

Pathogenesis of diseases of the gallbladder and biliary tract
Upload
irene-laneCategory
view
215download
1
Liver, Pancreas, Gallbladder, and Biliary Board Review
Elizabeth Paine, MDJuly 18, 2015
** I have no financial interests regarding the content of my presentation **
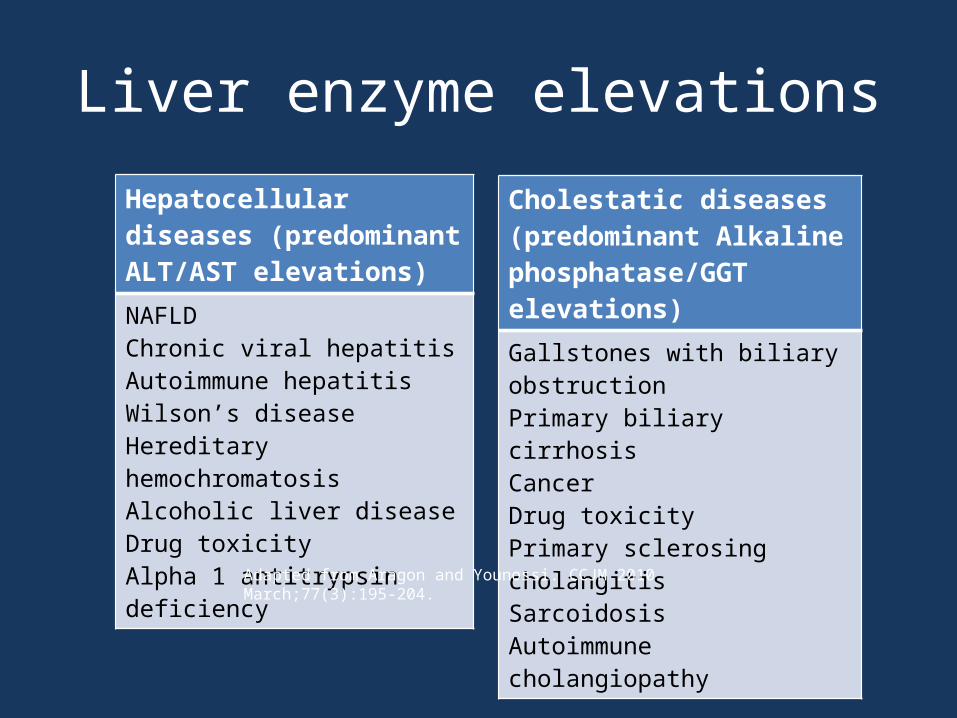
Liver enzyme elevationsHepatocellular diseases (predominant ALT/AST elevations)NAFLDChronic viral hepatitisAutoimmune hepatitisWilson’s diseaseHereditary hemochromatosisAlcoholic liver diseaseDrug toxicityAlpha 1 antitrypsin deficiency
Cholestatic diseases (predominant Alkaline phosphatase/GGT elevations)
Gallstones with biliary obstructionPrimary biliary cirrhosisCancerDrug toxicityPrimary sclerosing cholangitisSarcoidosisAutoimmune cholangiopathy
Adapted from Aragon and Younossi. CCJM 2010 March;77(3):195-204.

Elevated ALT/AST workup
Aragon and Younossi. CCJM 2010;77:195-204
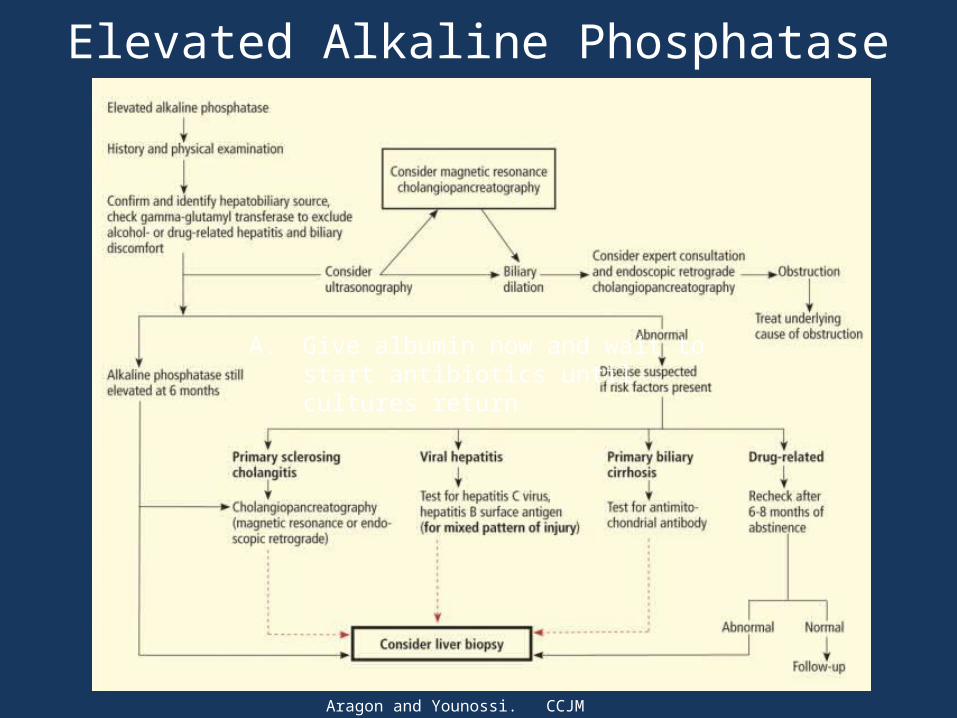
Elevated Alkaline Phosphatase
Aragon and Younossi. CCJM 2010;77:195-204
A. Give albumin now and wait to start antibiotics until cultures return

QuestionA 56 year old man with diabetes, hypertension and obesity (BMI 31) is found to have an ALT 67 and AST 40 with a normal albumin, total bilirubin, and alkaline phosphatase. He states that he has never been a drinker and has no family history of liver diseases. What is the most likely etiology of his abnormal liver enzymes from the choices below?
A. Autoimmune hepatitisB. Non-alcoholic fatty liver diseaseC. Wilson diseaseD. Hereditary hemochromatosis

QuestionA 56 year old man with diabetes, hypertension and obesity (BMI 31) is found to have an ALT 67 and AST 40 with a normal albumin, total bilirubin, and alkaline phosphatase. He states that he has never been a drinker and has no family history of liver diseases. What is the most likely etiology of his abnormal liver enzymes from the choices below?
A. Autoimmune hepatitisB. Non-alcoholic fatty liver diseaseC. Wilson diseaseD. Hereditary hemochromatosis

Nonalcoholic fatty liver disease (NAFLD)
• Broad term (steatosis cirrhosis)
• Associated with metabolic syndrome and obesity
• Diagnosis inferred by absence of other etiologies of liver disease
• TreatmentChalasani et al. Hepatology 2012;55(6): 2005-2023 http://liverbasics.com/hepatic-
steatosis.html

Autoimmune Hepatitis
• Range of presentations• Fatigue, jaundice,
malaise• Types 1 and 2• Autoantibodies seen:
ANA, ASMA, IgG, LKM1 • Treatments
Manns MP, Lohse AW, Vergani D. Autoimmune hepatitis – Update 2015. J. Hepatol. 2015 Apr;62(1S):S100-S111

Wilson’s disease
• Rare, autosomal recessive disorder
• Usually a young patient with neuropsychiatric symptoms
• Very low alkaline phosphatase• Low ceruloplasmin• Kayser-Fleischer rings• Can present in acute liver failure
http://www.wilsonsdisease.org/wilson-disease/kayserfleischerrings.php

Iron overload syndromes
• Hereditary hemochromatosis• Iron loading anemias (chronic hemolytic
anemias, sideroblastic anemia, thal major)• Chronic liver disease (alcoholic, viral hepatitis,
NAFLD)• Parenteral iron overload (RBC transfusions,
long standing HD)

Hereditary Hemochromatosis
• Most common genetic disease in Caucasians
• Iron saturation >45%• HFE genes C282Y and
H63D• Clinical features• Treatment:
phlebotomy with goal ferritin <50
https://cornellbiochem.wikispaces.com/Hereditary+Hemochromatosis

Viral Hepatitis
• Transmission- Fecal-oral: Hep A an E- Sexual: Hep B and D, also C
• Clinical features• Typical course

Question
Mr. Smith presents to your clinic and reports a 2 weeks history of fatigue and feeling “sick to my stomach.” He also reported that he saw another provider 1 week ago who mentioned something was abnormal with his liver. You order a CBC, CMP, and Hepatitis panel and find that he has positive IgM anti-HAV, positive Hepatitis B surface antibody, and elevated ALT/AST. What is the most likely etiology of his clinical picture?
A. Hepatitis BB. Hepatitis CC. Hepatitis AD. Hepatitis D

QuestionMr. Smith presents to your clinic and reports a 2 weeks history of fatigue and feeling “sick to my stomach.” He also reported that he saw another provider 1 week ago who mentioned something was abnormal with his liver. You order a CBC, CMP, and Hepatitis panel and find that he has positive IgM anti-HAV, negative IgG anti-HAV, positive Hepatitis B surface antibody, and elevated ALT/AST. What is the most likely etiology of his current clinical picture?
A. Hepatitis BB. Hepatitis CC. Hepatitis AD. Hepatitis D

Hepatitis B
• Incubation period• Multiple modes of
transmission• Can present with serum
sickness• Extraintestinal
manifestations: remember association with PAN

Hepatitis B
http://www.bio-rad.com/en-us/product/hepatitis-b/monolisa-anti-hbc-igm-eia

Hepatitis B serologiesHBsAg anti-HBs anti-HBc
IgManti-HBcIgG
HBeAg DX
+ - + - + Acute infection
+ - - + +/- Chronic infection
- + - - - Vaccinated
- + - + - Exposed immune
- - + - - Acute window
- - - + -Exposed, Ab lost

Hepatitis B treatment options
• Entecavir• Tenofovir• Adefovir• Lamivudine (if not resistant)• PEG IFN• Telbivudine

Hepatitis B treatmentHep B eAg HBV DNA ALT Treatment strategy
Positive >20K <2 x ULN Primarily observe until ALT elevated, can consider bx and tx if significant fibrosis
Positive >20K >2 x ULN Observe for 3-6 months and treat if no seroconversion
Negative >20K > 2x ULN Treat, endpoint not defined
Negative >2K 1-2 x ULN Treat if liver bx shows significant necroinflammation or fibrosis
Negative <2K < ULN Observe
Pos or Neg Detectable Cirrhosis If DNA > 2K, treat. If < 2K, consider tx if ALT elevated
Pos or Neg Undetectable Cirrhosis Compensated: observeDecompensated: refer for transplant
Adapted from Lok and McMahon. Chronic Hepatitis B: Update 2009. Hepatology September 2009.

Caveats with Hepatitis B
• If Hepatitis B eAg positive patient is treated, treat for 6 months after seroconversion to Hep B eAb positive
• Pregnancy and Hep B• HCC screening

Hepatitis C
• Risk factors• Genotypes – gt1 is most common in US• Screening: HCV Ab• Confirmation: PCR testing• CDC guidelines: Adults born 1945-1965
should be tested once (without prior ascertainment of HCV risk factors)
• Disease progression

Hepatitis C treatment
• Rapidly changing• Doubt this will be testable now since it is
changing by the month with new drugs
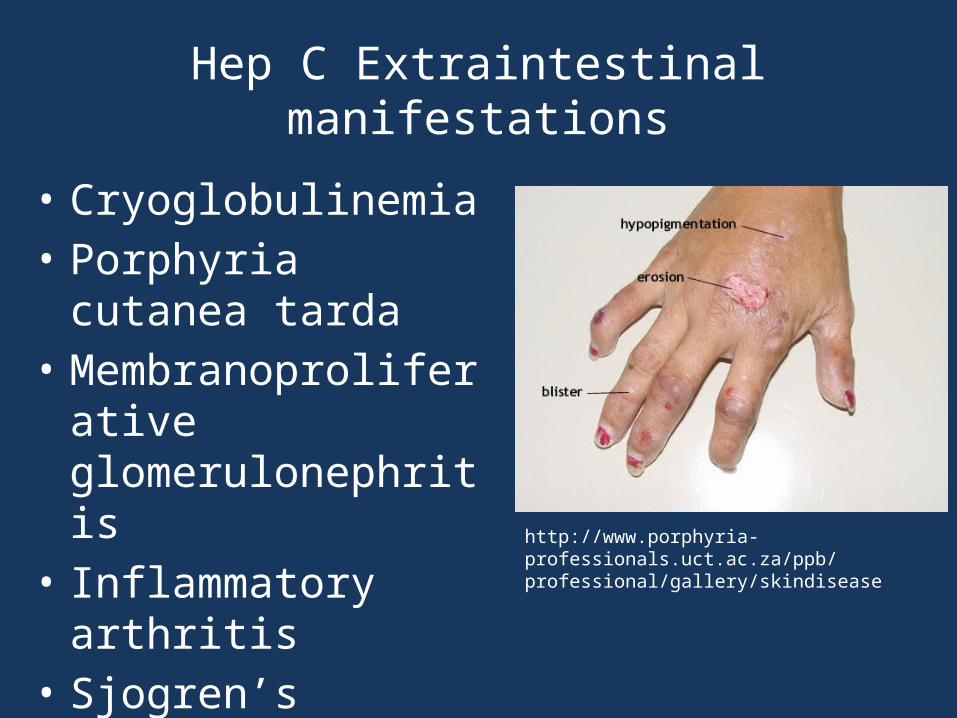
Hep C Extraintestinal manifestations
• Cryoglobulinemia• Porphyria cutanea tarda• Membranoproliferative
glomerulonephritis• Inflammatory arthritis• Sjogren’s syndrome
http://www.porphyria-professionals.uct.ac.za/ppb/professional/gallery/skindisease

Hepatitis D
• Requires co-existent Hepatitis B• Usually found in IVDA• Coinfection vs. superinfection• Diagnosis• Treatment
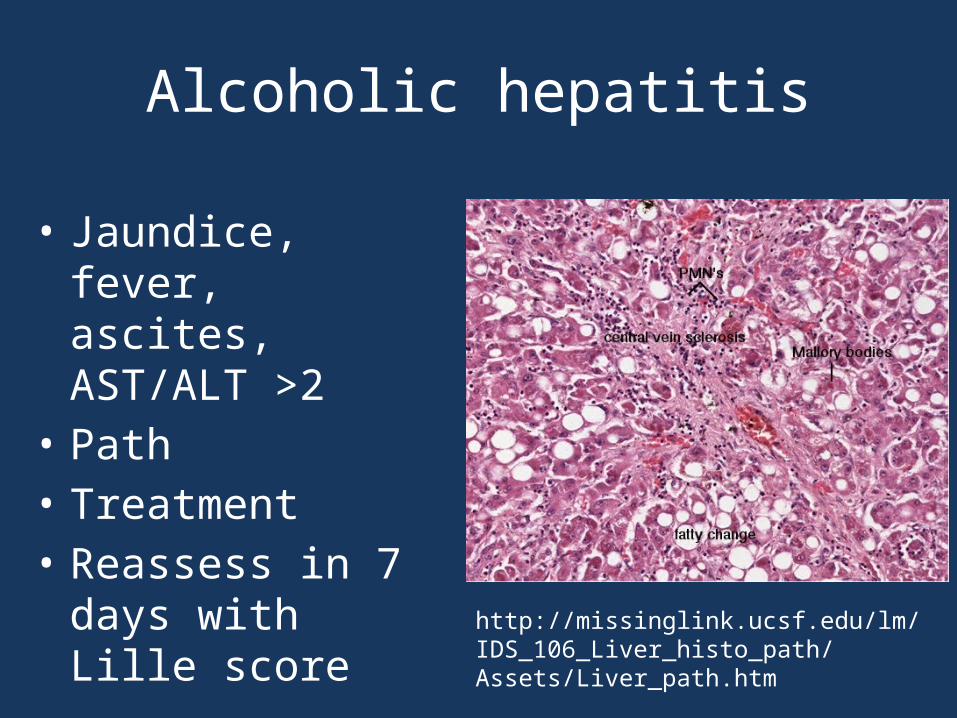
Alcoholic hepatitis
• Jaundice, fever, ascites, AST/ALT >2
• Path• Treatment• Reassess in 7 days
with Lille score
http://missinglink.ucsf.edu/lm/IDS_106_Liver_histo_path/Assets/Liver_path.htm

Primary biliary cirrhosis
• Usually middle aged female
• Itching and fatigue• Increased alkaline
phosphatase• Elevated AMA• Treat with ursodiol• Manage cirrhosis
https://www.pathology.med.umich.edu/greensonlab/pbc2.jpg

Primary Sclerosing Cholangitis
• Autoimmune• Fibrosis of large bile
ducts• RUQ pain, fatigue,
weight loss• 70% associated with UC• Increased risk of
cholangiocarcinoma• Diagnosed with MRCP
or ERCP
http://openi.nlm.nih.gov/detailedresult.php?img=2880347_ijgm-3-143f3&req=4
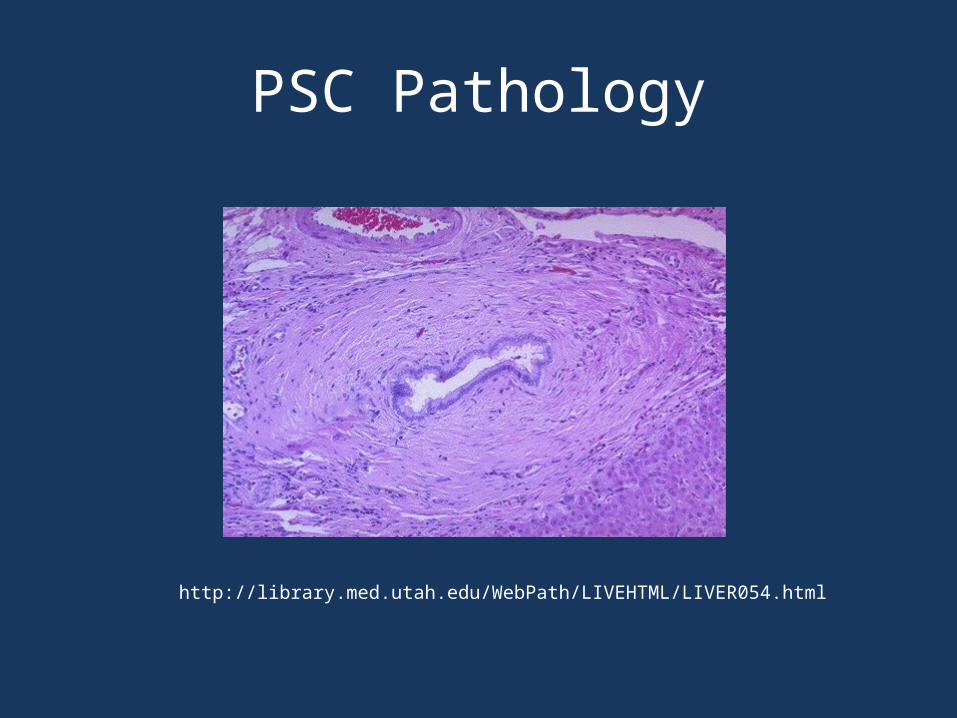
PSC Pathology
http://library.med.utah.edu/WebPath/LIVEHTML/LIVER054.html

Question
A 63 year old patient presents because of abnormal liver function tests including AST 123, ALT 143, alkaline phosphatase 143. He drinks 1 glass of wine daily. He takes amiodarone, losartan, and metformin. A liver biopsy is done and shows Mallory hyaline bodies consistent with fatty deposition. What is the most likely cause?
A. AlcoholB. MetforminC. AmiodaroneD. Losartan

Question
A 63 year old patient presents because of abnormal liver function tests including AST 123, ALT 143, alkaline phosphatase 143. He drinks 1 glass of wine daily. He takes amiodarone, losartan, and metformin. A liver biopsy is done and shows Mallory hyaline bodies consistent with fatty deposition. What is the most likely cause?
A. AlcoholB. MetforminC. AmiodaroneD. Losartan

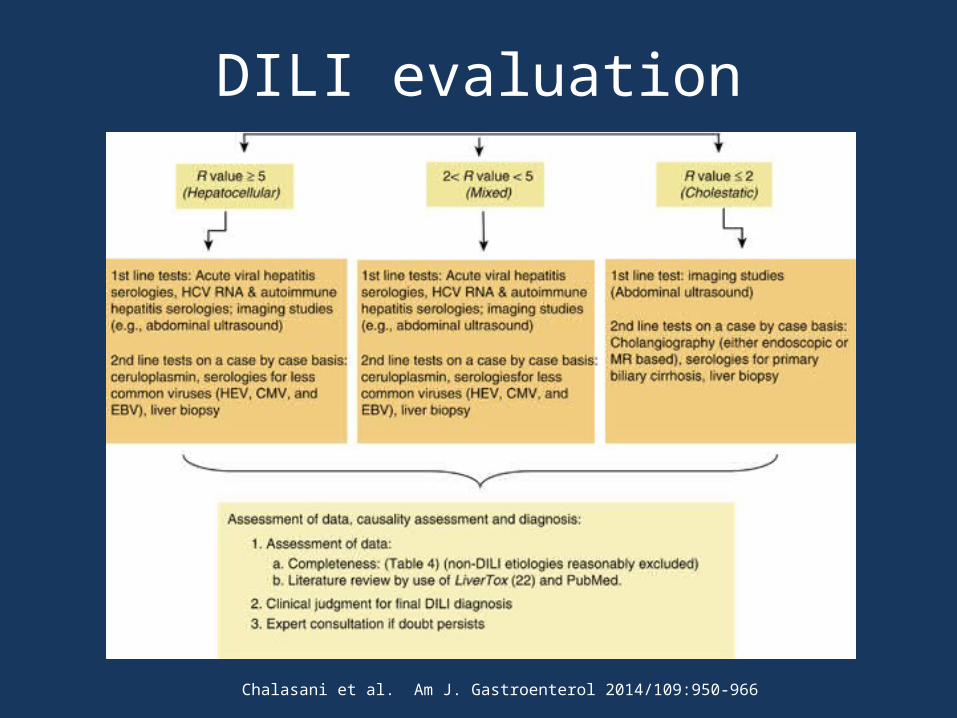
DILI evaluation
Chalasani et al. Am J. Gastroenterol 2014/109:950-966
DILI evaluation
Chalasani et al. Am J. Gastroenterol 2014/109:950-966

Drugs Commonly Associated with DILI
Drug Pattern Features
Amiodarone Macrovesicular fat “Bright” on non-contrast CT
Acetaminophen Acute hepatitis ALT >5000, renal injury
Amoxicillin/clavulanateTMP/SMX
Cholestasis May occur after treatment finished
Valproate Microvesicular fat Encephalopathy
NitrofurantoinMinocycline
Mimics autoimmune hepatitis
Can occur after months on the drug; may require steroids
Methotrexate Fibrosis Probably rare
Phenytoin Mixed Hypersensitivity features
Adapted from Mayo Clinic Gastroenterology and Hepatology Board Review 2013

QuestionA 22 year old woman who is 23 weeks pregnant presents to clinic complaining of itching. This itching is primarily on her palms and soles and is worse at night. She denies any tylenol usage or usage of other OTC medications except a prenatal vitamin. Her abdominal ultrasound is normal. Which of the following is the most likely diagnosis?
A. Intrahepatic cholestasis of pregnancyB. HELLP (Hemolysis, Elevated Liver Enzymes, Low
Platelets) syndromeC. Acute fatty liver of pregnancyD. Acute Hepatitis A
QuestionA 22 year old woman who is 23 weeks pregnant presents to clinic complaining of itching. This itching is primarily on her palms and soles and is worse at night. She denies any tylenol usage or usage of other OTC medications except a prenatal vitamin. Her abdominal ultrasound is normal. Which of the following is the most likely diagnosis?
A. Intrahepatic cholestasis of pregnancyB. HELLP (Hemolysis, Elevated Liver Enzymes, Low
Platelets) syndromeC. Acute fatty liver of pregnancyD. Acute Hepatitis A

Intrahepatic cholestasis of pregnancy
• Usually 3rd trimester, sometimes 2nd
• Pruritus - particularly palms and soles
• Less than ¼ develop jaundice• Treatment
Williamson and Geenes. Obstet Gynecol. 2014 July;124(1):120-33.

HELLP diagnosis
• Combination of clinical features• Abdominal imaging• Common lab features: H: LDH >600, abnormal smear EL: AST >70, AST/ALT elevation up to 10:10-20 fold LP: platelets <150,000

Acute Fatty Liver of Pregnancy
• Often presents as fulminant hepatic failure• Usually late 3rd trimester• Occurs in 1 in 6700 3rd trimester pregnancies• Associated factors• Treatment

Liver Diseases in Pregnancy
ICP HELLP AFLP
% Pregnancies 0.1% (USA) 0.2%–0.6% 0.005%–0.01%
Onset/trimester 25–32 weeks 3 or postpartum 3 or postpartum
Family history Often No Occasionally
Preeclampsia No Yes 50%
Typical clinical featuresPruritus, mild jaundice, increased bile acids, dec vit K
Hemolysis Thrombocytopenia
Liver failure with coagulopathy, HE hypoglycemia, DIC
Aminotransferases Mild to 10–20-fold ↑ Mild to 10–20-fold ↑ 300–500 but varies
Bilirubin <5 mg/dL <5 mg/dL unless massive necrosis
often <5 mg/dL, higher if severe
Hepatic imaging Normal Hepatic infarcts, hematomas, rupture Fatty infiltration
Histology Nl–mild cholestasis, no necrosis
Patchy/extensive necrosis, hemorrhage
Microvesicular fat in zone 3
Recurrence in subsequent pregnancies 45%–70% 4%–19% (LCHAD) defect—yes

Gilbert’s disease
• Unconjugated hyperbilirubinemia• Autosomal dominant• Jaundice worsens with stress and fasting• Usually not treated

Cirrhosis
Taylor CR. Cirrhosis Imaging. http://emedicine.medscape.com/article/366426-overview
Cirrhosis complications
• Ascites• Spontaneous bacterial peritonitis• Hepatic encephalopathy• Hepatorenal syndrome• Hepatocellular carcinoma
QuestionA 53 y/o man with DM2 and HTN presents to your clinic with a 2
month history of his pants becoming progressively tighter. He drinks a case of beer on the weekends but denies drug use. On exam, his BP is 99/55 with pulse of 75/minute and T 98.2°F. His abdomen is tense with no tenderness or rebound.
Labs: WBC 5, Hb 9.2, platelets 160,000, creatinine 2,albumin 3.4, AST 67, INR 1.4. Abdominal CT shows a large amount of ascites and some coarsening of the liver parenchyma. He underwent a 7L paracentesis with fluid studies as follows: fluid albumin 2, fluid total protein 1.5, fluid PMN’s 287.
Which of the following is the best next step?
A. Start Vancomycin 1g IV dailyB. Give albumin now and wait to start antibiotics until cultures returnC. Begin ciprofloxacin 250mg po weekly for SBPD. Start Cefotaxime and albumin

QuestionA 53 y/o man with DM2 and HTN presents to your clinic with a 2
month history of his pants becoming progressively tighter. He drinks a case of beer on the weekends but denies drug use. On exam, his BP is 99/55 with pulse of 75/minute and T 98.2°F. His abdomen is tense with no tenderness or rebound.
Labs: WBC 5, Hb 9.2, platelets 160,000, creatinine 2,albumin 3.4, AST 67, INR 1.4. Abdominal CT shows a large amount of ascites and some coarsening of the liver parenchyma. He underwent a 7L paracentesis with fluid studies as follows: fluid albumin 2, fluid total protein 1.5, fluid PMN’s 287.
Which of the following is the best next step?
A. Start Vancomycin 1g IV dailyB. Give albumin now and wait to start antibiotics until cultures returnC. Begin ciprofloxacin 250mg po weekly for SBPD. Start Cefotaxime and albumin

Ascites on CT
Poggi et al. International Journal of Case Reports and Images. 2013;4(1):32-36.
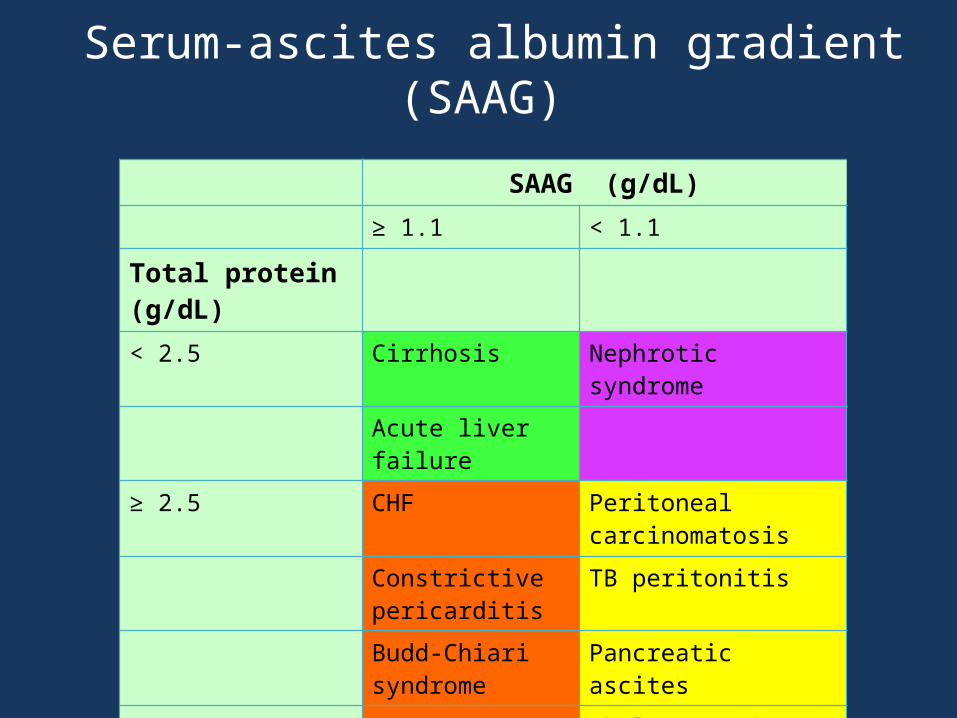
Serum-ascites albumin gradient (SAAG)
SAAG (g/dL)
≥ 1.1 < 1.1
Total protein (g/dL)
< 2.5 Cirrhosis Nephrotic syndrome
Acute liver failure
≥ 2.5 CHF Peritoneal carcinomatosis
Constrictive pericarditis
TB peritonitis
Budd-Chiari syndrome
Pancreatic ascites
Veno-occlusive disease
Chylous ascites

Ascites therapy: dietary and diuretics
• Sodium restriction < 2 grams/day• Spironolactone/furosemide in a ratio
of 100/40• Goal is weight loss of 0.5-1kg/day• Diuretics are titrated to achieve
weight loss without complications
Runyon and AASLD Practice Guideline Committee. Management of Adult Patients with Ascites Due to Cirrhosis. 2013.

Refractory ascites
• Definition• Reversible
factors• Treatment
options• TIPS
https://www.uic.edu/com/virtualpatient/part3/data/surgeryhtml/1310detail.htm
Runyon and AASLD Practice Guideline Committee. Management of Adult Patients with Ascites Due to Cirrhosis. 2013 .
Spontaneous bacterial peritonitis (SBP)
• Definition• Frequency• Clinical manifestations• Diagnosis: absolute
PMN > 250• Bacterial culture
Example ascitic fluid labs in patient with SBP:
WBC 5300/mm3
87% neutrophilsAlbumin <1
Runyon and AASLD Practice Guideline Committee. Management of Adult Patients with Ascites Due to Cirrhosis. 2013.
SBP treatment
• Need to control ascites• Cefotaxime 2g IV q8
hours• Uncomplicated SBP
outpatient can be treated with oral ofloxacin
• Albumin infusion
Runyon and AASLD Practice Guideline Committee. Management of Adult Patients with Ascites Due to Cirrhosis. 2013 .

Primary and secondary prophylaxis
• Primary prophylaxis: - IV cefotaxime or BID norfloxacin - Indicated for the following patients: cirrhotic with GI bleed (for 7 days) pts w ascitic fluid protein <1.5 and Cr≥1.2, BUN≥25, Na ≤130, CTP ≥9, bili≥3 (long term abx can be considered)
• Secondary prophylaxis: - Norfloxacin 400mg daily or bactrim/cipro daily. Daily dosing recommended over weekly dosing. - For patients who previously had SBP
Runyon and AASLD Practice Guideline Committee. Management of Adult Patients with Ascites Due to Cirrhosis. 2013.

Question
A 42 year old woman with cirrhosis presents to the ER with active hematemesis and an emesis basin full of bright red blood. What is the most likely etiology of her upper GI bleeding?
A. Dieulafoy lesionB. Portal hypertensive gastropathyC. Angioectasia/AVMD. Esophageal varices

Question
A 42 year old woman with cirrhosis presents to the ER with active hematemesis and an emesis basin full of bright red blood. What is the most likely etiology of her upper GI bleeding?
A. Dieulafoy lesionB. Portal hypertensive gastropathyC. Angioectasia/AVMD. Esophageal varices

Esophageal varices• ~1/4 to 1/3 of cirrhotics hemorrhage at least
once from varices• Have portal HTN with pressures > 12mmHg• Esophageal variceal hemorrhage• Management of bleeding esophageal varices
Garcia-Tsao et al. Hepatology 2007:46(3):922-934.

Esophageal varices
http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/hepatology/variceal-hemorrhage/

Question
A 65 year old man with cirrhosis is brought in to the clinic by his wife after he had several days of staying up all night and sleeping all day, along with intermittent periods of “not making sense.” He has asterixis on exam. What should be done for this patient?
A. Start lactulose and titrate for 3 loose stools dailyB. Restrict the protein in his dietC. Initiate metronidazoleD. Start furosemide
Question
A 65 year old man with cirrhosis is brought in to the clinic by his wife after he had several days of staying up all night and sleeping all day, along with intermittent periods of “not making sense.” He has asterixis on exam. What should be done for this patient?
A. Start lactulose and titrate for 3 loose stools dailyB. Restrict the protein in his dietC. Initiate metronidazoleD. Start furosemide

Hepatic encephalopathy
• Describes the spectrum of potentially reversible neuropsychiatric abnormalities in patients with liver dysfunction
• Presumed mechanism• Early feature is sleep disturbance• Later features are asterixis,
hyperactive DTRs, transient decerebrate positioning
Vistrup et al. Hepatology 2014 Aug;60(2):715-35.

Hepatic encephalopathy management
• Identification and avoidance of precipitants• Lactulose 30mL BID-TID, titrated for 2-4 BM daily
Rifaximin 550mg po BID• Protein restriction is no longer recommended for
most patients• Treatment of post-TIPs hepatic encephalopathy
Vistrup et al. Hepatology 2014 Aug;60(2):715-35.

QuestionA 55 year old man with history of cirrhosis and ascites undergoes his q6 month surveillance imaging. On ultrasound, he was found to have a new 2.6cm liver lesion. AFP was 532. Subsequent 3phase liver CT showed the same lesion with arterial enhancement and portal venous washout. What is the most likely diagnosis?
A. HemangiomaB. Hepatocellular carcinomaC. MetastasisD. Hepatic cyst

QuestionA 55 year old man with history of cirrhosis and ascites undergoes his q6 month surveillance imaging. On ultrasound, he was found to have a new 2.6cm liver lesion. AFP was 532. Subsequent 3phase liver CT showed the same lesion with arterial enhancement and portal venous washout. What is the most likely diagnosis?
A. HemangiomaB. Hepatocellular carcinomaC. MetastasisD. Hepatic cyst

Hepatocellular carcinoma
• Cirrhotic patients have increased risk for HCC
• Hep B patients can develop HCC without cirrhosis
• Common signs/symptoms
• Diagnosis
Bruix and Sherman. Management of Hepatocellular Carcinoma. AASLD guideline 2011.

Barcelona criteria
Sherman M et al. Current Oncology 2011. 18(5):228-240.

QuestionA 65 year old man with alcoholic cirrhosis is admitted to House Medicine with spontaneous bacterial peritonitis. He has not been taking NSAIDs or diuretics. His initial serum creatinine is 1.1 but 4 days later, his creatinine has risen to 3.6 and he is anuric. His creatinine does not improve after receiving 2 days of albumin infusions. Which of the following statements is true?
A. He likely has type I hepatorenal syndromeB. He likely has type II hepatorenal syndrome and will improve
without treatmentC. He should be given vasodilators to improve renal perfusionD. He should be given furosemide and aldactone in a 40/100
ratio
QuestionA 65 year old man with alcoholic cirrhosis is admitted to House Medicine with spontaneous bacterial peritonitis. He has not been taking NSAIDs or diuretics. His initial serum creatinine is 1.1 but 4 days later, his creatinine has risen to 3.6 and he is anuric. His creatinine does not improve after receiving 2 days of albumin infusions. Which of the following statements is true?
A. He likely has type I hepatorenal syndromeB. He likely has type II hepatorenal syndrome and will improve
without treatmentC. He should be given vasodilators to improve renal perfusionD. He should be given furosemide and aldactone in a 40/100
ratio
Hepatorenal syndrome diagnosis
Salerno et al. Gut 2007;56:1310-1318.
Diagnostic criteria (Salerno et. al 2007)
• Cirrhosis with ascites• Serum Cr >1.5• No improvement after 2 days of diuretic withdrawal
and plasma volume expansion with albumin (100g/day)
• Absence of shock• No current or recent nephrotoxic drugs or
vasodilation• Absence of parenchymal kidney disease with
proteinuria <500, no US evidence of obstructive uropathy or microhematuria

Hepatorenal syndrome
• Types: - Type 1 HRS - Type 2 HRS• Treatment - Prevention - Therapy
Runyon and AASLD Practice Guideline Committee. Management of Adult Patients with Ascites Due to Cirrhosis. 2013.

Schistosomiasis – Hepatic involvement
• In adults with chronic infection – “pipestem fibrosis”
• Portal HTN & splenomegaly• GI varices• Often no abnormalities in LFTs• Gold standard for dx is
microscopy of stool or urine sample for schistosome eggs
• Treatment: praziquantel 40-60 mg/kg
http://www.microbiologybook.org/parasitology/sch3.jpg

Acute pancreatitis
• Acute onset persistent epigastric abdominal pain
• Usually with nausea/vomiting
• Elevated amylase, lipase
• ImagingMunoz and Katerndahl. Am Fam Physician 2000 July 1;62(1):164-174

Etiologies of acute pancreatitis
• Alcohol abuse• Gallstones• Hypertriglyceridemia• Post-ERCP• Pancreatic malignancy• Medications• Hypercalcemia
Medications:FurosemideThiazidesEstrogensAzathioprine5-ASATetracyclinesSulfonamidesAnti-HIV drugsValproic acidSome diabetes drugs
Poor prognostic indicators in acute pancreatitis
• SBP <90 with HR >130• PO2 < 60mmHg• Urine output <50mL/hr• Altered mental status• Pancreatic necrosis• Altered mental status• Low calcium (<8mg/dL) and albumin <3.2 g/dL• Hemoconcentration (Hct > 44%)• APACHE 2 score > 8

Complications of acute pancreatitis
• Necrosis• Pseudocyst• Abscess• Shock• Left sided pleural
effusion• Splenic vein
thrombus http://www.top5plus5.com/Pseudocyst%20of%20the%20Pancreas_files/Pseudocysts%20Images.html

Management of acute pancreatitis
• Supportive care• NPO initially but early enteral feeding as able• IVF • Systemic antibiotics if infected or severe• Pain control• ERCP for cholangitis or sepsis

Chronic pancreatitis
• Usually result of chronic ETOH
• Early sx: recurrent abdominal pain
• Late sx: steatorrhea and DM
• Imaginghttp://www.nytimes.com/imagepages/2007/08/01/health/adam/1157PancreatitischronicCTscan.html

Complications of chronic pancreatitis
• Pancreatic cancer (~ 4% of pts with chronic pancreatitis >20 years)
• Brittle DM, prone to hypoglycemia• Splenic vein thrombosis• B12 malabsorption
Management of chronic pancreatitis
• Pancreatic enzymes (start with 500 lipase units/kg/meal) with antacids
• Decrease fat in diet• Add medium-chain TG• Avoid ETOH• Stop smoking

Autoimmune pancreatitis
• Often have painless obstructive jaundice
• Can have elevated IgG4
• Imaging findings• Tx: steroids
Chruch et al. Am. J. Gastroenterol 2007(102):2417-2425.

Pancreatic cancer
• Jaundice, weight loss, abdominal pain
• If in pancreatic head: painless jaundice
• If in body/tail: pain, weight loss
• Diagnosis• Treatment
http://www.aboutcancer.com/pancreas1_images.htm

Question
A 65 y/o veteran is found to have the following ultrasound but is asymptomatic with normal labs. What should be done next?
A. ObservationB. Referral to SurgeryC. Abdominal CTD. MRI

Question
A 65 y/o veteran is found to have the following ultrasound but is asymptomatic with normal labs. What should be done next?
A. ObservationB. Referral to SurgeryC. Abdominal CTD. MRI

Cholelithiasis
• Very common• Association with obesity, OCP, ileal
disease/resection• Symptoms: post-prandial RUQ pain• US to diagnose• If asymptomatic, do nothing• If symptomatic refer to surgery

Choledocholithiasis
• Stones in CBD• Elevated AlkPhos and
bilirubin• Can also see CBD
dilation on US• Tx: ERCP with
sphincterotomy in most cases http://www.healthhype.com/gallbladder-tests-
ultrasound-ct-hida-scan-ercp.html

Acute Cholecystitis
• RUQ pain, fever, leukocytosis• Calculous vs. acalculous• Frequently have positive “Murphy’s sign”• Ultrasound• HIDA scan• Tx: cholecystectomy (if good surgical
candidate), percutaneous cholecystotomy with abx if very sick

Acute cholangitis
• Charcot’s triad• Complication of choledocholithiasis or cancer• Need antibiotics• Also need ERCP with endoscopic
sphincterotomy or surgery if ERCP isn’t available

Liver/Biliary history pearls
• Pruritus/cholestasisPBC/PSC
• Undercooked food, oysters, daycareHepatitis A
• ICU, hypotension, right sided CHFHepatic congestion
• Neuropsych findingsWilson’s disease

Liver/Biliary history pearls
• Metabolic syndrome, mildly elevated ALT/ASTFatty liver
• HyperpigmentationHemochromatosis or PBC
• Kayser-Fleischer rings/sunflower cataractsWilson’s disease
Liver/Biliary history pearls
• SplenomegalyPortal hypertension or infiltrative process
• Pulsatile liverTricuspid insufficiency
• Hepatic bruitsHepatocellular carcinoma

Questions?


















