
Lies CMIOs Tell- Dr. David Allard, Henry Ford Health System
22
EMR Innovation R. David Allard, MD Chief Medical Information Officer Henry Ford Health System mHealth Israel: January 10, 2018
-
Upload
levi-shapiro -
Category
Health & Medicine
-
view
100 -
download
0
Transcript of Lies CMIOs Tell- Dr. David Allard, Henry Ford Health System
EMR Innovation
R. David Allard, MD
Chief Medical Information Officer
Henry Ford Health System
mHealth Israel: January 10, 2018
Goals
Discuss Why EMRs lag other innovation in Healthcare and other industries
Propose an approach to innovation
Discuss common issues with which CMIOs contend
Give a few examples of why there is hope
Medicine is the Highest Tech Low Tech Industry
Care techniques are advancing at a phenomenal
rate
– Gamma knife
– Precision Medicine
– DaVinci Surgery
– Et Cetera
The mechanisms we use to learn about these best
practices and deliver the techniques have
changed very slowly with healthcare and medicine
still acting like a cottage industry
Cottage Industry vs. Standards Driven High Reliability
Industry
Cottage Industry
Emphasis on craftsmanship
– Great doctor/provider
– “Centers of Excellence”
Highly individualized care
Highly variable in cost and outcome
Optimized for the craftsman
Hard to measure or predict outcomes levels
Standards Driven Industry
Emphasis on process and reliability
– Create processes that anyone (within reason) can do
Consistency, highly reliable
Transparency
Optimized for the end recipient
– (consider the airline industry)
Medicine is the Highest Tech Low Tech Industry
13% of physicians in the USA are still on paper
charts in 20171
53% of practices describe their EMR as “basic”
83% of residential care communities are on paper
(2010)
32% of EHRs can exchange information with other
provider’s systems (2014)
1https://www.cdc.gov/nchs/fastats/electronic-medical-records.htm
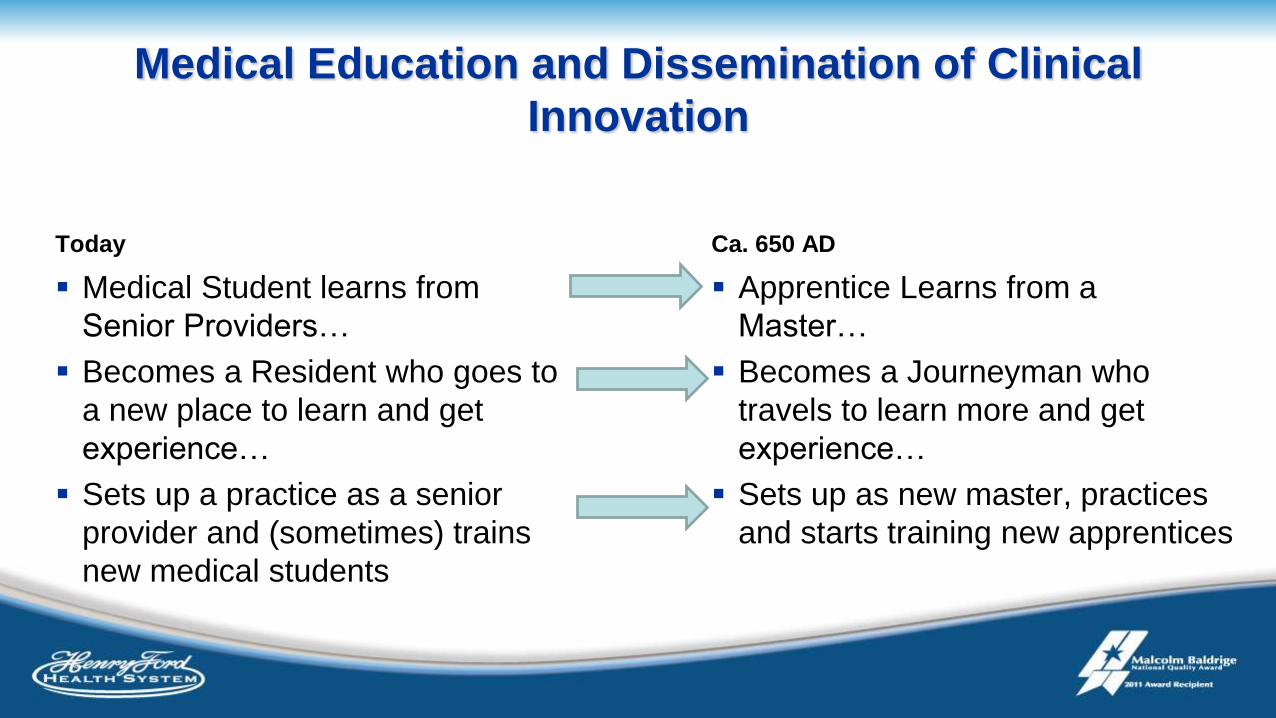
Medical Education and Dissemination of Clinical
Innovation
Today
Medical Student learns from
Senior Providers…
Becomes a Resident who goes to
a new place to learn and get
experience…
Sets up a practice as a senior
provider and (sometimes) trains
new medical students
Ca. 650 AD
Apprentice Learns from a
Master…
Becomes a Journeyman who
travels to learn more and get
experience…
Sets up as new master, practices
and starts training new apprentices
Why is This a Problem?
CMIO Lie #1 – Medicine is becoming a retail business
Is medicine a service industry or a consulting industry at its heart?
– Service industry
• We certainly do things to and for people
• The literature is full of articles about the retailization of healthcare
– Consulting industry
• At the core of Medicine is knowing what to do
• Population Health, Big data, machine learning,
• The management of information such that it is represented of knowledge and applying that
knowledge to benefit the health of populations and individual patients
Bytes → Data → Information → Knowledge → Wisdom
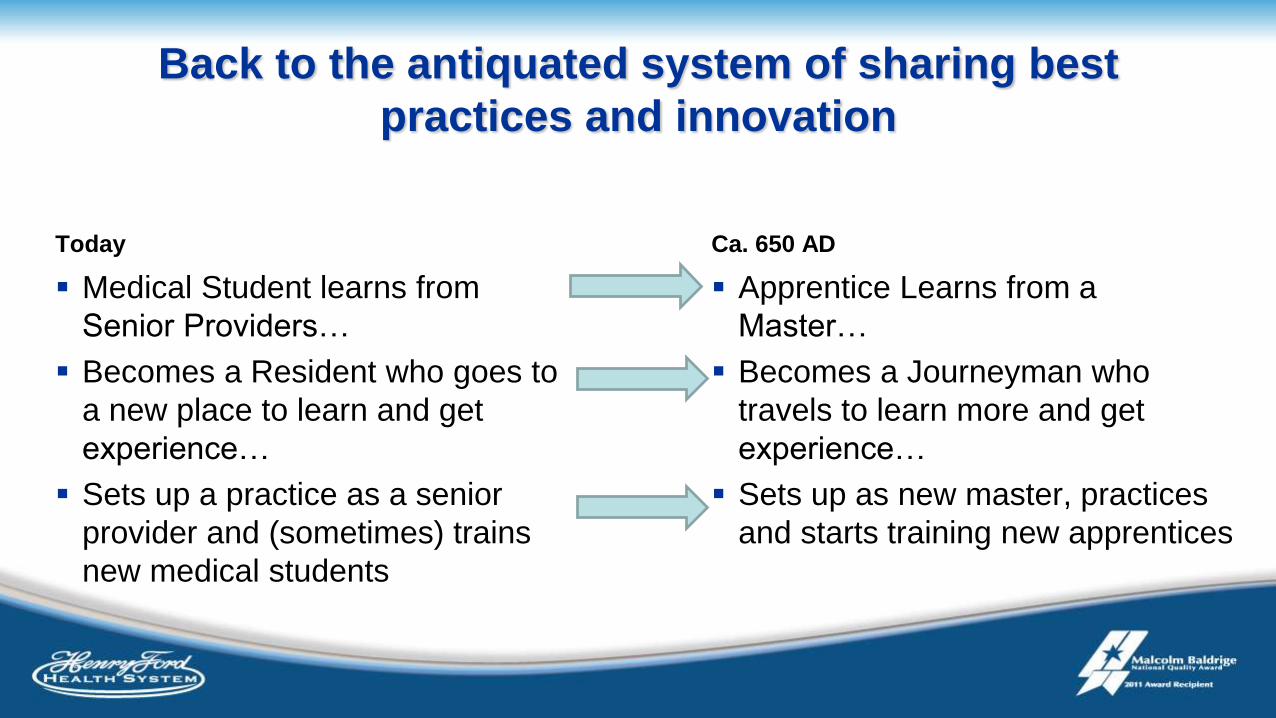
Back to the antiquated system of sharing best
practices and innovation
Today
Medical Student learns from
Senior Providers…
Becomes a Resident who goes to
a new place to learn and get
experience…
Sets up a practice as a senior
provider and (sometimes) trains
new medical students
Ca. 650 AD
Apprentice Learns from a
Master…
Becomes a Journeyman who
travels to learn more and get
experience…
Sets up as new master, practices
and starts training new apprentices
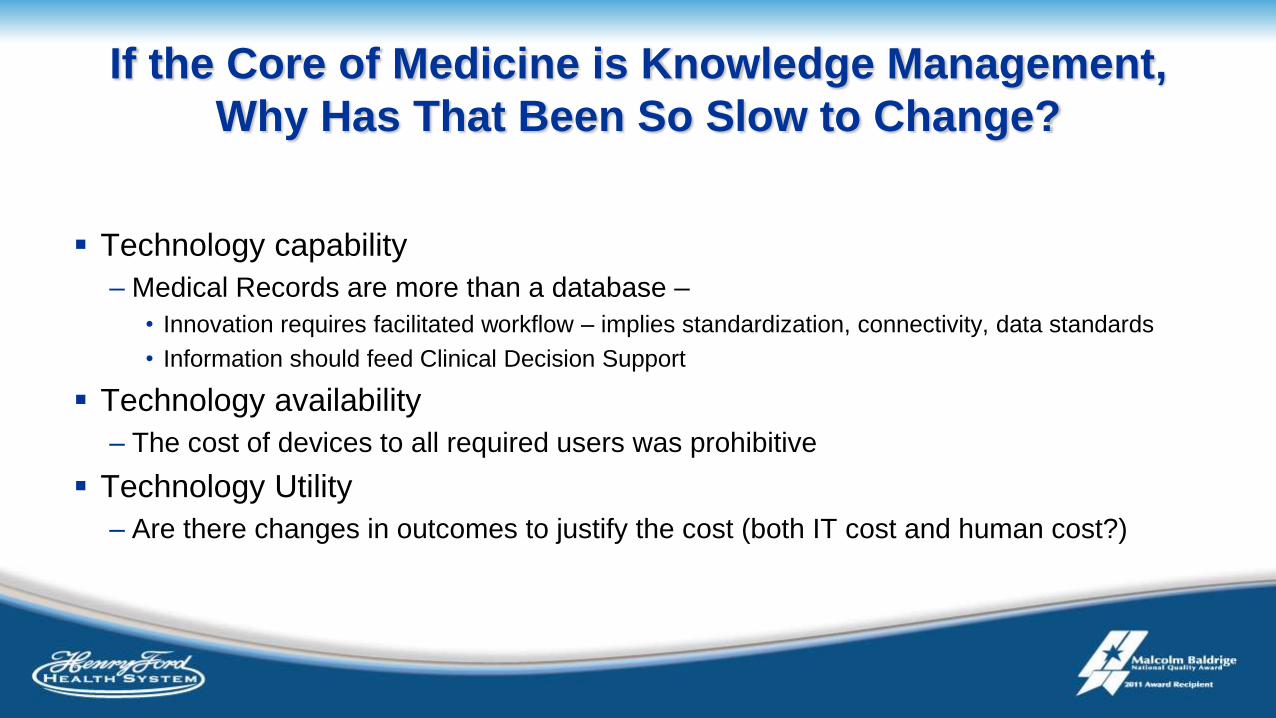
If the Core of Medicine is Knowledge Management,
Why Has That Been So Slow to Change?
Technology capability
– Medical Records are more than a database –
• Innovation requires facilitated workflow – implies standardization, connectivity, data standards
• Information should feed Clinical Decision Support
Technology availability
– The cost of devices to all required users was prohibitive
Technology Utility
– Are there changes in outcomes to justify the cost (both IT cost and human cost?)
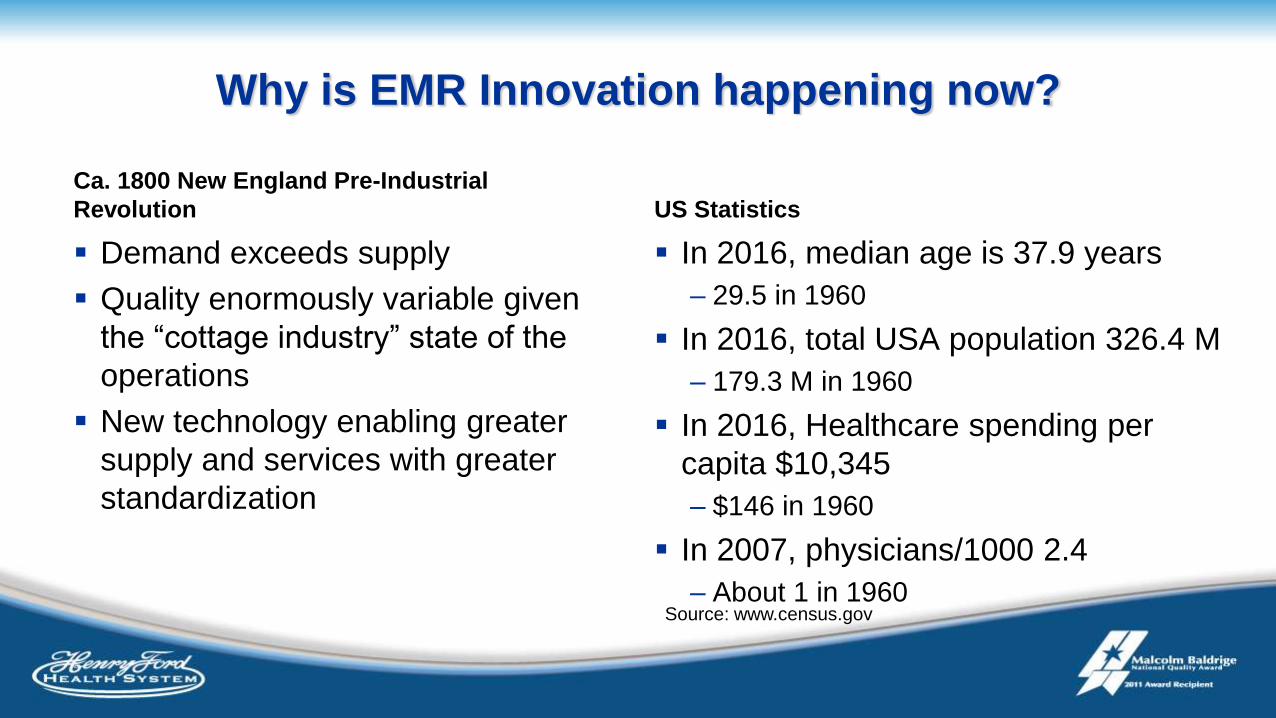
Why is EMR Innovation happening now?
Ca. 1800 New England Pre-Industrial
Revolution
Demand exceeds supply
Quality enormously variable given
the “cottage industry” state of the
operations
New technology enabling greater
supply and services with greater
standardization
US Statistics
In 2016, median age is 37.9 years
– 29.5 in 1960
In 2016, total USA population 326.4 M
– 179.3 M in 1960
In 2016, Healthcare spending per
capita $10,345
– $146 in 1960
In 2007, physicians/1000 2.4
– About 1 in 1960Source: www.census.gov
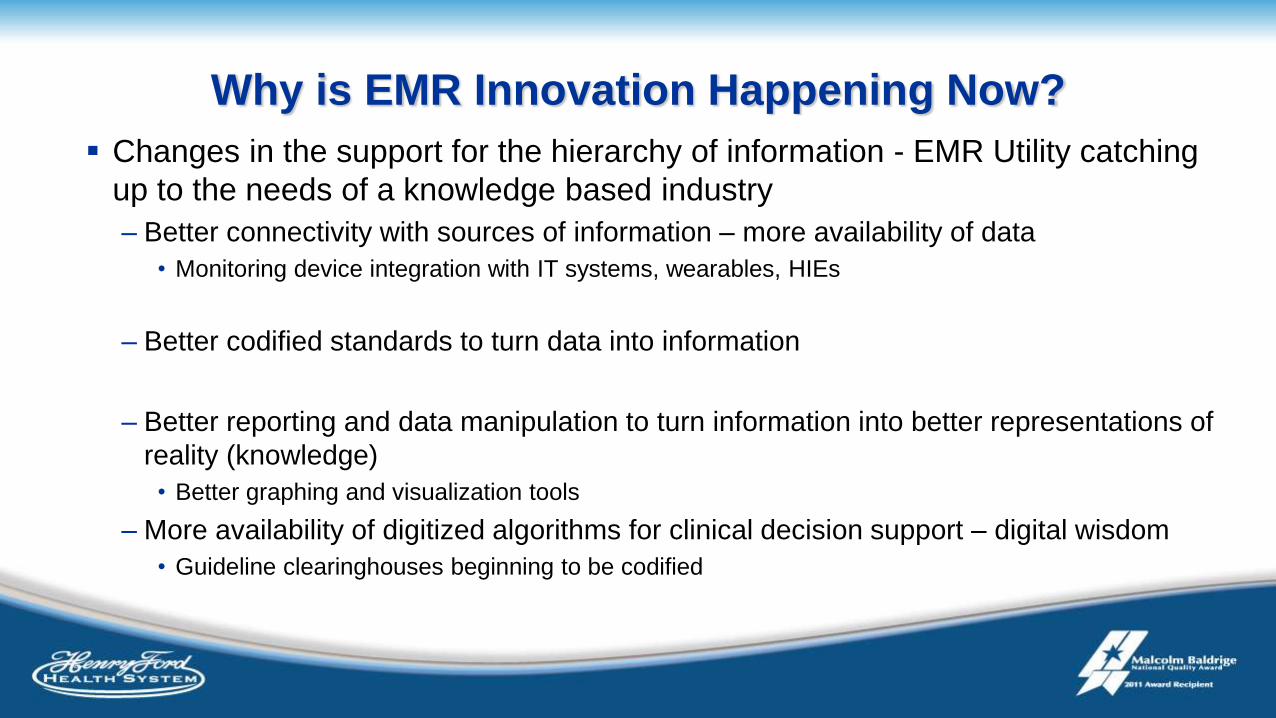
Why is EMR Innovation Happening Now?
Changes in the support for the hierarchy of information - EMR Utility catching
up to the needs of a knowledge based industry
– Better connectivity with sources of information – more availability of data
• Monitoring device integration with IT systems, wearables, HIEs
– Better codified standards to turn data into information
– Better reporting and data manipulation to turn information into better representations of
reality (knowledge)
• Better graphing and visualization tools
– More availability of digitized algorithms for clinical decision support – digital wisdom
• Guideline clearinghouses beginning to be codified
So Why do Doctors Hate EMRs?
So Why Do Doctors Hate EMRs
Data Entry is burdensome
New capabilities have created new work streams
– Regulatory requirements
– Expansion of the patient visit
– Incorporation of more data sources
Redistribution of work
Clerical perspective of the EMR
– Providers rarely view EMRs as a clinical competency – neither does almost anyone
else - but I would argue it is
Organization focus in change and innovation
CMIO Lie #2 – We want to be on the cutting edge of technology
Organizations must decide who they want to be from a digital standpoint (and
other innovations as well)
– Disruption
– Leading as a key differentiator
– Early adopter or follower
– Trailer
Is technology who we are or a tool we use?
Organization Focus in Change – More Ideas Than
Time
Device integration
Data Mining
New EMR modules
Machine learning
Enabling best practices (screening, risk scoring etc)
Supply chain management
Interaction with regulatory agencies
Decision support tools
Patient communication tools
Organization focus in change and innovation
Problems with leading innovation/disruption
– Higher risk
– Labor intensive, iterative work
– Opportunity cost
– May require a high focus in a small area of change
– May be difficult to scale
Most organization want to be leaders or adopters –
– Allows scalability
– Predictability of future state
Value of a change based on many domains
Domains of Value
Safety and Quality
User Experience
Patient Experience
System Stability
ROI
Information Portability
Regulatory Compliance
Domain relationships
Improving one area often leads to a
degradation in another
The Net Total Experience needs to
be positive
Projects need to coexist peacefully
and productively

Innovation in using tools vs. Innovation in making
more tools
New Tools
May be easier to control or
customize
Often more industry friendly since
each may represent separate
products
Creates new integration challenges
from data to scale to workflow
Using tools in new ways
More integrated but harder to build
Less highly customized to a specific
use case
Usually more cost controlled
Often more scalable
Desirable Projects
Highly defined scope
Specific goals related to organizational strategy
Fits into the landscape of the organization
Includes longer term support and planning
Approach to Innovation
Workflow integration
– Avoid creating separate parallel work streams
– Designs that are accessed when a clinician is already thinking about that patient
and – even better- that aspect of a patient
Recognize the skills of the team
– Have all members of a team operate to the top of their abilities
Data presentation
– Vetter visualization and digestion of data
– Data → information → knowledge → wisdom
Pay attention to User interfaces – simple and in line with other work
Pay attention to scalability -
Reasons for Hope
Video visits from providers to
smart phones
Real time delivery of patient
results – increasing patient
partnership in care
Wearable monitors populating
EMR data
Consolidating data from
multiple health systems
Big data use in
– Sepsis prediction
– Readmission risk
– Assessing social determinants of
care
Decision Support
– Better imaging test ordering
– Drug-drug and drug-disease
interaction













![[Francis Allard, Cristian Ghiaus] Natural Ventilat(BookZZ.org)](https://static.fdocuments.in/doc/165x107/563db8cf550346aa9a972ad2/francis-allard-cristian-ghiaus-natural-ventilatbookzzorg.jpg)




