Lipoproteins - Clinical Chemistry
13
Mutations in the Apolipoprotein (apo) B-100 Receptor-binding region: Detection of apo B-100 (Arg 3500 3 Trp) Associated with Two New Haplotypes and Evidence That apo B-100 (Glu 3405 3 Gln) Diminishes Receptor-mediated Uptake of LDL Eva Fisher, 1 Hubert Scharnagl, 2 Michael M. Hoffmann, 2 Klaus Kusterer, 3 Daniela Wittmann, 1 Heinrich Wieland, 2 Werner Gross, 1 and Winfried Ma ¨ rz 2* Background: Ligand-defective apolipoprotein (apo) B-100 is a major cause of hypercholesterolemia. For many years, apo B-100 (Arg 3500 3 Gln) has been the only mutation known to cause ligand-defective apo B-100. Methods: Using temperature gradient gel electrophore- sis, we screened 297 unrelated individuals with LDL- cholesterol >1.55 g/L and triglycerides <2.0 g/L for sequence variants of the putative LDL receptor-binding domain of apo B-100. Results: We found apo B-100 (Arg 3500 3Gln) in 21 indi- viduals (7.1%). When extrapolated to the general popula- tion, this corresponds to the highest prevalence of apo B-100 (Arg 3500 3Gln) reported to date. Furthermore, we identified three unrelated carriers (1%) of a silent substitution (CTG3CTA) affecting the codon for leucine 3350 , four carriers (1.3%) of apo B-100 (Glu 3405 3Gln), and two subjects (0.7%) with apo B-100 (Arg 3500 3Trp). apo B-100 (Arg 3500 3Trp) was assigned to two different, previously unknown haplotypes. The binding, uptake, and degradation of apo B-100 (Arg 3500 3Trp) was lower than that of normal LDL, but higher than with apo B-100 (Arg 3500 3Gln), imply- ing that the substitution of Trp 3500 for Arg may cause less severe reduction of binding than the substitution of Gln. LDL from individuals heterozygous for apo B-100 (Glu 3405 3Gln) bound to LDL receptors at the same rate as normal LDL, but was taken up and degraded at significantly reduced rates, suggesting that domains of apo B-100 involved in binding and uptake do not completely overlap. Conclusions: In Germany, apo B-100 (Arg 3500 3 Gln) may be more frequent than previously assumed. Both apo B-100 (Arg 3500 3 Trp) and apo B-100 (Glu 3405 3 Gln) may contribute to the phenotype of ligand-defective LDL. These variants will be missed if screening is confined to apo B-100 (Arg 3500 3 Gln) only. © 1999 American Association for Clinical Chemistry Nearly two-thirds of all circulating cholesterol is trans- ported by LDL particles. The receptor-mediated catabo- lism of LDL is an important determinant of the concen- tration of LDL-cholesterol (LDL-C) in the plasma (1). Apolipoprotein (apo) 4 B-100, the major protein constitu- ent of LDL, mediates the binding of LDL to the LDL receptor (2, 3). The domain of apo B-100 that interacts with the LDL receptor has been defined using several approaches (4–7). The proposed model of this binding region, comprising two clusters [A (3147–3157) and B (3359 –3367)] of basic amino acids that are linked through a disulfide bond between residues 3167 and 3297 (4, 7), has been further expanded through the discovery of 1 Gustav Embden-Centre of Biological Chemistry and 3 Department of Internal Medicine, Johann Wolfgang Goethe-University, Theodor Stern-Kai 7, 60590 Frankfurt am Main, Germany. 2 Division of Clinical Chemistry, Department of Medicine, Albert Lud- wigs-University, Hugstetter Strasse 55, 79098 Freiburg, Germany. *Author for correspondence. Fax 49-761-270-3444; e-mail [email protected] freiburg.de. Revision received April 9, 1999; accepted April 15, 1999. 4 Nonstandard abbreviations: apo B, apolipoprotein B; LDL-C, LDL-cho- lesterol; FDB, familial defective apo B-100; CAD, coronary artery disease; TGGE, temperature gradient gel electrophoresis; HLP, hyperlipoproteinemia; HDL-C, HDL-cholesterol; RFLP, restriction fragment length polymorphism; and SSCP, single-strand conformation polymorphism. Clinical Chemistry 45:7 1026 –1038 (1999) Lipids and Lipoproteins 1026 Downloaded from https://academic.oup.com/clinchem/article/45/7/1026/5643264 by guest on 01 December 2021
Transcript of Lipoproteins - Clinical Chemistry

Mutations in the Apolipoprotein (apo) B-100Receptor-binding region: Detection of apo B-100
(Arg35003Trp) Associated with Two NewHaplotypes and Evidence That apo B-100
(Glu34053Gln) Diminishes Receptor-mediatedUptake of LDL
Eva Fisher,1 Hubert Scharnagl,2 Michael M. Hoffmann,2 Klaus Kusterer,3
Daniela Wittmann,1 Heinrich Wieland,2 Werner Gross,1 and Winfried Marz2*
Background: Ligand-defective apolipoprotein (apo)B-100 is a major cause of hypercholesterolemia. Formany years, apo B-100 (Arg35003Gln) has been the onlymutation known to cause ligand-defective apo B-100.Methods: Using temperature gradient gel electrophore-sis, we screened 297 unrelated individuals with LDL-cholesterol >1.55 g/L and triglycerides <2.0 g/L forsequence variants of the putative LDL receptor-bindingdomain of apo B-100.Results: We found apo B-100 (Arg35003Gln) in 21 indi-viduals (7.1%). When extrapolated to the general popula-tion, this corresponds to the highest prevalence of apoB-100 (Arg35003Gln) reported to date. Furthermore, weidentified three unrelated carriers (1%) of a silentsubstitution (CTG3CTA) affecting the codon for leucine3350,four carriers (1.3%) of apo B-100 (Glu34053Gln), and twosubjects (0.7%) with apo B-100 (Arg35003Trp). apo B-100(Arg35003Trp) was assigned to two different, previouslyunknown haplotypes. The binding, uptake, and degradationof apo B-100 (Arg35003Trp) was lower than that of normalLDL, but higher than with apo B-100 (Arg35003Gln), imply-ing that the substitution of Trp3500 for Arg may cause lesssevere reduction of binding than the substitution of Gln.
LDL from individuals heterozygous for apo B-100(Glu34053Gln) bound to LDL receptors at the same rate asnormal LDL, but was taken up and degraded at significantlyreduced rates, suggesting that domains of apo B-100 involvedin binding and uptake do not completely overlap.Conclusions: In Germany, apo B-100 (Arg35003Gln)may be more frequent than previously assumed. Bothapo B-100 (Arg35003Trp) and apo B-100 (Glu34053Gln)may contribute to the phenotype of ligand-defectiveLDL. These variants will be missed if screening isconfined to apo B-100 (Arg35003Gln) only.© 1999 American Association for Clinical Chemistry
Nearly two-thirds of all circulating cholesterol is trans-ported by LDL particles. The receptor-mediated catabo-lism of LDL is an important determinant of the concen-tration of LDL-cholesterol (LDL-C) in the plasma (1 ).Apolipoprotein (apo)4 B-100, the major protein constitu-ent of LDL, mediates the binding of LDL to the LDLreceptor (2, 3). The domain of apo B-100 that interactswith the LDL receptor has been defined using severalapproaches (4–7). The proposed model of this bindingregion, comprising two clusters [A (3147–3157) and B(3359–3367)] of basic amino acids that are linked througha disulfide bond between residues 3167 and 3297 (4, 7),has been further expanded through the discovery of
1 Gustav Embden-Centre of Biological Chemistry and 3 Department ofInternal Medicine, Johann Wolfgang Goethe-University, Theodor Stern-Kai 7,60590 Frankfurt am Main, Germany.
2 Division of Clinical Chemistry, Department of Medicine, Albert Lud-wigs-University, Hugstetter Strasse 55, 79098 Freiburg, Germany.
*Author for correspondence. Fax 49-761-270-3444; e-mail [email protected].
Revision received April 9, 1999; accepted April 15, 1999.
4 Nonstandard abbreviations: apo B, apolipoprotein B; LDL-C, LDL-cho-lesterol; FDB, familial defective apo B-100; CAD, coronary artery disease;TGGE, temperature gradient gel electrophoresis; HLP, hyperlipoproteinemia;HDL-C, HDL-cholesterol; RFLP, restriction fragment length polymorphism;and SSCP, single-strand conformation polymorphism.
Clinical Chemistry 45:71026–1038 (1999) Lipids and
Lipoproteins
1026
Dow
nloaded from https://academ
ic.oup.com/clinchem
/article/45/7/1026/5643264 by guest on 01 Decem
ber 2021

familial ligand-defective apo B-100 (FDB) (8, 9). This hasled to the general view that residues 3130–3630 areimportant for the binding of apo B-100 to the LDLreceptor (10 ). FDB is an autosomal dominantly inheriteddisorder in which the cellular uptake of LDL from theblood is diminished because of mutations within the apoB-100 receptor-binding domain. The biochemical and clin-ical characteristics of FDB are moderately to severelyincreased LDL-C, tendon xanthoma, arcus lipoides, andpremature coronary artery disease (CAD).
To date, several point mutations of the putative recep-tor binding domain of apo B-100 have been identified(9, 11–16). Only three of these mutations have beenshown to produce binding-defective apo B-100 by appro-priate genetic and functional investigations (9, 11, 12).The first substitution to be discovered, and apparently themost frequent one, is apo B-100 (Arg35003Gln) (9 ). Theother two substitutions, apo B-100 (Arg35003Trp) (11 )and apo B-100 (Arg35313Cys) (12 ), occur less frequently.The Arg35313Cys mutation has been identified in twofamilies of different ethnic origin (12 ); in four CADpatients from the Great Salt Lake Basin area of the US, allof Caucasian origin (14 ); in two families in the UnitedKingdom (17 ); and two French individuals (18 ). Com-pared with apo B-100 (Arg35003Gln), the mutation atcodon 3531 is associated with a smaller increase in LDL-C(12, 17). Consistently, LDL that contained apo B-100(Arg35313Cys) exhibited less reduction of LDL receptorbinding in vitro than did LDL endowed with apo B-100(Arg35003Gln) (12 ). To date, apo B-100 (Arg35003Trp)has been described in just one family of European origin(11 ), twice in a mixed Chinese and Malayan hypercholes-terolemic cohort (15 ), in one family of Asian descentliving in the Glasgow region (11 ), and in another nineunrelated individuals from Taiwan (19 ). The receptorbinding of apo B-100 (Arg35003Trp) is considered similarto that of apo B-100 (Arg35003Gln) (11 ).
The apo B-100 (Arg35003Gln) mutation is observedwith an approximate frequency of 1 in 500 to 1 in 700 inpopulations of European (Caucasian) origin (20–22). Al-though primary hypercholesterolemia is a common met-abolic disorder in the middle European population, noadditional frequent molecular reasons for binding-defec-tive apo B-100 have yet been discovered. Hence, manyinvestigators have relied on methods specifically tailoredto detect the Arg35003Gln substitution (21, 23–30) todiagnose FDB. We examined a 2121-bp (codons 3131–3837) portion of the apo B gene, including the putativereceptor binding region, using PCR and temperaturegradient gel electrophoresis (TGGE) in 297 unrelatedindividuals with primary hypercholesterolemia to searchfor new genetic variants that affect the receptor binding ofapo B-100. Among these, 21 carriers of apo B-100(Arg35003Gln) and 2 carriers of apo B-100 (Arg35003Trp)were identified, which indicates a high prevalence of FDBin our area. Another three individuals revealed a silentsubstitution that changes the codon for Leu3350 from CTG
to CTA, and four carriers of apo B-100 (Arg34053Gln)were identified.
Materials and Methodssubjects
Two hundred ninety-seven consecutive individuals withLDL-C concentrations .1.55 g/L and triglycerides ,2.0g/L referred to the Frankfurt University Hospital outpa-tient clinics for differential diagnosis of hyperlipoprotein-emia (HLP) between 1992 and 1997 participated in thestudy. Individuals were included regardless of age, sex, orclinical history of cardiovascular or other diseases (142males and 155 females; mean age, 41.4 6 19.1 year; range,4–84 years). The lipoprotein concentrations reported herewere obtained on one single occasion, usually when thepatients presented for the first time at the study site. Tenpatients (3.4%) had hypothyreosis, and 17 patients (5.7%)had type 2 diabetes mellitus. Eleven patients (3.7%) pre-sented with tendon xanthoma and/or arcus lipoides. Fourmales and one female below 40 years suffered from CAD.Above that age, 17 of 73 males (23%) and 16 of 84 females(19%) had CAD. HLP was not specifically treated in 227patients (76.4%), neither with dietary recommendationsnor with lipid-lowering drugs. Sixty-two patients re-ceived lipid-lowering drugs at the time of blood sam-pling; among these, 17 (5.7%) reported adherence to alipid modified diet. In eight cases, records indicated thatdietary advise was given by the primary care physician.All procedures were in accordance with the HelsinkiDeclaration of 1975, as revised in 1983. Informed consentwas obtained from all study participants, and the studydesign was approved by the ethics review board at theJohann Wolfgang Goethe-University, Frankfurt.
blood samples
Blood was drawn into tubes containing potassium EDTA(final concentration, 3.8–5.0 mmol/L). The blood wascentrifuged (1500g for 30 min at 10 °C). The supernatantplasma was used for the analysis of lipids and lipoproteins;the white blood cells were used to extract genomic DNA.
lipids, lipoproteins, and apolipoproteins
Cholesterol and triglycerides were measured enzymati-cally with reagents from Roche Diagnostics HDL-choles-terol (HDL-C) was measured after precipitation of apoB-containing lipoproteins (31 ). LDL-C was calculatedaccording to Friedewald et al. (32 ), and apo B wasmeasured by kinetic nephelometry, using the ProteinArray System (Beckman Instruments). Lipoprotein(a) wasmeasured using a commercial immunoradiometric assay(Mercodia Diagnostics). Between-day CVs were #3.5%for total cholesterol, total triglycerides, and apo B; #4%for LDL-C; and #5% for HDL-C for the duration of thestudy.
Clinical Chemistry 45, No. 7, 1999 1027D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

dna preparation and oligonucleotides
Genomic DNA was prepared from white blood cells using“blood PCR” DNA isolation cartridges (Diagen), accord-ing to the manufacturer’s instructions. Oligonucleotideswere synthesized using the phosphoramidite method atMWG Biotech. The sequences of the oligonucleotides andtheir positions within the amplified region are given inTable 1 and Fig. 1, respectively.
pcr
apo B gene fragments were prepared by PCR in a finalvolume of 50 mL containing 0.1–0.2 mg of genomic DNA,60 pmol of oligonucleotide primers, 62.5 mmol/L KCl,12.5 mmol/L Tris-HCl, pH 8.3, 1.5 mmol/L MgCl2, 50mmol/L each dNTP, and 1.5 U of Taq DNA polymerase(Amersham Pharmacia). Three different PCR cycle condi-tions were used with respect to different annealing tem-peratures of primers. Fragments A, B, C, D, G, and H wereamplified with an initial denaturation step of 94 °C for 1min, followed by annealing at 55 °C for 1 min and finallyextension at 72 °C for 3 min. Fragment F was amplifiedwith an annealing temperature of 58 °C for 1 min andextension at 72 °C for 3 min, and fragment E was ampli-fies with extension at 74 °C for 2 min. Each PCR wasinitiated by hot start at 95 °C for 3 min, and Taq polymer-ase was added at 80 °C before starting cycles.
tgge
Parallel TGGE was performed in a horizontal gel electro-phoresis apparatus from Qiagen. PCR product (4 mL) wasmixed with 4 mL of denaturing buffer [8 mol/L urea, 400mmol/L 2-(N-morpholino)propanesulfonic acid, pH 8.0,20 mmol/L EDTA, 0.1 g/L bromphenol blue, 0.1 g/Lxylene xyanol FF]. Before loading, samples were dena-tured for 5 min at 95 °C and renatured for 15 min at 50 °Cto allow the formation of heteroduplex molecules; 6mL ofeach sample was loaded on the gel. The gels contained 80g/L acrylamide (at a ratio of acrylamide to N,N9-methyl-enebisacrylamide of 60:1), 8 mol/L urea, 20 mmol/L2-(N-morpholino)propanesulfonic acid, pH 8.0, 1 mmol/LEDTA, and 20 g/L glycerol. The running time was 3 to4.5 h (300 V), depending on the length of the amplifiedproduct. Silver staining was performed as described (33 ).The temperature gradient was 35 °C to 55 °C (or 50 °C,respectively) and was oriented parallel to the direction ofmigration.
dna sequencing
Homoduplex mutant bands were excised from the stainedpolyacrylamide gels, which had not been fixed in thatcase. Gel slices were incubated in diffusion buffer (0.5mol/L ammonium acetate, 10 mmol/L magnesium ace-tate, 1 mmol/L EDTA, pH 8.0, 1 g/L sodium dodecyl
Table 1. Positions and sequences of primers used for TGGE PCRs and RFLP typing.apoB-100amplifiedfragment
Primername Primer sequence
Nucleotidepositions in cDNAa Amino acids
Productsize, bp
A A1 59-TTGAAGGAATTCTTGAAAACGACAAAGCAAb 9.600–10.050 3131–3281 451A2 59-GAAGGACTGGCAGCTCTA
B B1 59-ccgcccgcccgcccgcccgcCGTGTGCCTTCATACACATT 9.999–10.220 3264–3337 222B2 59-AGCAACAATATCTGACTGGT
C C1 59-TTACCTATGATTTCTCCTTT 10.138–10.397 3310–3396 260C2 59-ccccgccgcccgccccgcgcCACTTCCATATTTTTCGTGGb
D D1 59-ccccgccgcccgccccgcgcGAAGTTAGCCACAGCTCTGT 10.307–10.567 3366–3453 261D2 59-TTGTGGTCAACTGCTCCTTTAGCGG
E E1 59-CCTACTGTCTCTTCCTCCATGGAA 10.482–10.810 3425–3534 329E2 59-GAATATATGCGTTGGAGTGTGGCTTCTCC
F F1 59-CCAACACTTACTTGAATTCCAAGAGCAC 10.678–11.122 3490–3638 445F2 59-AAGGATCCTGCAATGTCAAGGTGTGCCTTTb
G G1 59-ccgcccgccgcccgccgcccGAGCTTTCCAATGACCAAGA 11.073–11.386 3622–3726 314G2 59-AATGGGACATGGAACGTAGG
H H1 59-AATTCAGTTCTTGTCATGCC 11.349–11.720 3714–3837 372H2 59-ccgcccgccgcccgccgcccAATCTCAATGGTCTGCTCAG
MspI RFLP 59 59-CAAAGCCACCCTGGAACTCTCTCC 10.883–11.244 3558–3679 36239 59-TTGAAACACGAAGATGCTGTCTCC
EcoRI RFLP 59 59-CACTGGGACCTACCAAGAGTGG 12.539–12.826 4110–4206 28839 59-GAATATACCTGGGACAGTACCG
TaqI RFLP D3 59-CAGTGGCAACAACCACAAAAGtCc 10.399–10.567 3397–3453 169D2 59-TTGTGGTCAACTGCTCCTTTAGCGG
a According to Ludwig et al. (52).b Ref. (10).c Ref. (44).
1028 Fisher et al.: Ligand-defective apo B-100D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

sulfate) at 60 °C for 20 min, followed by 95 °C for 5 min,and DNA was extracted with a QIAEX II polyacrylamidegel extraction kit from Qiagen. The purified DNA (5 mL)was reamplified using Pfu DNA polymerase (Stratagene),buffers recommended by the manufacturer, and the pre-viously applied PCR conditions. The reamplificationproducts were electrophoresed in a 20 g/L agarose geland cleaned with QIAEX II (Qiagen), according to themanufacturer’s instructions. Sequencing was performedusing the ThermoSequenase cycle sequencing kit (Amer-sham) with fluorescently labeled primers, according tothe manufacturer’s instructions. DNA was electropho-resed in an ALF DNA Sequencer (Pharmacia BiotechEurope).
apo B gene haplotyping
Five apo B gene polymorphisms [signal peptide insertion(ins) or deletion (del), XbaI (ACT3ACC, Thr24883Thr)restriction fragment length polymorphism (RFLP), MspI(CGG3CAG, Arg36113Gln) RFLP, EcoRI (AAA3GAA,Lys41543Glu) RFLP, and the 39 hypervariable region(39VNTR)], were analyzed. The methods have been de-scribed previously (33, 34), except for the PCR conditionswe used to determine the EcoRI and the MspI RFLPs. Inthese cases we used the primer sequences given in Table1 and conditions as follows: The reaction volumes were 20mL and contained 10 pmol of each primer, 80 mmol/Leach dNTP, 20–40 ng of genomic DNA, and 0.5 U of TaqDNA polymerase. Thirty-five cycles were performed (de-naturation at 95 °C for 0.30 min, annealing at 60 °C for 1min, and elongation at 72 °C for 0.15 min). The PCRproducts were incubated at 37 °C for 3 h with 10 U of the
respective restriction enzyme and were subsequently an-alyzed by electrophoresis in 20 g/L agarose gels.
detection of point mutations byrestriction typing
After the sequencing of those DNA fragments producingirregular patterns on TGGE, we confirmed the presence ofthe suspected alleles with PCR and subsequent restrictionfragment analysis. The methods for Arg35003Gln andArg35003Trp are described elsewhere (25, 35). The G3Atransition (Leu33503Leu) creates a PstI restriction site infragment C (Table 1). Glu34053Gln was determined bydigesting fragment D, amplified using the primer pairD3-D2. D3 contains a mismatch (AGtC) that introduces aTaqI site in the mutant allele.
binding, uptake, and degradation of125i-labeled ldl
LDL (1.019 , d , 1.063 kg/L) was isolated using prepar-ative ultracentrifugation (36 ) and iodinated using theiodine monochloride method (37 ). The human skin fibro-blasts were from skin biopsies of normolipidemic individ-uals. Cells were grown in 24-well polystyrene plates, andbefore the experiments, the cells were preincubated for40 h in medium containing 100 mL/L human lipoprotein-deficient serum to up-regulate LDL receptors. The bind-ing, uptake, and degradation of 125I-labeled LDL weremeasured as described by Goldstein et al. (38 ) with slightmodifications (39 ). To measure cell surface binding, li-poproteins were incubated with the cells for 1 h at 4 °C inDMEM containing 10 mmol/L HEPES. To measure up-
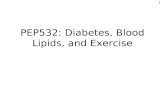
Fig. 1. Map of the amplified regions within exon 26 of the apo B gene.Lengths and nucleotide positions of PCR fragments are indicated. The relative positions of base changes detectable by our TGGE method are shown by vertical arrows.
Clinical Chemistry 45, No. 7, 1999 1029D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

take (surface binding plus internalization) and degrada-tion, cells were incubated for 4 h at 37 °C with 125I-labeledLDL in DMEM containing 24 mmol/L bicarbonate, pH7.4. The amount of 125I-labeled material associated withthe cells (binding and internalization) was determinedafter lysis in 0.3 mmol/L NaOH. Proteolytic degradationwas determined as 125I-labeled trichloroacetic acid-soluble(non-iodine) material in the conditioned medium.
Results
In our survey, we wished to examine the potential impor-tance of mutations of apo B-100 to the development ofhypercholesterolemia. We established a TGGE method toscreen for sequence variations within the region of the apoB gene that included the putative receptor-binding do-main of the molecule. Oligonucleotide primers (Table 1)were designed to amplify eight overlapping fragments (Athrough H) covering the cDNA sequence of amino acidresidues 3131–3837 of the apo B gene (see Fig. 1). PCRproducts were 222–451 bp in length. To increase thesensitivity of our assay, artificial high-melting domainswere incorporated into amplification products B, C, D, G,and H by the use of GC-clamped oligonucleotide primers.
For each fragment, the melting behavior was predictedusing a previously described algorithm (40, 41) and soft-ware supplied by Qiagen. Fragment F (codons 3490–3638)included the two mutations affecting codon 3500. Thesemutations were predicted to shift the melting temperatureby 0.83 °C (Arg35003Gln) and 1.03 °C (Arg35003Trp),respectively, suggesting that they could be distinguishedmerely by their TGGE pattern. A common MspI polymor-phism that changes amino acid 3611 from Arg (CGG) toGln (CAG) (42 ), and the Arg35313Cys mutation at codon3531 altered the calculated melting temperature of thisfragment as well. Nonetheless, TGGE was applied incombination with heteroduplex analysis; i.e., each PCR-amplified product was de- and renatured to allow homo-and heteroduplex formation. Heteroduplex strands couldbe easily distinguished from homoduplex strands.
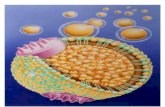
To evaluate the actual sensitivity of our assay, wesought documentation of its ability to detect knownsequence variations. As expected, apo B-100(Arg35003Gln), apo B-100 (Arg35003Trp), apoB-100(Arg35313Cys), and the MspI polymorphism at codon3611 could be distinguished (Fig. 2). Samples heterozy-gous for a particular mutation produced a characteristic
Fig. 2. TGGE of PCR fragments C, D, and F of exon 26 of the apo B gene.Electrophoresis was carried out in 80 g/L polyacrylamide gels, using a temperature gradient from 35 °C to 55 °C. Run times were 3 h (fragments C and D) and 4.5 h(fragment F) at 250–300 V. Fragment F: lane 1, subject without mutation; lane 2, apo B-100 (Arg35003Gln) homozygous individual; lane 3, apo B-100 (Arg35003Gln)heterozygous individual; lane 4, apo B-100 (Arg35003Trp) heterozygous individual; lane 5, apo B-100 (Arg35313Cys) heterozygous individual; lane 6, apo B-100(Arg36113Gln) heterozygous individual, MspI RFLP. Fragment D: lane 1, subject without mutation; lane 2, apo B-100 (Glu34053Gln) heterozygous individual. FragmentC: lane 1, subject without mutation; lane 2, heterozygous transition at the codon for Leu3350 (CTG3CTA).
1030 Fisher et al.: Ligand-defective apo B-100D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

four-band pattern, the faster migrating pair of bandsrepresenting the homoduplexes of the mutant and wild-type strands, respectively, and the slower migrating pairof bands corresponding to heteroduplexes of the twoalleles. A single homoduplex band halted at aberrantpositions in the gel was observed with DNA from anindividual homozygous for apo B-100 (Arg35003Gln).Downstream and upstream sequencing of purified andreamplified mutant homoduplex bands confirmed therespective nucleotide substitutions.
We studied samples from 297 unrelated individualswith LDL-C .1.55 g/L and triglycerides ,2.0 g/L. Ineach of the samples exhibiting irregular melting behavior,the presence of the suspected mutation was confirmedthrough restriction fragment analysis and DNA sequenc-ing where appropriate. Using this strategy, we identified21 carriers of apo B-100 (Arg35003Gln) and 2 carriers ofapo B-100 (Arg35003Trp). Four patients exhibited aber-rant migration of fragment D (Fig. 2); these subjects wereheterozygous for apo B-100 (Glu34053Gln). In three otherunrelated individuals, we detected an abnormality offragment C (Fig. 2) attributable to a silent transition thatchanged the codon for leucine at position 3350 from CTGto CTA. There was no carrier of the Arg35313Cys muta-tion detected in our sample. Two of the four mutations,apo B-100 (Arg35003Gln) and apo B-100 (Arg35003Trp),recently have been unequivocally linked to the develop-ment of hypercholesterolemia (11, 20). The frequency ofheterozygous apo B-100 (Arg35003Gln) carriers was 21 in297 (7.1%) in the entire patient group and 7 in 128 (5.5%)when we considered only individuals 40–65 years of age.A recent cross-sectional survey performed at our institu-tions revealed the prevalence of type IIa HLP (as definedby LDL-C .1.55 g/L and triglycerides ,2.0 g/L) to be atleast 25% among clinically healthy individuals betweenthe ages of 40 and 65 years (M.A. Nauck et al., unpub-lished results). If we assume that mutant forms of apoB-100 produce type IIa HLP only (which is a conservativeestimate because in some instances patients with FDBexhibit type IIb HLP), the calculated prevalence of het-erozygous ligand-defective apo B-100 would be at least
1.4% (1 in 71) among healthy individuals in the Rhein-Main area.
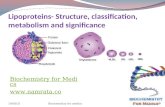
We were able to recruit 19 family members of 9 of the21 unrelated apo B-100 (Arg35003Gln) carriers. Amongthese subjects, 18 were heterozygous and 1 was homozy-gous for apo B-100 (Arg35003Gln). Using five polymor-phic markers of the apo B gene, we deduced partialhaplotypes in all apo B-100 (Arg35003Gln) subjects. Con-sistent with previous reports (43 ), they exhibited a con-sensus haplotype designated as ins, XbaI2, MspI1,EcoRI2, 39VNTR-49 haplotype 194, according to the bi-nary nomenclature of Ludwig and McCarthy (43 ). Hap-lotyping of carriers of the apo B-100 (Glu34053Gln) mu-tation and of the silent transition at codon 3350 revealedthe common genotypes del, XbaI1, MspI1, EcoRI1,39VNTR-37 and ins, XbaI2, MspI1, EcoRI1, 39VNTR-35,respectively (Table 2). Because family members were notavailable for further analyses, we tentatively consideredthese haplotypes to be associated with the respectivemutations. Family segregation analysis in the two familieswith apo B-100 (Arg35003Trp) revealed two new haplo-types unequivocally associated with the mutant (ins,XbaI1, MspI1, EcoRI1, 39VNTR-37 and del, XbaI1,MspI1, EcoRI1, 39VNTR-37, respectively, see Table 3 andFig. 3). These two haplotypes are distinct from thosefound previously in one Scottish family (XbaI1, MspI-,EcoRI1) and in Asian patients with apo B-100(Arg35003Trp) (XbaI-, MspI1, EcoRI1, 39VNTR-35).
The lipid, lipoprotein, and apolipoprotein concentra-tions in those subjects carrying different apo B mutationsare shown in Tables 2 through 4. The screening strategyproduced increased cholesterol, LDL-C, and apo B con-centrations in all patient groups. Three of the 21 apo B-100(Arg35003Gln) carriers suffered from coronary heart dis-ease, five were on lipid-lowering drugs, and only the apoB-100 (Arg35003Gln) homozygote revealed small xan-thelasmas of the upper eyelids and a mild arcus lipoidescorneae. apo B (Glu34053Gln) was detected in threesubjects with mild hypercholesterolemia (LDL-C, 1.56–1.69 g/L) and one subject with a LDL-C concentration of2.43 g/L who were not being treated with lipid-lowering
Table 2. Lipids, lipoproteins, and apo B-100 haplotypes in subjects with apo B-100 (Glu34053Gln) and apo B-100(Leu33503Leu).
SexAge,years
TC,a
g/LLDL-C,
g/LTG,g/L
HDL-C,g/L
apo B,g/L
Lp(a),g/L
SP, ins/delb XbaIb MspI EcoRI 3* VNTRb,c
Glu34053Gln M 64 2.37 1.69 1.22 0.44 1.61 0.08 ins/del 1/2 1/2 1/1 35/37M 59 2.34 1.56 1.91 0.40 1.70 0.01 ins/del 1/2 1/1 1/2 37/49M 52 2.38 1.57 0.92 0.63 1.43 0.07 del/del 1/1 1/1 1/1 33/37F 57 3.46 2.43 1.23 0.78 1.79 1.46 del/del 1/1 1/1 1/1 35/37
Leu33503Leu F 66 2.53 1.74 0.73 0.64 1.32 0.17 ins/del 1/2 1/1 1/2 35/49F 54 2.81 1.77 1.52 0.73 ND 0.15 ins/del 1/2 1/1 1/1 35/37M 59 2.84 2.04 1.18 0.57 1.60 0.07 ins/ins 2/2 1/1 1/1 35/35
a TC, total cholesterol; TG, triglyceride; Lp(a), lipoprotein(a); SP, signal peptide; 1, presence of cutting site; 2, absence of cutting site; ND, not determined.b Ref. (34).c Nomenclature according to Boerwinkle et al. (56).
Clinical Chemistry 45, No. 7, 1999 1031D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

drugs. One of the apo B (Glu34053Gln) carriers, a 52-year-old male with a LDL-C concentration of 1.57 g/L, hadCAD. We studied the interaction of LDL from this patientwith cultured fibroblasts. Confirming a recent report (44 ),the binding of LDL from the apo B-100 (Glu34053Gln)carrier was identical to LDL from normolipidemic donors.Unexpectedly, this was not matched by cellular uptakenor lysosomal degradation. Instead, both uptake anddegradation of the mutant LDL were decreased to 85%and 87.5%, respectively, with the differences reachingstatistical significance (P ,0.05) at the highest concentra-tion of radiolabeled 125I-LDL assayed (Fig. 4).
We were also interested in determining the phenotypicconsequences of the apo B-100 (Arg35003Trp) mutation.The two index patients heterozygous for apo B-100(Arg35003Trp) had no clinical signs of arterial occlusivedisease nor any symptoms frequently associated withFDB. Two members of the GR-098 family carried themutant allele. GR-098/I-2, the index patient, had a LDL-Cconcentration of 1.61 g/L while being treated with 20 mgof pravastatin daily. If we assume that this treatmentproduces a 25% reduction of LDL-C, his pretreatmentLDL-C should have been 2.15 g/L, which is close to theconcentration seen in GR-098/II-3 (2.33 g/L), his 13-year-old daughter who carried the mutation as well. Althoughstill slightly increased, the LDL-C concentration was ,2.0g/L in both unaffected family members (GR-098/I-1 andGR-098/II-4). A history of HLP on both maternal sides ofthe immediately preceding generation was quoted in theGR-098 family, but no samples from the mother of theindex patient or from the mother of his wife (GR-098/I-1)were available for analysis. This positive family historyfor HLP may, however, explain why GR-098/I-1 andGR-098/II-4 had increased LDL-C in the absence of apoB-100 (Arg35003Trp).
The other index patient (L-1193/II-7) was a 41-year-oldmale who had been first diagnosed with HLP type IIa in1987. In June 1996, his LDL-C was 2.84 g/L. Since then, hehad taken a hydroxymethylglutaryl-CoA reductase inhib-itor (10 mg of simvastatin once daily). In response totreatment, he experienced an ;40% reduction of plasmaLDL-C. In the L-1193 kindred, assessment of the pheno-typic consequences of the apo B (Arg35003Trp) mutationwas complicated because only one unaffected individualwas available and because there was some interindividualvariation of LDL-C among the mutation carriers. The66-year-old mother (L-1193/I-5) of the index patient hadbeen treated with micronized fenofibrate (200 mg oncedaily) for the last 10 years, which might explain why herLDL-C concentration was only 1.73 g/L. Her father diedof myocardial infarction at the age of 62. In 1995, she hadbeen diagnosed as having diabetes mellitus, which wasunder treatment as well. The two affected sons of L-1193/I-5, 13-year-old dizygous twins, had low LDL-C, whichwas, however, well above the 90th percentile for that age.Furthermore, it is in line with the assumption that apo B(Arg35003Trp) causes hypercholesterolemia that theLDL-C concentration in the only unaffected adult member(L-1193/I-6) was lower than in the two other adult carri-ers of the mutation.
We analyzed the interaction of LDL from two unre-lated individuals heterozygous for apo B-100(Arg35003Trp) with LDL receptors compared with theinteraction of LDL pooled from normolipidemic individ-uals and LDL from an apo B-100 (Arg35003Gln) heterozy-gous individual. At each of the concentrations studied,the binding, internalization, and degradation of LDL fromthe apo B-100 (Arg35003Trp) heterozygotes were substan-tially lower than normal (on average, 58% of the valuesobtained for normal LDL) but consistently higher com-
Table 3. Lipids, lipoproteins, and apo B haplotypes in the two apo B-100 (Arg35003Trp) subjects and their relatives.
Pedigreeposition Sex
Age,years
apo B-100(Arg
3500
3Trp)
apo Ea
pheno-type
TC,g/L
LDL-C,g/L
TG,g/L
HDL-C,g/L
apo B,g/L
Lp(a),g/L
BMI,kg/m2
SP,ins/del XbaI MspI EcoRI 3* VNTR
GR-098
kindred
1 II F 41 2/2 33 2.8 1.84 0.57 0.85 1.46 1.52 17.4 ins/del 1/2 1/1 1/2 39/47
2b,c I M 40 1/2 33 2.29 1.61 1.02 0.47 1.4 0.13 28.9 ins/ins 1/2 1/1 1/1 31/37
3 II F 13 1/2 33 3.11 2.33 1.38 0.5 1.88 1.15 20.2 ins/ins 1/2 1/1 1/2 37/47
4 II F 11 2/2 33 2.45 1.73 1.17 0.48 1.34 1.01 17.8 ins/ins 2/2 1/1 1/2 31/47
L-1193
kindred
5c I F 66 1/2 33 2.46 1.73 0.57 0.62 1.11 0.67 15.5 del/del 1/2 1/1 1/2 37/47
6 I M 72 2/2 42 2.29 1.59 1.3 0.45 1.06 0.68 22.5 ins/ins 1/2 1/1 1/2 37/49
7b II M 41 1/2 43 3.52 2.84 1.29 0.42 2.10 1.55 20.8 ins/del 1/1 1/1 1/1 37/37
8 III M 13 1/2 43 2.03 1.35 0.97 0.48 0.89 0.86 ND ins/del 1/2 1/1 1/1 33/37
9 III M 13 1/2 43 2.14 1.52 0.78 0.46 1.01 0.96 ND ins/del 1/2 1/1 1/1 33/37
a apo E, apoliprotein E; TC, total cholesterol; TG, triglyceride; Lp(a), lipoprotein(a); BMI, body mass index; SP, signal peptide.b Index patient.c On lipid-lowering treatment at the time of blood sampling.
1032 Fisher et al.: Ligand-defective apo B-100D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

pared with LDL from an apo B-100 (Arg35003Gln) het-erozygote (44% of the values obtained for normal LDL);the differences between apo B-100 (Arg35003Trp) LDLand normal as well as apo B-100 (Arg35003Gln) LDL were
statistically significant at all concentrations except thethree lowest ligand concentrations in the assay for bind-ing at 4 °C (Fig. 5). These observations were reproduciblein three experiments, all of which were conducted inde-
Fig. 3. Pedigrees of two families with apo B-100 (Arg35003Trp).Family members heterozygous for apo B-100 (Arg35003Trp) are indicated by L. LDL-C concentrations (g/L) are given below each symbol. Additional clinical informationon each individual is provided in Table 3. Haplotypes were constructed by analysis of the following five apo B gene polymorphisms: signal peptide insertion (ins) ordeletion (del), XbaI (ACT3ACC, Thr24883Thr) RFLP, MspI (CGG3CAG, Arg36113Gln) RFLP, EcoRI (AAA3GAA, Lys41543Glu) RFLP, and the 39VNTR region of the apoB gene. Construction of haplotypes was based on the assumption that there had been no recombination within the apo B gene. Dotted symbols represent familymembers who were not studied. 1, presence of restriction site; 2, absence of restriction site; circles, females; squares, males.
Clinical Chemistry 45, No. 7, 1999 1033D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

pendently, including labeling. However, we wished torule out that the differences were caused by differentdegrees of denaturation of the LDL during the iodinationprocedure. We therefore studied the interaction of mutantand normal LDL with fibroblasts in culture, utilizing them
as unlabeled competitors for iodinated normal LDL.Again, we performed three entirely independent experi-ments, all of which completely reproduced the differencesseen in the direct binding, uptake, and degradation stud-ies (Fig. 6).
Discussion
Defective binding of LDL to the LDL receptor is a majorcause of hypercholesterolemia. Alterations of the lipidcomposition of the LDL core aside, the three-dimensionalstructure of the receptor-binding domain of apo B-100 issubject to modification resulting from genetically deter-mined changes in the primary structure of apo B-100. Thebest understood genetic abnormality of that kind is FDBattributable to a substitution of Arg by Gln at position3500 of apo B-100. In Germany, apo B-100 (Arg35003Gln)previously had been estimated to occur at a frequency of1 in 700 (22 ). Individuals who have inherited one mutantallele develop moderate hypercholesterolemia; the fewhomozygous carriers of the mutation described to datehave LDL-C concentrations similar to those observed inheterozygous LDL-receptor deficiency (39, 45, 46).
For many years, the replacement of Arg by Gln atposition 3500 was the only mutation known to produceligand-defective apo B-100. Reports of other apo B-100variants (Arg35313Cys and Arg35003Trp) unequivocallylinked to hypercholesterolemia have appeared only twiceto date (11, 12), whereas several detailed investigations ofthe apo B-100 gene sequence that codes for its receptor-binding function failed to detect any relevant mutationbeyond apo B-100 (Arg35003Gln) (10, 13, 47–49).
Nevertheless, when commencing this study, we hy-pothesized that other binding-defective species of apoB-100 functionally comparable to these mutations existedin the human population. To identify such mutations, wedesigned a TGGE-based procedure that enabled us tosearch for sequence variations in the region coding for theputative receptor-binding domain of apo B-100. We choseTGGE because it affords a high sensitivity (.95%) forpoint mutations if experimental conditions are optimized.As demonstrated in Fig. 2, within a 445-bp segment, fourdifferent mutations could be detected simultaneously.
Table 4. Lipid and lipoprotein concentrations (means 6 SD, g/L) of the hyperlipidemic individuals heterozygous formutations in the apo B-100 receptor-binding domain.
Genotypesubjects
Arg35003Glna
(n 5 40)Arg35003Trpb
(n 5 6)Glu34053Glnc
(n 5 4)Leu33503Leuc
(n 5 3)
TCd 2.71 6 0.41 2.59 6 0.59 2.64 6 0.55 2.73 6 0.17LDL-C 2.03 6 0.43 1.9 6 0.57 1.81 6 0.42 1.85 6 0.16TG 1.0 6 0.55 1.0 6 0.3 1.32 6 0.42 1.14 6 0.4HDL-C 0.48 6 0.11 0.49 6 0.07 0.56 6 0.18 0.65 6 0.08apo B 1.62 6 0.39 1.4 6 0.49 1.63 6 0.15 1.46 6 0.2
a Five of 40 subjects (10%) in this group received lipid-lowering drugs at the time of blood sampling.b Three individuals were on a lipid-lowering drug at the time of blood sampling.c No subjects were on lipid-lowering drugs at the time of blood sampling.d TC, total cholesterol; TG, triglyceride.
Fig. 4. Interaction of LDL from a heterozygous carrier of apo B-100(Glu34053Gln) with cultured human skin fibroblasts.LDL samples were prepared by ultracentrifugation and labeled with 125I asdescribed in Materials and Methods. Healthy human skin fibroblasts were grownin DMEM with 100 mL/L fetal calf serum. Forty hours before the experiment, thecells were switched to medium containing 100 mL/L human lipoprotein-deficientserum. Cells then received 125I-labeled LDL from a 52-year-old heterozygouscarrier with apo B-100 (Glu34053Gln) (f) and from a pool of normolipidemicdonors (F). Binding, uptake, and degradation were determined as described inMaterials and Methods. Each data point represents the mean of two experi-ments, each performed in triplicate. p, P ,0.05 vs control. The error barscorrespond to standard deviations.
1034 Fisher et al.: Ligand-defective apo B-100D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

Even two transitions at codon 3500, apo B-100(Arg35003Gln) and apo B-100 (Arg35003Trp), were dis-tinguishable by virtue of the 0.2 °C difference in theirmelting temperatures. We are convinced that TGGE rep-resents a valid and convenient alternative to direct se-quencing (10, 47), single-strand conformation polymor-phism (SSCP) (13, 48), and denaturing gradient gelelectrophoresis (15, 47, 49), which have been used toinvestigate the sequence encoding the putative receptorbinding of apo B-100. Compared with SSCP, TGGE hasthe advantage that substantially larger DNA fragmentscan be analyzed without diminishing sensitivity. Showingthat SSCP failed to identify two of nine samples heterozy-gous for apo B-100 (Arg35003Gln), Henderson et al. (50 )questioned the use of SSCP as a reliable method ofdetecting unknown apo B-100 point mutations. Com-pared with denaturing gradient gel electrophoresis,
TGGE offers more technical simplicity (homogeneous gelsinstead of gradient gels) and shorter run times. Anothereasy and high-throughput approach to test simulta-neously for the three FDB mutations has been heterodu-plex analysis (51 ). This technique does not distinguishbetween the various types of mutations and does notallow identification of homozygosity for mutant andwild-type DNA.
We detected two sequence abnormalities with uncer-tain pathobiochemical relevance. The first one was a silentmutation in the third position of codon 3350, which wasalso detected recently by Ludwig et al. (14 ) and Gaffney etal. (16 ). The second abnormality was a known variation(52 ) that leads to the incorporation of the negativelycharged amino acid glutamic acid in the place of glu-tamine at codon 3405. In our study, heterozygous carriersof this variant occurred at a relative frequency of 1.3%.
Fig. 5. Interaction of LDL from heterozygous carriers of apo B-100(Arg35003Gln), heterozygous carriers of apo B-100 (Arg35003Trp),and normal LDL with cultured human skin fibroblasts.LDL samples were prepared by ultracentrifugation and labeled with 125I asdescribed in Materials and Methods. Normal human skin fibroblasts were grownin DMEM with 100 mL/L fetal calf serum. Forty hours before the experiment, thecells were switched to medium containing 100 mL/L human lipoprotein-deficientserum. Cells then received 125I-labeled LDL from two apo B-100 (Arg35003Trp)heterozygotes, GR-098/I-2 (f) and L-1193/I-5 (Œ); from an apo B-100(Arg35003Gln) heterozygote (F); and from a pool of normolipidemic donors (E).Binding, uptake, and degradation were determined as described in Materials andMethods. Each data point represents the mean of three experiments, eachperformed in triplicate. p, P ,0.05 vs control.
Fig. 6. Competition of LDL from heterozygous carriers of apo B-100(Arg35003Gln) and apo B-100 (Arg35003Trp) compared with normalLDL for binding, uptake, and degradation of 125I-labeled LDL.LDL samples were prepared by ultracentrifugation and labeled with 125I asdescribed in Materials and Methods. Normal human skin fibroblasts were grownin DMEM with 100 mL/L fetal calf serum. Forty hours before the experiment, thecells were switched to medium containing 100 mL/L human lipoprotein-deficientserum. Cells then received 125I-labeled LDL at a protein concentration of 5 mg/Land unlabeled LDL from two apo B-100 (Arg35003Trp) heterozygotes, GR-098/I-2 (f) and L-1193/I-5 (Œ); from an apo B-100 (Arg35003Gln) heterozygote (F);and from a pool of normolipidemic donors (E) at concentrations indicated on they-axis. Binding, uptake, and degradation were determined as described inMaterials and Methods. Each data point represents the mean of three experi-ments, each performed in triplicate. p, P ,0.05 vs control.
Clinical Chemistry 45, No. 7, 1999 1035D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

This percentage is strikingly similar to the prevalence of1.4% observed by Gaffney et al. (16 ) in a sample of 928hyperlipidemic individuals. Haplotyping of that particu-lar locus revealed the same, previously assigned haplo-type (del, XbaI1, MspI1, EcoRI1, 39VNTR-37) in allcarriers (four subjects), suggesting a common ancestralorigin of the Glu34053Gln substitution. Studies conductedwith LDL from a heterozygous carrier of this mutationsuggested that the binding of the mutant LDL to LDLreceptors was the same as for normal LDL. Unlike thebinding, however, the receptor-mediated internalizationand the degradation of the mutant LDL were lowercompared with pooled LDL from healthy donors, thedifferences attaining statistical significance at the highestligand concentration. The implications of this finding aredifficult to determine at present. Pullinger et al. (44 ) andLudwig et al. (14 ) communicated that the binding of apoB-100 (Glu34053Gln) to the LDL receptor was the same asthat of normal LDL. In contrast, Gaffney et al. (16 )claimed that the ability to promote the growth of U937cells of LDL from nine heterozygotes for apo B-100(Glu34053Gln) with normal triglycerides was, on average,87% of normal. Our findings are consistent with bothunimpaired binding on the one hand and impaired cellu-lar uptake on the other hand. A speculative explanationfor that divergence of binding and uptake might be thatresidue 3405 is not involved in the binding of apo B-100 tothe LDL receptor but plays a role in mediating theconformational change of the receptor that precedes in-vagination, also suggesting that those domains of the LDLreceptor mediating binding do not completely overlapwith those triggering uptake of the complex of the recep-tor and the ligand.
Among the hypercholesterolemic subjects studied, 21individuals were found to be heterozygous for apo B-100(Arg35003Gln), corresponding to a frequency of apoB-100 (Arg35003Gln) of 7.1%, or 1 in 14 in that selectedgroup. If individuals below the age of 40 and above theage of 65 were disregarded, the relative frequency of themutation was 5.5%. If we assume a prevalence of at least25% for type IIa HLP (defined as LDL-C .1.55 g/L andtriglycerides ,2.00 g/L) in the general population 40 to 65years of age, this suggests a frequency of apo B-100(Arg35003Gln) of 1.4% in the Rhein-Main area. It is notlikely that this estimate is biased by the inclusion ofindividuals with CAD, type 2 diabetes, or hypothyroid-ism in our survey. The prevalence of CAD in the screenedpopulation 40–65 years of age was approximately two-fold higher than in the general population. This is, how-ever, not unexpected because we selected for increasedLDL-C. The prevalence of both hypothyreosis and type 2diabetes were within the ranges observed in Westernsocieties, indicating that the subjects that we screenedwere representative for the general population with re-gard to these characteristics. Our frequency estimate maybe conservative for two reasons. First, LDL-C concentra-tions exceeding 1.55 g/L may actually be more frequent in
middle-aged individuals than assumed here. For exam-ples, .40% of healthy males and females 45 or older hadLDL-C concentrations .1.55 g/L (155 mg/dL) in theMunster Heart Study (PROCAM), the largest prospectivestudy of coronary heart disease risk factors in Germany(53 ). Second, we supposed that apo B-100 (Arg35003Gln)is not present in individuals with other types of HLP, anassumption that may not apply in general because wesporadically observe carriers of apo B-100 (Arg35003Gln)with increased triglycerides. Thus, apo B-100(Arg35003Gln) appears to be more prevalent in the Rhein-Main area than in Switzerland, where it has been esti-mated to occur at a frequency of 1 in 209 in the generalpopulation (54 ), the highest prevalence reported in theliterature to date. The high frequency of FDB in this areamay explain the first discovery of a patient homozygousfor apo B-100 (Arg35003Gln) in Frankfurt in 1992 (39 ),when FDB genotyping became established in the routineanalysis of HLP in our laboratory.
We identified two families that contained six carriers ofapo B-100 (Arg35003Trp). The LDL-C concentrations pre-sented in Table 3 are compatible with the assumption thatapo B-100 (Arg35003Trp) causes hypercholesterolemia.However, definite assessment of the phenotypic conse-quences of this mutation was not possible for severalreasons: First, two of the six affected individuals were onlipid-lowering drugs. Second, there was only one unaf-fected individual in the L-1193 kindred. Third, anothergenetic factor for increased LDL-C may have been presentin the GR-098 kindred. apo B-100 (Arg35003Trp) wasinitially described in one Scottish and one Asian family(11 ), and then became evident only in Asian HLP patients(15, 19). The screening of large samples of HLP patients inNorth America (n .800) (14 ), England (n 5 562) (35 ), andScotland (n 5 412) (17 ) did not reveal any additionalcarriers of that variant. Therefore, we were surprised todetect two unrelated apo B-100 (Arg35003Trp) heterozy-gotes, both of Caucasian descent, in our sample. Evenmore surprising was the finding that the mutation wasassociated with two apo B haplotypes different from theones reported earlier in the Scottish family and thecommon haplotype shared by Asian HLP patients carry-ing apo B-100 (Arg35003Trp). The apo B-100(Arg35003Trp) substitutions might, therefore, have arisenindependently in our area. The binding, uptake, anddegradation of apo B-100 (Arg35003Trp) LDL was highercompared with apo B-100 (Arg35003Gln) LDL. Thisstands in contrast to the first report of the apo B-100(Arg35003Trp) mutation (11 ), in which the two mutationsaffecting codon 3500 were indistinguishable in an assaythat relied on the ability of LDL to promote the growth ofU937 cells. The reason for this disagreement may lie in thetechniques used to study LDL function. An advantage ofthe U937 cell proliferation assay over the classic bindingand uptake method proposed by Goldstein et al. (38 ) isthat it does not involve manipulation of the LDL particlesduring the iodination procedure. However, we obtained
1036 Fisher et al.: Ligand-defective apo B-100D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

essentially identical results when we used the two mutantLDLs as unlabeled competitors for labeled wild-type LDL,essentially ruling out that the observed differences wererelated to modifications of LDL during labeling. In nor-mal apo B-100, Arg3500 interacts with Trp4369. Mutation ofArg3500 causes the carboxy terminus of apo B-100 tointerfere with the binding of the positively charged clusterof residues at positions 3358–3370 to the LDL receptor(55 ). The functional difference between apo B-100(Arg35003Trp) and apo B-100 (Arg35003Gln) may thusindicate that Trp3500 still weakly interacts with Trp4369
through aromatic–aromatic interaction (bond strength of1–2 kcal/mol), whereas this interaction is entirely dis-rupted in the presence of Gln at position 3500.
In conclusion, our observations confirm that apo B-100(Arg35003Gln) is the most prevalent cause of ligand-defective LDL. However, they also demonstrate that FDBmay be more heterogeneous than previously assumed.This has considerable bearing on the diagnosis of ligand-defective LDL at the molecular level. Detection methodsdesigned solely for apo B-100 (Arg35003Gln) have beenapplied in many laboratories to date, whereas the possi-bility that other variants exist has largely been disre-garded. We therefore strongly recommend the use ofscreening strategies, such as TGGE, capable of detectingall known functionally relevant sequence variations of theapo B-100 receptor-binding domain.
A portion of this study was supported by a grant from theCenter of Clinical Research II (cardiovascular diseases) atthe Albert Ludwigs-University, Freiburg to W.M. Dr.Evelyn S.C. Koay from the National University Hospitalin Singapore generously supplied a DNA sample with theapo B-100 (Arg35003Trp) mutation. The DNA samplewith the apo B-100 (Arg35313Cys) mutation was a giftfrom Clive R. Pullinger, Cardiovascular Research Insti-tute, University of California, San Francisco, CA. Wethank Angela Eser for excellent laboratory assistance.
References1. Brown MS, Goldstein JL. A receptor-mediated pathway for choles-
terol homeostasis. Science 1986;232:34–47.2. Kane JP, Havel RJ. Disorders of the biogenesis and secretion of
lipoproteins containing the B apolipoproteins. In: Scriver CR,Beaudet AL, Sly WS, and Valle D, eds. The metabolic andmolecular basis of inherited disease, 7th ed. New York: McGraw-Hill, 1995:1853–86.
3. Myant NB. Cholesterol metabolism, LDL, and the LDL receptor.San Diego: Academic Press, 1990:465pp.
4. Knott TJ, Pease RJ, Powell LM, Wallis SC, Rall SC, Innerarity TL, etal. Complete protein sequence and identification of structuraldomains of human apolipoprotein B. Nature 1986;323:734–8.
5. Yang CH, Chen SH, Gianturco SH, Bradley WA, Sparrow JT,Tanimura M, et al. Sequence, structure, receptor-binding domainsand internal repeats of human apolipoprotein B-100. Nature1986;323:738–42.
6. Pease RJ, Milne RW, Jessup WK, Law A, Provost P, Fruchart J-C, etal. Use of bacterial expression cloning to localize the epitopes for
a series of monoclonal antibodies against apolipoprotein B 100.J Biol Chem 1990;265:553–68.
7. Law A, Scott J. A cross-species comparison of the apolipoproteinB domain that binds to the LDL receptor. J Lipid Res 1990;31:1109–20.
8. Innerarity TL, Weisgraber KH, Arnold KS, Mahley RW, Krauss RM,Vega GL, Grundy SM. Familial defective apolipoprotein B-100: lowdensity lipoproteins with abnormal receptor binding. Proc NatlAcad Sci U S A 1987;84:6919–23.
9. Soria LF, Ludwig EH, Clarke HRG, Vega GL, Grundy SM, McCarthyBJ. Association between a specific apolipoprotein B mutation andfamilial defective apolipoprotein B100. Proc Natl Acad Sci U S A1989;86:587–91.
10. Dunning AM, Houlston R, Frostegard J, Revill J, Nilsson J, Hamsten A,et al. Genetic evidence that the putative receptor binding domain ofapolipoprotein B (residues 3130 to 3630) is not the only region ofthe protein involved in the interaction with the low density lipoproteinreceptor. Biochim Biophys Acta 1991;1096:231–7.
11. Gaffney D, Reid JM, Cameron LM, Vass K, Caslake MJ, ShepherdJ, Packard CJ. Independent mutations at codon 3500 of theapolipoprotein B gene are associated with hyperlipidemia. Arterio-scler Thromb 1995;15:1025-9.
12. Pullinger CR, Hennessy LK, Chatterton JE, Liu W, Love JA, MendelCM, et al. Familial ligand-defective apolipoprotein B: identificationof a new mutation that decreases LDL receptor binding affinity.J Clin Investig 1995;95:1225–34.
13. Ilmonen M, Ebeling T, Viikari J, Ojala J-P, Tikkanen MJ. Screeningof the 39 two-thirds of the coding area of the apo B gene in Finnishhypercholesterolemic patients. Report of six new genetic variants.Atherosclerosis 1997;128:191–9.
14. Ludwig EH, Hopkins PN, Allen A, Wu LL, Williams RR, Anderson JL,et al. Association of genetic variations in apolipoprotein B withhypercholesterolemia, coronary artery disease, and receptor bind-ing of low density lipoproteins. J Lipid Res 1997;38:1361–73.
15. Choong M-L, Koay ESC, Khoo K-L, Khaw M-C, Sethi SK. Denaturinggradient-gel electrophoresis screening of familial defective apoli-poprotein B-100 in a mixed Asian cohort: two cases ofarginine35003tryptophan mutation associated with a unique hap-lotype. Clin Chem 1997;43:916–23.
16. Gaffney D, Hoffs MS, Cameron IM, Stewart G, O9Reilly DSJ,Packard CJ. Influence of polymorphism Q3405E and mutationA3371V in the apolipoprotein B gene on LDL receptor binding.Atherosclerosis 1998;137:167–74.
17. Wenham PR, Henderson BG, Penney MD, Ashby JP, Rae PWH,Walker SW. Familial ligand-defective apolipoprotein B-100: detec-tion, biochemical features and haplotype analysis of the R3531Cmutation in the UK. Atherosclerosis 1997;129:185–92.
18. Rabes JP, Varret M, Saint-Jore B, Erlich D, Jondeau G, Krempf M,et al. Familial ligand-defective apolipoprotein B-100: simulta-neous detection of the Arg35003Gln and Arg35313Cys mutationsin a French population. Hum Mutat 1997;10:160–3.
19. Tai D-Y, Pan J-P, Lee-Chen G-J. Identification and haplotypeanalysis of apolipoprotein B-100 Arg35003Trp mutation in hyper-lipidemic Chinese. Clin Chem 1998;44:1659–65.
20. Innerarity TL, Mahley RW, Weisgraber KH, Bersot TP, Krauss RM,Vega GL, et al. Familial defective apolipoprotein B-100: a mutationof apolipoprotein B that causes hypercholesterolemia [Review]. JLipid Res 1990;31:1337–49.
21. Tybjaerg-Hansen A, Gallagher J, Vincent J, Houlston R, Talmud P,Dunning AM, et al. Familial defective apolipoprotein B-100: detec-tion in the United Kingdom and Scandinavia, and clinical charac-teristics of ten cases. Atherosclerosis 1990;80:235–42.
22. Rauh G, Keller C, Schuster H, Wolfram G, Zollner N. Familialdefective apolipoprotein B-100: a common cause of primaryhypercholesterolemia [Review]. Clin Investig 1992;70:77–84.
Clinical Chemistry 45, No. 7, 1999 1037D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021

23. Geisel J, Schleifenbaum T, Weibhaar B, Oette K. Rapid diagnosisof familial defective apolipoprotein B-100. Eur J Clin Chem 1991;29:395–9.
24. Hansen PS, Rudiger N, Tybjaerg-Hansen A, Faergeman O, Gre-gersen N. Detection of the apoB-3500 mutation (glutamine forarginine) by gene amplification and cleavage with MspI. J LipidRes 1991;32:1229–33.
25. Ruzicka V, Marz W, Russ A, Gross W. Apolipoprotein B (Arg35003Gln)allele specific polymerase chain reaction: large-scale screening ofpooled blood samples. J Lipid Res 1992;33:1563–7.
26. Schuster H, Rauh G, Muller S, Keller C, Wolfram G, Zollner N.Allele-specific and asymmetric polymerase chain reaction amplifi-cation in combination: a one step polymerase chain reactionprotocol for rapid diagnosis of familial defective apolipoproteinB-100. Anal Biochem 1992;204:22–5.
27. Rust S, Funke H, Assmann G. Mutagenically separated PCR(MS-PCR): a highly specific one step procedure for easy mutationdetection. Nucleic Acids Res 1993;21:3623–9.
28. Mamotte CDS, van Bockxmeer FM. A robust strategy for screeningand confirmation of familial defective apolipoprotein B-100. ClinChem 1993;39:118–21.
29. Lehmann R, Koch M, Pfohl M, Voelter W, Haring H-U, Liebich HM.Screening and identification of familial defective apolipoproteinB-100 in clinical samples by capillary gel electrophoresis. J Chro-matogr A 1996;744:187–94.
30. Hennessy LK, Pullinger CR. Nonradioactive PCR-SSCP assay todetect apoB Arg3500 to Gln mutation using a minigel format.Biotechniques 1997;22:446–7.
31. Marz W, Gross W. Analysis of plasma lipoproteins by ultracentrif-ugation in a new fixed angle rotor: evaluation of a phosphotungsticacid/MgCl2 precipitation and a quantitative lipoprotein electro-phoresis assay. Clin Chim Acta 1986;160:1–18.
32. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concen-tration of low-density lipoprotein cholesterol in plasma, without useof the preparative ultracentrifuge. Clin Chem 1972;18:499–502.
33. Marz W, Ruzicka V, Fisher E, Russ AP, Schneider W, Gross W.Typing of the 39 hypervariable region of the apolipoprotein B gene:approaches, pitfalls, and applications. Electrophoresis 1993;14:169–73.
34. Boerwinkle E, Lee SS, Butler R, Schumaker VN, Chan L. Rapidtyping of apolipoprotein B DNA polymorphisms by DNA amplifica-tion. Association between Ag epitopes of human apolipoproteinB-100, a signal peptide insertion/deletion polymorphism, and a 39flanking DNA variable number of tandem repeats polymorphism ofthe apolipoprotein B gene. Atherosclerosis 1990;81:225–32.
35. Talmud PJ, Tamplin OJ, Heath K, Gaffney D, Day INM, HumphriesSE. Rapid testing for three mutations causing familial defectiveapolipoprotein B100 in 562 patients with familial hypercholester-olaemia [Letter]. Atherosclerosis 1996;125:135–7.
36. Havel RJ, Eder HA, Bragdon JH. The distribution and chemicalcomposition of ultracentrifugally separated lipoproteins in humanserum. J Clin Investig 1955;34:1345–53.
37. Goldstein JL, Brown MS. Binding and degradation of low densitylipoproteins by cultured human fibroblasts. Comparison of cellsfrom a normal subject and from a patient with homozygous familialhypercholesterolemia. J Biol Chem 1974;249:5153–62.
38. Goldstein JL, Basu SK, Brown MS. Receptor-mediated endocyto-sis of low-density lipoprotein in cultured cells. Methods Enzymol1983;98:241–60.
39. Marz W, Baumstark. MW Scharnagel H, Ruzicka V, Buxbaum S,Herwig J, et al. Accumulation of “small dense” low densitylipoproteins (LDL) in a homozygous patient with familial defectiveapolipoprotein B-100 results from heterogeneous interaction of
LDL-subfractions with the LDL-receptor. J Clin Investig 1993;92:2922–33.
40. Poland D. Recursion relation generation of probability profiles forspecific sequence macromolecules with long range correlations.Biopolymers 1974;13:1859–71.
41. Gotoh O, Tagashira Y. Locations of frequently opening regions onnatural DNAs and their relation to functional loci. Biopolymers1981;20:1043–58.
42. Huang LS, de Graaf J, Breslow JL. ApoB gene. MspI RFLP in exon26 changes amino acid 3611 from Arg to Gln. J Lipid Res1988;29:63–7.
43. Ludwig EH, McCarthy BJ. Haplotype analysis of the human apoli-poprotein B mutation associated with familial defective apoli-poprotein B100. Am J Hum Genet 1990;47:712–20.
44. Pullinger CR, Love JA, Liu W, Hennessy LK, Ghassemzadeh M,Newcomb KC, et al. The apolipoprotein B Q3405E polymorphismhas no effect on its low-density-lipoprotein receptor binding affin-ity. Hum Genet 1996;98:678–80.
45. Gallagher JJ, Myant NB. The affinity of low-density lipoproteins andof very-low-density lipoprotein remnants for the low-density lipopro-tein receptor in homozygous familial defective apolipoproteinB-100. Atherosclerosis 1995;115:263–72.
46. Funke H, Rust S, Seedorf J, Brennhausen B, Chirazi A, Motti C,Assmann G. Homozygosity for familial defective apolipoproteinB-100 (FDB) is associated with lower plasma cholesterol concen-trations than homozygosity for familial hypercholesterolemia (FH).Circulation 1992;86(Suppl I):I-691.
47. Avoustin P, Mostachi H, Perret B, Cambou JP, Cambien F, dePreval C. A very conservative region of ApoB-100 in the putativebinding region to the LDL receptor in the Toulouse population.Hum Genet 1992;90:460–3.
48. Ilmonen M, Helio T, Ebeling T, Pyorala K, Uusitupa M, Palotie A,Tikkanen MJ. Screening for mutations in the exon 26 of theapolipoprotein B gene in hypercholesterolemic Finnish families bythe single-strand conformation polymorphism method. Hum Mutat1994;4:217–23.
49. Nissen H, Hansen PS, Faergeman O, Horder M. Mutation screeningof the codon 3500 region of the apolipoprotein B gene by denaturinggradient-gel electrophoresis. Clin Chem 1995;41:419–23.
50. Henderson BG, Wenham PR, Ashby JP, Blundell G. Detectingfamilial defective apolipoprotein B-100: three molecular scanningmethods compared. Clin Chem 1997;43:1630–4.
51. Kotze MJ, Langenhoven E, Peeters AV, Theart L, Oosthuizen CJJ.Detection of two point mutations causing familial defective apoli-poprotein B-100 by heteroduplex analysis. Mol Cell Probes 1994;8:513–8.
52. Ludwig EH, Blackhart BD, Pierotti VR, Caiati L, Fortier C, Knott T,et al. DNA sequence of the human apolipoprotein B gene. DNA1987;6:363–72.
53. Assmann G, Cullen P, Schulte H. The Munster Heart Study(PROCAM). Results of follow-up at 8 years. Eur Heart J 1998;19(Suppl A):A2–11.
54. Miserez AR, Laager R, Chiodetti N, Keller U. High prevalence offamilial defective apolipoprotein B-100 in Switzerland. J Lipid Res1994;35:574–83.
55. Innerarity TL, Boren J. The receptor- and proteoglycan-bindingsites of LDL: engineering a nonatherogenic LDL [Abstract]. 13thInternational Symposium on Drugs Affecting Lipid Metabolism,Florence, May 30–June 3, 1998:7.
56. Boerwinkle E, Xiong W, Fourest E, Chan L. Rapid typing oftandemly repeated hypervariable loci by the polymerase chainreaction: application to the apolipoprotein B 39 hypervariableregion. Proc Natl Acad Sci U S A 1989;86:212–6.
1038 Fisher et al.: Ligand-defective apo B-100D
ownloaded from
https://academic.oup.com
/clinchem/article/45/7/1026/5643264 by guest on 01 D
ecember 2021