Leukapheresis* by Continuous Flow Centrifugation (CFC) in - Blood
18
Leukapheresis* by Continuous Flow Centrifugation (CFC) in Patients with Chronic Myelocytic Leukemia (CML) By DE Bucic, ROBERT G. Giiw, JR., ROBERT J. EISEL, EDWARD S. HENDERSON AND SEYMOUR PERRY M ORTALITY associated with prolonged and severe pancytopenia, irres- pective of etiology, is high. The magnitude of this problem has increased with the use of intensive x-irradiation and potent chemotherapeutic agents for the treatment of malignancies and for immunosuppression in recipients of allografts. Infection is the major cause of death in patients with acute leukemia2 since hemorrhage from thrombocytopenia can be controlled by platelet and whole blood transfusions. Mortality from infection can be directly related to the degree and duration of granulocytopenia.3 To decrease the morbidity and mortality associated with granulocytopenia, three experimental modes of therapy have been attempted: 1 ) patient isolation with antibiotic suppression of endogenous flora,4 2) granulocyte replacement,57 and 3) bone marrow transplantation.8 The procurement of leukocytes from normal individuals and maintenance of granulocyte levels in aplastic recipients poses many problems which can be related to the kinetic and sedimentation properties of granulocytes. Granulo- cytes comprise only a small fraction of whole blood and their density overlaps that of red blood cells (RBC’s). Granulocytes are, therefore, difficult to separate and collect without significant contamination by RBC’s. It has been shown that the leukocytes from 40 or more units of normal whole blood are required to raise the peripheral blood granulocyte level by 1 X 10 per mm3 in a granulocytopenic recipient of one square meter body surface area.8 The one hour recovery of such transfused granulocytes is less than 5 per cent with a T3 of four to six hours.9 Because granulocyte counts in patients with chronic From the Medicine Branch, National Cancer Institute Bethesda, Md. First submitted June 28, 1968; accepted for publication September 27, 1968. C. DEAN BUCKNER, M.D.: Clinical Associate, Human Tumor Cell Biology Branch NC!; presently at U.S.P.H.S. Hospital, Seattle, Wash. ROBERT C. Gnw, JR., M.D.: Clinical As- sociate, Human Tumor Cell Biology Branch, NCI. ROBERT J. EI5EL. Medical Technician, Human Tumor Cell Biology Branch, NCI. EDWARD S. HENDERSON, M.D.: Head, Leukemia Service, Medicine Branch, NCI. SEYMOUR PERRY, M.D.: Associate Scientific Director for Clinical Trials, NC!. Reprint requests should be addressed to Dr. Seymour Perry, Bldg. 10, Rm. 6B17, National Cancer Institute, Bethesda, Md. 20014 #{176} Leukapheresis: The procedure of withdrawal of leukocytes from the Creek, Leuk = white + aph = away from + (h)airesis = taking. The elision of the initial h of hairesis leaves a single h in the compound word aphairesis which means a taking away or removal. This is a shorter version of leukocytopheresis.’ f The per cent recovery of transfused cells was determined by multiplying the post transfusion increment per ml. by the estimated blood volume and dividing by the number of cells infused. 353 For personal use only. on November 22, 2018. by guest www.bloodjournal.org From
Transcript of Leukapheresis* by Continuous Flow Centrifugation (CFC) in - Blood

Leukapheresis* by Continuous Flow Centrifugation (CFC)
in Patients with Chronic Myelocytic Leukemia (CML)
By DE� Bucic�, ROBERT G. Gii�w, JR., ROBERT J. EISEL,
EDWARD S. HENDERSON AND SEYMOUR PERRY
M ORTALITY associated with prolonged and severe pancytopenia, irres-
pective of etiology, is high. The magnitude of this problem has increased
with the use of intensive x-irradiation and potent chemotherapeutic agents
for the treatment of malignancies and for immunosuppression in recipients of
allografts. Infection is the major cause of death in patients with acute
leukemia2 since hemorrhage from thrombocytopenia can be controlled by
platelet and whole blood transfusions. Mortality from infection can be directly
related to the degree and duration of granulocytopenia.3 To decrease the
morbidity and mortality associated with granulocytopenia, three experimental
modes of therapy have been attempted: 1 ) patient isolation with antibiotic
suppression of endogenous flora,4 2) granulocyte replacement,57 and 3)
bone marrow transplantation.8
The procurement of leukocytes from normal individuals and maintenance
of granulocyte levels in aplastic recipients poses many problems which can be
related to the kinetic and sedimentation properties of granulocytes. Granulo-
cytes comprise only a small fraction of whole blood and their density overlaps
that of red blood cells (RBC’s). Granulocytes are, therefore, difficult to
separate and collect without significant contamination by RBC’s. It has been
shown that the leukocytes from 40 or more units of normal whole blood are
required to raise the peripheral blood granulocyte level by 1 X 10� per mm3
in a granulocytopenic recipient of one square meter body surface area.8 The
one hour recovery� of such transfused granulocytes is less than 5 per cent with
a T3� of four to six hours.9 Because granulocyte counts in patients with chronic
From the Medicine Branch, National Cancer Institute Bethesda, Md.First submitted June 28, 1968; accepted for publication September 27, 1968.
C. DEAN BUCKNER, M.D.: Clinical Associate, Human Tumor Cell Biology Branch NC!;presently at U.S.P.H.S. Hospital, Seattle, Wash. ROBERT C. Gn�w, JR., M.D.: Clinical As-
sociate, Human Tumor Cell Biology Branch, NCI. ROBERT J. EI5EL. Medical Technician,
Human Tumor Cell Biology Branch, NCI. EDWARD S. HENDERSON, M.D.: Head, Leukemia
Service, Medicine Branch, NCI. SEYMOUR PERRY, M.D.: Associate Scientific Director for
Clinical Trials, NC!.
Reprint requests should be addressed to Dr. Seymour Perry, Bldg. 10, Rm. 6B17, National
Cancer Institute, Bethesda, Md. 20014
#{176}Leukapheresis: The procedure of withdrawal of leukocytes from the Creek, Leuk =
white + aph = away from + (h)airesis = taking. The elision of the initial h of hairesisleaves a single h in the compound word aphairesis which means a taking away or removal.This is a shorter version of leukocytopheresis.’
f The per cent recovery of transfused cells was determined by multiplying the post
transfusion increment per ml. by the estimated blood volume and dividing by the number
of cells infused.
353
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

Fig. 1 .-NCI-IBM blood cell separator used in present studies.
354 BUCKNER ET AL.
myelocytic leukemia (CML) are often manyfold normal, several investigators
have used patients with CML as granulocyte donors.5’6 Schwarzenberg et al.5
and Freireich et al.6 have documented lysis of fever and clinical improvement
in granulocytopenic recipients associated with the transfusion of cells from
donors with CML. In addition, cells obtained from peripheral blood of patients
with CML appear to retain proliferative activity as demonstrated by myeloid’#{176}
and, rarely, erythroid grafts” that are obtained in a small but significant
number of recipients. Schwarzenberg et al. have also presented data consistent
with an antileukemic effect in recipients grafted with CML cells and which
they attributed to the “graft vs host” phenomenon.12
There are several centrifuges available for the separation and collection
of various components of the blood, but these have important disadvantages
and have not been widely employed.’3 The most notable of these is the
modified Cohn fractionator,14 which has been used by Bierman et al. in the
leukapheresis of human donors.”5 In an effort to facilitate the procurement
of large numbers of leukocytes, the National Cancer Institute and the Inter-
national Business Machines Corporation have jointly developed a continuous
flow centrifuge (NCI-IBM Blood Cell Separator) �1649 Studies in dogs utilizing
this centrifuge have demonstrated that large quantities of buffy coat cells
can be obtained without significant damage to leukocytes, platelets or RBC’s.’9
The present study was undertaken to establish the efficiency, safety, and
reliability of the continuous flow centrifuge technic utilizing donors with
CML.
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

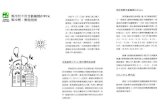
Fig. 2.-Diagrammatic cross section of centrifuge bowl.
MATERIAL AND METHODS
#{176}Filter from platelet recipient set, Fenwal Laboratories, Morton Crove, Illinois.
f Medical grade vinyl tubing, Becton, Dickinson and Company, Rutherford New Jersey.
LEUKAPHERESIS 355
TRANSPARENT TOP
FACE
� OUTER SHELL
INNER CORE-
Operation and Function of the NCI-IBM Blood Cell Separator (Figure 1)
The description of the blood cell separator and centrifugation technic used in theinitial animal studies has been published previously,19 and only the general principles
will be reviewed here. The instrument used in the work with human donors differs incertain respects and these will be discussed in greater detail. The essential components
of the Blood Cell Separator are the centrifuge bowl, the face seal, and the pumps. The
centrifuge bowl is composed of three separate parts made of polycarbonate (Fig. 2).
The rotating face seal is composed of two matching parts, a top half of stainless steelthat is stationary and a flat bottom half of ceramic that rotates with the centrifuge bowl.
The centrifuge bowl and tubing are primed with heparinized saline (one unit per
ml.) and all air is removed. A venous cannula is connected to the input line and whole
blood enters the centrifuge bowl via a stainless steel fitting on the upper half of theface seal after passing through a filter.#{176} A pressure-sensitive device, present on the
input line, automatically stops all pumps whenever venous obstruction or collapse occurs.
Blood then passes through the seal and downward through the center of the solidinner core, across the bottom and up the sides of the bowl into the flared portion at
the top. The process of separation occurs during the upward flow of blood with the
collection of RBC’s in the outer portion of the flared area, plasma in the central area,
and buffy coat cells at the plasma-RBC interface.
Three collecting ports in the transparent cover permit continuous collection from the
packed RBC layer, the plasma layer, and from the buff>’ coat layer at the plasma-RBC
interface. Separated components exit through the rotating face seal at a rate controlled
by individual peristaltic pumps. Red blood cells and platelet-rich plasma are recombined
so that buffy coat-poor blood is returned to the donor. If desired, the platelet-rich
plasma can be diverted to a separate bag, platelet concentrates prepared by routine
centrifugation technics, and the platelet poor plasma returned to the donor.A filter#{176} placed in the return line prevents clots from returning to the donor. The
filter also serves as an air trap and is connected to a weight sensitive device which
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

356 BUCKNER ET AL.
automatically stops the centrifuge pumps if air displaces 50 per cent of the blood in
the filter.The total volume of the bowl and tubing is 350 ml. By flushing the system with
saline at the end of a centrifugation all but 20 ml. of packed RBC’s can be returned
to the donor. Priming of the system with blood is not necessary.
Sterilization
The centrifuge bowl, seal and prefabricated tubing setst were sterilized with ethylene
oxide. The disassembled bowl and seal were precleaned by sonic vibration, exposed toa detergent solution for 12 hours followed by one hour of contact with peracetic acid,
then a thorough rinse in distilled water. The bowl was dried and reassembled prior to
final sterilization with ethylene oxide. Extensive testing has shown this procedure to be
effective in eliminating bacterial and pyrogen contamination.
Anticoagulation
Heparin, 1,000-3,000 units, was administered in a single IV injection immediately
after all tubing connections were made, and was infused continuously into the line
carrying whole blood to the centrifuge, at a rate sufficient to prolong the donor’s Lee
White clotting time to two to three times normal, as measured hourly from the venous
canula connected to the input line of the centrifuge. ( 50-75 units per minute).Clotting times prolonged greater than four times normal were routinely corrected by
the IV administration of protamine sulfate at the termination of the procedure. Buff>’
coat collections and platelet-rich plasma were collected in plastic bags#{176}containing 10
ml. and 35 ml. respectively of ACD NIH formula A.
Laboratory Methods and Calculations
Routine laboratory methods and calculations have been published elsewhere.’9 Blood
volume was estimated to be 2,500 ml. per m2 of body surface area.2#{176} The direct air-dry
technic of Tjio and Whang was used for chromosome studies of bone marrow aspirates.21
Donors
One female and 11 male patients with CML were utilized as donors (Table 1).Informed consents were obtained in all instances. The Philadelphia chromosome was
demonstrated in direct preparations of either bone marrow or peripheral blood in alldonors. Seven of the 12 patients were untreated during centrifugation and six remain
untreated to date. Three patients, CC., J.M., and J.H., who underwent single centrifuga-
tions, were receiving busulfan at the time of study. Two patients, W.C. and H.M.
received the drug between and following periods of centrifugation. Ferrous sulphate was
administered prophylactically to most donors, in addition to which, W.C., and H.M. received
a single blood tranfusion prior to the initial centrifugation.
Teflon cannulaef (13 or 15 gauge) were inserted into both antecubital veins of
the donor. Blood for separation was withdrawn from one vein which was connected
by vinyl tubing to the input line of the centrifuge. The contralateral vein was connected
to the output tubing and received the returning buff>’ coat-poor blood.
RESULTS
One hundred three centrifugations were attempted in 12 patients with CML.
Ninety-eight separate centrifugations were completed without major problems
and the results of these studies will be considered in detail. The remaining
five centrifugation attempts will be discussed separately. Table 1 shows
the details of centrifugation for each individual donor. Figure 3 presents the
#{176}Transfer packs, Fenwal Laboratories, Morton Grove, Illinois.f Becton, Dickinson and Company, Rutherford, New Jersey.
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

LEUKAPHERESIS 357
I ‘� �
0.,,� Ot-CC00’-�Lt)00CO©C)C’)’�’
-�CCC�50 t- CC CC C’) �4 © - t- 00 ci I
c’1Ci’,i�� ci-
� �OCC1.,�4tciciIt)�C00C’D1
o 00’� �‘ C’) - Ci )f) - C) I
�- I
�� #{176}.-I I� 0,.�I ICs �-I II �-. - � C’) C’) 1!) C’) C) If) �‘ CC ‘-4 I�E 0�I I#{231} F I�4 ‘�Ic� F-I I,.- �‘�I I01 �
z 0� 0QC)��� IE-Ci
�s�I �1I .S� I- ‘6EI I5� 0 I� � I��-ilf) C’)Ciz �C’) ,-4CS I
I � o#{243}ei � ‘-� i- ‘-� c’i in�4C’1C’) C’)C’)�-4 �-4I
01 I.� I
.‘�I’�l - -
�sI ICi
l0
Ic).I�’
�C0�
to
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

[ill
#{149}- ‘P’�*,’i,’f
C 0eciMc�’e C,00 5
I Ii EU1�PC(PESiS � I I I I Iii ill Ii 11111
358 BUCKNER ET AL.
�‘ � � �:�/�- �t\�
150 *8c
� 100
�b 75
50
25
C �0�JUNE��LY � ‘ AUGUST- � OCTOBER NOVEMB{� DECEMBER �‘ JANUARY ‘� FEBRUOPY
SEPTEMBER
Fig. 3.-Details of centrifugation and leukapheresis in patient C.L.
results of 11 months of intermittent CFC and conventional leukapheresis in
one donor.
Effects of the Procedure on Donors
All donors were in relatively good physical condition and most tolerated
the procedure well even when CFC was performed for many hours on several
consecutive days. All donors have been followed from one to six months
following centrifugation and no adverse effects have been noted.One donor developed chills and fever on two separate occasions. The first
episode occurred during his third study after one hour of centrifugation.
Tests for pyrogens and bacterial contamination were negative and the patient
subsequently developed signs and symptoms of an upper respiratory infection.
Five days later another centrifugation was attempted and discontinued after
one hour because of clotting within the tubing and centrifuge bowl. Immedi-
ately following this, a single unit conventional leukapheresis was performed.
Chills and fever developed during the return of his packed RBC’s; cultures
and pyrogen studies were again negative and he recovered fully. Repeat
centrifugation was not performed.
Results of Cell Separation and Collection
Leukocytes. Ninety-one centrifugations were performed at 500-600 r.p.m.
(20-25 g) yielding platelet-rich plasma that was returned to the donor in
84 instances and further processed to prepare platelet concentrates in seven
instances. The remaining seven centrifugations were performed at 650-950
r.p.m. (30-85 g). The results of buffy coat collection are shown in Table 2.
The efficiency of leukocyte separation and collection was variable from
patient to patient (Table 1) with median yields of 18-53 per cent. In each
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

LEUKAPHERESIS 359
Table 2.-CML Bully Coat Collections-98 Centrifugations
White BloodCells Granulocytes
MononuclearCells Platelets
Total Collected x 10” 2.4#{176} 1.5 0.9 1.2
(0.3-8.1 )f 0.1-3.4) (0.2-4.8) (0.02-10.0)
-BagCountsxlO3permm3 461.8 61% 39% 318.6and Differential (169.0-748.0) (28.1-80.0) (20.0-73.0) (51.0-1,000.0)
Yield % 39.3 34.5 47.5 8.2
(8.2-74.5) (7.1-63.4) (9.8-107.0) (0.1-46.0)
Number of Blood Volumes Cleared� 0.48 0.50 0.52 0.11 -
(0.1-0.9) (0.09-1.0)
Collection Volume (ml.)
(0.09-1.8) (0004-0.6)
490 (146-1316)R.B.C. (x 106 per mm3) 0.5 (0.1-1.0)
Time of Centrifugation (mm.) 180 (60-360)
R.P.M. 600 (450-950)Force (g) 30 (20-85)
Flow Rate (ml. per mm.) 40 (20-75)Total Volume Centrifuged 7.2 (2.4-20.3)No. B.V. Centrifuged 1.5 (0.4-3.2)
#{176}Median.fBrackets indicate range.� S Total cells collected
� Peripheral blood count per ml. at T0 x blood volume j
individual patient, however, cell separation was achieved with approximately
the same efficiency on repeated occasions. Leukocyte yields tended to be
lower in those patients with elevated platelet counts. A higher incidence of
platelet aggregation with resultant plugging of seal ports was observed in
patients with high initial platelet counts. In one patient, H.M., a reduction
of peripheral platelet counts from 700,000 to 250,000 per mm3 was followed
by an increase in median leukocyte yields from 27 to 45 per cent.
An attempt was made to compare the relative efficiency of CFC vs con-
ventional leukapheresis performed as described by Morse et al.22 for the
collection of CML leukocytes. In our laboratory, leukapheresis of one unit of
blood requires one hour and was compared to one hour of CFC. Donor C.L.
was subjected to leukaphereses of 34 units and to CFC of 143 hours (Table 1
and Figure 3). CFC yielded 0.8 X 1011 leukocytes per hour, while conven-
tional leukapheresis yielded 0.2 X 10” cells per hour. Peripheral WBC counts
were comparable during both procedures. An additional comparison was made
of a four unit conventional leukapheresis and four hours of CFC in the
same patient (Table 3). CFC yielded four times as many cells as conventional
leukapheresis in the same period of time.
In most instances it was impossible to collect buffy coat with a high con-
centration of mature granulocytes without RBC contamination (median RBC
count of 0.5 X l0� per ml. of bully coat). Attempts to reduce RBC con-
tamination resulted in buffy coat consisting predominantly of immature gran-
ulocytes and platelets.
Platelets. The number of platelets collected in the buffy coat increased
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

360 BUCKNER ET AL.
Table 3.-Efficiency of Leukocyte Collection in Donor CL.Comparison of CFC and Conventional Leukapheresis
TimePeripheral
WBCNo. WBC’s
Removed WBC YieldVolume of
Blood(Hours) (x 10’) (x l0�) (%) Processed
(L.)
Continuous 0-2 61.3 1.2 43 4.8
FlowCentrifugation 2-4 54.9 1.2 46 4.8
Total 4 2.4 9.6
Conventional 0-1 61.1 0.19 60 0.5
Leukapheresis1-2
2-33-4
-
-
65.3
0.13
0.160.16
40
5050
0.5
0.50.5
Total 4 0.64 2.0
with increasing peripheral counts while the per cent removed remained
relatively constant ( Table 4 ) . In most instances only a relatively small fraction
of the peripheral blood platelets were collected since platelet-rich plasma
was deliberately returned to the donor. However, platelet clumping within
the bowl and seal in patients with thrombocytosis prompted attempts to
increase the quantity of platelets collected. Platelets were removed by increas-
ing the g force in order to raise the platelet concentration in buffy coat,
or alternatively platelet-rich plasma was collected and platelet concentrates
obtained by conventional technics with return of platelet-poor plasma to the
donor (Table 5).
The preparation of platelet concentrates from ACD-platelet-rich plasma
proved the most efficient way to remove large quantities of platelets. Platelets
collected in buffy coat using higher g forces tended to clump irreversibly,
while the platelets obtained from platelet-rich plasma resuspend very easily.
In four instances platelet yields using the latter technic were greater than 50
per cent, despite cessation of platelet-rich plasma collection before termina-
tion of centrifugation. The number of platelets collected from platelet-rich
plasma was very large, up to 20 X 10”, which was equivalent to approximately
20 units of platelet concentrates. Transfusion of these platelets resulted in
satisfactory increments in thrombocytopenic patients.
Effects on Donor Peripheral Blood Elements
Red Blood Cells. Red blood cells were lost during CFC through contamina-
tion of the buffy coat layer (an average of 0.5 X l0� RBC’s per ml. of buffy
coat), in blood samples removed during centrifugation, and in the small
amount of residual blood remaining in the bowl and tubing at the completion
of centrifugation. The average total RBC loss per procedure was the equivalent
of 75-150 ml. of whole blood. Table 6 shows the median and ranges of donor
hematocrit changes for the total group. Hematocrit values declined one to
nine per cent following centrifugation in 70 of 98 studies: Patient C.L., who
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

LEUKAPHEBESIS 361
a C)
� ©CC� + � +� I� ‘-�
C’)If)
‘I’
0 0 0
0 C) C’)
�+0+
�� �C’ �
a.000
� �; If) if)
E �o
� C�.� �0
2
� J0 cB:�X C’)c� 00 �
� 0o - ..�
- -,0
.�
CS
a.� C’) If)
� C’) CC .;�i
� 0 5.
a.� .�
C0�.. ‘5 .�
0 0 a. 0g �C’) C’) �
� A V �
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

362 BUCKNER ET AL.
$ #{149}i�
00000000000000
S 0000iOOlf)if)©lf)0000if)na-. t- 0 if) C’) - CC t- 0 1- - C) CC t-
c3�� it) If) ‘1’ CC ‘�‘ if) ‘�4 C’) Ci C’) C’) Ci It)
E
1-.
00000000000000a4� o�oi#{244}ooino�o�ooo
if) if) C’) “1� CC If) t- If) 00 - if) 0 I’- 00:� B 00 CC It) If) t. 00 CC C’) � If) CC If) If)
CS..CS0
0
C)0 0 If C’) C’) 00 0 00 00 0 if)
0 �- - --- - - - CC If) CC I-
0a.0
0#{176}�#)Cs
� �-o � � C’) - C) - 0 ci -CS -a� Ci
-PC
..o--
Cs 0
� 0C’�f)CC0000’-4Ci1f)If)C’)�0 .�o -E4?
� .2
04
a4? � f)0�lf)If)00C’)0if)if)if)if)It)
0 C’)�’If)00C’)lf)C’)CiCic1CiCiCiCi.� �a
1f S
4? 0
2Cs
x
� 00000000000000n� 000 t)Oit)1f)1f)000000� N000)C)t-OOCCif)lf)CCCCCCCCCC �,
.�
00
C.2 0000If)I250000If)000
“0 Cs0--�E-’�--- Ci� t)CCt-00C)0ciC’)’�’ �
-----
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

LEUKAPHERESIS 363
Table 6.-Peripheral Blood Counts in CML DonorsBefore and After Centrifugation
WBC Platelets Hematocrit(xl0’) (xlO’) Vol.
(%)
Pre 85.5 *
(31.7-449.0)f
151.0
(73.0-960.0)
35.0
(23.0-47.0)
-Post 70.5
(31.1-354.0)
140.0
(68.0-800.0)
33.0
(22.0-45.0)
Change -13.6(-204.0--+8.0)
-27.0
(-400.0--+195.0)
-2.0
(-9.0-+4.0)
(%) Change -16.5
(-45.0-+1.0)-19.0
(-53.0-+69.0)
-5.0
(-22.0-+9.0)
* Median.I Brackets indicate range.
under�vent periods of intensive CFC and conventional leukapheresis, had
resultant hematocrit decrements of as much as six per cent associated with
an increase in reticulocytes of more than five per cent ( Figure 3).White Blood Cells. Peripheral WBC counts decreased in all but five in-
stances following centrifugation ( Table 6 ) . Decrements were generally in
proportion to the number of cells removed. In most patients whose peripheral
counts were followed, two to three days were required for the �S1BC counts
to return to baseline level. Patient CL. demonstrated ( Table 1 and Fig. 2)
the typical response to cell removal, although some patients had a more pro-
longed delay in return to baseline.
Platelets. The peripheral platelet count fell on an average of 27,000 per mm3
following centrifugation (Table 6). The per cent decline and fraction of
platelets removed was similar for all patients, and thus absolute platelet
decrements were greatest in those patients with the highest platelet counts.
The median per cent decrease in peripheral platelet counts following centri-
fugations was 19 ( Table 6) , while the estimated median per cent of original
circulating platelets removed was 11 ( Table 2 ) . The per cent decrease in
peripheral platelet count was greater than predicted in 50 of the 98 centrifuga-
tions, suggesting that in these instances, platelets were also lost from the
circulation by a mechanism other than external collection.
Plasma Protein. Protein losses occurred as result of plasma removal during
buffy coat collections, which averaged approximately 400 ml. per centrifuga-
tion. Patients who underwent several consecutive days of centrifugation had
decreases in albumin and globulin levels, but single centrifugations rarely
produced changes. Figure 3 shows the changes in albumin and globulin levels
in patient CL. who underwent the largest number of centrifugations.
Viability of Cells Collected and Recipient Data
Leukocytes collected by CFC from patients with CML appeared viable
both by phase and light microscopy and retained the ability to ingest latex
particles. Following these preliminary observations, CML leukocytes procured
by CFC were transfused on 109 separate occasions into 21 patients with
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

Table 7.-Details of Transfusion Studies in 22 Recipientsof CML Cells Procured by CFC
Recipient
-i-i M.D.
Diagnosis
CML
Total
No. ofLeukocytes
InfusedTransfusion ( x lOU) Bone Marrow Genetics f
Transfusion *Period( days)
5 5 8.5 Ph’ chromosome present
6 3 7.0 prior to transfusion
2.
3.
H.P.
J.Bl.
ALL
AML
217
5
275
1.6
12.1
9.0
+ days 6 and 13
+ days 4 and 14+ day 20
4. AR. AML 5 3 6.8 - day 11
5. S.S. ALL 14 3 7.8 - day and 8
6. MR. AML 20 5 15.0 day 5
7. A.O. AML 7 3 4.7 Unsatisfactory study
8. MO. AML 7 3 3.6 + day 4, - day 109. H.M. AML 11 2 4.5 Unsatisfactory study
10. W.G. AML 30 7 10.7 + day 6
11. H.Rr. ALL 10 4 8.3 No study
12. J.B. ALL 15 3 3.1 + days 1 and 313. R.C. AML 16
132
53.0
6.9
No study
14. P.C. ALL 118
34
6.07.5
No studyNo study
15. J.P. Aplastic
anemia
13 4 4.8 - days 10 and 24
16. M.G. ALL 2 2 2.2 No study
17. T.G. AML 5 5 11.0 - day 6
18. W.T. AML 7 4 7.0 - day 6
19. J.S. ALL 115
111
1.29.2
+ day 5+day3,-day5
20. C.S. AML 2 2 1.8 No study
21. D.C. ALL 21 9 19.4 +days2,4,and722. R.A. AML 1 1 1.3 No study
0 Number of days encompassed by transfusions; instances
elapsed between transfusions were considered separate periods.
t Results of studies for presence of Ph’ chromosome derived from donor. ( + ) indicates
presence and (-) indicates absence of Phi chromosome. The number of days followingthe last transfusion is indicated.
where more than 30 days
364 BUCKNER ET AL.
leukemia and one patient with aplastic anemia. Donor and recipient pairs
were matched for major RBC antigens in most instances, but some trans-
fusions were performed despite major incompatibilities when no red cell
compatible donors were available for patients with life threatening sepsis, and
in these cases the buffy coat was usually sedimented with high molecular
weight dextran to reduce RBC contamination. The majority of the recipients
regardless of compatibility experienced a sharp rise in fever and/or chilling
shortly following the leukocyte infusions which readily responded to aspirin
and Benadryl#{174}. This fever-chill response was seen with RBC consanguineous
transfusions as well as with the dextran-sedimented leukocytes. Recipients
were given 1.2-19.4 X 10� CML leukocytes over varying periods of time
( Table 7 ) . Most transfusions resulted in an increase in the leukocyte and
granulocyte counts of the recipients. Table 7 shows the cells infused and the
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

LEUKAPHEBESIS 365
one hour increments obtained following 40 transfusions into 16 recipients with
pretransfusion granulocyte counts of less than 1,000 per mm3 ( median of
300 per mm3 ) . The remaining recipients had granulocyte counts of 1,000 per
mm3 or greater, and in these, leukocyte increments and recoveries were signifi-
cantly higher.
In eight of the 22 recipients, donor cells were identified by cytogenetic
studies of bone marrow three days or longer following the last transfusion
( Table 7 ) . In general, these patients were not followed for sufficient length
of time to permit any conclusion concerning a possible leukocyte graft.
Technical Problems
Five of the 103 attempted centrifugations were technical failures. Two
studies were terminated due to extensive clotting in the centrifuge bowl and
tubing during the first hour of centrifugation. In two studies, venous flow
was inadequate to permit satisfactory centrifugation. One leukapheresis was
stopped when the donor developed chills and fever after one hour of centri-
fugation ( described above ) . In approximately 25 per cent of the remaining
98 centrifugations, there were additional technical problems which either
shortened centrifugation time or decreased the efficiency of separation. These
included clotting within the input needle with embolization into the seal
and bowl, and platelet clumping within the extracorporeal system, particularly
in the seal. The former was corrected by placing a filter on the input line;
the latter was most common in patients with thrombocytosis and was mm-
imized by intentionally lowering the peripheral platelet counts.
Long-Term Intermittent CFC
One donor will be presented in detail since he underwent the greatest
number of centrifugations over the longest period of time.
Donor C. L. was a 72-year-old white male referred to the National Cancer Institute inAugust of 1965. Bone marrow and peripheral blood examination confirmed the diagnosisAugust of 1965. Bone marrow and peripheral blood examination confirmed the diagnosis
of CML, Ph’ positive. On admission his WBC count was 402,000 per mm3, platelet
count 205,000 per mm3, and hemoglobin 11.0 Gm. per cent. He was treated with
busulfan, 4-12 mg. per day from August to November, 1965, and on one occasionreceived 50 r of x-irradiation to his spleen. At this time he was subjected to conventional
leukapheresis on many occasions with removal of buffy coat cells from 21 units ofwhole blood. In November of 1965, busulfan was discontinued when the WBC countwas 8,500 per mm3, platelet count 80-100,000 per mm3 and hematocrit 41 volumesper cent. No further chemotherapy was given and from November of 1965 to June of1967 the WBC count rose to levels of 60-90,000 per mm3, and platelets stabilized at
100-124,000 per mm3. The present study began in June of 1967. Details of leulcapheresisand CFC and the effects of these procedures on the peripheral blood cell counts andplasma protein levels are shown in Figure 3 and Table 1. There was no change in the
patient’s clinical condition, spleen size or bone marrow status during the period of study.
DIscussIoN
Previous studies in the dog have demonstrated that the NCI-IBM Blood
Cell Separator is a safe and reliable instrument for the collection of bully
coat cells by CFC.19 The effects of centrifugation on the various cellular
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

366 BUCKNER ET AL.
components were evaluated in detail by a variety of technics and indicated
that there was little or no effect on the survival or viability of RBC’s, lympho-
cytes, and granulocytes during prolonged centrifugation. Platelets appeared
to be the most easily damaged, but this could be minimized by centrifugation
at low g forces which returned platelet-rich plasma to the donor.
The results of the present study in patients with CML is consistent with
previous experience in dogs and man.16’#{176} The paucity of problems encoun-
tered in this series of 103 centrifugations in 12 patients attests to the safety
of the technic. One patient developed chills and fever after one hour of
CFC, but also developed the same symptoms while undergoing conventional
leukapheresis. The cause of this episode was never established although it
was assumed to be a pyrogen reaction. Visual increases in plasma hemoglobin
levels were not observed and donor hematocrit levels did not decrease out
of proportion to the quantity of RBC’s removed by this procedure.
It has been previously demonstrated that platelets were damaged and
lost from the circulation during CFC and that this loss increased with
increasing g forces.’#{176} The present studies tended to substantiate these observa-
tions. Thrombocytopenia was not a problem following CFC despite the proc-
essing of more than one blood volume per centrifugation. However, 50 per
cent of the centrifugations were followed by decreases in platelet counts in
excess of what would have been predicted by the number of platelets collected.
The difference between the expected and observed decreases in platelets were
greater in those patients with high platelet counts ( Table 4) . This small
loss of platelets can probably be explained by mechanical trauma resulting
in platelet clumping with subsequent sequestration of platelets in vivo. The
fact that donors with high platelet counts had a greater discrepancy between
predicted and observed values correlates with observed platelet clumping
within the extracorporeal system. Platelet clumping with consequent plugging
of ports in the seal and bowl was considered to be responsible also for the
poor leukocyte yields obtained in donors with thrombocytosis. This was sub-
stantiated by a significant improvement in leukocyte yields in one patient
following a decrease in platelet count.
Viability of the cells collected was shown by the increments in leukocyte
counts produced in granulocytopenic recipients after buffy coat transfusions.
The average per cent recovery per m2 body surface and increase in leukocyte
counts were almost identical to that obtained with CML leukocytes procured
by conventional technics.1#{176} Further evidence of cell viability was demon-
strated by the persistence of Ph’ chromosomes in bone marrow of recipients
following transfusion.
An attempt was made to compare the efficiency of CFC with conventional
leukapheresis technics. In a single donor, C.L., who had a peripheral WBC
count of 50-125,000 per mm3, the efficiency of CFC was four times that of
conventional leukapheresis. The group of patients who underwent CFC was
compared to the 10 patients who were subjected to conventional leukapheresis
and reported by Morse et al.22 In their 10 patients who had a median peri-
pheral WBC count of 200,000 per mm3, they were able to obtain a median
of 0.3 X 1011 leukocytes per unit of blood. In the present study, the patients
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

LEUKAPHERESLS 367
had a median WBC count of 85,000 per mm3 and 0.8 X 10�� leukocytes
per hour were obtained by CFC.
For practical purposes, conventional leukapheresis is satisfactory in those
donors with WBC counts greater than 100,000 per mm3, but sufficient cells
( 1-2 x 10” ) cannot be obtained easily by this technic from donors with
lower \VBC counts. For example, four hours of CFC yielded 2.4 X �
leukocytes in a donor with a peripheral WBC count of 50-60,000 per mm3
( Table 3 ) . In this same donor it would have been necessary to process
approximately 15 units of blood by conventional technics to obtain this quantity
of cells.
Previous studies in dogs have demonstrated that with this technic it is
possible to separate and collect large quantities of leukocytes from animals
with normal peripheral blood cell counts. Both the previous and present
study indicate that it, in common with all other available technics, in both
normal and CML donors, RBC contamination of the huffy coat is unavoidable.
However, CFC appears to be the best available technic for granulocyte
collections from CML donors with relatively low WBC counts. Studies
are now in progress to evaluate this technic in normal donors.
SUMMARY
A closed continuous flow centrifuge ( Nd-IBM Blood Cell Separator ) was
utilized to collect large quantities of leukocytes from donors with chronic
myelocytic leukemia. Ninety-eight separate centrifugations of one to six hours
duration were performed in 12 patients. Quantities of blood between 2.4-20.3
liters were processed during each centrifugation representing 0.4-3.2 donor
blood volumes. An additional five centrifugations were attempted unsuccess-
fully. Buffy coat cells were collected while plasma and red blood cells were
returned to the donor without change in flow or gravitational field. White
blood cell yields of up to 75 per cent were obtained while platelet yields
were electively varied from 0.1 per cent in donors with thrombocytopenia
to 61.0 per cent in donors with thrombocytosis.
Red blood cell hemolysis and excessive platelet losses with thrombocyto-
penia were not observed. One patient developed chills and fever of unknown
etiology on two separate occasions, once during and once following CFC
Leukocytes collected by this method and transfused into granulocytopenic
recipients resulted in granulocyte increments of 2.0 X 10� per mm3 per
1011 granulocytes per m2 of body surface area. The persistence of cells with
the Ph’ chromosome in the bone marrow of recipients demonstrated that
viable proliferating cells survived the procedure.
SUMMARIO IN INTERLINGUA
Un claudite machina centrifuge a fiuxo continue (le hemocytoseparator NCI-IBM)
esseva utilisate pro colliger grande quantitates de leucocytos ab donatores con chronic
leucemia myelocytic. Un total de 98 separate centrifugationes de un duration de inter une sex horas esseva effectuate in 12 patientes. Quantitates de sanguine de inter 2,4 e 20,3 L
esseva processate durante cata centrifugation, representante inter 0,4 e 3,2 total voluminessanguinee de donator. Cinque centrifugationes additional esseva tentate sin successo.Cellulas a coagulo blanc esseva colligite durante que le plasma e le erythrocytos essevaretornate al donator sin alteration in fluxo o campo gravitational. Rendimentos leucocytic
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

368 BUCKNER ET AL.
de usque a 75 pro cento esseva obtenite, durante que le rendimento de plachettas essevavariate electivemente inter 0,1 pro cento in donatores con thrombocytopenia e 61,0 pro
cento in donatores con thrombocytosis.
Hemolyse erythrocytic e excessive perditas de plachettas in casos de thrombocytopenianon esseva observate. Un del patientes disveloppava algor e febre de incognite etiologiain duo separate occasiones, un vice durante e un vice post le procedimento.
Leucocytos colligite per iste methodo e transfusionate ad in recipientes granulocytopenicresultava in augmentos de granulocytos de 2,0 X 10� per mm3 per 10’� granulocytos
per m2 de area de superfice corporee. Le persistentia de cellulas con chromosoma Ph’ inle medulla ossee de recipientes demonstrava que viabile cellulas proliferante supervivevale intervention.
ACKNOWLEDGMENTS
We are indebted to Mrs. Coralyn Jones for her assistance throughout these studies, to
Dr. Jacqueline Whang-Peng and Mrs. Turid Knutsen for performing the cytogeneticstudies, to Dr. Ronald A. Yankee for his advice and help in carrying out these studies, to
Mrs. Regina Dowling for performing the conventional leukapheresis studies and to Mr.George Judson and the staff of the Systems Development Division of IBM for engineering
support.
REFERENCES
1. Bierman, H. R., Marshall, C. J., Kelly,K. H., and Byron, R. L. : Leukapheresis in
man. III. Hematologic observations in pa-tients with leukemia and myeloid meta-plasia. Blood 21: 164, 1963.
2. Hersh, E. M., Bodey, C. P., Nies, B.A., and Freireich, E. J. : Causes of death
in acute leukemia. J.A.M.A. 193:105, 1965.3. Bodey, G. P., Buckley, M., Sathe, Y.
S., and Freireich, E. J.: Quantitative rela-tionships between circulating leukocytesand infection in patients with acute leu-
kemia. Ann. Intern. Med. 64:328, 1966.4. Levitan, A. A., and Perry, S.: The
use of an isolator system in cancer chemo-
therapy. Amer. J. Med. 44:234, 1968.5. Schwarzenberg, L., Mathe, C., De
Crouchy, J., Dc Nava, C., Vries, M. J.,Amiel, J. L., Cattan, A., Schneider, M.,and Schlumberger, J. R.: White blood celltransfusions. Israel J. Med. Sci. 1:925, 1965.
6. Freireich, E. J., Levin, R. H., Whang,
J., Carbone, P. P., Bronson, W., and Morse,
E. E.: The function and fate of trans-
fused leukocytes from donors with chronicmyelocytic leukemia in leukopenic recipi-ents. Ann. N.Y. Acad. Sci. 113:1081, 1964.
7. Eschbach, J. W., Epstein, R. B.,
Burnell, J. M., and Thomas, E. D.: Phys-iologic observations in human cross circu-
lation. New Eng. J. Med. 273:997, 1965.
8. Thomas, E. D., and Epstein, R. B.:Bone marrow transplantation in acute leu-kemia. Cancer Res. 25:1521, 1965.
9. Yankee, R. A., Freireich, E. J., Car-bone, P. P., and Frei, E., III: Replacement
therapy using normal and chronic mye-logenous leukemia leukocytes. Blood 24:844
1964.10. Levin, R. H., Whang, J., Tjio, J. H.,
Carbone, P. P., Frei, E., III, and Freireich,E. J. : Persistent mitosis of transfused homol-ogous leukocytes in children receiving anti-
leukemic therapy. Science 142: 1305, 1963.
11. Levin, R. H., Whang, J., Carbone,P. P., and Freireich, E. J.: Erythroid ho-mograft following leukocyte transfusion ina patient with acute leukemia. I. Clinicalstudies and implications. Blood 26:587,
1965.12. Schwarzenberg, L., Mathe, C., Amiel,
J. L., Cattan, A., Schneider, M., andSchlumberger, J. R.: Study of factors de-
termining the usefulness and complications
of leukocyte transfusions. Amer. J. Med. 43:206, 1967.
13. Judson, C., Jones, A., Kellogg, R.,
Buckner, D., Eisel, R., Perry, S., and Green-ough, W.: Closed continuous-flow centri-fuge. Nature 217:816, 1968.
14. Tullis, J. L., Tinch, R. J., Gibson, J.C., II, and Baudanza, P.: A simplified cen-
trifuge for the separation and processing
of blood cells. Transfusion 7:232, 1967.15. Kelly, K. H., and Bierman, H. B.:
The continuous flow separation of leuko-cytes from human blood. Amer. J. Med. Sci.240:483, 1960.
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

LEUKAPHERESIS 369
16. Freireich, E. J., Judson, C., and Levin,R. H.: Separation and collection of leuko-
cytes. Cancer Res. 25:1516, 1965.17. Perry, S., Judson, C., and Vogel, J.:
Studies with the NCI-IBM cell separator.
Exper. Hem. 9:38, 1966.18. Vogel, J. M., Buckner, C. D., and
Perry, S.: Continuous flow cell separation.
Conference on Plasmapheresis, XXth Sci-entific Meeting of Protein Foundation, Inc.,April, 1966.
19. Buckner, D., Eisel, R., and Perry, S.:
Blood cell separation in the dog by con-
tinuous flow centrifugation. Blood 31:653,1968.
20. Baker, B. J., Kozoll, D. D., andMeyer, K. A.: The use of surface area asa basis for establishing normal blood volume.Surg. Gynec. Obstet. 104:183, 1957.
21. Tjio, J. H., and Whang, J.: Chromo-some preparations of bone marrow cellswithout prior in vitro culture or in vivocolchicine administration. Stain Techn. 37:
17, 1962.22. Morse, E. E., Carbone, P. P., Frei-
reich, E. J., Bronson, \V., and Kliman, A.:
Repeated leukapheresis of patients withchronic myelocytic leukemia. Transfusion
6:175, 1966.
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom

1969 33: 353-369
SEYMOUR PERRYDEAN BUCKNER, ROBERT G. GRAW, JR., ROBERT J. EISEL, EDWARD S. HENDERSON and Chronic Myelocytic Leukemia (CML)
by Continuous Flow Centrifugation (CFC) in Patients with*Leukapheresis
http://www.bloodjournal.org/content/33/2/353.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on November 22, 2018. by guest www.bloodjournal.orgFrom