
Listeriosis and Colibacillosis
50
Listeriosis & Colibacillosis Muhammad Asfar Zaman Roll no. 106
-
Upload
muhammad-asfar-zaman -
Category
Education
-
view
34 -
download
3
Transcript of Listeriosis and Colibacillosis

Listeriosis & ColibacillosisMuhammad Asfar ZamanRoll no. 106Muhammad Asfar ZamanRoll no. 106


Introduction
• Listeriosis, a serious infection caused by eating food contaminated with the bacterium Listeria-Monocytogenes.
• Listeriosis primarily causes infections of the central nervous system.
• Common name is “Circling disease”.
Listeria Monocytogenes
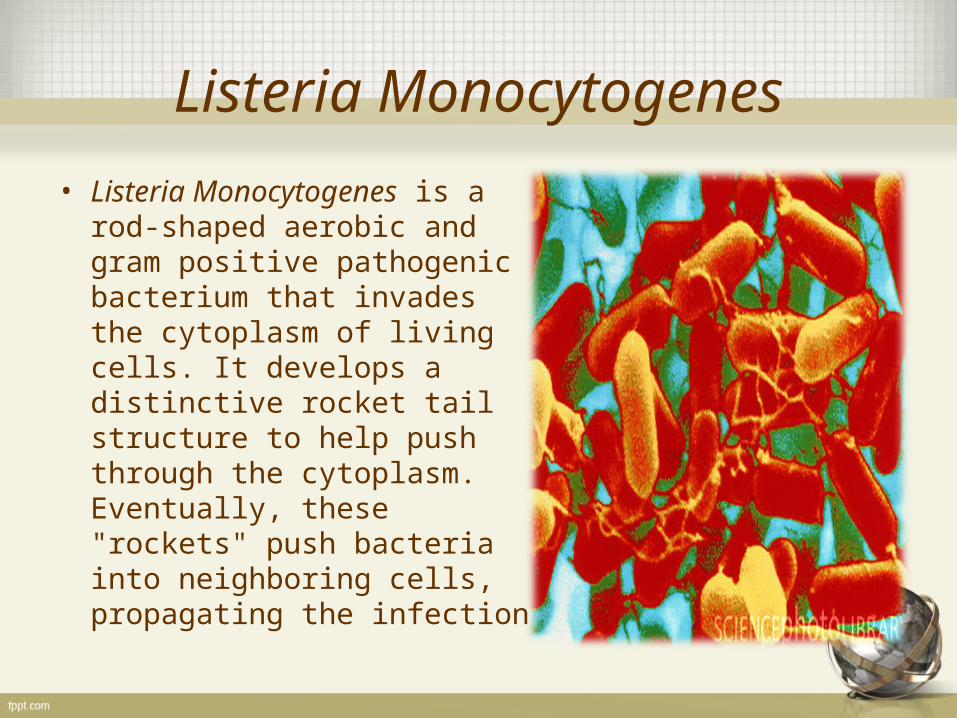
• Listeria Monocytogenes is a rod-shaped aerobic and gram positive pathogenic bacterium that invades the cytoplasm of living cells. It develops a distinctive rocket tail structure to help push through the cytoplasm. Eventually, these "rockets" push bacteria into neighboring cells, propagating the infection
Listeriosis
• More common in domestic animal (domestic mammal and poultry), especially ruminants, than in human beings.
• It can also occur in feral animals among others, game
animals as well as in poultry and other birds.• The causative bacterium lives in the soil and in poorly
made silage and is acquired by ingestion.• The disease is usually sporadic, but can occur as farm
outbreaks in ruminants.
Cont.
Three main forms are usually recognized throughout the affected species:
• encephalitis, the most common form in ruminants• late abortion• gastro-intestinal septicemia with liver damage,
in monogastric species as well as in preruminant calves and lambs

Common Hosts
Common hosts includes:• Sheep • Horses• Pigs• Dogs• Cats• Rabbits
• Humans.

Zoonotic

Effects
• Can cause meningitis and Meingoenphalitis
• In particularly in neonates and elderly
• Abortions in pregnant women, and still birth
• Asymptomatic colonization in vagina produces infertility

Who are at risk
• Pregnant women
• New-borns
• People with weakened immune systems
• People who are taking immuno-suppressing medication.
20 times more likely than other healthy adults to get
New-borns rather than the pregnant women themselves suffer the serious effects of infection in pregnancy.

Signs
• Vomiting • Nausea • Cramps• Diarrheal• Severe Headache • Constipation• Stiff Neck• Confusion• Persistent fever.

Events




Etiology
Listeria monocytogenes Gram-positive, rods.
Sheep blood agar haemolytic (virulence).
Soil (one year), decayed herbage, feces, saliva, grow at 3-45 ; C, pH 4.5 – 9.
Susceptible to common disinfectants.

Epidemiology
• Case fatality high.
• Source of infection by environmental even milk from infected dams in bacteraemia.
• Mode of infection ingestion abrasions in buccal cavity cranial nerve.

Predisposing factors
• Factors decrease the animal resistance (sudden change in weather, poor nutrition,)
• Feeding on silage with improper fermentation (pH > 5)

Pathgenesis
• Ingestion intestine bacteremia localized in various organs or septicaemia.
• invasion of placenta necrosis of placenta abortion.• inflammation of brainstem unilateral.

Clinical Signs
• Circling• Head deviation• unilateral facial paralysis• dropped jaw• drooling saliva• Ataxia with falling to one side,
recumbence• May be fever 40c• Death due to respiratory
failure.• Course 1-2 weeks.
Cont.
• Sporadic abortion• Last 3rd of pregnancy• Retained placenta• Some ewes die from
septicaemia• Start with fever• Diarrhoea• Die in 12 hours.

Postmortem Lesions
• Aborted lambs miliary gray-white necrotic foci on liver, placentitis.
• Microscopically; medulla oblongata, pons unilateral microabscessation,
• Acute vasculitis and prevascular cuffing.

Diagnosis
• Signs.• History of silage feeding.• Histopathology of brain.• Demonstrate the Listeria and
culturing it.• From CSF, Blood, and other
fluids

Treatment
• Penicillin 44,000 iu/kg especially after abortion and in early septicemia.
• Ampicillin – amoxicillin+ sulphonamide.• Gentamycin and Ampicillin on clinical basis.
• Intravenous Trimethoprim – Sulphmethoxazole• Cephalosporins and Fluroquinoles are not active against
l.monocytogens

Control
• Provide good silage; no mould, good fermented, no grazing in silage fields.
• Rodent control will prevent spread of bacteria. • Avoid spoiled or moldy silage and silage from the top
layer (few inches) which has been exposed to air. Any leftover silage should be removed from the feedbunk after feeding.
• Vaccines are available in some countries, however results are questionable, which leads to questions about the cost-benefit of vaccination.


Introduction
• Colibacillosis is a broad term that refers to any infection or disease caused by the bacteria Escherichia coli.
• These infections include colisepticemia, coligranuloma, veneral colibacillosis, coliform cellulitis, peritonitis, salpingitis, orchitis and enteritis.
• In mammals, colibacillosis is usually a primary intestinal or urinary tract infection.
• Colibacillosis in poultry is usually a secondary disease that occurs when the host’s immune system has become overwhelmed with virulent E. coli strains.

Cont.
• Diarrhea associated with Escherichia coli can occur in young within a few days of birth through well after weaning. Occasional cases of septicemia are attributable to E. coli.
• It is associated with many different kinds of diseases ranging from respiratory tract infection to swollen head syndrome in poultry to urinary tract infections.
• Colibacillosis is a common disease that is seen worldwide and is of significant economic importance concerning the loss of livestock.

Cont.
• There are many different types of E. coli, each of which may possess several of many virulence factors.
• Many outbreaks occur within the first week after birth.
• 1-2 weeks after weaning or following abrupt changes in environment or nutrition.
• E. coli can infect hosts as either a primary or secondary pathogen.

Common Hosts
It is the most common infectious bacterial disease in:
• Cattle.• Goats.• Poultry.• Pigs.• Most of avian species.• Some other mammals.

Etiology
• Pathogenic strains of E. coli are easily isolated, Gram-negative, flagellated bacilli. Most pathogenic strains form smooth to mucoid colonies; some are beta-hemolytic.
• Virulence factors include fimbria (pili), enterotoxins (exotoxins), endotoxins, and capsules. Fimbria are the small hair-like processes on the bacterial surface that allow attachment to specific receptors on the surface of mucosal enterocytes of the small intestine.

Epidemiology
• Potentially pathogenic E. coli are present in the intestinal tract and feces of many normal animals. Dams often act as immune carriers. Poor sanitation and chilling, can increase the risk of colibacillosis.
• Pathogenic coliforms are magnified by fecal shedding to further increase exposure of littermates. Disease occurrence and severity is related to dose ingested and the level of immunity derived from colostral immunity.
Cont.
• Pathogenic coliforms survive in contaminated buildings and can infect successive litters of other.
• Once present, E. coli tend to persist unless vigorous efforts are given to maintaining sanitation, husbandry, and environment.

Pathogenesis
• Ingested pathogenic E. coli adhere to receptors on microvilli of enterocytes via pili. There they colonize, proliferate, and elaborate enterotoxins that cause excessive secretion of fluid and electrolytes by crypt epithelial cells which markedly exceeds absorptive capacity resulting in a net flow of tissue fluids into the lumen. This reduces the absorption of electrolytes, water and endogenous secretions from the lumen.
• The large intestine, sometimes also affected, is unable to absorb the excess fluid and diarrhea results. Damage to epithelial cells sometimes leads to septicemia. Diarrhea usually continues until death results from dehydration and metabolic acidosis or from terminal septicemia.
• Environmental factors (temperature, humidity, sanitation, etc.) are critical.



Clinical signs
• Colibacillosis usually is signaled by the appearance of diarrhea. The severity of the diarrhea varies. The hypersecretory diarrhea usually has an alkaline pH but varies in color. It may be clear and watery, especially in neonates, but may be white or yellow, influenced by type of ingesta and duration of the disease.
• As diarrhea continues, there is progressive dehydration and the hair coat becomes roughened. Body temperature often is subnormal. Shivering often is noted unless an adequate supplementary heat source, such as heat lamps, is available
Signs
• Severe diarrhea • lack of appetite and water consumption• Unresponsiveness• lameness • Stunted growth

Severity
• Morbidity and mortality are very variable depending on which infection/infections the E. coli strain causes in a particular flock of animals. However, almost all flocks exhibit some degree of mortality due to an outbreak of colibacillosis.
• Highly virulent strains of E. coli cause the hosts to become sick and die within a few hours,
• Mildly affected flocks can take days to show morbidity.

Lesions
• Dehydration is the most obvious clinical sign.
• The small intestine and colon may contain excess watery fluid or may be distended and gas-filled.
• There may be mild reddening and congestion of the stomach.
• Microscopy of the mucosa of the small intestine reveals many coliforms adhered to microvilli of intestinal epithelial cells. Villi usually are intact. With some strains of E. coli, there may be necrosis of some villi and microvascular thrombosis in the lamina propria.
• E. coli is a common cause of septicemia in neonates. In those cases, there is fibrinous polyserositis and arthritis.

Diagnosis
• Typical signs and lesions are useful but not definitive.
• The isolation of a uniform and high population of smooth, mucoid, or hemolytic E. coli from the small intestine is suggestive of colibacillosis.
• Isolation, sero-typing, pathology. Aerobic culture yields colonies of 2-5mm on both blood and McConkey agar after 18 hours - most strains are rapidly lactose-fermenting producing brick-red colonies on McConkey agar.

Dx
Diagnostic labs often use one of the following methods to more specifically identify the pathogenic E. coli:
• A slide agglutination test can identify the serogroup but does not confirm pathogenicity.
• Adhesin(s) can be identified using monoclonal antibodies.
• A polymerase chain reaction (PCR) can identify the pathogen genetically.

Cont.
• Diagnostic methods do not identify important contributing factors such as chilling, poor sanitation or starvation. These often must be corrected if prevention or treatment is to be successful.
• Colibacillosis has to be differentiated from other diarrheal diseases of young. These include transmissible gastroenteritis (TGE), rotaviral infection, coccidiosis and Strongyloides parasitism. Starvation is also a major differential diagnosis.

Treatment and Prophylaxis in Travelers diarrhea
• Doxycycline,• Trimethoprim,• Norfloxacillin• Fluroquinolones• Avoid contaminated food,• Safe protected water ,prefer bottled water,• Hot foods, Hot Drinks,• Boiled milk

Treatment
• Amoxycillin
• Tetracyclines
• Neomycin (intestinal activity only)
• Gentamycin
• Ceftiofur (where hatchery borne)
• Potentiated sulphonamide
• Flouroquinolones.

Control & Prevention
• Colibacillosis is related largely to problems in housing and management which cause the disease secondarily.
• Breeding stock should be obtained from a single source with no problems of colibacillosis. Dams should be acclimatized together for 3-6 weeks prior to breeding and during gestation so they can develop immunity to endemically occurring pathogens. This allows for the production of an adequate amount of specific antibodies
in colostrum and milk.
Cont.
• To enhance the immunity by using vaccines made from bacterial pili or toxins or both.
• Pregnant dams often are vaccinated twice at 2-3 week intervals prior to birth.
• Increasing colostral antibodies is feeding some farrowing house waste to sows during late gestation.
• Use of the all in/all out system of raising is suggested.• Giving birth to young should occur in a facility thoroughly
cleaned, disinfected, and dried.• Clean, Dry and hygienic conditions in order to reduce
stress.
Cont.
• When precautionary efforts fail, a system should be available to treat young immediately if signs of colibacillosis appear. Antimicrobials can be administered to neonates orally or by injection.
• Antibiotics can be given in water.• Oral electrolyte replacement solutions sometimes are
used to help control dehydration.• Various products may aid in prevention of postweaning
colibacillosis. Plasma proteins, zinc oxide, organic acids, and probiotics are commonly used.

Cont.
• Some are genetically resistant to certain fimbriae of pathogenic E. coli. Breeding for genetically related resistance eventually may help control some forms of colibacillosis.


















