
Library Dissertation
201
LIBRARY DISSERATATION SOFT TISSUE RECONSTRUCTION
Transcript of Library Dissertation

LIBRARY DISSERATATION
SOFT TISSUE RECONSTRUCTION

CONTENTS:
INTRODUCTION o SKIN ANATOMY AND PHYSIOLOGY o SOFT TISSUE RECONSTRUCTION PRINCIPLES
FLAPS o HISTORY AND INTRODUCTION o PHYSIOLOGY o COMPLICATIONS
CLASSIFICATION OF FLAPS o LOCAL FLAPS
ADVANCEMENT FLAPS ROTATIONAL FLAPS TRANSPOSITIONAL FLAPS
o REGIONAL FLAPS EXTRA ORAL (LOCAL)
FORE HEAD FLAP NASOLABIAL FLAP AT-T FLAP CHEEK ADVACEMENT FLAP
EXTRA ORAL PECTORALIS MAJOR MYOCUTANEOUS FLAP TRAPEZIUS FLAP STERNOCLEIDOMASTOID FLAP TEMPORALIS MUSCLE FLAP MASSETER MUSCLE FLAP DELTOPECTORAL FLAP LATISMUS DORSI FLAP TEMPEROPARIETAL FLAP PLATYSMA MYOCUTANEOUS FLAP
INTRA ORAL BUCCAL FAT PAD TONGUE FLAP PALATAL FLAP
o FREE FLAPS FASCIOCUTANEOUS FLAP
RADIAL FOREARM FLAP LATERAL ARM FLAP THIGH FLAP ANTERIO LATERAL THIGH FLAP
MUSCULOCUTANEOUS FLAPS RECTUS ABDOMINUS FLAP LATISSMUS DORSI FLAP
SKIN GRAFTS o HISTORY AND INTRODUCTION o FULL THICKNESS GRAFTS o SPLIT THICKNESS GRAFTS o SKIN SUBSITUTES o SKIN STORAGE
RECONSTRUCTION o SCALP o FOREHEAD o EYES o NOSE o EAR o CHEEK o LIP o CHIN
TISSUE EXPANDERS

INTRODUCTION
The skin is a complex tissue that is transected, manipulated, and rearranged during cosmetic and reconstructive surgery.
If the skin is considered an organ, it is the heaviest organ, whereas the lung is the largest organ in surface area. However,
if the skin is considered a tissue, it is not the heaviest tissue. Goldsmith states that the weight of skin is approximately
3.79 kg, fourth heaviest tissue after fat, bone, and muscle.
The skin is not a uniform organ macroscopically, microscopically, physiologically, or when viewed in the fourth
dimension, time. There are regional and temporal variations in the epidermal thickness, dermal thickness, elastic fiber
content, presence and number of hair follicles, sebaceous glands, apocrine glands, and eccrine glands. Parts of the skin
are hair bearing and others are not. The skin may be dry as on the trunk or arms, moist as in the groin or axillae, or oily
as on the face. Skin makes up to 12-15% of an adult's body weight. Each square centimeter has 6 million cells, 5,000
sensory points, 100 sweat glands and 15 sebaceous glands.
ANATOMY OF SKIN
The skin is divided into three layers—the epidermis, the dermis, and the superficial fascia. Like the surface epidermis,
which appears differently in separate body areas, each of these three parts of the skin is different in separate areas of the
body. The average thickness of the skin is about 1 to 2mm.
In the sole of the foot, palm of the hand & in the interscapular region –thick (5mm) and thin over the eyelids
About 80%of the cells in the epidermis are keratinocytes. Keratinocytes are sub-classified by their location within the
epidermis and their degree of keratinization.
The epidermis is divided into five layers:-
1 .The basal cell layer, the stratum germinativum, is the bottom layer of the epidermis. It is composed of a
single layer of cuboidal cells, the basal cells.
Basal cells have a slightly basophilic cytoplasm and divide to give rise to the next layer above, the prickle cell
layer. The basal cells rest on the basement membrane and are connected to each other through desmosomes and to the
basement membrane by hemidesmosomes. Between some of the basal cells are melanocytes, the pigment-producing cells
of the body. For every 10 basal cells there exists about one or two melanocytes. However,this ratio varies in different
areas of the body.
2. The next layer above the basal cell layer is the prickle cell layer, the stratum spinosum. This layer is
usually three to four cells thick and is composed of polygonal cells with preformed keratin. This keratin gives these cells

a definite cytoplasmic eosinophilia. Even under light microscopy, the desmosomal attachments between the prickle cells
are evident. The attachments appear as small spines emanating from the cells and give rise to the name prickle cells.
3. The next layer above the prickle cell layer is the granular cell layer, the stratum granulosum. This layer is
one to four cells thick; the cells contain coarse cytoplasmic granules that are deeply basophilic and represent preformed
keratin granules, keratohyalin granules, that will coalesce to help form the next layer, the cornified layer, the stratum
corneum.
4. The stratum corneum is the outermost part of the epidermis and is formed from the extremely flattened,
anucleated keratinocytes and compacted keratin granules. The cell borders and their nuclei are lost as the keratin granules
fuse, and this layer often is described as having a basket-weave pattern. The stratum corneum is usually a number of cell
layers thick and may reach enormous proportions in the palms and soles.
5. On the palms and soles a fifth layer of epidermis is often identified, the stratum lucidum. This clear area
appears between the stratum corneum and the stratum granulosum. A clear band, separate this layer from the outer layer
of epidermis. Made up of flattened epithelial cells having degenerated nucleus
Cell Types
Keratinocytes – Within the stratum corneum, 60%of its mass and 85%of its cellular proteins are made up of keratin
filament. Keratin filaments are complex tubular structures formed first by three keratin polypeptide chains coiling
together to form a coiled coil, and then nine coils coming together to form a tubular structure. This aggregation occurs
because of a protein component of the keratohyalin granules known as profilaggrin. Profilaggrin undergoes
dephosphorylation and proteolysis to form filaggrin. It is filaggrin that catalyzes the aggregation of keratin filaments.

Certain keratin filaments are also known as tonofilaments and connect the desmosomes at the cell surface with the
nuclear membrane of the cell. Keratin filaments thus provide a cytoskeleton to the cell and may also serve as a
communication system between the cell surface and the nucleus.
Melanocytes - Melanocytes are found within the basal cell layer and are specialized to produce melanin pigment.
Melanocytes may be variable in appearance but appear with routine hematoxylineosin (H&E)–stained sections as
cuboidal cells with a clear cytoplasm and eccentrically placed, crescent-shaped nuclei. Under special stains, such as the
Dopa stain, melanocytes appear as stellate cells. The melanin granules produced by these cells are donated to adjacent
keratinocytes via their stellate projections. In blacks, these melanocytes are particularly active. The ratio of melanocytes
to basal cells is to and varies with anatomical location but not with race. With aging, the melanocytic density decreases
with each decade by 6%to 8%.In addition, the melanocytic enzyme tyrosine declines in activity with age. Therefore, the
elderly do not tan as easily as when they were young. Melanocytes in older skin also are somewhat pleomorphic as are
the keratinocytes. Melanocytes in the elderly may show some nuclear atypia and variations in size, shape, and staining
quality.
Langerhan’s cell - Langerhans’ cells are clear cells found mainlywithin the prickle cell layer. Under light microscopy
these cells resemble melanocytes. These cells are difficult to see unless a special stain, the gold-chloride stain, or
electron microscopy is used. With the gold-chloride stain, Langerhans’ cells appear dendritic. Langerhans’ cells contain
cytoplasmic organelles, Birbeck’s granules, seen under electron microscopy. Langerhans’ cells have many features of
monocytes and macrophages and are thought to migrate to the skin from the bone marrow.
The dendritic processes of the Langerhans’ cells efficiently capture and process antigens within the skin. The
Langerhans’ cells then present the antigen to the skin-specific lymphocytes. The number of Langerhans’ cells is greatly
enhanced during allergic reactions such as contact dermatitis. With aging or exposure to ultraviolet light the number of
Langerhans’ cells decreases.
Merkel’s cell - Merkel’s cell is found in the basal cell layer and, like Langerhans’ cell, is difficult to visualize under light
microscopy under electron microscopy, Merkel’s cell has membranebound granules similar to those found in
neuroendocrine tissue cells. Therefore, this cell is probably part of the amine precursor uptake decarboxylation (APUD)
system of the body and may be associated with the terminal nerves within the skin.
The Dermis
The dermis is divided into two parts, the papillary dermis and the reticular dermis. The papillary dermis is relatively thin
and is located just below the dermal–epidermal junction and is composed of loose collagen, blood vessels, and
fibrocytes. The reticular dermis is below the papillary dermis, is relatively thick, and makes up the rest of the dermis. The
reticular dermis is composed of compact collagen with few fibrocytes. Cutting across the dermis are peripheral branches
of the vascular and nervous systems, hair follicle units and epidermal appendages (i.e., pilosebaceous, apocrine, and
eccrine units).The papillary dermis surrounds the adnexal structures and is called the adventitial dermis.
Effects of Aging

With aging the normal and neat epidermal architecture is lost. Epidermal cells vary in size, shape, and staining qualities.
There is some loss of polarity, and the orderly progression from basal cell layer to granular cell layer is not so
pronounced. Cellular heterogenicity is seen.With aging the epidermis appears thinner under the microscope. It is believed
that the thin epidermis in the elderly is actually a misconception; in the young the epidermis appears thicker because the
dermis is more contractile. The time progression from the basal cell layer to the stratum granulosum is about 2 weeks;
from the lowest layer of the stratum corneum to the surface of the skin takes an additional 2 weeks. In the elderly the
epidermal replacement isdecreased by 30 to 50%and may account for slower wound healing. Cellular proliferation within
the epidermis may also be under control of various stimulatory substances that include nerve growth factor and epidermal
growth factor (EGF). EGF is predominantly located in the basal cell layer with lesser amounts in the more differentiated
cell layers. With increasing degrees of differentiation, EGF binding decreases. EGF has been found to be increased in
transitional cell carcinoma of the bladder where it was associated. With poor differentiation and invasion.
Function of Skin
There are 6 skin functions:
Sensation - the nerve endings in the skin identify touch, heat, cold, pain and light pressure.
Heat regulation - the skin helps regulate the body temperature by sweating to cool the body down when it overheats and
shivering creating 'goose bumps' when it is cold. Shivering closes the pores. The tiny hair that stands on end traps warm
air and thus helps keep the body warm.
Absorption - absorption of ultraviolet rays from the sun helps to form vitamin D in the body, which is vital for bone
formation. Some creams, essential oils and medicines (e.g. HRT, anti-smoking patches) can also be absorbed through the
skin into the blood stream.
Protection - the skin protects the body from ultraviolet light - too much of it is harmful to the body - by producing a
pigment called melanin. It also protects us from the invasion of bacteria and germs by forming an acid mantle (formed by
the skin sebum and sweat). This barrier also prevents moisture loss.
Excretion - Waste products and toxins are eliminated from the body through the sweat glands. It is a very important
function which helps to keep the body 'clean' from the inside.
Secretion - sebum and sweat are secreted onto the skin surface. The sebum keeps the skin lubricated and soft, and the
sweat combines with the sebum to form an acid mantle which creates the right ρH balance for the skin to fight off
infection.

SYSTEMATIC APPROACH TO FACIAL RECONSTRUCTION
1. Characterize defect:
- Skin color
- Skin thickness
- Tissue composition
- Internal lining (mucosa, conjunctiva)
- Structural layer (muscle, cartilage, bone)
- Outer lining (skin, vermilion)
- Location and subunits involved
2. Design reconstructive ladder for defect (list multiple options)
3. Account for key facial landmarks and ideal areas for tissue recruitment: (omit options that transgress nondistortable
landmarks)
4. Design flaps to align with resting skin tension lines
5. Account for patient history
- Radiation, immunocompromise, tobacco abuse, risk of recurrence (narrow options based on increased
survival/success of the flap
Reconstructive ladder
- Healing by secondary intention
- Primary closure
- Delayed primary closure
- Skin grafts
- Split-thickness skin graft
- Full-thickness skin graft
- Tissue expansion
- Local tissue transfer
- Random
- Axial
- Distant pedicled tissue transfer
- Free flap

FACIAL LANDMARKS
Nondistortable landmarks Tissue good for recruitment
- Hairline - Forehead (tight skin)
- Eyebrow - Cheek (lax skin)
- Eyelid and canthi - Chin
- Nasal tip - Submenton
- Nasal ala S- Neck (lax skin)
- Earlobe
- Philtrum
- Vermilion
- Oral commissure
Borges (1984) – “Relaxed Skin Tension Lines”
Excision or incision is planned so that the final scar will be parallel to the relaxed skin tension lines. Maximal contraction
occurs when a scar crosses RSTL the lines of minimal tension at a right angle.
Wrinkle lines are generally the same as the RSTL. RSTL lie perpendicular to the long axis of the underlying muscles and
parallel to Dermal Collagen bundles.

AESTHETIC UNITS OF FACE
(A) FRONTAL AND (B) PROFILE VIEWS OF THE AESTHETIC UNITS AND SUBUNITS OF THE FACE.
1, FOREHEAD UNIT
1A, CENTRAL SUBUNIT
1B, LATERAL SUBUNIT
1C, EYEBROW SUBUNIT
2, NASAL UNIT;
3, EYELID UNITS
3A, LOWER-LID UNIT
3B, UPPER-LID UNIT
3C, LATERAL CANTHAL SUBUNIT
3D, MEDIAL CANTHAL SUBUNIT
4, CHEEK UNIT
4A, MEDIAL SUBUNIT
4B, ZYGOMATIC SUBUNIT

FLAPS
HISTORY OF FLAP SURGERY
The term "flap" originated in the 16th century from the Dutch word "flappe," meaning something that hung broad and
loose, fastened only by one side. The history of flap surgery dates as far back as 600 BC, when Sushruta Samita
described nasal reconstruction using a cheek flap. The origins of forehead rhinoplasty may be traced back to
approximately 1440 AD in India. Some reports suggest flap surgeries were being performed before the birth of Christ.
For millennia it was tacitly assumed that all flaps were skin flaps. In the beginning, these were what today would be
considered random flaps, as the skin was raised without regard to any known blood supply other than to maintain the
presence of the subdermal vascular plexus.
The surgical procedures described during the early years involved the use of pivotal flaps, which transport skin to an
adjacent area while rotating the skin about its pedicle (blood supply). The French were the first to describe advancement
flaps, which transfer skin from an adjacent area without rotation. Distant pedicle flaps, which transfer tissue to a remote
site, also were reported in Italian literature during the Renaissance period.
Subsequent surgical flap evolution occurred in phases. During the First and Second World Wars, pedicled flaps were
used extensively. The next period occurred in the 1950s and 1960s, when surgeons reported using axial pattern flaps
(flaps with named blood supplies). In the 1970s a distinction was made between axial and random flaps (unnamed blood
supply) and muscle and musculocutaneous (muscle and skin) flaps. This was a breakthrough in the understanding of flap
surgery that eventually led to the birth of free tissue transfer.
In the 1980s the number of different tissues types used increased significantly with the development of fasciocutaneous
(fascia and skin) flaps, osseous (bone), and osseocutaneous (bone and skin) flaps.

FLAP PRINCIPLES
Over the past 50 years the development and application of several different flaps has led to reliable reconstruction of
facial defects. Most defects can be reconstructed immediately, leading to better restoration of form and function with
early rehabilitation.
Reconstructing facial defects can be both challenging and rewarding. Missing tissue most often results from either
trauma or oncologic surgery.
Commonly there is a wide range of options for repairing a given defect, including healing by secondary intention,
primary closure, placement of a skin graft, or mobilization of local or regional tissue. Compared to skin grafts, local flaps
often produce superior functional and esthetic results. A great advantage of local tissue transfer is that the tissue closely
resembles the missing skin in color and texture. These flaps can be rotated, advanced, or transposed into a tissue defect.
Regional tissue can also be recruited to repair facial defects.
When deciding which option to use, there should be a progression from simple to complex treatments. Consideration
should be given to primary closure or the use of skin grafts first, followed by local, then regional, and finally distant
pedicled or microsurgical free tissue transfer.
Flaps require additional incisions and tissue movement, which increase the risks of postoperative bleeding, hematoma,
pain, and infection. Confirmation of tumor free margins should be done prior to flap reconstruction if a malignant lesion
has been excised. Some defects are amenable to closure with a single flap, but others require a combination of flaps for
optimal results. An advantage of using multiple flaps is that they can be harvested from separate esthetic units. This
decreases the size of the secondary defect and may allow placement of scars between esthetic units, thus improving scar
camouflage leading to better cosmesis.
Often, separated repair of individual facial subunits with separate flaps provides a better cosmetic result than if a single
flap is used to reconstruct the entire defect.

Flaps differ from grafts in that they maintain their blood supply as they are moved. Abundant dermal and subdermal
plexus allow for predictable elevation of random cutaneous flaps.
A cutaneous flap may also have its arterial supply based on a dominant artery in the subcutaneous layer. Muscular
perforating arteries are important contributors to the cutaneous vascular bed. The most important variable for flap
viability is not the length-to-width ratio but, rather, the perfusion pressure and Vascularity at the pedicle base.
Because local flaps provide their own blood supply, they are particularly useful in patients with compromised recipient
sites such as those that have been irradiated. As local flaps heal, regaining of blood flow and cutaneous sensibility
increases. The rate of blood flow and two-point discrimination on the surface of local flaps is statistically no different
when compared with the corresponding area of the unoperated side.
The recovery of sensory nerve function in facial flaps is dependent on the intimacy of contact between the flap and the
recipient bed and on the viability of the type of restoration.
Relaxed skin tension lines (RSTLs) result from vectors within the skin that reflect the intrinsic tension of the skin at rest.
They are due to the microarchitecture of the skin and represent the directional pull on wounds
The RSTLs are generally parallel to the facial rhytids. Lines of minimal tension (rhytids) result from repeated bending of
the skin from muscular contraction. A permanent crease results from the adhesions between the dermis and deeper
tissues. These natural skin creases run perpendicular to the direction of muscle pull and can guide incision orientation for
optimal scar camouflage and cosmesis. The face is composed of esthetic subunits. The areas where these subunits meet
are referred to as anatomic borders. The esthetic subunit principle is based on the fact that our eyes see objects as a series
of block images that are spatially organized. Scars that are located at the junction of two adjacent anatomic subunits are
inconspicuous because one expects to see a delineation between these areas.
PRINCIPLE I: REPLACE LIKE WITH LIKE
This is a particularly important principle. When filling in a defect, replace like with like. Ralph Millard once said, "When
a part of one's person is lost, it should be replaced in kind, bone for bone, muscle for muscle, hairless skin for hairless
skin, an eye for an eye, a tooth for a tooth."
If this cannot be accomplished, use the next, most similar tissue substitute. For example, the surgeon can use scalp to
replace a beard and skin from the forehead to cover a nose wound. The goal is to camouflage the reconstruction as much
as possible.
Everyone can learn from Mother Nature's blending tricks. The surgeon's goal is to create an effect as subtle as a
chameleon changing colors as it moves through its surroundings.
An example of this can be found in the treatment of any eyelid injury. The best course of action when faced with a full-
thickness defect is to use eyelid skin from the contra lateral eye. If this is not possible, the next best substitute is a full-
thickness posterior auricular skin graft. This provides the most similar substitute tissue, with a satisfactory color match
and minimal tendency toward contracture.
If the surgeon's work can pass unnoticed, he is to be congratulated as having accomplished his task as a reconstructive
surgeon
PRINCIPLE II: THINK OF RECONSTRUCTION IN TERMS OF UNITS
According to Millard, human beings may be divided into seven main parts: the head, neck, body and extremities.
Each of these body parts can be further subdivided into units. The head, for example, is composed of several regional
units: scalp, face, and ears.

Consider that each of these units has its own unique features, and each feature has in turn multiple subunits with their
own special shapes. All of these different units and subunits must be considered and reproduced during reconstruction.
As emphasized by Millard, "The most important aspects of a regional unit are its borders, which are demarcated by
creases, margins, angles and hair liners."
Taking this a step further, perhaps the most important principle is the way in which the borders between units come
together and interact, rather than just the borders themselves.
It is important to adhere to these natural borders during reconstruction. Most often it is better to convert a defect that
covers only a partial unit to a whole-unit defect prior to reconstruction.
According to Millard, "If possible make the defect fit the flap or graft to that unit!"
PRINCIPLE III: ALWAYS HAVE A PATTERN AND A BACK-UP PLAN
As with all surgery, it is of utmost importance to compare the pros and cons of each surgical option. The reconstructive
ladder is a mental exercise that provides the surgeon with options ranging from the simplest to most complex.
Usually, it is best to keep things as simple as possible. This benefits both the surgeon and the patient; the simplest plan is
often the safest.
However, physicians should not sell themselves or patients short. Avoid settling for the simplest procedure just for the
sake of simplicity. More complex problems may require more complex solutions, and the simplest approach may be,
frankly, inadequate.
A sound plan must provide restoration of function and aesthetic form; these are the fundamental goals of plastic and
reconstructive surgery.
A nose, breast, or finger reconstruction should be designed to fit its use and location, rather like the philosophy used by
architects when designing buildings. In 1949, a pioneer of twentieth-century architecture, Frank Lloyd Wright, said,
"Form and function thus become one in design and execution if the nature of materials and methods and purposes are all
in unison." Several years earlier, Wright had been asked to build a hotel in Tokyo. As Japan was in an earthquake zone,
Wright designed the hotel to withstand shocks using a sea of mud to support the foundations. Following the Japanese
earthquake of 1923, Wright's hotel was apparently the only building left standing in Tokyo.
Once you have decided on a plan, rehearse it. Trace the defect or cut a pattern to fit the defect. Transpose the pattern and
experiment with it to decide on the best donor area and orientation. Omitting this step is akin to Lloyd Wright building
his hotel without a blueprint, and his materials were much cheaper than the surgeon's!
Finally, ask yourself "what do I do next if this fails?" Proceed to the operating room only after answering this question
definitively. Once in the operating room, it is important to keep an open mind and be ready to adjust the surgical plan as
the situation dictates.
PRINCIPLE IV: STEAL FROM PETER TO PAY PAUL
Apply the "Robin Hood" principal: steal from Peter to pay Paul, but only when Peter can afford it. Using what the body
has to reconstruct a deficit is essentially "robbing the bank." The goal to achieve is ultimate efficiency, or, according to
Millard, "getting something for almost nothing."

Do not make the naive mistake of merely advancing tissue to the deficient area unless this can be accomplished
completely without tension. Tension compromises the blood supply of the advanced tissue and ultimately results in flap
failure. Tension is to be feared the most. Recognize and prevent it or else use
PRINCIPLE V: NEVER FORGET THE DONOR AREA
Surgeons once believed in treating the primary defect without worrying about the secondary defect. Plastic surgery has
since progressed. Plastic and reconstructive surgeons now realize the importance of considering both defects equally.
The reality is that it is NOT possible to get something for nothing; a price usually must be paid following reconstruction
of a primary defect. The significance of providing coverage of a defect with minimal deformity and disability is one of
the foremost principles on which our specialty is based.
If reconstruction of the primary defect is too costly in terms of resultant deformity or disability, it is better to re-evaluate
and use another reconstructive option.
Remember that donor areas are not limitless. One cannot continuously use tissue without paying back in some way.
Carelessness or overuse of a donor area eventually causes damage that may be far greater than the original defect.
A skin flap is composed of skin and subcutaneous tissue that is transferred from one part of the body to another, with a
connection to the body or vascular pedicle preserved for its blood supply. The relationship of the vascular pedicle to the
flap may vary according to the orientation of the defect to the flap. In some cases, the vascular pedicle can be transected
and transferred to a distal site by microvascular anastomosis to another set of recipient (nourishing) vessels
(microvascular free flap). Microvascular free tissue transfer may include fascia and skin, or a composite of skin, muscle,
and bone.
Because of the inherent limited blood supply, random flaps had to be restricted to rigid length to width ratios to assure
viability. Such simplicity abruptly disappeared after Milton disproved the veracity of arbitrary length to width ratios, and
asserted instead that flap viability was directly proportional to the circulatory pattern captured within the given flap
territory.
Skin flaps are frequently needed because either the recipient site is poorly vascularized and is unable to nourish a free
skin graft or the transfer of a skin flap provides a better match of color and texture. When planning the reconstruction of
a facial defect, the surgeon must consider the location of the defect, visibility of the site, and the patient’s concern with
the final aesthetic appearance.
FLAP PHYSIOLOGY
Because of its thermoregulatory function, the rate of blood flow through the skin is one of the most variable in
the body. At baseline, blood flow to the skin is approximately 10 times that required for nutritional support. It is because
of this relative oversupply that random flaps are able to survive.
Skin derives its nutrient supply from a network of capillaries. Flow through these capillaries is controlled by
pre-capillary sphincters. Local hypoxemia and an increased level of metabolic products induce these sphincters to open.
Arteriovenous (AV) shunts also determine flow through the capillary network. Thus, pre-AV shunt sphincters
control both thermoregulation and systemic blood pressure. These sphincters are under sympathetic control. For
example, an increase in body temperature results in a decrease in norepinephrine release, which results in closure of the
AV shunts and increased blood flow to the skin.
Following transposition and insetting of a flap, the first 48 hours are a critical period with respect to determining
flap survival. During this time, there is a surge in the level of catecholamines locally, resulting in vasoconstriction; the
supply of catecholamines from traumatized nerves is exhausted after 48 hours. In addition, the inflammatory cascade
results in increased levels of Thromboxane A2 (also a powerful vasoconstrictor) and free radicals, as well as edema. All
of these factors result in either ischemia or direct injury to the flap. A fibrin layer forms at the recipient site within the
first 2 days. Neovascularization then begins at 3-7 days. Revascularization adequate for division of the flap pedicle has

been demonstrated by 7 days. Endothelial cells are responsible for the release of angiogenic factors responsible for
neovascularization.
There are four important concepts pertaining to flap physiology: stress, strain, creep, and stress relaxation. Stress refers to
the force applied per cross-sectional area. Strain refers to the change in length divided by the original length of the given
tissue to which a force is applied. Creep refers to the increase in strain seen when skin is under constant stress. This
occurs over a matter of minutes and is due to an extrusion of fluid from the dermis and a breakdown of the dermal
framework. Meanwhile, stress relaxation is the decrease in stress when skin is held in tension at a constant strain for a
given time. This occurs over a matter of days to weeks and is due to an increase in skin cellularity and the permanent
stretching of skin components. The concept of serial excision is based upon the fact that skin closed under tension will
display a certain amount of stress relaxation and creep over time.
The probability of tip necrosis is directly related to both length and tension. Thus, at equal closing tensions, longer
flaps display a higher probability of tip necrosis.
Undermining may not always represent the best means of correcting for excessive tension. Beyond 4 cm,
undermining has little effect on tension Studies in animals suggest that excessive undermining may increase flap
necrosis. It is not true that the surviving length of a flap depends entirely on the width of the base. The surviving
length of a random pattern flap is determined by the perfusion pressure within the arterioles and intravascular
resistance. Widening the base of a flap does not affect either of these factors. Thus, there is no benefit to widening the
base beyond a certain point. When perfusion pressure falls below the critical closing pressure of an arteriole, blood
flow through that arterial ceases. In general, most authors agree that a length to width ratio of 3 or 4 to 1 will result in
a viable random pattern flap on the face or scalp.
Delay of the insetting of a flap historically has been one of the only methods generally agreed to decrease the
incidence of flap failure due to ischemia. For random flaps, one incises along the long axis of the flap and undermines
without dividing either end of the flap. For axial flaps, one incises along all margins but the base of the flap (so as not
to cut across the pedicle) without undermining. In both cases, the flaps are left in place at the donor site and then
transposed and inset into the recipient bed after 1-2 weeks. The benefits of delay are lost if delayed beyond 3 weeks to
3 months. Three theories have been proposed to explain the delay phenomenon: first, that it improves blood flow
primarily by the reorientation of vascular channels and the formation of vascular collaterals; second, that it conditions
the tissue to ischemia; and third, that it closes the AV shunts.
PREOPERATIVE PLANNING AND SURGICAL TECHNIQUE
Patient factors that reduce flap viability include increasing age, malnutrition, diabetes, hypertension, peripheral
vascular disease, hyperlipidemia, smoking, immunosuppression, and a prior history of external beam irradiation
(XRT). XRT delays but does not eliminate neovascularization.
Patients who smoke 1 pack or more per day are three times more likely to develop flap necrosis, and if necrosis occurs,
it tends to be more severe than in nonsmokers. This deleterious effect is due to vasoconstriction caused by nicotine,
and systemic tissue hypoxia caused by increased levels of carbon monoxide. The patient should be sternly advised to
abstain from smoking for 48 hours before and 7 days after a flap, otherwise another means of reconstruction should be
sought.
Surgical factors that reduce flap viability include excessive thinning, aggressive electrocautery, crush injury secondary
to rough handling, and damage to axial vessels secondary to tension or traumatic dissection.
Several general rules should guide the performance of local skin flaps on the face. The best color and texture match is
obtained when the flap is taken from the same facial aesthetic unit as the defect. The skin to be moved should match
the color, texture, and appendageal characteristics of the recipient site. Donor skin should be elastic. The majority of
incisions for the flap should parallel the relaxed skin tension lines (RSTL). This also tends to direct wound tension
parallel to the lines of maximal extensibility (LME), which sit perpendicular to the RSTL. Any incision is least
conspicuous if it occurs at the junction of aesthetic units. Long, straight scars are best avoided unless they are hidden
within the hairline, a deep skin crease, or the junction between aesthetic units. Do not obliterate critical anatomic lines
or borders essential for aesthetics or function Closure cannot result in an unacceptable level of tension The secondary

defect must be capable of satisfactory closure. Meticulous hemostasis should be obtained before final suturing. Skin
hooks and finetoothed forceps should be used in tissue handling to avoid blunt trauma. Dead space deep to flaps
should be eliminated; tacking sutures should be used conservatively as needed.
When a defect crosses aesthetic units, it is best to compartmentalize the repair and design individual flaps to
construct separate components of the defect such that the junction between aesthetic units is preserved.
Before the flap is incised, the surgeon should undermine around the defect and beneath the donor site. The
surgeon should check skin laxity. On the one hand, primary closure might be possible. On the other hand, there might
not be enough laxity, necessitating the design of a different flap. At this point, the flap is incised and undermined, and
a few key sutures are placed. The face is then inspected for distortion, and flap blood supply is assessed. The donor
site should be closed first, which usually will decrease tension at the distal tip of the flap. If excessive tension is
present at this point, the key sutures can be repositioned, a back cut can be made, or one can undermine more tissue.
Once the flap is in its final position (and not before), standing deformities can be excised as Burow’s triangles. Final
closure is then performed in 2 layers.
Small defects of the forehead are generally amenable to primary closure. Larger defects of the forehead
usually require local flap closure. Here it is important to avoid distortion of the eyebrow, and incisions should be
placed in skin creases when possible. The hairline is available and should be used to hide incisions, although one
must avoid transposing hair-bearing skin into a non-hair bearing area. Around the eyebrow unilateral or bilateral
advancement flaps often work well because they take advantage of the horizontal skin creases of the forehead. In the
central, superior forehead, an A-to-T flap works well because it takes advantage of the hairline. Similarly, in the
temple area, A-to-T and rhomboid flaps both work well.
Defects of the medial canthus area measuring 1 cm or less may be left to heal by secondary intent.
Otherwise, larger defects are usually best closed with transposition flaps from the glabellar region.
The landscape of the nose is not uniform, which can make flap selection more challenging. The skin of the
upper 2/3 of the nose is thin and mobile, while the skin of the lower 1/3 is thick and immobile. For the upper nose,
the bilobed or rhomboid flaps work well. If the defect involves the mid-dorsum, the dorsal nasal flap is a good bet.
The bilobed flap is also very effective in closing defects 1.5 cm or less in diameter of the lower nose. For larger
defects, the paramedian forehead flap is the workhorse, though a nasolabial flap may also be used. However, a major
problem with the nasolabial flap is that it crosses the nasofacial angle and can result in blunting of this junction
between aesthetic units.
The cheek enjoys abundant soft tissue and laxity, which affords many options for repair, including primary
closure. For the lateral cheek, rhomboid and bilobed flaps may work nicely. For medial cheek or large defects, cheek
advancement, as well as cervicofacial rotation/advancement flaps may work well. Incisions in this case may be
hidden along the edge of the nose, in the nasolabial fold, along the infraorbital rim, and in the preauricular skin
crease.
The chin does not have as much subcutaneous tissue. The sublabial crease is useful in scar camouflage (e.g.,
with an A-to-T flap), but one must avoid incisions crossing this crease, which can result in a webbed scar.

TYPES OF FLAP
Classification:
According to distance from the defect:
a. Local flaps
b. Distant flaps
Blood supply
a. Random
b. Axial
i. Peninsular flaps
ii. Island flaps
iii. Free flaps
Tissue movement
a. Rotation
b. Advancement
c. Transposition
Mathes and Nahai Classification
a. One vascular pedicle (eg, tensor fascia lata)
b. Dominant pedicle(s) and minor pedicle(s) (eg, gracilis)
c. Two dominant pedicles (eg, gluteus maximus)
d. Segmental vascular pedicles (eg, sartorius)
e. One dominant pedicle and secondary segmental pedicles (eg, latissimus dorsi)
Flap Classification Based on Type of Tissue Transfer
a. Skin (cutaneous)
b. Fascia
c. Muscle
d. Bone
e. Visceral (eg, colon, small intestine, omentum)
f. Composite
Fasciocutaneous (eg, radial forearm flap)
Myocutaneous (eg, TRAM flap)
Osseocutaneous (eg, fibula flap)
Tendocutaneous (eg, dorsalis pedis flap)
Sensory/innervated flaps (eg, dorsalis pedis flap with deep peroneal nerve)

Random flaps - They are based on the rich perforating vascular plexus of the skin. They are random in their
blood supply, but also random in their design. These are Unpredictable, having a length:width ratio of 3:1 or 4:1,
however the ratio followed in the face is approximately 2:1.
Random flaps or random pattern flaps (local cutaneous flaps) are the most common type of flap employed in
reconstruction of cutaneous defects of the head and neck. These flaps are created by dissecting the flap at the level
of the subcutaneous fat. Their arterial supply comes from perforating musculocutaneous vessels at the flap base
arising from segmental vessels that underlie muscle and subcutaneous tissue
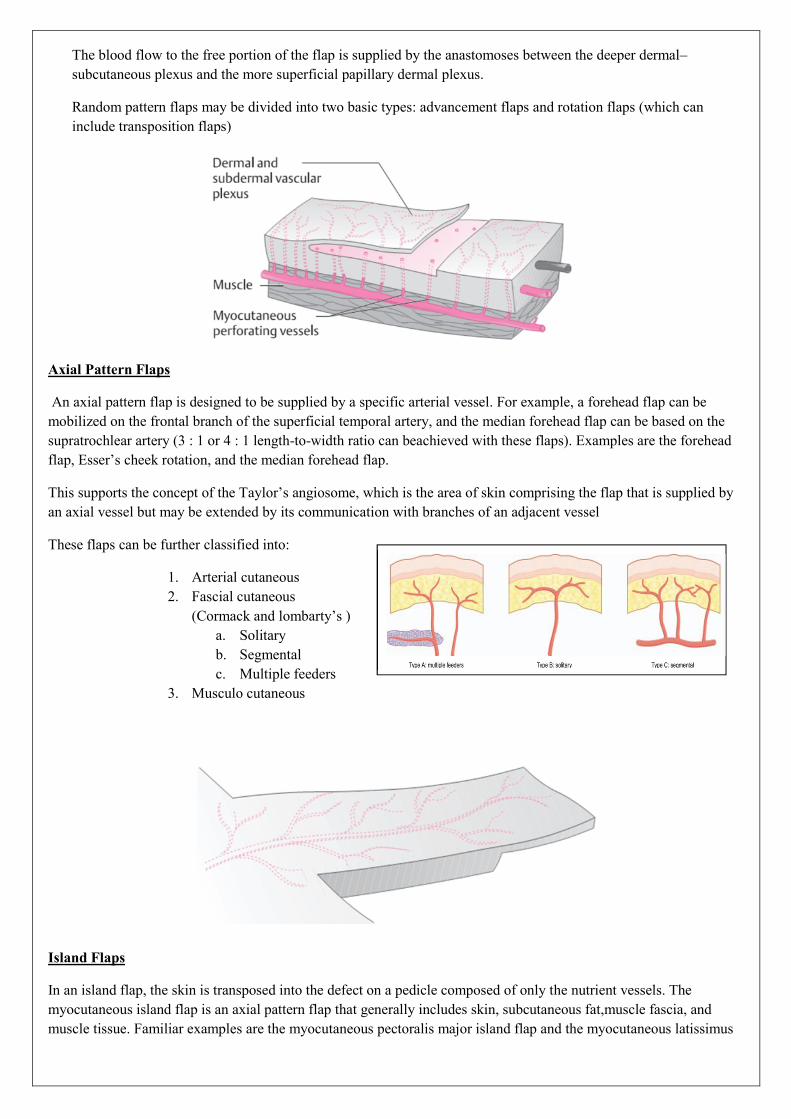
The blood flow to the free portion of the flap is supplied by the anastomoses between the deeper dermal–
subcutaneous plexus and the more superficial papillary dermal plexus.
Random pattern flaps may be divided into two basic types: advancement flaps and rotation flaps (which can
include transposition flaps)
Axial Pattern Flaps
An axial pattern flap is designed to be supplied by a specific arterial vessel. For example, a forehead flap can be
mobilized on the frontal branch of the superficial temporal artery, and the median forehead flap can be based on the
supratrochlear artery (3 : 1 or 4 : 1 length-to-width ratio can beachieved with these flaps). Examples are the forehead
flap, Esser’s cheek rotation, and the median forehead flap.
This supports the concept of the Taylor’s angiosome, which is the area of skin comprising the flap that is supplied by
an axial vessel but may be extended by its communication with branches of an adjacent vessel
These flaps can be further classified into:
1. Arterial cutaneous
2. Fascial cutaneous
(Cormack and lombarty’s )
a. Solitary
b. Segmental
c. Multiple feeders
3. Musculo cutaneous
Island Flaps
In an island flap, the skin is transposed into the defect on a pedicle composed of only the nutrient vessels. The
myocutaneous island flap is an axial pattern flap that generally includes skin, subcutaneous fat,muscle fascia, and
muscle tissue. Familiar examples are the myocutaneous pectoralis major island flap and the myocutaneous latissimus

dorsi island flap. With some flaps, sensory or motor nerves can be mobilized in addition to nutrient vessels. For
example,authors have transferred neurovascular island flaps from around the mouth for use in lip reconstruction.
Free Flaps
Microvascular free tissue transfer or free flaps have evolved over the past decade through the technologic advances in
the field of microvascular surgery. These techniques allow the reconstructive surgeon to transfer free axial-pattern
skin (fasciocutaneous), skin and muscle (musculocutaneous), or skin, muscle and bone (osteomyocutaneous or
osteocutaneous) flaps from a host donor site to a distant recipient site in a singlestage operation. The axial artery and
vein that supply the flap are anastomosed under the microscope, with recipient vessels
Method of Transfer
The most common method of classifying flaps is based on the method of transfer.
Advancement flaps are mobilized along a linear axis toward the defect.
Rotation flaps pivot around a point at the base of the flap. Although most flaps are moved by a combination of rotation
and advancement into the defect, the major mechanism of tissue transfer is used to classify a given flap.
Transposition flap refers to one that is mobilized toward an adjacent defect over an incomplete bridge of skin.
Examples of transposition flaps include rhombic flaps and bilobed flaps.
Interposition flaps differ from transposition flaps in that the incomplete bridge of adjacent skin is also elevated and
mobilized. An example of an interposition flap is a Z-plasty. Interpolated flaps are those flaps that are mobilized either
over or beneath a complete bridge of intact skin via a pedicle. These flaps often require a secondary surgery for
pedicle division.
Microvascular free tissue transfer from a different part of the body relies on reanastomosis of the vascular pedicle.
Designing the Flap
There are many options for reconstructing facial defects. Often the optimal method is not readily apparent. A stepwise
approach can be helpful in selecting and designing a flap. The characteristics of the defect and adjacent tissue must be
analyzed. These include color, elasticity, and texture of the missing tissue. The defect size, depth, and location are
evaluated as well as the availability and characteristics of adjacent or regional tissue.
It is important to determine the mobility of adjacent structures and to identify those anatomic landmarks that must not
be distorted. The orientation of the RSTLs and esthetic units should by analyze closely. Potential flap designs should
be drawn on the skin surface being careful to avoid those designs that obliterate or distort anatomic landmarks. The
final location of the resultant scar should be anticipated by previsualizing suture lines and choosing flaps that place the
lines in normal creases.
The secondary defect that is created as the tissue is transferred into the primary defect must be able to be closed easily.
When designing a flap, it is important to avoid secondary deformities that distort important facial landmarks or affect
function. Avoid obliterating critical anatomic lines that are essential for normal function and appearance. Proper
surgical technique involves gentle handling of the tissue by grasping the skin margins with skin hooks or fine-toothed

tissue forceps. Avoid traumatizing the vascular supply by twisting or kinking the base of the flap. Deep pexing sutures
minimize tension on the flap and eliminate dead space.
Excessive tension on the flap may decrease blood flow and cause flap necrosis. Meticulous hemostasis should be
achieved prior to final suturing so that a hematoma does not develop beneath the flap. It is important to adequately
mobilize and extend the flap, which should be of adequate size to remain in place without tension to minimize the
chance of dehiscence, scarring, or ectropion.
Advancement Flaps Advancement flaps have a linear configuration and are advanced into the defect along a single
vector. These flaps can be single or double. Advancement flaps are often chosen when the surrounding skin exhibits
good tissue laxity and the resulting incision lines can be hidden in natural creases. Advancement flaps limit wound
tension to a single vector with minimal perpendicular tension. They are often helpful in reconstructing defects
involving the forehead, helical rim, lips, and cheek. In these areas advancement flaps capitalize on the natural forehead
furrows without causing vertical distortion of the hairline superiorly or the eyebrow inferiorly. Advancement flaps are
created by parallel incisions approximately the width of the defect. Standing cutaneous deformities (“dog ears”) are
usually created and are managed with excision. A Z-plasty incision or Burow’s triangle may be performed at the base
of the flap, reducing the standing cutaneous deformities. A variation of the advancement flap
is the V-Y flap. A triangular island of tissue adjacent to the defect is isolated and attached only to the subcutaneous
tissue. It relies on a subcutaneous pedicle for blood supply. As it is advanced into the defect, the secondary defect is
closed primarily in a simple V-Y manner. These flaps are especially amenable for cheek defects along the alar facial
groove and are generally avoided where there are superficial nerves because of the depth of the incisions. Intraoral
uses of advancement flaps include covering oroantral fistulas and alveolar clefts. A disadvantage of buccal
advancement flaps is the decrease in vestibular sulcus depth.
Rotation Flaps
Rotation flaps have a curvilinear configuration. Defects reconstructed with rotation flaps should be somewhat
triangular or modified by removing normal tissue to create a triangular defect. These flaps have a large base and are
usually random in their Vascularity but may be axial. One or more rotation flaps are often used to reconstruct scalp
defects. Because of the relative inelasticity of the scalp tissue, these flaps must be large relative to the size of the
defect. Scoring of the galea is helpful in gaining additional rotation and advancement.
The axial frontonasal flap is a modified simple rotation flap with a back cut. It is useful for closing nasal defects. The
flap is based on a vascular pedicle at the level of the medial canthus. This pedicle consists of a branch of the angular
artery and the supraorbital artery.
Rotated palatal flaps are helpful for closing large oroantral fistulas. Fistulas < 5 mm in diameter usually close
spontaneously.18,19 Local flaps or grafts can be used to close larger fistulas. Two layer closures are less prone to
developing recurrence of oroantral fistulas. Approximately 75% of the palatal soft tissue can be rotated to cover
adjacent defects.
Transposition Flaps
These flaps are rotated and advanced over adjacent skin to close a defect. Examples of transposition flaps include
rhombic flaps and bilobed flaps. These flaps are advantageous in areas where it is desired to transfer the tension away
from closure of the primary defect and into the repair of the secondary defect. Transposition flaps have a straight
linear axis and are usually designed so that one border of the flap is also a border of the defect. An advantage of this
type of flap is that it can be developed at variable distances. Areas where these flaps are often used include the nasal
tip and ala, the inferior eyelid, and the lips. The rhombic flap is a precise geometric flap that is useful for many defects
of, the face. The traditional rhombic (“Limberg”) flap is designed with 60 and 120° angles and equal-length sides. The
angle of the leading edge of the rhombic flap is approximately 120° but may vary. The flap is begun by extending an
incision along the short axis of the defect that is equal to the length of one side of the rhombic defect. Another incision
is then made at 60° to the first and of equal length (Figure 38-9). Disadvantages of the rhombic flap are the significant
tension at the closure point as well as the amount of discarded tissue to transform a circular defect into a rhombus. The

bilobed flap is a transposition flap with two circular skin paddles. Esser is credited with the design of the bilobed flap
in 1918. It is useful for skin repairing of lateral nose and nasal tip defects up to 1.5 cm. The bilobed flap has a random
pattern blood supply. The flap is primarily rotated around a pivot point and the paddles are transposed over an
incomplete bridge of skin. The second lobe allows the transfer of tension further from the primary defect closure. The
bilobed design rotates around an arc that is usually 90 to 100°. In the bilobed flap the first lobe closes the defect and
the second closes the first lobe defect. The flap is designed with a pivot point approximately a radius of the defect
away from the wound margin. The first lobe is usually the same size as the defect, and the second lobe is slightly
smaller with a triangular apex to allow for primary closure. The axis of the second flap is roughly 90 to 100° from the
primary defect and undermined widely to distribute the tension. An advantage of the bilobed flap is that one can
construct a flap at some distance from the defect with an axis that is independent of the linear axis of the defect. A
disadvantage of this flap is that it leaves a circular scar that does not blend with the existing skin creases. During
healing the flap may become elevated (“pin cushioning”) because of the narrow pedicle that is prone to congestion,
scar tissue that impedes lymphatic drainage, and curvilinear scars that tend to bunch the flap up as they shorten.
Interpolation Flaps
Interpolation flaps contain a pedicle that must pass over or under intact intervening tissue. A disadvantage of these
types of flaps is that for those passing over bridging skin, the pedicle must be detached during a second surgical
procedure. Occasionally it is possible to perform a single-stage procedure by deepithelializing the pedicle and passing
it under the intervening skin.
Advantages of interpolation flaps include their excellent vascularity, and also their skin color and texture match. The
forehead flap (median and paramedian) is a commonly used interpolation flap and remains the workhorse flap for
large nasal defects. It is a robust and dependable flap.
Eg: The nasolabial flap (melolabial) is useful for reconstructing defects involving the oral cavity and those involving
the lower third of the nose. It can be used as an interpolation flap with either a single or staged technique.

LOCAL FLAPS
Types of Local Flaps
Extra Oral
Z-Plasty
Advancement Flaps
o U-Plasty
o H-Plasty
o V-Y Plasty
o Y-V Plasty
o Cheek Advancement Flap
o At-T Advancement Flap
Transpostional Flap/Kite Flap
Rotational Flap
o Scalp Advancement Flap
o Cervico Facial Flap
Bilobed Flap
Rhombic Flap
Deflourmental Flap
Forehead Flap
W-Plasty
Intra Oral Flap
Z-Plasty
Advancement Flap
Buccal Mucosal Flap
Buccal Pad Fat
Transpostional Flap
o Tongue Flap
o Palatal Flap
o Nasolabial Flap

Z-PLASTY
The Z-plasty is a procedure which involves the transposition of two interdigitating triangular flaps. Its name derives
from the fact that, drawn out on the skin, the three limbs of the flaps have the overall shape of a Z. Although hallowed
by long usage the name is not strictly accurate since the limbs are equal in length.
Transposition of the flaps has several effects of which two have special relevance:
1. There is a gain in length along the direction of the common limb of the Z.
2. The common limb of the Z becomes changed in direction.
It is exploitation of these effects which makes the Z-plasty one of the most useful as well as one of the most widely
used procedures in plastic surgery. Its worth has been established in two sets of circumstances, the treatment of
contractures
When we make use of the phenomenon of lengthening, and the management of facial scars when we make use of the
fact that the common limb changes in direction. Although both lengthening and change of direction occur together it is
usually only one of the two aspects which concern the surgeon at any particular time. The simultaneous and
inescapable accomplishment of the other is usually a bonus but it can be a nuisance.
Use in contractures
The basic maneuver when the Z-plasty is used in a contracture the common limb, i.e. the central limb of the Z, lies
along the line of the contracture to be released. The usual size of each of the angles of the Z is 60°, a compromise
figure which has been reached as a result of experience. The reasons for selecting this angle size and the effects of
altering it will be discussed later but 60° will be the size used in the present discussion
Constructed in this way the two triangles together have the shape of a parallelogram with its shorter diagonal in the
line of the contracture, its longer diagonal perpendicular to it. The two diagonals can conveniently be referred to as the
contractural diagonal and the transverse diagonal.

To understand the sequence of events when a Z-plasty is used in a contracture it is essential to bear in mind that the
common limb of the Z, being along the line of the contracture is under considerable tension. Because of this its ends
spring apart as the fibrous tissue band along the contracture line is divided when the flaps are raised. Springing apart
of the divided contracture has the effect of changing the shape of the parallelogram and causes the triangular flaps to
become transposed, the contractural diagonal to lengthen and the transverse diagonal to shorten.
It is important to appreciate that the surgeon does not actively transpose the Z flaps when a Z-plasty is used properly
to correct a linear contracture; flap transposition follows naturally from the change in shape of the parallelogram.
The changes in length are such that the length of the contractural diagonal after transposition equals that of the
transverse diagonal before transposition. Increase in length of the contractural diagonal has been achieved at the
expense of the transverse diagonal which has shortened as much as the contractural diagonal has lengthened.
Translated into practical terms this means that skin has been brought in from the sides with a tightening effect, as
shown by the shortening of the transverse diagonal, to achieve the lengthening of the contractural diagonal; the
difference in length of the two diagonals indicates the actual amount of lengthening and shortening.
The surgeon is naturally more interested in the lengthening than the shortening which inevitably accompanies it, but it
is crucial to successful Z- plasty practice to bear in mind that without the transverse shortening there will be no
lengthening. In practical terms, unless transverse slack is available to be taken up, equal in quantity to the length
difference between the axes of the Z, the method will not work.
Construction of the Z
Since the skin flaps must fit together in their transposed position the limbs of the Z must of necessity be equal in
length. The angles of the Z are also usually made equal in size. The factors in construction which do vary are angle
size and limb length and the ways in which these variable factors affect the result provide an explanation of why a
specific construction is used in a particular set of circumstances.
Angle size
Once the lengths of the limbs of the Z have been decided the lengthening to be expected depends entirely on the size
of the angle and as the angle increases so too does the amount of lengthening. With an angle of 30° there is
theoretically a 25% increase in length, with 45° a 50% increase, while with an angle of 60° the increase rises to 75%.
It must be stressed that at all times it is percentage increase of length which is controlled by size of angle.

These increases are theoretical and cannot be applied clinically with strict accuracy, although when account is taken of
variations in skin extensibility, presence of scarring, etc., it is surprising how well they do apply. The actual
lengthening is usually a little less than the theoretical value.
In theory angles of up to and beyond 90° could be used with steady increase in the amount of lengthening but in
practice limiting factors emerge which determine the optimal angle.
Reduction of the angle much below 60° would defeat the very object of the Z-plasty since the smaller angle would
produce less gain in length.
In addition, narrowing of the flap significantly would have a disastrous effect on its blood supply. Increase of the
angle much beyond 60° would increase the amount of lengthening but, as already stressed, this would entail an equal
amount of transverse shortening. Tissue for transverse shortening is seldom available in unlimited quantity and as the
angle increases beyond 60° the tension produced in the surrounding tissues tends to be so great that the flaps cannot
readily be brought into their transposed position.
For these reasons 60° is the compromise figure usually used for angle size.
Limb length
Just as angle size controls percentage increase of length so limb length controls the actual increase in length since the
increase is a proportion of the original length. A longer initial limb results in a greater increase of length for a
particular size of angle. Such an increase in the amount of lengthening naturally increases the tissue brought in from
the sides.
The factors which limit maximum and minimum angle size have resulted in the compromise use of 60° as the routine
Z-plasty angle and it is length of limb which provides the major variable in practice. Regardless of length of
contracture the amount of tissue available on either side determines the practicable limb length - a large amount will
permit a large Z, a small amount will correspondingly limit the size of the Z.
The single and the multiple Z
The search for ways of reducing the amount of transverse shortening without significantly affecting the amount of
lengthening has led to the development of the multiple Z-plasty and its advantages are such that it has virtually
replaced the single Z-plasty in many clinical situations.
In the single Z-plasty one large Z extends along virtually the entire length of the contracture; in the multiple Z-plasty
the contracture is divided into a number of segments on each of which a small Z is constructed.
The contrast between the two can best be appreciated by using a concrete example. If we construct a single Z which is
going to achieve 2 cm of lengthening and at the same time construct a series of four small Zs each equal in size to a
quarter of the single Z we can compare them from the point of view of lengthening and shortening.

Comparison of the lengthening and shortening produced by a single and a multiple Z-plasty. Note also how lateral
tension is concentrated by the single Z-plasty and diffused by the multiple Z-plasty.
The single Z achieves 2 cm of lengthening and at the same time there is 2 cm of shortening in the transverse axis.
The multiple Z behaves very differently. Each of the four Zs produces 0.5 cm of lengthening with a corresponding 0.5
cm of shortening at each transverse axis. The lengthening being in series is additive giving an overall lengthening of 2
cm; in contrast the shortening is in parallel and remains 0.5 cm at each Z.
In both the single and multiple Z then the amount of lengthening achieved is the same but the shortening has been
greatly reduced by using the multiple Z. Many situations exist in which a Z-plasty could be used to advantage where
the tissue cannot stand 2 cm of shortening but could tolerate 0.5 cm with ease. For those the multiple Z-plasty is a
possible solution.
The change from single to multiple Z-plasty also alters the type of lateral tension. From being concentrated in the line
of the transverse limb of the single Z, it is diffused over the several transverse limbs of the multiple Z-plasty in
addition to being reduced, and this has obvious advantages from a vascular point of view.
In the multiple, as in the single Z-plasty, the theoretical lengthening is probably not capable of being achieved for,
quite apart from the effect of scarring, etc., there tends to be some loss of lengthening in passage from one Z to the
next. Nevertheless the comparison between the two and the advantages of the multiple over the single are still valid.
Practice of the Z-plasty
From the theoretical discussion it follows that the Z-plasty is most effective where the contracture is narrow and the
surrounding tissues are reasonably lax since scarred and contracted tissue on either side can yield no 'slack' to allow
lengthening.
This fact explains why the post burn contracture is so seldom totally correctable by a Z-plasty, single or multiple. The
burn scar in contracting has contracted in all directions simultaneously. Although a contracture may be present
clinically, skin has really been lost in every axis; the contractural axis is only the most obviously tight. The transverse
axis is just as short and unable to shorten any further in the way needed for a successful Z-plasty.
Ideally the central limb of the Z extends the full length of the contracture but this requires a correspondingly large
quantity of tissue to be brought in from the sides, tissue which is not always available. It is in the limbs particularly
that this problem arises, for such tissue as is available is not concentrated at one point but is spread out along the
length of the limb. In such circumstances as have been discussed above the solution may be to construct a series of
short Zs instead of one large Z and so bring in from the sides small quantities of tissue all the way down the line of the
contracture.
A good measure of the planning and execution of a Z-plasty is the behavior of the flaps when the contracture is
released. If the maneuver is indicated and well planned the flaps should literally fall into their new transposed
position; indeed it should be difficult to get them back into their old relationship.
It is when the contracture is of the bowstring type that the Z-plasty is most effective. With the contracture more
diffuse in breadth and length it is less satisfactory and a stage is reached where it must be decided whether a Z-plasty
is an adequate procedure or whether fresh skin must be imported from elsewhere as a free skin graft. The answer is
usually to be found in the surrounding skin; skin must be present as slack at the sides if the contracture is to be
released and if it is not obviously available there the Z-plasty will fail and a free skin graft is the true answer to the
problem.
Planning the Z-plasty
It may be difficult in planning the procedure to decide where the flaps should be. A good method is to draw an
equilateral triangle on each side of the contracture and from the resulting parallelogram to select the more suitable of

the two sets of limbs. One set may have no particular advantage, in which case either may be used. Factors which
might favour one set rather than the other are:
1. The flap with the better blood supply is preferable; in particular one with scarring across the base should be
avoided.
2. One or other flap may give a scar which will fall into a better line cosmetically. The factors which would
influence the choice
3. The lie of the flaps and the surrounding skin may permit one set of flaps to rotate more readily into their
transposed position.
Skin which is scarred has lost much of its normal elasticity and this may affect slightly the planning of the flaps. A
flap of scarred skin should be made a little longer initially than its fellow of normal skin, otherwise the scarred flap
will be found to be too short when it is sutured to the unscarred flap.
It is usual although not absolutely essential to have the two angles of equal size. On occasion a line of scarring will
limit the angle of one flap and dissimilar angles may then have to be used. Lengthening in such a case becomes the
average of the amount to be expected from each angle alone. Indeed if the full quadrilateral of any Z is drawn
complete with contractural and transverse diagonals the transverse diagonal will indicate the actual length to be
expected when the flaps are transposed.
The Multiple Z-plasty
When a single large Z-plasty cannot be used for any of the reasons already discussed the alternative may be to use a
multiple Z-plasty. The line of the contracture is then regarded as a series of contracted segments and on each a small Z
is constructed creating a line of separate Zs. Such a construction, although it works perfectly well in practice, has been
taken a stage further to produce the continuous multiple Z-plasty where the Zs, instead of being individual, form a
continuous series giving the appearance of a long line along the contracture with multiple Z side limbs. This is the
type of multiple Z-plasty which is now routinely used and it can be constructed with the side limbs either parallel or
skew. The presence of scarring in a particular line
may influence the construction and make skew flaps preferable but the use of parallel limbs allows the flaps to rotate
uniformly in transposition, at the same time preventing the occurrence of the broad-tipped flap with its narrow base
which is undesirable from a vascular point of view and inevitable with the skew construction.
Whether a multiple Z-plasty must be used will largely depend on the depth of the bowstring. It is unwise to take the
side limbs much beyond the base of the bowstring and if the making of a large Z would encroach on the surrounding
flat skin to any extent, especially if it tends to be taut, then a multiple Z-plasty is safer and on the whole just as
effective.
Blood supply of the flaps
The most frequent complication of the Z-plasty is necrosis of the tip of a flap and it is particularly common if there has
been much scarring of the skin. Precautions to avoid necrosis can be taken at all stages of the procedure: by providing
the flaps with the maximum of vascular capacity, by avoiding tension and by meticulous haemostasis.
Provision of maximum vascular capacity
This is achieved by designing the flaps broad at the tip, by avoiding scarring across the base and by cutting the flaps as
thick as possible. The tip of the flap can be broadened without affecting the angle size by slightly modifying the shape
of the flap. The thickest flap practicable should always be cut using the levels of undermining.

Avoidance of undue tension
This can be a very difficult problem particularly when the contracture is a doubtful candidate for Z-plasty or free skin
graft. The large, single Z concentrates transverse tension while multiple, small Zs diffuse the tension making it less at
each individual Z so that embarrassment of the circulation from this cause is reduced to a minimum. While the
contracture may be placed under tension during the procedure to display its line and extent, the parts should be dressed
and bandaged in a mid-position to promote relaxation of tissues in all directions.
The modified shape of the Z-plasty flaps to give maximum vascular capacity.
Meticulous haemostasis
Quite apart from the role it can play in raising flap tension, haematoma predisposes to infection and infection is a
potent cause of flap necrosis. Careful haemostasis is consequently essential.
Use in scars
It is well recognized that scars in the face tend to be more cosmetically acceptable the more nearly they lie in a line of
election; a problem of acceptability is liable to arise when an otherwise satisfactory scar is more than 30° off the line
of election. When a Z-plasty is used to improve the appearance of a scar its effect is to break the line of the scar and
change its direction. This change takes place with the change in direction of the common limb of the Z. The most
desirable result is achieved postoperatively when this common limb is made to lie transversely in a line of election and
to this end careful planning is essential.
Siting the Z-plasty
The success of the method used to place the transverse common limb of the complete Z-plasty accurately in terms of
size, site and direction depends on two facts. First, if the Z-plasty incisions are made to end on the selected transverse
line, transposition of the flaps leaves the transverse common limb automatically lying along the line as planned.
Secondly, the limbs of the Z-plasty are equal in length.

If mistakes are to be avoided, the planning of the Z-plasty must be regarded as a formal procedure, to be marked out
carefully on the skin before any actual incision is made. The steps themselves are more easily illustrated than
described. With the scar outlined the line selected for the transverse common limb is drawn out on the skin with
Bonney's Blue, the line naturally being in a line of election. The length of the intended transverse common limb,
which determines the size of the Z-plasty, is measured out on the line of the scar, proportioned approximately evenly
on each side of the line selected and drawn out as the transverse common limb. From each extremity of this measured
length a line of equal length is marked out to meet the line drawn out as the transverse common limb. This gives three
lines of equal length and together they make the Z-plasty flaps. The fact that the two oblique lines have been made to
end on the selected transverse line means that transposition of the flaps brings the transverse common limb into the
desired line as planned, and this is true regardless of its direction. Altering its obliquity merely has the effect of
altering the size of the Z-plasty angle. Increase of obliquity reduces the angle and decrease of obliquity increases the
angle to a maximum of 60°, at which point the transverse limb becomes perpendicular to the line of the scar.
As the transverse limb departs from the perpendicular the flap becomes narrower and the blood supply to its tip
increasingly tenuous. Facial skin with its excellent blood supply is more tolerant of narrow flaps than skin elsewhere
on the body surface, but even in the face there is a limit to permissible narrowness; a tip angle of 35° is as narrow as
can be used with safety. The angle size can fortunately be gauged at the planning stage before any incision is actually
made.
ADVANCEMENT FLAP
It refers to flap created by incisions that allow for a sliding movement of the tissue.It best works in area of greater skin
elasticity.
Types
Unipedicle
Bipedicle
V-Y
Y-V
A-T
Cheek advancement flap
Useful applications of advancement flaps
Forehead
Medial cheek
Eyebrow
Helical rim
Unipedicle advancement flap (U-plasty)
Created by parallel incisions, which allow sliding movement of tissue in a single vector toward a defect.Triangular
skin excisions along the periphery of the wound.Typically are designed with a ratio of defect width-to-flap length of
1:3. Eg cheek advancement flap

Bilateral unipedicle advancement flap (H-plasty)
Helpful for repair of the central lips & chin Disadvantage is long suture line.
In both cases, advancement flaps are incised on opposite sides of the defect & advance toward each other.Two flaps
don’t necessarily have to be of the same length.First incise & elevate only one flap.
Advantage of bilateral flaps over a single flap for repair of these midline structures is that equal pull from the two
opposing flaps lessens tissue distortion & the propensity toward deviation of midline structures toward one side.
V-Y, Y-V Flap
It is a type of advancement flap where Y incision/defect is converted into V or V shaped incision is converted into Y

Transpostional flaps
It is made by moving a rectangle or square of skin and subcutaneous tissue on a pivot point to cover an
immediately adjacent defect. The end of the flap should extends beyond the defect. These type of flaps have a
Linear axis, a Pivot point and are very versatile. Its ability to harvest a flap at some distance from the location
of the defect.
Types
Classical flap
Bilobed flap
Rhombic flap
Deflourmental flap
Advantages
It can be designed in a number of configurations to adapt to irregular-shaped defects.
Ample quantities of subcutaneous fat may be left attached to the under surface of the flap to assist with filing
of deep facial defects.
Lengthy flap relative to the width of the base can be developed & this facilitates closure of the donor defect
without excessive wound closure tension.
Disadvantages
Potential for developing a trap–door deformity. This complication tends to occur a few weeks following
transfer.

Rotation flap
A rotation flap requires that you make the defect into a triangle, and then swing the skin around. It has to rotate on a
pivot point, the radius of the arc of rotation being the line of the greatest tension. Use rotation flaps on skin which has
a good blood supply.
They are particularly useful on the scalp, and but are unsuitable below the knee where the blood supply is poor. Make
a rotation flap three times bigger than necessary, so as not to over estimate elasticity of the skin

Indications:
Scalp defects
Large cheek defects greater than 3 to 4 cm in the lower preauricular area where recruitment of the upper
posterior cervical skin is required for wound closure.
Contraindications:
Parts of the body where a patient’s
Skin is tight, or his circulation is poor, as in his hand and below his knee.
Don’t make a rotation flap over bone
(other than the skull) or over tendon.
Advantages:
It has two only two sides ; thus, it lends itself to placing one side in a border between aesthetic regions of the
face.
The flap is broad based, there its vascularity tends to be reliable.
Great flexibility in the design & positioning of the flap.
Bilobed flap
Synonyms: Transposition flap, double transposition flap, cutaneous defect, bilobed rotational flap

The bilobed flap is a double transposition flap commonly used in reconstruction of facial skin defects. The bilobed
flap allows for the movement of more skin over a longer distance than that possible with a single transposition flap.
This flap is especially useful when it is applied to facial areas where skin is less mobile (eg, nasal tip, temporal
forehead), as it allows for reconstruction of the primary defect with skin of matching consistency and color.
History of the Procedure: In 1918, Esser first described the bilobed flap to repair nasal tip defects. He attributed the
increased versatility of the flap to the reduced arc of rotation required by using 2 flaps to reconstruct the defect instead
of 1.
Zimany is generally credited with popularizing the use of the bilobed flap. He defined this as a flap consisting of 2
lobes separated by an angle and based on a common pedicle.
The use of a bilobed flap is indicated when the tissue adjacent to a cutaneous defect is insufficiently mobile to close
the defect without causing tissue distortion.
Relevant Anatomy: The bilobed flap is a random transposition flap because its blood supply does not arise from a
segmental artery, and no defined pedicle is present.
Blood supply to the skin is via musculocutaneous and cutaneous arteries that perforate subcutaneous tissue. These
vessels ascend into the deep reticular and papillary dermis to supply deep and superficial microcirculatory plexus.
Rich anastomoses of vessels within these plexus provide blood flow into the most distant portion of the flap.
Procedure
The bilobed flap, as Esser first described, comprises 2 flaps identical in size and form and separated by angles of 90°.
Skin is transposed over 180°. This transposition commonly results in a noticeable pincushion effect or trapdoor
deformity, ie, domelike elevation or depression, respectively, of the flap relative to the surrounding skin. Esser's
design results in prominent tissue protrusion (i.e., dog-ear or standing cone) at the point of rotation. 1:1 length is to
width ratio should be followed
Modification of Esser's design has improved cosmetic results. In modified designs, the lobes are not identical in
size. The larger flap is slightly narrower than the defect it has to fill, and the second flap is half the width of the larger
flap. Their lengths are identical. Angles between the lobes are less than 90°. The second flap is often designed with an
elliptical tip to facilitate closure of its resulting defect. Each flap is transposed over 45°. Wide undermining is used to
reduce tension and pincushion effect.

As with all local flap designs, take care to place incisions in relaxed skin tension lines. Raise the flap just deep to the
subdermal plexus, leaving a small amount of subdermal fat on the undersurface of the flap. Position flaps in areas of
increased tissue laxity.
Bilobed flaps are extremely reliable when used properly. Given proper flap design, partial or complete failure is
unpredictable. Flaps designed with large length-to-width ratios increase the likelihood of distal compromise because
of the limited ability of the microcirculation to adequately perfuse the distal flap. Thinner flaps tend to increase the
risk of distal failure because thinning the flap and leaving insufficient adipose tissue can disrupt the deep
microcirculatory plexus. Because thinning may be necessary to improve the cosmetic result (i.e., to avoid a pincushion
effect), judicious use is recommended.
Typically, dog-ears occur when flap lobes are transposed. Moy et al described several useful ways to deal with this
problem. A Burrow triangle may be included in the flap design at the base of the defect.
Two other methods can be used to repair dog-ear defects. Excess tissue can be excised from the flap base, or it may be
excised from the skin adjacent to the flap. Some believe that the cosmetic result is superior when tissue is excised
adjacent to the flap because it breaks up the long, inferior scar line.
Rhombic flap
Because of the different sizes and shapes of defects, the conditions, availability, and extensibility of surrounding skin,
and the proximity of different anatomic structures, there is no single transposition flap to reconstruct all cheek defects.
However, the rhombic flap is frequently used for reconstructing small to moderate-sized cheek defects. While it is not
applicable in all cases, an understanding of its basic principles is often helpful in the plan and design of other
transposition flaps.
Indications
The rhombic flap, described by Limberg, is the one we use most for re- constructing cheek defects. It has a precise
geometric design, and knowledge of its principles helps to understand flap transfer and to plan and execute other
transposition flaps.
Anatomy
Axial-pattern (arterial) flaps are seldom used for reconstructing cheek defects. Random-pattern (cutaneous) flaps are
the rule, since there is very little concern about their viability because of the favorable blood supply to the cheek skin.
Random-pattern flaps of the cheeks are raised at a level that preserves the subdermal vascular plexus, which requires
that a layer of the subcutaneous tissue remain on the flap.

The skin of the cheek is richly vascular. Perfusion is mainly through the facial artery, which courses superiorly and
medially from the inferior border of the mandible to the nasofacial groove. Other arteries supplying the cheek skin
are the transverse facial artery (a branch of the superficial temporal), the buccal branch of the maxillary artery, the
infraorbital artery (one of the terminal branches of the maxillary artery), and the zygomatic branch of the lacrimal ar-
tery (a branch of the ophthalmic artery).
All the arteries supplying the cheek have corresponding veins that accompany them. The facial vein is the chief vein
of the cheek. It lies posterior to the facial artery and follows the course of the artery. It communicates with the
ophthalmic vein, which empties into the cavernous sinus, and with the infraorbital and deep facial veins, which
communicate with the cavernous sinus through the pterygoid plexus. It drains into the internal jugular vein in the up-
per neck
Flap Design and Dimensions
Transposition skin flaps use tissue adjacent to the defect but from a different plane to effect closure. Such flaps are
designed adjacent to the defect, so that they share a portion or all of one side of the defect. Although flap shapes may
vary, all can be thought of as having two sides, a distal end and a base. If excision of a lesion can be designed in the
shape of a rhombus, with adequate margins that do not excessively sacrifice normal tissue, the rhombus is marked
around the lesion with two sides parallel to the lines of maximum extensibility of the skin (LME), when possible.
The rhombic flap is designed to reconstruct a 60-degree rhombic defect (ADEF in Figure). In such a defect, the
length of all the sides and the short diagonal are equal, i.e., two equilateral triangles with a common base. The distal
end of the flap (D' C') is a continuation of the short diagonal of the defect (FD) and of equal length. The side of the
flap next to the defect (AD') is also a side of the defect (AD). The side of the flap farthest from the defect (BC') is
parallel to the near side (AD') and equal in length. All sides of the defect and the flap are equal in length.
Four potential donor sites are then mentally pictured, and the site with the most available skin is determined by
manual pinching, pushing, and pulling of the skin in these areas.

(This is also helpful in assessing the effect donor-site closure will have on surrounding anatomic structures.) The
rhombic flap is then drawn in the most favorable area and mentally transposed, checking the direction of the vectors
of tension (VOT) and looking for possible problems.
When possible, the flap should be planned so that the short diagonal of the flap donor site (DB) is in the same di-
rection as the lines of maximum extensibility. This facilitates. Closure of the donor site by taking advantage of the
extensibility of the skin in that direction. We accomplish this by designing the rhombic defect so that two parallel
sides are in the same direction as the lines of maximum extensibility. Of the four rhombic flaps possible, two will
have their short diagonals in the direction of the lines of maximum extensibility. One of these flaps should be
chosen for reconstruction, if there are no contraindications.
The near corner of the flap base is adjacent to the defect. The far corner is the width of the base away from the
defect and serves as the pivot point during transfer of the flap. In the description of the classic transposition flap, the
pivot point is assumed to be stationary. This requires that the flap be longer than the defect in order to reach the
distal end of the defect when it is transferred. However, in the type of transposition flaps we commonly use, the
pivot point is advanced toward the defect as the flap is transposed. This facilitates primary of the donor site and
obviates additional length requirement.
Lines of maximum extensibility: These lines run parallel to the relaxed skin tension lines (RSTL). The skin is most
extensible in the direction of the lines of maximum extensibility.
When the shape of a lesion is predetermined and it is not practicable to convert in to rhombus, the elements of design
of the rhombic flap are often useful in devising other transposition flap for closure. This is practically true for oval,
circular and teardrop shaped defects. A rhombus is drawn around the defect, and the most favorable donor site is
determined by using the same method already described for reconstruction of a rhombic defect. A rhombic flap is
drawn in that area. Inside the outline, a flap with dimensions and shape similar to the defect is drawn filling the
rhombic flap outline in same manner that defect fills its surrounding rhombus. The flap is then visual transposed in to
the defect, assessing the areas that will be under tension and the direction of the vectors of tension. If an area under
tension is near a mobile anatomic structure and the vector of tension pints toward that structure, it will probably be
distorted if that flap is used. In such cases, another flap should be considered.

W–PLASTIES
This is the only purely cosmetic procedure described here. A linear scar by can be camouflaged by cutting triangles of
skin out of the edges of the incision and sewing it up as a series of Ws. This will not give any added length in the
direction of the scar, so it is of no use in releasing contractures, for which Z–plasty is procedure of choice. W-
PLASTY Remove the scar along with 1 cm equilateral triangles of skin on either side of it. If the triangles are bigger,
they will be too conspicous. Carefull Plannig with a pattern has to be done, and make sure they fit together. The
triangles are to be planned the triangles carefully, and make thesame number each side.

EXTRA ORAL FLAPS
(LOCAL)

I. FOREHEAD FLAP The forehead flap is primarily based on the supratrochlear vessel, is relatively narrow, and uses a skin paddle from the
forehead region. The flap is supplied by a rich anastomosis between the supratrochlear and angular arteries. Because
of the marked vascularity, it is possible to incorporate cartilage or tissue grafts for nasal reconstruction. The forehead
flap has abundant tissue available, allowing resurfacing of the entire nasal unit with a single flap and provides a good
texture and color match to the native nose. The technique for elevating the forehead flap is straightforward. The flap
can be designed directly in the midline or in a paramidline location. A template of the defect is used to outline the flap.
Elevation of the flap proceeds in either a subgaleal or subcutaneous plane. The pedicle is always elevated in such a
way as to incorporate the frontalis muscle. The width of the pedicle is usually 1.0 to 1.5 cm, which allows for easy
rotation of the pedicle. Prior to inset the skin paddle is selectively thinned to match the native skin thickness. The
pedicle is divided approximately 3 weeks later, with the base of the pedicle inset into the glabellar area to reestablish
brow symmetry. The incision, and resulting scar, is perpendicular to the RSTLs but tends to heal well.
Midline Forehead Flaps
History
Nasal reconstruction originated almost 3000 years ago in India, where midforehead flaps were developed to
reconstruct noses. Nasal amputation was a form of punishment for various crimes from theft to adultery, and this
practice gave rise to the need for reconstruction. A seventh century CE Indian medical document, the Sushruta Samita,
described the approach. In the 15th century, Antonio Branca of Italy discovered an Arabic translation of the Sushruta
Samita and was the first to perform a similar procedure outside of India. In Europe, Italian surgeons used a pedicled
flap from the medial surface of the upper arm for nasal reconstruction until J.C. Carpue, in the late 18th century, found
a description of the Indian techniques.
Carpue first practiced these techniques on cadavers and later applied them to live patients, eventually publishing his
results. His use of the forehead flap subsequently spread across Europe and America, revolutionizing nasal
reconstruction. Carpue's basic techniques laid the foundation for modern nasal reconstruction for the next century.
Kazanjian advanced the development of the forehead flap by advocating primary closure of the forehead donor site.
These techniques were modified further and popularized by Millard in the 1960s and 1970s. He used a characteristic
gull-wing design with lateral extensions for alar reconstruction and extended the pedicle incisions below the brow to
provide greater flap length. Burget and Menick made significant contributions to the forehead flap by emphasizing
aggressive thinning of the skin paddle, narrowing the pedicle base for easier rotation and length, and modifying
defects to follow aesthetic subunits of the nose. The midline forehead flap is based on a narrow pedicle centered on the
medial brow area, often capturing the proximal supratrochlear artery with a skin paddle positioned in the precise
center of the forehead. An advantage of this flap is that the donor site scar is in a more aesthetic midline position,
consistent with principles of facial aesthetic units.
Problem
Nasal reconstruction poses the challenges of restoring aesthetics in a prominent area on the face while preserving
function. A full-thickness defect requires a multilayered reconstruction that addresses each of the 3 separate layers of
the nose (i.e., cutaneous surface, internal lining, and structural support). Once structural grafting is placed, its covering
must be durable and of similar thickness and texture to native nasal skin and it must have its own blood supply.
Ideally, this is accomplished with minimal donor site morbidity and with reproducible dependability.
Indication
Numerous nasal resurfacing techniques have been described, and all play roles in different circumstances, whether as
skin grafts or local bilobular flaps. For larger cutaneous defects, the forehead flap remains the standard and is often the
only feasible means of providing coverage over cartilaginous grafts. The forehead flap has no absolute indication, and
it is associated with greater morbidity (including the need for second operative stage) compared with many other local

nasal flaps. Whenever possible, repair nasal defects with simpler methods (eg, full-thickness skin grafts for very
superficial defects, bilobular flaps for smaller ones).
Other considerations include patients' aesthetic expectations (recognizing that simpler methods may leave contour
problems), poor color match, or some degree of alar base distortion and contraction. These outcomes can be
anticipated when using a skin graft for a deeper defect or when pushing the limits of a local nasal flap (creating
excessive tension). When these aesthetic results are unacceptable, the forehead flap is indicated.
Generally, cutaneous defects involving the nasal tip fare poorly with skin grafts, even thicker ones, and either a local
flap or a forehead flap is indicated. Conversely, native nasal skin of the upper third is much thinner and amenable to
grafts. Defects larger than 1.5 cm may exceed the limits of a local flap and often do better with an interpolated flap
from the forehead. Defect size is influenced by the consideration of the aesthetic nasal subunits that are often excised
when involved with the primary defect. Finally, any reconstruction that requires structural grafting necessitates a
resurfacing flap that has its own blood supply; a strong indication for the forehead flap.
Relevant Anatomy
Forehead flaps are based on the robust vasculature to the forehead via the supraorbital, supratrochlear, and terminal
branches of the angular vessels. The first anatomic point involves forehead flap terminology. The median forehead
flap is harvested from the mid forehead and has a wide pedicle based in the center of the forehead, which may capture
both supratrochlear vessels. The paramedian forehead flap is designed around a unilateral supratrochlear artery,
allowing for a much narrower pedicle. The skin paddle and pedicle are aligned vertically, with the supratrochlear
notch in the paramedian position of the forehead. The resultant donor scar is oriented vertically and aligns with the
medial brow.

The midline forehead flap is a hybrid of median and paramedian flaps, with the skin paddle harvested from the precise
center of the forehead. The associated pedicle runs obliquely and is based on a unilateral supratrochlear vessel and
collaterals from the medial brow area. Collateral flow from the angular artery can contribute to significant perfusion
pressure at the pedicle base. The body of the midline flap is harvested from the precise center of the forehead,
allowing a less conspicuous donor scar that is more consistent with facial aesthetic units. The pedicle may be based on
either side, allowing choices between flap length and the arc of pedicle rotation.
The rich anastomoses between vessels along the medial brow and glabellar areas provide perfusion pressure at the
proximal pedicle and sustain the midforehead flaps. The supratrochlear artery is the primary feeder vessel and exits at
the superior and medial corner of the bony orbit, approximately at the medial point of the eyebrow. It passes
superficial to the corrugator muscle and deep to the orbicularis, ascending in a paramedian position for approximately
2 cm before piercing the frontalis muscle. The supratrochlear artery then travels superiorly in the subcutaneous plane,
above the galea/frontalis muscle, maintaining numerous anastomoses with the contralateral vessels.
Forehead flap design is influenced by nasal anatomy. The thickness and mobility of the nasal skin varies across
different anatomic sites. The skin overlying the dorsum and sidewalls is thin and mobile, whereas the skin of the nasal
tip and nasal alae is thicker and less mobile. Nasal topography is a combination of convex and concave surfaces that
provide the foundation of nasal aesthetic subunits. These subunits are the block images the casual eye detects upon
viewing a nose. These images are then synthesized into the expected and familiar nose shape. Borders between these
subunits tend to be inconspicuous, and they provide optimal scar-concealment areas. When planning a nasal defect
reconstruction, replace the entire involved aesthetic subunit rather than just filling in the original hole

Infiltrate local anesthetic with epinephrine throughout the nose and forehead, even with patients under general
anesthesia. Carefully outline aesthetic subunits of the nose at the outset of the procedure to help define the defect in
terms of aesthetic units. Excise these units accordingly to strategically place the flap borders (and consequently the
final scars) along the borders of these units, thus rendering them less conspicuous.
Although strict adherence to a numerical value is unnecessary, 20% involvement generally results in complete
excision. The authors tend to be more aggressive when the additional excision does not mandate a longer forehead flap
(i.e., when the aesthetic unit of concern is cephalad to the original defect). On the other hand, when a defect only
marginally involves the superior border of a nasal tip unit, the physician is less likely to complete tip excision because
doing so requires extending the forehead flap superiorly and, possibly, into the hairline.
After involved subunits are excised and the defect shape is modified, cut and mold a malleable foil template (eg, a
suture package) to match the new defect. This template serves 2 purposes: (1) precisely describing the shape of the
defect (especially any irregular and sharp edges) and (2) demonstrating 3-dimensional contours often lost by simple
ruler measurements. Account for alar lobule convexity during the initial measurements. Unrecognized convexity
results in a flap that is too narrow and a lobule that is flat, without the normal acute alar-facial angle.
The foil template is then transferred to the exact midline of the forehead for markings (s. By placing the template (and
so the skin paddle of the flap) in the precise midline, the resultant scar is positioned strategically in the center of the
forehead and tends to be less conspicuous than paramedian scars.
Plan the vertical position of the template by rotating gauze from the pedicle base, near the medial brow, from the
defect site to the upper forehead. This technique assures that the planned flap reaches all defect borders. An ipsilateral
flap refers to a pedicle base on the same side as the nasal defect and has the advantage of an effective greater flap
length to reach the distal border of the defect. This comes at the expense of a greater arc of rotation, which
theoretically comprises the pedicle base.
Alternatively, a contralateral flap has less rotation at the pedicle base but may not reach as far caudally as the
ipsilateral flap. Additionally, the contralateral flap tends to cause less visual interference than the ipsilateral flap.
Midline defects have no advantage, and the decision is arbitrary.
Elevate the skin paddle of the flap in the subcutaneous plane, above the frontal muscle. Additional selective thinning
is then performed to better match variable skin thicknesses of different nose regions . If the patient has small vessel
disease and an intermediate stage is anticipated, lift the skin paddle and transfer it in the subgaleal plane, with planned
thinning after 3 weeks.
Elevate the pedicle portion of the flap in a subgaleal plane to the level of the orbital rim. At the inferior border of the
pedicle, the dissection continues under the corrugator muscle, allowing the supratrochlear artery to be kept between
the orbicularis oculi muscle and corrugator. The periosteum in this region can be incised and incorporated into the
pedicle base, allowing greater caudal reach and some rigidity to the base for vascular protection.
With the ipsilateral or contralateral flap or the midline versus paramedian flap, center the pedicle base on the medial
brow, capturing the supratrochlear artery, and narrow it to no more than 1 cm to facilitate rotation with less kinking at
the base. The pedicle base can be extended beyond the supraorbital rim and into the brow as needed for additional flap
reach without a compromise of flap perfusion. The supratrochlear foramen or notch may be palpated in some
individuals and can serve as a reference point. Some authors advocate using a Doppler probe to locate and follow the
course of the supratrochlear artery. This practice is used only very rarely because of the dependable anatomy and
robust vascular perfusion in this area. After flap and pedicle elevation, rotate them to fill the nasal defect using a
layered closure with eversion of the skin edges.
The cephalic border of the nasal defect is under the flap pedicle and is not closed. The forehead donor site is usually
closed primarily in a layered fashion, with attention to reapproximating the galeal layer. Donor site defects larger than
3.5 cm often cannot be closed primarily and are best allowed to heal by secondary intention rather than with secondary
local flaps or skin grafts. The forehead wound undergoes progressive contracture, and the center of the wound fills
with granulation tissue, resulting in a final scar that exceeds other techniques. The pedicle is usually loosely wrapped
with antibiotic-impregnated gauze and is changed regularly.
Some surgeons apply a skin graft to the pedicle undersurface to reduce wound weeping. The pedicle is divided safely
after 3 weeks. Aggressively thin the cephalic border of the flap from above to best match surrounding skin thickness;
however, exercise caution to avoid extending the level of undermining beyond 50% of the original skin paddle. The
vascular supply to the flap is retrograde from the recipient bed, and excessive undermining can jeopardize viability.
Trim the pedicle base, and either inset the base back into the glabellar region or excise it entirely and close primarily.
The pedicle inset method is dictated by brow position and symmetry; often the brow on the pedicle side is displaced
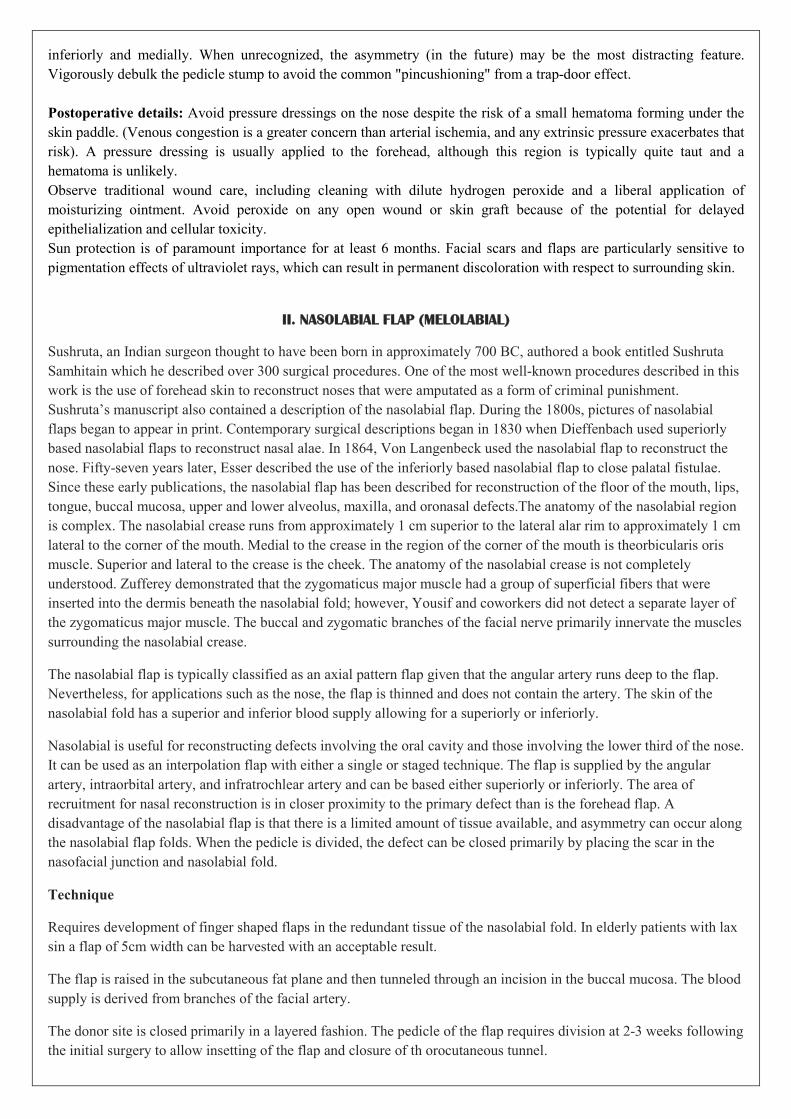
inferiorly and medially. When unrecognized, the asymmetry (in the future) may be the most distracting feature.
Vigorously debulk the pedicle stump to avoid the common "pincushioning" from a trap-door effect.
Postoperative details: Avoid pressure dressings on the nose despite the risk of a small hematoma forming under the
skin paddle. (Venous congestion is a greater concern than arterial ischemia, and any extrinsic pressure exacerbates that
risk). A pressure dressing is usually applied to the forehead, although this region is typically quite taut and a
hematoma is unlikely.
Observe traditional wound care, including cleaning with dilute hydrogen peroxide and a liberal application of
moisturizing ointment. Avoid peroxide on any open wound or skin graft because of the potential for delayed
epithelialization and cellular toxicity.
Sun protection is of paramount importance for at least 6 months. Facial scars and flaps are particularly sensitive to
pigmentation effects of ultraviolet rays, which can result in permanent discoloration with respect to surrounding skin.
II. NASOLABIAL FLAP (MELOLABIAL)
Sushruta, an Indian surgeon thought to have been born in approximately 700 BC, authored a book entitled Sushruta
Samhitain which he described over 300 surgical procedures. One of the most well-known procedures described in this
work is the use of forehead skin to reconstruct noses that were amputated as a form of criminal punishment.
Sushruta’s manuscript also contained a description of the nasolabial flap. During the 1800s, pictures of nasolabial
flaps began to appear in print. Contemporary surgical descriptions began in 1830 when Dieffenbach used superiorly
based nasolabial flaps to reconstruct nasal alae. In 1864, Von Langenbeck used the nasolabial flap to reconstruct the
nose. Fifty-seven years later, Esser described the use of the inferiorly based nasolabial flap to close palatal fistulae.
Since these early publications, the nasolabial flap has been described for reconstruction of the floor of the mouth, lips,
tongue, buccal mucosa, upper and lower alveolus, maxilla, and oronasal defects.The anatomy of the nasolabial region
is complex. The nasolabial crease runs from approximately 1 cm superior to the lateral alar rim to approximately 1 cm
lateral to the corner of the mouth. Medial to the crease in the region of the corner of the mouth is theorbicularis oris
muscle. Superior and lateral to the crease is the cheek. The anatomy of the nasolabial crease is not completely
understood. Zufferey demonstrated that the zygomaticus major muscle had a group of superficial fibers that were
inserted into the dermis beneath the nasolabial fold; however, Yousif and coworkers did not detect a separate layer of
the zygomaticus major muscle. The buccal and zygomatic branches of the facial nerve primarily innervate the muscles
surrounding the nasolabial crease.
The nasolabial flap is typically classified as an axial pattern flap given that the angular artery runs deep to the flap.
Nevertheless, for applications such as the nose, the flap is thinned and does not contain the artery. The skin of the
nasolabial fold has a superior and inferior blood supply allowing for a superiorly or inferiorly.
Nasolabial is useful for reconstructing defects involving the oral cavity and those involving the lower third of the nose.
It can be used as an interpolation flap with either a single or staged technique. The flap is supplied by the angular
artery, intraorbital artery, and infratrochlear artery and can be based either superiorly or inferiorly. The area of
recruitment for nasal reconstruction is in closer proximity to the primary defect than is the forehead flap. A
disadvantage of the nasolabial flap is that there is a limited amount of tissue available, and asymmetry can occur along
the nasolabial flap folds. When the pedicle is divided, the defect can be closed primarily by placing the scar in the
nasofacial junction and nasolabial fold.
Technique
Requires development of finger shaped flaps in the redundant tissue of the nasolabial fold. In elderly patients with lax
sin a flap of 5cm width can be harvested with an acceptable result.
The flap is raised in the subcutaneous fat plane and then tunneled through an incision in the buccal mucosa. The blood
supply is derived from branches of the facial artery.
The donor site is closed primarily in a layered fashion. The pedicle of the flap requires division at 2-3 weeks following
the initial surgery to allow insetting of the flap and closure of th orocutaneous tunnel.

AT-T flap
Bilateral advancement for triangular defect can be use in defects in relation to hairline, brow and lip
For defect in the lip For defects in the forehead

CHEEK ADVANCEMENT FLAP
It is a type of advancement flap can be use d with Some rotation. It can be used medial cheek, nasofacial sulcus
defects. Its main advantage is that it prevents ectropion.
CERVICO FACIAL FLAP
The cervicofacial flap is a large rotation flap. The base of the flap is inferior and anterior. It has the potential to restore
extensive skin defects. The initial design, was published in 1976 by Juri and Juri. The pectoral extension advocated by
Becker and Shestak et al allows for a wider arc of rotation and a larger surface of tissue availability
Indications
Large defects of the cheek with or without involvement of the lip commissure, the lateral aspect of the nose, or the
lower eyelid may be best served by using this flap. The largest defect that can be corrected can be upto a diameter of
10 cm.
Cervicofacial flaps have been used to reconstruct tissue loss resulting from extensive traumatic injuries or from
resection of basal cell carcinomas of the skin
the blood supply to the flap is random, because it is elevated just below the subcutaneous layer. Owing to the random
nature, there is a risk for compromised viability of the distal aspect of the flap
Technique
The first consideration in flap design is the location, shape, and extension of the defect to be reconstructed. Horizontal
defects of the cheek (usually of traumatic etiology) can be addressed by subcutaneous dissection of the cervical skin
and consequent advancement of the resulting flap. Small anterior andposterior defects can be addressed by midline
forehead flaps or by local skin advancement or rotation flaps from the remaining facial skin or from the submental or
submandibular regions. The bilobed cervicofacial flap has the advantage of using the retroauricular and the
preauricular skin, with the ability to cover defects 3 to 4 cm in diameter.
For large defects of the cheek up to 10 cm in diameter, the flap is extended into the cervical and thoracic regions. The
incision follows the occipital hairline and should continue through a virtual line located about 2 cm posterior to the
anterior border of the trapezius muscle. After passing the acromioclavicular joint, the incision turns vertically along
the axillary fold and then follows the lateral border of the pectoralis major muscle


INTRA ORAL FLAPS

BUCCAL FAT PAD FLAP
The first reported utilization of the buccal fat pad as a pedicled flap was by Egyedi.
He reported on the successful closure of oral-antral and/oral-nasal communications following resection of three
carcinomas and one benign mixed tumor of the palate.
These early flaps were skin grafted. Prior use of the fat pad as a free graft had been reported by Neder.
The buccal fat pad lies within the masticatory spaces, and termed a syssarcosis, as it enhances the motion of the
muscles. It is in intimate contact with the facial nerve, parotid duct and the muscles of mastication.
In 12 cadaver dissections by stuzin et al the average volume of the buccal fat pad was 9.6ml (8.3 -11.9ml). The authors
reported maintenance of bulk of the buccal fat pad even in cachectic cadaver specimens. the buccal fat pad receives
arterial blood supply from branches of the facial, transverse facial and internal maxillary arteries
Technique
The buccal fat pad is identified in the vestibule. It is accessed through a mucosal incision in this area, or directly at the
margin of a surgical resection in the posterior maxilla. The flap is carefully mobilized by blunt dissection. It is
delivered in to the defect passively once adequate mobility is obtained. The fat pad is typically encased within a thin
fascial envelope which aids in this dissection. The fat is sutured in to position with absorbable sutures. The pad was
allowed to heal secondarily. Rapid mucosalization takes place within weeks. The donor site exhibits slight edema for
the first few weeks. No permanent facial paralysis is seen. Minor alteration in the facial motor activity immediately
following surgery because of the presence of edema. A defect of 4 cm can usually be covered adequately with the
buccal fat pad flap. Necrosis can also result from inappropriate tension on the flap if it is transferred too great distance.
The most common utilization in the reconstruction of the posterior maxilla and soft palate.

TONGUE FLAP
Tongue flaps are excellent flaps for intraoral reconstruction. They use adjacent tissue, have an excellent blood supply,
and are associated with minimal morbidity. The tongue has excellent axial and collateral circulation, with the lingual
artery providing the main blood supply. Up to one-half of the tongue can be rotated for tissue coverage without
compromising speech, mastication, or deglutition. A variety of flap designs have been described including anterior-
and posterior-based tongue flaps. Some indications include repair of oral defects and fistula closure.
First described for use in intraoral reconstruction of a soft palate defect (Kloop and Schurter 1956), Variants of flap
design for temporary or definitive coverage of small defects(Conley 1966), Correction of lip deformities (Guerrero-
Santos)and reconstruction for treatment of electrical burns(Ortiz-Monasterio) and Closure of palatal fistulas (Jackson
1972)
These flaps are helpful for providing closure of large oroantral fistulas. Reconstruction following resection of oral
structures, resurfacing of oral defects, for fistula closure, Floor of mouth, for buccal mucosa, for alveolar clefts for
soft and hard palate defects, for tonsillar arch defects, for tongue reconstruction and it can also used for tongue upper
and lower lip reconstruction.
Types
Dorsal tongue flap (Randomn)
o Anteriorly based
o Posterior based
Lateral tongue flap

Double door tongue flap
Median transit tongue flap
Technique
A finger-shaped flap is marked out on the lateral surface of the lateral tongue from the circumvallate papillae to 1-2
cm behind the tongue tip. The size of flap is determined by dimension of the defect. In general approximately one
third of the tongue can be used. Silk traction sutures placed to provide traction and the flap is raised with combination
of blunt and sharp dissection through the tongue muscle. Multiple small bleeders of the tongue can be controlled by
electrocautery. The width of the resultant flap can be increased by longitudinally scoring the muscle with the scalpel
blade allowing to ‘un-roll’. The donor site is closed in two layers.
Advantages
Use of adjacent tissue excellent blood supply with low morbidity, property reinnervation from the
adjacent host tissue. It can provide 90 to 100 cm of mucosal tissue for rotation can be used in patients
post radiotherapy.
Main disadvantage is small size and limited arc of rotation. Also In cases of patients with ‘field changes’ the surgeon
runs the risk of transf erring the tissue to the site of the ablative operation that as potential for malignant degeneration.
Palatal flap
The palatal (island and nonisland) flaps have many advantages, including the use of like tissue, the
creation of a sensate flap, and minimal donor site morbidity. The palatal island flap was described for
ablative defects of the palate and retromolar trigone by Gullane and Arena in 1977. Advancements in
technique subsequently reported by these surgeons allowed a mucoperiosteal flap of the hard palate
basedon a singular neurovascular supply.

Surgical anatomy
The palatal mucosa is underlined by submucosa that is adherent to periosteum. The periosteum is attached to
the bone of the hard palate by dense Sharpey’s fibers. Although split-thickness and subepithelial connective
tissue grafts are frequently used in periodontal and periendosseous implant surgery, their use in reconstructive
surgery is limited. Full-thickness mucoperiosteal palatal flaps are used for reconstruction.
Muscles of the soft palate include the palatopharyngeus, palatoglossus, levator palate, tensor palate, and
uvular. Of these, the tensor and levator insert into the palatal aponeurosis. Of surgical significance is the
passing of the tensor around the hamulus before insertion. Fracturing of the ipsilateral hamulus can increase
laxity of the flap.
The vascular supply to the palate is derived primarily from the greater palatine artery, which is derived from
the descending palatine artery, a branch of the third division of the internal maxillary. descending palatine
artery arises in the pterygopalatine fossa and courses inferiorly to the greater palatine foramen. On exit from
the foramen, the artery is denoted as the greater palatine artery and courses on the lateral aspect of the palate,
giving off small branches along the palate until its ultimate destination at the incisive canal. At the incisive
canal, an anastomosis exists with the sphenopalatine artery descending from the nasal cavity. Additional
vascular supply is available to the soft palate through the lesser palatine artery, which arises from the
descending palatine and courses through the lesser palatine foramen.
The palatal flap is an axial flap based on the greater palatine artery. The connection between the two greater
palatine arteries across the midline has been termed the macronetand allows the entire flap to be based on a
single greater palatine arterial supply. This anatomy greatly increases the versatility of the flap. Additionally,
the ability of the flap to rotate 180 degrees and to be placed in the oral cavity mucosal side up or down allows
nearly 360-degree availability along the entire pedicle.
The nerve supply to the palate closely follows the vascular supply. The pterygopalatine ganglion associated with
the maxillary nerve, V-2, gives branches to the greater, lesser, and nasopalatine nerves. A sensate flap is
possible owing to the major contribution of the greater palatine nerve to the palatal tissue used in the flap.
Two types of flaps
Posteriorly based –ashe’s flap Anteriorly based – dharwad flap

EXTRA ORAL FLAPS
(REGIONAL)

I. PECTORALIS MAJOR
The pectoralis major muscle has been applied to the reconstruction of a variety of chest wall defects since 1947 when
Pickerel et al. reported its use as a turnover flap. Sisson et al. used the pectoralis major as a medially based flap to
provide great vessel protection and obliteration of dead space following mediastinal dissection for recurrent cancer of
the laryngostoma after total laryngectomy. In 1977, Brown et al. described the technique of bilateral island pectoralis
major flaps for the reconstruction of a midline upper chest and lower neck defect. The muscle was completely isolated
on its neurovascular pedicle following transsection of its origins and insertions. A skin graft was used for epithelial
coverage after bilateral muscle advancement. In 1968, Hueston and McConchie reported a case in which the pectoralis
major was used as a carrier for the overlying skin in reconstruction of an upper sternal defect. The authors designed
this flap with a broad base at the shoulder, which limited its arc of rotation. In addition, they performed a delay
procedure to’ ensure the vascularity of the skin.
It was not until the latter part of the 1970s that Ariyan and Cuono and Ariyan recognized the tremendous potential of
the musculocutaneous unit based on the pectoralis major for the reconstruction of a large number of head and neck
defects.
This discovery was of paramount importance because it enabled the single stage transfer of large amounts of well-
vascularized skin for almost all ablative or traumatic defects of the upper aerodigestive tract, face, and skull base. In
addition, the hardiness of the vascular supply permitted the creation of two skin paddles by deepithelialization of an
intermediate segment of skin so that the inner and outer lining could be transferred with a single flap for
reconstruction of complex, composite defects.
The impact of this new reconstructive technique on head and neck surgery was recognized almost immediately. It
rapidly replaced many of the existing reconstructive methods, and large series of cases from a variety of different
medical centers were reported as testimony to the-reliability, versatility, and ease of harvesting this flap.
Although various modifications of the original description of this flap have been reported, along with recognition of
its shortcomings, it is still the mainstay of head and neck reconstruction.
The pectoralis major is a large fan-shaped muscle that covers much of the anterior thoracic wall. To a variable extent,
it overlies the pectoralis minor, subclavius, serratus anterior, and intercostal muscles. The origins of the pectoralis
major are divided into two or, sometimes, three portions. The cephalad segment arises from the medial third of the
clavicle. The central, or sternocostal, portion has a broad origin from the sternum and the cartilages of the first six ribs.
The third origin of this muscle, from the aponeurosis of the external oblique, is variable in size. The muscle fibers of
this broad muscle converge to form a tendon that passes deep to the deltoid and inserts into the crest of the greater
tubercle of the humerus. As it narrows in its course toward the humerus, it forms the anterior axillary fold. The medial

aspect of the deltoid muscle is almost inseparable from the muscle fibers of the pectoralis major. The cleavage
between these two muscles is referred to as the deltopectoral groove, through which runs the cephalic vein, which is a
constant anatomic landmark.
The pectoralis major is surrounded by a layer of deep fascia. However, this is separate from the clavipectoral fascia
that surrounds the pectoralis minor and extends cephalad from that muscle to the clavicle. Prior to attaching to the
undersurface of the clavicle, this fascia splits to envelop the subclavius muscle. Both the vascular and nerve supply to
the pectoralis major pass through the clavipectoral fascia en route to the deep surface of the muscle.
The action of the pectoralis major is to adduct and medially rotate the arm. It becomes active in internal rotation of the
arm only when working against resistance. The upper muscle fibers help to flex the arm to the horizontal level; the
lower fibers assist in arm extension. Contraction of the pectoralis major helps to extend the arm to the individual's
side, but it plays no role in hyperextension beyond that point.
The loss of the dynamic activity of the pectoralis major appears to be well tolerated, although the true impact on
brachial function has not been studied extensively in any of the large series of pectoralis major musculocutaneous flap
transfers. The additional morbidity of combining the loss of pectoralis major function and a radical neck dissection has
also not been investigated in a systematic fashion. Much of the adductor activity is compensated for by the powerful,
latissimus dorsi muscle, which makes up the posterior axillary fold.
FLAP DESIGN AND UTILIZATION
The major advantages of the pectoralis major musculocutaneous flap that distinguished it from the three major
cutaneous flaps (deltopectoral, nape of neck, and forehead) that were in use at the time are the following:
1. Rich vascularity.
2. Large skin territory.
3. Ability to transfer without prior delay.
4. Improved arc of rotation.
5. Increased bulk.
6. Primary donor site closure.
7. Well-vascularized tissue coverage of the carotid artery in the event of a salivary fistula or cervical skin necrosis.
8. Ease of harvest in the supine position.
9. Ability to transfer two epithelial surfaces for inner and outer lining.

The pectoralis major is described as having three different heads of origin: clavicular, sternal-manubrial, and
external oblique. The clavicular portion is distinct from the central and inferior portions of the muscle, both in
function and in its neurovascular supply. The central portion of the muscle originates from the manubrium, the
sternum, and the cartilages of the first six ribs. The pectoralis major both adducts and medially rotates the arm.
The relationship of the cephalad portion of the rectus abdominis muscle to the caudal part of the pectoralis major
should be noted.
The total skin territory of the pectoralis major is often greater than 400 cm2. However, it is rare for the entire skin
territory to be required to satisfy the demands of the ablative defect. With extensive use of this flap, its limitations
have been identified, and modifications have been described to help overcome them. The major modifications are
discussed according to these problem categories.
Methods to Improve the Arc of Rotation
Early in the history of this flap, it was recognized that a distal skin paddle placed over the caudal extent of the muscle
was not only well vascularized but it also permitted a greater arc of rotation. Ariyan's original description of this flap
incorporated a long segment of skin that extended from the clavicle to the caudal extent of the muscle. The skin
component was oriented over the course of the pectoral branch of the thoracoacromial artery. The excess skin
resulting from this flap design often required secondary trimming. An additional benefit to placing the skin paddle
over the lower portion of the muscle was that it permitted the deltopectoral flap to be preserved for simultaneous or
later use. Magee et al. described the placement of the skin paddle over the lower portion of the pectoralis major, with
an extension overlying the rectus abdominis muscle. Not only did this skin placement lead to less disfigurement of the
breast in female patients, but as noted earlier, it also provided a mechanism to achieve a greater arc of rotation of this
flap to more cephalad defect.
Magee et al. described an array of vessels on the surface of the rectus sheath that necessitated the incorporation of this
fascia to ensure the blood supply to the overlying skin. Although it is widely recognized that a portion of "random
skin" can be harvested, it is also recognized that it may be unreliable. The foundation for the claim of Magee et al.,
that a segment of skin could be harvested entirely distal to the pectoralis, is tenuous. The general belief is that a
significant portion of the skin paddle must overlie the pectoralis major to capture a sufficient number of
musculocutaneous perforators.

A skin paddle has been designed over the caudal aspect of the pectoralis major and the cephalad portion of the
rectus abdominis; A portion of the anterior rectus sheath that is beneath the skin flap is incorporated to enhance
the skin's vascularity. A sufficient portion of the skin flap should overlie the pectoralis to ensure capture of the
musculocutaneous perforators.
Additional measures that have been used to enhance the arc of rotation are related to the method of transfer of the
muscular component of the flap. In the vast majority of cases, muscle is transposed over the clavicle and tunneled
deep to the cervical skin. This is helpful to provide coverage of the carotid artery and to augment the soft tissue deficit
following radical neck dissection. When a radical neck dissection is not performed, the bulk of the muscle may be
problematic, requiring the use of a skin graft to achieve coverage. In Ariyan's early description, the muscle was
completely exteriorized and later removed after neovascularization had occurred. Fabian and later Lee and Lore
proposed the removal of a segment of the clavicle to gain up to 3 cm of length. As a further modification of this
approach, Wilson et al. reported tunneling the muscle pedicle deep to the clavicle in a subperiosteal plane. They
warned of the potential risk related to vascular compression. De Azevedo described a similar modification by passing
the flap through a subclavicular tunnel. In addition, he reported the preservation of the clavicular portion of the muscle
by harvesting only a distal island of muscle beneath the desired skin paddle. The neurovascular supply to the proximal
muscle was preserved with this technique, which reportedly led to improved brachial function. In particular, he noted
that patients were able to move their arms forward and downward against resistance.
A parasternal skin paddle may be designed that crosses the opposite side of the sternum

Methods to Deal with Excessive Bulk
The body habitus of most patients with head and neck cancer rarely leads to concern about excessive bulk in a flap.
However, this may be a problem in certain patients, especially when tubing of the skin is required to reconstruct the
pharyngoesophagus, or the introduction of excess tissue in the oral cavity results in interference with normal lingual
function. To reduce the bulk of the skin and subcutaneous tissue, Sharzer et al. described harvesting a vertically
oriented "parasternal” skin paddle that extended across the sternum to the opposite internal mammary perforators.
Although the skin paddle had a substantial portion overlying the muscle, the component overlying the sternum
achieved a considerable reduction in bulk.
Alternative solutions to the problem of excessive flap bulk were achieved by eliminating the skin paddle entirely.
Murakami et al. described a two-stage procedure in which a split-thickness skin graft was placed over the muscle and
then followed 3 to 4 weeks later by the harvest of the muscle-skin graft unit. They used this thinner flap for the
reconstruction of the hypopharynx in four women in whom flap thickness was particularly problematic. This concept
was extended by Robertson and Robinson who reported the use of a quilted skin graft over the pectoralis major in a
one-stage reconstruction of the pharyngoesophagus.
Small mucosal defects pose the additional problem of requiring only small segments of skin for reconstruction. By
reducing the size of the skin paddle, there is a greater risk of missing a sufficient number of musculocutaneous
perforators to achieve adequate flap vascularity. To prevent the necessity of including a larger skin paddle than
needed, Johnson and Langdon reported their experience with seven patients whose oral defects were reconstructed
with the pectoralis major alone. Reepithelialization of the muscle was found to be rapid and produced a satisfactory
long-term result.
Methods to Achieve Two Epithelial Surfaces for Reconstruction of Compound Defects
“Gemini” flaps
The reconstruction of compound defects involving the mucosa and overlying skin can be challenging. Early in the
development of the pectoralis major flap, it was recognized that the rich vascularity of the skin permitted the design of
two epithelial surfaces by removing the intervening bridge of skin. This design placed an added requirement that the
flap be of sufficient length to allow it to be folded upon itself. This also produced additional bulk, which was either
advantageous or disadvantageous, depending on the location of the defect. Weaver et al. described a bilobular
"Gemini" flap in which two separate skin paddles were harvested side by side to achieve opposing epithelial surfaces.
These authors split the intervening skin and underlying muscle to achieve more complete separation between the two
skin paddles. Tobin et al. extended this concept one step further by raising two separate musculocutaneous units from

the same pectoralis major, i.e., one based on the lateral thoracic artery and the second based on the pectoral branch of
the acromiothoracic artery.
Methods to Include Vascularized Bone in the Musculocutaneous Flap
The incorporation of vascularized bone with the pectoralis major musculocutaneous flap expanded the use of this
technique to the reconstruction of composite defects of the head and neck. Experimental work in the early 1970s
demonstrated the advantage of using vascularized bone in a contaminated and irradiated field. Cuono and Ariyan were
the first to report the use of the pectoralis osteomusculocutaneous flap for oromandibular reconstruction. They
demonstrated the viability of the transferred fifth rib through fluorescence microscopy. Pulse labeling with different
color markers showed the deposition of new osteoid and, hence, indicated active metabolism. However, the tenuous
nature of the blood supply was reflected by additional investigators who used this composite flap and reported failure
rates of 21%, 28%, and 75%. Additional complications associated with rib harvest included Pneumothorax and pleural
effusion.
An alternative source of vascularized bone for transfer with the pectoralis major is the sternum. Green et al. described
the transfer of the outer cortex of the sternum with a parasternal skin paddle. The harvest of this composite flap was
associated with fewer pulmonary complications than was the rib, but this technique has not been embraced with much
enthusiasm.
Additional Flap Modifications to Manage the Muscular Pedicle in the Neck
In most cases, the pectoralis major muscle provides coverage to the carotid artery and augments the radical neck
dissection contour deformity. Depending on the muscular development of the individual patient, there may be a
significant bulge as the muscle passes over the clavicle. Transection of the medial and lateral pectoral nerves helps to
promote muscle atrophy. In patients who have not undergone prior radical neck dissection or in those patients with
heavily irradiated cervical skin, it may be difficult to achieve primary closure of the skin of the neck over the muscle.
In these cases, the cervical skin may be split and a skin graft placed over the exposed muscle. Alternatively, the
muscle can be completely exteriorized and then resected after a 2- to 3-week period to allow neovascularization of the
skin paddle. As noted previously, exteriorization of the muscle can provide additional length to the vascular pedicle.
Wei et al. described an alternative solution by harvesting a skin paddle over the sternocostal portion of the muscle.
The blood supply to that portion of the muscle was isolated from the vascular supply to the clavicular portion of the
muscle. These authors noted that the blood supply to the clavicular portion was derived from the acromial, deltoid, and
clavicular branches of the acromiothoracic pedicle; the pectoral branch supplies the sternocostal segment. Hence, the
sternocostal portion of the muscle could be isolated, and either it could be tunneled under the clavicular portion, or the
latter could be divided. In so doing, the bulk of tissue crossing the clavicle is greatly diminished to only that tissue
surrounding the vascular pedicle.
The ultimate solution to the problem of muscle bulk and limited reach was proposed by Reid et al. (45) who used
microvascular surgery to transfer a composite flap based on the clavicular head of the pectoralis major with a skin
island and a segment of the medial clavicle. They reported the successful use of this free flap in four patients with oral
cancer and one patient with a post-traumatic defect in the tibia. The thinness and mobility of the skin overlying the
clavicle was particularly advantageous for intraoral restoration. In addition, the authors discussed the potential for a
sensate flap through harvest of the supraclavicular sensory nerves.
FLAP DESIGN AND UTILIZATION
The enthusiasm surrounding the introduction of the pectoralis major musculocutaneous flap led to its application to
most of the major reconstructive challenges that had not been adequately solved by the available techniques. The early
experience with this flap included the reconstruction of mucosal defects of the oral cavity and pharynx and cutaneous
defects of the neck. Ariyan and Cuono and Ariyan reported the successful application of this flap to the reconstruction
of skull base defects following temporal bone resection and orbit maxillary resection. Full thickness defects of the

pharynx and cheek were easily reconstructed by any of the techniques described previously that achieve two epithelial
surfaces, including the use of the ipsilateral deltopectoral flap. In 1970, Snyder et al. described a number of techniques
to transfer vascularized bone to the head and neck using regional cutaneous flaps. The use of vascularized bone for
primary reconstruction of the mandible led to a flurry of activity, using the composite osteomusculocutaneous
pectoralis major flap. However, advances in microvascular surgery that occurred in the latter part of the 1970s and
early 1980s demonstrated that vascularized bone could be transferred from a number of distant sites to achieve a more
reliable and accurate restoration of mandibular continuity.
NEUROVASCULAR ANATOMY
The primary vascular supply to the pectoralis major muscle arises from the thoracoacromial artery, which is a
branch of the second part of the axillary artery. The lateral thoracic artery also supplies some degree of vascularity
to the pectoralis muscles, the extent of which is controversial. The lateral thoracic artery is variable in size and its
contribution may be completely replaced by the lateral intercostal perforators. The medial and lateral pectoral
nerves supply motor innervation to different regions of the muscle. The clavicular head is primarily supplied by the
lateral nerve; the sternocostal head is supplied by the medial nerve.
According to the classification scheme of Mathes and Nahai, the pectoralis major is a type V muscle with one major
vascular pedicle from the thoracoacromial artery and secondary segmental parasternal perforators that arise medially

from the internal mammary artery. The thoracoacromial artery is a branch from the second part of the axillary artery.
It commonly divides into four major branches: deltoid, acromial, clavicular, and pectoral. It is the latter branch, which
descends medial to the tendon of the pectoralis minor that supplies the pectoralis major.
The lateral thoracic artery is not commonly believed to contribute significantly to the vascularity of the pectoralis
major. However, Freeman et al. reported information to the contrary. In a cadaver study in which they examined the
vascular supply to the pectoralis major, they found that the lateral thoracic artery was present in all 17 specimens that
were examined. It arose from the axillary artery and pierced the clavipectoral fascia lateral to
The thoracoacromial axis classically divides into four main branches: the clavicular deltoid pectoral, and acromial
arteries. The lateral thoracic artery may also arise from this system but/more commonly, branches out separately
from the axillary artery. The thoracoacromial artery commonly divides into two major branches: the pectoral and
deltoid. The acromial and clavicular arteries variably arise from either division. The deltoid artery runs in the
deltopectoral groove with the cephalic vein, supplying both the pectoralis major and deltoid. It gives off a cutaneous
perforator in the midportion of the deltopectoral groove. The acromial branch contributes to a vascular plexus
along with branches from the deltoid, suprascapular, and posterior humeral circumflex vessels. The clavicular
branch runs a cephalad and medial course toward the sternoclavicular joint. The pectoral branch pierces the
clavipectoral fascia and then runs a cephalocaudal course on the deep surface of the pectoralis major, which it
supplies.
the tendon of pectoralis minor. In its course within the muscular fascia, it provided a significant vascular contribution
to the pectoralis major and the major cutaneous supply to the female breast. Through the injection of contrast material,
followed by xeroradiography, the authors found that the pectoral branch of the thoracoacromial artery supplied the
clavicular and upper sternal portion of the muscle; the lateral thoracic artery perfused the inferior and medial portions.
In their investigation of 10 aortic arch arteriograms and detailed dissections of 35 pectoralis major muscles, Moloy
and Gonzales corroborated these findings. These authors reported that, in all cases, the diameter of the lateral thoracic
artery was equal to or greater than the diameter of the pectoral branch of the thoracoacromial artery. Manktelow et al.
reported that a branch of the lateral thoracic artery, approximately 1 mm in diameter, entered the inferior one fifth of
the muscle in more than 70% of their dissections. Although the lateral thoracic artery is sacrificed by most surgeons to
improve the arc of rotation of the pectoralis major musculocutaneous flap, these anatomic studies suggest that it may
provide an important contribution to the vascular supply of this flap.
Reid and Taylor performed the most extensive study of the vascular supply of the pectoralis major that has been
reported in the literature. Their study included 50 dissections in fixed cadavers and 50 dissections in fresh cadavers. In
the latter group, injections of the arterial tree included both ink and barium contrast medium. Although their study

focused on the acromiothoracic axis, they reported no significant contribution from the lateral thoracic artery. They
found that the pectoralis major had a regional distribution of its blood supply, with the pectoral artery supplying the
sternocostal portion and the deltoid artery supplying the clavicular head. They reported only one instance of a very
small pectoral branch and none of complete absence of this branch. Ink-injection studies of the pectoral artery
revealed staining of the skin overlying the lateral and the sternocostal portion of the muscle. The clavicular head of the
muscle was not stained until the deltoid branch of the acromiothoracic axis was injected. The deltoid muscle and its
overlying skin were also stained by ink injection of the deltoid branch. There were two other interesting observations
in this study. The first was that a significant zone in the medial aspect of the pectoralis major was not stained with
injections of either the pectoral or deltoid branches. This zone was thought to be the primary territory of the internal
mammary perforators. The second observation was that the major vessels supplying the skin in the territory of the
pectoralis major were actually fasciocutaneous perforators that ran a course around the free lower and lateral border of
the muscle. These fasciocutaneous vessels were considerably larger than the musculocutaneous perforators exiting
from the muscle.
The superior thoracic artery provides a small vascular supply to the pectoralis major. The parasternal internal
mammary perforators perfuse the medial aspect of the muscle, which allows it to be used as a turnover flap for
reconstruction of midline chest wall defects.
The pectoral branch of the thoracoacromial artery and the lateral thoracic artery penetrate the clavipectoral fascia
along with the medial and lateral pectoral nerves. The two arteries are both accompanied by their venae comitantes.
After penetrating the clavipectoral fascia, they run in a cephalocaudal direction before entering the pectoralis major;
either the pectoral branch of the thoracoacromial artery or the lateral thoracic artery supplies branches to the pectoralis
minor near the clavicle. This explains the avascular plane of dissection between the pectoralis major and minor. The
deltoid branch of the thoracoacromial artery accompanies the cephalic vein in the deltopectoral groove. Either the
acromial or the deltoid branch gives off a direct cutaneous vessel at the most cephalad extent of the deltopectoral
groove. In addition, the deltoid artery commonly gives off a cutaneous perforator in the midportion of the groove.
The application of the angiosome concept to the blood supply of the anterior chest wall helps to explain the behavior
of the pectoralis major musculocutaneous flap. Taylor and Palmer defined an angiosome as a segment of tissue
supplied by a single source artery and vein. A system of "choke" arteries was described that connect adjacent
angiosomes. Based on clinical observations and injection studies, it appears that an adjacent angiosome can be reliably
"captured" after interrupting its source artery. However, when the area of tissue that is to be harvested is extended to
the subsequent angiosome, or the "angiosome once removed," then necrosis becomes more likely. Taylor and Palmer
surmised that this phenomenon was caused by the pressure gradient across the choke vessels that connect angiosomes.
The more angiosomes that are harvested in series, the greater the reduction in pressure is.
The pectoralis major and its overlying skin can be divided into vascular territories or angiosomes. There appears to be
some controversy as to whether the lateral portion of the muscle is supplied by the pectoral branch or by the lateral
thoracic artery.
It seems clear, however, that the medial portion of the muscle is supplied by the internal mammary perforators. The
skin overlying the rectus sheath is part of the angiosome of the superior epigastric artery and vein. It is no surprise;
therefore, that capture of this skin in the upper abdomen (based on the pectoral branch) is tenuous because it is part of
an angiosome that is once removed from the primary angiosome. This hypothesis maintains that the reduction of the
pressure gradient from the pectoral artery, as it traverses the system of choke vessels that surround the internal
mammary territory, leads to a tenuous blood supply in the skin overlying the upper abdomen. This was evident by the
poor staining of skin in this region following ink injections of the pectoral artery. Reid and Taylor noted the staining
of a network of vessels on the surface of the rectus sheath, which gives credence to the suggestion that this layer
should be harvested along with skin extensions distal to the territory of the pectoralis. These authors also advised great
caution in the technique utilized when interrupting the internal mammary perforators on the undersurface of the
muscle. They warned that the internal mammary branches should be either ligated or con trolled with bipolar cautery.
Excessive use of unipolar cautery may lead to ascending trauma of the vessels in the internal mammary angiosome,
which would further jeopardize the flow across this angiosome to the distal skin.

The nerve supply to the pectoralis major is from the lateral (C-5 to C-7) and medial (C-8 to T-1) pectoral nerves.
Manktelow et al. identified multiple nerves entering different parts of the pectoralis major, which numbered from four
to ten individual nerves entering the stemocostal portion of the muscle alone. This muscle has been transferred as a
dynamic free flap through anastomosis of these motor nerves to recipient motor nerves.
ANATOMIC VARIATIONS
Congenital absence of the pectoralis major is rare. In a clinic population, this anomaly was observed with a frequency
of approximately 1:11,000. Congenital absence of the stemocostal head of the pectoralis major was first reported by
Alfred Poland in 1841. This anomaly was described in conjunction with ipsilateral syndactyly, and this combination
bears the name Poland's syndrome or Poland's anomaly. It is reported to occur with an incidence of 1:25,000. The
potential causes for this condition include abortion attempts and leukemia.
The variability in the vascular supply to the pectoralis major was studied by Moloy and Gonzales (38). They evaluated
10 aortic arch arteriograms and 35 fresh cadaver dissections. The study revealed that the lateral thoracic artery was
equal to or larger in diameter to the pectoral branch of the thoracoacromial artery in 90% of cases. They found
extensive collateral flow between these two vessels in all cases. There was only one instance of a non visualized
thoracoacromial system in a patient with extensive atherosclerosis in the subclavian artery.
POTENTIAL PITFALLS
The overall reliability of the pectoralis major musculocutaneous flap is attested to by the low incidence of complete
flap failure. In several large series, the incidence of total flap necrosis was reported to be 1.0%, 1.5%, 3%, and 7%.
This low incidence of total flap necrosis is a reflection of the constancy of the anatomy and the ease of flap harvest.
Partial flap necrosis, however, has been reported at a much greater rate. Schusterman et al. noted a 14% incidence of
flap loss involving greater than 50% of the skin surface area. Other large series have reported partial necrosis rates in
the range of 4% and 7%. Partial necrosis rates were probably a function of how far caudal the skin flap was harvested.
Shah et al. reviewed their complications in 211 pectoralis major flaps during a 10-year period. Although figure
according to the number of skin paddles that were "placed" at the risk of partial necrosis by virtue of their caudal
extension over the rectus sheath. The authors identified a number of patient-related factors that were statistically
significant in their series for the development of flap necrosis as follows: age older than 70 years, female sex,
overweight, albumin level less than 4 g/dl, and oral cavity defects, in particular, subtotal or total glossectomy. In
addition, a variety of systemic diseases were also associated with an increased risk of necrosis. Although many of the
complications in this series did not require additional surgical procedures, they did lead to prolonged hospitalization.
The potential pitfalls in harvesting the pectoralis major musculocutaneous flap begin with flap selection. The use of
this donor site to resurface defects that extend more cephalad on the face or scalp calls for skin paddles designed over
the more caudal aspects of the chest wall and upper abdomen. As noted previously, this may result in high rates of
partial flap failure. Excessive bulk may be problematic, not only from a functional point of view, but also in terms of
wound healing. In wounds that are likely to pose problems with healing as a result of prior radiation and/or poor
nutrition, the effect of gravity can be extremely detrimental and may require the selection of an alternative
nondependent donor site.
Pedicle compression may result from external causes, such as tracheostomy tapes or circumferential dressings. The
creation of an inadequate tunnel for the pedicle may also cause vascular compromise. Shearing of the skin paddle and
the muscle may disrupt the musculocutaneous perforators, leading to partial or complete necrosis.
Donor site problems are rare. Hematomas usually occur because of a failure to control bleeding adequately following
transsection of the humeral head of the muscle.
The use of a large skin paddle may lead to excess wound tension in donor site closure. Necrosis of the skin of the
chest wall may result. In theory, excess tension in closure may also lead to restrictive pulmonary disease, although this

is rare. The incidence of radiologically evident and clinically significant pulmonary atelectasis was investigated by
Schuller et al who selected two groups of patients with head and neck cancer who underwent ablative surgery for their
disease. One group underwent re- construction with a pectoralis major flap, and the other did not. Both groups were
subdivided into patients with and without pre-existing pulmonary disease. In addition, the patients who underwent
pectoralis flap reconstruction were divided, based on whether the cutaneous paddle was greater than or less than 40
cm2. Although there was a fairly high rate of radiographic atelectasis in all patient groups, the incidence of clinically
significant pulmonary complications was low. The group of patients with pre-existing pulmonary disease and flaps
greater than 40 cm2 had the highest incidence of both major radiographic signs of atelectasis and clinical pulmonary
symptoms. However, no statistical analysis was reported in this study. It should be noted that the development of
postoperative pulmonary complications is probably multifactorial, with the preoperative nutritional status being a
potentially important factor not considered in this study. When bilateral pectoralis major flaps are harvested, it is not
uncommon that closure of the second side may require a skin graft. Exposure of the costochondral cartilage may lead
to serious infections, including chondritis.
In women, distortion of the breast following donor site closure may be minimized with an inflamammary skin
paddle.
The use of this donor site in male patients may lead to problems with excessive hair growth in the oral cavity or
pharynx. When radiation is given postoperatively, this problem is usually remedied. Finally, Schuller raised concern
about the ability to detect recurrences in the neck in a timely fashion because of the bulk of the muscle pedicle. He
also pointed out the significant morbidity to the shoulder when the pectoralis major is utilized on the side of a
denervated trapezius. As noted previously, this parameter has not been adequately studied.
POSTOPERATIVE CARE
The use of a suction drainage system in the chest wall donor site is imperative to help avoid the formation of a
seroma. Passive and active range of motion and strengthening exercises for the shoulder are instituted within a few
days after surgery.

II. TRAPEZIUS FLAP
There are three distinct musculocutaneous flaps that can be harvested from the trapezius muscle, making it unique
among the regional muscle flaps that are used in head and neck reconstruction. Conley, in 1972, is credited with being
the first to report the use of the trapezius muscle as a carrier for skin. The skin design of this flap was similar to the
one that was reported by Mutter in 1842. Mutter used this cutaneous flap, which was based at the midline of the upper
back and extended onto the shoulder, to release burn contractures of the neck. In 1957, Zovickian reported using a
"mastoid-occiput-based shoulder flap" to close pharyngeal fistulas. He staged these cutaneous flaps by putting a skin
graft on the undersurface for lining, and a skin graft on the recipient bed to close the donor defect. The flap was staged
one more time prior to transfer. Conley reported using the same skin design but incorporated the trapezius muscle in a
nondelayed flap. In addition, he reported that the trapezius muscle could be used as a vehicle to transfer a segment of
vascularized clavicle to the maxillofacial skeleton. Ariyan and McCraw and Dibbell popularized the flap design that
we now refer to as the superior trapezius flap, which is an extension of Conley's original work. The superior trapezius
flap, based on the paraspinous perforators, is a highly reliable flap, although limited in its utility because of its short
arc of rotation.
In 1978, Demergasso reported a bipedicle trapezius flap based on both the paraspinous perforators and the transverse
cervical artery (TCA) and vein (TCV). In the subsequent year, at the international meeting of the American Academy
of Facial Plastic and Reconstructive Surgery, both Demergasso and Panje introduced the unipedicle lateral island
trapezius flap, based solely on the TCA and TCV. This musculocutaneous flap was useful but limited because of its
short arc of rotation and variable vascular anatomy, which precludes the transfer of this flap in a significant percentage
of patients.
The third musculocutaneous flap, the lower trapezius island musculocutaneous flap (LTIMF), was introduced by Baek
et al. in 1980. The transfer of a skin island overlying the lower portion of the muscle provides an increased arc of
rotation, which is independent of the variable vascular anatomy of the TCA and TCV in the posterior triangle of the
neck. However, the need to place the patient in the lateral decubitus position for harvest has limited the widespread
use of the LTIMF.
MUSCLE ANATOMY
The trapezius muscle is a broad thin triangular muscle that covers much of the upper back and posterior neck. Its
major action is to raise the lateral angle of the scapula, which is important for adduction of the arm. It is helpful to
divide this muscle into three functional and anatomic units. The cephalad unit arises from the superior nuchal line,
external occipital protuberance, and ligamentum nuchae. The upper fibers insert into the lateral third of the clavicle,
defining the lateral boundary of the posterior triangle of the neck. The function of the upper trapezius fibers is to
elevate the tip of the shoulder.

The middle portion of the trapezius muscle takes its origin from the seventh cervical and the upper six thoracic
vertebrae. These muscle fibers have a transverse orientation and insert into the acromion and the upper border of the
scapular spine. The major activity of the midportion of the muscle is retraction of the shoulder.
The caudal fibers of the trapezius muscle originate from the lower six thoracic vertebrae and course in an oblique
cephalad direction to insert into the medial aspect of the scapular spine. This portion of the trapezius muscle overlaps
the upper medial border of the latissimus dorsi muscle. The caudal portion of the trapezius assists in the functional
activity of the upper portion by its downward pull on the root of the scapular spine, which helps in the rotation of the
scapula.
NEOROVASCULAR ANATOMY
The blood supply to the trapezius muscle is probably the most confusing of any of the regional flaps. Mathes and
Nahai classified the vascular pattern to the trapezius as a type II muscle with a dominant TCA and TCV and with
minor pedicles from the occipital artery and vein and the perforating posterior intercostal vessels of the cervical and
thoracic regions. However, this classification does not recognize the contributions to the distal muscle from the dorsal
scapular artery (DSA). Even though the DSA and the TCA commonly arise from the same parent vessel, they usually
enter the muscle at separate locations; their separate contributions to different regions of the muscle have been
described. In reporting the "potential pitfalls" of the trapezius musculocutaneous flap, Nichter et al. described a case in
which an "accessory vessel," arising at the level of the scapular spine, was ligated to achieve greater mobilization of
the muscle. However, the distal portion of the muscle and overlying skin showed signs of ischemia and became
necrotic soon after interruption of this blood supply, despite the fact that the TCA and TCV were intact. In an effort to
clarify this situation, it is easiest to begin by providing the classic description of the anatomy of these vessels before
diverging into the numerous variations.
As classically described, the TCA arises from the thyrocervical trunk and courses along the posterior triangle of the
neck toward the trapezius muscle. The TCA divides into a superficial branch, which passes over the levator scapulae
to run on the undersurface of the trapezius muscle, and a deep branch, which passes under the levator scapulae,
descending along the medial aspect of the scapula, deep to the rhomboid muscles. The superficial branch of the TCA
divides into descending and ascending branches. The former runs a caudal course on the undersurface of the muscle,
and the latter runs a more cephalad course, supplying the upper portions of the trapezius along with the occipital
artery. The deep branch of the TCA, portions of the trapezius along with the occipital artery. The deep branch of the
TCA, which we will refer to as the DSA, sends a significant branch to the caudal aspect of the trapezius muscle, which
emerges between the rhomboid major and minor and less commonly between rhomboid minor and levator scapulae.
Variations in the origin of the TCA and the DSA are the rule, rather than the exception. Both branches may arise
independently from the second or third part of the subclavian artery The importance of this variation is that the vessels
may then run a circuitous course, intertwined in the brachial plexus, before passing out of the posterior triangle either
over (TCA) or under (DSA) the levator scapulae. This variation has no bearing on the superior trapezius flap or the
LTIMF. However, the utility of the lateral island flap depends greatly on the complete mobilization of the TCA and
TCV, which is impossible when the artery courses through the brachial plexus.
Netterville and Wood studied the relationship between the TCA and DSA in supplying the trapezius muscle. They
found that, in most cases, there was a reciprocal relationship between these two vessels, with either one or the other
being dominant. In 50% of their dissections, the DSA was dominant, and the TCA was a branch of the DSA. In 30%
of the dissections, the TCA was dominant, and the DSA was a branch of the TCA. In the remaining 20% of cases, the
DSA and TCA appeared to be of equal dominance and size and had a separate takeoff from the subclavian artery. In
addition, ink-injection studies of the TCA and the DSA revealed that the former supplied the skin overlying the
trapezius above the rhomboid minor and the latter supplied the skin below the rhomboid minor. These findings
conflict with the results of selective intra-arterial injections of prostaglandin E1 by Maruyama et al. Following
selective catheterization of the transverse cervical artery, the authors reported that injection of prostaglandin E1 led to
flushing of the skin over the entire territory of the trapezius muscle. These findings can be explained by assuming that
the DSA was a branch of the TCA, and therefore, both the, proximal and distal blood supplies were probably injected
in Maruyama's study.

The trapezius is a broad thin muscle that arises from the superior nuchal line, the external occipital protuberance,
the ligamentum nuchae and the spinous process of the vertebrae of C-7 through T-12. The insertions of the
trapezius muscle are to the lateral third of the clavicle, the medial border of the acromion and the entire length of
the scapular spine. There is some variability in the cephalad and caudal extent of the origin of the trapezius
muscle, with the upper part failing to reach the skull and the lower part arising from the vertebrae from T-8 to L-2
The muscles lying deep to the trapezius include the (levator scapulae, rhomboid minor and rhomboid major. In its
lateral extent, the trapezius also overlaps the supraspinatus and infraspinatus. The upper portion of the trapezius
muscle is supplied by the TCA which exits the posterior triangle superficial to the levator scapulae The DSA
supplies the caudal portion of the trapezius muscle. It emerges between the rhomboid major and minor muscle or
less commonly between rhomboid minor and levator scapulae (dotted lines). Additional arterial supply to the
trapezius muscle is derived from occipital artery and the intercostal perforating arteries, which emerge in the
paraspinous region.
The venous anatomy is equally variable. Goodwin and Rosenberg identified three major patterns of TCV anatomy. In
the majority of cases, the TCV is a single vessel, but it may be a dual system. The TCV exits the trapezius muscle on
its deep surface, close to the point of entry of the TCA, which is 2 to 5 cm above the clavicle. Although the TCA
always runs deep to the omohyoid muscle, the TCV may be superficial in 25% of cases. In 60% of cases, the authors
found that the TCV traveled with the TCA; in 15%, it followed a course under or through the brachial plexus. In the

remaining 25%, the TCV ran a more caudal course beneath the clavicle, terminating in the subclavian vein. In the
majority of cases the TCV enters the medial subclavian vein. It can enter the lower portion of the external jugular vein
in one third of cases.
The accessory nerve, cranial nerve XI, provides motor innervation to the trapezius muscle after supplying
innervation to the sternocleidomastoid muscle. There are contributions to the nerve supply of the trapezius from C-2
through C-4, but the exact nature of this additional innervation is uncertain.
The anatomy of the TCA and the DSA in the posterior triangle is highly variable. A: The TCA is classically
described as arising from the thyrocervical trunk and running across the posterior triangle of the neck. It divides
into a superficial branch, which crosses over the levator scapulae, and a deep branch, which runs deep to the
levator scapulae. The superficial branch divides into an ascending branch and a descending branch, which supply
the upper and lower portions of the trapezius muscle, respectively. The deep branch of the TCA runs deep to levator
scapulae and then gives rise to a superficial branch that arises between either the levator scapulae and rhomboid
minor or, more commonly, between the rhomboid major and minor, supplying the distal portion of the trapezius
muscle. B: A common anatomic variation is shown in which the DSA arises separately from the second or third
part of the subclavian artery. The TCA may also arise directly from the subclavian artery. C: In some cases, the
DSA and the TCA may run a course below or intertwined in the brachial plexus. This variation is most important
to identify when harvesting a lateral island trapezius flap in which mobilization of the TCA is critical to achieving
an adequate arc of rotation.
SUPERIOR TRAPEZIUS FLAP
The superior trapezius flap is an extremely reliable source of coverage for defects of the posterolateral portion of the
neck that extend no further medially than the midline. In our review of the literature on this flap, we found no
instances of total flap failure. We have found it extremely reliable, with no instances of either partial or total necrosis
in more than 30 cases.

This flap is usually transferred as a peninsula of skin and muscle, which is based at the midline of the back.
However, an island of skin, overlying the lateral aspect of the muscle, may also be transferred. The primary blood
supply to this flap is derived from the paraspinous perforators, with some contribution from the occipital artery. This
flap is unique among the trapezius flaps in that its blood supply is unaffected by a prior radical neck dissection with
transsection of the transverse cervical vessels. In fact, the vascularity of the distal portion of this flap may be enhanced
through a delay phenomenon when the transverse cervical vessels have been previously interrupted.
The rationale for this hypothesis is based on the angiosome concept. Taylor et al. proposed that the delay
phenomenon is caused by the opening up of choke vessels between angiosomes located in series as a result of
interrupting the source artery in an adjacent angiosome. Under normal circumstances, without a delay, it was
hypothesized that only one adjacent angiosome could be captured, but not an angiosome once removed. This
hypothesis can be applied to the superior trapezius flap by dividing it into its component angiosomes. The primary
angiosome, which has its base at the midline posteriorly, is supplied by the paraspinous perforators. The adjacent
angiosome overlying the lateral aspect of the muscle is supplied by the transverse cervical vessels. Finally, the third
angiosome in line, or the angiosome once removed, which overlies the deltoid muscle, is supplied by a branch of the
thoracoacromial artery. Following interruption of the transverse cervical vessels during radical neck dissection, the
choke system of vessels between the three angiosomes becomes dilated, allowing a more favorable pressure gradient
by which the skin overlying the deltoid can be reliably captured by the medial angiosome supplied by the
paraspinous perforators.
The major use for this flap is to resurface cutaneous defects of the posterior and lateral aspects of the neck.
Following a radical neck dissection, the transfer of this flap is not only safe, but it also causes no further functional
deficit because the muscle is already denervated. It is especially advantageous for the coverage of heavily irradiated
wounds, including those in which the carotid artery is exposed. It is unique among the regional musculocutaneous
flaps in that it is superiorly based; therefore, gravity does not cause the flap to pull away from the recipient bed as
readily as is the case with other regional flaps with dependent muscles. The success of this flap in the "problem
wound" is enhanced by inserting the flap along its entire path to the site of the defect, even if intervening skin must be
excised to do so. The poorer aesthetic result of wrapping the flap around the neck is counterbalanced by the increased
chances of successful wound healing. More often than not, a skin graft is required for closure of the donor site.
Secondary correction of the "dog-ear" deformity below the auricle is often necessary.
LATERAL ISLAND TRAPEZIUS FLAP
The lateral island trapezius flap is the least reliable of the three musculocutaneous flaps because its arc of rotation is
dependent on favorable anatomy and meticulous mobilization of the TCA and TCV. Preliminary exploration of the
posterior triangle of the neck is essential to assess the suitability of these vessels. Because the musculocutaneous
island is completely isolated on the nutrient vascular pedicle, there are no alternative effluent routes through secondary
venous channels, such as might occur in a musculocutaneous flap in which the muscle is not completely detached. It is
therefore imperative that a patent TCV is present along, with the artery. The likelihood of both vessels being present
following radical neck dissection is small, and therefore, both the lateral island flap and the LTIMF should not be
selected in such patients.
The primary use of the lateral island flap is for external defects of the lateral and anterior neck. It may also be used
for mucosal defects of the pharynx and oral cavity. Panje described an extension of the lateral island flap, which he
classified as the trapezius musculocutaneous island paddle flap. In this design, a small island of muscle is used as a
carrier for an extended island of skin that is harvested well beyond the lower lateral border of the muscle in the
direction of the axilla. The proposed advantage of this flap is the large area of thin skin that can be harvested, which
improves the arc of rotation without completely interrupting shoulder function.
Ryan et al. described a novel use of the lateral island trapezius flap to achieve dynamic facial reanimation in a
variety of situations that led to facial paralysis. The surgical technique involved the transfer of an innervated and
vascularized segment of the trapezius muscle to the paralyzed side of the face. The muscle was inset into the corner of

Angiosomes of the superior trapezius flap. The superior trapezius flap is primarily supplied by the paraspinous
perforators that exit in the posterior cervical region. The primary angiosome (I) is shown in yellow; the adjacent
angiosome (II), supplied by the transverse cervical artery, is shown in blue. Finally, the third angiosome (III) in the
series, the angiosome once removed, is supplied by a branch of the thoracoacromial system, which is the primary
blood supply to the deltoid. Interruption of the TCA leads to a delay phenomenon of the skin overlying the deltoid
by opening up the choke vessels that separate these three angiosomes. The third angiosome in the series can be
more reliably captured by improving the hemodynamic pressure gradient across the middle zones.
the mouth and the temporalis fascia. In some cases, the vascular pedicle was not long enough to reach the defect, and
the pedicled muscle flap was converted to a free muscle flap. This technique was also used for composite cheek
defects by transferring an innervated musculocutaneous flap. By maintaining the accessory nerve intact, there was no
chance for denervation atrophy to occur. However, the disadvantage of this technique is that facial movement requires
a conscious effort by the patient to tense the ipsilateral shoulder.

Trapezius angiosomes: The primary angiosomes of the trapezius muscle are divided between the TCA (I) and the
DSA (II). The primary angiosome of the TCA is shared by the paraspinous perforators, which enter the muscle in
its medial cephalad region. The division between angiosomes 1 and II is signified by the underlying division
between rhomboid minor and rhomboid major through which the contribution from the DSA enters the
undersurface of the trapezius muscle. In harvesting the LTIMF, the position of the skin paddle may extend caudal
to the lower border of the trapezius muscle into the area of the latissimus muscle (III). The third angiosome in the
series, which is supplied by the paraspinous perforators entering the latissimus dorsi, may be reliably captured by
the trapezius flap by incorporating the dorsal scapular blood supply. However, if the dorsal scapular vessels are
interrupted and the flap is based solely on the TCA, then the third angiosome in the series may be less reliable. This
explains
some of the variability that we have encountered in harvesting this flap and the questionable reliability of this skin
paddle that has been reported in the literature. On the left hand side, two different skin paddles are drawn. The
solid line denotes a skin paddle that would be theoretically readily captured by the transverse cervical artery
because of the fact that it lies entirely within the territory of the adjacent angiosome (II). The dotted line indicates a
skin paddle that partially overlies the lower portion of the trapezius and extends into the territory of the latissimus
dorsi. The more caudal skin island has a greater arc of rotation. However, the reliable transfer of this more caudal
segment of skin would require preservation of the DSA. The disadvantage of this approach is that it requires the
harvest of a cuff of the rhomboid minor muscle to achieve an adequate arc of rotation. The advantage is that it
preserves the upper fibers of the trapezius muscle, which helps to stabilize the shoulder and preserve its function.
Our usual approach to harvesting skin paddles that extend more than 5 cm below the scapular border is to place a
temporary microvascular clamp on the dorsal scapular vessels and to observe the blood supply of the skin paddle to
determine whether interruption is safe.

POTENTIAL PITFALLS
Each of the three trapezius flaps has its own potential problems, which may cause an unsuccessful outcome. The
superior trapezius flap is probably the least problematic if its limited arc of rotation is respected and the extent of the
defect for closure does not cross the midline anteriorly.
The lateral island flap is technically easy to harvest, but it is imperative that the posterior triangle be carefully
explored to ensure that the anatomy of the TCA and TCV is favorable. Failure to identify and carefully isolate both an
artery and vein will lead to inevitable failure. Particular attention must be taken in preserving the TCV, which may be
in jeopardy because of its course superficial to the posterior belly of the omohyoid and its entry into the external
jugular vein. Both of these venous patterns must be sought when dissecting in this region to avoid inadvertent injury.
The most common error performed in harvesting the LTIMF is the failure to raise the trapezius muscle in the plane
superficial to the rhomboid major and minor muscles. This is best accomplished by identifying the lateral border of the
caudal portion of the trapezius muscle. Meticulous dissection in the plane deep to the trapezius muscle allows the
surgeon to identify the fibers of the rhomboid major muscle that run in a more transverse orientation and insert into
the medial border of the scapula. Krespi et al. described the combined rhombotrapezius flap, which reportedly
enhanced vascularity to the overlying skin, provided added bulk, and allowed transfer of vascularized bone from the
medial border of the scapula. The additional vascularity is undoubtedly a result of including the dorsal scapular system
by dissecting in the plane deep to the rhomboids. However, the harvest of the rhomboid major is not critical to
achieving this end. The bulk that is obtained by incorporating the thin rhomboid muscles is minimal after denervation
atrophy occurs. Finally, the medial border of the scapula is a thin bone that is not suitable for functional mandibular
reconstruction. The morbidity of a winged scapula that results from total disruption of the medial muscle group
outweighs the limited benefits of this flap design.
The LTIMF has been labeled an unreliable reconstructive technique, with complication rates caused by partial or total
flap necrosis ranging from 0% to 57% among the larger series of cases that used this donor site. The interpretation of
these complications must be placed in the context of the flap designs that were utilized in each series. Mathes and
Stevenson reported a 0% rate of complications when using the LTIMF for the repair of 13 posterior neck and skull
defects. Although these authors divided the dorsal scapular pedicle, the arc of rotation to the defects of the posterior
neck and skull allowed the skin paddle to be placed over the distal muscle.
Significant mobilization of the muscle was not required. Cummings et al. reported a 57% incidence of flap necrosis.
Although these authors noted that they extended the distal skin paddle beyond the lower border of the muscle in some
patients, they did not analyze their complications with this variable in mind.
In the largest series of 45 LTIMFs reported by Urken et al., there was a 6.5% incidence of major complications
denned as a greater than 20% flap loss. There was similarly a 6.5% incidence of minor (20%) flap loss. In no case in
this series was the dorsal scapular pedicle preserved. The lower border of the skin paddle was not extended beyond 5
cm below the scapular border in most patients. Of note was the fact that all but one case of flap necrosis occurred in
patients who underwent flap transfer on the side in which a prior neck dissection had been performed. It is evident
from this finding that a prior radical neck dissection should be considered a contraindication to harvesting an
ipsilateral LTIMF.
Donor site problems are rarely significant. However, seroma formation is common, and long-term suction drainage is
recommended.

III. STERNOCLEIDOMASTOID MUSCLE FLAP
The first reported use of the sternocleidomastoid (SCM) muscle in head and neck reconstruction was by Jiano in 1908
in which it was transposed to a paralyzed face to restore dynamic reanimation. Schottstaedt et al. used the SCM to
replace the masseter muscle in a child who had developed paralysis in the distribution of the trigeminal nerve, which
resulted from poliomyelitis. Additional cases were reported by Dingman et al. and Hamacher who transferred a
segment of the SCM muscle with its intact motor nerve and vascular supplies for replacement of the congenitally
absent or paralyzed masseter. Owens, in 1955, is credited with being the first to report a musculocutaneous flap based
on the SCM. He transferred a superiorly based flap but maintained a broad cutaneous attachment of the skin in the
region of the mastoid. Owens incorporated the platysma and the SCM to enhance the blood supply to the skin.
Bakamjian modified Owens flap by extending the skin territory below the level of the clavicle. Littlewood reported
additional experience in using the extended SCM flap and identified the contributions of the occipital and posterior
auricular arteries to the vascular supply of the muscle. O'Brien is credited with being the first to transfer an island of
skin overlying the caudal aspect of the neck with the SCM pedicled superiorly. Finally, Ariyan identified the inferior
vascular supply from the thyrocervical trunk and successfully transferred an inferiorly based flap.

The original SCM musculocutaneous flap described by Owens
The SCM flap has been extensively studied but not widely used. It has been criticized on oncologic grounds, which
are related to the safety of preserving this muscle when there are regional lymphatic metastases. The limited size of
Inferiorly based superiorly based
the musculocutaneous flap restricts its use to small defects. Finally, this flap has been criticized for the unreliability of
the skin paddle and for the contour deformity in the neck following flap transfer.
The SCM is a round muscle that originates from the manubrium and the medial aspect of the clavicle. It runs an
oblique course in the neck to insert on the mastoid process and the superior nuchal line. Contraction of the SCM leads
to tilting of the head, bringing the ipsilateral ear closer to the shoulder. The superficial layer of the deep cervical fascia
splits to provide coverage of the SCM on both its deep and superficial surfaces.
FLAP DESIGN AND UTILIZATION
The evolution in flap design since the introduction of the broad superiorly based musculocutaneous flap of Owens was
outlined in the introduction. The superiorly based and inferiorly based island musculocutaneous flaps are presently the
most commonly used SCM flaps. Although Bakamjian and Littlewood extended the skin territory below the clavicle
with the superiorly based "peninsular" flap, there has been little reported that substantiates such maximum dimensions
when the flap is harvested as an island of skin. In addition to transfer of the musculocutaneous unit, there have been
numerous reports of using the SCM to transfer clavicular periosteum and segments of the clavicular bone for
reconstruction of the mandible.
The problem of the donor site contour deformity was addressed by Alvarez et al. who reported the use of the split
SCM musculocutaneous flap in 1983. Transposition of the entire belly of the SCM produced an objectionable bulge in
the midneck and a concavity in the lower neck. Alvarez et al. described a series of cases in which either the sternal
head or the clavicular head of the muscle was transferred to the recipient site. They cautioned that this longitudinal
split could only be carried through approximately two thirds of the muscle's belly in its longitudinal direction.
The ability to transfer the SCM with the preservation of its vascular and neural supply led to the application of this
flap to reconstructive problems requiring dynamic activity. The early report by Jiano in restoring mimetic activity to
the paralyzed face was one such example. O’Brien used the SCM to reconstruct a total lower lip defect, with the skin

island providing the inner lining. The dynamic activity of the SCM was preserved and believed to have functional
value in restoring oral competence. In the introduction, it was noted that this flap was also applied to the problem of
dynamic restoration of the masticator muscle sling. Finally, Matulic et al reported the combination of the SCM muscle
flap with a forehead cutaneous flap to reconstruct the oral cavity following glossectomy. The forehead flap provided
the inner lining, and the SCM was transposed to provide dynamic tongue activity. As in many reconstructive
techniques that purport to restore motion, the documentation by electromyography of motor activity does not
necessarily translate into coordinated functional activity. An exception to this statement is in facial reanimation in
which muscle transposition has been shown to be an effective means of restoring mimetic activity. The SCM has been
supplanted by the temporalis and masseter muscles because of the improved axis of pull of the latter two muscles in
producing a symmetric smile.
The SCM muscle flap has also been used to restore a normal lateral facial contour following parotidectomy and
mandibular reconstruction. Hill and Brown transposed a superiorly based muscle flap over a free iliac bone graft to
achieve a more satisfactory lower facial contour in secondary mandibular reconstruction. Bugis et al. reported their
experience with the use of the SCM muscle flap to restore the facial contour in 31 patients following parotidectomy.
In addition, they reported the successful application of this flap in two patients who had postoperative salivary fistulas.
Despite these findings, the SCM muscle flap was not found to be an effective method to prevent Frey's syndrome in an
extensive series of patients reported by Kornblut et al. A group of 35 patients who underwent parotidectomy and SCM
muscle transposition into the parotid bed were compared with a control group of 35 patients who underwent
comparable ablative procedures but no muscle transposition. The rationale for transposing the muscle was to interfere
with the presumed mechanism of Frey's syndrome, which is the misdirection of auriculotemporal secret motor fibers
from their normal end organ, which is the salivary tissue. It is thought that the transsected nerves are rerouted to the
sweat glands of the overlying skin, thereby producing "gustatory sweating." Komblut et al. reported no difference in
the incidence of Frey's syndrome in the two study groups.
The SCM musculocutaneous flap has been used for oral and pharyngeal mucosal defects since Bakamjian's initial
report of the use of this flap to reconstruct the palate following radical maxillectomy. As noted previously, Bakamjian
used an extended peninsular skin muscle flap that was transferred through the posterior oral cavity. At a second stage,
the flap's pedicle was transsected, with closure of the orostoma. Ariyan reported 14 cases of either superior or inferior
musculocutaneous flaps used in the oral cavity or pharynx. He noted "partial epithelial loss" in seven cases, but only
one developed a salivary fistula. Re-epithelialization of the denuded areas of the oral cavity was reported, and biopsies
from the healed reconstructed site demonstrated preservation of the dermal layer. In this report, Ariyan also described
primary closure of the donor site defect through cutaneous advancement flaps rather than by application of a skin
graft. Additional reports on the SCM musculocutaneous flap cited varying degrees of skin viability. Sasaki used four
inferiorly based and one superiorly based flap to reconstruct the floor of the mouth and tonsillar regions. The skin of
the superiorly based flap underwent total necrosis; partial skin necrosis was reported in two of the remaining inferiorly
based flaps. Despite these complications, there were no cases of salivary fistulas, which Sasaki attributed to the
viability of the underlying SCM muscle. Marx and McDonald reported a more favorable experience with the
superiorly based flap in eight patients in whom they noted distal skin necrosis 2 cm from the tip of the flap. These 8
cases of oral cavity reconstruction represented a subset of the 16 reported cases of SCM flaps also used for a variety of
other indications. These authors emphasized the necessity of maintaining the vascular contributions from the superior
thyroid artery and vein. The importance of this contribution from the superior thyroid pedicle is discussed later in
detail. Finally, Ariyan reported closure of a cervical esophagostoma by using a superiorly based SCM flap for inner
lining followed by a superior trapezius flap for outer cutaneous coverage.
The use of vascularized segments of the clavicle supplied by adjacent soft tissue was introduced in the early 1970s as
a solution to the frustrating problem of restoring bone continuity following segmental mandibulectomy. Siemssen et
al. referred to two of the earliest reports that used portions of the clavicle to reconstruct the mandible, which dated
back to the beginning of the 20th century. They credited Rydygier with being the first to transfer an osteocutaneous
flap containing a portion of the clavicle. This was followed by Blair's description of composite flaps containing
clavicle and rib. Snyder et al. is credited with reviving this concept with a report issued in the current era in which
vascularized bone was used to restore bony defects of the maxillofacial skeleton. They reported several cases of
vascularized bone transfer based on regional cutaneous flaps. They transferred either full- or split-thickness segments

of clavicle with the overlying skin in a two-stage procedure. This publication was followed by Conley's report in 1972
of a series of 50 regional bone containing flaps for mandibulofacial reconstruction. Included in this series were a
variety of different composite flaps, including the deltopectoral acromion flap, the trapezius-scapular flap, the
temporalis-calvarial flap, and the SCM-clavicular flap. Although Conley reported three complete flap failures in this
series, there were few details regarding the actual techniques used for each of these donor sites. He warned about the
potential shoulder morbidity associated from segmental defects of the clavicle and advised that a sagital split be
performed to transfer only the outer cortex.
Siemssen et al. reported on a series of 18 patients who underwent mandibular reconstruction with either split or
segmental segments of the clavicle pedicled on the clavicular head of the SCM. Although seven bone flaps were
transferred in the primary setting, internal lining was achieved with either a forehead or deltopectoral flap. There were
significant complications in the group of five patients in this series who underwent split clavicle transfers, with
fractures occurring at both the donor and recipient sites. In the remaining patients in this series, a full segment of the
clavicle was harvested anterior to the attachment of the trapezius muscle. The authors reported little to no shoulder
morbidity in these patients. In addition, the clavicle was pedicled on the clavicular head of the SCM and passed under
the sternal head to avoid a contour deformity in the neck. Finally, they speculated about the possibility of
reconstructing a near-total mandibular defect by transferring the anterior portions of both clavicles with an intervening
segment of the manubrium pedicled on both SCM muscles. There was only one total flap necrosis in this series.
Barnes et al. reported a similar favorable experience with the use of this musculoclavicular flap in four primary and
one delayed mandibular reconstruction. The viability of the neomandible was confirmed with postoperative
technetium scans.
NEOROVASCULAR ANATOMY
The vascular supply to the SCM muscle and its overlying skin is arguably the most confusing of any flap used in head
and neck reconstruction. This is one explanation why this flap has not been embraced with a significant amount of
enthusiasm. The SCM has a type II vascular supply, according to the classification scheme of Mathes and Nahai.
There is one dominant pedicle arising superiorly from the occipital artery and vein and three minor pedicles: a branch
of the posterior auricular artery and vein, a branch of the superior thyroid artery and vein, and a branch of the
thyrocervical trunk. As noted previously, the segmental nature of the vascular supply allows this muscle to be pedicled
The dominant arterial supply to the SCM muscle is from the occipital artery. Minor vascular contributions arise
from branches of the posterior auricular artery, the superior thyroid artery, and the thyrocervical trunk.

either superiorly or inferiorly. The motor supply to the SCM is from a branch of the accessory nerve, which continues
across the posterior triangle of the neck to innervate the trapezius muscle as well. There remains some controversy as
to whether the contribution to the SCM's innervation from C-2 and C-3 is motor or sensory.
The successful transfer of skin as a musculocutaneous flap requires preservation of the vascular supply to the muscle
and capture of the musculocutaneous perforators that exit the superficial surface of the muscle. The relationship of the
SCM to the overlying cervical skin varies, depending on whether the caudal aspect of the neck or the region below the
mastoid tip is regarded. The reason for this difference is the presence of the platysma muscle, which is a sheet like
muscle of varying thickness that runs in the superficial fascia of the neck. It arises below the clavicle from the
muscular fascia overlying the pectoralis major and the deltoid. It courses obliquely across the neck at right angles to
the SCM to blend with the muscles inserting on the lower lip. The paired platysma muscles are deficient in the midline
of the neck; laterally, they overlap the SCM only to approximately the midlevel of the neck. Therefore, the caudal half
of the SCM is separated from the overlying skin by a layer of platysma; the cephalad half has no such intervening
layer. This difference can readily be felt by assessing the relative mobility of the lower neck skin compared with the
tightly adherent skin of the upper neck.
The platysma muscle is a vestige of the panniculus carnosus in lower animals. The skin is tightly adherent to this
muscle, and it has long been recognized that cervical skin flaps are more viable when the platysma is included. The
platysma has been successfully used as a carrier of cervical skin, as introduced by Futrell et al. in 1978. The platysma
is primarily supplied by the submental branch of the facial artery. The platysma musculocutaneous unit has been
shown to be reliable in subsequent reports.
What is unique about the superiorly based SCM island flap is that a successful outcome requires capture by a deeper
muscle (SCM) of a more superficial musculocutaneous unit (platysma). There is no other flap used in the head and
neck or perhaps elsewhere in the body in which the blood supply to the skin must traverse two distinct muscle layers.
The cephalad portion of the muscle appears to be a more favorable donor site to harvest skin because of the lack of the
intervening muscle layer. However, the inferiorly based flap is at a disadvantage as a result of the smaller vascular
pedicle entering the caudal aspect of the muscle.
Studies that have investigated the vascular supply to the cervical skin are helpful in shedding light on this problem.
One of the earliest reports that looked at the vascular contributions from the SCM to the cervical skin was by Jabaley
et al. In a series of cadaver dissections, these investigators reported an extreme paucity of musculocutaneous
perforators arising from the lower two thirds of the SCM. They did, however, identify a direct cutaneous branch from
the transverse cervical artery that penetrates the platysma to supply the supraclavicular skin.
Two publications from the University of Pittsburgh reported on a series of fresh cadaveric studies that also examined
the blood supply to the cervical skin. A summary of the findings in these two studies is enlightening. These
investigators corroborated the observations of Jabaley et al. that there are few musculocutaneous perforators from the
SCM and those that were present are extremely small. Direct cutaneous perforators were identified from a number of
sources, including the occipital, posterior auricular and superior thyroid arteries, which were the most consistent.
These three branches of the external carotid artery, therefore, supply feeders to the SCM muscle and direct perforators
to the skin. In 80% of the cadaver dissections, a large cutaneous vessel from the superior thyroid artery was identified
coursing around the anterior border of the SCM, which supplied the platysma and skin of the midneck. It is likely that
the success reported by Marx and McDonald in their series of superiorly based SCM flaps was directly related to the
preservation of the superior thyroid branches. Ink-injection studies of the cutaneous branch of the superior thyroid
artery caused staining of the skin of the middle and lower cervical regions. In one dissection, the direct cutaneous
branch from the superior thyroid system traveled on the undersurface of the SCM and then entered the platysma and
the overlying skin between the sternal and clavicular heads of the SCM.
This review of the vascular anatomy points out potential pitfalls in regard to both the superiorly and the inferiorly
based island flaps. The superiorly based flap preserves the dominant blood supply to the muscle but is problematic
because of the intervening layer of platysma. The inferiorly based flap relies on the nondominant contributions to the

muscle from the caudal aspect of the neck after transsecting the dominant cephalad muscular branches. However, the
skin overlying the cephalad portion of the SCM appears to be more favorably related to the muscle because of the
absence of the platysma. The peninsular skin flap, as described by Owens, should have an excellent chance of viability
because of the preservation of the dominant blood supply to the muscle and direct cutaneous feeders to the skin
entering from the occipital and posterior auricular branches. Muscle only or muscle plus periosteum, with or without
clavicle, also appear to be reliable flaps.
POTENTIAL PITFALLS
Many of the potential complications of this donor site have been discussed in this chapter. The viability of the skin of
either a superiorly or an inferiorly based flap is questionable. However, the experience of Marx and McDonald,
suggests that preservation of the superior thyroid artery may be extremely important, for the reasons mentioned. It
may be possible to mobilize the superior thyroid pedicle to enhance the arc of rotation.
One of the other major criticisms of this donor site is its intimate relationship to the region of most common nodal
metastases from the head and neck primaries. The necessity for a formal radical neck dissection eliminates this flap as
a surgical option. Modified neck dissections may allow preservation of the SCM, but its vascular supply is placed in
jeopardy. Transfer of a SCM flap from the contra lateral neck may be feasible. Arguments against violating a potential
site of regional metastases have been raised. However, the opposing point of view in this controversy is that, in raising
the SCM, the posterior fascial layer does not need to be violated and, therefore, the envelope of deep cervical fascia
that encloses the lymph node-bearing tissue can be preserved.
IV. TEMPORALIS MUSCLE FLAP
Because of its anatomical proximity to the midface and its ease of transfer, the temporalis muscle has been used for a
variety of reconstructive problems in the maxillo-facial region. Described in 1898 by Golovine, the temporalis flap is
one of the earliest reported muscle flaps. It was initially reported for use in obliterating the dead space following
orbital exenteration owing to the bulk and proximity of the temporalis muscle to the orbit. In the 1930s, Gillies
introduced the use of the temporalis as a method of rehabilitation of the paralyzed face. Sheehan also added to the
early development of this flap by describing the reduction or removal of the zygomatic arch to increase the arc of
rotation and to improve the problem of excessive bulk in the midface. In 1951, Anderson modified the Gillies
technique by using temporalis fascia, instead of the fascia lata, to reconstruct the eyelids in patients with facial
paralysis. In the 1970s and 1980s, May, McKenna et al., Rubin et al., Rubin, and Edgerton et al. added substantially to
the usefulness of this flap by their reports advocating the use of temporalis muscle in the management of the paralyzed
face. Rubin et al. and Rubin also clarified the application of this flap in oral commissure reanimation by carefully
categorizing human smile patterns and detailing the anatomic relationship between the orbicularis oris and the facial

muscles. These reports established the temporalis as a logical option for reanimation of the paralyzed face. Further
refinements in the transfer of the temporalis increased its clinical usefulness in managing contour defects following
maxillofacial resections and in eyelid and intraoral reconstruction
FLAP DESIGN AND UTILIZATION
The temporalis flap has gained acceptance for a variety of clinical purposes, including the augmentation of regional
tissue deficiencies and the elimination of scar contractures. It may also serve as a vascular surface for free skin
grafting, as protection for the carotid artery, as a myoosseous flap, and provide dynamic rehabilitation of the paralyzed
face.
The temporalis may be transferred in its entirety or in part, depending on the reconstructive challenge. The
dimensions of the muscle vary with the thicker aspect of the muscle located in the anterior third of the temporal fossa;
the middle and posterior thirds of the muscle are consistently thinner and slightly longer. The length of the muscle in
the middle third makes this portion ideal for use in the rehabilitation of the paralyzed face. Although some authors
have relied on the muscle for ocular and midfacial rehabilitation, it has been our experience that the independent
reconstruction of these two important functional zones of the face improves the overall outcome. This approach allows
the surgeon to limit the amount of the muscle transferred into the midface, thereby minimizing the degree of contour
irregularity over the zygomatic arch.
The temporalis has established itself as an important technique for the reconstruction of the paralyzed face. Although
criticized by many because of its lack of spontaneous facial movement, the transferred temporalis allows for
immediate reanimation of the paralyzed face and may be used when potential facial nerve recovery exists. The muscle
has many anatomical characteristics, which make it desirable for use in facial rehabilitation. It is relatively short (3 to
5 cm) and thin (2 to 3mm) and has a contraction capability of 1 to 1.5 cm. The midportion of the muscle has sufficient
strength to adequately mobilize the face and resist the forces of soft tissue contracture. An additional advantage when
using this muscle is the fact that it is innervated in a segmented pattern by the branches of the trigeminal nerve (branch
V2). This allows for independent segments of the muscle to be designed for use in the orbit and midface. For a muscle
transfer to be functional, it must have an origin and a point of insertion. The zygomatic arch can be used effectively to
provide the transferred muscle with a fixed point of origin after it is transposed into the midface.
Although the temporalis is firmly attached to the coronoid process and ramus, the surgeon can vary the point of
attachment of the distal transposed end of the muscle. This flexibility has been noted by Renner et al., Rubin et al, and
Rubin and allows the vectors of muscle contracture to be varied in an attempt to individualize the procedure to the
particular characteristics of the patient's smile, as analyzed on the normal side.
There have been several limitations noted when the temporalis is used for facial reanimation. Muscle contracture is
initiated by the fifth cranial nerve and is therefore not mimetic with the contralateral face. This drawback can be
improved by early and regular physical therapy. The other common concern with this technique has been the
management of the donor site. When the muscle is transferred over the zygomatic arch, the contour of the
temporoparietal scalp and the midface can become distorted. By limiting the amount of muscle that is transferred to a
2-cm width from the middle
third of the body of the muscle, the amount of bulk over the zygoma is minimized. The segmental neurovascular
supply allows the muscle to be safely divided in this fashion. The secondary depression in the infratemporal fossa has
conventionally been managed with synthetic implants. However, these implants have an unnatural feel and are
susceptible to extrusion. As an alternative solution to this problem, we have elevated an independent temporoparietal
fascial flap, based on the superficial temporal artery and vein, and used this flap to reliably re-establish the scalp
contour
of this region.
Cranial nerve injury is a common consequence of skull base procedures. Although the sensory function of the fifth
cranial nerve is commonly affected, the motor component of this nerve is rarely involved. The temporalis muscle is,
therefore, a viable option for the reconstruction of the paralyzed face when other cranial nerve-muscle units may not
be available.

The temporalis has been used to reconstruct a variety of midfacial defects by designing it as a turnover flap, with the
point of rotation based at the zygomatic arch. Because the flap has a rotational radius of 8 cm, it is possible to cover
defects of the mastoid, cheek, pharynx, and palate. The muscle is longer and thinner than the masseter, and therefore,
it can be placed throughout the midface, which allows muscle bulk to be transferred to anatomic locations that are not
within the rotational range of other regional muscle flaps. The arc of rotation can be improved by passing the
temporalis deep to the zygomatic arch, a maneuver that is often made simpler by osteotomies to remove and then
replace the bone. An additional advantage of the temporalis is that it readily accepts split-thickness skin grafts. This
feature may be useful in managing full-thickness defects of the middle third of the face.
The temporalis originates from the surface of the catvarium on the lateral aspect of the skull. The superior
attachment forms a gentle arc that is referred to as the inferior temporal line. The temporalis occupies the entire
temporal fossa and inserts into the coronoid process and the anterior aspect of the mandibular ramus. The
temporalis is covered by a thick fascial layer, the temporalis muscular fascia, which is described as being a second
point of origin of the muscle. The temporalis fascia is adherent to the skull at the superior temporal line where it is
continuous with the pericranium that covers the remainder of the skull. Inferiorly, the temporalis muscular fascia
splits into a deep and superficial layer approximately 2 cm cephalad to the arch. These two layers merge with the
periosteum of the medial and lateral surfaces of the zygomatic arch, respectively. The superficial layer of the deep
muscular fascia is continuous with the masseteric muscular fascia.
Although temporalis transposition has been used primarily for rehabilitation of the paralyzed face, it can also be
considered for the reconstruction of full-thickness defects in the midface. It provides adequate bulk to obliterate full-
thickness defects of the orbit and lateral oral cavity. Orbital cavity defects may be managed by a variety of techniques.
The temporalis should be a primary consideration because it will completely or partially fill the cavity without the
problem of limited excursion, and it also creates a favorable milieu for later prosthetic placement. The muscle has also
been successfully used in the closure of oroantral fistulas and for reconstruction of the lateral maxilla and skull base.
Craniofacial surgical procedures often produce a communication between the anterior cranial fossa and the nasal or
paranasal sinus cavities. Separation of these two regions is critical to minimize complications such as cerebrospinal
fluid leaks, epidural abscess, and meningitis. The temporalis has been successfully used for this purpose. It should be
noted that this muscle may be harvested without interfering with the vascular supply to the scalp when using a coronal
incision for exposure for the craniotomy.
The temporalis may also be used as a carrier of vascularized outer calvarial bone. This technique utilizes the
temporalis and its distal pericranial extension to provide a vascular basis for this myoosseous flap. The thinness and
contour of unicortical calvarial bone grafts makes this compound flap useful for palatal, orbital rim, and orbital floor
reconstruction. Although described for use in segmental defects of the lateral mandible, the limited bone stock of this
donor site pales in comparison with the bone stock of other donor sites currently in use for oromandibular

reconstruction. Vascularized calvarial bone grafts have also been used extensively as onlay bone grafts for contour
deformities of the maxillofacial skeleton resulting from congenital deformities, trauma, or ablative surgery.
The disadvantages of this flap are primarily related to the inability to transfer overlying skin with the muscle and the
relatively short arc of rotation, which limits the usefulness of this technique when reconstruction requires extension
beyond the nasolabial crease. To improve the distal excursion of the transfer, the zygomatic arch may be removed,
allowing an additional 2 to 3 cm of muscle length. The muscle flap may be skin grafted on both the medial and lateral
surfaces when required. However, contracture of the skin graft in the midface often leads to surface contour
deformities, although it may provide a satisfactory replacement of the inner mucosal defects. In addition to the limits
encountered with the transfer of this muscle, the management of the secondary contour deformity of the donor site is
also an important issue that has been discussed earlier.
NEOROVASCULAR ANATOMY
The temporalis is broadly based, arising from the inferior temporal line. It fills the entire temporal fossa and narrows
as it inserts onto the coronoid process of the mandible. It is covered by the temporalis muscular fascia (deep temporal
fascia) superficially. The temporalis functions in mastication, in conjunction with the masseter and pterygoid muscles,
to elevate and retract the mandible. The vascular supply to the temporalis is the deep temporal artery and vein, which
arise from the internal maxillary system deep to the zygomatic arch. The deep temporal vessels penetrate the under
surface of the temporalis, providing a segmental vascular pattern. The muscle is classified as having a type III pattern
of circulation (two dominant vascular pedicles), as described by Mathes and Nahai. An additional arterial supply to the
muscle arises from the middle temporal artery, which sends minor branches through the superficial aspect of the
muscle. The middle temporal artery arises from the superficial temporal artery and crosses over the zygomatic arch to
provide a separate vascular supply to the temporalis muscular fascia.
The temporalis muscular fascia inserts on the superior temporal line. In its caudal extent, it divides into two leaves,
approximately 2 cm above the zygomatic arch. The deep and superficial muscular fascial layers insert on the medial
and lateral aspects of the arch and are separated by a layer of fat. The muscular fascia fuses with the periosteum of the
arch to form a very dense fibrous layer. The temporal and zygomatic branches of the facial nerve cross the zygomatic
arch in the layer of the temporoparietal fascia, which is superficial to the muscular fascia-periosteal layer. The fatty
plane that separates the two layers of the temporalis muscular fascia may be used by the surgeon to protect the facial
nerve branches. By starting at the root of the zygomatic arch and incising the superficial layer of the temporalis
muscular fascia, the fatty plane is entered. If this incision is made at a 45-degree angle in the anterosuperior direction
and the zygomatic arch is uncovered in a subperiosteal plane, the facial nerve branches can be protected by reflecting
this fascial-periosteal layer in an anterior and inferior direction.
POTENTIAL PITFALLS
The use of the temporalis in midfacial reconstruction is a dependable technique; however, there are a number of
features of this flap that pose potential problems. As mentioned previously, the muscle transfer relies heavily on

capturing an adequate neural and vascular supply. In patients who have undergone extensive skull base or neck
surgery, interruption of the neurovascular supply can result in a muscle that is not suitable for transfer.
Another concern when transferring this flap in conjunction with the temporoparietal fascial flap is secondary alopecia
of the overlying scalp. This problem is of particular concern for patients who have undergone regional radiation
therapy and/or in whom a scalp incision has been used to gain access to the skull base. It has been our experience that
patients who have undergone occipital approaches to the skull base utilizing temporal incisions around the auricle are
not good candidates for the use of the temporoparietal fascial flap because partial devascularization of the auricle
occurs in a significant percentage of patients.
The frontal branch of the facial nerve is located in the temporoparietal fascia. Above the zygomatic arch, it runs
approximately 2.0 cm lateral to the lateral aspect of the eyebrow. Its course may be outlined by drawing a line from
the tragus to a point 2.0 cm above the lateral eyebrow. This nerve branch should be identified in this location and
avoided during the anterior dissection and elevation of the muscle. The auriculotemporal nerve, a branch of the third
division of the trigeminal nerve, courses under the zygomatic arch and then runs in a cephalad direction posterior to
the superficial temporal artery and vein. It supplies sensation to the anterior auricle, the external auditory meatus, and
the scalp of the temporal region, and this nerve must be identified and preserved if sensation of the temporoparietal
area is to be maintained.
PREOPERATIVE ASSESSMENT
Prior to surgery, it is imperative for the temporalis muscle to be examined by asking patients to clench their teeth to
ensure that the muscle exhibits normal strength and tone. This is particularly important in patients who have
undergone prior skull base procedures in which the viability of the fifth cranial nerve may be in question. Asymmetric
wasting of the temporal fossa is a telltale sign of denervation atrophy of the temporalis. It is also important to establish
the patency of the superficial temporal artery and vein to assess the viability of the temporoparietal fascia if this fascia
is to be used to obliterate the donor site defect that results from the harvest of this muscle.
POSTOPERATIVE WOUND CARE: MANAGEMENT OF THE DONOR SITE
Numerous techniques have been advocated for the management of the donor site created after temporalis
transposition. Alloplastic implants have become less popular in recent years because of the significant incidence of
secondary infection, extrusion, and implant mobility. In an attempt to reestablish adequate contour with autogenous
tissue, we have used vascularized temporoparietal fascia, with satisfactory results. This fascial flap is elevated prior to
harvesting the temporalis and is mobilized laterally during the elevation and transfer of the muscle segment. It is then
used to obliterate the temporal defect created after all or part of the temporalis is transposed into the midface. At the
completion of the procedure, a suction drain is placed in the temporoparietal scalp for 24 to 36 hours. A bulky
compressive dressing is used for the first 24 hours postoperatively to prevent hematoma formation and reduce facial
swelling.

V. MASSETER MUSCLE FLAP
Lexer and Eden are credited with being the first to use the masseter muscle for reconstructive purposes in 1911. They
reported using two slips of the anterior half of the muscle, transposed into the upper and lower lip, to reanimate the
paralyzed face. The early reports on masseter transfers showed this technique to be unreliable in a significant
percentage of cases. A review of the description of early harvesting techniques indicates that surgical violation of the
neural supply of the transposed muscle may have contributed to secondary atrophy and lack of coordinated movement
in these early reports.
The masseter has maintained its popularity in reanimation of the mouth in patients with facial paralysis. In addition,
it has been used for reconstruction of postablative mucosal defects of the posterior oral cavity. This muscle has a
number of advantages, including its ease of surgical transfer, its dependable neurovascular supply, and the fact that it
can be used to depress the paralyzed lower lip.
FLAP DESIGN AND UTILIZA TION
The most common application of the masseter transposition flap has been for facial reanimation in traumatic,
congenital, or postablative paralysis. It may be harvested through either an intraoral or extraoral approach for
transposition to the oral commissure. Baker and Conley advocated the harvest of the periosteal attachment of the
masseter to provide additional length and to provide better purchase for fixation of the masseter to the lateral
commissure of the mouth.
In patients with total hemifacial paralysis, rehabilitation of the eye requires the introduction of other techniques, which
include gold weights, eyelid springs, and tarsal tightening. The masseter transposition flap is only useful to restore
motion to the lower face. The dynamic activity produced by the masseter is triggered by the patient initiating a biting
motion and not by the involuntary emotional expression produced through the facial nerve.
In this respect, both the temporalis and masseter are similar in their common trigeminal nerve innervation. The
direction of pull with the masseter muscle is oriented more posteriorly than what is normally produced by the
temporalis. May commented on the additional bulk in the cheek that is caused by transposition of the masseter, which
may be advantageous in cases of tumor ablation where added bulk may improve the final facial contour. Transposition
of the temporalis muscle is also associated with a contour deformity resulting from the bulk of that muscle over the
zygoma and the secondary concavity in the temporal fossa.
The masseter has been used for a variety of other purposes following ablative surgery of the oral cavity and pharynx.
Conley and Gullane described several applications of this muscle flap following composite resections in which the
hemimandible was removed. They described suturing the masseter to the hyoid bone to assist in laryngeal elevation

during swallowing. They also reported using the muscle to cover the upper portion of the internal carotid artery. The
masseter has also been transposed into the nasopharynx and covered with a split-thickness skin graft to close mucosal
defects that extended to this region. The application of the masseter for these reconstructive purposes is only feasible
when the ramus of the mandible has been resected and not replaced.
The reconstruction of small defects of the posterior lateral oral cavity and, in particular, the retromolar trigone
region can be problematic when the mandible is left intact. Regional musculocutaneous flaps may not be easily
transferred because of excess bulk. Violation of the tongue to form a split-tongue transposition flap should be
condemned because of the interference in lingual function. The palatal island flap is a reasonable alternative option,
but it leaves a raw surface of palatal bone for closure by secondary intention and is not advisable following radiation
therapy. The masseter may be used to cover these mucosal defects by mobilizing the entire muscle, except for its
superior attachments to the zygoma. It is important to perform this mobilization in a subfascial plane of dissection to
avoid injury to the facial nerve. The masseteric fascia is elevated with the cheek flap to expose the entire muscle,
which is then freed from its attachments to the angle of the mandible. The muscle should not be mobilized above the
condylar notch to avoid injury to the neurovascular pedicle. The muscle is then transposed over the mandible and
sutured to the pharyngeal constrictors, mylohyoid, and digastric muscles.
A split-thickness skin graft may be placed on this muscle bed if mucosal approximation is not possible. Tiwari and
Snow reported using this technique in 24 patients with small posterolateral oral defects. One patient developed an
orocutaneous fistula and a second patient required lysis of a fibrous band that developed in the retromolar trigone
region and limited oral opening
.Zoller et al. described a modification of this technique in which the masseter muscle flap was combined with a
superiorly based cheek transposition flap. The combination of the muscle and mucosal flaps provided a reliable two-
layer closure of posterior oral cavity defects. The secondary defect resulted in exposed buccinator muscle, which was
allowed to close by secondary intention.
NEUROVASCULAR ANATOMY
The masseter is divided into deep and superficial bellies. The former arises from the anterior two thirds of the
zygomatic arch; the latter arises from the inner surface of the arch at its posterior third. Both bellies of the muscle
insert into the lateral surface of the ramus extending from the lower portion of the coronoid process to the mandibular
angle. The major action of the masseter muscle is to close the mandible. Because of the downward posterior
orientation of the muscle fibers, the masseter assists the lateral pterygoid in protraction of the mandible.
The neurovascular pedicle to the masseter enters the deep surface of the muscle through the mandibular notch. The
masseteric artery arises from the internal maxillary artery. Part of the venous outflow from the masseter goes to the
facial vein and part enters the pterygoid plexus and, ultimately, the internal maxillary vein. The masseteric nerve is a
branch of the mandibular nerve that arises from the trigeminal nerve.
Correia and Zani carefully documented the course of the nerve and advised that the safest way to preserve the
innervation was to transfer the entire muscle as a unit. They also recommended that any attempt to divide the muscle
with an inferiorly based longitudinal split should not exceed 3.5 cm. This division should begin at the inferior border
of the muscle at the junction of the anterior two thirds and the posterior third. A more cephalad division risks injury to
the nerve
ANATOMIC VARIATI ONS
In a series of 25 cadaver dissections, Correia and Zani found the dissection of the masseter nerve to be difficult.
They were able to dissect the nerve and its branches, however, by approaching it from a posterosuperior direction,
where it crosses the mandibular notch. Examination of the specimens resulted in the classification of the muscle into
two groups, according to its length. A long muscle was found in 17 cases (68%) and a short muscle, in 8 cases (32%).
In the short masseter type, the nerve was found to run obliquely forward and downward across the rectangle of the
muscle toward its anterior inferior quadrant. The nerve was found to end in diverging branches. In the long masseter
type, the course of the nerve was found to run obliquely forward and downward. As it travels downward, the nerve

tends to approach the anterior border, extending to a more inferior level than the nerve of the short masseter type. In
the long masseter type, the nerve most often ends in the anteroinferior segment of the muscle and exhibits a very
limited branching pattern.
POTENTIAL PITFALLS
Although contour defects may result there is little other donor site morbidity following transposition of the masseter
muscle. It has been our experience that this secondary defect is variable and dependent on the regional muscle
anatomy of the individual.
Additional problems in the transfer of the masseter may occur if the muscle's neurovascular pedicle is not
adequately visualized. This can be particularly troublesome when the muscle is approached through an intraoral
incision. This may lead to an inability to obtain adequate hemostasis and also a failure to identify carefully and
preserve the neural supply to the muscle.
The primary arterial supply to the masseter muscle arises from the internal maxillary artery. The venous drainage
is through the facial vein and the pterygoid plexus.
Preoperative assessment of the masseter relies on the clinical demonstration of active contraction of the muscle. Prior
to surgery, the patient should be examined to be sure that the muscle has normal strength and tone. This is particularly
important in patients who have undergone previous skull base procedures in which the viability of the fifth cranial
nerve may be in question. Careful review of prior operative reports is critical to be certain that the vascular supply has
not been compromised.
Post operative wound care
After the muscle is transferred, the face is secured with a bulky compressive dressing. This can be reinforced by the
use of Steri-Strips around the orbicularis oris to add additional support and immobilization to this area. It may be
advisable to use nasogastric feeding during the immediate postoperative period to eliminate additional motion caused
by mastication

VI. DELTOPECTORAL FLAP
The medially based deltopectoral flap, also referred to as the Bakamjian flap, was a major advance in head and neck
surgery when it was popularized in the early 1960s by V. Y. Bakamjian as a solution to the problem of
pharyngoesophageal reconstruction. The design of this flap, with its pedicle based at the sternum, represented a
divergence from the commonly held belief that the midline of the body was a relatively avascular territory. There
remains some controversy as to whether the flap reported in 1917 by Aymard for nasal reconstruction was the first
description of the deltopectoral flap. This flap was again described by Joseph in the 1930s in his book on plastic
surgery. Joseph referred to Manchofs description of the vascular territories of the body and clearly understood the
nature of the blood supply to this flap. For approximately 40 years, the deltopectoral flap remained essentially dormant
in the medical literature until Bakamjian described its versatility and wide application in head and neck reconstruction.
Along with the forehead flap introduced by McGregor, it was the primary method for resurfacing cutaneous and
mucosal defects until the late 1970s when musculocutaneous flaps were introduced. It remains a useful tool in the
reconstructive surgeon's armamentarium, although it has primarily been relegated for use in reconstructing external
cutaneous defects of the neck.
The major disadvantages of this flap include the requirement, in most cases, for a skin graft to close the donor site, and
the unreliability of the distal portions of this flap when extended over the deltoid region.
The deltopectoral flap is a fasciocutaneous flap based on the perforating branches of the internal mammary artery.
Although originally described as having a pedicle based on the first three perforators, it is now most commonly based
on the second and third. When a clearly dominant perforator is present, the entire flap could probably be based on that
single vascular pedicle. Primary transfer of the deltopectoral flap may be performed with a high degree of reliability
provided that it does not extend into the territory overlying the deltoid muscle. Distal flap necrosis occurs with
significant frequency when a flap extending onto the shoulder is raised without prior delay. Flap vascularity and the
reliability of different flap designs are discussed in detail later.

FLAP DESIGN AND UTILIZATION
A variety of different flap designs have been described to reconstruct many different defects in the head and neck.
Greater length and greater diversity can be achieved when a delay procedure is instituted. The body habitus of the
patient greatly influences the arc of rotation of the medially based flap. The optimal situation is a patient with broad
shoulders and a short neck.
There are several different ways to transfer this flap to the recipient site. The bridging portion of the flap can be tubed
over the clavicle and neck skin. A staged secondary procedure is required to either return or excise the tubed
component. Alternatively, the intervening skin between the defect and the clavicle may be excised to allow a one-
stage insertion of the entire length of the flap. Finally, an island flap can be created by de-epithelializing the proximal
portion of the flap, which is then buried beneath the cervical skin between the defect and the clavicle. When buried in
this fashion, a secondary procedure is not required.
Krizek and Robson described the vertically split flap in which an incision is made through the distal end of the skin
paddle creating two separate segments for restoration of the inner and outer lining. This design places less stress on
the vascularity to the tip than de-epithelializing a segment and folding the flap on itself. A transverse fold in the tip of
the flap allows the distal portion to be used for the internal lining of composite defects. However, this technique
requires that a longer flap be harvested, and the distal fold occurs in the least viable portion. Bakamjian et al.
described the L-shaped design of the deltopectoral flap, with the short limb of the L extending downward along the
upper arm. This flap design was used to obtain an inner lining by using a two-stage procedure. In the initial delay
procedure, the upper arm extension was folded under the deltoid component to produce a buried skin flap. The two
epithelial surfaces were then transferred at the time of the second procedure. An alternative solution to the requirement
for a double epithelial surface is the use of a skin graft on the undersurface of the flap. The graft may be buried at the
time of an initial delay procedure.
East et al. described the placement of a fenestration in the distal portion of the deltopectoral flap for reconstruction of
a tracheostoma. Although we would be wary of causing tip necrosis with this technique, the authors advised that the
short arc of rotation required to reach the tracheostoma allows the design of a short flap, and therefore, the fenestra
can be placed in a relatively well-vascularized portion of the flap.
The length of the deltopectoral flap that can be safely transferred without a delay is somewhat controversial. Kirkby
et al. reported that the end of the flap could be safely extended to the tip of the shoulder. When additional length was
required, these authors recommended the creation of a back cut from the inferior limb of the flap across the sternum
and then in a cephalad direction lateral to the contralateral internal thoracic perforators. However, the efficacy of this
maneuver is somewhat controversial in light of the contention of McGregor and Jackson that the arc of rotation of a
deltopectoral flap is more limited by the upper limb of the flap than by the inferior limb, as is most commonly
believed. The rationale for this contention is that the skin of the anterior axillary fold is intrinsically more redundant
than is the skin of the superior limb of this flap, which is located parallel and just inferior to the clavicle. It is easy to
demonstrate the relative redundancy of the skin in the anterior axillary fold by raising an arm above the head. Bilateral
deltopectoral flap transfers have been reported for complex reconstructions or recurrent cancers.
The deltopectoral flap was transferred as a microvascular free flap, as first reported by Harii et al. in 1974 and then by
Fujino et al. in the following year. Fujino et al’s publication described the transfer of a de-epithelialized dermis-fat
flap for augmentation of contour deformities of the head and neck. Percutaneous Doppler sonography was used to
localize the dominant perforator on which to base the flap. The free flap is usually harvested on the second internal
mammary perforator, which is most commonly the largest. The vascular pedicle for this flap is quite short and it is
rarely used for free tissue transfer due to the abundance of other donor sites which are available.

Back cut on the contralateral side of the sternum to improve the arc of rotation
David introduced the concept of an innervated deltopectoral flap for intraoral reconstruction with sensory restoration
reestablished through the supraclavicular nerves of the cervical plexus. Although he noted excellent sensation when
the nerves were mobilized and not transsected, he did not report sensory recovery when the nerves were transsected
and then reanastomosis to recipient sensory nerves in the neck. The potential for transfer of a sensate deltopectoral
free flap is readily apparent. The concept of transferring sensate skin to the oral cavity and pharynx to assist in
postoperative rehabilitation was not pursued until Urken et al. reported the first sensate radial forearm flap in
pharyngeal reconstruction.
The deltopectoral flap has been applied to a wide variety of reconstructive problems in the head and neck. As noted
previously, Bakamjian first described this flap as a solution to the problem of restoring continuity to the gullet
following laryngopharyngectomy. In a landmark publication in 1965, he reported a two-stage technique that involved
the transfer of a tubed deltopectoral flap. Following the initial procedure, a control salivary fistula was created at the
lower end of the tube that was positioned lateral and inferior to the tracheostoma, permitting a safer and more
manageable salivary egress. The stump of the esophagus was sutured in end-to-side fashion to the skin tube. After a 3-
to 5-week interval, the base of the deltopectoral flap was transsected and closed to complete the pharyngoesophageal
reconstruction. Bakamjian and Holbrook later described the use of a staged secondary reconstruction of the
pharyngoesophagus by tubing the deltopectoral flap on the chest wall prior to transfer.
Additional experience with the deltopectoral flap led to its application to intraoral reconstruction of the tongue, floor
of the mouth, tonsil, and pharynx. It has also been widely used for external defects of the neck, cheek, ear, and
mentum. Ingenious techniques, albeit through staged procedures, of reconstructing extensive mid and upper facial
defects have been reported by "waltzing" the pedicle to more cephalad regions. Resurfacing hemifacial and
orbitomaxillary defects have been described. A favorable body habitus and, more often, the institution of a prior delay
are critical to the use of this flap for more cephalad defects of the face. McGregor and Reid described the combined
use of the forehead flap to achieve internal lining and the deltopectoral flap for external lining when reconstructing
through-and- through defects of the cheek. Bakamjian and Poole described the use of the deltopectoral flap for
reconstructing the palate following ablative surgery. In most cases, except where an island flap is created, the use of
the deltopectoral flap for relining any part of the gullet required the creation of a control salivary fistula that was
subsequently closed at the time of returning the pedicle to the chest wall.
NEUROVASCULAR ANATOMY
The blood supply to the deltopectoral flap is derived from parasternal perforators of the internal mammary artery and
vein, which traverse the intercostal interspaces. The 2-cm zone lateral to the border of the sternum should not be
violated when raising this flap to avoid injury to these vessels. The second and third perforators are usually the largest
in size with external diameters in the range of 1.2 mm. The venae comitantes are usually equal or greater in diameter.

The deltopectoral is supplied by internal mammary perforators, which emerge from the second third intercostal
space in the parasternal region
The vessels of the deltopectoral flap run in a plane superficial to the fascia overlying the pectoralis major and deltoid
muscles. Although this flap is most commonly harvested with this fascial layer to protect the circulation, it is not an
absolute requirement to do so.
A number of articles have been written on the nature of the vascular supply to the deltopectoral flap and the
implications for safely harvesting skin overlying the deltoid muscle. A review of the vascular territories of the upper
chest provides a better understanding of the potential problems that may arise when using skin from distal portions of
this flap. The angiosome concept may be applied to this discussion by defining the source vessels that supply the
anterior thoracic skin. The primary region of the internal mammary perforators extends from the lateral border of the
sternum to the deltopectoral groove. This territory is also supplied by musculocutaneous perforators arising from the
pectoralis major. In the region of the deltopectoral groove, there is a direct cutaneous artery arising from the
thoracoacromial system, which supplies a small area of skin below the clavicle. The skin of the deltoid territory, lying
lateral to the deltopectoral groove, is supplied by musculocutaneous branches arising from the deltoid branch of the
thoracoacromial system and the anterior circumflex humeral artery. It is therefore evident that, in raising a
deltopectoral flap, the skin overlying the deltoid muscle and the deltopectoral groove, which were previously supplied
by musculocutaneous vessels and direct cutaneous vessels, respectively, must now be captured and made exclusively
dependent on the internal mammary perforators. In the angiosome model described by Taylor et al, the blood supply
to skin in immediately adjacent angiosomes is usually quite reliable. However, the pressure gradient of the nutrient
flow diminishes as one move to the angiosome next in line, or "once removed," from the primary source vessel. The
skin overlying the deltoid muscle is an angiosome once removed from the internal mammary angiosome, and
therefore, that skin is at risk for partial or total necrosis. It is possible that the variable pattern of reliability of the tip of
the deltopectoral flap is a function of the size of the acromiothoracic angiosome that is the middle territory in this
series. With a larger and more dominant cutaneous branch from the acromiothoracic axis, the deltoid skin may be
rendered less reliable.
The angiosome concept provides a framework for describing delay procedures that are used to increase the reliability
of the deltoid skin. To capture the blood supply of that territory, it is essential to reverse the direction of flow in the
adjacent thoracoacromial angiosome and the third angiosome in line overlying the deltoid region. It is critical that the

direction of flow across the choke arteries that connect adjacent angiosomes be uniformly oriented from the sternum to
the tip of the shoulder. The most promising delay procedures are those that interrupt the source arteries and veins in
the intermediate and distal angiosomes to allow reversal of flow and more favorable pressure gradients. This was
demonstrated by the fluorescein injection studies of McGregor and Morgan. A successful delay procedure for the
deltopectoral flap must interrupt the direct cutaneous branch of the thoracoacromial system and the distal
musculocutaneous branches of the deltoid achieved by raising the tip of the flap lateral to the deltopectoral groove and
undermining in the infraclavicular fossa.
The sensory nerve supply to the deltopectoral skin is derived from the supraclavicular nerves of C-3 and C-4 and the
anterolateral intercostal nerves of T-2, T-3, and T-4. The ability to maintain the sensory supply intact largely depends
on whether a radical neck dissection is performed. As noted previously, the report by David of a sensate deltopectoral
flap was the first successful restoration of sensation to the reconstructed oral lining.
OPERATIVE PROCEDURE
Pertinent Anatomy
1. Skin paddle
a. Covers the anterior-superior chest wall extending over the anterior shoulder from the clavicle to a line
drawn from axilla to fifth thoracic interspace. The lateral extension extends over the anterior deltoid
muscle. The blood supply to the extension of this flap beyond thoracoacromial artery and deltopectoral
groove is nonaxial and becomes random pattern. The risk of skin necrosis increases the farther onto the
shoulder the flap is extended. Flap failure is also increased if the perforating arteries are traumatized
during elevation and if the flap is placed under tension during its rotation and inset.
2. Blood Supply
a. Perforator arteries from the internal mammary artery that reach the skin paddle as they exit the chest
between the ribs along the sternum
b. Flap Elevation
i. The flap is outlined over the anterior chest wall and shoulder as noted above. The plane of
elevation is deep to pectoral and deltoid muscle fascia. Muscle fibers will be exposed as the flap is
elevated. Elevation should end 2 cm lateral to the sternal border taking care to avoid injury to
perforating arteries. Branches from thoracoacromial artery, which perforate through the pectoralis
major muscle laterally, are cut during elevation.
ii. Good tissue technique is required. Handle the flap with toothed pickups, skin hooks, or suture.
Avoid excessive use of monopolor electrocautery.
iii. Do not overly rotate, kick, or compress the proximal flap.
iv. To improve the survival of the distal portions of the flap, a delay technique may be valuable.
3. Closure
a. Donor site is covered with a split thickness skin graft; 0.015-inch thick and meshed 2:1. The skin graft is
placed with an emphasis on lateral shoulder coverage. If the flap is to undergo secondary transection, the
medial portion will return to the chest wall.
b. Close wound edge with standard deep (3-0 vicryl) and skin sutures (surgical clips, or 4-0 to 5-0 nylons).
4. Drains
a. A superficially placed (skin out) deltopectoral flap can be completed with a water-tight/air-tight closure
and can suction drains are usually placed.
b. A Penrose drain may be place under the rotated flap when a water-tight/air-tight closure is not obtained.
5. Dressing
a. Ointment is applied to chest incisions.
b. The skin graft site requires a light bolster dressing of fine mesh Xeroform gauze and gauze fluffs,
followed by Montgomery straps or silk tie down sutures. The dressing is moistened with saline.
6. POSTOPERATIVE CARE
a. Dressings

i. The skin graft bolster is removed on postoperative day 5 to 7. Keeping the dressing moist with
sterile saline may increase skin graft survival.
ii. Flap Monitoring
iii. No straps, ties, or cords should cover or compress the flap. It may be useful to write on the flap
itself and place a sign at the patients bed side: "No ties around patient's neck." The flap is
monitored by observation of color and needle prick bleeding. Pressure points and excessive torque
should be assessed and improved if possible. Distal sutures may need to be removed to decrease
the flap tension if flap blood supply appears compromised. Poor flap appearance may potentially
be improved with the use of IV dextran, steroids, and/or hyperbaric oxygen.
b. Proximal (Pedicle) Transection
In our current practice, transection of the base of the deltopectoral flap is rarely needed for its most common
uses (ie, skin or carotid coverage). When the flap is "walked" up from the chest to close a defect of the upper
aerodigestive tract, the proximal portion of the flap is returned to the chest after three to six weeks, at which
time the fistula is closed.
7. DELAY TECHNIQUES
i. This flap may be delayed to increase its survival after rotation. The most common method is to
complete the skin incisions and elevate the distal two-thirds of the flap. The skin flap is then
returned to its normal anatomic position. After 10 to 14 days, it is re-elevated and rotated into the
reconstructive position.
ii. Additional advantage may be gained by placing a split-thickness skin graft on the shoulder and
chest wall under the flap at the time of primary elevation.
POTENTIAL PITFALLS
The technique of deltopectoral flap harvest is so straightforward that it is rare to encounter problems leading to total
flap necrosis. The problem of partial tip necrosis has varied in different series, depending on the length of the flap and
the use of a delay procedure. Park et al. warned that factors contributing to flap loss included diabetes, wound
infection, and a radiated recipient bed. In a series of 51 deltopectoral flaps placed in irradiated beds, Krizek and
Robson reported only five major complications. Kirkby et al. noted an overall total flap failure rate of 26%, which
required secondary reconstructive procedures. Higher rates of flap failure were noted in flaps placed for internal lining
and for flaps used in an irradiated field. The total flap failure rate of 26% was considerably greater than that reported
in other large series, e.g., 9%, 12%, 16%, and 14%. Minor complications that did not require additional surgery ranged
from 14% to 26%.
Although extension of the flap over the deltoid leading to distal ischemia is the most common cause of partial
necrosis, there are a variety of other etiologic factors that have been implicated, e.g., placement of the flap over a
mandibular K wire, folding of the flap for inner and outer lining, head movement causing flap tension or kinking, and
inadequate oro- or pharyngostomal aperture through which to pass the deltopectoral flap for mucosal replacement. The
wide array of flaps that is available for oral and pharyngeal defects have limited the current role of the deltopectoral
flap to reconstruction of cervical cutaneous defects. For this purpose, the deltopectoral flap should be considered a
highly reliable technique.

VII. LATISSIMUS DORSI The latissimus dorsi myocutaneous flap was first myocutaneous flap described. Its use was reported by Tansini in
1896 for coverage of chest wall following radical mastectomy. the original description of the of the se of latissimus
dorsi myocutaneous flap in head and neck reconstruction was by Quillen et al in 1978.
The latissimus dorsi muscle, with its long vascular pedicle, can be converted to a flap of considerable length that,
combined with the substantial bulk and reliable vascular supply of the muscle, makes this muscle ideal for major head
and neck reconstruction Moreover, The length and diameter of the primary vascular supply allow the fashioning of an
excellent free flap.
Indications
The latissimus dorsi has proved to be especially useful in resurfacing the defects of check and lateral scalp. Although
most of neck can be reached for coverage by latissimus dorsi, the pectoralis major is generally preferred for neck and
intraoral reconstruction. The latissimus dorsi is used in this area when great deal of bulk or skin or both are needed.
Anatomy
The latissimus dorsi muscle is supplied by the thoracodorsal artery and vein. The thoracodorsal artery is terminal
branch of subscapular arterial system. There are two major arterial branches from the thoracodorsal artery that may
require ligation prior to rotation of flap- the angular artery which supplies the tip of the scapula, and a branch to the
serratus muscle.
The thoracodorsal artery consistently branch in to a medial and lateral component. The lateral branch is typically the
larger branch of the two. It parallel lateral margin of the muscle 1-4cm from the lateral margin of the muscle. The
medial branch generally travel 45 degree superior to the lateral branch. This anatomy allows splitting of the flap
depending upon the requirement of the defect.
The latissimus dorsi muscle arises from the lower six thoracic vertebrae, the lumbar vertebrae, the sacral vertebrae, the
tip of the scapula and the posterior iliac crest. The muscle has singular insertion on the humerus in the intertubercular
groove.
The muscle is thin and as a surface of 40 x 25 cm. the posterior axillary line serves as the important landmark for
identification of the muscle.
Operative Technique

The patient position is critical. The lateral decubitus position is used. Careful padding of the contralateral axilla is
necessary to prevent brachial plexus injury. The posterior axillary fold, spinous process of the lower six thoracic
vertebrae to the sacrum, the posterior iliac crest and tip of the scapula are marked out. A vertical line is drawn from
the superior extent of the posterior axillary fold to the midpoint of the posterior iliac crest.
An incision is made just beyond the free edge of the muscle to expose the vascular pedicle. The incision is carried
posteriorly to join the incised skin island, which is sutured to the muscle fascia early in the procedure to avoid
shearing any musculocutaneous perforators. The pedicle can be dissected up to the axillary vessels, dividing the
circumflex scapular vessels if necessary. The nerve also may be divided to cause later atrophy of the muscle that will
create better contour. The muscle is dissected superficial to the serratus anterior and the scapula. If a transfer of
vascularized rib is planned, the perforator to the rib is preserved; otherwise, all the posterior vessels are divided.
A tunnel for the passage of the flap into the neck is made in a subcutaneous plane over the pectoralis major muscle or
below the pectoralis major muscle but superior to minor muscle
. The tunnel must easily allow passage of the width of the hand to allow for adequate laxity without compression of
the vascular pedicle. The donor site is closed over a large suction drain in two layers. Primary closure is achieved if
the width of the harvest is limited to 10cm.
By severing the circumscapular artery the flap can be elevated to the vertex of the skull. This action can sometimes
result in the kinking of the thoracodorsal artery.
Modifications of the flap include its harvest as a muscle only flap or as a compound flap with the harvest as a muscle
only flap or as a compound flap with the harvest of the 10th rib.


VIII. TEMPOROPARIETAL FLAP
History
In 1898, the temporoparietal fascia flap was described nearly simultaneously for reconstruction of the external ear
(after a horse bite [Brown, 1898]) and for reconstruction of the lower eyelid (Monks, 1898). Despite these descriptions
of its utility for head and neck reconstruction, the flap remained an obscure and underused tool until an explosion of
new descriptions of its use (as either a pedicled or a microvascular free tissue transfer) resurrected it during the past 2
decades. In 1983, Brent et al reported the successful use of the flap as an axial-pattern fascial flap, a random-pattern
fascial flap, and a free fascial flap for secondary ear reconstruction, and in 1993, Cheney et al described 21 cases using
the flap for a variety of reconstructions in the head and neck. Today, the temporoparietal flaps remain the only single-
layered fascia flap that can be used as a pedicled vascular flap in the head and neck. The flap is thin and pliable, and it
readily accepts a skin graft. Temporoparietal flaps can drape into concavities and over convexities, such as those
present in the external ear, and they are highly vascular and resistant to infection. This reliability and versatility,
particularly in the setting of trauma and devascularized tissue beds, make it a flap limited only by the surgeon's
imagination.
Temporoparietal fascial flaps have been described for vascularized soft tissue coverage in a remarkable variety of
head and neck defects as follows:
Pedicled fascial flap for auricular reconstruction (primary and secondary)
Pedicle for vascularized calvarial bone grafts
Composite skin and cartilage graft from helical root for alar reconstruction
Composite fascia and hair-bearing skin for scalp and lip reconstruction, soft tissue filler in temporal and
parotid defects
Microvascular free tissue graft - Microvascular anastomosis use with or without a vein interposition graft to
obviate the limitation of the pedicle
Coverage of large scalp defects
Coverage of contralateral temporal defects

Double-layered fascial graft - Another description of the temporoparietal flap when it is harvested with
temporalis muscular fascia supplied by the middle temporal artery (This flap can accept cartilage and bone
grafts placed in the envelope between the 2 layers of fascia.)
Nasal reconstruction
Oral reconstruction
Relevant Anatomy
The relevant anatomy of the scalp is emphasized to every medical student with the following mnemonic:
S - Skin
C - Subcutaneous tissue
A - Aponeurosis and occipitofrontalis muscle
L - Loose subaponeurotic tissue
P - Pericranium
In the temporoparietal region, this mnemonic is an oversimplification. The literature surrounding this anatomy
contains a jumbling of nomenclature describing the various layers of temporal fascia, which can further frustrate
surgeons trying to master this flap.
To be accurate, the scalp in the temporoparietal area consists of more than 5 separate layers, and significant creativity
would be required to massage the mnemonic SCALP from them.
The first layer consists of the skin and subcutaneous tissue. Immediately deep and firmly bound to this layer is the
temporoparietal (sometimes called superficial temporal) fascia. This layer is contiguous with the superficial
musculoaponeurotic system (SMAS) as it passes over the zygomatic arch into the mid face, and it is contiguous with
the galea aponeurotica above the superior temporal line.
Beneath the temporoparietal fascia lies a loose areolar and avascular tissue layer that separates the fascia from the
temporalis muscular fascia (sometimes termed the deep temporal fascia). This areolar layer allows the superficial
scalp to move freely over the deeper and more fixed temporalis muscular fascia, temporalis muscle, and pericranium.
Confusing the issue further is the division of the temporalis muscular fascia as it splits into a superficial and deep layer
(of the deep temporal fascia) surrounding a fatty tissue pad at the temporal line of fusion, approximately 2 cm above

the zygomatic arch. The temporalis muscular fascia is contiguous with the pericranium above the superior temporal
line and is contiguous with the masseter muscle fascia below the arch.
The superficial temporal artery supplies the temporoparietal fascia flap. The artery emerges from the parotid tissue,
gives off the middle temporal artery, and traverses a tortuous course in the preauricular area. Approximately 3 cm
above the zygomatic arch, it divides into the terminal frontal and parietal branches. The superficial temporal vein
generally runs superficial to and with the artery, but variability, including branching or a posterior course, may be
encountered.
The auriculotemporal nerve, a sensory branch of the mandibular nerve, lies posterior to the superficial temporal artery
within the temporoparietal fascia. The frontal branch of the facial nerve traverses an oblique course over the
zygomatic arch, which can be estimated by a line connecting a point 0.5 cm inferior to the tragus to a point 1.5 cm
lateral to the superior brow. This nerve also lies within the temporoparietal fascia, and flap elevation anterior to the
frontal branch of the superficial temporal artery should proceed with caution to avoid injuring this nerve.
Contraindications
Although the temporoparietal fascia flap is highly vascular and reliable, prior injury to the temporal field could result
in flap necrosis. Radiation therapy, trauma, or previous surgery around the superficial temporal arteriovenous supply
may increase the risk of flap necrosis and should be considered relative contraindications. Preoperative Doppler
assessment of the superficial temporal artery and its branches can confirm vascular flow to the flap. Significantly, in a
1985 report, Brent has described successful elevation and skin grafting of a random temporoparietal flap in a
secondary microtia reconstruction when no axial vessels could be identified by Doppler assessment or surgical
dissection.
Prior trauma to the area may also increase the risk of postoperative alopecia, which is, which is always a risk anytime
this flap is harvested.
Preoperative details
Trauma, previous surgery, irradiation, or carotid occlusion may jeopardize the integrity of the temporoparietal fascia
flap. Doppler ultrasonography should be used preoperatively to determine the reliability of the superficial temporal
artery and to map the course of the main pedicle, frontal branch, and parietal branch.
Intraoperative details
The face and scalp are prepared and draped. The flap can usually be harvested without shaving hair if the hair is
carefully prepped out of the field with ointment and tape or rubber bands.
The important topography of the temporoparietal flap to mark on the scalp includes the superior temporal line, the
course of the superficial temporal artery trunk and the frontal and parietal branches, and the approximate course of the
frontal branch of the facial nerve. The incision is marked as a vertical incision from the root of the helix to the superior
temporal line. This incision can be extended as a V superiorly to gain additional access to the galea. The preauricular
portion of the incision is extended as a face-lift incision around the tragus as necessary.
The anterior and posterior scalp flaps are elevated in the subcutaneous plane immediately deep to the hair follicles.
The temporoparietal fascia adheres to this subcutaneous tissue,

and meticulous sharp dissection is necessary to avoid injuring either the vascular supply of the flap or the hair
follicles.
The frontal branch of the superficial temporal artery and the anterior edge of the flap are ligated. As with any frontal
dissection in the superficial planes, care should be taken anterior to this point to avoid injury to the frontal branch of
the facial nerve. If dissection becomes necessary anterior to this point, then the frontal branch should be identified and
carefully preserved.
After elevation of the skin flaps, the superior, posterior, and anterior edges of the flap are divided. A flap measuring
up to 17 X 14 cm can be harvested without extensive scalp undermining. The dissection then proceeds from superior
to inferior by dissecting the loose areolar tissue between the 2 layers of fascia. This plane is avascular and easily
identified, and dissection can proceed quickly during this portion of the operation.
As the surgeon approaches the root of the helix, dissection must proceed carefully to avoid injury to the vascular
pedicle. The pedicle is identified, and the flap base is narrowed to 2.0-2.5 cm, if necessary, to improve rotation.
Dissection inferior to the root of the helix is limited by the parotid gland and the risk of injury to the main trunk of the
facial nerve. As mentioned previously, 2 layers of vascularized fascia can be harvested by identifying and carefully
dissecting the temporalis muscular fascia with its nutrient middle temporal artery. The artery can be followed to its
origin from the superficial temporal artery in the region of the zygomatic arch.
The flap is draped carefully into the recipient site and fastened to the surrounding skin and soft tissue. The pliability of
the flap makes it uniquely suited to draping over irregular surfaces. A skin graft may be applied to the flap and held in
place with sutures and suction drainage. The wound is dried carefully with cautery and then irrigated. Suction drainage
is placed in the superior donor site away from the pedicle, and the wound is closed in layers. A pressure dressing is
applied to the scalp for 12-24 hours.

COMPLICATIONS
1. Alopecia
Alopecia is more common in the setting of scalp tissue previously compromised by trauma, irradiation, or surgery.
The surgeon can reduce the incidence of this complication by meticulous elevation of the scalp flaps in the proper
plane immediately deep to the hair follicles. Cauterization of the skin edges and hair follicles should be minimized.
2. Hematoma
3. Flap necrosis
Complete failure of this flap is rare, even in the presence of poor wound vascularity and contamination
IX. PLASTYMA MYOCUTANEOUS FLAP
A cervical apron flap was described by Ward and Hendrick in 1950 for reconstructing oral cavity defects. These
surgeons actually used a skin paddle based on the platysma muscle. A 1978 article byFutrell et al recognized this
and described the use of the platysma flap for reconstructing oral defects. Numerous articles were published in the
1980s on the use of this flap for oral or facial reconstruction. Nevertheless, with the advent of microsurgery in the
late 1980s and early 1990s, enthusiasm for the flapwaned. In 1997, Ariyan rekindled interest in the posteriorly
based version of the flap because of his dissatisfaction with the color match of the radial forearm Flap.
The advantages of the platysma flap include good color match, easy access to the donor site in the same operative
field, minimal donor site morbidity, ease in closing the donor site primarily, and appropriate flap thickness for oral
or facial defects (thin and pliable skin). Use of this flap results in minimal contour and mobility changes of the
neck. Donor site scarring is minimal and well accepted. The platysma flap can reliably be used even when an
ipsilateral neck dissection is performed, aslong as the surgeon takes care to preserve the vascular pedicle during
the dissection. When compared with the radial forearm microvascular free flap, the platysma flap has a better
color match, can be harvested in much less time 30min approx, and has significantly less donor site morbidity.
When compared with the pectoralis major myocutaneous flap, the platysma flap is less bulky, has a better color
match to facial skin, and is faster and easier to harvest with less morbidity. It provides for 70cm2 of tissue and the
procedure for harvesting is not technique sensitive.
Indications
i. The platysma flap may be used to close defects on the low er face, buccal mucosa, and floor of mouth.

ii. In selected cases, the flap w ill ex tend to the oropharynx ; how ever, depending on the body habitus of the
patient, closure of defects in the oropharynx may require excessive tension on the flap.
iii. The flap is ideally suited for reconstruction of deep chin and low anterior cheek defects in patients not
requiring neck dissection. The color match is good w ith facial skin. When used to resurface these areas, a dual
blood supply including the submental and superior thyroid arteries may be preserved.
Contraindications
i. Prior radiotherapy to the neck w ill significantly compromise the viability of the flap.
ii. The main blood supply to the flap derives from the submental branch of the facial artery and a cutaneous
branch of the superior thyroid artery. Neck dissections that interrupt these vessels are a relative contraindication
to the use of this flap.
iii. The flap is relatively thin, and the need for tissue bulk is a contraindication to the use of this flap.
iv. Flaps as large as 7 x 10 cm may be harvested in selected individuals; however, if the defect siz e is larger than
5 x 7 cm, an alternative reconstructive method should be considered.
v. Patients with extremely thin skin and a poorly-developed platysma muscle are not ideal candidates for this
procedure.
vi. The flap should not be used if the sternocleidomastoid muscle w ill be removed as a part of the planned neck
surgery.
Anatomy
The thin quadrangular-shaped, paired platysma muscles lies in the superficial fascia of the neck. The muscle
originates in the superficial fascia of the pectoral and deltoid muscles, coursing obliquely over the clavicle to its
insertion at the corner of the mouth and inferior part of the cheek. Immediately deep to the platysma is the superficial
layer of deep cervical fascia. Fibers of the platysma interdigitate with angle and depressor muscles of the lip and chin.
Theanterior fibers decussate over the chin with the contralateral platysma. When the muscle contracts, it pulls the
corner of the mouth inferiorly and laterally, partially contributing to mouth opening.
Branches of the transverse cervical artery supply the platysma muscle inferiorly. From the posterior triangle of the
neck, the muscle receives branches from the occipital and posterior auricular arteries. The superior thyroid artery
perfuses the muscle from the anterior triangle of the neck. Fasciocutaneous arterial perforators from the muscle itself
supply the overlying skin. At the posterior extent of the muscle lies the external jugular vein, providing for venous
drainage. The anterior jugular veins, the submental vein, and the anterior communicating veins also contribute to
venous drainage. Innervation of the platysma muscle is from the cervical branch of the seventh cranial nerve. These
branches are generally multiple and enter the muscle on the deep surface from a superior direction. The marginal
mandibular branch of the facial nerve is also found deep to the platysma, usually at or near the inferior border of the
mandible.

The posteriorly based platysma flap can be used with a supraomohyoid neck dissection or a selective neck dissection
that maintains the sternocleidomastoid muscle and its associated fascia, which contains the vascular supply to the
platysma.
Technique, The patient’s neck should be hyperextended. The skin paddle is marked on the ipsilateral submental area,
approximating the size of the defect. When designing the flap size, the surgeon must allow for a small amount of
primary contracture of the skin paddle. In either version of the platysma flap, the skin paddle can be outlined
anywhere within the limits of the muscle. The long axis of the skin paddle should be perpendicular to the muscle
fibers. The skin paddle should not cross the midline of the neck to avoid loss of skin at the distal aspect of the flap.
Typically, the skin paddle is elliptical in design, but other shapes can be used, depending on the nature of the defect .
The outlined skin paddle is incised, leaving the platysma muscle intact. A single horizontal incision extending
posteriorly from the already incised skin paddle is made through skin and subcutaneous fat to the level of the platysma
muscle, without damaging the muscle. This horizontal incision extends posteriorly past the anterior border of the
sternocleidomastoid muscle. Initially, the dissection proceeds cephalad with the elevation of a superior skin flap in the
supraplatysmal plane to the inferior border of the mandible. In a similar manner, an inferior skin flap is elevated.
One should visualize almost the entire platysma muscle and the anterior border of the sternocleidomastoid muscle. The skin paddle of the flap should be surrounded by at least 1 cm of platysma muscle circumferentially. Maintain the pedicle with a width of at least 3 to 4 cm in a superoinferior direction to provide an adequate number of arterial andvenous perforators.Once the platysma muscle is fully exposed, mobilization of the myocutaneous flap can be accomplished. The platysma is transected superiorly for its entire anteroposterior length, just below and parallel tothe inferior border of the mandible. Care should be taken to avoid the marginal mandibular branch of the facial nerve, which lies in fascia deep to the platysma. In a similar manner, the muscle is horizontally transected inferiorly, parallel to the superior incision, maintaining at least 3 to 4 cm of pedicle width. Anteriorly, any remaining tissue attachment of the muscle is excised. Posteriorly, the flap is now pedicled on the fascia associated with the sternocleidomastoid muscle, in which the vascular supply lies. At the base of the flap, the external jugular vein should be maintained for venous drainage. Once fully mobilized, the flap can be rotated into a defect through a subcutaneous tunnel or into the oral cavity. The donor site is closed in layers after a suction drain is placed. A Burow’s triangle typically forms at the midline of the neck and often needs to be revised.

III. Superiorly based flap, The dominant blood supply of the superiorly based platysma flap is from the submental branch of the facial artery at or near the inferior border of the mandible, whereas venous drainage is from the submental vein. The submental artery makes numerous anastomoses with the ipsilateral and contralateral lingual, inferior labial, and superior thyroid arteries although it is desirable to preserve the facial artery, the flap will usually do well even when the ipsilateral facial artery is ligated. The arc of rotation is suitable for reconstruction of the anterior and lateral floor of mouth, buccal mucosa, retromolar trigone, and skin of the lower cheek and parotid region. Motor innervation of the flap may be preserved by maintaining the cervical branch of the facial nerve, assisting with facial animation.
Technique, With the neck hyperextended, the proposed skin paddle is outlined on the ipsilateral neck, caudal to the inferior border of the mandible (Fig. 2). The superior incision is made first, and a dissection plane superficial to the platysma muscle is carefully developed cephalad to the inferior border of the mandible. A skin incision is then made at the inferior limb of the skin paddle, with additional exposure of the platysma muscle inferiorly. The platysma muscle is transected sharply at least 1 cm inferior to the edge of the skin paddle, with the subsequent development of a subplatysmal plane of dissection cephalad to just below the inferior border of the mandible. If the cervical branch of the facial nerve is to be incorporated, one must identify the nerve in the superficial layer of deep cervical fascia and carefully dissect and preserve the proximal portion of the nerve. Once both planes of dissection are fully developed, the platysma must be transected vertically, anteriorly and posteriorly, for full mobilization of the flap. As is true for the inferiorly based version, the flap can be introduced into the facial or oral defect by creating an appropriately sized soft tissue tunnel. This tunnel should be of adequate width to avoid strangulating the flap. Care should be taken to avoid twisting the flap or applying excessive traction, which could compromise the vascular supply. The donor site can usually be closed in layers with little difficulty to obtain an acceptable cosmetic result.
Complication of this flap surgery is vascular compromise. If the dominant arterial supply is lost, all or a portion of the flap will die. Unlike in other axial pattern flaps, such as the pectoralis major flap, the dominant artery is usually not visualized and typically not mapped with a Doppler study. By carefully staying within the dissection planes and being thoroughly familiar with the anatomy, the surgeon should be able to maintain the integrity of the arterial supply. If in the postoperative period the flap appears white with minimal capillary refill, urgently taking the patient back to the operating room will not likely be of benefit, as long as the surgeon is confident that the pedicle was not twisted, strangulated, or excessively stretched.

COMPLICATIONS AND THEIR MANAGEMENT
Potential complications following the use of local skin flaps include infection, hematoma, ischemia, flap necrosis
(most frequently partial necrosis of the distal flap/tip necrosis), dehiscence, and an undesirable cosmetic result.
Cyanosis of flaps occurring in the immediate post-operative period is usually secondary to insufficient venous
drainage. Signs include an edematous, purplish or bluish flap with dark colored blood on pinprick. In this case,
tight sutures should be removed. In some cases it may be worthwhile to explore the vascular pedicle to see if it is
kinked or being compressed by a hematoma. In addition, multiple punctures may be made with a 22-gauge needle
to relieve venous hypertension. One can also apply heparin-soaked gauze or medicinal leeches. If medicinal
leeches are applied, antibiotic prophylaxis should be administered to prevent Aeromonas infection.
Signs of ischemia (arterial insufficiency) include a pale flap with poor capillary refill, decreased temperature, and
an absence of bleeding with pinprick. Flaps can withstand arterial insufficiency for up to 13 hours, but venous
congestion can kill a flap within 3 hours. If arterial insufficiency is due to mechanical pressure, one can loosen a
wound dressing, drain a hematoma, or correct a kinked pedicle. Delaying the inset of a flap is beneficial only if
insufficient perfusion is determined before leaving the operating room; otherwise, returning the flap to its original
position may not achieve anything other than a necrotic flap in its original position.
Hyperbaric oxygen (HBO) is an important means of combating flap ischemia, demonstrating proven benefit in both
animals and humans. HBO involves the systemic delivery of 100% oxygen at 2-3 times atmospheric pressure. HBO
results in an increased amount of dissolved oxygen in plasma, which results in a 10-20 fold increase in oxygen
levels in the tissues. In order for HBO to work, the patient must have a competent cardiopulmonary system for
oxygen delivery. Transcutaneous oxygen measurements (TCOM) predict the success of hyperbaric oxygen in a
given patient. TCOM at room air is compared to TCOM with the patient breathing 100% oxygen. If there is an
increase, then the patient is likely to benefit from HBO. HBO is thought to be effective because it stimulates
capillary ingrowth, decreases tissue reperfusion injury, and induces vasoconstriction in healthy tissue (decreasing
edema) but not ischemic tissue. More importantly, HBO is thought to decrease hypoxia and retard cellular death
until the first 72 hours have passed and neovascularization has begun. In humans, HBO has demonstrated a 90%
salvage rate when performed 1-2 times per day for 3-5 days.
Complications of HBO include barotrauma to the middle ear, pneumothorax, seizure, pulmonary toxicity, myopia
(which typically resolves within 6 months following treatment), and an increased rate of cataract formation
(particularly in patients with preexisting cataracts). The incidence of oxygen-induced seizure is approximately
1:10,000 patients. Relative contraindications to HBO include emphysema, chronic lung disease, and seizure
disorder. Patients with a history of seizure disorder must be maintained on antileptic medications during HBO.The
risk of flap necrosis is increased in the presence of tension. Transposition flaps in general result in less tension on
the distal flap as compared to other types of flaps. In addition, thickening a flap may be more helpful than widening
the base of a flap in preventing tip necrosis. At the end of a case, the flap should be pink and capillary refill
immediate. In progression to necrosis, blanching and capillary refill become progressively more prolonged until
there is no capillary refill at all. The natural course of this process without intervention will move from ischemia to
cell death to superficial and/or full thickness eschar formation, to separation of the eschar, to healing by secondary
intent. Absolutely no debridement should be performed until the wound has marginated and the eschar has begun to
slough on its own. If managed conservatively, the eschar will act as a biological dressing. In cases of partial
necrosis of the distal flap, local wound care is typically all that is needed. Debridement is rarely, if ever needed. Of
course, another reconstructive surgery is always an option if more conservative measures fail.
Infection is relatively rare in head and neck local flaps because of the rich blood supply in the region. However,
the results of infection can be devastating, leading to dehiscence, widening or thickening of scar, flap necrosis, and
sepsis. Prevention of infection is paramount by observing sterile technique, employing gentle tissue handling,
avoiding aggressive hemostasis, performing a tension-free closure, and cleansing the wound postoperatively with
hydrogen peroxide (crusts enhance local bacterial load). Staph Aureus is the most common single pathogen
isolated from infected wounds. Antibiotic prophylaxis has proven effective for clean-contaminated surgery (e.g.,
delayed wound closure), but not necessarily for clean wounds. Infection typically presents around post-operative

day 3 to six. Appropriate management should include opening of a small area of the incision with drainage of pus.
The drainage should be sent for culture and sensitivities and the patient started on antibiotics. A wick and/or
packing should be placed in the wound until no more drainage occurs.
A hematoma may also lead to disastrous results. The most common causes of excessive bleeding leading to hematoma
include inadequate hemostasis at the time of surgery and drug-induced coagulopathy. Medications associated with
increased bleeding include aspirin, non-steroidal anti-inflammatories (NSAIDs), and herbal remedies (e.g., Vitamin E,
garlic, and feverfew). To be absolutely safe, the patient should be instructed to eliminate these medications for 2
weeks before and 1 week after the flap. For intraoperative control of bleeding, careful and selective electrocautery
should be the first step. If this does not work, then reverse Trendelenberg positioning and the application of cotton
pledgets soaked with an anesthetic combination containing epinephrine along with gentle pressure can be tried. If
oozing still occurs, then a sterile rubber band drain may be left in place overnight and the patient held for observation.
Administration of antiemetics and elevation of the head of the bed are helpful in the recovery room. If significant
bleeding occurs in the recovery room, the wound should be explored and hemostasis obtained. Hematomas cause
increased tension on the wound closure (potentially resulting in ischemia and dehiscence), increased risk of infection,
and an inflammatory response that directly interferes with flap circulation. Evacuation is easiest within the first 1 -2
days by creating a small opening and performing manual compression and lavage. Alternatively, a 22-gauge needle
and a 10-cc syringe may be tried first. If bleeding persists despite these measures, then the wound must be
reexplored. Beyond 2 days, the clot organizes and evacuation may require mechanical debridement. Resorption of
the hematoma begins after 10-14 days.
Dehiscence typically results from hematoma, infection, or tip necrosis, or from dynamic facial movement. The wound
is weakest at 1 week when inflammation subsides and collagen deposition begins. This is also approximately the time
of suture removal, thus it is prudent to apply steri-strips at the time of suture remove to bolster the wound. If
recognized within 24 hours, a simple dehiscence can be repaired. Otherwise, it is best to allow either an old
dehiscence or a complicated dehiscence to heal by secondary intent.
Several options exist for an undesirable scar or cosmetic result. Dermabrasion is good for smoothing height
differences between the flap and surrounding skin. It is especially useful in areas with thick, sebaceous skin such as
the nasal tip. The best results are obtained at 6-9 weeks post-operatively, when fibroblast activity is greatest.
For trapdoor defects, hypertrophic scarring, and keloids, steroid injection (kenalog-40) every six weeks may be
helpful. By definition, hypertrophic scars are confined within the original wound, while keloids extend beyond the
original wound.
Scar contracture is a normal event. However, it can lead to functional and/or cosmetic deformities when contracture
results in tension on free edges (e.g., ectropion, nasal ala asymmetry, etc.). If this occurs, the problem should be
corrected sooner rather than later. Avoidance is important and may be achieved via a tension-free closure and the
replacement of cartilage support when cartilage has been removed.
Surgical scar revision is another option. This is best delayed for at least 6 months, although scars tend to improve over
a course of 1-3 years, so it may be appropriate to wait longer. Simple excision of a scar is good for widened scars that
parallel RSTL or lie within the junction of aesthetic units. Long, straight scars may be excised and revised with a W-
plasty or geometric broken line closure. A Z-plasty is useful in lengthening and changing the direction of a scar,
which is very helpful in revising contracted scars. A Z-plasty can also be performed at the initial reconstruction to
ensure the long axis of the incision parallels the RSTL.
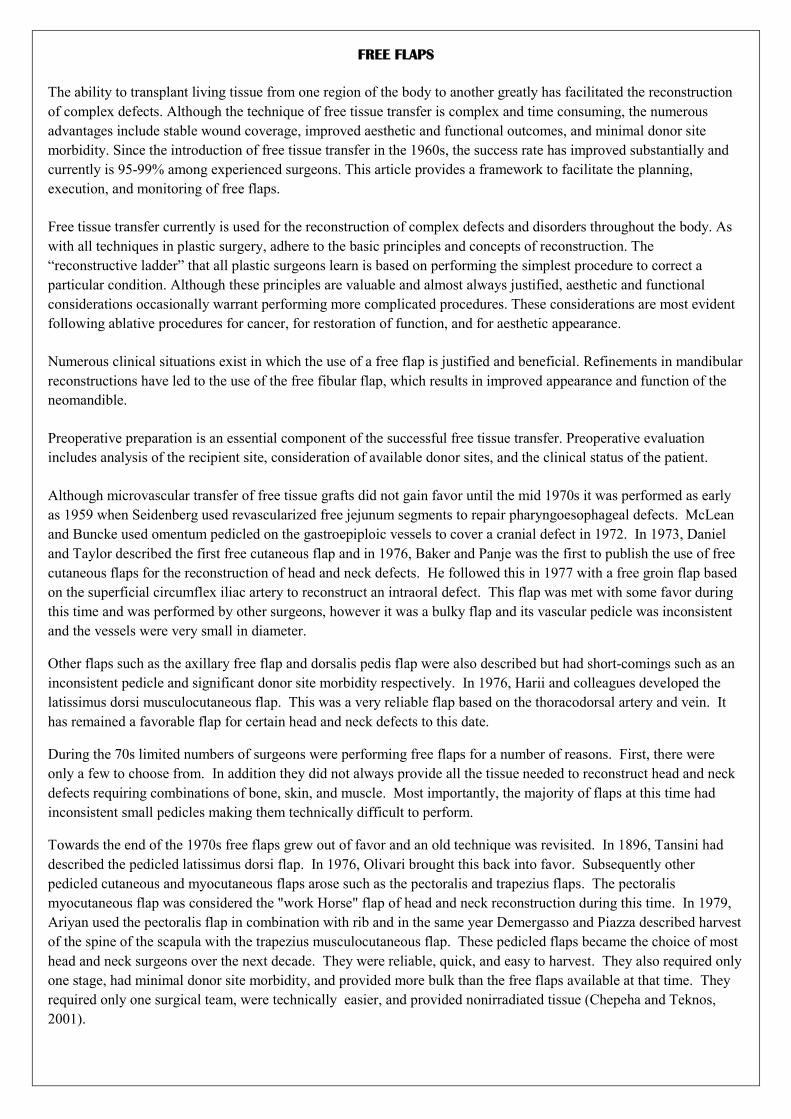
FREE FLAPS
The ability to transplant living tissue from one region of the body to another greatly has facilitated the reconstruction
of complex defects. Although the technique of free tissue transfer is complex and time consuming, the numerous
advantages include stable wound coverage, improved aesthetic and functional outcomes, and minimal donor site
morbidity. Since the introduction of free tissue transfer in the 1960s, the success rate has improved substantially and
currently is 95-99% among experienced surgeons. This article provides a framework to facilitate the planning,
execution, and monitoring of free flaps.
Free tissue transfer currently is used for the reconstruction of complex defects and disorders throughout the body. As
with all techniques in plastic surgery, adhere to the basic principles and concepts of reconstruction. The
“reconstructive ladder” that all plastic surgeons learn is based on performing the simplest procedure to correct a
particular condition. Although these principles are valuable and almost always justified, aesthetic and functional
considerations occasionally warrant performing more complicated procedures. These considerations are most evident
following ablative procedures for cancer, for restoration of function, and for aesthetic appearance.
Numerous clinical situations exist in which the use of a free flap is justified and beneficial. Refinements in mandibular
reconstructions have led to the use of the free fibular flap, which results in improved appearance and function of the
neomandible.
Preoperative preparation is an essential component of the successful free tissue transfer. Preoperative evaluation
includes analysis of the recipient site, consideration of available donor sites, and the clinical status of the patient.
Although microvascular transfer of free tissue grafts did not gain favor until the mid 1970s it was performed as early
as 1959 when Seidenberg used revascularized free jejunum segments to repair pharyngoesophageal defects. McLean
and Buncke used omentum pedicled on the gastroepiploic vessels to cover a cranial defect in 1972. In 1973, Daniel
and Taylor described the first free cutaneous flap and in 1976, Baker and Panje was the first to publish the use of free
cutaneous flaps for the reconstruction of head and neck defects. He followed this in 1977 with a free groin flap based
on the superficial circumflex iliac artery to reconstruct an intraoral defect. This flap was met with some favor during
this time and was performed by other surgeons, however it was a bulky flap and its vascular pedicle was inconsistent
and the vessels were very small in diameter.
Other flaps such as the axillary free flap and dorsalis pedis flap were also described but had short-comings such as an
inconsistent pedicle and significant donor site morbidity respectively. In 1976, Harii and colleagues developed the
latissimus dorsi musculocutaneous flap. This was a very reliable flap based on the thoracodorsal artery and vein. It
has remained a favorable flap for certain head and neck defects to this date.
During the 70s limited numbers of surgeons were performing free flaps for a number of reasons. First, there were
only a few to choose from. In addition they did not always provide all the tissue needed to reconstruct head and neck
defects requiring combinations of bone, skin, and muscle. Most importantly, the majority of flaps at this time had
inconsistent small pedicles making them technically difficult to perform.
Towards the end of the 1970s free flaps grew out of favor and an old technique was revisited. In 1896, Tansini had
described the pedicled latissimus dorsi flap. In 1976, Olivari brought this back into favor. Subsequently other
pedicled cutaneous and myocutaneous flaps arose such as the pectoralis and trapezius flaps. The pectoralis
myocutaneous flap was considered the "work Horse" flap of head and neck reconstruction during this time. In 1979,
Ariyan used the pectoralis flap in combination with rib and in the same year Demergasso and Piazza described harvest
of the spine of the scapula with the trapezius musculocutaneous flap. These pedicled flaps became the choice of most
head and neck surgeons over the next decade. They were reliable, quick, and easy to harvest. They also required only
one stage, had minimal donor site morbidity, and provided more bulk than the free flaps available at that time. They
required only one surgical team, were technically easier, and provided nonirradiated tissue (Chepeha and Teknos,
2001).

In the past fifteen years, limitations of pedicled flaps and desire by surgeons for new and better donor sites has
lead to a resurgence of free tissue transfer. Pedicled flaps were not well suited for reconstruction of defects requiring
very large bulk or those needing thin pliable tissue. In addition their reach was constrained by the length of their
pedicle. As further investigations continued new donor sites for free flaps emerged that possessed longer and larger
vascular pedicles and were made up of various tissues including skin, muscle, bone, and nerve. This allowed for much
more refined tailoring of harvested tissue to the recipient site. Free flaps can provide a much wider range of skin
characteristics that can match the host site well. In addition microvascular transfer makes much more efficient use of
harvested tissue as nearly all is used directly in the reconstruction. Pedicled flaps require less efficient use of tissue as
entire muscles are defunctionalized in order to safely transfer enough tissue to fill a defect. Because free flap donor
sites are often located at a distant location from the extirpative site, a two team approach can be used to decrease
operating room time. The excellent perfusion of free flaps significantly improves wound healing and serves to protect
against wound breakdown and osteoradionecrosis when postoperative radiotherapy or brachytherapy is utilized. Free
flap reconstruction also affords the ability for water-tight closures in skull base defects to prevent CSF leaks. Because
revascularized tissue transfers maintain their independent blood supply, they are not as subject to resorption, providing
for greater long-term stability and cosmesis to the reconstruction. Resorption, which plagued non-viable bony
transfers in the past, is virtually eliminated with free flap reconstruction. Finally, many of free flaps have the potential
for functional neurosensory and motor innervation from recipient nerves as well as the ability for primary placement
of osseointegrated implants for improve oromandibular function
In 1979, Taylor and colleagues described the iliac crest composite flap based on the deep circumflex iliac artery. This
was followed by the radial forearm fasciocutaneous flap (Yang, 1981), the scapular skin flap (dos Santos, 1980), the
parascapular skin flap (Nassif, 1982), the lateral arm fasciocutaneous flap (Song, 1982), the scapular osseocutaneous
flap (Swartz 1986), the lateral cutaneous thigh flap (Baek 1983), and the rectus abdominis myocutaneous flap (Drever,
1985).
Today microvascular free-tissue transfer to the head and neck has become an accepted method of reconstruction. This
is due primarily to increased success rates for free-flap surgery (93 to 94%, Schusterman, 1993 and Urken, 1994
respectively) and superior aesthetic and functional results. Increasing numbers of surgeons have become adept at this
surgical subspecialty for a number of reasons: (1) widespread application of microvascular techniques by a variety of
different surgical disciplines; (2) Advances in technique and instrumentation; and (3) expanding number of dedicated
training fellowships.
Pre op considerations.
Instruments
1. The operating microscope
The modern microscope with its refined optics and wide range of magnification enable surgeon to carry out techniques
that were otherwise impossible to be done with naked eye; Structures < 3mm
1921 – Nylen from Sweden first operating microscope for labrythine fistulas and fenestrations in rabbits with
magnification uptp 10 to 15 X.
A monocular microscope later developed by Nylen in 1954, 1972 with a magnification with 235 X
1n 1921, Holmgren, chief of Nylen introduced Zeiss binocular to otology
In 1946, Peritt in US used microscope in ophthalmology
Jacobson and Saurez in 1960 used microscope in peripheral nerve injury
2. Magnifying loupes
These are more practical than an operating microscope especially for microdissection.
Preliminary dissection is carried out till the stage is reached when only microscope can provide needed resolution and
control.
3. Micro-instruments
Adequate miniaturization of instrument and sutures are needed
Micro-instruments – simple, glare free, few in number
Require careful maintenance – silicone or rubber tubes for protection of fine tips

Non toothed forceps should be of good quality and resistant to staining and rusting. Tips – fine, smooth, uniform and
jaws meet precisely.
Scissors are spring operated with delicate sharp blades. Westcott scissors with straight or curved blades with sharp or
slightly rounded tips are useful to section or trim vessel ends.
Spring loaded needle holders, approximately 6 inches lomg rest on the web b/n thumb & forefinger. It is held like a
pencil and slowly rolled b/n index and middle fingers and thumb during motion of inserting sutures. Needle holders do
not have locking mechanism as they can be traumatic to the delicate tissues
A 2 or 5 ml syringe with an attached 2-3 cm fine caliber silastic intercath is useful for irrigating the Microvascular
field.
A background of contrasting colour against which a fine suture is more easily seen and is useful for performing small
anastomosis is employed
A millimeter ruler for easy measurement of vessel size is included. An ocular micrometer in the eye piece can be more
convenient and more accurate.
4. Clamps
Small, light weight atraumatic vascular clamps play an important role in successful Microvascular anastomosis. Many
variations in size and design are available.
They are gently applied across the vessel walls to be anastomosed as the surgeon looks through the microscope in
order to minimize damage to the intimal lining of the vessel walls. Excessive pressure if applied is known to cause
minimal damage as shown histologicallly. These are however not suitable for vessels < 1.5 mm and lymphatics.
5. Bipolar coagulator
It can be an invaluable aid in coagulating the small vessels during micro-dissection. It conducts current through the
tips of jeweler’s forceps and can safely coagulate small branches near the main vessel.
6. Doppler monitors
These are instruments with microprobes that detect blood flow in vessels 1mm or less in size, below the skin and to
map the course of blood flow in proposed Microvascular free flaps and to monitor microvascular free flaps.
7. Suction
Small amounts of blood in operative field can totally obscure the vision of surgeon. Small Fischer suction tube with a
Zollner fine tip can be used. If suction is too powerful, it can damage an anastomosis.
The Weck cell micro-sponge or moist hydrocellulose sponge or gauze can also be used.
Van Beek designed a suction tube through a perforated background plate.
8. Micro-sutures
The assessment of sutures that are satisfactory for microvascular repair depends on the size and consistency of the
vessel to be anastomosed. The ideal needle for micro-suturing should be the same size as the micro suture itself,
which is not as yet achieved.
High quality atraumatic microsutures of extremely small caliber are ideal. Nylon drawn into round, smooth,
monofilament fibers of small caliber and high tensile strength is better than Prolene which has poor contrast and easily
breaks down, has less surface tension, softer and adheres less to itself.
Analysis of recipient and donor sites
Factors related to the recipient site include the size, depth, and location of the defect; quality of the surrounding tissue;
exposure of vital structures or hardware; zone of injury; presence of bacterial colonization or infection; previous
irradiation; and functional and aesthetic c onsiderations. Factors related to the donor site include appropriate tissue
match; length of the vascular pedicle; caliber of recipient vessels; surface area, volume, and thickness of the flap; and
donor site morbidities. Flaps with a short vascular pedicle requiring a vein graft and flaps with a bone component are
associated with an increased rate of flap loss in some clinical series.

Clinical status of the patient
The clinical status of the patient depends on a variety of factors that also may impact the free flap. These include
advanced age, nutritional status, tobacco usage, and presence of underlying comorbidities (eg, diabetes mellitus,
cardiopulmonary disease, peripheral vascular disease). Although advanced age and tobacco use are not
contraindications to free-flap operations, poor nutritional status can impede wound healing and recovery. Patients with
poorly controlled diabetes mellitus and peripheral vascular disease require adequate glucose control and may require
revascularization procedures prior to free tissue transfer. Surgical clearance by a medical physician is recommended
for patients with multiple medical problems.
Donor tissues
Specific donor tissues are variable and are chosen based on recipient site requirements. Available tissues include
muscle, musculocutaneous, fasciocutaneous, osteocutaneous, and bone flaps. In general, free muscle flaps are
indicated for soft tissue coverage of bone and synthetic materials and to obliterate a large dead space.
Innervated muscle flaps are useful for facial reanimation operations and for upper extremity reconstruction.
Musculocutaneous free flaps are useful for large defects requiring aesthetic contouring.
Fasciocutaneous flaps permit tendon gliding in the extremities and provide excellent contouring of the head
and neck.
For the irradiated wound, free tissue transfer is recommended and has been demonstrated to be safe and well
tolerated, with no increased rate of partial or total free flap loss.
Timing
In the trauma patient, the timing of free-flap reconstruction is of prime importance. Free tissue transfer within 3-7 days
allows time for adequate debridement, declaration of the zone of injury, and prevention of chronic bacterial
colonization. Immediate free-flap reconstruction often is preferred for the acquired operative wound, especially in the
presence of vital structures and hardware and for aesthetic and functional considerations. Consider delayed free-flap
reconstruction when oncologic concerns are present.
Other considerations
Other factors requiring consideration include choice of anesthesia and patient position for the operation. Anesthetic
options include general, spinal, or epidural and depend on the nature and location of the reconstruction. General
anesthesia is preferred for most patients and can be administered via oral, nasal, or tracheal routes. Oral intubation is
preferred for trunk and extremity reconstructions; however, nasal and tracheal intubations are preferred for most
reconstructions involving the head and neck. Spinal anesthesia occasionally is used for lower extremity free flaps and
has the advantage of providing a transient sympathectomy that promotes vascular dilation. Epidural anesthesia
primarily is used for postoperative pain management.
The operative portion of the free tissue transfer requires absolute attention to detail. Numerous factors must be
considered to predictably obtain a successful outcome. These include use of appropriate medications and solutions,
properly functioning equipment and instruments, anastomotic issues, and flap insetting.
Intraoperative medications
Required medications include intravenous (IV) antibiotics, antibiotic solution for wound irrigation, IV heparin
administered 5 minutes prior to free flap harvest, 4% Xylocaine for topical vasodilatation, and heparin solution (100
U/cm3) for luminal irrigation. Studies evaluating the effects of various intraoperative anticoagulants have
demonstrated that the flap loss rate is lower in patients receiving a heparin bolus of 5000 U only or a heparin bolus of
2000-3000 U followed by postoperative infusion. Low-dose heparin does not increase the risk of hematoma or

postoperative bleeding. Other medications that may be used include Decadron 4-8 mg to reduce edema and swelling
(especially for reconstructions of the head), papaverine as an alternate vasodilator, and streptokinase or urokinase for
lysis of intraluminal thrombus.
Anastomoses issues
A variety of issues are related to the anastomoses.
The nursing staff and primary surgeon must inspect the micro-instruments and microscope to ensure proper
function.
The diameter of the artery and vein, both for the flap and recipient site, should be 1-3 mm to permit adequate
inflow and outflow.
Blood vessels must be free of all loose adventitia, and the vascular approximation must be tension free.
Acland clamps should facilitate vascular exposure and manipulation.
Complete the anastomosis using either a vascular coupler or sew it by hand. The author prefers to hand sew;
however, the coupler has demonstrated its usefulness, especially for venous anastomoses, in improving
patency and decreasing operative time.
Complete the hand-sewn anastomosis using 8-0, 9-0, or 10-0 nylon sutures placed in an interrupted fashion. In
general, anastomose larger caliber vessels (2-3 mm) using 8-0 or 9-0 sutures and smaller caliber vessels (1-2
mm) using 9-0 or 10-0 sutures.
Using operative loupes rather than a microscope has been reported; a minimum of 3.5-power magnification is
recommended.
Flap ischemia time does not contribute to flap demise if the ischemia time is less than 3 hours or less than the
time for no-reflow to occur.
Following completion of the anastomoses, inset the flap. Inspect the vascular pedicle for kinks, twists,
compression, and to ensure that no tension is present across the anastomosis. Inspect the distal aspect of the
flap for arterial and venous bleeding. Use a Doppler unit to assess arterial and venous flow through the pedicle
and in the flap. Finally, recheck the vascular pedicle to ensure a gentle, nontwisting course of the vessels
before completing the final suturing of the flap, especially if the patient's position has been changed.
Place a closed suction drain under the flap away from the anastomoses and suture the flap in position.
Postoperative medications
Using postoperative medications to inhibit clot formation at the anastomosis is controversial. Studies evaluating the
efficacy of heparin, dextran, and aspirin have demonstrated that none is absolutely necessary for an uncomplicated
anastomosis. However, the author prefers to run IV dextran-40 at 30 cm3/h for the first 12-24 hours, followed by oral
Ecotrin 325 mg daily for 2-4 weeks.
Techniques to monitor the free flap depend on the tissue composition and location of the flap. Specific monitoring
techniques include evaluation of color, capillary refill, turgor, surface temperature, presence of bleeding, skin graft
adherence, and auditory assessment of blood flow. Use of these techniques depends on whether the flap has a
fasciocutaneous component, is covered with a skin graft, or is buried and inaccessible to visual assessment.
Surface characteristics
For the fasciocutaneous, musculocutaneous, and osteocutaneous flaps, surface characteristics are important. Normal
flap color is similar to that of the recipient site. Normal capillary refill is 1-2 seconds. Surface temperature of the flap
can be monitored using adhesive strips (for an accurate number) or the back of the hand (to provide a comparative
assessment with the surrounding skin). Problems with arterial inflow are suggested when the flap is pale relative to the
donor site, cool to the touch, and when capillary refill is slow or absent. Problems with venous outflow are suggested
when the flap is congested, edematous, and when capillary refill is brisk and rapid. Color and appearance of congested
flaps can vary depending on whether the congestion is mild or severe and ranges from a prominent pinkish hue to a
dark bluish purple color.

Surface Doppler assessment for flaps with a fasciocutaneous component may yield a false positive result by picking
up signals from surrounding or deep blood vessels. Characteristics of blood from the flap following pinprick also can
provide clues. Dark venous blood suggests venous occlusion, and absence of bleeding suggests arterial occlusion.
Muscle flaps with skin grafts
The muscle flap covered with a skin graft often is easier to monitor. Surface temperature and capillary refill generally
are not used in these situations; however, color, turgor, skin graft adherence, and Doppler signals are useful. Signs of
venous outflow obstruction include flap congestion and edema, dark blood on pinprick, and loss of the venous
Doppler signal. Signs of arterial occlusion include a flat and pale flap, poor skin graft adherence to the flap, no
bleeding on pinprick, and loss of the arterial signal.
Deep or buried flap
The most difficult flap to monitor is the deep or buried flap (eg, fibula flap without a skin paddle). Surface Doppler
signals often are unreliable. In these situations, placing the temporary implantable Doppler probe adjacent to the artery
and vein at the time of operation is useful.
Monitoring the free flap during the postoperative phase is critical to ensure flap survival. When recognized early and
managed promptly (<6 h), compromised flaps have a 75% salvage rate when taken back to the operating room.
Studies have demonstrated that venous thrombosis alone is more common than either arterial or combined arterial and
venous thrombosis. Thrombosis typically occurs within the first 2 days in 80% of patients. Thus, all personnel
responsible for flap monitoring must be knowledgeable of the appearance and evaluation of the healthy and
compromised flap.
Following recognition of flap compromise, immediately transport the patient to the operating room for
exploration.
Administer intravenous heparin.
Inspect the vascular pedicle for kinks and compression and assess the patency of the anastomosis.
Identification of thrombus requires separation of the vessels at the anastomosis.
Perform embolectomy, proximally and distally, using a number 2 or 3 Fogarty catheter.
Administer intraarterial streptokinase or urokinase at a dose of 50,000-100,000 U as necessary.
Following restoration of adequate circulation, inset the flap again and maintain the patient on intravenous
heparin or dextran.
Failure to restore adequate circulation requires flap removal.
The use of medicinal leeches, Hirudo medicinalis, has demonstrated value in the treatment of venous congestion. This
option is indicated when arterial inflow is adequate but venous outflow is poor. The mechanism of action depends on
the active agent, hirudin, which is a selective thrombin inhibitor. Apply the leech to the surface of the flap and
surround it with a corral of moistened gauze to prevent leech migration. Prophylactic antibiotics are recommended to
prevent infection with Aeromonas hydrophila.
Advantages of free flaps over pedicled flaps
Limitations of pedicled flaps
In the past fifteen years, limitations of pedicled flaps and desire by surgeons for new and better donor sites has lead to
a resurgence of free tissue transfer.
Pedicled flaps were not well suited for reconstruction of defects requiring very large bulk or those needing thin pliable
tissue.
In addition their reach was constrained by the length of their pedicle.

Pedicled flaps require less efficient use of tissue as entire muscles are defunctionalized in order to safely transfer
enough tissue to fill a defect.
Advantages of free flaps
As further investigations continued new donor sites for free flaps emerged, that possessed longer and larger
vascular pedicles and were made up of various tissues including skin, muscle, bone, and nerve. This allowed
for much more refined tailoring of harvested tissue to the recipient site.
Free flaps can provide a much wider range of skin characteristics that can match the host site well.
In addition microvascular transfer makes much more efficient use of harvested tissue as nearly all is used
directly in the reconstruction.
Because free flap donor sites are often located at a distant location from the extirpative site, a two team
approach can be used to decrease operating room time.
The excellent perfusion of free flaps significantly improves wound healing and serves to protect against
wound breakdown and osteoradionecrosis when postoperative radiotherapy or brachytherapy is utilized. Free
flap reconstruction also affords the ability for water-tight closures in skull base defects to prevent CSF leaks.
Because revascularized tissue transfers maintain their independent blood supply, they are not as subject to
resorption, providing for greater long-term stability and cosmesis to the reconstruction.
Resorption, which plagued non-viable bony transfers in the past, is virtually eliminated with free flap
reconstruction.
Finally, many of free flaps have the potential for functional neurosensory and motor innervation from
recipient nerves as well as the ability for primary placement of osseointegrated implants for improve
oromandibular function
DONOR SITE:
1. Radial forearm
2. Lateral arm
3. Rectus abdominus
4. DCIA iliac
5. Lateral thigh
6. Scapular flap
7. Lattismus dorsi
8. Jejunum
9. Dorsalis pedis
I. RADIAL FOREARM FREE FLAP
The radial forearm flap is the workhorse in intraoral and hypopharyngeal reconstruction. First described by Yang this
flap is based on the radial artery, shows aconstant anatomy with a high-caliber and long pedicle. This flap is thin and
provides agood pliability. Intraoperative view of the harvested flap, the skin island and thereverse view including the
pedicle are demonstrated in figures 1 and 2 (the fascia over the tendon is not removed to improve postoperative range
of motion). Neverthelessthe donor site shows aesthetic and functional problems: if primary closure is notpossible, skin
graft is necessary.

The Chinese surgeons Yang and colleagues described the radial forearm fasciocutaneous flap as early as 1981.
Indications
1. It used to reconstruct defects in the oral cavity, such as the tongue, trachea,
oesophagus and the hypopharyngeal region.
2. For reconstruction of mandibular continuity defect
3. Class 1 defects of the maxilla.
Planning-
Patient selection is important in determining whether a particular patient is a candidate for free tissue transfer.
Advanced age alone does not contraindicate free tissue transfer but aging may be associated with diabetes mellitus,
hypercholesterolemia, and arteriosclerosis which may result in thickening of the walls of small arteries and overall
increased vessel fragility. Generally, patients with blood coagulopathies, collagen vascular diseases, and other
vascular disorders are not candidates for free tissue transfer. Malnutrition presents a problem because patients are at
risk for wound healing problems including flap failure. Prior irradiation can lead to decreased patency of vessels and
poorer tissue survival rates. Irradiation leads to loss of smooth muscle, vessel fibrosis and endothelial cell disruption.
Anatomy-
The radial forearm flap is supplied by the radial artery and venous drainage is provided by the paired vena comitantes
(deep venous system) which accompany the artery as well as the various subcutaneous veins of the forearm including
the cephalic vein. The radial artery arises from the brachial artery just distal to the antecubital fossa and travels
between the brachioradialis and flexor carpi radialis as it runs distally in the forearm. It runs in the lateral
intermuscular septum which separates the flexor and extensor compartments of the forearm. It supplies the skin over
the volar aspect of the forearm from elbow to wrist as well as portions of the radius. Generally, the skin is thin,
pliable, and usually hairless while the vascular pedicle may be up to 18 cm in length and the vessel diameters are
usually large (2 - 4 mm). Medial and lateral antebrachial cutaneous nerves can also be made part of this flap (the
lateral antebrachial cutaneous nerve is the primary sensory nerve to the forearm) and is most commonly used to create
a sensate flap.
Preoperative evaluation-

Preoperative evaluation includes examination of the forearm to see where a hairless skin paddle can be taken
(generally the skin paddle can be taken anywhere along the length of the pedicle). An Allen test should be performed
with compression of the radial artery to insure collateral circulation via the ulnar artery. Both radial and ulnar arteries
are occluded and the patient raises their hand over their heads and opens and closes their palm to exsanguinate their
blood. Then the hand is brought down to a neutral position and the ulnar pulse is released and blood should flow into
the thenar area. Venipuncture should not be performed on the on the forearm that is being harvested. Any evidence of
intravenous drug abuse or evidence of allen test failure should preclude a radial free flap even though interpositional
vein grafts have been described for the radial artery. Defects should be handled that can be managed with the thin
pliable skin of the forearm which allows not necessarily bulk to any particular defect but permits mobility of the
underlying structures and draping. This flap is ideally designed for this purpose.
Surgical technique
The vascular pedicle can be easily identified and marked before flap elevation because of its subcutaneous location.
The flap should be designed such that the skin paddle overlies the distal radial artery although any island of skin over
the volar aspect of the forearm may be designed because of the numerous muscular perforators. Islands may be created
to allow for two skin paddles. The arm is exsanguinated and a tourniquet is inflated to about 70 to 90 mm Hg greater
than the patient’s systolic blood pressure. The flap is first incised along the ulnar border down to fascia and a
subfascial dissection is begun heading radially towards the flexor carpi radialis tendon. Preserve paratenon over this
tendon to allow skin graft take. The distal flap is then incised and the brachial artery and paired vena comitantes are
isolated. The two venae comitantes are ligated and divided while the radial artery may be divided and a microvascular
clamp applied distally. Then the radial margin of the flap is incised down to brachioradialis with care to preserve the
small branches of the superficial portion of the radial nerve which allows postoperative sensation to the anatomical
snuffbox. Working from distal to proximal, the surgeon should be able to visualize the lateral intermuscular septum
and vascular pedicle separating the flexor and extensor compartments of the wrist. Continue to develop this plane
between the brachioradialis and flexor carpi radialis and the vascular pedicle may be followed to the bifurcation of the
radial artery just distal to the antecubital fossa. The proximal vascular pedicle is isolated with vascular loops. The
microvascular clamp may be released at this point with reveals retrograde flow through the radial artery indicating
palm perfusion. Important in this dissection is a relatively bloodless dissection with warm irrigant and precise
handling of the vessels to prevent thrombus formation. When the recipient site is prepared, the flap may be transferred
with an ischemia window of about 6 hours. Donor site care may include removal of the palmaris longus (the palmaris
is absent in about 14% of patients) and imbrication of the flexor carpi tendon to allow for a smooth bed to receive a
skin graft. The donor site defect may be reduced by attaching skin edges to the muscle. A thick split thickness skin
graft is applied (0.018 in) over defect and the wrist placed in a plaster splint kept in place for 5 to 7 days. The wrist
should be kept slightly extended with fingers in their functional position. The flap itself is usually insetted prior to
microvascular anastomosis. Microvascular anastomosis occurs in the usual fashion of donor vein being connected to
recipient vein (usually internal jugular) in an end to side fashion and arterial connection in an end to end connection to
any of the branches of the external carotid. Postoperatively, antibiotics may be given for 5 to 7 days and low
molecular weight dextran at 25 cc/hr to decrease vascular occlusion. The viability of the flap should be monitored with
doppler pencil probe every 1 to 2 hours for the first 72 hours. Alternatively, pricking the flap can also be performed
which should reveal a slow egress of bright red blood. Any deviation from normal should prompt a thorough search
for vascular occlusion including taking the patient back to the operating room to investigate the anastomosis. The
splint may be removed on day seven and a resting splint kept in place for the next several days. Range of motion
exercises can be begun for the wrist to prevent scar contracture and decreased motion of the wrist. Whether to use a
single or dual system of venous drainage from the radial forearm free flap remains a topic of controversy. Arguments
exist on both sides that including the relatively larger diameter subcutaneous veins (cephalic and basilic) would
presumably decrease venous congestion and lead to increased flap survival but these veins have more anatomic
variability than their venae comitantes counterparts. Also, some studies have shown that despite including multiple
venous anastomoses, this does not persay increase flap survival with the added cost of increased operative time and
morbidity. Also, to include dissection until the venae and superficial veins communicate with each other into a
common vein is not entirely practical. Sometimes, these connections do not occur until quite proximal making this
pedicle extremely long and unweildy. The dissection sometimes has to proceed dorsolaterally over the upper arm in

order to reach this connection. Basically, sound surgical technique, precise microvascular anastomosis, strict
postoperative monitoring prevent flap failure more than multiple anastomoses.
Flap variants
Double paddle fasciocutaneous flap
It is possible by the excision of a skin bridge to create skin paddles which may be used to resurface composite defects
of the ofofacial region. It is easier to excise the skin bridge prior to raising the paddles and the technique of raising the
flaps is no different from raising a single skin paddle.
Fascial flaps
These flaps composed purely of fascia and vascular pediclele are extremely useful for facial augmentation and provide
a watertight seal in craniofacial resections where local pericranial/galeal flaps or temporalis flaps are unavailable
because of previous surgery or infection.
It is claimed that this technique of excising the skin paddle is of use in intraoraI reconstruction where one is intending
to place osseointegrated implants in radial osteocutaneous flaps. It is felt that the fascia will re-epithelialize and
simu1ate attached gingivae, thus providing a better base prosthodontic rehabilitation
Postoperative details
Perfusion of the flap and the hand are closely monitored, as is the motor and sensory neural integrity of the hand and
fingers.
Keep the donor arm elevated. Take down the arm splint 5-7 days postoperatively and dress the donor site with a fresh
Xeroform gauze and cotton wrap dressing for protection during healing. Remove the arm sutures and/or staples
approximately 10 days postoperatively. Encourage the patient to perform normal movements with the donor arm after
splint removal.
Prophylactic internal fixation of donor radius and wound closure
Prophylactic internal fixation can be performed most efficiently after reinflating the arm tourniquet. Expose the dorsal
radius proximally and distally. Position an appropriately sized low-contact dynamic compression plate over the radius
and bend it to the contour of the bone. Typically, 14- to 18-hole plates are required, depending on the length of the
harvested radius graft. Distally, retract the radial wrist extensors (ie, abductor pollicis longus, extensor pollicis brevis,
extensor carpi radialis longus, extensor carpi radialis brevis) laterally and place at least 2 standard bicortical screws.
Proximally, visualize the supinator (S). With long-bone harvests, elevate this muscle subperiosteally and place the
plate beneath it. Take care to protect the posterior interosseous nerve, a branch of the deep radial nerve that pierces the
S. Place at least 2 (usually 3) bicortical screws proximally. To avoid the creation of additional stress risers, do not
place screws in the defect cavity
Using a dermatome, a STSG (0.015-in thickness) is harvested from the prepared thigh. Then, mesh the STSG and
bring it up to the donor arm. Dress the leg with Xeroform gauze (Sherwood Medical, St Louis, Mo) or occlusive
dressing.
Reinsert the PT tendon into the remaining radius or fixation plate as necessary. Using absorbable sutures, suture the
FPL remnant over the radius defect and plate. The FDS can usually be brought over the flexor carpi radialis (FCR)
tendon to the radial skin edge. This method provides a second muscular layer over the bony donor site and helps the
STSG take on the FCR tendon. Then, cover the defect with a 1.0:1.5 meshed STSG. Cover the donor site with
Xeroform gauze, cotton balls, and a gauze wrap. Finally, apply a rigid plaster ulnar-gutter splint and wrap with an
elastic bandage.

Follow-up care
Monitor the arm and leg wounds during routine postoperative follow-up as dictated by the head and neck problem.
Encourage normal wrist activity; physical therapy is needed only if limited range of motion or decreased strength is
encountered. Postoperative radiographs of the donor arm are needed only to investigate arm symptoms.
Complications
Donor site morbidity includes exposure of tendons,
poor aesthetics,
radiusfracture.
Advantages
1. It provides a vertical height of 1.3cm for mandibular replacement. This
vertical height sufficient for placement implants.
2. Thin, pliable skin
3. Often hairless
4. Ease of access
5. Long pedicle
Disadvantages
1. Donor site defect visible & usually needs skin grafts
2. Sensory defect
II. LATERAL ARM FREE FLAP
The lateral arm flap may be raised as a fasciocutaneous flap or as a composite graft with bone (humerus), and
two nerves, one of which (posterior cutaneous nerve of the arm) serves as sensory supply and the other (posterior
cutaneous nerve of the forearm or posterior antebrachial cutaneous nerve) as a vascularized nerve graft. The skin flap
that is raised is similar in texture, pliability and size as the RFFF but it has distinct advantages. First, the donor site
can be closed primarily and does not require a skin graft if the skin flap is limited to 6-8 cm, or one-third the
circumference of the arm. Second, its vascular supply is based on the profunda brachii, which is not essential to the
vascularity of the distal upper extremity. There is no risk of ischemia to the arm with this flap.

The pedicle to this flap is based on the terminal branches of the profunda brachii artery and the posterior radial
collateral artery (PRCA) and its venae comitantes. These vessels travel in the spiral groove with the radial nerve. As
the PRCA enters the lateral intermuscular septum, its average diameter is approximately 1.55mm. The blood supply
to the skin is derived from four to five septocutaneous perforators that arise from the PRCA. The maximum length of
the vascular pedicle is 8-10mm. This length can be achieved by extending the dissection proximally between the
lateral and long head of the triceps muscle. This involves creating a tunnel underneath the triceps insertion to gain
access to the spiral groove to access more of the vessel. This maneuver can risks the muscular branches of the radial
nerve to the triceps muscle. There are several disadvantages to the lateral arm flap. The donor site requires a pressure
dressing postoperatively which has been associated with radial nerve palsies. If a large flap is required, a STSG may
be required.
III. ANTERIOLATERAL THIGH FLAP The flap has emerged as a popular option for reconstruction of head and neck defects. Ithas the attributes of a
“workhouse” flap which include absence of patient repositioning, remote location from the potential defect, and a long
pedicle. The ALT was first described by Song in1984. It should be emphasized that the skin associated with this flap
is anterolateral thigh skin and that the pedicle is the descending branch of the lateral circumflex femoral artery. This
differs from the lateral thigh flap that was described by Baek in 1983 which involves posterolateral thigh skin and a
pedicle from the third cutaneous perforator off of the profunda femoris. After description of the ALT it mainly had
reported use in Asia. Proposed reasons for this trend were vascular anatomy variations, difficult dissection, and thick
thigh fat. However, in the last decade, the ALT has become a popular reconstructive option inWestern countries.
In designing an ALT, a line is drawn betweenthe anterior superior iliac spine and the lateral border of the patella. This
line approximates the septumbetween the rectus femoris and the vastus lateralis. Skin perforators are mapped with a
Doppler. As mentioned before, the pedicle is the descending branch of the lateral circumflex femoral artery.
Perforators come off of the descending branch and are labeled A, B, and C (A is the most proximal and C is the most
distal). Perforators range between0 and 3 per patient with the mean being 2. The perforators are classified as either
septocutaneous or musculocutaneous. Septocutaneous perforators run between the rectus femoris and vastus lateralis
and traverse the fascia lata to the skin. Musculocutaneous perforators traverse the vastus lateralis and deep fascia to
the skin. After mapping the perforators with the Doppler, the skin paddle is planned and an incision is made on the
medial aspect. Lateral dissection is performed to locate the perforators. Once the perforators have been identified, the
skinincision may be completed. Retrograde dissection of the perforators to the pedicle is performed to the descending
branch of the lateral circumflex femoral artery. Alterations in harvesting the flap based onthe defect size are instituted.
The flap may be harvested as a subcutaneous flap, a fasciocutaneous flap, a myocutaneous flap, or an adipofascial
flap. Additionally, the flap has the ability to be sensate via the lateral femoral cutaneous nerve which comes from L2
and L3.

The largest case series of ALTs was published by Wei. It involved 660 patients with 672 ALTs. A total of 484 flaps
were transplanted to the head and neck region. A total of 1.8% had total failure and 2.5% had partial failure. This is
consistent with the failure rate from other case reports which ranged from 2.2 to 3.3%.
Issues involving the recipient site with ALTs can be divided into functional outcomes and aesthetic outcomes. From a
functional perspective, problems encountered include speech problems, oral incompetence, swallowing problems,
facial pain, nasal obstruction, and flap contracture. From an aesthetic perspective, problems encountered include flap
sagging, color mismatch, hair growth, contour defect, and flap bulkiness. Issues involving the donor site with ALTs
can also be divided into functional outcome and aesthetic outcome. Functional issues include gait alteration, sensory
disturbance, and cold intolerance. Aesthetic issues include hypertrophicscarring,hypopigmentation/hyperpigmentation,
keloid formation, and contour defect.
Comparisons have been made between ALTsand other free flaps from a functional standpoint. Intraoral defects
repaired with an ALT versus a radial forearm free flap show no functional difference regarding swallowing,
aspiration, and speech. Repair of circumferential pharyngeal defects with ALTs compared to jejunal flaps showed
better function, quicker recovery, less cost, and similar complication rates with regards to ALTs.
ALTs have recently taken an increased role in head and neck reconstruction. It is a versatile flap with the necessary
“workhorse” attributes. The large skin paddle that can be harvested in combination with the potential harvest of
muscle allow for reconstruction of large defects. Additionally, it can be a sensate flap. Keeping these facts in mind,
ALTs will likely continue to be a quality reconstructive option for head and neck defects.
IV. LATERAL THIGH
First described by baek in 1983, The lateral thigh flap is a fasciocutaneous flap whose blood supply is based
on the third perforator of the profunda femoris artery and its venae comitantes. This flap, like the RFFF is used
primarily used in reconstruction of oral cavity and pharyngeal defects. It has many advantages including: (1) a long
vascular pedicle (up to 15cm); (2) large vessels (2-4mm); (3) large skin paddle (up to 10X20cm); (4) distant from the
head and neck allowing for a two team approach; (5) donor site can be closed primarily with minimal functional loss;
(6) the skin is pliable and usually hairless; and (7) the flap may be harvested as a sensate flap if the lateral femoral
cutaneous nerve of the thigh is preserved. In obese patients, particularly women, these flaps may be very bulky.
Other disadvantages include the difficulty of dissection deep in the leg near the profunda femoris artery requiring an
assistant to retract the vastus lateralis. The vascular pedicle is often inconsistent. The most common variation is for
the pedicle to arise from the fourth perforating branch of the profunda femoris artery.
Cutaneous perfortator origin

FREE MUSCLE AND MUSCULOCUTANEOUS FLAPS
I. RECTUS ABDOMINIS
The rectus abdominis is an extremely versatile free flap used for reconstruction of multiple soft tissue defects
in the head and neck. Most commonly it is used for large defects in the midface and cranial base region. It has also
been used on the scalp and in the oral cavity (particularly for patients undergoing total or subtotal glossectomy). The
flap may either be raised as a muscle flap or a musculocutaneous flap. The blood supply to the rectus abdominis
muscle is based on the deep superior and inferior epigastric arteries while the skin overlying it is based on
musculocutaneous perforators arising from these arteries within the muscle belly. The muscle is very large and can
fill in large defects and can reliably separate the oral from the cranial cavity in cranial base surgery. There are a large
numbers of musculocutaneous perforators that supply the overlying skin making it possible to create spatially
separated skin paddles. This allows for closure of defects involving more than one epithelial site such as the cheek
and the oral cavity or the buccal mucosa and the palate.
Other advantages of the rectus abdominis free flap include: (1) constant anatomy; (2) ease of flap elevation; (3)
change of position is not necessary allowing simultaneous elevation with extirpation of the primary; (4) large diameter
vessels (mean of 3.4mm) with a pedicle up to 8-10cm in length.
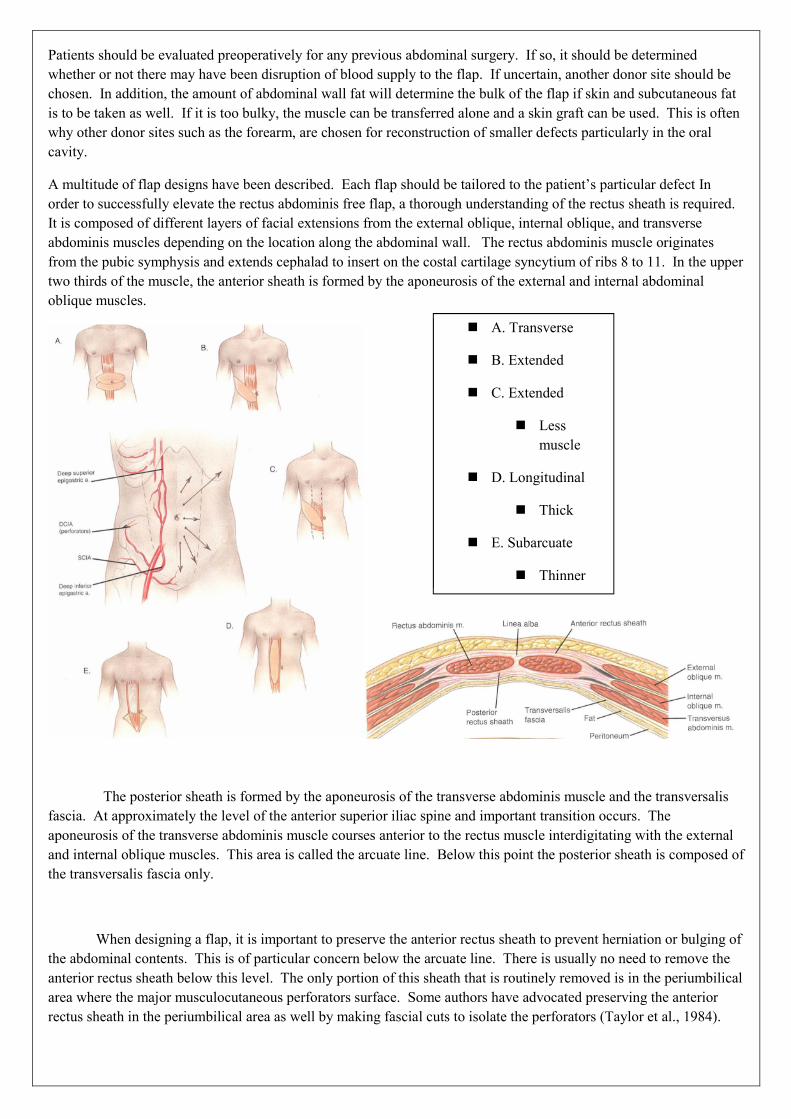
Patients should be evaluated preoperatively for any previous abdominal surgery. If so, it should be determined
whether or not there may have been disruption of blood supply to the flap. If uncertain, another donor site should be
chosen. In addition, the amount of abdominal wall fat will determine the bulk of the flap if skin and subcutaneous fat
is to be taken as well. If it is too bulky, the muscle can be transferred alone and a skin graft can be used. This is often
why other donor sites such as the forearm, are chosen for reconstruction of smaller defects particularly in the oral
cavity.
A multitude of flap designs have been described. Each flap should be tailored to the patient’s particular defect In
order to successfully elevate the rectus abdominis free flap, a thorough understanding of the rectus sheath is required.
It is composed of different layers of facial extensions from the external oblique, internal oblique, and transverse
abdominis muscles depending on the location along the abdominal wall. The rectus abdominis muscle originates
from the pubic symphysis and extends cephalad to insert on the costal cartilage syncytium of ribs 8 to 11. In the upper
two thirds of the muscle, the anterior sheath is formed by the aponeurosis of the external and internal abdominal
oblique muscles.
The posterior sheath is formed by the aponeurosis of the transverse abdominis muscle and the transversalis
fascia. At approximately the level of the anterior superior iliac spine and important transition occurs. The
aponeurosis of the transverse abdominis muscle courses anterior to the rectus muscle interdigitating with the external
and internal oblique muscles. This area is called the arcuate line. Below this point the posterior sheath is composed of
the transversalis fascia only.
When designing a flap, it is important to preserve the anterior rectus sheath to prevent herniation or bulging of
the abdominal contents. This is of particular concern below the arcuate line. There is usually no need to remove the
anterior rectus sheath below this level. The only portion of this sheath that is routinely removed is in the periumbilical
area where the major musculocutaneous perforators surface. Some authors have advocated preserving the anterior
rectus sheath in the periumbilical area as well by making fascial cuts to isolate the perforators (Taylor et al., 1984).
A. Transverse
B. Extended
C. Extended
Less
muscle
D. Longitudinal
Thick
E. Subarcuate
Thinner

II. LATISSIMUS DORSI
The latissimus dorsi flap (LDF) has long been a useful flap to reconstruct very large defects of the head and
neck. The latissimus dorsi muscle is a large fan shaped muscle that originates from the thoracolumbar fascia, lower
thoracic spinous processes, and the iliac crest and inserts onto the humerus. Its neurovascular supply is based on the
thoracodorsal artery with its paired vena comitantes, and the thoracodorsal nerve. The thoracodorsal artery is a
terminal branch of the subscapular artery. The pedicle based on this artery ranges from 7 to 10 cm. Additional length
can be obtained by ligating the circumflex scapular artery and including the subscapular artery with the pedicle. The
diameter of the artery in this area is 2 to 3 mm. The vein is approximately 3 to 5 mm. The thoracodorsal nerve can be
reanastomosed to a recipient nerve in the neck to reinnervate the muscle and prevent wasting.
The vascular supply to the skin paddle of the LDF is provided by musculocutaneous perforators branching
from the thoracodorsal artery which span a large surface area of skin. The skin flap that can be elevated is the second
largest available in the body next to the rectus abdominis flap. The difference between these two flaps is that the skin
of the latissimus flap is centered over muscle. This makes the flap extremely large. It is great for filling very large
defects but usually to thick to tube or use in the oral cavity. Multiple skin paddles can be designed with this flap.
The donor site for the latissimus flap is usually easily closed primarily with little cosmetic deformity.
Functional deficits from removing this muscle are prevented by the compensatory action of other muscles that act
across the glenohumeral joint. It is important to note that progressive morbidity to the shoulder does occur with the
sacrifice of the latissimus dorsi is combined with loss of either the trapezius muscle or the pectoralis major muscle.
To harvest this flap, the patient must be in a 30 to 45 degree lateral oblique position. Although synchronous head and
neck surgery can be performed, there may be some difficulty, especially if bilateral neck dissections must be
performed..

SKIN GRAFTS

DEFINITIONS
Skin grafts – skin is transplanted by completely detaching a portion of integument from its donor site and
transferring it to a host bed, where it acquires a new blood supply to ensure the viability of the transplanted
cells.
Skin flaps – consists of a portion of skin and subcutaneous tissue which is raised from the donor site – the
flap is left attached to the surrounding skin by a vascular pedicle.
Autografts (autogenous grafts) is a graft transferred from a donor to a recipient site in the same individual.
An allograft (homograft) is a transplant between genetically disparate individuals of the same species.
A xenografts (heterograft) is a graft transplanted between individuals of different species.
Isograft is the term employed in experimental transplantation to design an allograft between highly inbred
(genetically pure) strains of animals ; such grafts may also be called ‘synergic’.
HISTORY
1823 – Bunger – Skin graft from thigh to nose
1840 – Warren – Transplanted full thickness skin graft to ala of nose
1870 - Reverdin - First biologic transfer of skin
Pollock applied the first successful autograft to a burn wound.
1872 – Ollier – Clinical application of dermoepidermic graft 4 x 8 cm in size.
1874 – Thiersch – Thin split thickness grafts
Lawson, Lefort and Wolfe - Full-thickness grafts.
1929 - Blair and Brown - clinical use of thick split skin grafting .
1939 - Earl Padgett – Dermatomes
SKIN GRAFTS
Free skin grafts are pieces of skin that have been served from their local blood supply and transferred to
another location.
Free skin grafts are divided into 4 categories
FREE SKIN GRAFTS
FTSGs STSGs Composite graft Free cartilage graft
Composed of
epidermis and entire
thickness of dermis
Composed of full
thickness epidermis
and partial thickness
dermis
2-different tissue
types composed of
skin and cartilage
Consists of cartilage
with its overlying
perichondrium.
Thin
(0.005-0.012 inch).
Medium
(0.012-0.018 inch).
Thick
(0.018-0.030 inch).
Depending upon the amount of dermis
included

GILLES PRINCIPLES OF RECONSTRUCTIVE SURGERY
‘Losses must be replaced in kind’.
‘Treat the primary defect first’.
‘Thou shalt provide thyself with a lifeboat’.
‘Thou shalt not throw away a living thing’.
‘Replace things into their normal position by recreation of the defect’.
TYPES OF GRAFTS :
An important decision of skin grafting is selecting the ideal graft from the optimal donor site. The surgeon
must first decide between full thickness and split-thickness skin grafting and this requires an understanding of the
biology of grafts.
The very thin skin grafts used by early surgeons (Ollier, 1872 ; Thiersch 1874) have been replaced by thicker
spit-thickness grafts (Blair and Brown 1929), which include all of the epidermis and a variable fraction of dermis.
Types of skin grafts 1. ACCORDING TO ORIGIN
AUTOGRAFT
ALLOGRAFT
XENOGRAFT/ HETEROGRAFT
ISOGRAFT
2. ACCORDING TO THICKNESS SPLIT THICKNESS SKIN GRAFTS
i. THIN – 0.08 TO 0.012 MM
ii. MEDIUM- 0.012 TO 0.018MM
iii. THICK- 0.018 TO 0.030MM
FULL THICKNESS SKIN GRAFTS
SPLIT THICKNESS SKIN GRAFT FULL THICKNESS SKIN GRAFT
1. IT CONTAINS VARIABLE FRACTION OF
EPIDERMIS AND DERMIS.
1. IT CONTAINS WHOLE EPIDERMIS AND
DERMIS.
2. IT CAN BE GRAFTED IN LESS IDEAL
CONDITIONS. LESS VASCULARITY IS NEEDED.
IT CAN BE APPLIED TO GRANULATING WOUND.
2. EXCELLENT WOUND VASCULARITY IS
REQUIRED

3. IDEAL FOR CONTAMINATED LARGE WOUNDS. 3. IDEAL FOR UNCONTAMINATED WOUND OF
SMALL SIZE.
4. MORE CONTRACTION. 4.LESS CONTRACTION.
5. LACK OF GROWTH. 5. GROWTH OCCURS IN CHILDREN
6. ABNORMAL PIGMENTATION AND
OCCASIONAL LACK OF DURABILITY.
6.TEXTURE AND PIGMENTATION SIMILAR TO
NORMAL SKIN.
7. DONOR SITE HEALS SPONTANEOUSLY. 7. DONOR SITE SHOULD BE CLOSED PRIMARILY/
BY SPLIT THICKNESS SKIN GRAFTS.
MESH GRAFTS
It is also known as expanded grafts. It is indicated in massive burns when there is insufficient skin. It is also
indicated in case of convoluted surface of graft bed.
The disadvantage of the mesh graft is delay in wound healing, since the gaps in grafts should epethelilize
secondarily. The graft tends to contract significantly, so it is contraindicated over the joint, since it will impede
with the movements.
A mechanical mesher is used to expand the graft. It used multiply pierce the graft, allowing it to be expanded into a
mesh of varying size (longer the slits, the greater the expansion ratio)
Dermal overgrafting:
Webster 1954
Thomson 1960
Split thickness skin grafts are applied to a bed of dermis/ scar tissue after removal of surface epithelium.
Principle behind this type of grafting is a capillary circulation and lymphatic circulation in mature scar exists and
vascularizes overlying grafts.
Indications-
1. Extensive, unstable, contracted, pigmented/hypertrophic scars.
2. It may be grafted to foot to increase weight-bearing capacity of foot.
3. Venous stasis ulcer.
4. Extensive pigmented nevi.
5. Chronic radio dermatitis
Dermal fat grafting
For padding composite grafts of dermis and fat have been successfully used. Their limitation is
that fat tend to resorb, graft success depends on the grafted dermis.
Composite grafting
A composite graft includes more than one kind of tissue.
E.g. Wedge of ear. It contains skin and cartilage, ideal for reconstructing alar defects. A graft of nasal septum and
mucous membrane can be used for eyelid reconstruction. Composite grafts are necessarily limited in dimension
because they must derive blood supply from the recipient wound. Furthermore, the donor site must be closed
primarily. Recipient wound preparation, suture immobilization and graft handling must be flawless / else
vascularization will not take place.

FULL-THICKNESS SKIN GRAFTS :
Full thickness skin grafts which includes the entire thickness of epidermis is harvested from the donor site.
These grafts do not contract and do not change in colour or skin texture
FULL THICKNESS SKIN GRAFTS:
INDICATIONS :
Full-thickness grafts need excellent wound vascularity for survival, and in general are used on acute uncontaminated
wounds of a small size.
A contaminated / large wound may be initially closed with a split thickness grafts, which is later replaced by a
full thickness grafts to improve skin quality. Because they simulate normal uninjured skin, full-thickness grafts ideally
would be used on all wounds that required skin grafting. However this is obviously not possible, as wounds may be
too large to be covered with full-thickness skin, too contaminated, / of poor vascularity in which case split-thickness
skin grafting is selected. Lifespan of FTSGS when wrapped in gauze , moistened in saline & stored in fridge at 4
degree Celsius is 3 weeks.
DONOR SITES :
Are almost always harvested from areas where the skin is thin. Full thickness grafts to the face are often taken from
the upper eyelid, postauricular / supraclavicular region.
1. upper eyelid
2. pre auricular
3. nasolabial fold
4. supra clavicular
5. postauricular
6. 1st neck crease
7. Wirst (dorsal aspect)
8. Groin
9. Abdomen
10. Buttocks
Relatively large grafts (3 x 3 cm) can be harvested from behind the ear and the donor site closed primarily. Even
larger grafts of postauricular skin may be harvested in the donor site is resurfaced with a split – thickness skin graft.
Full-thickness grafts from the central abdomen and trunk are rarely used as the skin is thick and prone to necrosis;
hairless groin skin is thinner and may be used.
Large areas of full-thickness skin suitable for grafting can be obtained from the dorsum of the foot, if the donor site is
carefully closed with split grafting.
A final consideration in selecting a donor site for full-thickness skin is avoiding later hair growth. Since in most body
locations the hair follicles lie within the dermis, unwanted hair can be transplanted if it is not avoided. Particularly in
children, care must be taken to select an area that will in adult life be free of hair. This is especially important in the
grain, to avoid pubic hair growing in an unwanted visible location.

CUTTING : FULL-THICKNESS GRAFT :
INSTRUMENT :
Full thickness grafts are cut free-hand with a scalpel; no dermatome is used. Such grafts must be relatively
small and the donor site must be carefully selected.
TEMPLATE :
Usually a pattern of the defect to be grafted is made and transferred to the donor site where it is outlined.
PROCEDURE :
Procedure:

The wound pattern outlined over the donor region is enlarged by 3-5% to compensate for primary contracture, which
will occur due to the elastic fiber content of the graft dermis. The donor site - infiltrated with local anesthetic with or
without epinephrine. After incising the pattern, the skin - elevated with a skin hook, keeping a finger of the
nonoperating hand on the epidermal side of the graft. This provides tension and a sense of graft thickness while the
operating hand dissects the graft off of the underlying subcutaneous fat. Any residual adipose tissue - trimmed from
the underside of the graft because this fat is poorly vascularized and will prevent direct contact between the graft
dermis and the wound bed. Trimming of residual fat is best accomplished with sharp curved scissors with the graft
stretched over the nonoperating hand until only the white glistening dermis remains. Grafts may be pie-crusted to
allow egress of wound fluid from beneath the graft. These openings will not prevent graft loss from an underlying
hematoma.This technique - performed by making multiple stab wounds through the graft with a number 15 scalpel
blade.Once the graft is harvested reinspect the recipient site for hemostasis. Place the graft with the dermal side down
over the wound bed. Also take care to prevent wrinkling or excessive stretching of the graft.The graft then must be
secured in place to provide stability during initial adherence and healing.
Absorbable sutures are preferable because they do not require removal. Usually, 4 corner sutures are placed to hold
the graft in the proper orientation.Then a running suture is placed around the periphery. Perfect epidermal-to-
epidermal approximation ensures optimal cosmetic results. A dressing is chosen - provide uniform pressure over the
entire grafted area through a nonadherent, semi-occlusive, absorbent dressing material. Immobilize the graft, Prevent
shearing and Prevent hematoma formation beneath the graft. Another dressing choice for an irregularly contoured
wound or wound with high levels of exudate is vacuum-assisted closure (VAC) sponge: It conforms to the wound
surface by suction and promotes skin graft adherence on removing exudate and edema from surrounding tissues.
Finally, the graft may be treated open by placing no dressing except a layer of ointment to prevent desiccation.This
technique - susceptible to hematoma or seroma formation beneath the graft because no pressure is applied.This
technique is used only occasionally in facial grafting. Graft adherence - maximal in the first 8 hours postgrafting but
the initial dressing left in place for 3-7 days unless pain, odor, discharge occur.
CLOSURE :
The donor site is closed by undermining the skin edges and closing the wound primarily. On rare occasions a large
full-thickness donor site may be closed by local flap rotation / resurfacing with a split-thickness skin graft.
GRAFT UPTAKE AND SURVIVAL
An initial adherence to the wound bed via a thin fibrin network temporarily anchors the graft until definitive
circulation and connective tissue connections are established.
Begins immediately and probably is maximized by 8 hours postgrafting. The period of time between grafting and
revascularization of the graft - the phase of plasmatic imbibition. The graft imbibes wound exudate by capillary action
through the spongelike structure of the graft dermis and through the dermal blood vessels. This process is entirely
responsible for graft survival for 2-3 days until circulation is reestablished. During this time, the graft typically
becomes edematous and increases in weight by 30-50%.Revascularization of the graft begins at 2-3 days. Inosculation
is the establishment of direct anastomoses between graft and recipient blood vessels. Full circulation to the graft is

restored by 6 or 7 days. Without Initial adherence, Plasmatic imbibition, and vascularization, the graft will not
survive. Wound contraction may present serious functional and cosmetic concerns - depending on location and
severity.
On the face, it may produce
Ectropion,
Retraction of the nasal ala or
Distortion of the vermilion border.
Contraction - begins shortly following initial wounding, progressing slowly over 6-18 months following grafting.
Myofibroblast is believed to be responsible for this contraction.Deep dermal component is able to suppress
myofibroblast function.Hair is more likely to grow from full-thickness grafts than from split-thickness grafts Sweat
glands and sebaceous glands initially degenerate following grafting. Sweat gland regeneration is dependent on
reinnervation of the skin graft with recipient bed sympathetic nerve fibers.
Sebaceous gland regeneration is independent of graft reinnervation and retains the characteristics of the donor site.
Skin graft lacking normal lubrication of sebum produced by these glands is minimal and hence the graft may appear
dry and undergo scaling during this period. The graft becomes soft and pliable with time as sebaceous gland
regeneration occurs.
Reinnervation of the graft occurs from the recipient bed and from the periphery along the empty neurolemma sheaths
of the graft.Full-thickness grafts reinnervate more completely than do split-thickness grafts. Pain usually is the first
perceived sensation, followed later by touch, heat, and cold. Pigmentation returns gradually to full-thickness skin
grafts.
Graft is to be protected from direct sunlight for at least 6 months postgrafting or even longer.
Hyperpigmented graft is to be treated with dermabrasion and laser resurfacing.
GRAFT FAILURE
The most common reason for skin graft failure is Hematoma beneath the graft. Seroma formation may prevent graft
adherence to the underlying wound bed preventing the graft from receiving the necessary nourishment. Movement of
the graft or shear forces - lead to graft failure through disruption of the fragile attachment of the graft to the wound
bed. Poor recipient site and Technical error also may yield graft failure. Graft placed upside down will result in
complete graft loss and applying excess pressure, Stretching the graft too tightly, or Handling of the graft in other
traumatic ways may also lead to graft failure.
MUCOSAL GRAFTS :
Full thickness mucosal grafts to reconstruct nasal and conjunctival defects can be harvested from the inner aspect of
the cheek. Care must be taken to avoid injury to the parotid duct.
Nasal mucous membrane can be harvested from one side of the septum following submucosal injection of a
vasoconstricting anesthetic solution; the exposed surface closes by epithelial migration.
To support a lower eyelid, a composite graft of nasal mucous membrane with accompanying septal cartilage
may be removed. This leaves the remaining perichondrial surface of the nasal septum intact to avoid perforation.
A final type of mucous membrane grafting is that of conjuctival tissue to replace other conjunctival tissue to
replace other conjunctiva. This graft can be taken more easily if the donor tissue is distended by submucosal injection
of an anaesthetic solution. Only the fornix should be conjunctiva can be obtained because of the risk of eyelid
contraction.
Advantages
- Colour and texture of grafted skin are optimally maintained.
- More normal sweating and sebaceous activity maintained.
- Contraction at recipient site is limited.
- Hair is transferred with graft .

- Graft in children will grow as the child grows.
Disadvantages
- Grafts require careful care to ensure ‘TAKE’
- Donor sites will not heal secondarily and require separate closure.
SPLIT THICKNESS SKIN GRAFTS
Split thickness skin grafts consists of epidermis and a portion of the dermis.
These grafts vary in thickness from approximately 0.005-0.030 inches.
CLASSIFIED AS
DEPENDING On The Amount Of Dermis Included In The Graft
1) Thin split thickness skin grafts
(0.005-0.012 inches)
2) Medium thickness split thickness skin grafts
(0.012-0.018 inches)
3) Thick split thickness skin grafts
(0.018-0.030 inches)
Indications
1. Used to cover large defects, particularly those that cannot be covered by a flap or would heal too slowly by
granulation.
2. STSGs are very useful for large defects on the posterior ear where the perichondrium provides a limited vascular
bed.
3. Ideal for covering surgical defects at high risk for tumor recurrence, since deep recurrent tumor is usually visible
when growing through split thickness skin. STSGs can therefore serve as a ‘WINDOW’ for tumor recurrence. ( After
an appropriate time interval during which monitoring for tumor recurrence occurs, the graft can be excised and a
definitive reconstruction performed latter)
Advantages:
Donor sites heal spontaneously because of the remaining epidermal appendages - reharvested once healing is complete
Frequent lack of smooth texture and hair growth make split-thickness grafts more functional than cosmetic
Disadvantages:
They contract more during healing and do not grow with the individual. They tend to be abnormally pigmented or
hyperpigmented particularly in darker-skinned individuals. Grafts Thinness, Abnormal pigmentation, and Frequent
lack of smooth texture and hair growth are also disdvantages
Choice of donor site :
Can be taken from any area of the body, including the scalp and extremities. Common sites include the Upper anterior
surface of arms, Lateral thighs and Upper inner arm which is a cosmetically superior donor site. When possible, split-

thickness skin grafts should be taken from hidden areas such as the lateral buttock so that recreational clothing
camouflages the scar, an equal consideration in both sexes.
Lower extremities / trunk split-thickness grafts ideally should not be used in face, as such grafts tend to have a
yellowish-brownish color.
If split-thickness skin grafts are required for the face, skin harvested from ‘blush zones’ such as supraclavicular areas
and scalp is preferable.
If the split-thickness grafts are cut superficially enough in a hair area such as the scalp, hair should not grow in the
recipient area nor should baldness develop in the donor area.
A commonly used site for extremity / trunk skin grafts is the abdomen, as are the thighs and buttocks. If split-
thickness grafts are required in hand reconstruction / for fingertips, they should be harvested from the upper inner arm,
a cosmetically better location than the more accessible fore arm.
Mucosal split-thickness grafts as in conjunctival replacement can be harvested from within the oral cavity using a
specialized dermatome, castroviejo dermatomes. An important source of split-thickness grafts, occasionally
overlooked in trauma situations, is avulsed / surgically removed skin. The patient with large areas of avulsed skin can
have split-thickness grafts harvested from the otherwise discarded skin.
Avoid the groin and antecubital regions, where grafts cannot be harvested without risking exposure of subcutaneous
fat, and sub cutaneous contracture
Factors :
Since the harvesting of split-thickness grafts does leave a scar, selection of the donor site should consider scar
visibility as well as color match.
Ideally STSGs should be located in an area from which a broad area of tissue can be removed and still hidden under
clothing.
CUTTING: SPLIT THICKNESS GRAFTS
A variety of dermatomes are available for cutting split-thickness grafts. In general, air/electric powered dermatomes
and the free hand knife (eg, Humby knife, Weck blade, Blair knife) give grafts with irregular edges and varying
thicknesses and both are used to cut lengthwise on the extremity; drum dermatomes are used sidewise across the
extremity, since the rolling maneuver required for graft cutting is best accomplished across a convex surface.Most
commonly used technique involves use of a Dermatome, which provides rapid harvest of large uniform-thickness
grafts.
1. Power dermatomes :
A) Air/Electric Dermatome: Most split-thickness skin grafts in the U.S. are harvested with air/electric powered
dermatomes, which can cut large amount of skin rapidly. A power-driven dermatome uses a rapidly vibrating blade
driven by an electric motor / air turbine.

AIR DERMATOME BROWN ELECTRIC DERMATOME
The adjustable components work like a wood-cutting planer: a flat surface plat form can be raised /lowered, depending
on desired graft thickness. The width of the graft is determined by the width setting on the dermatome.
The thickness is determined by first closing the dermatome opening completely, then opening it by turning the setting
knob to the appropriate thickness. The average split-thickness skin graft is cut at 0.015 inch; this can be checked by
inserting a No.15 BP blade, which approximates that thickness.
Cutting of the graft is accomplished by setting the dermatome flat on the skin, turning on the power, and advancing it
flat across the skin surface with gentle downward pressure. An assistant can press on the skin in advance of the
dermatome, although experienced operator may dispense with this step.
An assistant can elevate the skin as it is cut from the dermatome, to allow graft thickness to be judged.
The thickness the graft, the more opaque it is; an ideal skin graft is slightly translucent. Graft thickness can also be
judged by the type of bleeding observed at the graft donor site. Superficial grafts leave behind many small bleeding
points; deeper cutting leaves fewer bleeding points, which bleed more and grafts cut to deeply expose fat.
Placing the dermatome flat on the skin and maintaining that flatness makes rapid uniform harvesting of skin possible.
Tilting the dermatome down may produce gouging and trenching of the skin.
The electric / gas powdered dermatome can also be used in shaving scars where there is hypertrophy without
contracture with the instrument set at 0.025 to 0.031 inch, scar can be shaved off by repeated strokes until there is a
thin sheet of scar overlying fat; this can be skin grafted, power dermatomes can also be used in tangential excision of
burns, with gradual removal of the burn eschar until bleeding points appear.
B) Castroviejo Dermatome :
This small electrical dermatome can be used for harvesting mucous membrane grafts for reconstruction of eyelid and
socket deformities. The motor moves a small cutting head with the blade that controls the thickness of the cut. Another
small electrical dermatome is produced by the Davol company, incorporating a disposable head. The rechargeable
handle drops into a sterile plastic bag, which is sealed. The disposable cutting heads are present at 0.015 inch and are
clipped into place.
They are used with mineral oil lubrication and can produce satisfactory small grafts. The cutting blades on the small
power dermatomes tend to lose their sharpness rapidly.
2. Drum Dermatomes :
I. Reese Dermatome :

The Reese dermatome a carefully machined instrument, is a modification of the Padgett-Hodd dermatome. An
accompanying set of shims permits careful calibration of the thickness of the graft. There is a disadvantage in that, if
the graft is too thick, it is difficult to change the calibration in the middle of a skin graft removal.
The skin is prepared by applying a topical antiseptic to the donor site, followed by a defatting agent, such as ether
/acetone. The donor site is painted with the dermatome cement, care being exercised that the glue on the brush is not
allowed to dry in order to avoid lumping of the prepared skin surface. Vaseline ointment can be applied around the
pattern to avoid cutting into the surrounding tissue with the dermatome.
While the prepared donor site is drying the dermatome can be assembled. The dermatome sites in a stand that holds
the full set of shims. The clamp bar that secures the carefully folded at both ends along the black lines. One end of the
dermatape is inserted beneath the clamp bar so that the folded edges fits over the face margin of the drum. The clamp
bar is returned to secure the dermatape and is locked in position.
The opposite end of the dermatape is inserted into a slot in the tightening spool. The crank is then rotated to turn the
spool and tighten the dermatape against the drum surface.
The tape is incised along both free surfaces of the drum, and the outer cover is peeled back to expose the adhesive
surface of the dermatape. A disposable blade and shim of desired thickness are inserted into the blade clamp. Round
nuts are tightened at either end to secure the blade clamp. While the instrument is being assembled, the skin is painted
with glue in single strokes. Three minutes should elapse for drying of the adhesive.
To remove the skin, the instrument is first pressed against the donor site along its free edge and then rotated slowly
until the skin begins to fall away at the margins of the burns but still does not become detached. The cutting is started
with almost no more forward force than is present in the weight of the blade assembly. The blade is moved from side
to side while the drum is rotated slowly (dorsiflexion of the wrist) but held steadily; at no time is the blade forced
forward.
If there is any tendency for the skin to pull away at the margins, the drum is pressed more firmly against the skin and
in addition, is rotated slightly toward the cutting blade to roll the skin up in front of the cutting edge.
If the blade tends to cut beyond the width of the drum, this is remedied by vertically lifting the drum away from the
skin and / having the assistant hold the skin away from the drum at each margin with a pair of hemostats. This
complication can also be avoided by spreading mineral oil over the edges of the drum. The completion of cutting can
be affected by lifting the drum and graft away from the donor site and, with a few deft strokes of the blade, cutting the
graft through; alternatively the dermatome may be turned back and the graft severed from the bed with a knife.
The graft is removed by gentle rubbing with a sponge gauze soaked in normal. Saline solution, leaving the glue on the
dermatome. When it becomes necessary to use a donor site such as the neck, chest, flank / other areas of the body
where there may be a depression / bony prominence, it is helpful to fill out such as depression / pad the prominence by
injecting normal saline until it becomes level with the surrounding area. This technique permits removal of grafts from
any area of the body
.

II. Padgett dermatome : It is lighter and can be used more readily. The distance between the blade and drum is calibrated in thousands of an
inch and is adjusted by turning a ratchet on one side of the blade arm. There is now available a plastic tape with glue
on both surfaces. The outer protective cover is removed from the tape, and the latter is applied to the drum of the
dermatome. The thickness of the cut must be increased approximately 0.004 inch to compensate for the thickness of
the tape. The graft can be removed as outlined above for the Reese dermatome, and the skin graft can be easily
removed from the tape.
SELECTION OF DRUM DERMATOMES:
The Reese dermatome provides only a 7 x 4 inch graft. Cutting size, whereas the Padgett dermatome is 8 inches along
and comes in three widths; small – 3 inches wide, medium-4inches wide, and giant – 5 inches wide.
Both drum dermatomes allows harvesting of different thickness of split-thickness graft, but only the Padgett allows
calibration while cutting is being accomplished. However, vigorous cutting with the Padgett dermatome can change
the thickness of the graft unintentionally a misshape that cannot occur with the Reese dermatome.
In terms of handling, the padegett dermatome is lighter and is easy to handle, while the Reese is a heavier instrument.
Both types of drum dermatomes require skin fixation, the Reese dermatome uses an adhesive tape that is applied to a
drum and a glue that is applied to the skin surface. Most Padgett dermatomes depend on the glue applied to both the
drum and the skin surface, although adhesive tapes that fit the Padgett dermatome are also available.
FREE HAND CUTTING OF SPLIT THICKNESS SKIN GRAFTS:

Before introduction of power-driven and drum dermatomes, all skin grafts were harvested with hand-held knives.
These were long, sharp blade with an adapter over the blade that facilitates the cutting of the graft and controlled the
graft thickness. Such knives allowed cutting of very large pieces of skin. However, even in the best of hands the edge
of the graft donor site were always irregular, a problem avoided with the power and drum dermatomes.
With all such knives blade, the basic maneuver is a gradual back and forth movement, similar to that of cutting bread.
Slicing is much more successful than pushing in cutting skin grafts.
The large Humby-type knives are less used today, but smaller knives are often helpful in cutting small grafts,
particularly in an outpatient setting where a dermatome might not be easily available.
Advantages
- Grafts take more readily
- Donor site heals more readily, allowing secondary harvesting at an earlier date.
- Recipient site contracts to a greater degree, limiting the size of the graft.
Disadvantages
- Colour and texture of grafted skin are not well maintained.
- Grafts are less likely to have normal sebaceous activity and sweating.
- Hair is not transferred with the graft (advantageous if hair- bearing donor site to be used for non- hair bearing
recipient site)
- Grafts in children will not grow as the child grows.
-
SKIN GRAFT KNIVES
Before introduction of power-driven and drum dermatomes, all skin grafts were harvested with hand-held knives.
Humby’s knife:
A roller is attached to the knife. By varying the distance between the roller and blade graft thickness can be varied.
Back and forth movement to given similar to slicing bread during skin graft harvest.
Humby knife as modified by Blair and Watson
Other skin graft knives are
1) The Blair-Brown knife
2) The watson knife
3) The cobbett knife
4) Silver’s Miniature Knife.

Procedure:
Positioning the patient:
A, the outer side of the arm.
B, the inner side of the arm.
C, the forearm,
D, the inner side of the thigh—usually the best place.
E, the back of the thigh with the patient’s prone.
F, the back of the thigh with the patient on his back.
G, the outerside ot the thigh.
Preparing the donor site for grafting :

Scrub the donor site with cetrimide and a scrubbing brush and then swab it with a mild antiseptic, such as
cetrimide or hexaclorphane soap. Don’t use iodine or spirit, because they may kill the graft.
Drape the donor site in towels.
Preparing to cut : place yourself comfortably before starting.
HUMBY KNIFE
EQUIPMENT : A skin grafting knife, two graft boards, liquid paraffin, skin hooks non-toothed forceps for handling
the graft, Vaseline gauze, a bowl of sterile saline to put the graft in, sterile cotton wool, and a sterile screw topped jar
staring excess graft.
Local anesthesia : Use plenty of a very dilute local anesthesia, such as 0.4% lignocaine with adrenaline, to puff out
the skin all over the donor site.
The leg : On the patient’s right side, and assuming you are the right handed, cut from below upwards, with a forehand
stroke. Assistant should support the skin of the patient’s thigh from underneath, so as to make its upper surface flat,
and under slight tension from side to side. This will allow to make a smooth cut with water edges.
Cutting the graft

In Humby knife the thickness of the skin to be cut is controlled by a rod. The position of this rod is controlled by a
screw at one end, and a graduated lock nut at the other. Hold the knife upto the light and vary the distance between the
blade and the rod. Make it too narrow rather than too wide, because if the graft is too thin, we can always thicken it. If
the rod touches the blade anywhere they are far too close. Make sure the blade and the knife are flexible, so the
thickness of the graft also depends on how hard you press. Lubricate the back of the knife with liquid paraffin. Keep it
clear of the roller, it may cause the graft to wind round it. Assistant should hold one board behind the knife, to keep
the board still, and to press as the skin so as to hold is flat and in tension as you move the knife.
The operator should hold the second board in the left hand, cut in front of the advancing knife blade. Advance the
board and the blade together along the limb. Apply the knife to the skin at a slight angle and use a regular sawing
movement as if, cutting a loaf of bread. Advance it slowly, and press gently.
The graft usually collects in folds on the knife. When we get to the end of the graft, either cut it with scissors, or bring
the knife to the surface.
Caution :
1) Don’t force the knife down the limb
2) Don’t stop or pull the knife backwards.
After once the graft is cut about 1 cm inspect it for thicknes. Assess this by –
Translucency – A very thin graft is translucent, like tissue paper. Thicker grafts are progressively more opaque.
The pattern of bleeding points. A thin graft produces many thin points, a thicker graft produces fewer and
larger bleeding points
Keep the graft covered with saline soaked swabs until it is ready to store or apply it. If there is much delay,
replace it temporarily on the donor area.
Advantages
Large number of cut blood vessels
Primary healing of donor site
More graft harvest
Disadvantages
Relatively Poor cosmetic result
Contraction
Abnormal pigmentation
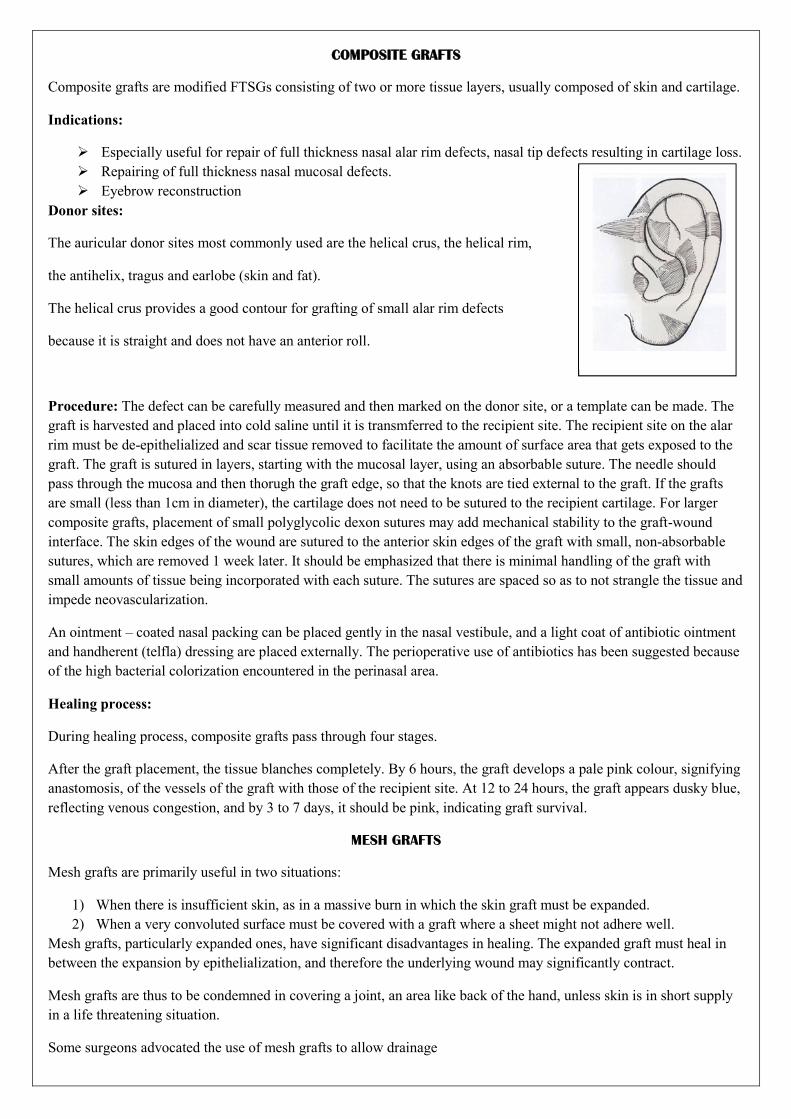
COMPOSITE GRAFTS
Composite grafts are modified FTSGs consisting of two or more tissue layers, usually composed of skin and cartilage.
Indications:
Especially useful for repair of full thickness nasal alar rim defects, nasal tip defects resulting in cartilage loss.
Repairing of full thickness nasal mucosal defects.
Eyebrow reconstruction
Donor sites:
The auricular donor sites most commonly used are the helical crus, the helical rim,
the antihelix, tragus and earlobe (skin and fat).
The helical crus provides a good contour for grafting of small alar rim defects
because it is straight and does not have an anterior roll.
Procedure: The defect can be carefully measured and then marked on the donor site, or a template can be made. The
graft is harvested and placed into cold saline until it is transmferred to the recipient site. The recipient site on the alar
rim must be de-epithelialized and scar tissue removed to facilitate the amount of surface area that gets exposed to the
graft. The graft is sutured in layers, starting with the mucosal layer, using an absorbable suture. The needle should
pass through the mucosa and then thorugh the graft edge, so that the knots are tied external to the graft. If the grafts
are small (less than 1cm in diameter), the cartilage does not need to be sutured to the recipient cartilage. For larger
composite grafts, placement of small polyglycolic dexon sutures may add mechanical stability to the graft-wound
interface. The skin edges of the wound are sutured to the anterior skin edges of the graft with small, non-absorbable
sutures, which are removed 1 week later. It should be emphasized that there is minimal handling of the graft with
small amounts of tissue being incorporated with each suture. The sutures are spaced so as to not strangle the tissue and
impede neovascularization.
An ointment – coated nasal packing can be placed gently in the nasal vestibule, and a light coat of antibiotic ointment
and handherent (telfla) dressing are placed externally. The perioperative use of antibiotics has been suggested because
of the high bacterial colorization encountered in the perinasal area.
Healing process:
During healing process, composite grafts pass through four stages.
After the graft placement, the tissue blanches completely. By 6 hours, the graft develops a pale pink colour, signifying
anastomosis, of the vessels of the graft with those of the recipient site. At 12 to 24 hours, the graft appears dusky blue,
reflecting venous congestion, and by 3 to 7 days, it should be pink, indicating graft survival.
MESH GRAFTS
Mesh grafts are primarily useful in two situations:
1) When there is insufficient skin, as in a massive burn in which the skin graft must be expanded.
2) When a very convoluted surface must be covered with a graft where a sheet might not adhere well.
Mesh grafts, particularly expanded ones, have significant disadvantages in healing. The expanded graft must heal in
between the expansion by epithelialization, and therefore the underlying wound may significantly contract.
Mesh grafts are thus to be condemned in covering a joint, an area like back of the hand, unless skin is in short supply
in a life threatening situation.
Some surgeons advocated the use of mesh grafts to allow drainage

but generally a wound that is producing so much fluid that meshing is
necessary is probably not yet ready for grafting, and measures
should be taken to control such drainage.
Mesh does not prevent loss of a graft from hematoma, if bleeding is profuse
at the time of skin grafting; delay of the grafting is more appropriate.
If mesh grafting is used, a semi occlusive dressing is applied
as there is less tendency for the graft edges to curs as they dry
and less dessication of the underlying wound.
Meshing of split skin graft is accomplished by placing the cut graft on a
plastic carrier and carefully advancing it through a mechanical meshes
by means of crank or by doing it manually
PINCH GRAFTS
Pinch graft can be harvested using Davol-Siman dermatome or the weck blade.
Pinch grafts have traditionally been used as wounds that are draining.
Treatment of the hypopigmentation in localized areas of vitiligo.
Technique :
The donor skin is held with pickups and then lifted. The elevated bit of skin is transected with iris scissors or a
scalpel. Multiple grafts (usually les than 1cm) are harvested and placed almost next to each other, and the spaces in
between heal by epithelialization.
Disadvantage :
The major drawback is the unsightly “HILLOCK” surface irregularity when these grafts heal. This results
from the irregular depth of the graft, which is due to the tenting effect.
To overcome this drawback, Robinson proposed, to use a punch biopsy to obtain a specimen of uniform depth
by limitation of the downward force, thereby limiting the depth to the deep dermis. The fat is trimmed once the plug is
removed, yielding a graft of uniform depth.

SKIN GRAFT “TAKE”
After detaching of the skin graft from the donor site, it becomes potentially a dead piece of tissue. Its life span while
detached depends on the ambient temperature but when wrapped in gauze, moistened in saline and stored in a fridge at
4 degree centigrade. It may be live for up to 3 weeks.
To survive permanently, it must be planted, become reattached and obtain a new blood supply from its new
surroundings and the various processes involved in achieving this are called ‘TAKE’
“THE THINNER THE GRAFT, THE BETTER THE TAKE;
THE THICKER THE GRAFT, THE BETTER THE RESULT.”
Graft take
- Is by fibrin and capillary budding
- Vascular bed is required
- Good opposition essential
- Well- covered bone is needed.
- Bone of palate, maxilla and zygoma. Take can be improved by drilling.
- Crane principle can help.
- Is threatened by prior radiotherapy
- Can be destroyed by fibrinolysing bacteria.
A skin graft adheres to its new bed by fibrin. This diffuses from the plasma bed and supplies the immediate nutritional
requiresments in the form of plasmatic circulation. This is enhanced by the outgrowth of capillary buds such that a
circulation of blood in the graft can be demonstrated at 48 hours. At the same time, fibres grow into the fibrin, which

convert the adhesive clot into a more definite fibrous tissue attachment that increases over the ensuing days so that by
5 days reasonable anchorage has occurred.
The speed and effectivess of this process depend on the provision of a non-infected vascular bed,good apposition of
the graft to the underlying bed without any intervening hematoma and the application of pressure to allow the process
to take place.
The graft bed must have a rich blood supply to enable this process to occur.
SURFACES THAT TAKE A GRAFT WELL ARE
- Granulation tissue
- The soft tissues of the face
- Muscle sascia and fat cartilage
- Bone covered with perichondrium and periosteum.
When tissue has received previous radiotherapy’ it may take a graft less well. Extensive induration and fibrosis with
small amounts of bleeding indicate that grafting may not be successful.
The adherence of a graft depends on fibrin anchorage and any surface which is considered suitable for grafting has
fibrinogen together with the enzymes which convert it into fibrin to facilitate adhesion.
Some organisms can destroy fibrin and prevent the fibrin to facilitate adhesion. The main organisms are beta
hemolytic streptococcus pyogenes and staphylococcus aureus produces fibrinolysin. The presence of these organisms
within the recipient bed requires that the process of grafting be deffered until they are eliminated.
FATE OF A SKIN GRAFT
PHASES OF SKIN GRAFT SURVIVAL
SERUM IMBITION PHASE: When the graft is initially placed on the recipient site, it is devoid of vascular
connections and depends on plasmatic circulation for fluid nourishment. This nutrion is provided by plasma exudates
from dilated capillaries in the host bed.
Immediately after application of the graft and during the subsequent 24 hours, the blood vessels of the grafts appear
less filled with blood and are not readily detected when compared with those in the surrounding skin.
↓
On the first day after grafting, many vessels in the donor tissue show early evidence of distention and are rapidly filled
with static blood.
↓
On the second day vessel distention continues, but blood circulation has not begun, although a sluggish flow of blood
may occasionally be seen in the peripheral vessels.
↓
A slow flow of blood occurs in the graft vasculature on the third or fourth day and continues to improve until the fifth
or sixth day.
↓
GRAFT REVASCULARIZATION

Graft revascularization
Garre (1889) made the following observations.
1.51/2 hours –endothelial mitosis in host bed.
2. 9 hours – presence of inflammatory cells in the grafts.
3.11 hours- invasion of white cells into the donor vessels.
4. third to fourth day- actual revascularization as an invasion of the graft by host capillary buds.
ORGANISATION PHASE: The fibrin clot fixes the graft to the host bed. As the graft revascularised the leukocytes
disappear. On the fourth day after transplantation fibroblasts infiltrate the fibrin net work.
By the seventh or eight day fibroblast infiltration continues as the fibrin clot is resorbed.
Deep layers of the graft are anchored to the host bed by the ningth day, with new vasculture and fibroblasts integrated
in the firm union.
The nerve supply to a transported skin graft is completely served, leaving no sensation in the newly integrated graft.
Within 2 months, neural structures begin to regenerate. The nerve fibres enter the graft through the base and sides,
following vacated neurilemmal cell sheaths.
Timing of replacement and preparation of wound:
Most skin graft failures can be ascribed to flaws in the recipient site, rather than to technical defects in the skin graft
cutting.
Blood supply:
All skin grafts are parasites in that they must depend on blood supply from the wound bed. Therefore, tissue with
limited blood supply bone, cartilage / tendon –does not accept a skin graft.
A surgeon faced with closing an avascular surface must either use a non parasitic tissue such as a flap, / modify the
wound so that it becomes vascular.
Membranous bone that is relatively vascular, as in the denuded orbit of a radical maxillectomy, may accept a skin
graft.
Exposed cartilage is usually removed to allow skin grafting, although occasionally multiple perforations allow
granulation tissue to form.
Chronic granulation tissue may not be sufficiently vascular to support skin grafts and should be resected down to
better vascularized tissue.
Nature of the injury:
The nature of the injury influences the ability of the wound to support a graft. A clean tissue avulsion may accept
immediate skin grafting, whereas crushed / infected tissue is less likely to do so.
Chronic wounds must be free from pus and should have a healthy pink to beefy red appearance with an ideal wound
pH of 7.4 / higher. Epithelial migration at the edges of the granulation surface may be a sign that the wound is ready
for application of a skin graft. Hypertrophic “proud flesh” accepts a skin graft poorly and needs to be either trimmed /
flattened with hypertonic (3%) saline pressure dressings.

Quantitative microbiology:
All granulation tissue contain bacteria, but not all are infected. The presence of more than 105 organisms per gram of
tissue, as shown by quantitative bacteriology, almost always leads to loss of the graft. Such quantitative bacteriology
may help surgeon to decide whether / not a wound will accept a skin graft. A high bacterial count should be reduced
judiciously with antibiotic and local wound therapy.
However, even a clean, healthy, granulating wound contains some bacteria, a situation that usually leads to use of a
split-thickness rather than a full-thickness skin graft.
Systemic Conditions: Whenever possible, underlying systemic conditions causing the wound should be corrected
before skin grafting is attempted.
Preparation of the wound: A chronic wound to be skin grafted must be free of necrotic tissue. This can be achieved
by the use of sharp debridement followed by local treatment with wet soaks of half strength Dakin’s solution (0.25%
NaCl). Other techniques, such as enzyme ointment / wet-to-dry dressings, are less effective.
Operating room treatment of the graft bed at the time of skin grafting is important in both acute and chronic wounds.
Scrubbing the graft bed with detergents can increase the rate of infection. The wound should be cleaned with a more
benign substance such as saline / betadine solution. Surgical debridement may cause profuse bleeding, and hemostasis
is essential for a graft to survive. Hemostasis can be achieved by electrocautery, ligation of vessels / application of
pressure.The use of hemostatis substance such as oxycel /gel foam is hazardous when skin grafting is to be done, as
they provide a nonvascular block between the recipient bed and graft. Placing a graft on a rapidly bleeding surface
results in hematoma formation and graft loss.
GRAFT IMMOBILIZATION AND POSTOPERATIVE CARE
For a skin graft to survive on its wound bed, it must adhere well enough to allow blood vessels to grow across the
gap. In most cases of skin grafting, the optimal dressing is a bolus or tie-over dressing. This is fashioned by placing
sutures around the periphery to hold the graft onto the wound bed.
Bolus or tie – over dressing

In placing the skin graft on the wound for a bolus tie-over dressing. The skin graft is laid over the bed but neither
stretched excessively nor wrinkled. The graft is sutured using 4.0 or 5.0 silk, with sutures as close together as
necessary, depending on the location. Facial sutures may be as close as 2 to 3 mm, whereas in other areas they may be
as far apart as 1.5 to 2.5 cm. The sutures are tied over a piece of fine mesh, ointment impregnated gauze, covered with
cotton sheeting or cotton balls. Care should be taken in placing the wadding material so that it is pressed down into
any recesses to allow the graft to sit evenly on the wound. The tied sutures gently press the dressing down onto the
skin graft, which in turn is pressed onto the wound bed. This maneuver immobilizes the wound bed. This maneuver
immobilizes the graft on the wound and prevents hematoma collection. An outer dressing may be applied if desired.
Before the tie-over dressing is applied, the surgeon should ensure that there are no blood clots underneath the graft.
These can be expressed by pressure, irrigated out with saline, or cleansed with small cotton-tipped applicators. This
step before application of the dressing provides better adherence of the graft and improved survival rates.
Objective
The Main Object Of The Tie-Over Dressing Is To Ensure Contact Between The Graft And The Host Bed. Such
Contact Can Also Be Achieved By Using A Circumferential Compression Dressing With An Extremity Skin Graft.
Dressing Removal
The Dressing Is Left In Place For Approximately Seven Days, At Which Time The Sutures Can Be Removed.
Skin Graft Inlay Method
A variation of the bolus method of dressing is the skin graft inlay method. The bolus dressing is often referred to as
the stent dressing, which has been derived from the skin graft inlay method. Dental compound used as the central
material in a graft placed in the oral sulcus. A skin graft is wrapped around dental compound, the dermal side out. This
combination of graft and dental compound can then be placed into the labial sulcus defect, where the graft will heal.
Such grafts should also be splinted for six months to resist contraction.
Skin graft outlay technique
The skin graft outlay technique is similar to the inlay technique but involves tying of sutures over the top of the
combination of dental compound and skin graft. This method allows placement of a large area of graft relative to the
defect.
Vaccum assisted closure
Another dressing choice for an irregularly contoured wound or wound with high levels of exudate is the vacuum-
assisted closure (VAC) sponge. These dressings conform to the wound surface by suction and promote skin graft
adherence while removing exudate and edema from the surrounding tissues. A nonadherent material such as Adaptic
must be placed as an interface between the skin graft and the sponge to prevent peeling the graft off when removing
the VAC sponge. Grafts placed on the extremities may be managed with elevation and compression dressing for the
entire extremity distal to the graft to prevent edema, which can prevent graft adherence.
Open technique
Requires an Ideal wound bed, without bleeding or fluid production.Cooperative or sedated patient.Limited motion is
allowed to the patient.Graft usually is pink, adherent and viable within 48 hrs.Crusts appearing around the margin may
be left in place to allow natural separation.
Other methods
Use of a cast or splint is useful when grafting over a mobile surface to prevent motion and shearing forces that
disrupt graft adherence, and when dealing with a poorly compliant patient unable to maintain a soft dressing. Burn
netting also may be useful for securing dressings in difficult locations such as the pelvic and shoulder regions.

Finally, the graft may be treated open with no dressing at all except a layer of ointment to prevent desiccation.
This technique is susceptible to hematoma or seroma formation beneath the graft, because no pressure is applied
and it is used infrequently.
WOUND CARE
Superior dressings have been shown to be of the semiocclusive variety. These products have been shown to have the
Fastest healing rates ( 9 days to re-epithelialization),
Lowest subjective pain scores,
Lowest infection rates (3%), and
Are among the lowest in cost.
Advantage of being transparent - allows ongoing inspection of the site - maintaining sterility.
Fluid collection - promotes moist wound healing - more rapid healing rates and decreased subjective pain
scores.
The rate of healing is proportional to the number of epithelial appendages remaining and inversely
proportional to the thickness of graft harvested.
PHASES OF SKIN GRAFT SURVIVAL
Hair rarely grows from split-thickness grafts. Sweat glands and sebaceous glands initially degenerate following
grafting. Sensation returns to the periphery of the graft and proceeds centrally. Split-thickness grafts reinnervate
more quickly. Grafts may remain pale or white or may become hyperpigmented with exposure to sunlight.It is
generally recommended that the graft be protected from direct sunlight for at least 6 months or even longer
postgrafting.
Serum imbibition :
Hubscher (1888) and Goldmann (1890) suggested that Thiersch grafts in human patients were nourished by
fluid from the host before the establishment of new vascular and lymphatic channels in the graft. They termed this
early process of fluid nourishment the “plasmatic circulation” of a graft.
Most investigators have generally accepted Hubscher’s original concept of plasmatic circulation as an
important factor in the early nourishment of skin grafts before the restoration of an adequate blood supply. However,
Clemmesen (1962; 1967) believed that the main role of the plasmatic circulation is not nutritional. He felt that it
serves to prevent desiccation of the graft and to keep the graft vessels open. Henry and associates (1962), working
with human skin grafts, reported that the donor skin derives its nutrition and oxygenation from the process of
plasmatic circulation for the process of plasmatic circulation for the first two days after grafting. Thereafter, this type
of nourishment is insufficient to maintain the viability of full-thickness grafts, unless it is supplemented by an
adequate vascular supply.
Smahel (1971; 1977) suggested that the existence, condition, and duration of the phase of plasmatic
circulation depend on the following factors:
1) The graft thickness
2) The length of time a recipient bed is allowed to remain open and heal before the graft is applied
3) The time lag between the excision of a skin graft from the donor site and its subsequent application to the
recipient site.
Studies on color changes in skin grafts: The graft when excised from the donor becomes chalk white and
blanched. Within a few hours after grafting it takes on a pinkish hue, which progresses to a bright pink during the next
few days.

Hynes (1954) observed that the blood vessels in a freshly cut human skin graft varying from split thickness to
full thickness, are collapsed and empty. The graft vessels, probably as the result of separation from the donor site,
undergo spasm, expelling most of the formed hemic elements through the severed ends of the vessels on the graft
undersurface. Within 24 hours after transplantation, the graft vessels are again dilated. By 48 hours, the vessels are
more distended and contain large numbers of erythrocytes. The exudate that accumulates at the line of demarcation
between the graft and host tissues consists of plasma, erythrocytes, and polymorphonuclear leukocytes. This fluid
exudate, after precipitating its fibrinogen in the form of fibrin on the surface of the host site, penetrates the overlying
graft vessels as a fibrinogen-free suspension of erythrocytes, thereby nourishing the grafts and explaining the rapid
color change that occurs within hours after transplantation.
Summary : The phase of serum imbibition may be described as a period during which the graft vessels fill
with fibrinogen-free fluid and cells from the host bed. The term “circulation” is actually a misnomer, because the fluid
absorbed by the graft from the host bed is passively trapped with the graft. Endothelial in growth from the host
progresses until a definitive vasculature is established. The stagnant fluid absorbed by the graft during the early phase
of serum imbibition is eventually drained by the newly established blood and lymphatic circulation. Clinically, skin
grafts usually appear edematous and their surfaces are elevated above the surrounding host skin during the early
postoperative period. Within a few days after grafting, however, the graft flattens and edema subsides. This
observation reflects the establishment of a plasmatic and hemic flow and evacuation of the fluid initially trapped in the
graft
GRAFT REVASCULARIZATION
Autografts and allografts :
Controversy has existed over the method of graft acceptance and the mode of graft vascularization. Several
research techniques have been developed to study the physiology of graft acceptance and vascularization.
Bert (1863) first noted an early connection between the blood vessels of the graft and host and employed the
term “abouchement” to illustrate the mouth-to-mouth apposition of the vessels. In 1874 Thiersch, studying the
histologic sections of experimental full-thickness skin grafts in man, used the term “inosculation” to signify the direct
connection between graft and host vessels.
Garre (1889), studying human skin grafts, reported evidence of endothelial mitosis in the host bed 5 ½ hours
after grafting, the presence of inflammatory cells in the grafts by 9 hours and invasion of white cells into the donor
vessels at 11 hours. He discounted the importance of the inosculatory process and described actual revascularization as
an invasion of the graft by host capillary buds, which began on the third or fourth day, after most of the original graft
vessels had become obliterated.
Braun (1899) believed that graft revascularization was achieved by a dual process of ingrowth of host vessels
and anastomoses between the host and original graft vasculatures.
These early changes may be summarized as follows: immediately after application of the graft to the recipient
bed and during the subsequent 24 hours, the blood vessels of the grafts appear less filled with blood and are not
readily detected when compared with those in the surrounding skin. On the first day after grafting, many vessels in the
donor tissue show early evidence of distention and are rapidly filled with static blood. On the second day vessel
distention continues, but blood circulation has not begun, although a sluggish flow of blood may occasionally be seen
in the peripheral vessels. A slow flow of blood occurs in the graft vasculature on the third or fourth day and continues
to improve until the fifth or sixth day. During subsequent days, a return of all blood vessels to normal caliber and
circulation occurs in all autografts.
In allografts, the similarity persists only until the onset of the allograft rejection. This rejection reaction is
heralded by increased distention in the vascular system, followed by the appearance of a sluggish circulation with
clumped elements. Complete cessation of blood flow and vascular occur between seven and ten days after grafting.

Initial healing
Skin Graft “Take.” When a skin graft is cut, it turns pale as it is separated from its blood supply. Vessels
within the graft constrict and squeeze out red blood cells. when the graft is placed on a wound, it slowly regains its
former pink color as circulation returns. The graft survival on its new blood supply is a clinical “take”. Pressure on the
graft after three or four days should lead to blanching and immediate refilling of the blood vessels.
If the graft does not become revascularized, partial or complete necrosis develops. If the graft is thick, the
upper portion of the graft may slough and yet deeper portions may remain, so watchful waiting is indicated.
Cellular Hyperplasia :
Within the first two weeks after graft healing a pronounced epidermal hyperplasia occurs, manifested by
surface scaling and crusting. Within the first week the thickness of the epidermis can increase seven to eight fold. The
hypertrophic epidermis has invasive characteristics at the edge of the graft; it can invade the surrounding dermis or
granulation tissue, lifting a picture-frame rim of tissue around the healing graft (Gillman and associates,1953). The
tendency for graft epithelium to spread may be seen on the undersurface of a graft chronically elevated by serum
(Littlewood, 1960). Since hair follicles and sebaceous sweat glands are exposed on the undersurface of a split-
thickness graft, a chronic seroma may lead to epithelial growth underneath the graft and cause that portion of the graft
to slough.
Dermal fibroblasts proliferate vigorously in healing skin grafts after an initial decrease of three days. By the
seventh to eighth day there is a marked hyperplasia of fibroblasts as the graft begins to heal (Converse and Ballantyne,
1962). These fibroblasts are probably derived from local tissue and new blood vessels synthesize collagen within the
skin graft to play a significant role in its eventual healing.
Maturation
After the grafts have become vascualrized and have “taken”, they undergo changes that continue for many months, a
remodeling process that has significant effects on the ultimate result of the skin graft.
Graft contraction. Contractile fibroblasts, known as myofibroblasts. Skin grafting can affect this process,
depending on the type of graft. Surgeons often speak of “skin graft contraction,” but in fact what is seen is a
combination of graft and wound contraction. Most likely it is the wound bed that contracts and the graft follows. Split-
thickness skin grafts contract more where the wound is pliable and mobile (as on the skull periosteum). On a similar
wound, full-thickness grafts contract minimally, while split-thickness grafts contract significantly.
The contraction of a healing graft and wound is referred to as secondary contraction. In contrast, primary contraction
refers to the immediate elastic recoil of a graft as it is cut. Primary contraction is greatest in full-thickness grafts and
least in thin split-thickness grafts. Secondary contraction is clinically more important.
The dermal component of grafted skin appears to exert the main influence on wound (secondary) contraction
(Rudolph, 1976). It has been said that thicker the skin graft, the less does wound contraction occur, a statement that is
not fully accurate. Very thick skin grafts obviously may slough and result in wound contraction.
Dermal Collagen Turnover:
Quantitative isotopic studies by Klein and Rudolph (1972, 1974) have shown a massive turnover of collage in skin
grafts. In all types of skin grafts, 85 to 88 per cent of the original collagen was lost by 140 days. Full thickness grafts
had significant new collagen synthesis, more collagen being synthesized than was lost as the grafts grew with the
animals. Split-thickness grafts, in contrast, lost surface area and never regained the total amount of collagen lost. Skin
grafts from older animals had a slower collagen turnover, a trend not reversed by grafting old skin onto young
syngeneic animals.
Pigment changes : A major problem with skin grafts is pigment mismatch. Full-thickness grafts maintain the best
pigment match and are thus preferred in areas such as the face. Facial full-thickness grafts from the postauricular or
supraclavicular areas, however may retain a permanent ruddy tone.

Split-thickness grafts often develop significantly dark pigmentation, particularly in darker-skinned patients. Skin
grafts from the buttocks and abdomen applied to the face may produce a major pigment mismatch as the grafts
develop a brownish-yellow hue. The best way to prevent hyperpigmentation is to use a well-matched, full-thickness
graft.
Epithelial appendages: Hair follicles undergo hyperplasia of the epithelium in the healing graft, a phenomenon
observed in the other epithelial structures. If a full-thickness graft is transplanted with intact hair follicles, the skin
often regrows hair in the same pattern as before. This is the basis of small plugs of hair-bearing skin being
transplanted to the scalp to correct male pattern baldness. Larger strips of skin can be used to replace missing
eyebrows. In a poorly healing graft, hair growth may be nonexistent, sporadic, or depigmented. Split-thickness grafts
rarely grow hair unless they are cut quite thick. Donor sites must be selected in children to avoid later unwanted hair
growth, for example, in full-thickness groin donor sites. Sweat glands ultimately resume function, with more complete
function in full-thickness than in split-thickness grafts. Following nerve regeneration, sweating in the graft is
dependent on the site to which it is transplanted rather than the site from which it came. Sebaceous glands are more
preserved in full-thickness grafts therefore tend to have a softer and more pliable appearance in their healed state. Both
split thickness grafts and their donor sites may scale and remain itchy and dry for many months because the
lubricating sebaceous glands have been temporarily devitalized. Lubrication with bland ointment such as lanolin or
cocoa butter helps to replace the lubricating function. Thicker split-thickness grafts and donor sites from thin grafts
usually regain normal sebaceous gland function. Such function is independent of nerve return.
Durability and Growth: Graft durability is related to its thickness. Thick grafts have greater resistance to trauma and
thus full-thickness grafts are preferable in areas such as the fingertips. Full-thickness grafts grow successfully in
children, whereas the growth of split-thickness grafts may be limited.
Innervation of Skin Grafts : Once a skin graft is placed on a wound bed, sensation is regained as nerves regrow into
the graft. In some areas, such as the fingertips, graft sensation return is particularly important. Full thickness grafts
appear to achieve better sensation than split-thickness grafts, although the rate of return of innervation is faster in split-
thickness grafts. Ponten (1960) found that touch and two point discrimination were accurate indicators of
reinnervation in humans. He reported that the sensory pattern of skin grafts becomes that of the recipient wound bed
rather than that of the original graft donor site. Fitzgerald and associates (1967) reported that sensation in skin grafts
returns from the margins toward the center.
Most patients with skin grafts do not obtain completely normal sensation, although they may have protective
sensation. The recovery of sensation in humans can begin as early as one to two months after surgery, and may be
abnormal during the first year or two. Pain may be more intense than in the surrounding skin, and touch, heat, and cold
may be perceived as painful. Pain sensation develops most rapidly; those of touch, heat, and cold return later. The
recipient site is important is determining the quality of sensation in skin grafts. Grafts placed on periosteum and
muscle usually do not acquire satisfactory sensation.
STORAGE
In storing any viable tissue, one must deal with the basic problem of controlling the destructive effects of hypoxic
metabolism. A tissue removed from its blood supply dies unless the metabolic activity of the cell is decreased, or
nutrients are provided to it. (Rudolph, Fisher, and Ninnemann, 1979).
Autograft Banking: The simplest type of banking is that which occurs when a skin graft has been cut and yet cannot
be used immediately because of inadequate bed hemostasis or suitability. Shepard (1972) has pointed out that a skin
graft can be placed back on its donor site and harvested within five days to be used in the recipient area. This may
cause pain and bleeding upon removal of the graft but is a useful clinical technique.
Skin grafts may also be stored fro longer periods, away from the patient, by being refrigerated. Such grafts may be
moistened in sterile saline with antibiotics as desired and then placed in a refrigerator, where they may retain viability
as long as 21 days.
Allograft storage: Perhaps the most successful and commonly used storage technique for skin grafts is that of cadaver
allografts. Specialized skin banks have been developed to store large amounts of cadaver skin for treatment of massive
burns. Standardized techniques for graft preservation use glycerol and rapid freezing with liquid nitrogen. The treated

allografts are thawed and used for temporary burn dressings to be changed every five days. Pigskin xenografts have
also been used fresh or frozen for burn treatment.
Recently devised artificial membranes, composite grafts composed of shark cartilage glycosaminoglycans, bovine
collagen, and autogenous epidermis tissue cultured cells and growth of large sheets of tissue that will take on patients
who have lost substantial areas of skin. Such techniques, if successful, may obviate the need for harvesting and tissue
banking of allograft skin.
DONOR SITE HEALING
Full-Thickness grafts:
These leave behind an open wound with no epithelial remnants. Most full-thickness grafts are cut so as to
allow direct primary closure of the donor site after undermining. Rarely, split-thickness grafting of the full thickness
donor site can be done. The healing full-thickness donor wound is generally under sufficient tension for hematoma not
to be a major problem, although a small drain can be placed for one to two days.
Split-thickness grafts:
When a split-thickness skin graft is cut there is an immediate blood loss measured by Robinson (1949) as 46 cc
from a 4 x 8 inch area. After graft cutting, there is an initial blood loss at the donor site, followed by an inflammatory
reaction with edema and exudation of protein. A scab of blood and fibrin soon forms over the surface of the wound.
Within the first 24 hours, epithelium begins to grow from the epithelial remnants in the dermis such as hair follicles,
sebaceous glands, and sweat glands. Epithelial migration also occurs at the wound margins. The more superficial a
split-thickness graft is cut, the faster the donor site will heal. This may be as soon as seven days in a thin split-
thickness graft. Donor sites from which thicker split grafts are cut may not heal for several weeks.
An important consideration is that the new epithelium on a split-thickness donor site is not durably attached to
the underlying dermis in the early stages. Tape removal can tear this fragile epithelium and must be guarded against.
Epithelial healing is fastest in areas with multiple accessory skin structures such as the face, and less so in areas with
scanty epithelial residual glands and hair follicles.
When a split-thickness graft is cut, the blood should first be absorbed with pads or sponges. A dressing is then
applied of a single layer of nonadherent Xeroform gauze, followed by a layer of Telfa and bulky gauze and Telfa can
be removed, leaving behind the Xeroform gauze, which can be allowed to air dry. A gentle heat lamp application
speeds epithelization. In an area where external contamination is likely, a large pad can be placed and left in place for
the expected time of healing.
DERMAL OVERGRAFTING
Application of split-thickness grafts to a bed of dermis or scar tissue after removal of the surface epithelium. First
described by Webster in 1954.
Principle
Mature scar possess capillary circulation capable of vascularising the overlying skin grafts – rapidly adherent.
Application of split thickness graft – restore the elastic dermal fat.
Indications
1. Extensive unstable, contracted, depressed, pigmented or hypertrophic mature scars.
2. Venous stasis ulcers.
3. Extensive pigmented nevi.
4. Chronic radiodermatitis.
Complications
1. Failure of survival of the grafts is unknown.
2. Appearance of epidermoid cysts in the graft or in the host dermis.

Causes of graft failure
1. Inadequate graft bed (poor vascularity)
2. Hematoma
3. Movement
4. Infection
5. Technical errors such as placement over epithelizing wound, grafts cut too thick or too thin, or upside-down
graft
6. Poor storage of grafts.
SKIN SUBSTITUTES
Types
Temporary - material designed to be placed on a fresh wound (partial thickness) and left until healed
Semi-permanent-material remaining attached to the excised wound, and eventually replaced by autogeneous
skin grafts
Permanent incorporation of an epidermal analog, dermal analog, or both as a permanent replacement
Ideal properties
Rapid and sustained adherence to wound surface
Impermeable to exogenous bacteria
Water vapor transmission similar to normal skin
Inner surface structure that permits cell migration, proliferation and in growth of new tissue
Flexibility and pliability to permit conformation to irregular wound surface, elasticity to permit motion of
underlying body tissue
Resistance to linear and shear stresses
Prevention of proliferation of wound surface flora
Tensile strength to resist fragmentation when removed
Biodegradability (important for "permanently" implanted membranes
Low cost
Indefinite shelf life
Minimal storage requirements
Absence of antigenicity
Tissue compatibility
Absence of local and systemic toxicity
AVAILABLE BIOLOGIC AND SYNTHETIC SKIN SUBSTITUTES
Naturally occurring tissues
- Cutaneous allografts
- Cutaneous xenografts
- Amniotic membranes
Skin substitutes
- Synthetic bilaminate
- Collagen based composites
Biobrane
TransCyte
Integra
Collagen based dermal analogs
- Deepithelized allograft
- Alloderm

Culture-derived tissue
- Bilayer human tissue (Apligraf)
- Cultured autologous keratinocytes
- Fibroblast seeded dermal analogs
- Collagen-glycosaminoglycan matrix
- Epithelial seeded dermal analog
Solid silicone polymers
Uniquely permeable to water vapor
Impermeable to bacteria and toxins
Control evaporative water loss
Flexible, durable, non-antigenic
Polyurethane, polyvinyl
Impermeable to bacteria, toxins
Minimally permeable to water vapor which can lead to fluid collections
Some flexibility
Difficult to add pores without weakening structure
Nylon
Can make into a fine weave markedly increasing surface area for contact
Can control adherence by type of weave
Can bond collagen
Durable, non-allergenic
Apligraf:
1. Apligraf is supplied as a living, bi-layered skin substitute.
2. Apligraf consists of living cells and structural proteins.
3. The lower dermal layer combines bovine type 1 collagen and human fibroblasts (dermal cells
4. The upper epidermal layer is formed by promoting human keratinocytes first to multiply and then to
differentiate to replicate the architecture of the human epidermis.
5. Unlike human skin, apligraf does not contain melanocytes, langerhans' cells, macrophages, and lymphocytes,
or other structures such as blood vessels, hair follicles or sweat glands.
Dermagraft :
• Dermagraft is a skin substitute that is made from living human cells known as fibroblasts.
• These cells are placed on a dissolvable mesh material.
• Over time, the cells grow and form a skin substitute and the mesh is absorbed.
• The dressing covers and protects wounds while supporting healing.
Transcyte
It is a bi layer, temporary skin substitute which contains both human biologically active healing factors in
direct contact with the wound surface as well as an external synthetic barrier against environmental insults
Indications for allografts and xenografts
ALLOGRAFTS
Autotransplantation of skin is widely used in reconstructive surgery and usually produces excellent results.

When a patient has a loss of full thickness skin coverage exceeding 30% of body surface autografts often are not
available in sufficient quantity temporary coverage can be obtained by skin allografts from volunteers, recently
deceased patients, or the patient’s relatives and friends and is often a life saving procedure.
Indications
• Extensive burn wounds.
• Denuded wounds.
• Biologic dressing.
Functions
-To clean granulating wounds prior to auto grafting.
-To protect open wounds from water and protein loss until autografts are available
-Pain relief.
-Promote healing in a better environment.
Disadvantages
• Graft rejection
• Coverage of STGS donor site with allograft and a subsequent graft rejection will convert the partial thickness
defect into a full thickness defect.
• Availability.
• To avoid graft rejection it has to changed every three to four days when used as biologic dressing.
XENOGRAFTS
Rogers and Converse (1958) used experimental fetal calf xenografts as biologic dressings in humans and observed a
surprising lack of host reaction to the xenografts even after 12 to 17 days of graft retention. Bromberg. Song, and
Mohn (1965) popularized the application of porcine xenografts as temporary biologic dressings.
Burleson and Eiseman (1973) felt that the efficacy of biologic dressings could be attributed to their ability to adhere to
tissue, and that the adherence was due to a fibrin-elastin biologic bonding system. the same authors (1972)
demonstrated that the unique adherent qualities of porcine skin were responsible for its antibacterial effect.
While xenografts have been most extensively used in covering large burn wounds before autografting, the use of
xenografts has also been extended to the temporary coverage of exposed vessels, tendons, leg ulcers, flap donor sites,
and skin graft donor sites.
Xenograft revascularization
The mode of vascularization and the morphology of vascular changes following the application of skin
xenografts have not been extensively investigated. It has been generally held that, because skin transplanted between
members of different species induces a more rapid and violet response than do allografts, the survival time of
xenografts is too restricted to permit a successful reestablishment of blood circulation.
In 1960 Woodruff stated that xenografts show little or no evidence of vascularization and that ischemia, rather
than immunologic rejection, is responsible for the failure of these grafts. Indeed, for a long time most authorities
agreed that xenografts invariably fail to receive a direct blood supply from the recipient before the onward rush of the
rejection phenomenon. However, during the past two decades there have been indications in the literature that skin
xenografts, particularly among certain rodents and between certain animal species, are capable of being revascularized
from the host bed. There have also been reports of vessel distention, breakdown of the endothelial wall, blood clots,
and focal hemorrhages in the dermis of a skin xenograft undergoing rejection, similar to those seen in allograft
rejection.

RECONSTRUCTION

I. FOREHEAD RECONSTRUCTION Peripheral units of face (eg, forehead, cheek) are like a picture frame. They complement the "painting" but are of secondary importance and are not critically analyzed in detail. Peripheral units are typically flat and expansive and relatively uninteresting. Their outline borders vary from face to face, hairline position, and style and expression. Peripheral units present a less demanding challenge to the surgeon. When reconstructing the peripheral forehead unit, methods of tissue transfer and of flap design can be chosen with specific unit requirements in mind. The forehead is flat, expansive, and uninteresting, covered by shiny tight, smooth skin of uniform quality Its
dimension and outline are variable. Its borders are not fixed but change from person to person with age, sex,
hairline position, hairstyle, and expression. The outline of its contralateral forehead subunit cannot be compared in
any view. The quality of the skin of the forehead and scalp are similar except for the presence or absence of
hair. Both are composed of skin, subcutaneous tissue, galeofrontalis, and a thin areolar layer separated from the
underlying periosteum and skull. The scalp forehead complex is richly perfused by multiple axial vessels.
Reconstructive options include:
1. Skin Grafts - Skin grafts heal with an unpredictable color and texture and so often stand out as an unsightly patch within normal adjacent forehead skin when used to resurface small to moderate forehead defects. However, a skin graft can be used to replace the entire forehead unit or a lateral subunit. It should extend into the dense hair abutting the hairline and brow on a bevel to ensure smooth contour transition. If the entire subunit is resurfaced, a shiny, tight skin graft may appear to be the expected shiny, tight forehead.
2. Secondary Intention Healing - When wounds heal secondarily, granulation spontaneously fills the defect. Simultaneously, adjacent normal tissue is expanded by contracting myofibroblasts, and any residual raw area epithelializes. The final shiny, flat scar, supported by the rigid underlying bony platform, blends well into the normally shiny, tight forehead surface.
3. Forehead-Scalp Rotation Flaps - Moderate-to-large forehead defects are ideally repaired with large, well vascularized local rotation flaps containing all layers of the forehead and scalp. The larger the flap, the easier the primary closure of both the recipient and donor sites. A shift of hairline position at the junction of forehead and scalp will pass unnoticed if a hairline notch is not created. A significant distortion of the borders of this peripheral, nonfixed unit does not occur because, although the hairline determines the height, width, and outline of the forehead unit, the hairline is normally variable in position from patient to patient, with age, and during expression. If less than one half of the vertical dimension of the hemiforehead defect is missing, sufficient skin
remains to permit the ipsilateral rotation of residual forehead skin and adjacent scalp. Primary closure of
both the recipient and donor sites is easily accomplished. A vertical incision from the defect is carried
upward to the hairline and then follows the hairline into the temple bay before passing into the scalp. This
avoids the creation of a hair-bearing step-off at the new hairline when the flap moves forehead. On
closure, the hair-bearing scalp flap slides along the junctional portion of the operative incision, which

parallels the old hairline. The hairline is lowered on the operated side, but a significant visible step-off
distortion of the hairline is avoided.
In larger hemiforehead defects, sufficient skin superior to
the defect does not remain, and a contralateral rotation
flap is used. An oblique incision can be made across the forehead
into the contralateral temple bay. Glabrous skin from the
opposite hemiforehead and scalp is shifted from the opposite
side to the defect, permitting primary closure of both recipient
and donor sites. Both techniques lower the forehead hairline,
but the forgiving nature of the forehead unit borders creates no distracting deformity.
Midline forehead reconstruction
The midline is the void of muscle fibres and may be considered the boundary between both paramedian
forehead subunits. The natural dehiscence and/or attenoution of the frontalis muscle in the midline center
offers possibilities to close a defect in a vertically oriented fashion with predictably good esthetic results.
Vertical closure may be contraindicated if the medial brows are brought too close together, which causes a
worried look. For defects slightly off centre, sufficient tissue should be removed to the medial edge of the
wound to create a symmetrical defect position, preferably directly over the midline.
Fusiform closure is performed by recruiting tissue laterally after subgaleal undermining. Even tissue from the
temporal region may be mobilised by extending the subgaleal undermining into the temporal region while
hugging the superficial layer of the deep temporalis fascia. Care should be taken to preserve the integrity of
the facial nerve branches, while detaching the temporal line and supraorbital ligament.M-plasty, that has its
limbs tucked into the natural foldof the glabella, would be acceptable in preventing too much narrowing of the
eyebrows. In the vertical midline closure tension on the skin edges should be reduced using various types of
buried galeal and subcuticular sutures.
Large rotation flaps may be created, by extending incisions in the relaxed skin tension lines on either side of
the defect, while excising a burrow triangle at the base of the defect, thus the round defect is converted to an
A-shaped defect and subsequently to a T-shaped closure line with the vertical limb in the midline and the
horizontal limb in the relaxed skin tension lines. Rectangular advancement flap in the midline are not very
useful because of the inelasticity of the skin and the described alternative of vertical midline closure.

Paramedian forehead Reconstruction
The paramedian forehead runs from the midline to the midbrow area. If the defect is too large for primary
repair or has a lengthy vertical orientation, advancement flaps are usually the preferred method of closure.
Given the inelasticity of the forehead skin a bilateral advancement flap (H-plasty) offers improved
redistribution of tension but creates more complex scarring. Flaps are usually created with an approximate 4 :
1 length to width ratio.
The depth of dissection of these flaps is determined by the depth of the defect as well as the weighted risk of
sensory loss. Dissection in the midsubcutaneous plane aims to maintain the neurovascular bundle. If the defect
extends to the depth of the galea-periosteum, the flaps are incised to the depth of periosteum, vertically
oriented nerve fibres are sacrificed and a deep-layer galeal closure is utilised.Thinning of the flaps should be
avoided. The horizontally oriented closure tension on the convex surface of the forehead may pull the natural
wound edges of the defect inward, while pushing the relative excess tissue bove and below the former defect
upward.
Transposition flaps from the midforehead tissue reservoir may be used for suprabrow defects in order to
maintain brow position and shape.
Transposition flaps from the midforehead tissue reservoir may be used for suprabrow defects in order to
maintain brow position and shape. Defects at the border of the anterior hairline may be closed with rotation
flaps, making use of the curve of the forehead while the additional incision comes to lie in the esthetic
junction of the forehead and hairline. Bilateral rotation flaps may be used in an A-T fashion.
Lateral forehead Reconstruction
The lateral forehead begins at the midbrow and extends to the lateral brow where it joins the upper temple.The
enhanced elasticity of the lateral forehead compared to the central part of the forehead yields a number of
reconstructive alternatives. Primary closure may be possible. The flat surface of the lateral forehead may yield
reasonable results with secondary intention healing. Elevation of the brow by scar contraction must be
prevented. The brow may be tacked down by sutures to the supraorbital rim.

Multiple types of transpositions flaps may be oriented so that donor site closure takes advantage of temporal
laxity latero-inferiorly. Designing skin flaps in the lateral forehead temporal region must take the course
andintegrity of the temporal branch of the facial nerve as an extremely important landmark. Subsequently
dissection should be in a subcutaneous plane to prevent injury to the motor nerve of the forehead.
Furthermore, flapsshould be designed in order to prevent distorsion of the eyebrow. A burrow wedged
advancement flap is created by extending an incision unilaterally along the base of the triangular defect and
creating a smaller triangular-burrow excision on the other side of the incision opposite thedefect. The lateral
burrow triangle may be hidden in the crowfeet. The wound may even be extended to the brow margin in order
to camouflage the releasing incision in the suprabrow transion zone. A number of other variations such as O-Z
repair may yield satisfactory results in the concave surface of the lateralforehead.
Temporal reconstruction
The eyebrow, scalp hairline and lateral canthus as well as zygoma compromise the esthetic boundaries of the
temporal region.When excisions and flap reconstruction are performed in the temporal region, the frontal
branch of the facial nerve which courses very superficial, may be at risk. Moreover, the skin and subcutaneous
soft tissues over the zygoma are very thin.In the lateral forehead proper, the nerve is better protected by the
frontalis muscle.
The temporal region is an ideal indicationfor secondary intension healing. Given its skin laxity primary
closure may definitively be an option. A variety of skin flaps are useful to close smaller defects within the
esthetic subunit or to recruit tissue for a larger defect. For example, tissue may be moved over a larger area
using single or bilobed transposition flaps (anteriorly or posteriorly based).
II. SCALP RECONSTRUCTION The scalp represents the thick, durable covering that provides protection for the vital underlying calvarium
and brain, serving as the first and likely most important barrier. It is composed of hair-bearing (temporal,
parietal and occipital) and non–hair-bearing skin (frontal), underlying occipitofrontalis muscle (connected by
the galea aponeurotica) gliding over a thin sheet of nourishing pericranium.
Scalp defects are notoriously difficult to close, due to the inelasticity of the skin and galea. However, the
vascular supply of the scalp makes wound closure under tension acceptable. Thus primary closure may be
obtained for scalp defects, measuring 3 cm. Wide undermining in the subaponeurotic space of loose fibrous
tissue may provide little additional tissue.
Defects larger than 3 cm almost always require flap movements, relaxing incisions, and/or the application of
skin grafts.Multiple rotation flaps using a subgaleal dissection plane are the mainstay for scalp wound closure.
Flaps may be raised in any region of the scalp without regard for specific anatomical distribution of the blood
vessels. A number of additional procedures help in decreasing closure tension.
Other reconstructive options for scalp reconstruction
1. Healing by secondary intention The simplest form of reconstruction is nonsurgical. Simple, good, meticulous and prolonged wound care has the ability to heal relatively large scalp defects surprisingly well. Healing by secondary intention works best in non–hair-bearing areas of the scalp or in relatively follicle-challenged areas of age related alopecia. It does cause some distortion of the immediately surrounding areas and

should be used with caution in the periorbital region because of potential brow distortion. The scars themselves tend to be atrophic and contain telangiectasias, which may be visually distracting. Nevertheless, the final aesthetic result is reasonable. If there is overlying pericranium, the healing process may be completed in as little as 3 weeks for defects less than 2 cm and in as long as 2 to 3 months for larger defects.
2. Skin Grafting for Scalp Defects In 1908, Robinson described successful skin grafting when these grafts were applied directly to an intact underlying pericranium. Traditionally, skin grafts have not done well when placed directly on exposed calvarium without first having had a granulation tissue bed beneath. The major difficulty with this has been lack of traction between the graft and underlying bare skull. Micromotion or macromotion will not allow for graft revascularization in time to save it from invariable dessication and loss. Skin grafts may be used for temporary coverage, minimizing wound care issues while preparing the scalp for definitive reconstruction, as during prolonged tissue expansion.
3. Free flaps 4. Flap reconstruction with rapid tissue expansion for upto 10 min.

EYELID RECONSTRUCTION
Eyelids are the protective mechanism of the eyes. The upper and lower eyelids have been formed for
their specific functions by Nature. Eyelid defects are encountered in congeni tal anomalies, trauma,
and postexcision for neoplasm. The reconstruction of eyelid should hence be based on both functional
and cosmetic aspects relating to eyelids.
The eyelids consist of various tissues layers. At the level of the eyelid margin, the various layers from
superficial to deep consist of skin, orbicularis, tarsus and conjunctiva.
Outside the tarsal level, from superior to deep, additional tissue layers can be recognised, skin, orbicularis,
orbital septum, periorbital fat, eyelid retractors and conjunctiva.
Skin and orbicularis compose what is called the anterior lamella, while conjunctiva, lid retractors and tarsus
are considered the posterior lamella.
The tarsus consists not of cartilage, but of dense, fibrous tissue and functions as stiffener. The height of the
tarsal plate differs from upper and lower eyelid. In the upper eyelid the vertical dimension ranges from 9-12
mm, in the lower eyelid from 3-5 mm.
The retractors attach to the free border and slightly anterior portion of the tarsus. The retractors of the upper
eyelid consist of the levator aponeurosis and Muller’s muscle.The capsulo-palpabral fascia in the lower
eyelid is analogous to the levator aponeurosis of the upper eyelid but contains no muscle fibres. The
capsulopalpabral fascia transmits contractions of the inferior rectus muscle while stabilising the tarsus of the
lower eyelid and acting as retractors of lower eyelid. The retractors provide function, opposing the
sphincteric action of the orbicularis muscle, as well as lid margin stability.
The orbital septum is a fascial membrane separating the eyelids from the deeper orbital structures including
periorbital fat.
The medial canthal complex constitutes the bony attachment of the eyelids, as well as the lacrimal collecting
and drainage system. Specifically the part of the medial canthal tendon which inserts posteriorly into the
orbit helps maintain apposition of the eyelids to the globe.
The lateral canthal area consists of 4 structures, including the lateral canthal tendon, Lockwood’s ligament,
check ligaments of the lateral rectus muscle, and the lateral horn of the levator aponeurosis.Addionally, it
encompasses the palpebral lobe of the lacrimal gland. The lateral canthal tendon attaches to Whitnall’s
tubercle, a bony promontory just within the bony rim. The lateral canthal tendon draws the eyelid laterally,
superiorly and posteriorly.
Periorbital defects are generally categorized according to location (zone I, upper eye lid, zone 2, lower
eyelid, zone 3, medial canthal region, zone 4 lateral canthal region), depth and size. In anterior lamellar
defects, part of the eyelid thickness remains. In full thickness defects, both the anterior and posterior lamella
must be reconstituted. The larger the percentage of the full thickness eyelid which is missing (0-25% / 25-
50%/ > 50%) the more complex the reconstruction.
The ideal goal of reconstruction is to provide global protection and normal aesthetics.
Prerequisites to attain this goal may be the following: 1. Lining maintaining lubrication while avoiding corneal irritation 2. Lid rigidity while allowig direct global apposition 3. Lid stability and orientation with proper medial and lateral canthal support 4. Opening and closing ability facilitated by adequate muscle power and tone, allowed by subtle skin covering.

The lid reconstruction may be divided into three main groups: Partial thickness lid defects not involving the lid margin Full thickness lid defects involving the lid margin Medial canthal defects
I. Reconstruction of Partial Thickness Lid Defects Distance between the skin tumor and the lid margin is important in choosing the excision technique:
If more than 4 mm from the lid margin, partial thickness excision is preferred If less than 4 mm from the lid margin, removed through full-thickness resection of the lid
o Closure of a partial thickness defects can be achieved by one of the following: Direct closure:
The wound should be orientated along the dynamic lines to minimize tension on the wound. An exception to this rule is a defect in the lower lid where closure along the line can shorten the anterior lamella leading to ectropion. This problem is especially common if the defect is large and there is lower lid laxity as in the elderly. To avoid this problem, close the defect vertically or if large, use skin graft.
Flap technique: Advantages:
• Anterior lamellae can be reconstructed with less contracture during healing •A viable vascular supply at the base of the flap increases the viability of the tissue compared with skin graft.
Three types of flaps are used in lid reconstruction: •Advancement flaps (tissue moves directly forward into a defect) •Rotation flaps •Transposition flaps

In rotation type, the flaps rotate about a pivot point whereas in transposition type, the flap is moved laterally to cover a defect; in practice both techniques are combined to a certain degrees. Therefore a flap tends to be called by its name rather than the principle which predominates (for example V-Y plasty or O-Z plasty). The length of a flap should be less than three times the width of the base to allow vascular supply at the base.
Skin grafts: There are two types of skin grafts:
•Full thickness skin graft containing the epidermis and full thickness of dermis •Split skin graft containing epidermis and a variable proportion of dermis
In oculoplastic surgery, the full thickness graft is preferred as the resulting graft resist contraction whereas split skin graft tends to shrink considerably. The most common sites for autologous skin grafts for oculoplastic surgery are:
•Upper eyelid skin •Post or pre-auricular skin •Supraclavicular skin
Skin grafts can fail. Some of the most common causes of skin graft failure include: •Presence of hematoma can prevent contact between the graft and the capillary bed of the recipient and subsequent revascularization •Infection •Movement of graft may disturb capillary link-up with the recipient bed. Essential steps in establishing a successful graft: •Ensure that bleeding or hematoma is removed from the recipient bed which may inhibit revascularization • All subcutaneous tissue such as fat is removed from the undersurface of the donor graft which may interfere with revascularization. •Use pressure to prevent formation of hematoma or movement of the graft. This can be done either by applying a patch directly over the graft (covering the whole eye) for about 5 to 7 days or using precise pressure over the graft such as the bolus method or tying a cotton roll over the graft.
Spontaneous granulation (laissez-faire): Spontaneous granulation is not recommended except for very small wound. Advantages:
• The excision margins are not distorted and therefore useful in confirming complete excision of malignant tumors such as malignant melanoma or sebaceous cell carcinoma (in which frozen section and Mohs’ technique have limitation in confirming complete excision)
Disadvantages: •Delayed healing •Increased contracture of the scar •Increased distortion of the surrounding tissue • Spontaneous granulation is most useful in the medial canthal region. This is because in this region, contraction occurs in a centripetal direction and tension is distributed at the wound perimeter. The result is less distortion of the lid and the surrounding structure.

II. Reconstruction of Full Thickness Lid Defects Reconstruction of the full thickness eyelid defect requires three elements:
Outer layer of skin Inner layer of mucosa Semi-rigid supporting structure (acting as the tarsal plate) interposed between them.
•Upper eyelid construction has unique requirements relative to the lower lid. Whereas the lower lid can be pulled as taut as possible, excessive tightness of the upper lid may result in ptosis. A small irregularity or aberrant lash in the lower lid may be tolerated, but the constant opening and closing of the upper lid makes a smooth margin lined by a mucous membrane an essential for cosmesis and comfort. Whereas the lower tarsal plate has a vertical height of only 4 mm, the upper one may require substance of 8 to 12 mm. • Compared with the upper lid, the lower lid is not as critical in maintaining the integrity of the cornea. Therefore, most of the techniques used (except Hughes flap) seldom utilize the upper lid component to reconstruct the lower lid as this may affect the upper lid function. For lid reconstruction, the full-thickness marginal defects are classified into: small (<25% of the horizontal dimension of the lid margin), medium (25%-50%), and large (> 50%).
Reconstruction of upper lid defects according to size: Small Defects: Upto 25% defect of the horizontal dimension can be closed directly after coverting
into pentagonal incision and v-shaped incision.
Medium Defects: Defects larger than 25% of the horizontal dimension of the upper lid cannot be
closed directly.The following techniques are useful in closing these defects: o Direct closure with lateral cantholysis of the superior crus of the lateral canthal tendon
releasing upto 5mm. o Tenzel semicircular: With upper lid reconstruction, the semicircle is directed downward,
whereas in lower lid reconstruction, it is directed upward. o Mustarde lid-switch: This is based on a small full-thickness flap of the lower lid based on the
marginal artery. The marginal artery is 3 to 4 mm inferior to the lid margin, and therefore the pedicle should be at least 3 to 6 mm in vertical height. The lower lid is closed using a sliding flap from the cheek.
Large Defects: Inlarger defects of more than 50% of the horizontal dimension, two methods are
commonly used:

o Cutler-Beard’s technique: In the first stage, the flap is designed 4 to 5 mm below the lid margin (so that marginal artery is kept in the bridging flap) and advanced upward and sutured to the defect. After 6 to 8 weeks, the second stage involves dividing the flap and rotating the conjunctiva over the reconstructed upper lid to prevent skin from coming into contact with the eye.
o Mustarde total lid switch technique: This is similar to the lid switch technique mentioned for medium defect, except that the flap is larger and the reconstruction for the lower lid requires a cheek rotation flap. The operation is carried out in two stages: the first stage†is the lid rotation and after about two weeks, the base of the pedicle is divided and the†lower lid is repaired with a cheek rotation flap.
Reconstruction of lower lid defects according to size: Small Defects: If the defect in the lower lid is <25% of the horizontal dimension of the lid, direct
closure is usually possible. In senile patients with lid laxity, more than 25% of lid defect may also be
approximated directly.
Medium defects: For lower lid defect of between 25 to 50 % of the horizontal dimension.
The approximation will require either:
o Lateral cantholysis of the inferior crus of the lateral canthal tendon.
lateral cantholysis insufficient, it should be combined with a local periorbital skin and
muscle flap. The flap should be within the orbital rim otherwise incision through the thicker
skin can leave prominent scarring.
Large Defects: Inlarger defects of more than 50% of the horizontal dimension, the lower eyelid may
be reconstructed using the following techniques:
o Two-stage tarsoconjunctival flap procedure with full thickness skin graft (Hughes procedure): 1st stage is the creation of a tarsoconjunctival flap, the horizontal incision is parallel to the lid margin and at least 4 mm above the inner surface margin. After suturing the flap to the defect, the area is covered with a skin graft. 2nd stage: 6 to 9 weeks after the first stage, the palpebral fissure is†opened by dividing the flap and create a conjunctiva lined lid margin
o Mustarde cheek advancement flap with chondromucosal graft

o Tripier or bipedicle muscle flap with chondromucosal graft
o Frickle flap
Reconstruction of lamellar defects:
Anterior lamella defects o Only very small defects (< 0.5 cm) are amandable to secondary intention healing. Anterior
lamella defects of less than 50% of the eyelid are usually closed with local muscular cutaneous sliding flaps from witin the eyelid itself. The orbicularis is included in the flap for enhanced vascularity and bulk. These local flaps are most often designed as uni- or bipedicled advancement flaps. The maximal tension is oriented in a plane parallel to the free border of the eyelid to prevent ectropion, while the incisions lie within the RSTL’s. Alternatively, O-Z plasty involves two opposing sliding rotation flaps.
Posterior lamellar defects
o In posterior lamella defectsusually tarsus and conjunctiva are missing. For posterior lamellar reconstruction, either a graft or conjunctical flap may replace both conjunctiva and tarsus. A large series with a variety of grafts described for reconstruction include autogenous composite mucosa-cartilage from the nasal septum, auricular chonchal cartilage graft, homologous tarsal grafts, scleral grafts, buccal mucosa, and hard palate mucosa grafts. Nasal septum and auricular chonchal cartilage grafts are obviously easily obtained, but frequently cause cosmetic inacceptable contour changes when used in the upper eyelid. Moreover, composite cartilage grafts may risk inadequate graft take. Buccal mucosa is too soft and shrinks substantially in the postoperative period. Nowadays, lateral hard palate mucosal grafts are favoured for posterior lamella reconstruction.Alternatively, tarsal-conjunctival advancement or transposition flaps can be applied from the upper to the lower lid. The anterior lamella is reconstructed separately along the guidelines described above.

Reconstruction of the Medial canthal defects: This can be achieved by a variety of methods:
Spontaneous granulation Full-thickness skin graft can provide an excellent method of reconstruction compared to the cicatrix
of spontaneous granulation. The thin nature of the full-thickness graft allows for early detection of recurrence of the tumor.
Transposition of median or glabellar forehead flaps.


NOSE RECONSTRUCTION
Aesthetic restoration of acquired nasal defects has intrigued reconstructive surgeons for centuries. Because
of the myriad reconstructive options, there is a need for a logical and sequential approach to the decision-
making process used in choosing the appropriate reconstruction for a specific nasal defect. Based on a
literature review and extensive clinical experience, a recommended outline is presented that is organized by
location and size of the nasal defect.
Historically, 3 basic techniques evolved over the years for major nasal reconstruction. The Indian
rhinoplasty, described as early as 2000 BC, used a pedicled forehead flap for nasal reconstruction. In the 15th
century, medical literature in Italy detailed the brachial or arm flap for nasal reconstruction. In the 19th
century, the French began reporting their work on the cheek flap for reconstruction of the nose
Anatomical considerations
The nose has been described as a separate aesthetic facial unit, consisting of concave and convex surfaces
that demarcate distinct nasal subunits.The tip is determined by the contour of the underlying lower lateral
cartilages (LLC). Each side of the tip has an elevation or dome that drops off and blends in with the ala
laterally and the nasal sidewall superiorly. A supratip depression marks the border of the tip and the dorsum.
The dorsum extends from the supratip depression to the glabella. The lateral border of the dorsum forms a
ridge that separates it from the nasal sidewall subunit. The lateral nasal sidewall extends from the lateral
edge of the dorsum to form the nasofacial groove. The alar subunit (lobule) consists of a C-shaped alar
groove that is shallow medially and deep laterally. There is no cartilaginous support to the alar subunit,
unlike the tip, which is supported by the LLC. Finally, the soft triangle (facet) is a shallow depression
between the arched caudal border of alar cartilage and nostril margin and is considered by most rhinoplasty
surgeons to be aesthetically pleasing and well worth preserving in nasal reconstructive surgery.
SOME NASAL TOPOGRAPHICAL LANDMARKS
Nasion Depression at root of the nose, corresponds to nasofrontal suture
Radix Continuous curve that descends from the superior brow to lateral
nasal wall
Sellion
Deepest point of nasofrontal angle, intersection of forehead slope
and the proximal bridge
Rhinion Junction of bony and cartilaginous nasal dorsum

Tip-defining point
(pronasalae)
Anterior-most projection of nasal tip, junction of intermediate and
lateral crura
Infratip lobule Located caudal to tip-defining point and cephalic to
columellar breakpoint
Columellar breakpoint Anterior-most point of soft tissue of
nasal columella, junction of intermediate and medial crura
Alar groove (supra
alar crease)
Crease located at cephalic border of ala Alar margin Margin along
nostril rim, located at caudal aspect of ala
Alar facial sulcus Junctional zone between cheek, upper lip, and alar base, represents
lateral continuation of alar groove
The simplest repair often provides the best functional and cosmetic result. When simpler reconstructive
methods result in excessive tension of skin edges or distortion of surrounding structures, a skin flap or graft
must be considered. Specific flaps are more useful in certain situations. However, it is imperative to
understand tissue movement and individualize each and every surgical defect before committing to one
particular closure option. Each patient should be approached with a mental exercise in which all available
reconstructive options are assessed. If a defect is particularly large with multiple areas of loose adjacent
tissue, it may be closed with a combination of flaps, or a combination of a flap and a skin graft.
To achieve the best aesthetic result, scars created must be placed between the regional subunits. Flaps are
designed to replace regional subunits rather than surgical defects. When a large part of a nasal subunit
(greater than 50%) has been lost, one should replace the entire subunit rather than merely patching the defect.
Whenever possible, camouflage scars within a wrinkle line or along borders of subunits.
Also Skin is thinner and more mobile over the dorsum; whereas, it is thicker and more adherent to the
underlying nasal framework at the nasal tip and alae
SURFACE RECONSTRUCIO OF LOWER ⅓ OF NOSE

Anatomy of the lower one third of the nose is distinctly different from the proximal two thirds. The skin here
has limited mobility and therefore cannot be recruited for closure for anything but small defects. The color
and sebaceous texture are unique so that neither distant nor local fl aps provide good match. Finally, the free
margins of the alar rims are mobile and easily distorted by imprecise closures. Reconstruction here is most
challenging, and preoperative planning must be precise.
Tip
o Primary closure
It is to be considered when the lesion is small and is in midline, oriented transversely of
verticall across and limited to nasal tip.
o Secondary intention (<1 cm)
Allowing a nasal defect to heal by secondary intention is a rarely used option, it is mentioned
first because it is certainly the simplest alternative and should be considered in smaller
defects of the nasal tip.
This is to be considered in lesions/defects that are
concave,
partial thickness,
less than 1 cm
debilitated or anticoagulated patients
With deeper defects on the tip, one may consider letting the wound granulate for 7 to 10
days, followed by a full-thickness skin graft to avoid a permanent concavity and healing by
secondary intention for larger tip defects may result in distortion of alar rims.
o Local flaps
Transposition flap (single) Less commonly used transposition flap used to repair
very small defects 0.5cm or less in size located on the nasal tip. However, tension
lines created often create contour deformities.

Bilobe flap
It is an excellent flap for closure of defects less than 1.5 cm on the lower one third of
the nose, especially around the tip. It is a double transposition flap and is useful
when the primary defect is located in inelastic skin and the adjacent skin is relatively
mobile. Elastic skin, by means of the double transposition, can indirectly be used
to close the inelastic skin of the primary defect. For the nasal tip, the double
transposition fl ap can borrow skin from the loose nasal dorsum or glabella to close
the defect in the tight nasal tip.
Reiger (dorsal nasal flap)
It is an alternative for repair of small to medium defects (1-3cm) involving the tip,
caudal dorsum, or sidewall. The technique has the disadvantage of causing
juxtaposition of thick skin from the glabella and thin skin of the medial canthus. The
dorsal heminasal flap avoids this disadvantage by maintaining the thin skin of the
cephalic nasal sidewall. It is a laterally based rotation-advancement flap, considered
to be both a random fl ap as well as an axial fl ap that is based on a branch of the
angular artery, joining with the supraorbital arteries. The pedicle is located lateral
and superior to the defect.
A curvilinear line is drawn from the defect laterally in the nasofacial sulcus,
medial to the medial canthus and into the superior aspect of the glabella. The
distance from the inferior glabella to the superior portion of glabellar portion of flap
should be 1.5 to 2 times the vertical height of the nasal defect.
A backcut is made to the contralateral medial canthus at a 30° to 45° angle. A wide
undermining in the bloodless plane just superficial to the cartilaginous and bony
nasal skeleton facilitates closure. The glabellar defect is closed in a V-Y
fashion.
Nasolabial/melolabial flap
It is a single transposition flap. It is not particularly useful for midline or nasal tip
defects because of the length needed to reach these areas. It is best suited for lateral
side wall, ala, and alar rim defects.

Interpolated melolabial flaps are based on cutaneous or subcutaneous tissue pedicles
and are used to transfer skin and soft tissue of the cheek to the region of the ala,
lateral tip, columella, and caudal nasal sidewall. Subcutaneous tissue pedicled flaps
may be delivered to the nose by passing the pedicle of the flap over or under the
intervening cheek skin.
The skin of the medial cheek is similar in thickness and texture to the thicker, more
sebaceous skin of the ala. It is for this reason that the interpolated melolabial flap is
the covering flap of choice for repair of subtotal or total cutaneous surface defects of
the ala. The utility of the flap may be expanded to include cutaneous defects of the
ala with limited (1 cm or less) involvement of the tip or caudal portion of the nasal
sidewall.
o Full thickness skin graft
The preauricular FTSG is generally the graft of choice for tip defects because of its thickness
and color match from sun exposure. The donor site is well camoufl aged in the preauricular
crease. For larger or rounded defects, the donor site can be closed with a rhombic
transposition fl ap. One must be careful not to harvest hair-bearing skin, especially in males
with a heavy beard.
o Split thickness skin graft
It is best used for coverage after removal of very high-risk malignancies and acts as a
window to monitor possible tumor recurrence. The disadvantage is that the STSG offers
poor color and texture match and is rarely used for tip reconstruction.
o Axial-pattern flaps
Midline forehead flap
Nasal ala
o Intact nostril margin
Nasolabial flap
Bilobe flap
o Absent nostril margin
<1-cm composite graft
Both the nasal ala and the auricle are essentially cartilaginous frameworks covered
by tightly adherent skin, making the auricle a logical choice for restoration of alar
rim defects.” Free composite grafts from the helical root are ideal for through and
through alar defects. These grafts provide a single-staged closure with good color
and texture match with nasal ala. The graft should be no more than 1.5 cm in size
and should include only non-hair-bearing skin from the preauricular area. Th e donor
site is easily closed by advancement superiorly of cheek skin.

The limitations include variability and unpredictability of ultimate flap survival. It
cannot be done in smokers or patients with small vessel disease such as diabetes or
coronary artery disease, and the defect must be less than 1.5 cm in size.To ensure
success of the free composite graft, it must be less than 1.5 cm in its greatest
dimension, be exposed to minimal intraoperative trauma, and be constantly kept
moist intraoperatively. It is important to use no intraoperative vasoconstrictors and
minimal electrocautery. A meticulous closure with 5-0 chromic suture for
intranasal mucous membrane and 6-0 Prolene suture for skin, as well as ostoperative
cooling for 72 hours, helps ensure flap viability.
>1-cm nasolabial flap or Midline forehead flap
UPPER AND MIDDLE 1/3RD RECONSTRUCTION OF NOSE
Primary closure
Rhombic transposition flap
Webster 30° flap
Cheek advancement flap
Reiger (dorsal nasal) flap
Median/paramedian forehead flap
FTSG
Total nose Coverage: MFF with or without other flap

EAR RECONSTRUCTION
Auricular reconstruction is a challenging reconstructive entity complicated by the high ratio of skin coverage to cartilage, inconsistent blood supply, and complex three-dimensional structure with subtle topographic details. The goal of reconstruction of the pinna is normal appearance, position, and symmetry with respect to the contralateral ear. Realistic expectations must be established with the patient prior to undertaking reconstruction.
In order to plan and perform a successful repair, several principles are important to apply:
1. The relationship of the periauricular skin and postauricular sulcus should be preserved with reconstructive efforts.
2. Thin and well-vascularized skin is a necessity. Furthermore, scar tissue, poorly vascularized tissue, and noncompliant skin must be replaced.
3. The surgeon must be able to anticipate the immediate and delayed consequences of tissue manipulation. Consider the effect of tissue manipulation on hair-bearing skin, but do not allow this to compromise your ultimate quest for contralateral symmetry as hair-bearing skin can be eliminated at a secondary stage.
History of ear reconstruction
Converse provided a detailed account of the early history of ear reconstruction. According to Converse, The Susruta, an Indian text of ancient medicine, noted a 900 bcecase of partial reconstruction of the earlobe with a cheek flap. In 1597, Tagliacozzi of Italy transferred a flap from the arm to reconstruct the auricle of a monk. Approximately 250 years later, Dieffenbach repaired a traumatic defect of the ear with a mastoid flap folded on itself. Converse explained that Roux and many of his contemporaries of the mid-19th century considered reconstruction of the auricle a surgical impossibility, but by 1930, Pierce had reported Post traumatic repairs that used autologous rib cartilage for reconstruction of the concha-antihelix and a thin roll of supraclavicular skin for helical reconstruction. Later, Peer placed diced autologous costal cartilage in a mold that was implanted in a subcutaneous abdominal pocket. When fusion of the fragments by connective tissue was complete, the framework was used in auricular reconstruction.
During the 1940s, ear reconstruction with fresh and preserved cartilage homografts and heterografts was reported. The results were uniformly dismal, characterized by late resorption and high complication rates. The modern era of auricular reconstruction began withclassic descriptions of the principles and technique of total ear reconstruction with autologous costal cartilage, as presented by Tanzer.
Anatomy
The ear is morphologically unique. The skeletal structure is composed of auricular elastic fibrocartilage which composes the upper two-thirds of the auricle. Auricular cartilage is flexible, yet it maintains form. The cutaneous coverage of the anterior-lateral surface of the ear differs from the posterior-medial surface. The anterior-lateral surface skin of the auricle lacks subcutaneous tissue and is adherent to the perichondrium. A layer of fascia containing a subdermal plexus of vessels separates the skin from the perichondrium. The posterior-medial surface skin has a deep subcutaneous fat layer that causes it to be less adherent to the cartilaginous framework.
The topographic features of the ear are incredibly important when considering reconstructive options. They are as follows:
Helix: prominent auricular rim Antihelix: prominence anterior to helix Fossa triangularis: superior space between superior and inferior antihelical crus Scapha: depression between helix and antihelix Concha: deep cavity posterior to external auditory meatus
o Cymba conchae: portion superior to crus of helix o Cavum conchae: portion inferior to crus of helix
Crus of helix: beginning of helix that divides concha Tragus: anterior to concha and partially covering external auditory meatus Antitragus: posteroinferior to tragus: separated by intertragic notch Lobule: inferior to antitragus

The blood supply of the auricle is supplied mainly by branches of the external carotid artery which include the superficial temporal artery and the occipital artery which gives off the posterior auricular artery. The posterior-medial surface of the ear is supplied by the posterior auricular artery. The anterior-lateral surface of the ear is supplied by both the posterior auricular artery and the superficial temporal artery, creating two arterial networks. The triangular fossa and scapha are supplied by the network arising from the superficial temporal artery. The concha is supplied by the network arising from the posterior auricular artery. Consideration should be given to the blood supply when planning and designing flaps. Venous drainage is via the postauricular vein, which drains into the external jugular vein. Supplemental venous drainage flows into the superficial temporal and retromandibular veins. Lymphatic drainage of the auricle is to the preauricular, infraauricular, and mastoid lymph nodes.
The auricle has sensory innervation from the following nerves: the greater auricular nerve (C2-3), the auricular-temporal nerve (V3), the lesser occipital nerve, and a branch of the vagus nerve (Arnold’s nerve) . The greater auricular nerve divides into an anterior branch, which innervates the lower half of the lateral auricle, and a posterior branch, which innervates the lower half of the medial auricle. The auricular-temporal nerve innervates the superolateral surface of the auricle. The lesser occipital nerve innervates the superomedial surface of the auricle. Arnold’s nerve innervates the concha.
The dimensions and proportions of the auricle are critical for reconstruction. The vertical height of the ear is roughly equal to the distance from the lateral orbital rim to the helical root at the level of the brow. The width of the ear is approximately 55% of its height. The helical rim protrudes between 20 and 30 degrees from the skull, which corresponds to 1 to 2.5cm. The vertical axis of the ear is tilted posteriorly (when relating the apex of the helix to the lobule) 15 to 20 degrees. The superior level of the ear is at the same height as the lateral brow. The inferior aspect of the ear is at the same height as the nasal base.
General Reconstructive Principles
Auricular reconstruction is dependent upon the defect. Auricular defects can be classified into the following categories: cutaneous and cutaneous-cartilaginous which can be full-thickness defects.
Cutaneous defects of the adherent lateral auricular surface can rarely be closed primarily. These defects are best treated with skin grafts provided there is intact perichondrium. The contralateral postauricular skin can serve as a full-thickness skin graft donor site. When lateral perichondrium is lost due to the nature of the defect, the cartilage may be removed if it is not a determinant of auricular

shape, and the full-thickness skin graft can be placed on the medial perichondrium or medial skin. Medial cutaneous defects involve a more pliable skin and are often repaired by primary closure. For the same reason, medial auricular skin is an excellent donor site for a full-thickness skin graft, as previously mentioned.
Cutaneous-cartilagenous defects may have preserved skin on one side of the defect or it may be a full-thickness defect. The main difference between this type of defect and a cutaneous defect alone is the alteration in auricular shape often caused by loss of supporting structure. Small defects may be amenable to primary closure once the defect has been converted to a full-thickness wedge excision. The decision is based on defect size and location, keeping in mind that a loss in vertical height of the auricle is inevitable. Generally, small defects in the helix or antihelix less than 0.15cm are best treated with wedge excision and primary closure. When this is performed, some central conchal cartilage must be excised to alleviate circumferential tension and prevent cupping of the auricle. Defects between 0.15cm and 2cm involving the helix or antihelix may be reconstructed by using a composite graft from the contralateral ear. In order to maintain symmetry between the auricles, the graft should be one-half the height of the defect. However, use of this technique potentially compromises the contralateral auricle, and is therefore not a first choice in reconstruction.
Many local flaps have been described for repair of full-thickness auricular loss. Basic principles of design prevail in most of the flaps ranging from chondrocutaneous advancement flaps to retroauricular island transposition flaps to tubed flaps. Vascular supply must be maintained and decreased tension with closure is necessary for viability. All flaps used to reconstruct the auricle must provide cutaneous coverage and maintain auricular structure including form and size. Regional flaps should be considered in place of local flaps when the vertical height of the auricle is decreased by more then 2cm. The most versatile regional flap used in auricular reconstruction is the temporoparietal fascia flap. This flap is often combined with an autogenous cartilage graft as a framework and can provide the required thin, highly vascular recipient site for a split-thickness skin graft.
Auricular Reconstruction Based on Defect Location
Conchal Bowl and Helical Root Defects
Conchal bowl cutaneous defects can be repaired with skin grafting. Likewise, when perichondrium or cartilage is absent, but skin remains on one side of the defect, skin grafting is used for repair. Conchal cartilage is not necessary for auricular form and can be resected without structural compromise. The retroauricular island transposition flap may be used for lateral skin and cartilage deficits. This same flap can be used in full-thickness defects involving both the

medial and lateral conchal skin and conchal cartilage by bivalving the flap. Defects of the helical root can be reconstructed using a helical advancement flap which includes advancing lateral skin and cartilage down towards the deficient area.
Upper One-Third Auricular Defects
The upper one-third of the auricle can be concealed by hair to conceal a cosmetic defect. However, in many patients this portion of the ear has a functional purpose in supporting eyeglasses. Options for reconstruction of these defects include primary wound closure, full-thickness skin grafts, helical advancement flaps, retroauricular and preauricular tubed flaps, and the use of autogenous cartilage framework combined with temporoparietal fascia and split-thickness skin graft coverage. Again, the choice of the flap is dependent upon the size and location of the defect.
Middle One-Third Auricular Defects
Defects of the middle one-third of the auricle are often obvious. Small defects may be closed primarily by converting the defect into a wedge. This has a direct impact on vertical height. Some larger defects are amenable to repair with helical chondrocutaneous advancement flaps. Tubed flaps should be limited to helical reconstruction only due to the lack of a cartilaginous framework for support. Larger defects are reconstructed using a two-stage retroauricular composite flap using full-thickness retroauricular skin and autogenous cartilage. The cartilage is usually harvested from the nasal septum or contralateral or ipsilateral conchal cartilage.
Lower One-Third Auricular Defects
The lower one-third of the auricle is easiest to reconstruct due to the pliability and laxity of auricular and periauricular skin in this area. Up to half of the lobule can be resected and closed primarily with minimal deformity. The lobule can also provide tissue for advancement flaps. Reconstruction of the entire lobule is more difficult. When defects involve the entire lower one-third of the auricle, a multi-staged reconstruction involving autogenous cartilage grafting becomes necessary.
PreauricularDefects
Options fro repair of preauricular defects include primary closure, advancement flaps, and transposition flaps. Careful planning can result in the scar resting in the preauricular crease. The facial nerve should always be kept in mind when addressing these defects.
Large Auricular Defects
Auricular defects that exceed one third of the auricle are increasingly difficult to reconstruct. Multiple techniques are necessary including autogenous cartilage grafting, skin grafting, and the temporal parietal fascia flap. In certain

circumstances, local skin may be adequate for coverage, but this is not the norm as the associated skin is usually absent or scarred.
Acquired deformities Principles of Acute Management The principles of management of acutely traumatized ears can be summarized as follows: • Thorough cleansing, minimal débridement, and skin suturing only after cleansing • Begin at known structures and progress to unknown • Close the skin in delayed reconstruction • Repair primarily after wedge excision of the wound if the defect is small and peripheral • Leave the wound open and reconstruct at a later date • When immediate closure is not feasible, cleanse the wound and change dressings frequently to avoid desiccation • Graft skin defects only where underlying perichondrium is present • Reattach small avulsed ear pieces as compromised grafts, especially in children
Techniques in Auricular Reconstruction
Cartilaginous Reconstruction with Costal Cartilage
Reconstruction of the auricular framework can be performed using autogenous cartilage or alloplastic implants. Some reconstructive surgeons speculate that patients adjust better, both physically and psychologically, to reconstruction with autogenous tissue compared to alloplastic implants. Additionally, alloplastic implants have the risk of extrusion and a higher rate of infection. When patients are over 60 years old, consideration must be given to the fact that cartilage is more brittle and may be ossified depending upon location. Costal cartilage provides a reliable donor site for autogenous cartilage, specifically the sixth, seventh, and eighth rib cartilage. The synchondrosis between the sixth and seventh ribs serves as the body of the framework, while the eighth rib accounts for the helix. Determination of the size and shape of the framework is obtained by making a template from the contralateral ear. The sixth and seventh ribs are contoured to create the concha, antitragus, and curve of the antihelix. The eighth rib cartilage is freed of perichondrium on one side and contoured to form the helix. The helix is fixed to the framework and the antihelix and fossa triangularis are created using gouges. Once the cartilaginous framework has been fashioned, thin, vascular, hairless tissue capable of accepting skin grafts must be used to cover the cartilage. The temporoparietal fascia flap satisfies all of these criteria. Other advantages of the temporoparietal fascia flap include the large quantity of tissue that can be harvested (14 X 12cm) and the fascia may be transferred to the contralateral auricular region using microvascular techniques.
The temporoparietal fascia flap is composed of superficial temporal fascia which is continuous with the superficial musculoaponeurotic system (SMAS) and the deep galea. The temporoparietal fascia is deep to the skin and subcutaneous tissue. It should not be confused with the deeper temporalis fascia which surrounds the temporalis muscle. The temporoporietal fascia is 2 to 3mm thick over the parietal area and is highly vascular. The blood supply is consistent and comes from the superficial temporal artery. In order to harvest the temporoparietal fascia flap, a 6cm vertical incision is made in the scalp immediately above the auricular defect to expose the temporoparietal fascia. Elevation of the flap should be performed in the loose connective tissue or areolar tissue which is between the temporoparietal fascia and the temporalis fascia. If this plane is maintained, it is deep to the hair follicles and will avoid alopecia. The vascular pedicle of the flap is identified and protected. The frontal branch of the facial nerve is the anterior limitation of flap elevation. The posterior aspect of the flap is elevated to the posterior branch of the superficial temporal artery. The flap is rotated 180 degrees in an arc that is rotated superiorly to inferiorly so that the lateral surface of the flap lies medially along the defect. The edges of the flap are tucked under the existing skin edges. Split-thickness skin grafts are then applied to the flap. Optimal drainage is supplied by a suction drain. The temporoparietal fascia flap often obliterates the supraauricular sulcus. As a result, a second stage procedure is often necessary to recreate this sulcus.
Biomaterials
Reconstruction of the total external ear has two major approaches- alloplastic prosthesis implantation and autogenous cartilage grafts. The advantages of alloplastic implants include widespread availability, consistent predetermined shape, and shortened operating time. The disadvantages are increased risk of infection, extrusion, biocompatibility, and uncertain long-term durability. To counteract some of the disadvantages, tissue engineering is being investigated using predetermined biodegradable polymers and cell isolates. Additional advantages include minimized donor site

morbidity, precise creation of a complex structure, donor tissues identical to recipient tissue, and the potential for implant growth.
Porous Polyethylene Implant (Medpor)
There are multiple alloplastic auricular implants including silicone, polypropylene, and polyethylene. The porous polyethylene implant has several advantageous qualities for auricular reconstruction as it can be easily shaped, sterilized, and implanted underneath appropriate soft tissue coverage. Additionally, it is non-toxic and causes little foreign body reaction. Most importantly, this implant allows for tissue ingrowth into the material which anchors it into position and provides resistance to infection.
Microvascular Techniques
Auricular injury involving sub-total or complete amputation makes for a more complex reconstruction. Microvascular techniques have been described in complete amputations in order to avoid necrosis and distortion of auricular cartilage due to a lack of blood supply. Arterial anastomosis makes use of the primary supplying branches off of the external carotid which are the superficial temporal artery and the posterior auricular arteries. Venous anastomosis is also important and is often more difficult than arterial anastomosis. Previous literature describes of a technique with arterial anastomosis without venous anastamosis. Use of this technique emphasizes the importance of thorough debridement of non-vital tissue to allow venous channels to form between the replant and the recipient bed.
Microsurgical replantation of the ear is technically challenging, but it allows for a single procedure option for auricular reconstruction. A more natural appearing pinna usually results with this technique compared to other techniques for auricular reconstruction. Important prerequisites for successful replantation include short ischemic intervals, appropriately preserved amputated parts (in saline on ice), and compliant patients. Upon performing microsurgical replantation, secondary reconstruction options should be preserved including the postauricular skin, the temporoparietal fascia, and the main superficial temporal vessels. Small vessel caliber makes this procedure challenging. The best results can be achieved with anastomosis of both the artery and vein. However, identification of a suitable vein and venous anastomosis is especially difficult. The necessity of venous repair has been questioned for ear replants. Studies have demonstrated that venous connections form in one week through neovascularization. It is the belief of several surgeons that failure of ear replantation without venous anastomosis is due to inadequate debridement, which in turn impacts neovascularization. Additionally, wider area of contact is believed to improve neovascularization which could be provided with ear replantation by removing postauricular skin. An ear replant with venous insufficiency needs venous drainage such as leeches or skin punctures.
Nonmicrosurgical Reconstruction: Mladick and Baudet Techniques
Microsurgical techniques have been reported in the literature for auricliar reattachment, but significant complexity limits wide practice of this technique. On the other end of the spectrum, simple reattachment as a composite graft is almost certain to fail. As a result, numerous techniques have evolved to improve survival of the replanted ear. In 1971, Mladick et al proposed the principle of a retroauricular pocket for non-microsurgical replantation. The amputated part was completely deepithelialized, followed by anatomic reattachment and burial in a retroauricular pocket. A second stage procedure involved elevation of the replanted cartilage from the retroauricular pocket and split-thickness skin grafting. In 1972, Baudet et al reported a case of ear replantation where the posterior pinna skin is excised from the amputated portion of the auricle, fenestrations are made in the cartilage to allow improved vascular access to the anterior pinna skin, and a postauricular skin flap is elevated. The anterior skin is then sutured to the amputated stump and to the postauricular flap. After three months, the ear is elevated and the postauricular area is reconstructed with a split-thickness skin graft.
Venous Congestion: Leeches
Use of leeches for medicinal blood letting dates back to 200BC and remained popular well into the 19th century. Popularity waned in the late 19th century and the first 75 years of the 20th century. Modern surgical techniques including pedicled and microvascular free tissue transfer have caused the use of leech therapy to reemerge. Blood-letting allows for a temporary bypass of venous outflow obstruction until revascularization from the surrounding soft tissues will allow the flap to survive. The mechanism behind the use of leeches lies in the affect of the anticoagulant called hirudin in the saliva of the leech. Hirudin provides a prolonged decongestive effect on a tissue flap by decreasing venous engorgement, decreasing capillary pressure, and increased tissue perfusion. Due to the above properties, leech therapy can be helpful with avulsion injuries to the face where arterial blood supply is present, but venous outflow is lacking. The sparing of soft tissue provides optimal results. Leech therapy duration is based upon

clinical evaluation of the involved tissue; if the tissue remains pink and viable, the leeches are no longer necessary. Once instituted, the leeches are replaced every 6 to 8 hours. Patients undergoing leech therapy should be placed on broad-spectrum antibiotics and prophylaxis against Aeromonas hydrophilia infection (second generation or greater cephalosporin, aminoglycosides, trimethoprim-sulfamethoxazol, or ciprofloxacin). Hematocrit must also be monitored in these patients. Skin punctures have also been described for venous congestion.
Antithrombotic Agent: Dextran
Dextran is a heterogeneous polysaccharide that is used after microsurgery for its antithrombotic effects on the microcirculation including alterations of platelet activity and fibrin network formation. The main advantage of dextran over other antithrombotic agents such as heparin and aspirin is the relatively lower risk of post-operative bleeding and hematoma formation. There is no clinical evidence to support the efficacy of dextran following free tissue transfer.
TPFF
The temporoparietal fascia is the most superficial fascial layer beneath the subcutaneous fat in the temporal region and is continuous with the superficial musculoaponeurotic system (SMAS) inferiorly and the galea superiorly. The superficial temporal artery supplies this area of the scalp and maintains a consistent posterior branch on which the temporoparietal fascial flap (TPFF) is normally based. The TPFF is a lateral extension of the galea and is continuous with the superficial musculoaponeurotic system of the face. It inserts on the zygoma. The TPFF has been extensively used in auricular reconstruction. The flap ranges from 2 to 4 mm in thickness and can be harvested in dimensions up to 17x14 cm. The TPFF is separate from the temporal muscle fascia, which is a thin layer of areolar tissue. The temporal muscle fascia is continuous with the pericranium above the superior temporal line. The TPFF is supplied by the STA, a terminal branch of the external carotid artery, which ascends behind the ramus of the mandible and becomes superficial 4 to 5 mm in front of the tragus. The STA lies anterior to the external ear and supplies the scalp, the external ear, face, and the parotid gland. In the majority of cases, the STA divides approximately 2 to 3 cm superior to the root of the helix into anterior (frontal) and posterior (parietal) branches. Before dividing, the artery gives rise to the middle temporal artery that supplies the temporal muscle fascia. The terminal course of the vascular pattern is variable. To protect the frontal branch of the facial nerve, the TPFF is normally raised on the posterior branch of the STA. The anterior branch is ligated approximately 3 to 4 cm from its takeoff. The distal STA arborizes over the parietal and temporal regions. The STA runs beneath the subcutaneous tissue and within the TPFF up to 12 cm above the superior attachment of the auricle. In this area of the scalp, the vessels become more superficial and anastomose with the subdermal vascular plexus. Because of the vascular architecture, this area represents the most cephalad extent of flap dissection. The superficial temporal vein runs parallel to the artery and slightly superficial to it in the majority of cases. The sensory innervation of the scalp in the area of the STA is supplied by the auriculotemporal nerve
TPFF Harvesting
The TPFF is harvested through a temporal extension of a preauricular (supratragal) facelift incision. The temporal extension should follow the curvilinear temporal line within hear bearing scalp. Dissection proceeds in a subcutaneous plane over the temporoparietal fascia to the zygomatic arch and frontal nerve. This dissection is best done sharply to avoid injury to the underlying superficial temporal vessels. The fascia is incised along the periphery of the dissection to match the dimensions of the defect. The flap can then be transposed or turned down and sutured to the periphery of the cutaneous defect. A split-thickness skin graft (usually harvested from the medial forearm or the lateral thigh) can then be applied to the TPFF.
Disadvantages of the TPFF include injury to the frontal branch of the facial nerve, hair loss from subdermal dissection, and ischemic necrosis of the distal flap if harvested beyond the temporal line.
Full-Thickness Skin Grafting
A prospective study performed in Australia between 1993 and 2002 monitored patients receiving Moh’s Micrographic Surgery for skin cancer removal followed by full-thickness skin graft repair. A total of 2673 patients were treated with the above criteria, of which 216 were auricular defects (8.1%). Eleven of these patients (5.1%) had complications including graft contracture, bleeding/hematoma, infection, and partial or complete failure.

Skin Grafting
The skin graft is a fundamental reconstruction option for coverage of surgical defects. A skin graft is defined as a cutaneous free tissue transfer that has intentional separation from a donor site followed by transplantation to a recipient site. The ultimate survival of a skin graft depends upon ingrowth of capillaries from the recipient site. Keeping this in mind, avascular recipient beds including exposed bone, cartilage without perichondrium, tendon, nerve, and fascia are not ideal recipients. Skin grafts generally are used when healing by secondary intention or primary closure is not a suitable option or when skin laxity prohibits the use of a skin flap.
There are three primary types of skin grafts: full-thickness skin grafts (FTSGs), split-thickness skin grafts (STSGs) and composite skin grafts. FTSGs consist of the entire epidermis and dermis with or without small amounts of subcutaneous tissue. STSGs consist of the entire epidermis of the skin with a variable amount of dermis and are classified by thickness. Composite grafts contain tissues from two or more germ layers (skin and cartilage).
Graft survival is dependent upon the establishment of a blood supply from the recipient site. The first 24 hours involves sustaining the graft by imbibition. Approximately 48 to 72 hours after grafting vascular anastomoses between the recipient bed and donor graft begin to form in a process called inosculation. Circulation is restored to the graft within 4 to 7 days.
FTSGs are relatively easy to harvest and easy to secure to the recipient site. They tend to be more prone to necrosis than STSGs, yet FTSGs tend to contract less than STSGs. FTSGs are excellent for the repair of defects on the nasal tip, dorsum, ala, and sidewall, as well as on the lower eyelid and ear. FTSGs should not be placed into infected wounds and smoking is a relative contraindication. Donor sites shoud be carefully chosen to match the texture, thickness, and color the recipient skin. Common donor sites for facial defects include preauricular, postauricular, supraclavicular, and calvicular areas. The recipient site must be clean and not actively bleeding. FTSGs must make direct contact with the underlying wound bed and must be immobilized in the post-operative period (typically with a bolster which should be in place for 1 week) to prevent separation of the graft from the recipient site. FTSGs are sewn into place with deep basting sutures and perimeter sutures. Complete or partial graft failure is the main complication of FTSG which results from hematoma, graft-bed contact disruption, infection, smoking, and excessive electrocoagulation of the wound base. If necrosis does occur, the tissue should not be debrided as it acts as a scaffold.
STSGs lack their innate vascular and adnexal structures. They are classified as thin, medium, and thick based on thickness. STSGs can be meshed to increase surface area coverage. They offer better survival characteristics than FTSGs due to reduced nutritional requirements. STSG should be a last resort when cosmesis is of primary concern. Additionally, STSG is the least durable form of wound closure and can experience contraction, pigment variation, and creation of an additional wound. Donor site is chosen based on desired size, the patient’s ability to care for the site, impact on patient’s activity, and cosmesis. STSGs are secured using basting and perimeter sutures. Dressings are placed to prevent shearing because if shearing of the graft occurs within the first twenty-four hours, graft failure is almost certain. Revascularization of STSGs takes about 3 to 5 days. Acute complications are identical to FTSGs. Additionally, contraction is a common and unpredictable occurrence. Composite grafts are an option in specific auricular defects with the donor site being the contralateral ear.
Complications
Standard complications with auricular reconstruction apply including infection, hematoma, scarring, and poor cosmetic outcome. When the auricular cartilage is involved in the injury or the repair, the risk of perichondritis and chondritis must be considered. Inflammation of the perichondrium or cartilage after trauma predisposes to tissue ischemia and the development of Pseudomonas infection, which may ultimately lead to suppurative chondritis. Liquefactive necrosis can then ensue leading to devastating complications. Therefore, manipulation of the cartilage should be performed carefully under sterile conditions with antibiotic prophylaxis.
Conclusion
Every ear defect is unique. Many options are available for reconstruction of auricular defects including direct closure, secondary epithelization, FTSG, composite grafts, and local flaps including direct advancement, rotational flaps, transposition flaps, and subcutaneous island flaps. Factors to consider prior to choosing a reconstructive plan include size, location, depth, medical history, smoking history, and esthetic concerns.

CHEEK SURFACE RECONSTRUCTION
Reconstruction of surface defects of the cheek after resection of skin lesions should be approached according to
zones of involvement. Arbitraryly subdivision of the cheek aesthetic unit into three overlapping zones:
Zone 1, suborbital and perioral medial cheek from eyelid to mandibular rim;
zone 2, temporal/preauricular;
zone 3, central cheek.
The nose and cheeks occupy prominent positions in facial aesthetics. Skin lesions, malignant or otherwise, usually
do not require full-thickness cheek resection. Surface defects that do not involve loss of bulk are usually reconstructed
with skin and composite skin/muscle flaps both in the superficial and deep plane of facial dissection. When very large
composite defects exist, microvascular and distant flap methods are used.The cheek is an aesthetic unit of the face that
is subdivided into three zones to categorize the available reconstructive options. This approach of dividing the cheek
into three zones serves to categorize the lesions and organize the strategies for reconstruction. In addition, the zoning
system allows to formulate clear and complete algorithms for restoration of cheek defects from simple to complex
solutions.
General principles for local flap reconstruction of cheek surface defects
1. In the central cheek, try to avoid vertical incisions anterior to a line dropped down from the lateral canthus (Z-line) extending from the lateral canthus directly downward to the margin of the mandible that represents the lateral border of the face in a direct anterior view. Incisions posterior to this line tend to be less noticeable, and thus surgical decisions are often predicated on this vertical line. Excellent reconstructive results for a given zone are predictable on the specific anatomic considerations for that zone). Direct or en face views tend to show this scar no matter how good the surgery is done.
2. Posteriorly based facial and cervicofacial skin flaps survive better than anteriorly based flaps because the transverse branches of the facial and superficial temporal arteries are preserved. Going into the deep plane, however, can augment the blood supply of the anteriorly based flaps.
3. For flaps extending to the posterior neck, the planned incision should be kept posterior to the anterior border of the trapezius to avoid webbing of the scar and the subsequent requirement for Z-plasty scar revision.
4. Dog ears do not settle down on the cheek no matter how long you look at them. The reconstructive flap should be completely flat at the time of surgery or a revision will subsequently be required to correct the dog ear deformity. If, however, the flap viability would be jeopardized by avoiding a dog ear, tell the patient about the residual dog ear before the first stage.
5. For melanoma in situ lesions there are four key recommendations: It may be difficult to delineate the margins of melanoma in situ clinically at the time of surgical excision. A Wood's lamp has proven to be helpful but not perfect in determining the lesion margins preopera- tively. It is important to show the patient the true size of the excision preoperatively because this is always larger than they believe it to be.
6. Consider delaying the reconstruction until the margins of the resection are proven clear by histological analysis. Special dyes marking the margins of the resection and serially sectioned pathological slides will indicate how to proceed.
The empiric 0.5 to 1.0-cm rule for safe surgical margins is a fallacy and can be broken as long as the final margins are
negative on serial histological analysis.

ZONE 1 DEFECTS
Direct elliptical excision can be used for lesions along the nasojugal/nasolabial fold and the marionette line that
extends from the medial canthus to the inferior border of mandible.
1. For smaller lesions (up to 1.5 cm) a small, posteriorly based facial flap, with or without a back cut, is feasible.
2. For larger lesions (greater than 3 cm), a large, posteriorly based facial or cervicofacial flap should be designed
with the following concepts in mind:
• A transposed flap from below the lesion may or may not cross the inferior border of the mandible.
• If the flap crosses the inferior border of mandible, prepare the younger patient for a secondary Z-plasty or W-
plasty revision at the area marked with "X" on Figure 6A.
• When tissue is mobilized from the lower face or neck, a transverse incision will occur on the cheek. This
incision looks fine in patients older than 50 years of age but may be obvious in younger patients. Inform younger
patients of this preoperatively.
3. For exceptionally large upper zone 1 lesions, an anteriorly based cervicofacial musculocutaneous flap can be
raised in the deep plane to avoid a large, horizontally oriented scar that extends across the face, as well as possible
loss of skin at the edge of the flap.
4. For larger inferior zone 1 lesions, a flap may be transposed from the neck with secondary correction of a
horizontally oriented dog ear.
ZONE 2 CHEEK DEFECTS
In approaching zone 2 defects it is important to specify if the lesion is superior or inferior within the zone.
Superior Part of Zone 2
Horizontal excision is possible especially in superior zone 2 with extension of the dog ear medially. A small flap is
acceptable for a zone 2 lesion, especially if the anterior vertical limb of the flap closure lies posterior to the Z-line (en
face line). The length of anterior limb of the transposition flap is determined by the width of the defect. Therefore, the
width of the defect determines the length of the dog ear.
If the defect becomes large in superior zone 2, requiring extensive mobility of the flap and suspension/fixation to
the periosteum above the defect, then the dissection should be in the deep plane, and the superior aspect of the flap
should be secured to the periosteum.
Inferior Zone 2
Inferior zone 2 defects should be reconstructed with flaps designed inferior to the lesion and posterior to the ear. Use
anteriorly based cervicofacial flaps. Options for zone 2 reconstruction include the following:
1. Skin grafting has a very low priority except with squamous cell carcinoma, which requires an interval of
observation.
2. In upper one third of zone 2 defects
• Direct excision is acceptable if a horizontal design is possible with extension of the dog ear medially (into a
lateral blepharoplasty incision) and laterally to avoid a vertical scar on the face.
• Deep plane cervicofacial hike flap: Aim to overcorrect, Leave excess skin fixed to the periosteum of inferior
orbital rim; and Leave excess skin under eye and along incision line in the preauricular area (revise later if
necessary).
In lower two thirds of zone 2 defects Small defects: Simple transposition facial flaps for Larger defects: Becker
flap procedures; stop at mid- neck or go on to chest.
ZONE 3 CHEEK DEFECTS
General options for zone 3 reconstruction:
1. Leave the defect alone. As a general rule a surgeon would not leave these defects alone. However, if a direct
excision will leave an inordinately long scar, then allowing the excision to heal secondarily is an option because
it will not distort the local anatomy. (This is unique to the zone 3 central cheek region where scarring will not give
an ectropion.) Ultimately, the final excision and closure may be smaller than an immediate reconstruction.
2. Full-thickness skin grafting is a very low preference for reconstructing zone 3 defects. Skin grafts in zone 3 violate
the middle of the cheek aesthetic unit and will be seen as a deformity consisting of a patch of lighter- colored skin.
3. for Simple (direct) closure. A vertically oriented scar is better than a horizontally oriented scar, and an attempt
should be made to keep the vertically oriented scar lateral to the Z-line. In addition, a lower zone 3 vertically
oriented scar looks better than an upper zone 3 vertically oriented scar. When scars are located on the cheek
prominence, the scar is more noticeable. In addition, the malar eminence or upper zone 3 area is non- bearded and
therefore offers less camouflage of scars.
4. Flap coverage.
FREE FLAP RECONSTRUCTION OF THE CHEEK
Free flaps are primarily indicated for reconstruction of large cheek defects involving the external skin, inner lining,
or full thickness. The radial forearm flap is our first option for reconstruction of such defects because of its thin
pliable skin paddle with minimal soft tissue. The lateral arm or anterior thigh fasciocutaneous flaps provide larger
amounts of skin and soft tissue volume and are therefore used for larger cheek defects. Once masticatory muscles,
the parotid gland, and/or the maxilla or mandible are included with the resection, cheek defects become more
complex, and larger soft tissue or composite free flaps are mandatory for reconstruction. The rectus abdominis
myocutaneous free flap has proved to be very useful for reconstruction of these massive defects, and the scapular or
latissimus dorsi free flap are secondary alternatives. Cheek defects including the ascending ramus of the mandible
are best reconstructed using an osteocutaneous scapular or radial forearm flap. Full-thickness cheek defects that
include the oral commissure and lips are more challenging to reconstruct. We advocate using a lip-switch procedure
to provide a functional stoma and using a free flap with two separate skin islands for lining and cover, but not for
reconstruction of the oral commissure.
The cheek is limited superiorly by a horizontal line that extends from the infraorbital rim to the root of the
auricular helix. Laterally, the cheek extends over the anterior border of the ear and continues inferiorly along
the mandibular border. The medial margin of the cheek is the lateral nasal wall and nasolabial crease.
Tumors involving the cheek may arise from a variety of different tissue components that make up this
complicated structure. Tumors may arise from the skin externally, the mucosa internally, or the muscles and
the parotid gland in between. If the skin or mucosa is resected, the defects are more likely to require some
form of plastic reconstruction.
These reconstructive problems become much more difficult if multiple layers of the cheek are involved, and even
more complex if adjacent structures such as the eyelid, nose, lips, commissure, and mandible or maxilla are

involved. The vast majority of small- and medium-size defects of the cheek may be closed primarily using
local or regional flaps. Free flaps are usually reserved only for reconstruction of large defects involving
external skin, intraoral lining, or both (full-thickness defects). They are usually essential if the resections
include the upper or lower jaw with soft tissue and skin. Free tissue transfer has also been described for
improvement of contour deformities that may be congenital or acquired in nature.
Indications for free tissue transfer
As with any reconstructive procedure, the simplest technique is usually selected if it will adequately achieve
the objectives of the reconstruction. When methods such as skin grafts, local flaps, or regional flaps are
unavailable or inadequate, a free flap becomes the method of choice. After applying these parameters for
reconstruction, the principal indications for using a free flap for cheek reconstruction include:
1) resurfacing of extensive external skin defects;
2) resurfacing of extensive intraoral defects;
3) moderate to large through-and-through defects;
4) extensive contour deformities;
5) smaller defects where local flaps are unreliable due to previous surgery, compromised blood supply, or
radiation therapy.
General considerations
There are several basic principles that must be applied to reconstruction of the three layers of the cheek
(external skin, internal lining, soft tissue fill). Resurfacing external cheek skin is principally an esthetic
endeavor, and issues such as contour, color match, texture, and appearance are of primary concern. The
principle of facial units should be adhered to as much as possible to optimize esthetic results thin pliable
skin in addition to multiple skin islands. These flaps can restore intraoral lining and cheek skin in one
stage, without a major increase in bulk.
The cheek may be considered a single total facial unit or may be divided into three smaller overlapping
subunits: 1) suborbital, 2) preauricular, and 3) buccomandibular (Fig 1). Although it may be occasionally
necessary to sacrifice adjacent normal tissue, final results are far superior when scars follow facial
subunits, thus

minimizing the appearance of a "patch. Restoration of intraoral cheek mucosa is essential to maximize the
functional aspects of speech and mastication.
With the introduction of microsurgical techniques, our ability to reconstruct massive intraoral defects has
improved substantially over the last two decades. More recently, the importance of sensation for adequate
function and meaningful quality of life after flap intraoral reconstruction has been emphasized. The capability
to sense ingested food in the mouth facilitates mastication and enhances swallowing function; it also
favors gustatory delectation, prevents pooling and drooling of saliva, and increases quality of speech. For
this reason, surgical techniques to provide sensate free tissue transfer and appropriate rehabilitation in
oromandibular reconstruction are becoming more popular.
Full-thickness cheek defects represent a difficult reconstructive challenge, because both esthetic and
functional issues must be addressed. Regional flaps are usually not large enough to provide both intraoral
lining and external skin. Although a combination of two regional flaps has been described for
reconstruction of through-and-through defects, these are usually extensive procedures that require two or more
stages and frequently create a bulky cheek that has poor function and poorer aesthetic results. Free flaps
have become the preferred method for reconstructing such extensive defects; they can provide large quantities of
thin pliable skin in addition to multiple skin islands. These flaps can restore intraoral lining and cheek skin
in one stage, without a major increase in bulk.
Definition of large cheek defects
large cheek defects are defined as those larger than 4 cm in diameter. This size is chosen to exclude defects
that can be closed primarily or repaired with a small local flap and include defects that require significant
tissue transfer with a large local, regional, or distant flap. Such defects may well include other structures,
such as part of the lips, nose, and even the orbit.
The goals of cheek reconstruction are to restore, as much as possible, normal appearance and function. Normal
function is achieved by obtaining a healed wound that does not leak and by maintaining sufficient tension on the
cheek so that it does not sag or develop pockets that can collect food debris. Normal appearance is approximated
by matching the color and texture of the repair to that of the surrounding skin and, when possible, by hiding
the scars in borders between adjacent facial aesthetic units. As in most types of reconstructive surgery, achieving
a normal contour takes priority over avoiding or camouflaging scars.
Cheek defects can be repaired with skin grafts, local flaps, regional flaps from the neck (cervicofacial flaps),
or distant flaps (myocutaneous regional flaps or free flaps). Each of these options has a place, and none is the
best choice for all defects or all patients. To choose the best option for any given patient, the surgeon must
assess both the defect and the tissue available for its repair. Factors such as skin color, previous radiotherapy,
and laxity in the adjacent tissues will help to determine the reconstructive technique of choice.
1. Split thickness skin grafts 2. Full thickness skin grafts 3. Loco-regional flaps
a. Deep plane cervicofacial flap b. Cevicofacial deltopectoral flap
4. Free flaps
FREE FLAP DONOR SITE SELECTION
The choice of free flap is dictated by the requirements of the defect. The defect should first be evaluated with
regard to:
1) The amount of external skin;
2) Intraoral lining requirement; and

3) soft tissue bulk required.
There are a variety of different skin and soft tissue flaps that can be used to reconstruct these complex
defects. The following free flaps tend to be the most useful for reconstruction of the cheek.
1.Radial forearm flap
2.lateral arm flap
3.anterolateralthigh flap
4. Scapular/Parascapular Flap
5. Rectus Abdominis Flap
APPROACH TO CHEEK RECONSTRUCTION BASED ON TYPE OF DEFECT
External Defects
a. External Skin Only:- These defects potentially require a large surface area of thin pliable skin with
minimal soft tissue. In a majority of these cases, the radial forearm fasciocutaneous flap provides the
ideal quantitiy of skin, with minimal bulk. To maximize esthetic results for these type of defects, it is
best to keep the facial subunit concept in mind. If necessary, the defect should be extended to the
junction lines between different facial subunits. In many cases, the radial forearm flap provides poor
color and texture match. One option to improve these esthetic results is to remove the skin at a later
date, and to apply full-thickness supraclavicular skin grafts over the subcutaneous portion of the flap,
to provide better color and texture match.
b. External Skin Plus Soft Tissue:- These defects tend to require both extensive skin surface area as well
as soft tissue volume. Many patients in this category have under gone parotidectomy in combination
with resection of the skin. In some cases, the facial nerve may be resected. If technically feasible, the
nerve should always be primarily grafted and then covered with the free flap. The choice of free flap
ranges from a radial forearm flap to a lateral arm flap, anterolateral thigh flap, or scapular flap,
depending on the increasing amount of soft tissue bulk that is required. In general, it is best to volume-
overcorrect these defects and then, if necessary, to revise them secondarily with traditional liposuction.
The lateral arm flap is found to be most useful for radical parotidectomy.
c. External Skin/Soft Tissue/Bone:- if the resection includes bone, the bone does not necessarily need to
be reconstructed. If the lateral aspect of the maxilla is missing, soft tissue coverage alone will usually
provide adequate contour restoration. If the ascending ramus of the mandible is resected, then a
combination of vascularized bone with skin and soft tissue is necessary. The scapular flap provides the
ideal solution to this complicated problem, because the bone is usually adequate to reconstruct the
mandible, and the skin/subcutaneous portion of the flap serves to cover the rest of the defect.
Internal Lining Defects
a. Mucosal Defects:- Most small mucosal defects of the cheek can be closed primarily. Defects that involve
the entire lining of the cheek, extending from maxillary to mandibu- lar sulci, will usually require a
free flap. These defects require a large surface area of very thin pliable skin; the radial forearm
fasciocutaneous flap remains the flap of choice. Many of these resections include a marginal
mandibulectomy, and in these situations, the flap can be sutured directly to the lingual mucosa
inferiorly. Care must be taken to inset just the right amount of flap. Too much flap will create an
insensate bulky mass in the oral cavity that may interefere with mastication. Too little flap may create
difficulties with mouth opening and functional trismus. It is felt by many authors that skin undergoes

"mucosalization" phenomena, which allow chewing with-out disruption of the oral lining integrity. The
hair on the forearm flap can sometimes become an esthetic problem, and we have found that
electrolysis for hair removal can be a useful adjunct to improving the final result. For patients with
resection of the ascending ramus of the mandible in combination with the intraoral and pharyngeal
lining, the forearm osteocutaneous flap provides an excellent solution, n The minimal amount of bone
that is provided by the radius is usually adequate for reconstruction of the mandibular defect, and the
skin provides excellent intraoral lining.
b. Full-thickness (Through-and-Through) Defects:- These are usually extensive tumors that involve the
intra- oral lining, cheek soft tissues, plus external skin. The ideal flap for reconstruction of this type of
defects is the radial forearm fasciocutaneous flap. The thin pliable skin provides both internal lining and
external coverage when the flap is folded on itself. It usually provides ad equate thickness and bulk to
maintain the contour of the cheek. The major drawback of this type of reconstruction is the poor quality of the
skin and the fact that the patient is usually left with a pin-cushioned type deformity externally as a result of the
circumferential nature of the defect. however, it does provide a good functional result. If the commissure of
the mouth is resected, generally it is not do advocated using a portion of the flap to reconstruct the
commissure. Instead, restoration of continuity by suturing the lip to itself and then using the free flap to
provide intraoral closure and external lining.
c. Mucosa/Soft Tissue/Skin/Bone:- These defects tend to be massive. Most of these patients have full-thickness
resection of the cheek in combination with segmental mandibulectomy, as well as portions of the
maxilla/orbit. These reconstructions require a flap that provides both extensive skin surface area as well as
substantial soft tissue bulk.There are basically two ways to approach this problem. A soft tissue reconstruction
alone can be provided. If the patient is not too obese, a rectus flap will provide multiple skin islands to restore
intraoral/palatal closure as well as a second skin island to resurface externally. The bulk of the flap will often
provide a surprisingly reasonable contour, despite the fact that mandibulectomy has been performed. Many of
these patients require revisionary procedures to improve contour. A second approach to this type of problem is
to reconstruct both the bony deficit as well as the intraoral and external lining. In this situation, a double free
flap is the only solution to the problem. The fibula osteocutaneous free flap can be used to reconstruct the
mandibular segmental deficit, with the skin used externally. A forearm flap can then be used to reline the
cheek introrally. In general, these massive defects will have poor esthetic results, but still function remarkably
well.
CHIN RECONSTRUCTION
When tissue loss occurs within the chin unit, options for repair are determined by the site, size, and depth of the defect, as well as the availability of local or distant tissues. A superficial defect may be covered with a full-thickness skin graft or a smaller defect repaired by primary closure. Other options include unilateral or bilateral horizontal advancement flaps, 1 a bilobed flap, 2 rhomboid flaps from the cheek or lip, a platysmal myocutaneous 3 flap, or a one-stage flap from the submental area. 4 Larger losses, especially when associated with missing lower lip, might employ a two-stage deltopectoral flap s or free radial forearm flap. A two-stage subunit flap taken from the submental excess can also be used for significant defects of skin and soft tissue of the chin. This subunit skin flap restores skin quality with adjacent matching facial submental skin. By positioning scars in the unit join between the lip, cheek and neck, the scars from reconstruction are less visible, and the convex contour of the chin is not disrupted by scarring or flap pin-cushioning within the chin pad. Chin projection can be augmented by including additional soft tissue. The contour of the cervical donor site is maintained by excision of subcutaneous and subplatysmal fat and platysmal tightening.

LIP RECONSTRUCTION
The lips are the primary aesthetic feature of the lower central face, with functional requirements that include speech,
containing oral contents, and kissing. A hallmark of the lips is their mobility, which is critical for natural appearance
and function. Reconstruction of lip defects is simple in that reconstruction, inmost cases, is feasible, but complex in
that a natural-appearing, dynamic reconstruction is often elusive
Topographic/Aesthetic anatomy of lips
1. Philtrum columns 2. Philtrum groove/dimple 3. Cupids bow 4. White roll upper lip 5. Tubercle 6. Commissure 7. Vermillion
Functional considerations
Lips help Oral competence, Communication of emotion, Deglutition, Speech (labial sounds: “b”, “m”, “w”, “p”)
(Labial-dental sounds: “f”, “v”)
Pathology incidence
Squamous Cell Carcinomas – 95% on Red lip (95%) – 90% on Lower lip versus 10% on Upper lip – Exophytic more common than ulcerative
Minor Salivary gland tumors – Adenoid cystic, adenocarcinoma, mucoepidermoid
Basal Cell – Usually on cutaneous white upper lip
Vermillion defects
The vermilion is a thin layer of nonkeratinized epithelium that is devoid of sebaceous glands and hair follicles. It gets
its unique color and spongy nature from the underlying dense capillary network. Beneath this capillary network is the
orbicularis muscle. The vermilion is bordered by the white roll, which is a myocutaneous ridge that sits just outside
the vermilion border.The upper-lip vermilion is thickest directly below the high points of the Cupid’s bow. Below the
depth of the bow, the vermilion often forms a tubercle. This is most obvious in children. The vermilion tapers off
toward the commissure wherethe white roll becomes less prominent.
Small, superficial vermilion defects can usually be closed primarily without elevation of flaps. Care must be taken to
evert the edges to prevent notching. Lateral, superficial defects more than 2 to 3 mm from the white roll can usually be
left to heal by secondary intention. This is less successful centrally where there can be a depression or a notching at
the site. Alternatively, V-to-Y advancements from inside the vermilion will result in minimally noticeable scars.

For larger vermilion defects that do not involve the white roll, flaps are indicated. These can include
vermilion flaps (lip flaps) or mucosal and tongue flaps (nonlip flaps). Vermilion flaps are best suited for
defects that are close to the white roll.They replace vermilion with vermilion and scars in the vermilion itself
usually heal well.
Techniques include vermilion advancements or vermilion switches from the opposite lip. Vermilion
advancements are best suited for central defects. These are robust flaps based on the labial vessel. The
external incision is made directly on the vermilion border and the intraoral incision is made well inside the
lip. These flapshave a distinct advantage, especially in central defects in that the normal vermilion taper is
preserved. This advantage is lostin more lateral defect. For more lateral defects, the distance from the
vermilion border to the wet–dry line is measured onboth sides of the defect. The taller side is tailored so that
the vermilion will not show a significant step off at the wet–dry line.
Vermilion switch flaps are extremely useful. The vermilion is cut exactly as in a vermilion advancement, but
is inset in the opposite lip. The reconstruction of the donor lip is with vermilion advancement at the time of
flap division. Theseflaps, like all lip flaps, are divided at 10 days. It is best not to delay division too long, as
significant secondary healing will make tailoring and inset time more difficult, especially in the donor lip.
Mucosal advancements are useful for broad defects that are remote from the vermilion border, as these defects will
have enough normal appearing vermilion spared. As mucosal flaps contract and retract, they will result in a thinner lip,
everted lip and this should be expected. These bipedicled flaps are elevated just below the minor salivary glands and
advanced to fill the defect.The donor site is treated with a mucosal graft.
Tongue flaps are another method of reconstruction. The anteriorly based lateral tongue flap is a useful tool as it can
provide significant bulk. It, like all other nonvermilion flaps, does not leave a normal-appearing lip and is therefore
best reserved for lateral defects. It is elevated from the lateral surface of the tongue, avoiding the papillary tongue.
Closure of the dono site is important as the lingual nerve may be exposed in larger flaps.
LOWER LIP RECONSTRUCTION OPTIONS

Wedge Excision & Primary Closure
For lesions involving < 1/2 lip Upper or lower
V-plasty/wedge excision and primary closureImprove vermilion-cutaneous matching with angulation of lateral Incision border
M-plasty is indicated for a larger lesion using wider inferior margin
Karapandzic Flap indicated in lesions involving upto 1/2 to 2/3 of Central Lower lip
Karapandzic Flap - technique
Skin and mucosa is incised preserving trigeminal and facial nerve branches, labial arteries, and muscle if possible this
technique may result in Mild microstomia, but with clinically acceptable results
Bernard-von Burrow Flap is indicated in lesions involving more than 2/3 of lip, in patients with adequate cheek
tissue but with midline defect or pathology of 4 cm in length can be corrected.
Technique:
Horizontal incisions through skin from the commissure to melolabial fold is created and triangles/cresents of skin and
subcutaneous tissue are excised adjacent to melolabial fold, facial muscle are not touched, triangles/cresents are also
excised lateral from menatla- labial groove as requird. Intra oral mucosal advancement flaps are created, flaps
advanced and sutured. Small ellipse of skin removed from superior portion of flap and mucosa advanced to create new
lower lip vermillion.

Nasolabial transpositional flaps also called as gilles fan flap
For reconstruction of 2/3 of upper or lower lip with lateral defects having adequate adjacent cheek tissue
UPPER LIP RECONSTRUCTION OPTIONS
Abbe sabbatni cross lip Flap
Defect of 1/2 - 2/3 of upper or lower lip where commissure are not involved
Technique: “V” shaped incision is diagrammed around the lower lip lesion and proposed upper lip flap outline, the
lesion is removed, flap transposed and sutured into the defect. Flap is designed with same height as defect but only
50% of width, resulting in equal witdth reduction of upper and lower lips. Pedicle is divided at 2 weeks, with
preferably Z-plasty being performed at donor site to prevent notching.
Technique:
1. For lower lip, start with full thickness incision medial to defect
2. Then, continue the full thickness incision laterally and around
the commissure
3. Then, follow the melolabial fold
4. Then, carry the incision down to the superior vermillion border
5. Advance flap and suture individual layers together

Estlander Flap is indicated for lesion involving 1/2 - 2/3 of upper or lower lip with Commissure being involved
Technique: “V” shaped incision diagrammed around lower lip lesion and proposed upper lip flap outlined, after
lesion is removed, flap rotated and sutured into the defect. Flap is designed with height 1-2 mm greater than defect to
reconstructed.
Modified Burrow Technique is indicated in 2/3 of upper lip, with midline defect having adequate adjacent cheek
tissue. The technique has a disadvantage of resulting in Mild microstomia and Loss of cupid’s bow.

ORAL CAVITY RECONSTRUCTION
Reconstruction of oral cavity poses a difficult challenge due its Complex anatomy and function. The Goals oral cavity
reconstruction include restore preoperative function and cosmesis. Patient status is important consideration as there are
variety of reconstruction options.
Anatomy
Anterioposteriorly from Vermilion of upper lip to junction
of hard and soft palate andInferiorly to infront of circumvallate papillae
and inferiorly bonded by floor of the mouth and palate superiorly and
laterally bonded by teeth and gingivobuccal sulcus.
Structures: lips, alveolar ridges, buccal mucosa, retromolar trigone, hard palate,
floor of mouth, mobile tongue
Functions: speech, mastication, bolus preparation and initiation of deglutition
Functional Considerations in oral cavity reconstruction include maintaining functionality tongue, Speech and
deglutition, Articulation of speech and Bolus manipulation in preparation for deglutition and lastly Sensory functions
which include proprioception, pain, taste which are helpful in Assisting in mastication and bolus processing.
Classification of defects according to Jaccobson et al
Group 1: reconstruction of floor of mouth, ventral tongue, cheek
Group 2: Reconstruction of anterior tongue, anterior floor of mouth
Group 3: Reconstruction lateral pharyngeal wall, soft palate

Floor of Mouth Reconstruction
Requires soft and mobile tissue
Requires mobility of oral tongue
Avoiding of scar contracture (i.e., secondary intention)
Avoiding flaps with bulk (glossoptosis, obliteration of lower lip sulcus)
For Smaller defects Split thickness skin graft harvest preferably from lateral thigh at 0.017 in Provides water-tight
closure, thin pliable skin, the graft is Stabilize with bolster.The graft is known to survive Survives over muscle and
cancellous bone (via imbibition and neovascularization) the graft is Also good for lateral FOM and retromolar trigone
reconstruction
For Moderate defects involving a portion of mylohyoid muscle, Nasolabial flap Based on angular artery is a good
option, it is better for older patients with lax skin. However, itsRequires two stages and there may be presence of
temporary fistula and constant use of bite block is necessary until flap division
The following regional flaps can also be considered for moderate defects.
Forehead flap: it is used rarely, based on superficial temporal artery, its more reliable 2/3rd distance across the forehead for FOM reconstruction its tunneled into cheek below zygoma requiring orocutaneous fistula, the donor site being covered with skin graft. After two weeks, the flap is divided, the fistula closed and the inset of forehead flap is done.
Submental artery flap: Thin, supple skin based on Submental branch of facial artery, primary closure of donor site is done after taking flap it has poor reliability if facial artery has been sacrificed and in case of persons with irradiated necks. The Submental Flap is an axial flap described by Martin et al in 1993 after successfully using it on 8 patients.
During that time the indications for medium size lesions in the maxillofacial region had been thoroughly
described. Theywere characterized by their thinness, versatility, mimicry with facial skin and minimal
morbidity in the donor zone. Nevertheless, their use in malign lesions is controversial becauseof the risk of
infecting the receiving neck area with cervical metastasic disease.
GENERAL CONSIDERATIONS o Indications
The submental flap may be used for intraoral reconstruction and repair of cutaneous facial defects.
Advantages of a submental flap include its minimal donor site morbidity; excellent cutaneous color, texture, and thickness match; and pliability. The thin skin and short distance to the recipient bed are advantageous for the reconstruction of mobile oral structures, such as the tongue and floor of mouth. In men, this may be particularly useful for reconstructing hair-bearing defects.
The width of the flap is determined by the laxity of the neck skin allowing primary closure ("pinch test"), and can be as large as 18 cm x 7cm. The vascular pedicle and length is designed according to the defect and can span from mandibular angle to angle if necessary, providing an arc of rotation extending from the medial canthus to the zygomatic arch. The pedicle length can reach 5 cm when the entire facial artery is retained (ref 8c).
o Contraindications Circumspection is advisable in the setting of oral cavity malignancy, which may
directly involve level 1 and more frequently metastasize to those lymph nodes. Prior radiotherapy to the neck will significantly compromise the viability of the flap.
Though use of the flap is not contraindicated, a split thickness skin graft for closure may improve donor site closure and wound healing.

Neck dissections that interrupt the submental branch of the facial artery are a relative contraindication to the use of this flap.
The flap is relatively thin, and the need for tissue bulk is a contraindication to the use of this flap.
For larger or more distant defects, an alternative reconstruction method or modification of this flap into a free flap should be considered.
o Pertinent Anatomy The submental island flap is an axial patterned flap based on the submental artery.
The submental artery is a consistent branch of the facial artery. It arises deep to the submandibular gland and may be deep (70%) or superficial (30%) (ref 8a) to the digastric muscle. It courses just superficial to the mylohyoid muscle as it passes forward and medially in level Ia of the neck to end behind the symphysis of the mandible. The artery then gives off a variable number of perforators that pierce the platysma muscle and supply the subdermal plexus.
Caution should be exercised during the dissection as there may be only one reliable perforator off the submental artery that will ultimately supply the flap. The location of this critical perforator is variable and can be lateral or medial to the digastric muscle. A modified technique is to include the mylohyoid in the flap, thereby protecting the vascular pedicle and limiting the vascular dissection necessary (ref 8b).
Venous drainage is achieved through a constant submental vein that generally drains into the facial vein. Less often, the submental vein can drain into the external jugular vein and therefore this vein should be kept flowing until the exact drainage pattern is understood. Pre-operative evaluation of the patient's imaging may be helpful.
Modifications of this flap which have been described include conversion to an osteocutaneous flap by incorporating a segment of the mandibular rim, and elongation of the pedicle by division of the facial vessels distal to the origin of the submental artery.
PREOPERATIVE PREPARATIONS o Evaluation
A careful history and physical examination should be undertaken to determine that there has been no prior neck surgery or radiation therapy that would contraindicate the flap.
o Potential Complications Flap failure and loss of the cutaneous paddle: Disruption of the critical perforator off
the submental artery risks skin necrosis. Compromise of oncologic control: isolation of the flap pedicle may compromise the
continuity of the neck dissection, particularly in the setting of oral cavity cancer and risk transferring malignant nodal tissue to the area of reconstruction
Injury to the mandibular branch of the facial nerve Distortion of the contour of the jaw line will occur to some degree with the use of this
flap and patients should be aware of that.
ANESTHESIA CONSIDERATIONS o General
The patient should not be paralyzed until after the mandibular branch of the facial nerve that will be required for the particular use of the flap is identified.
The patient is positioned and, in most cases, the bed will be turned 180° from the anesthesiologist.
In the vast majority of cases, the surgery is done under general anesthesia.
OPERATIVE PROCEDURE o The patient is placed in the supine position with the neck extended.

o The upper border of the flap is drawn at the inferior border of the mandibular arch and the maximal width of the flap is determined by a pinch test to assess how much donor site can be
closed primarily. It is usually designed in an elliptical fashion. o A subplatysmal dissection is carried out until the ipsilateral submandibular gland and bilateral
anterior belly of the digastric are identified. The facial and submental vessels are identified deep to the superior aspect of the gland, and are skeletonized with the subplatysmal skin island up to the lateral border of the mylohyoid. Care is taken to identify and protect the marginal mandibular nerve.
o Once the submental vessels are visualized until they proceed under the anterior belly of the digastric, the flap can be raised from distal to proximal. The contralateral aspect of the flap can be raised either in a sub-platysmal or supra-platysmal plane (this can reduce the risk of injury the the contralateral marginal mandibular branch)
o The overlying segment of the ipsilateral anterior belly of the digastric muscle is dissected off the mandible and the hyoid bone and included with the flap to protect the terminal vascular supply as it passes deep to the muscle.
o The underlying mylohyoid muscle is either cut or a strip is included with the pedicle if the flap needs to be tunneled medial to the mandible for intraoral reconstruction. The mylohyoid is detached from the mandible and the hyoid and is bluntly dissected off the ipsilateral geniohyoid muscle to complete the flap mobilization
o The remaining neck dissection is performed with preservation of the facial vessels and the internal jugular vein.
o The flap is tunneled subcutaneously or intraorally depending on the location of the defect. o Depending on the location of the defect, it may be necessary to perform several maneuvers to
increase arc of rotation. This includes dividing the facial artery and vein distal to the take off of the submental vessels. Division of the posterior belly of the digastric and skeletonizing the vessels to the external carotid and internal jugular vein can also improve reach. If necessary, the facial vein may also be divided and re-anastamosed using microvascular techniques to a vein (i.e. retromandibular vein) closer to the defect.
o Closure is performed in the usual fashion for neck dissection, utilizing suction drains.
POSTOPERATIVE CARE o Drains are removed when the output is less than 30 ml per day. o Tension on the flap is minimized if the patient’s head is turned toward the donor side. This
should be reinforced in the postoperative orders and accomplished with pillows or sandbags.
Platysma flap Facial artery musculomucosal flap (FAMM), its bases on branches of facial artery, it usually Contains
mucosa, buccinator muscle, and fat, 2 x 8 cm flap can be taken without injury to facial nerve.
Surgical Technique. The FAMM flap was based inferiorly (antegrade flow) for all patients. The flap was designed over the facial artery trajectory with an oblique orientation, from the retromolar trigone to the level of the ipsilateral labial sulcus. The length of the flap was tailored proportionally to the size of the defect. The orifice of the Stensen’s duct limits the width of the flap posteriorly which is kept under 3 cm to avoid tension at closure of the donor site. Anteriorly, the incision lies 1 cm posterior to the oral commissure. As a first step, the flap is marked on the buccal mucosa respecting the previously mentioned limits .

The dissection starts 1 cm lateral to the oral commissure by cutting through the mucosa, submucosa, and buccinator to identify the facial artery or one of its branches. The superior labial artery is usually identified at first place, then ligated and divided. The flap is elevated in the layer underneath the facial artery including the overlying
buccinator muscle and a small portion of orbi cularis close to the oral commissure.The facial artery is kept attached to the overlying tissues in the entire length of the flap. On the superior end of the flap the facial artery is ligated and divided. The venous drainage relies on a submucosal plexus and for this reason identification and preservationof the facial vein is notmandatory. A reasonable soft tissuebase is maintained to allow an adequate venous drainage.After elevation, the flap is rotated inferiorly and inset into the FOM defect.Sutures should not impair tongue mobility for optimal functional results . A biteblock is used temporally if the pedicle crosses over molar teeth.
Deltopectoral flap (historical significance)
Fasciocutaneous free flaps can also be considered for their thin nature and pliability providing tongue mobility and
free movement of food during deglutition.
Radial forearm flap Lateral arm flap Thigh flap
Tongue Reconstruction are very difficult to reconstruct because of tongues complex intrinsic musculature and
function for defects <50% can be closed primarily +/-STSG, Larger or composite defects require more bulk (i.e,
fasciocutaneous free flap) ,Lateral arm free flap is good for defects including posterior aspect of tongue/FOM.
Total Glossectomy Defects often accompany oral cavity defects with extensive disease, requiring bulk for
reconstruction, goals for total glossectomy reconstruction include direct secretions laterally, provide contact of neo-
tongue with palate, use flaps which will not atrophy over time and planning for palatal drop prosthesis. The various
options that maybe considered are:
1. Rectus abdominis free flap based on inferior and superior epigastric arteries and Motor nerve (intercostal) anastomosis retains bulk
2. Latissimus dorsi myocutaneous free flap having Thoracodorsal artery and motor nerve (thoracodorsal) and lastly
3. Pedicled flaps (PMMF, latissimus dorsi)
Buccal Cavity Reconstruction for small defects – primary closure possible, for larger superficial defects quilted
skin/mucosal grafts including allografts like collagen membrane. For Large full-thickness defects pedicled flaps like
Pectoralis major myocutaneous, Latissimus dorsi myocutaneous flap and Fasciocutaneous free flaps are to be
considered.
1.Mucosa & Submucoa, 2. Buccinators,
3.Facial Artery, 4. Facial Nerver, 5. Muscles Of
Facial Expression, 6. Molar Tooth, 7.
Mandible, 8. Gingiva Buccal Sulcus

TISSUE EXPANDERS
Introduction.
Although the genesis of modern-day tissue expansion is credited to innovators such as Radovan and Austad , the
technique takes some of its roots from early lessons in distraction osteogenesis. Bone traction with either internal or
External devices at the turn of the 20th century, paved the way for the concept that mechanical stress on tissue could
lead to lengthening. Putti extrapolated these ideas from bone to the surrounding soft tissue, by placing constant tension
on a composite tissue to obtain soft-tissue lengthening. In the middle 1950s, Neumann became the first surgeon to use
an expansile implant when he used a latex balloon to enlarge periauricular skin for a traumatic ear deformity.
20 years after Neumann’s report that tissue expansion was revisited. Charles Radovan, a resident at Georgetown,
reintroduced the concept of expansion when he inserted a contemporary device with an internally placed port. Shortly
thereafter, Eric Austad produced a self-inflating device.
Since that time expansion has been applied to a multitude of reconstructive problems with applications demonstrated
in both regional expansion and expansion at distant sites for subsequent graft and flap transfer.
Physiology
When a constant mechanical stress is applied to skin over time, two phenomena occur: mechanical creep and
biological creep. The former is based on morphologic changes that occur on a cellular level in response to the applied
stress—the cell is stretched. Disruption of gap junctions and increased tissue surface area then result in cell
proliferation (biologic creep).
Growth of the tissue by cell proliferation restores resting tension of the stretched tissue to baseline. The epidermis gets
thicker with concurrent thinning of the dermis and alignment of collagen fibrils. These effects are maximized at 6 to
12 weeks postexpansion. On a molecular level, a panoply of growth factors—cytokines, hormones, adhesion
molecules, cytoskeletal elements, and signal transduction proteins—are induced in response to expansion (6),
confirming that tissue expansion is a dynamic process.
One feature that makes an expanded flap so reliable is its improved vascularity. It has been demonstrated that the
vascularity of an expanded flap is superior to its nonexpanded counterpart in both number and caliber of vessels.
Moreover, angiogenic factors, such as vascular endothelial growth factor (VEGF), are expressed on the surface of
expanded tissue at a significantly higher level when compared to nonexpanded controls. This augmentation in blood
flow is attributable to the
capsule that forms around the expandable prosthesis. Because of the similarity between expanded and delayed
flaps in vessel caliber, tissue expansion is well regarded as a form of the delay phenomenon. An expanded flap,
therefore, is a delayed flap.
The expanded skin is more vascular than the normal adjacent skin. This has been shown experimentally and has also
been observed clinically by most of the surgeons. The flaps raised out of the expanded skin and hence have better
chances of survival. Increased vascularity is partly because of the presence of the capsule. The pattern of vascularity in
the expanded skin is comparable to that of the delayed flaps. An expanded flap may also be labeled as a delayed flap.
Temporary hypoxia caused by the pressure of the expander is one of the explanations for the increase in vascularity or
Angiogenesis
Types of prosthesis
Self inflating expanders and external inflating expanders exist.
Self inflating expanders are non textured and contain osmotic substance that causes migration of extracellular
water into the expander.

Based on shape, size, and type of filling valve. Expanders can be standard, customized, anatomic to the donor
site (breast), or differential in fill volume to provide tapering of tissue.
The more commonly used include the round and rectangular types; crescent-shaped (and croissant) prostheses,
originally developed to minimize dog-ears at the donor site, have fallen out of favor as it has been recognized that the
added tissue gained with rectangular expanders may increase the choices possible for flap design.
Expander volumes have a wide range and vary according to the anatomic site. Round expanders of 100 to 2,000 cm3
and rectangular expanders of 100 to 1,000 cm3
Saline is delivered in a controlled fashion via the valve port, which is either integrated into the prosthesis or connected
to the device by silicone tubing of customized length.
An integrated system offers the advantage of undermining a single pocket for expander placement,but also places the
implant at risk of perforation by a misplaced needle. Internal remote ports remove the danger of perforation away from
the prosthesis itself, but introduce the potential complications of overturn of the port, tube obstruction, and
migration.
An integrated system offers the advantage of undermining a single pocket for expander placement,but also places the
implant at risk of perforation by a misplaced needle. Internal remote ports remove the danger of perforation away from
the prosthesis itself, but introduce the potential complications of overturn of the port, tube obstruction, and migration.
Parts of tissue expanders
A tissue expander is composed of three parts, a elastic silicon balloon, a connecting tube injection port.
Indications:
• Post mastectomy reconstruction.
• Scar revision procedures.
Soft tissue expansion prior to bone augmentation in mandible
• A variety of procedures to develop an adjacent skin flap for correction of a defect for example in case of burns
Contraindications:
• Open cuts or sores at the implant site.
• Poor general patient health.
• Systemic disorders such as diabetes.
• Cardiovascular disease.
• Physiological and anatomical anomalies.
• Previous repeated contour correction failures.

• Inadequate tissue coverage.
• Tissue covering determined unsuitable by the surgeon. To varying degree, radiation damage,
• ulceration, compromised vascularity, or history of compromised wound healing may affect tissue
• covering suitability.
• Physiological condition determined by the surgeon to pose unduly high risk of surgical and /or
• postoperative complications. To varying degree, obesity, smoking, diabetes, autoimmune disease,
• coagulopathy, chronic lung or severe cardiovascular disease may affect patient suitability for surgical
implantation.
• Use of drugs that may result in high surgical risk and/or significant postoperative complications,
• including any drug that would interfere with blood clotting.
• Psychologically unsuitable patient, including negativism or lack of understanding, motivation, or
• cooperation. Sensitive over or underlying anatomy.
Advantages
The primary advantage of tissue expansion is that it provides a source of adjacent donor tissue whose colour and
texture are usually well matched to the recipient site
In addition, tissue expansion recruits both sensate and hair bearing tissue when required
Complications
Major complications involve infection, implant exposure, and flap ischemia.
Minor complications with expansion include transient pain with expansion, seroma, dog ears at the donor site, and
widening
of scars.


















