
Liu Advances in ID 4-12-14.ppt - UCSF Medical Education
17
4/16/2014 1 Skin and Soft Tissue Infections: MRSA and Beyond Catherine Liu, M.D. Assistant Professor of Clinical Medicine Division of Infectious Diseases University of California, San Francisco Overview • Purulent SSTI • Non‐purulent SSTI • Recurrent SSTI • Animal Bites • Necrotizing soft tissue infections • Potpourri of cases Case 1 20 y/o M presents with 3 days of an enlarging, painful lesion on his L arm that he attributes to a spider bite T 36.9 BP 118/70 P 82 What is the appropriate management of this patient? A. Incision and drainage alone B. Incision and drainage plus cephalexin C. Incision and drainage plus TMP‐SMX D. Cephalexin E. TMP‐SMX
Transcript of Liu Advances in ID 4-12-14.ppt - UCSF Medical Education

4/16/2014
1
Skin and Soft Tissue Infections: MRSA and Beyond
Catherine Liu, M.D.Assistant Professor of Clinical Medicine
Division of Infectious DiseasesUniversity of California, San Francisco
Overview
• Purulent SSTI
• Non‐purulent SSTI
• Recurrent SSTI
• Animal Bites
• Necrotizing soft tissue infections
• Potpourri of cases
Case 1
20 y/o M presents with 3 days of an enlarging, painful lesion on his L arm that he attributes to a spider bite
T 36.9 BP 118/70 P 82
What is the appropriate management of this patient?
A. Incision and drainage alone
B. Incision and drainage plus cephalexin
C. Incision and drainage plus TMP‐SMX
D. Cephalexin
E. TMP‐SMX

4/16/2014
2
What is the appropriate management of this patient?
A. Incision and drainage alone
B. Incision and drainage plus cephalexin
C. Incision and drainage plus TMP‐SMX
D. Cephalexin
E. TMP‐SMX
Abscesses: Do antibiotics provide benefit over I&D alone?
0%
20%
40%
60%
80%
100%
Rajendran '07 Duong '09 Schmitz '10
% patients cured
Placebo
Antibiotic
p=.25 p=.12 p=.52
Cephalexin TMP-SMX TMP-SMX
1Rajendran P AAC 2007; 2Schmitz G Ann Emerg Med 2010; 3Duong M Ann Emerg Med 2009
Antibiotic therapy is recommended for abscesses associated with:
• Severe, extensive disease, rapidly progressive with associated cellulitis or septic phlebitis
• Signs & sx of systemic illness
• Associated comorbidities, immunosuppressed
• Extremes of age
• Difficult to drain area (e.g. face, hand, genitalia)
• Failure of prior I&D
Liu C Clin Inf Dis 2011
Microbiology of Purulent SSTIs: ER Patients
Moran G NEJM 2006; Talan D Clin Inf Dis 2011
2004 2008

4/16/2014
3
Outpatient purulent cellulitis: Empiric Rx for MRSA
MRSA MSSA ‐hemolyticstrep
Comments
TMP/ SMX1‐2 DS tab BID
+ + ‐/? Low rates of resistance
Doxycycline, Minocycline100 mg BID
+ + ‐ Low rates of resistance
Clindamycin300‐450 TID
+/‐ + + C. diff risk
Linezolid600 mg BID
+ + + Most expensive option
Case 2
28 year old woman with erythema of her left foot x 48 hours. No purulent drainage, exudate or abscess.
T 37.0 BP 132/70 P 78 Eells SJ et al Epidemiology and Infection 2010
What is the appropriate management of this patient?
A. Clindamycin 300 mg PO TID
B. Cephalexin 500 mg QID
C. Cephalexin 500 mg QID and TMP/ SMX 2 DS tab PO bid
What is the appropriate management of this patient?
A. Clindamycin 300 mg PO TID
B. Cephalexin 500 mg QID
C. Cephalexin 500 mg QID and TMP/ SMX 2 DS tab PO bid

4/16/2014
4
Nonpurulent Cellulitis‐hemolytic strep vs. S. aureus?
• Prospective study, hospitalized patients (N=248)
Methods
– Acute and convalescent titers (ASO and anti‐DNaseB)
– Rx with ‐lactam antibiotics (cefazolin/oxacillin)
Results
– 73% due to ‐hemolytic strep; 27% no cause identified
– 96% response rate to ‐lactam antibiotic
Jeng A Medicine 2010
Cephalexin vs. Cephalexin + TMP‐SMX in patients with Uncomplicated Cellulitis
Pallin D Clin Inf Dis 2013
N=146
p=.66 p=.62p=1.0
Outpatient nonpurulent cellulitis: Empiric Rx for ‐hemolytic streptococci, +/‐MRSA
MRSA MSSA ‐hemolytic strep
Penicillin V‐K500 mg QID/ Amoxicillin 500 mg TID
‐ Rare +/‐ ‐ ‐ +
Dicloxacillin500 mg QID
‐ + +
Cephalexin500 mg QID
‐ + +
Clindamycin300‐450 mg TID
+/‐ + +
Linezolid600 mg BID
+ + +
Microbiology of SSTI: Hospitalized Patients
Jenkins T Clin Inf Dis 2010

4/16/2014
5
Antibiotic Utilization Among Hospitalized Patients with SSTI: Baseline
Jenkins T Arch Intern Med 2011
N=169
Antibiotic Utilization Among Hospitalized Patients with SSTI: Post‐QI Intervention
Jenkins T Arch Intern Med 2011
*Recommended empiric vanco*Discouraged gram neg/ anaerobic*Suggested Rx for 7 days
p<.001
Other Outcomes
• Median duration of Rx (13 vs. 10d, p<.001)
• No differences in clinical outcomes
– Clinical failure (7.7% vs. 7.4%, p=NS)
– Recurrent infection
– Rehospitalization due to SSTI
– Length of hospital stay
Jenkins T Arch Intern Med 2011
FDA Approved Agents for Treatment of Complicated SSTI
Antibiotic Adult
Vancomycin 15‐20 mg/kg IV Q8‐12
Linezolid 600 mg PO/ IV BID
Daptomycin 4 mg/kg IV QD
Telavancin 10 mg/kg IV QD
Ceftaroline 600 mg IV Q12
Tigecycline 100 mg IV x 1, then 50 IV Q12
4/16/2014
6
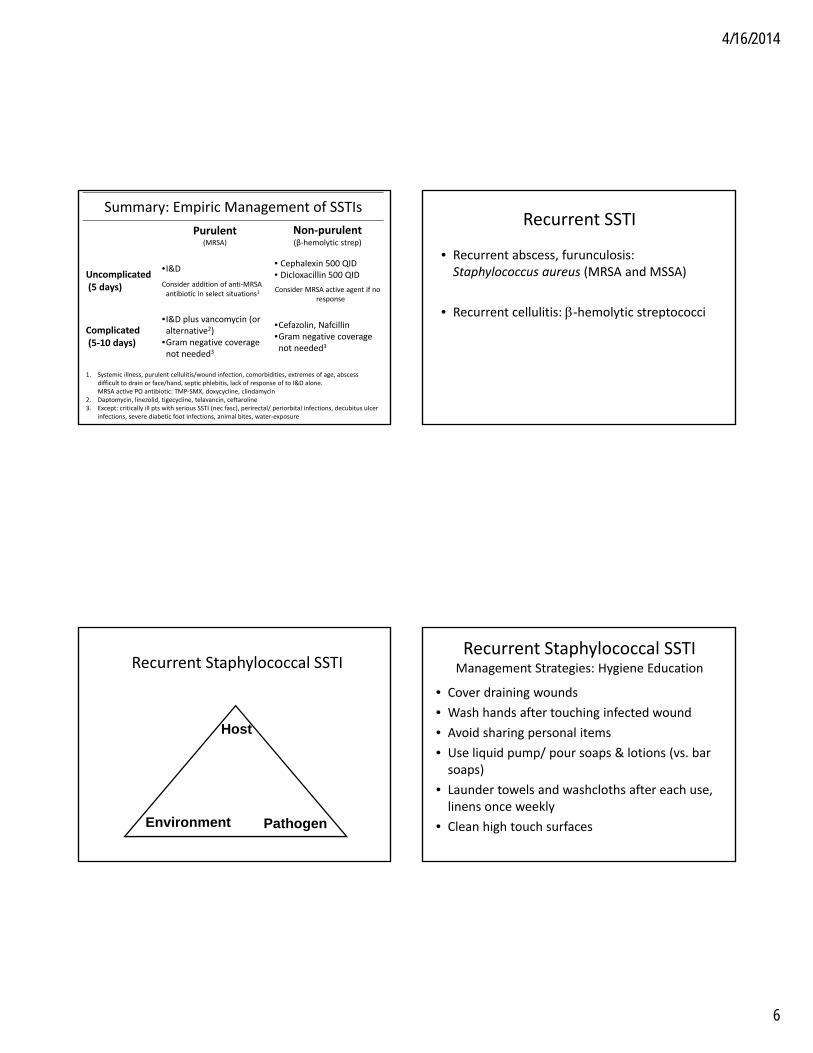
Summary: Empiric Management of SSTIs
Purulent(MRSA)
Non‐purulent(β‐hemolytic strep)
Uncomplicated(5 days)
•I&D
Consider addition of anti‐MRSA antibiotic in select situations1
• Cephalexin 500 QID• Dicloxacillin 500 QID
Consider MRSA active agent if no response
Complicated(5‐10 days)
•I&D plus vancomycin (or alternative2)
•Gram negative coverage not needed3
•Cefazolin, Nafcillin•Gram negative coverage not needed3
1. Systemic illness, purulent cellulitis/wound infection, comorbidities, extremes of age, abscess difficult to drain or face/hand, septic phlebitis, lack of response of to I&D alone. MRSA active PO antibiotic: TMP‐SMX, doxycycline, clindamycin
2. Daptomycin, linezolid, tigecycline, telavancin, ceftaroline3. Except: critically ill pts with serious SSTI (nec fasc), perirectal/ periorbital infections, decubitus ulcer
infections, severe diabetic foot infections, animal bites, water‐exposure
Recurrent SSTI
• Recurrent abscess, furunculosis: Staphylococcus aureus (MRSA and MSSA)
• Recurrent cellulitis: ‐hemolytic streptococci
Recurrent Staphylococcal SSTI
Host
Environment Pathogen
Recurrent Staphylococcal SSTIManagement Strategies: Hygiene Education
• Cover draining wounds
• Wash hands after touching infected wound
• Avoid sharing personal items
• Use liquid pump/ pour soaps & lotions (vs. bar soaps)
• Launder towels and washcloths after each use, linens once weekly
• Clean high touch surfaces

4/16/2014
7
Recurrent Staphylococcal SSTIManagement Strategies: Decolonization
• Mupirocin: 5 days/ mth x 1 year↓ recurrent SSTI among 34 MSSA nasal carriers
• Chlorhexidine (CHG) washes alone: Not effective
• Mupirocin + CHG: Household >> individual decol
• Bleach baths: No benefit vs hygiene education
• Oral antibiotics: Mupirocin + hexachlorophene + TMP‐SMX or doxy x 10 d ↓ recurrent MRSA SSTI (31 pts); Anecdotal experience with rifampin‐based therapy
Raz Arch Intern Med 1996; Whitman ICHE 2010; Fritz ICHE 2012; Kaplan CID 2013; Miller AAC 2012
Mupirocin vs Mupirocin + Chlorhexidine vs Mupirocin + Bleach
N=229
Fritz S Inf Control Hosp Epi 2011*All groups received hygiene education
*
Household vs. Individual Decolonization w/Mupirocin + CHG x 5 days
Fritz S Clin Inf Dis 2012
p=.12 p=.02 p=.008 p=.02
*All groups received hygiene education
Bleach Baths + Hygiene vs. Hygiene
Bleach Baths: Twice weekly for 15 minutes x 3 monthsKaplan S Clin Inf Dis 2013

4/16/2014
8
Recurrent Streptococcal CellulitisManagement Strategies
• Most patients have predisposing factor:
– Obesity, lymphedema, venous insufficiency, prior trauma/ surgery to area, tinea pedis
• Management approach:
– Treat underlying conditions whenever possible (e.g. compressive stockings, Rx interdigital maceration/ tinea, emollients to avoid dryness/ cracking, diuretics)
– Prophylactic antibiotics if frequent recurrence• Penicillin VK 250 mg PO twice daily
• Benzathine PCN 1.2 MU IM every 2‐4 weeks
Stevens D Clin Inf Dis 2005
PCN 250 BID vs. Placebo For Prevention of Recurrent Cellulitis
Thomas K NEJM 2013
N=274
Case 3
• 21 yo M is tossing a ball in Golden Gate Park with a friend. As he goes after the ball, he passes close to a dog that was resting in the shade with his owner. The dog jumps up and bites him on the leg inflicting several wounds on the calf.
In addition to wound care, what is the appropriate management of this patient?
A. No antibiotic prophylaxis needed
B. Antibiotic prophylaxis with clindamycin
C. Antibiotic prophylaxis with amoxicillin/ clavulanate
D. Administer rabies immunoglobulin and rabies vaccine for post‐exposure prophylaxis
E. C and D

4/16/2014
9
In addition to wound care, what is the appropriate management of this patient?
A. No antibiotic prophylaxis needed
B. Antibiotic prophylaxis with clindamycin
C. Antibiotic prophylaxis with amoxicillin/ clavulanate
D. Administer rabies immunoglobulin and rabies vaccine for post‐exposure prophylaxis
E. C and D
• Average 5 organisms (range 0‐16) per wound
Dogs Cats
Pasturella sp 50% 75%
Streptococcus sp. 46% 46%
Staphylococcus aureus 20% 4%
Anaerobes mixed w/ aerobes 48% 63%
Anaerobes alone 1% 0%
Talan D NEJM 1999
Microbiology of Animal Bites:What’s in their mouth and on your skin
• What you want to use but won’t work…– cephalexin
–dicloxacillin
– clindamycin
• What works…
–Amoxicillin/ penicillin
–doxycycline
– fluoroquinolones
Antibiotic Coverage for Pasteurella Animal bites
• Empiric treatment regimens
– Amoxicillin/clavulanic acid +/‐ anti‐MRSA
– Pen allergy: cipro + clindamycin or moxifloxacin
• Prophylaxis?
– Moderate‐severe bites
– Deep puncture wounds (i.e. cat bites, 50% infection risk)
– Bites involving face, hands
– Immunocompromised (splenectomized)

4/16/2014
10
Rabies – what type of bites are high risk?
Animal TypeEvaluation and
disposure of animalPost‐exposure prophylaxis
Dog, cats, ferrets
Suspected/confirmed rabid
Healthy
Animal lost
Prophylaxis
10 days observation/test
Contact DPH
Skunk, raccoons, foxes, bats
Regarded as rabid unless proven negative by lab test
Immediate prophylaxis
Livestock, small rodents, rabbits, large rodents
Consider individuallyAlmost never require prophylaxis
http://www.cdc.gov/rabies/resources/contacts.html
Case 4
• 39 yo M IVDU with L leg pain and erythema, worsening pain and swelling x 48 hours
• T 39.2 P 120 BP 90/60 R22 94%RA
• 18>38<90, Cr 2.4
What would your empiric therapy be in this case?
A. Vancomycin and piperacillin‐tazobactam
B. Vancomycin and piperacillin‐tazobactam, and
clindamycin
C. Call surgery, vancomycin and clindamycin
D. Call surgery, vancomycin, piperacillin‐
tazobactam, clindamycin
What would your empiric therapy be in this case?
A. Vancomycin and piperacillin‐tazobactam
B. Vancomycin and piperacillin‐tazobactam, and
clindamycin
C. Call surgery, vancomycin and clindamycin
D. Call surgery, vancomycin, piperacillin‐
tazobactam, clindamycin

4/16/2014
11
Cultures return positive for Group A streptococci. What changes, if any, would
you make to your antibiotics?
A. No changes, as patient remains critically ill, continue vancomycin, pip‐tazo, clindamycin
B. Vancomycin
C. Penicillin
D. Penicillin and clindamycin
Cultures return positive for Group A streptococci. What changes, if any, would
you make to your antibiotics?
A. No changes, as patient remains critically ill, continue vancomycin, pip‐tazo, clindamycin
B. Vancomycin
C. Penicillin
D. Penicillin and clindamycin
Necrotizing skin and soft infections
• Monomicrobial: Group A strep > S. aureus, Clostridia, gram neg rare
• Polymicrobial: gram +, gram ‐, anaerobes
– associated w/ abdominal surgery, decub ulcers, IVDU, spread from GU tract
Risk Factors for Necrotizing SSTI
• IVDU
• Diabetes
• Obesity
• Chronic immunosuppression
• Often no precipitating factor
Anaya DA. Clin Infect Dis. 2007

4/16/2014
12
Why is early diagnosis so important?
Wong CH. Jour of Bone and Joint Surg. 2003
Mortality rate: > 30%
Necrotizing soft tissue infections: physical findings on admission
Wong CH. Jour of Bone and Joint Surg. 2003
0
10
20
30
40
50
60
70
80
90
100
% of patients
Late findings
n=89; 14% dx with nec fasc on admit
Necrotizing soft tissue infections: radiographic techniques
• Plain films
– Low sensitivity
– Helpful if gas present
• CT and ultrasound
– May identify other Dx (abscess)
• MRI
– Enhanced sensitivity, low specificity
Dufel S J Fam Pract. 2006
Special consideration for the treatment of invasive Group A strep?
• Protein synthesis inhibitors (clindamycin)
– Decrease toxin production
– Not affected by inoculum size
– Acts on bacteria in stationary phase of growth
• IVIG (in toxic shock syndrome)– May be able to bind toxin

4/16/2014
13
Is IVIG useful in strep toxic shock syndrome?
Observational Study – ‘99•Improved 7 day survival and 30 day survival•But…Cases > Controls
– Clindamycin (95% vs. 55%, P=0.01)– Surgery (67% vs. 38%, P=0.04)
Double‐Blinded RCT – ‘03•Ended early due to poor enrollment, 21 patients
– Mortality (36% placebo vs. 10% IVIG, p=NS)
– 13 pts with nec fasc‐ no in time to no further progression of necrotizing fasciitis
Kaul R. Clin Infect Dis. 1999; Darenberg J. Clin Infect Dis. 2003
Summary: Management of necrotizing skin and soft tissue infections
• Early surgical consult/ intervention
• Empiric antimicrobial therapy– Piperacillin/tazobactam or carbapenem (group A strep, other gram pos, gram negs and anaerobes)plus
– Clindamycin(group A strep – toxin inhibition)plus
– Vancomycin(MRSA)
Case 5
53 yo M ER physician with 9 day h/o progressive cellulitis of L forearm.
Initially noted a pustule self I&D, started keflex+ clindamycin x 4 days.
Progressive erythema and drainage. Started IV vanco+ ceftriaxone, no improvement after 3 days
Further history…
• History of chronic “benign” neutropenia
• 3 weeks ago, trip to Arizona where cleared brush in order to replace a water drip line and scraped his arm
• 2 weeks ago, worked in home (Merced) vegetable garden clearing eggplant and pepper brushes
• 7 days ago, cleaned his fish tank
• No animal or tick bites
• Only recent travel to Arizona

4/16/2014
14
All of the following are possible causes of his infection EXCEPT:
A. Mycobacterium marinum
B. Coccidioides immitis
C. Nocardia brasiliensis
D. Brucella melitensis
E. Sporothrix schenkii
All of the following are possible causes of his infection EXCEPT:
A. Mycobacterium marinum
B. Coccidioides immitis
C. Nocardia brasiliensis
D. Brucella melitensis
E. Sporothrix schenkii
Gram stain from wound culture
Nocardia brasiliensis
Nocardia
• Soil inhabitant
• Worldwide distribution
• Incubation period: <1‐6 weeks
• Often with mild systemic symptoms
• Nocardia brasiliensis > asteroides for cutaneous disease
• Diagnosis: biopsy and culture– Partially acid‐fast, gram variable branching rods.
• Treatment: TMP‐SMX x 4‐6 months

4/16/2014
15
26 yo M with 6 week history of R hand papule ulcer
Multiple visits to ED and urgent care, Receives several courses of abx, noimprovement Leishmania panamensis
Which of the following reflect true infectious cellulitis?

4/16/2014
16
Which of the following reflect true infectious cellulitis?
David Derm Online J 2011
Which of the following reflect true infectious cellulitis?
David Derm Online J 2011
B
Which of the following reflect true infectious cellulitis?
David Derm Online J 2011
Which of the following reflect true infectious cellulitis?
David Derm Online J 2011
4/16/2014
17
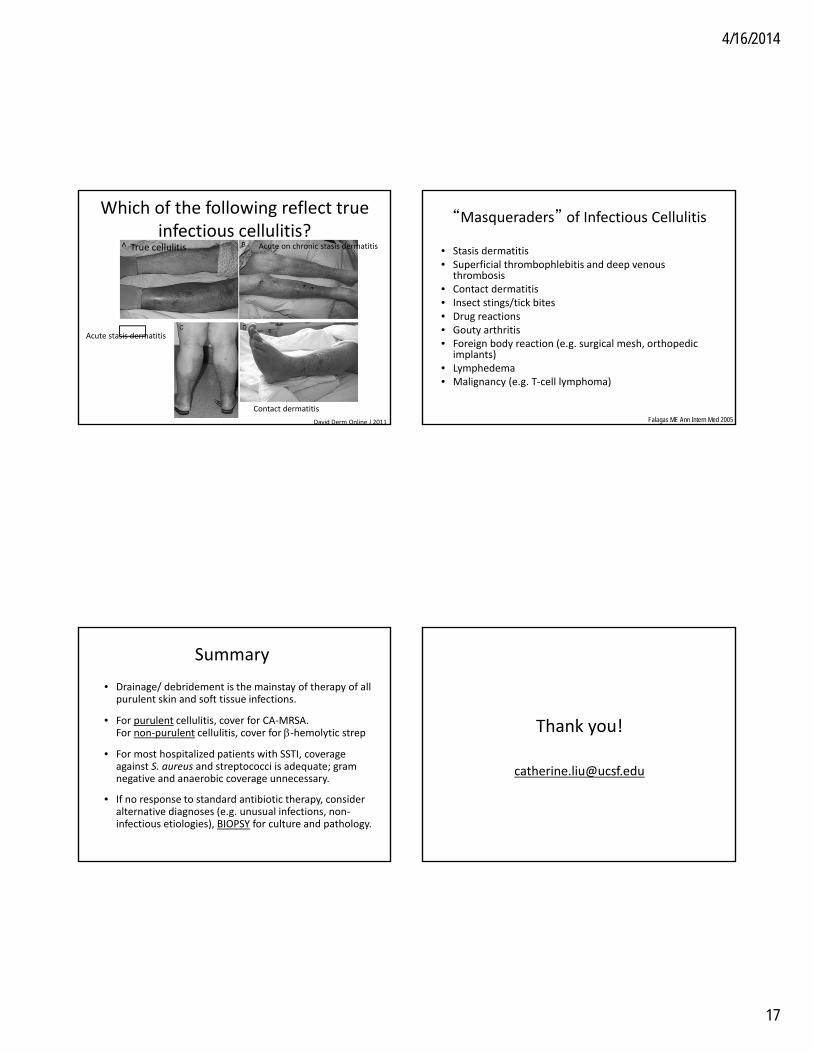
Which of the following reflect true infectious cellulitis?
True cellulitis Acute on chronic stasis dermatitis
Acute stasis dermatitis
Contact dermatitis
David Derm Online J 2011
“Masqueraders” of Infectious Cellulitis
• Stasis dermatitis• Superficial thrombophlebitis and deep venous
thrombosis• Contact dermatitis• Insect stings/tick bites• Drug reactions• Gouty arthritis• Foreign body reaction (e.g. surgical mesh, orthopedic
implants)• Lymphedema• Malignancy (e.g. T‐cell lymphoma)
Falagas ME Ann Intern Med 2005
Summary
• Drainage/ debridement is the mainstay of therapy of all purulent skin and soft tissue infections.
• For purulent cellulitis, cover for CA‐MRSA. For non‐purulent cellulitis, cover for ‐hemolytic strep
• For most hospitalized patients with SSTI, coverage against S. aureus and streptococci is adequate; gram negative and anaerobic coverage unnecessary.
• If no response to standard antibiotic therapy, consider alternative diagnoses (e.g. unusual infections, non‐infectious etiologies), BIOPSY for culture and pathology.
Thank you!


















