Line Insertion Technique & Follies
59
Line Complications Line Complications Dalhousie University Dalhousie University Critical Care Lecture Critical Care Lecture Series Series
-
Upload
andrew-ferguson -
Category
Health & Medicine
-
view
16.968 -
download
0
Transcript of Line Insertion Technique & Follies

Line ComplicationsLine Complications
Dalhousie UniversityDalhousie University
Critical Care Lecture SeriesCritical Care Lecture Series

ICUObjectivesObjectives
Know the indications and contraindications for central line insertion
Review the technique of central line insertion
Know the most common complications of central lines and arterial lines
Know how to prevent line complications
Know how to recognize and manage line complications
Examples

ICU CVP Catheter IndicationsCVP Catheter Indications
Pressure monitoring Mixed venous oxygen saturation Fluid administration during volume
resuscitation (may not be as good as large-bore peripheral lines!!)
Administration of corrosive or hypertonic fluids
Administration of vasoactive agents Lack of other sites

ICUCVP ContraindicationsCVP Contraindications
Severe coagulopathy Obstruction or congenital abnormality Patient refusal (if competent) Restless and uncooperative patient, unless
sedation can be utilized Lack of experience and no expert
supervision, OR previous failed attempt by experienced physician
Injury or infection at the site

ICU
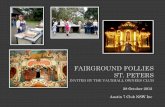
Normal CXR

ICUComplicationsComplications
More than 15% of all central lines have a complication Mechanical 5-19% Infectious 5-26% Thrombotic 2-26%

ICU
Mechanical Mechanical ComplicationsComplications

ICUMechanical InjuriesMechanical Injuries
Most common complications:
Type of complication
Number (/110)
Wire/catheter embolus 20
Cardiac tamponade 16
Carotid arteryCannulation/puncture
16
hemothorax 15
pneumothorax 14
Misc. (PA rupture,vessel injury, air embolism etc)
29Modified from Domino et al 2004

ICUPneumothoraxPneumothorax
More common in subclavian Incidence ranges from 0.3 to 3%
depending on experience Classic presentation =
hypoxemia/hypotension/pleuritic CP
Can be treated conservatively in non-ventilated patients

ICU

ICUTreatmentTreatment
Chest tube to expand lung
Insertion of chest tube may create hole in lung parenchyma leading to another complication:

ICU

ICUWrong VesselWrong Vessel
If finder needle or 18 g insertion needle in artery may remove and apply pressure
If CVC or PAC introducer is in artery remove catheter and apply pressure OR:
Consult CV surgeon/thoracic surgeon ? OR for thoracotomy, removal of catheter and repair of vessel

ICU

ICUThe Left Side is SinisterThe Left Side is Sinister
Left internal jugular has unique complications – thoracic duct injury
Left inominate vein can be lacerated hemothorax and OR
L IJ or SC catheter too proximal can lacerate SVC death

ICULeft Subclavian ArteryLeft Subclavian Artery

ICU

ICU

ICU
Prevention of Mechanical Prevention of Mechanical ComplicationsComplications

ICU
Prevention of Prevention of Mechanical Mechanical
ComplicationsComplications Ultrasound Guidance -Useful for internal jugular-Potentially prevents wrong vessel,
hemo/pneumothorax Pressure waveform monitor-Arterial cannulation/puncture CXR-Cardiac tamponade-Wire/catheter embolus

ICUUltrasound!Ultrasound!
Prevention is always better than treatment
Use ultrasound probe to localize vessel
Cannulate vessel under direct vision

ICU
Ultrasonographic Guidance:Ultrasonographic Guidance:Dynamic vs. StaticDynamic vs. Static
Dynamic Consists of ultrasonic
localization, and image-guided cannulation
More precise and “real time”
Difficult to keep sterility of transducer and site.
More hand to screen coordination, unless two persons involved
Static Consists of ultrasonic
localization and marking of landmarks only
Cannulation is not image-guided, but is separate
Time delay between marking and cannulation
Easy to keep sterility of transducer and site
Less technically demanding

ICUPressure WaveformsPressure Waveforms
Several options: Connect sterile tubing to
pressure tubing and flush Attach to needle in vessel and
confirm venous trace Remove syringe and confirm
non-pulsatile blood Compare arterial blood sample
with your sample

ICUIJ Insertion MethodIJ Insertion Method
Transverse orientation Longitudinal orientation

ICU Check Vein for PatencyCheck Vein for Patency
Thrombus
Vein should be free of clot and freely compressible
when pressure is applied with the probe

ICU
Transverse Orientation- Transverse Orientation- “Finger Wiggle”“Finger Wiggle”
Finger on one side of probe
Acoustic shadow of finger on same side of image

ICU
Orientation- “Mock Orientation- “Mock Poke”Poke”

ICU
Orientation- “Mock Orientation- “Mock Poke”Poke”
Acoustic “shadow” of the needle over the vein

ICUTechniqueTechnique
Steps: Obtain informed consent (unless emergency) Check radiograph for any existing pathology (put
line on the same side as pathology) Check coagulation studies, if indicated Position patient appropriately (see individual slides
for specifics) Prep/drape using sterile technique Inject local, making certain not to inject
intravascularly Using ultrasound, assess for proper orientation,
localize the vessel, and ensure patency Cannulate vessel and place catheter (see steps) Check radiograph to ensure correct position and to
evaluate for complications (can also use ultrasound to evaluate for pneumothorax and to look for incorrect placement, i.e., subclavian to IJ positioning)

ICUTechniqueTechnique
Sterile technique is extremely important Nosocomial bloodstream/catheter infections are very
prevalent, causing significant morbidity (and costing millions of dollars)
Most beginners make one of three mistakes: Contaminate gloves when putting them on Contaminate gloves when placing drapes Contaminate the wire by not paying close
attention to where it is/what it’s touching at all times
Use of ultrasound introduces more opportunity for contamination, SO BE CAREFUL

ICU

ICUIJ Insertion MethodIJ Insertion Method
After flash of blood, syringe is removed and a guidewire
is advanced to 20cm
The needle is then removed, leaving the guidewire in place

ICU
Position of guidewire in relation to neck anatomy
Make a small skin stab at wire insertion site.
Note control of guidewire with both hands
IJ Insertion MethodIJ Insertion Method

ICU
Dilate. If awake, tell
the patient “you’re going to feel some pressure.”
Advance the catheter over the wire. NEVER let go of the wire.
Grab it when it comes out the brown port
IJ Insertion MethodIJ Insertion Method

ICU
Most use infraclavicular approach (insert at “fossa” of deltopectoral groove, about 1-2 cm inferior to clavicle)
Poor choice in coagulopathy (difficult to compress) Higher PTX risk than internal jugular (1-5%) Less infection risk than IJ Trendelenburg’s position with towel roll under scapulae Direct needle toward sternal notch Keep needle parallel to floor; DO NOT AIM UNDER
CLAVICLE OR YOU WILL CAUSE PNEUMOTHORAX Constant suction in and out Ultrasound not as useful Again, think after inserting needle 5 cm deep
Insertion Method-Insertion Method-SubclavianSubclavian

ICU

ICUInsertion Site-FemoralInsertion Site-Femoral
Vein is medial to femoral artery In anatomic position
(legs apart), axis of vein is as pictured: toward umbilicus
Note the inguinal ligament!

ICU
Reverse Trendelenburg position (legs DOWN) to reduce chance of air embolus
Use for emergency access Try to remove after 72
hours Do not use if PA catheter
needs to be placed
At 45o angle to vessel, just medial to artery
Insertion Method-Insertion Method-FemoralFemoral

ICUImage and OrientationImage and Orientation

ICUInfectious ComplicationsInfectious Complications

ICU
Infectious Complications Infectious Complications PreventionPrevention

ICU
ManagemeManagementntof of
Line Line InfectionsInfections

ICU
Pulmonary Artery Pulmonary Artery CathetersCatheters
PAC have unique set of complications:
Arrhythmias inc. complete heart block
Knotting of the PAC
Pulmonary Artery infarction or rupture

ICUArterial LinesArterial Lines
Most common site = radial artery Rare complications 1983 Slogoff and Keats
prospective study 1699 radial artery cannulations
no ischemia or disability of hand Pseudoaneurysm of the radial
artery can occur
Bowdle Anesthesiology Clinics of NA 2002: 20

What’s Wrong With What’s Wrong With These Pictures?These Pictures?

ICU

ICU
ETT in too far

ICU
Chest tube in poor position

ICU
Left mainstem intubation

ICU
Feeding tube in lung

ICU
Feeding Tube in RLL

ICU
Subclavian going In wrong direction

ICU
Carotid Artery Insertion

ICU

ICU
HematomaAfterSubclavianArteryPuncture
NG
ETT

ICU

ICU
CTinsertionSubclavian
Line
NG Down LeftMainstem!!!!

ICU
ETT
SubclavianCrossingThroughinnominate

ICUSummarySummary
Ultrasound guided placement is becoming standard of care.
Consider waveform monitoring with all line insertions.
Do a CXR post line insertion and review it!
Three poke rule (get another person to do procedure)