jharkhand, further clarity will be sought as to the real picture of what is happening in India. Eminent public health professionals who are observing and commenting on the changing face of leprosy in India will be interviewed. Workers in local NGO’s in Jharkhand will also be interviewed to find out what the local procedures are in terms of diagnosis, surveillance and reporting of cases and whether, if at all, such procedures have changed in the past decade and how. All semi-structured interviews will be preceded by securing informed written consent. The qualitative data thus obtained will be transcribed, coded, analysed and correlated to the findings from the reviewing of literature and some understanding will be gained to answer the research question. ETHICAL CONSIDERATIONS: (Will you need ethical approval and research governance approval. If so, what have you done about this? Who will you approach, and when? By when do you expect approval and what are your alternatives if approval is not obtained in time?) Written, informed consent is to be obtained from all persons being interviewed. Local ethics approval is not required and informed consent should suffice. The literature review itself does not require ethical approval. FEASIBILITY ISSUES: (What could cause this project to fail? What plans do you have in case it fails? If you are to use existing data how will you obtain this data?) Access to people for interviewing, particularly in Jharkhand may become an issue, particularly considering the nature of the research question which can appear to be critical of the Government Leprosy Programme. However some amount of interviewing will be feasible particularly in relation to the key public health specialists as well as some key workers in Jharkhand. Contact has already been established with two local NGO’s running leprosy programmes in Jharkhand, to potentially conduct semi-structured interviews, observe & document first-hand how the grass-roots activities are being conducted. In the unlikely worst-case scenario of not being able to secure any relevant interviews, the literature review component itself should provide useful and sufficient

LSHTM Candidate Number 470127 57
insights to answer the research question. The literature review itself is likely to require considerable grey literature for greater depth of understanding and insight into the research question. REFERENCES: ‘Leprosy: what is being “eliminated”?’ Professor Paul Fine; WHO International Bulletin, Volume 85/1/06-039206 ‘Leprosy Elimination- A virtual phenomenon or a reality?’ Diana N J Lockwood; BMJ, 2002 June 22; 324(7352): 1516-1518. Professor Paul Fine & Dr. Diana Lockwood (personal communication). ‘Current Leprosy Situation in India as on March 2006’, NLEP current statistics report online. NLEP (National Leprosy Eradication Programme) Government of India website. WHO international and SEARO (South East Asian Regional Office) websites.

LSHTM Candidate Number 470127 58
Appendix 2: Anonymised copy of risk assessment form
TAUGHT COURSE STUDENT PROJECT RISK ASSESSMENT FORM 1. This summary and assessment must address all planned aspects of the student project. 2. The student, in conjunction with the project supervisor, must complete both pages of the assessment. 3. Sufficient detail should be provided so that the location of the project is clear. i.e. Give more detail than just
“London” in answer as to where the project is to be carried out. 4. Projects involving biological, chemical and radiological hazards must be referred to the Departmental Safety
Supervisor. 5. Itineraries and contact details for projects involving work overseas must be lodged with the Teaching Office before
the work starts. 6. This summary must be completed and all signatures obtained before work is started. 7. A copy of the completed form must be held by the Course Organiser, and retained for two years.
Full Name of Student XXXXXXXX
Course MSc. Public Health
Project Supervisor xxxxxx
Project Title
How could changes of case definitions, ascertainment procedures, and diagnostic and registration conventions have impacted on reductions in the prevalence of leprosy in India, reported over the last decade (taking the state of Jharkhand as a case study)?
Summary of project aims
Make recommendations to the Government of India addressing issues related to the assessment of leprosy prevalence in that country.
Where will the project be carried out?
London UK & the Indian state of Jharkhand
Will the project involve work overseas? If yes, where?
India, Jharkhand State
Will the project involve significant work away from LSHTM sites? If yes, where?
Yes, interviews with key informants in India and London, at the offices of NGO’s, Universities and Government Departments.
Does the project involve work with pathogenic organisms / human blood / radiochemicals?
No
If the Project involves work overseas:
Will the project be based in an established field station / research institute? If yes, where?
No. The overseas work will be based from Jharkhand and will involve interviewing key workers engaged in leprosy control work locally, at the offices of the NGO’s as well as on field trips in and around Jharkhand.
Is ethical approval required for the project? If yes, has it been granted?
Ethics approval sought from LSHTM. Locally, written informed consent of the persons interviewed.
What supervision arrangements are proposed while away from LSHTM?
Contact will be maintained by e-mail and when possible telephonically, with LSHTM project supervisor xxxx.
Give the contact details for the off-site supervisor where applicable
Not applicable.
Will the project involve lone / isolated work? If yes, state how you can contacted while working.
Project will involve accompanying workers on their field visits and one to one interviews either in those settings or at the project office. Contact will be maintained through mobile phone (local number will be intimated to LSHTM supervisor), telephone and email.
Has appropriate travel insurance been arranged?
I have ongoing travel insurance whenever I travel abroad.
If the Project involves significant work within the U.K., away from the LSHTM sites in London:
Will the project be based in an established college / hospital etc? If yes, where?
LSHTM Candidate Number 470127 59
Is ethical approval required for the project? If yes, has it been granted?
Will the project involve home / personal visits?
Will the project involve lone / isolated work?
What supervision / contact arrangements are proposed while away from LSHTM?
If Project Involves work with Pathogenic Organisms, Human Blood or Radiochemicals: (form to be signed by Departmental Safety Supervisor *)
Organism/s to be used
Potential Routes of Infection
Radiochemical/s to be used
Laboratories where work with pathogens / radioisotopes will be carried out
Disinfectants/Disposal
Health Surveillance required
Additional Information:
Are there any special needs, disability-related issues or other concerns that may need to be taken into account?
Do these need to be considered in planning arrangements?
Do these need to considered in relation to the location of the project?
Do they impact on supervision arrangements?
Do arrangements for access to specialist medical treatment need to be considered?
Student Signature
………………………………………………….. I agree to comply with the relevant safety requirements
Date
Supervisor Signature
………………………………………………….. I agree that is a reasonable summary of the project
Date
M.Sc. Course Organiser Signature ………………………………………………….. I agree that this project may proceed
Date
Departmental Safety Supervisor (only required if project involves work with pathogens or radiochemicals)
………………………………………………….. I agree that this project may proceed
Date
The table below must be completed for all potentially hazardous activities likely to be carried out during the
project, especially those identified above. Please refer to the Guidance Notes and School safety documentation for further information.
Project Title
Procedure Precautions

LSHTM Candidate Number 470127 60
(continue on additional sheets if required)

LSHTM Candidate Number 470127 61
Appendix 3: Anonymised copy of LSHTM ethics approval letter
London School of Hygiene & Tropical Medicine
Ethics application form : MSc research project (MSC1)
Section 2 : If your project is completely new or is collecting any new data from a previous study:
For use of Research Ethics Committee No ……………………………………… Date Rec’d ………………………………. Approved by …………………………. Date ……………………………………….
Overall assessment of quality of ethical application Excellent Good Satisfactory
(Approved without (Approved with (Approved after discussions) amendments) minor amendments)
Comment by Ethics Committee ………………………………………………………………..
1. Project Title
How could changes of case definitions, ascertainment procedures, and diagnostic
and registration conventions have impacted on reductions in the prevalence of leprosy in India, reported over the last decade (taking the state of Jharkhand as a case study)?
2. Give an outline of the proposed project. Sufficient detail must be given to allow the Committee to make an informed decision without reference to other documents.
(Expand box to answer)
(max 300 words) In 1991 the World Health Assembly (WHA) passed a resolution to “eliminate leprosy as a public health problem” by the year 2000, elimination defined in this context as a reduction in prevalence to below 1 per 10,000 population. India achieved elimination in December 2005 following a dramatic fall in prevalence, particularly between the years 2000-2005. Although some states like Jharkhand, as per Government of India figures continue to have prevalence above 1 per 10,000 such drastic reductions have left many in the scientific and NGO community sceptical about what has actually happened (‘Leprosy: what is being “eliminated”?’ Professor Paul Fine; WHO International Bulletin, Volume 85/1/06-039206; Professor Paul Fine & Dr. Diana Lockwood, personal communication). One theory is that changes to the diagnostic, surveillance and reporting procedures are creating ‘data artefacts’ that are obscuring the true picture of leprosy prevalence and control in India. This project is a health policy report aimed at gaining insight into the co-relationship between the steep fall of leprosy prevalence reported in India and changes to the

LSHTM Candidate Number 470127 62
diagnostic, surveillance and reporting procedures being followed, looking at the Indian state of Jharkhand as a case study. It will be in two phases, the first a review of published and unpublished literature to gain understanding on the issues related to assessment of prevalence. The findings of this review will inform the second phase of the project which is semi-structured oral interviews of key elimination programme functionaries involved in the delivery of leprosy control services in the Indian state of Jharkhand. This phase is aimed at understanding how the diagnostic and reporting system actually works in practise, in India. The findings from both the phases will be collated into the final report for the project.
3. Is project a randomised trial?
NO
4. Will any biological samples be collected and if so specify which
NO 5. Specify the number (with scientific justification for sample size), age, gender, source and
method of recruiting subjects for the study.
The researcher will endeavour to interview at least 10 individuals, through semi-structured interviews after securing informed and written consent. The number is based on an estimation of what is realistically possible, the nature of the interviews being qualitative. The intention is to interview: 1. A minimum of 6 professionals in the field of leprosy elimination locally in Jharkhand
from NGO & Government settings (General Health Services or specialized leprosy services), directly involved in diagnosis and case finding. They may be doctors, trained leprosy workers or programme managers
2. A minimum of 2 district level co-ordinators in Jharkhand from either or both NGO and governmental settings
3. 1 national level key informant 4. 1 international level key informant Informants in (1) will provide information related to actual activities in the field in relation to leprosy programmes. Interviewing functionaries in the NGO and Government sectors will provide a balanced perspective and may even provide some contrasting views and feedback. In (2) the district level co-ordinators will provide information from a more distal and overall perspective and about state level interventions. The international and national informants will be able to comment on a national and global strategic level as well as broader scientific, epidemiological and political perspectives. Recruitment: The researcher has established contact and co-operation from a regional level co-ordinator of leprosy elimination activities in Jharkhand as well as the lead of a key local general health provider in the region. This will enable the researcher to visit some of the leprosy centres or services and interview professionals in categories (1) & (2). The international level key informant has already been contacted and will be interviewed locally in London after categories (1), (2) & (3) informants have been interviewed. The feedback from these completed interviews will inform that interview. The national level informant is likely to be from WHO in Delhi, but will be interviewed telephonically.

LSHTM Candidate Number 470127 63
6. State the likely duration of the project, and where it will be undertaken.
The researcher is a half-time student, willing to commit time to the research which will be conducted over the span of the master’s course at LSHTM. Phase one research (Literature review) will be done in London, phase two in the Indian state of Jharkhand, through semi-structured interviews to be conducted in December ’07- January ‘08.
7. State the potential distress, discomfort or hazards, and their likelihood, that research subjects may be exposed to (these may include physical, biological and/or psychological hazards). What precautions are being taken to control and modify these hazards?
Not applicable
8. Specify how confidentiality will be maintained. When small numbers are involved, indicate how possible identification of individuals will be avoided. See Guidance notes at http://intra.lshtm.ac.uk/reference/ethicsstuds.html
The confidentiality of those interviewed will be safeguarded in the following ways: • aiming to interview ten key informants with similar job roles, so that there are enough
interviews to prevent the singling out of individuals • describing the findings without using any specific names or references in any part of the
report, that can help identify the key informant in the report • giving each participant the option in the consent form of not being quoted at all,
anonymously or otherwise, or included in any of the analyses • Use of written consent forms • Semi-structured interviews will be digitally recorded but no names will recorded,
anonymity will be preserved by assigning codes to each interview instead
9. State the manner in which consent will be obtained and supply copies of the information sheet and consent form. ◊ Written consent is normally required. Where not possible, explain why and confirm
that a record of those giving verbal consent will be kept. ◊ Where appropriate, please state if and how the information and consent form will be
translated into local language(s). See Guidance notes at http://intra.lshtm.ac.uk/reference/ethicsstuds.html
The participants will be verbally explained the nature of the research. The information sheet will be read out in English/ Hindi/ Bengali (depending on the preference of the interviewee) and informed written consent will obtained. The sample information sheets and consent form follow this form. NB. All languages are spoken fluently by the interviewer.
10. Local Ethical Approval. Give details of local approval to be obtained prior to the commencement of fieldwork. (If you cannot identify an Ethical Committee or if the study has been approved by several different organisations, eg. NGOs give this information and show that as much as possible has been done to obtain approval.)
Local ethical approval not required as interviewing staff about health care systems.
LSHTM Candidate Number 470127 64
Participant Information Sheet _____________________________________________________________________________________________
Study Title: How could changes of case definitions, ascertainment procedures, and diagnostic and registration conventions have impacted on reductions in the prevalence of leprosy in India, reported over the last decade (taking the state of Jharkhand as a case study)? Principle investigator XXXX _____________________________________________________________________________________________ Dear Participant You are being invited to take part in a research study. Before you decide to participate, it is important that you understand why the research is being done and what it will involve. Please take time to read the following information carefully and discuss it with others if you wish. If there is anything that is not clear or you would like to know more about, please ask the researcher [XXXX] in person. It is important that you think about whether you wish to take part so please take time to decide. Thank you for reading this. What is the purpose of the study? This research project is being carried out at the London School of Hygiene and Tropical Medicine as part fulfilment of a Masters degree in Public Health by XXXX. In 1991 the World Health Assembly (WHA) passed a resolution to “eliminate leprosy as a public health problem” by the year 2000, elimination defined in this context as reduction in prevalence to below 1 per 10,000 population. India achieved elimination in December 2005 following a dramatic fall in prevalence, particularly between the years 2000-2005, although some states like Jharkhand, as per Government of India figures continue to have prevalence above 1 per 10,000. This research is aimed at gaining insight into the co-relationship between the fall in prevalence and changes to the diagnostic, surveillance and reporting procedures being followed, looking at the Indian state of Jharkhand as a case study. What is the overall objective of the study, its importance and the reason why the subject’s cooperation is requested? The main objectives of this research project are: • To gain understanding about the change in leprosy prevalence in India over the
past decade. • To understand how the diagnostic and reporting system actually works in practise,
in India, informed by the interviews to be conducted in India. • To explore changes in diagnosis, reporting and surveillance systems in India over
the same period. In order to understand the current diagnostic, reporting and surveillance systems for leprosy in India, it is necessary to interview health providers engaged in leprosy control fieldwork. The reason your cooperation is requested is because you are involved in such delivery and can provide important information that will help this researcher to understand such systems better. Do I have to take part? It is up to you whether or not to take part in this research. If you decide to take part you will be given this information sheet to keep and be asked to sign a consent form.

LSHTM Candidate Number 470127 65
Even when you decide to take part, you are still free to withdraw at any time and without giving any reasons. What will happen to me if I take part? If you agree to take part, you will be asked questions related to the topics mentioned above. Questions will be asked in a private area, possibly your office. The interview will be recorded digitally, and notes of the discussion will be taken. If you do not feel comfortable to be recorded, the recorder will not be used. No names will be recorded and all files will be kept anonymously to ensure confidentiality. The interview will take about 30 to 45 minutes, depending on the amount of information you wish to share and the time you have at your disposal. Only this researcher will look at your answers given during the interview. You will NOT be asked to include your name; instead an identification code will be assigned to each interview ensuring that you remain ANONYMOUS. This means that no-one will know that you as an individual have participated in the research and given information. Because your name will not be written with your answers, no one will know what you said. No quotes or other results arising from your participation in this study will be included in any reports, even anonymously, without your agreement. Are there any reasons you should not participate? You should not participate if you do not want your views to be part of the analysis in the research study. What are the possible risks or discomforts? This researcher does not foresee the likelihood of any possible risks or discomforts as the questions are related to procedures and systems used in the field for leprosy cases. Will my taking part in this study be kept confidential? All information collected during the course of the research will be kept strictly CONFIDENTIAL and secured against unauthorised access. What will happen to the results of the research study? At the end of the study the findings will be written up into a policy report which will be submitted to the London School of Hygiene and Tropical Medicine. The report will be available in their library for 5 years. NO identifying information about you will be included in the report or any papers emanating from the research. Will you be paid for participating? You will not receive payment for participating in this research study. Contact for further information If you have any questions regarding this study please speak directly to XXXX. If you have questions after the interview is over, please contact him by phone or via email. Ethical Committees which have approved the study London School of Hygiene and Tropical Medicine Ethical Committee. _____________________________________________________________________________________________ Thank you for taking the time to read this information!

LSHTM Candidate Number 470127 66
Participant Consent Form _____________________________________________________________________________________________ Date: / /2007/08 Interview Identification Number: Study Title: How could changes of case definitions, ascertainment procedures, and diagnostic and registration conventions have impacted on reductions in the prevalence of leprosy in India, reported over the last decade (taking the state of Jharkhand as a case study)? Principle investigator XXXXX
Declaration (Please Tick appropriate boxes)
I confirm that I have read and understood the information sheet for the above study and have had the opportunity to ask questions.
I understand what is required of me and what will happen if I take part in the
study.
My questions concerning this study have been answered by the researcher.
I understand that my participation is voluntary and that I am free to withdraw at any time, without giving a reason.
I do / do not agree to quotes or other results arising from my participation in the
study being included, even anonymously in any reports about the study.
I agree for comments I give to be used in the written report of the above study.
I agree to take part in the above study. Subject's Agreement By signing your name on this sheet of paper, it means that you agree to voluntarily take part in this study. _______________________________________________________ ______________________________ Signature of Research Subject Date _______________________________________________________ Printed Name of Research Subject _______________________________________________________ _______________________________ Signature of Person Obtaining Consent Date _______________________________________________________ Printed Name of Person Obtaining Consent

LSHTM Candidate Number 470127 67
Appendix 4: Literature Review Search Strategy
Literature Review Search Strategy
# 1. TUBERCULOID LEPROSY/ or LEPROSY CONTROL/ or LEPROSY EPIDEMIOLOGY/ or
LEPROSY/ or LEPROSY VACCINE/ or LEPROMATOUS LEPROSY/ or
MULTIBACILLARY LEPROSY/ or BORDERLINE LEPROSY/ or PAUCIBACILLARY
LEPROSY/
# 2. leprosy.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]
# 3. Hansen's disease.mp. [mp=title, abstract, subject headings, heading word, drug trade name,
original title, device manufacturer, drug manufacturer name]
# 4. 1 or 2 or 3
# 5. case defin$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original
title, device manufacturer, drug manufacturer name]
# 6. exp Disease Classification/
# 7. Infection/ or Diagnostic Accuracy/ or Nerve Injury/ or Skin Disease/ or Leprosy/ or
Multibacillary Leprosy/ or Leprosy Control/
# 8. (case$ or case finding or case finding polic$).mp. [mp=title, abstract, subject headings, heading
word, drug trade name, original title, device manufacturer, drug manufacturer name]
# 9. (case diagnosis or diagnosis).mp. [mp=title, abstract, subject headings, heading word, drug
trade name, original title, device manufacturer, drug manufacturer name]
# 10. (leprosy case diagnosis or leprosy diagnosis).mp. [mp=title, abstract, subject headings, heading
word, drug trade name, original title, device manufacturer, drug manufacturer name]
# 11. (leprosy case$ or leprosy case finding or leprosy case finding polic$).mp. [mp=title, abstract,
subject headings, heading word, drug trade name, original title, device manufacturer, drug
manufacturer name]
# 12. (new case$ or new case$ defin$ or new case$ diagnos$).mp. [mp=title, abstract, subject
headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer
name]

LSHTM Candidate Number 470127 68
# 13. (leprosy new case$ or leprosy new case$ defin$ or leprosy new case$ diagnos$).mp. [mp=title,
abstract, subject headings, heading word, drug trade name, original title, device manufacturer,
drug manufacturer name]
# 14. 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13
# 15. (registration$ or registration convention$ or registration protocol$ or registration
procedure$).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original
title, device manufacturer, drug manufacturer name]
# 16. India/ or Leprosy Control/ or Leprosy/ or Health Program/ or Prevalence/ or Mycobacterium
Leprae/
# 17. leprosy prevalence.mp. [mp=title, abstract, subject headings, heading word, drug trade name,
original title, device manufacturer, drug manufacturer name]
# 18. exp PREVALENCE/
# 19. prevalenc$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original
title, device manufacturer, drug manufacturer name]
# 20. 16 or 17 or 18 or 19
# 21. 16 and 17 and 18 and 19
# 22. leprosy incidence$.mp. [mp=title, abstract, subject headings, heading word, drug trade name,
original title, device manufacturer, drug manufacturer name]
# 23. Mycobacterium Leprae/ or Leprosy/ or Incidence/
# 24. incidence$.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original
title, device manufacturer, drug manufacturer name]
# 25. exp INCIDENCE/
# 26. 22 or 23 or 24 or 25
# 27. 22 and 23 and 24 and 25
# 28. India.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]
# 29. Jharkhand.mp. [mp=title, abstract, subject headings, heading word, drug trade name, original
title, device manufacturer, drug manufacturer name]
# 30. 4 and 14 and 28
# 31. 4 and 15 and 28

LSHTM Candidate Number 470127 69
# 32. 30 and 31
# 33. 4 and 20 and 28
# 34. 4 and 26 and 28
# 35. 33 and 34
# 36. limit 30 to (human and english language and yr="1997 - 2007")
# 37. limit 31 to (human and english language and yr="1997 - 2007")
# 38. limit 32 to (human and english language and yr="1997 - 2007")
# 39. limit 33 to (human and english language and yr="1997 - 2007")
# 40. limit 34 to (human and english language and yr="1997 - 2007")
# 41. limit 35 to (human and english language and yr="1997 - 2007")
# 42. 7 or 10 or 11 or 13
# 43. 5 or 6 or 8 or 9 or 12
# 44. 4 and 28 and 42
# 45. limit 44 to (human and english language and yr="1997 - 2007")
# 46. limit 44 to (human and english language and yr="2002 - 2007")
# 47. 4 and 21 and 28
# 48. 4 and 27 and 28
# 49. from 45 keep 1,8,11-12,18,21,30-31,36-45,53,58-59,62,68,71,75,80,87,89,95,99-100,106-
107,109,112,120,132-133,142,148,152,165,168-169,172-173,180,188,198-199,225-
226,275,278,281,289,316-317,320,323,326
# 50. from 45 keep 323,326
# 51. from 45 keep 323,326
# 52. from 45 keep 9-10

LSHTM Candidate Number 470127 70
Appendix 5: Semi-structured Topic Guide
Interview topic guide for leprosy services in Jharkhand, India ______________________________________________________________ Semi-structured interview schedule for those involved in the delivery &/or management of regional leprosy elimination programmes and services. Aims of interviews: • To understand how the diagnostic and reporting system actually works in practice in India • To explore changes in diagnosis, reporting and surveillance systems in India All interviews are confidential, anonymous & will be recorded digitally unless the interviewee requests otherwise. Bulleted points following some questions are the prompts. ______________________________________________________________ 1. Introduction by interviewer and assigning anonymous identifier for
the interview 2. Introductory background questions
2.1. Could you tell me a little about yourself and your role in the service? • What is your title and your role here? • Could you describe your background (doctor &/or project manager/ other)? • Who do you work with? 2.2. How long have you been working in this setting and in the field of leprosy in general?
3. Leprosy case detection
3.1. Can you describe to me how cases are detected here? • Through active/ passive/ voluntary detection?
3.2. Can you tell me the way cases were detected in the past? For example before 2004?
Before 2000?
4. Leprosy case diagnosis
4.1. Can you tell me how new cases are diagnosed? • Is it by lesion count/ slit skin smear? • Definition of a new case? • Who does the diagnosis? 4.2. Can you describe how case diagnosis was done in the past? • For example before 2004? Before 2000? • In some countries, skin smear was used including India in the past. 4.3. What do you do to confirm the diagnosis?
LSHTM Candidate Number 470127 71
• If diagnosis is through skin lesion count alone, then are any smears done for doubtful cases of cases of indeterminate leprosy?
5. Case registration
5.1. Which cases are registered on records? • Do single lesion cases get registered? • What types of cases are included: new case/relapsed cases/ deformities/ reactions? • What is the actual process? 5.2. How long do they remain on the register? • Is a case that has received the full course of MDT considered cured and taken off the
register? 5.3. Can you tell me how case registration was done in the past? • How long were cases kept on the register in the past? • Were single lesion cases registered in the past? If so how long ago? 5.4. Can cases be re-registered? 5.5. Can you describe how this may happen?
6. Types of leprosy cases
6.1. Can you describe the range of types of leprosy cases you get here? • Are there more PB or MB cases seen at your centre? 6.2. What types of deformities do you see in patients? How common is it to see patients
with deformities/ disabilities? 6.3. Do you see children with leprosy? • Generally what type of leprosy? • Is there a family history of leprosy?
7. Treatment
7.1. Can you tell me how many months therapy you give to Paucibacillary and Multibacillary cases?
• Are single lesion PB cases given single dose ROM therapy? • Duration of treatment of PB cases? • Duration for MB cases 12 months or 24 months? 7.2. How long was the treatment duration in the past? • For example before 2004 &/or 2000? 7.3. For a diagnosed case of leprosy, is the treatment supervised MDT or accompanied? • Clarify what is meant by accompanied MDT. 7.4. When is a case no longer a case (cured)? 7.5. In the past, when was a case no longer a case?
8. Data recording & reporting
8.1. Can you tell me how you estimate and report prevalence data? Which cases are included in the prevalence?

LSHTM Candidate Number 470127 72
• What happens to cases treated in the early part of the year, are they included in the prevalence data for the year?
8.2. What sort of targets does the Government set locally? • Does the Government give you targets annually/ half-yearly/ quarterly or none at all? 8.3. What happens if you exceed the target or do not reach it? • If you find more cases than your target numbers, are these excess cases registered? • Is diagnostic accuracy considered in cases of under/ over achieving targets? 8.4. How do you feel about the targets? Do you feel they are usually realistic or do you
feel pressured to achieve them? • Pressure from whom?
8.5. Can you tell me who sets you the guidelines for the different aspects of the leprosy
programme? (Central/ State/ District/ Local) 8.6. How is the data from your centre collected and reported to the Government? Who do
you report to? • Is it sent out annually/ 6 monthly/ quarterly? • Actual process?
9. Quality of services (Diagnostic accuracy, validation, training, referrals)
9.1. What are the IEC activities conducted from your centre? • Frequency? • How is it done and who does it? 9.2. What is the next point of referral for your centre? 9.3. How is the referral done? 9.4. What happens to patients when they are referred? • What sort of health service is the next referral point? • What are the facilities and common reasons for referrals? • Actual processes? 9.5. What training/ refresher courses are offered to you/ your staff? • Who comes to do it? • What is the training for? • Duration and frequency? • Who receives the training? • Is it sufficient? 9.6. Have any validation tests been carried out at your centre? • To check whether the diagnosis is correct or not? 9.7. What measures are in place to ensure the quality of diagnosis? 9.8. Can you tell me of any past/present instances of over-diagnosis?
10. Opinions and views
10.1. Do you feel there is a real decrease in the number of leprosy cases in your area? 10.2. Do you feel that leprosy is no longer a public health issue in India?

LSHTM Candidate Number 470127 73
10.3. The leprosy control/elimination programme in India was a so-called ‘vertical’ programme in the past. Over the last five years or so, this approach has been replaced by a more integrated approach into general health services. Could you comment on what you feel the benefits and the drawbacks of either approach have been?
10.4. In your opinion have the current guidelines and practices for leprosy elimination
resulted in better case detection, diagnosis and treatment of leprosy? Is there anything more that could be done locally &/or at state level &/or nationally
11. Is there anything else you would like to add or comment upon?
LSHTM Candidate Number 470127 74
Appendix 6: Coding Scheme for interview analysis
Categories
1. Leprosy Elimination Programme 1.1. Village level 1.2. Block Level 1.3. District level 1.4. State level 1.5. National level 1.6. Roles & responsibilities
(Workers/NGO's/Govt.) 1.7. Referrals 1.8. Guidelines & policies 1.9. Targets 1.10. Funding 1.11. Campaigns 2. Leprosy case detection 2.1. Current 2.2. Past 2.3. Changes 3. Leprosy case diagnosis 3.1. Provisional 3.2. Clinical 3.3 Past 3.4. Changes in diagnostic conventions 3.5. Over-diagnosis 4. Case verification 4.1. Case confirmation/ validation 4.2. Quality assurance 5. Case registration 5.1. Registration procedure 5.2. Removal from the register 5.3. Re-registration
6. Range/ types of leprosy cases 6.1. PB/ MB/ single lesion 6.2. Children 6.3. Deformities and complications 7. Case treatment 7.1. Single lesion 7.2. Duration 7.3. Current 7.4. Past 7.5. Changes 7.6. Administration 7.7. Cured cases/ treatment completion 8. Prevalence data 8.1. Calculation 8.2. Reporting 8.3. Changes 8.4. Figures 9. Opinions 9.1. On case reductions 9.2. Leprosy as a public health issue 9.3. Vertical VS. Integrated 9.4. Improvements 9.5. Limitations/ shortcomings 9.6. Challenges 10. Values and attitudes 10.1. Stigma 10.2. Discrimination 10.3. Judgemental 10.4. Status & power (increased/
decreased/ changes) 10.5. Defensiveness 10.6. Resentment 10.7. Hostility 10.8. Guardedness

LSHTM Candidate Number 470127 75
References 1 WHO (1991). The “Final Push” strategy for elimination.
www.who.int/lep/strategy/wha/en/index.html 2 Fine PEM. Leprosy: what is being “eliminated”? WHO International Bulletin. 2006:
Volume 85/1/06-039206 3 Professor Paul Fine & Dr. Diana Lockwood, personal communication 4 Lockwood DNJ. Leprosy Elimination- A virtual phenomenon or a reality? British
Medical Journal. 2002: 324(7352): 1516-1518 5 International Leprosy Congress, Madrid. International Journal of Leprosy. 1953:
21:504. 6 Ridley DS, Jopling WH. International Journal of Leprosy.1966:34:255 7 Chacko CJG. A Manual of Leprosy, Thangaraj RH (ed).1980: The Leprosy Mission,
New Delhi 8 Harrison’s Principles of Internal Medicine. 16th Ed. 2005: 970-971. 9 WHO (1982). Expert Committee on leprosy. Technical Report. Series: 675. 10 WHO (2001). Weekly Epidemiological Record. No.20:18 May 2001. 11 Online NLEP Website. Current Leprosy Situation in India as on March 2008.
National Leprosy Eradication Programme. 12 Online NLEP Website. Data as on March 2008. National Leprosy Eradication
Programme 13 WHO (2000). Weekly Epidemiological Record. No.28:14 July 2000. 14 Online Govt. of Jharkhand website. Profile of Jharkhand. 2008. 15 Park, K. Park’s Textbook of Preventive & Social Medicine. 19th Ed. 2007: 350-351. 16 Fine PEM. Global leprosy statistics: a cause for pride, or frustration? Leprosy
Review. 2006: 77: 295–297. 17 Ganapati M. Doctors accuse India of massaging leprosy figures. British Medical
Journal. 2005: 330 (7500): 1104 18 Bernard Naafs. Treatment of leprosy: science or politics? Tropical Medicine and
International Health. 2006: 11 (3): 268 – 278

LSHTM Candidate Number 470127 76
19 WHO (1988). Expert Committee on leprosy. Technical Report. Series: 768. 20 Fine PEM, Warndorff DK. Leprosy by the year 2000- what is being eliminated?
Leprosy Review. 1997: 68: 201-202 21 Walker SL, Lockwood DNJ. Leprosy. Clinic in Dermatology. 2007: 25: 165-172. 22 Vettom L, Pritze S. Rehability of skin smear results: Experience with quality
control of skin smears in different routine services in leprosy control programmes. Leprosy Review. 1989: 60: 187-96
23 De Rijk AJ, Nilson T, Chonde M. Quality control of skin smear services in leprosy
programmes: Preliminary experience with inter-observer comparison in routine services. Leprosy Review. 1985: 56: 177-99
24 WHO (1995). A guide to eliminating leprosy as a public health problem.
WHO/LEP/95.1. 1st Ed. WHO, Geneva. 25 Becx-Bleumink M. Allocation of patients to paucibacillary or multibacillary
regimens for the treatment of leprosy- A comparison of methods based on skin smears as opposed to clinical methods- Alternative clinical methods for classification of patients. International Journal of Leprosy. 1991: 59:292-303
26 Van Brakel WH, de Soldenhoff R, McDougall AC. The allocation of leprosy
patients into paucibacillary and multibacillary groups for multidrug therapy, taking into account the number of body areas affected by skin or skin and nerve lesions. Leprosy Review. 1992: 63: 231-46.
27 WHO (1998). Expert Committee on leprosy. Technical Report. Series: 874. 28 Sehgal VN. Leprosy. Clinic in Dermatology. 1994: 12: 624-44. 29 Sehgal VN. Clinical Leprosy, 3rd Ed. New Delhi: Jay Pee Brothers, 1993. 30 Noordeen SK. Epidemiology of polyneuritic type of leprosy. Leprosy Review.
1972: 44: 90-6. 31 Bhattacharya SN, Sehgal VN. Leprosy in India. Clinic in Dermatology. 1999: 17:
159-170. 32 Uplekar MW, Anita NH. Clinical and histopathological observations on pure
neuritic leprosy. Indian Journal of Leprosy. 1986: 58: 513-1. 33 Talwar S, Jha PK, Tiwari VD. Neuritic leprosy: Epidemiology and therapeutic
responsiveness. Leprosy Review. 1992: 63: 263-8. 34 Mahajan PM, JogaikarDG, Mehta JM. A study of pure neuritic leprosy: Clinical
experiences. Indian Journal of Leprosy. 1996: 68: 137-41.

LSHTM Candidate Number 470127 77
35 Girdhar BK. Neuritic Leprosy. Indian Journal of Leprosy. 1996: 68: 35-42. 36 International Leprosy Association . Report on the International Leprosy Association
Technical Forum.: diagnosis and classification of leprosy. Leprosy Review. 2002: 73 Suppl: S24
37 WHO (2002b) Report on the third meeting of the WHO technical advisory group
on elimination of leprosy. (WHO/CDS/CPE/CEE/2002.29) WHO, Geneva. 38 Lockwood DNJ, Suneetha S. Leprosy: Too complex a disease for a simple
elimination paradigm. Bulletin of the World Health Organisation: 2005. 83: 230-235.
39 Waters M. F. Is it safe to shorten multidrug therapy of lepromatous (LL & BL)
leprosy to 12 months? Leprosy Review. 1998: 69: 110 – 111. 40 Naafs B. Viewpoint: leprosy after the year 2000. Tropical Medicine and
International Health. 2000: 5: 400-4003. 41 Kumar B, Dogra S & Kaur I. Epidemiological characteristics of leprosy reaction:
15 years of experience from north India. International Journal of Leprosy. 2004: 72: 125-133.
42 WHO (2002). The final push to eliminate leprosy as a public health problem:
questions and answers. Geneva: WHO, 2002. 43 Directorate General Health Services. Modified guidelines on MDT regimen to be
followed under NLEP. L. 19025/6/97, Government of India, New Delhi, 1997. 44 Gupte MD, Pannikar V, Manickam P. Leprosy Case Detection in India. Health
Administrator. 2006: XVIII (2): 28-36. 45 Narasimha Rao P, Lakshmi TSS. ‘Final push of leprosy’ in India: What is being
pushed? Indian Journal Dermatology Venereology and Leprology. 2005: 71: 226-9. 46 WHO (2005). National Programme Managers for Leprosy Elimination Report of
an Intercountry Meeting Kathmandu, Nepal, 6-8 January 2005.WHO Project: SEA-LEP-161: ICP CPC 600, New Delhi. www.searo.who.int/LinkFiles/Reports_Inter__mtgNepal.pdf
47 Krishnamurthy P. Hidden leprosy- who is hiding what from whom? Leprosy
Review. 2004: 75: 303 – 305. 48 Sample Survey in Dharmapuri District (1995), and Kanpur Nagar (1996). Damien
Foundation India Trust, India. Unpublished document.

LSHTM Candidate Number 470127 78
49 Murthy BN, Subbian M, Bhoopathi K, et al. Lot quality assurance sampling for
monitoring leprosy elimination in an endemic district in Tamil Nadu. Indian Journal of Leprosy. 2001: 73: 111-119.
50 Evaluation of fifth MLEC in eight states in India, 2004. International Federation of
Antileprosy Associations (ILEP). Unpublished document. 51 Rao CK. Leprosy elimination in India – So near. Guest Editorial. Indian Journal of
Leprosy. 2005: 77: 207 – 211. 52 Sundar Rao PSS. Impact Of Mdt On Leprosy Disease Transmission – Present
Status & Issues. Health Administrator. 2006 : XVIII (2) : 40-44. 53 National Institute of Epidemiology (NIE). Report of Independent Evaluation of
NLEP, India. Chennai: NIE, 2000. 54 Visschedijk J, van den Broek J, Eggens H, Level P, van Beers S and Klatser P.
Mycobacterium leprae – Millennium resistant! Leprosy on the control threshold of a new era. Tropical Medicine and International Health. 2000: 5:388-399.
55 Krishnamurty P. Update. Damien Foundation Newsletter January 2004. 56. Krishna Murthy P. Case-detection and diagnosis. Indian Journal of Leprosy. 2004:
76 (2): 153 – 156. 57 Mittal BN. The National Leprosy Eradication Programme in India. World Health
Statistics Quarterly. 1991: 44: 23-29. 58 Mittal BN. National strategy for elimination of leprosy in India. Indian Journal of
Leprosy. 1992: 64: 513-520. 59 Padma T. V. With scores still infected, India declares leprosy ‘eliminated’. Nature
Medicine. 2006: 12 (4): 372. 60 Editorial. The debate over leprosy elimination versus sustainability of leprosy
services. Indian Journal of Leprosy. 2005: 77(4): 299-304. 61 WHO (2004). Leprosy Elimination Project: status report 2002-2003. Geneva:
WHO: 2004. 62 Morgan LM (2001). Community participation in health: perpetual allure, persistent
challenge. Health Policy and Planning. 2001: 16:1020. 63 Sommerfelt H, Irgens L M and Christian M. Geographical Variations in the
occurrence of Leprosy possible roles played by Nutrition and some other environmental factors. International Journal of Leprosy. 1985: 53: 524-532.

LSHTM Candidate Number 470127 79
64 Lobo D, Narain JP. Progress in Leprosy Elimination in the South-East Asian
Region. Regional Health Forum. 2005: 9 (2): 21-27. 65 International Leprosy Association. Report of the International Leprosy Association
Technical Forum: epidemiology and control. Leprosy Review. 2002: 77: 1 – 8. 66 P. E. Fine. Leprosy: the epidemiology of a slow bacterium. Epidemiologic Reviews.
1982: 4: 161 – 188. 67 Kumar A, Girdhar A & Girdhar BK. Incidence of leprosy in Agra District. Leprosy
Review. 2007: 78: 131–136. 68 WHO (2002). Leprosy- global situation. Weekly Epidemiological Record. 2002: 77:
1-8. 69 Scollard DM. Leprosy Research declines. but most of the basic questions remain
unanswered. International Journal of Leprosy. 2005: 73: 25-7. 70 Gupte MD. Elimination of leprosy: forecasts and projections. Indian Journal of
Leprosy. 1994: 66:19-38. 71 Meima A, Gupte MD, van Oortmarssen GJ and Habbema JDF. Trends in leprosy
case detection rates. International Journal of Leprosy Other Mycobacterial Diseases.1997: 65:305-319.
72 WHO (2002). Leprosy Elimination Project. Status Report 2002. Geneva: WHO;
2002.


















