
LOCAL ANESTHETICS PHARMACOLOGY II Dr/ Abdulaziz bin saeedan Pharmacy College Pharmacy College 1.
30
LOCAL ANESTHETICS LOCAL ANESTHETICS PHARMACOLOGY II PHARMACOLOGY II Dr/ Abdulaziz bin saeedan Dr/ Abdulaziz bin saeedan Pharmacy College Pharmacy College 1
-
Upload
leslie-hunter -
Category
Documents
-
view
224 -
download
0
Transcript of LOCAL ANESTHETICS PHARMACOLOGY II Dr/ Abdulaziz bin saeedan Pharmacy College Pharmacy College 1.

LOCAL ANESTHETICSLOCAL ANESTHETICS
PHARMACOLOGY IIPHARMACOLOGY II
Dr/ Abdulaziz bin saeedanDr/ Abdulaziz bin saeedan
Pharmacy CollegePharmacy College1

Local Anesthetics - HistoryLocal Anesthetics - HistoryLocal Anesthetics - HistoryLocal Anesthetics - History
18601860 - Niemann isolated the active principle “Cocaine”Cocaine” from coca leaves.
Cocaine = Natural product
2

Local Anesthetics- HistoryLocal Anesthetics- History
18841884 - Koller used Cocaine for topical anesthesia in eye surgery.
18851885 - Halsted used Cocaine for regional anesthesia in the oral cavity to remove a wisdom tooth without pain.
3

Local Anesthetics- HistoryLocal Anesthetics- History
1886-1886- Coca-Cola and many other products contain Cocaine.
18981898 - C - Cocaine used in spinal anesthesia.
A number of adverse effects were observed with the clinical use of Cocaine.
Thus, other local anesthetics had to be developed. 19051905 - Einhorn synthesized ProcaineProcaine.
Procaine is the 1st synthetic local anesthetic introduced.
Used for more than 40 years.
4

Local Anesthetics- HistoryLocal Anesthetics- History
19431943 - Löfgren synthesized LidocaineLidocaine.
Lidocaine was the first “ modern ” local anesthetic agent. 19481948 - Lidocaine was marketed and is up to now the most commonly used local anesthetic
in dentistry worldwide.
Other local anesthetics were introduced into clinical use:
Etidocaine , Mepivacaine , Prilocaine, Ropivacaine 19601960 - Muschaweck synthesized Articaine
Articaine is today the most commonly used local anesthetic.
5

What are local anesthetics?What are local anesthetics?
• Local anesthetics are drugs which produce reversible loss of reversible loss of sensationsensation in a localized arealocalized area of the body without the loss of without the loss of consciousnessconsciousness.
Characteristics of Local AnestheticsCharacteristics of Local Anesthetics
• Soluble in water and stable in solution.
• Non irritant.
• Rapid onset of action.
• Intermediate or long duration: enough to perform a surgery.
• Low degree of systemic toxicity.
6

Local anesthetics - MechanismLocal anesthetics - Mechanism
• The nerve membrane contain ion pumps, the most important is the Na/K pump.
• Na/K pump act by pumping 2 K+ intracellular for every 3 Na+ extracellular.
Depolarization
• Local anesthetics inhibits the transport of Na and K ions through the nerve membrane i.e reduce the rate of depolarization of the nerve membrane SO inhibit the transmission of the impulses through the nerve.
lead to loss of sensation.
NOTE:NOTE:
Because these agents prevent depolarization, they are called membrane stabilizing agentsmembrane stabilizing agents.
7

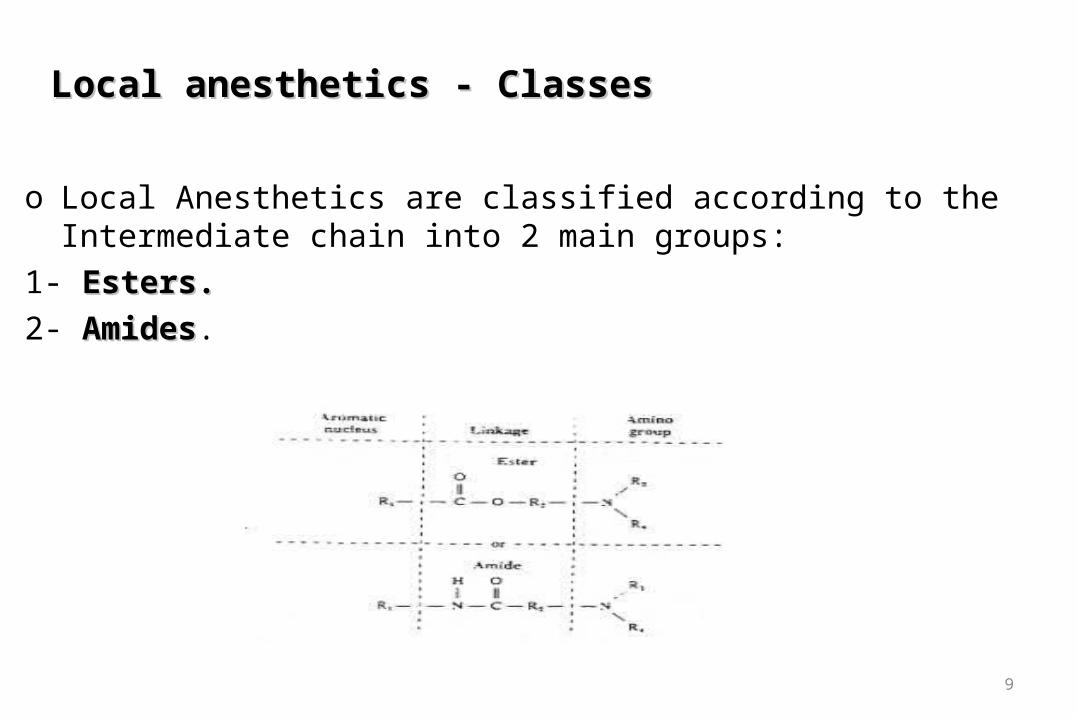
Local anesthetics - StructureLocal anesthetics - Structure
All local anesthetics have 3 main parts:
1- Aromatic group: 1- Aromatic group: It is the hydrophobic portion (Lipid-soluble) .
so the anesthetic molecule penetrate through the nerve membrane.
2- Amino group: 2- Amino group: It is the hydrophilic portion (water-soluble).
so the anesthetic molecule dissolve in water.
3- Intermediate chain (Linkage)3- Intermediate chain (Linkage): links between the Aromatic group and the Amino group.
8
Local anesthetics - ClassesLocal anesthetics - Classes
o Local Anesthetics are classified according to the Intermediate chain into 2 main groups:
1- Esters.Esters.
2- AmidesAmides.
9

Local anesthetics - ClassesLocal anesthetics - Classes
I- EstersI- Esters
• Cocaine
• Procaine (Novocaine)
• Tetracaine (Amethocaine)
II- Amides II- Amides
• Lidocaine (Xylocaine)
• Bupivacaine
• Prilocaine
• Articaine
10
NOTENOTE•All local anesthetic drugs are synthetic except cocaine.•Procaine is the 1st synthesized – the 1st injectable local anesthetic.
EstersEsters
• Relatively unstableunstable in solution (The ester linkage is more easily broken ).
• Rapidly metabolized Rapidly metabolized in plasma by cholinesterase enzymes.
The major metabolic product is para-amino benzoic acid (PABA).
• Allergic reactions to esters are usually due to PABA.
AmidesAmides
• Relatively stablestable in solution.
• Slowly metabolized Slowly metabolized by hepatic amidases.
• Allergic reactions to amides are very rare.
11
For these reasons amides are now more commonly used than esters. For these reasons amides are now more commonly used than esters.

Local anesthetics - FormulationLocal anesthetics - Formulation
Local anesthetics are presented as very dilute solutions which can be expressed as % OR g/100 mL solution
For example:For example: Lidocaine is available as 1% solution for injection. 1% solution = 1g of the drug dissolved in 100 mL. The number of mg/ml can easily be calculated by multiplying the value of % by 10.
ThereforeTherefore : 1% solution = 10 mg/mL 0.5 % solution = 5 mg/mL 0.25% solution = 2.5 mg/mL
12

Local anesthetics - VasoconstrictorsLocal anesthetics - Vasoconstrictors
Most local anesthetics produce some degree of vasodilation.
Leading to rapid absorption & Short duration. Consequently, vasoconstrictors are added to local anesthetics.
Epinephrine is the most commonly used vasoconstrictor.
It added to local anesthetic solutions in very dilute concentration, 5 ug/mL
Importance of Vasoconstrictors:Importance of Vasoconstrictors:
1- Decrease bleeding
2- Decrease the rate of absorption of the local anesthetic SO:
Localizing anesthesia
Decrease the risk of systemic toxicity of the local anesthetic.
Prolonging the duration of anesthesia.
13

Local anesthetics - VasoconstrictorsLocal anesthetics - Vasoconstrictors
Epinephrine containing solutions should never be used for infiltration around end-arteries i.e. fingers, ear lobes
severe vasoconstriction may lead to ischemia and necrosis.
What is the better combination (Lidocaine + Epinephrine) or (Lidocaine + What is the better combination (Lidocaine + Epinephrine) or (Lidocaine + Norepinephrine) and Why?Norepinephrine) and Why?
The vasoconstrictor effect of Norepinephrine is more potent than Epinephrine ….. But we prefere Epinephrine than Norepinephrine, because Norepinephrine will cause severe vasoconstriction which may lead to ischemia and necrosis.
14

Types of local anesthesiaTypes of local anesthesia
15
I. II. III.
Topical (Surface) anesthesia
Infiltration anesthesia
Regional anesthesia
1- Central techniques: 2- Peripheral techniques.
a- Spinal anesthesia
b- Epidural anesthesia
a- Nerve block anesthesia

I. Topical or surface anesthesiaI. Topical or surface anesthesia
Topical anesthesia is produced by direct application of a local anesthetic on the surface of skin.
Topical anesthetics are used in the form of gel, cream, ointment, spray.
Examples:Examples:
Lidocaine & Tetracaine.
Indications of topical anesthesia:Indications of topical anesthesia:
They are used to relieve pain and itching caused by conditions such as sunburns, minor burns, insect bites or scratches
16

II. Infiltration anesthesiaII. Infiltration anesthesia
Infiltration anesthesia is produced by SC injection of the anesthetic solution in the area of terminal nerve endings.
Infiltration affect the injected area only. Anesthetic action is rapid in onset.
Examples: Examples: Lidocaine, Prilocaine There is a sensation of pain immediately after SC injection of
local anesthetic solutions. This sensation is due to the acidic nature of these solutions. The addition of sodium bicarbonate to local anesthetic solutions
can reduce the pain sensation (due to neutralization).
Indications of infiltration anesthesia:Indications of infiltration anesthesia:1- Suturing 2- Wound irrigation 3- Foreign body removal
17

III. Regional anesthesiaIII. Regional anesthesia
Regional anesthesia is produced by injection of the anesthetic solution around nerve around nerve trunktrunk that supply specific area of the body such as a limb (arm or leg) or the lower half of the body.
Techniques of Regional Anesthesia can be divided into:
1- Central techniques:1- Central techniques:
a- Spinal anesthesia
b- Epidural anesthesia
2- Peripheral techniques. 2- Peripheral techniques.
a- Nerve block anesthesia
18
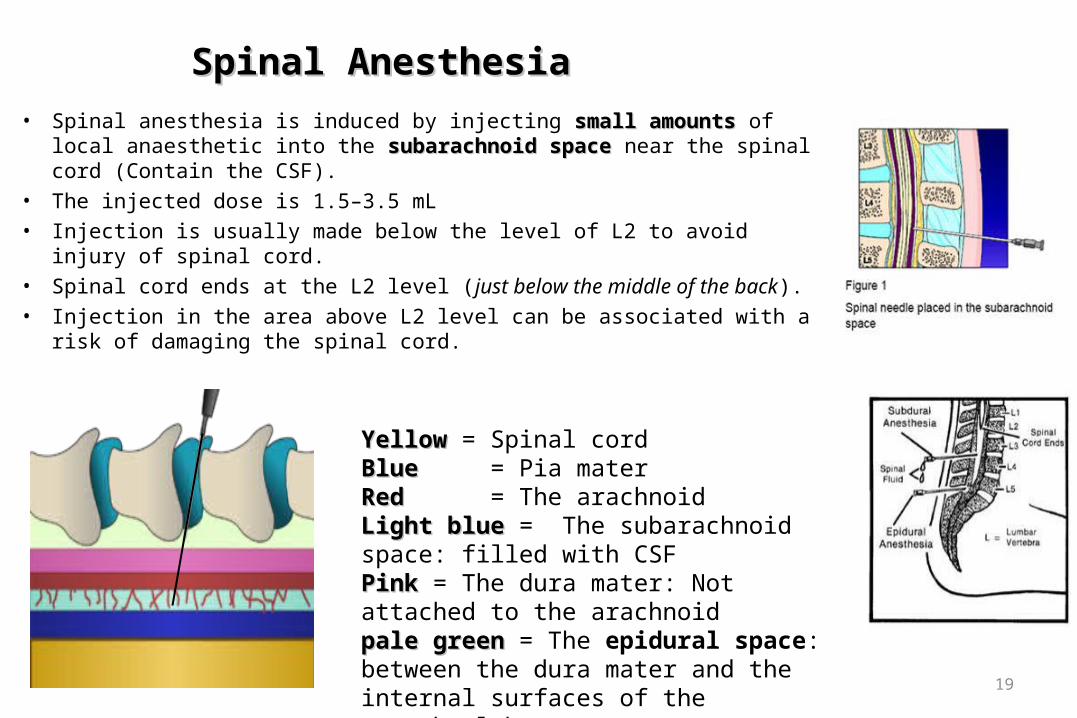
Spinal AnesthesiaSpinal Anesthesia
• Spinal anesthesia is induced by injecting small amountssmall amounts of local anaesthetic into the subarachnoid spacesubarachnoid space near the spinal cord (Contain the CSF).
• The injected dose is 1.5–3.5 mL
• Injection is usually made below the level of L2 to avoid injury of spinal cord.
• Spinal cord ends at the L2 level (just below the middle of the back).
• Injection in the area above L2 level can be associated with a risk of damaging the spinal cord.
19
YellowYellow = Spinal cordBlue Blue = Pia materRedRed = The arachnoid Light blueLight blue = The subarachnoid space: filled with CSFPinkPink = The dura mater: Not attached to the arachnoidpale greenpale green = The epidural space: between the dura mater and the internal surfaces of the vertebral bones.

Characters of Spinal Anesthesia:Characters of Spinal Anesthesia:
1- Anesthetic effect is:
Rapid in onset: 5 min.
Long in duration: 1 – 3 h.
2- Effective for any surgery occurring on the lower abdomen and legs (below the umbilicus).
Risks of Spinal Anesthesia:Risks of Spinal Anesthesia:
1- Effects on blood pressure and heart rate:
Hypotension (low blood pressure) and bradycardia (low heart rate).
2- Headache : Spinal headache.
3- Mild pain in the area of the back .
4- Infection.
5- Meningitis .
20

Indications of Spinal AnesthesiaIndications of Spinal Anesthesia
• Spinal anesthesia is best indicated for:
1- Older patients.
2- Operations in the lower abdomen and legs (below the umbilicus): For caesarean section. In obstetrics: it is ideal for manual removal of a retained placenta. Urological operations Genitalia operations Operations of the leg except amputation
Examples:
Lidocaine, Bupivacaine
21

Epidural AnesthesiaEpidural Anesthesia
Epidural anesthesia is induced by injecting local anesthetic into the epidural spaceepidural space.
Epidural anesthesia may be given at any level of spinal cord:
Cervical, Thoracic, or Lumbar sites.
The injected dose is 10–20 mL The onset of action: 15–30 min.
Examples:Examples:
Lidocaine, Bupivacaine
Indications of Epidural AnesthesiaIndications of Epidural Anesthesia
• Epidural anaesthesia is best indicated for operations on:
1- Thorax
2- Abdomen.
3- Lower limbs 22

Nerve Blocks AnesthesiaNerve Blocks Anesthesia
Nerve block anesthesia is induced by injecting local anesthetic around plexus (group of nerves) to anesthetize a larger area.
• The most common nerve blocks: o Maxillary nerve block (for upper jaw) o Brachial plexus block (for shoulder and upper arm).
23

Types of anestheticsTypes of anesthetics
The most commonly used anesthetics are: The most commonly used anesthetics are:
• Tetracaine (amethocaine-pontocaine)
• Lidocaine (Xylocaine)
• Prilocaine
• Bupivicaine
• Articaine
A combination of anesthetics may be used. Most agents come in 2 forms: with and without epinephrine .
24

Procaine (Novocaine)Procaine (Novocaine)
It is a local anesthetic drug belonging to the Ester group. The 1st synthesized – the 1st injectable local anesthetic. It has no topical anesthetic effect.
Procaine is a vasodilator .
Often coadministered with epinephrine to induce vasoconstriction
Vasoconstriction helps to reduce bleeding and prevents the drug from reaching systemic circulation in large amounts.
Metabolized in plasma (into PABA) and excreted by the kidney. Allergic reaction to procaine are not in response to procaine itself , but to PABA. Procaine is rarely used today:is rarely used today:
because more effective alternatives exist.
25

Tetracaine Tetracaine (Amethocaine - Pontocaine)(Amethocaine - Pontocaine)
is a potent local anesthetic belonging to the Ester group. More potent than procaine (10 times). More toxic than procaine (10 times).
It is mainly used topically. Metabolized in plasma (into PABA) and excreted by the kidney. Allergic reaction to procaine are not in response to procaine itself , but to PABA.
26

Lidocaine (Xylocaine)Lidocaine (Xylocaine)
The 1st Amide type of local anesthetics. It is a common local anesthetic drug. It has a rapid onset of action (2 min vs 6-10 min compare to procaine). It is the shortest acting of all local anesthetics.
because it has greater vasodilating properties. Metabolized in liver and excreted by kidney. Allergy to Amide is rarely to occur.
27

Prilocaine Prilocaine
It is a local anesthetic drug belonging to the Amide group.
Prilocaine is available:
Without vasoconstrictor: The duration of infiltration lasts about 5-10 min for pulpal anesthesia and 1-2 h for soft
tissue anesthesia. The duration of nerve block lasts 40 – 60 min for pulpal anesthesia and 2 – 4 h for soft
tissue anesthesia.
With a vasoconstrictor: anesthesia extend 60-90 min for pulpal anesthesia and 3-8 h for soft tissue anesthesia.
28
BupivacaineBupivacaine
It is a local anaesthetic drug belonging to the Amide group. It is a long acting anesthetic with approximately 4 times the potency of other amides. It is 4 times less toxic than Lidocaine. It has slow onset of action than Lidocaine (6-10 min).
It has no topical anesthetic effect.
Not used as topical anesthetic
Used for infiltration, nerve block and epidural anaesthesia
Metabolized in liver and excreted by kidney. It is only available with a vasoconstrictor.
It provides pulpal anesthesia for 1.5 - 5 h and soft tissue anesthesia for 4-9 h.
29

ArticaineArticaine
Articaine is a dental local anesthetic drug belonging to the Amide group. It is the most widely used local anesthetic in dentistry. It is only available with a vasoconstrictor. Its duration of anesthesia for pulpal tissue is 45-75 min and soft tissue anesthesia is about
3-6 h.
It is the preferred anesthetic for dental procedures of relatively short duration,
30












![Pharmacology – II [PHL 322] CNS Depressants Dr. Abdulaziz Bin Saeedan.](https://static.fdocuments.in/doc/165x107/5697bfa41a28abf838c9702b/pharmacology-ii-phl-322-cns-depressants-dr-abdulaziz-bin-saeedan.jpg)



