Liver Harvesting Surgical Technique for the Treatment of Retro-Hepatic Caval Thrombosis Concomitant...
9
European Urology European Urology 45 (2004) 194–202 Liver Harvesting Surgical Technique for theTreatment of Retro-Hepatic Caval Thrombosis Concomitant to Renal Cell Carcinoma: Perioperative and Long-Term Results in 15 Patients without Mortality Michele Gallucci a , Domenico Borzomati b,* , Gerardo Flammia c , Antonio Alcini c , Giuseppe Albino a , Marco Caricato b , Alessandro Esposito b , Bruno Vincenzi d , Massimo Rossi e , Roberto Coppola b , Pasquale Berloco e a Department of Urology, ‘‘Regina Elena’’ Institute, Rome, Italy b Department of General Surgery, Campus Bio-Medico University, Via Longoni, 49 00155 Rome, Italy c Department of Urology, Campus Bio-Medico University, Rome, Italy d Department of Oncology, Campus Bio-Medico University, Rome, Italy e Department of Transplant Surgery, ‘‘La Sapienza’’ University, Rome, Italy Accepted 9 September 2003 Published online 3 October 2003 Abstract Objective: Radical surgical treatment improves the prognosis of patients affected by Inferior Vena Cava (IVC) thrombosis concomitant to renal carcinoma. However, thrombus extension above the infrahepatic IVC represents a major technical topic for surgeons because of the possible occurrence of uncontrollable haemorrhages and tumor fragmentation. We report the results of an innovative surgical approach to caval thrombosis including the isolation of the IVC from the liver as routinely performed during liver harvesting. In the presence of retro-hepatic IVC thrombosis, this technique improves vascular control and allows to perform a large cavotomy with an en-bloc removal of the thrombus and the tumor. Methods: From January 1995 through June 2003, 15 patients with renal cancer and caval thrombosis were treated at our Institution. Four, ten and one patients were respectively affected by an infrahepatic (Level I), retro-hepatic (Level II) and atrial (Level III) IVC thrombosis. Results: All patients underwent radical surgical treatment. In presence of Level II caval thrombosis, the patients underwent the above reported surgical technique. Perioperative mortality was absent; major morbidity occurred in one patient (6.7%). The thrombus was radically removed in all cases. After a mean follow-up of 53.9 months (5–100 months) all patients but one are still alive. One patient died 9 months after surgery with multiple bilateral pulmonary metastases. Conclusions: Isolation of the retro-hepatic IVC is a safe and effective manoeuvre to significantly reduce perioperative mortality and morbidity in patients affected by Level II caval thrombosis concomitant to renal carcinoma. # 2003 Elsevier B.V. All rights reserved. Keywords: Inferior Vena Cava Thrombosis; Renal carcinoma; Surgical technique; Liver 1. Introduction Inferior Vena Cava (IVC) involvement occurs in about 10% of patients affected by renal cell carcinoma [1–10]. In the past IVC invasion by tumor was considered a poor * Corresponding author. Tel. þ39-335-6183775; Fax: þ39-06-22541444. E-mail address: [email protected] (D. Borzomati). 0302-2838/$ – see front matter # 2003 Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2003.09.004
-
Upload
michele-gallucci -
Category
Documents
-
view
214 -
download
2
Transcript of Liver Harvesting Surgical Technique for the Treatment of Retro-Hepatic Caval Thrombosis Concomitant...

EuropeanUrology European Urology 45 (2004) 194–202
Liver Harvesting SurgicalTechnique for theTreatment ofRetro-Hepatic CavalThrombosis Concomitant toRenal Cell Carcinoma: Perioperative and Long-TermResults in15 PatientswithoutMortalityMichele Galluccia, Domenico Borzomatib,*, Gerardo Flammiac, Antonio Alcinic,Giuseppe Albinoa, Marco Caricatob, Alessandro Espositob, Bruno Vincenzid,Massimo Rossie, Roberto Coppolab, Pasquale Berlocoe
aDepartment of Urology, ‘‘Regina Elena’’ Institute, Rome, ItalybDepartment of General Surgery, Campus Bio-Medico University, Via Longoni, 49 00155 Rome, ItalycDepartment of Urology, Campus Bio-Medico University, Rome, ItalydDepartment of Oncology, Campus Bio-Medico University, Rome, ItalyeDepartment of Transplant Surgery, ‘‘La Sapienza’’ University, Rome, Italy
Accepted 9 September 2003
Published online 3 October 2003
AbstractObjective: Radical surgical treatment improves the prognosis of patients affected by Inferior Vena Cava (IVC)thrombosis concomitant to renal carcinoma. However, thrombus extension above the infrahepatic IVC represents amajor technical topic for surgeons because of the possible occurrence of uncontrollable haemorrhages and tumorfragmentation. We report the results of an innovative surgical approach to caval thrombosis including the isolation ofthe IVC from the liver as routinely performed during liver harvesting. In the presence of retro-hepatic IVCthrombosis, this technique improves vascular control and allows to perform a large cavotomy with an en-blocremoval of the thrombus and the tumor.Methods: From January 1995 through June 2003, 15 patients with renal cancer and caval thrombosis were treated atour Institution. Four, ten and one patients were respectively affected by an infrahepatic (Level I), retro-hepatic(Level II) and atrial (Level III) IVC thrombosis.Results: All patients underwent radical surgical treatment. In presence of Level II caval thrombosis, the patientsunderwent the above reported surgical technique. Perioperative mortality was absent; major morbidity occurred inone patient (6.7%). The thrombus was radically removed in all cases. After a mean follow-up of 53.9 months (5–100months) all patients but one are still alive. One patient died 9 months after surgery with multiple bilateral pulmonarymetastases.Conclusions: Isolation of the retro-hepatic IVC is a safe and effective manoeuvre to significantly reduceperioperative mortality and morbidity in patients affected by Level II caval thrombosis concomitant to renalcarcinoma.# 2003 Elsevier B.V. All rights reserved.
Keywords: Inferior Vena Cava Thrombosis; Renal carcinoma; Surgical technique; Liver
1. Introduction
Inferior Vena Cava (IVC) involvement occurs in about10% of patients affected by renal cell carcinoma [1–10].In the past IVC invasion by tumor was considered a poor
* Corresponding author. Tel. þ39-335-6183775;
Fax: þ39-06-22541444.
E-mail address: [email protected] (D. Borzomati).
0302-2838/$ – see front matter # 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.eururo.2003.09.004

prognostic factor and a ‘‘no touch’’ policy has beenadvocated by authors [2,11–17]. However, non-surgicaltreatments offer poor results and short survival timewithout long-term survivors has been reported amongpatients not undergoing radical surgery because ofdistant metastases or inadequate performance status[18–23]. Improvement in surgical techniques andperioperative management in the 1970s changed theapproach to renal tumors with caval thrombosis. Ifcomplete thrombus removal from IVC is performed,it has been shown that caval thrombosis does not affectthe prognosis of patients with renal cancer [4,19,20,24–26]. Thus, an increasing number of patients with renaltumor and caval thrombosis underwent radical surgicaltreatment. In 1998 Babu proposed a classification ofcaval thrombosis concomitant to renal tumors. Accord-ing toa cephalic extension pattern, infrahepatic (Level I),retro-hepatic/thoracic (Level II) and atrial (Level III)caval thrombosis were considered [5]. All series pub-lished in the last 20 years confirmed that radical surgeryis an effective treatment for patients [3,6,7,27–34] evenin presence of distant metastases [8,35]. In spite of itsoncological effectiveness surgical treatment of cavalthrombosis still results in significant rates of majorperioperative morbidity (11–71.4%) and mortality(3.4–16%) [1,3,6,7,18,28,33,35–38]. As expected, thesefigures change according to the cephalic extension ofthe thrombus with a lower risk for infrahepatic cavalthrombosis. On the other hand, poorer perioperativeresults have been reported if the surgical treatment ofLevel II–III thrombosis is considered [1,5,33,35,38,39].In these cases massive pulmonary embolisms andhemorrhages are undesired reported events [5,35]. Inorder to safely approach caval thrombosis, surgeonshave adopted several different surgical strategies.However, most of these experiences failed to achievea safe and effective vascular control of the IVC. Largethoraco-abdominal access with cardio-circulatory arresthas been described as the best surgical approach toatrial thrombosis [1,34,35,39,40,59]. The thrombus isremoved via a large thoraco-abdominal cavotomy andatriotomy. Perioperative results are excellent and manycenters adopted this technique. This strategy has beenrecently advocated also for patients with a thrombusextension ‘‘limited’’ to the retro-hepatic IVC. However,it cannot be considered an ideal treatment of an entirelyabdominal disease because of invasivity and possibleincrease in morbidity. Moreover, increase in costs islikely to occur. According to the results of the presentseries, adequate results can also be achieved if anentirely abdominal access with careful mobilizationof the retro-hepatic portion of the IVC is performed.The isolation of the IVC from the posterior margin of
the liver is a manoeuvre routinely performed by trans-plant surgeons during liver harvesting. Its use, in pre-sence of a thrombus extended to retro-hepatic IVC,allows the surgeon to achieve an effective vascularcontrol of the vein. In collaboration with liver transplantsurgeons we prospectively planned to perform in pre-sence of retro-hepatic caval thrombosis and renal cancera surgical procedure including a complete detachment ofthe liver from the IVC as used in liver transplant surgeryand a large infra- and retro-hepatic cavotomy with an en-bloc removal of the thrombus and the tumor. The presentpaper reports perioperative and long-term results of thissurgical technique performed in 15 consecutively trea-ted patients affected by caval thrombosis concomitantwith renal cell carcinoma without mortality.
2. Materials andmethods
From January 1995 through June 2003, 122 patients affected byrenal cell carcinoma were surgically treated at our Institution. Toprospectively evaluate our surgical approach to caval thrombosis,all patients affected by renal cancer observed at Campus Bio-Medico University of Rome entered in a database that recorded: (1)preoperative clinical data, (2) results of pre- and postoperativework-up, (3) intraoperative data (including operative time, time ofhepatic pedicle, controlateral renal vessels and caval clamping,blood loss, surgical and anesthesiological complications), (4)perioperative major and minor morbidity, (5) length of stay, (6)postoperative time of common habits’ resumption, (7) follow-up(that included laboratory parameters and instrumental controls ofiliac and caval axis blood flow).
In 15 out of 122 cases (12.3%) tumor propagation through therenal vein in the IVC was identified. Of the 15 patients 10 (66.7%)were males and 5 (33.3%) females. Median age was 65.9 years(range: 52–79 years). Symptoms and/or signs on physical exam-ination indicating the presence of a caval thrombosis were presentin 7 out of 15 patients (46.7%). Edema of the lower extremity waspresent in 5 (33.3%), dispnea and/or chest pain in 1 (6.7%). Three(20.0%) patients were affected by a totally asymptomatic thrombusof the IVC while in 4 (26.6%) the clinical signs of caval thrombosiswere the only clinical evidence of the renal tumor. All patientsunderwent US color Doppler of iliac-caval axis, abdominal andchest CT scan and/or MRI. Cavography was performed in 6 caseswhile cardiac trans-esophageal US in 11 cases. Imaging examsrevealed that 4 (26.6%), 10 (66.7%) and 1 (6.7%) patients wereaffected by Level I, II and III caval thrombosis. No radiologicalevidence of caval infiltration by the tumor was pointed out by MRIand/or cavography. Primitive tumor originated from right and leftkidney in 12 (80.0%) and 3 (20.0%) patients respectively. Onepatient affected by a Level III thrombosis was also affected by adistal right lung metastases that was synchronously resected, as well.
3. Surgical technique
The following surgical procedure has been used inall patients of our series affected by Level II cavalthrombosis.
M. Gallucci et al. / European Urology 45 (2004) 194–202 195
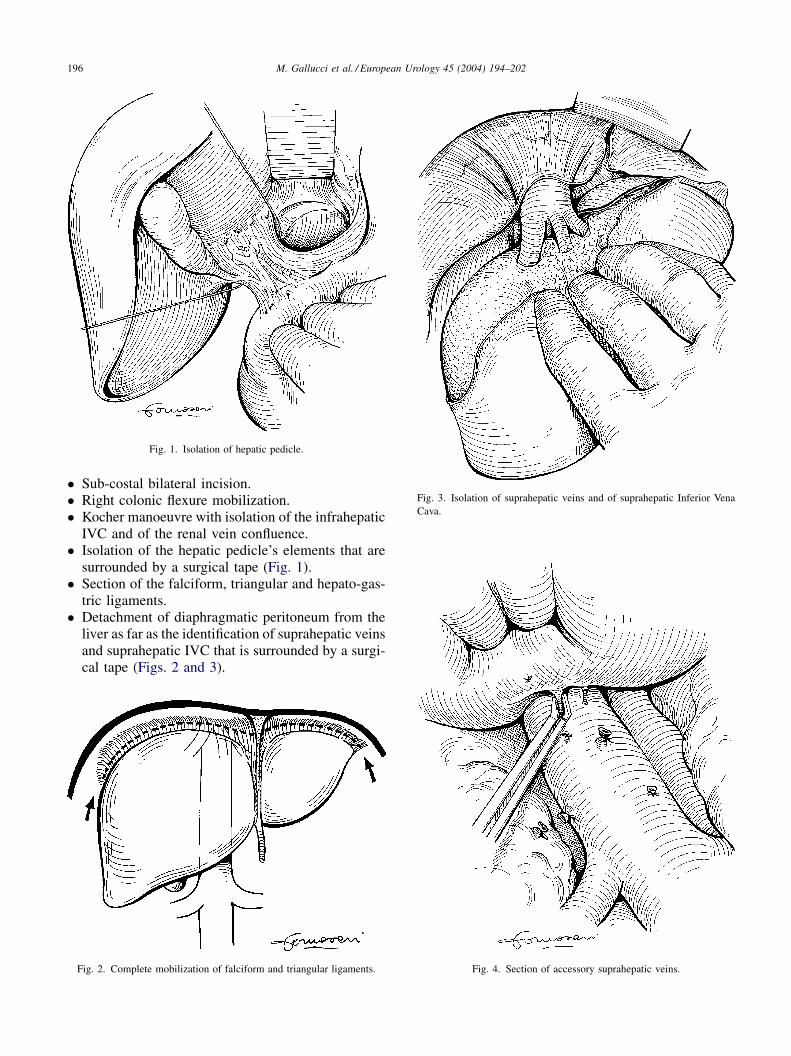
� Sub-costal bilateral incision.� Right colonic flexure mobilization.� Kocher manoeuvre with isolation of the infrahepatic
IVC and of the renal vein confluence.� Isolation of the hepatic pedicle’s elements that are
surrounded by a surgical tape (Fig. 1).� Section of the falciform, triangular and hepato-gas-
tric ligaments.� Detachment of diaphragmatic peritoneum from the
liver as far as the identification of suprahepatic veinsand suprahepatic IVC that is surrounded by a surgi-cal tape (Figs. 2 and 3).
Fig. 1. Isolation of hepatic pedicle.
Fig. 2. Complete mobilization of falciform and triangular ligaments.
Fig. 3. Isolation of suprahepatic veins and of suprahepatic Inferior Vena
Cava.
Fig. 4. Section of accessory suprahepatic veins.
196 M. Gallucci et al. / European Urology 45 (2004) 194–202
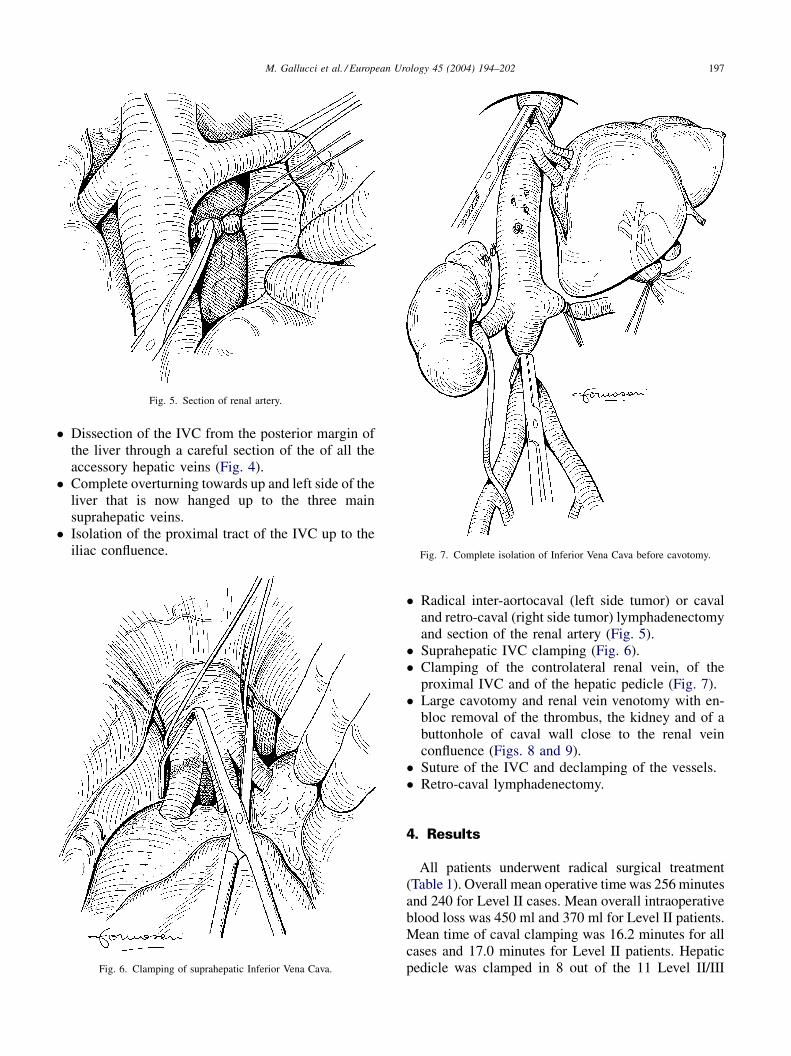
� Dissection of the IVC from the posterior margin ofthe liver through a careful section of the of all theaccessory hepatic veins (Fig. 4).
� Complete overturning towards up and left side of theliver that is now hanged up to the three mainsuprahepatic veins.
� Isolation of the proximal tract of the IVC up to theiliac confluence.
� Radical inter-aortocaval (left side tumor) or cavaland retro-caval (right side tumor) lymphadenectomyand section of the renal artery (Fig. 5).
� Suprahepatic IVC clamping (Fig. 6).� Clamping of the controlateral renal vein, of the
proximal IVC and of the hepatic pedicle (Fig. 7).� Large cavotomy and renal vein venotomy with en-
bloc removal of the thrombus, the kidney and of abuttonhole of caval wall close to the renal veinconfluence (Figs. 8 and 9).
� Suture of the IVC and declamping of the vessels.� Retro-caval lymphadenectomy.
4. Results
All patients underwent radical surgical treatment(Table 1). Overall mean operative time was 256 minutesand 240 for Level II cases. Mean overall intraoperativeblood loss was 450 ml and 370 ml for Level II patients.Mean time of caval clamping was 16.2 minutes for allcases and 17.0 minutes for Level II patients. Hepaticpedicle was clamped in 8 out of the 11 Level II/III
Fig. 5. Section of renal artery.
Fig. 6. Clamping of suprahepatic Inferior Vena Cava.
Fig. 7. Complete isolation of Inferior Vena Cava before cavotomy.
M. Gallucci et al. / European Urology 45 (2004) 194–202 197
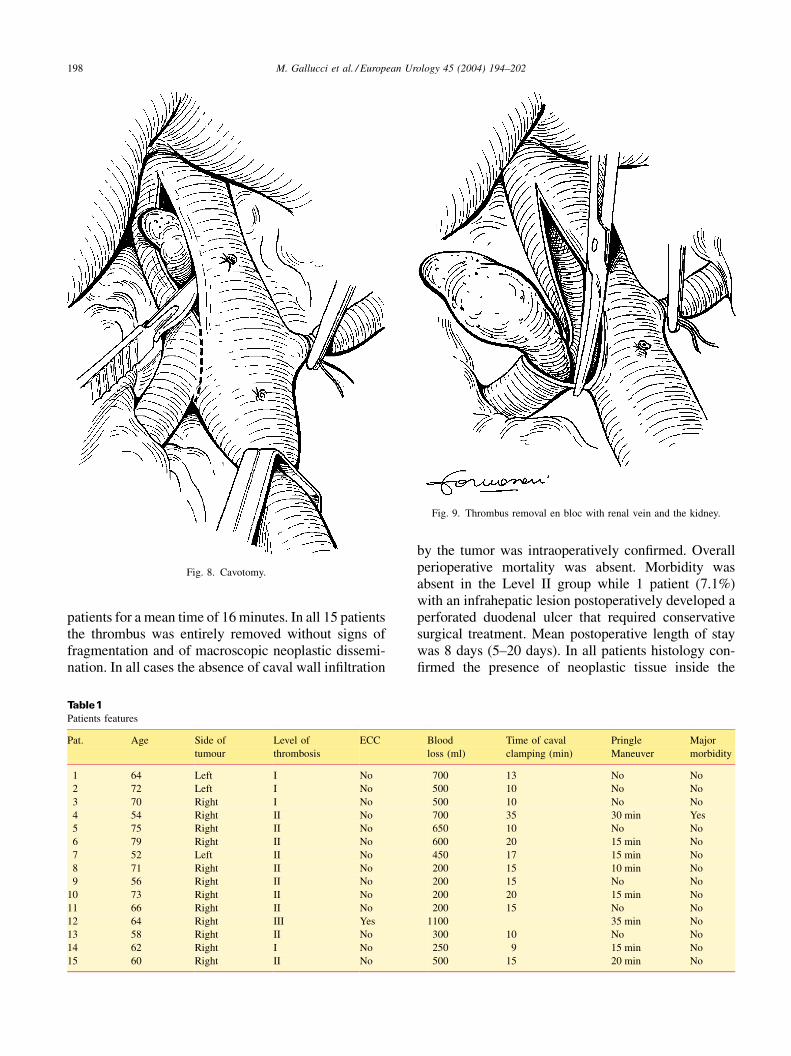
patients for a mean time of 16 minutes. In all 15 patientsthe thrombus was entirely removed without signs offragmentation and of macroscopic neoplastic dissemi-nation. In all cases the absence of caval wall infiltration
by the tumor was intraoperatively confirmed. Overallperioperative mortality was absent. Morbidity wasabsent in the Level II group while 1 patient (7.1%)with an infrahepatic lesion postoperatively developed aperforated duodenal ulcer that required conservativesurgical treatment. Mean postoperative length of staywas 8 days (5–20 days). In all patients histology con-firmed the presence of neoplastic tissue inside the
Fig. 8. Cavotomy.
Fig. 9. Thrombus removal en bloc with renal vein and the kidney.
Table1Patients features
Pat. Age Side of
tumour
Level of
thrombosis
ECC Blood
loss (ml)
Time of caval
clamping (min)
Pringle
Maneuver
Major
morbidity
1 64 Left I No 700 13 No No
2 72 Left I No 500 10 No No
3 70 Right I No 500 10 No No
4 54 Right II No 700 35 30 min Yes
5 75 Right II No 650 10 No No
6 79 Right II No 600 20 15 min No
7 52 Left II No 450 17 15 min No
8 71 Right II No 200 15 10 min No
9 56 Right II No 200 15 No No
10 73 Right II No 200 20 15 min No
11 66 Right II No 200 15 No No
12 64 Right III Yes 1100 35 min No
13 58 Right II No 300 10 No No
14 62 Right I No 250 9 15 min No
15 60 Right II No 500 15 20 min No
198 M. Gallucci et al. / European Urology 45 (2004) 194–202
thrombus. Peri-renal fat resulted infiltrated by the tumorin 8 of the 15 cases. The synchronously resectedpulmonary lesion in the only Level III lesion resultedas a distant metastases from renal cell carcinoma. Noneof the patients were lost at follow-up. After a meanfollow-up of 53.9 (5–100) months one patient died 9months postoperatively for the disease because of theappearance of multiple bilateral pulmonary metastases.Autopsy did not reveal tumoral caval recurrence. All theremaining 14 patients (93.3%) are alive; two patientsshowed at follow-up distant metastases (lung, lung þbone), 12 patients are free of disease. MRI and USDoppler imaging showed the presence of an adequateiliac and caval flow in all cases.
5. Discussion
Caval thrombosis is a relatively common eventoccurring in about 10% of patients affected by renaltumor [1–10]. Extension does not take place by vas-cular invasion but via tumor progression inside thelumen of the renal vein and subsequently of the IVC.Caval thrombosis is not considered a contraindicationto radical surgical treatment; on the contrary surgicalremoval of the tumor and the thrombus, improves theprognosis [3,6,7,27–34], even in the presence of distantmetastases [8,35]. Five-year survival rates of patientswith renal tumor and caval thrombosis undergoingradical surgery range from 25% to 64% [3,31–35,38,40]. The validity of this treatment in presenceof disease extension to perinephric tissues and regionalnodes remains unclear [3,6–8,29–35,37,38,40,41].Despite the oncological effectiveness, surgical treat-ment of patients with a cephalic thrombus’ extensionabove the suprahepatic tract of the IVC (Level II and IIIlesions) is affected by significant rates of morbidity andmortality [1,3,6,7,18,28,33,35–38]. In the past severaldifferent surgical approaches to Level II–III cavalthrombosis were proposed to improve perioperativeresults. Only surgical approaches including largecavotomy, usually with cardio-circulatory arrest, sig-nificantly lowered mortality rates [2,42–45] reducingblood losses, thrombus fragmentation and pulmonaryembolism. Retro-hepatic IVC is a complex anatomicalregion. As a consequence, the surgical removalof a thrombus extended to this tract is a high-riskprocedure requiring an effective complete surgicalcontrol of the vessel. The shortness of the main supra-hepatic veins, the presence of hyper-vascularized tissueand of a variable number of accessory suprahepaticveins are the causes of the strict anatomical connectionbetween the IVC and the posterior margin of the liver.
In addition, the caval wall in this portion is fragile; inspite of several attempts [46–58] a systematic classi-fication of accessory suprahepatic veins has never beenachieved because of an extreme variability of number,diameter and site of confluence in the IVC. Theremoval of a thrombus extended to this portion ofthe IVC without an adequate control can be the causeof two undesirable events: thrombus fragmentationwith possible pulmonary embolism and uncontrollablehemorrhages due to lumbar, adrenal and suprahepaticveins bleeding. Tumor fragmentation is a well-described life-threatening event that can determinethrombus’s detachment and massive pulmonary embo-lism. ‘‘Blind’’ removal of the thrombus can determinean intraluminal persistence of a thrombus’ fractionwith possible postoperative embolisms and early dis-ease’s recurrence. According to previous papers, ourexperience confirmed that surgical strategy and peri-operative results radically change according to thecephalic extension of the thrombus. An infrahepaticthrombus (Level I) can be safely removed via a com-pletely abdominal isolation of the IVC, clamping andcavotomy. On the other hand, a thrombus extended tothe right atrium requires a mandatory large thoraco-abdominal access with cardio-circulatory arrest. Sur-gical approach to Level II caval thrombosis remains adebatable issue. Involvement of the retro-hepatic tractrepresents approximately 50% of all patients with cavalthrombosis from renal tumors. In the past surgicalremoval of these lesions was usually done throughan infrahepatic cavotomy and thrombus extraction withcephalic Foley’s catheter passages up to the thoracicIVC [38]. However, this technique allows an increasedrisk of pulmonary embolism and early recurrence ofdisease because of frequent tumor fragmentation.More recently, IVC has also been approached throughthoraco-abdominal access with [1,34,35,39,40,59] orwithout [31] use of cardio-circulatory arrest. An alter-native approach has been described by Ohwada whocompletely isolated the retro-hepatic IVC via the seg-mentectomy of the caudate lobe [60]. Thoraco-freno-laparotomy is now widely accepted for the treatmentof retro-hepatic thrombosis, but the use of a doublethoracic and abdominal access without complete liverisolation from the IVC seems not able to significantlydecrease perioperative risks. In a series of 53 patientswith caval thrombosis (Level II 24 cases, 45.3%)undergoing thoraco-abdominal approach in presenceof retro-hepatic lesions, Skinner reported an overallmortality (including Level I cases) of 13.2% and anaverage blood loss of 5466 ml [3]. Langenburgdescribed a similar approach in 1994 with an overallmortality of 8% [1]. In a series of 26 patients affected
M. Gallucci et al. / European Urology 45 (2004) 194–202 199

by retro-hepatic caval thrombosis undergoing thoraco-abdominal access, Nesbitt reported a significantlylower rate of mortality (overall 2.7%) and the reductionof intraoperative blood loss [35]. Surgical strategyreported by Nesbitt included in all cases a carefulmobilization of the liver and a large cavotomy asdescribed in the present study. The combined use ofthoraco-abdominal access and cardio-circulatory arrestfor the treatment of retro-hepatic and thoracic lesionshas also been recently suggested by other authors[3,5,18,28,32,33,35–37,39,59,61,62]. This approachallows minimal intraoperative blood loss with reducedrates of major morbidity and mortality. However, anincrease in invasivity and economical costs can beassumed. Chest opening can result more frequentlyin respiratory postoperative complications with delay’sof patient’s recovery and discharge. The present studyreports the results of a fully abdominal surgical tech-nique used for the treatment of patients affected byLevel II caval thrombosis. Our approach is directlyimported from liver transplant surgery. It includes thecomplete overturning of the liver and the isolation ofthe entire tract of the infra-, retro- and suprahepaticIVC as commonly used for the removal of both donorand recipient liver. Recently Ciancio showed that thistechnique can also be used for the removal of cavalthrombosis [63,64]. In presence of a retro-hepatic cavalthrombus, the isolation of the IVC from the liver offersthe surgeon the possibility to entirely isolate the tract ofIVC filled by the thrombus. After proximal and distalIVC and hepatic pedicle clamping, a large cavotomyincluding the entire thrombus is performed. At thismoment the surgeon can safely remove the entirethrombus, a small ‘‘buttonhole’’ of the caval wall closeto the renal vein confluence and the kidney. Minimalblood loss and the complete opening of the IVC allowto reduce the risk of thrombus fragmentation duringthe removal. In our experience no perioperative clin-ical, laboratoristic or instrumental signs of pulmonaryembolisms were observed. Perioperative mortality was
absent and macroscopic examination of all lesionsextended to the retro-hepatic IVC revealed no evidenceof rupture or fracture. The vein wall can be accuratelyexplored in a bloodless field. Moreover, blood loss canbe avoided by the careful section of all accessorysuprahepatic veins and the effective vascular controlof renal, adrenal, lumbar and major suprahepatic veins.During removal of Level II lesions we experienced amean blood loss of less than 500 ml, not significantlyhigher than observed for surgical treatment of Level Ithrombosis. In 2 of 10 Level II patients, the thrombusexceeded the confluence of the major suprahepaticveins and reached the intra-thoracic tract of the IVC.In this situation a thoraco-abdominal access withcardio-circulatory arrest has been proposed by severalauthors. In our experience, our surgical approach canbe safely performed even in presence of a thoracicextension of the thrombus. After detachment of thediaphragmatic peritoneum from the liver and completeisolation of the suprahepatic portion of the IVC, asmall incision of the pericaval diaphragmatic muscleis made and a thoracic window is created. By this waythe level of caval clamping can be further extended.According to our results, the avoidance of chest open-ing reduces length of postoperative stay and overallrecovery time of patients. Finally, our results sug-gested that a complete thrombus removal in absenceof fragmentation can also reduce tumoral cellsspread and intracaval recurrence of the disease. Thishypothesis seems to be confirmed by our follow-upresults. After a mean follow-up of 53.9 months 14/15patients (93.3%) are still alive; only 2 patients devel-oped distant metastases and 12 patients are alive anddisease free. Postoperative and long-term work-upnever showed intra-caval tumor recurrence. In con-clusion, our study confirms that careful detachmentof the IVC from the liver as commonly performed intransplant liver surgery is a safe and effective surgicalprocedure for patients affected by Level II cavalthrombosis.
References
[1] Langenburg SE, Blackbourne LH, Sperling JW, Buchanan SA,
Mauney MC, Kron IL, et al. Management of renal tumors involving
the inferior vena cava. J Vasc Surg 1994;20:385–8.
[2] Marshall VF, Middleton RG, Holswade GR, Goldsmith EI. Surgery
for renal cell carcinoma in the vena cava. J Urol 1970;103:414–20.
[3] Skinner DG, Pritchett TR, Lieskovsky G, Boyd SD, Stiles QR. Vena
caval involvement by renal cell carcinoma. Surgical resection
provides meaningful long-term survival. Ann Surg 1989;210:387–92.
[4] Skinner DG, Pfister RF, Colvin R. Extension of renal cell carcinoma
into the vena cava: the rationale for aggressive surgical management.
J Urol 1972;107:711–6.
[5] Babu SC, Mianoni T, Shah PM, Goyal A, Choudhury M, Eshghi M,
et al. Malignant renal tumor with extension to the inferior vena cava.
Am J Surg 1998;176:137–9.
[6] Neves RJ, Zinck H. Surgical treatment of renal cancer with vena cava
extension. Br J Urol 1987;59:390–5.
[7] O’Donohoe MK, Flanagan F, Fitzpatrick JM, Smith JM. Surgical
approach to inferior vena caval extension of renal carcinoma. Br J
Urol 1987;60:492–6.
[8] Slaton JW, Balbay MD, Levy DA, Pisters LL, Nesbitt JC, Swanson
DA, et al. Nephrectomy and vena caval thrombectomy in patients
with metastatic renal cell carcinoma. Urology 1997;50:673–7.
200 M. Gallucci et al. / European Urology 45 (2004) 194–202
[9] Emmott RC, Hayne LR, Katz IL, Scribner RG, Tawes Jr RL.
Prognosis of renal cell carcinoma with vena caval and renal vein
involvement. An update. Am J Surg 1987;154:49–53.
[10] Ljungberg B, Stenling R, Osterdahl B, Farrelly E, Aberg T, Roos G.
Vein invasion in renal cell carcinoma: impact on metastatic behavior
and survival. J Urol 1995;154:1681–4.
[11] Berg AA. Malignant hypernephroma of the kidney. Its clinical course
and diagnosis, with a description of the author’s method of radical
operative cure. Surg Gynecol Obstet 1913;17:463.
[12] Rehn E. Gefasskomplikationen und ihre Beherrschung bei dem
Hypernephrom. Z Urol Chir 1922;10:326.
[13] Walters W, Pirestley JT. Survey of the inferior vena cava. Clinical
and experimental studies. Ann Surg 1934;99:167.
[14] Myers GH, Fehrenbaker LG, Kelelis PP. Prognostic significance of
renal vein invasion by hypernephroma. J Urol 1968;100:420.
[15] Ney C. Thrombosis of the inferior vena cava associated with
malignant renal tumors. J Urol 1946;55:583.
[16] McDonald JR, Priestly JT. Malignant tumours of the kidney: surgical
and prognostic significance of tumor thrombosis of the renal vein.
Surg Gynecol Obstet 1943;77:295.
[17] Svane S. Tumor thrombus of the inferior vena cava resulting from
renal carcinoma. A report of 12 autopsied cases. Scand J Urol
Nephrol 1969;3:245–56.
[18] Sosa RE, Muecke EC, Vaughan Jr ED, McCarron Jr JP. Renal cell
carcinoma extending into the inferior vena cava: the prognostic
significance of the level of vena caval involvement. J Urol 1984;
132:1097–100.
[19] Schefft P, Novick AC, Straffon RA, Stewart BH. Surgery for renal
cell carcinoma extending into the inferior vena cava. J Urol 1978;
120:28–31.
[20] Cherrie RJ, Goldman DG, Lindner A, deKernion JB. Prognostic
implications of vena caval extension of renal cell carcinoma. J Urol
1982;128:910–2.
[21] Kearney GP, Waters WB, Klein LA, Richie JP, Gittes RF. Results of
inferior vena cava resection for renal cell carcinoma. J Urol
1981;125:769–73.
[22] Dekernion JB, Berry D. The diagnosis and treatment of renal cell
carcinoma. Cancer 1980;45:1947–56.
[23] Dekernion JB, Ramming KP, Smith RB. The natural history of
metastatic renal cell carcinoma: a computer analysis. J Urol
1978;120:148–52.
[24] Cummings KB, Li WI, Ryan JA, Horton WG, Paton RR.
Intraoperative management of renal cell carcinoma with supradiaph-
ragmatic caval extension. J Urol 1979;122:829–32.
[25] Heney NM, Nocks BN. The influence of perinephric fat involvement
on survival in patients with renal cell carcinoma extending into
inferior vena cava. J Urol 1982;128:18–20.
[26] Abdelsayed MA, Bissada NK, Finkbeiner AE, Redman JF. Renal
tumors involving the inferior vena cava: plan for management. J Urol
1978;120:153–5.
[27] Sogani PC, Herr HW, Bains MS, Whitmore Jr WF. Renal cell
carcinoma extending into inferior vena cava. J Urol 1983;130:660–3.
[28] Libertino JA, Zinman L, Watkins Jr E. Long-term results of resection
of renal cell cancer with extension into inferior vena cava. J Urol
1987;137:21–4.
[29] Vale JA, Hendry WF, Kirby RS, Whitfield HN, Lumley JS.
Diagnostic and surgical aspects of renal carcinoma with involvement
of the inferior vena cava. Br J Urol 1991;68:345–8.
[30] Pagano F, Dal Bianco M, Artibani W, Pappagallo G, Prayer Galetti T.
Renal cell carcinoma with extension into the inferior vena cava:
problems in diagnosis, staging and treatment. Eur Urol 1992;22:
200–3.
[31] Tongaonkar HB, Dandekar NP, Dalal AV, Kulkarni JN, Kamat MR.
Renal cell carcinoma extending to the renal vein and inferior vena
cava: results of surgical treatment and prognostic factors. J Surg
Oncol 1995;59:94–100.
[32] Hatcher PA, Anderson EE, Paulson DF, Carson CC, Robertson JE.
Surgical management and prognosis of renal cell carcinoma invading
the vena cava. J Urol 1991;145:20–3.
[33] Montie JE, el Ammar R, Pontes JE, Medendorp SV, Novick AC,
Streem SB, et al. Renal cell carcinoma with inferior vena cava tumor
thrombi. Surg Gynecol Obstet 1991;173:107–15.
[34] Swierzewski DJ, Swierzewski MJ, Libertino JA. Radical nephrect-
omy in patients with renal cell carcinoma with venous, vena cava,
and atrial extension. Am J Surg 1994;168:205–9.
[35] Nesbitt JC, Soltero ER, Dinney CP, Walsh GL, Schrump DS, Swanson
DA, et al. Surgical management of renal cell carcinoma with inferior
vena cava tumor thrombus. Ann Thorac Surg 1997;63:1592–600.
[36] Bintz M, Cogbill TH, Klein AS. Surgical treatment of renal cell
carcinoma involving the inferior vena cava. J Vasc Surg 1987;6:566–71.
[37] Pritchett TR, Lieskovky G, Skinner DG. Extension of renal cell
carcinoma into the vena cava: clinical review and surgical approach.
J Urol 1986;135:460–4.
[38] Suggs WD, Smith III RB, Dodson TF, Salam AA, Graham Jr SD.
Renal cell carcinoma with inferior vena caval involvement. J Vasc
Surg 1991;14:413–8.
[39] Stewart JR, Carey JA, McDougal WS, Merrill WH, Koch MO,
Bender Jr HW. Cavoatrial tumor thrombectomy using cardiopul-
monary bypass without circulatory arrest. Ann Thorac Surg
1991;51:717–21.
[40] Kuczyk MA, Bokemeyer C, Kohn G, Stief CG, Machtens S, Truss
M, et al. Prognostic relevance of intracaval neoplastic extension for
patients with renal cell cancer. Br J Urol 1997;80:18–24.
[41] Glaze AA, Novick AC. Long-term follow-up after surgical treatment
for renal cell carcinoma extending into the right atrium. J Urol
1996;155:448–50.
[42] Vaislic CD, Puel P, Grondin P, Vargas A, Thevenet A, Fontan F, et al.
Cancer of the kidney invading the vena cava and heart. Results after
11 years of treatment. J Thorac Cardiovasc Surg 1986;91:604–9.
[43] Marshall FF, Reitz BA. Supradiaphragmatic renal cell carcinoma
tumor thrombus: indications for venal caval reconstruction with
pericardium. J Urol 1985;133:266–8.
[44] Marshall FF, Reithz BA, Diamand DA. A new technique for
management of renal cell carcinoma involving the right atrium:
hypothermia and cardiac arrest. J Urol 1984;131:103–7.
[45] Novick AC, Cosgrove DM. Surgical approach for removal of renal
cell carcinoma extending into the vena cava and the right atrium. J
Urol 1980;123:947–50.
[46] Dell’Isola C, Tucci GF. Ricerca anatomo-chirurgica sull’isolamento
del segmento retroepatico della vena cava inferiore. Gior Chir
1993;14:7–11.
[47] Camargo AM, Teixeira GG, Ortale JR. Anatomy of the ostia venae
hepaticae and the retrohepatic segment of the inferior vena cava. J
Anat 1996;188:59–64.
[48] Gibson JG. The hepatic veins in man and their sphincter
mechanisms. J Anat 1959;93:368–79.
[49] Goldsmith NA, Woodburne RT. The surgical anatomy pertaining to
liver resection. Surg Gynecol Obstet 1957;105:310–8.
[50] Kennedy PA, Madding GF. Surgical anatomy of the liver. Surg Clin
North Am 1977;57:233–44.
[51] Nakamura S, Tsuzuki T. Surgical anatomy of the hepatic veins and
the inferior vena cava. Surg Gynecol Obstet 1981;152:43–50.
[52] Chevallier JM, Hannoun L. Anatomic based for liver transplantation.
Surg Radiol Anat 1991;13:7–16.
[53] Chevallier JM. Le carrefour hepatico-cave: aspects anatomo-
chirurgicaux actuels. J Chir 1986;123:689–99.
[54] Rex H. Beitrage zur morphologie des saugerleber. Morphol Jahrd
1888;14:517–617.
[55] Huard P, Meyer MJ. Recherches sur l’anatomie chirurgicale du foie.
Trav Inst Anat Ecole Med Indochine Hanoı 1933;153–84.
[56] Coinaud C. Le foie, etudes anatomiques et chirurgicales. Paris:
Masson; 1956.
M. Gallucci et al. / European Urology 45 (2004) 194–202 201

[57] Chevallier JM. Anatomic basis of vascular exclusion of the liver.
Surg Radiol Anat 1988;10:187–94.
[58] Chang RWH, Shan-Quan S, Yen WWC. An applied anatomical study
of the ostia venae hepaticae and the retrohepatic segment of the
inferior vena cava. J Anat 1989;164:41–7.
[59] Hedderich GS, O’Connor RJ, Reid EC, Mulder DS. Caval tumor
thrombus complicating renal cell carcinoma: a surgical challenge.
Surgery 1987;102:614–21.
[60] Ohwada S, Satoh Y, Nakamura S, Tanahasi Y, Otani Y, Lino Y, et al.
Left-sided approach to renal cell carcinoma tumor thrombus
extending into suprahepatic inferior vena cava by resection of the
left caudate lobe. Angiology 1997;48:629–35.
[61] Giuliani L, Giberti C, Martorana G, Rovida S. Surgical management
of renal cell carcinoma with vena cava tumor thrombus. Eur Urol
1986;12:145–50.
[62] Marshall FF, Reithz BA. Technique for removal of renal cell
carcinoma with suprahepatic vena caval tumor thrombus. Urol Clin
North Am 1986;13:551–7.
[63] Ciancio G, Hawke C, Soloway M. The use of liver transplant
techniques to aid in the surgical management of urological tumors. J
Urol 2000;164:665–72.
[64] Ciancio G, Soloway M. Renal cell carcinoma invading the hepatic
veins. Cancer 2001;92:1836–42.
202 M. Gallucci et al. / European Urology 45 (2004) 194–202

![CONCOMITANT SYMPTOMS & REMEDIEShomoeopathybooks.com/Repertory of Concomitant Symptoms-1/Repe… · CONCOMITANT SYMPTOMS & REMEDIES :- GRAPH., KALI FACE :[ABDOMEN] : ... aconite if](https://static.fdocuments.in/doc/165x107/5aac6f627f8b9a8f498d0756/concomitant-symptoms-reme-of-concomitant-symptoms-1repeconcomitant-symptoms.jpg)