Lisa Stevens, D.O.. Injury to cells---series of damaging events--- initiation of healing process...
203
Tissue Renewal, Regeneration, and Repair Lisa Stevens, D.O.
-
Upload
isaac-freeman -
Category
Documents
-
view
214 -
download
0
Transcript of Lisa Stevens, D.O.. Injury to cells---series of damaging events--- initiation of healing process...
Tissue Renewal, Regeneration, and RepairLisa Stevens, D.O.

Background
Injury to cells---series of damaging events---initiation of healing processRegeneration
Complete restitution of lost or damaged tissueRepair
May restore some original structures Can cause structural derangements
Healthy tissuesHealing (regeneration/repair)
Occurs after any insult that causes tissue destruction
Essential for the survival of the organism


Regeneration
Proliferation of cells and tissues to replace lost structuresGrowth of an amputated limb in
amphibiansMammalian whole organs and complex
tissues Rarely regenerate after injury Applied to liver growth after partial
resection or necrosis• Compensatory growth rather than true
regeneration

Regeneration
Hematopoietic system, skin, GI tractHigh proliferative capacityRenew themselves continuously Regenerate after injury

Repair
Combination of regeneration and scar formationDeposition of collagen
Contribution of regeneration and scarringAbility of the tissue to regenerateExtent of the injuryExample
Superficial skin wound • Heals through the regeneration of the surface
epithelium


Repair
Chronic inflammationAccompanies persistent injuryStimulates scar formation
Local production of growth factors and cytokines• Promote fibroblast proliferation and collagen
synthesis

Fibrosis
Extensive deposition of collagen Extracellular matrix (ECM)
Components are essential for wound healing Provide the framework for cell migration Maintain the correct cell polarity for the re-
assembly of multilayer structures Participate in angiogenesis (formation of
new blood vessels)

Fibrosis
Extracellular matrix (ECM)Fibroblasts, macrophages, and others
Produce growth factors, cytokines, and chemokines• Critical for regeneration and repair

Normal Cell Proliferation Adult tissues
Size of cell populations Determined by rate of cell proliferation,
differentiation, and deathIncreased cell numbers may result
Increased proliferation Decreased cell death
Apoptosis Physiologic process required for tissue
homeostasisInduced by a variety of pathologic stimuli


Normal Cell Proliferation Terminally differentiated cells
Differentiated cells incapable of replication
Impact of differentiation Depends on the tissue under which it
occurs• Differentiated cells are not replaced• Differentiated cells die but are continuously
replaced by new cells generated from stem cells

Cell Proliferation
Stimulated by physiologic and pathologic conditionsPhysiologic proliferation
Proliferation of endometrial cells under estrogen stimulation during the menstrual cycle
Thyroid-stimulating hormone-mediated replication of cells of the thyroid that enlarges the gland
Stimuli may become excessive, creating pathologic conditions

Cell Proliferation
Stimulated by physiologic and pathologic conditionsPathologic proliferation
Nodular prostatic hyperplasia • Dihydrotestosterone stimulation
Nodular goiters in the thyroid• Increased serum levels of thyroid-stimulating
hormone

Cell Proliferation
Controlled by signals from the microenvironmentStimulate or inhibit proliferationExcess of stimulators or a deficiency of
inhibitors Leads to net growth and, in the case of
cancer, uncontrolled growth

Tissue Proliferative Activity Tissues of the body
Divided into three groups Basis of the proliferative activity of their
cells• Continuously dividing (labile tissues)• Quiescent (stable tissues)• Nondividing (permanent tissues)

Tissue Proliferative Activity
Continuously dividing tissues (labile tissues)Cells proliferate throughout life
Replaces destroyed cellsSurface epithelia
Stratified squamous epithelia of the skin, oral cavity, vagina, and cervix
Lining mucosa of all the excretory ducts of the glands of the body• Salivary glands, pancreas, biliary tract
Tissue Proliferative Activity
Continuously dividing tissues (labile tissues)Surface epithelia, cont’d
Columnar epithelium of the GI tract and uterus
Transitional epithelium of the urinary tract Cells of the bone marrow and
hematopoietic tissuesMature cells are derived from adult stem
cells Tremendous capacity to proliferate

Tissue Proliferative Activity
Quiescent tissues (stabile tissues)Low level of replicationCells from these tissues
Undergo rapid division in response to stimuli
Capable of reconstituting the tissue of origin
Parenchymal cells of liver, kidneys, and pancreas
Mesenchymal cells Fibroblasts and smooth muscle

Tissue Proliferative Activity
Quiescent tissues (stabile tissues)Vascular endothelial cellsLymphocytes and other leukocytesExample
Ability of liver to regenerate• Partial hepatectomy• Acute chemical injury

Tissue Proliferative Activity
Quiescent tissues (stabile tissues)Fibroblasts, endothelial cells, smooth
muscle cells, chondrocytes, and osteocytes Quiescent in adult mammals Proliferate in response to injury Fibroblasts proliferate extensively

Tissue Proliferative Activity
Nondividing tissues Contain cells that have left the cell cycleCannot undergo mitotic division in
postnatal lifeNeuronsSkeletal muscle cellsCardiac muscle cells

Tissue Proliferative Activity
Nondividing tissues Neurons in the central nervous system
(CNS) Destruction of cells• Replaced by the proliferation of the CNS-
supportive elements Glial cells

Tissue Proliferative Activity
Nondividing tissues Mature skeletal muscle
Cells do not divide Regenerative capacity• Through the differentiation of the satellite
cells Attached to the endomysial sheaths
Cardiac muscle Very limited regenerative capacity Large injury to the heart muscle• Myocardial infarction
Followed by scar formation

Stem Cells
Characterized by:Self-renewal propertiesCapacity to generate differentiated cell
lineages Need to be maintained during the life
of the organismAchieved by two mechanisms
Obligatory asymmetric replication• With each stem cell division, one of the
daughter cells retains its self-renewing capacity while the other enters a differentiation pathway

Stem Cells
Need to be maintained during the life of the organismAchieved by two mechanisms
Stochastic differentiation• Stem cell population
Maintained by the balance between stem cell divisions that generate either two self-renewing stem cells or two cells that will differentiate


Stem Cells
Embryonic stem cells (ES cells)Pluripotent
Generate all tissues of the body Give rise to multipotent stem cells• More restricted developmental potential• Eventually produce differentiated cells
Three embryonic layers

Stem Cells
Adult stem cells (somatic stem cells)Restricted capacity to generate different
cell typesIdentified in many tissuesReside in special microenvironments
Niches• Composed of mesenchymal, endothelial, and
other cell types• Niche cells generate or transmit stimuli that
regulate stem cell self-renewal and the generation of progeny cells

Embryonic Stem Cells
Inner cell mass of blastocysts in early embryonic developmentContains pluripotent stem cells (ES cells)Cells isolated from blastocysts
Maintained in culture as undifferentiated cell lines
Induced to differentiate into specific lineages• Heart and liver cells

Embryonic Stem Cells
ES cells may in the future be used to repopulate damaged organs
Effectiveness of these procedures in animals Under intense study
Much debate about the ethical issues associated with the derivation of ES cells from human blastocytes

Reprogramming of Differentiated Cells Induced Pluripotent Stem Cells
Differentiated cells of adult tissues can be reprogrammed to become pluripotent Transferring their nucleus to an enucleated
oocyte Oocytes implanted into a surrogate
mother can generate cloned embryos that develop into complete animals• Reproductive cloning
Successfully demonstrated in 1997 by the cloning of Dolly the sheep

Reprogramming of Differentiated Cells Great hope that the technique of
nuclear transfer to oocytes may be used for therapeutic cloning in the treatment of human diseasesNucleus of a skin fibroblast from a
patient Introduced into an enucleated human
oocyte • Generate ES cells, which are kept in culture,
and then induced to differentiate into various cell types

Reprogramming of Differentiated Cells In principle, these cells can then be
transplanted into the patient to repopulate damaged organsTherapeutic as well as reproductive
cloning are inefficient and often inaccurate Deficiency in histone methylation in
reprogrammed ES cells• Results in improper gene expression


Adult Stem Cells
Adult organismStem cells are present in tissues
Continuously divide• Bone marrow, skin, and the lining of the GI
tract Stem cells may also be present in organs• Liver, pancreas, and adipose tissue
Do not actively produce differentiated cell lineages
Adult Stem Cells
Transit amplifying cellsRapidly dividing cells generated by
somatic stem cellsLose the capacity of self-perpetuationGive rise to cells with restricted
developmental potential Progenitor cells

Adult Stem Cells
TransdifferentiationChange in the differentiation of a cell
from one type to another Developmental plasticity
Capacity of a cell to transdifferentiate into diverse lineages
Stem Cells in Tissue Homeostasis Stem cells
Bone marrowSkinGutLiverBrainMuscleCornea

Bone Marrow
Contains hematopoietic stem cells (HSCs)
Contains stromal cellsAKA multipotent stromal cells,
mesenchymal stem cells or MSCs Hematopoietic Stem Cells
Generate all of the blood cell lineages Reconstitute the bone marrow after
depletion Caused by disease or irradiation

Bone Marrow
Hematopoietic Stem CellsWidely used for the treatment of
hematologic diseasesCollected directly from:
Bone marrow Umbilical cord blood Peripheral blood of individuals receiving
cytokines• Granulocyte-macrophage colony-stimulating
factor, which mobilize HSCs

Bone Marrow
Marrow Stromal Cells (MSCs)MultipotentPotentially important therapeutic
applications Generate chondrocytes, osteoblasts,
adipocytes, myoblasts, and endothelial cell precursors • Depends on the tissue to which they migrate
Migrate to injured tissuesGenerate stromal cells or other cell lineagesDo not participate in normal tissue
homeostasis

Liver
Contains stem cells/progenitor cells in the canals of HeringJunction between the biliary ductular
system and parenchymal hepatocytes Give rise to a population of precursor
cells Oval cells• Bipotential progenitors• Capable of differentiating into hepatocytes
and biliary cells

Liver
Oval cellsFunction as a secondary or reserve
compartmentActivated only when hepatocyte
proliferation is blockedProliferation and differentiation
Fulminant hepatic failure Liver tumorigenesis Chronic hepatitis and advanced liver
cirrhosis

Brain
Neurogenesis from neural stem cells (NSCs)Occurs in the brain of adult rodents and
humansAKA neural precursor cellsCapable of generating neurons,
astrocytes, and oligodendrocytesIdentified in two areas of adult brains
Subventricular zone (SVZ) Dentate gyrus of the hippocampus
Skin
Human epidermis has a high turnover rate About 4 weeks
Stem cells are located in three different areas of the epidermisHair follicle bulge
Constitutes a niche for stem cells that produce all of the cell lineages of the hair follicle
Skin
Stem cells are located in three different areas of the epidermisInterfollicular areas of the surface
epidermis Stem cells are scattered individually in the
epidermis and are not contained in niches Divide infrequently Generate transit amplifying cells• Generate the differentiated epidermis
Sebaceous glands

Intestinal Epithelium
Small intestineCrypts
Monoclonal structures Derived from single stem cells Stem cells regenerate the crypt in 3 to 5
daysVillus
Differentiated compartment Contains cells from multiple crypts


Skeletal Muscle
Skeletal muscle myocytes do not divide, even after injury
Growth and regeneration of injured skeletal muscleOccur by replication of satellite cells
Located beneath the myocyte basal lamina
Constitute a reserve pool of stem cells Generate differentiated myocytes after
injury

Cornea
Transparency of the corneaIntegrity of the outermost corneal
epithelium Maintained by limbal stem cells (LSCs)• Located at the junction between the
epithelium of the cornea and the conjunctiva


Cell Cycle
Replication of cellsStimulated by growth factorsStimulated by signaling from ECM
components Integrins

Cell Cycle
Cell goes through a tightly controlled sequence of eventsCell cycle
G1 (presynthetic) S (DNA synthesis) G2 (premitotic) M (mitotic) phases Quiescent cells that have not entered the
cell cycle are in the G0 state

Cell Cycle
Each cell cycle phaseDependent on the proper activation Dependent on completion of the
previous oneCycle stops at a place at which an
essential gene function is deficient Cell cycle has multiple controls and
redundanciesParticularly during the transition
between the G1 and S phases
Cell Cycle
Cells can enter G1
From G0 (quiescent cells) Cells first must go through the transition
from G0 to G1
• Involves the transcriptional activation of a large set of genes Including various proto-oncogenes Genes required for ribosome synthesis and
protein translation
After completing mitosis (continuously replicating cells)

Cell Cycle
Cells in G1 Progress through the cycleReach a critical stage at the G1/S
transition Restriction point• Rate-limiting step for replication
Upon passing this restriction point Normal cells become irreversibly
committed to DNA replication

Cell Cycle
Progression through the cell cycle, particularly at the G1/S transitionTightly regulated by:
Proteins called cyclins Associated enzymes called cyclin-
dependent kinases (CDKs)
Cell Cycle
Activity of cyclin-CDK complexes Tightly regulated by CDK inhibitorsSome growth factors shut off production of
these inhibitors Embedded in the cell cycle are
surveillance mechanismsGeared primarily at sensing damage to DNA
and chromosomesQuality control checks are called checkpoints
Ensure that cells with damaged DNA or chromosomes do not complete replication

Cell Cycle
G1/S checkpointMonitors the integrity of DNA before
replication
G2/M checkpointChecks DNA after replicationMonitors whether the cell can safely enter
mitosis When cells sense DNA damage…
Checkpoint activation delays the cell cycleTriggers DNA repair mechanisms

Cell Cycle
DNA damage--too severe to be repairedCells are eliminated by apoptosisEnter a nonreplicative state called
senescence Checkpoint defects that allow cells
with DNA strand breaks and chromosome abnormalities to divideProduce mutations in daughter cells that
may lead to neoplasia


Growth Factors
Proliferation of many cell types driven by polypeptides
Restricted or multiple cell targets Promote cell survival, locomotion,
contractility, differentiation, and angiogenesis
Function as ligands that bind to specific receptorsDeliver signals to the target cells
Stimulate the transcription of genes that may be silent in resting cells

Epidermal Growth Factor (EGF) and Transforming Growth Factor α (TGF-α)
Belong to the EGF family Share a common receptor (EGFR) EGF
Mitogenic for a variety of epithelial cells, hepatocytes, and fibroblasts
Widely distributed in tissue secretions and fluids

Epidermal Growth Factor (EGF) and Transforming Growth Factor α (TGF-α)
TGF-α Originally extracted from sarcoma virus-
transformed cells Involved in epithelial cell proliferation in
embryos and adultsMalignant transformation of normal cells to
cancerHomology with EGF, binds to EGFR, and shares
biologic activities of EGF EGFR1 mutations and amplification
Detected in cancers of the lung, head and neck, and breast, glioblastomas, and other cancers

Hepatocyte Growth Factor (HGF) Originally isolated from platelets and
serum Identical to a previously identified
growth factor isolated from fibroblastsScatter factor
Mitogenic effectsHepatocytes and most epithelial cells
Biliary epithelium, and epithelial cells of the lungs, kidney, mammary gland, and skin

Hepatocyte Growth Factor (HGF) Morphogen in embryonic
development Promotes cell scattering and
migration Enhances survival of hepatocytes Produced by fibroblasts and most
mesenchymal cells, endothelial cells, and liver nonparenchymal cells

Platelet-Derived Growth Factor (PDGF)
Family of several closely related proteinsEach consisting of two chains
Three isoforms of PDGF (AA, AB, and BB) are secreted as biologically active molecules
Platelet-Derived Growth Factor (PDGF)
Produced by a variety of cellsActivated macrophages, endothelial
cells, smooth muscle cells, and many tumor cells
Migration and proliferation of fibroblasts, smooth muscle cells, and monocytesAreas of inflammation and healing skin
wounds
Vascular Endothelial Growth Factor (VEGF)
Family of homodimeric proteins Potent inducer of blood vessel
formation in early development (vasculogenesis)
Central role in the growth of new blood vessels (angiogenesis) in adults
Promotes angiogenesis in chronic inflammation, healing of wounds, and in tumors

Fibroblast Growth Factor (FGF) Family of growth factors Containing more than 20 members Contribute to:
Wound healing responses Re-epithelialization of skin wounds

Fibroblast Growth Factor (FGF) Contribute to:
Hematopoiesis Differentiation of specific lineages of blood
cells and development of bone marrow stroma
AngiogenesisDevelopment
Skeletal and cardiac muscle development Lung maturation Specification of the liver from endodermal
cells

Transforming Growth Factor β (TGF-β) and Related Growth Factors
Superfamily of about 30 members Homodimeric protein Produced by a variety of different cell
typesPlatelets, endothelial cells, lymphocytes,
and macrophages

Transforming Growth Factor β (TGF-β) and Related Growth Factors
Potent fibrogenic agent Stimulates fibroblast chemotaxisEnhances the production of collagen,
fibronectin, and proteoglycansInhibits collagen degradation
Decreasing matrix proteases Increasing protease inhibitor activities
Development of fibrosis in a variety of chronic inflammatory conditionsLungs, kidney, and liver

Cytokines
Important functions as mediators of inflammation and immune responses
Tumor necrosis factor (TNF) and IL-1Participate in wound healing reactions
TNF and IL-6Involved in the initiation of liver
regeneration

Tissue Renewal, Regeneration, and Repair
Part 2Lisa Stevens, D.O.

Signaling Mechanisms
Receptor-mediated signal transductionActivated by binding
Ligands, growth factors, and cytokines to specific receptors
Three general modes of signalingBased on the source of the ligand and
the location of its receptorsAutocrine, paracrine, and endocrine

Signaling Mechanisms
Autocrine signalingCells respond to the signaling molecules
that they themselves secrete Establishes an autocrine loop• Tumors overproduce growth factors and their
receptors Stimulating their own proliferation
Autocrine growth regulationPlays a role in liver regenerationProliferation of antigen-stimulated
lymphocytes


Signaling Mechanisms
Paracrine signaling One cell type produces the ligand
Acts on adjacent target cells that express the appropriate receptor
Responding cells Close proximity to the ligand-producing
cell

Signaling Mechanisms
Paracrine signaling Paracrine stimulation
Common in connective tissue repair of healing wounds• Factor produced by one cell type
(macrophage) has a growth effect on adjacent cells (fibroblast)
Necessary for:• Hepatocyte replication during liver
regeneration • Notch effects in embryonic development,
wound healing, and renewing tissues


Signaling Mechanisms
Endocrine signalingHormones synthesized by cells of endocrine
organs Act on target cells distant from their site of
synthesis• Carried by the blood• Growth factors may also circulate and act at
distant sites HGF
Several cytokines Associated with systemic aspects of
inflammation• Act as endocrine agents


Receptor Types
Properties of the major types of receptorsImportance:
How they deliver signals to the cell interiorPertinent to an understanding of normal
and unregulated (neoplastic) cell growth

Receptors: Intrinsic Tyrosine Kinase Activity
Ligands for receptors with tyrosine kinase activityMost growth factors
EGF, TGF-α, HGF, PDGF, VEGF, FGF, c-KIT ligand, and insulin
Receptors belonging to this familyExtracellular ligand-binding domainTransmembrane regionCytoplasmic tail that has intrinsic
tyrosine kinase activity

Receptors:Intrinsic Tyrosine Kinase Activity
Binding of the ligand induces:Dimerization of the receptorTyrosine phosphorylationActivation of the receptor tyrosine
kinase Active kinase phosphorylates• Activates downstream effector molecules
Molecules that mediate effects of receptor engagement with a ligand

Receptors:Lacking Intrinsic Tyrosine Kinase Activity
Recruit kinases Ligands for these receptors include
many cytokinesIL-2, IL-3, and other interleukinsInterferons α, β, and γErythropoietinGranulocyte colony-stimulating factor
(GCSF)Growth hormoneProlactin

Receptors--Lacking Intrinsic Tyrosine Kinase Activity
Receptors transmit extracellular signals to the nucleus Activates members of the JAK (Janus
kinase) family of proteins JAKs link the receptors and activate
cytoplasmic transcription factors • STATs (signal transducers and activation of
transcription) Directly shuttle into the nucleus and activate
gene transcription

G Protein-Coupled Receptors
Receptors transmit signals into the cell through trimeric GTP-binding proteins (G proteins)
Contain seven transmembrane α-helices
Constitute the largest family of plasma membrane receptorsNonodorant G protein-coupled receptors
accounting for about 1% of the human genome

G Protein-Coupled Receptors
A large number of ligands signal through this type of receptorChemokines, vasopressin, serotonin,
histamine, epinephrine and norepinephrine, calcitonin, glucagon, parathyroid hormone, corticotropin, and rhodopsin Large number of pharmaceutical drugs
target above receptors

Steroid Hormone Receptors
Receptors located in the nucleus Function as ligand-dependent
transcription factorsLigands diffuse through the cell membraneBind the inactive receptors
Causes their activation• Activated receptor then binds to specific DNA
sequences Hormone response elements within target genes
Bind to other transcription factors

Steroid Hormone Receptors
Other ligands that bind to members of this receptor familyThyroid hormone, vitamin D, and retinoids
Group of receptors belonging to this family Peroxisome proliferator-activated receptors
Nuclear receptors Involved in a broad range of responses• Adipogenesis, inflammation, and
atherosclerosis


Transcription Factors
Transfer of information to the nucleus Modulate gene transcription
Through action of these factors
Transcription factors that regulate cell proliferation Products of several growth-promoting genes
c-MYC and c-JUN Products of cell cycle-inhibiting genes
P53
Modular design Contain domains for DNA binding and for
transcriptional regulation

Mechanisms of Tissue and Organ Regeneration
Urodele amphibiansNewt can regenerate their tails, limbs, lens,
retina, jaws, and even a large portion of the heart
Capacity for regeneration of whole tissues and organs has been lost in mammals
Inadequacy of true regeneration in mammals Absence of blastema formation
Source of cells for regenerationRapid fibroproliferative response after
wounding

Mechanisms of Tissue and Organ Regeneration
Wnt/β-cateninHighly conserved pathway Participates in the regeneration of:
Planaria flatworms Fin and heart regeneration in zebra fish Blastema and patterning formation in limb
regeneration in newts

Mechanisms of Tissue and Organ Regeneration
MammalsWnt/β-catenin
Modulates stem cell functions• Intestinal epithelium, bone marrow, and
muscle Participates in liver regeneration after
partial hepatectomy Stimulates oval cell proliferation after liver
injury
Mechanisms of Tissue and Organ Regeneration
Liver illustrates the mechanisms of regenerationEven this process is not one of true
regeneration Resection of tissue does not cause new
growth of liver Triggers a process of compensatory
hyperplasia in the remaining parts of the organ

Mechanisms of Tissue and Organ Regeneration
Other organs capable of compensatory growthKidney, pancreas, adrenal glands,
thyroid, and the lungs of very young animals
Display it in less dramatic form than the liver

Mechanisms of Tissue and Organ Regeneration
New nephrons cannot be generated in the adult kidneyGrowth of the contralateral kidney after
unilateral nephrectomy Involves nephron hypertrophy Replication of proximal tubule cells

Mechanisms of Tissue and Organ Regeneration
PancreasLimited capacity to regenerate exocrine
components and isletsRegeneration of pancreatic beta cells
Beta-cell replication Transdifferentiation of ductal cells Differentiation of putative stem cells

Liver Regeneration
Human liverRemarkable capacity to regenerate
Demonstrated by its growth after partial hepatectomy• Tumor resection or for living-donor hepatic
transplantation
Popular image of liver regenerationDaily regrowth of the liver of PrometheusEaten every day by an eagle sent by Zeus
Zeus was angry at Prometheus for stealing the secret of fire• Did he know that Prometheus's liver would
regenerate?

Liver Regeneration
Human liverResection of approximately 60% of the liver
in living donors Doubling of the liver remnant in about one
month
Portions of the liver that remain after partial hepatectomy Constitute an intact "mini-liver" Rapidly expands and reaches the mass of the
original liver Restoration of liver mass
Achieved without regrowth of resected lobes
Liver Regeneration
Growth occurs by enlargement of the lobes that remain after the operationCompensatory growth or compensatory
hyperplasia End point of liver regeneration after
partial hepatectomyRestitution of functional mass rather
than the reconstitution of the original


Liver Regeneration
Almost all hepatocytes replicate during liver regeneration after partial hepatectomy
Hepatocytes are quiescent cellsSeveral hours to enter the cell cycleProgress through G1
Reach the S phase of DNA replication

Liver Regeneration
Wave of hepatocyte replicationSynchronizedFollowed by synchronous replication of
nonparenchymal cells Kupffer cells, endothelial cells, and stellate
cells

Liver Regeneration
Hepatocyte proliferation in the regenerating liverTriggered by the combined actions of
cytokines and polypeptide growth factors
Exception: Autocrine activity of TGF-α

Liver Regeneration
Two major restriction points for hepatocyte replication G0/G1 transition that bring quiescent
hepatocytes into the cell cycle G1/S transition needed for passage through
the late G1 restriction point
Gene expression in the regenerating liver proceeds in phasesStarts with the immediate early gene
response Transient response that corresponds to the
G0/G1 transition

Liver Regeneration
Quiescent hepatocytesBecome competent to enter the cell
cycle through a priming phase Mediated by the cytokines TNF and IL-6,
and components of the complement system
Priming signals activate several signal transduction pathways as a necessary prelude to cell proliferation

Liver Regeneration
Quiescent hepatocytesUnder the stimulation of HGF, TGFα, and
HB-EGF, primed hepatocytes enter the cell cycle and undergo DNA replication
Norepinephrine, serotonin, insulin, thyroid and growth hormone Act as adjuvants for liver regeneration• Facilitates the entry of hepatocytes into the
cell cycle

Liver Regeneration
Individual hepatocytesReplicate once or twice during regenerationReturn to quiescence in a strictly regulated
sequence of events Intrahepatic stem or progenitor cells
Do not play a role in the compensatory growth that occurs after partial hepatectomy
No evidence for hepatocyte generation from bone marrow-derived cells during this process

Extracellular Matrix and Cell-Matrix Interactions
Tissue repair and regeneration Depends on:
Activity of soluble factors Interactions between cells and the
components of the extracellular matrix• Regulates the growth, proliferation,
movement, and differentiation of the cells

Extracellular Matrix and Cell-Matrix Interactions
The ECMs various functions include: Mechanical support
Cell anchorage and migration, and maintenance of cell polarity
Control of cell growth ECM components can regulate cell
proliferation by signaling through cellular receptors of the integrin family
Maintenance of cell differentiation Type of ECM proteins affect the degree of
differentiation of the cells in the tissue

Extracellular Matrix and Cell-Matrix Interactions
The ECMs various functions include: Scaffolding for tissue renewal
Maintenance of normal tissue structure• Requires a basement membrane or stromal
scaffold Integrity of the basement membrane or
the stroma of the parenchymal cells• Critical for the organized regeneration of
tissues

Extracellular Matrix and Cell-Matrix Interactions
The ECMs various functions include: Establishment of tissue microenvironments
Basement membrane• Boundary between epithelium and underlying
connective tissue • Forms part of the filtration apparatus in the
kidneyStorage and presentation of regulatory
molecules Growth factors FGF and HGF are secreted and
stored in the ECM in some tissues• Allows rapid deployment of growth factors after
local injury or during regeneration

Extracellular Matrix
Composed of three groups of macromoleculesFibrous structural proteins
Collagens and elastins Provide tensile strength and recoil
Adhesive glycoproteins Connect the matrix elements to one
another and to cellsProteoglycans and hyaluronan
Provide resilience and lubrication

Extracellular Matrix
Molecules assemble to form two basic forms of ECM: Interstitial matrix
Found in spaces between epithelial, endothelial, and smooth muscle cells, as well as in connective tissue
Consists mostly of fibrillar and nonfibrillar collagen, elastin, fibronectin, proteoglycans, and hyaluronan
Basement membranes Closely associated with cell surfaces Consist of nonfibrillar collagen (mostly type IV),
laminin, heparin sulfate, and proteoglycans

Collagen
Most common protein in the animal worldProvides extracellular framework for all
multicellular organisms No collagen = human would be reduced
to a clump of cells, like the "Blob" interconnected by a few neurons “Gelatinous horror from outer space" of
1950s movie fame) Currently, 27 different types of collagens

Collagen
Each collagen is composed of three chains Form a trimer in the shape of a triple helix
Types I, II, III and V, and XIFibrillar collagensTriple-helical domain is uninterrupted for
more than 1000 residuesProteins are found in extracellular fibrillar
structures

Collagen
Type IV collagensLong but interrupted triple-helical
domainsForm sheets instead of fibrils Main components of the basement
membrane, together with laminin

Collagen
Collagen fibril formationAssociated with the oxidation of lysine and hydroxylysine
residues by the extracellular enzyme lysyl oxidase Cross-linking between the chains of adjacent molecules
Major contributor to the tensile strength of collagen
Vitamin CRequired for the hydroxylation of procollagen
Requirement that explains the inadequate wound healing in scurvy
Genetic defects in collagen production Inherited syndromes
Ehlers-Danlos syndrome and osteogenesis imperfecta

Elastin, Fibrillin, and Elastic Fibers
Blood vessels, skin, uterus, and lungRequire elasticity for their function
MorphologicallyElastic fibers consist of a central core
made of elastin Surrounded by a peripheral network of
microfibrils
Substantial amounts of elastinFound in the walls of large blood vessels
Aorta, and in the uterus, skin, and ligaments

Elastin, Fibrillin, and Elastic Fibers
Fibrillin350-kD secreted glycoproteinAssociates either with itself or with other
components of the ECMScaffolding for deposition of elastin and the
assembly of elastic fibers Influence the availability of active TGFβ in the
ECM Inherited defects in fibrillin
Formation of abnormal elastic fibers in Marfan syndrome• Changes in the cardiovascular system (aortic
dissection) and the skeleton

Cell Adhesion Proteins
Most adhesion proteins AKA CAMs (cell adhesion molecules)
Function as transmembrane receptors Sometimes stored in the cytoplasm
Can bind to similar or different molecules in other cells Interaction between the same cells (homotypic
interaction) Different cell types (heterotypic interaction)
Classified into four main families: Immunoglobulin family CAMs Cadherins Integrins Selectins

Cell Adhesion Proteins
Integrins Bind to ECM proteins such as fibronectin,
laminin, and osteopontin Provides a connection between cells and ECM
and adhesive proteins in other cells Establishing cell-to-cell contact
ECM Proteins Fibronectin
Large protein Binds to many molecules (collagen, fibrin,
proteoglycans, and cell surface receptors) Consists of two glycoprotein chains, held together
by disulfide bonds
Cell Adhesion Proteins
ECM ProteinsFibronectin
Fibronectin messenger RNA has two splice forms• Tissue fibronectin and plasma fibronectin
Plasma form binds to fibrin Stabilize the blood clot that fills the gaps created
by wounds Substratum for ECM deposition and formation of
the provisional matrix during wound healing

Cell Adhesion Proteins
ECM ProteinsLaminin
Most abundant glycoprotein in the basement membrane
Binding domains for both ECM and cell surface receptors
Mediates the attachment of cells to connective tissue substrates

Cell Adhesion Proteins
Cadherins and integrinsLink the cell surface with the
cytoskeleton Binding to actin and intermediate
filaments Linkages • Mechanism for the transmission of
mechanical force• Activation of intracellular signal transduction
pathways

Cadherin
Name derived from the term "calcium-dependent adherence protein"
Participates in interactions between cells of the same typeConnect the plasma membrane of adjacent
cells forming two types of cell junction Zonula adherens• Small, spotlike junctions located near the apical
surface of epithelial cells Desmosomes• Stronger and more extensive junctions, present
in epithelial and muscle cells

Cadherin
Diminished function of E-cadherinContributes to certain forms of breast
and gastric cancer

Other Secreted Adhesion Molecules
SPARC (secreted protein acidic and rich in cysteine)AKA osteonectinContributes to tissue remodeling in
response to injuryFunctions as an angiogenesis inhibitor
ThrombospondinsFamily of large multifunctional proteinsSome of which are similar to SPARCInhibit angiogenesis

Other Secreted Adhesion Molecules
Osteopontin (OPN)Glycoprotein that regulates calcificationMediator of leukocyte migration involved
in inflammation, vascular remodeling, and fibrosis in various organs
Tenascin familyConsist of large multimeric proteinsInvolved in morphogenesis and cell
adhesion

Glycosaminoglycans (GAGs)
Make up the third type of component in the ECM
Consist of long repeating polymers of specific disaccharides
Linked to a core protein, forming molecules called proteoglycans

Glycosaminoglycans (GAGs)
Four structurally distinct families of GAGsHeparan sulfateChondroitin/dermatan sulfateKeratan sulfateHyaluronan (HA)
Produced at the plasma membrane by enzymes called hyaluronan synthases
Not linked to a protein backbone First three of these families
Synthesized and assembled in the Golgi apparatus and rough endoplasmic reticulum as proteoglycan

Proteoglycans
Originally described as ground substances or mucopolysaccharidesMain function was to organize the ECM
Diverse roles in regulating connective tissue structure and permeability

Proteoglycans
Integral membrane proteins Act as modulators
Inflammation, immune responses, and cell growth and differentiation
Binding to other proteinsActivation of growth factors and
chemokines

Hyaluronan
Polysaccharide of the GAG family Found in the ECM of many tissues Abundance in:
Heart valves, skin and skeletal tissues Synovial fluid, vitreous of the eye, and umbilical cord
Huge molecule Many repeats of a simple disaccharide stretched end-to-end
Binds a large amount of water About 1000-fold its own weight Forms a viscous hydrated gel
Gives connective tissue the ability to resist compression forces

Hyaluronan
Provides resilience and lubrication to connective tissueNotably for the cartilage in joints
Concentration increases in inflammatory diseasesRheumatoid arthritis, scleroderma,
psoriasis, and osteoarthritis

Hyaluronan
HyaluronidasesEnzymes that fragment hyaluronan
Lower molecular weight moleculesProduced by endothelial cellsBinds to the CD44 receptor on leukocytesPromotes recruitment of leukocytes to
sites of inflammationStimulates production of inflammatory
cytokines and chemokines by white cells recruited to the sites of injury

Part 3Lisa Stevens, D.O.
Tissue Renewal, Regeneration, and Repair

Repair by Connective Tissue
Severe or persistent tissue injury Damage to parenchymal and
stromal cells Leads to a situation in which repair
cannot be accomplished by parenchymal regeneration alone
RepairOccurs by replacement of
nonregenerated parenchymal cells with connective tissue

Repair by Connective Tissue
RepairFour components of this
process Angiogenesis Migration and proliferation of
fibroblasts Deposition of ECM Remodeling (maturation and
reorganization of the fibrous tissue)

Tissue Repair
Tissue repair begins within 24 hours of injuryStimulate the emigration of
fibroblastsInduction of fibroblasts and
endothelial

Tissue Repair
By 3-5 days of tissue repair a specialized type of tissue appearsCharacteristic of healing
“granulation tissue” Name from pink soft appearance of
tissue (seen beneath scab, for example)
Characterized by fibroblast proliferation and new, thin walled delicate capillaries
Outcome is formation of dense fibrosis (scarring)

Angiogenesis
Blood vessels are assembled by two processesVasculogenesis
Assembly of primitive vascular network - from angioblast
Angiogenesis or neovascularization Pre-existing blood vessels send out
capillary sprouts

Angiogenesis
Critical process in the healing at sites of injury
Development of collateral circulations at sites of ischemiaStimulate following MI or atherosclerosis
Allows tumors to growInhibit to “starve” tumor growth

Angiogenesis
VasodilationResponse to nitric oxideVEGF-induced increased permeability of
the preexisting vessel Proteolytic degradation of the
basement membrane of the parent vesselMatrix metalloproteinases (MMPs)Disruption of cell-to-cell contact between
endothelial cells by plasminogen activator

Angiogenesis
Migration of endothelial cellsToward the angiogenic stimulus
Proliferation of endothelial cellsJust behind the leading front of migrating
cells

Angiogenesis
Maturation of endothelial cellsIncludes inhibition of growth and
remodeling into capillary tubes Recruitment
Periendothelial cells, pericytes and vascular smooth muscle cells to form the mature vessel

Angiogenesis
• Many factors induce angiogenesis• Most important
• bFGF (basic fibroblast growth factor)• VEGF (vascular endothelial growth factor)

Cutaneous Wound Healing
Divided into three phases Inflammation
Initial injury causes platelet adhesion and aggregation
Formation of a clot in the surface of the wound Proliferation
Formation of granulation tissue, proliferation and migration of connective tissue cells, and re-epithelialization of the wound surface
Maturation Involves ECM deposition, tissue remodeling, and
wound contraction Phases overlap; separation is somewhat
arbitrary


Wound Healing
Simplest type of cutaneous wound repairHealing of a clean, uninfected surgical
incision Approximated by surgical sutures Referred to as healing by primary union
or by first intention

Wound Healing
IncisionDeath of a limited number of epithelial
and connective tissue cellsDisruption of epithelial basement
membrane continuityRe-epithelialization to close the wound
Occurs with formation of a relatively thin scar


Wound Healing
Excisional wounds Repair process is more complicatedCreate large defects on the skin surface
Extensive loss of cells and tissue

Wound Healing
Healing of these wounds More intense inflammatory
reactionFormation of abundant
granulation tissueExtensive collagen depositionLeading to the formation of a
substantial scar Generally contracts Healing by secondary union or by
second intention



Formation of Blood Clot
Wounding causes the rapid activation of coagulation pathwaysFormation of a blood clot on the wound
surface Entrapped red cells, fibrin, fibronectin,
and complement components Clot serves to stop bleeding and as a
scaffold for migrating cells • Attracted by growth factors, cytokines and
chemokines released into the areaRelease of VEGF
Increased vessel permeability and edema

Formation of Blood Clot
Dehydration occurs at the external surface of the clotForms a scab that covers the wound
Within 24 hours, neutrophils appear at the margins of the incisionUse the scaffold provided by the fibrin
clot to infiltrate inRelease proteolytic enzymes that clean
out debris and invading bacteria

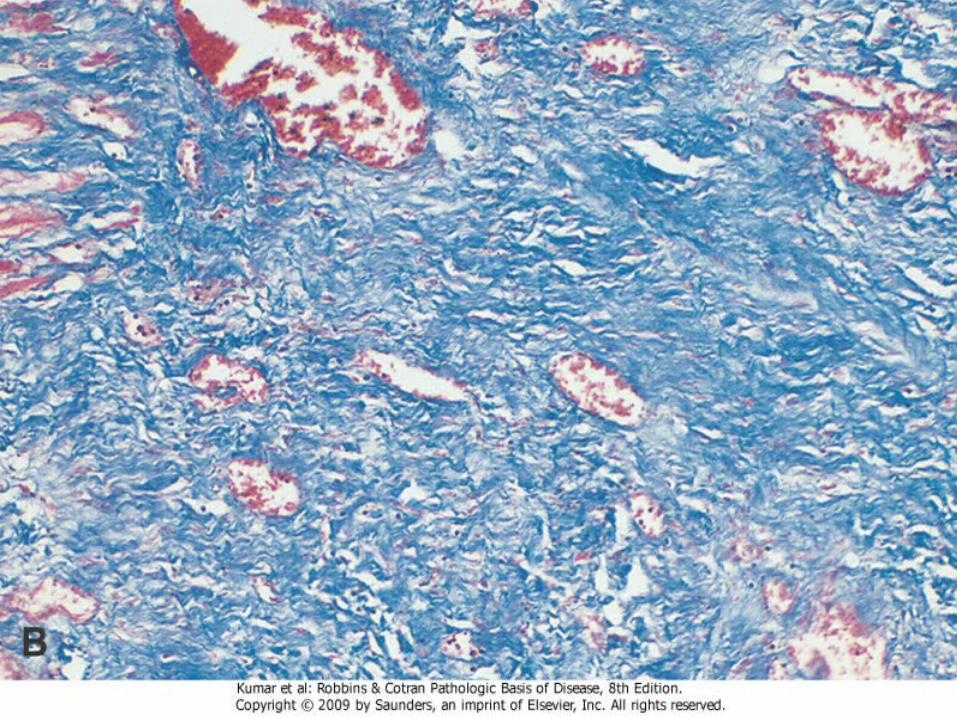
Formation of Granulation Tissue
Fibroblasts and vascular endothelial cellsProliferate in the first 24 to 72 hours of
the repair processForm a specialized type of tissue
Granulation tissue• Hallmark of tissue repair
Formation of Granulation Tissue
Granulation tissuePink, soft, granular appearance on the
surface of woundsHistologic feature
Presence of new small blood vessels (angiogenesis)
Proliferation of fibroblasts

Formation of Granulation Tissue
Granulation tissueNew vessels are leaky
Allow the passage of plasma proteins and fluid into the extravascular space
New granulation tissue is often edematousProgressively invades the incision space

Formation of Granulation Tissue
Granulation tissueAmount of granulation tissue
that is formed depends on: Size of the tissue deficit created
by the wound Intensity of inflammation
Much more prominent in healing by secondary union
By 5 to 7 days, granulation tissue fills the wound area and neovascularization is maximal


Cell Proliferation and Collagen Deposition
Neutrophils Largely replaced by macrophages by 48
to 96 hours Macrophages are key cellular constituents
of tissue repair• Clearing extracellular debris, fibrin, and
other foreign material at the site of repair• Promoting angiogenesis and ECM deposition


Cell Proliferation and Collagen Deposition
Migration of fibroblasts to the site of injuryDriven by chemokines, TNF, PDGF, TGF-
β, and FGFProliferation is triggered by multiple
growth factors PDGF, EGF, TGF-β, FGF, and the cytokines
IL-1 and TNF • Macrophages are the main source for these
factors

Cell Proliferation and Collagen Deposition
Collagen fibers are present at the margins of the incisionAt first these are vertically oriented
Do not bridge the incision
24 to 48 hours, spurs of epithelial cells move from the wound edge along the cut margins of the dermis, depositing basement membrane components as they move. Fuse in the midline beneath the surface scab
Producing a thin, continuous epithelial layer that closes the wound

Cell Proliferation and Collagen Deposition
Full epithelialization of the wound surfaceMuch slower in healing by secondary
union Gap to be bridged is much greater Subsequent epithelial cell proliferation
thickens the epidermal layer

Cell Proliferation and Collagen Deposition
MacrophagesStimulate fibroblasts
Produce FGF-7 (keratinocyte growth factor) and IL-6, which enhance keratinocyte migration and proliferation
Signaling through the chemokine receptor CXCR 3 also promotes skin re-epithelialization

Cell Proliferation and Collagen Deposition
Concurrently with epithelializationCollagen fibrils become more abundantBegin to bridge the incision
Provisional matrix containing fibrin, plasma fibronectin, and type III collagen is formedReplaced by a matrix composed
primarily of type I collagen

Cell Proliferation and Collagen Deposition
TGF-β is the most important fibrogenic agent Produced by most of the cells in
granulation tissueCauses fibroblast migration and
proliferation, increased synthesis of collagen and fibronectin, and decreased degradation of ECM by metalloproteinases

Cell Proliferation and Collagen Deposition
Leukocytic infiltrate, edema, and increased vascularityDisappear during the second weekBlanching begins
Increased accumulation of collagen within the wound area and regression of vascular channels

Cell Proliferation and Collagen Deposition
Original granulation tissue scaffolding is converted into a pale, avascular scar
By the end of the first monthScar is made up of acellular
connective tissue devoid of inflammatory infiltrate, covered by intact epidermis

Wound contraction
Generally occurs in large surface wounds
Contraction helps to close the wound by decreasing the gap between its dermal edges and by reducing the wound surface areaImportant feature in healing by
secondary union Replacement of granulation
tissue with a scarInvolves changes in the
composition of the ECM

Recovery of Tensile Strength
Fibrillar collagens (mostly type I collagen) Form a major portion of the connective
tissue in repair sitesEssential for the development of
strength in healing wounds Net collagen accumulation
Depends not only on increased collagen synthesis but also on decreased degradation

Recovery of Tensile Strength
Length of time for a skin wound to achieve its maximal strengthSutures are removed from an incisional
surgical wound End of the first week, wound strength is
approximately 10% that of unwounded skin Wound strength increases rapidly over the
next 4 weeks Slows down at approximately the third
month after the original incision Reaches a plateau at about 70% to 80% of
the tensile strength of unwounded skin

Recovery of Tensile Strength
Lower tensile strengthHealed wound area may persist for life
Recovery of tensile strengthResults from the excess of collagen
synthesis over collagen degradation during the first 2 months of healing
Structural modifications of collagen fibers (cross-linking, increased fiber size) after collagen synthesis ceases

Factors that influence wound healing
Adequacy of wound repair may be impaired by systemic and local host factors
Systemic factors include: Nutrition
Protein deficiency: Esp vitamin C deficiency, inhibit collagen synthesis and retard healing
Metabolic status Diabetes mellitus is associated with
delayed healing• Consequence of the microangiopathy

Factors that influence wound healing
Circulatory statusModulate wound healing Inadequate blood supply, usually caused
by arteriosclerosis or venous abnormalities (e.g., varicose veins) that retard venous drainage, also impairs healing
Hormones Glucocorticoids
Well-documented anti-inflammatory effects Influence various components of
inflammation Agents also inhibit collagen synthesis

Factors that influence healing
InfectionResults in persistent tissue injury and
inflammation Mechanical factors
Early motion of wounds, can delay healing
Compressing blood vessels and separating the edges of the wound

Factors that influence healing
Foreign bodiesUnnecessary sutures or fragments of steel,
glass, or even bone, constitute impediments to healing
Size, location, and type of woundRichly vascularized areas, such as the face,
heal faster than those in poorly vascularized ones, such as the foot
Small incisional injuries heal faster and with less scar formation than large excisional wounds or wounds caused by blunt trauma


Complications in Wound Healing
Arise from abnormalities; three categoriesDeficient scar formationExcessive formation of the repair
componentsFormation of contractures
Deficient Scar Formation
Lead to two types of complicationsWound dehiscence
Rupture of a wound is most common after abdominal surgery
Due to increased abdominal pressure• Vomiting, coughing, or ileus
Ulceration Inadequate vascularization during healing Areas devoid of sensation
Excessive Formation
Excessive formation of the components of the repair process can give rise to hypertrophic scars and keloidsAccumulation of excessive
amounts of collagen may give rise to a raised scar Hypertrophic scar• Develop after thermal or
traumatic injury Involves the deep layers of the
dermis

Excessive Formation
Keloid Individual predispositionMore common in African
Americans


Excessive Formation
Exuberant granulationDeviation in wound healingFormation of excessive amounts of
granulation tissueProtrudes above the level of the
surrounding skinBlocks re-epithelializationMust be removed by cautery or surgical
excision Permit restoration of the continuity of the
epithelium

Contraction
Important part of the normal healing process
Exaggeration of this processGives rise to contractures
Results in deformities of the wound and the surrounding tissues
Contractures are particularly prone to develop on the palms, the soles, and the anterior aspect of the thorax
Contractures are commonly seen after serious burns and can compromise the movement of joints


Fibrosis
Denote the excessive deposition of collagen and other ECM components in a tissue
Deposition of collagen in chronic diseases