Life expectancy at birth - UNSCN · Metabolic Programming CHO, Lipids, Proteins...
6
Addressing The Challenge Of The Double Burden Of Disease In Developing Countries Objectives: 1. Examine Progress in Addressing the Challenge of Nutrition/Physical Activity Related Chronic Diseases (NRCDs) in Latin America; lessons learnt from successes and failures. 2. Update on the Implementation of Global Strategy for the Prevention and Control of NRCDs The Nutrition-Infection complex determines in great part, how children grow physically and develop mentally. Diet-Physical Activity interactions greatly affect what diseases we most likely will suffer during our life span and finally how we will age and die. The lifecourse approach to health and nutrition 0 25 50 75 100 20 40 60 80 100 120 1930 1960 2000 Foetus / Infants / Children • LBW/IUGR • Stunting and wasting • Micronutrient deficiency (Vit A,I,Fe,Zn ) • Infection (HIV/AIDS) • Accidents Adults / Elderly • Cardiovascular Stroke, • Obesity /Diabetes/dyslipidemia • Cancer • Osteoporosis • Healthy Aging Ideal % survival Disability Physical /Mental • Accidents Life expectancy at birth Life expectancy at birth Life expectancy at birth Developed and developing countries, 1955–2002 1940 1960 1980 2000 2020 80 70 60 50 40 30 20 10 0 Life expectancy at birth (years) Developed Developing: low mortality high mortality Developed Developed Developing: low mortality Developing: low mortality high mortality high mortality Albaneide Peixinho 1960 1970 1980 1990 2000 LIFE EXPECTANCY AT BIRTH 1960-2000 McMichael THE LANCET Vol 363 2004 1960 1970 1980 1990 2000 LIFE EXPECTANCY AT BIRTH 1960-2000 McMichael THE LANCET Vol 363 2004 Albaneide Peixinho Cause of Death by WHO region WHR 2002
Transcript of Life expectancy at birth - UNSCN · Metabolic Programming CHO, Lipids, Proteins...

1
Addressing The Challenge Of The Double Burden Of Disease In
Developing Countries
Objectives:
1. Examine Progress in Addressing the Challenge of Nutrition/Physical Activity Related Chronic Diseases (NRCDs) in Latin America; lessons learnt from successes and failures.
2. Update on the Implementation of Global Strategy for the Prevention and Control of NRCDs
Years of age
The Nutrition-Infection complex determines in great part, how children grow physically and develop mentally. Diet-Physical Activity interactions greatly affect what diseases we
most likely will suffer during our life span and finally how we will age and die.
The lifecourse approach to health and nutrition
0
25
50
75
100
20 40 60 80 100 120
1930
1960
2000
Foetus / Infants / Children• LBW/IUGR • Stunting and wasting• Micronutrient deficiency (Vit A,I,Fe,Zn ) • Infection (HIV/AIDS) • Accidents
Adults / Elderly• Cardiovascular Stroke,• Obesity /Diabetes/dyslipidemia• Cancer• Osteoporosis
• Healthy Aging
Ideal
%
surv
ival
DisabilityPhysical /Mental
• Accidents
Life expectancy at birthLife expectancy at birthLife expectancy at birthDeveloped and developing countries, 1955–2002
1940 1960 1980 2000 2020
80
70
60
50
40
30
20
100
Life e
xpec
tancy
at bi
rth (y
ears)
DevelopedDeveloping: low mortality
high mortality
DevelopedDevelopedDeveloping: low mortalityDeveloping: low mortality
high mortalityhigh mortality
Albaneide Peixinho1960 1970 1980 1990 2000
LIFE EXPECTANCY AT BIRTH 1960-2000
McMichael THE LANCET Vol 363 2004
1960 1970 1980 1990 2000
LIFE EXPECTANCY AT BIRTH 1960-2000 McMichael THE LANCET Vol 363 2004
Albaneide Peixinho
Cause of Death by WHO region WHR 2002

2
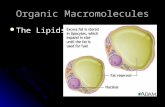
Deaths, by broad cause group and by age(2000 WORLD)
0-4 5-14 15-29
45-59
30-44
Noncommunicablediseases
Injuries
Communicable, maternal,perinatal and nutritionalconditions
60-69 70-79 80+
Source: WHR 2002 Database
Deaths attributable to 16 leading risk factors: all countries, 2001
30003000 60006000 70007000 8000800000 10001000 20002000
Deaths (000)Deaths (000)40004000 50005000
Low mortality – Developing countriesHigh mortality – Developing countries
Developed countries
Adapted from World Health Report 2003
Blood pressureTobacco Use
CholesterolUnderweight
Unsafe sexFruit & vegetableHigh body mass IndexPhysical inactivityAlcohol
Unsafe water, hygiene
Indoor smoke/fuelsIron deficiency
Urban air pollutionZinc deficiencyVitamin A deficiencyUnsafe health/injections
Albaneide Peixinho
Developed countriesDeveloping countries
High Mortality Low Mortality
= Major NCD risk factor
1 Underweight Alcohol Tobacco
2 Unsafe sex Underweight Blood pressure
3 Unsafe water Blood pressure Alcohol
4 Indoor smoke Tobacco Cholesterol
5 Zinc deficiency Body mass index Body mass index
6 Iron deficiency Cholesterol Low fruit & veg. intake
7 Vitamin A deficit Iron deficiency Physical inactivity
8 Blood pressure Low fruit & vegetable intake Illicit drugs
9 Tobacco Indoor smoke from solid fuels Underweight
10 Cholesterol Unsafe water Iron deficiency
Source: World Health Report 2002
Leading 10 risk factors that contribute to the burden of disease
= Major undernutrition risk factor
Albaneide Peixinho
% of total DALYs lost
Energy Imbalance
Under nutrition
… those who need less energy have more than
they spend
Those who needmore food have less
..while...
ArgentinaChile
Peru
BoliviaCosta RicaUruguay
MexicoBrazil
NicaraguaPanama
BarbadosJamaicaColombia
Venezuela
El SalvadorSaint Lucia
HondurasSurinameHaiti
Guyana
Trinidad and Tobago
Guatemala
Dominican Republic
-10 -5 0 5 10 15
% emaciación (P/T<-2 DE) % sobrepeso (P/T>+2 DE)% Underweight (W/H <- 2 SD) % Obese (W/H <+ 2 SD)
Under and Overweight in Latin American Children
De Onis et al IJO 2004

3
,
Globalization of Unhealthy Consumption
Branding is used to promote
consumption through marketing
Interest in foreign investment is used to preclude government
regulation
GLOBAL Obesity Epidemic
Addressing The Challenge Of The Double Burden Of Disease In
Developing Countries16:05-17:00 Focus On The Nutrition Transition In Latin America
Can we Control and Prevent Malnutrition while Addressing the Challenge of Nutrition/Physical Activity Related Chronic DiseasesJuan Rivera (INSP Cuernavaca, Mexico) 15
Addressing the Inequalities in the Distribution of Nutrition/ Physical Activity Related Chronic DiseaseCarlos Monteiro (Public Health USP Sao Paulo, Brazil) 15 min
Taking Effective Action in the Prevention and Control of Nutrition /Physical Activity Related Chronic Disease: Successes and Failures.Fernando Vio (INTA U of Chile, Santiago, Chile) 15 min
General discussion 10 minutes
Addressing The Challenge Of The Double Burden Of Disease In
Developing Countries
17:00- 17:20 Implementation of the WHO Global Strategy for the Prevention and Control of NRCDs: What Should/Can Developing and Transitional Countries Actually Do (Denise Cointinho).
17:20-17:30 FAO update on Global Food Systems in Transition (Kraisid Tontisirin).
17:30 -17:55 General discussion
17:55 Concluding remarks R. Uauy
Infection and other
EnvironmentalFactors
Brain Development
Growth muscle/boneWeight & HEIGHTBody composition
Metabolic ProgrammingCHO, Lipids, Proteinshormone,receptor,gene
Fetal & Infant
nutrition
Short term
Immunity
Work Capacity
DiabetesObesityCardiovascularDisease,Stroke Hyper-tensionCancerAging
Cognitivecapacity & Education
Long termNutritionDiet
Age (years)
302826242220181614121086420
BMI '
Z Sc
ore'
.4
.3
.2
.1
0.0
-.1
-.2
Population average
Diabetic/IGT
Age (years)
302826242220181614121086420
BM
I 'Z
Sco
re'
.7
.6
.5
.4
.3
.2
.1
0.0
-.1
-.2
Population average
Hypertension
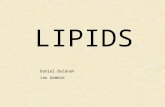
Early Origins of Adult Health Diabetes/IGT
Hypertension
BM
IZ
Age yrs
BM
IZ
Age yrs

4
Albaneide Peixinho
BMI SD Score from birth to adulthood(forthose developing impaired GTT or Diabetes)
Bhargava SK et al NEJM 350: 865-875 2004Albaneide Peixinho
Height SD Score from birth to adulthood (for those developing impaired GTT or Diabetes)
Bhargava SK et al NEJM 350: 865-875 2004
Intergenerational effectsIntergenerational effects
ADULTSMalnourished
AdolescentStunted
PregnancyLow Weight
Gain
ElderlyMalnourished
ChildStunted
BabyLow Birth
Weight
Higher maternal mortality
Inadequate food, health &
care
Inadequate food, health
& care
Inadequate food,
health & care
Reduced mental
capacity
Reduced mental
capacity
Reduced capacity to
care for baby
Foetal Malnutrition
Higher mortality
rateImpaired mental
development
Untimely / inadequate weaning
Frequent infections
Inadequate food, health
& care
Inadequate growth
Visceral obesity, BP, Diabetes
Rapid catch-upweight not length
Energy Excess CHO/FAT
Albaneide Peixinho
G Eriksson BMJ 2001;322:949–53
BMJ 2001
Albaneide Peixinho Albaneide Peixinho
Each red dot is 5000 deaths per year
Global Death in Children < 5years old (WHO 2000)

5
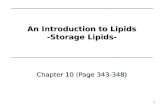
Sources:For cause-specific mortality: EIP/WHO using 1999 data.For deaths associated with malnutrition: Caulfield LE, Black RE. Malnutrition and the global burden of disease: underweight and cause-specific mortality.
Diarrhoea12%
Other29%
Pneumonia20%
Malaria8%
Measles5%HIV/AIDS
4%
Perinatal22%
Major causes of death among children under five, global, 2000
Deaths associated with undernutrition
60%
Albaneide Peixinho
**
**
**
**
Risks Associated to Global Deaths 2000*
**
(x 000)
Albaneide Peixinho
1961
1999
Dietary energy Supply (DES)
Kcal/kg/dGNP US $ per caput
% Obesity by GNP & Education
Monteiro and Popkin 2004
Very poor Poor
More educated
Less educated
0 20 40 60 80
Chile
Mexico
Colombia
Brasil
Ecuador
Peru
Bolivia
Haiti
Guatemala
80's
95's
Prevalence of Stunting in Children < 3yrs
% Height for age < 2 SDWHO/PAHO 2000
Albaneide Peixinho
Progress in MDGs Latin America
Albaneide Peixinho

6
- Fundo Nacional de Desenvolvimento da Educação
“VAMOS CRIAR AS CONDICIONES PARA QUE TODAS AS PESSOAS NO NOSSO PAÍS POSSAM COMER DECENTEMENTE TRÊS VEZES AO DIA, TODOS OS DIAS.
O BRASIL ÑAO PODE CONTINUAR CONVIVENDO COM TANTA DESIGUALDADE. PRECISAMOS VENCER A FOME, A MISÉRIA E A EXCLUSION SOCIAL.
NOSSA GUERRA ÑAO É PARA MATAR NINGUÉM – É PARA SALVAR VIDAS”
LUIZ INÁCIO LULA DA SILVAPRESIDENTE DA REPÚBLICA DO BRASIL
Consultation Process Consultation Process
Memberstates
Memberstates
Civil SocietyCivil
SocietyPrivatesector
Privatesector
UN agencies
UN agenciesPh
ase
II
WHO Strategy on Diet, Physical Activity and HealthWHO Strategy on Diet, Physical Activity and Health
WHA 2004WHA 2004
EB Jan 2004EB Jan 2004SecretariatSecretariatReference
groupReference
group
Phas
e III
Preparation of consultation process and finalization of expert report
Preparation of consultation process and finalization of expert report
Phas
e I