Life Won't Wait Capstone Presentation - final presentation
20
Life Won’t Wait: Reducing Fatal Drug Overdoses In British Columbia Jordan Westfall Thesis Defense April 2 nd , 2015. 10:00 A.M.
-
Upload
jordan-westfall -
Category
Documents
-
view
103 -
download
4
Transcript of Life Won't Wait Capstone Presentation - final presentation
LifeWon’t Wait:Reducing Fatal Drug OverdosesIn British Columbia
Jordan WestfallThesis DefenseApril 2nd, 2015.10:00 A.M.
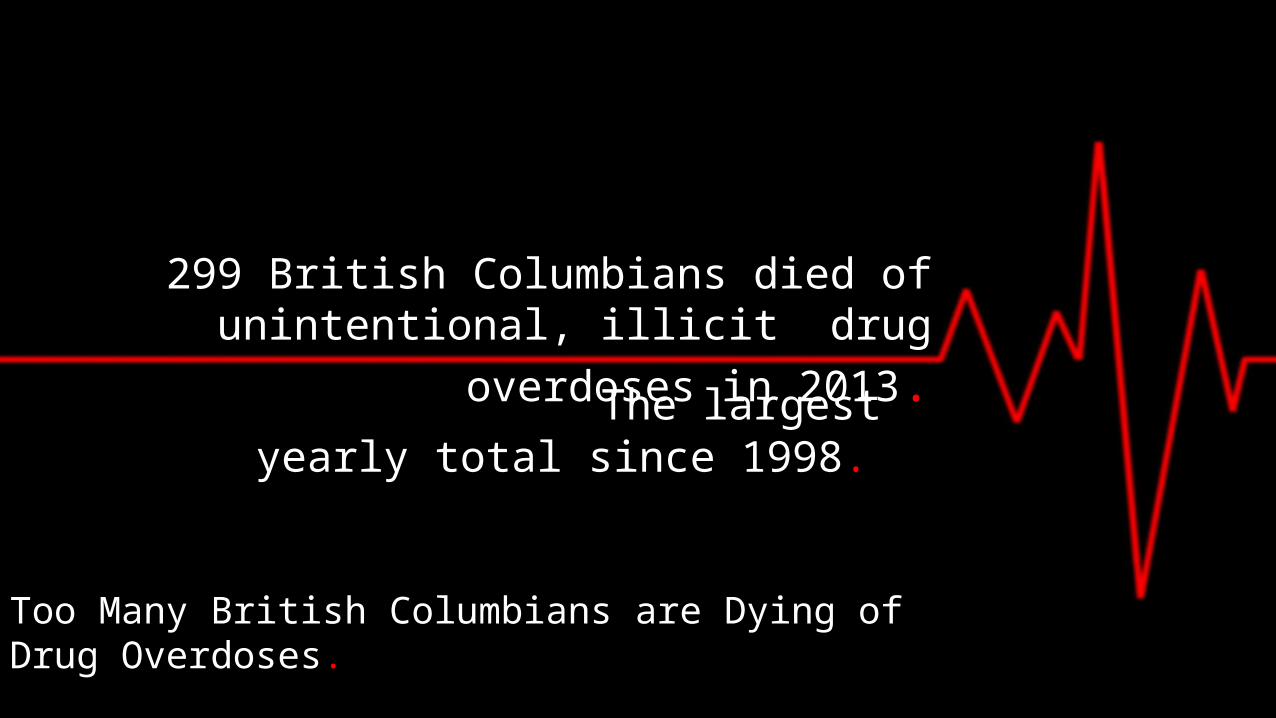
299 British Columbians died of unintentional, illicit drug overdoses in
2013. The largest yearly total since 1998.
Too Many British Columbians are Dying of Drug Overdoses..
What happened?
OxyContin, a prescription drug is taken off the market.Fentanyl sold as OxyContin or heroin illicitly. Led to worst weekend in Insite’s history for overdoses (31).
Prescription pain killer overdoses are also increasing.Chronic Pain, 22% of BC adults (Corneil, 2014).
Interior Region- 25, 000 people on opioid medications (Corneil, 2014).
Overdose Prevention in British Columbia• Take home naloxone program.
• Provides Overdose Education and Naloxone Training (OENT).
• OENT consists of:• Prevention of OD • Recognition/Response to OD.
Challenges:• Available by physician’s prescription only.• Must take training course.• Must have a history of opioid use.
How is policy is practiced?
Knowledge Gaps
• Barriers to enhancing overdose prevention.
• Drug user awareness of current policy.• Good practices from other jurisdictions.
Purpose of Research
• AIM: To develop policy at the provincial level to reduce drug overdose fatalities. • What role can public policy play in reducing fatal drug
overdoses in BC?• How can provincial legislation reduce fatal drug overdoses in
BC? • How have other jurisdictions reduced fatal drug overdoses?• Are drug users in Vancouver aware of the VPD’s overdose
prevention policy?
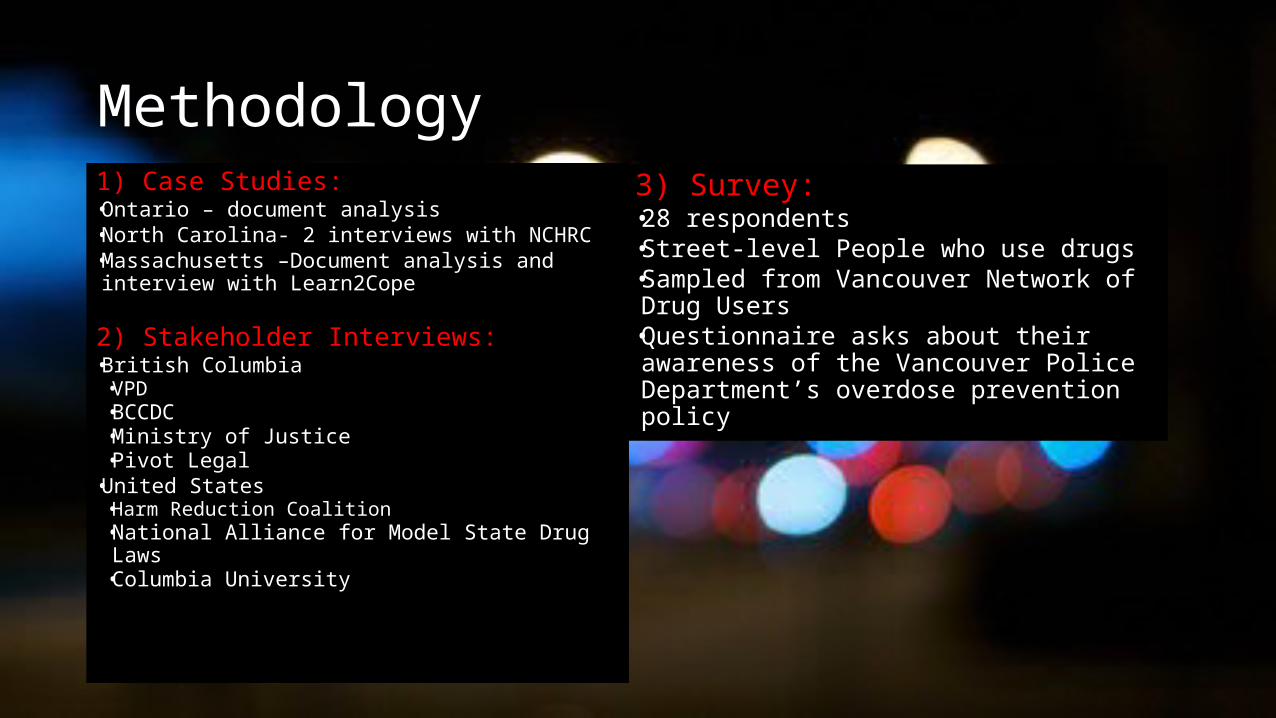
Methodology1) Case Studies:• Ontario – document analysis• North Carolina- 2 interviews with NCHRC• Massachusetts –Document analysis and
interview with Learn2Cope
2) Stakeholder Interviews: • British Columbia
• VPD• BCCDC• Ministry of Justice• Pivot Legal
• United States• Harm Reduction Coalition• National Alliance for Model State Drug
Laws• Columbia University
3) Survey: • 28 respondents• Street-level People who use drugs• Sampled from Vancouver Network of
Drug Users• Questionnaire asks about their
awareness of the Vancouver Police Department’s overdose prevention policy
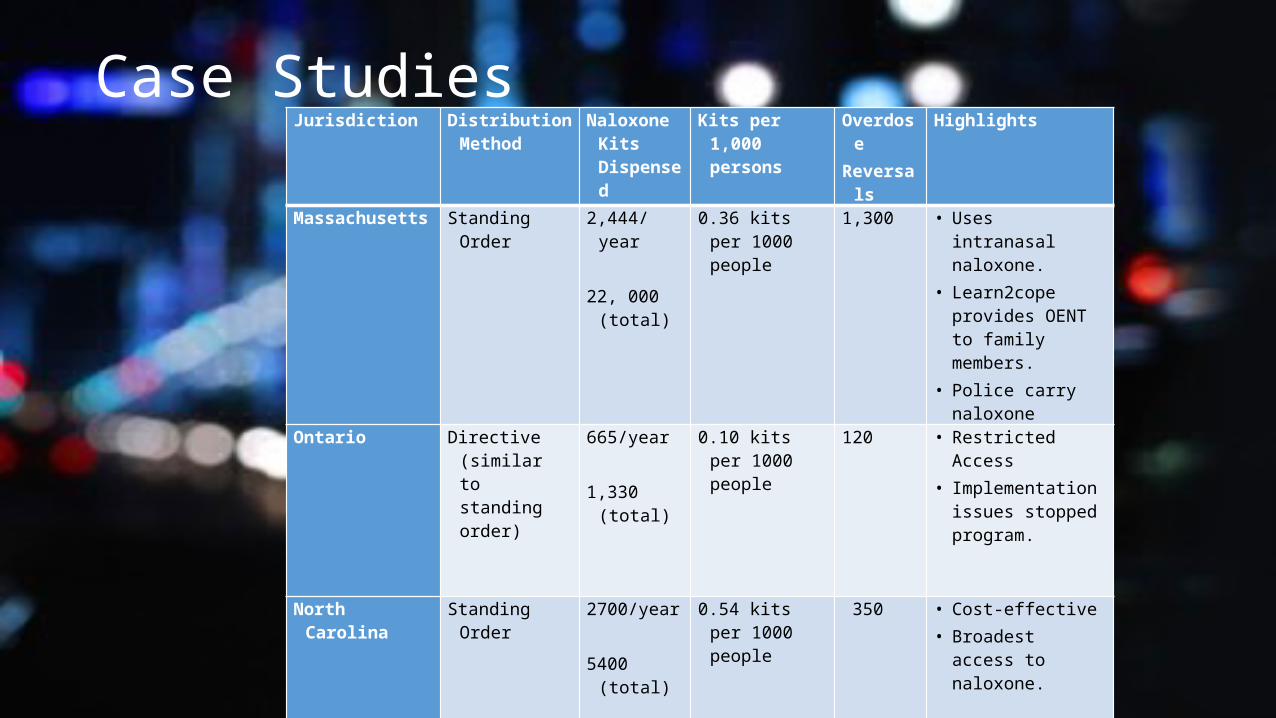
Case StudiesJurisdiction Distribution
MethodNaloxone Kits Dispensed
Kits per 1,000 persons
Overdose
Reversals
Highlights
Massachusetts
Standing Order
2,444/year
22, 000 (total)
0.36 kits per 1000 people
1,300 • Uses intranasal naloxone.
• Learn2cope provides OENT to family members.
• Police carry naloxone
Ontario Directive (similar to standing order)
665/year
1,330 (total)
0.10 kits per 1000 people
120 • Restricted Access• Implementation
issues stopped program.
North Carolina
Standing Order
2700/year
5400 (total)
0.54 kits per 1000 people
350 • Cost-effective• Broadest access
to naloxone.
British Columbia
Physician’sprescription
650/year1300
(total)
0.30 kits per 1000 people
125 • Comparative purposes only.
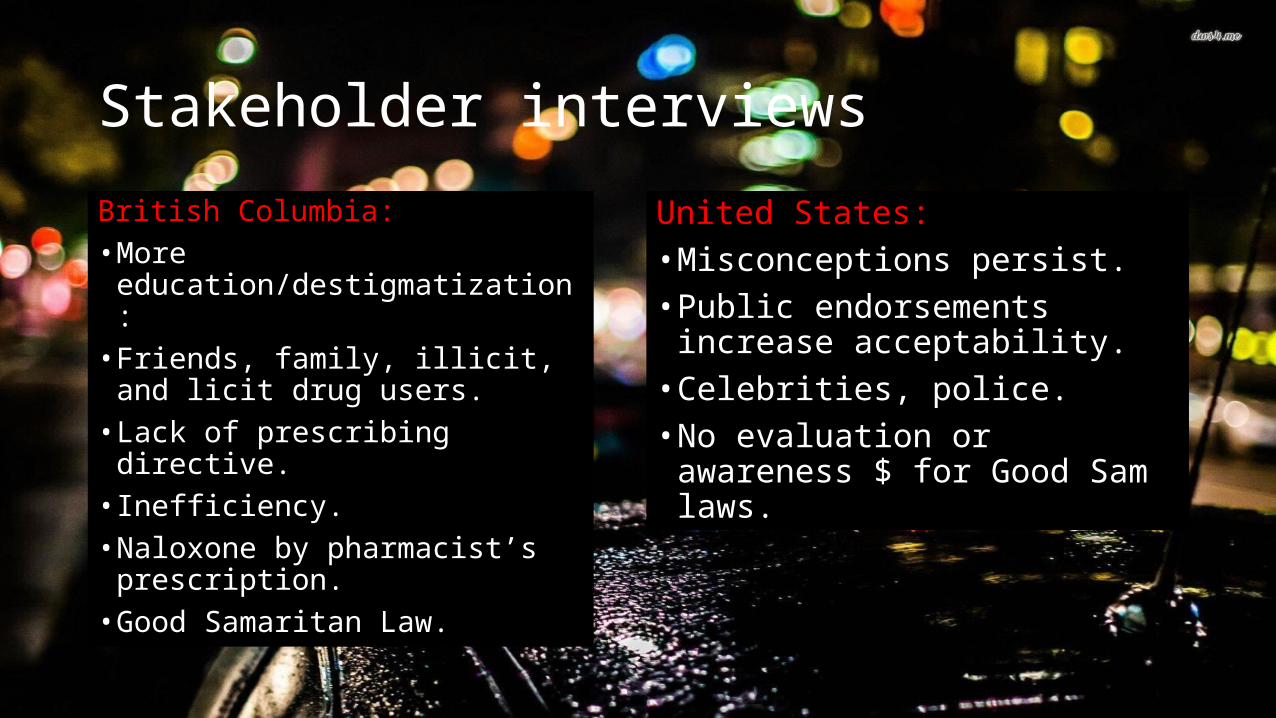
Stakeholder interviews
British Columbia:• More
education/destigmatization:• Friends, family, illicit, and
licit drug users.• Lack of prescribing
directive.• Inefficiency.• Naloxone by pharmacist’s
prescription.• Good Samaritan Law.
United States:• Misconceptions persist.• Public endorsements
increase acceptability.• Celebrities, police. • No evaluation or awareness
$ for Good Sam laws.
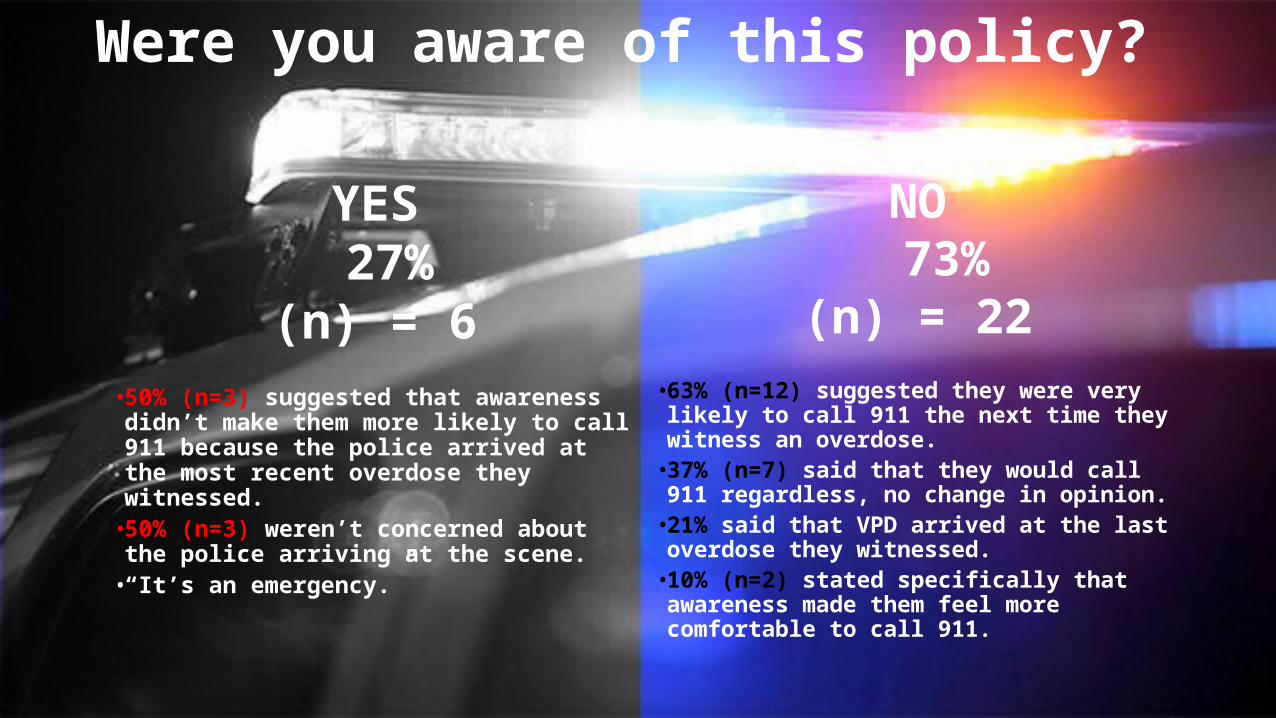
Were you aware of this policy?
YES 27%
(n) = 6• 50% (n=3) suggested that
awareness didn’t make them more likely to call 911 because the police arrived at the most recent overdose they witnessed.
• 50% (n=3) weren’t concerned about the police arriving at the scene.
• “It’s an emergency.”
NO 73%
(n) = 22• 63% (n=12) suggested they were
very likely to call 911 the next time they witness an overdose.
• 37% (n=7) said that they would call 911 regardless, no change in opinion.
• 21% said that VPD arrived at the last overdose they witnessed.
• 10% (n=2) stated specifically that awareness made them feel more comfortable to call 911.
Other policy considerations
Both VPD and drug users need to be considered. • Why not implement a Good Samaritan
law?
• Out of scope.
Intranasal naloxone.• Federal restrictions.
Staggered welfare cheque distribution.• No evidence thus far.
IM naloxone- cost effective
Policy Options are divided into two categories:1.) Overdose Education and Naloxone Training (OENT)2.) Naloxone Distribution
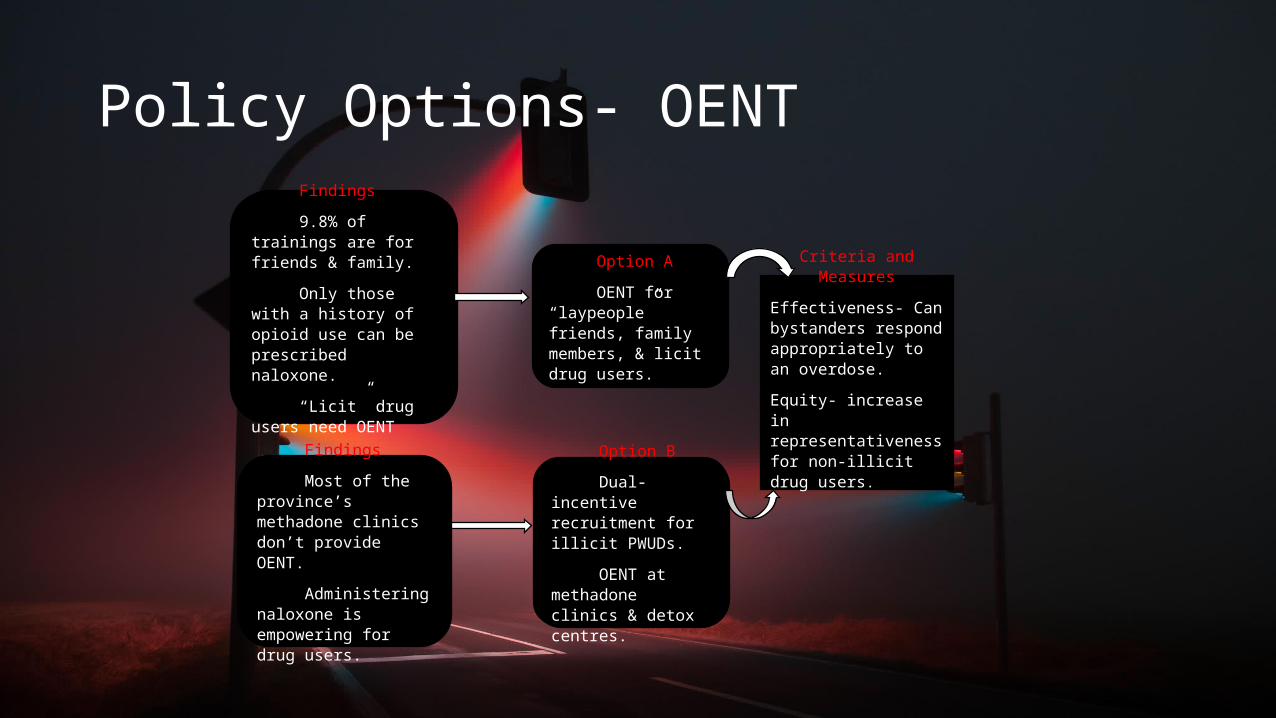
Policy Options- OENT
Findings
9.8% of trainings are for friends & family.
Only those with a history of opioid use can be prescribed naloxone.
“Licit” drug users need OENT
Findings
Most of the province’s methadone clinics don’t provide OENT.
Administering naloxone is empowering for drug users.
Option A
OENT for “laypeople” friends, family members, & licit drug users.
Option B
Dual-incentive recruitment for illicit PWUDs.
OENT at methadone clinics & detox centres.
Criteria and Measures
Effectiveness- Can bystanders respond appropriately to an overdose.
Equity- increase in representativeness for non-illicit drug users.

Policy Options- Naloxone Distribution
Findings
Having a physician prescribe naloxone is inefficient.
Licit drug users are overdosing at an increasing rate.
Adding naloxone to provincial formulary would make it free for Blue Cross members.
Findings
Overdose is leading cause of death among homeless in BC.
Jurisdictions that have liberalized access to naloxone have higher amounts of OD reversals.
Option A
Naloxone available by pharmacist’s prescription.
Option B
Nurse’s Decision Support Tool. (DST)
Criteria and Measures
Health & Safety- # of overdose reversals.
Effectiveness- # of naloxone kits dispensed.
OENT Option AStrengths• OENT for underrepresented
groups (family and friends).• Provides an access point
for support services• Addresses licit ODs.• Effective under current
regulations. when laypersons cannot receive naloxone kit.
Weaknesses• No support for illicit drug
users.
OENT Option B
Strengths• Empowerment for drug
users.• Reduced “enacted” and
“self-stigma”• Methadone clinics• Secondary trainings
Weaknesses• PWUDs already well represented
under current efforts (less of an impact)• Ideological resistance from
detox centres.
Naloxone Distribution Option A
Strengths• Convenience.
• Access for licit drug users and methadone patients.
• Easy to get follow-up kits.
• Reduces prescribing burden on physicians.
• Added to Blue Cross
• No need to use Telehealth in rural regions.
Weaknesses • Pharma Net.
• Negative externalities.
• Licit drug users have to make separate trips for OENT and kit.
Naloxone Distribution Option B
Strengths
• Cohesion with OENT options.
• Reduces physician prescriber burden.
• Outreach efforts (street nurses, etc)
Weaknesses
• Cost inefficiencies
• Clinic or other healthcare visit required.
• Follow up kits require healthcare visit.
Recommendations• OENT efforts should be expanded to
focus on friends, family members and licit drug users.
• Nurse’s DST: helpful for homeless populations.
• Naloxone distribution by pharmacist’s prescription for the rest of the population.
• Each naloxone distribution option is cost effective.
Future Considerations
• Reduce waitlists for drug rehabilitation services.
• Drug reformulations can increase overdoses.
• Instruct police departments not to respond to overdose 911 calls.
Conclusions
BC is leading Canada toward a rational, scientific drug policy.
Naloxone is not a “magic-bullet”.
But we’re losing ground
to the United States. Liberal access to naloxone.
Good Samaritan Laws.
Housing, employment training, rehab services.
These things help people stay
off of drugs.