Logic, Argument and Medicine Sanjay Modgil Advanced Computation Lab Cancer Research UK Logic,...
29
Logic, Argument and Medicine Sanjay Modgil Advanced Computation Lab Cancer Research UK Logic, Argument and Medicine Medical Thinking, London, 22-23 June 20
-
Upload
julia-preston -
Category
Documents
-
view
214 -
download
1
Transcript of Logic, Argument and Medicine Sanjay Modgil Advanced Computation Lab Cancer Research UK Logic,...
Logic, Argument and Medicine
Sanjay Modgil
Advanced Computation Lab
Cancer Research UK
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006

Logic, Argument and Medicine
Logic based reasoning in Medical AI systems
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Logic and Argumentation
• Argumentation based reasoning: decision making, deliberation…
• Communication and Education
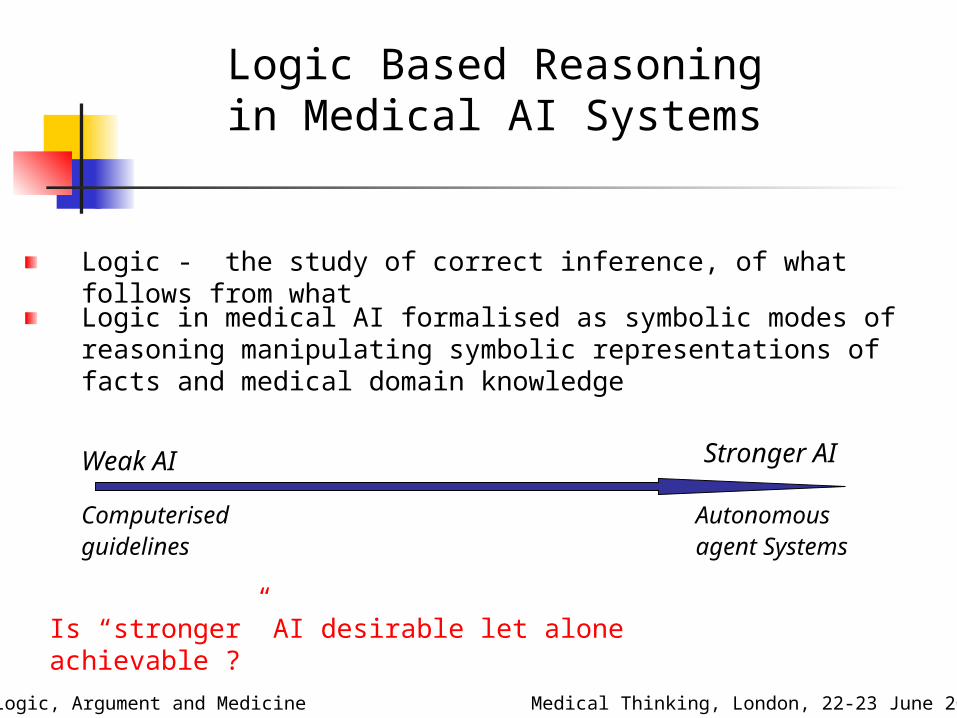
Logic Based Reasoning in Medical AI Systems
Logic - the study of correct inference, of what follows from what
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Logic in medical AI formalised as symbolic modes of reasoning manipulating symbolic representations of facts and medical domain knowledge
Weak AI Stronger AI
Computerised guidelines
Autonomous agent Systems
Is “stronger” AI desirable let alone achievable ?

Logic Based Reasoning in Medical AI Systems
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Symbolic logical representation of knowledge
- Facts (patient data)
- Rules (medical knowledge) +
Rules of Inference
e.g
Conclusions/Inference:
- the way the world is (beliefs)
- what one ought to do (actions)
Control
abductive/deductive
backward/forward

Inferring conclusions about the way the world is
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
disease(P,myo_infarct) symptom(P,short_breath) symptom(peter,
short_breath)
disease(peter, myo_infarct)

Inferring conclusions about the way the world is
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
disease(P,myo_infarct) symptom(P,abnorm_ecg) disease(peter,
myo_infarct)
symptom(peter, abnorm_ecg)
patient investigation
disease(peter, myo_infarct)

Inferring how one ought to act
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
b1,b2
b1,b2 b3
b3 b4
b1,b2,b3,b4… b1,b2,b3,b4, a e
(belief1,..beliefn, action effect , effect goal)
e g
e

Inferring how one ought to act (belief1,..beliefn, action effect
effect goal)
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
b1,b2
b1,b2 b3
b3 myo_infarct
myo_infarct
myo_infarct , aspirin reduced_platelet_adhesion
reduced_platelet_adhesion prevent_blood_clotting
myo_infarct , chlopidogrel reduced_platelet_adhesion
reduced_platelet_adhesion prevent_blood_clotting
gastritis , aspirin gi_bleed
gi_bleed
gastritis

Logic-based Reasoning in Medical Applications
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Expert and Decision Support Systems for :
• Diagnostic Assessment (e.g., MYCIN, EMYCIN)
• Risk Assessment (e.g., RAGS)
• Therapy Planning and Critiquing (ONCOCIN, CAPSULE, DAT)
• Decision Support embedded in computerised guidelines (e.g., ASBRU, PROforma based applications,…)
Current and Future Directions – Argumentation
and Medicine
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Argumentation theory, or argumentation, is the science of effective civil debate or dialogue
Potential advantages of argumentation in medical AI
• Argumentation based Decision Support
• Communication of information from healthcare workers to patients
• Medical Education
What is an Argument (1) ?
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
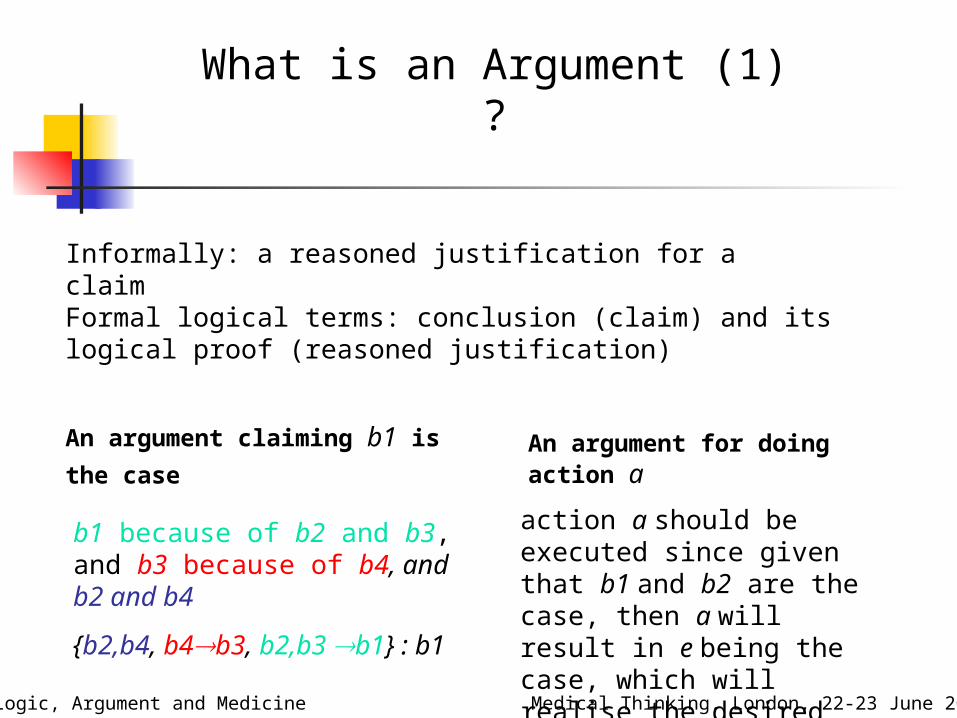
Informally: a reasoned justification for a claim
Formal logical terms: conclusion (claim) and its logical proof (reasoned justification)
An argument claiming b1 is
the case An argument for doing action a
b1 because of b2 and b3, and b3 because of b4, and b2 and b4
{b2,b4, b4b3, b2,b3 b1} : b1
action a should be executed since given that b1 and b2 are the case, then a will result in e being the case, which will realise the desired goal g

What is an Argument (2) ?
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Influential Toulmin argument schema:
Data Claim , Qualifier
Warrant
Backing
myo_infarct
aspirin , 0.7
myo_infarct , aspirin reduced_platelet_adhesion prevent_blood_clotting
Clinical trial A
Logical models of Argumentation (1)
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
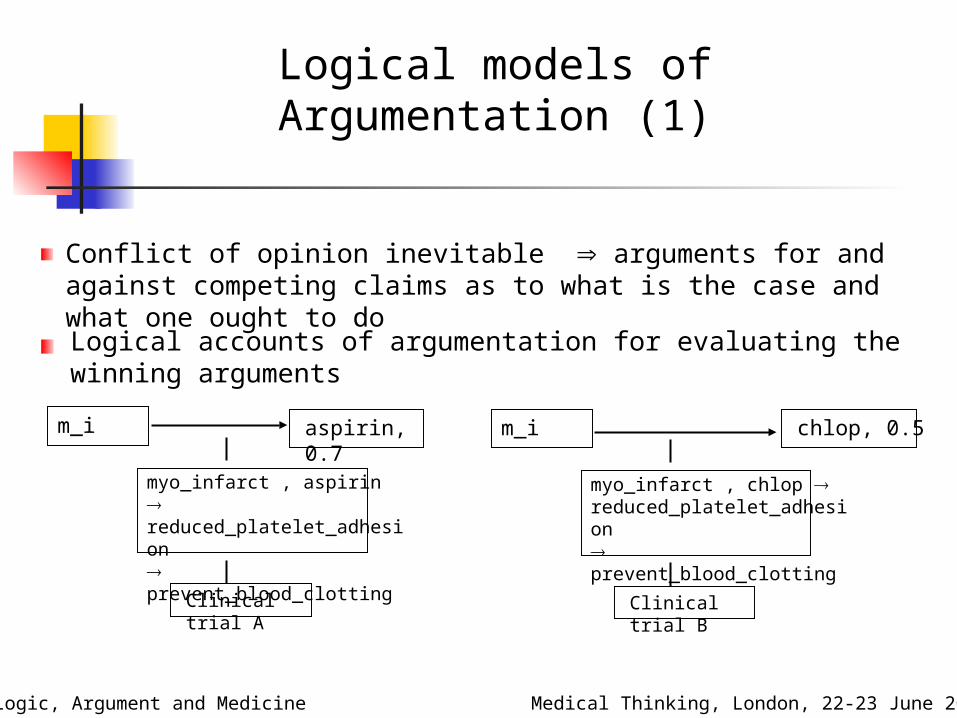
Conflict of opinion inevitable arguments for and against competing claims as to what is the case and what one ought to doLogical accounts of argumentation for evaluating the winning arguments
m_i aspirin, 0.7
myo_infarct , aspirin reduced_platelet_adhesion prevent_blood_clotting
Clinical trial A
m_i chlop, 0.5
myo_infarct , chlop reduced_platelet_adhesion prevent_blood_clotting
Clinical trial B
Logical models of Argumentation (2)
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
chlo asp
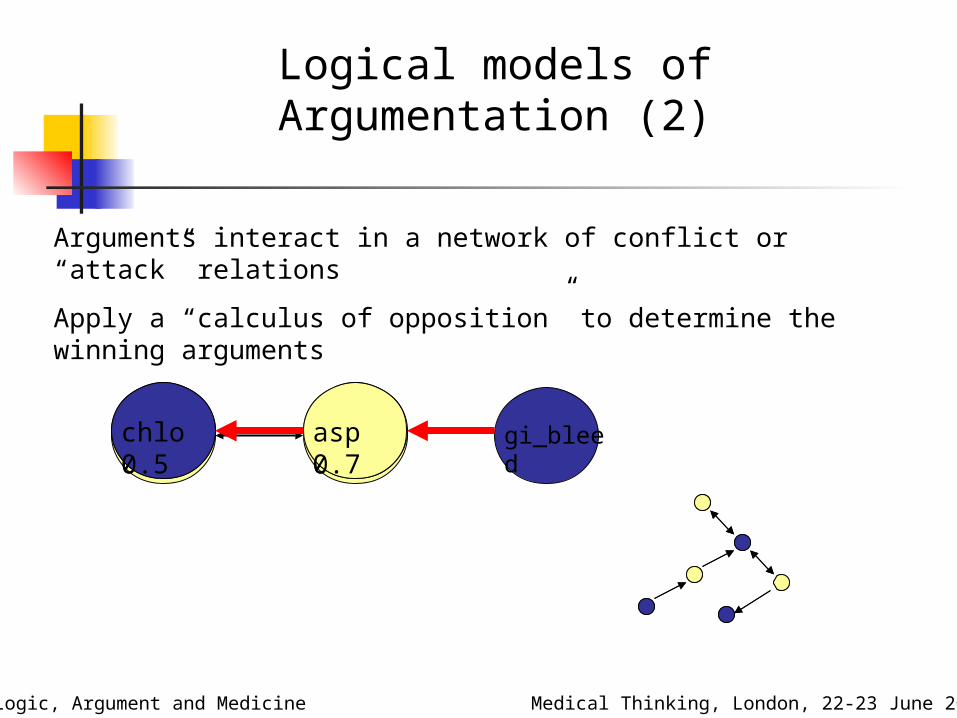
Arguments interact in a network of conflict or “attack” relations
Apply a “calculus of opposition” to determine the winning arguments
chlo 0.5
asp 0.7
gi_bleedchlo 0.5
asp 0.7
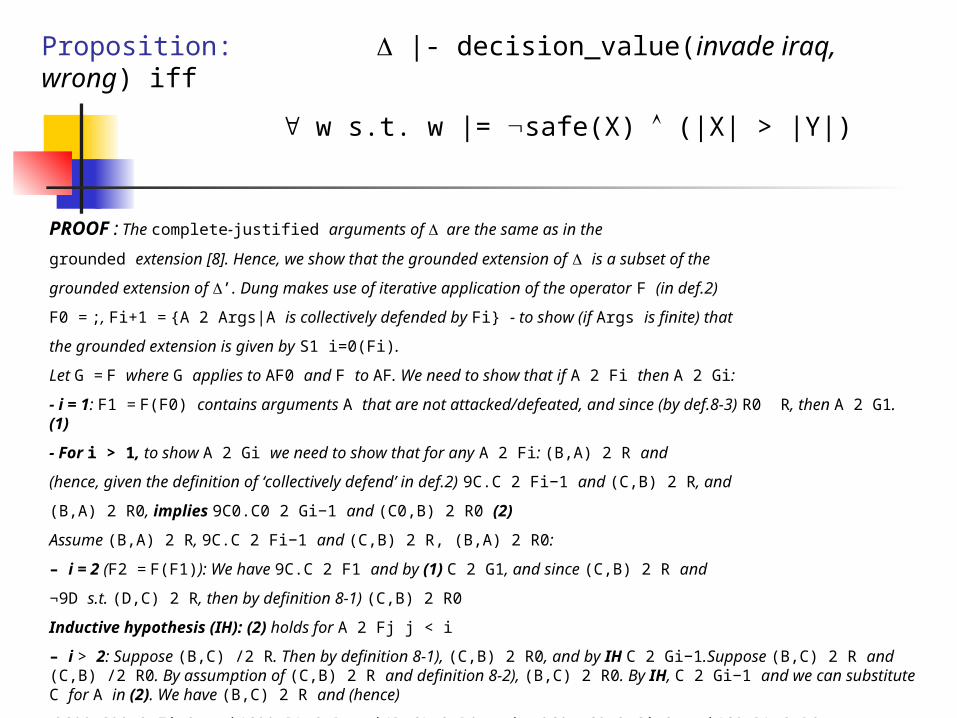
PROOF : The complete-justified arguments of are the same as in the
grounded extension [8]. Hence, we show that the grounded extension of is a subset of the
grounded extension of ’. Dung makes use of iterative application of the operator F (in def.2)
F0 = ;, Fi+1 = {A 2 Args|A is collectively defended by Fi} - to show (if Args is finite) that
the grounded extension is given by S1 i=0(Fi).
Let G = F where G applies to AF0 and F to AF. We need to show that if A 2 Fi then A 2 Gi:
- i = 1: F1 = F(F0) contains arguments A that are not attacked/defeated, and since (by def.8-3) R0 R, then A 2 G1. (1)
- For i > 1, to show A 2 Gi we need to show that for any A 2 Fi: (B,A) 2 R and
(hence, given the definition of ‘collectively defend’ in def.2) 9C.C 2 Fi−1 and (C,B) 2 R, and
(B,A) 2 R0, implies 9C0.C0 2 Gi−1 and (C0,B) 2 R0 (2)
Assume (B,A) 2 R, 9C.C 2 Fi−1 and (C,B) 2 R, (B,A) 2 R0:
– i = 2 (F2 = F(F1)): We have 9C.C 2 F1 and by (1) C 2 G1, and since (C,B) 2 R and
¬9D s.t. (D,C) 2 R, then by definition 8-1) (C,B) 2 R0
Inductive hypothesis (IH): (2) holds for A 2 Fj j < i
– i > 2: Suppose (B,C) /2 R. Then by definition 8-1), (C,B) 2 R0, and by IH C 2 Gi−1.Suppose (B,C) 2 R and (C,B) /2 R0. By assumption of (C,B) 2 R and definition 8-2), (B,C) 2 R0. By IH, C 2 Gi−1 and we can substitute C for A in (2). We have (B,C) 2 R and (hence)
9C00. C00 2 Fi−2 and (C00,B) 2 R, and (B,C) 2 R0 and so 9C0. C0 2 Gi−2 and (C0,B) 2 R0.
Proposition: |- decision_value(invade iraq, wrong) iff
w s.t. w |= safe(X) (|X| > |Y|)

Argumentation based Decision Support – Argument as
Explanation
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
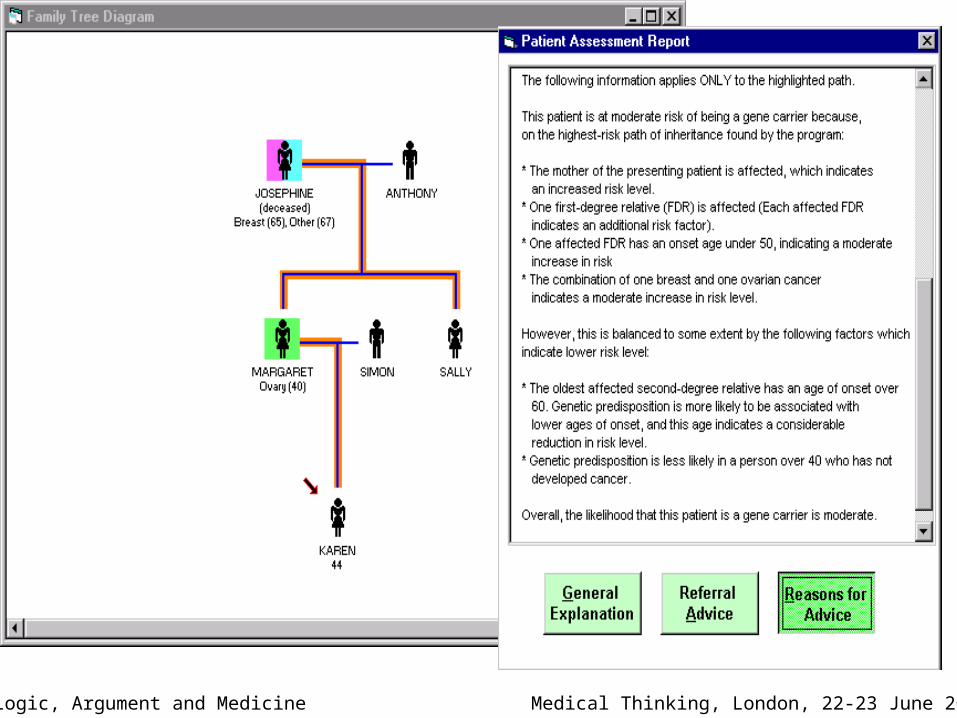
RAGs (Risk Assessment in Genetics)
For use by doctors advising people with a family history of cancer
Makes use of weighted rules to formulate arguments for and against a person belonging to given category of risk of being genetically predisposed to cancer
e.g., If person has 2 or more first-degree relatives diagnosed with breast cancer and both relatives were diagnosed under the age of 40 then this is an argument for person being at strong risk for genetic predisposition to the disease
Identical to classification by a statistical risk assessment packageStructuring and presentation of information as arguments represents clear and intuitive way of communicating information to patients
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Argumentation for Consumers of Healthcare
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
Enhancing the quality of doctor-patient communication by structuring and presentation of knowledge in the form of arguments and their conflict based interactions
(AAAI Spring Symposium, March 2006, Stanford)
Persuasive argumentation to change health-related behaviourPatient Tailored Explanation
Lay orientated explanation of conflicting views in the medical literature
Negotiation with Patients about treatment regimes

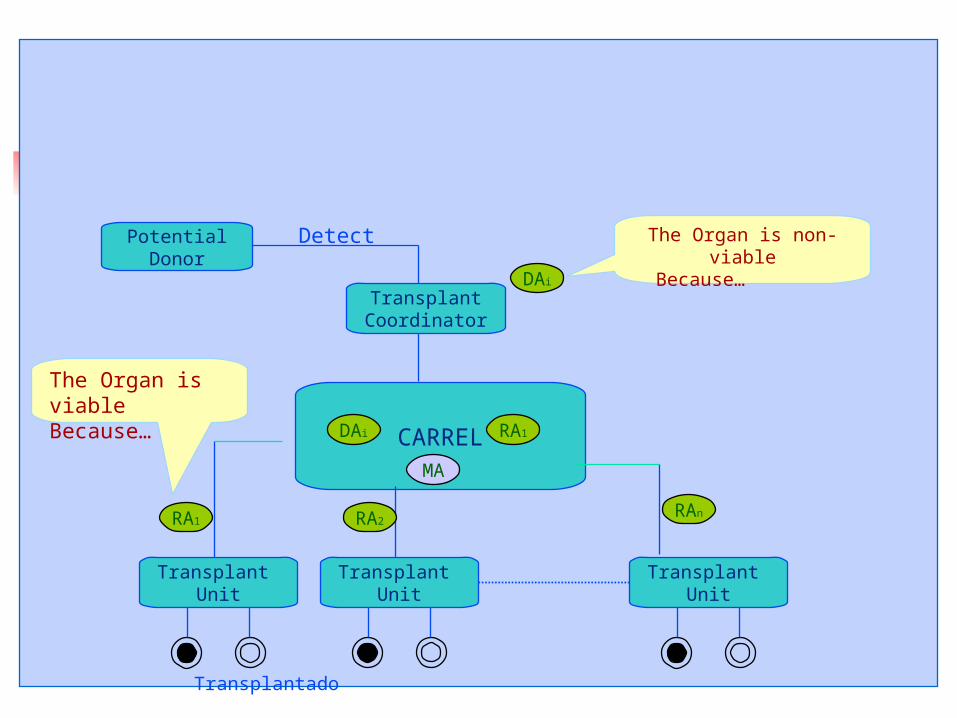
Argumentation based Collaborative Decision Making – the CARREL
project
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
CARREL framework developed at the University of Catalonia for managing the human organ and tissue transplant process
However, many organs potentially available for transplantation are discarded (not extracted)
In Catalonia (a world leader in transplantation) 15 % livers 20% kidneys 60% hearts 85% kidneys 95% pancreas are discarded

Argumentation based Collaborative Decision Making – the CARREL
projectPotentialDonor
Donor Agent
CARREL
Recipient Agent 3 Recipient Agent 1Recipient Agent 2
Viable /offer
Detect
Discard
No-viable

Argumentation based Collaborative Decision Making – the CARREL
project
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
*ASPIC (Argumentation Services with Integrated Components) - www.argumentation.org
Current assignment ignores possibility of difference of opinion, e.g.,
- history of smoking implies non-viable
- smoking history but no history of COPD implies viable
Hence CARREL is being extended to allow recipient agents and donor agents to argue over the viability of an organ
Winning argument for viability means that organ will be transplanted rather than discarded
Work being undertaken as part of the ASPIC* project
PotentialDonor
TransplantCoordinator
CARREL
Transplant Unit
Transplant Unit
Transplant Unit
Transplantado
Detect
DAi RA1
The Organ is viableBecause…
The Organ is non-viable Because…
DAi
RA1 RA2RAn
MA

Argumentation based Collaborative Decision Making – the CARREL
project
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
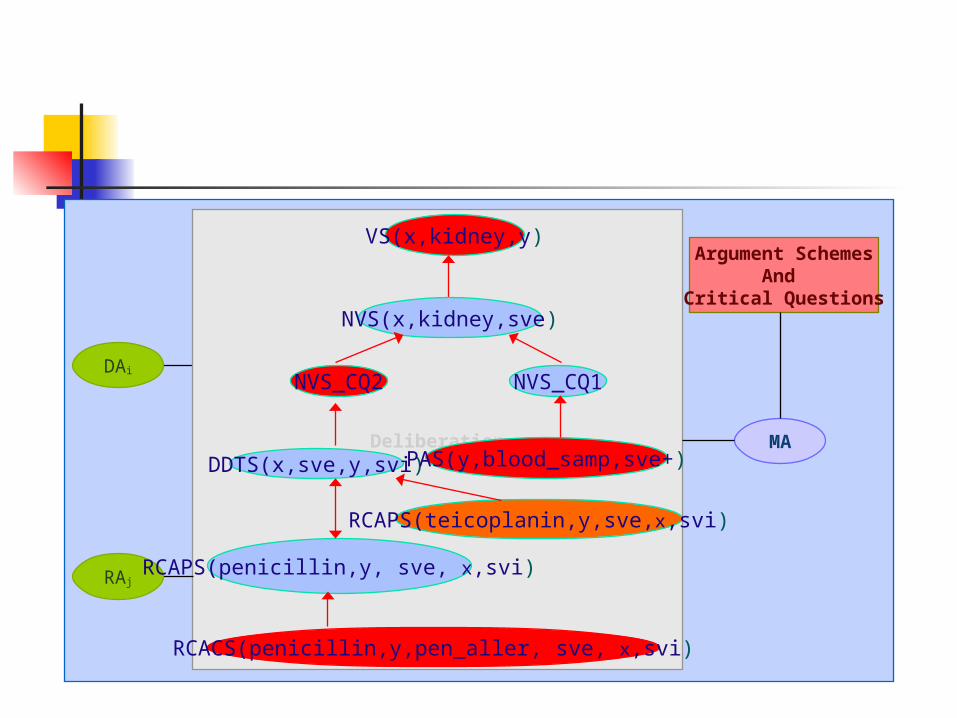
Mediator agent directs agents in dialogical exchange of arguments by referencing 40 + schemes and critical questions
Schemes and critical questions identify possible challenges andcounter-arguments at each stage in the dialogue
Schemes and critical questions are template representations of arguments and their interactions, for specialisation when arguing about a particular case

Argumentation based Collaborative Decision Making – the CARREL
project
Logic, Argument and Medicine
Non-Viability scheme:
Donor D of organ O had condition C which is a contraindication for donating O Therefore, organ O is non-viable.
Is it the case that condition C is a contraindication for donating O ?
Disease Transfer Contraindication Scheme: Transplanting O from D with condition C leads to recipient R having E, which is harmful Therefore C is a contraindication
Action Prevention scheme Action A on R prevents C leading to E in R, and A is intended
Non-Viability scheme:
Donor j of organ kidney had sve And sve is a contraindication for donating kidney Therefore, kidney is non-viable.
Is it the case that a history of sve is a contraindication for donating kidney?
Disease Transfer Contraindication Scheme: Transplanting kidney from j with condition sve leads to recipient m having svi, which is harmful Therefore sve is a contraindication Action Prevention scheme
action pencillin on m prevents sve leading to svi in m, and pencillin is intended

Argument SchemesAnd
Critical Questions
MADeliberation
DAi
RAj
VS(x,kidney,y)
DDTS(x,sve,y,svi)
RCAPS(penicillin,y, sve, x,svi)
NVS(x,kidney,sve)
NVS_CQ1NVS_CQ2
PAS(y,blood_samp,sve+)
RCAPS(teicoplanin,y,sve,x,svi)
RCACS(penicillin,y,pen_aller, sve, x,svi)
Argument SchemesAnd
Critical Questions
MADeliberation
DAi
RAj
VS(x,kidney,y)
DDTS(x,sve,y,svi)
RCAPS(penicillin,y, sve, x,svi)
NVS(x,kidney,sve)
NVS_CQ1NVS_CQ2
PAS(y,blood_samp,sve+)
RCAPS(teicoplanin,y,sve,x,svi)
RCACS(penicillin,y,pen_aller, sve, x,svi)

Benefits
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
• Reduce disparity between supply and demand
• Schemes and critical questions can be instantiated by:
- arguments in natural language by human physicians (weaker AI) –physicians thus directed to exploring all possible line of reasoning / argument in a rigorous manner that does not compromise patient safety
- arguments constructed in a logic programming language by computerised donor and recipient agents (stronger AI)
Benefits
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
• Educating medical professionals – evidence suggesting that the way physicians reason follows from the way they have been educated
- Difficult to teach decision analysis techniques
- Argumentation is a familiar way of reasoning
- Scheme and critical question approach encourages comprehensive and rigorous deliberation in a natural and intuitive way

Conclusions
Logic, Argument and Medicine Medical Thinking, London, 22-23 June 2006
• Review of uses of logic in medical reasoning about what to believe and how to act logic based models of argument
• Applications of argumentation theory in the medical domain:
- Decision making
- Communication of health information
- Education
• Argumentation theory gaining ground in the AI community – parallel development of memetics