LIFE EVENTS AND SUBSEQUENT ILLNESS - Johns ... of weighting is not the best way to measure...
13
AMERICAN JOURNAL OF EPIDEMIOLOGY Vol. 104, No. 2 Copyright © 1976 by The Johns Hopkins University School of Hygiene and Public Health Printed in U.SA. LIFE EVENTS AND SUBSEQUENT ILLNESS 1 EVELYN L. GOLDBERG 2 AND GEORGE W. COMSTOCK 2 Goldberg, E. L. (Training Center for Public Health Research, Johns Hopkins School of Hygiene and Public Health, P.O. Box 2067, Hagerstown, MD 21740) and G. W. Comstock. Life events and subsequent illness. Am J Epidemiol 104:146-158, 1976. The objective was to examine for relationships between stress, as measured by life events, and hospitalization or death during the following 6 to 12 months, using a case-control design. As part of the Community Mental Epidemiology Program, life events data for the preceding year were gathered on a random sample of the population at two sites, and health data for the interval between interviews were collected at follow-up. A case is defined as anyone becoming ill and being hospitalized or dying during the interval between interviews. Each case was individually matched by several variables to a control who had neither been sick nor hospitalized. There were no significant demographic differences between cases and controls in either site or between sites. When life events were examined by various scoring methods, there were no differences between cases and controls. This finding is important since most longitudinal studies that have shown a positive relationship between life events and subsequent illness have had methodologic limitations or have been based on healthy, young, male populations who generally did not become seriously ill during the study period. The results of this study plus the lack of generalizability of pre- vious findings and their somewhat conflicting results raise serious questions about the etiologic relationship of life events to subsequent illness. death; health surveys; hospitalization; life events; stress INTRODUCTION general way since the early days of re- The effects of mental stress on the body C0 J ded , history - H [PP ocrates discussed and its functions have been recognized in a physical symptoms brought on by specific emotional states (1). Major scientific tests Received for publication December 10, 1975, and in of this belief began with Cannon who final form March 2,1976. reported in 1929 that strong emotions could 1 From the Center for Epidemiologic Studies^ Na- cause defm i te physiologic changes (2). tional Institute of Mental Health, Rockville, MD; the . . ° . ° ' Department of Epidemiology and Training Center for Among the clinical applications of this Public Health Research, School of Hygiene and Pub- work was Adolf Meyer's teaching that a lie Health, Johns Hopkins University, Baltimore, chart of i mpor tant events in a person's life MD; and the greater Kansas City Mental Health . . Foundation, Kansas City, MO. could often be helpful in arriving at a 2 Training Center for Public Health Research, medical diagnosis (3). This was followed by ^ Hopkins School of Hygiene and Public Health, oth k m the field of psyc hosomatic P.O. Box 2067, Hagerstown, MD 21740 (address for v J reprints). Supported in part by Contracts PH 43-67-1324 and Hornstra, Director, Greater Kansas City Mental HSM 42-71-32 from the National Institute of Mental Health Foundation for permission to use their data. Health, and Research Career Award HL 21,670 from The authors also appreciate the assistance and en- the National Heart and Lung Institute. couragement given by the staff of the Center for The authors wish to express their thanks to Dr. Epidemiologic Studies, and the careful collection and Robert E. Markush, former Chief, and Ben Z. Locke, coding of the basic information by the staffs of the Acting Chief, Center for Epidemiologic Studies, Na- Greater Kansas City Mental Health Foundation and tional Institute of Mental Health, and Dr. Robijn K. the Training Center for Public Health Research. 146
Transcript of LIFE EVENTS AND SUBSEQUENT ILLNESS - Johns ... of weighting is not the best way to measure...

AMERICAN JOURNAL OF EPIDEMIOLOGY Vol. 104, No. 2
Copyright © 1976 by The Johns Hopkins University School of Hygiene and Public Health Printed in U.SA.
LIFE EVENTS AND SUBSEQUENT ILLNESS1
EVELYN L. GOLDBERG2 AND GEORGE W. COMSTOCK2
Goldberg, E. L. (Training Center for Public Health Research, Johns HopkinsSchool of Hygiene and Public Health, P.O. Box 2067, Hagerstown, MD 21740)and G. W. Comstock. Life events and subsequent illness. Am J Epidemiol104:146-158, 1976.
The objective was to examine for relationships between stress, as measuredby life events, and hospitalization or death during the following 6 to 12 months,using a case-control design. As part of the Community Mental EpidemiologyProgram, life events data for the preceding year were gathered on a randomsample of the population at two sites, and health data for the interval betweeninterviews were collected at follow-up. A case is defined as anyone becoming illand being hospitalized or dying during the interval between interviews. Eachcase was individually matched by several variables to a control who had neitherbeen sick nor hospitalized. There were no significant demographic differencesbetween cases and controls in either site or between sites. When life eventswere examined by various scoring methods, there were no differences betweencases and controls. This finding is important since most longitudinal studiesthat have shown a positive relationship between life events and subsequentillness have had methodologic limitations or have been based on healthy,young, male populations who generally did not become seriously ill during thestudy period. The results of this study plus the lack of generalizability of pre-vious findings and their somewhat conflicting results raise serious questionsabout the etiologic relationship of life events to subsequent illness.
death; health surveys; hospitalization; life events; stress
INTRODUCTION general way since the early days of re-
The effects of mental stress on the body C0Jded , h i s t o r y - H [ P P o c r a t e s discussedand its functions have been recognized in a p h y s i c a l symptoms brought on by specific
emotional states (1). Major scientific tests
Received for publication December 10, 1975, and in of this belief began with Cannon whofinal form March 2,1976. reported in 1929 that strong emotions could
1 From the Center for Epidemiologic Studies^ Na- c a u s e d e f m i t e physiologic changes (2).tional Institute of Mental Health, Rockville, MD; the . . ° . ° 'Department of Epidemiology and Training Center for Among the clinical applications of thisPublic Health Research, School of Hygiene and Pub- work was Adolf Meyer's teaching that alie Health, Johns Hopkins University, Baltimore, c h a r t o f i m p o r t a n t events in a person's lifeMD; and the greater Kansas City Mental Health . .Foundation, Kansas City, MO. could often be helpful in arriving at a
2Training Center for Public Health Research, medical diagnosis (3). This was followed by^ Hopkins School of Hygiene and Public Health, o t h k m t h e field o f p s y c hosomat icP.O. Box 2067, Hagerstown, MD 21740 (address for v J
reprints).Supported in part by Contracts PH 43-67-1324 and Hornstra, Director, Greater Kansas City Mental
HSM 42-71-32 from the National Institute of Mental Health Foundation for permission to use their data.Health, and Research Career Award HL 21,670 from The authors also appreciate the assistance and en-the National Heart and Lung Institute. couragement given by the staff of the Center for
The authors wish to express their thanks to Dr. Epidemiologic Studies, and the careful collection andRobert E. Markush, former Chief, and Ben Z. Locke, coding of the basic information by the staffs of theActing Chief, Center for Epidemiologic Studies, Na- Greater Kansas City Mental Health Foundation andtional Institute of Mental Health, and Dr. Robijn K. the Training Center for Public Health Research.
146

LIFE EVENTS AND SUBSEQUENT ILLNESS 147
medicine implicating stressful events asprecursors of disease (4, 5).
Following Meyer's work, a variety ofresearch instruments including open-ended interviews and structured question-naires have been used in attempts to quan-tify the impact of life events. Holmes andMasuda, working with others, used a lifechart device to study events that precededthe onset of various diseases (6). This workled to the Social Readjustment RatingQuestionnaire in which each life event wasgiven a weight obtained by using themethods of psychophysics (7, 8). The scaleis based on the concept that any change,pleasant or unpleasant, is considered astressor (9). A list of 43 events "whoseadvent is either indicative of or requires asignificant change in the ongoing life pat-tern of the individual" was presented to394 subjects (10). They were asked to rateeach event against marriage as a standard,which was given a weight of 500. A valuewas given to each event depending onwhether it would take more or less adjust-ment than marriage. Based on the entiresample, the weight for each event becamethe mean value divided by ten (7). Theseweights were found to be similar for differ-ent demographic subgroups. Adding theweights for each reported item yields atotal Life Change Unit score for an individ-ual.
Since then, several studies have com-pared the rankings of the life events of theSocial Readjustment Rating Questionnaireamong a variety of populations. Masudaand Holmes showed that the rankingsgiven by Japanese and American sampleswere similar (11). Rahe demonstrated cor-relations ranging from .62 to .94 betweenrank orderings of the life events by avariety of population samples, includingwhite, black, Hawaiian and Mexican Ame-ricans, and Japanese, Danish, and Swedishpeople (12). Harmon et al. administeredthe Social Readjustment Rating Question-naire to samples of the French, Belgian and
Swiss populations. They found the weightsgiven to life events by those groups to besimilar to the weights from the Americangroups and a composite European group(13). Other methodologic studies have alsosupported the finding that a variety ofpeople agree on the seriousness of lifeevents (14, 15). Differences noted in theranking of certain individual events, havebeen attributed to the cultural backgroundsof the subjects (8, 12, 13).
Although Dohrenwend, when examiningthe psychologic effect of stressful lifeevents, felt that "change rather thanundesirability is the characteristic of lifeevents that should be measured for themore accurate assessment of their stress-fulness" (16), some authors feel that thiskind of weighting is not the best way tomeasure stressfulness of life events. Lifeevents have been categorized as gains orlosses, according to their independence ofeach other and their desirability; and asexits and entrances of important personsfrom the social field of the individual(17-22). There is much overlap among theitems considered to be losses, undesirable,or exits as well as among events catego-rized as gains, desirable, or entrances byvarious workers.
A number of retrospective studies haveshown positive relationships between phys-ical and mental illnesses and prior lifeevents, expressed as numbers of events,weighted scores, or number of independentevents (17, 23-28). However, the validity ofthese studies has been questioned becauselife events were gathered after the illnesshad been identified, raising the possibilitythat sick persons recalled or reported anexcess of events in looking for explanationsof their illnesses.
Rahe et al. examined medical records of50 servicemen discharged because of psy-chiatric illness and found that clusters oflife events occurred during the year preced-ing a cluster of illnesses or a single illness(29). Unfortunately, it is not clear when the

148 GOLDBERG AND COMSTOCK
data of the social histories in the healthrecords were gathered. If this informationwas recorded at the time of the illness, thisstudy is open to the same criticisms asother retrospective studies.
Using a prospective design, approxi-mately 2500 servicemen aboard three U.S.Navy ships were asked about recent lifeevents before starting on cruises whichlasted from six to eight months. When theships returned, the medical records for thecruise period were examined. A positiverelationship was found between the num-ber and intensity of the subject's lifechanges for the six months before the startof the cruise, and illness reported duringthe cruise periods. However, only a smallpercentage of the people accounted for alarge percentage of the illnesses; most ofthe sickness reported was minor; and thefew life events reported were also minor(30, 31).
Two similar studies were carried out byRubin et al., one involving the entireenlisted crew of a battleship and the othera third of the crew of an attack carrier(32, 33). In both cases, a history of recentlife events was taken for the 18-monthperiod prior to the start of cruises. Illnessesoccurring during the cruise period werelater abstracted and tabulated. Utilizingdata from a randomly selected half of thesubjects, a new weighting system for thelife events was derived by stepwise multi-ple regression analysis. The events preced-ing illnesses among unrated seamen weredifferent from those preceding illnesses ofpetty officers. Among unrated seamen thepreceding events were different for the twoships. Life Change Units derived fromnon-military populations did not predictfuture illness among the men in thesestudies, but the weighting systems specificto each ship did so, with persons having thehighest Life Change Unit scores having themost illnesses. The authors state the needfor caution in interpreting these findingsbecause weights derived from one-half of
the population predicted illnesses poorlyamong the other half (32). In addition, theillness rate on the attack carrier was so lowthat the standard deviations were oftenhigher than the mean number of illnesses.
Other prospective studies among youngpeople were based on relatively few seriousillnesses. Nevertheless, Cline and Chosyfound that Life Change Unit scores for an18-month period preceding a part-timeofficers' training program were positivelyassociated with health changes reportedduring the following year (34). In anotherstudy, students who sought medical carehad significantly higher mean scores on alife change inventory than did those notseeking care (35). However, because therelationship between severity of illness andpreceding life change inventory scores ac-counted for only a small portion of thevariance, it was not felt to be very helpfulin a practical sense. These authors con-cluded that "the role of physiologic dys-functioning in relationship to life stressand seeking treatment for illness remainsunclarified" (36).
Casey et al., when studying a group ofarmy inductees, failed to find a significantrelationship between Life Change Unitscores and the occurrence of illness, al-though they did show a statistically signifi-cant difference between these scores andthe levels of health care obtained. A largerpercentage of persons with high scoresreceived high levels of health care thanpersons with lower scores (37).
A modified version of the Schedule ofRecent Events was used by Thurlow in aprospective study of 111 employees of aCanadian brewery. Various indices of lifechange showed significant relationshipswith the number of days off for illnessduring a subsequent two-year period. How-ever, these relationships did not hold upwhen the effects of other independent vari-ables were controlled by multiple regres-sion. When analyzed retrospectively for afive-year period, a relationship was shown
LIFE EVENTS AND SUBSEQUENT ILLNESS 14!
between the subjective items of the Sched-ule of Recent Experience, the number ofillnesses experienced, and the number ofdays off for illness. Even though this rela-tionship remained significant when otherindependent variables were held constant,the author concluded that past illnesseswere the best predictor of future illnessesand past absenteeism best predicted theoccurrence of future absences (38).
The most extensive prospective studywas reported by Theorell et al. (39). In apopulation of 9097 middle-aged males,these authors were unable to demonstraterelationships between high life eventsscores and deaths from all causes or mosttypes of illnesses which occurred during a12- to 15-month follow-up period. Therewere exceptions, however. Neurosis in thefollow-up period was more common amongmen with high scores initially. A similarassociation was noted for all illnesses com-bined among men 41 to 51 years of age butnot among men 52 to 61 years of age.Several of the individual life events werealso related to deaths from all causes andto some illness categories.
A positive concurrent relationship be-tween life events, as scored by a variety ofmethods, and psychophysiologic status asmeasured by a modification of the HealthOpinion Survey and the Langner 22-ItemSymptom Scale has also been reported (21,22, 40). In addition, Uhlenhuth et al.reported that in a randomly selected sam-ple of the population in Oakland, Califor-nia, a positive relationship was shownbetween the intensity of psychiatric symp-toms and life stress. The psychiatric symp-toms were measured by 54 items from theHopkins Symptom Checklist and life stresswas measured by a list of life events (41).
Two longitudinal studies, with subjectsrandomly selected from the general popu-lation, have reported that when stressfullife events occur, symptoms of psychologicdisturbance are also likely to occur (42, 43).However, the correlation between life
events and psychophysiologic symptom!could be built in to some extent (44). Botrof the scales used to measure symptomsthe Health Opinion Survey and th<Langner Scale, include questions aboulsymptoms of illness that would unavoidably correlate to life events relative to illness.
None of the evidence that stresses, froman accumulation of life events, can in sormway cause illness is incontrovertable. Theretrospective studies have been criticizedon the grounds of possibly biased historiesof life events obtained from patients (45).interaction between the occurrence of theevent and the illness (20, 46), and a varietvof methodologic problems (46, 47). Thelongitudinal studies have shown mixedresults and, for the most part, have dealtwith healthy, young, male populations whorarely became seriously ill during the studyperiod. Because of the unsettled impor-tance of stress from life events as precur-sors of disease, findings from large-scaleprospective studies in two general popula-tions were utilized to examine the relation-ship between illness and prior life events.
MATERIALS AND METHODS
The Community Mental Health Epide-miology Program was conducted similarlyin Kansas City, Missouri, and in Washing-ton County, Maryland. In Kansas City,cluster sampling was utilized to obtain arandom sample of dwelling units. In Wash-ington County, dwelling units were se-lected by systematic sampling from a ran-dom start, using as the frame an updatedprivate census originally carried out in1963 (48). In both locations the individualto be interviewed was randomly chosenfrom adults 18 years of age or older in theselected household.
Interviewing began in Kansas City inOctober 1971 and continued through Janu-ary 1973. Twenty-eight dwelling units wereselected each week for a total of 1792.There were 173 which were either vacant,

150 GOLDBERG AND COMSTOCK
torn down or contained no household (e.g.,a building containing no household mightcontain a store), leaving 1619 available forinterview. From these households 1173 in-terviews were obtained, a response rate of72 per cent.
Interviewing for this study in Washing-ton County, Maryland, was carried outbetween December 1971 and July 1973.During the first 13 months, a sample of 33dwelling units was drawn weekly. For thebalance of the study, monthly samples of100 each were drawn. This method resultedin the selection of 2269 dwelling units ofwhich 199 were either vacant or torn down,leaving 2070 available for interviews. Atotal of 1673 persons was interviewed, aresponse rate of 80 per cent.
In addition to questions about a varietyof demographic, health and psychosocialvariables, the initial questionnaire in-cluded a life events list based on Holmesand Rahe (7) and revised by Dohrenwendand Dohrenwend (49) (see table 2). At thisinterview, each subject reported whether ornot the event had taken place during theprevious year.
In Kansas City, 343 people were reinter-viewed between July 1973 and December1973, twelve months after the initial inter-view. A response rate of 78 per cent wasobtained. Between August 1973 and April1974 a second round of interviews wasrequested from a group of the originalrespondents in Washington County. Sixhundred sixty persons were reinterviewedfor an overall response rate of 79 per cent.The reinterview utilized a shortened ver-sion of the first questionnaire. Several ofthe scales were dropped and detailed ques-tions about illnesses, disability, and hospi-talization were added. Questionnaires forboth the original interview and the reinter-view were the same in Kansas City andWashington County.
In Washington County only, variableintervals between interviews (6 and 12months) were chosen to allow an estimate
of the point at which the best balancecould be obtained between memory lapsesand losses from follow-up, both of whichlead to decreasing information with time;and length of the follow-up interval, whichleads to increasing information. Becausethere were no statistically significant dif-ferences between the respondents for thevarious time intervals by sex, race, age,marital status, income, education or geo-graphic locations within the county, datafrom these two follow-up groups were com-bined.
Subjects for this study were the respond-ents to the follow-up questionnaire at bothsites, confining the selection to whitesbecause of the small number of non-whiterespondents. A case is defined as anyperson who died or was hospitalized duringthe follow-up interval for an illness startingafter the first interview. Of the cases, 67were hospitalized and 16 had died. Con-trols were selected from respondents to thereinterview who did not report any newillnesses or hospitalizations during the in-terval. A control was individually matchedto each case by length of follow-up interval,sex, employment status, education, in-come, and age within five years in eachdirection.
RESULTS
The final study group is composed of 83matched pairs of cases and controls, 36from Kansas City and 47 from WashingtonCounty (see table 1). Almost 68 per cent ofthe Kansas City cases were female, 39 percent were in the age group of 45-64, and 42per cent were working at the time of theinterview. In the Washington County sam-ple, 66 per cent of the cases were female,most were in the age group 18-44, and abare majority (51 per cent) of the caseswere working when first interviewed.
No statistically significant differenceswere found between cases and controls onany variable used for matching in eithercommunity. In addition, there were no

LIFE EVENTS AND SUBSEQUENT ILLNESS 151
TABLE 1
Characteristics of cases and controls by demographicvariables used for matching: Washington County,
MD, and Kansas City, MO
Characteristic
LocationWashington CountyKansas City
SexFemaleMale
Age18-4445-6465 and over
Occupational StatusWorkingHousewifeRetired/studentNot working but looking for work
Educational StatusCollege degree or better1 yr, to <4 yrs. collegeHigh school degree7-11 grades< 7 grade
Income< 4,0004,000-7,9998,000-11,999
12,000-15,99916,000-25,999Other
Interval6 months
12 months
N =
Cases
56.743.3
66.333.7
39.833.726.5
47.024.125.3
3.6
12.016.922.936.112.0
31.318.112.021.7
9.67.2
6.094.0
83 pairs
Controls
56.743.3
66.333.7
42.228.928.9
49.425.322.9
2.4
7.215.733.734.98.4
24.118.122.920.59.64.8
6.094.0
differences in any of the matching varia-bles between the two sites. All Kansas Cityrespondents were urban dwellers, whileWashington County respondents includedurban, suburban, rural and small townresidents.
Because the case-control relationshipswere similar for both study locations, theKansas City and Washington County re-sults have been combined for the rest ofthis presentation.
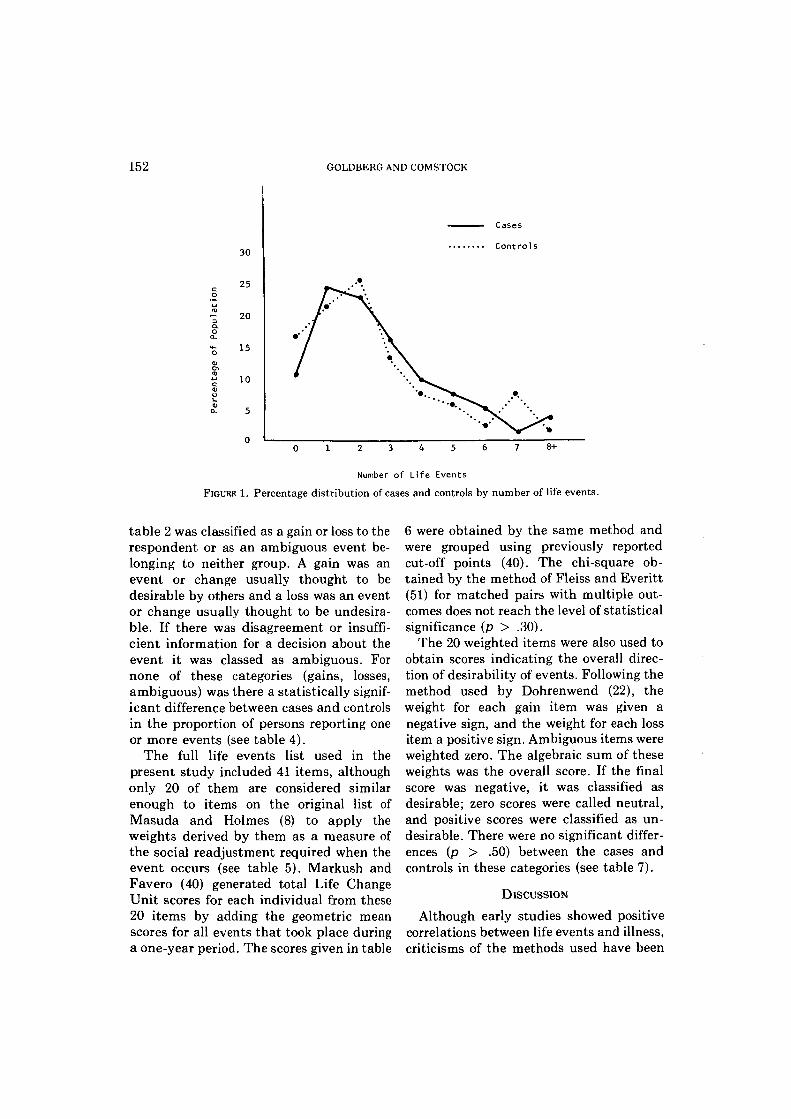
Subjects did not report many life eventsoccurring during the one-year period beforethe first interview. The median number ofevents for cases and controls was 2.2 and2.0, respectively. The distributions forcases and controls shown in figure 1 paral-lel each other closely. Both curves areskewed to the right; the majority of both
cases (57.8 per cent) and controls (62.7 percent) have scores of two or less. Each grouphad 14 (16.8 per cent) persons with scoresof five or more.
Table 2 displays the number of cases andcontrols who reported the occurrence ofeach event. There are 13 events which werereported by no more than one person ineither group. Taking a vacation was themost frequently reported event by bothgroups. The most serious events reportedin any quantity were related to the healthof the respondent or the death of a personimportant to the respondent. Fifteenevents were reported by more cases thancontrols and 12 events were reported bymore controls than cases.
Because many of the events were re-ported by very few people, differences be-tween individual events were examinedonly for those which were reported by atleast five persons in either group. Results ofthe matched pairs analysis using McNe-mar's test (50) are given in table 3. Therewere no statistically significant differencesbetween the cases and controls althoughfor the event "illness or injury" the esti-mated relative risk of subsequent hospitali-zation or dying is 1.8 for the cases ascompared to the control group.
Various methods of scoring life eventsbased on the work of others were replicatedfor comparative purposes. A commonlyused method is to compare the number ofpersons in various groups who reported theoccurrence of at least one event during aspecified time period (17, 21, 26). The totalcount shown in table 4 shows little differ-ence between cases and controls, althoughfewer controls than cases reported at leastone event.
Many authors feel that the quality of theevent taking place is an important factor tobe taken into account when studying theeffects of life events, rather than the simpleaccumulation of events (17, 21, 25, 26).Based upon work performed by Dohren-wend and Dohrenwend (49) each event on
152 GOLDBERG AND COMSTOCK
30
25
20
•* 15
10
Cases
Controls
0 1 2 3 4 5 6 7 8 +
Number o f L i f e E v e n t s
FIGURE 1. Percentage distribution of cases and controls by number of life events.
table 2 was classified as a gain or loss to therespondent or as an ambiguous event be-longing to neither group. A gain was anevent or change usually thought to bedesirable by others and a loss was an eventor change usually thought to be undesira-ble. If there was disagreement or insuffi-cient information for a decision about theevent it was classed as ambiguous. Fornone of these categories (gains, losses,ambiguous) was there a statistically signif-icant difference between cases and controlsin the proportion of persons reporting oneor more events (see table 4).
The full life events list used in thepresent study included 41 items, althoughonly 20 of them are considered similarenough to items on the original list ofMasuda and Holmes (8) to apply theweights derived by them as a measure ofthe social readjustment required when theevent occurs (see table 5). Markush andFavero (40) generated total Life ChangeUnit scores for each individual from these20 items by adding the geometric meanscores for all events that took place duringa one-year period. The scores given in table
6 were obtained by the same method andwere grouped using previously reportedcut-off points (40). The chi-square ob-tained by the method of Fleiss and Everitt(51) for matched pairs with multiple out-comes does not reach the level of statisticalsignificance (p > .30).
The 20 weighted items were also used toobtain scores indicating the overall direc-tion of desirability of events. Following themethod used by Dohrenwend (22), theweight for each gain item was given anegative sign, and the weight for each lossitem a positive sign. Ambiguous items wereweighted zero. The algebraic sum of theseweights was the overall score. If the finalscore was negative, it was classified asdesirable; zero scores were called neutral,and positive scores were classified as un-desirable. There were no significant differ-ences (p > .50) between the cases andcontrols in these categories (see table 7).
DISCUSSION
Although early studies showed positivecorrelations between life events and illness,criticisms of the methods used have been

LIFE EVENTS AND SUBSEQUENT ILLNESS 153
TABLE 2
Occurrences of life events as classified by Dohrenwend and Dohrenwend (49) for cases and controls for bothWashington County, MD, and Kansas City, MO (N = 83 matched pairs)
Life event
Classified as gainEngagedMarriedOther new love relationship or important friendshipBirth of first childImprovement in healthStarted school or training program, etc.Graduated from school or training program etc.Started to work—first timeJob or own business improved in responsibility, type, location or some other wayMajor gains in income not due to change in workAcquisitions of propertyReleased from prison, acquitted of other than minor traffic offensesChanged residence for better oneStarted new hobby or recreational activityAcquired a petTook a vacation
Classified as lossWidowedDivorcedSeparatedOther broken love relationship or important friendshipMiscarriage or stillbirthFamily member left homeIllness or injuryDeath of loved one or other important personQuit or failed school or training program, etc.Job or own business downgraded in responsibility, type, location or some other wayLaid off or fired from job or own business failedMajor loss of income not due to change in work.Serious property lossArrested, indicted, convicted of other than minor traffic offensesChanged residence for worse oneDropped hobby or recreational activityLost a pet
Classified as ambiguousPregnancyBirth of child other than firstNew person in home other than birth of new childEntered armed servicesLeft armed servicesRetired from workStarted at a new type of workOther major event
No. of personshaving event
Cases
1261
22221
106106
131336
001216
2819023110038
40400352
Controls
1050
1822294306
141140
010205
1920
123200128
22400183
Differences
Casesless
controls
0++++00-++-00-+-
0_+0+++--00-+0_+0
+_000+_-
increasing (19, 45, 47, 52, 55). A review ofthe literature shows methodologic limita-tions and conflicting findings. The lack ofany statistically significant differences be-tween the cases and controls in this study,regardless of scoring method used, lendsweight to the cautious interpretations ofsome (32, 33, 36) and the negative findingsof others (37, 38, 45, 55).
An attempt has been made in this work
to avoid some of the pitfalls encounteredby previous studies. Specifically, the prob-lems addressed include retrospective studydesign, use of limited samples, little re-porting of serious illness among subjects,and inappropriate controls. Although thepresent analysis is based on case-controlcomparisons, the study was prospective innature. While information concerning theoccurrence of the listed life events was

154 GOLDBERG AND COMSTOCK
TABLE 3
Matched pairs analysis* of individual events reported by at least five persons: Washington County, MD, andKansas City, MO (N = 83 matched pairs)
Event
Other new love/important relationshipNew person in homeFamily member left homeIllness or injuryImprovement in healthDeath of loved one/important personJob/business improvedStarted new type workMajor gain in incomeChanged residence—betterStarted new hobbyAcquired a petLost a petTook a vacation
Bothmembers
1018544010523
24
Caseonly
545
20171565568
115
12
Controlonly
444
111316
583699516
Reported by
eit er
7375734448486870747161617031
aX
0.13
02.1
.3000
.31
.13
.080
.05
.10
.29
Significancelevel
NSNSNSNSNSNSNSNSNSNSNSNSNSNS
* McNemar's Test using 1 degree of freedom (50).
TABLE 4
Matched pairs analysis* of life events by various scoring methods: Washington County, MD, and Kansas City,MO (N = 83 matched pairs)
Scoring methods
Total countGain countLoss countAmbiguous
Bothmembers
6146243
One or more life events reported by
Caseonly
13132414
Controlonly
8182014
Neither
16
1552
x2
0.760.500.200.04
Significancelevel
z z
z z
CO
CO
CO
CO
* McNemar's Test using 1 degree of freedom (50).
gathered retrospectively at the initial in-terview for the preceding 12 months, ahistory of illness for the subsequent timeperiod was obtained at a second interview.This method eliminates the possibility ofincreased recall of life events by sick sub-jects that might occur when data on bothlife events and illness were gathered at thesame time.
Subjects of much of the previously re-ported prospective research have beenyoung, healthy males who were members ofthe armed services or students. Onestrength of the present study is that bothcases and controls were drawn from two
independent populations with a broadrange of characteristics. The conclusionsneed not, therefore, be limited to specificage, sex, occupational or educationalgroups. Furthermore, matching on theseand other independent variables virtuallyeliminates any effects these variablesmight have had on the analysis, therebyimproving the generalizability of the find-ings.
Because of the youthfulness and healthof subjects in previous studies, most of thereported illnesses were minor in nature. Inthis study, cases were restricted to personswith illnesses serious enough to require

LIFE EVENTS AND SUBSEQUENT ILLNESS 155
TABLE 5
Life change units derived from Masuda and Holmes (8) as classified by Dohrenwend and Dohrenwend (49)
EventLife
changescore
Classified as gainMarriageBirth of first childStart of school or training, etc.Graduate of school or training, etc.Improvement in responsibility, type, location of job or own businessChange of residence for betterStarted new hobby or recreational activityTook a vacation
Classified as lossWidowhoodDivorceSeparationIllness or injuryDeath of a loved one or other important personDowngrading in responsibility, type, location of job or own businessUnemployment or failure of businessChange of residence for worseDropped hobby or recreational activity
Classified as ambiguousPregnancyBirth of child other than firstRetirement
50033719119124314012774
771593516416469308378140127
284337361
TABLE 6
Matched pairs analysis* of weighted^ life eventsscores: Washington County, MD, and Kansas City,
MO
Controls0-335
336-642643+
TotalN
Cases
0-335 336-642
18118
37= 83 matched
df = 2
1674
27pairs
NS
643+
964
19
X2 = 1-68
Total
43241683
* Fleiss and Everitt statistic using 2 degrees offreedom (51).
t Each item weighted by geometric mean obtainedby Masuda and Holmes (8).
hospitalization or to cause death, therebylimiting the results to undeniably impor-tant measures of ill health.
The second most frequently reported lifeevent in these two populations was illness
TABLE 7
Matched pairs analysis* of scores weighted to indicatedesirability or undesirability (22): Washington
County, MD, and Kansas City, MO
Cases
Controls
Desirable scoreNeutral scoreUndesirable scoreTotal
N = 83
Desirablescore
93
1224
matcheddf = 2
Neutralscore
457
16pairs
NS
Undesirablescore
14131643
X2 = 1-35
Total
27213583
* Fleiss and Everitt statistic using 2 degrees of freedom(51).
or injury during the preceding year. Al-though the difference between the casesand controls on this event does not reachthe level of statistical significance, morecases than controls reported illness duringthe previous year at the i:-aial interviews.This is in the direction of the results ofothers, such as Hinkle and his coworkers,

156 GOLDBERG AND COMSTOCK
who found that people with a history offrequent illnesses were most likely to be-come sick in the future. Hinkle also arguesthat life events are much more likely toprecipitate illness among frequently ill per-sons who seem to have some kind of suscep-tibility (56). Thurlow's work corroboratesthis to the extent that past illnesses werethe best predictor of future illnesses amonghis study subjects (38). One problem withmany lists of life events, including the oneused in this study, is that one cannot becertain that the illnesses reported as lifeevents were truly independent of the subse-quent illnesses counted as outcomes. In-deed, it can be argued that when illness isthe outcome, illness should not be anindependent variable. If illness were re-moved from the life events list used in thisstudy, the slight tendency for cases to havemore life events than controls would disap-pear.
Change per se is the concept upon whichmuch of the research using life events as ameasure of stress is based. A count of allpersons reporting one or more events, andtotal scores of 20 items weighted to indicateamount of readjustment required when theevent occurred were two methods of analy-sis used here to examine change. Becauseno differences were shown between casesand controls by either method, it appearsthat change, in and of itself, is not aprecursor of serious illness.
A further group of studies has been basedon the concept that only socially negativeevents are related to subsequent ill health.To examine this hypothesis, items consid-ered as socially defined losses and gainswere grouped; a score for desirability wasalso generated. Again, it was not possibleto corroborate the finding by others thatevents with negative connotations weremore highly associated with illness thanpositive events (17, 26, 28).
Given the state of knowledge concerningthe relationship between life events andsubsequent illness, what direction should
further research take? A first step wouldseem to be a reevaluation of the use of listsof life events as indicators of the stresswhich the occurrence of such events mayevoke, possibly followed by the develop-ment of a different measurement instru-ment. Additional investigation of the asso-ciation of life events with important ill-nesses could then follow. Further retro-spective studies seem impractical both be-cause of biased recall and because of possi-ble interaction between events and dis-eases, particularly mental illnesses. Morein order are well designed prospective stud-ies using random samples of the popula-tion, a range of outcome illnesses, outcomevariables clearly distinguishable from in-dependent variables, and an account of theeffects of mediating factors. As for theevents themselves, they should be countedas stressors only if seen that way by therespondent himself (20, 56, 57). The possi-bility of using life events as indicators ofthe kinds of stress that may lead to illnessis still sufficiently attractive to warrantfurther well planned and properly con-ducted investigations.
REFERENCES
1. Levine EB: Hippocrates. New York, TwaynePublishers, Inc, 1971
2. Cannon WB: Bodily Changes in Pain, Hunger,Fear and Rage. New York, D Appleton andCompany, 1929
3. Meyer A: The life chart and the obligation ofspecifying positive data in psychopathologicaldiagnosis. The Collected Papers of Adolf Meyer,Vol III. Edited by E Winters. Baltimore, TheJohns Hopkins Press, 1951, pp 52-56
4. Graham DT, Stevenson I: Disease as response tolife stress. Psychological Basis of Medical Prac-tice. Edited by HI Lief, VF Lief, NR Lief. NewYork, Harper and Row, 1963, pp 115-136
5. Wolff HG, Wolf SG, Hare CC (Eds): Life Stressand Bodily Disease. Baltimore, Williams & Wil-kins, 1958
6. Holmes TH, Masuda M: Life change and illnesssusceptibility. Stressful Life Events: Their Na-ture and Effects. Edited by BS Dohrenwend, BPDohrenwend. New York, John Wiley and Sons,1974, pp 45-72
7. Holmes TH, Rahe RH: The social readjustmentrating scale. J Psychosom Res 11:213-218, 1967
8. Masuda M, Holmes TH: Magnitude estimations
LIFE EVENTS AND SUBSEQUENT ILLNESS 157
of social readjustments. J Psychosom Res11:219-225, 1967
9. Selye H: The Stress of Life. New York, McGrawHill Book Company, 1956
10. Holmes TH, Rahe RH: The social readjustmentrating scale. J Psychosom Res 11:217, 1967
11. Masuda M, Holmes TH: The social readjustmentrating scale: a cross-cultural study of Japaneseand Americans. J Psychosom Res 11:227-237,1967
12. Rahe RH: Multi-cultural correlations of lifechanges scaling: America, Japan, Denmark, andSweden. J Psychom Res 13:191-195, 1969
13. Harmon DK, Masuda M, Holmes TH: The socialreadjustment rating scale: a cross-cultural studyof Western Europeans and Americans. J Psy-chosom Res 14:391-400, 1970
14. Ruch LO, Holmes TH: Scaling of life change:comparison of direct and indirect methods. JPsychosom Res 15:221-227, 1971
15. Mendels J, Weinstein N: The schedule of recentexperiences: a reliability study. Psychosom Med34:527-531, 1972
16. Dohrenwend BS: Life events as stressors: a meth-odological inquiry. J Health Soc Behav 14:174,1973
17. Paykel ES, Myers JK, Dienelt MN, et al: Lifeevents and depression: a controlled study. ArchGen Psychiatry 21:753-760, 1969
18. Dohrenwend BP: Problems in defining and sam-pling the relevant population of stressful lifeevents. Stressful Life Events: Their Nature andEffects. Edited by BS Dohrenwend, BP Dohren-wend. New York, John Wiley and Sons, 1973, pp275-310
19. Brown GW: Meaning, measurement and stress oflife events. Stressful Life Events: Their Natureand Effects. Edited by BS Dohrenwend, BPDohrenwend. New York, John Wiley and Sons,1973, pp 217-244
20. Dohrenwend BS, Dohrenwend BP (Eds): Stress-ful Life Events: Their Nature and Effects. NewYork, John Wiley and Sons, 1973
21. Myers JK, Lindenthal JJ, Pepper MP: Life eventsand psychiatric impairment. J Nerv Ment Dis152:149-157, 1971
22. Dohrenwend BS: Life events as stressors: a meth-odological inquiry. J Health Soc Behav14:167-175, 1973
23. Hawkins NG, Davies R, Holmes TH: Evidence ofpsychosocial factors in the development of pulmo-nary tuberculosis. Am Rev Tuberc Pulmonary Dis75:768-780, 1957
24. Rahe RH, Meyer M, Smith M, et al: Social stressand illness onset. J Psychosom Res 8:35-44, 1964
25. Antonovsky A, Kats R: The life crisis history as atool in epidemiologic research. J Health SocBehav 8:15-21, 1967
26. Brown GW, Birley JLT: Crises and life changesand the onset of schizophrenia. J Health SocBehav 9:203-214, 1968
27. Rahe, RH, Bennett LK, Romo M, et al: Subjects'recent life changes and coronary heart disease inFinland. Am J Psychiatry 130: 1222-1226, 1973
28. Cooper B, Sylph J: Life events and the onset ofneurotic illness: an investigation in general prac-tice. Psychol Med 3:421-435, 1973
29. Rahe RH, McKean JD, Arthur RJ: A longitudinalstudy of life change and illness patterns. J Psy-chosom Res 10:355-366, 1967
30. Rahe RH, Gunderson EK, Arthur RJ: Demo-graphic and psychosocial factors in acute illnessreporting. J Chron Dis 23:245-255, 1970
31. Rahe RH, Mahan JL, Arthur RJ: Prediction ofnear-future health change from subjects' preced-ing life changes. J Psychosom Res 14:401-406,1970
32. Rubin RT, Gunderson EK, Arthur RJ: Prior lifechange and illness onset in an attack carrier'screw. HI. Arch Environ Health 19:753-757, 1969
33. Rubin RT, Gunderson EK, Arthur RJ: Life stressand illness patterns in the U.S. Navy. V. Prior lifechange and illness onset in a battleship's crew. JPsychosom Res 15:89-94, 1971
34. Cline DW, Chosy JJ: A prospective study of lifechanges and subsequent health changes. ArchGen Psychiatry 27:51-53, 1972
35. Spilkin AZ, Jacob MA: Prediction of illnessbehavior from measures of life crisis, manifestdistress and maladaptive coping. Psychosom Med33:251-264, 1971
36. Spilkin AZ, Jacob MA: Prediction of illnessbehavior from measures of life crisis, manifestdistress, and maladaptive coping. PsychosomMed 33:263, 1971
37. Casey RL, Thoresen AR, Smith FJ: The use of theschedule of recent experience questionnaire in aninstitutional health care setting. J Psychosom Res14:149-154, 1970
38. Thurlow HJ: Illness in relation to life situationand sick role tendency. J Psychosom Res15:73-88, 1971
39. Theorell T, Lind E, Floderus B: The relationshipof disturbing life-changes and emotions to theearly development of myocardial infarction andother serious illnesses. Int J Epidemiol 4:281-293,1975
40. Markush RE, Favero RV: Epidemiologic assess-ment of stressful life events, depressed mood, andpsychophysiological symptoms—a preliminaryreport. Stressful Life Events: Their Nature andEffects. Edited by BS Dohrenwend, BP Dohren-wend. New York, John Wiley and Sons, 1973, pp171-190
41. Uhlenhuth EH, Lipman RS, Baiter MB, et al:Symptom intensity and life stress in the city.Arch Gen Psychiatry 31:759-764, 1974
42. Myers JK, Lindenthal JJ, Pepper MP, et al: Lifeevents and mental status: a longitudinal study. JHealth Soc Behav 13:398-406, 1972
43. Dohrenwend BP, Dohrenwend BS: Social Statusand Psychological Disorder: A Causal Inquiry.New York, John Wiley and Sons, 1969
44. Seiler L: The 22-item scale used in field studies ofmental illness: a question of method, a question ofsubstance and a question of theory. J Health SocBehav 14:252-264, 1973
45. Hudgens RW, Robins E, Delong WB: The report-

158 GOLDBERG AND COMSTOCK
ing of recent stress in the lives of psychiatricpatients. Br J Psychiatry 117:635-643, 1970
46. Brown GW: Meaning, measurement and stress oflife events. Stressful Life Events: Their Natureand Effects. Edited by BS Dohrenwend, BPDohrenwend. New York, John Wiley and Sons,1973, pp 217-244
47. Hudgens, RW: Personal catastrophe and depres-sion. Stressful Life Events: Their Nature andEffects. Edited by BS Dohrenwend, BP Dohren-wend. New York, John Wiley and Sons, 1973, pp119-134
48. Comstock, GW, Abbey H, Lundin FE Jr: Thenonofficial census as a basic tool for epidemiologicobservations in Washington County, Maryland.The Community as an Epidemiologic Laboratory.Edited by II Kessler, ML Levin. Baltimore, JohnsHopkins Press, 1970, pp 73-99
49. Dohrenwend BS, Dohrenwend BP: Personal Com-munication, 1971
50. McNemar Q: Note on the sampling error of thedifference between correlated proportions or per-centages. Psychometrika 12:153-157, 1947
51. Fleiss JL, Everitt BP: Comparing the marginaltotals of square contingency tables. Br J MathStat Psychol 24:117-123, 1971
52. Brown GW, Sklair F, Harris TO, et al: Life eventsand psychiatric disorders. I. Some methodologicalissues. Psychol Med 3:74-87, 1972
53. Cobb S: A model for life events and their conse-quences. Stressful Life Events: Their Nature andEffects. Edited by BS Dohrenwend, BP Dohren-wend. New York, John Wiley and Sons, 1974, pp151-156
54. Mechanic D: Discussion of research programs onrelations between stressful life events and epi-sodes of physical illness. Stressful Life Events:Their Nature and Effects. Edited by BS Dohren-wend, BP Dohrenwend. New York, John Wileyand Sons, 1974, pp 87-97
55. Wershow H, Reinhart G: Life change andhospitalization—a heretical view. J PsychosomRes 18:393-401 1974
56. Hinkle LE: The effect of exposure to culturechange, social change and changes in interper-sonal relationships on health. Stressful LifeEvents: Their Nature and Effects. Edited by BSDohrenwend, BP Dohrenwend. New York, JohnWiley and Sons, 1974, pp 9-44
57. Graham S: The sociological approach to epidemi-ology. Am J Public Health 64:1046-1049, 1974